Evidence-Based & Evidence-Informed Practices in Suicide Prevention


Evidence-Based Practices in Gastrointestinal, Colorectal and
Hepatobiliary Surgery
Jayp
ee B
rothe
rs

Evidence-Based Practices in Gastrointestinal, Colorectal and
Hepatobiliary Surgery
EditorGovind Nandakumar MD FACS FASCRS
Chief of Gastrointestinal Surgery and Gastrointestinal Oncosurgery Columbia Asia Hospitals, Bengaluru, Karnataka, India
Courtesy FacultyWeill Cornell Medical College
New York, USA
The Health Sciences PublisherNew Delhi | London | Panama
Forewords
Jeffrey W Milsom MD
Fabrizio Michelassi MD
Nandakumar Jairam MBBS MS
Jayp
ee B
rothe
rs

Jaypee Brothers Medical Publishers (P) Ltd
HeadquartersJaypee Brothers Medical Publishers (P) Ltd.4838/24, Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhone: +91-11-43574357Fax: +91-11-43574314E-mail: [email protected]
Jaypee-Highlights Medical Publishers Inc.City of Knowledge, Bld. 235, 2nd Floor, ClaytonPanama City, PanamaPhone: +1 507-301-0496Fax: +1 507-301-0499E-mail: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd.17/1-B, Babar Road, Block-B, ShaymaliMohammadpur, Dhaka-1207BangladeshMobile: +08801912003485E-mail: [email protected]
Overseas OfficesJP Medical Ltd.83, Victoria Street, LondonSW1H 0HW (UK)Phone: +44-20 3170 8910Fax: +44(0)20 3008 6180E-mail: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd.Bhotahity, Kathmandu, NepalPhone: +977-9741283608E-mail: [email protected]
Website: www.jaypeebrothers.comWebsite: www.jaypeedigital.com
© 2017, Jaypee Brothers Medical Publishers
The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book.All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronic, mechanical, photo copying, recording or otherwise, without the prior permission in writing of the publishers. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book.Medical knowledge and practice change constantly. This book is designed to provide accurate, authoritative information about the subject matter in question. However, readers are advised to check the most current information available on procedures included and check information from the manufacturer of each product to be administered, to verify the recommended dose, formula, method and duration of administration, adverse effects and contra indications. It is the responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for any injury and/or damage to persons or property arising from or related to use of material in this book.This book is sold on the understanding that the publisher is not engaged in providing professional medical services. If such advice or services are required, the services of a competent medical professional should be sought.Every effort has been made where necessary to contact holders of copyright to obtain permission to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to make the necessary arrangements at the first opportunity.
Inquiries for bulk sales may be solicited at: [email protected]
Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
First Edition: 2017
ISBN: 978-93-5152-939-2
Printed at
Jayp
ee B
rothe
rs

DedicationThis book is dedicated to my family, teachers and mentors
To my mother and first teacher, Rameshwari Nandakumar who instilled in me the passion to do better every day.
To my father, Dr Nandakumar Jairam who has been a close friend and a mentor
throughout my life and career.
To my brother and best friend, Krishna Nandakumar who has helped me through several difficult situations.
To my soul mate and the love of my life, Dr Pallavi Patri who has stood by me and
been an immense support. She has helped me excel in my career and
has given meaning to everything I do.
To my children, Dhruv and Maya who have given up family time
for the sake of my career.
Thanks to the mentorship and guidance of
Dr Fabrizio Michelassi and Dr Jeffrey Milsom.
They were instrumental in training me and guiding me in my career.
A special mention to Dr TS Jairam, my grandfather and the person
who has inspired me.
Jayp
ee B
rothe
rs

Christopher T Aquina MD
General Surgery Resident Research FellowDepartment of SurgeryUniversity of Rochester Medical CenterRochester, New York, USA
Antonios Arvelakis MD MPH
Assistant Professor of SurgeryIcahn School of Medicine at Mount SinaiRecanati/Miller Transplantation InstituteMount Sinai HospitalNew York, USA
Erman Aytac MD FTBS
Staff SurgeonDepartment of Colorectal Surgery Digestive Disease InstituteCleveland Clinic, Ohio, USA
Philip S Barie MD MBA Master FCCM
FDSA FACS
Professor of SurgeryProfessor of Public Health in MedicineWeill Cornell MedicineAttending SurgeonNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Savio George Barreto MS PhD MBBS
Consultant Cancer Surgeon Department of Gastrointestinal SurgeryGastrointestinal Oncology and Bariatric SurgeryMedanta—The Medicity Gurgaon, Haryana, India
Joseph Batac MD
Plastic Surgery FellowNassau University Medical CenterNew York, USA
John-Paul Bellistri MD
Department of SurgeryMontefiore Medical CenterBronx, New York, USA
Debra Beneck MD
Professor of Clinical PathologyWeill Cornell Medical CollegeNew York, USA
Jason R Bingham MD
Department of SurgeryMadigan Army Medical CenterFort Lewis, Washington, USA
Christine Boumitri MD
Gastroenterology Research AssistantDivision of Gastroenterology Weill Cornell MedicineNew York, USA
Douglas Brylka MD
Assistant Professor of Radiology Body Imaging DivisionCo-Director, Imaging Data Evaluation and Analytics LaboratoryDepartment of RadiologyWeill Cornell Medical CollegeNew York Presbyterian HospitalNew York, USA
Thomas Cataldo MD FACS FASCRS
Instructor in SurgeryHarvard Medical SchoolBeth Israel Deaconess Medical CenterBoston, Massachusetts, USA
Christina Cellini MD FACS FASCRS
Assistant Professor of Surgery and OncologyDivision of Colorectal SurgeryUniversity of Rochester Medical CenterRochester, New York, USA
Gregory Charak MD
Resident, General SurgeryNew York Presbyterian HospitalColumbia University College of Physicians and SurgeonsNew York, USA
Natarajan A MS DNB FRCS
Consultant SurgeonMinimal Invasive and Bariatric SurgeryColumbia Asia Hospital Bengaluru, Karnataka, India
Amit K Agarwal MD
Department of SurgeryThe University of Texas Medical School Houston, Texas, USA
Hasan Aldailami MD
Cardiothoracic Surgery FellowBaylor Medical Center Dallas, Texas, USA
Chung Yaw-Fui Alexander MBBS FRCS
Professor of SurgeryDepartment of Hepatopancreatobiliary and Transplant SurgerySingapore General HospitalDuke-National University of Singapore Medical SchoolSingapore
Azah A Althumairi MD
Fellow, Colorectal SurgeryJohns Hopkins University School of MedicineBaltimore, Maryland, USA
Melissa M Alvarez-Downing MD
Assistant Professor of SurgeryIcahn School of Medicine at Mount SinaiDivision of Colorectal SurgeryMount Sinai St Luke’s andRoosevelt HospitalsNew York, USA
Chukwuma Apakama MD
Surgeon, Critical Care SurgeryDepartment of Acute and Emergency SurgeryBarnes-Jewish Hospital Washington UniversitySt Louis, Missouri, USA
Contributors
Jayp
ee B
rothe
rs

viii Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
Lilian Chen MD
Assistant ProfessorDivision of Colon and Rectal SurgeryDepartment of General SurgeryTufts University School of MedicineBoston, Massachusetts, USA
Neel P Chudgar MD
Resident Physician in General SurgeryNew York Presbyterian Hospital Weill Cornell Medical CollegeNew York, USA
John Creasy MD
ResidentDepartment of SurgeryWeill Cornell MedicineNew York, USA
Gregory Dakin MD FACS
Associate Professor of SurgeryDepartment of SurgeryWeill Cornell Medical CollegeNew York, USA
Desmond M D’Souza MD
Assistant Professor of SurgeryOhio State University Columbus, Ohio, USA
Soumitra R Eachempati MD FACS FCCM
Professor of SurgeryProfessor of MedicineDivision of Medical EthicsNew York Presbyterian HospitalWeill Cornell Medical CollegeWeill Cornell Medical CenterNew York, USA
Michelle E Ernst MS LCGC
Genetic CounselorSmilow Cancer Genetics and PreventionYale-New Haven HospitalNew Haven, Connecticut, USA
Thomas J Fahey III MD
Johnson and Johnson ProfessorVice Chair, Department of SurgeryChief, Endocrine SurgeryDirector, Endocrine Oncology ProgramNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Evan N Feldman MD FACS FASCRS
Attending SurgeonPiedmont Atlanta Hospital Atlanta, Georgia
Leandro Feo MD FACS
Colorectal SurgeonDepartment of Surgery Colorectal DivisionCatholic Medical CenterManchester, New Hampshire, USA
Alessandro Fichera MD FACS FASCRS
Research FellowProfessor and Section Chief Gastrointestinal SurgeryDivision of General SurgeryDepartment of SurgeryUniversity of Washington Medical CenterSeattle, Washington, USA
Brendan M Finnerty MD
Surgical ResidentDepartment of SurgeryNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
James Fleshman MD
Helen Buchanan and Stanley Joseph Seeger Professor and ChairmanDepartment of SurgeryBaylor University Medical CenterProfessor of Surgery Texas A&M Health SciencesDallas, Texas, USA
Sander Florman MD FACS
DirectorRecanati/Miller Transplantation InstituteMount Sinai Health SystemThe Charles Miller, MD Professor of SurgeryIcahn School of Medicine at Mount Sinai, New York, USA
Todd D Francone MD MPH FACS
Director of Robotic SurgeryColon and Rectal SurgeryAssociate Program Director Residency in Colon and Rectal SurgeryAssistant Professor of SurgeryDepartment of Colon and Rectal SurgeryLahey Hospital and Medical CenterTufts University School of MedicineBoston, Massachusetts, USA
Pankaj Kumar Garg MS DNB MCh
(Surg Oncol) MNAMS
Assistant ProfessorDepartment of SurgeryUniversity College of Medical Sciences and Guru Teg Bahadur HospitalUniversity of DelhiNew Delhi, India
Kelly A Garrett MD FACS FASCRS
Assistant ProfessorDepartment of SurgeryDivision of Colon and Rectal SurgeryNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Mahesh Goel MBBS MS
Associate ProfessorGI and Hepatopancreatobiliary Surgical OncologyGI Disease Management GroupTata Memorial HospitalMumbai, Maharashtra, India
Benjamin Golas MD
Assistant ProfessorDepartment of SurgeryWeill Cornell MedicineNew York, USA
Emre Gorgun MD FACS FASCRS
Staff SurgeonDepartment of Colorectal Surgery Digestive Disease Institute Cleveland Clinic, Ohio, USA
Lester Gottesman MD FASCRS
Associate Professor of SurgeryIcahn School of Medicine at Mount SinaiNew York, USA
Sanjay Govil MS FRCS
Senior Consultant HPB Surgery and Liver Transplantation Global HospitalChennai, Tamil Nadu, India
Anand Govindarajan MD MSc FRCSC
Assistant ProfessorDepartment of SurgeryMount Sinai HospitalUniversity of TorontoToronto, Ontario, Canada
Jayp
ee B
rothe
rs

Contents ix
Katherine D Gray MD
Research Resident in General Surgery (PGY4)New York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Alexis L Grucela MD FACS FASCRS
Assistant Professor of SurgeryDivision of Colon and Rectal SurgeryNYU Langone Medical CenterNew York, USA
Ramraj Vemala Nagendra Gupta MBBS DNB (Gen. Surgery) FMIS (RGUHS)
FBMS (RGUHS) FIAGES FACRSI
SurgeonDepartment of Minimal InvasiveGI and Bariatric SurgeryColumbia Asia HospitalBengaluru, Karnataka, India
Usmaan Hameed MD
FellowDepartment of Surgical Oncology University of TorontoToronto, Ontario, Canada
Kelly Hicks MSN AGNP-BC CWOCN
Adult-Gerontology Nurse PractitionerWound, Ostomy and Continence NurseColon and Rectal SurgeryNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
David P Horowitz MD
Assistant ProfessorNew York Presbyterian HospitalColumbia University Medical CenterNew York, USA
Vanessa Hui MD
General Surgery ResidentDepartment of General Surgery Montefiore Medical CenterAlbert Einstein School of MedicineBronx, New York, USA
Steven R Hunt MD
Associate ProfessorDepartment of SurgeryWashington University in St. LouisSaint Louis, Missouri, USA
Danielle Hunton MA RN CCRN CWOCN
Wound, Ostomy and Continence NurseDepartment of NursingNew York Presbyterian HospitalWeill Cornell Medical College New York, USA
Kareem Ibrahim MD
Vascular Surgery FellowWeill Cornell Medical Center New York, USA
Jumana Jaloudi DO
Resident Physician The Wright Center for Graduate Medical Education Pennsylvania, USA
Stefan S Kachala MD
ResidentDepartment of SurgeryNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Michel Kahaleh MD AGAF FACG FASGE
Professor of MedicineChief of Endoscopy Medical Director, Pancreas ProgramDivision of Gastroenterology and HepatologyDepartment of MedicineWeill Cornell MedicineNew York, USA
Tomoaki Kato MD
Chief, Division of Abdominal Organ Transplantation New York Presbyterian HospitalSurgical Director, Liver and Gastrointestinal TransplantationNew York, USA
Prashant Kedia MD
Medical Director of Innovative Interventional EndoscopyMethodist Dallas Medical Center Dallas, Texas, USA
Kristin N Kelly MD, MPH
Resident TraineesDepartment of SurgeryUniversity of Rochester Medical CenterRochester, New York, USA
Maria Ximena Traa Kiely MD MPH
Resident in General SurgeryDepartment of SurgeryTufts Medical CenterBoston, Massachusetts, USA
Michael D Kluger MD MPH
Assistant Professor of SurgeryCollege of Physicians and SurgeonsNew York Presbyterian HospitalColumbia University Medical CenterNew York, USA
Mukta K Krane MD FACS
Associate ProfessorDivision of General SurgeryDepartment of SurgeryUniversity of Washington Medical CenterSeattle, Washington, USA
Ziad N Kronfol MD
Colorectal Surgery FellowDivision of Colorectal SurgeryMount Sinai St Luke’s and Roosevelt HospitalsNew York, USA
Nikhil Kumta MD MS
Assistant Professor of Medicine Icahn School of Medicine at Mount Sinai, New York, USA
Steven Lee-Kong MD
Assistant Professor of SurgeryDepartment of SurgeryColumbia University College of Physician and SurgeonsNew York, USA
Rebecca A Levine MD FACS
Assistant Professor of SurgeryColon and Rectal SurgeryAlbert Einstein College of MedicineMontefiore Medical CenterBronx, New York, USA
Adam Levy MD
ResidentDepartment of SurgeryWeill Cornell Medical CollegeNew York, USA
Jayp
ee B
rothe
rs

x Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
Baoqing Li MD
Assistant ProfessorClinical Radiation OncologyWeill Cornell Medical CollegeNew York, USA
Alissa J Ritter Lupu RD CDN CNSC
Clinical GI DietitianCenter for Advanced Digestive CareNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Josep Marti-Sanchez MD PhD
Surgical AttendingCentre Médico-Chirurgical de Tronquiéres, Aurillac, France
Abhishek MathurAssistant in Clinical SurgeryDivision of Abdominal Organ TransplantationNew York Presbyterian HospitalColumbia University Medical CenterNew York, USA
Abhishek Mitra MBBS MS
FellowGI and Hepatopancreatobiliary Surgical OncologyDepartment of Surgical OncologyTata Memorial HospitalMumbai, Maharashtra, India
Rohin Mittal MS DNB MRCS
Associate ProfessorColorectal SurgeryDepartment of Surgery (Unit 2) Christian Medical CollegeVellore, Tamil Nadu, India
Oliver J Muensterer MD PhD
Professor of Pediatric SurgeryDepartment of Pediatric SurgeryUniversity Medicine of the Johannes Gutenberg University MainzMainz, Germany
Govind Nandakumar MD FACS FASCRS
Chief of Gastrointestinal Surgery and Gastrointestinal Oncosurgery Columbia Asia Hospitals Bengaluru, Karnataka, IndiaCourtesy Faculty Weill Cornell Medical CollegeNew York, USA
Rahul Narang MD
Assistant Professor of SurgeryMontefiore Medical CenterAlbert Einstein College of MedicineBronx, New York, USA
Garrett M Nash MD MPH FACS
Assistant Attending SurgeonColorectal Surgery ServiceMemorial Sloan Kettering Cancer CenterNew York, USA
John Ng MD
Assistant ProfessorDepartment of Radiation OncologyWeill Cornell Medical CollegeNew York, USA
Nabeel R Obeid MD
Chief ResidentGeneral SurgeryAcademic and QI Chief ResidentDepartment of SurgeryNew York University School of MedicineNew York, USA
Paul RA O’Mahoney MD
Research FellowColon and Rectal SurgeyNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Melanie Ongchin MD
Assistant Professor of SurgeryGeneral Surgery/Surgical OncologyWeill Cornell MedicineNew York, USA
Nicole C Panarelli MD
Assistant Professor of Pathology and Laboratory MedicineWeill Cornell Medical CollegeNew York, USA
Durgatosh Pandey MS DNB MCh
(Surg Oncol)
Department of Surgical OncologyDr BRA Institute Rotary Cancer HospitalAll India Institute of Medical Sciences New Delhi, India
Rambha Pandey MD
Assistant ProfessorDepartment of Radiation OncologyDr BR Ambedkar Institute Rotary Cancer HospitalAll India Institute of Medical Sciences New Delhi, India
Samir Pandya MD
Assistant Professor of Surgery and PediatricsDepartment of SurgeryDivision of Pediatric SurgeryNew York Medical CollegeValhalla, New York, USA
Manish Parikh MD
Associate ProfessorDepartment of SurgeryChief, Perioperative ServicesBellevue Hospital CenterNew York University School of MedicineNew York, USA
Subroto Paul MD
Associate Professor of Cardiothoracic SurgeryAssociate Professor of Health Policy and Research in Cardiothoracic SurgeryDepartment of Cardiothoracic SurgeryNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Benjamin Perakath MS FRCS(G)
Professor and HeadColorectal SurgeryDepartment of Surgery (Unit 2) Division of SurgeryChristian Medical CollegeVellore, Tamil Nadu, India
Carrie Y Peterson MD
Assistant ProfessorDepartment of SurgeryDivision of Colorectal SurgeryMedical College of WisconsinMilwaukee, Wisconsin, USA
Michael Polcino MD FACS
Director of Colon and Rectal SurgerySaint Barnabas HospitalBronx, New York, USA
Jayp
ee B
rothe
rs

Contents xi
Alfons Pomp MD FACS FRCSC
Leon C Hirsch ProfessorVice Chairman, Department of SurgeryChief, GI, Metabolic and Bariatric SurgeryWeill Cornell MedicineNew York Presbyterian HospitalNew York, USA
Vitaliy Y Poylin MD FACS FASCRS
Assistant Professor in SurgeryHarvard Medical SchoolBeth Israel Deaconess Medical CenterBoston, Massachusetts, USA
Christian P Probst MD MPH
Resident TraineesDepartment of SurgeryUniversity of Rochester Medical CenterRochester, New York, USA
Pejman Radkani MD MPH
Visiting SurgeonTransplant SurgeryKorea and France
Siva Raja MD PhD
Staff SurgeonThoracic and Cardiovascular SurgeryCleveland ClinicCleveland, Ohio, USA
Maria Camilla Ramirez MD
Surgical ResidentMount Sinai St Luke’s and Roosevelt Hospital, New York, USA
Ashwin Rammohan MS MCh
Consultant HPB and Liver Transplant SurgeonInstitute of Liver Surgery and TransplantationGlobal Hospital Chennai, Tamil Nadu, India
Ankesh Rawat MBBS
Junior RegistrarMedanta—The MedicityGurgaon, Haryana, India
Christine J Ren-Fielding MD
Professor, Department of SurgeryChief, Division of Bariatric SurgeryNYU Langone Medical CenterNew York University School of MedicineNew York, USA
R Taylor Ripley MD
Thoracic SurgeonThoracic and GI Oncology BranchCenter for Cancer ResearchNational Cancer InstituteBethesda, Maryland, USA
Kayvan Roayaie MD PhD
Division of Abdominal Organ Transplantation Oregon Health Sciences University Portland, Oregon, USA
Sasan Roayaie MD
Chief, Hepatobiliary SurgeryLiver Cancer ProgramNorth Shore-LIJ Health SystemLenox Hill HospitalNew York, USA
Jessica A Rotman MD
Resident PhysicianDepartment of RadiologyNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Rashmi S MBBS Diplomat in Pathology (India)
MD Pathology (US)
Fellow Surgical and GI Pathology Department of PathologyMD Anderson Cancer Center University of TexasHouston, Texas, USA
Bashar Safar MD
Assistant ProfessorColorectal Surgery Johns Hopkins University School of MedicineBaltimore, Maryland, USA
Gayle Rudofsky Salama MD
Radiologist in TrainingDepartment of RadiologyNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Tushar Samdani MD MS DNB
(General surgery), MRCS (Edin)
Laparoscopic Colorectal and General SurgeonMedStar Saint Mary’s HospitalLeonardtown, Maryland, USA
Nora Sammon BSN RN CWOCN
Wound, Ostomy and Continence NurseDepartment of NursingNew York Presbyterian HospitalWeill Cornell Medical CenterNew York, USA
Allen Sanchez MD
Radiologist in TrainingDepartment of RadiologyNew York Presbyterian HospitalWeill Cornell Medical CollegeNew York, USA
Inderpal S Sarkaria MD FACS
Vice Chairman, Clinical AffairsDirector, Thoracic Robotic SurgeryCo-Director, Esophageal and Lung Surgery InstituteDepartment of Cardiothoracic SurgeryUniversity of Pittsburgh Medical Center Pittsburgh, Pennsylvania, USA
Felice Schnoll-Sussman MD
Associate Professor of Clinical MedicineDepartment of MedicineWeill Cornell Medical CollegeDivision of Gastroenterology and HepatologyNew York, USA
Beth Schrope MD PhD FACS
Associate Professor of SurgeryColumbia University College of Physicians and SurgeonsNew York, USA
Daniele Scoglio MD
Research FellowDepartment of SurgeryUniversity of Washington Medical Center Seattle, Washington, USA
Elliot Servais MD
Thoracic SurgeonDepartment of Thoracic SurgeryLahey Hospital and Medical CenterTufts University School of MedicineBurlington, Massachusetts, USA
Jayp
ee B
rothe
rs

xii Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
Joongho Shin MD
Assistant Professor of Clinical SurgeryDivision of Colorectal SurgeryUniversity of Southern CaliforniaLos Angeles, California, USA
HV Shivaram MS FAIS FICS FRCS
Consultant Surgeon and Head of GI, Minimal Invasive and Bariatric SurgeryColumbia Asia HospitalsBengaluru, Karnataka, India
Shailesh V Shrikhande MBBS MS
Professor and ChiefGI and Hepatopancreatobiliary Surgical Oncology Convener GI Disease Management GroupTata Memorial HospitalMumbai, Maharashtra, India
Parul J Shukla MD MS(Gen Surg)
FRCS(Glasg) FACRSI(Hon)
Associate ProfessorDepartment of SurgeryNew York Presbyterian HospitalWeill Cornell Medical College New York, USA
Alpana P Shukla MD MRCP(UK)
Assistant Professor of Research in MedicineClinical Research ManagerComprehensive Weight Control CenterDivision of EndocrinologyDiabetes and MetabolismWeill Cornell Medical CollegeNew York, USA
Bhawna Sirohi MBBS FRCP
Consultant Medical Oncologist—GI and Breast Cancers Head of Medical Oncology Mazumdar Shaw Cancer CentreNarayana Health Bengaluru, Karnataka, India
Amir Soumekh MD
Assistant Professor of Clinical MedicineDepartment of MedicineDivision of Gastroenterology and HepatologyWeill Cornell Medical CollegeNew York, USA
Scott R Steele MD
ChairmanDepartment of Colon and Rectal SurgeryCleveland Clinic, ClevelandProfessor of SurgeryCase Western Reserve UniversitySchool of MedicineCleveland, Ohio, USA
Randolph M Steinhagen MD
Chief, Division of Colon and Rectal SurgeryIcahn School of Medicine at Mount SinaiNew York, USA
Emily Steinhagen MD
ResidentDepartment of Colon and Rectal SurgeryUniversity of Chicago School of MedicineChicago, Illinois, USA
Samuel Sultan MD
Fellow Abdominal Transplant SurgeryUniversity of Maryland Medical CenterBaltimore, Maryland, USA
Parissa Tabrizian MD
Assistant Professor of SurgeryIcahn School of Medicine at Mount SinaiRecanati/Miller Transplantation InstituteMount Sinai HospitalNew York, USA
Adam D Talenfeld MD
Assistant ProfessorDepartment of RadiologyWeill Cornell Medical CollegeNew York, USA
Aida Taye MD
Assistant Professor of SurgeryEndocrine and General SurgeryIcahn School of Medicine at Mount SinaiNew York, USA
Francesca Tubito MS CGC
Genetic CounselorThe Jay Monahan Center for Gastrointestinal HealthThe Center for Advanced Digestive CareNew York Presbyterian HospitalWeill Cornell MedicineNew York, USA
Diana Moglia Tully MS CGC
Genomics ConsultantGeneDx, Inc.Gaithersburg, Maryland, USA
Joshua A Tyler MD
Chief, Colon and Rectal SurgeryKeesler Medical CenterKeesler Air Force BaseOcean Springs, Mississippi, USA
Nestor Villamizar MD
Associate Professor of Clinical SurgeryAssociate Program Director Cardiothoracic FellowshipMiller School of MedicineUniversity of MiamiMiami, Florida, USA
Vikram Wadhera MD
Assistant Professor of SurgeryIcahn School of Medicine at Mount SinaiRecanati/Miller Transplantation InstituteMount Sinai HospitalNew York, USA
Tony JC Wang MD
Associate ProfessorNew York Presbyterian HospitalColumbia University Medical CenterNew York, USA
Anthony Watkins MD FACS
Assistant Professor of SurgeryAssistant Program DirectorDirector, Skills Acquisition and Innovation Lab, New York Presbyterian Hospital, Weill Cornell Transplant CenterNew York, USA
Jon Wee MD
Co-Director of Minimally Invasive Thoracic SurgeryDirector of Robotic in Thoracic SurgeryAssociate Program DirectorDivision of Thoracic SurgeryBrigham and Women’s HospitalHarvard Medical SchoolBoston, Massachusetts, USA
Jared Wong MD
Fellow, Colorectal SurgeryBaylor University Medical CenterDallas, Texas, USA
Jayp
ee B
rothe
rs

