Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in ......Acute stent thrombosis. The 1 case...
4
250 The Journal of Invasive Cardiology ® Original Contribution Brief Communication Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in the Setting of Percutaneous Coronary Intervention Phillip A. Weeks, PharmD, BCPS 1 , Haider M. Alkhateeb, MD 2 , Stephen E. Michaud, PharmD, BCPS 1 , Jose G. Diez, MD 3 ABSTRACT: Background. Bivalirudin has emerged as a suitable alternative anticoagulant to unfractionated heparin and low-molecu- lar-weight heparins during percutaneous coronary intervention (PCI) procedures in the management of coronary artery disease and acute coronary syndromes (ACS). In clinical trials, bivalirudin dosing was standardized, and activated clotting time (ACT) did not influence dosing adjustments. The role of ACT monitoring of bivalirudin in PCI is not defined based on current practice guidelines. Hypothesis. The hypothesis of this study is that hyper- and hypo-ACT responses to bivalirudin in PCI may be associated with excessive bleeding or thrombotic complications. Methods. The planned protocol screened all patients who received bivalirudin therapy and ACT monitoring during PCI in a single center’s cardiac catheterization laboratory from July 2009 to June 2010. The first ACT monitored 5 to 60 minutes af- ter bivalirudin initiation was screened for inclusion. Values above 800 seconds and below 300 seconds were included as hyper- and hypo- ACT responses, respectively. Outcomes assessed include thrombotic and bleeding complications. Results. There were 32 patients identi- fied as hyper-responders and 20 patients identified as hypo-respond- ers. There were no significant thrombotic or bleeding complications in the hyper-responder group. There was 1 case (1/20, 5%) of angio- graphically confirmed acute stent thrombosis immediately following the placement of 5 adjoining bare-metal stents in the right coronary artery of a hypo-responder. Conclusions. Hyper-ACT responses to bi- valirudin therapy in PCI were not associated with additional bleeding risk. Bivalirudin may not adequately protect hypo-ACT responders against thrombotic complications during PCI. J INVASIVE CARDIOL 2013;25(5):250-253 Key words: acute coronary syndromes, anticoagulation Coronary artery disease (CAD) remains one of the most sig- nificant contributors to morbidity and mortality in the United States and around the world, and a significant portion of pa- tients with stable CAD and acute coronary syndrome (ACS) will undergo percutaneous coronary intervention (PCI) procedures at some point to treat this disease. Current guidelines for PCI recommend a combination of antithrombotic and antiplatelet medication therapies to treat ongoing ischemia or infarction and minimize peri- and postprocedural thrombotic complications. 1-4 Traditionally, unfractionated heparin and low-molecular weight-heparins (LMWHs), such as enoxaparin, have been used as anticoagulant agents during PCI, but bivalirudin, a bivalent intravenous direct thrombin inhibitor, has emerged as an alterna- tive anticoagulant with similar efficacy and less major bleeding. 5-9 Importantly, the study protocols spared routine glycopro- tein IIb/IIIa inhibitor (GPI) use with bivalirudin, allowing it provisionally compared to routine use of GPI in the groups receiving unfractionated heparin and LMWH. The dosing strategies utilized in the studies evaluating bivalirudin use in PCI were standardized doses without dose adjustment recom- mendations for activated clotting times (ACTs) assessed. Un- fractionated heparin infusions are recommended to be adjusted based on ACT values depending on the use of GPI and the device used to assess the ACT. 1-3 Heparin dosing should be adjusted to an ACT range of 200- 250 seconds in patients receiving GPI regardless of the device used. In patients not receiving GPI, ACT target ranges of 250-300 or 300-350 seconds should be used when assessed by the Hemotec or Hemochron devices, respectively. Current Food and Drug Admin- istration (FDA) approval for bivalirudin use in PCI suggests that an ACT be performed 5 minutes after the 0.75 mg/kg bolus dose and a 0.3 mg/kg additional bolus dose be administered if needed 10 ; however, there is no guidance regarding what value of ACT war- rants an additional bolus and the utility of ACT monitoring in bivalirudin therapy remains uncertain in the setting of PCI. Limitations of ACT monitoring of bivalirudin therapy have been demonstrated previously, with the correlation between From the Departments of 1 Pharmacology, 2 Internal Medicine, and 3 Cardiology, St Luke’s Episcopal Hospital, Houston, Texas, Texas Heart Institute, Houston, Texas. Disclosure: The authors have completed and returned the ICMJE Form for Dis- closure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein. Manuscript submitted October 22, 2012, provisional acceptance given December 3, 2012, final version accepted December 12, 2012. Address for correspondence: Haider Alkhateeb, MD, Texas Tech University Health Sciences Center, Internal Medicine, 4800 Alberta Avenue, El Paso, TX 79905. Email: [email protected] Figure 1. Study flow chart showing inclusion and exclusion criteria. ACT = activated clotting time; PCI = percutaneous coronary intervention. For Personal Use. Copyright HMP 2013
Transcript of Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in ......Acute stent thrombosis. The 1 case...

