EUROPEAN SOCIETY OF - British Cardiovascular Society · The European Society of Cardiology is...
56
Update 2008
Transcript of EUROPEAN SOCIETY OF - British Cardiovascular Society · The European Society of Cardiology is...

Co
re Curriculum
for th
e Gen
eral Card
iolo
gist
EUROPEANSOCIETY OFCARDIOLOGY ®
EUROPEAN SOCIETY OF CARDIOLOGY2035, ROUTE DES COLLES
LES TEMPLIERS - BP 17906903 SOPHIA ANTIPOLIS CEDEX - FRANCE
PHONE: +33 (0)4 92 94 76 00 FAX: +33 (0)4 92 94 76 01E-mail: [email protected]
Update 2008

EUROPEANSOCIETY OFCARDIOLOGY ®
The ESC Core Curriculum for the
General CardiologistPrepared by the Education Committee of the European Society of Cardiology
ESC Education Committee 2006 – 2008
Peter Kearney, IrelandChairman of the ESC Education Committee
Jean-Pierre Bassand, FranceCarina Blomström-Lundqvist, Sweden
Martin Cowie, UKFilippo Crea, Italy
Frank Flachskampf, GermanyDan Gaita, Romania
Lino Gonçalves, PortugalRoger Hall, UK
Erhard Kaiser, GermanyJose Luis Lopez-Sendon, Spain
Jean Marco, MonacoIraklis Mavrakis, Greece
Peter Mills, UKTomasz Pasierski, Poland
Peter Polak, The NetherlandsJuerg Schwitter, Switzerland
Other contributorDon Poldermans, The Netherlands
ESC StaffKeith McGregor, FranceClaire Bramley, France
Dominique Poumeyrol-Jumeau, FranceEUROPEANSOCIETY OFCARDIOLOGY ®

© 2008 The European Society of Cardiology. No part of this document may be translated or reproduced in any form without written permission from the ESC, 2035 Route des Colles, Les Templiers, 06903 Sophia Antipolis, France, www.escardio.org
Published by The European Society of Cardiology
The right of the Authors to be identifi ed as the Authors of this Work has been asserted in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced in any form or by any electronic or mechanical means, including information storage and retrieval systems, without permission in writing from the publisher, except by a reviewer who may quote brief passages in a review.
First published 2006

Foreword IV
Preface V
Introduction VI
• Rationale – Summary of the Clinical Field of Cardiology VII
• General Aspects of Training in the Specialty VIII
• Requirements for Training Institutions IX
• Requirements for Trainers IX • Assessment Methodology X
• Learning Objectives – Chapters in the Curriculum XI
• Acknowledgements XII
1. History taking and clinical examination 1 2. The Electrocardiogram: standard ECG, ambulatory ECG, exercise ECG 2
3. Non Invasive Imaging – Echocardiography, CMR, Cardiac CT and Nuclear techniques 4
4. Invasive Imaging – Cardiac Catheterisation andAngiography 7
5. Genetics 9
6. Clinical Pharmacology 10
7. Cardiovascular Disease Prevention: Risk Factors, Assessment and Management 11
8. Acute Coronary Syndromes (ACS) 14
9. Chronic Ischaemic Heart Disease 16
10. Myocardial Disease 18
11. Pericardial Disease 19
12. Cardiac Tumours 20
13. Congenital Heart Disease in Adult Patients 21
14. Pregnancy and Heart Disease 23
15. Valvular Heart Disease 25
16. Infective Endocarditis 26
17. Heart Failure (HF) 27
18. Pulmonary Arterial Hypertension 29
19. Rehabilitation and Exercise Physiology 30
20. Arrhythmias 31
21. Atrial Fibrillation 33
22. Syncope 34
23. Sudden Cardiac Death (SCD) and Resuscitation 36
24. Diseases of the Aorta and Trauma to the Aorta and Heart 37
25. Peripheral Arterial Vascular Diseases 38
26. Thromboembolic Venous Disease 39
27. The Cardiac Consult 41

