Evar in inflammatory aaa
33
EVAR in Inflammatory AAA Fady Haddad, MD, FACS Vascular & Endovascular Surgery American University Of Beirut Medical Center ASVS, Turkish Society & Asian Venous Forum meeting Istanbul, October 2013
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
206 -
download
0
Transcript of Evar in inflammatory aaa

EVAR inInflammatory AAA
Fady Haddad, MD, FACSVascular & Endovascular Surgery
American University Of Beirut Medical Center
ASVS, Turkish Society & Asian Venous Forum meeting
Istanbul, October 2013

Inflammatory AAA
• EVAR has changed the way we look at AAA.
• More than 50 % of overall cases in the US today are done using endovascular approach.
• Large data supports at least early and mid term reduced mortality & morbidity, particularly in high risk patients. 1, 2, 3
1.Giles KA, et al. Decrease in total aneurysm-related deaths in the era of endovascular aneurysm repair. J Vasc Surg
2009;49:543-51.
2.Schermerhorn ML et al. Endovascular vs. open repair of abdominal aortic aneurysms in the medicare population.
N Engl J Med 2008; 358:464-47.
3.Greenhald R et al. Endovascular Repair of Abdominal Aortic Aneurysm. N Engl J Med 2008; 358:494-501.

• Inflammatory AAA (I-AAA) constitutes around 5% of all AAA.
• It carries its own challenges in terms of anatomic and technical difficulties, procedural morbidity, and associated retroperitoneal fibrosis and inflammation.
• Little is known about singularities of this disease in the endovascular era
• Recent literature suggests efficiency and safety of EVAR in I-AAA .*
*Coppi G, et al. Inflammatory Abdominal Aortic Aneurysm Endovascular Repair into the Long-Term Follow-Up. Ann Vasc Surg. 2010; 24(8):1053-9
Inflammatory AAA

• 67 y male, smoker
• Back pain 6 month
• Hx of spine disease
• US abdomen AAA5.5cm
• CT angio: – 5.5cm AAA with
periaortic inflammation up to 7cm
– Bilateral hydronephrosismore on the left.
Inflammatory AAA
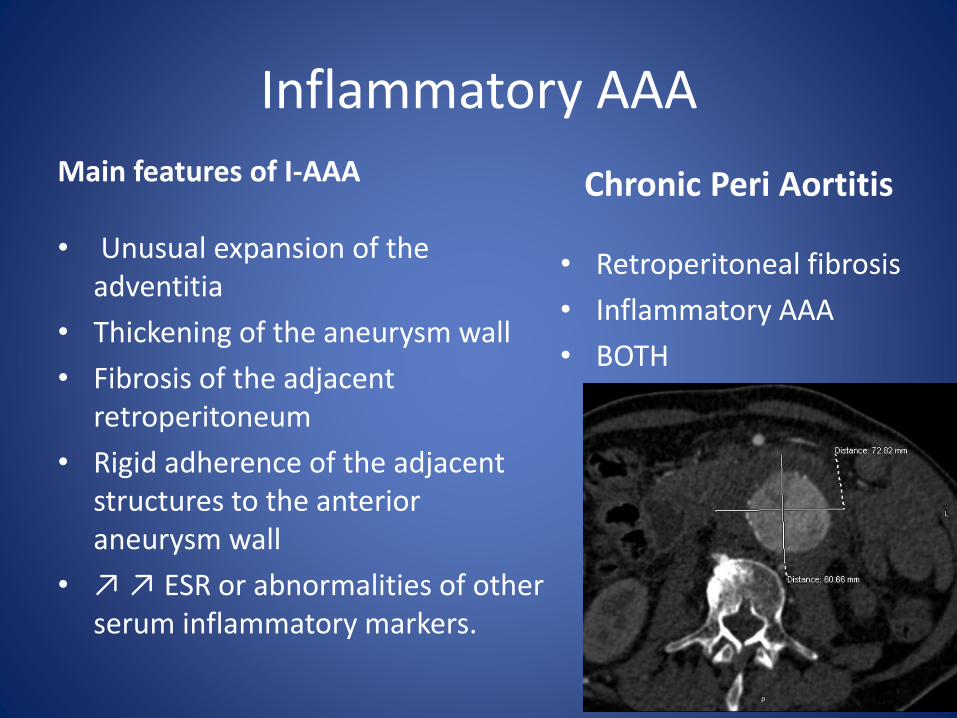
Main features of I-AAA
• Unusual expansion of the adventitia
• Thickening of the aneurysm wall
• Fibrosis of the adjacent retroperitoneum
• Rigid adherence of the adjacent structures to the anterior aneurysm wall
• ↗ ↗ ESR or abnormalities of other serum inflammatory markers.
Chronic Peri Aortitis
• Retroperitoneal fibrosis
• Inflammatory AAA
• BOTH
Inflammatory AAA