Contents xiii
Teo Jin Yao MBBS (Sing), MRCS
(Edinburgh), FRCS (Edinburgh)
Associate ConsultantDepartment of Hepatopancreatobiliary and Transplant SurgerySingapore General HospitalSingapore
Lee Ser Yee MBBS M Med(Surgery) MSc
FAMS FRCS(Ed)
Senior Consultant SurgeonDepartment of Hepatopancreatobiliary and Transplant SurgerySingapore General HospitalAssociate Professor (Adj)Duke-National University of Singapore Medical SchoolSingapore
Heather Yeo MD MHS
Assistant Professor of SurgeryAssistant Professor of Healthcare Policy and ResearchDepartment of SurgeryWeill Cornell MedicineNew York, USA
Chan Chung Yip MBBS MMed FRCS MD
Senior Consultant SurgeonDepartment of Hepatopancreatobiliary and Transplant SurgerySingapore General HospitalDuke-National University of Singapore Medical SchoolSingapore
James Yoo MD
Chief, Colon and Rectal SurgeryDepartment of SurgeryTufts Medical CenterBoston, Massachusetts, USA
Rasa Zarnegar MD
Associate Professor of SurgeryWeill Cornell Medical CollegeAssociate Attending Surgeon Department of SurgeryNew York Presbyterian Hospital Weill Cornell Medical CenterNew York, USA
Jayp
ee B
rothe
rs

Foreword
The field of gastrointestinal surgery is changing dramatically. Laparoscopy and minimally invasive surgery began this “revolution” in the 1990’s. What next? Working within the lumen of the bowel (endoluminal surgery) combined with better, cheaper endoscopes and tools will lead the way. Biomaterials and advanced imaging methods are the other essential elements for revolutionizing digestive disease care. Dr Govind Nandakumar has been my student since 2000 and over the years, he has learned, developed and improved many of the thoughts and concepts I have believed in. This book brings together all the relevant specialties in gastrointestinal surgery. Chapters on innovative approaches will hopefully stimulate new approaches to the care of patients with digestive disorders. Dr Nandakumar used his experience at the Center for Advanced Digestive Care (CADC) at the New York Presbyterian Hospital, New York, USA and is in the process of developing a similar center called the Integrated Digestive Liver and Cancer Centre (IDLCC) at Columbia Asia Hospitals, Bengaluru, Karnataka, India. This book talks about many of the concepts that address integrated care and will be a valuable tool for any gastrointestinal surgeon.
Jeffrey W Milsom MD
Chief, Section of Colon and Rectal SurgeryJerome J DeCosse Distinguished Professor
Executive Director, Center for Advanced Digestive CareWeill Cornell Medicine, New York Presbyterian Hospital
New York, USA
Jayp
ee B
rothe
rs

Foreword
The field of gastrointestinal surgery has seen impressive innovations in recent years. Dr Govind Nandakumar, an experienced gastrointestinal surgeon, has edited a very comprehensive book on the topic with contributions from an outstanding group of authors. The book will be valuable to the aspiring gastrointestinal surgeon or a junior consultant as it provides an easy read on several complex gastrointestinal topics. The chapters are comprehensive and yet concise to read efficiently prior to a difficult case. The evidence-based approach and the section on “Landmark Trials” gives the necessary background information and yet encourage the reader to constantly review and update the ever changing literature. The inclusion of nonsurgical topics and techniques helps in guiding and formulating a multidisciplinary care of the patient. The step-by-step procedural review is a nice tool to prepare for an operation quickly. This book is a valuable adjunct to well-established textbooks as it provides a practical, concise and evidence-based approach to the surgical care of the complex gastrointestinal and hepatobiliary patient.
Fabrizio Michelassi MD
Lewis Atterbury Stimson Professor and ChairmanSurgeon-in-Chief
Department of SurgeryWeill Cornell Medicine
New York, USA
Jayp
ee B
rothe
rs

Foreword
I have witnessed the evolution of surgery over the last four decades. Health care is changing rapidly and faster than ever before. Better and more efficient patient care and clinical outcomes are an automatic sequel. Analysis of why this occurred indicates changing trends in communication and advancing technology, which amongst other things, makes it easier for global merger of clinical practice. Also available are newer and efficient surgical tools which drive procedures and practices much more than in the past. Subspecialties such as surgical gastroenterology are creating an identity for themselves. Focused care of disorders of the gastrointestinal tract is more possible today than ever before. All this has created an abundance of knowledge and information that needs to be dissipated. Dispersal of knowledge, now needs to be very different—accurate, focused, concise and yet comprehensive. Dr Govind Nandakumar has chosen a topic and authors list to dissipate knowledge in the field of surgical gastroenterology in an evidence-based, comprehensive and yet concise manner. Global authorship, well-defined chapters that address topics of relevance and importance are delivered with clarity.
Nandakumar Jairam MBBS MS
Chairman and Group Medical DirectorColumbia Asia Hospitals
Bengaluru, Karnataka, India
Jayp
ee B
rothe
rs

Preface
The field of Gastrointestinal Surgery has grown tremendously and is rarely practiced as one field with superspeciality services like Hepatobiliary, Colorectal and Bariatric Surgery blossoming. The goal of this book was to provide a high quality, state-of-the-art, evidence-based book that is efficient to read and could be a quick reference for a busy trainee or a junior surgeon. There are several good textbooks that address the pathophysiology and basic science of surgical gastroenterology, so our book is focused on a practical approach to these diseases. The value of multidisciplinary care of Complex Gastrointestinal (GI) diseases is understated. This book includes chapters on several allied specialties that are required to take care of the complex GI patient. The book addresses the basics and fundamentals of each disease process while reviewing new and innovative approaches. We have listed key randomized trials for each section to facilitate rapid access to relevant content. Progress in the field of gastrointestinal and liver diseases has created a wealth of knowledge. Imparting and absorbing the knowledge efficiently has become increasingly difficult. We have made an effort to present important and relevant content in a manner that is easy to read. Dr Subroto Paul has done fantastic job with gathering an elite panel of surgeons to cover the section on esophageal diseases. This section would not have been possible without his help.
Govind Nandakumar MD FACS FASCRS
Chief of Gastrointestinal Surgery and Gastrointestinal OncosurgeryColumbia Asia Hospitals, Bengaluru, Karnataka, India
Courtesy Faculty, Weill Cornell Medical CollegeNew York, USA
Jayp
ee B
rothe
rs

Acknowledgments
I would like to thank all the authors who have spent significant time and effort contributing to this book. A special thanks to Dr Subroto Paul who was instrumental in compiling and editing the Esophageal section. I would also like to thank Mr Jitendar P Vij (Group Chairman), Mr Ankit Vij (Group President), Ms Chetna Malhotra Vohra (Associate Director—Content Strategy), Ms Nedup Denka Bhutia (Development Editor) and the entire Jaypee team for their relentless efforts in designing and completing this book.
Jayp
ee B
rothe
rs

Contents
Section 1: General Chapters
1. Topics in Intraoperative Gastrointestinal Pathology for Practicing Surgeons 3Nicole C Panarelli, Debra Beneck • Review 3
2. Hepatic, Biliary, and Pancreatic Imaging 14Allen Sanchez, Gayle Rudofsky Salama, Douglas Brylka
• Imaging of the Liver 14• Lesions of the Liver 19• Metastases 30• Imaging of the Biliary System 32• Imaging of the Pancreas 43
3. Interventional Radiology Techniques 69Jessica A Rotman, Adam D Talenfeld
Part I: Percutaneous Treatment of Benign Liver Disease 69• Portal Hypertension 69• Biliary Obstruction 73
Part II: Percutaneous Treatment of Primary and Metastatic Hepatic Malignancy 77• Percutaneous Tumor Ablation 77• Transarterial Interventions 81
4. Radiotherapy for Gastrointestinal and Liver Pathology 102John Ng, Baoqing Li, Tony JC Wang, David P Horowitz
• Evidence-Based Review 103• Landmark Trials 107• Conclusion and Future Directions 107
5. Novel Techniques in Advanced Endoscopy 110Christine Boumitri, Nikhil Kumta, Prashant Kedia, Michel Kahaleh • Interventional Endoscopic Ultrasound 110
6. Pediatric Gastrointestinal and Hepatobiliary Surgery 136Oliver J Muensterer, Samir Pandya
• General Aspects of Surgery in Children 136• Pediatric Foregut Surgery 136• Midgut and Hindgut Pediatric Surgery 143• Hepatobiliary Surgery in Children 152• Conclusion and Future Directions 159
Jayp
ee B
rothe
rs

xxvi Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
7. Early Recovery after Gastrointestinal Surgery 162Benjamin Perakath, Rohin Mittal
• Aim and Rationale of the ERAS Pathway 162• Components of ERAS 162• Preoperative Interventions 162• Perioperative Interventions 164• Postoperative Interventions 165• Audit 166• Outcomes of the ERAS Pathway 166
8. Nutrition for the Gastrointestinal and Hepatobiliary Surgery Patient 169Alissa J Ritter Lupu
• Preoperative Nutrition Optimization 169• Enteral and Parenteral Nutrition Support 173• Selection of EN Formula 174• Oral Diet Advancement 175• Postoperative Medical Nutrition Therapy Guidelines 175• Medical Nutrition Therapy for Specific Surgeries 178
9. Stoma Care 182Kelly Hicks, Nora Sammon, Danielle Hunton
• Preoperative Considerations 182• Stomal Complications 182• Peristomal Skin Complications 184• Other Skin Complications 189• Psychological Impact 189
10. Genetic Counseling and Genetic Testing for Colorectal Cancer Risk— A Case-based Review 192Francesca Tubito, Diana Moglia Tully, Michelle E Ernst
• Genetic Counseling 192• Introduction to Hereditary Colorectal Cancer Syndromes 197• Hereditary Colorectal Cancer Syndromes without Significant Polyposis 199• Adenomatous Polyposis Syndromes 210• Hamartomatous Polyposis Syndromes 225• Other Polyposis Syndromes 231• Other Hereditary Syndromes with GI Findings 232• Types of Genetic Tests and Technologies 232
Section 2: Esophagus Section Editor—Subroto Paul
11. Benign Disorders of the Esophagus 245Subroto Paul
• Overview 245
Jayp
ee B
rothe
rs

Contents xxvii
12. Gastroesophageal Reflux Disease 246Stefan S Kachala, Brendan M Finnerty, Rasa Zarnegar • Review of Landmark Studies 246• Minimally Invasive Gastric Fundoplication 247• Operative Tips 251
13. Surgical Options for Achalasia 253Jon Wee, Nestor Villamizar • Laparoscopic Heller Myotomy 253• Peroral Endoscopic Myotomy (POEM) 260• Conclusion and Future Directions 263
14. Surgical Treatment of Esophageal Diverticula 265Desmond M D’Souza, Siva Raja • Zenker’s Diverticulum 265• Diverticulectomy and Myotomy 265• Thoracic Diverticula 267• Conclusion and Future Directions 269
15. Endoscopic Treatment for Achalsia: Peroral Endoscopic Myotomy 271Nikhil Kumta, Christine Boumitri, Michel Kahaleh • Evidence-Based Review 271• Procedure 271• Outcomes 274• Conclusion and Future Directions 275
16. Barrett’s Esophagus 277Amir Soumekh, Felice Schnoll-Sussman • Preoperative Planning 280• Surgical Anatomy 280• Step-by-Step Illustration of Procedure 280• Operative Tips 280• Complications 280• Outcomes 280• Conclusion and Future Directions 281
17. Malignant Disorders of the Esophagus 283Subroto Paul
• Overview 283
18. Short- and Long-Term Outcomes in Esophageal Cancer 284Subroto Paul • Postoperative and Short-Term Outcomes 284• Long-Term Survival 286
19. Esophagectomy 291Elliot Servais
• Overview 291
Jayp
ee B
rothe
rs

xxviii Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
• Preoperative Evaluation 292• Open Esophagectomy 292• Minimally Invasive Esophagectomy 294• Future Directions 296
20. Robotically Assisted Minimally Invasive Ivor Lewis Esophagectomy 299R Taylor Ripley, Inderpal S Sarkaria
• Evidence-Based Review 299• Preoperative Planning 299• Anesthetic Considerations 300• Procedure and Surgical Anatomy 300• Postoperative Care 303• Illustrations 303• Complications 303• Outcomes (Literature Review) 303• Conclusion and Future Directions 308
Section 3: Stomach
21. Gastric Bypass and Biliopancreatic Diversion 313Adam Levy, Katherine D Gray, Gregory Dakin
• Evidence-Based Review: Indications 313• Evidence-Based Review: Physiology 314• Landmark Trials 315• Procedures 315• Operative Tips 319• Complications 319• Outcomes in Bariatric Surgery 321
22. Laparoscopic Adjustable Gastric Banding and Sleeve Gastrectomy 325Nabeel R Obeid, Christine J Ren-Fielding, Manish Parikh
• Evidence-Based Review 325• Landmark Trials 326• Preoperative Planning 327• Surgical Anatomy 327• Procedure: Laparoscopic AGB 328• Procedure: Laparoscopic SG 334• Conclusion and Future Directions 340
23. Role of Surgery in Developing Economies 342HV Shivaram, Natarajan A • Synergism of Growing Economies and Illnesses 342• Evidence-Based Review 343
Jayp
ee B
rothe
rs

