
evidence-based medicine for EMS protocols Annual Meeting Handouts/2014 MD… · evidence-based...
38
Andrew Travers, MD, MSc, FRCPC [email protected] 1 evidence-based medicine for EMS protocols Andrew Travers MD MSc FRCPC Provincial Medical Director Emergency Health Services Halifax, Nova Scotia Conflict of Interest • Academic – ILCOR • Financial – None [email protected] www.gov.ns.ca/health/ehs
Transcript of evidence-based medicine for EMS protocols Annual Meeting Handouts/2014 MD… · evidence-based...
Andrew Travers, MD, MSc, FRCPC [email protected]
1
evidence-based medicinefor EMS protocols
Andrew Travers MD MSc FRCPCProvincial Medical Director
Emergency Health ServicesHalifax, Nova Scotia
Conflict of Interest
• Academic– ILCOR
• Financial– None
www.gov.ns.ca/health/ehs
Andrew Travers, MD, MSc, FRCPC [email protected]
2
“The National Association of EMS Physicians (NAEMSP) recently entered into a cooperative agreement with the National Highway Traffic Safety Administration (NHTSA) to develop a national strategy for the promotion and implementation of prehospital evidence-based guidelines.”
Christian Martin-Gill, MD, MPH
Assistant Professor of Emergency Medicine
University of Pittsburgh School of Medicine
Evidence BasedDecision Making
Decision BasedEvidence Making
Evidence Based Medicine
2.1.1.2.1Evidence guided development of medical care protocols
3.1.Evidence-based Practice
Andrew Travers, MD, MSc, FRCPC [email protected]
3
NAEMSP 2014: Tucson
NB
A
NF
L
Asl
eep
Com
fy C
hair
Che
ckin
g E
mai
ls
Che
ckin
g E
mai
ls
Che
ckin
g E
mai
ls
..beer..
OMG! Too much caffeine!
Culture
ClinicalParamedic
AdministrativeParamedic
AcademicParamedic
Academic Centre
Regulator Contractor
Evidence-BasedPractice Culture
Andrew Travers, MD, MSc, FRCPC [email protected]
4
57 EMS Professionals
‘Living Document’
Academic Emergency Medicine 2009. 16(7): 668-673.
Andrew Travers, MD, MSc, FRCPC [email protected]
5
#10Cone and McManusTop 10 EMS Research Articles of 2009NAEMSP 2010
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
iPhone 10The Tallest iPhone Yet
Andrew Travers, MD, MSc, FRCPC [email protected]
6
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
Evidence based medicine is the judicious and conscientious use of the best evidence from research, combined with clinical experience, and applied to patient problems.
Andrew Travers, MD, MSc, FRCPC [email protected]
7
Evidence based medicine is the judicious and conscientious use of the best evidence from research, combined with clinical experience, and applied to patient problems.
Evidence based medicine is the judicious and conscientious use of the best evidence from research, combined with clinical experience, and applied to patient problems.
Evidence based medicine is the judicious and conscientious use of the best evidence from research, combined with clinical experience, and applied to patient problems.

Andrew Travers, MD, MSc, FRCPC [email protected]
8
Evidence based medicine is the judicious and conscientious use of the best evidence from research, combined with clinical experience, and applied to patient problems.
the EBM cyclehow to formquestionshow to
evaluateperformance
how toapply
clinicallyhow to
criticallyappraise
how tosearch
Evidence-Based Practice
Practice-Based Evidence
Andrew Travers, MD, MSc, FRCPC [email protected]
9
Evidence-Based MedicineCriticisms
Some people use EBM the way a drunk uses a lamppost – for support rather than illumination.
What on *&^%$# earth is ‘knowledge translation’?
http://www.cihr-irsc.gc.ca/e/29418.html
Knowledge translation is a dynamic and iterative process that includes synthesis, dissemination, exchange and ethically sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the health care system.
Andrew Travers, MD, MSc, FRCPC [email protected]
11
Operational
Cultural
Published Evidence
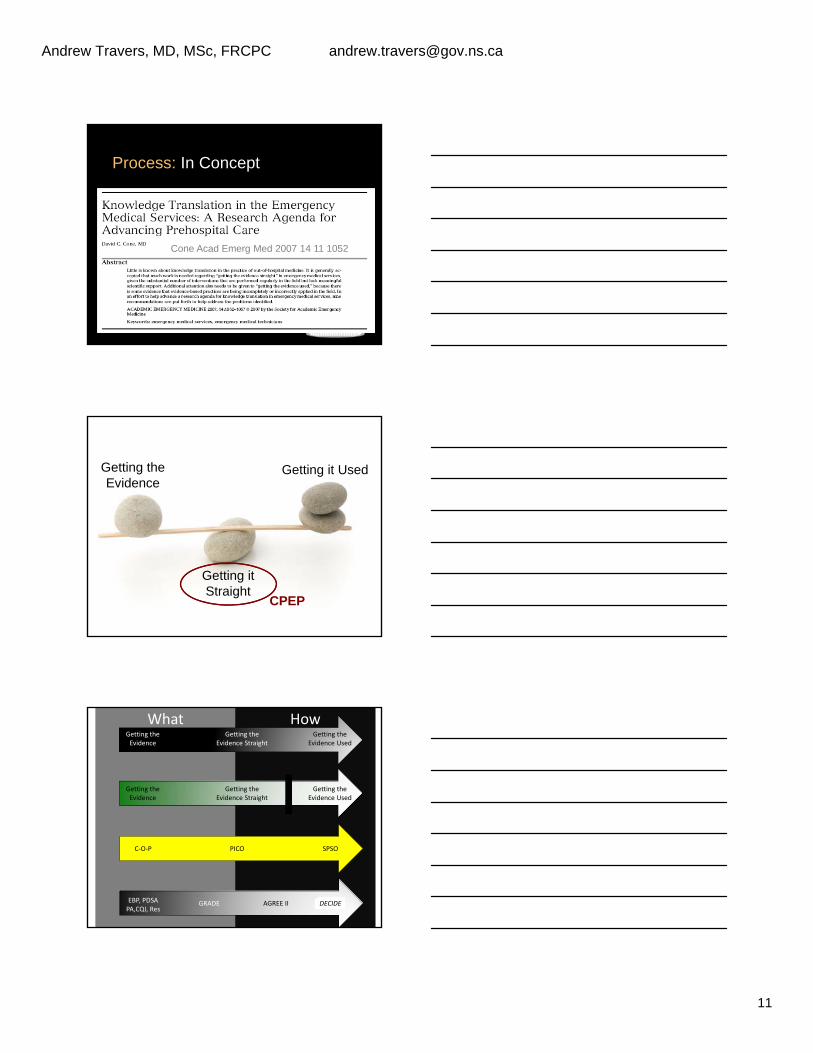
Process: In Concept
Appraisal
FormalSearch
Topic Selection
EvaluatePerformance
OperationalizationDissemination
Protocol
Evidence
GettingThe
EvidenceStraight
GettingThe
EvidenceUsed
Cone Acad Emerg Med 2007 14 11 1052
Getting theEvidence
Getting it Used
Getting itStraight
CPEP
WhatWhat HowHowGetting theEvidence
Getting theEvidence Straight
Getting theEvidence Used
Getting theEvidence
Getting theEvidence Straight
Getting theEvidence Used
C‐O‐P PICO SPSO
EBP, PDSAPA,CQI, Res
AGREE II DECIDEGRADE
Andrew Travers, MD, MSc, FRCPC [email protected]
12
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
twd
Andrew Travers, MD, MSc, FRCPC [email protected]
13
We would like to speak to you about a research study….
