X ray spine. SPINE TRAUMA CERVICAL SPINE INJURY THORACO-LUMBAR SPINE INJURY.
Upload
love2jaipalCategory
view
231download
0EVALUATION OF CERVICAL SPINE INJURY
SRI SIDDHARTHA MEDICAL COLLEGE,TUMKURDEPARTMENT OF ORTHOPAEDICSTOPIC:Cervical Spine Injury: Evaluation & Management
Chairperson:prof. & HOD Dr.Mahesh K.UDept. of OrthopaedicsModerator:prof. Dr. Govindaraju D.KDept. of OrthopaedicsPresenter:Dr. Jaipalsinh MahidaDept. of Orthopaedics
EVALUATION OF CERVICAL SPINE INJURYPrehospital careHospital careHistory and physical examination.Neurological examinationSensation to light touch , Pinprick Motor strength Deep tendon reflexes and pathological reflexes also should be checked.Motor and sensory evaluation of the rectum and perirectal area is mandatory. bulbocavernous reflexbowel or bladder
Prehospital:- ABC, immobilize, if intubation required head shuld not be moved much.Hospital care:- maintain hemodynamics, BP >100mmhg, differenciate betwen neurogenic and hypovolemic shockPhysical : -supine, neck motion should not be evaluated -mental status also should be assessed -The head for lacerations and contusions and palpated for facial fractures.-The ear canals should be inspected to rule out leakage of spinal fluid or blood behind the tympanic membrane, which is suggestive of a skull fracture.- The spinous processes should be palpated from the upper cervical to the lumbosacral region. A painful spinous process may indicate a spinal injury. -Palpable defects in the interspinous ligaments may indicate disruption of the supporting ligamentous complex.
Neurological examination: -neck motion should not be evaluated - Sensation to light touch , Pinprick -Motor strength -Deep tendon reflexes and pathological reflexes also should be checked.-Motor and sensory evaluation of the rectum and perirectal area is mandatory.- bulbocavernous reflex-bowel or bladder
2
3
Neurological evaluation GLASGOW COMA SCALE
Eyes Open Spontaneous 4 To sound 3 To pain 2 Never 1 Best Verbal Response Oriented 5 Confused conversation 4 Inappropriate words 3 Incomprehensible words 2 None 1
Best Motor Response Obeys commands 6 Localizes pain 5 Flexion withdrawal 4 Abnormal 3 Extension 2 None 1
4
Sensory examination performed with light touch, then pinpricks (using a sterile needle), beginning at the head and neck and progressing distally, to examine specific dermatome distributions Important dermatome landmarks are the nipple line (T4), xiphoid process (T7), umbilicus (T10), inguinal region (T12, L1), perineum and perianal region (S2, S3, and S4). The skin should be marked where sensation is present before proceeding to motor examination. Evidence of sacral sensory sparing establishes the diagnosis of an incomplete spinal cord injury. The only area of sensation distal to an obvious cervical lesion in a quadriplegic patient may be in the perianal region
5
Motor examinationshould be systematic, beginning with the upper extremities.A protruded cervical disc /unilateral dislocated facet may produce an isolated nerve root paralysis. key muscle groups and their corresponding nerve root levels +/- of sacral motor sparing should be determined by voluntary rectal sphincter / toe flexor contractions. prognosis for recovery of motor function is good if presentreflexes should be documented.
7
Myotomes
IMAGING STUDIESCT scans for screening, considered more cost-effective as well as more sensitive compared to plain radiographs. radiographs often fail to capture the occipitocervical and cervicothoracic junctions. Occipital condylar fractures, occipitocervical dislocations, and upper cervical injuries are often underappreciated on radiographs. Radiographs may be used for screening A lateral radiograph can be used in polytrauma patients presenting in extremis. The necessity for plain film imaging may be informed by the NEXUS low-risk criteria or the Canadian C-spine rules.MRI is the most sensitive to evaluate the cervical spine and will detect discoligamentous injuries that would otherwise be missed by CT scanning alone.
