Evidence Based Pediatric Work Group€¦ · counseling, anticipatory guidance) Prevention of...
74
What Medical Professional is the Most Adequate for Primary Health Care to children and adolescents in Europe? A Systematic Review. Evidence Based Pediatric Work Group
Transcript of Evidence Based Pediatric Work Group€¦ · counseling, anticipatory guidance) Prevention of...

What Medical Professional is the Most Adequate for Primary Health Care to children and
adolescents in Europe? A Systematic Review.
Evidence Based Pediatric Work Group

THE IMPORTANCE OF PRIMARY CARE PEDIATRICS IN EUROPE:
From Concepts to Evidences
What Medical Profession is the Most
Adequate for Primary Health Care to
children and adolescents in Europe? A
Systematic Review.

3rd annual meeting of ECPCP (European Confederation of Primary
Care Pediatricians)
THE IMPORTANCE OF PRIMARY CARE PEDIATRICS IN EUROPE:
From Concepts to Evidences
Buñuel Álvarez JC, García Vera C, González Rodríguez P, Aparicio
Rodrigo M, Barroso Espadero D, Cortés Marina RB y cols. ¿Qué
profesional médico es el más adecuado para impartir
cuidados en salud a niños en Atención Primaria en
países desarrollados? Revisión sistemática. Rev Pediatr
Aten Primaria. 2010;12:s9-s72.
Published in Internet: 31/03/2010
22, June 2012

3rd annual meeting of ECPCP (European Confederation of Primary
Care Pediatricians)
THE IMPORTANCE OF PRIMARY CARE PEDIATRICS IN EUROPE:
From Concepts to Evidences
What medical professional is the most adequate, in developed
countries, to provide health care to children in primary care?
Systematic review Authors:
Buñuel Álvarez JC, García Vera C, González Rodríguez P, Aparicio Rodrigo
M, Barroso Espadero D, Cortés Marina RB, Cuervo Valdés JJ, Esparza Olcina
MJ, Juanes de Toledo B, Martín Muñoz P, Montón Álvarez JL, Perdikidis
Oliveri L, Ruiz-Canela Cáceres J
3rd annual meeting of ECPCP (European Confederation of Primary Care Pediatricians) / 22, June 2012

What medical professional is the most adequate to
provide health care to children in primary care in
developed countries? Systematic review
http://www.pap.es/files/1116-1430-pdf/sup_21_ingles.pdf
http://pap.es/FrontOffice/PAP/front/Articulos/Articulo/_IXus5l_LjPoo2J2KDAbNm8JCpYgBV
PcRGWJA9CjMLzZ8IMZsjMmv_g
Translated by: Domingo Barroso Espadero, Paz González Rodríguez, Ana
Benito Herreros, Pilar Aizpurua Galdeano, M.ª Jesús Esparza Olcina, Álvaro
Gimeno Díaz de Atauri y Leo Perdikidis Oliveri (members of the Grupo de Trabajo de
Pediatría Basada en la Evidencia (Evindece-based Pediatrics Work Group) that belongs to the
Asociación Española de Pediatría de Atención Primaria (AEPap/Primary Care Pediatrics
Spanish Association) and to the Asociación Española de Pediatría (AEP/Spanish Association
of Pediatrics).

3rd annual meeting of ECPCP (European Confederation of Primary Care
Pediatricians)
THE IMPORTANCE OF PRIMARY CARE PEDIATRICS IN EUROPE:
From Concepts to Evidences
- Our Systematic Review
JUSTIFICATION
http://www.pap.es/files/1116-1052-pdf/S9-S72_Que%20profesional%20medico%20es%20el%20mas%20adecuado.pdf

Justification for this Systematic Review:
In Spain, the presence of pediatricians in Primary Care is frequently and periodically questioned.
The increasing scarcity of pediatrics specialist available.
Total absence of studies having as their main objective the comparison, in Primary Care, of the clinical performance by pediatricians, working in Primary Care, versus the clinical practice by general practitioners (GP)/family doctors (FP), providing healthcare for children.

Answering the question, in developed countries, about
what medical professional is the most adequate to
provide health care to children in primary care.
Presentation of the results from a Systematic Review.
Our Systematic Review (SR)
Objectives & participants

Objectives & participants
The aim of this SR is to compare the clinical practice between PED and FP/GP in providing health care to children and adolescents at the primary health-care level.
PARTICIPANTS: PED, FP and GP who developed their clinical practice in PC and hospital emergency departments.