Andrew Travers, MD, MSc, FRCPC [email protected]
14
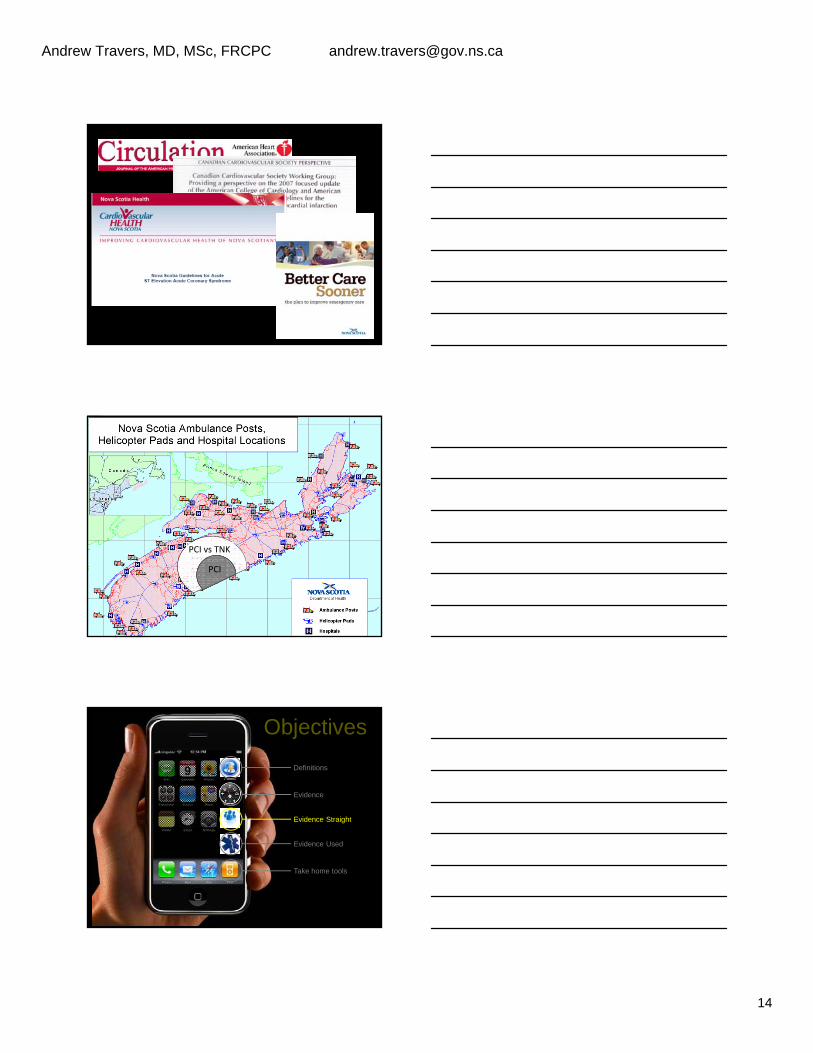
DOI: 10.1161/CIRCULATIONAHA.110.971028 2010;122;S787-S817 Circulation
Demetris Yannopoulos Egan, Chris Ghaemmaghami, Venu Menon, Brian J. O'Neil, Andrew H. Travers and Robert E. O'Connor, William Brady, Steven C. Brooks, Deborah Diercks, Jonathan
CareGuidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
Part 10: Acute Coronary Syndromes: 2010 American Heart Association
PCI vs TNK
PCI
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
Andrew Travers, MD, MSc, FRCPC [email protected]
15
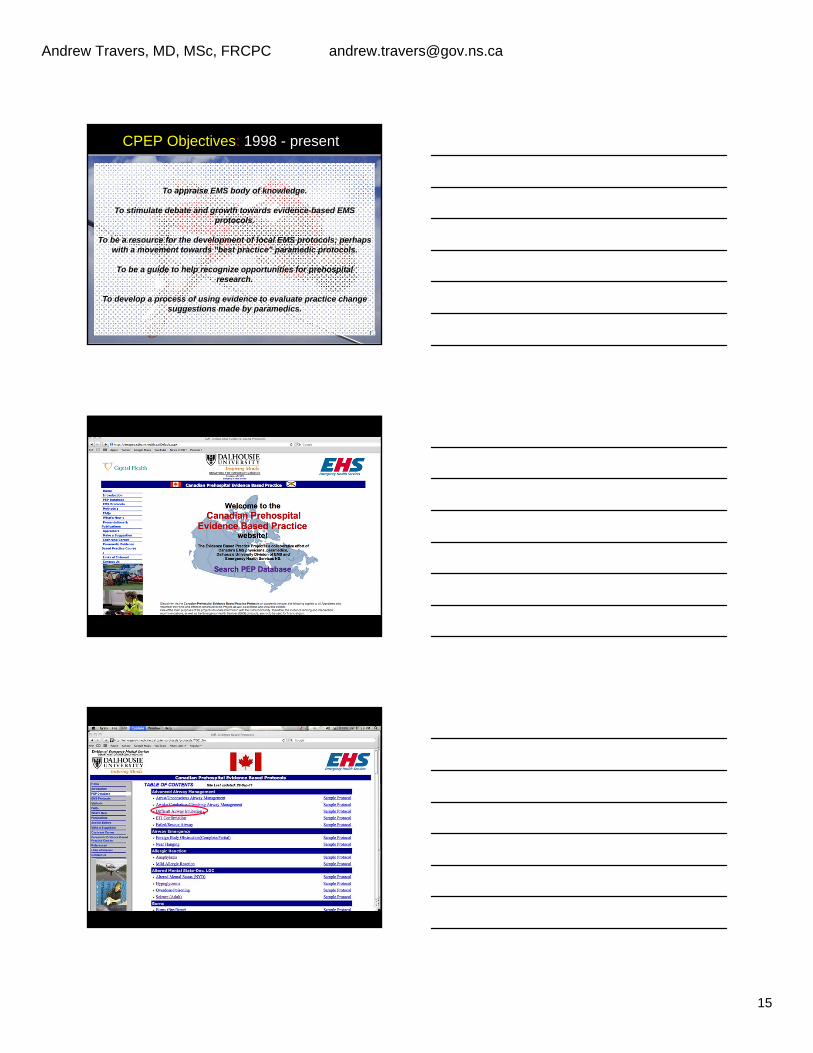
CPEP Objectives: 1998 - present
To appraise EMS body of knowledge.
To stimulate debate and growth towards evidence-based EMS protocols.
To be a resource for the development of local EMS protocols; perhaps with a movement towards "best practice" paramedic protocols.
To be a guide to help recognize opportunities for prehospital research.
To develop a process of using evidence to evaluate practice change suggestions made by paramedics.
Andrew Travers, MD, MSc, FRCPC [email protected]
16
• BC Ambulance Service
• Alberta Emergency Health Services
• BC Ambulance Service
• NS Emergency Health Services
Andrew Travers, MD, MSc, FRCPC [email protected]
17
• BC Ambulance Service
• Alberta Emergency Health Services
• BC Ambulance Service
• NS Emergency Health Services
Andrew Travers, MD, MSc, FRCPC [email protected]
18
• BC Ambulance Service
• Alberta Emergency Health Services
