
Krebsfrüherkennung in Deutschland 2014. Evidenz aktueller ...

Evidenz-Tabelle Literatur Bauchlage
Referenz
Nr.1
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
Abroug et al Intensive Care Med (2008)34:1002-1011 The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: a meta-analysis.
Metaanalyse 6 Studien 1372 Patienten
Prospektive RCT, alle Patienten hatten ALI /ARDS, mit bilateralen Infiltraten, Ausschluss Pulmonale Hypertonie, Horrowitz<300,
Bauch/Rückenlage innerhalb von 24h
5 Studien: Mortalität & Horrowitz
4 Studien VAP Inzidenz
3 Studien ICU Aufenthaltsdauer
BL versus Rückenlage
28 Tage -Mortalität (Prim. EP)
Horrowitz
VAP Inzidenz
Komplikationen
ICU Verweildauer
Kein Signifikanter Effekt , -3% (OR 0,97,95% Confidence Intervall)
Signifikanter Anstieg durch BL 25mmHg P=0,00001
Nicht signifikante Reduktion, 23%, p=0,09
Keine vermehrten Atemwegskompl. (OR 1,01)
Nicht signifikant erhöht, 0,96 d
Große Variation: BL für 7-17h, für 4 d bis zum gesamten Aufenthalt
Pro Arm
713 BL 659 RL
Zusammenfassende Beurteilung: QE 1a****
Bauchlage ist nicht assoziiert mit einer Verminderung der Mortalität, obwohl der horrowitzindex signifikant ansteigt unter Bauchlage.
Bauchlage ist sicher und verringert tendenziell die VAP-Inzidenz. Problematisch ist die Heterogenität der Studien, so dass großangelegte Studien zur Festlegung der optimalen Bauchlagen-Dauer und Beatmungsstrategie notwendig sind. Alle Studien waren unterpowert.

Referenz
Nr.2
Studientyp Teilnehmer (Anzahl und Charakteristika)
Kontrolle Hauptergebnis Bemerkung
insgesamt Abroug et al Critical Care 2011 An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury
study-level meta-analysis
7 RCTs that compared ventilation of adult patients with ALI/ARDS in prone versus supine position were included in this study-level meta-analysis. Analysis was made by a random-effects model. The effect size on intensive care unit (ICU) mortality was computed in the overall included studies and in two subgroups of studies: those that included all ALI or hypoxemic patients, and those that restricted inclusion to only ARDS patients. A relationship between studies’ effect size and daily prone duration was sought with meta-regression. They also
computed the effects of prone positioning on major adverse airway complications
1675 adult patients
The effects of prone positioning differed according to the type of study. Overall, prone ventilation did not reduce ICU mortality (odds ratio = 0.91, 95% confidence interval = 0.75 to 1.2; P = 0.39), but it significantly reduced the ICU mortality in the four recent studies that enrolled only patients with ARDS (odds ratio = 0.71; 95% confidence interval = 0.5 to 0.99; P = 0.048; number needed to treat = 11). Metaregression on all studies disclosed only a trend to explain effect variation by prone duration (P = 0.06). Prone positioning was not associated with a statistical increase in major airway complications.
Pro Arm
862 in prone position
Zusammenfassende Beurteilung: QE 1a****
Long duration of ventilation in prone position significantly reduces ICU mortality when only ARDS patients are considered.

Referenz
Nr.3
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(
n)
Haupt-ergebnis Bemerkung
insgesamt Allen Gillmann B. and Parsons Polly Curr Opin Anaesthesiology 2005 18:209-215 Acute lung injury:significance, outcome and treatment
Review Verbesserung der Oxygenierung
Geringere VAP Inzidenz
Kein Überlebensvorteil
Höhere Rate an Komplikationen
Genannte Studien von 2004Guerin et al JAMA und Gattinoni et al 2001 N Engl. J Med
Pro Arm
Zusammenfassende Beurteilung: QE 4**

Referenz
Nr.4
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Inter-
Vent.
Kontr. Zielgröße Hauptergebnis
insgesamt Alsaghir A. et. al. Crit. Care Med 2008 Vol36, No 2 Effect of prone positioning in patients with acute respiratory distress syndrome: A meta-analysis
Metaanalyse
RCT ≥ 6h Bauchlage
Nicht verblindet
5 RCT, 1316 Patienten
≥6h Bauchlage vs. Rückenlage bei Erwachsenen mit ARDS
39-780 Patienten, Baseline-Charakteristiken waren nicht signifikant unterschliedlich.
Bei Guerin et al wurden 11 Patienten ausgeschlossen
Bei Mancebo et al wurden 6 Patienten ausgeschlossen
BL RL Mortalität
Oxygenierung
Beatmungstage
VAP-Inzidenz
3 Studien untersuchten ICU Mortalität Kein signifikanter Unterschied.
(OR 0,79, 95% CI, 0,45-1,39)
3 Studien untersuchten 28-d Mortalität Kein signifikanter Unterschied (OR 0,95, 95% CI 0,71-1,28)
4 Studien untersuchten 90-d Mortalität Kein signifikanter Unterschied (OR 0,99, 95% CI 0,77-1,27)
Subgruppemanalyse SAPS II>50: Signifikante Abnahme der Mortalität (OR 0,29, 95% CI 0,12-0,70)
Signifikante Verbesserung in Bauchlage in der frühen Phase WMD 51,5 (CI95%, 6,95-96,05), in der mittleren Phase WMD 43,87 (CI95%, 13,86-73,88) und in der späten Phase WMD 24,89 (CI95%, 15,3-34,48)
2 Studien kein signifikanter Unterschied zwischen BL und RL bzgl. Beatmungsdauer
3 Studien Kein signifikanter Unterschied
Pro Arm
Zusammenfassende Beurteilung: QE 1a****
Bauchlage verbessert die Oxygenierung bei ARDS Patienten hat aber keinen Einfluss auf die Mortalität der Patienten, ausser eventuell bei Patienten mit höherer Erkrankungsschwere.
Kritikpunkte: 2 Studien vorläufig gestoppt wegen Finanzierungsproblemen und fehlender Motivation. 2 Studien hatten eine zu kleine Patientenpopulation. Eine Studie erlaubte croos over von RL nach BL obwohl sie eine intention to treat analyse durchführten. In 2 Studien wurde mit zu hohen TV beatmet, da die ARDSnet Studie noch nicht publiziert wurde.

Referenz
Nr.5
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Anca-Oana et al. Haemodynamic impact of prone position for acute respiratory distress syndrome in cardiac intensive care Nur Poster, als Word Datei verfügbar.
Retrospective study 43 ARDS patients ventilated in the prone position at some stage between Jan 2000 and Dec 2009. Demographic data, diagnostic interventions and complications were recorded
Parameters registered for 12 hour periods before, during and after PP were: PaO 2, oxygenation index (PaO 2 /FiO 2 ), PaCO 2 , haemodynamic data (mean arterial pressure (MAP), systolic arterial pressure (SAP), central venous pressure (CVP), systolic pulmonary artery pressure (PAP), pulmonary capillary wedge pressure (PCWP), cardiac output (CO), cardiac index (CI), systemic vascular resistance (SVR) and pulmonary vascular resistance (PVR).
43 patients (21 male, 22 female, mean age 57±15 yr) were ventilated in PP for a mean duration of 11.5±3.7 days (range 5-20). There were 37 (86%) cardiac surgical patients, 27 (62.7%) with drainage tubes, 6 (34.8%) had simultaneous IABP, renal replacement therapy (CRRT) and chest drainage. During PP there was an insignificant variation of SAP (±5%), PAP (±7%), CI (±6%), CVP (±17%), PCWP (±12%) compared to the period before PP. After PP there was an insignificant variation of SAP (±2%), PAP (±3%), CI (±8%), CVP (±14%), PCWP (±10%) compared to the period before PP. The in-hospital mortality in our group was 49.5%
Pro Arm
Zusammenfassende Beurteilung: QE 3 **(*)
The results suggest that PP has a minor impact upon haemodynamic parameters in cardiac intensive care. The poor outcome was related with the severity of illness and number of organ
failure.

Referenz
Nr.6
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kont Hauptergebnis
insgesamt Andersen et al. Acta Anaesth Scand. Does rotation of the head during surgery in the prone position affect the oxygen saturation in the frontal lobes? A prospective controlled study Nur Poster, als Word Datei verfügbar.
Controlled observational study
48 patients with a median age 59.5 yrs (range 26-79) were analyzed. Patients without symptoms from the neck or stenosis of vessels in the neck could be included.
One NIRS sensor was attached to each side of the forehead. The pads were connected to an INVOS oximeter. A series of measurements were carried out during anaesthesia (steady state) with the head placed 1) in the neutral position (baseline), rotated to the left, rotated to the right, and again placed in the neutral position (control). Each of the four series consisted of three measurements: one with the head resting on the head support, one during head lift (to relieve the pressure on the tissue below the sensor(s)), and one again with the head resting on the head support. To simulate a "normal" situation without pressure on the tissue below the sensors, the measurements during head lift were used for comparisons between the neutral and the rotated positions.
For neither of the sensors a statistically significant difference was found. However, in a few patients a reduction greater than 10 units of rScto2 was registered. There was no correlation between age and the size of the difference. When the head was lifted from the head support the rScto2 generally was measured higher, but with a great variability between patients.
Pro Arm
Zusammenfassende Beurteilung: No statistically significant difference was found in rScto2 between the neutral and the rotated positions. In a few patients, however, a considerable difference was registered, which may be a concern when placing the patients with the head turned to the side. We suggest that if NIRS measurements are to be used, the head of the patient should be lifted for a short while to reveal the influence on the measurement from the compressed tissues below the sensors.

Referenz
Nr.7
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis Bemerkung
insgesamt Aufmkolk et al., Eur J Trauma 2005;31:33-8 Effect of Prone Position on Lung Surfactant Composition and Function in Multiple Trauma Patients with Respiratory Dysfunction
Prospective, randomisiert
18 Trauma Patienten ISS>17, Abbreviated Injury Scale Chest >3, primary admission, Horrowitz>300mmHg <24h oder <200mmHg <8h within 14d after trauma
Bbendet wenn Horrowith >300mmHg >24h
Messung von Phospholipiden, Surfactant Protein A und Surfactant Funktion BAL an Tag 0,1,2,5,14
1Pat in each group worst case
1 Pat in each group died
BL 8h bis max 24h/dund Messung von von Phospholipiden, surfactant protein A und surfactant functionin BAL an Tag 0,1,2,5,14
Horrowitz-Index
ARDS rate
MOV
Sepsis rate
Duration of ventilation
Phospholipids and surfactant
No difference during the whole observational period
All patients developed pulmonary failure.
ARDS rate significant higher in the prone group p=0,05
MOV was higher in prone group (p=0,29)
Sepsis was more frequent in prone group (p=0,01)
One patient in each group was deemed as worst case, one patient in each group died of MOV
Duration of ventilation was significant longer in prone group p=0,03
No significant difference for the total phospholipids. The amount decreases In the prone group and an increase in supine group with max at day 2.
Nor difference in surfactant function
Pro Arm
Supine n=9 Prone n=9
Zusammenfassende Beurteilung: QE 3**
Body position has no influence on surfactant composition and function and Horrowitz-Index.
Fragwürdiges Studiendesign, Zielparameter

Referenz
Nr.8
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt Bajwa et al. J Intensive care Med 2010 25:121 Automated prone positioning and axial rotation in critically ill, nontrauma patients with ARDS
Retrospektive Studie 17 ARDS Patienten
Automatisierte Lagerung mit Bauchlage und axialer Rotation im Kinetic Therapie Bett
4-5 Stunden Lagerung mit 1-2 Stunden Rückenlage zwischen den Lagerungsintervallen
11° OK Hochlage in der Bauchlage
40°Rotation zu jeder Seite
Verhältnis BL:RL wurde individuell bestimmt
Dokumentation von demografischen Daten, APACHE 2 Score, SOFA Score, Beatmungs-MODE in BL, BGA 30Min nach BL zur Bestimmung des Horrowitz-Index
Braden Score und Dokumentation von Hautläsionen
11 Pat. starben Mortalität 65%
BL und axiale Rotation
keine Bei 16 von 17 Pat.
In BL und RotationVerbesserung des Horrowitz-Index 89±33 zu 224±92 (p<0,001)
Keine signifikante Reduktion von CO2 oder Mean Airway Pressure in BL
Nicht-signifikanter Trend der CO2 Reduktion bei extrapulmonaler ARDS Ursache
(p= 0,0899)
Trend von vermehrtem Überleben bei Patienten mit erhöhter CO2 Elimination in BL
Keine signifikante Änderung des SOFA Score
Mediane Lagerungsdauer 6d
Beatmungsdauer 16d, ICU Liegedauer 22d Braden-Score von 14±2 auf 10±2
Alle Pat. entwickelten konjunktivale Ödeme, die meisten entwickelten Druckulcera
Keine accidentiellen Dislozierungen von Tubus oder Katheter
Pro Arm
Die meisten Pat. waren weiblich, häufigste Diagnose Sepsis, gefolgt von Pneumonie, meist PCV Beatmung, APACHE Score 30±9.
Alle Horrowitz<200
Zusammenfassende Beurteilung: QE 3**
Automatisierte axiale Rotationstherapie mit einem Spezialbett resultiert in einem hoch signifikanten Anstieg der Oxygenierung ohne lebensbedrohliche Komplikationen in nichttraumatisierten ARDS Patienten.

Referenz
Nr.9
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Hauptergebnis Bemerkung
insgesamt Ball Ch. J. Trauma Volume 68, Number 4, April 2010 Intra-abdominal Hypertension, Prone Ventilation, and Abdominal Suspension
Fallbericht 1 Patientin mit Adipositas per magna, akutes Abdomen (perforiertes, ischämes Kolon)
Entwicklung eines ARDS und abdominellen Kompartments
Bauchlage
Verschlechterung des Gasaustauschs Bauchlage ohne Entlastung des Abdomens
Antieg des IAP auf 24mmHg (vorher 20mmHg), gleichzeitiger Anstieg des Beatmungsdruckes auf 40cm H2O
Entlastung des Abdomens, danach Absinken des IAP auf 22mmHg und auch des Beatmungsdruckes auf 14cmH2O
Pro Arm
Zusammenfassende Beurteilung: QE:4***
Die Lagerung des Abdomens und die abdominelle Situation (z.B intraabdominelle Drücke) spielen eine wesentliche Rolle für die erfolgreiche Durchführung der Bauchlage

Referenz
Nr.10
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Bassi et al. New insights in positioning tracheally intubated and mechanically ventilated patients
Review
Pro Arm
Zusammenfassende Beurteilung: QE 4**
Here, we describe the main indications, pulmonary effects, and controversies regarding the use of semirecumbent, prone, and lateral positions in critically ill, mechanically ventilated patients. We also discuss new insights from experimental and clinical studies and how the translation of these new findings into clinical practice might improve outcomes of tracheally intubated and mechanically ventilated patients.

Referenz
Nr.11
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Haupt-ergebnis
insgesamt
Bein Th. et al. Dtsch Ärzteblatt 2007;104 (28-29): A2048-53 Beatmung in Bauchlage beim akuten Lungenversagen
Review systematisch 348 publizierten Studien BL vs. RL Bei Patienten mit akutem Lungenversagen bewirkt die BL eine Verbesserung der Oxygenierung durch
Homogenisierung der Atemgasverteilung
Homogenisierung der pulmonale Perfusion
Reduktion des Ventilations-/Perfusionsmissverhältnisses
Steigerung der Zwerchfelldynamik
Verbesserung der Atemmechanik
Wiedereröffnung dorsobasaler Atelektasen
Reduktion des intrapulmonales Shunts
Evidenz:
V.a. bei Pat. Mit posttraumatischem ALI/ARDS guter Effekt
≥12h und Wiederholung bessere Wirkung
Kein Nachweis einer Verminderung der Letalität, aber Studienprotokolle sehr unterschiedlcih bezüglich Population, Lagerungsprotokoll und Beatmungsstrategie
Durchführung& Empfehlungen:
Gute Vorbereitung notwendig ( Analgosedierung, Kreislaufstabilisierung, Sicherung von Tubus und Kathetern)
Notfallalgorithmus
Mehrere Pflegekräfte und ein Arzt
Gute Polsterung und Kontrolle der gefährdeten Hautareale
Anpassung der Beatmung
Dauer 8-12h, dann nach 8- 12h Rückenlage erneute Kontrolle
Aussetzen der enteralen Ernährung während der BL
Bei PaO2 ≤88mmHg empfohlen
Kontraindikationen:
Akuter Schock
Instabile Wirbelsäule
= absolute KI
Aktues Abdomen, v.a. mit Netzeinlage oder inkompletten Bauchwandverschluss
SHT
Schwere Mittelgesichtsverletzungen
= relative KI
Pro Arm
Zusammenfassende Beurteilung: QE 4 ***
Bei beatmeten Intensivpatienten mit akutem Lungenversagen ist eine intermittierende BL für ca. 12h im Wechsel mit der Rückenlagerung geeignet, den pulmonalen Gasaustausch zu verbessern (durch Verminderung des V/P- Missverhältnisses). Der Nachweis einer Reduktion der Letalität fehlt bisher. Eine sorgfältige Planung der Durchführung mit einer guten Vorbereitung des Patienten und entsprechendem Risikomanagement sind erforderlich.

Referenz
Nr.12
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Haupt-ergebnis Bemerkung
insgesamt Bein et al Intensive Care Med. DOI 10.1007/s00134-013-3165-8 Suprising physiologic side effects of an alternating pressure air mattress during prone position in an ARDS patient
Fallbericht 80 J. Patient, 78kg schweres ARDS nach VU Thoraxtrauma,
Bauchlage auf einer APAM, Noradrenalin 0,3µg/kg/min, RR 130mmHg
ZVK in V.jug. int. li., Lagekontrolle mit Röntgen Thx erfolgt.
Bauchlage mit APAM Matratze Wechsledruckzyklus 10 Min.
Nach Start der Wechseldruckzyklen konnten Oszillationen von HF, systolischem Blutdruck und Pulsoxymetrie beobachtet werden, die mit dem Zyklus der Wechseldruckmatratze korrelierten.
In der Rückenlage waren diese Effekte nicht zu beobachten
Im statischen Programm der Matratze stoppten die Oszillationen.
Keine Unterschiede im Laktat (BL vs. RL)
Erklärung:
Die Wechseldruckzellen generieren Drücke zwischen 0-30mmHg. Möglicherweise gibt es einen Einfluss auf den transthorakalen oder intraabdominellen Druck, so dass es zu einer zyklischen Änderung der Hämodynamik und Oxygenierung kommt.
Pro Arm
Zusammenfassende Beurteilung: QE4***
s.o.

Referenz
Nr.13
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Beitler Intensive Care Med (2014) 40:332–341 Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume
Metaanalyse Included were randomized trials evaluating the effect on mortality of prone versus supine positioning during conventional ventilation for ARDS. 7 trials were identified including 2,119 patients
Supine Position The primary outcome was risk ratio of death at 60 days meta-analyzed using random effects models. Analysis stratified by high (>8 ml/kg predicted body weight) or low (≤8 ml/kg PBW) mean baseline tidal volume was planned a priori.
Overall, prone positioning was not significantly associated with the risk ratio of death (RR 0.83; 95 % CI 0.68–1.02; p = 0.073; I2 = 64 %). When stratified by high or low tidal volume, prone positioning was associated with a significant decrease in RR of death only among studies with low baseline tidal volume (RR 0.66; 95 % CI 0.50–0.86; p = 0.002; I2 = 25 %). Stratification by tidal volume explained over half the between-study heterogeneity observed in the unstratified analysis.
Pro Arm
1088 PP 1031 SP
Zusammenfassende Beurteilung: QE 1a**** Prone positioning is associated with significantly reduced mortality from ARDS in the low tidal volume era. Substantial heterogeneity across studies can be explained by differences in tidal volume.

Referenz
Nr.14
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Blanch Minerva Anaethesiologica Vol 78-No9 Back to bench:inhalated iloprost and prone positioning in ARDS
Editorial
Pro Arm
Zusammenfassende Beurteilung: QE: 4**(*)
Bauchlage verbessert den Gasaustausch durch Reduktion des Shunts und Verbesserung der Atemgasverteilung. Bachlagerung ist assoziiert mit Verringerung der Atelektasen und Lungenödemen (im Tiermodel und in klinischen Studien Broccard 2000, Pelosi 2003). Ein Review (Sud 2010, Gattinoni2010) beschreibt, dass Tidavolumen und Spitzendruck in BL auf eine größere Alveolenanzahl verteilt werden und dadurch in Bauchlage die Scherkräfte etc. reduziert sind. Dies reduziert die Mortalität. Inhalatives NO, Prostacyclin und Sildenafil verbessern V/P Missmatch, reduzieren pulmonale Hypertonie und Hypoxie. Eine Verbesserung des Überlebens konnte nicht gezeigt werden. Mortalität und renale Dysfunktion scheinen erhöht zu sein (Banch 1997, Kaisers 2003, Cornet 2010, Adhikari 2007). Bauchlage verbessert die Oxygenierung unabhängig von der ARDS Ursache, wohingegen NO vorwiegend bei ARDS pulmonalen Ursprunges wirkt. Senturkk et al. untersuchten in einer Schweinestudie den additiven Effekt von Iloprost und Bauchlage und konnten keinen additiven Effekt finden. Zu Therapie von pulmonaler Hypertonie und Hypoxie ist eine Therapie mit Iloprost und Bauchlage notwendig. Mehrere Studien zeigten, dass BL den Totraum reduziert, die alveoläre Rekrution verbessert und die Scherkräfte reduziert.

Referenz
Nr. 15
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle
Zielgröße Hauptergebnis Bemerkung
insgesamt
Brücken et al.
Acta Anaesth. Scand 2011;55:1061-1067
Influence of Prone Posititoning on the measurement of transpulmonary thermodilution- derived variables in critically ill patients
Nicht kontrollierte nicht randomisierte Kohortenstudie,
16 Patienten mit ARDS oder ALI Keine Angabe 135° Lage für 8-10h
Gesunde Lunge nach unten
Wenn beide Lungen betroffen waren nach dem Zufallsprinzip
PICCO plus-Messung, 5f A.femoralis catheter, 15ml<8°C
Sedierung mit Propofol und/oder midazolam, PCV
EVLWI von 10ml/kg angepeilt, ansonsten Volumengabe, bzw Diuretika
keine EVLWI steigt in 135° an und bleibt erhöht bis zum Ende der 135° Lagerung
GEDVI bleibt unverändert nach der Lagerung und fällt nach drehen in Rückenlage ab.
cGEDVI steigt in 135° Lagerung und fällt nach Reposition in RL.
Keine signifikanten Änderungen des PVPI
Keine Angabe zur Beatmung (TV, Peep, etc…)
Keine Randomisierung
Kleine Fallzahl
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
EVLWI und GEDVI werden möglicherweise durch eine 135° Lagerung beeinflusst, trotz statistischer Signifikanz sind die Unterscheide gering und am ehesten ohne klinische Relevanz.
Referenz
Nr.16
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Hauptergebnis Bemerkung
insgesamt
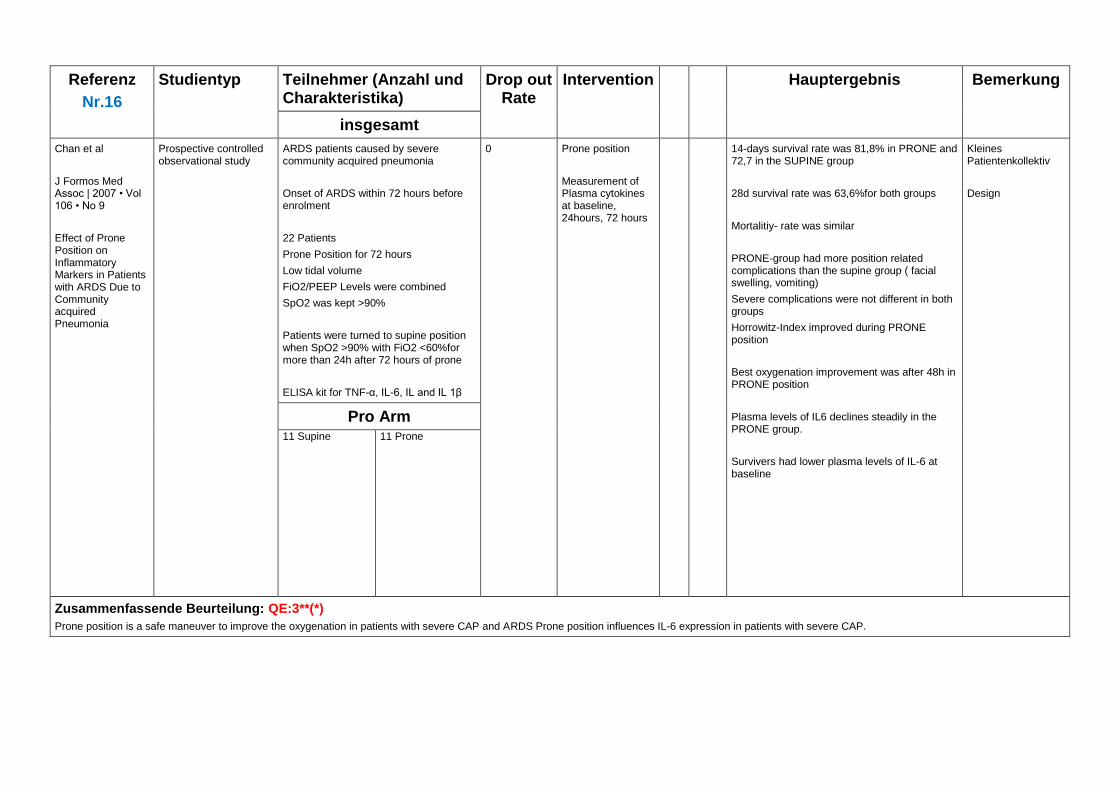
Chan et al
J Formos Med Assoc | 2007 • Vol 106 • No 9
Effect of Prone Position on Inflammatory Markers in Patients with ARDS Due to Community acquired Pneumonia
Prospective controlled observational study
ARDS patients caused by severe community acquired pneumonia
Onset of ARDS within 72 hours before enrolment
22 Patients
Prone Position for 72 hours
Low tidal volume
FiO2/PEEP Levels were combined
SpO2 was kept >90%
Patients were turned to supine position when SpO2 >90% with FiO2 <60%for more than 24h after 72 hours of prone
ELISA kit for TNF-α, IL-6, IL and IL 1β
0 Prone position
Measurement of Plasma cytokines at baseline, 24hours, 72 hours
14-days survival rate was 81,8% in PRONE and 72,7 in the SUPINE group
28d survival rate was 63,6%for both groups
Mortalitiy- rate was similar
PRONE-group had more position related complications than the supine group ( facial swelling, vomiting)
Severe complications were not different in both groups
Horrowitz-Index improved during PRONE position
Best oxygenation improvement was after 48h in PRONE position
Plasma levels of IL6 declines steadily in the PRONE group.
Survivers had lower plasma levels of IL-6 at baseline
Kleines Patientenkollektiv
Design
Pro Arm 11 Supine 11 Prone
Zusammenfassende Beurteilung: QE:3**(*)
Prone position is a safe maneuver to improve the oxygenation in patients with severe CAP and ARDS Prone position influences IL-6 expression in patients with severe CAP.

Referenz
Nr. 17
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Cesana et al Minerva Anestesiologica Vol 76, No 11 Positive end-expiratory pressure, prone positioning, and activated protein C: a critical review of meta-analyses
Review über Metaanalysen von Sud, Alsaghir, Kopterides, Abroug, Gattinoni
Pro Arm
Zusammenfassende Beurteilung: QE 4***
QE der vorkommenden Metaanalysen 1a

Referenz
Nr. 18
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Chadwick J Trauma Nurs 2010;4 Prone positioning in trauma patients: nursing roles and responsibilities
Pro Arm
Zusammenfassende Beurteilung: QE 4**
This article will explain the nursing roles and responsibilities in the initiation, continuation, and cessation of intermittent prone positioning.

Referenz
Nr.19
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Cornejo et al Am J Respir Crit Care Med VOL 188 2013 no..4; 440-448 Effects of prone positioning on lung protection in patients with acute respiratory distress syndrome
Observational intervention study
24 patients with ARDS
24-72h mech. Ventilation (VC)
6ml/kg ideal body weight
CT scan during breath-holding sessions in supine and prone position
PEEP 5,15,45 cmH2O
A recruitement was performed before PEEP change
ICU:
Ventilation with 5cmH2O and with 15cmH2O for 20 min., starting with a recruitement at 45cmH2O before each period.
Assessment of:
Respiratory mechanics
Oxygenation
Hemodynamic parameters
CT:
Whole lung CT during breath holding sessions at 5,45,15 cmH2O,
Afterwards Cine CT were performed on a fixed thoracic transverse slice at PEEP 5 and 15 cmH2O
CT scan were repeated in supine and prone position
Lung recruitment
Cyclic recruitment/derecruitment
Tidal hyperinflation
Prone position has no significant effect on gas exchange or compliance compared to supine position at PEEP 5cm H2O
Increasing PEEP from 5 to 15cmH2O increased oxygenation and compliance, decreased non-aerated tissue and increased well aerated tissue. These effect was observed for both (PRONE and SUPINE)
In PRONE the effect was bigger than in SUPINE
(decrease of non-aerated tissue)
Combination of Prone position and PEEP 15cmH2O significantly decreased cyclic recruitment and de-recruitment
Tidal hyperinflation was increased in SUPINE with 15cmH2O PEEP
PEEP induces hyperinflation was significantly reduced by PRONE position
Cyclic recruitment and de-recruitment only decreased, when high PEEP and PRONE position were combined
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
Prone positioning enhances lung recruitment and decreases alveolar instability and hyperinflation observe at high PEEP in patients with ARDS

Referenz
Nr. 20
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Haupt-ergebnis
insgesamt Chiumello et. al. Critical Care Vol 10 No 3 Effects of thoraco-pelvic supports during prone position in patients with acute lung injury/acute respiratory distress syndrome: a physiological study
Kohortenstudie mit Randomisierung der Patienten in die Gruppe mit thoracopelvic support und ohne thoraco-pelvic support
11 patients
ALI/ARDS
VC ventilation, sedated, paralysed
1 hour supine position
2 hours prone position (1h with and 1h without support)
Prone position with or without thoraco-pelvic support for 1h period without changing the ventilation setting ( TV 7,2±1,4ml/kg KG, HF 17,1±3,5/min.,FiO2 0,43±0,04
PEEP 10,8±1,8cmH2O
In four healthy subjects the pressures were between the body and the contact surface (with and without the thoraco-pelvic support)
Supine (baseline)
Prone without support
With thorco-pelvic supports, the contact pressures almost doubled in comparison with those measured without supports.
The oxygenation related variables were not different in prone position with or without thoraco-pelvic support.
The lung volumes were similar in the prone position with/or without support
Chest wall compliance was significant decreased by thoraco-pelvic support
Pleural pressure was significantly increased in prone position with support
With support heart rate increased significantly, stroke volume index decreased significantly
Zusammenfassende Beurteilung: QE 2b***
Prone position with thoraco-pelvic supports, as compared with the prone position without thoraco-pelvic support did not affect gas exchange and lung volume, but decreased the chest wall compliance, increased the pleural pressure and slightly modified the hemodynamic pattern. They confirmes a positive effect on the oxygenation, when ARDS patients were shifted to prone position.

Referenz
Nr. 21
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Zielgröße(n) Haupt-ergebnis
Insgesamt
Chiumello et al Intensive Care Med (2012)38:221-229 Long term outcomes in survivors of acute respiratory distress syndrome ventilates in supine or prone
Observational prospective study
26 Patients (mean age 54,1±208; BMI 24,5±1,4kg/m2; Horrowitz-Index 117±49mmHg) Evaluation after 12 Month
Pulmonary function CT Scan Health related quality of life St George´s Respiratory questionnaire ,
No significant differences in demograohic data, illness serverity or outcome between prone and supine goups Overall survival rate 40% Pulmonary function in normal range without any difference between the two groups Quantitative lung CT Scan showed similar amounts for not aerated, poorly aerated and well-aerated lung regions Over aerated lung region were slightly higher in prone vs. supine group No differences in Quality of life were observed
Pro Arm
13 Patients 13 Patients
Zusammenfassende Beurteilung: QE 2b**(*)
No differences in pulmonary function or quality of life in ARDS survivors after 12 month, treated in prone versus supine position.

Referenz
Nr. 22
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Charron et al. Critical Care 2011, 15:R175 PaCO2 and alveolar dead space are more relevant than PaO2/FiO2 ratio in monitoring the respiratory response to prone position in ARDS: a physiological study
Prosepective cohort study
13 patients ARDS ( Horrowitz<100mmHg after 24- Measurement of Pplat, PEEP, blood gas analysis and endexspiratory CO2. In spupine before movement and after 3,6,9,12,15 hours at prone
Responders to prone position: After 15h of PP by an increse in horrowitz index>20mmHg or by an decrease of CO2 >2mmhg
Significant increase of horrowitz index after 15h of PP Significant decrease of PaCO2, with lowest value after 9hours Pplat was significantly reduced in PP Compliance significantly improved in PP VDalv/VT ratio was significantly reduced with the lowest value after 3hours in PP. Changes in VDalv/VT ratio were correlated with changes ind compliance but not with changes in Horrowitz-index When the response was definded by Horrowitz-Index, no significant differences between responders and nonresponders were observed When the response was defindes by PaCo2, 4 patients were differently classified and responders had a greater decrease in VDalv/VT ratio and in Pplat and a greater increase in Horrowitz-index and in compliance
Pro Arm
Zusammenfassende Beurteilung: QE3**(*)
Prone position decreases VDalv/VT ratio and improves respiratory mechanics. The respiratory response to PP seems to be more relevant when paCo2 rather than Horrowitz-Index was used.

Referenz
Nr. 23
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Charron et al
Intensive care Med (2011) 37:785-790
Routine prone positioning in patients with severe ARDS: feasibility and impact on prognosis
Retrospective analysis 218 patients ( Age 57+/- 16) SAPSII 58+/-22, 84% with vasopressor, Mortality 38,5%, SMR 0,60)
Standard mortalitiy rate (SMR) = provided mortality/predicted mortality (SAPS)
11 Patients in PP group died
PaO2/FiO2 74 ± 19,
PaCO2 54 ± 10 mmHg. The
Lung injury score was 3.13 ± 0.15.
Tidal volume was 7 ± 2 mL/kg,
PEEP 5.6 ± 1.2 cmH2O, and plateau pressure 27 ± 3 cmH2O.
Prone sessions lasted 18 h/day and
3.4 ± 1.1 sessions were required to obtain an FiO2 below 60%.
60-day mortality was 19% and death occurred after 12 ± 5 days.
Ratio between observed and predicted mortality was 0.43.
In patients with a
PaO2/FiO2 below 60 mmHg, the 60-day mortality was 28%.
Logistic regression analysis showed that
PP appeared to be protective with an odds ratio of 0.35 [0.16–0.79].
Pro Arm
161 without PP
Horrowit >100mmHg after 24-48h
Age 59+/- 17
SAPSII 61+/-20, 93% with vasopressor, Mortality 45%, SMR 0,64)
57 patients with PP:
Horrowit <100mmHg after 24-48h
Age 51+/- 16
SAPSII 49+/- 14, 58% with vasopressor, Mortality 19%, SMR 0,43)
3,4+/- 1,1 prone Sessions were needed to achieve the PaO2 above 60%
Zusammenfassende Beurteilung: QE 3**(*)
PP in patients with a PaO2/FiO2 below 100 mmHg after 24–48 h prone position is feasible. When combined with a low stretch ventilation strategy it is protective with a high survival rate.

Referenz
Nr. 24
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt
Chergui et al
Anesthesiology 2007; 106:1237–9
Prone Positioning for a Morbidly Obese Patient with Acute Respiratory Distress Syndrome: An Opportunity to Explore Intrinsic
Positive End- expiratory Pressure–Lower Inflexion Point
Interdependence
Fallbericht 1 patient
BMI 42 with ARDS
Prone position Reduction of intrinsic PEEP and lower inflection point after prone position
Improvement of oxygenation
Pro Arm
Zusammenfassende Beurteilung: QE 4**(*)
This clinical case report questions the physiologic basis of the open lung approach compared with the prone positioning strategy when applied to morbidly obese patients, and at the same time highlights interdependence between PEEPi and the lower inflection point, especially in morbidly obese ARDS patients.

Referenz
Nr. 25
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Cortes et al Minerva Anestesiol 78 (2012);No 3 343-357 Acute respiratory distress syndrome: evaluation and management
Review
Pro Arm
Zusammenfassende Beurteilung: QE 4**(*)

Referenz
Nr.26
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Cuartero et al. Intensive Care Medicine Seite 356 Effect of prone position on intraabdominal pressure and renal function Nur Poster!!!
Observational study Adult ARDS patients who were ventilated using the protective strategy defined by ARDS Network criteria and who needed prone position to improve oxygenation 18 patients (14 male) admitted to a medical-surgical ICU over a one-year period.
We collected respiratory data (ventilator parameters and gas exchange) and hemodynamic variables (heart rate, systolic, diastolic and mean arterial pressure). IAP was measured using the Abdo-Pressure(TM) bladder transducer following World Society of Acute Compartment Syndrome recommendations. Abdominal perfusion pressure was calculated as mean arterial pressure minus IAP. Main renal parameters were: filtration gradient (FG), creatinine clearance, fractional excretion of sodium (FENa) and urea (FEUrea). Patients were classified according to RIFLE score after each manoeuvre. All data were recorded in prone and in supine position at least once per day.
Mean age was 47.3 +- 17.8 and length of ICU stay was 23 +- 18 days. All 18 patients had primary ARDS and 9 had received nephrotoxics. ICU mortality reached 50%. We recorded at least 3 manoeuvres per patient (A, B, C). Prone positioning improved PaFiO 2 ratio from 101.5 ± 5 to 150 ± 72 (p = 0.027). IAP showed a small increase from 6.1 ± 2.7 to 8.9 ± 2.9 mmHg (A; p = 0.004), from 8.4 ± 3.4 to 11.2 ± 3.7 mmHg (B; p = 0.038) and from 7.6 ± 1.3 to 9.9 ± 0.8 mmHg (C; p = 0.001). There were no statistically significant changes in hemodynamic parameters or abdominal perfusion pressure. Renal function parameters (FG, creatinine clearance, FENa and FEUrea) showed no modification after each prone positioning. In contrast, when patients were classified according to RIFLE score, we observed a trend towards worsening, though this was not statistically significant.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
Prone positioning improved arterial oxygenation in primary ARDS patients and was associated with an increase in IAP. However, creatinine clearance and glomerular filtration remained unchanged.