Purpose of the study: to look into the current
situation of the problem, by means of a SR of the
literature. Comparison of the clinical practice of primary care pediatricians to the
corresponding same clinical practice of FPs/GPs, regarding the following
9 CATEGORIES with aspects of the health care of children:
1. - Antibiotic (ATB)
prescription in respiratory tract
infections (RI) of probable viral
etiology.
2.- Otitis media treatment.
3.- Management of asthma in
children.
4.- Management of fever in
children.
5.- Management of children with
psychiatric disorders, like
depression, obsessive compulsive
disorder (OCD), attention deficit
hyperactivity disorder (ADHD)
6.- Immunizations: attitudes,
beliefs, coverage and implementation
of the official immunization schedules.
7.- Cardiovascular prevention.
8.- Other preventive activities.
9.- Use of diagnostic tests.

Bibliographic Search
Data Bases:
Meta Search Engines:
Databases:
Search Engines:
List of References of the articles
Without language restriction. Until December, 2008.

59 publications : 1 investigation with a before-after study design. 10 cohort studies (many of them retrospective historical cohort studies). 3 cases-control studies. 45 transversal studies (mainly cross-sectional studies) .

59 papers.
TYPES OF INVESTIGATIONS:
o Professional mail surveys
o Cross-sectional surveys to providers.
o Consult of population based databases.
o Consult of clinical register and medical records (computerized or not)
59 researches →173 COMPARISONS

22, June 2012

Statistical analysis
-Whenever possible, and based on results of every individual study, the
following estimators of effect were calculated (if the were not already
offered by the authors):
Relative risk (RR) for cohort studies.
OR in case control studies.
Prevalence ratio / Relative Prevalence (RP / PR) in cross sectional
studies.
With confidence intervals (CI 95%) for each estimator.
When if was possible, we calculated the global effect size resulting from combining the outcomes by means of using a global estimated combined estimator: the combined OR.

3rd Annual Meeting of ECPCP 3rd Annual Meeting of ECPCP / 20ème Congrès
National AFPA

Types of COMPARISONS included
o Medication prescription habits: •(Ex.: antibiotics, patterns of ATB prescription: number of prescriptions / first-line ATB medication versus second-line or non recommended high-cost antibiotics)
•prescriptions of non recommended medications (like decongestants) •selective serotonin reuptake inhibitors (SSRIs) antidepressants prescription…
oThe therapeutic-diagnostic attitudes for prevalent medical problems (Ex.: otitis media = OM)
o Attitude of professionals in relation to recommendations (adequateness of the doctors in following recommendations from clinical practice guidelines (CPGs) / degree of adherences to recommendations…)

Types of COMPARISONS included (II)
Thresholds for adequate referring of children to hospital or
other services.
Comparison of outcome on the control of prevalent
conditions ( asthma / ADDH)
Management of clinical acute presentation symptoms
in children (Ex.: fever: health outcomes, management of fever
without source; comparison of the degree of compliance with the
recommendations, laboratory test ordered…).
Attitudes and likelihood of incorporating the
recommendations from new GPCs (Ex.: for the diagnostic
assessment and the treatment of disorders like ADHD and for other
psychiatric disorders )

Types of COMPARISONS included (III)
Some comparisons were made in relation to a
reference standard (that could be: a CPG, an
expert consensus, or a laboratory method that
confirmed the diagnosis of the disease)
Some other compared directly the clinical
practice of PEDs and FPs / GPs without a standard
reference.

Types of COMPARISONS (Example)
Non-cardiovascular preventive activities.
Health education activities (recommendations,
counseling, anticipatory guidance)
Prevention of medical problems of unintentional
injuries or poisoning,
Teaching of self-care and self-diagnostic
activities (Ex.: testicular self-examination in
adolescents, etc.)
Use of diagnostic tests.

Types of COMPARISONS (Example II)
Cardiovascular prevention.
Diagnosis and prevention activities (health education activities
/ healthy habits promotion and counseling about diet and
exercise) on overweight-obesity, on toxic habits (tobacco and
alcohol consumption in adolescents, with counseling and active approach to
obtain the cessation of consumption).
Screening for identification of cardiovascular risk factors in
primary care: (Ex.: cholesterol routine screening in the
general population, screening for hypercholesterolemia in
at risk population); screening of arterial hypertension…
Initiation of treatment when indicated (Ex.:
hypercholesterolemia ),