• BC Ambulance Service
• NS Emergency Health Services
Andrew Travers, MD, MSc, FRCPC [email protected]
21
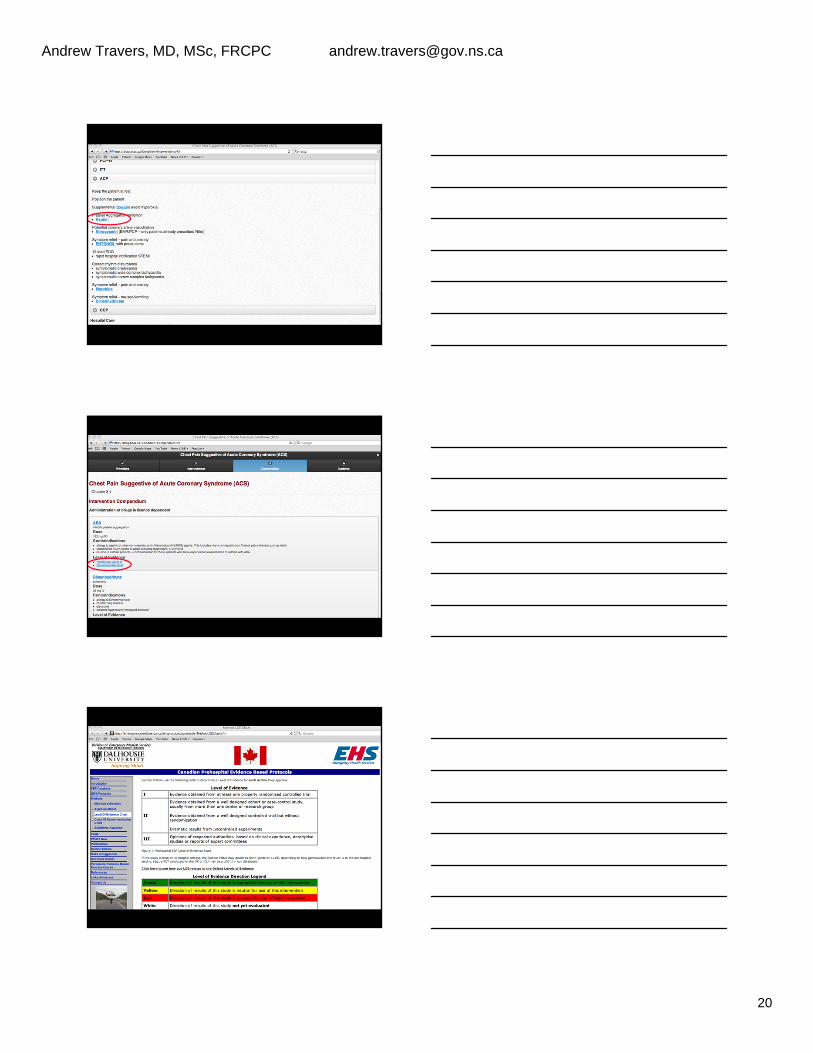
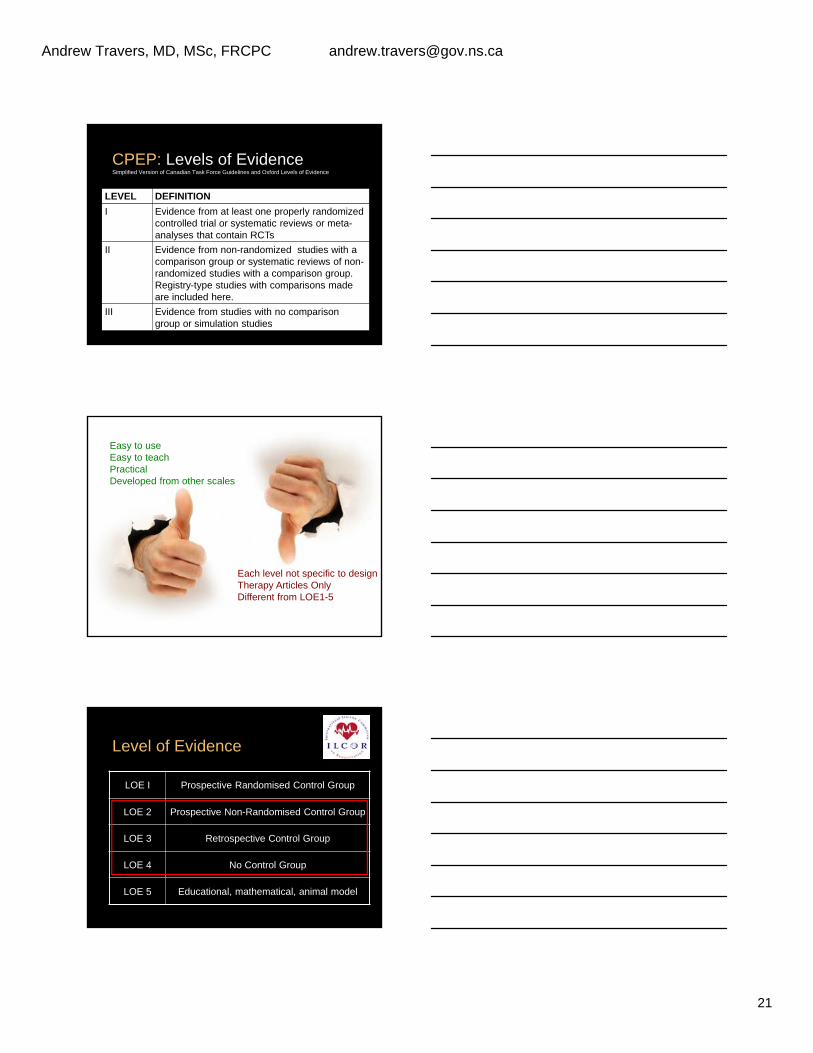
CPEP: Levels of EvidenceSimplified Version of Canadian Task Force Guidelines and Oxford Levels of Evidence
LEVEL DEFINITION
I Evidence from at least one properly randomized controlled trial or systematic reviews or meta-analyses that contain RCTs
II Evidence from non-randomized studies with a comparison group or systematic reviews of non-randomized studies with a comparison group. Registry-type studies with comparisons made are included here.
III Evidence from studies with no comparison group or simulation studies
Easy to useEasy to teachPracticalDeveloped from other scales
Each level not specific to designTherapy Articles OnlyDifferent from LOE1-5
Level of Evidence
LOE I Prospective Randomised Control Group
LOE 2 Prospective Non-Randomised Control Group
LOE 3 Retrospective Control Group
LOE 4 No Control Group
LOE 5 Educational, mathematical, animal model
Andrew Travers, MD, MSc, FRCPC [email protected]
22
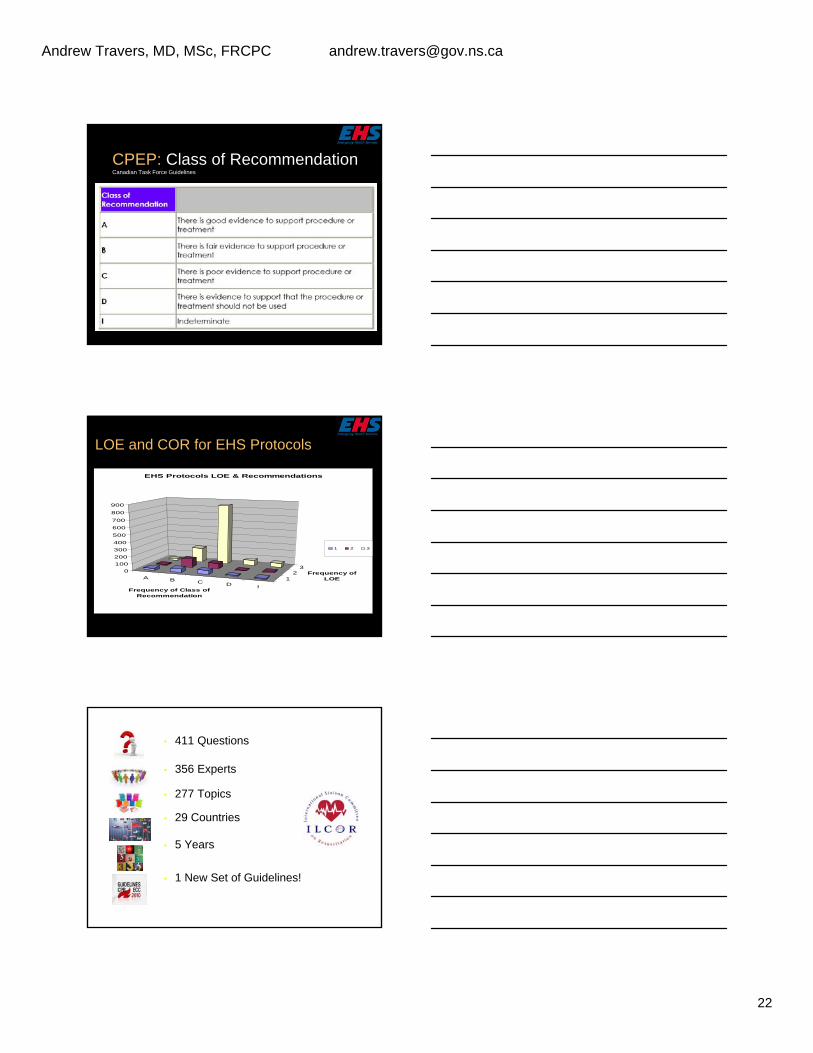
CPEP: Class of RecommendationCanadian Task Force Guidelines
LOE and COR for EHS Protocols
A B C D I
12
30
100
200
300
400
500
600
700
800
900
Frequency of Class of Recommendation
Frequency of LOE
EHS Protocols LOE & Recommendations
1 2 3
• 411 Questions
• 356 Experts
• 277 Topics
• 29 Countries
• 5 Years
• 1 New Set of Guidelines!