Contents xxix
• Landmark Trials 360• Procedures 361• Surgical Anatomy and Operative Technique 363• Conclusion and Future Directions 371
24. Metabolic Surgery 378Alpana P Shukla, Alfons Pomp • Mechanisms of Glycemic Control after Metabolic Surgery 378• Outcomes of Metabolic Surgery 379• Patient Selection and Surgical Options for the Obese Patient with T2DM 380
25. Gastric Cancer 384Savio George Barreto, Ankesh Rawat, Parul J Shukla • Etiology 384• Classification of Gastric Cancer 384• Signs and Symptoms of Gastric Cancer 384• Diagnosis and Staging of Gastric Carcinoma 386• Treatment of Gastric Cancer 387
Section 4: Liver
26. Anatomic Resections of the Liver 399Neel P Chudgar, Govind Nandakumar • Anatomy 399• Preoperative Planning 404• Procedures 405• Postoperative Care 412• Operative Tips 413• Outcomes 414• Conclusion and Future Directions 414
27. Benign Tumors of the Liver 416Ashwin Rammohan, Sanjay Govil
• Introduction and Classification 416• Incidental Liver Tumors 416• Cavernous Hemangioma 418• Focal Nodular Hyperplasia 420• Hepatocellular Adenoma 421• Benign Cystic Tumors 423• Hepatobiliary Cystadenoma with OS 424• Hepatobiliary Cystadenoma without OS 425• Intraductal Papillary Mucinous Neoplasm of the Bile Duct 426
28. Hepatocellular Carcinoma 429Teo Jin Yao, Lee Ser Yee, Chan Chung Yip, Chung Yaw-Fui Alexander • Risk Factors 429
Jayp
ee B
rothe
rs

xxx Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
• Evidence-Based Review 429• Landmark Trials 433• Procedure 434• Surgical Anatomy 436• Step-by-Step Illustration of Procedure 439• Parenchymal Transection 447• Laparoscopic Resections 447• Robotic Liver Surgery 450• Operative Tips 451• Postoperative Complications 452• Outcomes 453• Conclusion and Future Directions 456
29. Intrahepatic and Perihilar Cholangiocarcinoma: Surgical Management 459Kayvan Roayaie, Sasan Roayaie
• Epidemiology 459• Risk Factors 460• Intrahepatic Cholangiocarcinoma 460• Perihilar Cholangiocarcinoma 463• Liver Transplantation for PCCA 466
30. Colorectal Liver Metastasis 468Ramraj Vemala Nagendra Gupta, Govind Nandakumar • Surgical Anatomy 469• Diagnosis 469• Management 471• Landmark Trials 473• Operative Tips 474• Outcome and Surveillance 475• Future 475
31. Gallbladder Cancer 478Pankaj Kumar Garg, Rambha Pandey, Durgatosh Pandey • Evidence-Based Review of Different Aspects of Surgical Management of GBC 480• Radical Cholecystectomy 482• Conclusion and Future Directions 486
32. Ex Vivo Resection of Complex Abdominal Masses 489Abhishek Mathur, Tomoaki Kato
• Ex Vivo Surgery in Liver Pathology 489• Ex Vivo in Cholangiocarcinomas and Klatskin Tumors 489• Ex Vivo in HCC 491• Ex Vivo and Colorectal Metastases 492• Ex Vivo for Benign Liver Lesions or Lesions with Low Malignant Potential 492• Ex Vivo and Pancreatic Adenocarcinoma 496
Jayp
ee B
rothe
rs

Contents xxxi
• Ex Vivo for Pancreatic Lesions with Low Malignant Potential 497• Ex Vivo for Lesions at the Root of the Mesentery 500
33. Operative Techniques for Liver Transplantation 506Pejman Radkani, Vikram Wadhera, Sander Florman • History 506• Preoperative Planning 506• Operative Techniques 507
34. Perioperative Management of Liver Transplantation 513Parissa Tabrizian, Josep Marti-Sanchez, Antonios Arvelakis, Sander Florman • Pathophysiology and Preoperative Evaluation 513• Intraoperative Monitoring 514• Surgical Techniques 516• Challenges Associated with Transplantation 516• Postoperative Care after Liver Transplantation 517• Complications 518
35. Indications and Contraindications for Liver Transplantation 522Parissa Tabrizian, Sander Florman • Allocation Systems 522• Preoperative Evaluation 523• Indications 523• Contraindications 527• Living Donor Liver Transplantation 528
Section 5: Pancreas
36. Management of Acute and Chronic Pancreatitis: Focus on Surgical Management 533Beth Schrope • Acute Pancreatitis 533• Chronic Pancreatitis 543• Conclusion and Future Directions 563
37. Pancreatic Cancer 566Jumana Jaloudi, Michael D Kluger • Diagnostic Approach 568• Surgical Management 570• Other Procedures 581• Outcomes and Considerations 585• Landmark Trials 585
38. Borderline Resectable Pancreatic Cancer 589Abhishek Mitra, Bhawna Sirohi, Mahesh Goel, Shailesh V Shrikhande
• Evidence-Based Review 589• Landmark Trials 593• Preoperative Planning 594
Jayp
ee B
rothe
rs

xxxii Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
• Surgical Anatomy 594• Operative Tips for Vein Resection 596• Postoperative Management and Complications 598• Outcomes 599• Future Trends 599
39. Endocrine Tumors of the Pancreas 603Kareem Ibrahim, Hasan Aldailami, Thomas J Fahey III
• Anatomy and Physiology of the Pancreas 603• Diagnosis 605• Insulinoma 606• Gastrinoma 609• Glucagonoma 612• Somatostatinoma 613• Incidentaloma 613• Operative Strategies 614
40. Pancreas Transplantation 619Samuel Sultan, Anthony Watkins
• Evidence-Based Review 619• Landmark Trials 621• Donor Procurement 622• Pancreas Transplantation 624• Operative Tips 628• Complications 631• Outcomes 632• Conclusion and Future Directions 632
Section 6: Small Bowel and Abdomen
41. Crohn’s Disease of the Small Bowel 637Daniele Scoglio, Alessandro Fichera
• Preoperative Planning 637• Surgical Procedure 638• Operative Technique: Gastrojejunostomy 638• Operative Technique: Strictureplasty 640• Operative Technique: Laparoscopic Ileocolic Resection 644
42. Gastrointestinal Stromal Tumors 652John Creasy, Benjamin Golas, Melanie Ongchin
• Pathology 652• Prognostic Features and Risk Stratification 654• Clinical Presentation 654
Jayp
ee B
rothe
rs

Contents xxxiii
• Diagnosis 654• Treatment and Prognosis 657• Future Directions 664
43. Carcinoid Tumors of the Gastrointestinal Tract 667Tushar Samdani, Vanessa Hui, Rashmi S, Govind Nandakumar
• Clinical Presentations and Symptoms 667• Pathological Diagnosis and Reporting of NET 669• Management of Locoregional Unresectable or Metastatic Carcinoid Tumors 671• Landmark Trials 672• Outcomes 674• Conclusion and Future Directions 675
44. Trauma of the Gastrointestinal Tract 678Soumitra R Eachempati, Philip S Barie
• Initial Diagnosis of Abdominal Injuries 678• Management of Hollow Viscus Injuries 678• Injuries to the Stomach 679• Duodenal Injuries 680• Small and Large Bowel Injuries 680• Rectal Injuries 681• Injuries to the Spleen 682• Liver Injuries 684• Injuries to the Pancreas 687
Section 7: Colon
45. Volvulus 693Evan N Feldman
• Sigmoid Volvulus 693• Cecal Volvulus 695• Ileosigmoid Knotting 695• Volvulus of the Transverse Colon or Splenic Flexure 695• Colonic Volvulus in Pregnant Women 696
46. Diverticulitis 697Gregory Charak, Chukwuma Apakama, Steven Lee-Kong
• Evidence-Based Review 697• Trials 699• Rationale for Minimally Invasive Approach 699• Conclusion and Future Directions 704
47. Surgical Management of Constipation 705Christopher T Aquina, Christian P Probst, Kristin N Kelly, Christina Cellini
• Prevalence 705
Jayp
ee B
rothe
rs

xxxiv Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
• Etiology and Risk Factors 705• Classification 705• Diagnosis and Workup of Constipation 705• History and Physical Exam 706• Overview of Diagnostic Schema 708• Disordered Defecation Studies 708• Colonic Transit Studies 709• Lifestyle Modification 710• Medication Therapy 710• Biofeedback 712• Surgical Options for Slow Transit Constipation 712• Surgical Options for Defecatory Disorders 715
48. Surgical Management of Ulcerative Colitis 719Vitaliy Y Poylin, Thomas Cataldo
• Preoperative Planning 722
49. Surgical Management of Crohn’s Colitis 732Mukta K Krane
• Clinical Presentation 732• Indications for Surgery 732• Failure of Medical Management 733• Procedures 733
50. Hereditary Nonpolyposis Colorectal Cancer Syndromes 739Joongho Shin
• Hereditary Nonpolyposis Colorectal Cancer Syndromes (Lynch Syndrome, LC) 739• Hamartomatous Tumor Syndrome 739• Conclusion and Future Directions 743
51. Inherited Polyposis Syndromes 745Maria Ximena Traa Kiely, Lilian Chen, James Yoo
• Investigation of Polyposis Syndromes 748• Management 748• Prevention 756• Conclusion and Future Directions 756
52. Difficult Polypectomy 760Erman Aytac, Emre Gorgun
• Endoscopic Mucosal Resection 761• Endoscopic Submucosal Dissection 762• Combined Endoscopic and Laparoscopic Surgery 769
53. Laparoscopy for Colon Cancer 773Jared Wong, James Fleshman
• Colon Cancer 773
Jayp
ee B
rothe
rs

Contents xxxv
• Right Colectomy 775• Hepatic Flexure Mobilization 777• Splenic Flexure Mobilization 781
54. Cytoreductive Surgery and Intraperitoneal Chemotherapy 787Michael Polcino, Leandro Feo, Garrett M Nash
• Technique 787• Evidence-Based Review and Outcomes 791
Section 8: Rectum
55. Rectal Prolapse 803Azah A Althumairi, Bashar Safar
• Clinical Presentation and Patient Evaluation 803• Evidence-Based Review and Landmark Trials 803• Surgical Procedures 805• Outcomes 808• Conclusion and Future Directions 809
56. Transanal Endoscopic Microsurgery 811Joshua A Tyler, Steven R Hunt
• Clinical Anatomy 811• Preoperative Evaluation 811• Operative Steps 812• Postoperative Care 815• Clinical Tips and Pitfalls 815
57. Rectal Cancer 816Usmaan Hameed, Anand Govindarajan
• Evidence-Based Review and Landmark Trials 816• Procedures 819• Complications 821• Conclusion and Future Directions 821
58. Management of Recurrent Rectal Cancer 823Paul RA O’Mahoney, Govind Nandakumar, Heather Yeo
• Risk Factors for Recurrence 823• Classification of Local Recurrence 823• Presentation and Incidence 825• Patient Selection 826• Preoperative Planning 826• Anatomic Considerations and Consultants 826• Imaging 826• Operative Technique 827• Intraoperative Radiation Therapy 828
Jayp
ee B
rothe
rs

xxxvi Evidence-Based Practices in Gastrointestinal, Colorectal and Hepatobiliary Surgery
• Postoperative Care 829• Complications 829• Palliative Treatment 830• Future Directions 830
59. Laparoscopic Proctectomy 833Alexis L Grucela, John-Paul Bellistri, Aida Taye
• Evidence-Based Review 833• Preoperative Preparation and Prevention 834• Surgical Anatomy 837• Step-by-Step: Laparoscopic Low Anterior Resection 839• Operative Tips 846• Outcomes and Complications 847• Future Directions 850• Landmark Trials and Key Studies 850
60. Robotic Proctectomy 855Carrie Y Peterson, Govind Nandakumar
• Indications 855
61. Acute and Chronic Pouch Complication 867Lilian Chen, Joseph Batac, Todd D Francone
• Acute Complications 867• Chronic Complications of IPAA 872• Pouch Dysfunction 876
62. Retrorectal Tumors 887Rebecca A Levine, Rahul Narang
• Evidence-Based Review 887• Procedure 893• Complications 896• Outcomes 896• Future Directions 897
Section 9: Anus
63. Hemorrhoids 903Ziad N Kronfol, Melissa M Alvarez-Downing
• Surgical Anatomy 903• Preoperative Planning 905• Closed Hemorrhoidectomy (Ferguson) 905• Open Hemorrhoidectomy (Milligan-Morgan) 907• Stapled Hemorrhoidopexy (Procedure for Prolapse and Hemorrhoids, PPH) 908
Jayp
ee B
rothe
rs