The ESC Core Curriculum for the General Cardiologist is a major step forward towards the coordination of the training of cardiologists in Europe. With increasing workforce movement it is of great importance to assure that practical skills and theoretical knowledge of a general cardiologist are independent of the country where he or she has been trained. Over the coming months the Curriculum will be incorporated into an electronic platform that could form the basis of formative assessment necessary for certifi cation and revalidation. The ESC and UEMS (cardiology section) working through the National Societies are committed to delivering a European standard for cardiology that may prove to be a model for other medical specialties.
In addition, cardiology as a specialty is expanding, and many subspecialties, such as interventional cardiology, electrophysiology or cardiovascular imaging, to name just
a few, are emerging. In this context, defi nition of the core knowledge, required for all cardiologists, independent of their subspecialty, appears to be even more relevant.
Obviously, the success of the Core Curriculum depends on its adoption on the national level. Broad participation of specialists representing different National Societies of Cardiology, as well as the Working Groups, Associations and Councils, makes us hope that this document will gain universal acceptance and will form a base for training in most European countries.
Finally, we hope that well trained physicians across the continent will be able to contribute to achieve the mission of the European Society of Cardiology – reducing the burden of cardiovascular disease in Europe.
IV
Kim Fox, President European Society of Cardiology
Roberto Ferrari, President ElectEuropean Society of Cardiology
Foreword

Preface
The fi rst European Curriculum for General Cardiology was published in 2006. Building on the ESC Core Syllabus published two years previously, it provided for the fi rst time a detailed framework for harmonizing the training of Cardiologists in Europe, aimed at improving the quality and reliability of care of patients with Cardiovascular Diseases.
It was predicted that a curriculum for such a dynamic fi eld would require early and frequent revision and accordingly this fi rst revision of the curriculum comes just two years after its launch. Changes are generally modest but a number of important omissions from the fi rst edition have been addressed.
The Core Syllabus was intended primarily as a summary of the core knowledge base for Continuing Medical Education for trained cardiologists and thus omitted a fundamental subject for trainees, namely the Cardiovascular History and Physical Examination; this has been included and a chapter on the Cardiac Consultation has been added. Appropriate amendments to existing chapters have been made in response to the helpful feed back from representatives of ESC Constituent Bodies of National Societies, Associations, Working Groups and Councils as well as interested individuals.
The Curriculum will prove to be worthwhile and only achieve its aims if it is widely implemented. A signifi cant and exciting step is now underway as the European Board for the Specialty of Cardiology (EBSC), a joint venture between the European Society of Cardiology and the UEMS Cardiology Section, embarks on the creation of an electronic platform to deliver the Curriculum. This will serve a number of important functions. It will outline the curriculum to trainees and trainers on a repeated basis, link to the appropriate knowledge base incorporating regular formative assessment, and will detail and document the assessments appropriate for each of the necessary skills and behaviours. In short it will provide structure and facilitate documentation of a trainee’s progress through the curriculum.
We believe this revision has improved the curriculum, although the next is likely to be particularly important and potentially far reaching, based as it will be on feedback from two important sources. The fi rst will be those involved in building the electronic platform who will scrutinize the curriculum in the greatest of detail as they devise links to a knowledge base and assessments for each component. The second will follow from the fi eld testing of the users of the electronic platform.
We hope you fi nd this version of the Curriculum useful and look forward to your active participation in its implementation.
V
Peter KearneyChairman of the ESC Education Committee

Introduction
Cardiology is a clinical specialty in the fi eld of Medicine. Its practitioners have a particular interest and skills in the treatment of patients with diseases of the heart and the blood vessels, including the circulation to the lungs. The term “Cardiovascular Medicine” is an acceptable alternative title to “Cardiology”.
The Core Curriculum of the European Society of Cardiology aims to provide an agreed framework for the purposes of training doctors in the specialty. Furthermore, it provides a basis for the development of continuing medical education (CME) for trained, practicing Cardiologists.
The European Society of Cardiology (ESC) Core Syllabus, published in 2004, summarizes subject matter considered integral to the specialty. This serves two functions, 1) to defi ne the boundaries of the specialty and 2) determines the knowledge base on which the Curriculum is developed. The Core Curriculum goes signifi cantly beyond the Syllabus, in outlining the knowledge, skills and attitudes required of a General Cardiologist. More broadly it provides structure for the educational activities of the European Society of Cardiology both within its own organisation as well as in discussion with outside bodies. Ultimately, aiming to improve training standards for Cardiologists, the Core Curriculum offers an opportunity to favourably infl uence the European political agenda, thereby improving care for patients with cardiological disorders throughout Europe.
The European Society of Cardiology is committed to reviewing and revising the Curriculum on a regular basis. These reviews will cater for developments in the diagnostic and treatment modalities of this rapidly changing fi eld.
The process of creating and revising the Core Curriculum recognises two important dynamic infl uences.
The fi rst is that currently there are very different levels of curriculum development throughout Europe and indeed what subjects or activities are considered core to the specialty varies signifi cantly between different countries. The current document aims to offer a consensus as to what knowledge, skills and attitudes should be possessed by General Cardiologists in Europe.
Second, the Core Curriculum aims to defi ne what every Cardiologist should know. The European Board for the Specialty of Cardiology (EBSC) is coordinating curriculum development for the various sub-specialties in cardiology. The sub-specialty curricula defi ne the greater depth of knowledge and understanding expected of a sub-specialist in, for instance, Interventional Cardiology, Cardiac Imaging Modalities or Invasive Electrophysiology. It is clear that the interface between “core” and “sub-specialty” Cardiology will be a dynamic one, and will be revisited in future years. This interface is also modulated by the local degree of acceptance of formal sub-specialties, which differs considerably from country to country. It is understood that all Cardiologists with sub-specialty interests have completed training in General Cardiology. Additionally, an ongoing interest in the general breadth of the specialty is considered both necessary and important to ensure best practice of sub-specialty cardiology.
VI

