
Evidence-based Guideline for Peer ... - School of Nursing Wai Ying Oma.pdf · “Evidence-based...
65
Abstract of dissertation entitled “Evidence-based Guideline for Peer Support Service to Increases Breastfeeding Outcomes” Submitted by Yu Wai Ying Oma For the degree of Master of Nursing at The University of Hong Kong in August 2016 Exclusive breastfeeding (EBF) is highly recommended by healthcare professionals worldwide for babies below six months old. In Hong Kong, despite the high initiation rate of breastfeeding at hospitals, the EBF rate drops significantly when measured in community and so as the breastfeeding (BF) rate. Supportive measures for breastfeeding are present in community for long time. These include breastfeeding workshops for pregnant women at antenatal period and breastfeeding support groups for breastfeeding mothers at postnatal period. Both of these interventions are nurse-led. However, new evidences suggested that peer-led breastfeeding intervention is more effective in raising EBF and BF rate. This innovation is called peer support service. It is a provision of breastfeeding support by peers who have similar backgrounds or experiences to the pregnant women from antenatal to postnatal period. The support can be in forms of information, knowledge, skills, encouragement, etc. The aim of this paper is to explore the evidences of peer support service to increase breastfeeding outcomes, analyze its implementation potential to apply in Hong Kong setting and develop an evidence-based guideline for application. Finally, recommendations on its implementation and evaluation are stated at the end.
Transcript of Evidence-based Guideline for Peer ... - School of Nursing Wai Ying Oma.pdf · “Evidence-based...

Abstract of dissertation entitled
“Evidence-based Guideline for Peer Support Service
to Increases Breastfeeding Outcomes”
Submitted by
Yu Wai Ying Oma
For the degree of Master of Nursing
at The University of Hong Kong
in August 2016
Exclusive breastfeeding (EBF) is highly recommended by healthcare professionals
worldwide for babies below six months old. In Hong Kong, despite the high initiation rate of
breastfeeding at hospitals, the EBF rate drops significantly when measured in community and so
as the breastfeeding (BF) rate. Supportive measures for breastfeeding are present in community
for long time. These include breastfeeding workshops for pregnant women at antenatal period
and breastfeeding support groups for breastfeeding mothers at postnatal period. Both of these
interventions are nurse-led. However, new evidences suggested that peer-led breastfeeding
intervention is more effective in raising EBF and BF rate. This innovation is called peer support
service. It is a provision of breastfeeding support by peers who have similar backgrounds or
experiences to the pregnant women from antenatal to postnatal period. The support can be in
forms of information, knowledge, skills, encouragement, etc.
The aim of this paper is to explore the evidences of peer support service to increase
breastfeeding outcomes, analyze its implementation potential to apply in Hong Kong setting and
develop an evidence-based guideline for application. Finally, recommendations on its
implementation and evaluation are stated at the end.

Eight randomize-controlled studies of peer support service were identified after conduction
of a systematic literature review. Critical appraisal was done and the level of evidence was
graded according to the Scottish Intercollegiate Guidelines Network (SIGN) for each of the
studies. Then the implementation potential of the peer support service was assessed based on its
transferability, feasibility and cost-benefit ratio. Evidence-based practice guideline was
developed based on the level of evidence with grades of recommendation stated. Communication
plan and pilot study plan were suggested under the implementation plan. Finally evaluation plan
was discuss to evaluate the effectiveness of the innovation. With the implementation of this peer
support service in the community, breastfeeding mothers will be better supported and thus the
EBF and BF rate should be extended.

Evidence-based Guideline for Peer Support Service to Increase Breastfeeding
Outcomes
by
Yu Wai Ying Oma
BSc. (Hons) Nursing HKPU
A thesis submitted in partial fulfilment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong.
August 2016

i
Declaration
I declare that this thesis represents my own work, except where due acknowledgement is
made, and that it has not been previously included in a thesis, dissertation or report submitted to
this University or to any other institution for a degree, diploma or other qualifications.
Signed………………………………………………………………………………
Yu Wai Ying Oma

ii
Acknowledgements
I would like to convey my deepest gratitude to my supervisor, Dr. Elizabeth Hui, for her
guidance, patience and expert advice in the process of writing this dissertation.
I would also like to thank the Department of Health for providing the sponsorship for me to
complete this Master of Nursing program. Special thanks must be said to the nursing officers in
my center and all of my colleagues. Without your support and help, I could not be released for all
the lectures on time and attend those urgent date-changed lectures.
Finally, I would like to thank my groupmates and peers who studied the same track with me
in these two years. My study would not be that smooth and happy without you.

iii
Contents
Declaration ....................................................................................................................................... i
Acknowledgements ......................................................................................................................... ii
Table of Contents ........................................................................................................................... iii
Chapter 1: Introduction ................................................................................................................... 1
1.1 Background ....................................................................................................................... 1
1.2 Affirming the Need ........................................................................................................... 2
Current breastfeeding rate ............................................................................................... 2
Current strategies ............................................................................................................ 3
Innovation ....................................................................................................................... 4
1.3 Objectives and Significance .............................................................................................. 5
Objectives ....................................................................................................................... 5
Significance..................................................................................................................... 6
Chapter 2: Critical Appraisal .......................................................................................................... 7
2.1 Search and Appraisal Strategies ........................................................................................ 7
Search strategies.............................................................................................................. 7
Inclusion criteria ............................................................................................................. 7
Exclusion criteria ............................................................................................................ 8
2.2 Results ............................................................................................................................... 8
Quality assessment ........................................................................................................ 10
2.3 Summary and Synthesis .................................................................................................. 12
Subject characteristics ................................................................................................... 13
Intervention ................................................................................................................... 13
Control .......................................................................................................................... 14
Peer supporters .............................................................................................................. 15
Methodological quality ................................................................................................. 16
Chapter 3: Implementation Potential and Clinical Guideline ....................................................... 18
3.1 Transferability of the Findings ........................................................................................ 18
Target setting ................................................................................................................. 18
Target population .......................................................................................................... 18
Philosophy of care......................................................................................................... 19
Number of beneficial clients ......................................................................................... 19
Time frame .................................................................................................................... 20
3.2 Feasibility ........................................................................................................................ 20
Nursing autonomy and current staff function ............................................................... 20
Administrative and organizational support ................................................................... 21
Risk of friction .............................................................................................................. 21
Resources and equipment ............................................................................................. 22
Evaluation ..................................................................................................................... 22
3.3 Cost-benefit Ratio ........................................................................................................... 23
Potential risks ................................................................................................................ 23
Potential benefits ........................................................................................................... 23

iv
Cost of implementation ................................................................................................. 24
Evidence-based practice guideline ................................................................................ 25
Chapter 4: Implementation Plan ................................................................................................... 26
4.1 Communication Plan ....................................................................................................... 26
Stakeholders .................................................................................................................. 26
Communication team .................................................................................................... 27
Communication with administrators ............................................................................. 27
Communication with frontline staffs and peer supporters ............................................ 27
4.2 Pilot Study Plan............................................................................................................... 28
Time frame of pilot study .............................................................................................. 28
Evaluation of pilot study ............................................................................................... 29
4.3 Evaluation Plan ............................................................................................................... 29
Intervention outcomes and measurement ...................................................................... 29
Nature of clients ............................................................................................................ 31
Sample size ................................................................................................................... 31
Data analysis ................................................................................................................. 32
4.4 Basis for Implementation ................................................................................................ 32
4.5 Conclusion ...................................................................................................................... 32
References: .................................................................................................................................... 34
Appendix I: Methodology Checklist for Randomized Controlled Trial ....................................... 40
Methodology Checklist 2: Controlled Trials ................................................................................ 40
Appendix II: Modified PRISMA 2009 Flow Diagram ................................................................. 42
Appendix III: Table of Evidence ................................................................................................... 43
Appendix IV: Quality Assessment Using SIGN Methodology Checklist for Controlled Trials ... 47
Appendix V: Budget Plan ............................................................................................................. 49
Appendix VI: Grade of Recommendations ................................................................................... 51
Appendix VII: Practicing Guideline ............................................................................................. 52
Appendix VIII: Evaluation Form for Peer Supporter ................................................................... 57
Appendix IV: Evaluation Form for Service Recipient .................................................................. 58

1
Chapter 1: Introduction
Breastfeeding has countless benefits to babies, mothers and the societies. Despite of these
benefits, the exclusive breastfeeding rate in Hong Kong is low and the duration is short.
Although the government has implemented the breastfeeding policy in public hospitals, after the
newborns were discharged to homes, breastfeeding could not be maintained. Intervention focus
on community setting like peer support service may be a possible solution for this problem. In
this chapter, the current breastfeeding practices, the needs and significant of change in current
interventions will be discussed and peer support service will be introduced.
1.1 Background
Exclusive breastfeeding for 6 months is the optimal way of feeding babies. About 800 000
children lives would be saved every year if they were fed in this optimal way (Black et al., 2013).
Even in developed countries where artificial feeding is affordable, clean water is available and
good hygienic conditions for preparing and feeding infant formula exist, all mothers should be
encouraged to breastfeed their babies. World Health Organization (WHO) recognized
breastfeeding as an economical, safe and effective strategy to solve undernutrition problem in
infancy. It recommended early initiation of breastfeeding within 1 hour of birth, exclusive
breastfeeding for the first 6 months of life and continuation of breastfeeding up to 2 years or
beyond together with complementary foods start at 6 months. Exclusive breastfeeding (EBF)
means that a baby only receives breast milk without any additional food or drink, not even water
(WHO et al., 2008). It should be fed on baby’s demand, as often as the baby wants in day and
night.
In 1989, WHO together with United Nations Children’s Fund (UNICEF) issued a joint

2
statement of “ten steps to successful breastfeeding” (WHO & UNICEF, 1989) as a guideline for
facilities which provide maternity or infant care service to implement practices that protect,
promote and support breastfeeding. It stated in step 10 that the facility should foster the
establishment of breastfeeding support groups and refer mothers to them on discharge from the
hospital or clinic. Peer support is one of the examples of breastfeeding support that can be
provided to breastfeeding mothers in public healthcare setting. In general, peer is defined as
people other than parents, siblings or relatives who have the same or similar experience as the
target people. In this paper, peer is a lay woman who has breastfeeding experience or living in
the same neighborhood as the clients with proper training of breastfeeding knowledge and skills.
Peer support service in this paper refers to the service provided by the peer to mothers with the
aim to motivate their determinacies of breastfeeding, solve their breastfeeding problems and
prolong their breastfeeding duration. This includes breastfeeding information provision,
demonstration and return demonstration of breastfeeding positioning, giving practical advice or
suggestion, emotional validation, counselling, sharing of breastfeeding experience, etc.
1.2 Affirming the Need
Current breastfeeding rate
Despite of numerous benefits of breastfeeding over formula milk feeding, exclusive
breastfeeding has not been practiced by the majority of public. When asked of future feeding
method, most pregnant women in Hong Kong planned of breastfeeding during antenatal period.
But when asked again after delivery for some days, most of them said they had ever tried
breastfeeding but only some of them continued breastfeeding. If asked in details, the number of
mothers who exclusively breastfed their babies was scanty and the breastfeeding duration was
short, especially those who planned to resume to work after maternal leave. According to a