Contents xxxvii
• Ligasure Emorrhoidectomy 910• Transanal Hemorrhoidal Devascularization or Hemorrhoidal Artery Ligation 911
64. Surgical Therapy for Fecal Incontinence 915Kelly A Garrett
• Etiology 915• Assessment 917• Physiologic Testing 917• Treatment 919
65. Perianal Crohn’s Disease 929Emily Steinhagen, Randolph M Steinhagen
• Evaluation 929• Treatment 929• Skin Tags 930• Anal Fissure and Ulceration 930• Stricture 931• Abscess and Fistula 931• Carcinoma 934
66. Anorectal Sexually Transmitted Diseases 937Maria Camilla Ramirez, Lester Gottesman
• Bacterial STD 937
67. Anal Cancer and Anal Intraepithelial Neoplasia 943Jason R Bingham, Amit K Agarwal, Scott R Steele
• Evidence-Based Review 945• Landmark Trials 951• Preoperative Planning 952• Surgical Anatomy 952• Abdominoperineal Resection 954• Technique for AIN 963• Conclusion and Future Directions 965
Index 971
Jayp
ee B
rothe
rs

Video 12.1. Robotic Nissen Fundoplication
Video 21.1. Gastric Bypass and Biliopancreatic Diversion
Video 22.1. Laparoscopic Sleeve Gastrectomy and Hiatal Hernia Repair
Video 23.1. Mini Gastric Bypass
Video 30.1. Laparoscopic Segment IVB Colorectal Liver Metastatectomy
Video 46.1. Sigmoid Colectomy
Video 52.1. Submucosal Saline Injection
Video 52.2. Marking of the Lesion
Video 52.3. Repair of a Mucosal Defect Developed during ESD with Endoclips in a Patient with Large Cecal Polyp
Video 59.1 Laparoscopic Proctectomy
Video 60.1 Robotic Proctectomy
Video 67.1 Laparoscopic Abdominal-perineal Resection
Video Legends Available on emedicine360.com
Jayp
ee B
rothe
rs

Additional Videos
• Transanal Minimally Invasive Surgery • Laparoscopic Left Hemicolectomy • Laparoscopic Total Proctocolectomy with J-Pouch • J-Pouch Creation
Available on emedicine360.com
Jayp
ee B
rothe
rs

Pancreas Transplantation40Samuel Sultan, Anthony Watkins
BACKGROUNDType 1 diabetes mellitus affects ∼30 million people world-wide and the incidence has been increasing recently, by about 3% per year.1 Prior to the discovery of insulin, the average life expectancy was only 2 years after being diagnosed with diabetes. The advent of purified insulin improved the prognosis significantly; however, it conse-quently led to the recognition of a number of long-term sequelae of hyperglycemia including neuropathy, retino-pathy, and nephropathy. In 1966, Kelly and Lillehei described the first simultaneous pancreas-kidney trans-plants (SPK), performed at the University of Minnesota for a uremic diabetic patient.2 The goal was to simulta-neously restore functioning β cells allowing adequate insulin production, thus preventing recurrent diabetic nephropathy in the renal allograft. Although initial results were dismal, outcomes significantly improved with the advent of improved immunosuppression and modifica-tions in surgical technique. The Diabetes Control and Complications Trial estab-lished that tight glycemic control is imperative to avoid the development of secondary complications.3 Unfortunately, these complications are not reversed by intense insulin therapy and there are risks of iatrogenic hypoglycemia. Currently, no form of exogenous insulin administration is able to achieve the euglycemic, insulin-independent state that is possible with pancreas transplantation (PTx). The American Diabetes Association (ADA) recommends that SPK transplantation should be considered for type 1 diabetics who require kidney transplantation (KTx), and pancreas transplantation alone (PTA) for patients with brittle diabetes or episodes of hypoglycemic unaware-ness. Recent studies have also documented a benefit of PTx in a select group of patients with type 2 diabetes.4
Almost a half-century later, SPK transplantation remains the definitive and optimal treatment for patients with both type 1 diabetes mellitus and end-stage renal
disease (ESRD). During this time, there have been numer-ous developments and modifications to PTx, and several innovations still remain on the horizon.
EVIDENCE-BASED REVIEWThe immediate goal and benefit of PTx are to achieve a euglycemic state without the need for exogenous insulin. In addition, PTx adds the potential to not only halt the progression of some secondary diabetes-associated com-plications, but also lead to resolution of some of these processes.5 Lastly, several studies have demonstrated a survival benefit associated with SPK in comparison to uremic patients who remain on hemodialysis and reci-pients of KTx alone.6-8
While the kidney remains the most commonly trans-planted organ, the number of PTx has been limited for several reasons. First, as is the case with organ transplan-tation in general, a significant discrepancy exists between organ supply and demand. In addition to the limited sup-ply, pancreas allograft acceptance is more highly selective than other organs. In this case, the possibility of underu-tilization has been examined. Finally, optimal selection of recipients is equally important to ensure successful out-comes, particularly since the surgery is more extensive. While deceased donation experienced a significant increase from 2002 to 2007, coinciding with the inception of the Organ Donation Breakthrough Collaborative spon-sored by Health Resources and Services Administration, PTx rates decreased during the same time period.9-11 Several groups have attempted to define the challenges with pancreata utilization. Based on the data from the United Network for Organ Sharing, Stratta and Bennett noted that only 60% of the pancreas grafts recovered were transplanted. The reasons cited for discard were often labeled as unknown, indicating the need for improved data tracking.12 Wiseman et al. examined Organ Procurement and Transplantation Network data from 2005 to 2007 and
Jayp
ee B
rothe
rs

620 Pancreas
identified a subgroup of 1,763 potential pancreas donors (PPDs) defined by age (19–40 years), body mass index (BMI; <30 kg/m2), successful liver donation, and negative viral serology testing, which were not used.13 They discov-ered that 85% of the 1,763 donors declined for pancreas procurement were reported as relating to donor age/qua-lity. They were neither able to define specific medical or social or behavioral characteristics of PPD that precluded successful donation nor able to identify a correlation with donor service area (DSA), making it difficult to clearly ascertain the reason for such high discard rates. Geographic variability in utilization of potential trans-plantable pancreata led to the development of the pan-creas donor risk index (PDRI). This tool was established to assess the differential impact of organ quality on PTx out-comes, specifically as a function of the type of transplant [SPK, pancreas after kidney transplants (PAK), and PTA] and recipient severity of illness to help guide the clinician to optimize pancreas utilization.14 Retrospective analy-sis of all PTx from the Scientific Registry of Transplant Recipients from 2000 to 2006 was performed using a Cox regression analysis controlling for the donor and reci-pient characteristics. Ten donor variables including age, BMI, race, and serum creatinine, and one transplant fac-tor (cold ischemia time) were used to develop the PDRI. The median risk donor was defined as a 28-year-old non-black, non-Asian man, with a BMI of 24 kg/m2, a height of 173 cm, non-cerebrovascular accident (CVA) as the cause of death, pancreas preservation time of 12 hours, non-donation after cardiac death (DCD) and serum creatinine <2.5 mg/dL. Increasing PDRI was associated with a significant, graded reduction in 1-year pancreas graft survival. Importantly, recipients of PTAs or PAKs whose organs came from donors with an elevated PDRI (1.57–2.11) experienced a lower rate of 1 year graft sur-vival (77%) compared with SPK recipients (88%). Further investigations have supported these findings with nega-tive prognostic donor factors including donor BMI ≥30 [hazard ratio (HR) 1.87, p = 0.005), donor Cr ≥ 2.5 (HR 3.16, p = 0.007), donor age >50 (HR 1.73, p = 0.082), and preservation time >20 hours (HR 2.17, p < 0.001).15
In addition to the importance of a carefully selected donor, a comprehensive pretransplant recipient workup is essential. A multidisciplinary approach that consists of a thorough medical, surgical, and psychosocial evalua-tion common to the evaluation of a potential KTx recipi-ent is necessary. A major focus of the recipient evaluation
is the cardiac assessment because cardiovascular disease is responsible for the largest fraction of recipient deaths and the majority of waitlist deaths.16 While there is no absolute age cutoff for PTx, many institutions have placed age limitations on potential pancreas transplant recipi-ents due to some data suggesting that age is a risk factor for inferior outcomes. For example, in one study, recipi-ents ≥ 50 years of age had higher incidence of graft throm-bosis and bleeding requiring re-exploration, as well as a higher incidence of pulmonary infections.17 Other studies have also shown a lower patient survival for older patients (≥45 years) undergoing PTx.18,19 However, it is important to point out that there are data showing good outcomes in carefully selected older patients. Afaneh et al. found com-parable outcomes between patients of ≥50 years of age versus younger patients in relationship to surgical mor-bidity, incidence of infections, and acute rejection (AR) rates.20 A group from Indiana University similarly found that recipient age had no statistically significant effect on PTx outcomes, in which 18 of the 405 patients were >60 years of age, suggesting that older patients should not necessarily be excluded from PTx solely on the basis of age, as long as they are otherwise carefully screened.21
Additional factors that affect outcomes include the type of pancreas transplant performed and technical aspects of the procedure. SPK transplantation has been shown to have superior outcomes in comparison to PAK and PTA. The most recent report from the International Pancreas Transplant Registry (IPTR), a database that has been collecting allograft and patient survival outcomes since 1980, demonstrated 1-year allograft survival rates of 86% and 93% for the pancreas and kidney, respec-tively, after SPK.22 Following PAK and PTA, 1 year allo-graft survival reached 80% and 78%, respectively. These differences in outcomes are partly related to the benefit of earlier recognition of rejection in the SPK due to the concordant nature of rejection in 60–70% of cases. Since renal function abnormalities (i.e. creatinine rise) are detectable earlier than pancreas dysfunction (amylase, lipase, or hyperglycemia), rejection is often detected and treated more promptly in these cases. Early outcomes were marred with graft loss due to technical complica-tions. In all three categories, early technical graft loss rates have decreased significantly over time, now affect-ing ~8–9% of patients; however, they remain a challenge. The 1-year and 5-year PTx allograft survivals when per-formed SPK are 86.4% and 72%, respectively. In addition,
Jayp
ee B
rothe
rs

Pancreas Transplantation 621
the 1-year KTx allograft survival is 93% in the SPK group. The 1-year and 5-year allograft survivals for PTAs were lower at 75.4% and 48.3%, respectively. The 1-year and 5-year allograft outcomes for the PAK allografts are mod-estly superior to the PTA group with survivals approach-ing 80% and 58%, respectively. The options for venous drainage include portal via the superior mesenteric vein (SMV) or systemic via the iliac or inferior vena cava (IVC). Portal venous drainage has the potential advantage of replicating the natural physi-ology by allowing first-pass degradation of insulin in the liver. Systemic drainage leads to hyperinsulinemia, which is thought to be an independent risk factor for increased ischemic cardiovascular disease, although in clinical practice no cardiovascular adverse effects have been dem-onstrated. Most importantly, studies have demonstrated similar outcomes with both types of venous drainage.23,24 In recent series, the prevailing mode is systemic drainage. Drainage of exocrine secretions can be performed by either bladder or enteric anastomoses. Bladder drainage provides the advantage of having the ability to monitor the rejection by measuring urinary amylase, less severe complications, and the ability to perform a cystoscopic biopsy. The disadvantages of bladder drainage include electrolyte abnormalities, chronic acidosis, dehydration, and urinary tract infections. Urologic complications such as hematuria, cystitis, urethritis, and bladder stones may also occur. The solution for poorly tolerated complica-tions of bladder drainage is re-exploration with conver-sion to enteric drainage.25,26
Enteric drainage can be accomplished by anastomo-sing the allograft duodenum to the recipient intestine. This is commonly performed with a hand-sewn anasto-mosis, although techniques for stapled anastomosis using an end-to-end anastomotic (EEA) stapler device are also described.27 The main advantage of the enteric drainage technique is that it is more physiologic and avoids the metabolic and urologic complications associated with bladder drainage. The disadvantages include a loss of the ability to monitor the exocrine pancreatic secretions and higher, more severe complication rate. Recent IPTR data show that >80% of transplants are done with enteric drainage.28
As opposed to whole PTx, an alternative and deve-loping option is islet cell transplantation. First performed in 1977 at the University of Minnesota, islet transplants emerged in the setting of the early discouraging results for whole PTx.29 Islet cell transplantation involves the
extraction of islets of Langerhans from multiple pan-creata through the use of a complex purification process. These cells are then typically injected into the portal vein where they engraft in the parenchyma of the liver and secrete insulin. The Edmonton protocol established the safety and effectiveness of islet transplantation, given a sufficient number of islets.30 Refinement of isolation and digestion of the pancreas to obtain islets has allowed ∼3,000 islets/kg of recipient weight, a key element in the Edmonton protocol. The major challenges with islet trans-plants include obtaining optimal engraftment and poor long-term results in relationship to insulin independence. As further improvements in islet cell transplantation are attained, this approach could supplant PTx as a more attractive option due to its less invasive nature.
LANDMARK TRIALSPancreas transplantation began with poor graft and patient survival rates; therefore, very few procedures were initially performed. The major improvements in outcomes were derived from better immunosuppression and refinements in surgical technique. As such, these landmark trials provided insight into these new discov-eries and innovations that led to successful PTx and wide-spread recognition of its benefits. • Kelly WD, Lillehei RC, Merkel FK, et al. Allo-
transplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61(6):827-37.
• Najarian JS, Sutherland DE, Matas AJ, et al. Human islet transplantation: a preliminary report. Transplant Proc. 1977;9(1):233-6.
• The effect of intensive treatment of diabetes on the development and progression of long-term compli-cations in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Eng J Med. 1993;329(14):977-86.
• Sollinger HW, Odorico JS, Knechtle SJ, et al. Experience with 500 simultaneous pancreas-kidney transplants. Ann Surg. 1998;228:284-96.
• Fioretto P, Steffes MW, Sutherland DE, et al. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Eng J Med. 1998;339:69-75.
• Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplan-tation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regi-men. N Eng J Med. 2000;343(4):230-8.
• Sutherland DER, Gruessner RW, Dunn DL, et al. Lessons
Jayp
ee B
rothe
rs