Referenz
Nr. 27
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Haupt-ergebnis
insgesamt Davis et al. J Trauma. 2007;62:1201–1206 Prone ventilation in trauma or surgical patients with acute lung injury and adult respiratory distress
Retrospective systematic Review
61 (53 trauma and 8 general surgery patients)
19 death (18 in supine and 1 in prone group)
There was no difference between the groups in age, CVP, ISS, RTS, base deficit, head AIS score, chest AIS score, abdominal AIS score, or probability of survival. The PaO2/FiO2 ratios were not different at study entry (149 vs. 153, p = NS), and both groups showed improvement in PaO2/FiO2 ratios. The prone group had better PaO2/FiO2 ratios than the supine group by day 5 (243 vs. 200, p = 0.066). The prone group had fewer days on the ventilator (13.6 vs. 24.2, p = 0.12), and shorter hospital lengths of stay (22 days vs. 40 days, p = 0.08). There were four patients who failed to improve with supine kinetic therapy that were changed to prone kinetic therapy. These patients had significant improvements in PaO2/ FiO2 ratio, and significantly lower FiO2 requirements. There were 18 deaths (7 pulmonary related) in the supine group and 1 death in the prone group (p < 0.01 by Χ2 test).
Pro Arm
44 supine 13 prone, 4 patients were moved to prone later
Zusammenfassende Beurteilung: QE 4**(*)
ALI/ARDS patients who received prone kinetic therapy had greater improvement in PaO2/FiO2 ratio, lower mortality, and less pulmonaryrelated mortality than did supine positioned patients. The use of a prone-oscillating bed appears advantageous for trauma and surgical patients with ALI/ARDS and a prospective, randomized trial is warranted.

Referenz
Nr. 28
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Deniz Rev. Bras. Anestesiol. 2013;63(2):209-212 The effect of head rotation on intraocular pressure in prone position: a randomized trial
RCT 45 patients
18-80a
PCNL (Department of urology)
Measurement of IOP (intra ocular pressure) before procedure in supine position, during procedure in prone position and after procedure
Group II with head position 45° laterally to the right side
Group I in a neutrally position, with straight neck
IOP IOP increased in prone position in both groups
IOP in 45° laterally position is significant lower in the upper eye compared to IOP in group I and in group II (lower eye)
Pro Arm
23 group I 22 group II
Zusammenfassende Beurteilung: QE 2b***
Prone position increases IOP, moderate lateral position may have advantage to protect glaucoma affected eyes.

Referenz
Nr. 29
Studientyp Teilnehmer (Anzahl und Charakteristika)
Hauptergebnis
insgesamt
Diaz et al
Crit Care Med 2010 Vol. 38, No. 8
Therapeutic strategies for severe acute lung injury
Review Although prone positioning has failed to demonstrate a survival benefit in four randomized, clinical trials, the two trials that placed patients prone for 20 hrs per day did report beneficial trends in mortality rates (Taccone, Mancebo, Gattinoni)
The initial trial, which failed to enroll the number of patients needed to detect the predetermined effect size, reported a trend for decreased intensive care unit mortality (43% vs. 58%;p= .12) in the prone-treated group and significant improvements in oxygenation and plateau airway pressure when compared to the supine group (Mancebo).
The subsequent trial (Taccone) compared protocolized delivery of prone position and lung-protective ventilation strategy to protocolized lung-protective ventilation strategy alone and reported similar low mortality levels in both groups (31% vs. 32.8%; p=0,72)
In patients with severe hypoxemia there was a trend toward a decreased 28-day mortality rate (37.8% vs. 46.1%; p _ .31) in the prone-treated group.
Pro Arm
Zusammenfassende Beurteilung: QE 4**
Consider placing patients prone if they have severe ARDS with life-threatening hypoxemia and/or elevated plateau airway pressures. Develop guidelines to prevent complications. Placing patients prone for a total of at least 20 hrs per day seems to be associated with greater benefit; however, intermittent time in the supine position may be necessary for nursing care and procedures. If there is no improvement in oxygenation by the end of the day, then do not continue with prone positioning and proceed promptly to another therapy (expert opinion).

Referenz
Nr. 30
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt
D´Iggnazio
MINERVA ANESTESIOL 2007;73:467-70
Postraumatic ARDS: how to place patients who may offer technical problems in a prone position
Casereport 2 patients
Pro Arm
Zusammenfassende Beurteilung: QE 4**(*)
Prone position in patients with trauma of the spine is possible when an immobilization- technique is used

Referenz
Nr. 31
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Dirkes et al.
Crit Care Nurs Q
Prone positioning: is it safe and effective?
Review
Pro Arm
Zusammenfassende Beurteilung: QE 4**
With the utilization of a standardized protocol and a trained and dedicated critical care staff, prone positioning can be performed safely.

Referenz
Nr. 32
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Essat
Nurs Stand
Prone positioning in patients with acute respiratory distress syndrome
Pro Arm
Zusammenfassende Beurteilung: QE4*
This article examines the aetiology of ARDS and how nurses can identify this condition. Patient groups that benefit most from prone positioning are considered as well as the research
evidence on the use of prone positioning in the treatment of ARDS. This article addresses nurse involvement in delivering therapy and suggests that nurses alert members of the
multidisciplinary team to the possible use of this therapy.

Referenz
Nr. 33
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Farag et al. Anesthesiology 2012; 116:807–15 Effects of Crystalloid versus Colloid and the α-2 Agonist Brimonidine vs. Placebo on Intraocular Pressure during Prone Spine Surgery
RCT Complex spine surgery in prone position
Prone position increased IOP on average by SD of 12 ± 6 mmHg. IOP increased to 38 ± 10 mm Hg at the end of anesthesia (approximately 5.5 h). In twelve of 65 patients IOP exceeded 50 mm Hg after approximately five hours of surgery The increased IOP during surgery and consequently decreased OPP would explain the prolonged anesthesia time as risk factor for POVL after spine surgeries
Pro Arm
Zusammenfassende Beurteilung: QE 1b***
Prone positioning increased IOP a mean ± SD of 12±6 mmHg. IOP increased to 38±10 mmHg at the end of anesthesia (approximately 5.5 h).
Referenz
Nr. 34
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße Hauptergebnis
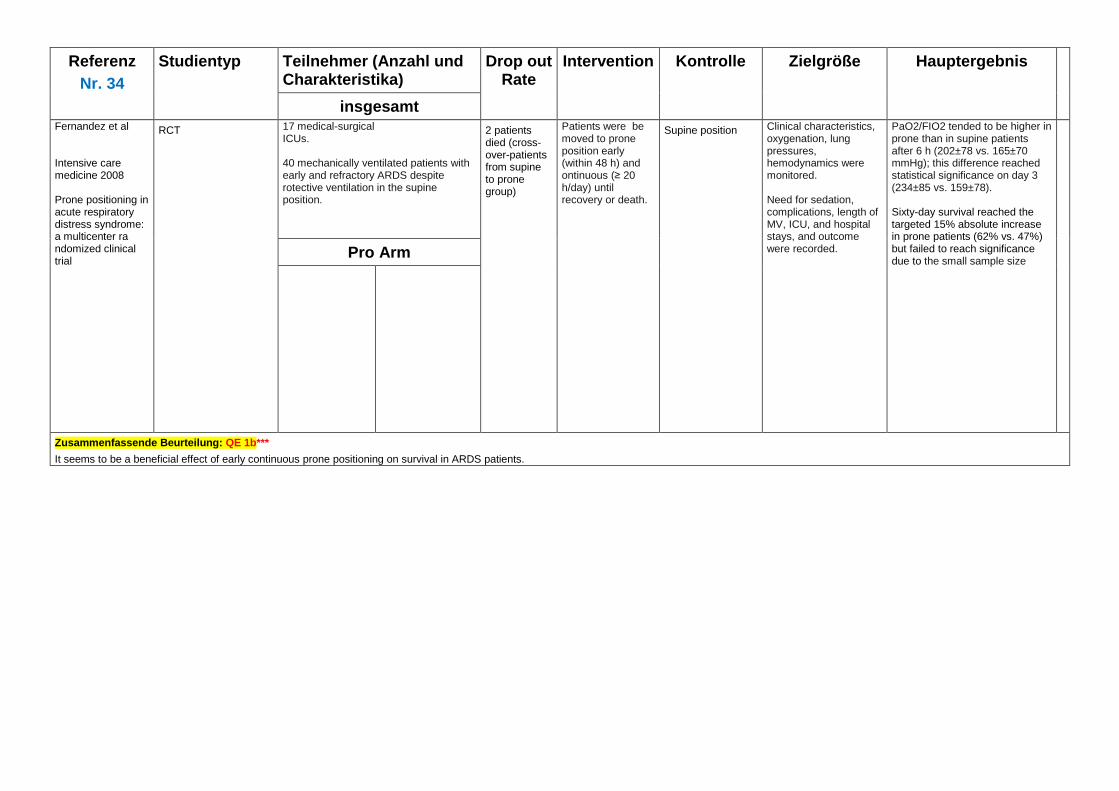
insgesamt Fernandez et al Intensive care medicine 2008 Prone positioning in acute respiratory distress syndrome: a multicenter ra ndomized clinical trial
RCT 17 medical-surgical ICUs. 40 mechanically ventilated patients with early and refractory ARDS despite rotective ventilation in the supine position.
2 patients died (cross-over-patients from supine to prone group)
Patients were be moved to prone position early (within 48 h) and ontinuous (≥ 20 h/day) until recovery or death.
Supine position Clinical characteristics, oxygenation, lung pressures, hemodynamics were monitored. Need for sedation, complications, length of MV, ICU, and hospital stays, and outcome were recorded.
PaO2/FIO2 tended to be higher in prone than in supine patients after 6 h (202±78 vs. 165±70 mmHg); this difference reached statistical significance on day 3 (234±85 vs. 159±78). Sixty-day survival reached the targeted 15% absolute increase in prone patients (62% vs. 47%) but failed to reach significance due to the small sample size
Pro Arm
Zusammenfassende Beurteilung: QE 1b***
It seems to be a beneficial effect of early continuous prone positioning on survival in ARDS patients.
Referenz
Nr. 35
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Fessler et al. RESPIRATORY CARE; JANUARY 2010 VOL 55 NO 1 Should prone positioning be routinely used for lung protection during mechanical ventilation?
Review
Pro Arm
Zusammenfassende Beurteilung: QE 4 **(*)

Referenz
Nr. 36
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Haupt-ergebnis
insgesamt
Fletcher et al
Clinical Intensive Care, 2006; 17: 109-112
The effect of prone ventilation on intra-abdominal pressure
Cohort study 10 patients with ARDS Prone position without support
IAP was measured by instilling 50 ml sterile saline into the urinary bladder and measuring the intravesical
pressure by electronic manometer through the bladder catheter after equilibration [
IAP
Secondary outcome variables (arterial blood pressure, central venous pressure, urine output, total respiratory compliance, FiO2, and arterial pH, pO2, pCO2) at baseline (supine),
IAP appeared to fall with time, and although the
confidence intervals overlap, time series regression analysis with time as a covariate and supine/prone as
a factor showed that the fall in IAP was statistically
significant (likelihood ratio chi-squared on 2 degrees
of freedom=17.24, p=0.0002).
Pro Arm
Zusammenfassende Beurteilung: QE: 3**(*)
Prone position does not increase IAP

Referenz
Nr. 37
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße Hauptergebnis
insgesamt Galiatsou Am J Respir Crit Care Med Vol 174. pp 187–197, 2006 Prone position augments recruitment and prevents alveolar overinflation in acute lung injury
Prospective observational
21 patients with ALI
1. Recruitment maneuver was applied in the supine position 2. Multislice spiral computed tomography (CT) scan 3. Patients were turned prone 4. A second CT scan was performed.
1. Patients with diffuse and lobar ALI/ARDS presented with a significant amount of nonaerated lung and a high potential for recruitment soon after an RM in the supine position. 2. Prone position and RM had an additive effect on oxygenation. The prone position recruited the edematous lung in dependent areas more than the RM had achieved, and reversed overinflation of ventral areas. 3. These effects of the prone position were more pronounced in lobar ALI/ARDS. Patients with the diffuse pattern responded to the prone position with recruitment of nonaerated areas but showed no reversal of ventral overinflation. 4. There was no redistribution of nonaerated areas toward the ventral compartment in the prone position . 5. There was no evidence of end-expiratory “de-recruitment” in the prone position. In other words, the prone position resulted in decreased “dispersion” of aeration and decreased alveolar overinflation, an effect that is possibly protective against ventilator-induced lung injury.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
Prone position recruited the edematous lung further than recruitment maneuvers and reversed overinflation, resulting in a more homogeneous distribution of aeration. The effects of the prone position were more pronounced in patients with lobar ALI.

Referenz
Nr 38
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n)
Haupt-ergebnis
insgesamt Gattinoni et al MINERVA ANESTESIOLOGICA, Vol. 76 - No. 6 Prone positioning improves survival in severe ARDS: a pathophysiologic review and individual patient meta-analysis
Systematic Review Prone position Supine position PP reduces the non-physiological stress and strain associated with mechanical ventilation PP decreases the risk of ventilator-induced lung injury An individual patient meta-analysis of the four major clinical trials available clearly shows that with prone positioning, the absolute mortality of severely hypoxemic ARDS patients may be reduced by approximately 10%. On the other hand, all data suggest that long-term prone positioning may expose patients with less severe ARDS to unnecessary complications.
Pro Arm
Zusammenfassende Beurteilung: QE 4**(*)

Referenz
Nr. 39
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Gattinoni Anesthesiology 2010; 113:1262– 4 Prone positioning: beyond physiology
Editorial PEEP Wirkung in Bauchlage unterscheidet sich bei Patienten mit ARDS von Patienten mit einer gesunden Lunge.
Pro Arm
Zusammenfassende Beurteilung: QE 4***
Editorial über die Wirkung von PEEP in prone position mit Bezug auf die Petterson Studie 2010. Diese schlussfolgerten aus ihren Ergebnissen, dass ein niedrigerer PEEP in Bauchlage zu bevorzugen sei. Die Ergebnisse wurden an Patienten ohne ARDS erhoben.

Referenz
Nr. 40
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Gattinoni Intensive Care Med (2013) 39:1909–1915 Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure: impact and clinical fallout through the following 20 years
Review
Pro Arm
Zusammenfassende Beurteilung: QE: 4**(*)
Guter und aktueller Überblick über die Effekte der Bauchlagerung. Auch die aktuellen Studien sind erwähnt.

Referenz
Nr. 41
Studientyp Teilnehmer (Anzahl und Charakteristika)
Haupt-ergebnis
insgesamt Gattinoni Commentary Prone ventilation is not recommended in the routine management of acute lung injury and ARDS, but it
can be used as a rescue maneuver in cases of severe hypoxemia. Experimental evidence suggests that prone ventilation can prevent or attenuate ventilator-induced lung injury. The possible survival benefit of prone ventilation in subgroups of patients with ALI or ARDS remains to be determined.
Pro Arm
Zusammenfassende Beurteilung: QE 4**(*)
Beurteilung der Metaanalyse von Sud et al

Referenz
Nr. 42
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontr. Zielgröße(n) Hauptergebnis
insgesamt Girard et al. Intensive Care Med (2014) 40:397–403 The impact of patient positioning on pressure ulcers in patients with severe ARDS: results from a multicenter randomized controlled trial on prone positioning
RCT (Daten aus der RCT von Guerin et al 2013)
Pressure ulcers were assessed at the time of randomization, 7 days later and on discharge from the intensive care unit (ICU), using the four-stage Pressure Ulcers Advisory Panel system.
SP The primary end-point was the incidence (with reference to 1,000 days of invasive mechanical ventilation or 1,000 days of ICU stay) of new patients with pressure ulcers at stage 2 or higher from randomization to ICU discharge.
At randomization, the number of patients with pressure ulcers was not significantly different between groups. The incidence of new patients with pressure ulcers from randomization to ICU discharge was 20.80 and 14.26/ 1,000 days of invasive mechanical ventilation (P = 0.061) and 13.92 and 7.72/1,000 of ICU days (P = 0.002) in the prone and supine groups, respectively. Position group [odds ratio (OR) 1.5408, P = 0.0653], age [60 years (OR 1.5340, P = 0.0019), female gender (OR 0.5075, P = 0.019), body mass index of[28.4 kg/m2 (OR 1.9804, P = 0.0037), and a Simplified Acute Physiology Score II at inclusion of [46 (OR 1.2765, P = 0.3158) were the covariates independently associated to the acquisition of pressure ulcers.
Pro Arm 237 PP 229 SP
Zusammenfassende Beurteilung: QE 1b****
In patients with severe ARDS, prone positioning was associated with a higher frequency of pressure ulcers than the supine position. Prone positioning improves survival in patients with severe ARDS and, therefore, survivors who received this intervention had a greater likelihood of having pressure ulcers documented as part of their follow-up. There are risk groups for the development of pressure ulcers in severe ARDS, and these patients need surveillance and active prevention.

Referenz
Nr. 43
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Haupt-ergebnis
insgesamt Grant et al Anesthesiology 2010; 112:57– 65 Effects of prone and reverse Trendelenburg positioning on ocular parameters
Prospective observational study
10 helathy volunteers 10 healthy volunteers
IOP measurement, choroidal thickness and optic nerve diameter assessment on a Jackson table during 5 h horizontal prone and 5 h 4-degree reverse Trendelenburg positioning.
Measurements were assessed as initial supine, initial prone, and hourly thereafter.
Vital signs were recorded at each position and time point.
In healthy volunteers, intraocular pressure and choroid/optic nerve width increase progressively over 5 h in the prone position Elevating the head of the bed 4° minimally affects these variables, suggesting that such positioning may not protect against ischemic optic neuropathy
Pro Arm
Zusammenfassende Beurteilung: QE 3***
Prolonged prone positioning increases IOP, choroid layer thickness, and optic nerve diameter independent of anesthetics and intravenous fluid infusion and 4 degrees of table inclination (15 cm of head to foot vertical disparity) may not attenuate these effects.
Referenz
Nr. 44
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Gritti et al. J Anesth No2 (27), 2013 The use of inhaled nitric oxide and prone position in an ARDS patient with severe traumatic brain injury during spine stabilization
Casereport 37a patient
Pro Arm
Zusammenfassende Beurteilung: QE 4**
Use of both inhaled nitric oxide and the prone position together in the operating room in a patient with head injury and ARDS who underwent column stabilization.

Referenz
Nr.45
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Guérin C, Reignier J, Richard JC, et al; PROSEVA Study Group. N Engl J Med. 2013; 368:2159-68. Prone positioning in severe acute respiratory distress syndrome.
RCT, doubleblinded
474 adults (mean age 59 y, 68% men, mean Sepsis-related Organ Failure Assessment [SOFA] score 10.0) who had severe ARDS (confirmed as severe after 12 to 24 h of mechanical ventilation in the ICU) and were treated with mechanical ventilation for 16 hours before randomization.
Prone position for 16 consecutive h/d for ≥ 28 days during mechanical ventilation. Prone positioning began within 1 hour after randomization and was stopped if there was improvement in oxygenation when in the supine position for 4 hours, 20% decrease in PaO2–FIO2 ratio during 2 consecutive prone sessions relative to the ratio in the supine position, or a complication during a prone session. Patients in the prone group could be returned to the prone position from the supine position if criteria for oxygen saturation level and/or PaO2 were met.
Supine/ semi recumbent position
The primary end point was mortality at day 28. Secondary end points were mortality at day 90, the rate of successful extubation, the time to successful extubation, the length of stay in the ICU, complications, the use of noninvasive ventilation, the tracheotomy rate, the number of days free from organ dysfunction, and ventilator settings, measurements of arterial blood gases, and respiratory-system mechanics during the first week after randomization.
A total of 237 patients were assigned to the prone group, and 229 patients were assigned to the supine group. The 28-day mortality was 16.0% in the prone group and 32.8% in the supine group (P<0.001). The hazard ratio for death with prone positioning was 0.39 (95% confidence interval [CI], 0.25 to 0.63). Unadjusted 90-day mortality was 23.6% in the prone group versus 41.0% in the supine group (P<0.001), with a hazard ratio of 0.44 (95% CI, 0.29 to 0.67). The incidence of complications did not differ significantly between the groups, except for the incidence of cardiac arrests, which was higher in the supine group.
Pro Arm
Prone position
(n = 240)
Supine or semirecumbent position
(n = 234)
Zusammenfassende Beurteilung: QE 1b**** Erste Studie, die ein Überlebensvorteil für die Bauchlage bei ARDS Patienten zeigen konnte! In conclusion, this trial showed that patients with ARDS and severe hypoxemia (as confirmed by a Pao2:Fio2 ratio of <150 mm Hg, with an Fio2 of ≥0.6 and a PEEP of ≥5 cm of water) can benefit from prone treatment when it is used early and in relatively long sessions.
Referenz
Nr. 46
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Guerin Intensive Care Med (2005) 31:1012–1013 Prone positioning: do not turn it off!
Editorial The authors found that: (a) PaO2/FIO2 ratio increased after each of the three PP sessions relative to the previous supine position (b) after the first PP trial oxygenation remained improved 3 h after supine position resumption, and (c) the first PP trial was associated with removal of a significant amount of respiratory secretions.
Pro Arm
Zusammenfassende Beurteilung: QE 4***
Editorial über die Studie von Reignier J et al (2005) Short-term effects of prone position in COPD patients with severe acute hypoxemic and hypercapnic respiratory failure.
Referenz
Nr.47
Studientyp Teilnehmer (Anzahl und Charakteristika)
Hauptergebnis
insgesamt Guerin Curr Opin Crit Care 2014, 20:92–97 Prone position
Review Prone position has several physiologic benefits in ARDS, namely improvement in oxygenation and prevention of VILI. Two meta-analyses and a single recent trial showed that prone position can improve patient survival in the most severely hypoxemic patients. Prone position is a full component of the lung protective ventilation strategy and should be used early in severe ARDS for long sessions.
Pro Arm
Zusammenfassende Beurteilung: QE: 4**(*)
guter und aktueller (2014) Review

Referenz
Nr. 48
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Guerin Current Opinion in Critical Care 2006, 12:50–54 Ventilation in the prone position in patients with acute lung injury/acute respiratory distress syndrome
Systematic review
Pro Arm
Zusammenfassende Beurteilung: QE 4***

Referenz
Nr. 49
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Hojlund Anesthesiology Research and Practice Volume 2012, Article ID 647258 Effect of head rotation on cerebral blood velocity in the prone position
Observational study 22 helathy subjects Mean arterial blood pressure (MAP), stroke volume (SV), and CO were determined, together with the middle cerebral artery mean blood velocity (MCA Vmean) and jugular vein diameters bilaterally in the prone position with the head centered, respectively, rotated sideways, with and without positive pressure breathing (10 cmH2O)
The prone position reduced SV (by 5.4 ± 1.5%; P < 0.05) and CO (by 2.3 ± 1.9%), and slightly increased MAP (from 78 ± 3 to 80 ± 2 mmHg) as well as bilateral jugular vein diameters, leaving MCA Vmean unchanged. Positive pressure breathing in the prone position increased MAP (by 3.6 ± 0.8 mmHg) but further reduced SV and CO (by 9.3 ± 1.3% and 7.2 ± 2.4% below baseline) while MCA Vmean was maintained. The head-rotated prone position with positive pressure breathing augmented MAP further (87 ± 2 mmHg) but not CO, narrowed both jugular vein diameters, and reduced MCA Vmean (by 8.6 ±
3.2%)
Pro Arm
Zusammenfassende Beurteilung: QE 3***
During positive pressure breathing the prone position with sideways rotated head reduces MCA Vmean ∼10% in spite of an elevated MAP. Prone positioning with rotated head affects both CBF and cerebrovenous drainage that optimal brain perfusion requires head centering.

Referenz
Nr. 50
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Jong et al CHEST 2013; 143(6):1554–1561 Feasibility and effectiveness of prone position in morbidly obese patients with ARDS: a case-control clinical study
Case control study Between January 2005 and December 2009, 149 patients were admitted for ARDS.
Morbidly obese patients (BMI _ 35 kg/m 2 ) with ARDS (Pa O 2 /F IO 2 ratio _ 200 mm Hg) were matched to nonobese (BMI , 30 kg/m 2 ) patients with ARDS in a case-control clinical study. The primary end points were safety and complications of PP; the secondary end points were the effect on oxygenation (Pa O 2 /F IO 2 ratio at the end of PP), length of mechanical ventilation and ICU stay, nosocomial infections, and mortality
nonobese (BMI , 30 kg/m 2 ) patients with ARDS
Primary endpoint: safety and complications of PP Secondary endpoint: Oxygenation
PP duration was 9 h (6-11 h) in obese patients and 8 h (7-12 h) in nonobese patients (P =0 .28). We collected 51 complications: 25 in obese and 26 in nonobese patients. The number of patients with at least one complication was similar across groups (n 5 10, 30%). Pa O 2 /F IO 2 ratio increased significantly more in obese patients (from 118± 43 mm Hg to 222 ± 84 mm Hg) than in nonobese patients (from 113 ± 43 mm Hg to 174 ± 80 mm Hg; P = .03). Length of mechanical ventilation, ICU stay, and nosocomial infections did not differ significantly, but mortality at 90 days was significantly lower in obese patients (27% vs 48%, P=0.05).
Pro Arm
33 obese 33 nonobese
Zusammenfassende Beurteilung: QE:3**(*) PP seems safe in obese patients and may improve oxygenation more than in nonobese patients. Obese patients could be a subgroup of patients with ARDS who may benefi t the most of PP.

Referenz
Nr. 51
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Jozwiak et al Am J Respir Crit Care Med Vol 188, Iss. 12, pp 1428–1433, Dec 15, 2013 Hemodynamic Effects of Prone Positioning
Observational study 18 patients with ARDS ventilated with protective ventilation and an end-expiratory positive pressure titrated to a plateau pressure of 28–30 cm H2O. Before prone positioning, preload reserve was assessed by a passive leg raising test.
Before and within 20minutes of starting prone positioning, hemodynamic, respiratory, intraabdominal pressure, and echocardiographic data were collected.
In all patients, prone positioning increased the ratio of arterial oxygen partial pressure over inspired oxygen fraction, the intraabdominal pressure, and the right and left cardiac preload. The pulmonary vascular resistance decreased along with the ratio of the right/left ventricular end-diastolic areas suggesting a decrease of the right ventricular afterload. In the nine patients with preload reserve, prone positioning significantly increased cardiac index (3.0 [2.3–3.5] to 3.6 [3.2–4.4] L/min/m2). In the remaining patients, cardiac index did not change despite a significant decrease in the pulmonary vascular resistance.
Pro Arm
Zusammenfassende Beurteilung: QE:3**(*)
In patients with acute respiratory distress syndrome under protective ventilation and maximal alveolar recruitment, prone positioning increased the cardiac index only in patients with preload reserve, emphasizing the important role of preload in the hemodynamic effects of prone positioning. Limitations: First, they could not directly assess alveolar recruitment by the quasistatic respiratory system compliance. Second, they did not investigate patients with a very high IAP, in whom PP could collapse the inferior vena cava and decrease cardiac output. Third, the results cannot be extrapolated to PP performed by using thoracic and pelvic supports and with conventional foam mattress, because these factors may affect the effects of PP on the abdominal pressure. Fourth, they could not assess preload responsiveness in the prone position. In particular, it was not possible to use pulse pressure and stroke volume respiratory variations for this purpose, because the low tidal volume and/or low lung compliance associated with ARDS preclude using it for assessing preload dependence. Fifth, they did not measure the pleural pressure and they could not assess the transmission of the IAP and the intrathoracic pressure to cardiac pressures. Thus, they could not assess whether the transmural pressures varied to the same extent than the intramural pressures with PP. Finally, the abdominal and cardiac pressures were not measured with the same reference level.
Referenz
Nr.52
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Kirkpatrick et al Critical Care 2010, 14:232 Clinical review: Intra-abdominal hypertension: does it influence the physiology of prone ventilation?
Review über IAP and prone postition
Modest elevations in IAP without marked physiologic effects after proning. The evidence as to whether proning itself induces important changes in IAP therefore remains inconsistent and is unhelpful to guide clinical practice.
Pro Arm
Zusammenfassende Beurteilung: QE: 4***
Guter Review über die Datenlage von Bauchlage und IAP

Referenz
Nr. 53
Studientyp Teilnehmer (Anzahl und Charakteristika)
Zielgröße(n) Hauptergebnis
insgesamt Kopterides Journal of Critical Care (2009) 24, 89–100 Prone positioning in hypoxemic respiratory failure: meta-analysis of randomized controlled trials
Metaanalyse 1271 patients 4 RCT´s
Mortality Duration of mechanically ventilation Risc for adverse effects
The pooled odds ratio (OR) for the ICU mortality in the intention-to-treat analysis was 0.97 (95% confidence interval [CI], 0.77-1.22), for the comparison between prone and supine ventilated patients. Interestingly, the pooled OR for the ICU mortality in the selected group of the more severely ill patients favored prone positioning (OR, 0.34; 95% CI, 0.18-0.66). The duration of mechanical ventilation and the incidence of pneumothorax were not different between the 2 groups. The incidence of VAP was lower but not statistically significant in patients treated with prone positioning (OR, 0.81; 95% CI, 0.61-1.10). However, prone positioning was associated with a higher risk of pressure sores (OR, 1.49; 95% CI, 1.17-1.89) and a trend for more complications related to the endotracheal tube (OR, 1.30; 95% CI, 0.94-1.80)
Pro Arm
662 Prone 609 Supine
Zusammenfassende Beurteilung: QE 1a****
Despite the inherent limitations of the meta-analytic approach, it seems that prone positioning has no discernible effect on mortality in patients with HRF. It may decrease the incidence of VAP at the expense of more pressure sores and complications related to the endotracheal tube. However, a subgroup of the most severely ill patients may benefit most from this intervention.

Referenz
Nr. 54
Studientyp Teilnehmer (Anzahl und Charakteristika)
Hauptergebnis
insgesamt Lee et al Korean J Intern Med Vol. 25 no.1, 2010 Clinical Meaning of Early Oxygenation Improvement in Severe Acute Respiratory Distress Syndrome under Prolonged Prone Positioning
Retrospective study 96 patients (mean age, 60.1 ± 15.6 years; 75% men) with severe ARDS (PaO2/FiO2 ≤ 150 mmHg) admitted to a medical intensive care unit
The terms “PaO2 response” and PaCO2 response” represented responses that resulted in increases in the PaO2/FiO2 ratio of ≥ 20 mmHg and decreases in PaCO2 of ≥ 1 mmHg, respectively, 8 to 12 hours after first placement in the prone position.
The mean duration of prone positioning was 78.5 ± 61.2 hours, and the 28-day mortality rate after ICU admission was 56.3%. No significant difference in clinical characteristics was observed between PaO2 and PaCO2 responders and non-responders. The PaO2 responders after prone positioning showed an improved 28-day outcome, compared with non-responders by Kaplan-Meier survival estimates (p < 0.05 by the log-rank test), but the PaCO2 responders did not.
Pro Arm
Zusammenfassende Beurteilung: QE 3**
The early oxygenation improvement after prone positioning might be associated with an improved 28-day outcome and may be an indicator to maintain prolonged prone positioning in patients with severe ARDS Limitations: Design, small number of patients

Referenz
Nr. 55
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Leamsson Intensive Care Med (2006) 32:1987–1993 Does gas exchange response to prone position predict mortality in hypoxemic acute respiratory failure?
Retrospective investigation from a randomized controlled multicenter study (Guerin et al 2004)
370 prone position sessions Arterial blood gas was measured in supine position before proning and in prone position at the end of the session. Gas exchange improvement was defined as increase in the PaO2/FIO2 ratio of more than 20% (PaO2R) or decrease in PaCO2 of more than 1 mmHg (PaCO2R).
Aims: (a) to study the relationship between gas exchange response during first PP session to patient outcome and (b) to characterize the factors associated with PaO2 and PaCO2 response during the first PP session.
The 28-day mortality rate was 26.5% in PaO2R–PaCO2R, 31.7% in PaO2R–PaCO2NR, 38.9% in PaO2NR–PaCO2R, and 43% in PaO2NR–PaCO2NR (log-rank 14.02, p = 0.003). In a Cox proportional hazards model the gas exchange response was a significant predictor to patient outcome with a 82.5% increase in risk of death in the case of PaO2NR–PaCO2R or PaO2NR–PaCO2NR, relative to the gas exchange improvement response (odds ratio 1.825). However, after adjusting for the difference in oxygenation between day 2 and day 1 the gas exchange response does no longer reach significance.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
In patients with hypoxemic acute respiratory failure initial improvement in gas exchange in the first PP session was associated with a better outcome, but this association disappeared when the change in oxygenation from day 1 to day 2 was taken into account, suggesting that underlying illness was the most important predictor of mortality in this patient population.

Referenz
Nr. 56
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Mancebo et al Am J Respir Crit Care Med Vol 173. pp 1233–1239, 2006 A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome
RCT 136 patients within 48 h of tracheal intubation for severe ARDS
6 (2 died sp, 1 died in pp, 1 data lacking, 1 high PCWP)
Continuous prone
ventilation treatment for 20 h/d.
Supine position The intensive care unit mortality was 58% (35/60) in the patients ventilated supine and 43% (33/76) in the patients ventilated prone (p = 0.12). The latter had a higher simplified acute physiology score II at inclusion. Multivariate analysis showed that simplified acute physiology score II at inclusion (odds ratio [OR], 1.07; p = 0.001), number of days elapsed between ARDS diagnosis and inclusion (OR, 2.83; p = 0.001), and randomization to supine position (OR, 2.53; p = 0.03) were independent risk factors for mortality. A total of 718 turning procedures were done, and prone position was applied for a mean of 17 h/d for a mean of 10 d. A total of 28 complications were reported, and most were rapidly
reversible
Pro Arm
76 Prone 60 Supine
Zusammenfassende Beurteilung: QE 1b****
Prone ventilation is feasible and safe, and may reduce mortality in patients with severe ARDS when it is initiated early and applied for most of the day.

Referenz
Nr. 57
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Marini et al. Intensive Care Med (2010) 36:559–561 Prone positioning for ARDS: defining the target
Editorial
Pro Arm
Zusammenfassende Beurteilung: QE 4**
Editorial über die großen Studien von Mancebo, Gattinoni, Sud, Guerin

Referenz
Nr. 58
Studientyp Teilnehmer Intervention Zielgröße Hauptergebnis
insgesamt Mekontso Intensive Care Med (2011) 37:430–434 Trans-esophageal echocardiography in prone position during severe acute respiratory distress syndrome
Prospective study 34 patients with ARDS
10 healthy volunteers
16 patients underwent TEE in both positions
TEE in pp
Two-microphone acoustic reflection method to assess the duct cross-section of the oropharyngeal tract in ten healthy adult volunteers in three positions: supine, and PP with head rotation either to the right or to the left (see ESM).
The minimal area of the
oropharyngeal cavity (from incisors to the glottis) was calculated for all subjects in each position.
Feasibility
Tolerance,
Therapeutic implications
Probe insertion was successful in all but one patient, and vital signs did not change during insertion. All standard views and measures could be obtained, except for patent foramen ovale in one patient, and cardiac output assessment in four patients. TEE examinations were all conclusive and led to therapeutic change proposal in 23 patients (70%). TEE was performed in both supine and PP in 16 patients within a median delay of 3 days. There was no difference between the two examinations in terms of feasibility, tolerance, therapeutic implication, and image quality. In ten healthy individuals, we also explored the minimal cross-sectional area of the oropharyngeal duct with the acoustic reflection technique; it was found identical in supine and PP.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
TEE can be performed safely and efficiently in severe ARDS patients in PP. PP is not associated with a significant change in the oropharyngeal tract cross-section in healthy individuals.

Referenz
Nr. 59
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n)
Hauptergebnis
insgesamt Mentzelopoulos Eur Respir J 2005; 25: 259–268 Prone position improves expiratory airway mechanics in severe chronic bronchitis
Observational study A total of 10 severe chronic
bronchitis patients Partitioned respiratory system (RS)
mechanics during iso-flow experiments (flow50.91 L/s, tidal volume(VT) varied within 0.2–1.2 L), hemodynamics, gas-exchange, expiratory airway resistance (Raw,exp), functional residual capacity (FRC), change in FRC (DFRC), end-expiratory lung volume (EELV), expiratory airway resistance at EELV (Raw,exp,EELV), intrinsic positive end-expiratorypressure (PEEPi), and mean end-expiratory flow were determined in baseline semirecumbent (SRBAS), prone, and post-prone semirecumbent (SRPP) postures.
Pronation versus SRBAS resulted in significantly reduced Raw,exp (at VT ≥0.8 L), Raw,exp,EELV (18.3±1.4 versus 31.6±2.6 cm H2O× L-1×s-1), inspiratory airway resistance (at VT≥1.0 L), static lung elastance (at VT ≤ 0.6 L), ‘‘additional’’ RS/lung resistance (at a range of VTs), DFRC (0.35±0.03 versus 0.47± 0.03 L), EELV (4.92±0.49 versus 5.65±0.65 L), RS/lung PEEPi 6.7±1.1/5.4±0.6 versus 8.9±1.7/7.8¡1.1 cm H2O), mean end-expiratory flow (63.9±4.2 versus 47.9±4.0 mL×s-1), and shunt fraction (0.16±0.03 versus 0.21±0.03); benefits were reversed in SRPP. In severe chronic bronchitis, prone positioning reduces airway resistance and dynamic hyperinflation.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)
Pronation of anaesthetised, volume-controlled mode ventilated, severe chronic bronchitis patients reduces airway resistance and attenuates dynamic hyperinflation. This is probably attributable to improved parenchyma mechanics inducing an increase in airway calibre during the respiratory cycle.

Referenz
Nr. 60
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Mentzelopoulos Eur Respir J 2005; 25: 534–544 Prone position reduces lung stress and strain in severe acute respiratory distress syndrome
Observational study A total of 10 anesthetised/paralysed, mechanically ventilated
Mechanically ventilation (VT59.0,0.9 mL/kg predicted body weight; flow50.91¡0.04 L/s1; PEEP59.4,1.3 cmH2O) patients with early/severe ARDS were studied in pre-prone semirecumbent (SRBAS), prone, and SRPP positions. Partitioned respiratory mechanics were determined during iso-flow (0.91 L?s-1) experiments (VT varied within
0.2–1.0 L), along with hemodynamics, gas exchange, and EELV.
Compared with SRBAS, pronation/SRPP resulted in reduced peak/plateau PL at VTs ≥0.6 L; static lung elastance lung resistance decreased and chest wall elastance (in prone position) increased EELV increased (23–33%); VT/EELV decreased (27–33%); Arterial oxygen tension/inspiratory oxygen fraction and arterial carbon dioxide tension improved (21–43/10–14%, respectively), and shunt fraction/physiological dead space decreased (21–50/20–47%, respectively).
Pro Arm
Zusammenfassende Beurteilung: QE:3**(*)
In early/severe acute respiratory distress syndrome, pronation under positive end-expiratory pressure optimization may reduce ventilator-induced lung injury risk. Pronation benefits may be maintained in post-prone semirecumbent position.