3
survey done by UNICEF Baby Friendly Hospital Initiatives Hong Kong Association in 2015, the
breastfeeding rate on discharge was 86.3% while the EBF rate was 27.4%. At 6 month, the
breastfeeding rate was lowered by half to 41% while the EBF rate dropped to 1.2% (Department
of Health, 2015). The findings reflected that majority of Hong Kong mothers initiated
breastfeeding in hospitals but gradually changed to formula milk in 6 month time. The EBF rate
is low with partial BF is the main form of breastfeeding.
Current strategies
To promote breastfeeding, multiple strategies have been used and cooperation between
different organizations was required in order to facilitate and support breastfeeding mothers and
babies. In 1994, the Baby Friendly Hospital Initiative Hong Kong Association (BFHIHKA) was
registered with the aim of supporting mothers to breastfeeding. Activities such as the world
breastfeeding week in Hong Kong are held every year to raise public awareness of breastfeeding.
It also encourages all hospitals with maternity units to become “baby friendly”. Currently four
public hospitals namely Queen Elizabeth Hospital, Queen Mary Hospital, Kwong Wah Hospital
and Prince of Wales Hospital had started their Baby Friendly Hospital accreditation process.
Practices of “Ten steps to successful breastfeeding” and “International code of marketing of
breastmilk substitutes” were implemented in these hospitals as well as in some other hospitals.
Now over 90% of hospitals in Hong Kong including private hospitals have a written
breastfeeding policy to all health care staff and training of staff in skills necessary to implement
this policy.
Another public healthcare service provider which fully supports breastfeeding is maternal
and child health centers (MCHCs) under Department of Health (DH). There are 32 MCHCs all
over Hong Kong to provide maternal health service to pregnant and postnatal women and child

4
health service to children from newborn to age of 6. Breastfeeding promotion starts as early as
initial antenatal service by delivery of breastfeeding booklets and breastfeeding hotline. At third
trimester, pregnant women can join breastfeeding workshops to know more about benefits of
breastfeeding and learn different breastfeeding positions. When they come with their babies for
child health service, breastfeeding coaching can be provided to improve their breastfeeding skills
and solve their breastfeeding problems. A nurse-led breastfeeding support group is held monthly
in each MCHC with aims to share of breastfeeding experiences and prolong breastfeeding
duration. However, the attendance rates of this support group are low and thus the support to
breastfeeding mothers maybe insufficient.
Innovation
Although breastfeeding is a choice made by mothers, many factors can affect how they
make this choice. For example, their knowledge about breastfeeding, misconceptions of
breastfeeding, previous breastfeeding experiences and support from husbands, families and
friends. Peer support service can be a means to deliver the knowledge, correct the
misconceptions and share of breastfeeding experience while providing support to the mothers. A
recent study focused on factors contributing in early breastfeeding cessation in Chinese women
also suggested that greater postnatal breastfeeding support after mothers returned home would
increase their confidence in breastfeeding (Tarrant, Dodgson & Wu, 2014). Peer support service
has already shown positive effective especially in empowerment in mental illness patients, breast
cancer patients and parents of disabled children (Castelein, Bruggeman, Davidson & Gaag, 2015;
Mollica et al., 2014; Shilling, Bailey, Logan & Morris, 2015). Besides, evidence was found that
the provision of breastfeeding support, no matter from healthcare professionals or non-healthcare
professionals, might increase the number of women to continue breastfeeding (Oakley,

5
Henderson, Redshaw & Quigley, 2014; Tarrant et al., 2010). Peer support as an intervention to
raise EBF and BF rate was demonstrated by a numbers of studies (Chapman, Damio, Young &
Pérez-Escamilla, 2004; Kushwaha et al., 2014; Morrow et al., 1999; Tylleskär et al., 2011).
Evaluation of a peer support intervention showed a positive feedback from mothers, peer
supporters and also from the health care professionals (Ingram, 2013). Participated mothers
reported of an increase in confidence to breastfeed and thought it should be available to all
women. WHO also recognized breastfeeding support as one of the key element in successful
breastfeeding that need to be promoted. It seems that peer support service has the potential to
replace current breastfeeding support group and improve the low EBF rate and short duration in
current practice. The latest systematic review of the effectiveness of peer support in
breastfeeding was done in 2012 by Kaunonen and his colleagues. Their definition of peer
supporter was anyone who supported breastfeeding exclude healthcare professionals. This
included clients’ partners, grandmothers, relatives and friends and was different by definition
from the peer supporter mentioned in this paper. Also the reviewed studies were published
between 2000 and 2008. There is a need for an updated systematic view to include new
evidences from studies so as to explore the efficacy of this innovation in community level rather
than family level.
1.3 Objectives and Significance
Objectives
This paper is writing to answer a searchable clinical question “Can peer support
intervention increase breastfeeding outcomes in Hong Kong?” The target population is pregnant
women in Hong Kong. The intervention is the breastfeeding peer support service with
comparison to no peer support or standard care in current practice. The primary outcome was the

6
exclusive breastfeeding rate and secondary outcome was the duration breastfeeding. The
objectives of this paper are to (1) review published evidences of peer support to increase EBF
and BF rates, (2) critically appraise these evidences, (3) assess the feasibility of setting up peer
support service in Hong Kong, (4) develop of evidence-based practice guidelines of peer support
service, (5) recommend an implementation plan and (6) propose of an evaluation plan.
Significance
The phenomenon of high breastfeeding initiation rate but low exclusive breastfeeding rate
and short overall breastfeeding duration indicated that breastfeeding mothers were under support.
Local studies explored factors contributing to early breastfeeding cessation among Hong Kong
Chinese mothers revealed that unnatural expectation, uncertainty, insufficient breastmilk and left
to figure it out were the main reasons for weaning of breastfeeding (Tarrant, Dodgson & Wu,
2014; Wang, Lau, Chow & Chan, 2014). Since breastfeeding is “natural”, some mothers
expected it would come naturally and easily. But in reality, especially at the first few days after
delivery, they experienced insufficient breastmilk and uncertain whether babies were fed enough.
They would be prone to discontinue breastfeeding if left alone. Peer support service can help
mothers at this critical period. By sharing the experience from peer supporters, mothers would
have a more realistic expectation of breastfeeding and learn ways to increase breastmilk
production and breastfeeding skills. When they have uncertainties about breastfeeding, they
could contact peer supporters. Thus peer support service is a tailor-made breastfeeding service to
increase mothers’ confidence in breastfeeding and prolong breastfeeding duration and
exclusivity.

7
Chapter 2: Critical Appraisal
After affirming the needs and significance of using peer support service as an intervention
to boost the EBF and BF rate in Hong Kong, this chapter will review and assess the evidences of
its effectiveness.
2.1 Search and Appraisal Strategies
Search strategies
Three databases were searched for identifying literatures, namely PubMed, CINAHL
Plus(EBSCOhost) and OVIDSP Databases. Two sets of keywords were used when searching.
The first set was “peer” or “peer support” or “peer counsel”. The second set was “exclusive
breastfeed” or “exclusive breastfeeding” or “exclusively breastfeed”. Two trials of search were
done with each trial only used one set of keywords. After that in the third trial, the search was
done by combining all the results of the two trials together. The year of publication was set to
between 2000 and 2015. Manual search was done by reading the reference lists of literatures
related to peer support in breastfeeding. After screening and selection of studies, the resulted
studies were appraised by using the checklist for randomized controlled trail according to the
Scottish Intercollegiate Guidelines Network (SIGN) 2014 (Appendix I) to assess their quality
and level of evidence. Literatures were identified according to the following criteria.
Inclusion criteria
Studies using peer support as an intervention were included. The support could be started in
antenatal or postnatal period without time restriction. There was no restriction on the delivery
ways of support. It could be done by hospital visiting, home visiting or telephone interview. But
the peer must not be family members or relatives of participants and must share some similarities
with participants such as having breastfeeding experience or living in the same neighborhood as
http://eproxy.lib.hku.hk/login?url=http://search.ebscohost.com/login.asp?profile=ehost&defaultdb=jlh

8
the participants. The content of peer support must be limited to breastfeeding. This includes
promoting the benefits of breastfeeding, solving breastfeeding difficulties faced by participants,
helping participants to psychologically prepare and continue for breastfeeding, etc. Both paid and
voluntary peers were included. To increase the recognition level of evidences which later be
extracted to develop guideline for practice, only randomized controlled trial studies were
included.
Exclusion criteria
Mothers or pregnant women who had mental illness or other medical conditions that
affected breastfeeding were excluded. There was no restriction on the age of participants as long
as they were fit for breastfeeding. However, in known case of HIV in Hong Kong, mothers are
advised to feed formula milk instead of breastfeed due to the chance of HIV transmission to
babies. So known HIV positive women were excluded but screening of HIV status was not
compulsory for participants. Those mothers of babies with congenital abnormality, significant
illness and needed to stay in intensive care unit or special care unit were excluded. The gestation
of pregnancy was not limited as long as the babies born were healthy and abled to be breastfed
but twins or multiple births were excluded.
The primary outcome of current innovation is the prevalence of exclusive breastfeeding
while the secondary outcome is the prevalence of breastfeeding. Studies which did not measure
the prevalence of exclusive breastfeeding was excluded. Measurement of secondary outcome
was optional.
2.2 Results
The searching was done on 1st October 2015. Among a total of 124 studies, 76 studies were
found by PubMed, 9 studies were found by CINAHL Plus (EBSCOhost) and 39 studies were

9
found by OVIDSP Databases. Three studies were identified by manual search from reference
lists. After removal of duplicated studies, 81 studies were left for further filtering according to
the inclusion and exclusion criteria as stated before. At this stage, 63 studies were screened out,
and among the remaining 18 studies, only 12 of them were full-text articles in English and able
to be assessed. Four studies were screened out as they were either currently on-going controlled
trial without result released or unmatched study groups. Finally, 8 studies met all the criteria for
critical appraisal. The flow of selection can be referred to appendix II.
Eight studies were identified after searching and filtering. Two studies took place in Asia, 2
in Africa, 1 in South America and 3 in North America. The sample size in the studies was
ranging from 103 to 2,579. The publication year of the studies was between 2000 and 2015. All
were written in English. Five studies compared mothers with peer support service to those
without such service/standard care. Four of them found raised EBF rate (Dennis, Hodnett, Gallop
& Chalmers, 2002; Haider, Ashworth, Kabir & Huttly, 2000; Leite, Puccini, Atalah, Da Cunha &
Machado, 2005; Tylleskär et al., 2011) while 1 found raised BF rate as well (Dennis et al., 2002)
but 1 found no such effect on neither EBF nor BF rate (Srinivas, Benson, Worley & Schulte,
2015). Other 3 studies had 2 intervention arms. Mothers with breastfeeding peer support were
compared to mothers with childcare peer support and those without any peer support service. The
result was that breastfeeding peer support service raised both EBF and BF rate (Agrasada,
Gustafsson, Kylberg & Ewald, 2005). Two studies tried high and low frequency of peer support
service compare to standard care. One found no difference in breastfeeding outcomes between
high and low frequency but BF rate was raised (Reeder, Joyce, Sibley, Arnold & Altindag, 2014).
Another study found peer support raised both EBF and BF rate, especially the high frequency
service (Ochola, Labadarios & Nduati, 2013). The effect size of all the eight studies varied from

10
-2% to 64%. Four studies (Agrasada et al., 2005; Haider et al., 2000; Leite et al., 2005; Tylleskär
et al., 2011) delivered support by home visit while two studies delivered by telephone (Dennis et
al, 2002; Reeder et al., 2014). Other two studies used mix approach of home visit and
center-based (Ochola et al., 2013) or telephone and center-based (Srinivas et al., 2015). The
subject characteristic varied in different studies. Some with majority of uniparous, educated
women but others were multiparous, low education level women. The findings in each study
were summarized into table of evidences which can be referred to appendix III.
Quality assessment
All the 8 studies were assessed according to the SIGN 2014 (Appendix I) with methodology
checklist of randomized controlled trials. It included 10 aspects to assess whether a randomized
controlled trial is well conducted or not. All of the 8 studies addressed and focused clearly on the
effectiveness of peer support intervention in exclusive breastfeeding prevalence plus or minus
breastfeeding prevalence. Randomization method was mentioned in all the 8 studies. Three
studies (Ochola et al., 2013; Reeder et al., 2014; Tylleskär et al., 2011) used the computer
generated random numbers while another 3 studies (Agrasada et al., 2005; Haider et al., 2000;
Leite et al., 2005) used random number table. Srinivas and her colleagues (2015) used strata in
blocks of 4 method while Dennis and her colleagues (2002) invited a biostatistician who was not
involved in the recruitment process to construct the random numbers. Randomization was done
to the zones, villages or clusters rather than the women or mother-baby pairs in 3 studies (Haider
et al., 2000; Ochola et al., 2013; Tylleskär et al., 2011). Only three studies described concealment
method such as using sealed envelopes and coding (Agrasada et al.,2005; Dennis et al, 2002;
Leite et al., 2005). Other studies did not mention about it. Due to the nature of current
intervention, it was impossible to blind the subjects about the intervention or the peers who