622 Pancreas
learned from more than 1,000 pancreas transplants at a single institution. Ann Surg. 2001;233:463-501.
• Humar A, Ramcharan T, Kandaswamy R, et al. Pancreas after kidney transplant. Am J Surg. 2001;182(2):155-61.
• Kaufman DB, Leventhal JR, Koffron AJ, et al. A prospec-tive study of rapid corticosteroid elimination in simul-taneous pancreas-kidney transplantation: Comparison of two maintenance immunosuppression protocols: tacrolimus/mycophenolate mofetil versus tacrolimus/sirolimus. Transplantation. 2002;73:169-77.
• Kaufman DB, Burke GW III, Bruce DS, et al. Prospective, randomized, multi-center trial of antibody induction therapy in simultaneous pancreas-kidney transplanta-tion. Am J Transplant 2003;3:855.
• Humar A, Ramcharan T, Kandaswamy R, et al. Technical failures after pancreas transplants: why grafts fail and the risk factors—a multivariate analysis. Transplantation. 2004;78:1188-92.
• Gruessner AC, Sutherland DE. Pancreas transplant outcomes for United States (US) and non-US cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR) as of June 2004. Clin Transplant. 2005;19(4):433-55.
• Stratta RJ, Alloway RR, Lo A, et al. A prospective, randomized, multicenter study evaluating the safety and efficacy of two dosing regimens of daclizumab compared to no antibody induction in simulta-neous kidney-pancreas transplantation: results at 3 years. Transplant Proc. 2005;37:3531.
• Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplanta-tion. N Eng J Med. 2006;355:1318-30.
• Zhang R, Florman S, Devidoss S, et al. The long-term survival of simultaneous pancreas and kidney transplant with basiliximab induction therapy. Clin Transplant. 2007;21(5):583-9.
• Muthusamy AS, Vaidya AC, Sinha S, et al. Alemtuzumab induction and steroid-free maintenance immuno-suppression in pancreas transplantation. Am J Trans-plant 2008;8(10):2126-31.
• Schneeberger S, Biebl M, Steurer W, et al. A pro-spective randomized multicenter trial comparing histidine-tryptophan-ketoglutarate versus University of Wisconsin perfusion solution in clinical pancreas transplantation. Transplant Int. 2009;22:217-24.
DONOR PROCUREMENT
Preoperative PlanningCareful evaluation and recovery of the pancreas is criti-cal to the success of the subsequent transplant regard-less of the approach. While the use of living donors has been described, our focus will be limited to the deceased donor. Although donor selection criteria may vary among surgeons and transplant centers, the primary criteria, as mentioned before, include age, BMI, cause of death, and, most importantly, the gross appearance of the organ (evidence of inflammation, fibrosis or fatty infiltration) at the time of recovery. Again, factors such as older age (>40–50), obesity and stroke as the cause of death have been shown to negatively affect graft survival.14
Surgical Anatomy
The pancreas serves as both an endocrine and an exo-crine gland, and lies in the retroperitoneum at the level of the second lumbar vertebrae. The exocrine function includes the secretion of digestive enzymes, water, electro lytes, and bicarbonate, which are delivered to the duodenum via the pancreatic duct of Wirsung. The endocrine function is comprised of the secretion of insulin, glucagon, and somatostatin by the islets of Langerhans, A cells and D cells, respectively. The pancreas is divided into five parts including the head, uncinate process, neck, body, and tail. The head of the pancreas lies to the right of the superior mesen-teric artery (SMA). The uncinate process is a variable posterolateral extension of the head that passes behind the retropancreatic vessels and lies anterior to the IVC and aorta. The neck is defined as the portion of the gland overlying the superior mesenteric vessels. The body and tail lie to the left of the mesenteric vessels; there is no meaningful anatomic division between the body and tail. The arterial supply to the duodenum and pancreas is derived from the celiac axis and the SMA. The head of the pancreas receives blood supply from the gastroduodenal artery (anterior and posterior superior pancreaticoduodenal arteries) and SMA (providing the anterior/posterior inferior pancreaticoduodenal arteries). The splenic artery supplies the neck, body and tail of the pancreas. The venous drainage follows the arteries to provide tributaries to the splenic vein and SMV, which drain into the portal vein.
Jayp
ee B
rothe
rs

Pancreas Transplantation 623
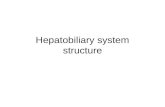
Step-by-Step Illustration of Procedure1. Dissection begins with mobilizing the spleen so that
it can be used as a handle allowing a “no touch” approach to the pancreas dissection (Fig. 1).
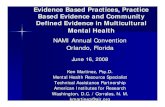
2. The duodenum is kept long by dividing distal to the pylorus and distal to the ligament of Treitz with a gastrointestinal (GI) stapler (Fig. 2).
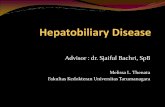
3. The portal vein is divided about halfway between the pancreas and the liver, leaving at least 1.5 cm of portal vein length above the superior pancreatic border (Fig. 3).
4. The common bile duct and gastroduodenal and splenic arteries are ligated and divided (Fig. 4).
5. The SMA is divided at the aorta (Fig. 5). 6. The root of the small bowel mesentery is stapled
(Fig. 6). 7. Remove a segment of the donor common; internal
and external iliac arteries are removed for Y graft creation.
Operative TipsIt is important to coordinate the pancreas procurement with other surgical teams when present. While pancreas
Fig. 1: “No touch” approach to pancreas dissection. The spleen is used as a handle to minimize direct manipulation of the pancreas.
Fig. 2: Duodenal division. The duodenum is kept long by dividing distal to the pylorus and distal to the ligament of Treitz with a gastrointestinal anastomosis stapler.
Fig. 3: Division of the portal vein. The portal vein is divided about halfway between the pancreas and the liver, leaving at least 1.5 cm of portal vein length above the superior pancreatic border.
Fig. 4: Division of the common bile duct, gastroduodenal and splenic artery. The splenic artery is tagged with a fine suture to later aid in identification.
Jayp
ee B
rothe
rs

624 Pancreas
dissection can be performed either prior to or after cross-clamp, we prefer to perform this dissection in the warm (prior to crossclamp) to assist with better hemostasis upon reperfusion in the recipient operation. Although isolated procurement of the pancreas is described above, an alternative option includes the en-bloc recovery tech-nique that involves removal of the pancreas with the liver followed by separation on the backtable.31,32 At some point prior to crossclamp it is important to advance a nasogas-tric tube into the duodenum to instill 500 mL of ampho-tericin solution (50 mg/L) into the second portion of the duodenum. This helps decontaminate this portion of the GI tract and combat future infectious issues. Avoid dissection of splenic artery into the pancreas parenchyma where the dorsal pancreatic artery can be injured. While either University of Wisconsin or histi-dine-tryptophan-ketoglutarate (HTK) solutions can be used, there are several reports of higher rates of AR, graft pancreatitis and worse graft survival with HTK.33-35 Some surgeons limit pancreatic flush to 1–2 L by occluding the SMA with a vessel loop.
PANCREAS TRANSPLANTATION
Preoperative PlanningThe selection of a candidate for transplant is a complex process that ensures that a detailed medical and surgical history is obtained, including a focused review of diabe-tes history. Typically, type 1 diabetes begins before the
age of 30, causes ketoacidosis, frequently requires insu-lin administration, and is not associated with excessive weight. However, patients do not always present as the prototypes of either type 1 or type 2, and such a distinc-tion may be an oversimplification. Nonetheless, patients who have had multiple episodes of diabetic ketoacidosis or hypoglycemic unawareness are typically considered to be absolute indications for PTx. In order to identify other patients who would benefit from PTx, a careful risk–benefit analysis should be performed, accounting for the type of pancreas transplant, depending on the renal function, and the patient’s overall risk profile. The recom-mended indications for transplant according to the ADA are shown in Table 1.36 Conversely, there are a number of important contraindications, both absolute and relative. The main absolute contraindications relate to a significant cardiac impairment—namely, significant and untreatable coronary artery disease, a recent myocardial infarction, or an ejection fraction <30%—or an active infection. Other contraindications include a history of untreated or recent malignancy, human immunodeficiency virus, hepatitis B (surface-antigen positive), substance abuse, major psy-chiatric illness, noncompliance, a life-limiting systemic illness, or significant hepatic or pulmonary dysfunction.37 Specific surgical aspects of the preoperative evaluation should include a detailed history of prior abdominal sur-gery, and focus on issues that would increase the risk of complications, including obesity and peripheral vascular disease (PVD).37
Fig. 5: Division of superior mesenteric artery. If there is a replaced right hepatic artery then division would need to be just distal to that takeoff.
Fig. 6: Division of root of small bowel. It should be stapled at least 3 cm away from the head of the pancreas and uncinate process to avoid injury to the inferior pancreaticoduodenal arcade.
Jayp
ee B
rothe
rs

Pancreas Transplantation 625
Diagnostic testing for a preoperative evaluation should include standard testing for major abdominal surgery, as well as testing relevant to transplantation, including viral serologic panels and tissue typing, and finally laboratories pertinent to both the pancreatic function—a C-peptide and hemoglobin A1c level—and renal function, possibly including a kidney biopsy, and a 24-hour urine collection for protein and creatinine clearance. Standard screen-ing for cancer should be performed, for breast, cervical, colorectal, and prostate cancer, as applicable, given the increased risk of cancer post-transplantation. For patients with a history of cancer, a variable waiting time is required depending on the type of cancer.37 Radiologic evaluation should include either an abdominal ultrasound, or more typically a computed tomography (CT) scan; such testing should look for any abnormal masses, gallstone disease, any kidney pathology, and/or significant vascular disease. Given the high prevalence of cardiovascular disease in this population, typical evaluation includes a stress test, whether exercise or pharmacologic, and an electrocar-diogram and echocardiogram. Other general measures include smoking cessation, blood pressure control, cor-rection of hyperlipidemia, increased exercise tolerance, and weight reduction. Ultimately, a thorough preopera-tive evaluation is best performed via a multidisciplinary collaboration, synthesizing input from surgery, medicine, and psychosocial.
Surgical AnatomyRegardless of the type of PTx performed, the approach is similar where the colon is mobilized or is to expose the retroperitoneal vessels including the IVC and iliac vessels.
Step-by-Step Illustration of Procedure There are four key components to the recipient opera-tion: (1) bench preparation, (2) incision and exposure, (3) revascularization, and (4) duct management.
Bench Preparation
1. The initial step involves a thorough inspection of the gland’s color, consistency, and fat content, looking for any injuries to the parenchyma or to the duodenum, and ensuring that the vasculature is adequate for reconstruction (Fig. 7).
2. The splenectomy is typically performed first utilizing either stapler device or individually ligating vessels with silk ties ligation (Fig. 8).
3. Excess fat and surrounding tissues are removed from the body and tail of the pancreas (Fig. 9).
4. The portal vein and splenic and superior mesenteric arteries are then dissected free by removing excessive tissue (Fig. 10).
5. Excessive duodenum is then removed with a gastro-intestinal anastomosis stapler and the staple line is oversewn (Fig. 11).
Table 1: Indications for pancreas transplantation.
Type of transplant Criteria
Simultaneous kidney and pancreas transplant • CKD stages 4 or 5 (creatinine clearance <30 mL/min) with type 1 diabetes and with other diabetic complications
• Prior renal transplant which is failing in a type 1 diabetic
Pancreas after kidney transplant • Prior functioning kidney transplant in type 1 diabetic with other diabetic complications
Pancreas transplant alone • Hyperlabile diabetes defined by frequent acute severe metabolic complications (hypoglycemia, marked hyperglycemia, and ketoacidosis) requiring medical attention
• Clinical and emotional problems with insulin therapy that are incapacitating • Consistent failure of insulin-based management to prevent complications • Presence of (two or more) diabetic complications that are progressive and
unresponsive to intensive insulin therapy • Early diabetic nephropathy • Proliferative retinopathy • Symptomatic peripheral or autonomic neuropathy • Vasculopathy with accelerated atherosclerosis
Jayp
ee B
rothe
rs