Referenz
Nr.61
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis
insgesamt
Michelet et al.
Critical Care Vol 9
No 3
Influence of support on intra-abdominal pressure, hepatic kinetics of indo cyanine green and extravascular lung water during prone positioning in patients with ARDS: a randomized crossover study
;
prospective, randomized, crossover study
20 patients with ARDS Measurements were made at baseline and repeated after 1 and 6 hours of two randomized periods of 6 hours of PP with one of two support types: conventional foam mattress or air-cushioned mattress.
After logarithmic transformation of the data, an analysis of variance (ANOVA) showed that IAP and PDRICG were significantly influenced by the type of support during PP with an increase in IAP (P < 0.05 by ANOVA) and a decrease in PDRICG on the foam mattress (P < 0.05 by ANOVA). Conversely, the measurements of EVLW did not show significant modification between the two supports whatever the posture. The ratio of the arterial oxygen tension to the fraction of inspired oxygen significantly increased in PP (P < 0.0001 by ANOVA) without any influence of the support.
Pro Arm
Zusammenfassende Beurteilung: QE3***
In comparison with a conventional foam mattress, the use of an air-cushioned mattress limited the increase in IAP and prevented the decrease in PDRICG related to PP in patients with ARDS. Conversely, the type of support did not influence EVLW or oxygenation. Comment Puttensen: The increase in IAP in the prone position depends on the used mattress type. Compared with air-cushion beds, conventional foam mattresses resulted in a greater increase in IAP which was associated with a decrease in the plasma diappearance rate of indocyanin green (PDRICG) indicating inadequate heptosplanchnic function.
Referenz
Nr. 62
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Mounier et al Eur Respir J 2010; 35: 795–804 Study of prone positioning to reduce ventilator-associated pneumonia in hypoxaemic patients
Prospective observational study
multicenter
2409 patients
Inclusion criteria MV for o2 days, started within 48 h after ICU admission, with an arterial oxygen tension/inspiratory oxygen fraction ratio (Pa,O2/FI,O2) ≤ 300 during the first 2 days of MV with bilateral infiltrates with classic absence of clinical evidence of left atrial hypertension according to the protocol of each ICU.
MV: Tidal volume was set to maintain a plateau pressure of ,30 cmH2O in most patients and f35 cmH2O in all patients
Prone position for
6 h/d Patients ventilated only in supine position, supine position always semirecumbent
VAP Risc factors:
male sex; pneumonia diagnosis at admission; chronic respiratory failure; acute respiratory failure at admission; septic shock at admission; use of vasoactive agents within the first 48 h in the ICU; temperature; cardiac frequency (fC); Pa,O2/FI,O2 ratio; and the need for an arterial catheter. VAP incidence was similar in the PP and control groups (24 versus 13 episodes, 1,000 patientdays MV-1 respectively, p=0.14). After adjustment, PP did not decrease VAP occurrence (HR 1.64 (95% CI 0.70–3.84); p=0.25) but significantly delayed hospital mortality (HR 0.56 (95% CI 0.39– 0.79); p=0.001), without decreasing 28-day mortality (37% in both groups). Post hoc analyses indicated that PP did not protect against VAP but, when used for >1 day, might decrease mortality and benefit the sickest patients (Simplified Acute Physiology Score .50).
Pro Arm
201 (8%)
received PP
Zusammenfassende Beurteilung: QE 2b-3**(*)
In ICU patients with hypoxaemic acute respiratory failure, PP had no effect on the risk of VAP. PP delayed mortality without decreasing 28-day mortality. PP .1 day might decrease mortality, particularly in the sickest patients.

Referenz
Nr. 63
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Hauptergebnis
insgesamt Muellenbach Perfusion 2014, Vol. 29(2) 171– 177 Kinetic therapy in ARDS patients treated with extracorporeal membrane oxygenation
Retrospective case series
nine patients with severe ARDS The patients received 20 (15–86) hours (median, 25th and 75th percentile) of positioning therapy while being treated with vvECMO Positioning therapy included 135 degrees prone, prone positioning and continuous lateral rotational therapy.
The initial PaO2/FiO2 index was 64 (51–67) mmHg and the arterial carbon dioxide tension was 60 (50–71) mmHg. During the first three days, the oxygenation index improved from 47 (41–47) to 12 (11–14) cmH2O/mmHg. The lung compliance improved from 20 (17–28) to 42 (27–43) ml/cmH2O. Complications related to positioning therapy were facial oedema (n=9); complications related to vvECMO were entrance of air (n=1) and pump failure (n=1). However, investigation of root causes revealed no association with the positioning therapy and had no documented effect on the outcome.
Pro Arm
Zusammenfassende Beurteilung: QE 4**
The reported cases suggest that positioning therapy can be performed safely in ARDS patients treated with vvECMO, providing appropriate precautions are in place and a very experienced team is present.

Referenz
Nr. 64
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Nekludov Acta Anaesthesiol Scand 2006; 50: 932–936 Oxygenation and cerebral perfusion pressure improved in the prone position
prospective study Eight patients with traumatic brain injury or subarachnoid hemorrhage (SAH) 36-73a GCS 3-8 Exclusion criteria: high or unstable ICP (intermittent drainage of liquor to maintain ICP below 20 mmHg, circulatory unstable, e.g. severe dysrhythmias, or treated with high doses of inotrope agents, as patients on hemodialysis
mechanically ventilated at a pressure-trigged volume control mode FiO2 and other settings of mechanical ventilation were unchanged patients were placed onto a Stryker frame (Stryker SurgiBed 965; Stryker, Kalamazoo, MI), which can be rotated 1808, shifting from supine to prone and back again. The entire bed was sloped, with the head of the patient 108 upward, regardless of supine or prone positioning A continuous infusion of norepinephrine was used to keep cerebral perfusion pressure (CPP) at 60 mmHg or higher.
A significant improvement in PaO2 was observed in the prone position, from 12.6 _ 1.4 kPa to 15.7 _ 3.2 kPa (P ¼ 0.02). Both intracranial pressure and mean arterial pressure increased in the prone position, from 12 _ 6 to 15 _ 4 mmHg (P ¼ 0.03) and from 78 _ 8 to 88 _ 8 mmHg (P ¼ 0.005), respectively. Arterial pressure increased to a greater extent than ICP, resulting in improved CPP, from 66 _ 7 to 73 _ 8 mmHg (P ¼ 0.03) in the prone position.
Pro Arm
Zusammenfassende Beurteilung: QE 3***
The prone position can be used to improve the oxygenation as well as CPP in patients with traumatic brain injury or SAH. However, this method results in raised ICP, and should be used cautiously in patients with reduced intracranial compliance.

Referenz
Nr. 65
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Hauptergebnis
insgesamt Oczensky Crit Care Med 2005 Vol. 33, No. 1 Recruitment maneuvers during prone positioning in patients with acute respiratory distress syndrome
Prospective, interventional study.
15 Patients with early ARDS After 6 hrs of pp, a sustained inflation was performed with 50 cm H2O maintained for 30 s. Data were recorded in supine position, after 6 h of prone positioning, at 3, 30, and 180 mins following the sustained inflation.
Response to prone positioning was observed in nine of 15 patients leading to an improvement of PaO2/FIO2 (147 ±37 torr vs. 225± 77 torr, p = .005) and venous admixture (35.4±8.3% vs. 28.9±9.8%, p=.001). Six patients did not respond to prone positioning. Following the sustained inflation, the responders to prone positioning showed a further increase of PaO2/FIO2 and decrease of venous admixture at 3 mins (PaO2/FIO2, 225±77 torr vs. 368± 90 torr, p = .018; venous admixture, 28.9 ± 9.8% vs. 18.9 ±6.7%, p = .05). In all six non-responders to prone positioning, an improvement of PaO2/FIO2 and venous admixture occurred at 3min following the sustained inflation (128±18 torr vs. 277±59 torr, p=.03; venous admixture, 34.2±6.0% vs. 23.8±6.3%, p=.05). The beneficial effects of the sustained inflation remained significantly elevated over 3 h in responders and non-responders to prone positioning.
Pro Arm
Zusammenfassende Beurteilung:QE 3**(*)
In patients with early extrapulmonary acute respiratory distress syndrome, a sustained inflation performed after 6 hrs of prone positioning induced further and sustained improvement of oxygenation and venous admixture in both responders and nonresponders to prone positioning.

Referenz
Nr. 66
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle
Zielgröße(n) Hauptergebnis
insgesamt Papazian Crit Care Med 2005 Vol. 33, No. 10 Comparison of prone positioning and high-frequency oscillatory ventilation in patients with acute
Randomized prospective
39 patients with ARDS Eligible patients met the following criteria: PaO2/FIO2 ratio <150 mm Hg while on PEEP ≥5 cm H2O, bilateral radiographic pulmonary infiltrates, and pulmonary artery occlusion pressure of ≤18 mm Hg.
After 12 h on conventional lung-protective mechanical ventilation (tidal volume 6 mL/kg of ideal body weight, plateau pressure not exceeding the upper inflection point, and a maximum of 35 cm H2O; supine-CV), 39 patients were randomized to receive one of the following 12-hr periods: conventional lung-protective mechanical ventilation in prone position (prone-CV), HFOV in supine position (supine-HFOV), or HFOV in prone position (prone-HFOV).
Prone-CV (from 138 ± 58 mm Hg to 217 ± 110 mm Hg, p < .0001) and prone-HFOV (from 126 ± 40 mm Hg to 227 ± 64 mm Hg, p < 0.0001) improved the PaO2/FIO2 ratio whereas supine-HFOV did not alter the PaO2/FIO2 ratio (from 134 ± 57 mm Hg to 138 ± 48 mm Hg). The oxygenation index ([mean airway pressure x FIO2 x 100]/PaO2) decreased in the prone-CV and prone-HFOV groups and was lower than in the supine-HFOV group. Interleukin-8 increased significantly in the bronchoalveolar lavage fluid (BALF) in supine-HFOV and prone-HFOV groups compared with prone-CV and supine-CV. Neutrophil counts were higher in the supine-HFOV group than in the prone-CV group.
Pro Arm
Zusammenfassende Beurteilung: QE:3***
Although HFOV in the supine position does not improve oxygenation or lung inflammation, the prone position increases oxygenation and reduces lung inflammation in ARDS patients. Prone-HFOV produced similar improvement in oxygenation like prone-CV but was associated with higher BALF indexes of inflammation. In contrast, supine-HFOV did not improve gas exchange and was associated with enhanced lung inflammation.

Referenz
Nr. 67
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Protti Intensive Care Med (2009) 35:1011–1017 Relationship between gas exchange response to prone position and lung recruitability during acute respiratory
Retrospective analysis 32 patients who underwent prone ventilation within 72 h from the assessment of lung recruitability by CT scan.
Gas exchange variables (PaO2:FiO2 and arterial carbon dioxide tension, PaCO2), minute ventilation, positive endexpiratory pressure (PEEP), respiratory system compliance (the ratio of tidal volume to the difference between inspiratory plateau pressure and PEEP) in supine position and after an average period of 4 h of prone position, while the ventilator setting was kept constant. Whole lung CT scans obtained at 5 and 45 cm of water of airway pressure with the patient lying supine were analyzed. Potential lung recruitability was defined as the difference in the amount of non-aerated lung tissue (density equal to or above -100 HU) at these two levels of airway pressure, expressed as the percentage of total lung weight. We also studied the regional recruitability of the ventral and dorsal halves of the lung, ideally separated by a transverse line crossing the vertical mid-point in each sectional image.
No relationship was found between increased oxygenation in prone position and lung recruitability. In contrast, the decrease of PaCO2 was related with lung recruitability (R2 0.19; P = 0.01). Patients who decreased their PaCO2 more than the median value (-0.9 mmHg) had a greater lung recruitability (19 ± 16 vs. 8 ± 6%; P = 0.02), higher baseline PaCO2 (48 ± 8 vs. 41 ± 11 mmHg; P = 0.07), heavier lungs (1,968 ± 829 vs. 1,521 ± 342 g; P = 0.06) and more non-aerated tissue (1,009 ± 704 vs. 536 ± 188 g; P = 0.02) than those who did not.
Pro Arm
Zusammenfassende Beurteilung: QE : 3**(*)
During prone position, changes in PaCO2, but not in oxygenation, are associated with lung recruitability which, in turn, is associated with the severity of lung injury.

Referenz
Nr. 68
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Hauptergebnis
insgesamt Reignier et al. Intensive Care Med (2005) 31:1128–1131 Short-term effects of prone position in chronic obstructive pulmonary disease patients with severe acute hypoxemic and hypercapnic respiratory failure
Prospective observational
study
11 consecutive COPD patients with persistent hypoxemia (PaO2/FIO2 ≤200 mmHg with FIO2 ≥0.6) and hypercapnia requiring invasive mechanical ventilation. Patients with ARDS or left ventricular failure were excluded. Mean age was 73±11 years, mean weight 86±31 kg, mean SAPS II 53±10, and ICU mortality 36%
Patients were turned every 6 h.
A response to PP (20% or greater PaO2/FIO2 increase) was noted in 9 (83%) patients. Blood gases were measured in the PP and supine (SP) positions 3 h after each turn, for 36 h, yielding six measurements sets (SP1, PP1, SP2, PP2, SP3, and PP3). PaO2/FIO2 was significantly better in PP: 190±26 vs. 113±9 mmHg for PP1/SP1, 175±22 vs. 135±16 mmHg for PP2/SP2, and 199±24 vs. 151±13 mmHg for PP3/SP3. After PP1 PaO2/FIO2 remained significantly improved, and the PaO2/ FIO2 improvement from SP1 to SP2 was linearly related to PaO2/FIO2 during PP1 (r=0.8). The tracheal aspirate volume improved significantly from SP1 to PP1. PaCO2 was not significantly affected by position.
Pro Arm
Zusammenfassende Beurteilung: QE:3 **

Referenz
Nr. 69
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Reignier et al. Clin Nutr Before-after study of a standardized ICU protocol for early enteral feeding in patients turned in the prone position
Observational intervention study
Eligible patients receiving EN and mechanical ventilation in PP were included within 48h after intubation in a before-after study.
Patients were semi-recumbent when supine.
Intolerance to EN was defined as residual gastric volume greater than 250ml/6h or vomiting.
In the before group (n=34), the EN rate was increased by 500ml every 24h up to 2000ml/24h;
Patients were flat when prone and received erythromycin (250mgIV/6h) to treat intolerance.
In the intervention group (n=38), the EN rate was increased by 25ml/h every 6h to 85ml/h, 25 degrees head elevation was used in PP, and prophylactic erythromycin was started at the first turn.
Compared to the before group, larger feeding volumes were delivered in the intervention group (median volume per day with PP, 774ml [IQR 513-925] vs. 1170ml [IQR 736-1417]; P<0.001) without increases in residual gastric volume, vomiting, or ventilator-associated pneumonia.
Pro Arm
n=34 (before) n=38 (supine)
Zusammenfassende Beurteilung: QE 3**(*)
An intervention including PP with 25 degrees elevation, an increased acceleration to target rate of EN, and erythromycin improved EN delivery.

Referenz
Nr. 70
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Hauptergebnis
insgesamt Richard et al. Crit Care Med 2008 Vol. 36, No. 8 Effects of prone position and positive end-expiratory pressure on lung perfusion and ventilation
Experimental study 6 pigs After oleic acid-induced lung injury, all animals were studied in supine and prone position at both positive end-expiratory pressure 0 and positive end-expiratory pressure 10 cm H2O.
Positive end-expiratory pressure was associated with significant alveolar recruitment (130 ± 85 and 65 ± 29 g of lung in supine and prone position, respectively [p < 0.05 vs. 0]), whereas recruitment induced by posture was not statistically significant (77 ± 97 g with positive end-expiratory pressure 0 and 13 ± 19 g with positive end-expiratory pressure 10 [p > 0.05 vs.
0]).
Regardless the posture, positive end-expiratory pressure redistributed both perfusion and ventilation toward dependent regions. Recruitment by positive end-expiratory pressure was restricted to dorsal regions in supine position, but extended diffusely along the ventral-to-dorsal dimension in prone position. Prone position was associated with recruitment in dorsal regions with concomitant derecruitment in ventral regions, magnitude of this being reduced by positive end-expiratory pressure. Prone position redistributed ventilation toward dorsal and ventral regions at positive end-expiratory pressure 0 and positive endexpiratory pressure, respectively. Prone position redistributed perfusion toward ventral regions, to an extent amplified by positive end-expiratory pressure.
Pro Arm
Zusammenfassende Beurteilung: QE 3**
Positive end-expiratory pressure and posture act synergistically by redistributing lung regional perfusion toward ventral regions, but have antagonistic effects on regional ventilation.

Referenz
Nr. 71
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Robak et al. Critical Care 2011, 15:R230 Short-term effects of combining upright and prone positions in patients wi th ARDS: a prospective randomized study
Prospective randomized crossover trial
After turning them prone from a supine position, we randomized the patients to a prone position or combined prone and upright position. After 2 hours, the position was changed to the other one for another 6h. The gas exchange and static compliance of the respiratory system, lungs, and chest wall were assessed in the supine position as well as every hour in the prone position.
The PaO2/FiO2 ratio improved significantly from the supine to the prone position and further significantly increased with additional upright position. Fourteen (70%) patients were classified as responders to the prone position, whereas 17 (85%) patients responded to the prone plus upright position compared with the supine position (P = n.s.). No statistically significant changes were found with respect to compliance.
Pro Arm
Zusammenfassende Beurteilung: QE 2b***
Combining the prone position with the upright position in patients with ALI or ARDS leads to further improvement of oxygenation Commentary: In summary, the use of prone and upright positioning should not be considered as opposing and mutually exclusive strategies, but more as complementary ones. Even if the level of evidence is debatable, combining prone and upright positioning seems to enhance the response rate in terms of oxygenation. Whenever the prone position is used, combining it with the upright position should be considered to improve oxygenation further and limit lung derecruitment. Th is strategy is easy to implement at no additional cost and with a low risk of major complications.

Referenz
Nr. 72
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Hauptergebnis
insgesamt Romero et al Journal of Critical Care (2009) 24, 81–88 Extended prone position ventilation in severe acute respiratory distress syndrome: a pilot feasibility study
Prospective interventional study
Fifteen consecutive patients with severe ARDS, previously unresponsive to positive end expiratory pressure adjustment, were treated with PPV
Prone position ventilation for 48 hours or until the oxygenation index was 10 or less (extended PPV).
The elapsed time from the initiation of mechanical ventilation to pronation was 35 ± 11 hours. Prone position ventilation was continuously maintained for 55 ± 7 hours. Two patients developed grade II pressure ulcers of small extent. None of the patients experienced life-threatening complications or hemodynamic instability during the procedure. The patients showed a statistically significant improvement in PaO2/FiO2 (92 ± 12 vs 227 ± 43, P < .0001) and oxygenation index (22 ± 5 vs 8 ± 2, P < .0001), reduction of PaCO2 (54 ± 9 vs 39 ± 4, P < .0001) and plateau pressure (32 ± 2 vs 27 ± 3, P < .0001), and increment of the static compliance (21 ± 3 vs 37 ± 6, P < .0001) with extended PPV. All the parameters continued to improve significantly while they remained in prone position and did not change upon returning the patients to the supine position.
Pro Arm
Zusammenfassende Beurteilung: QE: 3**(*) The results obtained suggest that extended PPV is safe and effective in patients with severe ARDS when it is carried out by a trained staff and within an established protocol. Extended PPV is emerging as an effective therapy in the rescue of patients from severe ARDS.

Referenz
Nr. 73
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße Hauptergebnis
insgesamt Grensemann/ Sakka Anesth Analg 2013;116:820–6 The influence of prone positioning on the accuracy of calibrated and uncalibrated pulse contour-derived cardiac index measurements
Prospective observational
16 critically ill and mechanically ventilated patients (11 men, 5 women, aged 20–71 years) with acute lung injury or acute respiratory distress syndrome.
Patients were monitored by TPTD with an integrated calibrated pulse contour technique (PiCCO®) and by uncalibrated pulse contour analysis (FloTrac/Vigileo™). Before prone positioning, cardiac index (given in L·min−1·m−2) was measured by TPTD (CITPTD) and CIPC was calibrated. After positioning, CIPC and CIVIG were read from the monitor and CITPTD was measured. After 8 to 10 hours, prone positioning was completed and measurements were performed analogously. Bland-Altman analysis based on a random-effects model was used to calculate limits of agreement (LOA) and percentage errors. Polar plots were used for trend analysis. Baseline measurements (SUPINE1) were obtained 10 minutes before the patient was brought from supine to 135° prone position. A second time point (PRONE1) was defined 10 minutes after prone positioning, to allow system stabilization. Between 8 and 10 hours after prone positioning, a third time point (PRONE2) was defined 10 minutes before returning the patient into supine position. A last measurement (SUPINE2) was taken 10 minutes after returning the patient into supine position.
Supine CITPTD was 3.3 ± 0.9 (mean ± SD) and CIVIG was 3.1 ± 0.8. After proning, CIPC was 3.5 ± 0.8, CIVIG 3.3 ± 0.8, and CITPTD 3.6 ± 0.8. Before repositioning, CITPTD was 3.5 ± 0.7 and CIVIG 3.3 ± 1.0. After repositioning, CITPTD was 3.1 ± 0.7, CIPC 3.3 ± 0.7, and CIVIG 2.9 ± 0.6. Mean bias pooled for proning and repositioning was −0.1 (LOA −0.7 to 0.6) for CIPC (percentage error 19%) and 0.3 (LOA −1.3 to 1.9) for CIVIG (percentage error 48%). Changes in CI were too small for trending analysis.
Pro Arm
Zusammenfassende Beurteilung: QE 3**
Although calibrated CI measurements are only marginally influenced by prone positioning, according to the criteria of Critchley and Critchley, uncalibrated CI values show a degree of error, too high to be considered clinically acceptable.
Referenz
Nr. 74
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Sharma S. Clinical Evidence 2010;11:1511 Acute respiratory distress syndrome
Review 3 systematical reviews and 2 RCT´s
Pro Arm
Zusammenfassende Beurteilung: QE 4*** guter Review folgende Studien werden bzgl. Bauchlage berücksichtigt:
Kopterides P, Siempos II, Armaganidis A, et al. Prone positioning in hypoxemic respiratory failure: meta-analysis of randomized controlled trials. J Crit Care 2009;24:89–100.[ Alsaghir AH, Martin CM. Effect of prone positioning in patients with acute respiratory distress syndrome: a meta-analysis. Crit Care Med 2008;36:603–609.[ Sud S, Sud M, Friedrich JO, et al. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ: Can Med Assoc J 2008; 178:1153–1161. Taccone P, Pesenti A, Latini R, et al. Prone positioning in patients with moderate and severe acute respiratory distress syndrome: a randomized controlled trial. JAMA 2009;302:1977–1984 Fernandez R, Trenchs X, Klamburg J, et al. Prone positioning in acute respiratory distress syndrome: a multicenter randomized clinical trial. Intensive Care Med 2008;34:1487–1491
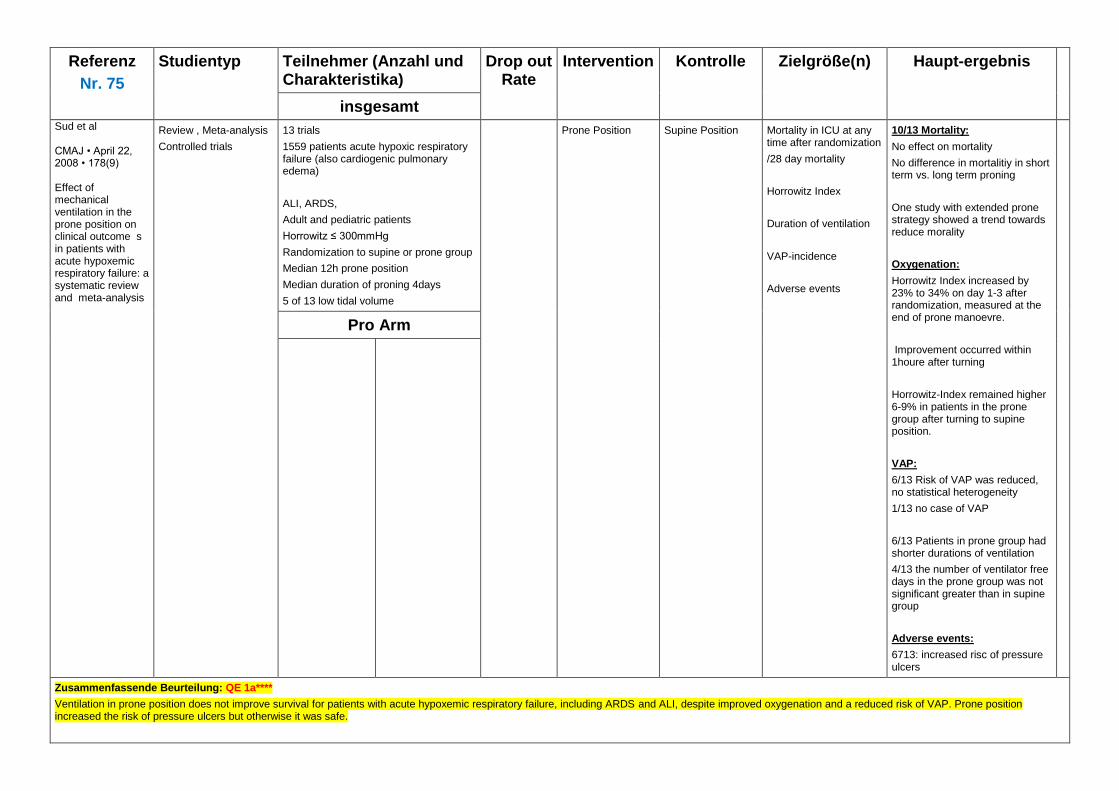
Referenz
Nr. 75
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
insgesamt Sud et al CMAJ • April 22, 2008 • 178(9) Effect of mechanical ventilation in the prone position on clinical outcome s in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis
Review , Meta-analysis
Controlled trials
13 trials
1559 patients acute hypoxic respiratory failure (also cardiogenic pulmonary edema)
ALI, ARDS,
Adult and pediatric patients
Horrowitz ≤ 300mmHg
Randomization to supine or prone group
Median 12h prone position
Median duration of proning 4days
5 of 13 low tidal volume
Prone Position Supine Position Mortality in ICU at any time after randomization
/28 day mortality
Horrowitz Index
Duration of ventilation
VAP-incidence
Adverse events
10/13 Mortality:
No effect on mortality
No difference in mortalitiy in short term vs. long term proning
One study with extended prone strategy showed a trend towards reduce morality
Oxygenation:
Horrowitz Index increased by 23% to 34% on day 1-3 after randomization, measured at the end of prone manoevre.
Improvement occurred within 1houre after turning
Horrowitz-Index remained higher 6-9% in patients in the prone group after turning to supine position.
VAP:
6/13 Risk of VAP was reduced, no statistical heterogeneity
1/13 no case of VAP
6/13 Patients in prone group had shorter durations of ventilation
4/13 the number of ventilator free days in the prone group was not significant greater than in supine group
Adverse events:
6713: increased risc of pressure ulcers
Pro Arm
Zusammenfassende Beurteilung: QE 1a****
Ventilation in prone position does not improve survival for patients with acute hypoxemic respiratory failure, including ARDS and ALI, despite improved oxygenation and a reduced risk of VAP. Prone position increased the risk of pressure ulcers but otherwise it was safe.

Referenz
Nr. 76
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Sud et al. Intensive Care Med (2010) 36:585–599 Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta-analysis
Metaanalyse
(Fernandez, Voggenreiter, Chan, Taccone, Mancebo, Guerin, Gattinoni, Beuret, Watanabe, Curley /Päd)
Ten trials (N = 1,867 patients) met inclusion criteria Adults or postneonatal children with acute hypoxemic respiratory failure (defined by PaO2/FiO2 ≤ 300 mmHg); randomly assigned patients to two or more groups, including a treatment group, ventilated at least once in the prone position and a controlgroup ventilated in the supine position, with an intervention period of at least 48 h in duration; and reported any of our primary or secondary outcomes
The primary outcome was hospital mortality in patients with AHRF and PaO2/FiO2\100 mmHg.
Prone ventilation reduced mortality in patients with PaO2/ FiO2<100 mmHg [risk ratio (RR) 0.84, 95% confidence interval (CI) 0.74–0.96; p = 0.01; seven trials, N = 555] but not in patients with PaO2/FiO2 ≥100 mmHg (RR 1.07, 95% CI 0.93–1.22; p = 0.36; seven trials, N = 1,169). Risk ratios differed significantly between subgroups (interaction p = 0.012). Post hoc analysis demonstrated statistically significant improved mortality in the more hypoxemic subgroup and significant differences between subgroups using a range of PaO2/FiO2 thresholds up to approximately 140 mmHg Prone ventilation improved oxygenation by 27–39% over the first 3 days of therapy but increased the risks of pressure ulcers (RR 1.29, 95% CI 1.16–1.44), endotracheal tube obstruction (RR 1.58, 95% CI 1.24–2.01), and chest tube dislodgement (RR 3.14, 95% CI 1.02–9.69). There was no statistical between-trial heterogeneity for most clinical outcomes
Pro Arm
Zusammenfassende Beurteilung: QE 1a****
Prone ventilation reduces mortality in patients with severe hypoxemia. Given associated risks, this approach should not be routine in all patients with AHRF, but may be considered for severely hypoxemic patients

Referenz
Nr. 77
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Taccone JAMA, November 11, 2009—Vol 302, No. 18 Prone positioning in patients with moderate and severe acute respiratory d istress syndrome: a randomized controlled trial
RCT The Prone-Supine II Study, a multicenter, unblinded, randomized controlled trial conducted in 23 centers in Italy and 2 in Spain. Patients were 342 adults with ARDS receiving mechanical ventilation, enrolled from February 2004 through June 2008 and prospectively stratified into subgroups with moderate (n=192) and severe (n=150) hypoxemia. .
Prone Position for 20h/d using a rotational bed
tidal volumes be limited to a maximum of 8 mL/kg of ideal body weight and airway plateau pressures be limited to 30 cmH2O. During the 28-day study period, Sequential Organ Failure Assessment (SOFA) scores17 were collected daily to evaluate the severity of organ dysfunction
Supine Position
In the supine group, prone positioning could be used only as a rescue maneuver in cases of life-threatening hypoxemia (eg, PaO2 ≤55 mm Hg at FIO2=1.00 and PEEP ≥15 cm H2O).
The primary outcome was 28-day all-cause mortality. Secondary outcomes were 6-month mortality and mortality at intensive care unit discharge, organ dysfunctions, and the complication rate related to prone positioning
Prone and supine patients from the entire study population had similar 28- day (31.0% vs 32.8%; relative risk [RR], 0.97; 95% confidence interval [CI], 0.84- 1.13; P=.72) and 6-month (47.0% vs 52.3%; RR, 0.90; 95% CI, 0.73-1.11; P=.33) mortality rates, despite significantly higher complication rates in the prone group. Outcomes were also similar for patients with moderate hypoxemia in the prone and supine groups at 28 days (25.5% vs 22.5%; RR, 1.04; 95% CI, 0.89-1.22; P=.62) and at 6 months (42.6% vs 43.9%; RR, 0.98; 95% CI, 0.76-1.25; P=.85). The 28-day mortality of patients with severe hypoxemia was 37.8% in the prone and 46.1% in the supine group (RR, 0.87; 95% CI, 0.66-1.14; P=.31), while their 6-month mortality was 52.7% and 63.2%, respectively (RR, 0.78; 95% CI, 0.53-1.14; P=.19).
Pro Arm Prone 168
Supine 174
Zusammenfassende Beurteilung: QE 1b****
Data from this study indicate that prone positioning does not provide significant survival benefit in patients with ARDS or in subgroups of patients with moderate and severe hypoxemia. Kritik: Unterpowert, lange Zeitspanne bis zum Einschluß (72h) , PEEP Manipulation auf 10cmH2O

Referenz
Nr. 78
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Hauptergebnis
insgesamt Thelanderson et al. Acta Anaesthesiol Scand 2006; 50: 937–941 Prone position in mechanically ventilated patients with reduced intracranial compliance
A consecutive, prospective pilot study
11 patients admitted to the neuro intensive care unit (NICU) due to traumatic brain injury or intracerebral haemorrhage
ICP, cerebral perfusion pressure (CPP), heart rate (HR), mean arterial blood pressure (MABP), arterial partial pressure of oxygen (PaO2), arterial partial pressure of carbon dioxide (PaCO2), arterial oxygen saturation (SaO2) and respiratory system compliance were measured before, three times during and two times after the patients were placed in the prone position.
.No significant changes were
demonstrated in ICP, CPP
or MABP.
PaO2 and SaO2 were significantly
increased in the prone position.
HR was significantly increased in
the prone position and after 10 min
in the supine post-prone position
and the respiratory system
compliance was increased after 1 h
in the supine post-prone position.
Pro Arm
Zusammenfassende Beurteilung: QE 3***
Turning NICU patients from the supine to the prone position did not influence ICP, CPP or MABP, but significantly improved patient PaO2, SaO2 and respiratory system compliance.

Referenz
Nr. 79
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Tiruvoipati Efficacy of prone ventilation in adult patients with acute respiratory failure: a meta-analysis
Metaanalyse:
Gattinoni 2001
Mancebo 2006
Guerin 2004
Voggenreiter 2005
Watanabe 2002
Prone ventilation was not
associated with reduction in
mortality, but improvement in
oxygenation was statistically
significant (mean difference,
21.2 mm Hg; P b .001).
There was no significant
difference in incidence of
pneumonia, ICU stay, and
endotracheal tube complications.
There was a trend toward an
increased incidence of pressure
sores in prone ventilated patients
(odds ratio =1.95; 95%
confidence interval, 0.09-4.15; P
= .08).
The data on other outcomes were
not suitable for meta-analysis.
Pro Arm
Zusammenfassende Beurteilung: QE 1a****
The results confirm that the use of prone ventilation improves oxygenation in patients with acute severe hypoxemic respiratory failure. Reduction in mortality was not shown by any of the
included studies or by the pooled analysis. No significant effect was noted in terms of reducing the incidence of ventilation-associated pneumonia or complications related to ET tubes. There
is a trend toward increased incidence of pressure sores with prone ventilation.

Referenz
Nr. 80
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Hauptergebnis
insgesamt Vieillard-Baron Chest/ 132 / 5 / November 2007 Prone positioning unloads the right ventricle in severe ARDS
Between January 1998 and December 2006, 42 ARDS patients were treated by PP to correct severe oxygenation impairment (PaO2/fraction of inspired oxygen ratio, < 100 mm Hg). Inclusion criteria: Patients with “severe” ARDS, leading to a Pao2/fraction of inspired oxygen (Fio2) ratio of < 100 mm Hg after 48 h of respiratory support with our “low-stretch” respiratory strategy; and treatment by PP during the first week of respiratory support
RV function was evaluated by bedside transesophageal echocardiography, before and after 18 h of prone-position ventilation. RV enlargement was measured by RV/left ventricular (LV) enddiastolic area ratio in the long axis. Septal dyskinesia was quantified by measuring short-axis systolic eccentricity of the LV.
Before PP, 21 patients (50%) had acute cor pulmonale, defined by RV enlargement associated with septal dyskinesia (group 1), whereas 21 patients had a normal RV (group 2). PP was accompanied by a significant decrease in airway pressure and PaCO2. In group 1, this produced a significant decrease in mean (± SD) RV enlargement (from 0.91 ± 0.22 to 0.61 ± 0.21) after 18 h of PP (p = 0.000) and a significant reduction in mean septal dyskinesia (from 1.5 ± 0.2 to 1.1 ± 0.1) after 18 h of PP (p = 0.000).
Pro Arm
Zusammenfassende Beurteilung: QE 3***
In conclusion, despite airway pressure limitation, patients with severe ARDS with a Pao2/Fio2 ratio < 100 mm Hg after 48 h of respiratory support still exhibit an abnormally high incidence of acute cor pulmonale. In this specific setting, PP, which permits an additional limitation in airway pressure, associated with a slight reduction in hypercapnia, might represent the best therapeutic strategy for treating this dreaded complication.

Referenz
Nr. 81
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Vieillard-Baron Intensive Care Med (2005) 31:220–226 Prone position improves mechanics and alveolar ventilation in acute respiratory distress syndrome
Prospective observational study
11 ARDS patients Six women and five men, with a mean age of 45±13 years, and an average body weight of 68±14 kg. No patient had previously presented chronic obstructive pulmonary disease. Inclusion criteria: Presene of ARDS as defined by the North American–European Consensus Committee criteria for ARDS; Persistence of severe oxygenation impairment defined as PaO2/FIO2≤100 mm Hg after 48 h of respiratory support Hemodynamic stability with a systolic arterial pressure greater than 90 mm Hg without any hemodynamic support presence of a substantial slow compartment (≥70 ml) measured at zero endexpiratory pressure (ZEEP) during a prolonged exhalation
Patients treated by ventilation in the prone position because of a major oxygenation impairment (PaO2/ FIO2≤100 mm Hg) mechanical and blood gas changes were measured, produced by a low PEEP (6±1 cm H2O), ventilation in the prone position, and the two combined.
All patients were sedated with midazolam and sufentanyl, and paralyzed with cisatracurium. They were all ventilated in volumecontrolled mode, with a low-stretch strategy including a limited plateau pressure (<30 cm H2O).
Ventilation in the prone position: Significantly reduced the expiratory time constant from 1.98±0.53 s at baseline with ZEEP to 1.53±0.34 s, Significantly decreased PaCO2 from 55±11 mm Hg at baseline with ZEEP to 50±7 mm Hg. This improvement in alveolar ventilation was accompanied by a significant improvement in respiratory system mechanics, and in arterial oxygenation, the latter being markedly increased by application of a low PEEP (PaO2/ FIO2 increasing from 64±19 mm Hg in supine position with ZEEP to 137±88 mm Hg in prone with a low PEEP).
Pro Arm
Zusammenfassende Beurteilung: QE:3**
In severely hypoxemic patients, prone position was able to improve alveolar ventilation significantly by reducing the expiratory time constant.