Andrew Travers, MD, MSc, FRCPC [email protected]
23
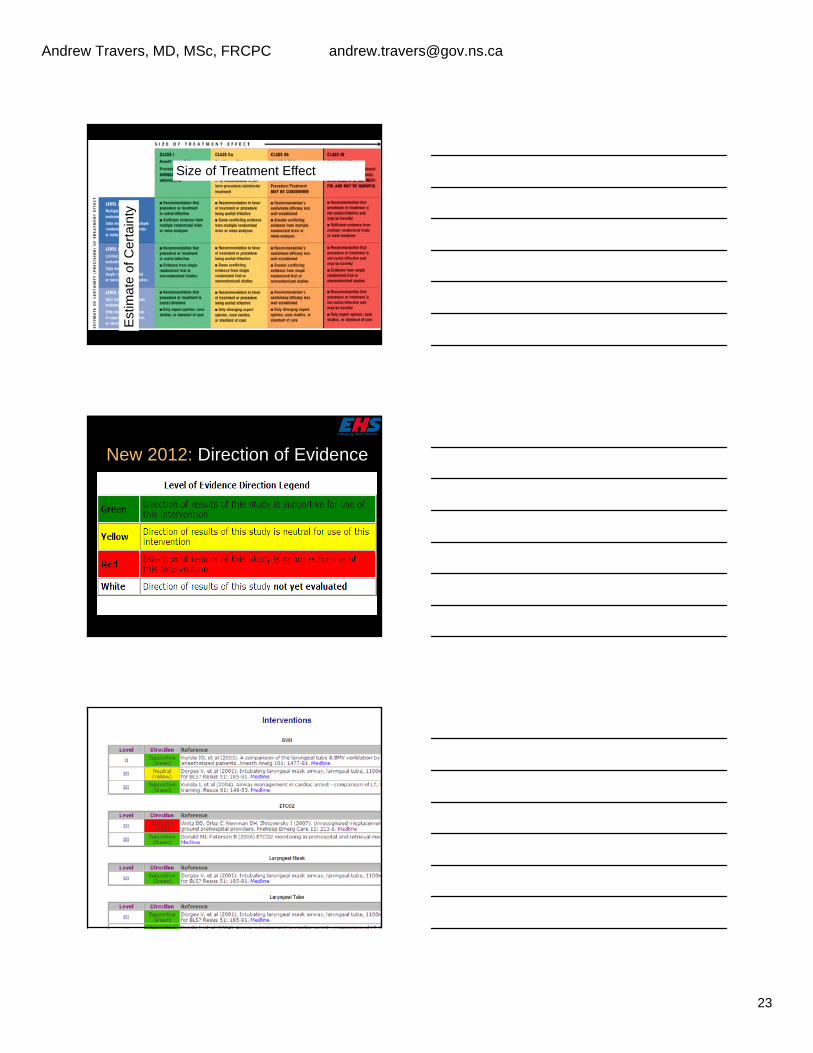
Size of Treatment Effect
Est
imat
e of
Cer
tain
ty
New 2012: Direction of Evidence
Andrew Travers, MD, MSc, FRCPC [email protected]
24
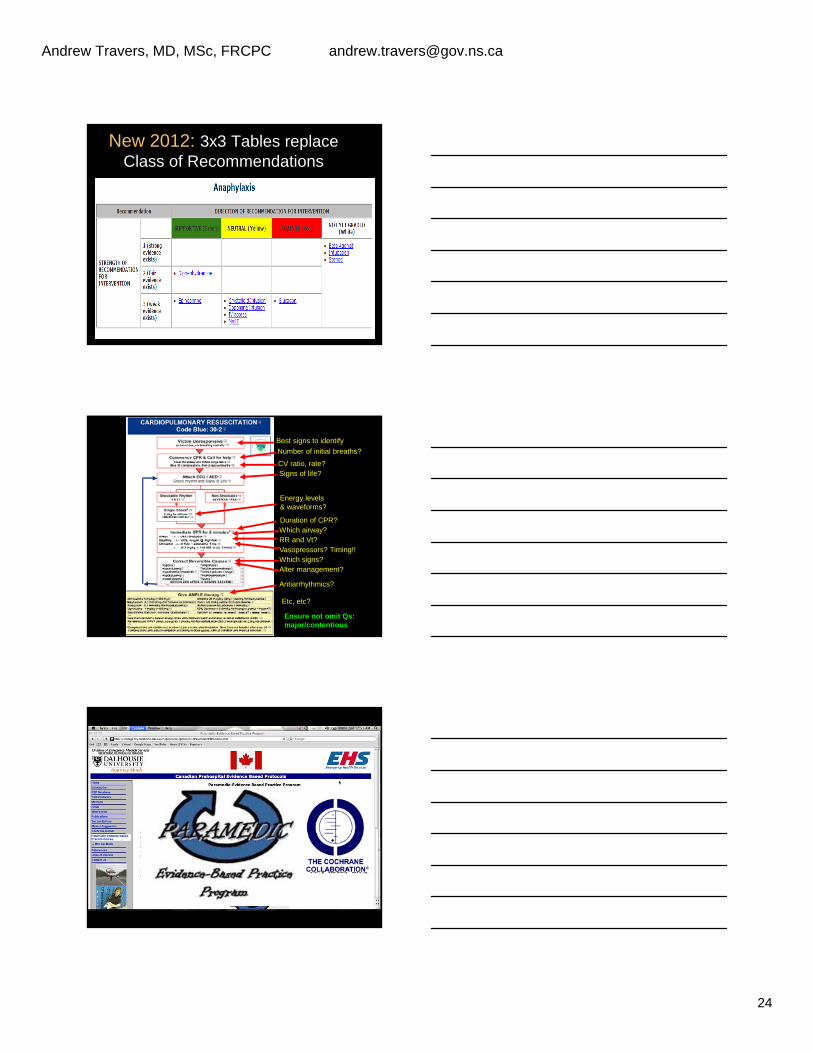
New 2012: 3x3 Tables replace Class of Recommendations
Best signs to identify
Number of initial breaths?
CV ratio, rate?Signs of life?
Energy levels & waveforms?
Duration of CPR?Which airway?RR and Vt?Vasopressors? Timing!!Which signs?Alter management?
Antiarrhythmics?
Etc, etc?
Ensure not omit Qs:major/contentious
Andrew Travers, MD, MSc, FRCPC [email protected]
25
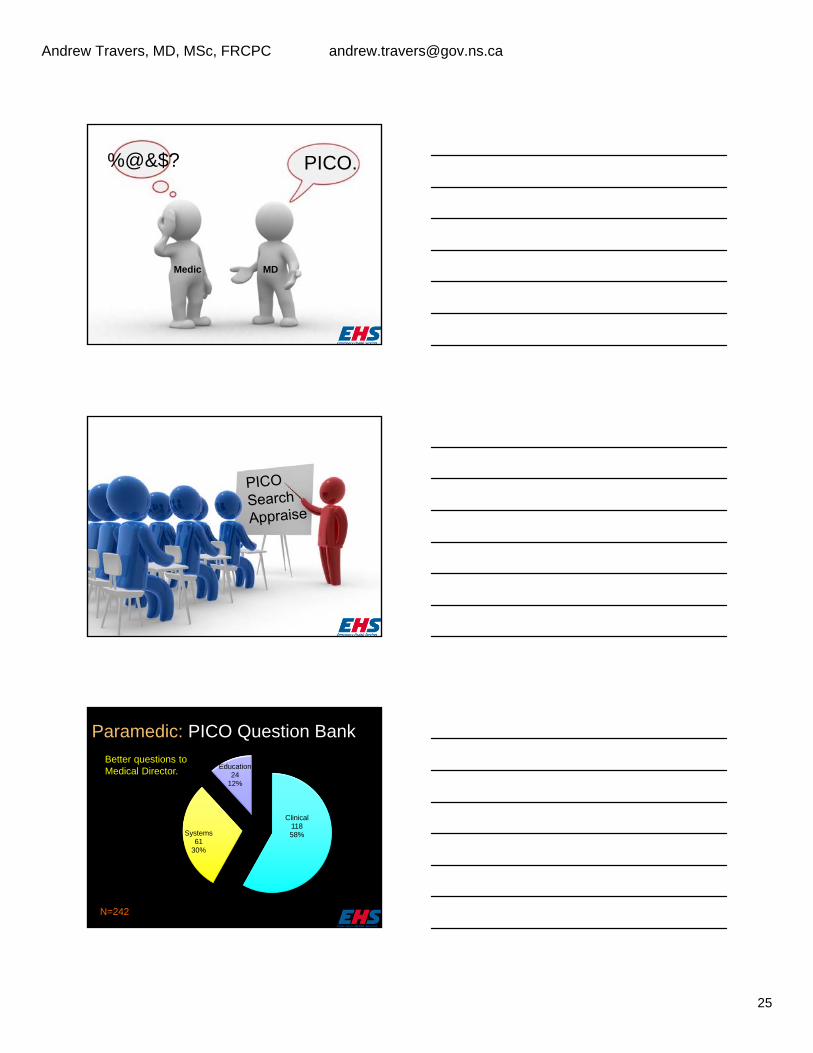
%@&$? PICO.
Medic MD
Paramedic: PICO Question Bank
Clinical11858%Systems
6130%
Education24
12%
N=242
Better questions toMedical Director.