626 Pancreas
6. The root of the small bowel mesentery should be rein-forced for hemostasis with a running 4-0 polypropy-lene suture (Fig. 12).
7. The arterial reconstruction begins by preparing the donor iliac artery by removing excessive tissue (Fig. 13).
8. The Y graft is then used to create an end-to-end anastomosis between the hypogastric and the splenic artery and between the external iliac and SMA using 6-0 Prolene (Fig. 14).
Fig. 7: Inspection of pancreas. This step is important to confirm that there are no issues with the pancreas that could prevent successful transplantation.
Fig. 9: Removal of excess fat and surrounding tissues are from body and tail of the pancreas. The splenic artery and inferior mesenteric vein can be used as landmarks for medial dissection.
Fig. 10: The portal vein and splenic (red arrow) and superior mesenteric artery (yellow arrow) are then dissected free by removing surrounding tissue.
Incision and Exposure 1. There are two main options for the choice of incision:
a lower quadrant extraperitoneal incision or a midline intraperitoneal approach (Figs. 15 and 16).
2. Upon opening the peritoneal cavity, a Bookwalter self-retaining retractor or similar retractor should be used (Fig. 17).
3. The right colon is mobilized to expose the retroperi-toneal vessels (Fig. 18).
Fig. 8: Splenectomy. Care should be taken to avoid injuring the tail of the pancreas during this procedure.
Jayp
ee B
rothe
rs

Pancreas Transplantation 627
Revascularization 1. For systemic drainage, the right common iliac artery
and IVC and/or right common iliac veins should be dissected free (Fig. 19).
2. Portal venous drainage is performed via an end-to-side anastomosis from the allograft portal vein to the recipient SMV (Fig. 20).
Duct ManagementBladder drainage 1. The bladder anastomosis is performed between the
anti mesenteric border of the duodenum and the dome of the bladder in a two-layered hand-sewn fash-ion (Fig. 21).
Fig. 11: Removal of excessive duodenum is then removed with gastrointestinal anastomosis stapler and the staple line is oversewn. (SMA: Superior mesenteric artery; SMV: Superior mesenteric vein).
Fig. 12: The root of the small bowel mesentery should be reinforced for hemostasis with a running 4-0 polypropylene suture. (SMA: Superior mesenteric artery; SMV: Superior mesenteric vein).
Fig. 13: The donor iliac artery is prepared for Y graft creation. Avoid excessive tension in the area of bifurcation to prevent intimal damage and the limbs should be trimmed to no greater than 1–1.5 cm to minimize risk of kinking.
Jayp
ee B
rothe
rs

628 Pancreas
2. Alternatively, an EEA stapler can be used to perform
this anastomosis (Fig. 22).
Enteric drainage 1. Either a loop of adjacent small bowel or a Roux en Y
limb is aligned with the duodenum (Fig. 23).
2. A hand-sewn, two-layered anastomosis is performed
using a nonabsorbable suture for the outer layer and
the absorbable inner layer. The bowel is opened using
electrocautery (Fig. 24).
OPERATIVE TIPSThe backbench preparation of the pancreas requires substantial work, even more so than other solid organ transplants, and is considered paramount to successful transplantation. The allograft should remain immersed in
Fig. 14: The Y graft is then used to create an end-to-end anasto-mosis between the hypogastric/splenic artery and the external iliac/superior mesenteric artery. This anastomosis is usually performed a fine suture such as 6-0 Prolene.
Fig. 15: Right lower quadrant extraperitoneal incision.
Fig. 16: Midline incision for intraperitoneal approach. Fig. 17: A Bookwalter self-retaining retractor used for exposure.
Jayp
ee B
rothe
rs

Pancreas Transplantation 629
a cold preservation solution-surrounded by slushed ice, in a large sterile basin during this preparation. While the length of the duodenal segment does not need to be pre-cise, care should be taken to avoid an excessively lengthy segment, which may be at risk for ischemia, bearing in
Fig. 18: The right colon is mobilized (arrows) to expose the retro-peritoneal vessels.
Fig. 19: The common iliac artery and inferior vena cava and/or common iliac veins are dissected free. Branches should be ligated (dashed lines) and divided to allow adequate mobilization (arrow).
Fig. 20: Portal venous drainage is performed via an end-to-side anastomosis from the allograft portal vein to the recipient superior mesenteric vein. The arterial anastomosis is similar to the techniques used for systemic drainage with the addition of an aortic conduit.
Fig. 21: The bladder anastomosis is performed between the antimesenteric border of the duodenum and the dome of the bladder in a two-layered hand-sewn fashion. Here the arrow illustrates completion of the anastomosis.
mind that the entire perfusion is dependent on retrograde flow through the inferior pancreaticoduodenal artery. The limbs of the Y graft should be kept short, typically <1 cm, to minimize the risk of twisting or kinking. Various approaches exist in regard to the recipient portion such as the initial incision, the position of the graft, the artery and vein used for anastomosis, the type of exocrine drainage, the use of staplers, and the use and location of abdominal drains.38 The key is to adhere to surgical principles so that regardless of the approach, good outcomes will be achieved. For example, with the extraperitoneal approach, it is advisable to open the peri-toneum to allow for drainage of peripancreatic fluid.39
Jayp
ee B
rothe
rs

630 Pancreas
The more common, systemic drainage was described. For portal venous drainage, the SMV is isolated and uti-lized. When the common or external iliac vein is used for systemic drainage, it should be completely mobilized in order to facilitate tension free anastomosis. Since it is a larger vessel, when anastomosing to the IVC only enough
of the vein needs to be dissected to allow for vascular control, thereby saving time and enabling a less difficult anastomosis. The head of the pancreas can either be oriented supe-riorly or inferiorly, and the type of exocrine drainage or surgeon’s preference determines positioning. Of note, an
Fig. 22: An alternative approach includes using an EEA stapler. With this approach one end of the duodenum (arrow) and a separate site on the bladder (dashed arrow) is opened to allow placement of the stapler and the anvil, respectively. (EEA: End-to-end anastomotic).
Fig. 23: Either a loop of adjacent small bowel (yellow arrow) or a Roux-en-Y limb is aligned with the duodenum (blue arrow).
Fig. 24: A hand-sewn, two layered anastomosis is performed using a nonabsorbable suture for the outer layer (arrow) and absorbable inner layer. An alternative approach is a standard bowel anastomosis using a gastrointestinal anastomosis stapler.Ja
ypee
Brot
hers

Pancreas Transplantation 631
intraperitoneal approach is preferred when bladder drain-age is utilized. Also, since the head of the pancreas is ori-ented downward, the vessel anastomoses are approached slightly differently. The iliac vein is often used for venous drainage and requires complete mobilization with divi-sion and suture ligation of all branches to allow correct orientation of the portal vein and Y graft. In addition, the arteriotomy and venotomy are placed in a fashion that allows medial placement of pancreas allograft. Since the iliac vessels tend to be more superficial in the right lower quadrant, right-sided implantation is typically pursued. This allows a technically easier anastomosis and left-sided implantation has been correlated with increased risk for graft thrombosis.40
After the allograft is reperfused, bleeding is controlled with the help of suture ligatures and clips. Inspection and palpation over the entire length of the graft should be per-formed to ensure adequate perfusion.
COMPLICATIONSIn the earlier stages of PTx, in the 1980s, nearly 25% of pancreas transplants failed due to surgical complica-tions.41 More contemporary series demonstrate that there has been significant improvement over the last few dec-ades, with technical failure rates now typically <10%.42 Nevertheless, complications after PTx are not uncommon and typically cause significant morbidity. The most nota-ble complications include thrombosis, pancreatitis, anas-tomotic leak, infection, rejection, and bowel obstruction. As previously mentioned, additional complications that are unique to the use of bladder drainage include cysti-tis, metabolic acidosis, bleeding at the duodenal cuff, and fluid losses causing dehydration. Overall, the most com-mon serious surgical complication is vascular thrombo-sis, which affects approximately up to 12% of transplants, and is the main cause of nonimmunologic graft failure.43 Thrombosis usually presents as hyperglycemia, tender-ness over the graft, graft enlargement, and in bladder drainage with hematuria and decreased urinary amylase levels. The diagnosis is made based on ultrasound, CT angiography, magnetic resonance angiography, or con-ventional angiography. A key piece in preventing com-plications involves identifying the relevant risk factors. An analysis of vascular thrombosis revealed several risk factors: donor age, death from vascular disease (cardiac or cerebral), the use of an aortic Carrel patch, reconstruc-tions other than the Y-graft, left-sided implantation, and
graft pancreatitis.40 In addition to mitigating or avoiding such risk factors, there are various protocols for treating the patient with a form of anticoagulation, whether a heparin infusion, acetylsalicylic acid, or even warfarin.44
The management of vascular thrombosis typically entails exploration and removal of the graft, in order to prevent a leak and sepsis—doing so promptly reduces the risk of morbidity and mortality.41 Rarely, a thrombo-sis may be safely managed nonoperatively, or with endo-vascular interventions.45,46 As an alternative to complete removal of the graft, partial removal has been described in the setting of a partially thrombosed graft with a via-ble remainder.47 Another consolation in the management of thrombosis involves the possibility of simultaneous retransplantation at the time of pancreatectomy of the thrombosed graft, provided the patient is stable.48
Aside from thrombosis, another possible complica-tion is pancreatitis, which can occur either early (typically defined as within 3 months) or late after transplant. In the early period, it can be difficult to diagnose, given that hyperamylasemia is seen in up to 35% of patients post-transplant.49 Late-stage pancreatitis occurs on average 28 months after transplant.50 Similar to native pancrea-titis, graft pancreatitis typically presents with tenderness over the graft, and may lead to further complications such as abscess, necrosis, fistula, or pseudocyst. Risk factors for early pancreatitis include donor age and obesity, and cold ischemia time. An analysis of late graft pancreatitis, on the other hand, did not reveal any significant risk fac-tors.50 A CT scan may be useful in determining the pan-creatic parenchymal viability and the possible need for debridement of pancreatic necrosis. Patients with bladder drainage may be treated with a urinary catheter to prevent reflux as a possible cause of pancreatitis. And for cases of recurrent reflux-induced pancreatitis, it may necessitate a revision to enteric drainage. Otherwise, treatment is similar to that for native pancreatitis, primarily involving bowel rest, along with percutaneous drainage and anti-biotics as needed, and outcomes are typically favorable. Anastomotic leak represents a significant complica-tion, but it has variable significance depending on the method of drainage, whether bladder or enteric. In blad-der drainage, duodenal leaks typically occur within the first 3 months postoperatively, are readily diagnosed with a cystogram, and are often not devastating. Such leaks can be managed with prolonged indwelling cath-eterization to decompress the bladder, which is effective
Jayp
ee B
rothe
rs

632 Pancreas
treatment in the majority of cases.51 More complex cases may require surgical repair, or conversion to enteric drainage.52 On the other hand, leakage from an enteric-drained graft typically causes sepsis and peritonitis due to enteric spillage. Leaks may occur at any time, although early leaks are technically related, whereas late leaks may be caused by rejection, infection, or ischemia. Leaks are best diagnosed by the CT scan. Once diagnosed, prompt surgical re-exploration is warranted, with a conversion to a Roux en Y drainage, or even graft pancreatectomy if the contamination is severe or the patient is unstable. Intra-abdominal infection may occur with or without an associated anastomotic leak. Such infections typi-cally occur within the first 30 days postoperatively, and are usually bacterial, but occasionally may be fungal in origin. Risk factors include older donor age, retransplan-tation, pretransplant peritoneal dialysis, extended preser-vation time, graft pancreatitis, and immunosuppression with sirolimus. In stable patients, a CT scan is helpful in determining the extent of the infection, and also in diag-nosing an associated anastomotic leak. For an isolated infection without a leak, percutaneous drainage and anti-biotics are the recommended treatment, and are effective in over 80% of cases.49
Like any transplant, PTx can be complicated by immune-mediated rejection. As such, a more complete discussion of rejection can be found elsewhere.53 However, there are several unique aspects of pancreatic rejection. Monitoring for rejection typically includes measurement of glucose levels, and serum amylase and lipase levels, and in the case of bladder drainage, urinary amylase levels. Yet, such measurements are not highly accurate gauges of rejection, and a tissue biopsy is required to firmly establish a diagnosis of rejection, and its subtype. In a large series, biopsy of the pancreas graft has been shown to have a low rate of clinically significant com-plications.54 Alternatively, especially in centers with less experience in pancreas biopsy, a sentinel organ is often biopsied, whether from the kidney graft in the case of a SPK, or from the duodenal patch, though studies have found approximately a 20% rate of discordance between biopsies of a sentinel organ compared to the pancreas graft.55 Similar to rejection, the long-term infectious com-plications of PTx are related to the immunosuppression, and are similar to that of other solid organ transplants. In comparison to whole-organ transplantation, islet transplantation is associated with significantly fewer and less severe complications. The rate of serious complications
is ∼10%, including the possibilities of portal vein throm-bosis and intra-abdominal hemorrhage.56 Longer-term complications are similar to that of whole-organ trans-plantation, and relate mostly to infectious complications due to the immunosuppression. Additionally, there is a potential for sensitization and the formation of anti-bodies.
OUTCOMESCardiac function improves within 6 months of PTx, and other peripheral vascular disease PVD may stabilize, although the data are mixed. Most studies show some improvement in neuropathy and gastroenteropathy after transplant. Early nephropathy improves after pancreas transplant, but not retinopathy. Respondents report bet-ter quality of life after transplant.
Graft and Patient SurvivalNow 3-year patient survival rates after PTx are 89%, with 3-year graft survival rates of 65%. A higher risk of graft failure is associated with solitary pancreas transplants, which leads some centers to have more stringent selec-tion criteria for PTA and PAK.
CONCLUSION AND FUTURE DIRECTIONSSince its inception nearly 50 years ago, there have been numerous advancements in the field of PTx. As such it has taken root as the definitive treatment for patients with type 1 diabetes and ESRD, and is useful in various other circumstances. As outcomes continue to improve, and complications reduced, the indications for trans-plant may expand further, particularly for the large pool of patients with type 2 diabetes. There are several developments on the horizon span-ning the entirety of the transplant process, ranging from refining the surgical technique to exploring new immuno-suppressive agents. In 2012, Boggi et al. reported their experience with the world’s first robotic-assisted pancreas transplant.57 The future role of robotics in PTx is yet to be determined, although it may offer a solution for reduc-ing the persistently high rate of surgical complications.58 Immune therapy has evolved significantly both in efficacy and minimization of toxicity, and there are numerous new drugs being developed and tested, such as the pro-tein kinase C inhibitor–sotrastaurin, the JAK 3 inhibitor—tofacitinib, the proteasome inhibitor—bortezomib, the
Jayp
ee B
rothe
rs

