European Society of Multimodality imaging of penile ... Penile emergencies M BERTOLOTTO.pdf ·...
42
ATHENS 4-6 October 2018 European Society of Urogenital Radiology 2nd ESUR Teaching Course Multimodality Imaging Approach to Scrotal and Penile Pathologies Penis - Section IX- Multimodality Imaging of Penile Pathology Multimodality imaging of penile emergencies Michele Bertolotto Dept Radiology - University of Trieste (IT)
Transcript of European Society of Multimodality imaging of penile ... Penile emergencies M BERTOLOTTO.pdf ·...

AT
HEN
S
4-6
Oct
ob
er
20
18
European Society of Urogenital Radiology
2nd ESUR Teaching Course Multimodality Imaging Approach to Scrotal and Penile Pathologies
Penis - Section IX- Multimodality Imaging of Penile Pathology
Multimodality imaging of penile emergencies
Michele Bertolotto
Dept Radiology - University of Trieste (IT)

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Essentially clinical diagnosis?
Surgical management in all cases?
Imaging not indicated?
“Awareness of mode of trauma and clinical
features is all that required for diagnosis
and no more investigation is desirable.
Surgical exploration is ideal for its
management”
PENILE EMERGENCIES
Non-penetrating penile traumas

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
o Do not require surgery, provided that a firm preoperative
diagnosis of intact tunica albuginea is reached
o Surgical exploration in equivocal cases
o Imaging (US, MRI) identify laceration of
the tunica albuginea
Non-penetrating penile traumas
Last update: March 2018
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Urologists’ expertise in US is often inadequate
for evaluation of penile traumas
Radiologists often are not able to provide
satisfactory and clinically targeted information
PENILE EMERGENCIES
Non-penetrating penile traumas

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Flaccid or erect
Different injuries depending on firmness, mobility, deformability, and position differences
o Penile fracture
o Intracavernosal haematoma
o Isolated septal haematoma
o Extra-albugineal haematoma
o High-flow priapism
Imaging: differential diagnosis between surgical
and non-surgical lesions
Non-penetrating penile traumas
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Surgical emergency, if unrepaired, it may lead
to deformity and erectile dysfunction
Forceful bending of the erect penis
Cracking sensation and severe pain
followed by rapid detumescence
Eggplant deformity of the penis
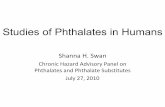
Penile fracture
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Imaging: differential diagnosis between
surgical and non-surgical injuries
In expert hands US as potential to detect interruption of the tunica albuginea
o High-end equipment, high-frequency broadband probes
MRI has much higher contrast resolution
o Better and easier evaluation of albugineal disruption
o More panoramic than US
PENILE EMERGENCIES
Penile fracture

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Impractical in the acute setting (especially if requested outside the normal working hours)
Often US is the only available imaging modality
*
CC * CC
Non-penetrating penile traumas - MRI
PENILE EMERGENCIES
2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture – limitations of US
A 44yo patient experienced severe pain after accidental bending of the penis during
intercourse followed by rapid detumescence and bleeding from the urethra when he
was abroad spending his holidays. He was able to void. Eggplant deformity of the
penis rapidly developed. He presented to the emergency room of the local hospital
where he was advises to present in an hospital with dedicated expertise in this field.
He presented to our hospital 4 days after the trauma
Fracture of the penis with injury of the urethra were obvious clinically. US was requested in emergency to have a more panoramic view of the extension of the trauma before operation
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture – limitations of US
A 4 days after the trauma the haematomas are largerly organized, and the contrast
resolution between the blood collections and the erectile bodies is markedly reduced
Diagnosis: o Ventral rupture of the right corpus cavernosus o Urethral injury not identified, but clinically obvious
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture – limitations of US
A 4 days after the trauma the haematomas are largerly organized, and the contrast
resolution between the blood collections and the erectile bodies is markedly reduced
Diagnosis: o Ventral rupture of the right corpus cavernosus o Urethral injury not identified, but clinically obvious
At surgery: rupture of the left corpus cavernosum as well!
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile fracture – associated vascular injuries
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Difficult to identify at US
Retrograde urethrography can be done
Flexible cystoscopy is recommended above
retrograde urethrography in penile fracture with
associated suspected urethral injury
Last update: March 2018
Penile fracture – Urethral injuries
Flexible cystoscopy can be performed under
anaesthesia during exploration/repair
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
*
Penile fracture – associated urethral injuries
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
*
Early Early 1 wk
Cavernosal haematomas
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Recently identified trauma to the erect penis
Peyronie’s disease with septum
involvement is a predisposing factor
Can result in septal fibrosis with penile deformity
Brant WO, J Urol 2007
Isolated septal haematoma
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Isolated septal haematoma & Peyronie’s disease
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
1
2 3
1- Skin 2- Colles’ fascia
3- Buck’s fascia
Extra-albugineal haematomas
PENILE EMERGENCIES
Below the Buck’s fascia Above the Buck’s fascia