Rationale - Summary of the Clinical Field of Cardiology
The clinical subject of Cardiology aims to deliver competent care for patients presenting with disorders of the heart, the pulmonary vasculature and the systemic arterial and venous systems. Currently, the commonest cardiovascular pathology is atherosclerosis as it affects the coronary and systemic arterial systems. An understanding of the risk factors and their modifi cation to minimise the long term adverse effects of atherosclerosis as well as the treatment of the complications of atherosclerosis, such as the acute coronary syndrome or heart failure, are major components of Cardiology. Many other important diseases affect the myocardium, the pericardium and the cardiac valves. Systemic diseases such as arterial hypertension or diabetes
affect not only cardiac, but also vascular structures, notably the arteries. Disorders of heart rhythm range from the benign to the life threatening. A comprehensive knowledge of these disorders, their diagnosis, including the array of imaging modalities of heart and vascular structure, and of the rapidly expanding pharmacologic, percutaneous, device-based, and surgical treatments for them are integral parts of the Core Curriculum. These topics are gathered together in this Core Curriculum to provide the standards for Training in Cardiology as well as a template for the maintenance of Clinical Competence for qualifi ed Cardiologists.
VII
Candidates for training should be licenced physicians in an EU country or have an equivalent qualifi cation approved by the host country.
It is understood that a common trunk of General Professional Training should be completed before Postgraduate Specialist training is undertaken. General Training should include a signifi cant knowledge of and exposure to the acute and chronic presentation of a broad range of medical conditions. It includes acquisition of generic knowledge and skills including communication training, bioethics, biostatistics, and the ability to analyse, interpret and utilize medical literature, elements of training and practice that are further reinforced during ongoing training. The trainee must have the necessary linguistic ability to communicate with patients and colleagues in the country of training.
The recommended minimum duration of postgraduate education is six years, to include two years of common trunk and a minimum of four years training in Cardiology, one of which is fl exible, and may be devoted to internal medicine, cardiovascular research, cardiovascular pharmacology, cardiovascular epidemiology, cardiovascular preventive medicine or rehabilitation, angiology or general cardiology or other related aspects of cardiovascular disease.
In order to gain suffi cient experience the trainee should be involved in the management of an appropriate mix and number of in-patients and out-patients. A full time position for at least one year is recommended. Part-time positions may make up the remaining training period which must be correspondingly prolonged. Practical participation in the clinical management of inpatients, including the coronary care unit and provision of cardiac
consultations for other services, should constitute a minimum of one year of training, preferably in the fi rst or second year. Supervised involvement in the management of outpatients, including new and return cases, should be undertaken at least once a week, for at least one year of training. The trainee should have an on-call commitment for Cardiology (rather than General Internal Medicine or unselected medical emergencies) of at least 100 nights during cardiology training. The training programme should include structured training sessions of at least two hours per week. Trainees should perform a suffi cient number of practical procedures of suffi cient diversity, as detailed in the Core Curriculum.
Not all elements of training (such as direct exposure to cardiac surgery) may be accessible at a single training centre. Candidates should have the opportunity to obtain training in all aspects of the curriculum, which may involve rotation through different training institutions or sessional attendance for training in centres providing treatments or technologies (such as a Adult Congenital Heart Disease clinic or Cardiac MRI) that are not widely available.
The training programme should be clearly defi ned, incorporate annual assessment of the trainee’s progress, and should itself be assessed on at least a fi ve yearly basis.
VIII
General Aspects of Training in the Specialty