11
provided support. But 3 of the studies had 2 intervention arms (differencing in frequency of peer
support or content of peer support), and the subjects were not informed of other intervention
arms (Agrasada et al., 2005; Ochola et al., 2013; Reeder et al., 2014). To minimized the bias,
blinding to data collectors was achieved in 7 studies (Agrasada et al., 2005; Dennis et al., 2002;
Haider et al., 2000; Leite et al., 2005; Ochola et al., 2013; Reeder et al., 2014; Tylleskär et al.,
2011).
Six studies reported no significant difference between intervention and control groups for
baseline characteristics (Agrasada et al.,2005; Haider et al., 2000; Leite et al., 2005; Reeder et al.,
2014; Srinivas et al., 2015; Tylleskär et al., 2011). One study (Dennis et al, 2002) reported higher
percentage of subjects in peer support group decided to breastfeed before pregnancy while
another study (Ochola et al., 2013) reported higher percentage of subjects in peer support group
knew that breastfeeding should be started within 1 hour after delivery. The only difference
between intervention and control groups was the presence of peer support service in all the 8
studies. But as mentioned before, 3 studies had 2 intervention arms, so the frequency of peer
support service was different between the two intervention arms. In Agrasada study, 1
intervention group was breastfeeding peer support while another intervention group was
childcare peer support. The difference between intervention and control groups was only the
presence of peer support but with different content. All the primary outcome of 8 studies was
measured in form of prevalence of EBF at particular time interval. Some studies also measured
breastfeeding or non-exclusive breastfeeding prevalence as secondary outcomes. Two studies
were analysis in intention to treat approach (Agrasada et al.,2005; Tylleskär et al., 2011). The
dropout rate of 8 studies ranged from 0% to 27.5% in time of 1 month to 6 months. Two studies
had a dropout rate more than 20% (Haider et al., 2000; Ochola et al., 2013). Three studies were

12
carried out at more than one site. But only 1 study (Tylleskär et al., 2011) listed the result of
intervention and control group with corresponding districts and the results were comparable for
all sites. The results in the other 2 studies of different villages or zones were merged together
with significant findings (Haider et al., 2000; Ochola et al., 2013). After reviewing the quality of
the 8 studies, 1 study was rated as 1++ as majority of criteria met with little risk of bias
(Agrasada et al., 2005). 2 studies were rated as 1+, indicating most criteria met with associated
risk of bias (Dennis et al, 2002; Leite et al., 2005). The rest of the studies were rated as 1-, as
allocation concealment were not mentioned and so with some risk of bias (Haider et al., 2000;
Ochola et al., 2013; Reeder et al., 2014; Srinivas et al., 2015; Tylleskär et al., 2011). The
summary of the quality assessment can be referred to appendix IV
2.3 Summary and Synthesis
The primary outcome of all the 8 studies was prevalence of EBF and some with secondary
outcome as breastfeeding prevalence. The quality of all the 8 studies was graded from 1- to 1++.
The measurement of the studies started as early as discharge and up to 24 weeks. Only one study
with quality of 1- found no positive effect of peer support on EBF rate or BF duration (Srinivas
et al., 2015). One 1++ study, two 1+ studies and four 1- studies demonstrated peer support can
increase the EBF rate (Agrasada et al.,2005; Dennis et al, 2002; Haider et al., 2000; Leite et al.,
2005; Ochola et al., 2013; Tylleskär et al., 2011). In addition, 3 of them also demonstrated
prolong BF duration in peer support groups (Agrasada et al.,2005; Dennis et al, 2002; Reeder et
al., 2014). One study showed the positive effect was partial. Peer support could increase the BF
rate but not the EBF rate (Reeder et al., 2014). The diversity of findings may be the results of the
following factors.

13
Subject characteristics
Previous study suggested that giving birth at older age, having higher years of education,
living with a partner, having had previous pregnancies, were associated with increased likelihood
of 6-month exclusive breastfeeding (Al-sahab, Lanes, Feldman & Tamim, 2010). In the 7
identified studies, majority subjects were aged around 24 - 34. However, one study did not report
the age of subjects and only this study found no positive effect on breastfeeding outcomes
(Srinivas et al., 2015). The education level of the subjects varied in different studies, from mean
of 4.2 year to undergraduate university level. Majority of the subjects were married except those
in South Africa. Subjects in 3 studies were mainly uniparous (Agrasada et al.,2005; Dennis et al,
2002; Leite et al., 2005) while they were mainly multiparous in another 3 studies (Haider et al.,
2000; Srinivas et al., 2015; Tylleskär et al., 2011). It seems that education level, marital status
and frequency of pregnancy are not linked with breastfeeding likelihood in the 8 studies while
age of mother may be a factor.
Intervention
There were 3 modes of delivery of peer support in the 8 studies. The first one was by
telephone counseling (Dennis et al, 2002; Reeder et al., 2014). Participants in intervention group
received peer service by telephone in addition to standard care.
It is a convenient method to reach the clients as nowadays nearly everyone has a smart phone. In
addition to instant direct phone conversation, photos, videos, texts, emoji or voice messages
could be sent and read whenever peer supporters or mothers were free to do so. Timing is no
longer a problem in this type of peer support service. The second type was home visiting
(Agrasada et al.,2005; Haider et al., 2000; Leite et al., 2005; Tylleskär et al., 2011). Peer
supporters delivered support by visiting the homes of intervention clients. The number of visit

14
varied from 5-15 times in the studies. This allowed face-to-face interactions between peers and
mothers. Observation and modification of BF technique was possible in this type of support. The
last one was clinic-based meeting. Due to the personal safety of peer supporters, peer service
took place in clinic rather than client’s home in Srinivas (2015) study. Clinic-based peer service
also adopted in Ochola (2013) study where one of the intervention groups was clinic-based
meeting while another one was home visiting. In that study, both of the intervention groups had
positive results in prevalence of EBF. So all the three modes of support delivery seemed work in
peer support service and the support was on individual basis in all the 8 studies.
The peer support service commenced at 2 main different periods. Five studies initiated at
antenatal period (Haider et al., 2000; Ochola et al., 2013; Reeder et al., 2014; Srinivas et al.,
2015; Tylleskär et al., 2011). They began at third trimester or first week after enrollment. Other 3
studies initiated at postnatal period (Agrasada et al.,2005; Dennis et al, 2002; Leite et al., 2005).
The first service was provided within 2 days to 5 days after baby born or discharged. The
postnatal period was the most critical period as all the studies had peer service during the first
week of baby born. The frequency would be less intense as babies grew. Finally all the peer
services in the 8 studies ended between 10 weeks and 5.5 months after baby born.
Control
The control groups in 7 studies were without provision of peer support service (Agrasada
et al.,2005; Dennis et al, 2002; Haider et al., 2000; Leite et al., 2005; Ochola et al., 2013; Reeder
et al., 2014; Srinivas et al., 2015). They could still enjoy standard usual care from hospitals or
child health service for breastfeeding advice and support. In the study done by Tylleskär and her
colleagues (2011), control group mothers from South Africa had a peer supporter like those in
intervention group. But the supporters only helped in obtaining birth certificates and social

15
welfare grants without promotion of breastfeeding. So the control groups in all the 8 studies did
not receive any breastfeeding advice or breastfeeding support from the peer supporters.
Peer supporters
The peer supporters were paid in 4 studies (Haider et al., 2000; Leite et al., 2005; Reeder et
al., 2014; Srinivas et al., 2015). They were hired as part-time or paid equivalent of the local
minimum wage. 2 studies (Agrasada et al.,2005; Dennis et al, 2002) recruited volunteers as peer
supporters while another 2 studies (Ochola et al., 2013; Tylleskär et al., 2011) did not mention it.
All the peer supporters were female. Most of them had breastfeeding experiences and some even
had EBF for 6 months or breastfeeding for at least 1 year. They lived in the same area as the
subject samples or had been the clients of the same intervention centers within 5 years. Those
supporters in Burkina Faso had the lowest education level as none of them had more than 2-6
years schooling (Ochola, Labadarios & Nduati, 2013). In contrast, majority of the supporters in
Toronto had postsecondary education (Dennis et al, 2002).
Training was provided to peer supporters before they delivered support to mothers in all the
8 studies. The content of training was similar, mainly focused on breastfeeding and counselling
skills. The benefits of breastfeeding, position and attachment, milk transfer as well as
breastfeeding myths and communication skills were usually addressed. 3 studies reported the
course content was modified from the WHO/UNICEF breastfeeding counselling course (Haider
et al., 2000; Ochola et al., 2013; Tylleskär et al., 2011). Although peer supporters were taught to
assist mothers to solve breastfeeding problems, they could refer clients for professional help in
case of difficulties. Also, supervisors were presented in 2 studies to monitor and facilitate the
peer supporters (Haider et al., 2000; Tylleskär et al., 2011). In Dennis (2002) study, activity logs
written by peer supporters were reviewed to monitor compliance.

16
Methodological quality
The sample size in the 8 studies varied from 103 to 2,579. Three studies were large scale with
over 1,000 subjects (Leite et al., 2005; Reeder et al., 2014; Tylleskär et al., 2011). 4 studies were
in medium scale with 200 – 800 subjects (Agrasada et al.,2005; Dennis et al, 2002; Haider et al.,
2000; Ochola et al., 2013). However, 1 study was relatively small scale with 120 subjects
enrolled and 103 were included in the analysis since they had follow-up to at least 1 month
(Srinivas et al., 2015). At the end of this study, less than 90 of them could actually be contacted
and this 25% of loss contact subjects may be the cause of negative result to peer support service.
Although the drop-out rate of 2 studies was higher than 20%, their sample sizes were much
bigger and thus the effect of peer support service could still be measured (Haider et al., 2000;
Ochola et al., 2013).
Overall, peer support is an effective intervention to promote EBF rate and breastfeeding
duration. Only 1 study with small sample size and high percentage of loss contact subjects did
not find such effect. The support could be delivered in various forms, such as face-to-face
interview, telephone or home visit. The selection and training of peer supporters is crucial. Peer
supporters should be friendly and enthusiastic to encourage target mothers to breastfeeding and
help them to solve breastfeeding problems no matter they are paid or not. They should share
same characteristics to their target clients like having breastfeeding experiences, living in the
same neighborhood so that they can build the rapport with their targets more easily and exchange
their experiences. They should be properly trained with guidance or supervision to ensure their
breastfeeding knowledge or skills passing to the clients are correct. The contact may start during
pregnancy or at postnatal period. The contact would be most frequent right after delivery to
provide support on breastfeeding position, baby attachment and breastfeeding problems faced by

17
the mothers. The number of contact would be reduced as the clients gained confidence in
breastfeeding. This intervention was applicable to mothers of both uniparous and multiparous at
child-bearing age with any education level.
In conclusion, six randomized control trial studies with quality from 1- to 1++ using peer
support as intervention were identified to have positive effect on breastfeeding outcomes. One
study with quality 1- only found partial positive effect while another one study with quality 1-
found no such effect. Overall, the peer support service is considered to be effective in raising
EBF rate and prolong BF duration.