Relevant lab results:
– CRP 83mg/l (Nl <5)
– ESR 100mm first hour
– Creatinine 1.4mg/dl
– ANA, C-ANCA, p-ANCA negative
– Urine Cx negative
Double J stenting

Copyright © 2012 American Medical
Association. All rights reserved.
From: Inflammatory Abdominal Aortic Aneurysm
JAMA. 2007;297(4):395-400. doi:10.1001/jama.297.4.395

Treatment of I-AAA
• The aim of surgical treatment is to prevent rupture.
• Data suggest that an inflammatory AAA is less liable to rupture.*
• Intervention appears prudent once the diameter exceeds 5.5 cm.
*Lindblad B, Almgren B, Bergqvist D, et al. Abdominal aortic aneurysm with perianeurysmalfibrosis: experience from 11 Swedish vascular centers. J Vasc Surg. 1991;13:231-239.

• Open repair for I-AAA remain a very challenging surgery.
• Complication rates are still slightly higher than atherosclerotic aneurysm*
• Over the past decade, outcome has significantly improved with better knowledge of the disease and some modifications of the technique.*
* Hellmann DB, Grand DJ, Freischlag JA. JAMA 2007; 297(4):395-400
Inflammatory AAA
*Lindblad B et al. J Vasc Surg. 1991;13:231-239.

• EVAR recently reported to adequately exclude the I-AAA and reduce the size of the sac.
• Review of the Eurostardata on I-AAA cases:– No difference in technical
success in anatomically suitable cases with ~90% sac ↘
– No difference in Mortality 1.9 vs 2.2% (NS)
C. Lange et al, On Behalf of the EUROSTAR Collaborators: Results of Endovascular Repair of Inflammatory Abdominal Aortic Aneurysms. A Report from the EUROSTAR Database Eur J Vasc Endovasc Surg 29, 363–370 (2005
Inflammatory AAA

C. Lange et al, On Behalf of the EUROSTAR Collaborators: Results of Endovascular Repair of Inflammatory Abdominal Aortic Aneurysms. A Report from the EUROSTAR Database Eur J Vasc Endovasc Surg 29, 363–370 (2005)

Procedural details and outcomes (Eurostar)
Inflammatory 52
Non-Inflammatory 3613
P-
Device related Complications
6(11.5%) 261(7.2%) 0.16
Device Migration 0(0.0%) 48(1.3%)
Device Limb Stenosis/occlusion
2 (3.9%) 9 (0.3%) 0.0005
IIA occlusion 13 (25.0%) 488 (13.5%) 0.01
Mortality<30d 1 (1.9%) 81 (2.2%) 0.66
C. Lange et al, On Behalf of the EUROSTAR Collaborators: Results of Endovascular Repair of Inflammatory Abdominal Aortic Aneurysms. A Report from the EUROSTAR Database Eur J Vasc Endovasc Surg 29, 363–370 (2005)

• This patient underwent EVAR 2 days after bilateral ureteral stenting.
• Zenith flex endograft was used.
• No endoleaks on completion.
• Still no or very little excretion from the left kidney.