Training institutions should be recognized by a National Training Authority as eligible to provide complete or partial training. They should offer the opportunity for interaction with other major specialties, have a library and internet facilities offering access to the current world scientifi c literature, specifi cally major international journals relating to Cardiology and Internal Medicine, and should provide the necessary physical infrastructure for training including conference rooms and allocated offi ce space for trainees.
The training institution or combination of institutions making up any given training programme should have the necessary facilities to ensure that trainees can fulfi ll all aspects of the curriculum, and the following facilities as a minimum: A fully equipped out-patient department for cardiological patients, including emergencies, a suffi cient number of beds for in-patients and for intensive care medicine. The intensive care unit should have at least 6 beds, fully equipped for electrocardiographic and haemodynamic monitoring, anti-bradycardiac pacing, cardioversion and
defi brillation and preferably haemodynamic support devices (intra-aortic balloon pumps, haemofi ltration etc.). The programme must incorporate an institution providing cardiac surgery. Equipment should be available for all types of non-invasive investigation and procedures such as X-ray, ECG, exercise testing, ambulatory ECG monitoring, echocardiography including Doppler echocardiography and transoesophageal echocardiography (TEE), pacemaker check-up and cardiac magnetic resonance imaging , cardiac computed tomography, and nuclear medicine facilities. The programme must include centres that provide invasive cardiology, including diagnostic and therapeutic cardiac catheterization and electrophysiological studies.
Trainers should be based in an eligible Training Centre, should be accredited, should have experience in Research and Teaching and should be recognized as a designated Trainer by the National Training Board. There should be a minimum number of senior trained specialists in the unit to ensure expert training for a range of areas included in the Core Curriculum, and suffi cient protected teaching time
and continuity of training. An equal number of trainers and trainees is recommended. Delivery of the curriculum may be facilited by a structure which includes a Director of Training (National/Regional), a Training Mentor, and multiple Clinical Trainers.
IX
Requirements for Training Institutions
Requirements for Trainers

Assessment is a key driver of learning and is an essential component of curricular development. Whereas summative tests are used to confi rm attainment of a stipulated level of competence and to rank candidates, assessment should as far as possible play a formative or active educational role. For each component of the curriculum, the relevant knowledge, skills and attitudes/behaviours require different and varied assessment methods. All methods have some limitations in terms of their validity to predict an individual’s competence in a reproducible manner. It is therefore recommended that a variety of suitable different methods involving a number of different observers be applied over time during training.
Knowledge: Tests of knowledge including multiple choice questionnaires are a familiar form of assessment. They are readily produced, are valid when properly designed and executed, but cannot constitute the only or predominant method of assessment.
Skills: A logbook, based on the curriculum, is an important means of documenting experience. It may provide a simple count of different procedures or conditions encountered or may encourage refl ection by including items such as complications. Structured skills evaluation methods such as DOPS (Direct Observation of Procedural Skills) should also be incorporated.
Attitudes/behaviours. A traditional method of assessing performance is a supervisor’s report, including considerations relating to clinical, clerical and team performance A more contemporary approach is the Multisource Feedback or 360˚assessment which is more objective, balanced and potentially more informative. This
entails a blinded, structured assessment of the candidate by colleagues from various disciplines (medical, nursing, paramedic, technician) and their patients. Whichever methods are adopted, the training programme should incorporate a series of interactive meetings between trainee and supervisor and trainee and the local or national director of training, during which the documentary evidence of training, including the portfolio, can be systematically considered. The portfolio includes a record of clinical experience, audit activity, presentations, and evidence of self directed learning. It should also include documentation of Research undertaken and completed by the candidate, considered essential for all Cardiologists in training.
Assessment methodology
X