Pancreas Transplantation 633
CD28-CD80/CD86 costimulatory pathway blocker—bela-tacept, and the C5 binding monoclonal antibody—eculi-zumab.53 Finally, islet cell transplantation has continued to improve, and holds promise for the future. Ultimately the future of PTx is unpredictable, but the overall outlook is encouraging, and the long-term prospects are open to the imagination, to be filled with the possibilities of sur-gical innovation, pharmacogenetics, personalized medi-cine, stem cells, and cellular reprogramming.59
REFERENCES 1. Aanstoot H-J, Anderson BJ, Daneman D, et al. The global
burden of youth diabetes: perspectives and potential. Pediatr Diabetes. 2007;8(Suppl 8):1-44.
2. Kelly WD, Lillehei RC, Merkel FK, et al. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61(6):827-37.
3. The effect of intensive treatment of diabetes on the devel-opment and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329(14):977-86.
4. Margreiter C, Resch T, Oberhuber R, et al. Combined pancreas-kidney transplantation for patients With end-stage nephropathy caused by type-2 diabetes mellitus. Transplantation. 2013;95(8):1030-6.
5. Dunn TB. Life after pancreas transplantation: rever-sal of diabetic lesions. Curr Opin Organ Transplant. 2014;19(1):73-9.
6. Tyden G, Bolinder J, Solders G, et al. Improved survival in patients with insulin-dependent diabetes mellitus and end-stage diabetic nephropathy 10 years after combined pancreas and kidney transplantation. Transplantation. 1999;67(5):645-8.
7. Smets YF, Westendorp RG, van der Pijl JW, et al. Effect of simultaneous pancreas-kidney transplantation on mortal-ity of patients with type-1 diabetes mellitus and end-stage renal failure. Lancet. 1999;353(9168):1915-9.
8. Mohan P, Safi K, Little DM, et al. Improved patient survival in recipients of simultaneous pancreas-kidney transplant compared with kidney transplant alone in patients with type 1 diabetes mellitus and end-stage renal disease. Br J Surg. 2003;90(9):1137-41.
9. Tuttle-Newhall JE, Krishnan SM, Levy MF, et al. Organ Donation and Utilization in the United States: 1998-2007. Am J Transplant. 2009;9(4 Pt2):879-93.
10. Leichtman AB, Cohen D, Keith D, et al. Kidney and pan-creas transplantation in the United States, 1997–2006: The HRSA Breakthrough Collaboratives and the 58 DSA Challenge. Am J Transplant. 2008;8(4p2):946-57.
11. McCullough KP, Keith DS, Meyer KH, et al. Kidney and pancreas transplantation in the United States, 1998-2007: Access for Patients with Diabetes and End-Stage Renal Disease. Am J Transplant. 2009;9(4p2):894-906.
12. Stratta RJ, Bennett L. Pancreas underutilization according to united network for organ sharing data. Transplant Proc. 1998;30(2):264.
13. Wiseman AC, Wainright JL, Sleeman E, et al. An analysis of the lack of donor pancreas utilization from younger adult organ donors. Transplantation. 2010;90(5):475-80.
14. Axelrod DA, Sung RS, Meyer KH, et al. Systematic evalua-tion of pancreas allograft quality, outcomes and geographic variation in utilization. Am J Transplant. 2010;10(4):837-45.
15. Finger EB, Radosevich DM, Dunn TB, et al. A compos-ite risk model for predicting technical failure in pancreas transplantation. Am J Transplant. NIH Public Access; 2013;13(7):1840-9.
16. Hage FG, Smalheiser S, Zoghbi GJ, et al. Predictors of sur-vival in patients with end-stage renal disease evaluated for kidney transplantation. Am J Cardiol. 2007;100(6):1020-5.
17. Ablorsu E, Ghazanfar A, Mehra S, et al. Outcome of pancreas transplantation in recipients older than 50 years: a single-centre experience. Transplantation. 2008;86(11):1511-4.
18. Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Ann Surg. 2001;233(4):463.
19. Gruessner AC, Sutherland DE. Pancreas transplant out-comes for United States (US) and non-US cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR) as of June 2004. Clin Transplant. 2005;19(4):433-55.
20. Afaneh C, Rich BS, Aull MJ, et al. Pancreas transplantation: does age increase morbidity? J Transplant. 2011;2011(2):1-7.
21. Shah AP, Mangus RS, Powelson JA, et al. Impact of recipi-ent age on whole organ pancreas transplantation. Clin Transplant. 2012;27(1):E49-E55.
22. Gruessner AC. 2011 update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the International Pancreas Transplant Registry (IPTR). Rev Diabet Stud. 2011;8(1):6-16.
23. Petruzzo P, Lefrancois N, Berthillot C, et al. Impact of pancreatic venous drainage site on long-term patient and graft outcome in simultaneous pancreas-kidney transplan-tation. Clin Transplant. 2008;22(1):107-12.
24. Petruzzo P, Da Silva M, Feitosa LC, et al. Simultaneous pancreas-kidney transplantation: portal versus systemic venous drainage of the pancreas allografts. Clin Transplant. 2000;14(4 Pt 1):287-91.
25. Burke GW, Gruessner R, Dunn DL, et al. Conversion of whole pancreaticoduodenal transplants from bladder to enteric drainage for metabolic acidosis or dysuria. Transplant Proc. 1990;22(2):651-2.
26. Sollinger HW, Sasaki TM, D’Alessandro AM, et al. Indications for enteric conversion after pancreas transplantation with bladder drainage. Surgery. 1992;112(4):842-5. Discussion 845-6.
27. Fridell JA, Milgrom ML, Henson S, et al. Use of the end-to-end anastomotic circular stapler for creation of the duodenoenterostomy for enteric drainage of the pancreas allograft [corrected]. J Am Coll Surg. 2004;198(3):495-7.
Jayp
ee B
rothe
rs

634 Pancreas
28. Adamec M, Janousek L, Lipar K, et al. A prospective comparison of bladder versus enteric drainage in vas-cularized pancreas transplantation. Transplant Proc. 2004;36(4):1093-4.
29. Najarian JS, Sutherland DE, Matas AJ, et al. Human islet transplantation: a preliminary report. Transplant Proc. 1977;9(1):233-6.
30. Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplanta-tion in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343(4):230-8.
31. Boggi U, Vistoli F, Del Chiaro M, et al. A simplified tech-nique for the en bloc procurement of abdominal organs that is suitable for pancreas and small-bowel transplanta-tion. Surgery. 2004;135(6):629-41.
32. Moon JI, Nishida S, Butt F, et al. Multi-organ procurement and successful multi-center allocation using rapid en bloc technique from a controlled non-heart-beating donor. Transplantation. 2004;77(9):1476-7.
33. Englesbe MJ, Moyer A, Kim DY, et al. Early pancreas transplant outcomes with histidine-tryptophan-ketoglut-arate preservation: a multicenter study. Transplantation. 2006;82(1):136-9.
34. Alonso D, Dunn TB, Rigley T, et al. Increased pancrea-titis in allografts flushed with histidine-tryptophan-ketoglutarate solution: a cautionary tale. Am J Transplant. 2008;8(9):1942-5.
35. Stewart ZA, Cameron AM, Singer AL, et al. Histidine-tryptophan-ketoglutarate (HTK) is associated with reduced graft survival in pancreas transplantation. Am J Transplant. 2008;9(1):217-21.
36. Robertson RP, Davis C, Larsen J, et al. Pancreas and islet transplantation in type 1 diabetes. Diabetes Care. 2006;29(4):935.
37. Kasiske BL, Cangro CB, Hariharan S, et al. The evaluation of renal transplantation candidates: clinical practice guide-lines. Am J Transplant. 2001;1(Suppl 2):3-95.
38. Di Carlo V, Castoldi R, Cristallo M, et al. Techniques of pan-creas transplantation through the world: an IPITA Center survey. Transplant Proc. 1998;30(2):231-41.
39. Adamec M, Janousek L, Saudek F, et al. 100 pancreas transplantations with extraperitoneal graft placement. Ann Transplant. 2001;6(2):41-2.
40. Troppmann C, Gruessner AC, Benedetti E, et al. Vascular graft thrombosis after pancreatic transplantation: univari-ate and multivariate operative and nonoperative risk factor analysis. J Am Coll Surg. 1996;182(4):285-316.
41. Troppmann C, Gruessner AC, Dunn DL, et al. Surgical complications requiring early relaparotomy after pan-creas transplantation: a multivariate risk factor and eco-nomic impact analysis of the cyclosporine era. Ann Surg. 1998;227(2):255-68.
42. Gruessner AC, Sutherland DER. Pancreas transplant outcomes for United States (US) cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR). Clin Transplant. 2008;182(4):45-56.
43. Troppmann C, Gruessner AC, Benedetti E, et al. Vascular graft thrombosis after pancreatic transplantation: univari-ate and multivariate operative and nonoperative risk factor analysis. J Am Coll Surg. 1996;182(4):285-316.
44. Kandaswamy R, Humar A, Gruessner AC, et al. Vascular graft thrombosis after pancreas transplantation: compari-son of the FK 506 and cyclosporine eras. Transplant Proc. 1999;31(1-2):602-3.
45. Ciancio G, Julian JF, Fernandez L, et al. Successful surgi-cal salvage of pancreas allografts after complete venous thrombosis. Transplantation. 2000;70(1):126-31.
46. Stockland AH, Willingham DL, Paz-Fumagalli R, et al. Pancreas transplant venous thrombosis: role of endovas-cular interventions for graft salvage. Cardiovasc Intervent Radiol. 2009;32(2):279-83.
47. Maraschio MA, Kayler LK, Merion RM, et al. Successful surgical salvage of partial pancreatic allograft thrombosis. Transplant Proc. 2003;35(4):1491-3.
48. Hollinger EF, Powelson JA, Mangus RS, et al. Immediate retransplantation for pancreas allograft thrombosis. Am J Transplant. 2009;9(4):740-5.
49. Troppmann C. Complications after pancreas transplanta-tion. Curr Opin Organ Transplant. 2010;15(1):112-8.
50. Small RM, Shetzigovski I, Blachar A, et al. Redefining late acute graft pancreatitis: clinical presentation, radiologic findings, principles of management, and prognosis. Ann Surg. 2008;247(6):1058-63.
51. Nath DS, Gruessner A, Kandaswamy R, et al. Late anas-tomotic leaks in pancreas transplant recipients—clinical characteristics and predisposing factors. Clin Transplant. 2005;19(2):220-4.
52. West M, Gruessner AC, Metrakos P, et al. Conversion from bladder to enteric drainage after pancreaticoduodenal transplantations. Surgery. 1998;124(5):883-93.
53. Kimelman M, Brandacher G. Trends in immunosuppres-sion after pancreas transplantation: what is in the pipeline? Curr Opin Organ Transplant. 2013;18(1):76-82.
54. Atwell TD, Gorman B, Larson TS, et al. Pancreas transplants: experience with 232 percutaneous US-guided biopsy pro-cedures in 88 patients. Radiology. 2004;231(3):845-9.
55. de Kort H, Roufosse C, Bajema IM, et al. Pancreas trans-plantation, antibodies and rejection: where do we stand? Curr Opin Organ Transplant. 2013;18(3):337-44.
56. Owen RJT, Ryan EA, O’Kelly K, et al. Percutaneous tran-shepatic pancreatic islet cell transplantation in type 1 dia- betes mellitus: radiologic aspects. Radiology. 2003;229(1): 165-70.
57. Boggi U, Signori S, Vistoli F, et al. Laparoscopic robot-assisted pancreas transplantation: first world experience. Transplantation. 2012;93(2):201-6.
58. Tzvetanov I, D’Amico G, Bejarano-Pineda L, et al. Robotic-assisted pancreas transplantation: where are we today? Curr Opin Organ Transplant. 2014;19(1):80-2.
59. Gioviale MC, Bellavia M, Damiano G, et al. Beyond islet transplantation in diabetes cell therapy: from embryonic stem cells to transdifferentiation of adult cells. Transplant Proc. 2013;45(5):2019-24.
Jayp
ee B
rothe
rs