250 The Journal of Invasive Cardiology®
Original ContributionBrief Communication
Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in the Setting of Percutaneous Coronary Intervention
Phillip A. Weeks, PharmD, BCPS1, Haider M. Alkhateeb, MD2, Stephen E. Michaud, PharmD, BCPS1,Jose G. Diez, MD3
ABSTRACT: Background. Bivalirudin has emerged as a suitable alternative anticoagulant to unfractionated heparin and low-molecu-lar-weight heparins during percutaneous coronary intervention (PCI) procedures in the management of coronary artery disease and acute coronary syndromes (ACS). In clinical trials, bivalirudin dosing was standardized, and activated clotting time (ACT) did not influence dosing adjustments. The role of ACT monitoring of bivalirudin in PCI is not defined based on current practice guidelines. Hypothesis. The hypothesis of this study is that hyper- and hypo-ACT responses to bivalirudin in PCI may be associated with excessive bleeding or thrombotic complications. Methods. The planned protocol screened all patients who received bivalirudin therapy and ACT monitoring during PCI in a single center’s cardiac catheterization laboratory from July 2009 to June 2010. The first ACT monitored 5 to 60 minutes af-ter bivalirudin initiation was screened for inclusion. Values above 800 seconds and below 300 seconds were included as hyper- and hypo-ACT responses, respectively. Outcomes assessed include thrombotic and bleeding complications. Results. There were 32 patients identi-fied as hyper-responders and 20 patients identified as hypo-respond-ers. There were no significant thrombotic or bleeding complications in the hyper-responder group. There was 1 case (1/20, 5%) of angio-graphically confirmed acute stent thrombosis immediately following the placement of 5 adjoining bare-metal stents in the right coronary artery of a hypo-responder. Conclusions. Hyper-ACT responses to bi-valirudin therapy in PCI were not associated with additional bleeding risk. Bivalirudin may not adequately protect hypo-ACT responders against thrombotic complications during PCI.
J INVASIVE CARDIOL 2013;25(5):250-253
Key words: acute coronary syndromes, anticoagulation
Coronary artery disease (CAD) remains one of the most sig-nificant contributors to morbidity and mortality in the United States and around the world, and a significant portion of pa-tients with stable CAD and acute coronary syndrome (ACS) will undergo percutaneous coronary intervention (PCI) procedures at some point to treat this disease. Current guidelines for PCI recommend a combination of antithrombotic and antiplatelet medication therapies to treat ongoing ischemia or infarction and minimize peri- and postprocedural thrombotic complications.1-4
Traditionally, unfractionated heparin and low-molecular weight-heparins (LMWHs), such as enoxaparin, have been used as anticoagulant agents during PCI, but bivalirudin, a bivalent intravenous direct thrombin inhibitor, has emerged as an alterna-tive anticoagulant with similar efficacy and less major bleeding.5-9
Importantly, the study protocols spared routine glycopro-tein IIb/IIIa inhibitor (GPI) use with bivalirudin, allowing it provisionally compared to routine use of GPI in the groups receiving unfractionated heparin and LMWH. The dosing strategies utilized in the studies evaluating bivalirudin use in PCI were standardized doses without dose adjustment recom-mendations for activated clotting times (ACTs) assessed. Un-fractionated heparin infusions are recommended to be adjusted based on ACT values depending on the use of GPI and the device used to assess the ACT.1-3
Heparin dosing should be adjusted to an ACT range of 200-250 seconds in patients receiving GPI regardless of the device used. In patients not receiving GPI, ACT target ranges of 250-300 or 300-350 seconds should be used when assessed by the Hemotec or Hemochron devices, respectively. Current Food and Drug Admin-istration (FDA) approval for bivalirudin use in PCI suggests that an ACT be performed 5 minutes after the 0.75 mg/kg bolus dose and a 0.3 mg/kg additional bolus dose be administered if needed10; however, there is no guidance regarding what value of ACT war-rants an additional bolus and the utility of ACT monitoring in bivalirudin therapy remains uncertain in the setting of PCI.