EVAR for I-AAA: follow up
• Longest F/U in the literature , favourable reduction in periaortitisand sac diameter
• Tech success 100%
• Sac reduction 89%
• PAF ↘ or resolved in 77% and the rest unchanged.
• No endoleaks at F/U
• ! Hydronephrosispersisted when it was present.
Coppi G, et al. Inflammatory Abdominal Aortic Aneurysm Endovascular Repair into the Long-Term Follow-Up. Ann Vasc Surg. 2010; 24(8):1053-9

• Trend toward lower mortality and complications in EVAR for I-AAA is becoming solid; however is it enough?
• Hydronephrosis, does seem to respond less or SLOWER to EVAR*;
I-AAA Preop Early Late
11 Patient 5 (45%) 4 (36%) 3 (27%)
*Van Bommel EF, et al. Persisitent chronic peri-aortitis (‘inflammatory aneurysm’) after AAA repair: systemic review of the literature. Vasc Med 2008; 13 (4):293-303
Additional info on 11 patients from Eurostar

• Persistent PAF and hydronephrosis is a source of morbidity and increased mortality.
• Substantial targets for success should include the treatment of ureteral obstruction and regression of periaortic fibrosis.
*Van Bommel EF, et al. Persisitent chronic peri-aortitis (‘inflammatory aneurysm’) after AAA repair: systemic review of the literature. Vasc Med 2008; 13 (4):293-303

• Is EVAR a safer option for patients with peri-aneurysmal fibrosis? The debate still stands.
• To balance this, available data suggests that additional medical treatment should be considered at an earlier stage with EVAR
EFH van Bommel et al. Persistent peroartitis after AAA repair: systematic review.Vascular Medicine 2008; 13: 293–303
• Steroids therapy remain the backbone, with objective evidence of improvement.
– Side effects of long term steroids
– Some patients may not respond
• Corticosteroid-sparing agents, such as methotrexate, cyclophosphamide, and azathioprine, have also been reported effective.
Hellmann DB, Grand DJ, Freischlag JA. Inflammatory Abdominal Aortic Aneurysm. JAMA2007; 297(4):395-400.
I-AAA: medical therapy

I-AAA: medical therapy
• Chronicity of the PAF seems to be important in the response:*
– Old vs Yong PAF
• Cell to Fibrosis ratio<1 tends to respond less or slower
*Stella, A, et al. Postoperative course of inflammatory abdominal aortic aneurysms.
Ann Vasc Surg 1993; 7 (3): 229–238.
4 months F/U

• Our patient here was initiated on steroid– Initially 30mg daily
• Developped DM • Azathioprine added at 3
months to reduced the steroid– 50mg daily
• Patient developed neutropenia and UTI.
• Immunosuppressant stopped. Steroids tapered to 10mg and shortly after stopped.
• Addition or alternative to steroid therapy:– Azathioprine– Tamoxifen:*
• Anti-inflammatory• Anti Oxidant• Antiproliferative• Cardioprotective effect
• No available guidelines to help in the role or duration of those agents
I-AAA: medical therapy
Van Bommel et al. Tamoxifen therapy for nonmalignant retroperitoneal fibrosis. Ann ntern Med 2006;144:101-106

PAF and urinary obstruction
• In 15-30 % of I-AAA one or both ureterscould be involved
• Combination of renal drainage to medical therapy is important in some cases*
• Poor responders may have recurrent hydronephrosis.
*Deleersnijder R, et al. Endovascular Repair of Inflammatory Abdominal Aortic Aneurysms with Special Reference to Concomitant Ureteric Obstruction. Eur J VascEndovasc Surg 2002: 24 (2):146-149
6 Months F/U

Evolution PAF & Ureteral ObstructionOpen vs Endo
EFH van Bommel et al. Persistent peroartitis after AAA repair: systematic review.Vascular Medicine 2008; 13: 293–303

Follow up after I-AAA treatment
• Persistent PAF (no regression)
– 14% after open repair
– Up to 40% after EVAR (p<0.0001)
• Persistent Ureteral obstruction more frequent after EVAR than after open repair (56% vs32%, p=0.09)*
• Time to regression of PAF, at least 4-6 months.
*Amongs patients who had it; excluding those with ureterolysis.
EFH van Bommel et al. Persistent peroartitis after AAA repair: systematic review.Vascular Medicine 2008; 13: 293–303