These are specifi c statements of intent which express what the learner will be able to do at the end of the educational intervention. They are framed in terms of learners’ capabilities in specifi c tasks. Objectives are classifi ed under the headings of knowledge, skills and attitudes/behaviours.
Knowledge: The knowledge base trainees require. The subject matter is defi ned by the ESC Core Syllabus. In the curriculum it is framed in terms that refl ect how the trainee should handle this knowledge.
Skills: The effective application of knowledge to problem solving, clinical decision making and performing procedures, acquired from experience and training
Attitudes and behaviours: What attitudes or beliefs trainees develop and demonstrate in respect of the subject, and their impact on how they behave in real world practice.Each objective defi nes what is to be achieved, how it will be achieved (conditions or workplace context) and the standard required.
Categories / Levels of CompetenceIn the next section of the curriculum, mention is made of different levels of competence expected for a given area of subject matter. These are defi ned as follows.
Level I – Experience of selecting the appropriate diagnostic modality and interpreting results or choosing an appropriate treatment for which the patient should be referred. This level of competency does not include performing a technique. Examples are advanced methods of imaging or specialized interventions such as catheter ablation.
Level II – Practical experience but not as independent operator (has assisted in or performed a particular technique or procedure under the guidance of a superior). Examples are electrophysiological study or interventional cardiology.
Level III – Is able to independently perform the technique or procedure unaided (for the general cardiologist, these include; ECG, 24 hour long term ECG monitoring, pacemaker implantation, transthoracic echocardiography, and diagnostic cardiac catheterization.
Indicative NumbersFirst hand exposure and practical experience play an important role in the learning of techniques. Of itself,
the number of procedures engaged in by a trainee is not a suffi cient measure of his/her competence but reporting indicative numbers has a role in ensuring adequate exposure. The numbers in the following table are based on the European Board for the Specialty of Cardiology’s last update of the Cardiology section of Chapter 6 of the UEMS Charter for Medical Training in 2003, with appropriate additions and modifi cation where necessary. These fi gures relate to basic Cardiology training and clearly those sub-specialising in a particular aspect of cardiology will require greater numbers and higher levels of competence than stated for the relevant techniques. It is also recognised that in some countries the stated numbers may be diffi cult to achieve for some techniques due to the organisation of care. The numbers may be considered aspirational at the present time for such countries, but will likely be achievable as resources increases. Rotation of trainees through reference training centres offers an opportunity for most trainees in Europe to achieve these aims. Simulation training promises to play an increasingly important role in technical skills training and will likely reduce the numbers of actual procedures to which a trainee must have direct exposure to achieve competence.
LEARNING OBJECTIVESChapters in the Curriculum:
Technique NumberLevel of competence
ECG 1000 Level III
Ambulatory ECG 200 Level III
Exercise ECG testing 300 Level III
Ambulatory BP monitoring 100 Level III
Echo-Doppler studies 350 Level III
Transoesophageal echocardiography 50 Level II
Stress Echocardiography 50 Level II
Nuclear studies 50 Level II
Cardiac CT 50 Level II
MRI 50 Level II
Coronary and LV angiography 300 Level III
Percutaneous Intervention 50 Level II
Temporary pacemaker implantation 25 Level III
Pacemaker/ICD programming 50 Level II
Pacemaker implantation 50 Level II
ICD implantation 30 Level I
CRT implantation 10 Level I
Electrophysiological studies 50 Level II
Atrial Flutter/Atrial Fibrillation ablation 10 Level I XI

Acknowledgements
XII
This revision of the Core Curriculum has benefi ted from active contributions of National Cardiac Societies, ESC Associations, Working Groups, Councils and the European Board for the Subspecialty of Cardiology, all of which deserve our thanks. All members of the Education Committee of the ESC have devoted considerable time and energy to the process, but special mention must go to Dr. Frank Flachskampf who provided outstanding leadership and co-ordination of the revision and to Dr. Peter Mills for his contributions based on unique wisdom and experience in the fi eld. Our colleagues in Heart House, Dominique Poumeyrol-Jumeau, Claire Bramley, Celine Carrera and Keith McGregor have again provided outstanding support.