18
Chapter 3: Implementation Potential and Clinical Guideline
After critical appraisal of the 8 studies, peer support service was found to be effective to
increase EBF rate and breastfeeding duration. However, none of these studies was carried out in
Hong Kong setting. This chapter explores the potential of applying this innovation in Hong Kong
in terms of transferability, feasibility and cost-benefit ratio. Finally evidence-based guidelines of
the peer support service will be developed based on these studies.
3.1 Transferability of the Findings
Target setting
The breastfeeding peer support service is proposed to be implemented in Maternal and
Child Health Centers (MCHCs). There are totally 31 MCHCs located in different districts in
Hong Kong. The two main service populations of MCHC are children from birth to age of 5 and
women under age of 65. In child service, growth and nutrition monitoring, breastfeeding
coaching, developmental surveillance, immunization and parenting are included. In women
service, antenatal and postnatal checkup, family planning and cervical smearing screening are
provided (Family Health Service, 2016). MCHC is a public setting for providing health service
for both children and women. In previous studies, breastfeeding peer support service also
delivered in public health setting such as hospitals and women, infants and children (WIC)
clinics.
Target population
The target population of this innovation is pregnant women who wish to breastfeeding. In
the selected studies, participants were mainly between twenty and thirty of age, with education
level from low to high and included both uniparous and multiparous mothers (Agrasada et
al.,2005; Dennis et al., 2002; Haider et al., 2000; Leite et al., 2005; Ochola et al., 2013; Reeder et

19
al., 2014; Srinivas et al., 2015; Tylleskär et al., 2011). Clients attended for maternal service in
MCHCs also share these characteristics. Since it is a public service for all entitled citizens,
women of any education qualifications are welcome. There is no restriction of their gravidities,
parities or their ages. But usually fertile females are aged between twenty and forty.
Philosophy of care
MCHC is under of the Family Health Service (FHS) in Department of Health. FHS was set
up with the aim to lead the community in promoting the health and well-being of children,
women and families in Hong Kong by developing evidence-based programs to meet the
changing needs of the community and empowering individuals, families and communities to
improve their health (Family Health Service, 2016). The breastfeeding peer support service is an
evidence-based intervention to promote the health of both infants and mothers as reflected by
various randomize controlled trial studies (Agrasada et al.,2005; Dennis et al, 2002; Haider et al.,
2000; Leite et al., 2005; Ochola et al., 2013; Reeder et al., 2014; Tylleskär et al., 2011). It is
consistent with the core value of FHS.
Number of beneficial clients
The number of clients benefited from peer support service is optimistic especially if it runs
in long term. In 2010, the overall attendance rate for maternal service was 152 000 in MCHCs
(Cheung, 2011). The child service in MCHC is also well supported by parents. Although private
clinics or hospitals also provide vaccinations to children by charge, majority parents bring their
newborns to MCHCs. In 2012, about 78% of all local newborns received services in MCHCs
(Department of Health, 2013). The good quality of service of MCHCs also attracts parents from
mainland China, especially to the MCHC where locates near to Lo Wu entry port. There were
about 4000 new cases for child service registered in that MCHC last year. Due to the “two-child

20
policy” of China, the number of new cases is believed to rise. There will be sufficiently large
number of babies and mothers benefited from this innovation.
Time frame
The peer support service can be launched within short time once the approval is obtained.
The first step is to recruit voluntary peer supporters. In general, 15 peer supporters can be
recruited in 2 months. After recruitment, training will be provided to equip the supporters with
breastfeeding knowledge which will take another month. At the same time, target population can
start enrolling during antenatal revisit sessions. Due to the high breastfeeding intention rate in
Hong Kong, targets meeting inclusion criteria of peer support service can be recruited within 1
month (Wang et al., 2014). Once the training is finished, peer support service can be started. The
evaluation of the peer support service can be done when participated mothers bring babies back
to MCHCs for child service. Usually they will come according to vaccination schedule at one,
two, four, six, twelve and eighteen months. Therefore, the time from implementation to
evaluation is seven to eight months.
3.2 Feasibility
Nursing autonomy and current staff function
Currently the breastfeeding peer support service in MCHCs is led by a nurse with
participated mothers actively shared their experiences during the group meeting. One nurse is
assigned to hold this breastfeeding support group every month. In the new service, a nurse will
train peer supporters and let these supporters to provide support to the participated mothers. The
format of peer support service is changed but it is still the nurses duties to run the peer support
service. Nurses do not have the autonomy to reject her assigned duties. In case they found
difficulties when carrying out their duties, they can seek help from and report to nursing officers.

21
Also, once the new service starts, the old peer support service stops. So it will not interfere
inordinately with current staff functions.
Administrative and organizational support
According to the breastfeeding policy of the Department of Health, it is committed to create
a positive environment to support breastfeeding clients and implement “Ten steps to successful
breastfeeding”. So if evidences revealed that the innovation is more effective than current service
to promote and support breastfeeding, the administration would be supportive to the innovation.
In fact, many of the MCHCs staffs have personal breastfeeding experiences. It is not limited to
nursing staffs, doctors and clerks also continued breastfeeding when they resumed to work after
maternity leaves. The whole organization climate welcomes breastfeeding.
Risk of friction
Increased workload may be a reason that frontline staffs resist to this innovation. Before
initiation of this innovation, some preparation works are needed. For example, decoration of
notice board to introduce the new service, designing leaflets for promotion of the service, editing
notes for training of peer supporters, etc. But all these materials and products made can be used
in subsequent peer support service. Also the workload will resume to current practice as the
existing peer support service stops if the new service starts. Another possible friction to the
innovation is the fear of change by some staffs. Basically, all RNs in MCHCs have been trained
for breastfeeding skills. No additional training of staff is need before implementation of the
innovation. But the format of peer support service is new to the staffs. They may have worries on
the flow of the service, the content of training, etc. Therefore, there is a need to develop clinical
guidelines for staffs to reference to.

22
Resources and equipment
The most demanding resource in the peer support service is the time for training peer
supporters. From previous studies, peer supporters were trained from 2.5 hours to 40 hours on
breastfeeding knowledge and counselling skills (Agrasada et al.,2005; Dennis et al, 2002; Haider
et al., 2000; Leite et al., 2005; Ochola et al., 2013; Srinivas et al., 2015; Tylleskär et al., 2011).
Since the peer supporters in this innovation are supposed to provide supplementary help to
mothers rather than replacing the duties of breastfeeding coaching nurses in MCHCs, 20 hours is
enough to cover necessary breastfeeding knowledge during the training. The venue of training
and meeting between peer supporters and breastfeeding mothers can be set in education room of
MCHCs where routine health talks or workshops take place. Equipment such as tables, chairs,
computer, projector and breastfeeding models are present in that room. Besides, printers, color
papers, photocopy machines and binding machines are already available in MCHCs for editing
the notes for peer supporters. References such as breastfeeding pamphlets and breastfeeding
coaching guidebooks are also available in the library of MCHCs.
Evaluation
The feeding practices of babies are routinely asked during interview in child service when
they come back for vaccination at 1, 2, 4, 6, 12 and 18 months. So the exclusivity and duration of
breastfeeding of the participated mothers-babies pairs can be traced with their case numbers.
Four months after starting each round of the peer support service, a reunion session will be held
in MCHC for peer supporters. A certificate of appreciation and incentives will be given to the
peer supporters who completed the service and evaluation can be done at that time.

23
3.3 Cost-benefit Ratio
Potential risks
Peer support service is an additional support offered to encourage mothers for breastfeeding.
For those who do not join the service, they can still enjoy existing breastfeeding service provided
in MCHCs. There is no potential risk of not trying this innovation. In previous studies, home
visit was provided by the peer supporters. However, with regard to the personal safety of both
the peer supporters and participated mothers, peer support service in this innovation does not
include home visit. Instead, they are advised to contact by phone or meet up at public places such
as hospitals or MCHCs when providing the service.
Potential benefits
The potential benefits of peer support service are numerous. In addition to the benefits to
babies and mothers which have already been discussed in previous section, the community and
society can also be benefited from it. The bonding within the community will be strengthened. In
peer support service, MCHC acts as a bridge to connect peer supporters and mothers within the
neighborhood. On one hand, peer supporters earn satisfaction and respect by providing voluntary
service. On the other hand participated mothers gain support and confidence in breastfeeding.
This win-win service will bring harmony to the community. The economic burden of the society
will also be lowered if this service can be implemented. Strong evidences have been shown that
breastfeeding protected babies from gastrointestinal (GI) illness, lower respiratory tract infection
(LRTI) and acute otitis media (AOM). It was estimated that if 21 % of British mothers
exclusively breastfeed their babies for 4 months, 1.2 million pounds per year could be saved due
to reduction of hospital cost associated with GI and 2 million pounds per year could be saved in
LRTI hospitalization costs. The potential cost saving from avoiding the need to treat AOM in
24
primary care was 0.28 million pounds per year. (Pokhrel et al., 2015; Renfrew et al., 2012) The
actual money saved by increasing breastfeeding rate and duration would be much more as
breastfeeding protect babies and mothers from more than the above listed diseases.
Cost of implementation
The cost of this innovation is mainly spent on materials for clients and as salary of staff.
Since printers and color papers are available in the MCHC, printing is free but decoration of
notice board may need money. Notes which include summary of the training content will be
prepared for every peer supporters. Although the service is in voluntary basis, certificate of
appreciation and incentives will be given to peer supporters who completed the service. As initial
start of the service, one nurse is given for 2 sessions (8 hours) to prepare the notes and content of
the training workshop. There will be 3 rounds of peer support service in a year. For every round
of the service, it will take 20 hours to train the peer supporters. At the end of each round of the
service, a half session (2 hours) will be needed to gather all the peer supporters together for
evaluation of the service and awarding certificates and incentives. Another half session (2 hours)
will be needed to trace the breastfeeding outcomes of the participated mothers-babies pairs and
do the statistical report. So to run the service, 24 hours is needed for 1 round of the service and
thus 72 hours in a year. However, once the proposed innovation started, the existing peer support
service will be cut, freeing 1 session (4 hours) monthly. As a result, extra 24 hours per year
needed to implement this innovation. Assuming the breastfeeding subject nurse reached the
maximum salary point, her hourly salary is $250 ($ 43105 4 weeks 44 hours/week) (Civil
Service Bureau, 2016). The estimated cost of implementing this innovation for a year is $ 12,600.
It was estimated that if exclusive breastfeeding rate increased to 45%, £2.49 and £ 9.44 per infant
could be saved due to treating GI and respiratory tract infection respectively (Pokhrel et al.,
25
2015). There were 62,305 babies born in Hong Kong in 2014 (Census and Statistic Department,
2015). Assume the admission rates of these diseases are same as a local cohort study findings,
$239,323 can be saved in a year which is more than to cover the cost of the innovation (Tarrant
et al., 2010). The cost-benefit ratio is calculated by dividing the cost ($12,600) by benefit
($239,323) and the ratio is 1:0.05 Details of the calculations refer to Appendix V.
Evidence-based practice guideline
A set of practice guidelines is developed to provide recommendations based on the latest
evidence for the best practice of the peer support service. It is applicable in MCHC setting and
should be followed by all MCHC staffs. The levels of evidence and grades of recommendations
are graded according to the rating scheme for the strength of the evidence of Scottish
Intercollegiate Guidelines Network based on previous appraised RCT studies. Details of the
guideline can be referred to appendix VI and VII.
26
Chapter 4: Implementation Plan
In previous chapter, breastfeeding peer support service is concluded to be transferable,
feasible and cost-beneficial to apply in Hong Kong MCHC setting. Before putting it into service,
detail planning of whole progress is needed to ensure smooth and well function of the service.
This chapter deliberates communication plan, pilot study plan, evaluation plan and basis for
implementation when running the peer support service.
4.1 Communication Plan
Stakeholders
Stakeholders are the people who have influences in or are affected by the proposed
innovation. Their attitudes, responses and commitments to the innovation will directly affect the
success of it. The stakeholders in this innovation are mainly divided into 3 groups. The first
group is the administrative group. It includes Nursing Officers (NO) in MCHCs, Senior Nursing
Officers, Cluster Nursing Officers and Principal Nursing Officer. Medical staffs are also involved
in daily function of MCHCs, especially in setting protocols and guidelines. So Medical Officers
in-charge, Senior Medical Officers, Principal Medical Officer as well as the Director of Health
are also belongs to this group. Any changes about service provision in MCHCs must be informed
and permitted by them. In addition, they are in charge of resources and manpower allocation.
Funding for operation of the innovation must be granted before it starts and responsible staff for
training peer supporters must be set ahead. The second group is the frontline staffs who carry out
the innovation and directly face the clients. Examples in this group are Registered Nurses (RN),
Enrolled Nurses (EN) and Medical Officers (MO). The frontline staffs are expected to recruit
peer supporters and potential breastfeeding mothers, train the peer supporters, pair up the peer
supporters and participated mothers, monitor the progress of peer supporters, interview and