Andrew Travers, MD, MSc, FRCPC [email protected]
26
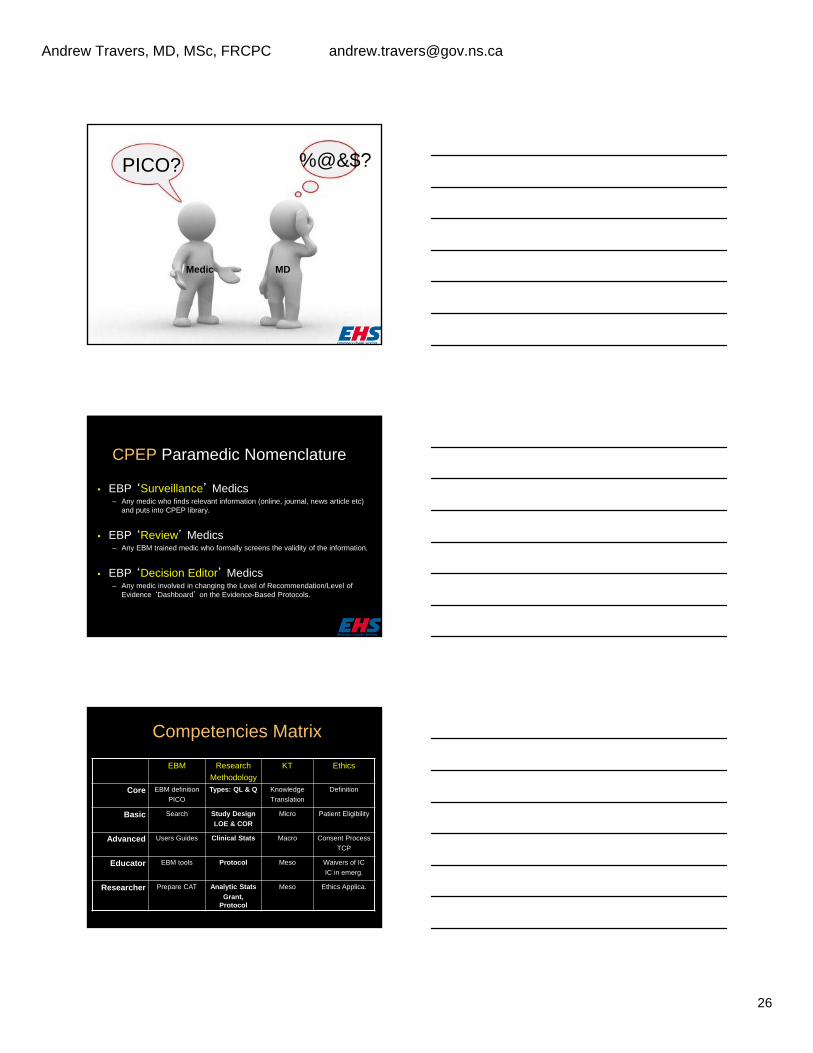
Medic MD
%@&$?PICO?
CPEP Paramedic Nomenclature
• EBP ‘Surveillance’ Medics– Any medic who finds relevant information (online, journal, news article etc)
and puts into CPEP library.
• EBP ‘Review’ Medics– Any EBM trained medic who formally screens the validity of the information.
• EBP ‘Decision Editor’ Medics– Any medic involved in changing the Level of Recommendation/Level of
Evidence ‘Dashboard’ on the Evidence-Based Protocols.
Competencies Matrix
EBM Research
Methodology
KT Ethics
Core EBM definition
PICO
Types: QL & Q Knowledge
Translation
Definition
Basic Search Study Design
LOE & COR
Micro Patient Eligibility
Advanced Users Guides Clinical Stats Macro Consent Process
TCP
Educator EBM tools Protocol Meso Waivers of IC
IC in emerg.
Researcher Prepare CAT Analytic Stats
Grant, Protocol
Meso Ethics Applica.
Andrew Travers, MD, MSc, FRCPC [email protected]
27
CAT: Critically Appraised Topic
The EBM Cycle & Paramedic Practice
Current Practice/Paramedic Protocols
EvidenceAppraisal
Re-evaluate Practice/Protocol
Question Practice/Develop Research
Question
Design & ConductStudy = Results
Jan Jensen ACP
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
Andrew Travers, MD, MSc, FRCPC [email protected]
28
Assessment- crackles
- increased JVP- hx CHF, MI
- acuity
Mild /Moderate- able to speak
sentences- crackles base only
- O2 sat >92%
Severe- resp. distress
- crackles throughout- O2 sat <92%
morphine2.5-5mg IV
O2 100% BVM
furosemide IV(only if currently
on a diuretic)
see advancedairway
management
protocols*
nitro S/Lrepeat q5min
prn
salbutamol**
Deteriorating(see near death)
Deteriorating(see severe)
Transport
Near Death- decreased LOC
-cyanosis- dropping sats
- ineffective resp.drive
Yes
No
nitro S/Lrepeat q5min
prn
Yes
No
ICPACPCCP
ACPCCP
ACPCCP
ICPACPCCP
PCPICPACPCCP
PCPICPACPCCP
PCPICPACPCCP
Department of Health
Protocol: Pulmonary Edema (CHF) PDN: 6282.05 Subject: Respiratory Distress (SOB) Page 1
IV saline lockICPACPCCP
PCPICPACPCCP
nitro S/Lrepeat q5min
prn
furosemide IV(only if currently
on a diuretic)
ACPCCP
ACPCCP
morphine2.5-5mg IV
salbutamol**
PCPICPACPCCP
ACPCCP
*ACP, CCP may give PEEP at 5-10cmH2O**only if wheezes present
Last Updated: March 26, 2004
O2 to maintainsats >92%
PCPICPACPCCP
High flow withreservoir
PCPICPACPCCP
Andrew Travers, MD, MSc, FRCPC [email protected]
29
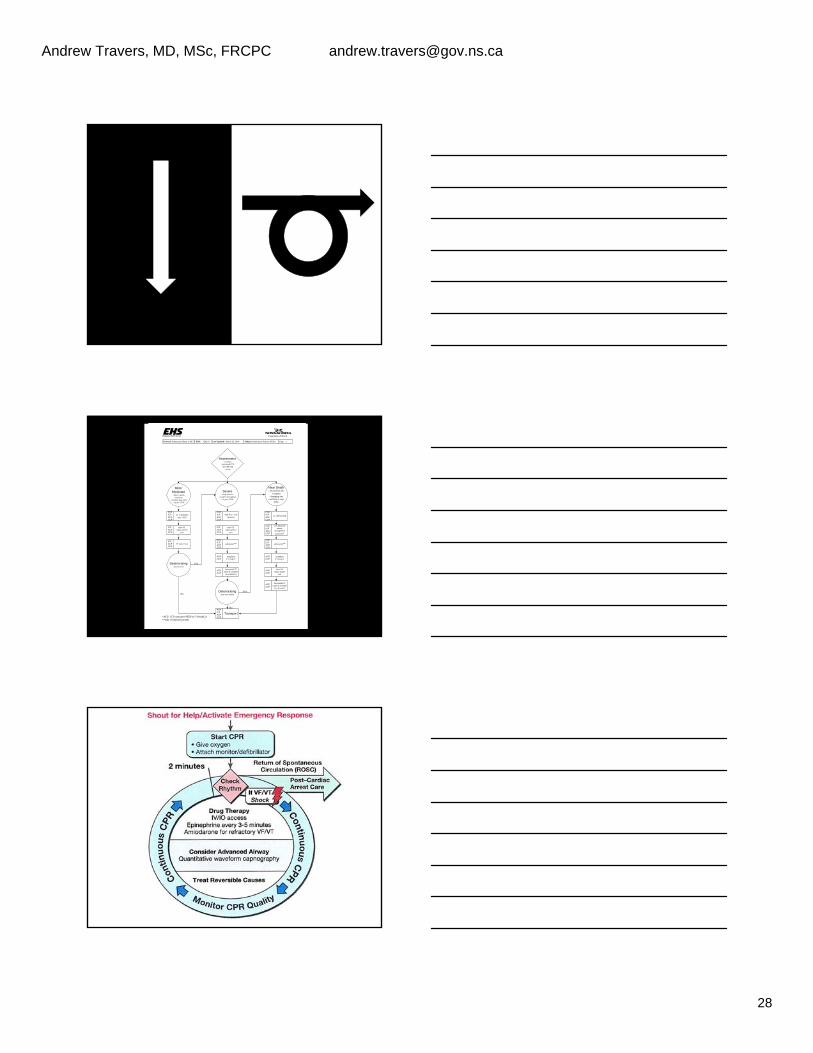
Out of-Hospital Universal Algorithm
EHS has made every effort to ensure that the information, tables, drawings and diagrams contained in the Clinical Practice Guidelines issued XXX is accurate at the time of publication. However, the EHS guidance is advisory and has been developed to assist healthcare professionals, together with patients, to m ake decisionincluding treatments. It is intended to support the decision making process and is not a substitute for sound clinical judgment. Guidelines cannot always contain all the information necessary for determining appropriate care and cannot address all individual situations; therefore individuals using these guidelines must ensure they have the appropriate knowledge and skil ls to enable appropriate interpretation.
INTRODUCTION CPR is a series of life-saving actions that improve the chances of survival. Although, all components of CPR are important (e.g. airway management, ventilations, defibrillation), the provision of quality chest compressions are the most important intervention. Integrating the critical components of CPR requires the prehospital clinician to pay attention to their own rescuer proficiency, the victim, and the available resources.