RADIOGRAPHSVIEWS: - AP lateralopen-mouth odontoid views ObliqueFlexion & extensionSwimmers view
The swimmers for evaluating the relationship of the cervicothoracic junction and upper thoracic vertebrae C7 through T3.11
Oakley introduced a simple system (radiological ABC) for analyzing plain films:
A1: appropriateness: correct indication and right patientA2: adequacy: extent (occiput to T1, penetration, rotation/projection)A3: alignment: anterior aspect of vertebral bodies,posterior aspect of vertebral bodies,spinolaminar line (bases of spinous process),tips of spinous process,
B: bonesC: connective tissues: pre-vertebral soft tissue,pre-dental space,intervertebral disc spaces,interspinous gaps
LATERAL VIEW Power RatioCalculated by dividing distance between basion & posterior C1 arch by distance between opisthion & anterion C1 arch.Ratio >1 means atlantooccipital dislocationHarris measurement also called rule of 12measurement of the Basion-Axis Interval and the Basion-Dens Interval, both of which should measure less than 12 mm if the occipitocervical articulation is intact.
LATERAL VIEW Atlanto-Dens interval(ADI)Measured from posterior surface on anterior C1 arch to anterior surface of odontoid process.Normal - < 3mmWidening indicates disruption of transverse ligamnet.Posterior Atlanto Dens interval (PADI)measured from posterior surface of dens to anterior portion of C1 posterior arch,Represents AP diameter of spinal canal at C1Normal - < 13mm
A+B > 7mm indicates rupture of transverse ligament
At the C2 level, displacement and angulation of odontoid fractures are thought to influence the risk of nonunion and direct the need for surgical intervention. The Spine Trauma Study Group recommends that displacement of odontoid fractures be measured between two tangents drawn along the anterior cortex of the odontoid and C2 vertebral body, respectively Angulation is determined by the angle created by the intersection of extrapolated lines drawn along the posterior cortex of the odontoid and the C2 vertebral body.
For pars interarticularis fractures, the so-called hangmans fracture, angulation may be assessed by the endplate method or posterior tangent technique. The endplate method uses the angle created by lines extrapolated from the inferior endplates of C2 and C3 posterior tangent technique utilizes lines extrapolated from the C2 and C3 posterior vertebral bodies .
For subaxial cervical evaluation,Comminution of fracture fragments should be appreciated if present and primary fracture lines outlined.
Segmental kyphosis can be determined using an endplate (Cobb) technique or
posterior vertebral body tangent similar to that described for hangmans fractures.
Subaxial cervical translation is assessed by determining the distance between extrapolated lines extending from the posterior vertebral bodies White and Panjabi advised that translation greater than 3.5 mm was suggestive of mechanical instability.
Determination of vertebral body height loss is performed by measuring the percentage difference between anterior and posterior vertebral body heights at the injured level compared with an average measurement obtained from adjacent levels above and below.
PRE VERTEBRAL SOFT TISSUE SHADOWSNasopharyngeal space (C1) - 10 mm (adult)
Retropharyngeal space (C2-C4) - 5-7 mm
Retrotracheal space (C5-C7) - 14 mm (children), 22 mm (adults)
Extremely variable and nonspecific
Contour is more important than measurements
The laminar space is the distance from posterior aspect of the articular pillars (1) tothe spinolaminar line (2)indicate rotational injuries of the cervical spine
A line (white line ) drawn through C1-3 should intercept the C2 spinolaminar line.displacement in this line may be an indication of subtle traumatic vertebral injury/dislocation. A displacement more than 2 mm, is abnormal
Anteroposterior viewassess alignmentsymmetry of pediclescontour of bodiesVertebral body height should be uniform.height of disc spacesDisc space should be uniformcentral position of spinous processes
facet joints oriented at 45 degree angle from coronal plane -- thus not seen on AP viewif facet is clearly identified on ap, articular pillar or pedicle fracturex with rotation is likely
Flexion-Extension FilmsMay be helpful in ligament injuriesBut Frequently useless due to muscle spasmShould not be done in acute settingPatient must be alert, awake, not intoxicated, able to sit or stand, able to understand commands, and without neurologic deficit.