1
1. H
isto
ry t
akin
g a
nd
clin
ical
exa
min
atio
n
• •
• • • • •
• • • •
• • • • • • • • • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To o
btai
n a
hist
ory
from
the
patie
nt
rele
vant
to c
ardi
ovas
cula
r diso
rder
s:£ T
he p
atie
nt’s
spo
ntan
eous
acc
ount
of
sym
ptom
s£ Q
uest
ions
from
the
Car
diol
ogist
fo
cuse
d on
the
pres
ence
or a
bsen
ce o
f po
ssib
le c
ardi
ovas
cula
r sym
ptom
s £ T
he p
ast m
edic
al h
istor
y£ S
ympt
oms
of a
ny c
o-m
orbi
ditie
s£ T
he s
ocia
l hist
ory
£ C
urre
nt a
nd p
ast d
rug
ther
apy
To b
e ab
le to
des
crib
e th
e ra
nge
of, a
nd
the
mea
ning
of,
wor
ds u
sed
by p
atie
nts
to d
escr
ibe
card
iova
scul
ar s
yste
ms
To re
cogn
ize
clas
sical
sym
ptom
s of
ca
rdio
vasc
ular
dise
ase,
that
pat
ient
s w
ith c
ardi
ac c
hest
pai
n m
ay n
ot p
rese
nt
with
cla
ssic
al s
ympt
oms
and
to re
cogn
ize
the
char
acte
ristic
s of
non-
card
iac
ches
t pai
n To
reco
gniz
e ty
pica
l and
aty
pica
l sy
mpt
oms
of c
ardi
ovas
cula
r dise
ase
To re
cogn
ize
card
iova
scul
ar ri
sk fa
ctor
s fro
m th
e pa
tient
’s h
istor
yTo
kno
w th
e na
mes
and
sid
e ef
fect
s of
dr
ugs
used
To
kno
w th
e sy
mpt
oms
and
trea
tmen
ts
of th
e co
-mor
bidi
ties
ofte
n as
soci
ated
w
ith c
ardi
ovas
cula
r dise
ase.
To a
naly
se a
nd in
tegr
ate
the
info
rmat
ion
obta
ined
by
taki
ng a
hi
stor
y fro
m a
pat
ient
to c
ontr
ibut
e to
the
deve
lopm
ent o
f an
ove
rall
asse
ssm
ent
To b
e ab
le to
ass
ess
glob
al
card
iova
scul
ar ri
sk (w
ww
.hea
rtsc
ore.
org)
To e
stab
lish
a re
latio
nshi
p w
ith th
e pa
tient
bas
ed o
n em
path
y an
d tr
ust
To a
llow
the
patie
nt ti
me
to e
xpre
ss h
is or
her
sym
ptom
s in
thei
r ow
n w
ords
To b
e ab
le to
sym
path
etic
ally
dire
ct
open
end
ed q
uest
ions
to th
e pa
tient
To ta
ke in
to a
ccou
nt th
e im
port
ance
of
bot
h co
-mor
bidi
ties
and
soci
al
circ
umst
ance
s in
rela
tion
to
card
iova
scul
ar d
isord
ers
Clin
ical
exa
min
atio
n£ T
o co
mpl
emen
t the
sub
ject
ive
fi ndi
ngs
from
the
clin
ical
hist
ory,
w
ith th
e ob
ject
ive
fi ndi
ngs
on c
linic
al
exam
inat
ion
of th
e ca
rdio
vasc
ular
sy
stem
£ T
o pe
rform
a g
ener
al e
xam
inat
ion
of th
e pa
tient
sea
rchi
ng fo
r evi
denc
e of
co-
exist
ing
illnes
s, a
s w
ell a
s m
anife
stat
ions
of
card
iova
scul
ar
dise
ase
£ T
o ex
amin
e th
e pe
riphe
ral,
arte
rial a
nd
veno
us s
yste
ms.
£ T
o ex
amin
e th
e he
art
To b
e ab
le to
reco
gnise
the
feat
ures
on
gen
eral
exa
min
atio
n ca
used
by
card
iova
scul
ar d
iseas
eTo
kno
w h
ow to
exa
min
e th
e ar
teria
l pu
lse a
t diff
eren
t art
erie
s fo
r rat
e, rh
ythm
an
d ha
emod
ynam
ic pr
ofi le
, and
how
to
mea
sure
art
eria
l blo
od p
ress
ure
T o b
e ab
le to
exa
min
e th
e ve
nous
sys
tem
an
d in
par
ticul
ar to
be
able
to c
linica
lly
estim
ate
the
right
atri
al p
ress
ure
To b
e ab
le to
exa
min
e th
e pr
ecor
dial
impu
lseTo
und
erst
and
the
phys
iolo
gy a
nd
path
o-ph
ysio
logy
of t
he c
ardi
ac c
ycle
an
d th
eref
ore
to u
nder
stan
d ho
w
norm
al h
eart
sou
nds,
abn
orm
al h
eart
so
unds
and
sys
tolic
and
dia
stol
ic
mur
mur
s ar
e ge
nera
ted
and
how
to
best
aus
culta
te th
emTo
und
erst
and
the
path
o-ph
ysio
logy
of
the
clin
ical
sig
ns o
f und
er p
erfu
sion
and
fl uid
rete
ntio
nTo
und
erst
and
the
ankl
e-br
achi
al in
dex
as a
mea
sure
of p
erip
hera
l art
eria
l di
seas
e
To b
e ab
le to
mak
e an
d re
cord
acc
urat
e ob
serv
atio
ns a
bout
the
clin
ical
sta
te o
f th
e pa
tient
with
par
ticul
ar e
mph
asis
on
the
card
iova
scul
ar s
yste
m.
To b
e ab
le to
use
a s
teth
osco
pe a
nd
bloo
d pr
essu
re c
uff t
o m
axim
ise
the
info
rmat
ion
to b
e ga
ined
abo
ut
abno
rmal
ities
of t
he h
eart
and
blo
od
vess
els.
To b
e ab
le to
obt
ain
the
ankl
e-br
achi
al
inde
x as
a s
ign
of p
erip
hera
l art
eria
l di
seas
e
To e
xam
ine
the
patie
nt w
ith d
ue re
gard
fo
r the
pat
ient
s di
gnity
.To
con
tinua
lly s
eek
or c
orre
late
fi nd
ings
on
exa
min
atio
n w
ith s
ubse
quen
t fi n
ding
s at
ech
ocar
diog
raph
y or
sur
gery
, th
us e
mph
asisi
ng li
fe lo
ng le
arni
ng.