Limitations of ACT monitoring of bivalirudin therapy have been demonstrated previously, with the correlation between
From the Departments of 1Pharmacology, 2Internal Medicine, and 3Cardiology, St Luke’s Episcopal Hospital, Houston, Texas, Texas Heart Institute, Houston, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Dis-closure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 22, 2012, provisional acceptance given December 3, 2012, final version accepted December 12, 2012.
Address for correspondence: Haider Alkhateeb, MD, Texas Tech University Health Sciences Center, Internal Medicine, 4800 Alberta Avenue, El Paso, TX 79905. Email: [email protected]
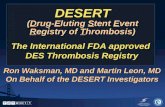
Figure 1. Study flow chart showing inclusion and exclusion criteria. ACT = activated clotting time; PCI = percutaneous coronary intervention.
For Personal Use.
Copyright HMP 2013

Vol. 25, No. 5, May 2013 251
Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in the Setting of PCI
bivalirudin plasma concentration and activity not accurately reflected by the ACT value.11
An analysis of four PCI clinical trials conducted to assess the correlation of ischemic and thrombotic complications with dif-ferent quartiles of maximum ACT values in response to unfrac-tionated heparin previously demonstrated no association with thrombotic complications, but an increase in minor bleeding as ACT values increase.12
The purpose of the present study was to evaluate the clinical outcomes associated with hyper-ACT (>800 seconds) and hypo-ACT (<300 seconds) responses to bivalirudin therapy during PCI.
MethodsStudy design. This study was a single-center retrospec-
tive observational analysis of the documented outcomes among patients receiving bivalirudin anticoagulation dur-ing PCI. The research protocol was approved by the institu-tional review board of St Luke’s Episcopal Hospital, and the
requirement for informed consent and patient authorization was waived. Research was conducted in compliance with stan-dards set forth in the Declaration of Helsinki.
Study population and procedures. All patients undergo-ing PCI who received bivalirudin anticoagulation from July 2009 to June 2010 and had an ACT assessed 5-60 minutes after bivalirudin bolus of <300 seconds or >800 seconds were in-cluded. Patients were excluded if they did not receive any inter-vention at the time of their catheterization (angiography only), they did not receive bivalirudin anticoagulation, they had ini-tial ACT responses of 300-800 seconds, or they did not receive ACT monitoring 5-60 minutes after bivalirudin initiation.
Figure 1 describes this inclusion and exclusion criteria, in-cluding the number of patients falling into each group. Patients were originally identified for inclusion from a database main-tained by the cardiac catheterization laboratory at the study in-stitution. After patient identification, pharmacy software and electronic medical record data were reviewed to evaluate the clinical outcomes of interest.
Endpoints. The primary outcomes assessed for hyper-re-sponders include TIMI-defined minor and major bleeding and GUSTO-defined moderate and severe bleeding.13 Transfusion of blood products to treat bleeding or anemia following PCI was also assessed. The primary outcomes assessed for hypo-re-sponders include thrombotic complications of stent thrombosis and periprocedural myocardial infarction. Definitions utilized for stent thrombosis include the criteria adopted by the Aca-demic Research Consortium describing early, late, or very late and definite, probable, or possible.14
Statistical analysis. Descriptive statistics were utilized as there was no need for comparative statistical analysis based on the type of study performed. All ACT events described are rep-resented graphically by data points on scatter plots. Clinical events associated with hyper- and hypo-ACT responses were to be described in greater detail.