27
report the feeding outcomes of babies of the participated mothers and help to solve breastfeeding
problems faced by participated mothers. The last group is the peer supporters. They are
volunteers recruited for providing breastfeeding support to participated mothers. On one hand,
they are recipients of breastfeeding knowledge and skill taught by nurses. On the other hand,
they are service provider who directly face and contact participated mothers. All these three
groups of people are essential to the innovation.
Communication team
In order to put the innovation into practice and connect all the 3 groups of stakeholders
together, there is a need to build a communication team. The communication team consists of 1
MO, 1 NO and 4 RNs. The innovation proposer (a RN) is definitely in the team as she is the one
who suggested the idea and presented it to the MOs and NOs in the MCHC. One of the MOs and
NOs are engaged in the team because they have windows to reach the administrative
stakeholders. The RNs in the team mainly deal with frontline staffs and peer supporters.
Communication with administrators
The MO and NO in the communication team can bring the innovation up to the
administrative group by emails or through regular meetings with them. They have to present the
needs of changing current peer support service, the benefits of it, the budget plan and workflow
of implement by PowerPoint slides or in form of proposal. After the innovation starts, they also
have to report the progress and outcomes to them.
Communication with frontline staffs and peer supporters
As discussed before, some staffs may concern of increase workload and have fear to change.
To gain their co-operation, the benefits and workflow of the innovation will be introduced to
them prior to implementation at clinic weekly meeting by PowerPoint slides. The evidence-based

28
guidelines of the new peer support service will be prepared before the start of the service. The
progress of peer supporters will be monitored by the nurses who hold the peer support service at
that round. Two nurses will hold one round of peer support service together so that they can
share the duties and ensure the training of peer supporters will not be affected due to sick leave
of the trainer. Phone follow-up allows peer supporters report any difficulties they faced during
the service. In general it can be finished within 5 minutes and the nurses can make use of the
time after daily interviews to do it without needing extra session. Two of the RNs in the
communication team will hold the first round of peer support service, allowing more time for the
rest of the frontline staffs to observe and adapt. Also staffs are welcomed to give feedback at any
time and guidelines may be reviewed if necessary based on the outcomes and evidences.
4.2 Pilot Study Plan
In order to detect any unforeseeable limitations and difficulties which may be faced in
actual implementation, a pilot study is essential for a trial run of the proposed innovation. The
number of clients involved in the pilot study will be fewer and the time frame of the study will
be shorter than proposed in the innovation since the aim of the pilot study is to test the feasibility
of the peer support service rather than to increase breastfeeding exclusivity and duration. Based
on the results of the pilot study, refinements and modifications can be made to ensure the success
of the innovation.
Time frame of pilot study
A pilot study will start as soon as the approval of the innovation granted from the
administrators. Members in communication team will start preparing the content and materials
needed in training peer supporters and introducing the peer support service to the frontline staffs.
The rest of the staffs will help in recruiting peer supporters and potential breastfeeding mothers

29
during interviews in child sessions and antenatal sessions respectively. The recruitment criteria of
both peer supporters and service recipients are same as the innovation. In a month time, 2
volunteer supporters will be recruited for training of the peer support service. The 20-hour
training will be provided in 5 consecutive mornings from nine am to one pm and 2 RNs will take
turns to hold the training sessions. At the end of the training, one 37-week pregnant woman will
be paired up with a peer supporter and the peer support service will start. After 2 weeks, a nurse
will contact the peer supporters for their progresses.
Evaluation of pilot study
Evaluation for peer supporters will be done when they came back for certificates of
appreciation and incentives at 2 months after the service started. Evaluation for participated
mothers will be done when they bring back their babies for vaccination at 1 month old. The
evaluation forms for both peer supporters and participated mothers can be referred to appendix
VII and VIII respectively. After collection of the feedbacks from both peer supporters and
participated mothers, communication team members will report the results of the pilot study
during clinic weekly meeting. All staffs can reflect their opinions about the pilot study during the
meeting and the guidelines may be refined according to the result of the evaluation.
4.3 Evaluation Plan
The purpose of the evaluation plan is to assess the effectiveness of the peer support service.
Intervention outcomes and measurement, nature and number of clients involved, data analysis
will be taken into account in the evaluation.
Intervention outcomes and measurement
Participated mothers and babies outcomes
The primary outcome of the peer support service is the exclusive breastfeeding rate at 4

30
month. It can be measured when participated mothers bring their babies back to MCHC for
vaccination at 4 months. Routine nurse interview will be conducted which includes asking for
feeding pattern of babies. In addition, evaluations form (Appendix IV) will be given to the
mothers to fill in so as to assess their satisfactory levels. The secondary outcome of the service is
breastfeeding rate (non-exclusive) at 6 months. Since solid food should be introduced at 6
months, it is common for babies to have both solid food and breastfeeding at this age. By
definition, it is not exclusive breastfeeding and so breastfeeding rate instead of exclusive
breastfeeding rate is measured at 6 months. Again, this outcome can be measured when mothers
bring their babies back to MCHC at 6 months vaccination schedule during routine nurse
interview.
Peer supporters outcome
The participation of peer supporters is crucial in this innovation because they are the ones
who provide support directly to the mothers. So their application of knowledge and skills to
mothers is another key outcome. An evaluation form (Appendix VIII) will be given to them to
fill in when they come back for reunion session 4 months after the start of the service. Also, they
are encouraged to give verbal feedback to the nurses at the end of each training sessions.
Healthcare professional outcome
One of the duties of staffs in DH is to promote breastfeeding. So the problem faced when
carrying out the innovation rather than their satisfaction to the innovation is the intervention
outcome for frontline staffs. From time to time, all staffs should report to their NOs or MOs
when they have problems in carrying out their duties. Also, the communication team members
may randomly approach frontline staffs and ask for their opinions for running the peer support
service. If no problems are reported, this outcome is achieved.
31
System outcomes
The system outcome can be reflected by the length of recruitment period. Since the quota of
clients for each round of service is set, the shorter the recruitment period indicates the higher
popularity of service. The quota of clients may be adjusted in the future depending on the
popularity of the service. The actual cost of launching the innovation is another system outcome.
It should be compared with the budget plan to ensure if it is cost effective.
Nature of clients
The clients in this innovation are Chinese pregnant women at 36 week or above who wish to
breastfeed their single born babies. They and their babies should be physically fit with no
congenital abnormality or condition that affects breastfeeding. They should attend the same
MCH for both maternal and child service and come back for service according to routine
schedule. For peer supporters, they should have breastfeeding experience of at least 6 months
and able to read and speak Chinese. All the clients, peer supporters should live in the same
district as the MCH located.
Sample size
Two-tailed z test for testing one proportion was used to calculate the sample size. The level
of significance was set to 5% with power of 80%. According to a local breastfeeding survey, the
current exclusive breastfeeding rate at 4 month is 27% (Department of Health, 2015). From
previous studies, the effect size of the intervention on exclusive breastfeeding ranged from -2%
to 64% in 12 to 24 weeks. Assuming the effect size is 20% when implement in Hong Kong
setting, the number of sample needed is 42. From previous studies, the drop-out rate of the
innovation is about 10%, thus 45 clients are needed. The number of peer supporters recruited in
each round was 15, so 1 peer supporter will be paired with 3 clients.

32
Data analysis
The collected data will be analyzed by a computerized Statistical Package for Social
Science (SPSS) software. Both the primary outcome of EBF rate at 4 month and secondary
outcome of BF rate at 6 month will be compared to current EBF and BF rate of MCHC
respectively by using one sample t-test to determine any difference after the implementation of
peer support service. Chi-square test will be used to determine whether clients and peer
supporters satisfied with the service.
4.4 Basis for Implementation
The ultimate goal of the peer support service is to increase EBF rate and prolong BF
duration so as to promote the health of babies, mothers as well as the families as a whole. The
effectiveness of the service is based on whether the primary outcome can be achieved. In
previous studies, the effect size of the service varied from -2% to 64% which is quite a large
variation. But focusing on the studies using telephone or clinic based peer support service, the
effect size contracted to between 1% and 23.9%. Since the peer support service in Hong Kong
will mainly be delivered by clinic based and telephone contact, the service will be regarded as
effective if the increased EBF rate is around 20%. The satisfaction levels of mothers towards the
service also play an important part in the innovation. The innovation will be fully implemented if
at least 60% of them showed “strongly agree” or “agree” in the service satisfaction in the
evaluation form.
4.5 Conclusion
Exclusive breastfeeding is the best way of feeding for babies under 6 months old. Babies,
mothers as well as the society can all be benefited from breastfeeding. However, local exclusive
breastfeeding rate and breastfeeding duration is below standard. More efforts should be put in

33
promoting breastfeeding in public health setting. Peer support service may be a solution to this
problem. Randomized controlled studies with low to high qualities showed that peer support
service is effective in boosting the exclusive breastfeeding rate and breastfeeding rate in foreign
countries. With regard to the transferability, feasibility and cost-benefit ratio, the peer support
service can be translated into Hong Kong setting. An evidence-based clinical guideline is also
developed to provide guidance for frontline staff when carrying out the peer support service.
After the pilot testing, it is believed that potential difficulties and problems will be identified and
tackled before the implementation of the service. Evaluations will be done to determine the
effectiveness of this local peer support service.

34
References:
Al-sahab, B., Lanes, A., Feldman, M. & Tamim, H. (2010). Prevalence and
predictors of 6-month exclusive breastfeeding among Canadian women: A national survey.
BMC Pediatrics. 10(20):1–9. doi: 10.1186/1471-2431-10-20.
Agrasada, G. V., Gustafsson, J., Kylberg, E. & Ewald, U. (2005). Postnatal peer counselling on
exclusive breastfeeding of low-birthweight infants: a randomized, controlled trial. Acta
Paediatr. 94(8):1109-15.
Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z. A., Christian, P., De Onis, M., Ezzati, M.,
Grantham-McGregor, S., Katz, J., Martorell, R. & Uauy, R. (2013). Maternal and child
undernutrition and overweight in low-income and middle-income countries. The Lancet,
382(9890), 427-451. doi: 10.1016/S0140-6736(13)60937-X
Castelein, S., Bruggeman, R., Davidson, L. & Gaag, Mv. (2015). Creating a Supportive
Environment: Peer Support Groups for Psychotic Disorders. Schizophr Bull, 41(6):1211-3.
doi: 10.1093/schbul/sbv113
Chapman, D. J., Damio, G., Young, S. & Pérez-Escamilla, R. (2004). Effectiveness of
breastfeeding peer counseling in a low-income, predominantly Latina population: A
randomized, controlled trial. Arch Pediatr Adolesc Med. 158:897–902.
Census and Statistic Department. (2015). Hong Kong Monthly Digest of Statistics: The
fertility trend in Hong Kong, 1981-2014. Retrieved from
http://www.censtatd.gov.hk/hkstat/sub/sp160.jsp?productCode=FA100090
Cheung, K. C. M. (2011, April 6). Written reply of Legislative Council questions. Retrieved from
http://www.lwb.gov.hk/eng/legco/06042011_1.htm

35
Chung, S. H., Kim, H. R., Choi, Y. S., & Bae, C. W. (2013). Trends of
Breastfeeding Rate in Korea (1994-2012): Comparison with OECD and
Other Countries. Journal of Korean medical science, 28(11), 1573-1580. doi:
10.3346/jkms.2013.28.11.1573
Civil Service Bureau. (2016, February 9). Master pay scale. Retrieved from
http://www.csb.gov.hk/english/admin/pay/42.html
Dennis, C-L., Hodnett, E., Gallop, R. & Chalmers, B. (2002). The effect of peer support on
breast-feeding duration among primiparous women: a randomized controlled trial. CMAJ.
66:21–28.
Department of Health. (2015). Breastfeeding survey 2015. Hong Kong : Hong Kong
Government.
Department of Health. (2013). Department of Health Annual Report 2012/2013. Hong Kong :
Hong Kong Government. Family Health Service. (2016, January 29). Home. Retrieved
from http://www.fhs.gov.hk/english/
Furuta, M., Sandall, J., Cooper, D. & Bick, D. (2015). Severe maternal morbidity and
breastfeeding outcomes in the early post-natal period: a prospective cohort study from one
English maternity unit. Matern Child Nutr. Retrieve September 20, 2015,
http://onlinelibrary.wiley.com.eproxy2.lib.hku.hk/doi/10.1111/mcn.12176/epdf. doi:
10.1111/mcn.12176
Häggkvist, A. P., Brantsæ ter, A. L., Grjibovski, A. M., Helsing, E., Meltzer, H. M., Haugen, M.
(2010). Prevalence of breast-feeding in the Norwegian Mother and Child Cohort Study and
health service-related correlates of cessation of full breast-feeding. Public Health
Nutr.13(12):2076-86.