Referenz
Nr. 82
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt Voggenreiter et al. The Journal of trauma 2005 Prone positioning improves oxygenation in post-traumatic lung injury--a prospective randomized trial
prospective randomized trial
40 Patients with ALI/ARDS
Patients were documented as non-responders if the increase of the PaO2: FiO2 ratio after a maximum of 24 hours was below 10% of
baseline.
Patients in the prone group were kept prone for at least 8 h and a max of 23 h per day. Prone positioning was continued until a PaO2:FiO2 ratio of more than 300 was present in prone as well as supine position over a period of 48h Patients in the supine group were positioned according to standard care guidelines. PEEP 5-20cmH2O, TV 6-8mk/kg KG, PIP<35cmH2O
Primary end points: Duration of mechanical ventilation. This was defined as continuous breathing without pressure support or extubation for more than 24 hours Secondary end points were days with ARDS (PaO2:FiO2 ratio below 200) and ALI (PaO2:FiO2 ratio between 200 and 300), days with lung injury score (LIS) _ 2,17 course of PaO2:FiO2 ratio, Qs/Qt, total static lung compliance, PIP, PEEP, LIS, TISS-28,18 SOFA-score, sepsis,19 prevalence of pneumonia, mortality (within the 90 days of study period), and complications/adverse events and ARDS following ALI.
The duration of ventilator support did not differ significantly (30 ± 17 days in the prone group and 33±23 days in the supine group). Worst case analysis (death and deterioration of gas exchange) displayed ventilatory support for 41 ± 29 days in the prone group and 61±35 days in the supine group (p = 0.06). The PaO2:FiO2 ratio increased significantly more in the prone group in the first 4 days (p = 0.03). The prevalence of acute respiratory distress syndrome (ARDS) following acute lung injury (p = 0.03) The prevalence of pneumonia (p = 0.048) were reduced also. One patient in the prone and three patients in the supine group died due to multiorgan failure (p = 0.27).
Pro Arm
Prone:
21
Supine:
19
Zusammenfassende Beurteilung: QE 2-3 **(*)
Intermittent prone positioning was not able to reduce the duration of mechanical ventilation in this limited number of patients. However the oxygenation improved significantly over the first 4 days of treatment, and the prevalence of ARDS and pneumonia were reduced The present study is underpowered to obtain differences in ventilator time and mortality.

Referenz
Nr. 83
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Hauptergebnis
insgesamt Walkey et al. Crit Care Med. 2011 June ; 39(6): 1322–1328 Utilisation patterns and patient outcomes associated with differences in ventilator time and mortality.
Secondary analysis of multi-center, randomized-controlled trial data from the National
Heart, Lung and Blood Institute (NHLBI) ARDS Clinical Trials Network (ARDSNet).
Subjects enrolled in 6 ARDSNet trials occurring between1996–2005
2632 Patients
We compared survival between the two most commonly utilized rescue therapies: prone positioning and inhaled vasodilators. Baseline characteristics were used to generate propensity scores for receipt of either therapy. Models were then constructed using the propensity score for rescue therapy type to control for confounding due to both baseline variables and covariates measured at the time of rescue.
166/2632 (6.3%) of subjects received rescue therapy. subjects who received rescue therapy were younger, with lower PaO2/FiO2, higher PEEP, and higher peak and plateau airway pressures. In addition, those given rescue therapy were more likely to be of non-white racial background and to have pneumonia as an ALI risk factor. Though the relationship was not linear, the proportion of subjects receiving inhaled vasodilators increased over time while use of prone positioning decreased).
At the time of rescue therapy, 25% of subjects had PaO2/FiO2 less than 55, while median PaO2/FiO2 was 80. No differences were found in use of rescue therapy according to study randomization groups
Subjects who received inhaled vasodilators were younger than those treated with prone position (prone: 48.3 ± 15.0 vs. inhaled vasodilator: 40.6 ± 15.5 years, p=0.0085) and had higher peak airway pressures at time of rescue (prone: 37.0 ± 9.0 vs. inhaled vasodilator: 43.8±13.8 cm H2O, p=0.005). Significant multivariate predictors of prone positioning as compared with inhaled vasodilator therapy included presence of sepsis [OR: 0.14 (0.03–0.73), p=0.02)], peak airway pressure [(OR per 5 cm H2O increase 0.62 [(0.46–0.84), p=0.002)], and study order [OR per subsequent ARDSNet study: 0.32, (0.14–0.70),p=0.004)]. The final propensity score model for prone positioning as compared with inhaled vasodilator (Hosmer-Lemeshow chi square = 1.54, c statistic of 0.85) also included the following variables with p<0.20 : age [OR per 10 years: 1.50, (0.95–2.36), p=0.079] presence of ARDS vs. ALI [OR 7.20, (0.95–54.6), p=0.056]. Unadjusted survival was not different between subjects who received prone positioning versus inhaled vasodilators [HR 1.23, (0.68–2.12), p=0.48, n=144, Figure 2a). After adjustment for the propensity score for use of prone position versus inhaled vasodilator, prone position was associated with HR 0.87 [(0.86–2.10), p=0.76, n=86]; adjusting further for peak airway pressure and PaO2/FiO2 at time of rescue, prone positioning was associated with a HR 0.95 [(0.35–2.57), n=65, p=0.92) for survival as compared with inhaled vasodilator therapy.
Pro Arm
Zusammenfassende Beurteilung: QE 1b-2****
Rescue therapies are utilized in younger patients with more severe oxygenation deficits. Patterns of rescue therapy utilization appear to be changing over time. Within the limits of an observational study design, we did not find evidence of a survival benefit with use of rescue therapies in ALI.

Referenz
Nr. 84
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis
insgesamt Weig et al Weig et al. European Journal of Medical Research 2012, 17:30 Abdominal obesity and prolonged prone positioning increase risk of developing sclerosing cholangitis in critically ill patients with influenza A-associated ARDS
Retrospective analyse Twenty-one patients (5 female, 16 male, 46.3 ± 10.8 years) with severe ARDS due to H1N1 pneumonia were retrospectively divided into two groups, A large array of clinical data, laboratory parameters, and multi-detector computed tomography-derived measures were compared.
2 patients died
Both patient groups showed severe pulmonary impairment. Severity of disease on admission day and during the first 14 days of treatment showed no difference. The patients developing SC-CIP had a higher body mass index (BMI) (37.4 ± 6.0 kg/m2 vs. 29.3 ± 6.8 kg/m2; P = 0.029) and a higher volume of intraperitoneal fat (8273 ± 3659 cm3 vs. 5131 ± 2268 cm3; P = 0.033) and spent a longer cumulative period in the prone position during the first 14 days (165 ± 117 h vs. 78 ± 61 h; P = 0.038).
Pro Arm Presence (n = 5) of SC-CIP
Absence of SC-CIP (n = 16).
Zusammenfassende Beurteilung:QE:3**(*)
Our results suggest that obesity, intraperitoneal fat volume, and a longer cumulative duration spent in the prone position may put patients with ARDS at risk of developing SC-CIP. These results lead us to propose that the prone position should be carefully deployed, particularly in abdominally obese patients, and that frequent checks be made for early hepatic dysfunction.

Referenz
Nr. 85
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt J. Karsten/ Vahrenhorst Applied Cardiopulmonary Pathophysiology, 15: 81-86, 2011 Bedside-measurements of electrical impedance tomography and functional residual capacity during
Case study 53-year old patient,
ARDS due to fungal pneumonia
The patient was
positioned prone with
upper chest and pelvic
support to ensure free
movement of the
abdomen. The patient
was kept prone for 12
hours per day for
5 consecutive days.
The aim of this case study was to describe the ability of EIT and FRC measurement to detect changes in regional ventilation and lung volume in an ARF patient, who was treated by alveolar recruitment maneuver and intermittent prone position. An increase in FRC was observed in parallel of gas exchange improvement immediately after the recruitment.
During prone position, FRC decreased constantly while a redistribution of ventilation among dorsal lung regions was detected by EIT. These two tools were compared but without a gold standard.
Pro Arm
Zusammenfassende Beurteilung: QE:4**(*)
The reported case shows that EIT and FRC measurements are two different methods, which are difficult to compare. As they do not present a good correspondence, the respective results may be under- or overestimated but the measures indicated some tendencies. Nevertheless the combination of both could be a meaningful monitoring supplementation in the respiratory therapy of ARF patients.

Referenz
Nr. 86
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Zoonies et al. Oxygenation improvement with prone positioning in ECMO patients during post-traumatic ARDS Nur Poster
Prospective intervention 16 trauma patients ECMO and PP Sixteen trauma patients underwent ECMO and PP with a mean duration of 175 +/- 105 hrs. The mean age and injury severity score was 25.9 +/- 12.7 years and 55.9 +/- 11.1. At 1- and 6- hrs PP, P:F ratios increased from 152 +/- 74 to 230 +/- 77* and 229 +/- 73* respectively (*p=0.006). The improvement persisted 1-hr RTS (224 +/- 90, p=0.02). FiO2 was reduced at 6-hr PP and persisted 1-hr RTS (0.6 +/- 0.2 vs. 0.5 +/- 0.1# and 0.5 +/- 0.2#, #p=0.02). EBF rate was reduced by 1-hr RTS (3.1 +/- 0.7 to 2.4 +/- 0.6 L/min, p=0.01). Three patients died and 13 survived to discharge with a mean ICU LOS of 12.8 +/- 11.9 days.
Pro Arm
Zusammenfassende Beurteilung: QE:3**(*)
The addition of prone positioning to ECMO significantly improved oxygenation in the acute hypoxic period. This observed improvement persisted after the post-intervention period

Referenz
Nr. 87
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Weick/ Irlbeck et al. J Crit Care2014 Influence of abdominal obesity on multiorgan dysfunction and mortality in acute respiratory distress syndrome patients treated with prone positioning
PDF fehlt
Retrospective study Patients with ARDS (n = 82) were retrospectively divided into 2 groups characterized by presence (n = 41) or absence (n = 41) of abdominal obesity as defined by a sagittal abdominal diameter of 26 cm or more.
There was no difference in cumulative time abdominally obese patients were placed in prone position from admission to day 7 (41.0 hours [interquartile range, 50.5 hours] vs 39.5 hours [interquartile range, 61.5 hours]; P = .65) or in overall intensive care unit mortality (34% vs 34%; P = 1). However, abdominally obese patients developed renal failure (83% vs 35%; P < .001) and hypoxic hepatitis (22% vs 2%; P = .015) more frequently. A significant interaction effect between abdominal obesity and prone position with respect to mortality risk (likelihood ratio, P = .0004) was seen if abdominally obese patients were treated with prolonged cumulative PP.
Pro Arm
n=41 obese N= non-obese
Zusammenfassende Beurteilung: QE:3***
A cautious approach to PP should be considered in abdominally obese patients.

Referenz
Nr. 88
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Sud et al. CMAJ 2014
Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis.
Metaanalysis and systematical review
Relevant randomized controlled trials (RCTs) published through August 2013 were searched. iRCTs that compared prone and supine positioning during mechanical ventilation in patients with ARDS were included. Risk of bias were obsessed and they obtained data on all-cause mortality (determined at hospital discharge or, if unavailable, after longest follow-up period). They used random-effects models for the pooled analyses.
They identified 11 RCTs (n = 2341) that met our inclusion criteria. In the 6 trials (n = 1016) that used a protective ventilation strategy with reduced tidal volumes, prone positioning significantly reduced mortality (risk ratio 0.74,
95% confidence interval 0.59-0.95; I2 = 29%)
compared with supine positioning. The mortality benefit remained in several sensitivity analyses. The overall quality of evidence was high. The risk of bias was low in all of the trials except one, which was small. Statistical heterogeneity
was low (I2 < 50%) for most of the clinical and
physiologic outcomes.
Pro Arm
Zusammenfassende Beurteilung: QE 1****
This analysis of high-quality evidence showed that use of the prone position during mechanical ventilation improved survival among patients with ARDS who received protective lung ventilation.

Referenz
Nr. 89
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Kipping V. et al Int J Artif Organs 2013 Dec 12;36(11):821-32 Prone position during
ECMO is safe and improves oxygena
tion. PDF fehlt
Retrospective analysis Retrospective analysis of complications, gas exchange, and invasiveness of mechanical ventilation during first and second PrP on ECMO at specified time points (before, during, and after PrP).
In 12 ECMO patients, 74 PrPs were performed (median ECMO duration: 10 days (IQR: 6.3- 15.5 days)). No dislocations of intravascular catheters/cannulae, endotracheal tubes or chest tubes were observed. Two PrPs had to be interrupted (endotracheal tube obstruction, acute pulmonary embolism). PaO2/FiO2-ratio increased associated with the first and second PrP (p = 0.002) and lasted after PrP in 58% of these turning procedures ("responders") without changes in ECMO blood flow, respiratory pressures, minute ventilation, portion of spontaneously triggered breathing, and compliance. Hemodynamics did not change with exception of increased mean pulmonary arterial pressure during PrP and decrease after PrP (p<0.001), while norepinephrine dosage decreased (p = 0.03) (MANOVA).
Pro Arm
Zusammenfassung: QE 3*** Prone position during ECMO is safe and improves oxygenation even after repositioning. This might ameliorate hypoxemia and reduce the harm from mechanical ventilation.

Referenz
Nr. 90
Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Zielgröße(n) Hauptergebnis
insgesamt
Nyren et al Lung Ventilation and Perfusion in Prone and Supine Postures with Reference to Anesthetized and Mechanically Ventilated Healthy Volunteers Anesthesiology 2010; 112:682–7
A prospective observational crossover study
7 healthy volunteers Seven healthy volunteers were studied at two different occasions during general anesthesia and controlled mechanical ventilation. One occasion studied ventral to dorsal V and Q distributions in the supine posture and the other in the prone posture. Imaging was performed in supine posture at both occasions. A dual radiotracer technique and single photon emission computed tomography were used. V and Q were simultaneously tagged with 99mTc-Technegas (Tetley Manufacturing Ltd., Sydney, Australia) and 113mInlabeled macroaggregates of human albumin (TechneScan LyoMAA, Mallinckrodt Medica, Petten, The Netherlands), respectively.
ventilation (V) and lung perfusion (Q) distributions during general anesthesia ventilation to perfusion ratio (V/Q ratio) .
No differences in V between postures were observed. Q differed between postures, being more uniform over different lung regions in prone posture and dependent in supine posture. The contribution of the vertical direction to the total V/Q ratio heterogeneity was larger in supine (31.4%) than in prone (16.4%) (P=0.0639, two-tailed, paired t test) posture.
Pro Arm
Zusammenfassende Beurteilung: QE 2b***
During mechanical ventilation, prone posture favors a more evenly distributed Q between lung regions. V distribution is independent of posture. This results in a tendency toward lower V/Q gradients in the ventral to dorsal direction in prone compared with supine posture.
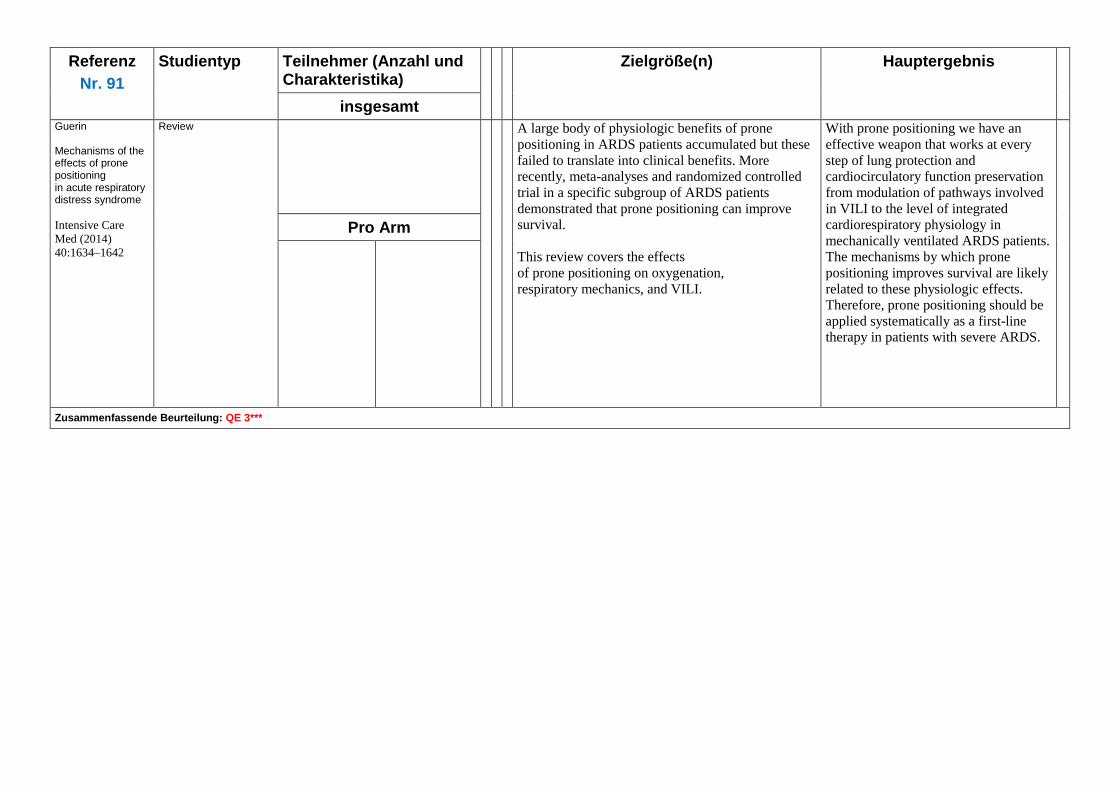
Referenz
Nr. 91
Studientyp Teilnehmer (Anzahl und Charakteristika)
Zielgröße(n) Hauptergebnis
insgesamt Guerin Mechanisms of the effects of prone positioning in acute respiratory distress syndrome
Intensive Care
Med (2014)
40:1634–1642
Review A large body of physiologic benefits of prone
positioning in ARDS patients accumulated but these
failed to translate into clinical benefits. More
recently, meta-analyses and randomized controlled
trial in a specific subgroup of ARDS patients
demonstrated that prone positioning can improve
survival.
This review covers the effects
of prone positioning on oxygenation,
respiratory mechanics, and VILI.
With prone positioning we have an
effective weapon that works at every
step of lung protection and
cardiocirculatory function preservation
from modulation of pathways involved
in VILI to the level of integrated
cardiorespiratory physiology in
mechanically ventilated ARDS patients.
The mechanisms by which prone
positioning improves survival are likely
related to these physiologic effects.
Therefore, prone positioning should be
applied systematically as a first-line
therapy in patients with severe ARDS.
Pro Arm
Zusammenfassende Beurteilung: QE 3***

Referenz
Nr. 92
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Saez de la Fuente et al. Enteral Nutrition in Patients Receiving Mechanical Ventilation in a Prone Position JPEN J Parenter Enteral Nutr published online 1 October 2014
Prospective
observational study
34 mechanically ventilated intensive
care patients who were turned to the
prone position over a 3-year
period
End points related to efficacy
and safety of EN support
were studied
The mean days under EN were 24.7 ±
12.3.
Mean days under EN in the supine position
were significantly higher than in PP (21.1 vs
3.6; P < .001), but there were no significant
differences in gastric residual volume adjusted
per day of EN (126.6 vs 189.2; P = .054) as
well as diet volume ratio (94.1% vs 92.8%; P
= .21).
No significant differences in high gastric
residual events per day of EN (0.06 vs 0.09; P
= .39), vomiting per day of EN (0.016 vs 0.03;
P = .53), or diet regurgitation per day of EN (0
vs 0.04; P = .051) were found.
Pro Arm
Zusammenfassende Beurteilung: QE 2b***
EN in critically ill patients with severe hypoxemia receiving mechanical ventilation in PP is feasible, safe, and not associated with an increased risk of gastrointestinal complications. Larger studies are needed to
confirm these findings.

Referenz
Nr. 93
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Linn et al. Administration of enteral nutrition to adult patients in the prone position. Intensive Crit Care Nurs. 2014 Sep 24 PDF ist bestellt
Review? Outcome associated with EN
Four studies were identified that met our inclusion criteria.
Only two of the included studies were specifically designed to compare outcomes associated with EN in the prone versus supine position.
The remaining two studies did not specifically compare EN in the prone versus supine position, but did provide some insight on the tolerability of EN in the prone position.
Overall, administration of EN to patients in the prone position results in gastric residual volumes similar to those seen in the supine position and does not appear to increase the risk of vomiting or ventilator associated pneumonia.
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*) There is limited evidence proving the safety and tolerability of EN administered to patients in the prone position; however, it does not substantially increase the rate of complications when compared to EN administered in the supine positioning.

Referenz
Nr. 94
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Zielgröße(n) Hauptergebnis
insgesamt Athota KP et al. A practical approach to the use of prone therapy in acute respiratory distress syndrome Expert Rev Respir Med. 2014 Aug;8(4):453-63
PDF ist bestellt
Review
Pro Arm
Zusammenfassende Beurteilung: QE 3**(*)

Evidenztabelle: CLRT/Seitlage:
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 1 Aries, Marcel J. H.; Aslan, Adnan; Elting, Jan Willem J.; Stewart, Roy E.; Zijlstra, Jan G.; Keyser, Jacques de; Vroomen, Patrick C. A. J. Journal of clinical nursing 2012
Intra-arterial blood pressure reading in intensive care unit patients in the lateral position
observational prospective study
3 **(*)
20 Patienten intra-arterial blood pressure recordings in the supine and lateral positions with the correction of hydrostatic height compared with a fixed reference point (phlebostatic level).
MAP readings in the lateral positions were, ~ 5 mmHg higher than in the supine position (p < 0.001). No significant differences between MAP recordings in the left and right lateral position (p = 1.0). No important differences in oxygenation and heart rate were observed. After correction for covariates, the effects persisted.
Seitlage
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Our study demonstrated an increase, albeit small, in blood pressure in the lateral positions. No major differences between the left and right lateral position were found. No important differences in oxygenation and heart rate were observed. Relevance to clinical practice. Turning haemodynamically stable patients in the intensive care unit has no important effects on blood pressure measurements when continuous hydrostatic height correction is applied. Schlussfolgerung des Begutachters: Kleine Fallzahl, Observationsstudie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention
Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt 2
Bein, T.; Ritzka, M.; Schmidt, F.; Taeger, K.
Der Anaesthesist 2007
Positioning therapy in intensive care medicine in Germany. Results of a national survey
national survey
3 -4 **(*)
1736 Intensivstationen angeschrieben
702 Fragebogen auswertbar
beantwortet (40,4%).
12 Fragen (komplexe), die vorstrukturiert waren durch Ankreuzen zu beantworten
Die Daten wurden deskriptiv ohne Signifikanzberechnungen oder -vergleiche bearbeitet
„konventionelle“ manuelle regelmäßige Seitlagerung auf nahezu allen ITS zur Dekubitusprophylaxe am ehesten wird 135°-Lagerung favorisiert (50%) 180°-Bauchlage kommt nur bei ca. 25% der ITS regelmäßig zum Einsatz. kontinuierlichen axialen Drehung auf deutschen ITS in weniger als 20% eingesetzt Befürworter der Bauchlagerung nennen geringere Kosten und den besseren Effekt als Argument vs der KLRT.
Komplikationen während einer Lagerungstherapie sind häufig: hämodynamische Instabilität (73,6%), Tubus-/Katheterdislokation (50,4%) und Intoleranz des Patienten (40,7%). Nur 8,6% der Anwender sehen die Maßnahme als komplikationsfrei an.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie 135°-Lagerung ist auf deutschen Intensivstationen die häufigste Lagerungsmethode zur Steigerung des Gasaustausches. Bauchlagerung und KLRT kommen seltener zum Einsatz. Die Lagerungstherapie ist mit einer hohen Komplikationsquote und erheblichen Anpassungen der übrigen Intensivtherapie verknüpft. Die Autoren nehmen an, dass die Formulierung klarer Leitlinien und praktischer Algorithmen zu mehr Routine, sicherer Anwendungspraxis und zur Reduktion von Komplikationen führt. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und
Charakteristika) Drop out
Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 3 Bein, Thomas; Ploner, Franz; Ritzka, Markus; Pfeifer, Michael; Schlitt, Hans J.; Graf, Bernhard M.
Clinical physiology and functional imaging 2010
No change in the regional distribution of tidal volume during lateral posture in mechanically ventilated patients assessed by electrical impedance tomography
Pilot study
(Cohort study)
3 (-4??)***
7 patients assessessment of distribution of regional lung ventilation during 3 positions (supine, 60°-left and 60°-right-dependent) using electrical impedance tomography (EIT) in mechanically ventilated patients patients were placed on a kinetic treatment table
A calibration procedure of arbitrary units (AUs) versus ventilator-derived VT showed a significant correlation between VT in supine, left and right lateral positions with the corresponding arbitrary units (AUs ) In right lateral positions, a broader variation of VT with a trend towards an increase in the dependently positioned lung was observed in comparison with supine
.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie . Lateral positioning promotes the redistribution of ventilation to the ventral regions of the lung. In our study, in contrast to recent findings, a change in lateral positions did not induce a significant change in regional tidal volume distribution The use of EIT technology might become a helpful tool for understanding and guiding posture therapy in mechanically ventilated patients Schlussfolgerung des Begutachters:
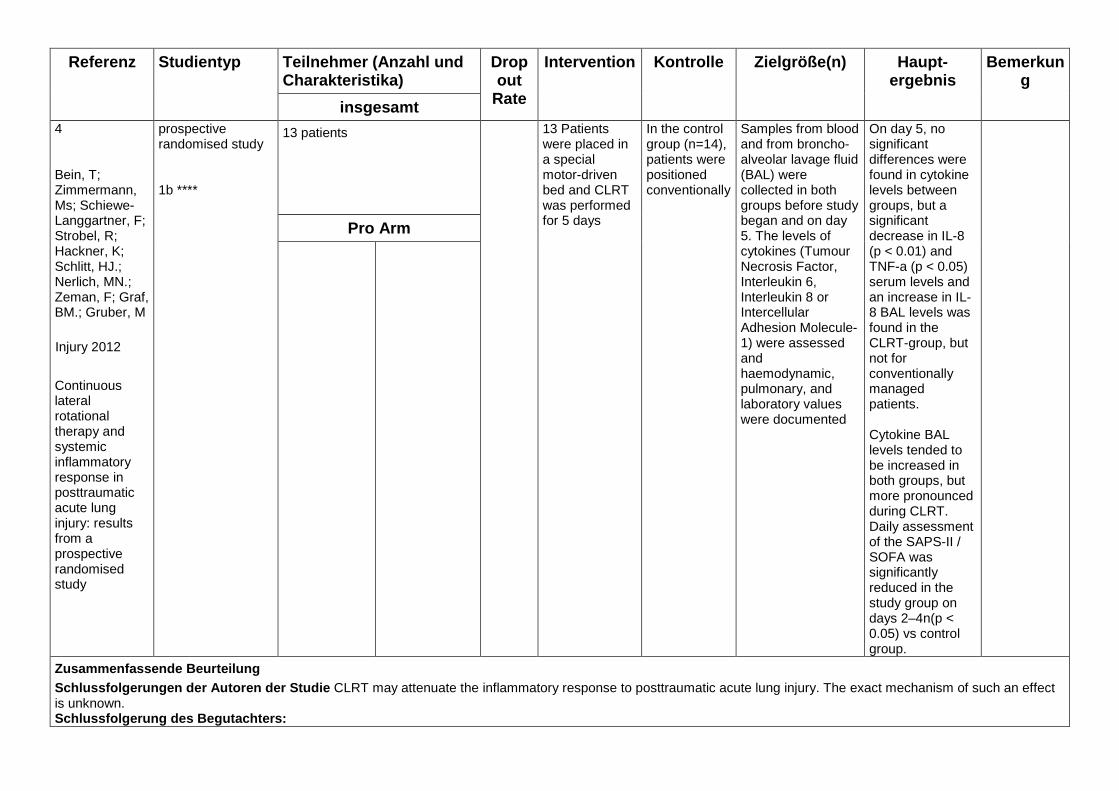
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 4 Bein, T; Zimmermann, Ms; Schiewe-Langgartner, F; Strobel, R; Hackner, K; Schlitt, HJ.; Nerlich, MN.; Zeman, F; Graf, BM.; Gruber, M
Injury 2012
Continuous lateral rotational therapy and systemic inflammatory response in posttraumatic acute lung injury: results from a prospective randomised study
prospective randomised study 1b ****
13 patients 13 Patients were placed in a special motor-driven bed and CLRT was performed for 5 days
In the control group (n=14), patients were positioned conventionally
Samples from blood and from broncho-alveolar lavage fluid (BAL) were collected in both groups before study began and on day 5. The levels of cytokines (Tumour Necrosis Factor, Interleukin 6, Interleukin 8 or Intercellular Adhesion Molecule-1) were assessed and haemodynamic, pulmonary, and laboratory values were documented
On day 5, no significant differences were found in cytokine levels between groups, but a significant decrease in IL-8 (p < 0.01) and TNF-a (p < 0.05) serum levels and an increase in IL-8 BAL levels was found in the CLRT-group, but not for conventionally managed patients. Cytokine BAL levels tended to be increased in both groups, but more pronounced during CLRT. Daily assessment of the SAPS-II / SOFA was significantly reduced in the study group on days 2–4n(p < 0.05) vs control group.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie CLRT may attenuate the inflammatory response to posttraumatic acute lung injury. The exact mechanism of such an effect is unknown. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 5 Berra, Lorenzo; Cressoni, Massimo; Li Bassi, Gianluigi; Kolobow, Theodor; Panigada, Mauro; Zanella, Alberto
Critical care medicine 2010
Continuous lateral rotation therapy to prevent ventilator-associated pneumonia: the neglected effects of gravity on pathogenesis of ventilator-associated pneumonia
Letter to the editor
4 **
We have read with interest the recent publication by Staudinger et al, which claims that continuous lateral rotation therapy (CLRT) is effective in preventing ventilator-associated pneumonia (VAP)
we believe that evidence must be considered to interpret the current results of Staudinger et al. Indeed, based on the pathophysiological approach, and considering effects of gravitational force, the preventive strategy proposed by the authors would have been orders of magnitude more effective if the patient had been positioned in either the lateral or prone position with the trachea oriented below horizontal.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 6 Chandy, Dipak; Sahityani, Rachna; Aronow, Wilbert S.; Khan, Safdar; DeLorenzo, Lawrence J.
American journal of therapeutics 2007
Impact of kinetic beds on the incidence of atelectasis in mechanically ventilated patients
Observational Study
Retrospective data analysed
3 **
71 mechanically ventilated patients before kinetic therapy
83 mechanically ventilated patients after kinetic therapy
bronchoscopies performed for atelectasis on mechanically ventilated patients 50 kinetic beds, 20 continuous lateral rotation therapy modules, and 20 percussion and vibration modules were introduced to the institution.
Before kinetic therapy 71 patients developed atelectasis while being mechanically ventilated.
After kinetic therapy 83 patients developed atelectasis while being mechanically ventilated.
Of these, 48 (58%) patients had left-sided atelectasis, 30 (36%) had right-sided atelectasis, and 5 (6%) had bilateral atelectasis.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie There was no decrease in the incidence of atelectasis in mechanically ventilated patients at our institution after the introduction of kinetic beds and vibration, percussion, and rotation modules despite their widespread availability. The absence of benefit with regard to atelectasis that we demonstrated is more likely to be due to inadequate usage of kinetic therapy than to its lack of effectiveness.
Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis B emerkung
insgesamt 7 Fleegler, B.; Grimes, C.; Anderson, R.; Butler, M.; MacFarlane, G.
Dimensions of critical care nursing 2009
Continuous lateral rotation therapy for acute hypoxemic respiratory failur e: the effect of timing
Kontrollierte Kohortenstudie
Retrospektive Kontrollgruppe
2b ***
? Prospectively enrolled subjects receiving CLRT based on predetermined indications were compared with retrospectively identified control subjects who met the same inclusion criteria from a similar time period in the previous year.
The objective of the study was to determine if the use of a CLRT protocol would decrease mortality and morbidity, mean ventilator days, and/or intensive care unit and hospital length of stay in patients with a pulmonary diagnosis. The study also analyzed the effect of the lag time to the initiation of therapy
Early initiation of continuous lateral rotational therapy resulted in significant decreases in ventilator days and intensive care unit length of stay. The therapeutic benefit of CLRT may be enhanced with early identification and treatment of appropriate patients.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie The current study suggests that there may be universal benefit to the early application of a CLRT protocol. - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle
Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
8
Godoy, A. C.; Vieira, R. J.; Capitani, E. M.;
Jornal brasileiro de pneumologia 2008 Endotracheal tube cuff pressure alteration after changes in position in pa tients under mechanical ventilation
RCT
1b **(*)
patients randomly divided into 2 groups. GroupA: patients moved to the lateral decubitus position, facing away from the ventilator (measurement designated Pcuff A1), returned to the initial position (Pcuff A2), moved to a lateral decubitus position,facing the ventilator (Pcuff A3) and then returned to the initial position (Pcuff A4); Group B, patients were moved to the lateral decubitus position, facing the ventilator (Pcuff B1), returned to the initial position (Pcuff B2), moved to the lateral decubitus position; facing away from the ventilator (Pcuff B3) and then returned to the initial position (Pcuff B4).
The study comprised 70 patients, 31 allocated to group A and 39 allocated to group B. Values >22 mmHg were observed in 142(50.7%) of the 280 Pcuff measurements taken, and values <18 mmHg were observed in 14 (5%). When moved from the 35° semi-Fowler position to the lateral decubitus position, facing away from the ventilator, 58 (82.2%) of the patients presented mean Pcuff values in the higher range (>22 mmHg).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Changes in body position can cause significant Pcuff variations in patients under mechanical ventilation
- Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 9 Goldhill, David R.; Imhoff, Michael; McLean, Barbara; Waldmann, Carl
American journal of critical care 2007
Rotational bed therapy to prevent and treat respiratory complications: a review and meta-analysis
review and meta-analysis
1a ***
15 nonrandomized, uncontrolled, or retrospective studies. 20 prospective randomized controlled trials on rotational therapy published between 1987 and 2004
Meta-analysis suggests that rotational therapy decreases the incidence of pneumonia but has no effect on duration of mechanical ventilation, number of days in intensive care, or hospital mortality. Rotational therapy may be useful for preventing and treating respiratory complications in selected critically ill patients receiving mechanical ventilation
Bereits in alter LL enthalten
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 10 Hamlin, Shannan K.; Hanneman, Sandra K.; Wachtel, Sheryln; Gusick, Gary
Dimensions of critical care nursing 2008
Adverse hemodynamic effects of lateral rotation during mechanical ventilation
Review
4 ***
In this article, we have reviewed the physiological basis of compromised hemodynamic function from mechanical ventilation and later rotation.
Clinicians should closely monitor the hemodynamic response to turning mechanically ventilated patients, and if compromise is observed, the degree and duration of compromise may provide guidance to the appropriate intervention.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 11 Kredel, M.; Bischof, L.; Wurmb, Te; Roewer, N.; Muellenbach, Rm
Perfusion 2013
Combination of positioning therapy and venovenous extracorporeal membrane oxygenation in ARDS patients
Case series
4 (-3??) ***
A retrospective cohort of nine patients
patients received 20 (15–86) hours of positioning therapy while being treated with vvECMO. The initial PaO2/FiO2 index was 64 (51–67) mmHg and the arterial carbon dioxide tension was 60 (50–71) mmHg. Positioning therapy included 135° prone, prone positioning and continuous lateral rotational therapy.
During the first 3 days, the oxygenation index improved from 47 (41–47) to 12 (11–14) cmH2O/mmHg. The lung compliance improved from 20 (17–28) to 42 (27–43) ml/cmH2O. Complications related to positioning therapy were facial oedema (n=9); complications related to vvECMO were entrance of air (n=1) and pump failure (n=1). However, investigation of root causes revealed no association with the positioning therapy and had no documented effect on the outcome
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie The reported cases suggest that positioning therapy can be performed safely in ARDS patients treated with vvECMO, providing appropriate precautions are in place and a very experienced team is present Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Kontrolle Zielgröße(n)
Haupt-ergebnis Bemerkung
insgesamt
12 Lizy, C.; Swinnen, W.; Labeau, S.; Blot, S.
Critical Care 2013
Effect of body position changes on endotracheal tube cuf pressure in ventilated patients
Observational study Nur als Abstract publiziert! 3 *
12 orally intubated and sedated patients
192 measurements
neutral start position (backrest, head of bed elevation (HoB) 30° , head in neutral position) and CP set at 25 cmH2O.
16 different position changes were performed: anteffexion head, hyperextension head, left and right lateral flexion of head, left and right rotation of the head, semirecumbent position (HoB 45° ), recumbent position (HoB 10° ), horizontal position, trendelenburg (-10° ), left and right lateral positioning over 30° , 45° and 90° . Once the patient was correctly positioned, CP was recorded during an end-expiratory ventilatory hold. CP observed was compared with CP at start position
In every position a significant deviation in CP was observed. In total, 40.6% of values exceeded the upper limit of 30 cmH2O. No values beneath the lower target limit of 20 cmH2O were observed. In each position the upper target limit was exceeded at least once
Pdf Seite 57-58
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Simple changes in patient positioning may result in potentially harmful CP (>30 cmH 2 O). These observations call for strict CP monitoring. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle
Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 13 M. Mayer, P. Brunner, F. Smolle-Jüttner, A. Maier, N. Neuböck, Hermann Scharfetter
IFMBE Proceedings 2007
Determination of local phase changes in lung ventilation by EIT during continuous postural changes
Observational study
3 **(*)
6 healthy males lying in a rotating bed
All measurements started in supine position, then the body was rotated to the left by -62 ° at a speed of approximately 30 ° per minute. Then a continuous slow rotation was performed to the right until reaching 62 °. The maneuver was accomplished by rotating back to the supine position and leafing the subject in rest for five minutes. Then we analysed the magnitude and phase of relative impeditivity changes in each ROL Whereby the reference phase was taken as the average over the whole lung.
we compared state-differential images measured by electricalimpedance tomography (EIT) which has been divided into four regions of interest (ROI): left anterior, left posterior, right anterior and right posterior. For the detection of local changes a mean signal for each region of interest and a reference signal as the median over all pixels inside the lung was calculated.
The phase difference seems to be a very sensitive indicator for changes in the regional ventilation during postural changes. This might give important information about lung mechanics during a kinetic therapy used in intensive care units for patients with lung injury
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Haupt-ergebnis Bemerkung
insgesamt 14 Mauri, T; Berra, L; Kumwilaisak, K; Pivi, S; Ufberg, JW.; Kueppers, F; Pesenti, A; Bigatello, LM.
Respiratory care 2010
Lateral-horizontal patient position and horizontal orientation of the endotracheal tube to prevent aspiration in adult surgical intensive care unit patients: a feasibility study
feasibility study
prospective pilot trial with 2 consecutive phases. 3 (-4) ***
Ten adult intensive care unit patients
Patients were ventilated for 64 hours in the standard semi-recumbent position, and ten for 12–24 hours in the lateral-horizontal position. Tracheal secretions were collected every 8 hours and every 4 hours, respectively, and tested for pepsin, which is a marker of gastric contents. We also recorded clinical, physiologic, and outcome variables.
The patients remained stable during ventilation in the lateral-horizontal position, and no adverse events occurred. Pepsin was detected in the trachea of 7 semi-recumbent patients and in five of the lateral-horizontal patients The number of ventilator-free days was 8 days (range 0–21 days) in the semi-recumbent patients, versus 24 days (range 12–25 days) in the lateral-horizontal patients (P = .04).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Implementing the lateral-horizontal position for 12–24 hours in adult intubated intensive care unit patients is feasible, and our patients had no adverse events. The incidence of aspiration of gastric contents in the lateral-horizontal position seems to be similar to that in semi-recumbent position Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 15 Sachdev, G.; Napolitano, L. M. Surgical Clinics of North America
2012
Postoperative Pulmonary Complications: Pneumonia and Acute Respiratory Failure
Review
4 **
The recumbent (45°) position in mech. ventilatied patients has been associated with a reduced incidence of VAP. A prospective randomized trial with 86 patients found a significant drfference in the incidence of VAP. Patients who were supine compared with those with the head of the bed at 45° had a significant difference in VAP rates.
Supine position and mechanical ventilation >7 days were independent risk factors for VAP
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 16 Schellongowski, P; Losert, H; Locker, GJ.; Laczika, K; Frass, M; Holzinger, U; Bojic, A; Staudinger, T Intensive care medicine 2007 Prolonged lateral steep position impairs respiratory mechanics during continuous lateral rotation therapy in respiratory failure
Prospective observational study 3 ***
Twelve consecutive patients suffering from acute lung injury or adult respiratory distress syndrome undergoing continuous rotation therapy
Blood gas analysis, static lung compliance, blood pressure, cardiac index and pulmonary shunt fraction were measured in supine as well as in left and right lateral steep position at 62° during continuous rotation therapy (phase I). Rotation was then stopped for 30 min with the patients in supine position, left and right lateral steep position, and the same measurements were performed every 10 min (phase II).
Phase I and II revealed no significant changes in PaO2/FiO2 ratio, mean arterial blood pressure, pulmonary shunt fraction, or cardiac index. Significantly lower static compliance was observed in lateral steep position than in supine position (p < 0.001). Concomitantly, PaCO2 was significantly lower in supine position than in left and right lateral steep position (p < 0.01).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Lateral steep positioning impairs the compliance of the respiratory system. Prolonged lateral steep position does not lead to benefits with respect to oxygenation or hemodynamics. Individual response to the different positions is unpredictable. The pauses in “extreme” positions should be as short as possible. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt 17 Simonis, G; Steiding, K; Schaefer, K; Rauwolf, T; Strasser, RH.
Clinical research in cardiology 2012
A prospective, randomized trial of continuous lateral rotation ("kinetic therapy") in patients with cardiogenic shock
prospective, randomized open-label trial
1b ****
Forty-five patients were randomized to KT, and
44 to SC
Patients with cardiogenic shock requiring ventilator therapy for more than 24 h were included. Trial was performed to compare KT using oscillating beds (TryaDyne Proventa, KCI) with standard care (SC).
Continuous lateral rotation [‘‘Kinetic therapy’’
(KT)]
Vs
standard care (SC)
Primary endpoint was the occurrence of hospital-acquired pneumonia. Secondary endpoints were the occurrence of pressure ulcers during the hospital stay and 1-year all-cause mortality.
more patients in SC were subject to resuscitation before inclusion. Hospital-acquired pneumonia occurred in 10 patients in KT and 28 patients in SC (p\0.001); pressure ulcers were seen in 10 versus 2 patients (p\0.001). Hospital mortality tended to be lower in KT, and 1-year all-cause mortality was 41 % in KT and 66 % in SC (p = 0.028).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie The use of KT reduces rates of pneumonia and pressure ulcers as compared to SC. Moreover, in this study, patients with KT had a better outcome. The study suggests that KT should be used in patients with cardiogenic shock requiring ventilator therapy for a prolonged time. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 18 Staudinger, T.; Bojic, A.; Holzinger, U.; Meyer, B.; Rohwer, M.; Mallner, F.; Schellongowski, P.; Robak, O.; Laczika, K.; Frass, M.; Locker, G. J.; Critical care medicine 2010 Continuous lateral rotation therapy to prevent ventilator-associated pneumonia
Prospective, randomized, clinical study
1b ****
150 patients were enrolled into the study, 75 into each group
Rotation therapy was performed continuously in a specially designed bed over an arc of 90°. Additional measures to prevent VAP were equally standardized in both groups including semirecumbent position
Patients were randomized to CLRT or standard care if they were mechanically ventilated for <48 hrs and free from pneumonia.
Primary study end point was development of VAP.
Radiologists were blinded to randomization whereas clinical outcome assessors were not
VAP frequency during the ICU stay was 11% in the rotation group and 23% in the control group (p=.048), respectively. Duration of ventilation (8±5 vs. 14±23 days, p = .02) and length of stay (25±22 days vs. 39 ± 45 days, p=.01) were significantly shorter in the rotation group. In a forward stepwise logistic regression model including the CLRT, gender, Lung Injury Score, and SAPSII, CLRT just failed to reach statistical significance with respect to development of VAP (p = .08). Intolerance to CLRT during the weaning phase was observed in 29
patients (39%). Mortality was comparable in both groups.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie VAP prevalence was significantly reduced by CLRT. CLRT led to shorter ventilation time and length of stay. CLRT should be considered in ventilated patients at risk for VAP as a feasible method exerting additive effects to other preventive measures. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 19 Swadener-Culpepper, Leslie; Skaggs, Rita L.; Vangilder, Catherine A.
Critical care nursing quarterly 2008
The impact of continuous lateral rotation therapy in overall clinical and financial outcomes of critically ill patients
Kontrollierte Kohortenstudie
Single center
(nicht randomisiert, retrospektive Kontrollgruppe)
2b ***
95 patients CLRT
75 patients retrospective (historical) comparison group
Patients at risk for pulmonary complications as defined by Pao2/Fio2 ratio < 300, Fio2 > 50% for more than 1 hour, PEEP > or = 8, or a Predicus score of > or = 5 were compared with a historical comparison group that met the high-risk criteria given above and did not receive CLRT.
Patients who received CLRT were separated into 2 groups , early CLRT group (began therapy within 48 hours, n = 49) or late CLRT group (n = 46).
The early CLRT group had a reduction in critical care LOS, (P = .04) as compared with the non-CLRT group. Total hospital costs were reduced (P = .01) in the early intervention group compared to the late intervention group, as well as ICU LOS (P = .02). Nonsignificant trends were seen in reduced ventilator days and hospital LOS. Reintubation rates and readmissions to critical care were also lower in the early intervention group.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Continuous lateral rotation therapy, when introduced early in course of treatment of high-risk patients, reduces critical care LOS and cost to treat. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention
Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt 20 Thomas, P. J.; Paratz, J. D.
Anaesthesia and intensive care 2007
Is there evidence to support the use of lateral positioning in intensive care? A systematic review
Systematic Review
3-4 ***
One review article and 11 empiric studies, which were mostly of low methodological quality, met the eligibility criteria.
Large individual variations in PaO2 response to lateral positioning were demonstrated. Greatest improvement in PaO2 occurred in patients with unilateral pulmonary infiltrates positioned with the bad lung up versus bad lung down (average difference = 33.6 mmHg (range 0-58), effect size 1.13 (95% CI: 0.44, 1.19, P = 0.001)) or supine (average difference =27 mmHg (range 5-42), effect size 0.58 (95% CI: 0.11, 1.06, P = 0.017)).
Lung compliance was not affected by lateral positioning
Haemodynamic compromise was evident with lateral positioning of greater than 60° to the right side in patients requiring vasopressors and/or with right ventricular dysfunction; or with lateral positioning in postoperative coronary artery bypass graft patients. No studies were found that had investigated the effect of routine applications of the lateral positioning to improve, prevent or treat pneumonia, decrease mortality or influence other long-term outcomes.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie The results of this review demonstrate the limited evidence available to support the use of lateral positioning in the
intensive care environment. More data reporting the long-term effects of lateral position on long-term outcomes would aid clinical decision making and may improve the application of patient positioning in critical care environments.
- Schlussfolgerung des Begutachters:
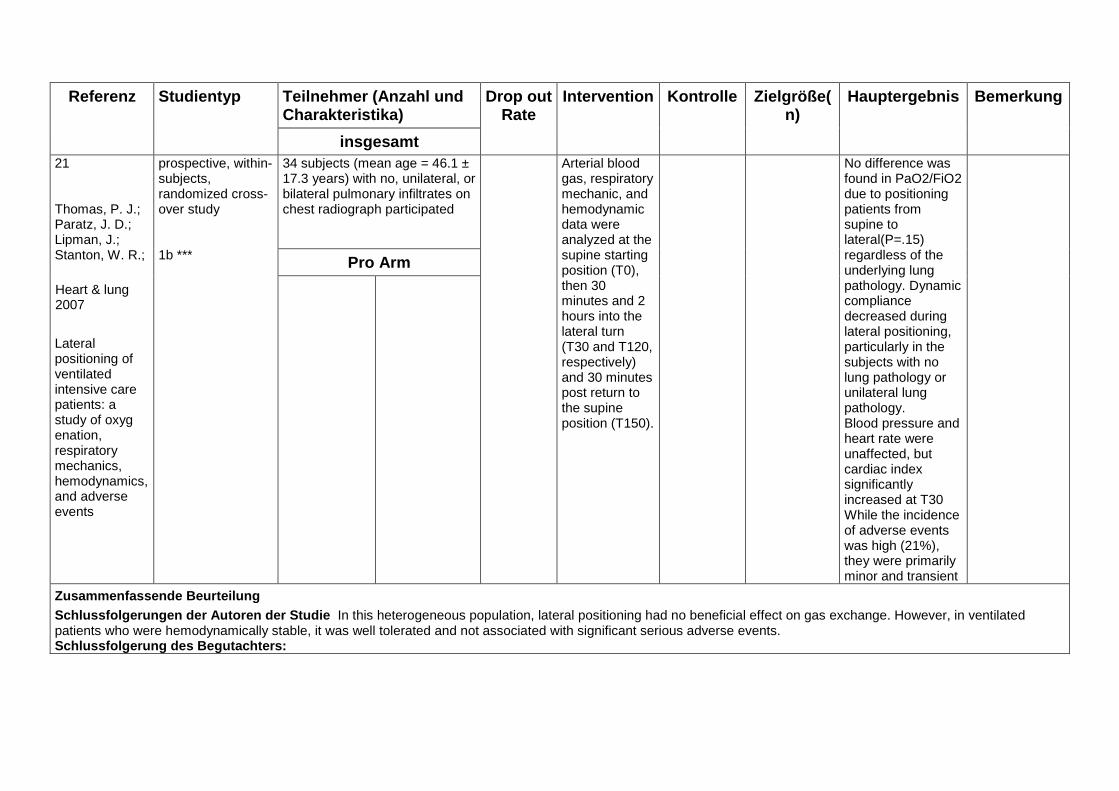
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 21 Thomas, P. J.; Paratz, J. D.; Lipman, J.; Stanton, W. R.;
Heart & lung 2007
Lateral positioning of ventilated intensive care patients: a study of oxyg enation, respiratory mechanics, hemodynamics, and adverse events
prospective, within-subjects, randomized cross-over study 1b ***
34 subjects (mean age = 46.1 ± 17.3 years) with no, unilateral, or bilateral pulmonary infiltrates on chest radiograph participated
Arterial blood gas, respiratory mechanic, and hemodynamic data were analyzed at the supine starting position (T0), then 30 minutes and 2 hours into the lateral turn (T30 and T120, respectively) and 30 minutes post return to the supine position (T150).
No difference was found in PaO2/FiO2 due to positioning patients from supine to lateral(P=.15) regardless of the underlying lung pathology. Dynamic compliance decreased during lateral positioning, particularly in the subjects with no lung pathology or unilateral lung pathology. Blood pressure and heart rate were unaffected, but cardiac index significantly increased at T30 While the incidence of adverse events was high (21%), they were primarily minor and transient
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie In this heterogeneous population, lateral positioning had no beneficial effect on gas exchange. However, in ventilated patients who were hemodynamically stable, it was well tolerated and not associated with significant serious adverse events. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 22 Tongyoo, Surat; Vilaichone, Warakarn; Ratanarat, Ranistha; Permpikul, Chairat
Journal of the Medical Association of Thailand 2006
The effect of lateral position on oxygenation in ARDS patients: a pilot study
Volltext nicht verfügbar (kann nur in Thailand bestellt werden)
Prospective observational study
3 **
18 ARDS patients To determine whether placing the patient in a lateral position has any effect on oxygenation in ARDS.
comparing oxygenation in ARDS patients between supine, right and left lateral positions (> or = 60°).
There was no significant change in mean PaO2, arterial blood gas parameters, respiratory mechanics and hemodynamic parameters between the supine and decubitus positions in the overall group. There was a trend toward increasing the mean PaO2 during right lateral position compared with the supine position. 9 patients who responded to the right lateral position 4 of these patients had predominant left pulmonary infiltration and 5 patients had equally bilateral pulmonary infiltration on chest X-ray.
Unfortunately, the PaO2 in 3patients decreased more than 10 mmHg during right lateral decubitus.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie The PaO2 increased while in the right lateral position in patients with predominant left pulmonary infiltration or bilateral infiltration. This effect may be due to the small sample size. A further large-sized randomized controlled study is needed.
Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 23 Wanless, Stephen; Aldridge, Matthew
Nursing in critical care 2012
Continuous lateral rotation therapy - a review
Review
3-4 **(*)
While there is some data to suggest that CLRT may have an impact on prevention of and treatment for nosocomial infections acquired by ventilated patients, there still remains insufficient evidence to its inclusion as a fully validated treatment. Clearly, there is a requirement for more robust, in-depth research into the efficacy of this proposed treatment.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention
Kontrolle Zielgröße(n)
Haupt-ergebnis Bemerkung
insgesamt 24 Wyen, Hendrik; Wutzler, Sebastian; Maegele, Marc; Lefering, Rolf; Nau, Christoph; Seidel, Dorthe; Marzi, Ingo
Injury 2013
Rotational bed therapy after blunt chest trauma: a nationwide online-survey on current concepts of care in Germany
Survey
4 ***
32-item online-questionnaire to 155 hospitals The overall response rate was 35.5% (55/155) and responses were received from 10 level I (47.6%), 17 level II (32.1%) and 24 level III (29.6%) trauma centres.
35 of the responders (63.6%) declared to be able to perform lateral rotational bed therapy. For level I and II trauma centres more than 80% were able to apply kinetic positioning in contrast to only 50% of level III trauma centres. Although 42.9% of the participants reported on the existence of standardized treatment protocols, 57.1% failed to report a standardized operating procedure for CLRT. The annual mean number of patients per centre treated via CLRT was 15 (0–130). Treatment modalities such as PEEP and the duration of CLRT also showed great variability. Against this background 3 out of 4 centres declared an urgent need for further clinical research in the field
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Our data reflect the wide range of different CLRT treatment strategies performed for blunt pulmonary trauma involving lung contusions in German trauma centres. We conclude that a highquality randomized-controlled trial is warranted to critically assess the role of CLRT in multiple trauma patients with blunt chest trauma to provide a sound basis for future clinical guidelines Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt 25 Yamaguti, Wellington Pereira dos Santos; Paulin, Elaine; Shibao, Simone; Kodaira, Sergio; Chammas, Maria Cristina; Carvalho, Celso Ricardo Fernandes
Jornal brasileiro de pneumologia 2007
Ultrasound evaluation of diaphragmatic mobility in different postures in healthy subjects
cross-sectional observational study.
3 **(*)
seven healthy female volunteers The average mobility of the right diaphragm in right decubitus (51.30 ± 9.69 mm) was significantly higher (p = 0.03) than that observed in left decubitus (45.93 ± 10.37 mm).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: The results suggest that, during spontaneous ventilation, the dependent portion of the diaphragm presents greater mobility than the nondependent portion, and that the technique used was sufficiently sensitive to detect variations in diaphragmatic mobility related to changes in posture
- Schlussfolgerung des Begutachters:

Evidenztabelle Oberkörperhochlagerung:
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
1 Acevedo, F.; DeMuro, J.; Hanna, A.; McNelis, J.
Critical care medicine
2011
Evaluation of twenty-four hour compliance of head of bed elevation
Prospektive Kohortenstudie
Nur als Abstract publiziert!
4 *
26 beatmete Patienten
60 Tage Zeitspanne
24h Aufzeichnung der Zeit >30° und <30° Lagerung
HOB<30°14,2h
HOB >30° 9,4h
Somit 59,9% der Zeit nicht optimal gelagert, nur 40,1% der Beatmungszeit >30° gelagert
Pdf Seite 224
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Trotz entsprechender Studien und Bundles wird die Empfehlung zu OK Hochlagerung nicht eingehalten, erneute
Studie soll nach entsprechender Schulung des Personals erfolgen - Schlussfolgerung des Begutachters: Empfehlung einer Kontrolle / Bundle zum Überprüfen der Umsetzung der Lagerungsempfehlungen.

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
2 Alexiou, V. G.; Ierodiakonou, V.; Dimopoulos, G.; Falagas, M. E. Journal of critical care 2010 Semirecumbent position to prevent ventilator-associated pneumonia is not evidence based
Letter to the editor
4 *
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt 3 Alexiou, Vangelis G.; Ierodiakonou, Vrettos; Dimopoulos, George; Falagas, Matthew E. Journal of critical care 2009 Impact of patient position on the incidence of ventilator-associated pneumonia: A meta-analysis of randomized controlled trials
meta-analysis of randomized controlled trials
1a ****
3 RCTs studying the semirecumbent 45°
4 RCTs studying the prone position with a total of 337 and 1018 patients, respectively.
The odds of developing clinically diagnosed VAP were significantly lower among patients in the semirecumbent 45° position compared to patients in the supine position (OR = 0.47; 95% CI, 0.27-0.82; 337 patients).
The comparison of prone vs supine position group showed a moderate trend toward better outcomes regarding the incidence of clinically diagnosed VAP among patients in the prone position (OR = 0.80; 95% CI, 0.60-1.08; 1018 patients).
The subanalysis regarding the incidence of microbiologically documented VAP, the length of ICU stay, and the duration of mechanical ventilation showed that patients in the semirecumbent 45° position have a moderate trend toward better clinical outcomes.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie This meta-analysis provides additional evidence that the usual practice of back-rest elevation of 15° to 30° is not sufficient to prevent VAP in mechanically ventilated patients. Patients positioned semirecumbently 45° have significantly lower incidence of clinically diagnosed VAP compared to patients positioned supinely. On the other hand, the incidence of clinically diagnosed VAP among patients positioned pronely does not differ significantly from the incidence of clinically diagnosed VAP among patients positioned supinely. Schlussfolgerung des Begutachters:
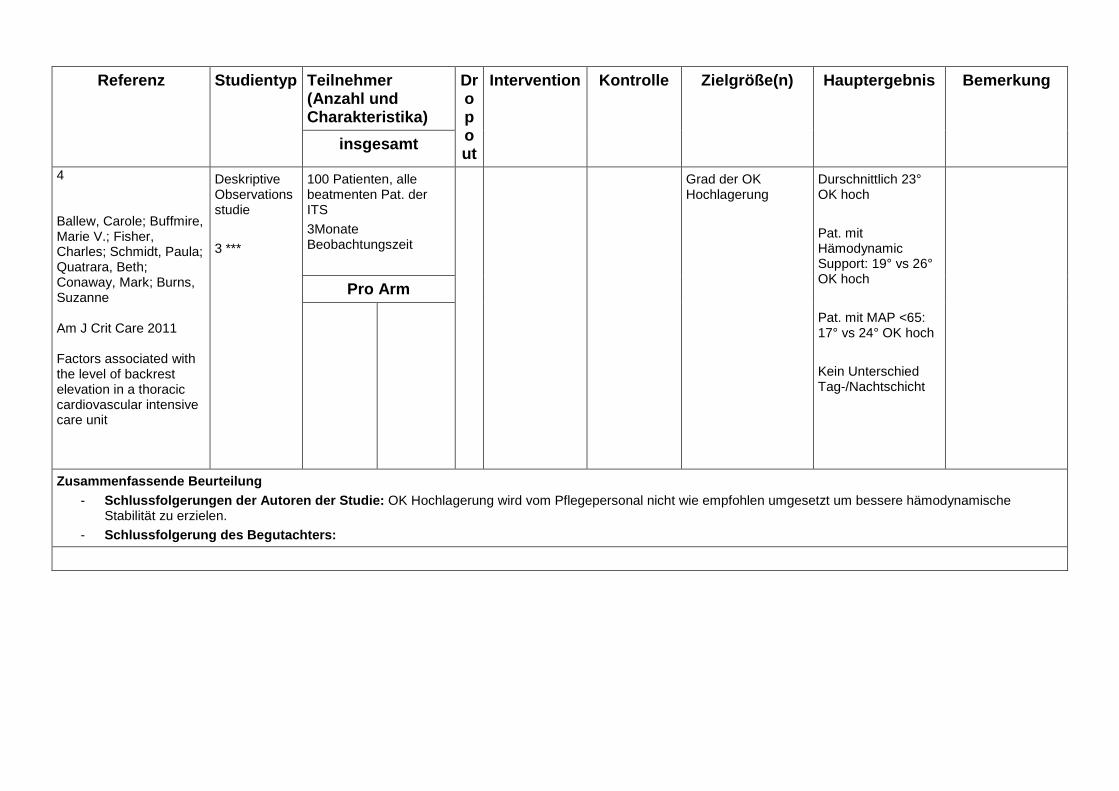
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
4 Ballew, Carole; Buffmire, Marie V.; Fisher, Charles; Schmidt, Paula; Quatrara, Beth; Conaway, Mark; Burns, Suzanne Am J Crit Care 2011 Factors associated with the level of backrest elevation in a thoracic cardiovascular intensive care unit
Deskriptive Observationsstudie
3 ***
100 Patienten, alle beatmenten Pat. der ITS
3Monate Beobachtungszeit
Grad der OK Hochlagerung
Durschnittlich 23° OK hoch
Pat. mit Hämodynamic Support: 19° vs 26° OK hoch
Pat. mit MAP <65: 17° vs 24° OK hoch
Kein Unterschied Tag-/Nachtschicht
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: OK Hochlagerung wird vom Pflegepersonal nicht wie empfohlen umgesetzt um bessere hämodynamische
Stabilität zu erzielen. - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
5 Balonov, Konstantin; Miller, Andrew D.; Lisbon, Alan; Kaynar, A. Murat
Intensive Care Med 2007
A novel method of continuous measurement of head of bed elevation in ventilated patients
Deskriptive Observationsstudie
Prospektiv.
3 **(*)
29 beatmete Patienten
24h Beobachtung an 3 Tagen
Kontinuierliche Messung der OK Hochlagerung in °
Nur um 7Uhr (Schichtwechsel) nahezu 30° OK Hochlagerung,
sonst stets signifikant <30°
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Die vorgestellte Methode zur kont. Messung der HOB Elevation kann mit hoher Reliabilität angewandt werden,
empfohlenen Lagerung mit >30° OK Hochlagerung wird klinisch nicht umgesetzt. - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
6 Barbara S Niël-Weise Critcal Care 2011 An evidence-based recommendation on bed head elevation for mechanically ventilated patients
Systematic Review of RCTs
1a ****
3 Studien
337 Patienten
- kein eindeutiger Beweis für Benefit der HOBE
-ebenso Gefahren (Thrombembolien, Hämodyn Instabilität) unklar
- HOBE nur "Bevorzugte Position" mit den nötigen Einschränkungen
- Experten empfehlen HOBE
- 24h HOBE ist nicht praktikabel
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Experten empfehlen OK Hochlagerung als "Bevorzugte Position" mit allerdings den nötigen Einschränkungen. - Schlussfolgerung des Begutachters: Prisma Guidelines + Delphiverfahren! Nur RCTs!

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
8 Bassi, G. L.; Zanella, A.; Cressoni, M.; Stylianou, M.; Kolobow, T. Critical care medicine 2008 Following tracheal intubation, mucus flow is reversed in the semirecumbent position: Possible role in the pathogenesis of ventilator-associated pneumonia
Prospective randomized animal study.
3**(*)
Sixteen healthy sheep. Spontaneously breathing or mechanically ventilated sheep were randomized to be positioned with the orientation of the trachea above (40 degrees, trachea-up) or below (5 degrees, trachea-down) horizontal. Tracheal mucus velocity measured through radiographic tracking of radiopaque tantalum disks, insufflated into the trachea. After 24 hrs, sheep were euthanized, and samples from the airways and lungs were taken for microbiological analysis.
In trachea-down sheep, all mucus moved toward the glottis at mean velocity 2.1±1.1 mm/min. In all trachea-up sheep, abnormal tracheal mucus clearance was found. Mucus moved toward the glottis at mean velocity of 2.2 ± 2.0 mm/min and accumulated at the inflated endotracheal tube cuff. From the proximal trachea, mucus moved toward the lungs on the dependent part of the trachea, leading to an “intratracheal route” of colonization. Pneumonia was found in 6/8 of trachea-up sheep and the same microorganisms were isolated from the lungs and the proximal trachea. No pneumonia was found in trachea-down sheep (p=.007).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie following tracheal intubation gravitational force influences tracheal mucus clearance. When the trachea is oriented above horizontal, a flow of mucus from the proximal trachea toward the lungs is highly associated with bacterial colonization of the airways and pneumonia Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
9 Bloos, F.; Muller, S.; Harz, A.; Gugel, M.; Geil, D.; Egerland, K.; Reinhart, K.; Marx, G. British journal of anaesthesia 2009 Effects of staff training on the care of mechanically ventilated patients: a prospective cohort study
Prospective cohort study
3 ***
133 patients before and 141 patients after staff training
Application of a ventilator bundle consisting of semirecumbent positioning, lung protective ventilation in patients with acute lung injury (ALI), ulcer prophylaxis, and deep vein thrombosis prophylaxis (DVTP) was assessed before and after staff training in post-surgical patients requiring mechanical ventilation for at least 24 h.
bundle adherence increased from 15 to 33.8% (P<0.001). Semirecumbent position was achieved in 24.9% of patient days before and 46.9% of patient days after staff training (P<0.001). Days on mechanical ventilation were reduced from 6 to 4 (P=0.017). Rate of VAP, ICU length of stay, and ICU mortality remained unaffected. In patients with VAP, the median ICU length of stay was reduced by 9 days P=0.04
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Staff training by an ICU change team improved compliance to a pre-defined ventilator bundle. This led to a reduction in the days spent on mechanical ventilation, despite incomplete bundle implementation. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
10 Burk, Ruth Srednicki; Grap, Mary Jo Heart Lung 2012 Backrest position in prevention of pressure ulcers and ventilator-associated pneumonia: conflicting recommendations
Review
3 (-4)***
Keine ges. Zahl genannt.
- evtl. 10-30° als Kompromiss zur VAP Prophylaxe und noch niedrigem Risiko für Druck Ulkus?
- eine Studie zeigt dass Flachlage in den ersten 24h wichtiger Faktor für VAP, danach evtl. Fokus mehr auf Ulkusprophylaxe?
Zahlreiche Studien zu sämtlichen Themen, keine klaren Kriterien zur Beurteilung der Studien, Ergebnisse als Fragen formuliert!
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie:
- Schlussfolgerung des Begutachters: Empfehlungen als Fragen formuliert!! Keine Systematik!

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
11
Burns, S. M.
Practical Gastroenterology 2007
Prevention of aspiration pneumonia in the enterally fed critically ill ventilated patients: Keeping the head up takes a village!
Allg. Artikel über Ernährung und Aspirationsprophylaxe bei MV Pat.
3**
HOBE einer der wichtigsten Risikofaktoren für VAP
Alle Team Mitglieder sollen bez. HOBE geschult werden
Monitoring für HOBE sollte etabliert werden
30° Lagerung scheint eher erreichbar als 45°
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Allgemeiner Artikel zum Thema - Schlussfolgerung des Begutachters: Relevanz für LL????

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
12 Daihua, Yu; Wei, Chai; Xude, Sun; Linong, Yao; Changjun, Gao; Hui, Zhao Journal of critical care 2012 The effect of body position changes on stroke volume variation in 66 mechanically ventilated patients with sepsis
Randomisierte Korrelationsstudie
3 ****
Sixty patients with sepsis were studied during mechanical ventilation.
All patients were randomly placed in the supine, 30 degrees head-up 30 degrees left or right recumbent, or prone position. In addition to standard hemodynamic monitoring, SVV, central venous pressure, cardiac index (CI), SV
index (SVI), global end-diastolic volume index (GEDVI), and global ejection fraction (GEF) were recorded at each position after stabilization
Stroke volume variation had strong negative correlation with CI, SVI, GEF, and GEDVI (P < .0001). After the change to the 30 degrees head-up or the prone position, SVV increased significantly, whereas CI, SVI, GEF, and GEDVI decreased dramatically. Stroke volume variation in the supine position did not correlate with 30 degrees head-up- or prone-induced changes in CI (P < .05). All variables did not differ between 30 degrees left or right recumbent and supine positions.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Body position changes may affect the correlation of SVV with hemodynamic variables. The 30 degrees head-up and prone positions increased SVV because of the associated decreased SV. The 30 degrees left or right recumbent position does not affect SVV and SV.
Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
13 Dellamonica, J.; Lerolle, N.; Sargentini, C.; Hubert, S.; Beduneau, G.; Di Marco, F.; Mercat, A.; Diehl, J. L.; Richard, J. C. M.; Bernardin, G.; Brochard, L.
Intensive Care Med 2013
Effect of different seated positions on lung volume and oxygenation in acute respiratory distress syndrome
Prospektive Multicenter Studie
Nicht-kontrollierte Kohortenstudie.
3 ***
40 beatmete Pat. mit ARDS/ALI
Lagerung OK Hoch um
1. 15-20°
2. 45°
3. 60°+legdown
4. 15-45°
Jeweils 45-60Min
"Responders" wenn PaO2/FiO2 Anstieg um >20%
Messung von BGA, EELV (exp. lung vol) mittels N2 washout, stat. compliance
OK Hochlagerung erhöht Lungenvolumen, aber nur Responders verbessern EELV/PBW (predict. body weight)
Effekt teilweise anhaltend wenn erneut Rückenlage
Responders hatten niedrigeres EELV/PBW sitzend und geringer compliance als nonresponder
Kein Zusammenhang Lungenvolumen und Oxygenierung
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie Oxygenierung in 32% der Pat. verbessert, OK Hoch/Sitzende Lagerung ist leicht durchführbar, - Schlussfolgerung des Begutachters: keine Randomisierung! Hämodynamische Auswirkungen nicht aufgeführt,

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
14 Deye, N.; Lellouche, F.; Maggiore, S. M.; Taille, S.; Demoule, A.; L'Her, E.; Galia, F.; Harf, A.; Mancebo, J.; Brochard, L.
Intensive Care Med 2013
The semi-seated position slightly reduces the effort to breathe during difficult weaning
Prospektiv, randomisierte Crossover klinische Studie, Monozentrisch, Offen
2b ***
24 beatmetet Patienten, Weaningversager
3 Positionen:
Liegend (o°)
Halbsitzend (45°)
Sitzend (45°OK hoch + Beine 90° runter)
Atemarbeit leicht aber signifikant abfallend in 45° OK hochlagerung
Patientenkomfort in 45° Hochlage am besten
Sitzende Position hat die höchsten Werte für Atemarbeit
PEEPi und PEEPi rel Work in 45° Lage leicht aber sign. höher als in den andere Positionen
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie Halbsitzende Position für difficult weaning Patienten empfohlen - Schlussfolgerung des Begutachters: nur 24 Patienten.
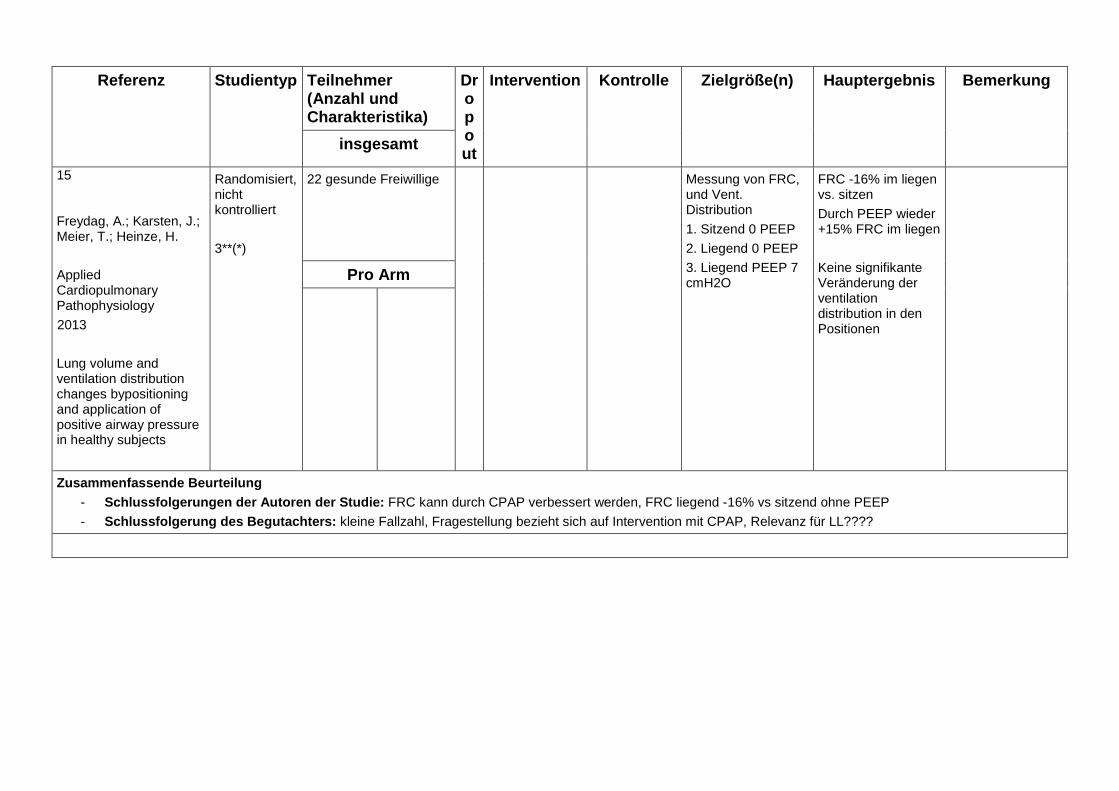
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
15 Freydag, A.; Karsten, J.; Meier, T.; Heinze, H.
Applied Cardiopulmonary Pathophysiology
2013
Lung volume and ventilation distribution changes bypositioning and application of positive airway pressure in healthy subjects
Randomisiert, nicht kontrolliert
3**(*)
22 gesunde Freiwillige Messung von FRC, und Vent. Distribution
1. Sitzend 0 PEEP
2. Liegend 0 PEEP
3. Liegend PEEP 7 cmH2O
FRC -16% im liegen vs. sitzen
Durch PEEP wieder +15% FRC im liegen
Keine signifikante Veränderung der ventilation distribution in den Positionen
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: FRC kann durch CPAP verbessert werden, FRC liegend -16% vs sitzend ohne PEEP
- Schlussfolgerung des Begutachters: kleine Fallzahl, Fragestellung bezieht sich auf Intervention mit CPAP, Relevanz für LL????

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
16 Gocze, Ivan; Strenge, Felix; Zeman, Florian; Creutzenberg, Marcus; Graf, Bernhard M.; Schlitt, Hans J.; Bein, Thomas Critical care 2013 The effects of the semirecumbent position on hemodynamic status in patients on invasive mechanical ventilation - prospective randomized multivariable analysis
Prospective, RCT
Self-controlled
1b ****
200 hemodynamically stable adults on invasive mechanical ventilation
HBE positions (0°, 30°, and 45°) was adopted in random order, and MAP and ScvO2 were measured at each position. Patients acted as their own controls. indentify risk factors for hypotension during HBE, defined as MAP <65 mmHg.
Changing HBE from supine to 45° caused significant reductions in MAP (from 83.8 mmHg to 71.1 mmHg, P < 0.001) and ScvO2 (76.1% to 74.3%, P < 0.001). Pressure-controlled ventilation was the most influential risk factor for hypotension when HBE was 45° (odds ratio (OR) 2.33, 95% CI, 1.23 to 4.76, P = 0.017).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie HBE to the 45° position is associated with significant decreases in MAP and ScvO2 in mechanically ventilated patients. Pressure-controlled ventilation, higher (SAPS II) score, sedation, high catecholamine, and PEEP requirements were identified as independent risk factors for hypotension after HOBE. Patients at risk may need positioning at 20° to 30° to overcome the negative effects of HBE, especially in the early phase of intensive care unit admission Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
17 Goldhill, D. R.; Badacsonyi, A.; Goldhill, A. A.; Waldmann, C. Anaesthesia 2008 A prospective observational study of ICU patient position and frequency of turning
Deskriptive Observationsstudie, prospektiv
3 ***
393 sets of observation
40 british ICUs
We prospectively recorded patient position every hour over two separate days
Five patients were prone at any time and 3.8% (day 1) and 5% (day 2) were on rotating beds. Patients were on their back for 46.1% of observations, turned left for 28.4% and right for 25.5%, and head up for 97.4%. A turn was defined as a change between on back, turned left or turned right. The average time (SD) between turns was 4.85 (3.3) h. There was a significant difference between hospitals in the frequency with which patients were turned
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
18 Grap, Mary Jo; Munro, Cindy L.; Hummel, Russell S. 3rd; Elswick, R. K. [JR]; McKinney, Jessica L.; Sessler, Curtis N.
Am J Crit Care 2005
Effect of backrest elevation on the development of ventilator-associated pneumonia
Nonexperimental, longitudinal, descriptive pilot study
3 **(*)
2005publiziert
66 beatmete Patienen, 7 Tage Beobachtung
(276 patient days of mech ventilation)
Ø OK Hochl. 21.7º No direct association between height of backrest and VAP was found VAP was more likely to develop in patients who were more seriously ill and spent greater time at backrest elevations of<30º during first day of intubation To reduce risk of VAP it is especially important to maintain backrest elevation of at least 30º during the first 24 hours of mechanical ventilation.
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters: Beobachtungsstudie

Referenz Studientyp
Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
19 Hiner, Chad; Kasuya, Tomoyo; Cottingham, Christine; Whitney, JoAnne
Am J Crit Care 2010
Clinicians' perception of head-of-bed elevation
Querschnittsstudie + Survey
4 **
175 klinisch Tätige Angestellte (Pflege, Physio etc)
"Testpatient" im Bett gelagert: 3 Fragen:
- abschätzen der höhe der HOBE
- welche Lagerung optimal für VAP Prävention
- wie überpfrüfen sie die höhe der Lagerung im klin. Alltag.
Ca 50% der Pflege und Physiotherap. schätzen höhe richtig (ges. 50-86%)
80-95% wussten die optimale höhe zur VAP Prophylaxe
58% nutzen ein Messgerät im Alltag
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: HOBE sollte nicht nur durch "Augenmaß" erfolgen, - Schlussfolgerung des Begutachters: Wiederspruch zu anderen Studien (Grap: höhe wird richtig geschätzt), Praktische Durchführung

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
20 Hojlund Rasmussen, J.; Mantoni, T.; Belhage, B.; Pott, F. C.
Eur J Appl Physiol 2007
Influence of upper body position on middle cerebral artery blood velocity during continuous positive airway pressure breathing
Experimentelle Studie?
3? **
in 11 healthy subjects cerebral blood flow (CBF) and cerebral blood volume (CBV) evaluated by middle cerebral artery mean blood velocity (MCA Vmean) and the near-infrared spectroscopy determined frontal cerebral hemoglobin content (cHbT) evaluated during CPAP at different body positions (15° head-down tilt, supine, 15°, 30° and 45° upper body elevation)
supine position, CPAP 10 cmH2O reduced MCA Vmean by 9 ± 3% and increased cHbT 4 ± 2 µmol/L headdown position, CPAP increased cHbT to 13 ± 2 µmol/L but left MCA Vmean unchanged. 15° attenuated the CPAP associated reduction in MCA Vmean (-7 ± 2%), while cHbT returned to baseline (1 ± 2 µmol/L). With larger elevation of the upper body MCA Vmean decreased progressively to -17 ± 3%, while cHbT remained unchanged from baseline.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie :upper body elevation by ~ 15° during 10 cmH2O CPAP prevents an increase in cerebral blood volume with minimal effect on cerebral blood Flow. with larger HOBE MCA decreased progessively while cHbT remained unchanged Schlussfolgerung des Begutachters : physiologische Grundlage, Allg. Durchführung/Komplikationen. Kleine Fallzahl.