Travers et al. Ci rculation 2010. 122: s676-S684
How they provide CPR will depend on these three items and this is reflected in the above diagram Also important is the integration of resuscitation systems to optimize the chances of recovery from cardiac arrests. These systems need to integrate together with achievable goals to increase the chances of survival. These systems include community (goal: early access, effective chest compressions), EMS (goal: provide CPR and defibrillation), ED (Goal: therapeutic hypothermia); and hospital system (Goal: post-arrest care). SAFETY Ensure that you, your team, the patient, and that any bystanders are safe throughout all phases of care. ASSESSMENT AND MANAGEMENT Rescuers should provide immediate chest compressions upon recognizing a cardiac arrest based on the following assessment. Recognition
Adult Children Infant Unresponsive (for all ages)
No Breathing Not breathing
normally (gasping)
Not breathing or only gasping
No pulse palpated within 10 seconds
CPR Sequence C-A-B for adults, children & infants
Chest Compressions
Best hands first on patient Delegate team appropriately -DEPTH-RECOIL-PAUSES Focus on High Quality CPR
o Rate at least 100/min. o Depth at least 5 cm. o Allow complete recoil. o Minimise pauses in compressions.
Less than 10 seconds Change compressors every two minutes
Airway Management
Defer invasive airway until end of six
minutes, unless multiple rescuers/resources allow coordinated care.
Initial airway of OPA and NRM Focus on effective oxygenation rather than
method ETI / EGD / BMV all considered acceptable
methods
Ventilation
2 rescuers o Defer 30:2 until 4+ minutes in which
other goals (defib and meds established)
Multirescuers o 30:2 immediately upon setup
Avoid excessive ventilation. Ventilate 1 second per breath. No Advanced Airway
o 30:2 for all when single rescuer o 30:2 ratio for adults & multirescuer o 15:2 child/infant & multirescuer
Advanced Airway (adult, child, infant) o Asynchronous with compressions o 1 breath every 6-8 seconds o 8-10 breaths min o Visible chest rise o
Defibrillation
Car
diac
Arr
est &
Out of-Hospital Universal Algorithm
EHS has made every effort to ensure that the information, tables, drawings and diagrams contained in the Clinical Practice Guidel ines i ssued XXX is accurate at the time of publication. However, the EHS guidance is advisory and has been developed to assist healthcare professionals, together with patients, to m ake decisionincluding treatments. It is intended to support the decision making process and is not a substitute for sound clinical judgment. Guidelines cannot always contain all the information necessary for determining appropriate care and cannot address all individual situations; therefore individuals using these guidelines must ensure they have the appropriate knowledge and skills to enable appropriate interpretation.
Attach and use defibrillator ASAP Minimize interruptions in chest
compressions before and after shock, resume CPR beginning with compressions immediately after each shock
Adult o Non escalating 200J
Infants/Children o 2J/kg 1st then 4J/kg 2nd o NTE: 10J/kg or adult dose
Immediate resumption of compressions with no pulse check
Shock-break < 2 seconds Check rhythm after conclusion of 2 minute
compression cycle Minimize delays in rhythm analysis
IV Access & Drug Administration
Access obtained when feasible without interrupting chest compressions IV Access when feasible
Epinephrine 1 mg IV q4min Lidocaine XXX
Prehospital Post Arrest Care
Employ passive cooling methods o Remove clothing o Cool environment o Ice packs groin/axillary
to adults, children and infants TRANSFER OF CARE For patients with ROSC it is important to provide all relevant details to the receiving facility in terms of the resuscitation up to that time. It is expected that
-
hypothermia, neurological, cardiovascular, and metabolic support, as well as potential transfer to the PCI lab. For patients without ROSC despite ongoing resuscitation it is critical to ensure quality chest compressions during the transfer of care and to provide support as needed to the hospital team. CHARTING In addition to the mandatory fields it is important to document the following in the ePCR text fields:
Bystander CPR(bCPR) in progress Form of bCPR (30:2 vs compression only) XXX
TIPS Pre-Arrival Tips
[1] Determine the down time if possible. [2] Plan team configuration. Team leader=highest trained CPR Rotation q5cycles or 2 min
On Scene Tips [1] Access/Egress Plan exit strategy Anticipate delays Anticipate patient size factors [2] Arrest Type Witnessed vs Unwitnessed Shockable vs non-schockable Bystander CPR vs None [3] Positioning Move to adequate space Provide hard surface [4] Ensuring CPR Quality Throughout Transport Tips
[1] Secure patients & equipment [3] Ensure CPR quality [4] Expose pt and use A/C cooling [5] Communicate with ED early
Resource Utilisation Tips
[1] Early recognition of additional needs [3] Use OLMC readily [4] Expose pt and use A/C cooling
Patient Termination Tips Tissue Donation
[1] Age < 80 yrs [2] Ho HIV, HBV, HCV [3] No leukemia or lymphoma
[5] No fulminate sepsis
Key Points - Resuscitation
Quality chest compressions is critical.
Car
diac
Arr
est &
A
hti
Out of-Hospital Universal Algorithm
EHS has made every effort to ensure that the information, tables, drawings and diagrams contained in the Clinical Practice Guidelines issued XXX is accurate at the time of publication. However, the EHS guidance is advisory and has been developed to assist healthcare professionals, together with patients, to make decisionincluding treatments. It is intended to support the decision making process and is not a substitute for sound cl inical judgment. Guidelines cannot always contain all the information necessary for determining appropriate care and cannot address all individual situations; therefore individuals using these guidelines must ensure they have the appropriate knowledge and skills to enable appropriate interpretation.
Adequate rate, recoil and minimal pauses are critical
Depth of CPR will be improved with CPR
feedback devices
C-A-B sequencing for all
CPR choreography of care is critical
Teamwork, Teamwork, Teamwork KNOWLEDGE GAPS Published evidence on the universal approach to cardiac arrests does not necessarily reflect the phases of prehospital care. For example, the scene survey/management, assessment, extrication, and transport are not reflected in the 2010 Resuscitation Guidelines. Practitioners need to translate this published knowledge into practice. RESEARCH OPPORTUNITIES XXX EDUCATION IMPLICATIONS Importance to maintain practice and certification in CPR and the provision of chest compressions. Recommendations include: XXX QUALITY IMPROVEMENT IMPLICATIONS Importance to maintain [1] appropriate performance, [2] measurement, [3] benchmarking, and [4] feedback change. Key Challenges to Improving CPR Quality
Travers et al. Circulation 2010. 122: s676-S684
REFERENCES http://www.ilcor.org (description) http://www.hsfc.ca (description) http://emergency.medicine.dal.ca/ehsprotocols/protocols/toc.cfm (description) METHODOLOGY Provide tools on searching and evaluating the literature.
Car
diac
Arr
est &
Out of-Hospital Universal Algorithm
EHS has made every effort to ensure that the information, tables, drawings and diagrams contained in the Clinical Practice Guidelines issued XXX is accurate at the time o f publication. However, the EHS guidance is advisory and has been developed to assist healthcare professionals, together with patients, to m ake decisionincluding treatments. It is intended to support the decision making process and is not a substitute for sound clinical judgment. Guidelines cannot always contain all the information necessary for determining appropriate care and cannot address all individual situations; therefore individuals using these guidelines must ensure they have the appropriate knowledge and skills to enable appropriate interpretation.