2
2. T
he
Elec
tro
card
iog
ram
:
sta
nd
ard
EC
G, a
mb
ula
tory
EC
G, e
xerc
ise
ECG
•• • • • • •
• •
• • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To s
elec
t, pe
rform
and
inte
rpre
t eac
h of
th
e th
ree
non-
inva
sive
ECG
tech
niqu
esU
se th
ese
mod
aliti
es to
iden
tify
the
norm
al E
CG
and
EC
G a
bnor
mal
ities
,in
par
ticul
ar:
£ ar
rhyt
hmia
s£ bu
ndle
bra
nch
bloc
ks£ hy
pert
roph
y£ ac
ute
and
chro
nic
ische
mia
£ Q
T ab
norm
aliti
es£ pe
ricar
ditis
£ el
ectr
olyt
e ab
norm
aliti
es£ pa
cem
aker
dys
func
tions
Cho
ose
the
appr
opria
te te
chni
ques
fo
r spe
cifi c
clin
ical
situ
atio
ns in
clud
ing
a th
orou
gh u
nder
stan
ding
of t
he
Baye
sian
appr
oach
.C
hoos
e te
chni
ques
mod
aliti
es a
nd
prot
ocol
s in
a c
linic
al u
sefu
l and
cos
t-ef
fect
ive
way
, avo
idin
g ov
er-
and
unde
r-ut
ilisat
ion
of te
sts
Inte
grat
e da
ta fr
om d
iffer
ent
elec
troc
ardi
ogra
phic
tech
niqu
es, a
s w
ell
as fr
om o
ther
non
-inva
sive
and
inva
sive
tech
niqu
es.
ECG
Des
crib
e th
e ph
ysio
logy
and
ana
tom
y of
the
cond
uctio
n sy
stem
.D
escr
ibe
the
cellu
lar a
nd m
olec
ular
m
echa
nism
s in
volv
ed in
the
elec
tric
al
activ
ity o
f the
hea
rt.
Des
crib
e th
e ba
sic p
rinci
ples
of E
CG
.U
nder
stan
d th
e no
rmal
evo
lutio
n of
the
elec
tric
al v
ecto
rs d
urin
g th
e ca
rdia
c cy
cle.
Reco
gnise
the
norm
al E
CG
, and
exp
lain
ho
w it
is fo
rmed
. D
escr
ibe
and
expl
ain
the
ECG
ch
arac
teris
tics
of a
tria
l and
ven
tric
ular
hy
pert
roph
ies,
bun
dle
bran
ch
bloc
ks a
nd o
ther
con
duct
ion
bloc
ks,
tach
ycar
dias
, bra
dyca
rdia
s, a
cute
an
d ch
roni
c m
yoca
rdia
l isc
hem
ia,
peric
ardi
tis a
nd m
yoca
rditi
s, e
lect
roly
te
abno
rmal
ities
, pre
exci
tatio
n, Q
T ab
norm
aliti
es, p
acem
aker
dys
func
tion.
Perfo
rm a
nd in
terp
ret E
CG
in th
e cl
inic
al
cont
ext (
a do
cum
ente
d in
dica
tive
num
ber b
eing
100
0) to
ach
ieve
leve
l III
com
pete
nce.
Dem
onst
rate
pro
fi cie
ncy
in s
elec
ting
the
follo
win
g EC
G te
chni
ques
nec
essa
ry fo
r th
e pa
tient
s’ m
anag
emen
t.
Reco
gnise
the
stre
ngth
s an
d w
eakn
esse
s of
EC
G in
a c
linic
al
situa
tion.
Coo
pera
te w
ith in
terv
entio
nal
card
iolo
gist
s, e
lect
roph
ysio
logi
sts,
an
aest
hetis
ts, c
ardi
ac s
urge
ons,
as
wel
l as
with
oth
er d
octo
rs in
volv
ed in
em
erge
ncy
med
icin
e an
d in
tens
ive
care
.Re
cogn
ise th
at th
e di
agno
sis a
nd
trea
tmen
t of s
ome
arrh
ythm
ias
need
so
met
imes
a m
ultid
iscip
linar
y ap
proa
ch.
Expl
ain
to p
atie
nts
and
thei
r fam
ily
the
impl
icat
ions
of t
he re
sults
of t
he
elec
troc
ardi
ogra
m.