COMPARISONS (by Categories / Example III ) Classification by categories of the types of outcome measures used:
Antibiotic prescription (ATB) in respiratory tract
infections (RI) of probable viral etiology.
Comparison of the likelihood to prescribe and the patterns of prescription of
antibiotic (ATB) for upper RI (URI) of probable viral etiology or non-infectious
diseases (acute wheezing episodes in children with asthma).
Comparison of the type of antibiotic, the prescription habits, the therapeutic-
diagnostic attitude for prevalent medical problems like persistent otitis media
with effusion (OME), otitis media (OM), or acute purulent rhinitis.
Adequateness of the doctors in following recommendations from clinical
practice guidelines (CPGs): on ATB treatment, likelihood to prescribe second-
line antibiotics or non recommended ATB for frequent infectious diseases like
AOM or acute pharyngitis, and for other infections of probable viral origin.

COMPARISONS (by Categories / Example IV) Classification by categories of the types of outcome measures used:
Management of asthma in children.
Comparison of the degree of adherence to the
recommendations of an asthma guideline: about
diagnosis (peak flow monitoring, use of spirometry for the
diagnosis, adequateness of the test ordered), or about
the suitability of the treatment and medications
prescribed. Comparison of outcome on the control of
asthma (visits to hospital emergency department…).

COMPARISONS (by Categories / Example V)
Management of children with psychiatric
disorders, like depression, obsessive compulsive
disorder (OCD), attention deficit hyperactivity
disorder (ADHD)
Comparison of the different attitudes and likelihood of
incorporating the recommendations from GPCs for the diagnostic assessment and the treatment of disorders like childhood depression, [selective serotonin reuptake inhibitors (SSRIs) antidepressants prescription / likely to use referrals to the specialist in mental health], also for the attention-deficit/hyperactivity disorder (ADHD) and for other psychiatric disorders.

Types of COMPARISONS included
(Example VI) Immunizations: Recommended vaccine and official
immunization schedules.
Comparison of the professionals in the likelihood to administer immunizations
and differences in attitudes and beliefs, knowledge and behaviors regarding
immunizations (perceptions of the safety of giving immunizations when not
specifically contraindicated, percentage of properly immunized children,
likelihood to routinely immunize at different type of visits, and likelihood to have
protocols for adolescent immunization).
Comparison of the degree of adoption of the official recommendation about
different current immunization recommendations and standards (adoption of the
universal immunization, identification of undervaccinated children,
systematically registering vaccinations and using immunization charts for
children, vaccination of high-risk children and others).

RESULTS

Use of antibiotics in upper airway
infections of probable viral origin (I)
Studies conducted by means of consulting
population-based databases
Data were combined from those studies which met the
following requirements:
1) information extracted from registers of databases for health care in which
diagnosis and treatment were indicated;
2) studies with design compatible with historical cohort.
3) studies located in primary care.
These criteria were met by seven studies.

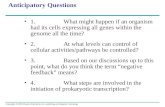
The combined odds ratio
was 1.48 (95 % CI: 1.11 to
1.98) indicating that FP/GP
have a 1.48 greater
probablity of perscribing
antibiotics for URI in
comparison to PED
(59,188 registers)
1) Studies conducted by means of consulting population-based databases.
2) Designs compatible with historical cohort studies
3) Located in primary care settings and/or hospital emergency settings.
RESULTS: Use of antibiotics in upper airway infections of
probable viral origin (meta analysis)

SUMMARY OF THE CATEGORY:
17 studies. 10 Population based databases ( 9 of them
retrospective cohort studies, 7 of them were combined)
The other 7 were cross-sectional studies (surveys)
Pulled together, the results about better adherence to standars of ATB prescription for URI favor: 34 comparisons (Best: PED 29)
17 studies: (Best performance: PED 15 / Similar 0/ FP-
GP 2)
RESULTS: ATB use for URI (individual, n = 17)

Ten studies analyzed the attitude of PED and
FP/GP in relation to diagnosis and treatment of
AOM (table 2). Seven were cross-sectional studies
and three were historical cohort studies.
10 studies:
•17 comparisons
(Best: PED 13 / similar 2 / FP-GP 2)
•10 studies:
(Best: PED 8 / Similar 1/ FP-GP 1)
RESULTS: AOM management (individual studies, n = 10)