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
To confirm location
To assess the integrity of
the tunica albuginea
Extra-albugineal haematomas -US
Below the Buck’s fascia Above the Buck’s fascia
1
2 3
1- Skin 2- Colles’ fascia
3- Buck’s fascia
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
*
Extra-albugineal haematomas -MRI
To confirm location
To assess the integrity of the tunica albuginea
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Ischemic (low-flow or veno-occlusive)
Stuttering High-flow
Partial (acute segmental thrombosis)
“Malignant”
Colour Doppler US: differentiate ischemic from
arterial priapism as an alternative or adjunct to
blood gas analysis (LE:2b)
MRI: controversial role. Evaluation of viability of the corpora
cavernosa and presence of fibrosis in ischemic priapism
(LE:3), and assessment of malignant priapism
Priapism - Classification
PENILE EMERGENCIES
Last update: March 2018

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
≥ 4h: Hypoxia, accumulation of acidic metabolic products
≥ 24h: destruction of the sinusoidal endothelium, exposure
of the basement membrane and thrombocyte adherence
≥ 48h: thrombi in the sinusoidal spaces, smooth muscle
necrosis with fibroblast-like cell transformation
Sanli O, Int J Impot Res 2004
Ul-Hasan M, J Urol 1998 Broderick GA, Int J Impot Res 1994
Juenemann KP, Urol Int 1986
≥ 12h: trabecular interstitial oedema
Ischemic Priapism
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Clinics
Corporal aspiration of non-oxygenated blood
Imaging usually
not necessary for
the diagnosis
Low-flow priapism - diagnosis
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Imaging: diagnostic confirmation and prognosis
Cocaine induced priapism lasting since 10 hours
Resolution following corporal aspiration and cavernosal injection
𝛼-adrenergic agonists
Low-flow priapism - diagnosis
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Imaging: diagnostic confirmation and prognosis
Low-flow priapism - diagnosis
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Similar to ischaemic priapism (low-flow)
If left untreated, can result in significant penile damage
Sickle cell disease, often idiopathic (LE:3)
Repetitive and painful episodes of prolonged erections
Erections are self-limited, with intervening periods of detumescence
The duration of the erectile episodes is
generally shorter than in ischemic priapism
The frequency and/or duration of the erectile episodes is variable. A single
episode can sometimes progress into a major ischemic priapic episode
Stuttering Priapism (intermittent or recurrent)
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Stuttering Priapism - Imaging
No specific features (similar to normal erection)
Differentiation from arterial priapism (EAU Guidelines, March 2017)
Findings - color Doppler US
o High velocity (30-40 cm/s or more) flows are commonly found
o Velocities reduce in rigid erection
o End diastolic velocity depens on the degree of penile rigidity
o Echogenicity of the cavernosal bodies is often increased in priapism lasting >10-12h, but can be restored during the follow-up
Likely edema, not fibrosis!
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Stuttering Priapism - Imaging