COMPUTED TOMOGRAPHYCT scans are more sensitive than plain radiographs in identifying fractures and subtle osseoarticular abnormalities. Facet, lamina, and pedicle fractures are notorious difficult to identify on plain radiographs but may be more easily appreciated on axial CT studies. Spinous process fractures will also be easily visualized.Vertebral body translation and frank dislocation are also demonstrable on axial CT scans.The absence of opposed articular surfaces may result in an empty facet sign. In facet dislocations, the inferior articular process of the level above will be visualized anterior to the superior articular process of the caudal vertebrae.
Paramedian sagittal cuts through the facet joints may help appreciate dislocations, subluxations, and estimations of fracture fragment size
Retropulsion of fracture fragments into the canal, and resultant compromise, can best be estimated on a midsagittal CT scan.
MEGNETIC RESONANCE IMAGINGMRI is known to be superior to computed tomography in terms of visualizing cervical soft-tissue structures, spinal cord, cervical nerve roots, intervertebral discs, and posterior ligamentous complex (PLC), epidural hematomas, and vertebral artery injury , undisplaced fractures of the vertebral bodies.
MRI scan is obtained in cases of cervical spine trauma when any of the following criteria are met: the patient presents with a neurologic deficit, the integrity of the PLC is unclear and injury to this structure would have a direct influence on treatment, such as determining the need for surgery, and the patient presents with a facet dislocation where there is concern regarding disc herniation into the spinal canal that may prevent safe reduction and cause difficulty in deciding on the correct approach for surgical intervention. Magnetic resonance arteriography can be employed in the assessment of vertebral artery injury and patency.
32
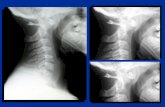
Fig. on left: sagittal T2 image showing C6 body fracture (thin black arrow)posterior log. Lig. (small thin black arrow)large black arrow normal lig. Flavumlarge white arrow disrupted lig. Flavum
Fig. On right: axial T2 through C1 ringshowing intact transverse lig. (arrow heads)o odontoid process33
TREATMENT OPTIONSprimary goal is maintenance, or restoration, of neurologic function & reduce pain. By decompression of the spinal cord and neural structures or reduction and realignment of facet dislocations or displaced fractures. In most instances, stability is restored via surgical intervention and instrumentation of the spine, although closed means, such as halo-fixation have been employed effectively in the past.
Secondary goals include fracture healing, diminution of pain, mitigation of disability, and restoration of function. Even after complete spinal cord injury, surgical intervention and spinal fusion may be necessary to allow a patient to sit upright in a wheelchair, maintain forward gaze, and ameliorate long-term issues such as chronic pain or Charcot arthropathy of the spine. In patients with stable cervical fractures, in the absence of neurologic impairment, bracing and external orthoses have been employed successfully to potentiate healing.
Non-operative Treatment ModalitiesCERVICAL ORTHOSES
Most cervical orthotics use three-point pressure to restrict motion, mandible and occiput proximally, Clavicle and the sternal notch anteroinferiorly, andT3 spinous process and scapular spines posteriorly.Cervical orthoses limit movement of the cervical spine by buttressing structures at both ends of the neck, such as the chin and the thorax.Used for stable fractures.
However, applied pressure over time can lead to complications such as:pressure sores and skin ulcersweakening and atrophy of neck musclescontractures of soft tissuesdecrease in pulmonary functionchronic pain syndrome
CollarsSoft collars have a limited effect on controlling neck motion.
The Philadelphia collar has been shown to control neck motion, especially in the flexion/extension plane, much better than the soft collar.Disadvantages of the Philadelphia collar are the lack of control for flexion/extension control in the upper cervical region and lateral bending and axial rotation.