Table 3. Studies that compare clinical practice of PED vs FP/GP in the management of asthma.
Author/year of
publication/country Design/quality Participants Comparison Main outcome Results
Results
favor:
Finkelstein JA, 2000. USA27
Cross-sectional,
survey to providers. Medium/Low
quality.
Sample of PEDs
and FPs from
three managed
care
organizations. A total of 407.
Adherence to
CPG for asthma. 1.- OR adjusted of clinical
essay with beta 2- agonists, X-
ray of sinus, thorax X-ray, skin
prick test or RAST test. To recommend daily peak flow
measurement. To use spirometry in diagnosis
(OR FP vs PED) 2.- To refer to an asthma
specialist according to CPG.
Clinical essay, X-ray, prick, RAST:
no significant difference. 0.30 (95% CI 0.10 – 0.50) 5.90 (95% CI 2.40 – 14.60) Measurement of four items:
compliance of FP with criteria for
referral to specialist was
appropriate in two and no
appropriate in the rest.
BOTH
Kozyrskyj AL, 2006.
(Canada)14 Retrospective
cohort study. Clinical registers
from MHSIP. Medium quality.
32,746 visits in
7791 asthmatic
children for
wheezing
episodes.
To examine the
determinants of
ATB use.
1.- OR FP vs PED for ATB
prescription within 2 days after
an ambulatory physician visit
for a wheezing episode in
children with asthma. 2.- ATB within 7 days of the
episode (RR)
2.10 (95% CI 1.82 – 2.53) 1.25 (95% CI 1.23 – 1.27)
PED
Sun HL, 2006. Taiwan 28
Retrospective
cohort study. Clinical registers. Medium quality
222,537
prescriptions in
children aged<
16 years.
Prescribing
patterns of anti-
asthma drugs.
Inhaled beta2-agonist
prescription. Inhaled corticosteroids
prescription. RR of prescribing only a drug
(no significance) Xanthine derivatives
prescription. Oral beta-2 agonist
prescription.
14.9% FP vs 3.1 % PED (p< 0.05) 5.6 FP vs 7.8% PED (p< 0.05) FP vs PED 0.76 (95% CI 0.74 – 0.77) 0.56 (95% CI 0.53 – 0.59) 1.50 (95% CI 1.45 – 1.56)
BOTH
RESULTS: ASTHMA management (individuals studies, n = 3)

Table 3 in the SR summarizes the
main characteristics of the three
reviewed studies.
3 studies.
1 cross-sectional study (survey) / 2 retrospective
cohort studies from clinical registers.
14 comparisons (Best: PED 6 / similar or not
significance 3 / FP-GP 5)
3 studies: (Best: PED 1 / Similar 2/ FP-GP 0)
RESULTS: ASTHMA management (individuals studies, n = 3)

Table 4 summarizes the main characteristics of the three reviewed
studies: Prospective cohort study (Leduc 1982)
Zerr et al.( published in 1999) / Cross-sectional survey to providers.
Boulis (vignettes / clinical scenarios) / Cross-sectional survey to providers.
SUMMARY:
8 comparisons (Best: PED 8 / no differences or no
significance 0 / FP-GP 0)
3 studies: (Best: PED 3 / Similar 0/ FP-GP 0)
RESULTS: FEVER management (individual studies, n = 3)

RESULTS: PSYCHIATRIC PROBLEMS (individual studies, n = 3)
Three selected studies(summarized in table 5) Cross-
Sectional survey to providers.
13 comparisons
(Best: PED 8 / similar or not significance 1 / FP-GP 4)
3 studies: (Best: PED 1 / Similar 2/ FP-GP 0)

RESULTS: INMUNIZATIONS (individual researches, n = 16)
The main characteristics of the selected studies are summarized in table 6 (in the SR)
This topic was reviewed in 16 studies: 14 cross-sectional descriptive studies and
two historical cohort studies.
32 comparisons
(Best: PED 31 / similar or not significance 1 / FP-GP 0)
16 studies: (Best: PED 15 / Similar 1/ FP-GP 0)

RESULTS: Cardiovascular risk factors (Studies; n: 10)
Ten studies All studies were cross-sectional design, using surveys, except one, which was
based on computerized register data. They are described in table 7 in more detail.
35 comparisons
(Best: PED 22 / similar or not significance 3 / FP-GP 10)
10 studies: (Best: PED 4 / Similar 3/ FP-GP 3)

RESULTS: other PREVENTIVE ACTIVITIES (studies, n = 6)
The delivery of other clinical preventive services, besides vaccination, as well as other
health education activities, was assessed in six studies. Additional information on these
services is shown in table 8.
6 studies. All of them, but one retrospective cohort study (Bocquect, 2005), were cross-
sectional studies (surveys)
17 comparisons
(Best: PED 12 / similar 2 / FP-GP 3)
6 studies: (Best: PED 4 / Similar 2/ FP-GP 0)