ResultsA total of 833 patients were identified for screening from the
cardiac catheterization laboratory system to have received bivali-rudin during PCI with an ACT assessed 5-60 minutes after bi-valirudin initiation. We excluded 781 of these patients for having “normal” responses to bivalirudin by study criteria with ACT val-ues of 300-800 seconds. Twenty patients (2.4%) were identified as hypo-responders and 32 (3.8%) as hyper-responders from the 833 eligible patients screened. The baseline characteristics, PCI procedures performed, and use of other antithrombotic agents peri- and postprocedurally are reported in Table 1.
Outcomes among hypo-responders. Of the 20 patients identified as hypo-responders, there was 1 documented case (5%) of angiographically confirmed definite acute stent throm-bosis based on criteria established by the Academic Research Consortium.14 The details of this episode are documented in a subsequent section. There were no deaths prior to hospital dis-charge in any patients in the hypo-responder group, and there were no noted TIMI minor or major or GUSTO moderate or severe bleeding events in the hypo-responder patients. The hy-po-responder events are graphically displayed in Figure 2.
Figure 2. Scatter plot showing hypo activated clotting times.
Figure 3. Scatter plot showing hyper-activated clotting times.
Figure 4. Scatter plot showing the time frame (in minutes) of medication administration to activated clotting time (ACT) values recorded.
For Personal Use.
Copyright HMP 2013

252 The Journal of Invasive Cardiology®
WEEKS, et al.
Outcomes among hyper-responders. Of the 32 patients identified as hyper-responders, there were no TIMI minor or major bleeding events. There were also no GUSTO moderate or severe bleeding events. No patients in this group required the transfusion of any blood products to treat bleeding or ane-mia following PCI, and no deaths were observed prior to dis-charge from the hospital. There were no noted postprocedural thrombotic complications in the hyper-responder patients. The hyper-responder events are graphically displayed in Figure 3.
Acute stent thrombosis. The 1 case of definite acute stent thrombosis occurred in a 58-year-old Hispanic male originally presenting to the hospital with a recent acute coronary syndrome for a staged PCI procedure. It was de-termined that his right coronary artery had the most severe disease and this would be the first target of intervention. The patient was premedicated with prasugrel 60 mg and was taking aspirin daily prior to admission. The patient received a 0.75 mg/kg intravenous bolus dose of bivalirudin followed
by a 1.75 mg/kg/hour infusion. Five inter-locking bare-metal stents were deployed to revascularize the two 90% stenosed lesions in the mid and distal segments of the right coronary artery, and at the time following deployment of stents the best TIMI flow grade achieved was estimated at TIMI 2 flow. No ACT was assessed during the ini-tial portion of the procedure.
The patient was brought into the post-procedure recovery area and began to expe-rience severe chest pain accompanied by sig-nificant ST-segment elevations. The patient was immediately brought back to the cath-eterization lab, where it was angiographi-cally determined that the recently stented right coronary artery had thrombosed at the proximal segment of the stented ter-ritory. Bivalirudin therapy was reinitiated with a 0.75 mg/kg bolus followed by a 1.75 mg/kg/hour infusion. During this stage of the procedure, the ACT was assessed mul-tiple times, four of which were below 300 seconds. An intracoronary abciximab 0.25 mg/kg bolus dose was administered, fol-lowed ultimately by an intravenous bolus of 8000 units of unfractionated heparin. The ACT assessed after the dose of unfraction-ated heparin achieved an ACT response >300 seconds. The right coronary artery was not adequately revascularized by ex-tensive efforts to eliminate and control the thrombosis. The time frame of medication administration to ACT values recorded is represented in Figure 4.
The procedure was eventually termi-nated and the patient was transferred to the coronary care unit in stable condition.
DiscussionAlthough there are no specific recommendations to guide the
adjustment of bivalirudin dosing in current PCI guidelines, ACT monitoring continues to be a common, yet not routine practice among many cardiovascular interventionalists performing PCI procedures when bivalirudin is the chosen anticoagulant. Product labeling suggests consideration of an additional 0.3 mg/kg bolus dose if needed based on the ACT assessed, but the goal ACT tar-get is not specified.10 Due to the highly variable responses noted between patients given a standard dosing regimen of bivalirudin in PCI and the poor correlation of bivalirudin and ACT demon-strated in previous studies, the clinical question of what signifi-cance these ACT values may have on outcomes was raised.