• EVAR offers reduced perioperative morbidity and mortality, specially in I-AAA.*
• Draw-back seems to be higher persistent or slower regression of PAF and Ureteral obstruction
• Watchful waiting before initiating medical therapy is accepted after open repair
• May not be the case after EVAR**
*Lindblad B et al. J Vasc Surg. 1991;13:231-239.*Ockert et al, Long term outcome of operated I-AAA. Vascular 2006;14;206211
**EFH van Bommel et al. Vascular Medicine 2008; 13: 293–303
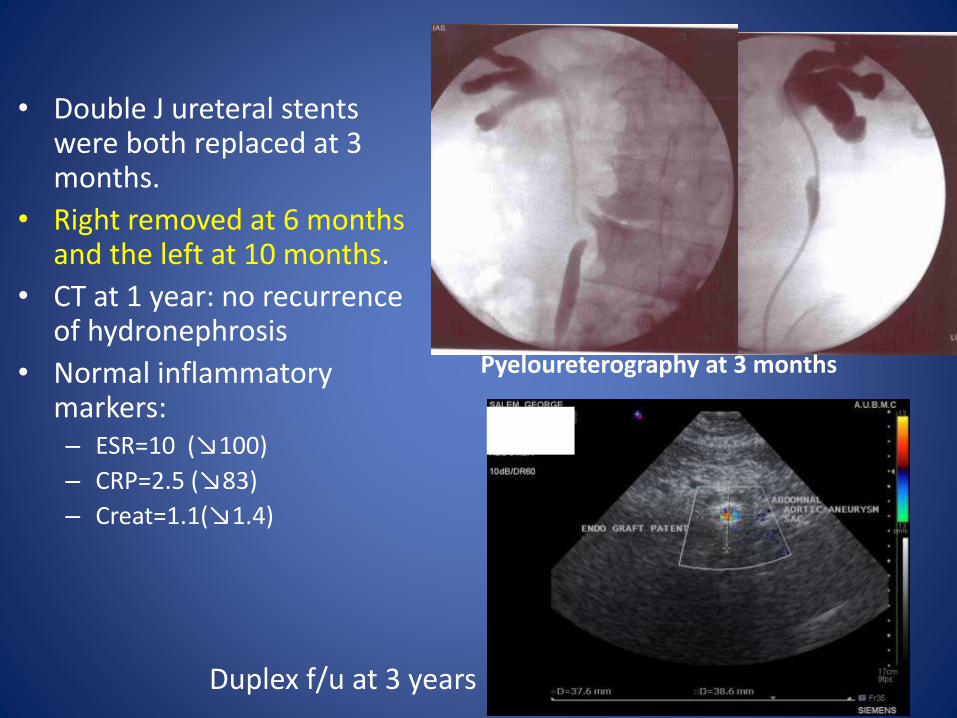
• Double J ureteral stents were both replaced at 3 months.
• Right removed at 6 months and the left at 10 months.
• CT at 1 year: no recurrence of hydronephrosis
• Normal inflammatory markers:– ESR=10 (↘100)
– CRP=2.5 (↘83)
– Creat=1.1(↘1.4)
Pyeloureterography at 3 months
Duplex f/u at 3 years

• After EVAR– Low threshold for urinary drainage (Stents or PNS)
– Early initiation of medical therapy (steroids, Azathioprine, Tamoxifen, combinations) may balance the higher post operative PAF.
• Most available data comes from registries and retrospective studies. Still no clear cut recommendation.
• ?Ground for a prospective study specifically looking at I-AAA?
Follow up after I-AAA treatment

• Concerns:
– In this era of endovascular thrive, will surgeons accept to randomize and subject anatomically suitable patients to an open repair
– In the hands of new generation vascular specialists, more exposed to EVAR, will we have outcomes in I-AAA comparable to historical series done by more experienced “open” surgeons.

In summary,
• EVAR is effective and safe for I-AAA
• Procedural success and aneurysm shrinkage comparable to atherosclerotic aneurysms
• Both Retroperitoneal fibrosis and Ureteralobstruction, when present respond significantly less than with open repair
• Low threshold for ureteral drainage
• Early medical treatment may balance the persistent RPF

The Cedars, February 2012



EFH van Bommel et al. Persistent peroartitis after AAA repair: systematic review.Vascular Medicine 2008; 13: 293–303

• CT scan done 7 months in this patient showed significant reduction in peria