Full erection Release of erection
Early after the priapism
episode 1 wk later
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Perineal blunt trauma producing
cavernosal artery tear
It is not an emergency
Clinics
o Painless, usually incomplete erection
o Increased rigidity with sexual stimulation
Diagnosis
o History, clinics
o Aspiration of oxigenated cavernosal blood
o Colour Doppler US
Pompei, house of Vettii
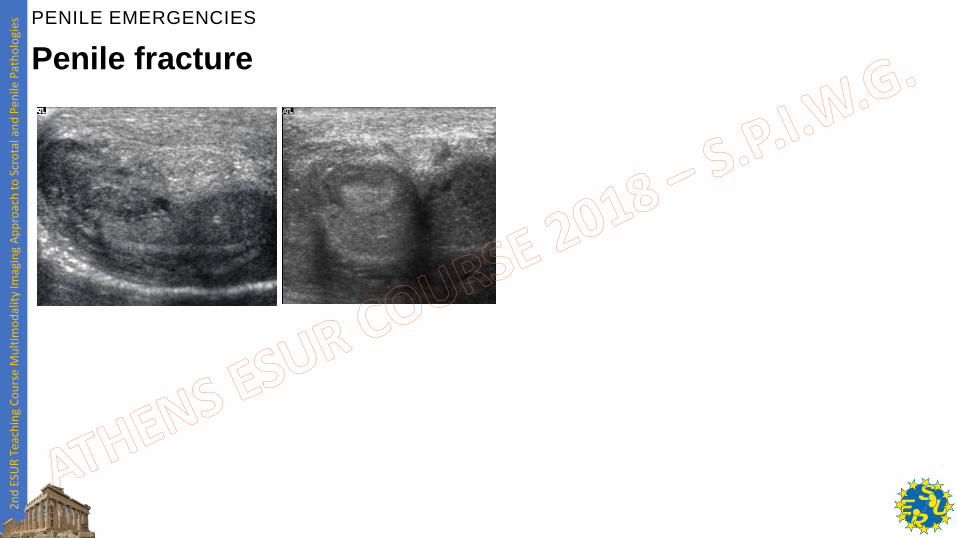
High-flow Priapism
PENILE EMERGENCIES
2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Grey-scale US: identification of the injury
Colour Doppler US: identification of the cavernosal artery tear and feeding vessels, guidance to PW-Doppler interrogation
PW-Doppler: diagnosis confirmation
*
High-flow Priapism
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
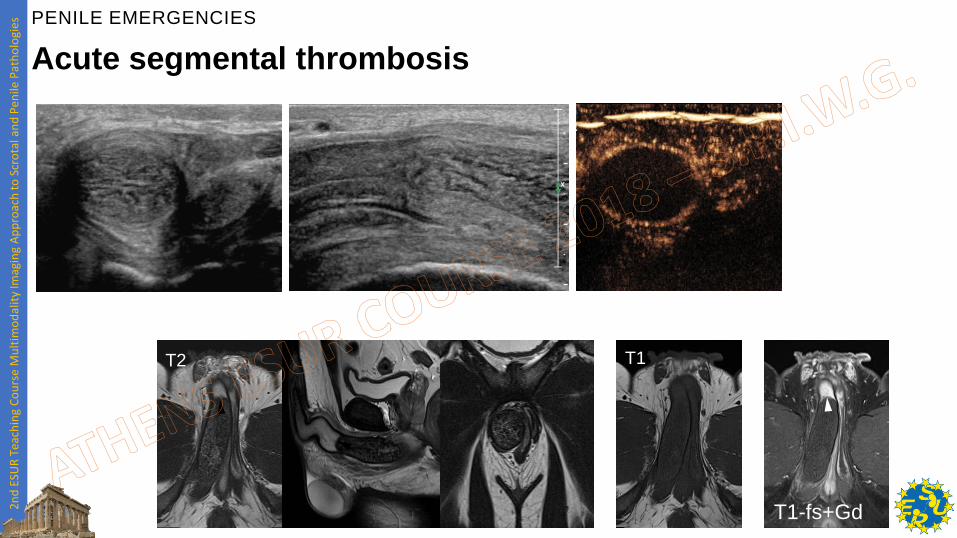
Uncommon, usually unilateral, can be bilateral
Idiopathic, or associated to microtraumas o Excessive bicycling, drug abuse, haematological diseases
Presents clinically with a painful lump Involving the
crus of the corpus. Can mimic a tumour
Conservative management with use of
anticoagulation is the treatment of choice
Acute segmental thrombosis
PENILE EMERGENCIES
2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Acute segmental thrombosis
T1 T2
T1-fs+Gd
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
T2 T1 T1-fs+Gd T1-FS
Subtraction
T1 T2 T1fs T1fs + Gd Subtraction
Acute segmental thrombosis
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
64yo patient with acute urinary retention and
painless penile induration involving the entire shaft.
«Malignant Priapism»
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
T1 T2 T1+ Gd
Final diagnosis: poorly
differentiated squamous cell
carcinoma with infiltrative
growth pattern likely arising
from the proximal portion of
the penile urethra
«Malignant Priapism»
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Penile inflammation
(Cutaneous and urethral disease)
Cellulitis, abscess formation, cavernositis
Diagnosis is based on clinics. Imaging indicated in severe
inflammation to evaluate the extension of the disease
US in most of cases, MRI in equivocal cases and
when an underlying mass must be ruled-out
Abscess Cellulitis Cavernositis
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
A 79yo diabetic patient presenting with acute urinary retention and
enlarging, painless swelling of the penis from 3 days. Clinically, the
external urethral orifice was obliterated. 14,000 WBC. The patient denied
trauma. He reported on a small penile lump already present before the
onset of symptoms. MR was performed
Inflammation is present.
Are cavernosal bodies involved?
Is there an underlying tumour?
Penile inflammation
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
T2 T1-fs+Gd
Penile inflammation
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
T2 T1-fs+Gd
Penile inflammation
PENILE EMERGENCIES

2n
d E
SUR
Tea
chin
g C
ou
rse
Mu
ltim
od
alit
y Im
agin
g A
pp
roac
h t
o S
cro
tal a
nd
Pen
ile P
ath
olo
gies
Thank you
Lorenzo Derchi – Genova (IT)
Pietro Pavlica – Bologna (IT)
Giovanni Serafini – Pietra Ligure (IT)
…with a little help from my friends
PENILE EMERGENCIES