36
Haider, R., Ashworth, A., Kabir, I. & Huttly, S. R. (2000). Effect of community-based peer
counsellors on exclusive breastfeeding practices in Dhaka, Bangladesh: a randomised
controlled trial. Lancet. 56(9242):1643-7.
Ingram, J. (2013). A mixed methods evaluation of peer support in Bristol, UK: mothers',
midwives' and peer supporters' views and the effects on breastfeeding. BMC Pregnancy
Childbirth. 13:192. doi: 10.1186/1471-2393-13-192.
Kaunonen, M., Hannula, L. & Tarkka, M. T. (2012). A systematic review of peer support
interventions for breastfeeding. J Clin Nurs. 21(13-14):1943-54. doi:
10.1111/j.1365-2702.2012.04071.x
Kushwaha, K. P., Sankar, J., Sankar, M. J., Gupta, A., Dadhich, J. P., Gupta, Y. P., Bhatt, G. C.,
Ansari, D. A. & Sharma, B. (2014). Effect of peer counselling by mother support groups
on infant and young child feeding practices: the Lalitpur experience. PLoS One. 9(11):
e109181. doi: 10.1371/journal.pone.0109181
Leite, A., Puccini, R., Atalah, A., Da Cunha, A. & Machado, M. (2005). Effectiveness of
home-based peer counselling to promote breastfeeding in the northeast of Brazil: A
randomized clinical trial. Acta Paediatrica. 94:741–746.
Liu, P., Qiao, L., Xu, F., Zhang, M., Wang, Y. & Binns, C. W. (2013). Factors associated with
breastfeeding duration: a 30-month cohort study in northwest China. J Hum Lact.
29(2):253-9. doi: 10.1177/0890334413477240
37
Mollica, M. A., Nemeth, L. S., Newman, S. D., Mueller, M. & Sterba, K. (2014). Peer navigation
in African American breast cancer survivors. Patient Relat Outcome Meas, 7(5):131-44.
doi: 10.2147/PROM.S69744
Morrow, A. L., Guerrero, M. L., Shults, J., Calva, J. J., Lutter, C., Bravo, J., Ruiz-Palacios, G.,
Morrow, R. C. & Butterfoss, F. D. (1999). Efficacy of home-based peer counselling to
promote exclusive breastfeeding: a randomised controlled trial. Lancet.
353(9160):1226-31.
Oakley, L. L., Henderson, J., Redshaw, M. & Quigley, M. A. (2014). The role of support and
other factors in early breastfeeding cessation: an analysis of data from a maternity survey
in England. BMC Pregnancy Childbirth. 26;14:88. doi: 10.1186/1471-2393-14-88
Ochola, S. A., Labadarios, D. & Nduati, R. W. (2013). Impact of counselling on exclusive
breast-feeding practices in a poor urban setting in Kenya: a randomized controlled trial.
Public Health Nutr. 16(10):1732-40. doi: 10.1017/S1368980012004405
Pokhrel, S., Quigley, M. A., Fox-Rushby, J., McCormick, F., Williams, A., Trueman, P., Dodds,
R. & Renfrew, M. J. (2015). Potential economic impacts from improving breastfeeding
rates in the UK. Arch Dis Child. 100(4):334-40. doi: 10.1136/archdischild-2014-306701
Reeder, J. A., Joyce, T., Sibley, K., Arnold, D. & Altindag, O. (2014). Telephone peer counseling
of breastfeeding among WIC participants: a randomized controlled trial. Pediatrics.
134(3):e700-9. doi: 10.1542/peds.2013-4146
Renfrew, M. J., Pokhrel, S., Quigley, M., McCormick, F., Fox-Rushby, J., Dodds, R., Duffy, S.,
Trueman, P. & Williams, A. (2012). Preventing disease and saving resources: the potential
contribution of increasing breastfeeding rates in the UK. UNICEF.

38
Santos, F. S., Santos, F. C., Santos, L. H., Leite, A. M. & Mello, D. F. (2015). Breastfeeding and
protection against diarrhea: an integrative review of literature. Einstein (Sao
Paulo).13(3):435-40. doi: 10.1590/S1679-45082015RW3107
Shilling, V., Bailey, S., Logan, S. & Morris, C. (2015). Peer support for parents of disabled
children part 1: perceived outcomes of a one-to-one service, a qualitative study. Child Care
Health Dev, 41(4):524-36. doi: 10.1111/cch.12223
Srinivas, G. L., Benson, M., Worley, S. & Schulte, E. (2015). A clinic-based breastfeeding peer
counselor intervention in an urban, low-income population: interaction with breastfeeding
attitude. J Hum Lact. 31(1):120-8. doi: 10.1177/0890334414548860
Tarrant, M., Dodgson, J. E. & Wu, K. M. (2014). Factors contributing to early breast-feeding
cessation among Chinese mothers: an exploratory study. Midwifery. 30(10):1088-95. doi:
10.1016/j.midw.2014.03.002
Tarrant, M., Fong, D. Y., Wu, K. M., Lee, I. L., Wong, E. M., Sham, A., Lam, C. & Dodgson, J. E.
(2010). Breastfeeding and weaning practices among Hong Kong mothers: a prospective
study. BMC Pregnancy Childbirth. 29;10:27. doi: 10.1186/1471-2393-10-27
Tarrant, M., Kwok, M. K., Lam, T. H., Leung, G. M. & Schooling, C. M. (2010). Breast-feeding
and childhood hospitalizations for infections. Epidemiology. 21(6):847-54. doi:
10.1097/EDE.0b013e3181f55803
Tylleskär, T., Jackson, D., Meda, N., Engebretsen, I. M., Chopra, M., Diallo, A. H., Doherty, T.,
Ekström, E. C., Fadnes, L. T., Goga, A., Kankasa, C., Klungsøyr, J. I., Lombard, C.,
Nankabirwa, V., Nankunda, J. K., Van de Perre, P., Sanders, D., Shanmugam, R.,

39
Sommerfelt, H., Wamani, H., Tumwine, J. K. & PROMISE-EBF Study Group. (2011).
Exclusive breastfeeding promotion by peer counsellors in sub-Saharan Africa
(PROMISE-EBF): a cluster-randomised trial. Lancet. 378(9789):420-7. doi:
10.1016/S0140-6736(11)60738-1
UNICEF Baby Friendly Hospital Initiatives Hong Kong Association. (2015). World
Breastfeeding Week Annual Survey 2015. Retrieved September 20, 2015,
http://unicef.org.hk:8080/download/WBWReport2015_E.pdf
Wang, W., Lau, Y., Chow, A. & Chan, K. S. (2014). Breast-feeding intention, initiation and
duration among Hong Kong Chinese women: a prospective longitudinal study. Midwifery.
30(6):678-87. doi: 10.1016/j.midw.2013.07.015
World Health Organization. (2015). Infant and young child feeding. Retrieved September 20,
2015, http://www.who.int/mediacentre/factsheets/fs342/en/
World Health Organization & UNICEF. (2003). Global strategy for infant and young child
feeding. World Health Organization. Geneva, Switzerland: World Health Organization and
UNICEF.
WHO & UNICEF. (1989). Joint statement on protecting, promoting and supporting
breast-feeding: The special role of maternity services. Geneva: World Health Organization
World Health Organization, UNICEF, the United States Agency for International Development,
the Food and Nutrition Technical Assistance project, the University of California at Davis
& International Food Policy Research Institute. (2008). Indicators for assessing infant and
young child feeding practices, Part I: Definitions. Geneva: World Health Organization

40
Appendix I: Methodology Checklist for Randomized Controlled Trial
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Guideline topic: Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design
algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial
questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison
Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised. Yes
Can’t say
No
1.3 An adequate concealment method is used.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment
allocation.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial. Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation. Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each

41
treatment arm of the study dropped out before the study was completed?
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise
bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.

42
Appendix II: Modified PRISMA 2009 Flow Diagram
Records identified through database searching
(n = 124 )
Scre
enin
g El
igib
ility
Id
enti
fica
tio
n Additional records identified
through other sources (n = 3 )
Records after duplicates removed (n = 81 )
Records screened (n = 18 )
Records excluded (n = 63 )
Full-text articles assessed for eligibility
(n = 12 )
Full-text articles excluded, due to on-going studies
without results, unmatched study group
(n = 4 )
Studies included in qualitative synthesis
(n = 8 )
Incl
ud
ed
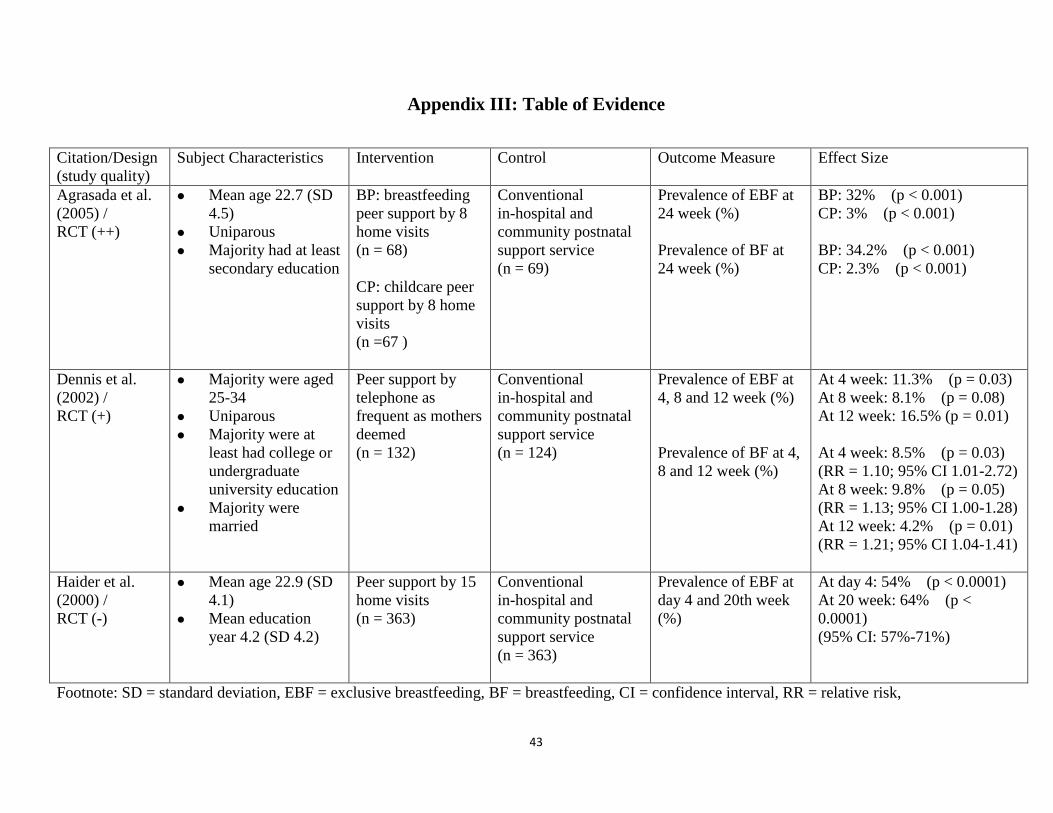
43
Appendix III: Table of Evidence
Citation/Design
(study quality)
Subject Characteristics Intervention Control Outcome Measure Effect Size
Agrasada et al.
(2005) /
RCT (++)
Mean age 22.7 (SD
4.5)
Uniparous
Majority had at least
secondary education
BP: breastfeeding
peer support by 8
home visits
(n = 68)
CP: childcare peer
support by 8 home
visits
(n =67 )
Conventional
in-hospital and
community postnatal
support service
(n = 69)
Prevalence of EBF at
24 week (%)
Prevalence of BF at
24 week (%)
BP: 32% (p < 0.001)
CP: 3% (p < 0.001)
BP: 34.2% (p < 0.001)
CP: 2.3% (p < 0.001)
Dennis et al.
(2002) /
RCT (+)
Majority were aged
25-34
Uniparous
Majority were at
least had college or
undergraduate
university education
Majority were
married
Peer support by
telephone as
frequent as mothers
deemed
(n = 132)
Conventional
in-hospital and
community postnatal
support service
(n = 124)
Prevalence of EBF at
4, 8 and 12 week (%)
Prevalence of BF at 4,
8 and 12 week (%)
At 4 week: 11.3% (p = 0.03)
At 8 week: 8.1% (p = 0.08)
At 12 week: 16.5% (p = 0.01)
At 4 week: 8.5% (p = 0.03)
(RR = 1.10; 95% CI 1.01-2.72)
At 8 week: 9.8% (p = 0.05)
(RR = 1.13; 95% CI 1.00-1.28)
At 12 week: 4.2% (p = 0.01)
(RR = 1.21; 95% CI 1.04-1.41)
Haider et al.
(2000) /
RCT (-)
Mean age 22.9 (SD
4.1)
Mean education
year 4.2 (SD 4.2)
Peer support by 15
home visits
(n = 363)
Conventional
in-hospital and
community postnatal
support service
(n = 363)
Prevalence of EBF at
day 4 and 20th week
(%)
At day 4: 54% (p < 0.0001)
At 20 week: 64% (p <
0.0001)
(95% CI: 57%-71%)
Footnote: SD = standard deviation, EBF = exclusive breastfeeding, BF = breastfeeding, CI = confidence interval, RR = relative risk,