CERVICOTHORASIC ORTHOSES:Minerva Brace/CastA Minerva cervical brace is a cervicothoracal orthosis with mandibular, occipital and forehead contact points.This brace provides adequate immobilization between C1 and C7, with less rigid immobilization of the occipital-C1 junction. The addition of the forehead strap and occipital flare assists in immobilizing C1C2.
Traction:The Gardner-Wells tongs can be applied using local anesthesia. The pin application sites should be a finger breadth above the pinna of the auricle of the ear in line with, or slightly posterior to, the external auditory canal.Rule out atlanto-occipital dislocation or discoligamentous disruption before applying traction.
application of gardner wells tongs can be useful in reducing fracture and dislocation.
Neutral position is just proximal to external auditory meatus, 1 cm above pinna. By placing ping anteriorly extension movement can be applied. By placing posteriorly flexion movement can be applied.41
HaloThe halo vest is the first conservative choice for unstable lesions.Its clinical failure is due to:pin track problemsaccurate fitting of the vesta lack of patient compliance
SURGICAL TREATMENT
APPROACHES:Anterior approache:Occiput to C3Anterior transoral approachAnterior retropharyngeal approachC2 to C7C3 to C7Cervicothorasic junction, C7 to T1
Retropharyngeal approach
C3 to C7
Cervicothorasic junction
Posterior ApproachOcciput to C2C3 to C7
SURGICAL PROCEDURES:Anterior DecompressionReconstructionAnterior Instrumentationposterior DecompressionPosterior Instrumentation and Fusion of the Cervical Spine
COMPLICATIONS OF SURGERYCOMPLICATIONS WITH ANTERIOR APPROACH:DysphagiaRecurrent laryngeal nerve palsy > dysphoniaSuperior laryngeal nerve injury rare -> dysphagia and loss of high phonationHorners syndrome damage to the vertebral artery or esophagus -> life thretaning
COMPLICATIONS WITH POSTERIOR APPROACH: Vertebral artery damageThe risk of postoperative infection; wound problems, such as hematoma or dehiscence; pulmonary complications; and venous thromboembolic disease have been reported to be higher with a posterior approach relative to the anterior approach.persistent CSF leak following durotomy with the posterior approach
TREATMENT OPETIONS FOR SPECIFIC INJURIESOCCIPITOCERVICAL DISLOCATIONS(C0-C1):These injuries are grossly unstable, primarily ligamentous, and have little chance of healing with external immobilization alone.
Nonoperative Treatment :Indications Little roleHalo immobilization is most often used as a temporary means of stabilization, or a means of reducing injury, until surgery can be safely performed.Longitudinal traction is contraindicated in this setting.
OPERATIVE TREATMENT: Indications
Recently, wiring contoured rods to the vertebrae provided more mechanical stability, but the fixation was insufficient to obviate the need for external immobilization.
OPERATIVE TREATMENT: Indications
The introduction of plate and screw fixation was an immediate precursor to modern screw-rod systems. The so-called Y plate allowed screws to be inserted directly into the occiput, Cl, and C2 and provided rigid internal fixation, although fatigue fracture was a common complication due to stresses across the occipitocervical junction.
54
The current generation of occipital plates can be connected to polyaxial screws in the upper cervical spine and have been found to result in extremely stable and versatile constructs
Pt had previously undergone anterior corpectomy & fusion in subaxial region.A posterior occipitocervical fusion performed55
OCCIPITAL CONDYLE FRACTURE:
Anderson & Montesano classification:type I : impacted fracture Injuriestype II : basilar skull fracture involving condylestype III : displaced avulsion fractures.56
ATLAS FRACTURE(C1):
Gehweiler classification:Type I : fracture of the anterior archType II : fracture of the posterior archType III : combined fracture of both the anterior and the posterior arch = Jefferson fracture Type IV : fracture of massa lateralisType V: fracture of the transverse process57
ATLANTOAXIAL INSTABILITY
Atlantoaxial instability results from either:a purely ligamentous injury or avulsion fractures.These injuries are significant, because complete bilateral dislocation of the articular processes can occur at approximately 65 of atlantoaxial rotation.When the transverse ligament is intact, a significant narrowing of the spinal canal and subsequent potential spinal cord damage is possible
Fielding et al. four types:Type I: rotatory fixation with no anterior displacement (transverse ligament intact) and the dens working as pivot.Type II: rotatory fixation with anterior displacement of 35mmand one lateral articular process acting as the pivotType III: rotatory fixation with anterior displacement of more than 5 mm.Type IV: rotatory fixation with posterior displacement.