RESULTS: Use of Diagnostic Test (studies, n = 10)
Ten studies performed some kind of comparison in this field of the
clinical practice. Six had a cross-sectional design and four were cohort
studies (one prospective and three historical cohort studies). Further
details of these studies are provided in the table 9 of the SR.
20 comparisons (Best: PED 12 / no differences or no significance 4 / FP-GP 4)
10 studies: (Best: PED 6 / Similar 1/ FP-GP 4)

RESULTS: Use of Diagnostic tests (studies n = 10)

Summarized Results Results
• On average, FP/GP prescribed more ATB than PED in upper respiratory tract infections of probable viral etiology (OR: 1.4; confidence interval; 95% CI: 1.1-1.8).
• PEDs were more likely to adhere to clinical guidelines recommendations on febrile syndrome management (OR: 9; 95% CI: 3-25) and on ADHD (OR: 5; 95% CI: 3-11). Pediatricians showed, as well, more resolution capacity on other highly prevalent conditions in children and adolescents, such as asthma and AOM.
• PED showed higher vaccination coverage than FP/GP in all the studies assessing this result.

Summarized Results In CARDIOVASCULAR PREVENTION:
Interventions related to prevention of tobacco consumption
and to increasing physical exercise → better accomplished by
FP/GP. Obesity screening and treatment, hypercholesterolemia screening, and
blood pressure measurement → more frequently accomplished by PEDs.
• In OTHER PREVENTIVE ACTIVITIES: PEDs were more
active than GPs in counseling about preventing accidents,
intoxications and rickets.
FP/GP → more active in preventing toxic consumption.

Summarized Results III Use of a diagnostic test in primary care was better performed
by PEDs.
• Number of test ordered: PEDs ordered fewer chest X-rays
motivated by suspicion of pneumonia [Risk Difference (RD)
PED vs GP: -6.90; 95% CI: -8.80 to -4.90]; more blood test in
the young infant with fever (RD PED vs GP: 12.50; 95% CI:
10.00 to 14.30); and more diagnostic test for streptococcal
throat infection in sore throat (OR GP/FP vs PED: 0.46; 95%
CI: 0.32 to 0.66).
• Higher probability of finding an abnormal result, among the x-
ray ordered by PEDs than among those ordered by GPs (RR:
2.6; 95% CI: 1.1 to 6.6)

• Few analytical design studies ( no clinical trial, and a absence of prospective
studies)
• Studies based on clinical records were a minority (22)
• Mostly cross-sectional designs (self-administered questionnaires with low
response rates) . The percentages of responders usually not distributed equally
between PEDs and FPs/GPs: (PEDs responded more often)
• The general level of quality of the studies.
• In most of the studies the research was not designed for this comparison
(between the clinical practice of PEDs and FPs/GPs ) as theirs main outcome
variable.
• SR about an under investigated problem, in general terms, (not at all studied in
Spain)
• “Conflict of interest”
Limitations of the SR

• This one is the first review (with methodology of SR) that compares clinical practice between PEDs and FPs / GPs in PPC (Pediatric Primary Care)
• In most studies retrieved the objective of the researchers was not to determine what type of professional (PEDs or GP / FP) provided better clinical services to children and adolescents.
• Despite the heterogeneity inter-studies found, it could be seen a clear trend towards PED performing better...
Strengths of the SR

DISCUSSION (HIGHLIGHTED POINTS)

Conclusions:
The current situation could be summarized in the following highlighted
points:
• A better pattern of drug prescription (fewer overall prescriptions and
better adapted to the disease being treated. PEDs prescribe fewer ATBs
and performed better in other like psychotropic drugs)
• PEDs adhere better to the recommendations of clinical practice
guidelines (CPG). A higher degree of compliance with the
recommendations about diseases with high incidence and prevalence in
children and adolescents (RI, AOM, OME, fever, bronchial asthma, ADHD and overweight-obesity)

Discussion
1. A more rational use of diagnostic tests(e.g. chest x-ray, GABHS
testing or oropharyngeal culture) PEDs order fewer diagnostic
tests and “have a better aim when firing a shot” (more
pathologic findings and more positive results).
2. PEDs show lower percentages of referral to the specialized
attention level in diseases with high incidence and prevalence.
(higher resolution capacity of PEDs for diseases that pose a major
economic and care burden for health systems)

Discussion (INMUNIZATIONS) PEDs → more adequate implementation of vaccination (the main
primary prevention activity) recommendations and a better fulfilment
of the official immunization calendars.
PEDs took advantage more frequently of acute illness visits for
administering vaccines.
Had fewer assumptions about false hypothetical
contraindications for immunization.
Better at immunization information registering and at tracking
undervaccinated children and adolescents.
All the studies agreed in that, if PEDs are responsible for this
activity (Vaccination), it is carried out in a more complete way.