44
Citation/Design
(study quality)
Subject Characteristics Intervention Control Outcome Measure Effect Size
Leite et al.
(2005) /
RCT (+)
Average age 23.6
Majority were
married
Majority were
uniparous
Average education
year ranged 6.2
Peer support by 6
home visits
(n = 503)
Conventional
in-hospital and
community postnatal
support service
(n = 500)
Prevalence of EBF
at 16 week (%)
At 16 week: 5.3%
(p = 0.044)
Ochola,
Labadarios &
Nduati. (2013) /
RCT (-)
Mean age ranged
24.5-24.8 (SD 5.4)
Majority were
married
All had at least
primary education
HP: Peer support by
7 sessions in health
center/home visit
(n = 120)
FP: Peer support by
1 sessions in health
center
(n = 120)
Conventional
in-hospital and
community postnatal
support service
(n = 120)
Prevalence of EBF
at 4 and 24 week
(%)
At 4 week:
HP: 87%
RR = 1.21; 95% CI 1.04,
1.39 (p = 0.011)
FP: 84.3%
RR = 1.17; 95% CI 1.00,
1.36 (p = 0.041)
At 24 week,
HP: 23.9%
RR = 4.20; 95% CI 1.66,
10.64 (p = 0.002)
FP: 9.2%, RR = 1.64;
95% CI 0.56, 4.81 (p =
0.371)
Footnote: SD = standard deviation, EBF = exclusive breastfeeding, BF = breastfeeding, CI = confidence interval, RR = relative risk,

45
Citation/Design
(study quality)
Subject Characteristics Intervention Control Outcome Measure Effect Size
Reeder et al.
(2014) /
RCT (-)
Mean age ranged
26.9 -27.3
More than half
were married
More than half had
high school
diploma
*Low frequency peer
support by 4 telephone
contacts
(n = 646)
*High frequency peer
support service by 8
telephone contacts
(n = 645)
Conventional
in-hospital and
community postnatal
support service
(n = 657)
Prevalence of EBF
at 4, 12, 24 week
(%)
Prevalence of BF at
4, 12, 24 week (%)
At 4 week: 7% (p > 0.1)
At 12 week: 10% (p >
0.1)
At 24 week: 1% (p > 0.1)
At 4 week: 16% (p <0.01)
At 12 week: 19% (p
<0.01)
At 24 week: 18% (p
<0.01)
Srinivas et al.
(2015) /
RCT (-)
Majority did not
complete high
school
Majority were
multiparous
Majority had no
prior breastfeeding
experience
Peer support by 12
clinic / hospital visit ±
telephone contacts
(n = 50)
Conventional
in-hospital and
community postnatal
support service
(n = 53)
Prevalence of EBF
at 4 and 24 week
(%)
Prevalence of BF at
4 and 24 week (%)
At 4 week: -5%
(p = 0.51, RR = 0.75;
95% CI 0.33-1.72)
At 24 week: -2%
(p = 0.51, RR = 0.47;
95% CI 0.05-4.89)
At 4 week: 15%
(p = 0.14, RR = 1.22;
95% CI 0.93-1.60)
At 24 week,
0% (p = 0.96, RR = 0.97;
95% CI 0.26-3.56)
*Remarks: Authors did not find any difference in breastfeeding outcomes between high and low frequency treatment groups, so the 2 treatment arms
were combined into a single category.
Footnote: EBF = exclusive breastfeeding, RR = relative risk, CI = confidence interval

46
Citation/Design
(study quality)
Subject Characteristics Intervention Control Outcome Measure Effect Size
Tylleskär et al.
(2011) /RCT (-)
Majority were
married in Burkina
Faso and Uganda
but opposite in
South Africa
Majority were
multipara in
Burkina Faso and
Uganda, around
half were
multipara in South
Africa
Year of education
ranged 0-12
Peer support by at
least 5 home visits
In Burkina Faso
(n = 392)
In Uganda
(n = 396)
In South Africa
(n = 535)
Conventional
in-hospital and
community postnatal
support service
In Burkina Faso
(n = 402)
In Uganda
(n = 369)
In South Africa
(n = 485)
Prevalence of EBF
at 12, 24 week (%)
At 12 weeks
Burkina Faso : 45%
(Prevalence ratio 2.29,
95% CI: 1.33-3.92)
Uganda: 38%
(Prevalence ratio 1.89,
95% CI: 1.70-2.11)
South Africa: 4%
(Prevalence ratio 1.72,
95% CI: 1.12-2.63)
At 24 weeks
Burkina Faso : 51%
(Prevalence ratio 3.33,
95% CI: 1.74-6.38)
Uganda: 44%
(Prevalence ratio 3.83,
95% CI: 2.97-4.95)
South Africa: 1%
(Prevalence ratio 5.70,
95% CI: 1.33-24.26)
Footnote: EBF = exclusive breastfeeding, CI = confidence interval

47
Appendix IV: Quality Assessment Using SIGN Methodology Checklist for Controlled Trials
Section 1: Internal Validity
Agrasada et
al. (2005)
Dennis et al.
(2002)
Haider et al.
(2000)
Leite et al.
(2005)
Ochola et al.
(2013)
Reeder et al.
(2014)
Srinivas et al.
(2015)
Tylleskär et al.
(2011)
Clearly Focused
Question
Yes Yes Yes Yes Yes Yes Yes Yes
Randomization Yes Yes Yes Yes Yes Yes Yes Yes
Allocation
Concealment
Yes Yes No Yes No No No No
Blinding No No No No No No No No
Comparable Groups Yes No Yes Yes No Yes Yes Yes
Treatment is the Only
Difference
Yes Yes Yes Yes Yes Yes Yes Yes
Valid and Reliable
Outcome Measures
Yes Yes Yes Yes Yes Yes Yes Yes
Drop-out Rate BP: 13.3%
CP: 10.4%
C: 14.5%
I: 0%
C: 1.6%
I: 20.7%
C: 21.5%
I: 15.1%
C: 13.6%
FP: 27.5%
HP: 25.8%
C: 25.8%
LP: 3.3%
TP: 3.1%
C: 3.3%
I: 18%
C: 13.2%
I: 10.2%
C: 11.5%
Intention to Treat
Analysis
Yes No No No No No No Yes
Comparable Results
from All Site
Not
applicable
Not
applicable
Can’t say Not
applicable
Can’t say Not
applicable
Not
applicable
Yes
Footnote: BP = breastfeeding peer support, CP = childcare peer support, C = control, I = intervention, FP = facility-based peer support, HP = home-based peer
support, LP = low frequency of peer support, TP = high frequency peer support,

48
Quality Assessment Using SIGN Methodology Checklist for Controlled Trials
Section 2: Overall Assessment
Agrasada et
al. (2005)
Dennis et al.
(2002)
Haider et al.
(2000)
Leite et al.
(2005)
Ochola,
Labadarios &
Nduati. (2013)
Reeder et
al. (2014)
Srinivas et
al. (2015)
Tylleskär et
al. (2011)
Risk of Bias
Minimized
++ + - + - - - -
Overall Effect
due to
Intervention
Alone
Yes Yes Yes Yes Yes Yes Yes Yes
Result
Applicable to
Target Group
Yes Yes Yes Yes Yes Yes Yes Yes
Notes Raise
exclusive
breastfeeding
rate
Extend
breastfeeding
duration
Raise
exclusive
breastfeeding
rate
Extend
breastfeeding
duration
Raise
exclusive
breastfeeding
rate
Raise
exclusive
breastfeeding
rate
Raise
exclusive
breastfeeding
rate
Raise
exclusive
breastfeedin
g rate
Extend
breastfeedin
g duration
Raise
exclusive
breastfeeding
rate
Extend
breastfeeding
duration
Raise
exclusive
breastfeeding
rate
Level of
Evidence
1++ 1+ 1- 1+ 1- 1- 1- 1-

49
Appendix V: Budget Plan
Item Estimated cost (HKD $) per year Subtotal (HKD $)
Decoration of notice board
(promotion of innovation)
100 100
Leaflets (promotion of
innovation)
0 (Free printing in MCHC) 0
Notes 0 (Free printing in MCHC) 0
Certificate of appreciation 0 (Free printing in MCHC) 0
Incentives $100 x 15 peer supporters x 3 rounds) 4,500
One-off preparation time for
training workshop
8 hours x 250 2,000
Extra time needed of running
3 rounds of service in a year
24 hours x 250 6,000
Total 12,600
Potential cost saving per infant
Percentage of exclusive
breastfeeding for 4 months
Disease needing
treatment
Potential cost saving
per infant (£)
Potential cost saving per
infant (HKD $) (correct to
the nearest dollar)
21%
GI
0.92 11
LRTI + AOM
3.47 42
45%
GI
2.49 30
LRTI + AOM
9.44 113
65%
GI
3.81 46
LRTI + AOM
14.41 173
Remarks:
GI = gastrointestinal illness; LRTI = lower respiratory tract infection; AOM = acute otitis media
1£ ⋍ HKD$ 12