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
21 Huynh Thi Loan; Parry, J.; Nguyen Thi Ngoc Nga; Lam Minh Yen; Nguyen Thien Binh; Tran Thi Diem Thuy; Nguyen Minh Duong; Campbell, J. I.; Thwaites, L.; Farrar, J. J.; Parry, C. M. Transactions of the Royal Society of Tropical Medicine and Hygiene 2012 Semi-recumbent body position fails to prevent healthcare-associated pneumonia in Vietnamese patients with severe tetanus
randomised controlled trial
1b **(*)
229 adults and children (aged≥1 year) with severe tetanus No patients were orally intubated!
we compared the occurrence of HCAP in patients with severe tetanus nursed in a semi-recumbent (30◦) or supine position Patients were randomly assigned to a supine (n = 112) or semi-recumbent (n = 117) position.
there was no significant difference between the two groups in the frequency of clinically suspected pneumonia 20.8%) vs 25.0%; p = 0.464, pneumonia rate/1000 intensive care unit days (13.9 vs 14.6; p = 0.48) and pneumonia rate/1000 ventilated days (39.2 vs 38.1; p = 0.72). Mortality in the supine patients was 9.8% compared with 14.5% in the semi-recumbent patients (p = 0.277). The overall complication rate 50.9% vs 65.0%; p = 0.03] and need for tracheostomy 45.5% vs 58.9%; p = 0.04 was greater in semi-recumbent patients.
The overall complication rate, and the need for a tracheostomy, was significantly greater in the semi-recumbent patients compared with those in the supine posi
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Semi-recumbent body positioning did not prevent the occurrence of HCAP in severe tetanus patients. The overall complication rate, and the need for a tracheostomy, was significantly greater in the semi-recumbent patients The need for mechanical ventilation, hypotension and autonomic instability also occurred more frequently in the semi-recumbent group but the differences were not significant Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
22 Johnson, Karen L.; Meyenburg, Tim AACN advanced critical care 2009 Physiological rationale and current evidence for therapeutic positioning of critically ill patients
Review
4 **
In patients with unilateral disease, optimal gas exchange occurs when the patient is placed with the "good lung down"
Strong evidence exists that HOB elevation prevents VAP; more research is needed to identify the optimal degree of HOB elevation to prevent VAP and development of pressure ulcers
The current standard of repositioning patients every 2 hours, yet there is little physiological or scientific evidence to support this standard
Research has shown that rotation therapy decreases VAP
More research is needed to understand physiological and scientific basis of optimal positioning in select critically ill patient populations such as obese and elderly patients
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
23 Kaye, M. G.; Tilton, L. E. Chest 2007 The effect of continuous head-of-bed monitoring on compliance with semi-recumbent positioning in patients on mechanical ventilation
prospektiv kontrollierte Studie
nur als Abstract publiziert!
2b *
90 patients on mechanical ventilation were enrolled in this controlled,.
An electronic sensor attached to the bed frame provided continuous monitoring and recording of HOB angle; whenever HOB was >30 degrees, the sensor activated a light and timer on the monitor device. For the control group, the light was disabled, the monitor stored out of view, and the nursing staff blinded to the time measurements. For the intervention group, connections to the light were enabled and the monitor placed on top of the ventilator, where the light and timer were clearly visible to the nursing staff. To control for a possible training effect, data collection ceased at a maximum of 8,640 ventilator minutes (6 days)
The first 45 consecutive patients were enrolled in the control group, the next consecutive 45 patients in the intervention group.
The percentage of time with HOB elevated >30° was significantly greater (p<0.0001) in the intervention group, with a median of 81% (interquartile range 70-91%) vs a median of 17% in the control group (interquartile range 4-51%). The intervention group had modestly longer median total ventilator time than the control group (4.1 days vs 3.0 days, p=0.1 for difference). However analysis of variance showed that while the group assignment remained highly significant (p<0.0001), there was no relationship between total ventilator minutes and percentage of time with HOB >30° (p=0.83).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Continuous HOB monitoring utilizing an indicator light significantly increases the time mechanically ventilated patients have the HOB elevated >30°. Continuous HOB monitoring may decrease the incidence of VAP by improving compliance with semi-recumbent positioning
Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
24 Keane, M. G.; Kapoor, R. Critical Care 2009 Study of the ability of ICU staff to set a bed to the semi-recumbent position
Deskriptive Kohortenstudie.
Nur als Abstract publiziert
4? **
55 members of ICU staff
Members were asked to set the angle of the head of a standard ICU bed to 30° and 45°. The estimated bed angle was then measured accurately using a Mathey Dearman protractor.
When estimating the head of the bed, nursing staff were the most accurate (Table 1) while other staff significantly underestimated the angle of the bed. We also found that greater experience of working in the ICU is likely to improve ability to estimate the angle of the head of bed accurately.
Pdf Seite 194-195
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie we have found estimating the angle of a bed by eye is difficult and often inaccurate. Aids to set the angle of the bed should be introduced in common practice to improve compliance with VAP guidelines Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
25 Keeley, Libby Nursing in Critical Care 2007 Reducing the risk of ventilator-acquired pneumonia through head of bed elevation
Pilot study, randomized controlled trial, quantitative
2b ***
30 Patienten Adult ventilated patients randomly assigned to 45° HOBE or 25° HOBE (control group)
29% (five) in the treatment group and 54% (seven) in the control group contracted VAP (P < 0,176).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie There was a trend towards a reduction in VAP in the patients nursed at 45°. However, because of the sample size this difference did not reach statistical significance Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
26 Keulenaer, B. L. de; Waele, J. J. de; Powell, B.; Malbrain, M. L. N. G. Intensive Care Med 2009 What is normal intra-abdominal pressure and how is it affected by positioning, body mass and positive end-expiratory pressure?
Review
4 **(*)
??
5 Studien: IAP in non obese patients
7 Studien: Comparison of IAP among diff weight groups
6 Studien: Effect of PEEP on IAP
9 Studien: Effect of body pos. on IAP
Measuring IAP via the bladder in the supine position is still the accepted standard method, but in patients in the semi-recumbent position (HOBE to 30° and 45°), the IAP on average is 4 and 9 mmHg, respectively, higher. Small increases in IAP in stable patients without IAH, turned prone, have no detrimental effects. The role of prone positioning in the unstable patient with or without IAH still needs to be established.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Future research should be focused on developing and validating predictive equations to correct for supine IAP towards the semirecumbent position. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
27 Lemyze, M; Mallat, J; Duhamel, A; Pepy, F; Gasan, G; Barrailler, S; Vangrunderbeeck, N; Tronchon, L;Thevenin, D Crit Care Med2013 Effects of Sitting Position and Applied Positive End-Expiratory Pressure on Respiratory Mechanics of Critically Ill Obese Patients Receiving Mechanical Ventilation
Prospektive Kohortenstudie
2b **
30 Patienten
(15 Obese mit BMI >35
15 Kontrollgruppe mit BMI<30
Parameter: plateau pressure auto-PEEP flow-limited volume jeweils Messung: ohne PEEP im liegen und sitzen mit PEEP im liegen und sitzen
expiratory flow limitation 59.4% vs. o% in Kontrollgruppe greater auto-PEEP (10 vs 0.7 cmH2O) in controls
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: In critically ill obese patients under mechanical ventilation,sitting position constantly and significantly relieved expiratory flow limitation and auto-positive end-expiratory pressure resulting in a dramatic drop in alveolar pressures. Combining sitting position and applied positive end-expiratory pressure provides the best strategy. Schlussfolgerung des Begutachters: Untergruppe Übergewichtige Patienten!

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
28 Li Bassi, Gianluigi; Torres, Antoni Current Opinion in Critical Care 2011 Ventilator-associated pneumonia: role of positioning
Literatur Review
3-4 ***
3 RCT supine semirecumbent vs. horzontal position on incidence of VAP
6 RCT prone vs supine
2 experim. Tierstudien
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie The semirecumbent position has proven benefits and should be routinely used but there is still limited evidence to recommend the lowest orientation of the bed at which the patient can be safely maintained. Results from pioneering laboratory investigation call attention to new possible positions, that is lateral Trendelenburg position, aimed to avoid pulmonary aspiration and to enhance mucus clearance in intubated patients. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
29 Li TST; Joynt, G. M.; So, H. Y.; Gomersall, C. D.; Yap FHY Critical Care and Shock 2008 Semi-recumbent position in ICU
Deskriptive Observationsstudie.
(Audit)
3***
295 occasions, 4 month observation academic intensive
care unit
Unannounced ad hoc inspections were made on patients receiving mechanical ventilation in the intensive care unit. During inspections, the angle of HOBE was formally measured by a manual technique using a hand-held protractor. The nurse at bed-side was also asked to estimate the angle of elevation of bed without referring to the built-in protractor and interviewed with a structured questionnaire
the minimum target semi-recumbent position of 30 ° was achieved only 40% of the time Nurses consistently overestimated the angle of HOBE and the presence of a built-in bedside protractor was not associated with a greater compliance with the target backrest elevation angle..
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: Strictly enforced protocols, education programs for nurses and doctors and regular audit may improve compliance with HOBE targets Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
30 Li Xiao Yuan Qiang; Wang, L. i.; Sun Xin Deng Lijing; Cochrane Database of Systematic Reviews 2012 Semi-recumbent position versus supine position for the prevention of venti lator-associated pneumonia in adults requiring mechanical ventilation
Protocol for a Review
4*
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
31 Liu, Jing-tao; Song, Hai-jing; Wang, Yu; Kang, Yan; Jiang, Li; Lin, Si-han; DU, Bin; Ma, Peng-lin
Chin Med J 2013
Factors associated with low adherence to head-of-bed elevation during mechanical ventilation in Chinese intensive care units
Prospektiv multicenter Längschnittstudie
3 **(*)
314 Patienten währen 2842 Beatmungstage
Ges. 8647 Messungen
33 chinesische ICUs
Messung der HOBE 4x tägl. in 5-7h Intervallen
Nur 27,8% der Messungen >30° HOBE
Ca 60% mind eine 24h Periode in der HOBE ziel nicht dokumentiert wurde
Keine korrelation mit APACHE II score oder Vasopressordosis
"nurese workload" als wichtigster faktor für non-compliance bez. HOB Ziel
Außerdem mangelnde Kenntnis bez. VAP Bundles
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: HOBE wird nicht eingehalten, Hauptgrund ist Arbeitsbelastung der Pflege und mangelnde Kenntnis bez VAP
Bundles - Schlussfolgerung des Begutachters: Längsschnittstudie, gleiches Ergebnis wie bereits weitere genannte Studien.

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
32 Lyerla, Frank; LeRouge, Cynthia; Cooke, Dorothy A.; Turpin, Debra; Wilson, Lisa
Am J Crit Care 2010
A nursing clinical decision support system and potential predictors of head-of-bed position for patients receiving mechanical ventilation
Modified interrupted time-series dsign
3 **(*)
43 Patienten und 33 Schwestern
Mehrfach tägl. Messung der HOBE, 3 Phasen
1. 2Monate vor
2. 1und3Monate nach
3. 4und5. Monate nach Einführung des Clinikal decision support system (CDSS)
CDSS in Form einer Erinnerung am Computer bei Dokumentation der Lagerung kann die Einhaltung der Leitlinien bez. HOBE verbessern
Pat. mit pulmonaler DIagnose und Sondenernährung hatten durchschnittlich höhe HOBE
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters: keine Randomisierung, keine Kontinuierliche Messung der HOBE

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
33 Marklew, Anna Nursing in critical care 2006 Body positioning and its effect on oxygenation--a literature review
Literature review
4 **
6 reviews, 1 editorial, 12 research and clinical investigations, 3 reflective articles and 2 articles written for educational purposes
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie nurses need to be aware of how different positions can affect patients' oxygenation. Further research on exploring patients' experience of positioning within the critical care environment and nurses' understanding of positioning and oxygenation is needed Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
34 McBeth, Paul B.; Zygun, David A.; Widder, Sandy; Cheatham, Michael; Zengerink, Imme; Glowa, Judy; Kirkpatrick, Andrew W.
American journal of surgery 2007
Effect of patient positioning on intra-abdominal pressure monitoring
Prospektive Observationsstudie
3 ***
300 Messungen an 37 Patienten
Messung des IAP (Blasenkatheter) von 0° bis 45° HOBE
Signifikant positiver Zusammenhang zwischen IAP und HOBE
Klinisch relevanter Anstieg des IAP ab >20° HOBE
Unterschied von 10° uns 20° war klein, aber Anstieg von 30° auf 45° klinisch relevant!
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie - Schlussfolgerung des Begutachters: Nur 37 Patienten! Klinische Relevanz? evtl. nur für Pat. mit Risiko für IAH???)
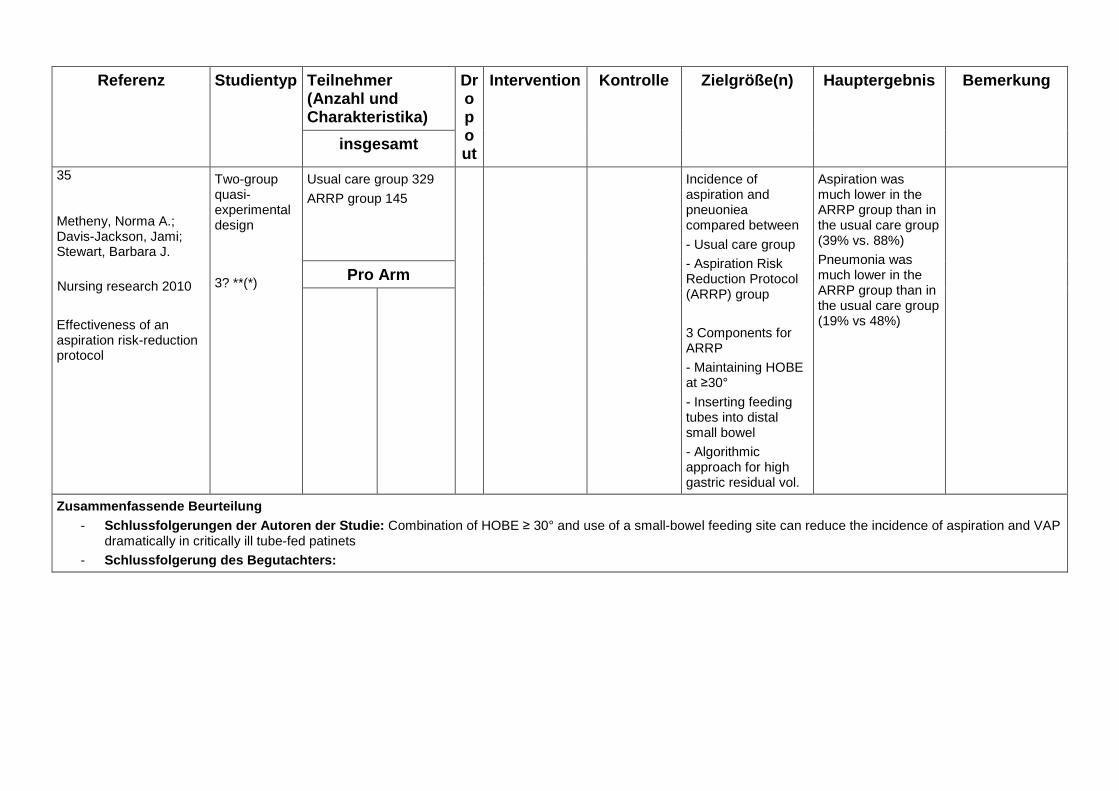
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
35 Metheny, Norma A.; Davis-Jackson, Jami; Stewart, Barbara J.
Nursing research 2010
Effectiveness of an aspiration risk-reduction protocol
Two-group quasi-experimental design
3? **(*)
Usual care group 329
ARRP group 145
Incidence of aspiration and pneuoniea compared between
- Usual care group
- Aspiration Risk Reduction Protocol (ARRP) group
3 Components for ARRP
- Maintaining HOBE at ≥30°
- Inserting feeding tubes into distal small bowel
- Algorithmic approach for high gastric residual vol.
Aspiration was much lower in the ARRP group than in the usual care group (39% vs. 88%)
Pneumonia was much lower in the ARRP group than in the usual care group (19% vs 48%)
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Combination of HOBE ≥ 30° and use of a small-bowel feeding site can reduce the incidence of aspiration and VAP
dramatically in critically ill tube-fed patinets - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
36 Metheny, Norma A.; Frantz, Rita A.
Critical care nurse 2013
Head-of-bed elevation in critically ill patients: a review
Review
4 ***
Guidelines (10Studien)
HOBE und VAP/Aspiration (8Studien)
HOBE und Druckulkus (7 Studien)
Conflicting guidelines about use of HOB
45°HOB favored Aspiration is a more immediate concern than PU Early studys show that 45° HOB is superior to a “flat in bed” position in preventing aspiration. •No RCT compare aspiration while patients are at a 30° HOBE vs 0°, or a 30° HOBE vs 45° elevation. 30° HOB elevation is recommended in practice settings, there is no direct evidence that it is as effective as a 45°HOBE in reducing aspiration.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: Unless medically contraindicated, maintain an HOBE of 45° in patients who are receiving mechanical ventilation and tube feedings; for comfort is posibile to lower the HOBE to 30° periodically; For critically ill patients at less risk for aspiration maintain an HOBE of at least 30°; optimal HOBE to balance the risks for aspiration and pressure ulcers is unknown. Schlussfolgerung des Begutachters: kein Systematisches Review! Gute Zusammefassung der Literatur.

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
37 Perrie, H.; Windsor, S.; Scribante, J.
Southern African Journal of Critical Care 2007
Nurses' accuracy in estimating backrest elevation
prospective, cross-sectional, descriptive study
3 **
39 nurses Estimated angles were correlated with measured angles and
this was correlated with demographic characteristics
42% of the nurses were accurate in their estimation of bedrest angle (correlation,0.6232). Demographic characteristics had little effect on accuracy.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Nurses could benefit from assistance in accurately estimating backrest elevation angle, as well as from education regarding strategies to decrease the incidence of VAP Schlussfolgerung des Begutachters: kleine Fallzahl, Journal??

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
38 Peterlini, Maria Angelica S.; Rocha, Patricia K.; Kusahara, Denise M.; Pedreira, Mavilde L. G.
Heart & lung 2006
Subjective assessment of backrest elevation: magnitude of error
Prospektive Studie Querschnittsstudie
4 **(*)
160 Teilnehmer (97 nurses, 48 nursing students, 15 nursing assistants
"Vorführen" von 20, 30, 35, 40 und 45° Lagerung
Schätzen des eingestellten Winkels durch Studienteilnehmer
Dann Messung des Tatsächlichen Winkels
14,9% korrekt eingeschätzt, 61,6% Überschätzt, 23,5% Unterschätzt
Pro Arm
Zusammenfassende Beurteilung - Schlussfolgerungen der Autoren der Studie: Objektivere Methode zur Umsetzung der richtigen HOBE nötig - Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
39 Peterson, M.; Schwab, W.; McCutcheon, K.; van Oostrom, J. H.; Gravenstein, N.; Caruso, L.
Critical care medicine 2008
Effects of elevating the head of bed on interface pressure in volunteers
Deskriptive Observationsstudie
3 ****
15 gesunde Erwachsene
Interface pressure profiles of the sacral area obtained for the 0°, 10°, 20°, 30°, 45°, 60°, and 75° HOBE positions Measurements obtained using a thin pressure-sensing pad placed under the sacral region
After repeated-measures analysis of variance,the HOB positions of 45°, 60°, and 75° all caused significant increases in affected areas compared with the supine measurement (P< .001) the areas with>32 mm Hg interface pressure at the HOB positions of 45°, 60°, and 75° were all significantly different from all other HOB positions The 30° HOB elevation was different from the 10° and the 20° HOB elevation positions (P< .02)
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Raising the HOB to ≥30° significantly increases the skin–support surface interface pressure, and a ≥45° HOB elevation significantly increases the area of skin exposed to a pressure >32 mm Hg Schlussfolgerung des Begutachters: kleine Fallzahl
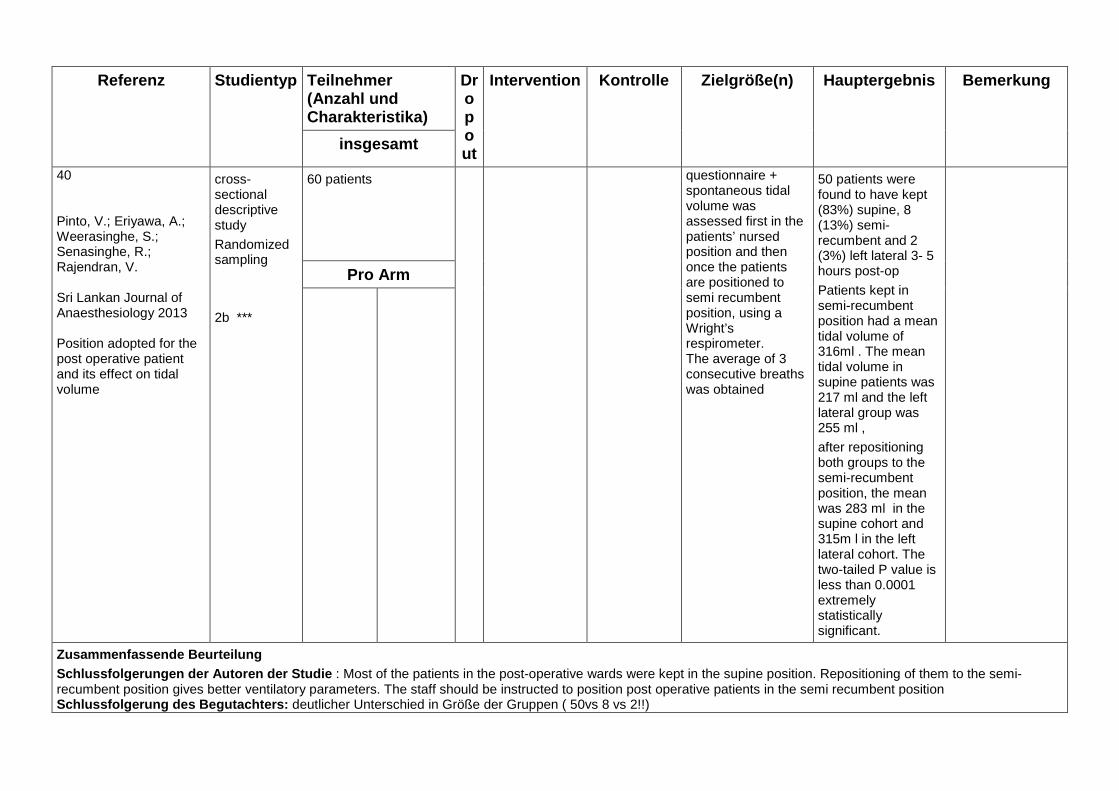
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
40 Pinto, V.; Eriyawa, A.; Weerasinghe, S.; Senasinghe, R.; Rajendran, V. Sri Lankan Journal of Anaesthesiology 2013 Position adopted for the post operative patient and its effect on tidal volume
cross-sectional descriptive study
Randomized sampling
2b ***
60 patients questionnaire + spontaneous tidal volume was assessed first in the patients’ nursed position and then once the patients are positioned to semi recumbent position, using a Wright’s respirometer. The average of 3 consecutive breaths was obtained
50 patients were found to have kept (83%) supine, 8 (13%) semi-recumbent and 2 (3%) left lateral 3- 5 hours post-op
Patients kept in semi-recumbent position had a mean tidal volume of 316ml . The mean tidal volume in supine patients was 217 ml and the left lateral group was 255 ml ,
after repositioning both groups to the semi-recumbent position, the mean was 283 ml in the supine cohort and 315m l in the left lateral cohort. The two-tailed P value is less than 0.0001 extremely statistically significant.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie : Most of the patients in the post-operative wards were kept in the supine position. Repositioning of them to the semi-recumbent position gives better ventilatory parameters. The staff should be instructed to position post operative patients in the semi recumbent position Schlussfolgerung des Begutachters: deutlicher Unterschied in Größe der Gruppen ( 50vs 8 vs 2!!)

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
41 Rooban, Nirooshan; Regli, Adrian; Davis, Wendy A.; Keulenaer, Bart L. de Annals of intensive care 2012 Comparing intra-abdominal pressures in different body positions via a urinary catheter and nasogastric tube: a pilot study
prospective observational study
single-centre
Pilot Study
3 **(*)
20 patients IAP was recorded simultaneously via the bladder catheter (bladder pressure, IBP) and via nasogastric tube (gastric pressures, IGP) in the supine and HOB30 position. Each patient had three sets of IAP measurements performed at least 4 h apart
In supine position, mean IBP was 12.3 ± 4.5 mmHg compared to IGP of 11.8 ± 4.7 mmHg. The bias between the 2 groups was 0.5 and precision of 3.7. At 30°, mean IBP was 15.8 ±4.9 mmHg compared to IGP of 13.1 ± 6.1 mmHg. The bias between both groups was 2.7 with a precision of 5.5 Comparing IBP in the supine position with IGP at 30° showed a bias of -0.8 and precision of 5.6(LA, -10.1 to 11.6 mmHg).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie IAP measured via a nasogastric tube was less influenced by changing the body position from supine to HOB30 than was bladder pressure Schlussfolgerung des Begutachters: Pilot Study!
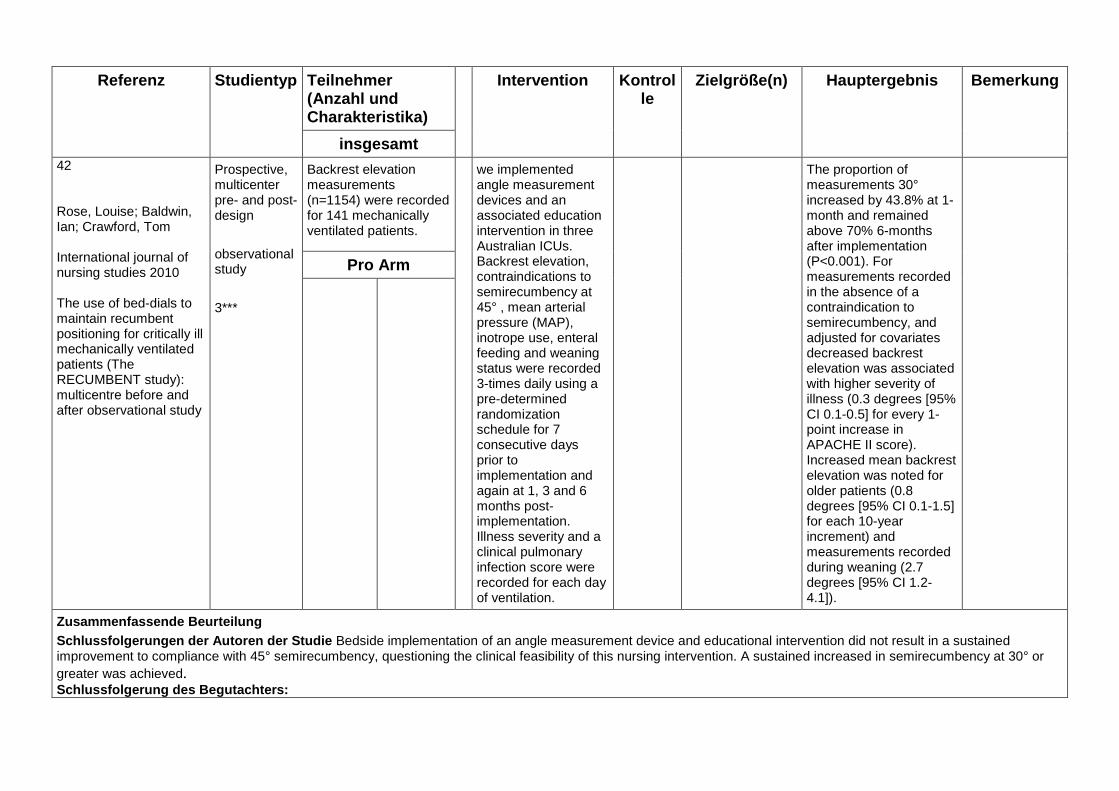
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Intervention Kontrolle
Zielgröße(n) Hauptergebnis Bemerkung
insgesamt 42 Rose, Louise; Baldwin, Ian; Crawford, Tom International journal of nursing studies 2010 The use of bed-dials to maintain recumbent positioning for critically ill mechanically ventilated patients (The RECUMBENT study): multicentre before and after observational study
Prospective, multicenter pre- and post-design
observational study
3***
Backrest elevation measurements (n=1154) were recorded for 141 mechanically ventilated patients.
we implemented angle measurement devices and an associated education intervention in three Australian ICUs. Backrest elevation, contraindications to semirecumbency at 45° , mean arterial pressure (MAP), inotrope use, enteral feeding and weaning status were recorded 3-times daily using a pre-determined randomization schedule for 7 consecutive days prior to implementation and again at 1, 3 and 6 months post-implementation. Illness severity and a clinical pulmonary infection score were recorded for each day of ventilation.
The proportion of measurements 30° increased by 43.8% at 1-month and remained above 70% 6-months after implementation (P<0.001). For measurements recorded in the absence of a contraindication to semirecumbency, and adjusted for covariates decreased backrest elevation was associated with higher severity of illness (0.3 degrees [95% CI 0.1-0.5] for every 1-point increase in APACHE II score). Increased mean backrest elevation was noted for older patients (0.8 degrees [95% CI 0.1-1.5] for each 10-year increment) and measurements recorded during weaning (2.7 degrees [95% CI 1.2-4.1]).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Bedside implementation of an angle measurement device and educational intervention did not result in a sustained improvement to compliance with 45° semirecumbency, questioning the clinical feasibility of this nursing intervention. A sustained increased in semirecumbency at 30° or greater was achieved. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
43 Rose, Louise; Baldwin, Ian; Crawford, Tom; Parke, Rachael American journal of critical care 2010 Semirecumbent positioning in ventilator-dependent patients: a multicenter, observational study
multicenter, observational study
3 ***
371 ventilator patients in 32 ICUs Measurements (n = 2112)
backrest elevation, mean arterial pressure, use of inotropic agents, enteral feeding, and weaning status were recorded 3 times per day by using a predetermined randomization schedule for 7 consecutive days (maximum 21 observation episodes). Severity of illness was recorded daily by using SOFA score
HOBE at ≥45º was noted for 112 of 2112 (5.3%; 95% CI, measurements; elevation ≥30º but <45º for 472 of 2112 (22.3%; 95% CI. Increased backrest elevation occurred during enteral feeding (2.2º, P < .001) and weaning (3.1º, P < .001). Decreased backrest elevation was associated with inotropic support (2.8º, P < .001), decreased mean arterial pressure (0.7º/10 mm Hg, P < .001), and organ failure For measurements recorded with no contraindication to semirecumbency, weaning status (P = .003) and SOFAmax score (P = .008)
remained associated with the degree of HOBE
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie backrest elevation was less than recommended and was influenced by clinical practices and patient condition Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
44 Shuster, Melanie Horbal; Sekula, L. Kathleen; Kern, John C.; Vazquez, Jorge A. Am J Crit Care 2011 Measuring intrabladder pressure with the head of the bed elevated 30 degrees
prospective, randomized, and experimental study
3? **(*)
120 Patienten intrabladder pressure measured first positioned supine with a 30° head-of-bed elevation and 25 mL of saline instilled into the bladder and again after patients were randomly repositioned to supine without any HOBE (flat) or with a 30° HOBE while supine or in right lateral or left lateral position with either 25, 50, or 200 mL of saline instilled into the patient’s bladder.
Intrabladder pressures measured with the patient in all 3 HOBE positions were higher than pressures measured with patients supine and flat after instillation of 25 mL of saline into the bladder but intrabladder pressure did not differ between the 30° HOBE positions and the supine and flat positions when 50 or 200 mL of saline was instilled into the bladder. Two-way analysis of variance showed a significant interaction between volume of saline instilled (P = .05), patient’s position (P = .007), and bladder instill volume and position interaction (P = .004).
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie repositioning patients from the S-30 to the supine position solely to measure IBP yields IBP values that are significantly lower, by approximately 5.2 mm Hg (see Figure, group 1). No significant changes in IBP occurred when the patients were repositioned from the S-30 to LL-30 or RL-30 position.. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
45 Silvestri, Luciano; Gregori, Dario; van Saene, Hendrick K. F.; Belli, Roberto; Blazic, Miranda Journal of critical care 2010 Semirecumbent position to prevent ventilator-associated pneumonia is not evidence based
Letter to the editor
4 **
meta-analysis by Alexiou et al
We believe that the authors' conclusion on semirecumbent position seems a personal opinion rather than interpretation of data. The authors are correct in saying that their findings may support the guidelines of various scientific societies on the prevention of VAP suggesting semirecumbent 45° positioning of mechanically ventilated patients. In these guidelines, the statements on semirecumbency are also based on expert opinion rather than on evidence.
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
46 Tange, K.; Kinoshita, H.; Minonishi, T.; Hatakeyama, N.; Matsuda, N.; Yamazaki, M.; Hatano, Y. Minerva Anestesiol 2010 Cerebral oxygenation in the beach chair position before and during general anesthesia
Deskriptive Observationsstudie
3 ***
30 Patienten mit Schulter OP in Beach chair Lagerung
Messung von NIRS und MAP präOP, nach Narkoseeinleitung in 30° und 60° Lagerung
MAP decreased upon anesthesia but did not further change when the patient was placed in the 30- and 60-degree head-up tilt positions However, TOI values did not change with induction of general anesthesia or placement of the patients in the beach chair position
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Under general anesthesia, the beach chair position does not alter cerebral oxygenation in patients showing normal preoperative cerebral TOI values. Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
47 van Beers, F.; van Rosmalen, J.; van Hees, A.; van Berkom, P.; Van Oers JAH Intensive Care Medicine 2010 Cardiac chair position improves ventilation and oxygenation in mechanical ventilated obese ICU patients
Pilot Study
Deskriptiv
Observationsstudie
Nur Abstract publiziert
3 *
10 obese Pat, mechanical ventilated
Position 30° HOBE with legs horizontal (semirecumbent position). Half an hour after stabilisation, end tidal CO2, tidal volume, breathing frequency and oxygen saturation were measured. Thereafter legs were placed as down as possible (cardiac chair position).
Mean SpO2 horzontal legs 96,9% vs mean SpO2 low legs 97,6%
Mean ET CO2 horzontal legs 4,9% vs mean ET CO2 low legs 4,7%mean RR/Vt horizontal legs 28,6% vs RR Vt low legs 27,2%
SpO2 and ET-CO2 signigicant changend,
RR/VT index not signigcant changend
Pdf Seite 339
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: Legs down improve ventilation and oxygenation in supported invasive ventilation Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
48 Vasquez, Donald G.; Berg-Copas, Gina M.; Wetta-Hall, Ruth The Journal of surgical research 2007 Influence of semi-recumbent position on intra-abdominal pressure as measured by bladder pressure
prospective, cross-sectional study
2b **(*)
54 trauma patients Patients underwent bladder pressure measurements at 0, 15, 30, 45° HOB position and 30° HOB position plus 15° of reverse Trendelenburg tilt; these measurements were performed in counterbalanced fashion and assessed by built-in angle indicators on the bed rails of each bed. Study participants were connected to an IAP monitoring kit via their indwelling Foley catheter.
A total of 675 bladder pressure measurements were obtained with 135 measurements at each of five HOB elevations (0°, 15°, 30°, 45°, 30° +15° tilt).
Statistically significant differences occurred between all HOB elevations. Statistically significance differences also occurred at different BMI statuses. Elevating HOB significantly increases bladder pressure measurement. Bladder pressure measurements in nonsupine positions may not provide valid interpretation for IAP, and more so in cases of increased body mass index
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie In conclusion, this study found that elevations of HOB from the supine position (positions commonly used in ICU settings) consistently and significantly increased bladder pressure measurements Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
49 Williams, Zev; Chan, Rodney; Kelly, Edward Critical care medicine 2008 A simple device to increase rates of compliance in maintaining 30-degree head-of-bed elevation in ventilated patients
Prospektiv, single-center two-phase study
3 **(*)
268 bed measurements, cohort of intubated patients,
70 nurses
4wk trial 2wks measurment of HOBE without, with angle indicator, Survey to assess satisfaction with the divice.
Average HOBE 21.8° without the device and 30,9° with the device
Compliance (defined as HOBE ≥ 28°): 23% without device, 71,5% with the device
RR 2,2
OR 9,25
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie: The Angle Indicator improved rates of adherence to bed-elevation guidelines, and hospital staff found it helpful Schlussfolgerung des Begutachters:

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
50 Wolken, Robert F.; Woodruff, Russell J.; Smith, Jan; Albert, Richard K.; Douglas, Ivor S. Respiratory care 2012 Observational study of head of bed elevation adherence using a continuous monitoring system in a medical intensive care unit
Observational study
Prospective cohort study
2b ***
98 Patient beds over a 7,5 month period
Continuous monitoring of HOBE Angle Data displayed on bedside monitors
HOBE was ≥ 30° for 76% of hours when data were displayed on bedsied monitors, and 61% of hours when not (OR 2,3
Intermittend bedside checks for HOBE ≥ 30°found 97% adherence
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie Real-time monitoring of head of bed elevation is feasible, and when combined with audible alarms and visual cues, improves > 30° elevation adherence.Intermittent bedside checks over-estimate actual adherence. Schlussfolgerung des Begutachters:
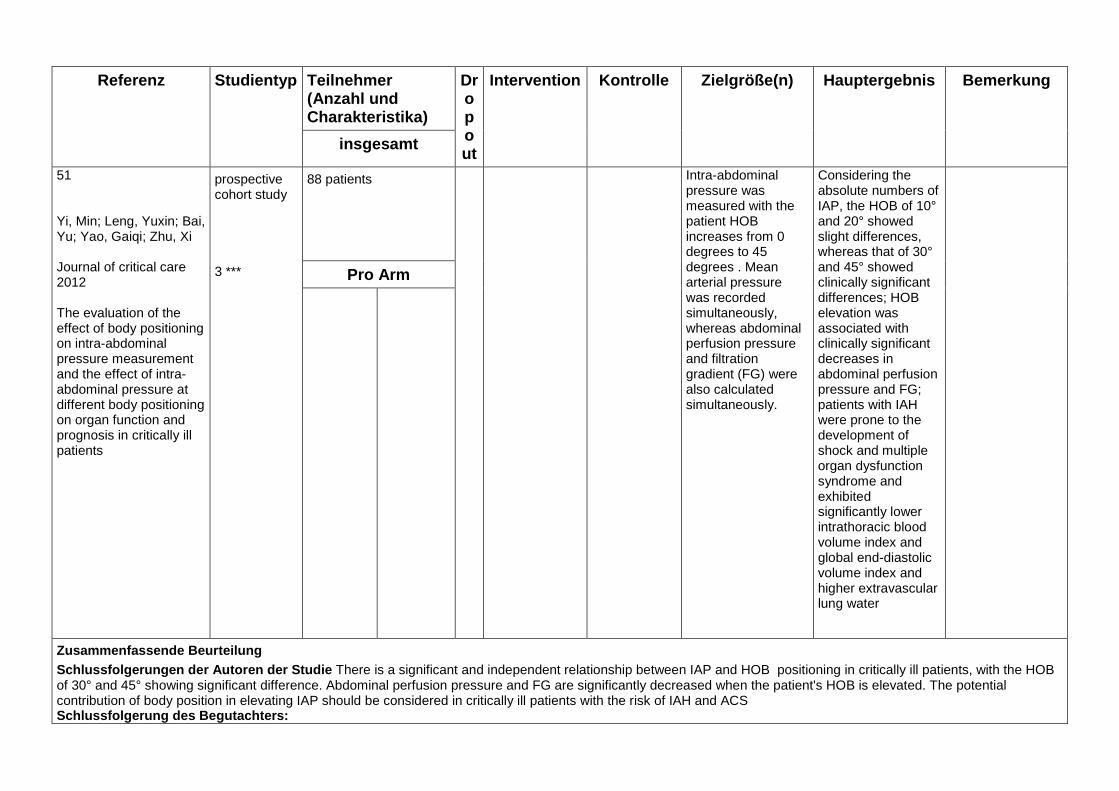
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Intervention Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
51 Yi, Min; Leng, Yuxin; Bai, Yu; Yao, Gaiqi; Zhu, Xi Journal of critical care 2012 The evaluation of the effect of body positioning on intra-abdominal pressure measurement and the effect of intra-abdominal pressure at different body positioning on organ function and prognosis in critically ill patients
prospective cohort study
3 ***
88 patients Intra-abdominal pressure was measured with the patient HOB increases from 0 degrees to 45 degrees . Mean arterial pressure was recorded simultaneously, whereas abdominal perfusion pressure and filtration gradient (FG) were also calculated simultaneously.
Considering the absolute numbers of IAP, the HOB of 10° and 20° showed slight differences, whereas that of 30° and 45° showed clinically significant differences; HOB elevation was associated with clinically significant decreases in abdominal perfusion pressure and FG; patients with IAH were prone to the development of shock and multiple organ dysfunction syndrome and exhibited significantly lower intrathoracic blood volume index and global end-diastolic volume index and higher extravascular lung water
Pro Arm
Zusammenfassende Beurteilung Schlussfolgerungen der Autoren der Studie There is a significant and independent relationship between IAP and HOB positioning in critically ill patients, with the HOB of 30° and 45° showing significant difference. Abdominal perfusion pressure and FG are significantly decreased when the patient's HOB is elevated. The potential contribution of body position in elevating IAP should be considered in critically ill patients with the risk of IAH and ACS Schlussfolgerung des Begutachters:

Evidenztabelle VAP/CAP:
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention
Kontrolle
Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
1
Bundesgesundheitsbl 2013
Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut Prävention der nosokomialen beatmunsassoziierten Pneumonie
Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut
? ****
- Die bisherige Lehrmeinung, eine Oberkörperhochlagerung bei Intensivpatienten als unabhängigen protektiven Faktor zur Prävention der VAP anzusehen, wurde aufgrund der zwischenzeitlich vorliegen-den Studien verlassen.
- Es gibt keine Evidenz für eine Oberkörperhochlagerung von beatmeten Patienten zur Senkung der Pneumonierate außer als Bestandteil in sog. Präventionsbündeln.
- Eine Therapie mit kinetischen Betten zur Prävention einer VAP kann zurzeit nicht empfohlen werden.
- Die Rolle der Lagerung für die Prävention der beatmungsassoziierten Pneumonie ist ungeklärt. Die Lagerung des Patienten muss unter klinischen Gesichtspunkten festgelegt werden
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
2 Abad, C.; McKinley, L.; Safdar, N. Journal of Clinical Outcomes Management 2008 Measures to prevent ventilator-associated pneumonia: Which are efficacious?
Review of the literature
4**(*)
Semirecumbent patient positioning has negligible costs, is a highly effective strategy to prevent VAP, and is recommended for use in all eligible patients
Nonpharmacologic strategies such as semirecumbent positioning and hand hygiene must be emphasized in an infection control program.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
3 Abbott, C. A.; Dremsa, T.; Stewart, D. W.; Mark, D. D.; Swift, C. C. Worldviews on Evidence-Based Nursing 2006 Adoption of a ventilator-associated pneumonia clinical practice guideline
3**(*) the results of 69 studies were used to establish a clinical practice guideline to prevent VAP
A clinical practice guideline was developed for the prevention of VAP and included five nursing activities: (a) head-of-bed elevation; (b) oral care; (c) ventilator tubing condensate removal; (d) hand hygiene; and (e) glove use. The effect of the CPG, inclusive of an educational intervention, was measured using an observational, prospective, quasi-experimental design.
Observation data were collected to evaluate adoption of the clinical practice guideline while caring for 106 ventilated patients. VAP rates changed at both hospitals although the change was not statistically significant. Additionally, the ICU length of stay declined at both facilities, causing cost savings.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention
Kontrolle Zielgröße(n) Hauptergebnis Bemerkung
insgesamt
4 Albertos, Raquel; Caralt, Berta; Rello, Jordi
Current opinion in gastroenterology 2011
Ventilator-associated pneumonia management in critical illness
Review
4 **(*)
it can be concluded that the implementation of care bundles on the general management of ventilated patients in daily practice has reduced the VAP rates. The main pharmacological measures to prevent VAP are... shortening weaning period,..., prevent bio-film deposition in endotracheal tube, aspiration of subglottic secretions, maintenance of adequate pressure of endotracheal cuffs, semi-recumbent position and adequate enteralfeeding.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
5 Berra, L.; Sampson, J.; Fumagalli, J.; Panigada, M.; Kolobow, T. Minerva anestesiologica 2011 Alternative approaches to ventilator-associated pneumonia prevention
Review
4 ***
Specifically, we found that keeping ventilated patients in a lateral position, which eliminates gravitational forces, is feasible and possibly advantageous
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
6 Alexiou VG, Ierodiakonou V, Dimopoulos G, Falagas ME Database of Abstracts of Reviews of Effectiveness 2009 Impact of patient position on the incidence of ventilator-associated pneumonia: a meta-analysis of randomized controlled trials
meta-analysis of randomized controlled trials
1a ****
3 RCT´s The odds of developing VAP were significantly lower among patients in the semirecumbent 45° position compared to patients in supine position The comparison of prone vs supine position group showed a moderate trend toward better outcomes regarding the incidence of VAP among patients in the prone position The subanalysis regarding the incidence of microbiologically documented VAP, the length of ICU stay, and the duration of mechanical ventilation showed that patients in the semirecumbent 45° position have a moderate trend toward better clinical outcomes.
Pro Arm
Zusammenfassende Beurteilung
Schlussfolgerungen der Autoren der Studie This meta-analysis provides additional evidence that the usual practice of back-rest elevation of 15° to 30° is not sufficient to prevent VAP in mechanically ventilated patients. Patients positioned semirecumbently 45° have significantly lower incidence of clinically diagnosed VAP compared to patients positioned supinely. On the other hand, the incidence of clinically diagnosed VAP among patients positioned pronely does not differ significantly from the incidence of clinically diagnosed VAP among patients positioned supinely Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
7 Bird, D; Zambuto, A; O'Donnell, C; Silva, J; Korn, C; Burke, R; Burke, P; Agarwal, S
Archives of surgery 2010
Adherence to ventilator-associated pneumonia bundle and incidence of ventilator-associated pneumonia in the surgical intensive care unit
Prospektive Observationsstudie
3***
VAP bundle was instituted at the beginning of the study and included head-of-bed elevation, extubation assessment,sedation break, peptic ulcer prophylaxis, and deep vein thrombosis prophylaxis
Prior to initiation of the bundle, VAP was seen at a rate of 10.2 cases/1000 ventilator days. Compliance with the VAP bundle increased over the study period from 53% and 63% to 91% and 81% in each respective SICU. The rate of VAP decreased to 3.4 cases/1000 ventilator days. A cost savings of $1.08 million was estimated.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie Initiation of the VAP bundle is associated with a significantly reduced incidence of VAP in patients in the SICU and with cost savings.
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
8 Blot, Stijn; Rello, Jordi; Vogelaers, Dirk
Current opinion in pulmonary medicine 2011
What is new in the prevention of ventilator-associated pneumonia?
Review
4**
It seems advantageous to implement care bundles rather than single prevention Measures
Intermittent subglottic secretions drainage, continuous lateral rotation therapy, and polyurethane cuffed endotracheal tubes decrease the risk of pneumonia
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
9 Bouadma, L; Mourvillier, B; Deiler, V; Le Corre, B; Lolom, I; Regnier, B; Wolff, M; Lucet, JC
Critical care medicine 2010
A multifaceted program to prevent ventilator-associated pneumonia: impact on compliance with preventive measures
Pre- and postintervention observational study
3**(*)
A total of 1649 ventilator-days were observed
Compliance with all other preventive measures was initially low and increased steadily over time (before 2-yr level, p < .0001): backrest elevation (5% to 58%).
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Haupt-ergebnis Bemerkung
insgesamt
10 Bukhari, Syed Z.; Hussain, Waleed M.; Banjar, Abdulhakeem A.; Fatani, Mohammad I.; Karima, Talal M.; Ashshi, Ahmad M. Saudi medical journal 2012 Application of ventilator care bundle and its impact on ventilator associated pneumonia incidence rate in the adult intensive care unit
Prospectiv longitudinal observation study
3 ***
2747 patients The individual bundle compliance rates were as follows: head-of-bed elevation - 99.9%; ... At the beginning, VAP rate was 2.5/1000 ventilator days, and reduced to 0.54 in the next month. The overall VAP incidence rate in 2010 was found to be 1.98 with a reduction of 1.41 by comparing with the same data of year 2009 collected retrospectively.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
11 Charles, MP; Easow, JM.; Joseph, NM.; Ravishankar, M.; Kumar, S; Umadevi, S The Australasian medical journal 2013 Incidence and risk factors of ventilator associated pneumonia in a tertiary care hospital
Observationsstudie
3 ***
76 patients Univariate analysis showed chronic lung failure, H2 blockers usage, and supine head position were significant risk factors for VAP.
Logistic regression revealed supine head position as an independent risk factor for VAP.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie
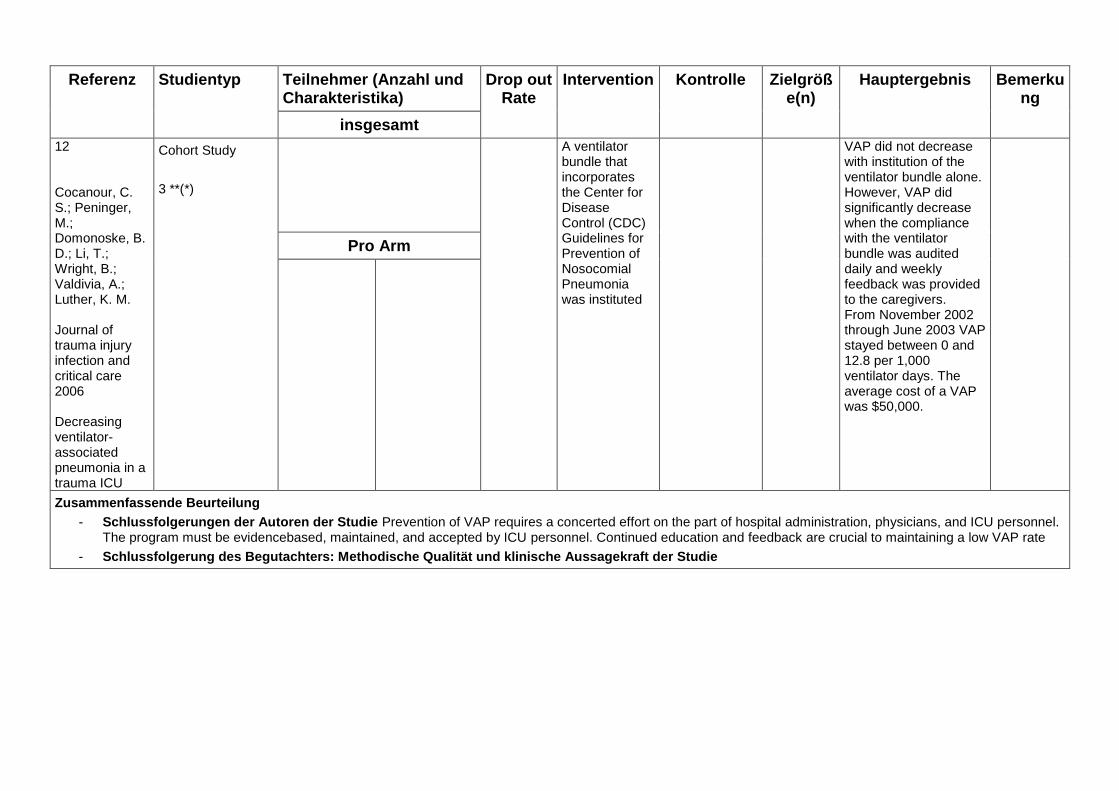
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
12 Cocanour, C. S.; Peninger, M.; Domonoske, B. D.; Li, T.; Wright, B.; Valdivia, A.; Luther, K. M. Journal of trauma injury infection and critical care 2006 Decreasing ventilator-associated pneumonia in a trauma ICU
Cohort Study
3 **(*)
A ventilator bundle that incorporates the Center for Disease Control (CDC) Guidelines for Prevention of Nosocomial Pneumonia was instituted
VAP did not decrease with institution of the ventilator bundle alone. However, VAP did significantly decrease when the compliance with the ventilator bundle was audited daily and weekly feedback was provided to the caregivers. From November 2002 through June 2003 VAP stayed between 0 and 12.8 per 1,000 ventilator days. The average cost of a VAP was $50,000.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie Prevention of VAP requires a concerted effort on the part of hospital administration, physicians, and ICU personnel. The program must be evidencebased, maintained, and accepted by ICU personnel. Continued education and feedback are crucial to maintaining a low VAP rate
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
13 Coppadoro, A.; Bittner, E.; Berra, L. Critical Care 2012 Novel preventive strategies for ventilator-associated pneumonia
Review
4 ***
Positioning of the intubated patient is believed to be a relevant factor for the development of VAP. Th e 45° semirecumbent position is widely recommended, but recent data suggest that the lateral position may be superior to prevent VAP
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
14 Delaney, A; Gray, H; Laupland, KB.; Zuege, DJ.
Critical care 2006
Kinetic bed therapy to prevent nosocomial pneumonia in mechanically ventilated patients: a systematic review and meta-analysis
systematic review and meta-analysis
1a ****
Fifteen prospective clinical trials were identified, which included a total of 1,169 participants. No trial met all the validity criteria.
There was a significant reduction in the incidence of nosocomial pneumonia (pooled odds ratio (OR) 0.38, 95% confidence interval (CI) 0.28 to 0.53), but no reduction in mortality (pooled OR 0.96, 95%CI 0.66 to1.14), duration of mechanical ventilation (pooled standardized mean difference (SMD) -0.14 days, 95%CI, -0.29 to 0.02), duration of intensive care unit stay (pooled SMD -0.064 days, 95% CI, -0.21 to 0.086) or duration of hospital stay (pooled SMD 0.05 days, 95% CI -0.18 to 0.27).
Pro Arm
Zusammenfassende Beurteilung
Schlussfolgerungen der Autoren der Studie While kinetic bed therapy has been purported to reduce the incidence of nosocomial pneumonia in mechanically ventilated patients, the
overall body of evidence is insufficient to support this conclusion. There appears to be a reduction in the incidence of nosocomial pneumonia, but no effect on mortality, duration of mechanical ventilation, or intensive care or hospital length of stay. Given the lack of consistent benefit and the poor methodological quality of the trials included in this analysis, definitive recommendations regarding the use of this therapy cannot be made at this time.
Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle
Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
15 Gadani, Hina; Vyas, Arun; Kar, Akhya Kumar
Indian journal of anaesthesia 2010
A study of ventilator-associated pneumonia: Incidence, outcome, risk factors and measures to be taken for prevention
Cohortstudy
3**(*)
The study was conducted over a period of 1.5 years, in an intensive care unit (ICU) of a tertiary care centre. A total of 100 patients who were kept on mechanical ventilator were randomly selected
The risk factor significantly associated with VAP in our study was found to be .... , supine position... Promoting nasogastric feeding. Although necessary for critically ill patients, it should be
given keeping the patients in a semi-recumbent position with the head end elevated to 45° because the supine position promotes aspiration
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
16 Gillespie, R. Southern African Journal of Critical Care 2009 Prevention and management of ventilator-associated pneumonia - The Care Bundle approach
? The key components of the Ventilator Care Bundle are: ...
• Elevation of the head of the bed 30 - 45°
...
The evidence available presents a strong argument to consider a team approach to reducing the incidence of VAP in our own critical care units; even one less episode is worth the effort.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
17 Grap, MJ; Munro, CL.; Unoki, T; Hamilton, VA; Ward, KR.
The Journal of emergency medicine 2012
Ventilator-associated pneumonia: the potential critical role of emergency medicine in prevention
Review
4**
Specifically, we recommend... continuous backrest elevation of 30-45°,...
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
18 Klompas, Michael
Expert review of anti-infective therapy 2010
Prevention of ventilator-associated pneumonia
Review
4 **
There is a paucity of studies assessing head-of-bed elevation; there appears to be a strong correlation between supine position, enteral
feeding and aspiration pneumonia but insufficient data to assess the impact of head-of-bed elevation on patient outcomes
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
19 Lawrence, Petra; Fulbrook, Paul Nursing in critical care 2012 Effect of feedback on ventilator care bundle compliance: before and after study
before and after study
3**
These increases were mostly small and statistically insignificant. ICU B’s overall compliance increase was statistically significant (p = 0·005), but its ‘all or nothing’ compliance increase (19%), whilst arguably clinically significant, did not reach statistical significance. Both ICUs achieved 100% compliance with gastric ulcer prophylaxis for all of phase 2. Head of bed elevation was the least complied with element in phase 1, and increased in ICU B only in phase 2.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out
Rate
Intervention
Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
20 Li Bassi, Gianluigi; Torres, Antoni Current opinion in critical care 2011 Ventilator-associated pneumonia: role of positioning
Review
4 ***
The most recent studies on the semirecumbent position failed to achieve an orientation of the head of the bed higher than 30° and did not corroborate any benefit of the semirecumbent position on VAP, as reported in earlier studies. To date, there is clear evidence that the supine horizontal body position increases risks of pulmonary aspiration and VAP, particularly when patients are enterally fed. Laboratory reports are emphasizing the importance of an endotracheal tube–oropharynx–trachea axis below horizontal to avoid VAP. The prone position potentially increases drainage of oropharyngeal and airways secretions and recent evidence is supporting its beneficial effects. However, several associated adverse effects preclude its regular use as a VAP preventive strategy for patients other than those with acute respiratory distress syndrome. Summary
Pro Arm
Zusammenfassende Beurteilung
Schlussfolgerungen der Autoren der Studie. The current evidence recommends avoidance of supine horizontal position in order to prevent aspiration of colonized gastric contents. The semirecumbent position has proven benefits and should be routinely used but there is still limited evidence to recommend the lowest orientation of the bed at which the patient can be safely maintained. Results from pioneering laboratory investigation call attention to new possible positions, that is lateral Trendelenburg position, aimed to avoid pulmonary aspiration and to enhance mucus clearance in intubated patients. Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
21 Loeb, Mark Clinical evidence 2010 Community-acquired pneumonia
Systematic review
GRADE evaluation of the quality of evidence for interventions
1?***
15 systematic reviews, RCTs, or observational studies that met our inclusion criteria
In this systematic review we present information relating to the effectiveness and safety of the following interventions: antibiotics (oral, intravenous), different combinations, and prompt administration of antibiotics in intensive-care settings, early mobilisation, influenza vaccine, and pneumococcal vaccine
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
22 McCoy, Tonia; Fields, Willa; Kent, Nanette Journal of nursing care quality 2012 Evaluation of emergency department evidence-based practices to prevent the incidence of ventilator-acquired pneumonia
Observationsstudie
3 ***
This project evaluated 3 post intubation evidence-based practices in the emergency department: oral care, head-of-bed elevation, and suctioning above the endotracheal tube balloon.
Ventilator-acquired pneumonia cases decreased 83% after implementing these practices. There is no need to wait for the patient to be admitted to intensive care to begin these evidence-based practices.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie: Early implementation of the EBC guidelines helps to reduce the VAP-Incidence. There is no need to wait for the patients to be admitted to the ICU to start with these procedures.
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
23 Mietto, Cristina; Pinciroli, Riccardo; Patel, Niti; Berra, Lorenzo Respiratory care 2013 Ventilator associated pneumonia: evolving definitions and preventive strategies
Review
4***
Current guidelines recommend the semi-recumbent position to reduce gastric reflux. Acting on gravitational forces, the lateral Trendelenburg position may enhance mucus flow out of the lungs and avoid leakage of contaminated oropharyngeal secretions. Its beneficial effects are highlighted by the results of numerous animal studies that have shown a reduction in VAP incidence and lung colonization associated with the orientation of the tracheal/ ETT axis slightly below horizontal. Two clinical trials assessed its safety and feasibility on humans and now a large international randomized clinical trial is ongoing to assess the efficacy of the lateral Trendelenburg position in VAP prevention.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
24 Morris, Andrew Conway; Hay, Alasdair W.; Swann, David G.; Everingham, Kirsty; McCulloch, Corrienne; McNulty, Jane; Brooks, Odette; Laurenson, Ian F.; Cook, Brian; Walsh, Timothy S. Critical care medicine 2011 Reducing ventilator-associated pneumonia in intensive care: impact of implementing a care bundle
before-and-after study
3**(*)
Compliance with head-of-bed elevation and ... were 95%–100%; ...giving overall bundle compliance rates of 70%. Compared to the preintervention period, there was a significant reduction in ventilator-associated pneumonia in the postintervention period (32 cases per 1,000 ventilator days to 12 cases per 1,000 ventilator days; p < .001).
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
25 Muscedere, John; Dodek, Peter; Keenan, Sean; Fowler, Rob; Cook, Deborah; Heyland, Daren Journal of critical care 2008 Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia: prevention
Guideline We recommend: that ... head of bed elevation to 45° (when impossible, as near to 45° as possible should be considered).
Consider: the use of rotating beds; oral antiseptic rinses.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
26 O´Keefe-McCarth, S.; Santiago, C.; Lau, G. Database of Abstracts of Reviews of Effectiveness 2008 Ventilator-associated pneumonia bundled strategies: an evidence-based prac tice
Review
4 ***
Evidence shows that VAP Bundles practices decrease VAP rates. Bundled practices result in decreased ventilator days, intensive care unit length of stay, and mortality rates. A strong association was seen, with an increased clinician compliance with VAPB protocols with decreased VAP rates
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Haupt2rgebnis Bemerkung
insgesamt
27 Ramirez, Paula; Bassi, Gianluigi L.; Torres, Antonio Current opinion in critical care2012 Measures to prevent nosocomial infections during mechanical ventilation
Review
4 **(*)
Recent experimental evidence has challenged the benefits associated with the use of the semirecumbent position; yet, these findings need to be corroborated in clinical trials A few studies suggest that causative VAP pathogens reach the lower airways primarily driven by gravity; thus, a position utterly opposite to the recommended semirecumbent, that is, lateral with a slight Trendelenburg, theoretically could have additional advantages, avoiding pulmonary aspiration of pathogen-laden oropharyngeal secretions and ultimately VAP
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
28 Rawat, N; Yang, T; Speck, K; Helzer, J; Barenski, C; Berenholtz, S American journal of medical quality 2013 An Evaluation of Ventilator-Associated Pneumonia Process Measure Sampling Strategies in a Surgical ICU
Observational study
3**(*)
The results of this study suggest that sampling HOB elevation twice as compared with once daily is unlikely to change the estimate of performance, oral care need not be frequently sampled, and high oral care compliance may predict chlorhexidine oral care compliance.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
29 Rello, J.; Lode, H.; Cornaglia, G.; Masterton, R. Intensive Care Medicine 2010 A European care bundle for prevention of ventilator-associated pneumonia
Care bundle
? **
The resulting VAP care bundles for prevention were: nonventilatory circuit changes unless specifically indicated, alcohol hand hygiene, appropriately educated and trained staff, incorporation of sedation control and weaning protocols into patient care, and oral care with clorhexidine. Adoption of these care bundles should rationalise VAP prevention practises and improve outcomes, such as length of stay
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
30 Sedwick, M. B.; Lance-Smith, M.; Reeder, S. J.; Nardi, J. Critical Care Nurse 2012 Using Evidence-Based Practice to Prevent Ventilator-Associated Pneumonia
ventilator bundle
? **
ventilator bundle includes protocols for mouth care and hand washing, head of- bed alarms, subglottic suctioning, and use of an electronic compliance feedback tool.
Adherence to practices included in the bundle increased. Compliance rates were greater than 98% for prophylaxis for peptic ulcer disease and deep-vein thrombosis, interruption of sedation, and elevation of the head of the bed. The compliance rate for the oral care protocol increased from 76% to 96.8%. Readiness for extubation reached at least 92.4%. Rates of ventilator-associated pneumonia decreased from 9.47 to 1.9 cases per 1000 ventilator days. The decrease in rates produced an estimated savings of approximately $1.5 million.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
31 Siempos, I. I.; Dimopoulos, G.; Falagas, M. E. Infectious Disease Clinics of North America 2009 Meta-analyses on the Prevention and Treatment of Respiratory Tract Infections
Review of Meta-analyses of RCTs
4 ***
This article evaluates published meta-analyses dealing with the prevention and/or treatment of respiratory tract infections of bacterial origin in adult immunocompetent patients. The infections studied were otitis, sinusitis, tonsillitis/tonsillopharyngitis, acute exacerbations of chronic obstructive pulmonary disease, community-acquired pneumonia, and nosocomial pneumonia (including ventilator-associated pneumonia)
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
32 Tolentino-DelosReyes, Arlene F.; Ruppert, Susan D.; Shiao, Shyang-Yun Pamela K. American journal of critical care 2007 Evidence-based practice: use of the ventilator bundle to prevent ventilator-associated pneumonia
Observations studie
3 **(*)
Changes in the nurses’ practices related to ventilator-associated pneumonia, including elevation of the head of the bed to 30º to 45º, were observed in 99 intubated patients.
After the education sessions, the nurses performed better on 8 of the 10 items tested (P from .03 to <.001). The areas of most significant improvement were elevation of the head of the bed (P < .001), charting of the elevation of the head of the bed (P=.009), ... Contraindications to elevation of the head of the bed did not appear to affect the nurses’ practices (P=.38).
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
33 Wip, Charity; Napolitano, Lena Current opinion in infectious diseases 2009 Bundles to prevent ventilator-associated pneumonia: how valuable are they?
Review
4 **(*)
The Ventilator Bundle contains four components, elevation of the head of the bed to 30–45°,..., aimed to improve outcome in mechanically ventilated patients, but not all are associated with VAP prevention. Although a small prospective, randomized clinical study documented that the semirecumbent position was associated with a significant reduction in VAP, more recent studies have documented that the semirecumbent position is difficult to maintain in mechanically ventilated patients and may not impact VAP reduction. The Ventilator Bundle is an effective method to reduce VAP rates in ICUs.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
34 Wren, Sherry M.; Martin, Molinda; Yoon, Jung K.; Bech, Fritz Journal of the American College of Surgeons2010 Postoperative pneumonia-prevention program for the inpatient surgical ward
A pilot prevention program was designed and implemented based on literature review
3***
The program consisted of education of physicians and ward staff and a standardized postoperative electronic order set consisting of ... head-of-bed elevation.
There was a significant decrease in ward pneumonia incidence from 0.78% in the preintervention group compared with 0.18% in the postintervention group (p = 0.006), representing an 81% decrease in incidence from 2006 to 2008. The pneumonia-prevention program was very successful in diminishing postoperative pneumonia on the surgical ward.
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie

Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n)
Hauptergebnis Bemerkung
insgesamt
35 Zanella, A.; Cressoni, M.; Epp, M.; Hoffmann, V.; Stylianou, M.; Kolobow, T. Intensive Care Medicine 2012 Effects of tracheal orientation on development of ventilator-associated pneumonia: An experimental study
Animal study
Randomized
1b? ***
26 mini pigs The incidence of VAP was evaluated in swine with orientation of trachea and tracheal tube above horizontal (model of semirecumbent position, currently recommended in patients) and below horizontal.
All eight pigs kept orientated with the trachea 45° above horizontal developed VAP and respiratory failure (PaO2/ FiO2 = 132 ± 139 mmHg) with a median of 5.5 pulmonary lobes out of 6 colonized. None of the 18 pigs kept oriented with the trachea below horizontal developed VAP; 16 had sterile lungs, while 2, ventilated for 7 days, developed a low level of colonization. Orientation of the trachea above horizontal was uniformly associated with VAP and respiratory failure; positioning the trachea below horizontal consistently prevented development of VAP
Pro Arm
Zusammenfassende Beurteilung
- Schlussfolgerungen der Autoren der Studie
- Schlussfolgerung des Begutachters: Methodische Qualität und klinische Aussagekraft der Studie
1
Bewertung der Literatur „Frühmobilisation“ (Prof. Dr. Thomas Bein) Legende: Jede Literatur wurde einem Evidenzgradschema zugeordnet. Es wurde das gleiche einfache System wie bei der Ersterstellung der Leitlinie angewendet: Methodisch geeignete Meta-Analyse von RCTs 1A Geeignete RCTs mit schmalem Konfidenzintervall 1B Gut angelegte kontrollierte Studien ohne Randomisierung 2A Kontrollierte Kohortenstudien, RCTs mit eingeschränkter Methode 2B Nicht-kontrollierte Kohortenstudien, Fall-Kontrollstudien 3 Expertenmeinungen, Editorials, Fallberichte 4 Darüber hinaus wurde eine persönliche Gesamtbewertung von * bis **** vorgenommen. Literatur mit ** soll nicht in das Verzeichnis aufgenommen werden. Es gibt nach Meinung des Bearbeiters einige „Grenzfälle“ [gekennzeichnet mit **(*) ], die möglicherweise trotz methodischer schwäche interessante Aspekte enthalten. Hier muss eine gemeinsame Entscheidung hergeführt werden.
Bei Pdf bestellt warten wir noch auf den Volltext
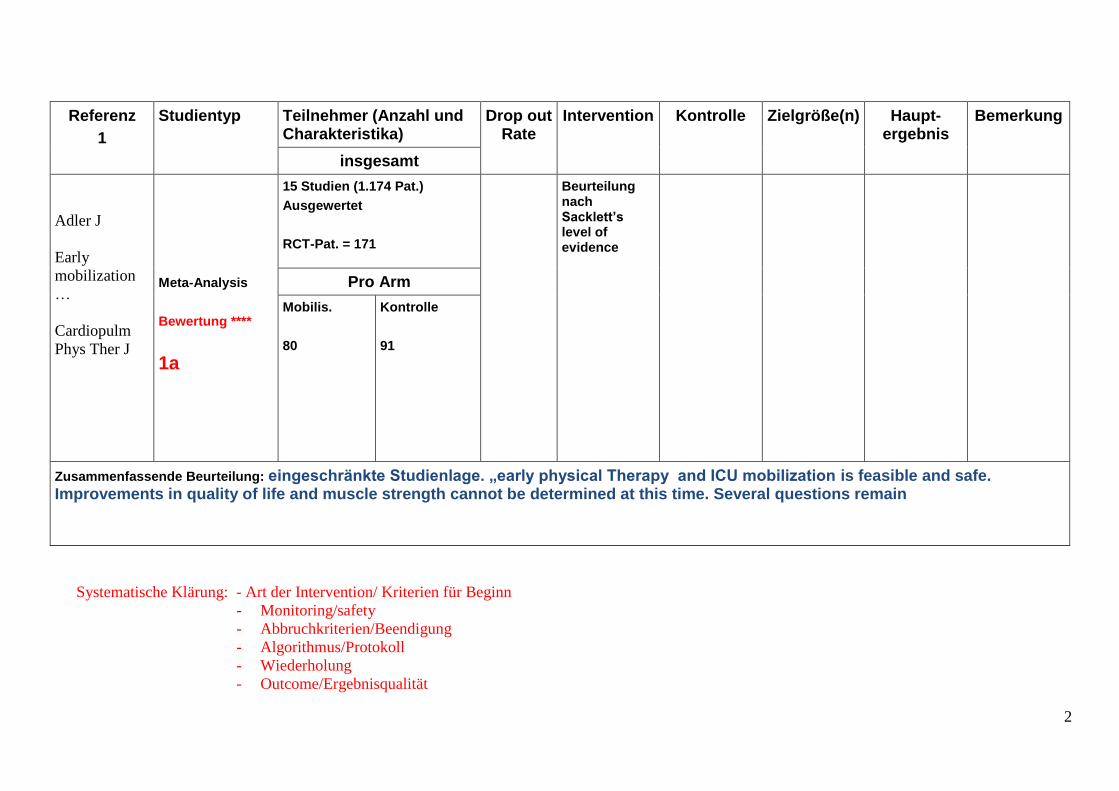
2
Referenz
1
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Adler J
Early
mobilization
…
Cardiopulm
Phys Ther J
Meta-Analysis
Bewertung ****
1a
15 Studien (1.174 Pat.)
Ausgewertet
RCT-Pat. = 171
Beurteilung nach Sacklett’s level of evidence
Pro Arm
Mobilis.
80
Kontrolle
91
Zusammenfassende Beurteilung: eingeschränkte Studienlage. „early physical Therapy and ICU mobilization is feasible and safe. Improvements in quality of life and muscle strength cannot be determined at this time. Several questions remain
Systematische Klärung: - Art der Intervention/ Kriterien für Beginn
- Monitoring/safety
- Abbruchkriterien/Beendigung
- Algorithmus/Protokoll
- Wiederholung
- Outcome/Ergebnisqualität

3
Referenz
2
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Ambrosino N
Physiotherapy
in critically ill
patients
Rev Port
Pneumol 2011
Systematic review
Bewertung **
4
Pro Arm
Zusammenfassende Beurteilung: comprehensive programs including physiotherapy should be implemented to speed-up the patients functional recorvery…early mobilisation and muscle training can improve functional outcome…still limited scientific evidence to support such a comprehensive approach to all critically ill patients.

4
Referenz
3
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Ambrosino
Minerva
Anest 2013
Review
4 **
6 Studien bei ARDS-Patienten (n = 814, keine RCT)
ARDS-Patienten!
Pro Arm
Zusammenfassende Beurteilung: active mobilisation may substantially contribute to the patients recorvery…reductions in ICU and hospital length of stay

5
Referenz
4
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Ambrosino
Eur Respir J
2012
Review
4 **
Pro Arm
Zusammenfassende Beurteilung: despite the beneficial literature, scientific evidence is limited, further studies with solid clinical short- and long-term outcome are now welcomed

6
Referenz
5
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Amidei C
Intensive and
Critical Care
Nursing 2012
Systematic review
4 **
17 Artikel
Pro Arm
Zusammenfassende Beurteilung: only one standardised tool was found that could be suitable as a safety measure, the Borg Rating of Perceived Exertion
Wichtig: beschäftigt sich mit physiologischen Variablen zur Kontrolle des Effektes der Mobilisation

7
Referenz
6
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Amidei C
Intensive and
Critical Care
Nursing 2012
Pages 73-81
Systematic review,
Concept analysis
4**
61 Artikel
Pro Arm
Zusammenfassende Beurteilung: Disciplines vary in applications of mobilization, and therapy parameters are essentially undefined.
Wichtig: Mobilisation: Konzept-Analyse, Definition
Pdf bestellt!

8
Referenz
7
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Bahadur K
Physiotherapy
2008
prospective observational study
3 **
30 Pat.
Kleine Patientenzahl,
fazit nicht abgesichert,
lediglich „feasability“:
Mobilisierung tracheotomierter Patienten ist möglich
Pro Arm
Zusammenfassende Beurteilung: 63 % sat out of bed during ICU stay. Patients not sitting out of bed demonstrated a higher mortality rate…
Pdf bestellt

9
Referenz
8
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Bailey
Crit Care Med
2007
Prospective observational cohort study
2a ***
1449 activity events in 103 patienten, davon 593 bei beatmeten Pat.
Sit on bed (16%)
Sit in chair
( 31 %)
Ambulate (42 %)
Safety and adverse events
Fall to knees
Tube removal
SBP > 200
SBP < 90
SaO2 < 80 %
< 1 % activity related adverse events
Pro Arm
Zusammenfassende Beurteilung: early activity is safe and feasible, early activity is a candidate therapy…

10
Referenz
9
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Bailey
Crit Care Med
2009
Expert opinion
4 **
Diskussion und Bewertung 83 references
Pro Arm
Zusammenfassende Beurteilung: early mobility is facilitated by change in intensive care unit culture: reorganize and manage, create a strategy, link effective practice with outcome

11
Referenz
10
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Balas
J Gerontol
Nurs 2013
Prospective case study
Pro Arm
Zusammenfassende Beurteilung:
Pdf bestellt

12
Referenz
11
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Banerjee Curr opin anesth 2011
Review
4 ***
Pro Arm
Zusammenfassende Beurteilung: ABCDE-bundle: early mobilisation may mitigate delirium and ICU-aquired weakness..
Weist auf den komplexen Zusammenhang zwischen Delirium, Sedierung und Immobilisierung hin: erläutert ABCDE-bundle
- Awakening
- Breathing
- Choice of sedation
- Delirium monitoring
- Early mobilisation
13
Referenz
12
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Bassett
Intensive and
Critical Care
nursing 2012
Prospective interventional cohort study
3 **
13 ICUs in 8 hospitals Integration of a mobility programme
Improvement of the culture of mobility
Team focus
Process of mobility
Reduction in ventilator days pre (3.0) vs 2.1 post (p = 0.06)
Statistik nicht überzeugend!
Pro Arm
Zusammenfassende Beurteilung: Improvements in team culture, communication and resources can improve adoption of early mobility…

14
Referenz
13
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Bourdin
Respiratory
Care 2010
Prospective interventional cohort study
2A ***
275 interventions in 20 Patienten
33 % während Beatmung
Chair-sitting (56%)
Tilting up arms (25 %)
Walking (11%)
feasibility Chair sitting:
-Abnahme von HR und RR, keine Änderung von SaO2 und MAP
Walking: Anstieg von HR and RR, signifikante Reduktion von SaO2
Adverse, but not harmful events in 3 %
Pro Arm
Zusammenfassende Beurteilung: Early rehabilitation is feasible and safe in patients in the ICUfor longer than 1 week.