Timeline Reference Chart
Disposition Reference Chart
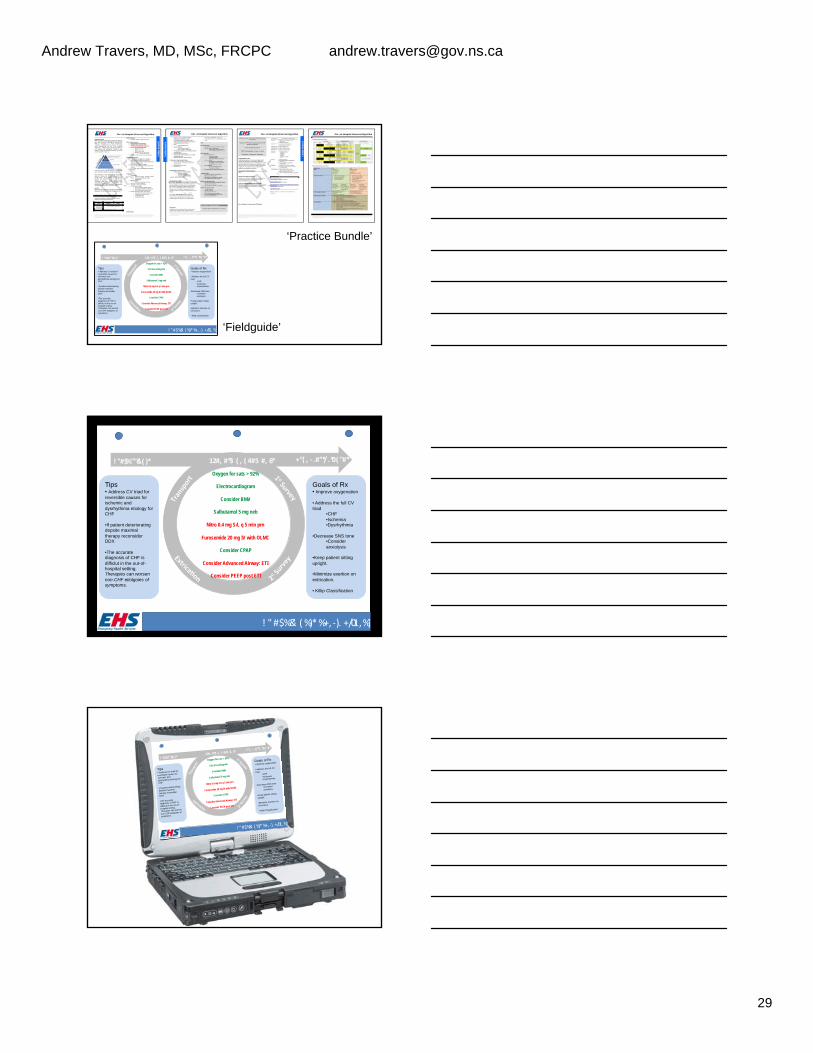
! "#$%""&' ( )* +"( , ‐ .#"*/ .*0( "#*12#, #*3 ( , ( 4#5 #, 6*
! "#$%&' (%)*%+,‐). +/01,%)
Tips • Address CV triad for reversible causes for ischemic and dysrhythima etiology for CHF
• If patient deteriorating depsite maximal therapy reconsider DDX
• The accurate diagnosis of CHF is difficlut in the out-of-hospital setting. Therapies can worsen non-CHF etiolgoies of symptoms.
Goals of Rx • Improve oxygenation
• Address the full CV triad
• CHF • Ischemia • Dysrhythmia
• Decrease SNS tone • Consider anxiolysis
• Keep patient sitting upright.
• Minimize exertion on extrication.
• Killip Classification
Oxygen for sats > 92%
Electrocardiogram
Consider BMV
Salbutamol 5 mg neb
Nitro 0.4 mg S/L q 5 min prn
Furosemide 20 mg IV with OLMC
Consider CPAP
Consider Advanced Airway: ETI
Consider PEEP post ETI
‘Practice Bundle’
‘Fieldguide’
! "#$%""&' ( )* +"( , ‐ .#"*/ .*0( "#*12#, #*3 ( , ( 4#5 #, 6*
! " #$%&' (%)*%+, ‐). +/01,%)
Tips • Address CV triad for reversible causes for ischemic and dysrhythima etiology for CHF
• If patient deteriorating depsite maximal therapy reconsider DDX
• The accurate diagnosis of CHF is difficlut in the out-of-hospital setting. Therapies can worsen non-CHF etiolgoies of symptoms.
Goals of Rx • Improve oxygenation
• Address the full CV triad
• CHF • Ischemia • Dysrhythmia
• Decrease SNS tone • Consider anxiolysis
• Keep patient sitting upright.
• Minimize exertion on extrication.
• Killip Classification
Oxygen for sats > 92%
Electrocardiogram
Consider BMV
Salbutamol 5 mg neb
Nitro 0.4 mg S/L q 5 min prn
Furosemide 20 mg IV with OLMC
Consider CPAP
Consider Advanced Airway: ETI
Consider PEEP post ETI
! "#$%""&' ( )*
+"( , ‐ .#"*/ .*0( "#*
12#, #*3 ( , ( 4#5 #, 6*
! "#$%&' (%)*%+, ‐). +/01,%)
Tips • Address CV triad for
reversible causes for
ischemic and
dysrhythima etiology for
CHF
• If patient deteriorating
depsite maximal
therapy reconsider
DDX
• The accurate
diagnosis of CHF is
difficlut in the out-of-
hospital setting.
Therapies can worsen
non-CHF etiolgoies of
symptoms.
Goals of Rx • Improve oxygenation
• Address the full CV
triad • CHF
• Ischemia
• Dysrhythmia
• Decrease SNS tone
• Consider
anxiolysis
• Keep patient sitting
upright.
• Minimize exertion on
extrication.
• Killip Classification
Oxygen for sats > 92%
Electrocardiogram
Consider BMV
Salbutamol 5 mg neb
Nitro 0.4 mg S/L q 5 min prn
Furosemide 20 mg IV with OLMC
Consider CPAP
Consider Advanced Airway: ETI
Consider PEEP post ETI
Andrew Travers, MD, MSc, FRCPC [email protected]
30
! "#$%""&' ( )*
+"( , ‐ .#"*/ .*0( "#*
12#, #*3( , ( 4#5
#, 6*
! "#$%&' (%)*%+,‐). +/01,%)
Tips
• Address CV triad for
reversible causes for
ischemic and
dysrhythima etiology for
CHF • If patient deter iorating
depsite maxim
al
therapy reconsider
DDX • The accurate
diagnosis of CHF is
difficlut in the out-of-
hospital setting.
Therapies can worsen
non-CHF etiolgoies of
symptom
s.
Goals of Rx
• Improve oxygenation
• Address the full CV
triad • CHF
• Ischemia
• Dysrhythmia
• Decrease SNS tone
• Consider
anxiolysis
• Keep patient sitting
upright.
• Minim
ize exertion on
extrication.
• Kill ip Classi fication Oxygen for sats > 92%
Electrocardiogram
Consider BMV
Salbutamol 5 mg neb
Nitro 0.4 mg S/L q 5 min prn
Furosemide 20 mg IV with OLMC
Consider CPAP
Consider Advanced Airway: ETI
Consider PEEP post ETI
!"#$%""&'()*
+"(,‐.#"*/.*0("#*
12#,#*3
(,(4#5#,
6*
!"#$%&'(%)*%+,‐).+/01,%)
Tip
s •
Ad
dres
s C
V tr
iad
for
reve
rsib
le c
aus
es
for
isch
emic
and
dy
srhy
thim
a e
tiolo
gy fo
r C
HF
• If p
atie
nt d
eter
iora
ting
deps
ite m
axim
al
ther
apy
reco
nsid
er
DD
X
• The
acc
urat
e
diag
nosi
s of
CH
F is
di
fficl
ut in
the
out-
of-
hosp
ital s
ettin
g.
The
rapi
es c
an w
orse
n no
n-C
HF
etio
lgoi
es o
f sy
mpt
om
s.
Go
als
of R
x •
Impr
ove
oxyg
enat
ion
• Add
ress
the
full
CV
tr
iad
• C
HF
• I
sche
mia
• D
ysrh
ythm
ia
• Dec
reas
e S
NS
ton
e
• Con
side
r a
nxio
lysi
s
• Ke
ep p
atie
nt s
ittin
g up
right
.
• Min
imiz
e ex
ert
ion
on
ex
tric
atio
n.
• K
illip
Cla
ssifi
catio
n
Oxy
gen
for s
ats
> 92
%
El
ectr
ocar
diog
ram
Con
side
r BM
V
Salb
utam
ol 5
mg
neb
N
itro
0.4
mg
S/L
q 5
min
prn
Furo
sem
ide
20 m
g IV
with
OLM
C
C
onsi
der C
PAP
C
onsi
der A
dvan
ced
Airw
ay: E
TI
C
onsi
der P
EEP
pos
t ETI
CPEP
Andrew Travers, MD, MSc, FRCPC [email protected]
31
Grading of Recommendations Assessment, Development and Evaluation
Grading the quality of evidence and strength of recommendations.