50
Number of babies born in 2014 = 62,305
Admission rate of GI in first 3 months = 1.13%
Admission rate of LRTI + AOM in first 3 months = 3.1%
Number of admission due to GI = 62305 x 1.13% = 704 (correct to the nearest people)
Number of admission due to LRTI + AOM = 62305 x 1.13% = 1931 (correct to the nearest people)
Estimated cost saving
Percentage of
exclusive
breastfeeding
for 4 months
Disease Number of
admission
(correct to
the nearest
people)
Potential cost
saving per infant
(HKD$) (correct to
the nearest dollar)
Potential cost
saving
(HKD$)
Total Potential
cost saving
(HKD$)
21%
GI 704 11 7744 88,846
LRTI +
AOM
1931 42 81102
45%
GI 704 30 21120 239,323
LRTI +
AOM
1931 113 218203
65%
GI 704 46 32384 366,447
LRTI +
AOM
1931 173 334063
Remarks:
GI = gastrointestinal illness; LRTI = lower respiratory tract infection; AOM = acute otitis media
Cost-benefit ratio = $12,600 : $239,323
Cost-benefit ratio = 1: 0.05 (Correct to 2 decimal places)

51
Appendix VI: Grade of Recommendations
(Scottish Intercollegiate Guidelines Network, 2011)
Grade A At least one meta-analysis, systematic review, or RCT rated as
1++, and directly applicable to the target population; or
a body of evidence consisting principally of studies rated as
1+, directly applicable to the target population, and
demonstrating overall consistency of results
Grade B A body of evidence including studies rated as 2++, directly
applicable to the target population, and demonstrating overall
consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
Grade C A body of evidence including studies rated as 2+, directly
applicable to the target population, and demonstrating overall
consistency of results; or
Extrapolated evidence from studies rated as 2++
Grade D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
Grade E Recommended best practice based on the clinical experience
of the guideline development group

52
Appendix VII: Practicing Guideline
Guidelines for breastfeeding peer support service
Aim: To provide guidance to staff when deliver of peer support
service
Objectives: To build a breastfeeding friendly environment in the
community
To promote breastfeeding and prolong breastfeeding
duration of pregnant women
To support breastfeeding mothers in community
Setting: MCHC
Target users: MCHC staffs
Recommendation
1. Target mothers should not include those with history of
mental illness
(Grade A)
Available evidence:
Mothers taking medications that may compromise
breastfeeding were excluded. (Agrasada et al., 2005; Haider
et al., 2000)(1++)
Mothers were excluded if they had a factor that could
significantly interfere with breastfeeding. (Dennis et al.,
2002 (1+) ; Ochola, Labadarios & Nduati, 2013 (1-) ;
Tylleskär et al., 2011 (1-) )
Discussion:
Breastfeeding is a stressful event for mothers especially at the
first few days before “milk come in”. Together with hormonal
changes after delivery, their mood may fluctuate a lot.
Professional support rather than peer support is more suitable for
these clients.

53
Recommendation
2. Target mothers should deliver of a singleton baby
(Grade A)
Available evidence:
Mothers were eligible if they had delivered a singleton.
(Agrasada et al., 2005 (1++) ; Dennis et al., 2002 (1+) ;
Tylleskär et al., 2011 (1-) )
Mothers were excluded in cases of multiple births. (Haider
et al., 2000 (1-) ; Leite et al., 2005 (1+) )
Discussion:
Mothers of twins or multiple births usually already have more
support than those who deliver a singleton. Also peer supporters
may not have experience in breastfeeding of twins or multiple
babies.
Recommendation
3. Peer supporters should have breastfeeding experience
(Grade A)
Available evidence:
Selected breastfeeding peer supporter had previous positive
personal breastfeeding experience. (Agrasada et al.,
2005(1++) ; Haider et al., 2000 (1-) ; Leite et al., 2005
(1+) )
Selection criteria of peer supporters: previous breastfeeding
experience of at least 6 months’ duration. (Dennis et al.,
2002 (1+) ; Reeder et al., 2014 (1-) )
Discussion:
With personal breastfeeding experience, peer supporters would
be easier to understand the feeling of breastfeeding mothers and
the difficulties they encounter. Thus peer supporters can act as
role model of successful breastfeeding.

54
Recommendation
4. Peer supporters should be trained before providing the
service
(Grade A)
Available evidence:
40 hours of training was provided for training of peer
supporters. (Agrasada et al., 2005 (1++) ; Haider et al.,
2000 (1+) ; Ochola, Labadarios & Nduati., 2013 (1-) ).
Selection criteria of peer supporters: completion of a 2.5
hours orientation session. (Dennis et al., 2002) (1+)
Peer supporters participated in a 20 hours breastfeeding
training course. (Leite et al., 2005) (1+)
Training was provided to peer supporters. (Reeder et al.,
2014) (1-)
Peer supporters were trained for 1 week by the national
research teams. (Tylleskär et al., 2011) (1-)
Discussion:
Training prior to service boosts peer supporters confidence in
providing the service. Also, it unifies how the supporters to
provide the support.
Recommendation
5. Content of the training should include breastfeeding
benefits, breastfeeding positioning and attachment,
identification of feeding cues, effective suckling and social
skills
(Grade A)
Available evidence:
The orientation session included telephone support and
referral skills while the handbook incorporated various
topics such as breastfeeding benefits, general breastfeeding
information and principles and breastfeeding myths.
(Dennis et al., 2002) (1+)
Parts of the WHO/UNICEF breastfeeding counselling
course were used as guides. (Haider et al., 2000 (1-) ;
Ochola, Labadarios & Nduati, 2013 (1-) ; Tylleskär et al.,
2011 (1-) )
Training course adapted from “Breastfeeding counselling: a

55
training course” (Leite et al., 2005) (1+)
The training covered technical breastfeeding topics,
methods of providing peer support, scope of practice and
the benefits of breastfeeding. (Reeder et al., 2014) (1-)
Discussion:
Content of the training should be practical and applicable to real
life situations that facilitate peer supporters to provide the
service.
Recommendation
6. Peer support service should be started at third trimester
of pregnancy
(Grade C)
Available evidence:
First visit started in the third trimester of pregnancy.
(Haider et al., 2000 (1-) ; Ochola, Labadarios & Nduati,
2013 (1-) ; Tylleskär et al., 2011 (1-) )
Discussion:
Time is needed for peer supporters and target mothers to build
up rapport. Also, maternal leave usually starts at third trimester
so that target mothers have time to meet up with their peer
supporters.
Recommendation
7. Peer support service should be provided within 1 week
after delivery
(Grade A)
Available evidence:
The first home visit started at infant age day 3-5. (Agrasada
et al., 2005) (1++)
Peer supporters were asked to contact the new mother
within 48 hours after hospital discharge. (Dennis et al.,
2002) (1+)
One visit provided within 48 hours of delivery. (Haider et
al., 2000) (1-)

56
First home visit was on the 5th
day from birth. (Leite et al.,
2005) (1+)
One visit or call was during the first week after delivery.
(Ochola, Labadarios & Nduati, 2013 (1-) ; Reeder et al.,
2014 (1-) ; Tylleskär et al., 2011 (1-) )
Discussion:
Breastfeeding problems may arise as soon as baby starts feeding.
So target mothers, especially those without breastfeeding
experience before, need support as soon as they deliver
Recommendation
8. Contact frequency should be intense when baby first
born and sparse as time passed by
(Grade A)
Available evidence:
Eight home visits were scheduled at infant age days 3-5, 7-10,
21 and at 1.5 month and then monthly up to 5.5 month.
(Agrasada et al., 2005) (1++)
Four visits were in the first month of delivery, then monthly
between months 2 and 5. (Haider et al., 2000) (1-)
Six home visit were on 5th
day from birth, 15th
, 30th
, 60th
, 90th
and 120th
. (Leite et al., 2005) (1+)
First visit was in third trimester, then first week after delivery
and then monthly up to 5 months. (Ochola, Labadarios &
Nduati, 2013) (1-)
2 calls were at antenatal, then at 1st and 2
nd week of postpartum
and then monthly up to 4 months. (Reeder et al., 2014) (1-)
Discussion:
As time pass by, mothers learn the feeding habit of their babies
and are more skillful in breastfeeding than before. So the contact
frequency can be decreased.
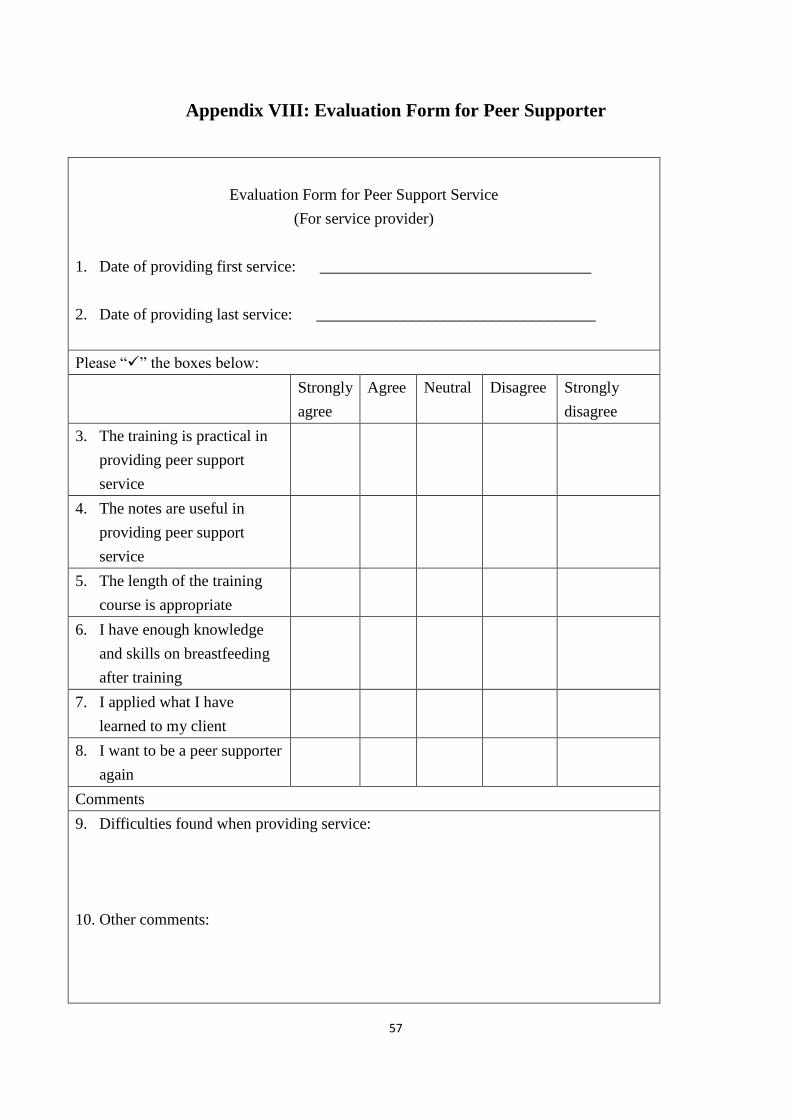
57
Appendix VIII: Evaluation Form for Peer Supporter
Evaluation Form for Peer Support Service
(For service provider)
1. Date of providing first service: __________________________________
2. Date of providing last service: ___________________________________
Please “” the boxes below:
Strongly
agree
Agree Neutral Disagree Strongly
disagree
3. The training is practical in
providing peer support
service
4. The notes are useful in
providing peer support
service
5. The length of the training
course is appropriate
6. I have enough knowledge
and skills on breastfeeding
after training
7. I applied what I have
learned to my client
8. I want to be a peer supporter
again
Comments
9. Difficulties found when providing service:
10. Other comments:

58
Appendix IV: Evaluation Form for Service Recipient
Evaluation Form for Peer Support Service
(For service recipient)
1. Date of receiving first service: __________________________________
2. Date of receiving last service: ___________________________________
Please “” the boxes below:
Strongly
agree
Agree Neutral Disagree Strongly
disagree
3. My peer supporter is nice
and friendly
4. My peer supporter is helpful
5.
6. The frequency of contact is
appropriate
7. I learned knowledge and
skills on breastfeeding from
my peer supporter
8. I am satisfied with the peer
support service
9. I will recommend this
service to my friends
Comments:
10. Difficulties found when providing service:
11. Other comments:


