Type III and IV were only observed in non-traumatic conditions.
58
With a deficient transverse ligament, complete unilateral dislocation can occur at approximately 45 with similar consequences.
In addition, the vertebral arteries can be compromised by excessive rotation which may result in brain stem or cerebellar infarction and death.As an adjunct to both operative or nonoperative management, traction can be an effective method of reducing sagittal C1-C2 instability.
Fielding et al. four types:Type I: rotatory fixation with no anterior displacement (transverse ligament intact) and the dens working as pivot.
Type II: rotatory fixation with anterior displacement of 35mmand one lateral articular process acting as the pivotType III: rotatory fixation with anterior displacement of more than 5 mm.Type IV: rotatory fixation with posterior displacement.
Type III and IV were only observed in non-traumatic conditions.
59
Nonoperative Treatment :In a patient who is neurologically intact, nonoperative treatment in a collar or a halo vest can be used, provided the ADI can be held in a reduced position.
Operative Treatment:Surgical treatment of sagittal C1-C2 instability without fracture usually consists of posterior atlantoaxial stabilization and fusion.If a patient has an associated spinal cord injury, surgical treatment should be strongly considered regardless of the degree of instability. Patients with ADIs greater than 5 mm should also undergo C1-C2 fusion.
Fielding et al. four types:Type I: rotatory fixation with no anterior displacement (transverse ligament intact) and the dens working as pivot.
Type II: rotatory fixation with anterior displacement of 35mmand one lateral articular process acting as the pivotType III: rotatory fixation with anterior displacement of more than 5 mm.Type IV: rotatory fixation with posterior displacement.
Type III and IV were only observed in non-traumatic conditions.
60
ODONTOID FRACTURES(C2):
According to the classification of Anderson and DAlonzo:Type I: oblique fractures through the upper portion of the odontoid process. Type II: across the base of the odontoid process at the junction with the axis body.Type III: through the odontoid that extends into the C2 body.
61
Dens Fractures
62
Dens Fractures
63
Dens Fractures
Transarticular atlantoaxial screw fixation according to Magerl [113] with additional wire cerclage and fusion with a bicortical bone graft (Gallie)
Alternative screw-rod fixation according to Harms64
HANGMANS FRACTURE(TRAUMATIC SPONDYLOLISTHESIS, (C2-C3):
Levins & Edwards classification:type I: minimally displaced, no translation or angulation, no Injury to C2-C3Type II : both angulation & translation, injury to C2-C3Type IIA : fracture as result of flexion, marked angulation with minimal translation Type III : any C2 pars fracture associated with dislocation of C2- C365
SUAXIAL CERVICAL FRACTURES & DISLOCATIONS(C3-C7):
Compression Fractures: Nonoperative Treatment IndicationsPatients with cervical compression fractures without posterior ligamentous injuryFor C3-C6 injuries, a rigid cervical collar usually suffices. For injuries of C7 or Tl, a cervicothoracic brace may provide better immobilization. Attempts to correct minor kyphotic deformities are usually fruitless and ultimately unnecessary. Compression fractures are usually healed by 3 months, at which tithe flexion-extension views should be obtained to rule out occult instability.
Allen and Ferguson classification :1) compressionflexion injuries2) vertical compression injuries3distractionflexion injuries4) compressionextension injuries5) distractionextension injuries6) of lateral flexion injuries66
Compression Fractures: Operative Treatment IndicationsSurgical stabilization via an anterior or posterior approach should be considered for patients with evidence of posterior ligamentous injury. Posterior ligamentous injury is suggested by a segmental kyphosis greater than 11 degrees or a substantial amount of vertebral body wedging; Threshold values for the degree of height loss or PLC injury beyond which surgery is indicated; have not been defined. MRI can be used as a means to determine the integrity of posterior soft-tissue structures in a compression fracture.