This study was undertaken to analyze any complications that may be associated with extremely high or low ACT values as-sessed after initiation of bivalirudin therapy. Prior to the study initiation, it was expected that extremely high ACT values would potentially be associated with greater bleeding complications and
Table 1. Baseline characteristics.
Characteristic Hypo-Responders (n = 20)
Hyper-Responders (n = 32)
Past medical history
Hypertension 11 (55%) 23 (79.1%)
Diabetes mellitus 4 (20%) 14 (43.8%)
Heart failure 7 (35%) 8 (25%)
Creatinine clearance
>50 mL/min 15 (75%) 27 (84.4%)
30-50 mL/min 2 (10%) 5 (15.6%)
<30 mL/min; not on dialysis 0 (0%) 0 (0%)
Dialysis dependant 3 (15%) 0 (0%)
Presenting coronary disease
Elective PCI 8 (40%) 8 (25%)
Unstable Angina 7 (35%) 12 (37.5%)
NSTEMI 4 (20%) 7 (21.9%)
STEMI 1 (5%) 5 (15.6%)
PCI performed
Drug-eluting stent placement 17 (85%) 30 (93.8%)
Bare-metal stent placement 2 (10%) 1 (3.1%)
Balloon angioplasty only 1 (5%) 1 (3.1%)
Other antithrombotic medications
Aspirin 16 (80%) 30 (93.8%)
Clopidogrel 17 (85%) 28 (87.5%)
Prasugrel 2 (10%) 3 (9.4%)
Abciximab 3 (15%) 3 (9.4%)
Eptifibatide 1 (5%) 1 (3.1%)
Unfractionated heparin 3 (15%) 1 (3.1%)
Enoxaparin 0 (0%) 1 (3.1%)
Intracoronary alteplase 1 (5%) 0 (0%)
For Personal Use.
Copyright HMP 2013

Vol. 25, No. 5, May 2013 253
Evaluation of Bivalirudin Hyper- and Hypo-ACT Responses in the Setting of PCI
extremely low ACT values would potentially be associated with greater thrombotic complications.
Based on the cases identified in the study time frame, there was not a clear association of excessive bleeding risk when ACT values were greater than 800 seconds. Based on this study, there is no evidence that an ACT value of this degree should warrant discontinuation or dose reduction of the bivalirudin continu-ous infusion during PCI.
The 1 case of acute stent thrombosis that occurred in the 20 hypo-responders identified poses some concern, but definitive conclusions drawn from this observation should be limited for several reasons. The fact that this was only a single case poses ob-vious limitations regarding the external applicability of this event. Other factors that may confound the notion of bivalirudin resis-tance are details related to the patient in which this complication occurred. The total length of stents deployed may have posed an increased risk to the occurrence of stent thrombosis due to the extent of substrate for which platelets to adhere and thrombo-sis to occur. Also, underdeployment or poor size selection of the stents placed may have contributed to this poor revascularization result. A genetic hypercoagulability diagnosis was not pursued in this patient, but if present may have contributed to the occur-rence of stent thrombosis despite the presence of antiplatelet and anticoagulant therapies. Also, the possibility remains that this complication was entirely attributed to chance as these events do occur in clinical practice and the low ACT response may only have been a coincidental finding in this specific case. Important-ly, since the end of the study period, there was an additional stent thrombosis event identified in a patient undergoing PCI with an ACT response to bivalirudin below 300 seconds.
We speculate that the biological plausibility for direct thrombin inhibitor resistance exists, but this has never be-fore been described in medical literature. Bivalirudin, unlike the univalent direct thrombin inhibitors argatroban and dabi-gatran, interacts with the thrombin molecule at the active site and an exosite.15 We hypothesize that the bivalent nature of the bivalirudin molecule may interact with different phenotypes of thrombin differently, with more or less affinity to the receptor sites based on the critical distance between the exosite and ac-tive site expressed on a patient’s thrombin protein.
Study limitations. There are many limitations of this study, most notably the retrospective observational methods used to as-sess this subject. Also, the number of patients identified as hyper- and hypo-responders is small, making this analysis hypothesis-generating only.