HIGH Quality
Moderate Quality
Low Quality
Very Low quality
Andrew Travers, MD, MSc, FRCPC [email protected]
32
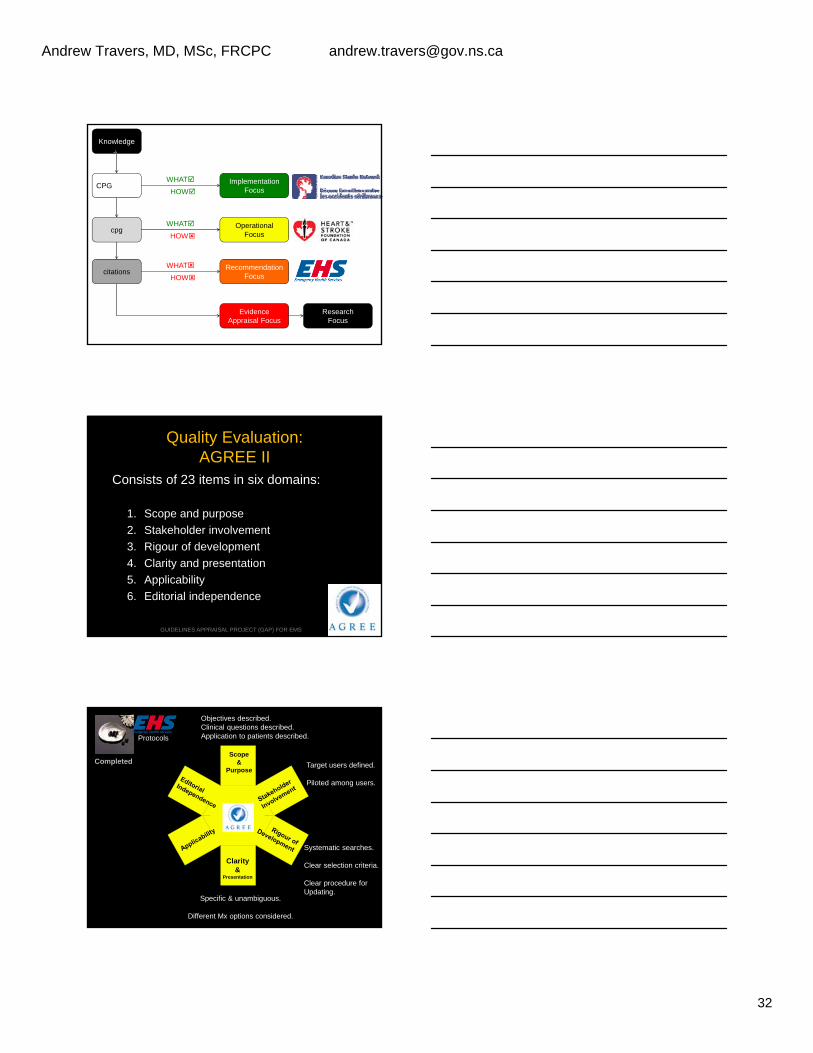
Knowledge
ImplementationFocus
OperationalFocus
CPG
cpg
citationsRecommendation
Focus
WHAT
HOW
WHAT
HOW
WHAT
HOW
EvidenceAppraisal Focus
ResearchFocus
Quality Evaluation:AGREE II
Consists of 23 items in six domains:
1. Scope and purpose
2. Stakeholder involvement
3. Rigour of development
4. Clarity and presentation
5. Applicability
6. Editorial independence
GUIDELINES APPRAISAL PROJECT (GAP) FOR EMS
Objectives described.Clinical questions described.Application to patients described.
Target users defined.
Piloted among users.
Specific & unambiguous.
Different Mx options considered.
Systematic searches.
Clear selection criteria.
Clear procedure for Updating.
Scope&
Purpose
Clarity&
Presentation
Completed
Protocols
Andrew Travers, MD, MSc, FRCPC [email protected]
33
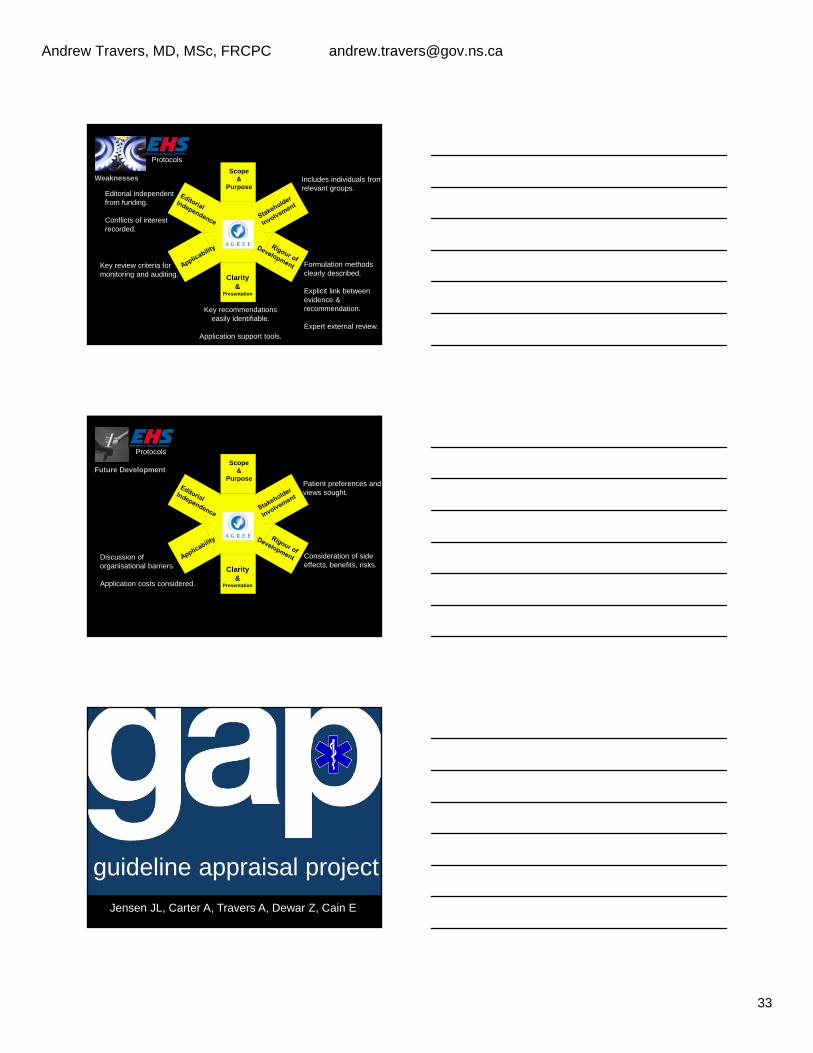
Includes individuals fromrelevant groups.
Editorial independentfrom funding.
Conflicts of interestrecorded.
Key recommendationseasily identifiable.
Application support tools.
Formulation methodsclearly described.
Explicit link between evidence & recommendation.
Expert external review.
Scope&
Purpose
Clarity&
Presentation
Weaknesses
Key review criteria formonitoring and auditing.
Protocols
Patient preferences andviews sought.
Discussion oforganisational barriers.
Application costs considered.
Consideration of sideeffects, benefits, risks.
Scope&
Purpose
Clarity&
Presentation
Future Development
Protocols
guideline appraisal project
Jensen JL, Carter A, Travers A, Dewar Z, Cain E

Andrew Travers, MD, MSc, FRCPC [email protected]
34
GUIDELINES APPRAISAL PROJECT (GAP) FOR EMS
GAP: objectives• To systematically review published clinical
practice guidelines (CPGs) for quality and relevance to prehospital practice
• To identify knowledge gaps in prehospitalareas of care– Paramedic protocol areas without relevant, high
quality published CPGs
Methods: Search• Systematic review of the English literature for
published CPGs
• Structured search strategy in 19 databases
• Review for Inclusion by two independent reviewers, third party adjudication
GUIDELINES APPRAISAL PROJECT (GAP) FOR EMS
Methods: Quality and Relevance
• Medical directors and paramedics from across Canada were recruited to serve as appraisers
• Every appraiser completed on on-line tutorial on AGREE II, a validated CPG quality evaluation tool
• www.agreetrust.org
GUIDELINES APPRAISAL PROJECT (GAP) FOR EMS
Andrew Travers, MD, MSc, FRCPC [email protected]
35
Methods
• Included CPGs were categorized as EB or non-EB• *Systematic search (systematic = search terms stated) of
>= 1 database
• *Reference list included with CPG
• +/- Formal question or clearly stated objectives
• Only those which were evidence-based moved on for full AGREE appraisal
• Each CPG was randomly assigned to 2 reviewers
• All guidelines appraised for relevance to EMS and posted on PEP website.
GUIDELINES APPRAISAL PROJECT (GAP) FOR EMS
44% are ‘evidence-based’Respiratory most common
54% of protocols have no CPG
223 Included
481 CPG
Andrew Travers, MD, MSc, FRCPC [email protected]
37
Towards National Evidence-Informed Practice Guidelines for Canadian EMS
Evidence Straight
Evidence Used
Take home tools
Objectives
Evidence
Definitions
Closing Remarks: CPEP
• Inventory of CPGs: EMS, implementation, operation
• NOT meant to reproduce CPGs
• Platform for enabling evidence mapping.
• Knowledge sharing network for EBP culture
• Dashboard of EMS evidence: appraisal & gaps
• Examples of EMS protocols in current practice.