Discussion About psychiatric disorders, GPs were more
likely to prescribe SSRIs for all the diseases
studied. For some of them, these drugs are not
indicated at all (enuresis, ADHD).
A high degree of awareness of the
recommendations of a CPG about the ADHD,
and a better compliance with them by PEDs

Discussion
(Cardiovascular Risk preventive activities):
PEDs provide more preventive services and
more health counseling.
Cardiovascular Risk preventive activities: It could be concluded that FPs were
more likely to perform preventive activities in the absence of overweight and obesity
(diet, smoking and exercise counselling)
but PEDs were more likely to
Detect obesity/overweight and to solve them.
Order a cholesterol screening test when positive family history of
hypercholesterolemia was noticed.
To record smoking by a parent, as a problem for the child.

Discussion
Consequences of the high incidence of diseases in
children with a better pattern of medications
prescription by PEDs:
• Significant impact on the pharmaceutical budget
• Less generation of antimicrobial resistances
• Fewer iatrogenic factors.

3rd annual meeting of ECPCP
(European Confederation of
Primary Care Pediatricians)
THE IMPORTANCE OF
PRIMARY CARE
PEDIATRICS IN EUROPE:
From Concepts to
Evidences
- Our Systematic
Review
- Conclusions
22, June 2012

Main conclusion
The main conclusion is that, in
developed countries, primary health
care delivered by PEDs result in better
immunization practices and better
compliance with guidelines of frequent
diseases than those delivered by
GPs/FPs.

Main conclusion
Most of the results obtained were studied in outcome variables of great
importance for physicians, patients and health service managers, since
small variations in the provision of those care services can have enormous
impact fact in terms of health or otherwise.
No cost analysis study was identified in the conducted search, comparing
the clinical practice between PEDs and FPs / GPs. However, the assessed
data suggest that the health care provided by PEDs in PC could be cost
saving for those health systems which have PEDs in their primary care
settings.

Main conclusion:
With these findings in mind, it seems to be
recommendable to maintain the PED in the PC teams, and to strengthen their specific role as
the children’s first contact point with the health care system.
The Pediatric Primary Care (PPC) is an
essential public health issue. Therefore, the
professionals chosen to perform it out should be
those most qualified and trained to provide care
to children and adolescents.

Discussion
Several implications for further research can be drawn
from this review. There is a need for observational studies
(cohort or case control) in which differences in clinical
practice between PEDs and GPs should be compared in
specific areas such as drug prescription, institutional CPG
implementation, and the percentage of referrals to
emergency department or specialized attention.

In brief:
We, the PEDIATRICIANS are needed in the
Primary Care Health level.
• We should play a “more active role” in our self-promotion as
the doctors for the Pediatric Primary Care (PPC)…
…working close and in collaboration with (not against)
FPs/GPs.
• Measures should be taken, by all the actors involved in this issue, to
ensure that every child is assigned to a primary care general
pediatrician.
• There is a need of further prospective investigations that could help
to fill the gaps of the many under investigated and the many unsolved
points of the problem.


PAPERS PUBLISHED AFTER THE Systematic Review*
Synthesized summary of a preliminary (“at a glance”) overview (no rigorous
methodological analysis applied)
* What medical professional is the most adequate to provide health care to children in primary care in developed countries? Systematic review
Bibliographic Search terms and search strategic offered for consult (pdf) on demand:

Number of new articles found: 22 (Date of the Bibliographic Search: 22-May-2012)
31 [Initial Search +
List references]
22 [Valid]
17
+ 5 [Out of checking reference lists]
[Rejected] 9

NUMBER OF COMPARISIONS CONTAINED IN THE PAPERS
TOTAL NUMBER: 97
USEFUL COMPARISONS
91
Not useful
6

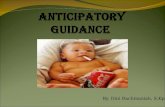
USEFUL COMPARISONS Distribution by type of professional that showed
the most adequate performance:
THE RESULTS FAVOR:
N [ type of PROFESSIONAL]
¿Defined most adequate medical
professional? Total
91
YES (78) 72 [PED]
6 [FP/GP]
NOT (13) 13[EQUAL]