SUAXIAL CERVICAL FRACTURES & DISLOCATIONS(C3-C7):
BURST Fractures: Nonoperative Treatment IndicationsIn neurological intact patients with little vertebral body comminution and only the mildest degree of canal compromise. Any kyphotic deformity should measure less than 5 degrees, and there should be, no indication of posterior ligamentous injury.Patients should be followed weekly for the first month and immobilization maintained for at least 12 weeks. Any subsidence, focal collapse or kyphosis is a strong indication for surgery.
Allen and Ferguson classification :1) compressionflexion injuries2) vertical compression injuries3distractionflexion injuries4) compressionextension injuries5) distractionextension injuries6) of lateral flexion injuries68
Compression Fractures: Operative Treatment IndicationsAnterior Corpectomy and Stabilization :Patients with neurologic deficit, regardless of the integrity of the PLC, should be surgically stabilized Posteriorly displaced vertebral body fragments are most readily removed through a direct anterior approach. The anterior column reconstructed with a bone graft or strut. Insert a rigid titanium mesh cage filled with salvaged bone in addition to cancellous iliac crest autograft. Bone should be tightly packed into the cage, which may also enhance the surface area contact with the endplates. An anterior cervical-plate is then applied to restore anterior stability. If the PLC appears to be disrupted, perform a posterior instrumented fusion, either during the same operation or in a staged fashion
Compression Fractures: Operative Treatment IndicationsPosterior Instrumentation and Fusion :reserved for patients who are neurologically intact and demonstrate evidence of posterior ligamentous disruption. If posterior fixation is planned as the only treatment, the vertebral burst fracture should demonstrate biomechanical integrity, with no comminution, kyphosis, or posterior retropulsion of fragments. Otherwise, the posterior construct will have a high risk of failure.
SUAXIAL CERVICAL FRACTURES & DISLOCATIONS(C3-C7):
Flexion-Type Teardrop Fractures: Nonoperative Treatment IndicationsDefinite role for nonoperative, treatment Minimally displaced fractures with little kyphosis and no PLC injury are stable. treated with rigid cervical collar or CTO, depending on the level of injury.Halo treatment can also be used to treat these injuries. Halo maintained for 3 months, provided acceptable alignment has been maintained. After the, halo has been removed flexion-extension radiographs are necessary to confirm that stability has been achieved.
Allen and Ferguson classification :1) compressionflexion injuries2) vertical compression injuries3distractionflexion injuries4) compressionextension injuries5) distractionextension injuries6) of lateral flexion injuries71
Flexion-Type Teardrop Fractures:
Operative Treatment IndicationsIn patients with a neurologic deficit, anterior corpectomy is usually performed to remove the posteriorly displaced vertebral body followed by anterior strut grafting and rigid plate fixation.In unstable teardrop fracture and neurologically intact patient.anterior surgery entails a nondecompressive corpectomy, with resection of the majority of the vertebral body back to, but not through, the posterior wall. translational deformity, exceeding 3 to 3.5 mm, and the facet joints appear to be widened, posterior surgery is recommended as an adjunct to provide additional stability.
SUAXIAL CERVICAL FRACTURES & DISLOCATIONS(C3-C7):
Facet Fractures :
Allen and Ferguson classification :1) compressionflexion injuries2) vertical compression injuries3distractionflexion injuries4) compressionextension injuries5) distractionextension injuries6) of lateral flexion injuries73
SUAXIAL CERVICAL FRACTURES & DISLOCATIONS(C3-C7):
Facet Dislocations:
Allen and Ferguson classification :1) compressionflexion injuries2) vertical compression injuries3distractionflexion injuries4) compressionextension injuries5) distractionextension injuries6) of lateral flexion injuries74
Thank You