ConclusionBased on the results found in this analysis, ACT responses great-
er than 800 seconds were not found to increase the risk of clinically significant bleeding; however, ACT responses less than 300 sec-onds may be associated with thrombotic risks. Furthermore, only 81.7% of all patients undergoing PCI in our study with the use of bivalirudin had their ACT monitored during the procedure after
administration of bivalirudin, which means that although measur-ing ACT after bivalirudin administration is a common practice among many cardiovascular interventionalists, it is not a routine procedure that is being carried out during all PCIs. Serious compli-cations, such as immediate intrastent thrombosis, although uncom-mon, may happen and need to be considered as a possible com-plication. Our recommendation is that ACT should be monitored routinely during all PCI procedures where bivalirudin is being used and a bail-out strategy should be identified when the ACT is lower than 300 seconds, which includes adding a second bolus of bivali-rudin and rechecking the ACT afterward as recommended on the package insert of bivalirudin, and adding unfractionated heparin or GPI such as abciximab. This bail-out strategy was used in our case of acute stent thrombosis when ACT continued to be less than 300 seconds after administration of the second bivalirudin bolus.
More robust analysis of contemporary randomized con-trolled trials of bivalirudin in PCI should be undertaken to clar-ify any potential dangers associated with hypo- and hyper-ACT responses to bivalirudin anticoagulation in PCI, and continued research should be undertaken to identify the most optimal monitoring and dosing strategy for this agent.
References1. Smith SC, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline
update for percutaneous coronary intervention. Circulation. 2006;113(7):e166-e286.2. King SB, Smith SC, Hirshfeld JW Jr, et al. 2007 Focused update of the ACC/AHA/
SCAI 2005 guideline update for percutaneous coronary intervention. J Am Coll Car-diol. 2008;51(2):172-209.
3. Kushner FG, Hand M, Smith SC, et al. 2009 focused updates: ACC/AHA guide-lines for the management of patients with ST-elevation myocardial infarction and ACC/AHA/SCAI guidelines on percutaneous coronary intervention. Circulation. 2009;120(22):2271-2306.
4. Wijns W, Kolh P, Danchin N, et al. Guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology and European Association for Cardio-Thoracic Surgery. Eur Heart J. 2010;31(20):2501-2555.
5. Bittl JA, Chaitman BR, Feit F, et al. Bivalirudin versus heparin during coronary angio-plasty for unstable or postinfarction angina: final report reanalysis of the Bivalirudin Angioplasty Study. Am Heart J. 2001;142(6):952-959.
6. Lincoff AM, Kleiman NS, Kereiakes DJ, et al. Long-term efficacy of bivalirudin and provisional glycoprotein IIb/IIIa blockade vs heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary revascularization: REPLACE-2 Random-ized Trial. JAMA. 2004;292(6):696-703.
7. Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355:2203-2216.
8. Stone GW, Ware JH, Bertrand ME, et al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management: One-year results from the ACUITY Trial. JAMA. 2007;298(21):2497-2506.
9. Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med. 2008;358(21):2218-2230.
10. Angiomax® (bivalirudin) product package insert. The Medicines Company. 2010.11. Carroll RC, Chavez JJ, Simmons JW, et al. Measurement of patients’ bivalirudin
plasma levels by a Thromboelastograph ecarin clotting time assay: a comparison to a standard activated clotting time. Anesth Analg. 2006;102(5):1316-1319.
12. Brener SJ, Moliterno DJ, Lincoff AM, et al. Relationship between clotting time and ischemic or hemorrhagic complications: analysis of 4 recent randomized clinical trials of percutaneous coronary intervention. Circulation. 2004;110(8):994-998.
13. Rao SV, O’Grady K, Pieper KS, et al. A comparison of the clinical impact of bleeding measured by two different classifications among patients with acute coronary syn-dromes. J Am Coll Cardiol. 2006;47(4):809-816.
14. Mauri L, Hsieh W, Massaro JM, et al. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356(10):1020-1029.
15. Schaden E, Kozek-Langenecker SA. Direct thrombin inhibitors: pharmacology and application in intensive care medicine. Intensive Care Med. 2010;36(7):1127-1137.
For Personal Use.
Copyright HMP 2013