COMPARISONS WIHT A MOST ADEQUATE MEDICAL PROFESSIONAL
(PERCENTAGES IN RELATION TO THE TOTAL NUMBER OF USEFUL COMPARISONS FOUND)

PERFORMANCE OF MEDICAL PROFESSIONAL (PCP) (Best adequateness expressed in percentages)

NUMBER OF COMPARISONS WITH A TYPE OF PROFESSIONAL SHOWING A MOST ADEQUATE
PERFORMANCE (% relate to the total number of useful comparisons)

The MOST ADEQUATE (by Categories*) CATEGORIES
N of papers (n of
comparisons)
COMPARISONS (best : FP / GP)
Number
COMPARISONS
(best: PED)
Number
COMPARISONS (Similar)
Number
MOST ADEQUATE
ALLERGIES 1 (16) 1 15 PED
OMA / URTI / PHARINGITIS 3 (6) 4 2 PED
Child Abuse 2 (16) 14 2 PED
ASTHMA 1 (12) 2 9 1 PED
Referral 2 ( 3) 2 1 PED
Immunizations 5 (8) 7 1 PED
PSYCHIATRIC Problems 2 (8) 2 4 2 PED
Preventive Activities (CARDIOV) 1 (2)
2 PED
Preventive Activities (Other**) 3 (8) 8 0 PED
Chronic diseases 1 (5) 1 3 1 PED
Antibiotics 1 (7) 4 3 PED
*All the comparisons have been incorporated to one, and only one Category, but, in fact, many of them could apply to more than one (Ex: Asthma + immunizations)
** Two of the papers of the Category “Preventive Activities” were about dental health.

LIST OF NEW PAPERS FOUND
(researches published after the bibliographic search for the SR) Search Date: 15, May 2012

1. Huang TT, Borowski LA, Liu B, Galuska DA, Ballard-Barbash R, Yanovski SZ, Olster DH, Atienza AA, Smith AW. Pediatricians' and family physicians' weight-related care of children in the U.S. Am J Prev Med. 2011 Jul;41(1):24-32.
PMID: 21665060 http://www.ncbi.nlm.nih.gov/pubmed/21665060 2. Paediatric asthma outpatient care by asthma nurse, paediatrician or general practitioner:
randomised controlled trial with two-year follow-up. Kuethe M, Vaessen-Verberne A, Mulder P, Bindels P, van Aalderen W. Prim Care Respir J. 2011 Mar;20(1):84-91. PMID: 21311842 Related citations (Reviewer remark: not clear if the “pediatricians” were PCP) 3. Cadieux G, Abrahamowicz M, Dauphinee D, Tamblyn R. Are physicians with better clinical
skills on licensing examinations less likely to prescribe antibiotics for viral respiratory infections in ambulatory care settings? Med Care. 2011 Feb;49(2):156-65. Erratum in: Med Care. 2011 May;49(5):527-8.
PMID: 21206293 http://www.ncbi.nlm.nih.gov/pubmed/21206293 4. Abbas S, Ihle P, Heymans L, Küpper-Nybelen J, Schubert I. Differences in antibiotic prescribing
between general practitioners and pediatricians in Hesse, Germany. Dtsch Med Wochenschr. 2010 Sep;135(37):1792-7. Epub 2010 Sep 7. German.
PMID: 20824600 http://www.ncbi.nlm.nih.gov/pubmed/20824600

5. Wortberg S, Walter D.Recallsystems in primary care practices to increase vaccination rates against seasonal influenza. Dtsch Med Wochenschr. 2010 Jun;135(22):1113-7. Epub 2010 May 7. German.
PMID: 20455199 Related citations http://www.ncbi.nlm.nih.gov/pubmed/20455199 6. Otto O, Peleg R, Press Y. Streptococcal pharyngitis among children: comparison of attitudes
between family physicians and pediatricians. Harefuah. 2009 Aug;148(8):511-4, 573. [Article in Hebrew] http://www.ncbi.nlm.nih.gov/pubmed/19899252 7. The choking game: physician perspectives. McClave JL, Russell PJ, Lyren A, O'Riordan MA, Bass NE. Pediatrics. 2010 Jan;125(1):82-7. Epub 2009 Dec 14. PMID: 20008424 [PubMed - indexed for MEDLINE] Free Article ARTICLE 9 Related citations 8. Gundogdu Z, Gundogdu O.Parental attitudes and varicella vaccine in Kocaeli, Turkey. Prev
Med. 2011 Mar-Apr;52(3-4):278-80. Epub 2011 Jan 26. PMID:21277890 Parental attitudes and varicella vaccine in Kocaeli, Turkey. [PubMed - indexed for MEDLINE]