15
Referenz
14
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Brower
Crit Care Med
2009
Expert opinion
4 ***
Pro Arm
Zusammenfassende Beurteilung: Bed rest can cause several complications that may delay or prevent recovery from critical illnesses
Excellenter Übersichtsartikel über die pathophysiologische Rationale zur (Früh)-Mobilisierung!

16
Referenz
15
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Burtin Crit
Care Med
2009
Randomized controlled trial
2B ***
90 Intensivpatienten mit erwarteter ICU Zeit > 7 tage eingeschlossen, bei 58 komplette Studie
Beide Gruppen: tägl. Physiotherapie
U-Gruppe: zusätzlich 20 min active exercise training (bedside ergometer)
Quadriceps force
Functional status
Six-minute walking
Adverse events
Hospital discharge:
6-min walking, quadriceps force and functional weel-being signific. Highe in U-Gruppe (p <0.05)
U Pro Arm C
26 32
Zusammenfassende Beurteilung: Early exercise training in critically ill patients enhanced recorvery of functional capacity, muscle force and self-perceived status

17
Referenz
16
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Casey
Journal of
Gerontology
nursing
2013
Systematic review
4 ***
Pro Arm
Zusammenfassende Beurteilung:
Focus auf Gerontologie!
Pdf bestellt

18
Referenz
17
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Centre for
reviews and
dissemination
Zhiqiang
Archives of
Physical
Medicine and
rehabilitation
2013
Meta-analysis
(narrative)
1A ****
7 RCT, 1 quasi-RCT, 1 PCS, 1 RCS for effectiveness
2 RCT, 1 PCS, 7 CS for safety
Active mobilization
Muscle strength, functional independence, ability to wean, ICU-days,
One-year mortality
↑
↓ (1 study)
Pro Arm
Zusammenfassende Beurteilung: Active mobilisation appears to have a positive effect….early active mobilization protocols may may be initiated safely in the ICU setting

19
Referenz
18
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Chang
Respiratory
care 2011
Randomized controlled trial
2b ***
34 Pat. beatmet Chair-sitting mind. 30 min für mind. 6 tage
Heart rate blood pressure resp frequ.
Muscle function, max insp pressure
Kein Unterschied zwischen den Gruppen
C Pro Arm I
18 16
Zusammenfassende Beurteilung:Six days of chair-sitting did not significantly improve respiratory muscle function in mechanically ventilated patients.

20
Referenz
19
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Cheung
Crit Care Med
2012
(abstract)
Prospective interventional cohort study
4 **
??? Phase 1: chair with sling and dangling 3/day
Phase 2: standing and walking 3/day
Incidence of pressure ulcers
Kein Unterschied in der incidence von Druckgeschwüren bei early mobility, aber significant erhöhte PU-free days.
Pro Arm
Zusammenfassende Beurteilung: The implementation of an early mobility protocol did not decrease unadjusted ICU-aquired pressure ulcer rates, but significantly increased PU-free days.
Spezifischer Fokus auf Druckgeschwüre: Einfluss der Früh-Mobilisierung
Pdf bestellt

21
Referenz
20
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Choi J
Biological
Research for
Nursing
2008
(Systematic) review
4 **
Januar 1990 – July 2007
10 „relevant“ articles, davon 5 RCT
Whole body physical therapy
Electrical stimulation
Arm exercise
Inspiratory muscle training
Prolonged mechanical ventilation in literature = 2 – 29 Tage !!
Pro Arm
Zusammenfassende Beurteilung: Overall there is support for the ability of mobility interventions to improve outcomes in patients on PMV but limitied evidence how to best accomplish this goal.
Unklare Definition von “prolonged mechanical ventilation, daher wenig Aussagekraft!

22
Referenz
21
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Clark D
Physical
Therapy
2013
Retrospective cohort with historical control
2A ***
2176 Patienten Trauma & Burns ICU
1044 historische kontrolle,
1132 early mobility program
4 levels of intervention
Early sitting
Move arms against gravity
Move leg against gravity
Standing, walking
Significant kürzere Hospital-tage
Signifkant weniger kardio-pulmonale komlikationen
Sign. Weniger psychiatr. Kompl.
Signifikant weniger Pneumonien + Thrombosen
Pro Arm
Zusammenfassende Beurteilung: Early mobilization of patients in a TBICU was safe and effective.

23
Referenz
22
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Clum SR
Crit Care Clin
2007
Review
4**
Analyse von 27 Studien zur Früh-Tracheotomie
unklar Unklare Definition von „Früh-Tracheotomie“
Pro Arm
Zusammenfassende Beurteilung:

24
Referenz
23
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Chen
Journal of
Formosan
Medical
association
2011
Randomized controlled trial
1b ****
34 Supervised physical therapy training for 6 weeks:
Weight lifting
Strengthening exercise limbs
Active transfer to chair
Standing up walking
Unsupervised training for more 6 weeks
Signifikante verbesserung für
Functional independence measurement
Ventilator free days
One-year survival (70% versus 25 %)
Gute gemachte Studie, kleine Patientenzahl!
I Pro Arm C
18 16
Zusammenfassende Beurteilung:

25
Referenz
24
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Collings
Crit Care
2013
(abstract)
Prospective randomised controlled trial
With repeated cross-over
4 **(*)
5 Patienten Oxygen consumption und carbon dioxide production steigt tendenziell mit aktiver Mobilisierung, keine Statistik
Pro Arm (cross over)
5 Pat.
Passive chair transfer
5 Pat.
Active sitting
Zusammenfassende Beurteilung: a higher rate of oxygen consumption when sitting…important consequences for early mobilization….

26
Referenz
25
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Crawford J
Am Phys Ther
Ass
2011
Prospective interventional cohort
3 **
24 Patienten assessed, 10 enrolled, 7 survived
Pro Arm
Zusammenfassende Beurteilung: it was possible to standardize early mobilization procedures among rehabilitation specialists
Sehr kleine Fallstudie
Geriatrische Patienten: feasibility mit Physiotherapeut

27
Referenz
26
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Dickinson S
Crit Care
Nursing Q
2013
Prospective interventional observational study
3**
???? Inzidenz von Druckgeschwüren unter Frühmobilisierung
Pro Arm
Zusammenfassende Beurteilung: Despite implementation of the early mobility protocol, we did not see an improvement in the pressure ulcer rate overall
Pdf bestellt

28
Referenz
27
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Doiron K
Cochrane
Library 2013
Issue 10
Protokoll der
Cochrane Meta-analysis
1A ***
GRADE System
Pro Arm
Zusammenfassende Beurteilung:
Methodischer Teil wichtig: welche Patienten, welche Fragestellungen, welche Methoden, Definitionen

29
Referenz
28
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Drolet
Phys Ther
2013
Prospective interventional cohort study
3***
542 Pat. in ICU and IMC
Erhöhung der Frühmob-Rate durch Protocol
Frühmob < 72 h:
ICU: von 6,2 % auf 20,2 %
IMC: von 15,5 % auf 71,8 %
Pro Arm
Zusammenfassende Beurteilung: a nurse-driven protocol increases the rate of patient ambulation during the first 72 hrs
Protokoll zur Frühmob. ist als appendix dabei

30
Referenz
29
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Duey
Crit Care Med
2012
(abstract)
Prospective interventional cohort study
(case control)
3 ***
30, verglichen mit histor. Kontrolle (case control)
2 X 20 min /d
Im kreg tilt bed mit Steigerung des Winkels 15 Grad tägl.
Rate of perceived exertion from
1,46 to 4,5 (p< 0.001)
No difference between groups!
Pro Arm
Zusammenfassende Beurteilung: Early mobility was safe and feasible. Subjects experience functional improvement.

31
Referenz
30
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Dzierba
Crit Care Med
2012
(abstract)
Retrospective cohort
3 *
661 Patienten Sedation protocol +
Early mobilization
Sedierungs-Verbrauch, Mobilisierung
Sedierung signif. Reduziert,
effekte auf Frühmob nicht dargestellt
Pro Arm
Zusammenfassende Beurteilung: keine aussage zum Effekt auf die Frühmob

32
Referenz
31
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Engel
Crit Care Med
2013
Systematic Review:
Description of three
Prospective interventional cohort projects
2a ***
Dezidiertes Früh-Mobilisierungs-konzept
Reduced ICU and hospital length of stay at 3 institutions,
Decreased rates of delirium and sedation
Pro Arm
Zusammenfassende Beurteilung:
Wichtig: sehr guter praktisch orientierter Früh-Mobilisierungsplan!

33
Referenz
32
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Engels PT
Crit Care Med
2013
Systematic review
2b ***
103 Artikel Ausführliche Darstellung der Empehlungen zur mobilisation bei unterschiedlichen Verletzungsarten
Pro Arm
Zusammenfassende Beurteilung:
Sorgfältige Darstellung der Empfehlungen für einzelne Verletzungsmuster: spine, facial, chest etc

34
Referenz
33
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Dull JL
Physical
therapy 1983
Randomized controlled trial
1b ***
49 Patienten, 3 Interventionen:
Exercise 1: 16
Exercise 2: 16
Exercise 3: 17
Exercise 1:
Early mob. 2x/d:
Hinsetzen aufstehen
Exercise 2: 1 + max. Atemübungen
Exercise 3: 1 + incentive spirometer
Keine signifikanten Unterschiede zwischen Übungsprogrammen bzgl .Lungenvolumen und post. Komplikat.
Pro Arm
Zusammenfassende Beurteilung: maximale inspiratorische Atemübungen und/oder incentive Spirometrie + Frühmobilisation sind der Frühmobilisation alleine nicht überlegen bzgl. Verbesserung lungenfunktion + post. pulmonale Komplitationen

35
Referenz
34
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Everingham K
Crit Care
2010
(abstract)
Prospective interventional cohort study
3***
49 Patienten 1 Sitzung Physiotherapie
RASS und BPS (Behavioural Pain scale) vor während und nach der anwendung
33 % erlebten Agitation und 98 % erlebten Schmerzen
Pro Arm
Zusammenfassende Beurteilung: The majority of patients experienced pain, while only one-third experienced agitation. Adequate levels of analgesia are achieved.
Wichtiger Aspekt: Schmerzen und Agitiertheit während Physiotherapie/Mobilisierung

36
Referenz
35
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Fan E
Respir Care
2012
Systematic review
4***
Pro Arm
Zusammenfassende Beurteilung:
Ausführliche und gut zusammengefasste Begründung für Frühmobilisation und Sichtung aktueller Studien

37
Referenz
36
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Files D
Crit Care
2013
abstract
Randomized controlled study
4**
100 Gruppe 1: 1x pro Tag Physiotherapie/Mobilisierung
Gruppe 2: „usual care“
Short Physical Performance Battery (SPPB)
Kein unterschied in Beatmung, ICU days, hospital days und mortality
SPPB im Trend (p = 0.06) besser in Gruppe 1
Pilot studie
Pro Arm
50 50
Zusammenfassende Beurteilung: In this pilot study early ICU rehabilitation was safe and was associated with numerically although not statistically improvement.

38
Referenz
37
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Flanders
Advanced Crit
Care 2009
Review ??
4**(*)
Pro Arm
Zusammenfassende Beurteilung: ???
Pdf bestellt

39
Referenz
38
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Garzon-
Serrano
PM R 2011
Prospective interventional observational study
2b***
63 pat.: 179 mobilizations Bed mobility
Transfer out of bed, gait training
SICU optimal mobilization scale
Patients level of mobilization achieved by physical therapists was higher (p<0.001) compared with nurses.
Different barriers for mobilization were identified. No mobilization-assoziated adverse events were observed.
Pro Arm
Zusammenfassende Beurteilung: Physical Therapists mobilize their critical ill patients to highe levels compared with nurses Different barriers for mobilization exist.
Wichtig: Physiotherapie hat einfluss auf mobilisierungslevel!
Pdf bestellt

40
Referenz
39
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Genc
Cardiopulm
Phys Ther J
2012
Retrospective observational study
3***
31 obese patients 37 Mobilsierungen
Veränderungen von Sättigung und hämodynamik
Significant:
Resp. Rate ↑
SpO2 ↑
Respiratory reserve ↑
Hämodynamik ≈
Pro Arm
Zusammenfassende Beurteilung: Early mobilisation in in obese patients is safe and promotes respiratory reserve

41
Referenz
40
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Genc
Intensive Care
Med 2010
abstract
Prospective observational study
3**(*)
87 abdominal injury patients with pre sufficent and pre insufficient cardiac and respiratory reserve
Mobilization
(sitting, standing, walking)
Cardiac and respiratory reserve
Kein Unterschied in Hämodynamik und Atemverhalten zwischenRR- pre-insuffcient und RR-pre-sufficient Patienten während Mobilisierung, aber signif. Unterschiede bei CR-Gruppen
Pro Arm
Zusammenfassende Beurteilung:It is important to consider respiratory and hemodynamic parameters before and while mobilization

42
Referenz
41
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Gosselink R
Intensive Care
Med 2008
Sytematic review +
Statement/Recommendations of ESICM/ERS
1A ****
117 Artikel Active or passive mobilization should be instituted early (C )
Pro Arm
Zusammenfassende Beurteilung: There is a need to standardize pathways, to define the professional profile of physiotherapists and increase the awareness of the benefits of prevention and treatment of immobility
Ausführliche Beschreibung der gegenwärtigen Evidenz, praktische anwendungsempfehlungen + Definitionen, Algorithmen

43
Referenz
42
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Gosselink R
Curr Opin Crit
Care 2012
Expert opinion
4 **(*)
86 Artikel
Pro Arm
Zusammenfassende Beurteilung: Daily evaluation of every critically ill patient should include evaluation oft he need for bedrest and immobility. Interdisciplinare team with physical therapists, occupational therapists, nurses and medical staff

44
Referenz
43
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Cuesy
J Stroke Cereb
rovasc Dis
2010
Randomzied controlled trial
1b***
223 patients with acute ischemic stroke < 48hrs
Group A
“turn mob”: turning and passive mobilization
Group B:
Standard treatment
Incidence of nosocomial pneumonia < 14 d
Group A:
12,6 %
Group B:
26,8 %
P= 0.008
A Pro Arm B
111 112
Zusammenfassende Beurteilung: The turn mob program applied on patients during the acute phase of ischemic stroke decreases the incidence of nosocom,ial pneumonia

45
Referenz
44
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Haines
Physiotherapy
2013
Prospective observational cohort study
3***
72 patients with high-risk abdominal surgery
Mobilise away from the bed
Incidence of pulmonary complications
Barriers to mobilize
39 % incidence
3x höhere Wahrscheinlichkeit für pulm. Kompl. Für jeden postop Tag ohne Mobilisierung
52 % Hindernis für Mobil am 1. Post Tag
(Hypotension)
Pro Arm
Zusammenfassende Beurteilung: Association between delayed postoperative mobilisation und postop pulmonalen komplikationen.
Pdf bestellt

46
Referenz
45
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Hanekom
Clinical
Rehabilitation
2011
Expert opinion/systematic review
(Delphi-process)
1A ****
28 klinische Algorithmen 34 statements
Pro Arm
Zusammenfassende Beurteilung:
Internationaler Delphi-prozess mit klinischen Empfehlungen und Algorithmen

47
Referenz
46
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Hanekom
Crit Care
2012
Prospective interventional cohort study
2A ****
193 Pat. Surgical ICU Protocol care
(3 weeks):
Physiotherapy service exclusively providing early mobility
Usual care
(3 weeks)
Protocol care:
Intubation RR 0,16
Extubation failure RR 0,23
TISS-28 differenz 1,99 (p = 0.04)
Hospital discharge 4 days earlier (p = 0.05)
Barthel-Index im trend besser
Pro Arm
Zusammenfassende Beurteilung:

48
Referenz
47
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Herridge M
CMAJ 2008
Editorial
4 **(*)
Pro Arm
Zusammenfassende Beurteilung: A cultural shift in the ICU to greater mobility and increased wakefulness may decrease the morbidity oft he ICU stay

49
Referenz
48
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Hodgson
Crit Care
2013
Clinical review
4**
58 Artikel
Pro Arm
Zusammenfassende Beurteilung:
Kritik: Definition von „early mobility“, Qualität der bisherigen Studien…

50
Referenz
49
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Hopkins
Crit Care Clin
2007
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung:
51
Referenz
50
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Hough
Curr opin Crit
Care 2013
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung:

52
Referenz
51
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kalisch B
J Nursing
Care Qual
2013
Systematic review
4**(*)
24 Studien, die sich mit „safety“ während Mobilisation beschäftigen
Pro Arm
Zusammenfassende Beurteilung: The findings from from these studies suggest that early mobilization of hospitalized adults is safe
Pdf bestellt

53
Referenz
52
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kasotakis
Crit Care Med
2012
Prospective non-interventional cohort study
3**
113 SICU-patients Anwendung des Surgical Intensive Care Unit Optimal Mobility Score
ICU stay
Hospital stay
Grip strength
Multivarianzanalyse:
Score: einziger unabhängiger predictor für mortality
Score
Hypotension
Hypernatremia:
Independent predictors of ICU-stay
Pro Arm
Zusammenfassende Beurteilung:
Kritik: ICU-stay kein guter Parameter heutzutage!

54
Referenz
53
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kayambu G
Crit Care Med
2013
Systematic review + meta-analysis
1A ****
10 randomized clinical trials Physical therapy
Signifcant positive effect:
Quality of life
Physical function
Peripheral muscle strength
Respiratory muscle strength
ICU stay
Hospital stay
No effect on survival
Pro Arm
Zusammenfassende Beurteilung: Physical therapy in the ICU appears to confer signifcant benefit….
“early mobilization”: 1. Postoperative day – 96 hrs….
Fliessender Übergang zwischen passive Bewegung und aktiver Mobilisierung…

55
Referenz
54
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kirkeby-
Garstad
Acta
Anesthesiol
Scand 2005
Prospective observational cohort study
3***
31 patients after coronary artery bypass grafting
Mobilization on postop day 1 + 2:
Patient stood up and walked on the spot for 3 min
SVO2, cardiac index, oxygen delivery
Cardiac index and oxygen delivery were reduced (p =0.000)
Oxygen consumption increased (p = 0.000)
Pro Arm
Zusammenfassende Beurteilung: Patients with CABG exhibit a marked desaturation during early postoperative mobilisation

56
Referenz
55
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kocan
Crit Care Nurs
Quat 2013
Expert opinion
4**(*)
Pro Arm
Zusammenfassende Beurteilung:
Spezielle Aspekte der Mobilisierung bei neurochirurg. Patienten
Pdf bestellt

57
Referenz
56
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kress
Crit Care Med
2009
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: With preliminary studies demonstrating remarkable feasibility and successes, further prospective studies studies are needed

58
Referenz
57
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Kress
Crit Care Clin
2013
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: Early mobilization is possible in patients who are alert, even during mechanical ventilation and has been associated with significant improvements in ICU patient outcomes.

59
Referenz
58
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Leditschke
Cardiopulm
Phys Ther J
2012
Prospective observational cohort study
3**
106 patients mixed medical surgical iCU
4-week prospective audit
Number of mobilization
Type of mobilization
Adverse events
Reasons for immobilize
Mobilization in 54% patient days
2 episodes of adverse events (1,1 %)
In 47 % of non-immobilization, potential avoidable factors identfied
Pro Arm
Zusammenfassende Beurteilung: Critically ill patients can be safely mobilized for much of their ICU stay

60
Referenz
59
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Lipshutz
Anesthesiolog
y 2013
Review/Education
2b***
5 RCT’s
Pro Arm
Zusammenfassende Beurteilung: Early mobilization is safe and feasible in most ICU patients and improves outcomes.
Didaktisch gute Darstellung der ICU weakness und der wichtigsten RCT’s zur Frühmobilisation
61
Referenz
60
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Lipshutz
ICU Director
2012
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: Early mobilization is safe and feasible in most ICU patients and improves outcomes.

62
Referenz
61
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Lord
Crit Care Med
2013
Expert opinion/financial modeling
4**(*)
900 admissions/per year ICU Early physical rehabilitation programme
22 % length of stay reductions
=
Einsparung von 817.000 $ per year
Pro Arm
Zusammenfassende Beurteilung: Investment in an ICU early rehabilitation programme can generate net financial savings for U.S. hospitals.
USA-Kalkulation von Kostenersparnis durch frühe Rehab-Maßnahmen auf der ICU. Interessanter Ansatz, allerdings nicht auf D übertragbar

63
Referenz
62
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Lunardi
ICU Director
2012
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung:

64
Referenz
63
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Mah
Am J Surg
2013
Prospective interventional cohort study with non-randomized control
4**
59 Pat. Surgical ICU Team-based resource efficient mobility program
Both groups improved on all measures
Sitting balance was better in the intervention group
Intervent. Pro Arm
28 31
Zusammenfassende Beurteilung: a team based resource-efficient apporach to early mobilisation is feasible and effective in the ICU
Unklare “Randomisierung”, schwaches Studiendesign, schwacher outcome-Parameter

65
Referenz
64
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Malkoc
Int J Rehab
Research
2009
Prospective interventional cohort study with historic control
3***
510 Patienten, mechanically ventilated
Chest physiotherapy program
No chest physiotherapy program
Ventilator dependency ↓
(p < 0.05)
Length of stay in ICU ↓
(p < 0.05)
Pro Arm
Zusammenfassende Beurteilung: Physiotherapy has a great impact on ventilatory dependency and length of stay in the ICU
Pdf bestellt

66
Referenz
65
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Mendez-
Telles
Respir Care
2012
Systematic review
2b ***
Pro Arm
Zusammenfassende Beurteilung: growing evidence demonstrating the feasibility and safety of early physical rehabilitation as well as their benefit on patients outcome

67
Referenz
66
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Morris
Crit Care Med
2008
Prospective interventional cohort study and historic control
2b ***(*)
330 Mobility protocol within 48hrs of mechanical ventilation
Out of bed:
Protocol day 5
Control day 11
(p<0.001)
ICU stay:
Protocol 5.5 d
Control 6,9 d
(p=0.025)
Hospital stay:
Protocol 11.2d
Control 14.5 d
(p=0.006)
I Pro Arm c
165 165
Zusammenfassende Beurteilung:
68
Referenz
67
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Morris
Am J Med Sci
2011
Retrospective observational cohort
3**
Fragebogen an 280 Überlebende nach akuter resp. Insuffizienz und Teilnahme an 1. Studie (Ref 66)
Lack of early mobility (OR 1.77) predicted readmission or death within 1 year
Pro Arm
Zusammenfassende Beurteilung: may provide further support for early mobilization

69
Referenz
68
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Mulamula A
Am J Respir
Crit Care Med
2010
(abstract)
Prospective observational cohort study
3**(*)
166 Pat. 616 Mobilisierungen Programm zur Durchführung der Mobilisierungen ohne zusätzliches Personal
Zustimmung der Pflegekräfte für dieses Programm = 64 %, erheblicher aufwand
Pro Arm
Zusammenfassende Beurteilung:
Interessanter Versuch, mit bestehenden Personal-Resourcen ein Mobilisierungsprogramm aufzustellen

70
Referenz
69
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Nava S
Arch Phys
Med Rehabil
1998
Randomized controlled
Trial
1b ****
80 COPD patients on ICU Pulmonary rehabilitation program
Passive mobilization
Early deambulation
Muscle training
treadmill
„standard care“
6-min walking distance in intervention group ↑ (p<0.001)
Maximal insp. Pressure in intervention group ↑ (p<0.05)
Dyspnea-VAS in intervention group more ↑
I Pro Arm C
60 20
Zusammenfassende Beurteilung: COPD-ICU-patients

71
Referenz
70
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Needham D
Arch Phys
Med Rehabil
2010
Prospective interventional cohort study
2A ***
57 ventilated patients 4 d or longer “compared with before”
Early physical Medicine and rehabilitation programme with fulltime physical therapists
Standard care Benzodiazepines ↓ (p=0.002)
Delirium + sedation scores ↓ (p=0.003)
More rehabilitation per patient (7/1) p<0.001)
Higher functional mobility (p=0.03)
Trend for ICU- and hospital stay ↓
Pro Arm
Zusammenfassende Beurteilung:
72
Referenz
71
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
O’Connor
Crit Care
Resusc
2009
Systematic review
1A ****
59 Studien Pooled data show a non-significant mortality benefit in favour of early mobilisation
Pro Arm
Zusammenfassende Beurteilung:
Sehr gute sorgfältige Übersicht + praktischer Algorithmus Frühmobilisation

73
Referenz
72
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Olkowski B
Phys Ther
2013
Retrospective cohort
25 Patienten mit zerebr. Aneurysma + SAB
Early mobilisation (< 48 h)
86.1 % early mob possible
Begin at 3,2 d after event
In total 11,4 sessions
Adverse events in 5,9 %
Pro Arm
Zusammenfassende Beurteilung:

74
Referenz
73
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Olsen
Crit Care Med
2010
(abstract)
Prospective interventional cohort, comparison with historical cohort
4**
145 „benchmark
366 study period
Referenz Studientyp Teilnehmer (Anzahl und Charakteristika)
Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Pro Arm
Zusammenfassende Beurteilung:
Early mobility (< 24h)
ICU days from 14.5 to 7.0 days
Hospital days from 16.1 to 8.7 days
Hospital mortality from 32.4 % to 23.8 %
ICU costs from 56.187 to 50.271 $
Pro Arm
Zusammenfassende Beurteilung: Mobility protocol: substantial cost saving for the hospital (2.887.008 $ a year), reduction in hospital length of stay and mortality

75
Referenz
74
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
Insgesamt
Olsen MF
World J surg
2011
Systematic review
15 articles, davon 3 RCT Fast-track in abdominal + thoracoabdominal surgery
Pro Arm
Zusammenfassende Beurteilung:

76
Referenz
75
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Paratz JD
Phys Ther
Rev
2011
Review
4**
Pro Arm
Zusammenfassende Beurteilung: controlled clinical trials are needed…

77
Referenz
76
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
Insgesamt
Patel
Curr Opin
Anesth
2013
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung:
78
Referenz
77
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Patel
Am J Respir
Crit Care Med
2010
(abstract)
Retrospective analysis of a prospective RCT
3**(*)
100 patients after participation of early mobilization study
Complications of critical illness
VAP
Gastrointest. Hemorrhage
Bacteremia
Barotrauma
Thrombosis
Cholestasis
Sinusitis
Skin ulcer
Equal number of complications between groups
(p=0.88)
I Pro Arm C
48 52
Zusammenfassende Beurteilung: The benefit of early mobilization is not explained by the avoidance of complications of critical illness

79
Referenz
78
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Pawlik A
Crit Care Nurs
Clin N Am
2012
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: Mobilizing patients early in the course of critical illness may improve outcomes

80
Referenz
79
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Perme C
Am J Crit
Care
2009
Educational expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: …a collaborative effort oft he multidsziplinary team to provide safe mobilization….

81
Referenz
79a
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Perme
Cardiopulm
Phys Ther J
2013
Prospective observational cohort study
3**(*)
77 Patienten mit Femoralketheter
210 separate physiotherpy sessions with 630 mobility activities
No catheter related complications
Pro Arm
Zusammenfassende Beurteilung: …Standing and waking were feasible in patients with femoral catheters…

82
Referenz
80
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Priyakshi
Bezbaruah
Intern J
Health &
Allied Scie
2012
Randomized controlled trial
2b***
15 Patienten on mechnical ventilator
Graded early mobilization
Mobilized as soon as their vital signs were stable
Heart rate < 110
MAP 60-110
FIO2 < 0.6
SaO2 > 88%
Routine physiotherapy after extubation
First day out of bed:
I = 2.5
C = 7.8
Length of ICU stay:
I = 5,6
C = 8
P<0.001
I Pro Arm C
8 7
Zusammenfassende Beurteilung: early mobilization showed better outcome compared to routine physiotherpay in length of stay
ICU length of stay ist ein schlechter outcome-Parameter!

83
Referenz
81
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Rahimi RA
Phys Ther
2013
Case report
4**
3 patients on ECMO Versuch der mobilisierung mit ECMO
Bei 2 von 3 Pat. War die Mobilisierung mit ECMO nicht möglich
Pro Arm
Zusammenfassende Beurteilung: greater expereience is needed to more fully evaluate the safety of rehabilitation on ECMO

84
Referenz
82
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Abrams
Crit Care
2014
Retrospective cohort
3**(*)
100 patients with ECMO 35 % with active physiotherapy
7,2 physiotherapy sessions on ECMO
18 patients ambulated
No PT-related complications
Pro Arm
Zusammenfassende Beurteilung: Active physiotherapy including ambulation can be achieved safely and reliably in ECMO patients with an experienced multidisciplinary team
Bisher größte Datensammlung zur Mobilisierung bei ECMO-Patienten

85
Referenz
83
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Rukstele
Crit Care Nurs
Q
2013
Expert opinion
4**(*)
Pro Arm
Zusammenfassende Beurteilung: this article describes the process of incorporating family into an intensive care unit early, progressive mobility protocol
Interessanter Aspekt: Einbeziehung der Familie in die Frühmobilisierung
Pdf bestellt

86
Referenz
84
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Schweickert
Lancet 2009
Randomized controlled trial
1B ****
104 sedated patients on mechanical ventilation < 72 hrs
Early exercise and mobilization with sedation interruption
Wenn hämodynamisch + respiratorisch stabil
Standard care Independent functional status at hospital discharge:
I = 59 %
C = 35 %
(p=0.02)
Duration of delirium:
I = 2 d
C = 4 d
(p=0.02)
Ventilator-free-days:
I = 23,5 d
C = 21,1 d
(p=0.05)
One serious adverse event (SaO2 < 80 %)
In 498 therapy sessions
Discontinuation of therapy in 4 %
I Pro Arm C
49 55
Zusammenfassende Beurteilung:

87
Referenz
85
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Schweickert
Chest
2011
Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: The benefits of early mobilization include reductions in length of stay as well as improvements in strength and functional status

88
Referenz
86
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Stiller
Physiotherapy
Theory &
Practice
2004
Prospective interventional cohort study
3**(*)
31 patients in ICU with „marginal“ cardiac and/or respiratory reserve, 50 % der Pat. beatmet
Mobilisation: sitting and standing
Hämodynamik + Oxygenation
„deterioration in clinical status“
Heart rate ↑
Blood pressure ↑
Significance
Oxygen saturation ↓
Non-significance
In 4.3 % deterioration during mobilisation =
intervention
Pro Arm
Zusammenfassende Beurteilung:
Wichtiger Aspekt: hämodynamische + respiratorische Effekte der mobilisierung

89
Referenz
87
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Stiller
Crit Care Clin
2007
Expert opinion
Educational
4**
Pro Arm
Zusammenfassende Beurteilung:
Praktischer Algorithmus zur Prä-Evaluation vor Mobilisierung und zum Monitoring wähtend Mobilisierung

90
Referenz
88
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Stiller
Chest 2013
Systematic review
1A****
55 Studien
Pro Arm
Zusammenfassende Beurteilung:

91
Referenz
89
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Talley
Crit Care Nurs
Q
Prospective observational cohort study + literature review
3***
109 patients on cont. Renal rpelacement therapy
mobilisation Safety, adverse events
No significant adverse patients events
Pro Arm
Zusammenfassende Beurteilung: This deliberate intervention allows CRRT patients to safely engage in mobility activities to improve this populations outcome.
Spezielles Pat. Kollektiv: Mobilisierung während kont. Hämofiltration Pdf bestellt

92
Referenz
90
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Taylor
J Burn Care &
Research
2013
(abstract)
Prospective interventional cohort study mit historischer Kontrolle
4**
180 patienten histor Kontrolle
225 Patienten mit Intervention
Early mobility project
Pressure ulcer rate:
Historisch 41,7 % per month
Intervention 7,1% per month
Reduktion der „restraints“ (Fixierung) von 156.9/month auf 63.55/month
Pro Arm
Zusammenfassende Beurteilung:mobilizing patients with burns is safe and effective. An early mobility protocol can help to reduce the incidence of pressure ulcers and use of restraints.
Mobilisierung bei Verbrennungspatienten

93
Referenz
91
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Thomsen
Crit Care Med
2008
Prospective interventional cohort study, vergleich mit historischer kontrolle
3**(*)
104 beatmete Patienten (> 4 d) with transfer to ICU where early activity is priority
Early activity protocol
Incidence of ambulation
3X höhere Inzidenz der Frühmobilisierung nach ICU-Verlegung
Femal gender (p=0.019), absence of sedatives (p=0.009), lower APACHE-score (p=0.017) predict early ambulation
Pro Arm
Zusammenfassende Beurteilung:

94
Referenz
92
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Timmerman
Dimens Crit
Care Nurs
2007
Education – expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: Nurses…are in an ideal position to prevent the adverse outcomes associated with immobility

95
Referenz
93
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Titsworth
J Neurosurg
Spine 2012
Prospective interventional cohort study mit historischer kontrolle
2A****
Pre-intervention: 8025 patient days
Intervention: 4455 patient days
Comprehensive mobility initiative utilizing the Progressive Upright Mobility Protocol (PUMP)
Incidence and safety of mobilization,outcome
Mobility increase by 300 %
Reduction in ICU-days (p< 0.004) 4.0 – 3.5
Reduction in Hospital days (p<0.004): 12.0 – 8.6
Reduction in VAP (p<0.001): 2.1 – 0 /1000 days
No increase in adverse events
Pro Arm
Zusammenfassende Beurteilung:
Hochwertige und sorgfältige studie bei neurochirurgischen Patienten

96
Referenz
94
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Truong
Crit Care
2009
Bench-to-bedside review/Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung:

97
Referenz
95
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Umei
Crit Care Med
2012
(abstract)
Retrospective cohort
4**
23 Patienten Mobility therapy
Mobility therapy within 6.6 d after ICU admission
PaO2/FIO2 increase after mobility
Pro Arm
Zusammenfassende Beurteilung: Mobility therapy is safe and improves oxygenation in in critically ill patients.
Pdf bestellt

98
Referenz
96
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Van Wijk
Cerebrovasc
Dis
2009
(abstract)
Randomized controlled study
4**(*)
71 patients with stroke (< 24 hrs)
Very early mobility < 24hrs
Standard care Intervention
Mobility 18,1 hrs after stroke, control 30.8 hrs (p< 0.001)
More sessions per day and more time out of bed
Pro Arm
? ?
Zusammenfassende Beurteilung: A trial protocol promoting earlier and more frequent mobilization was feasile even for those with severe stroke.

99
Referenz
97
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Vollman
Crit Care
Nurse
2010
Education/Expert opinion
4**
Pro Arm
Zusammenfassende Beurteilung: kurzer Überblick über die folgen der Immobilisierung und die Effekte der moblisierung

100
Referenz
98
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Vollman
Crit Care
Nurse Q
2013
Education – expert opinion
Practical approach
4**(*)
Pro Arm
Zusammenfassende Beurteilung:
Pdf bestellt

101
Referenz
99
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Warren
Crit Care Med
2011
(Abstract)
Prospective interventional cohort study
4**
Implementation of a multidsc. Early mobilization program (EMP)
Mobilization increased by 47 %
Pro Arm
Zusammenfassende Beurteilung: implementation of a EMP led to an increase in the number of mobilization activities
Onkologische ICU-Patienten

102
Referenz
100
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Yanase
Stroke
2013
abstract
Prospective observational cohort study
4**
Stroke mobility protocol
Fall rate/1000 patient days
Pre-implementation fall rate = 6.3
Post-implementation fall rate = 1.4
(p=0.38)
Pro Arm
Zusammenfassende Beurteilung: Early mobilization does not lead to prolonged neurologic deterioration or more falls.

103
Referenz
101
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Yanez-Brage
BMC Pulm
Med
2009
Prospective interventional cohort study
3**(*)
263 CABG patients
159 received pre-op physiotherapy
Postop early physiotherapy and mobilization
Post-operative actelectasis
Pre-op + post-op PT:
17 % actelectasis
Post-op PT:
36 % atelectasis
P=0.01
Pro Arm
Zusammenfassende Beurteilung: Receiving physiotherapy is the variable with an independent effect on predicting atelectasis
Bedeutung der additiven prä-operativen Physiotherapie

104
Referenz
102
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Yang
Kaohsiung J
Med Sci
2010
Prospective observational cohort study
3**(*)
126 Patienten, davon erhielten 55 Pat. Physio + Mobilisierung
30-min of physio-sessions/d incl. sitting, standing, walking
Rapid shallow breathing index (RSBI)
Barthel-Index
RSBI-Anstieg nicht isgnifikant
Barthel-Index Anstieg von 0.8 zu 1.9 (p<0.05)
Successful weaning 58,2 % vs. 40.9 %
Pro Arm
Zusammenfassende Beurteilung:

105
Referenz
103
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Zanni
J Crit Care
2010
Prospective observational cohort study
3***
32 patienten mit 4 d Beatmung Physician orders for rehabilitation
Physiotherapy only in 21 patients
50 rehab treatments to 19 patients
=
12 % of medical ICU days
Pro Arm
Zusammenfassende Beurteilung:
Diese Observationsstudie bildet wohl die derzeitige (traurige) Realität ab!

106
Referenz
104
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Zeppos
Austr J
Physiother
2007
Prospective observational cohort study
3***
12 281 Physiotherapie-sessions bei ICU-Patienten
Documentation of adverse events
27 adverse events (0,2 %):
Predom hemodynamic alterations
Risk factors:
Vasopressors
Unstable baseline
Previous cardiac comborbidities
Pro Arm
Zusammenfassende Beurteilung: The incidence of adverse events during physiotherapy is low….demonstrating that physiotherapy in ICU is safe
Sehr sorgfältige Untersuchung, exakte Definition von adverse events + gute statist. Auswertung

107
Referenz
105
Studientyp Teilnehmer (Anzahl und Charakteristika)
Drop out Rate
Intervention Kontrolle Zielgröße(n) Haupt-ergebnis
Bemerkung
insgesamt
Zomorodi
Crit Care Res
Pract
2012
Educational/expert opinion + observational pilot study
(3 Patienten)
4 **(*)
Pro Arm
Zusammenfassende Beurteilung:
Interessante und ausführliche Darstellung der Mobilisierung mit Algorithmus/protocol und Ausschlusskriterien


