9. Food allergy knowledge, attitudes, and beliefs of primary care physicians.
Gupta RS, Springston EE, Kim JS, Smith B, Pongracic JA, Wang X, Holl J. Pediatrics. 2010 Jan;125(1):126-32. Epub 2009 Dec 7. PMID: 19969619 10. Barriers to vitamin D supplementation among military physicians. Sherman EM, Svec RV. Mil Med. 2009 Mar;174(3):302-7. PMID: 19354096 11. Discussion of maternal stress during pediatric primary care visits. Brown JD, Wissow LS. Ambul Pediatr. 2008 Nov-Dec;8(6):368-74. Epub 2008 Oct 25. PMID: 19084786 [PubMed - indexed for MEDLINE] 12. Primary care physician perspectives on reimbursement for childhood immunizations. Freed GL, Cowan AE, Clark SJ. Pediatrics. 2008 Dec;122(6):1319-24. PMID: 19047252 13. Physician perspectives regarding annual influenza vaccination among children with asthma. Dombkowski KJ, Leung SW, Clark SJ. Ambul Pediatr. 2008 Sep-Oct;8(5):294-9. Epub 2008 Aug 20. PMID: 18922502 Related citations 14. Comfort level of pediatricians and family medicine physicians diagnosing and treating child and adolescent psychiatric
disorders. Fremont WP, Nastasi R, Newman N, Roizen NJ. Int J Psychiatry Med. 2008;38(2):153-68. PMID: 18724567 [PubMed - indexed for MEDLINE] ARTICLE 16

15. Okumura MJ, Heisler M, Davis MM, Cabana MD, Demonner S, Kerr EA. Comfort of general internists and general pediatricians in providing care for young adults with chronic illnesses of childhood. J Gen Intern Med. 2008 Oct;23(10):1621-7. Epub 2008 Jul 26.
PMID: 18661191
http://www.ncbi.nlm.nih.gov/pubmed/18661191
16. Chatterjee JS, Mahmoud M, Karthikeyan S, Duncan C, Dover MS, Nishikawa H. Referral pattern and surgical outcome of sagittal synostosis. J Plast Reconstr Aesthet Surg. 2009 Feb;62(2):211-5. Epub 2008 Mar 10.
PMID: 18329351
Related citations
17. Feder HM Jr, Collins M. How Connecticut primary care physicians view treatments for streptococcal and nonstreptococcal pharyngitis. Clin Ther. 2008 Jan;30(1):158-63.
http://www.ncbi.nlm.nih.gov/pubmed/18343252
18. Training pediatric health care providers in prevention of dental decay: results from a randomized controlled trial.
Slade GD, Rozier RG, Zeldin LP, Margolis PA.
BMC Health Serv Res. 2007 Nov 2;7:176.
PMID: 17980021
Related citations

18. [Pediatric Otolaryngology at the Public Health System of a city in Southeastern Brazil].
Guerra AF, Gonçalves DU, Werneck Côrtes Mda C, Alves CR, Lima TM.
Rev Saude Publica. 2007 Oct;41(5):719-25. Portuguese.
PMID: 17923892 [PubMed - indexed for MEDLINE]
20 [Vaccination practices following the end of compulsory BCG vaccination. A cross-sectional survey of general practitioners and pediatricians].Wattrelot P, Brion JP, Labarère J, Billette de Villemeur A, Girard-Blanc MF, Stahl JP, Brambilla C.Arch Pediatr. 2010 Feb;17(2):118-24. Epub 2009 Dec 2. French. PMID: 19959346
21 Awareness and knowledge of child abuse amongst physicians - a descriptive study by a sample of rural Austria.Kraus C, Jandl-Jager E.Wien Klin Wochenschr. 2011 Jun;123(11-12):340-9. Epub 2011 May 4.PMID: 21538034.
22. - Starling SP, Heisler KW, Paulson JF, Youmans E. Child abuse training and knowledge: a national survey of emergency medicine, family medicine, and pediatric residents and program directors. Pediatrics. 2009 Apr;123(4):e595-602.
Child abuse training and knowledge: a national survey of emergency medicine, family medicine, and pediatric residents and program directors.

More details & Specifications of the papers found after the publication of the SR. available on demand (unpublished data / May, 2012)