3
The
Elec
tro
card
iog
ram
:st
and
ard
EC
G, a
mb
ula
tory
EC
G, e
xerc
ise
ECG
(con
tinue
d)
•
• • •
• •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Long
-ter
m a
mbu
lato
ry E
CG
and
EC
G
Loop
Rec
ordi
ngId
entif
y th
e in
dica
tions
Reco
gnise
the
limita
tions
Perfo
rm a
nd in
terp
ret a
mbu
lato
ry
ECG
s/lo
op re
cord
er E
CG
s in
the
clin
ical
co
ntex
t (a
docu
men
ted
indi
cativ
e nu
mbe
r bei
ng 2
00) t
o ac
hiev
e le
vel I
II co
mpe
tenc
e.
Reco
gnise
str
engt
hs a
nd w
eakn
esse
s of
am
bula
tory
EC
Gs/
loop
reco
rder
EC
Gs
in a
clin
ical
situ
atio
n.Ex
plai
n to
pat
ient
s an
d th
eir f
amily
the
impl
icat
ions
of t
he re
sults
obt
aine
d fro
m a
mbu
lato
ry E
CG
s/lo
op re
cord
er
ECG
s.
E
xerc
ise E
CG
Tes
ting
Reco
gnise
the
mai
n in
dica
tions
:£ Ev
alua
tion
of is
chem
ia£ Ev
alua
tion
of v
alvu
lar d
iseas
es£ Ev
alua
tion
of h
yper
trop
hic
card
iom
yopa
thy
£ Ev
alua
tion
of tr
eatm
ent r
espo
nse
£ Ev
alua
tion
of fu
nctio
nal c
apac
ity£ Ev
alua
tion
of in
duci
ble
arrh
ythm
ias
£ Id
entit
y th
e co
ntra
indi
catio
nsRe
cogn
ise th
e m
ain
limita
tions
:£ Id
entit
y th
e cr
iteria
for s
topp
ing
the
test
ing
£ Id
entif
y th
e co
mpl
icat
ions
and
thei
r tr
eatm
ent
Perfo
rm a
nd in
terp
ret e
xerc
ise E
CG
te
stin
g in
the
clin
ical
con
text
(a
docu
men
ted
indi
cativ
e nu
mbe
r bei
ng
300)
to a
chie
ve le
vel I
II co
mpe
tenc
e.M
anag
e co
mpl
icat
ions
in a
pro
per a
nd
timel
y w
ay.
Reco
gnise
str
engt
hs a
nd w
eakn
esse
s of
exe
rcise
EC
G te
stin
g in
a c
linic
al
situa
tion.
Expl
ain
to p
atie
nts
and
thei
r fam
ily
the
impl
icat
ions
of t
he re
sults
of t
he
elec
troc
ardi
ogra
m.
• ••
•
•
•
4
3. N
on
Inva
sive
Imag
ing
Ech
oca
rdio
gra
ph
y, C
MR,
Car
dia
c C
T an
d N
ucl
ear
tech
niq
ues
•• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
App
ropr
iate
ly s
elec
t fro
m th
e fo
ur im
agin
g m
odal
ities
of:
- Ec
hoca
rdio
grap
hy-
Car
diac
Mag
netic
Res
onan
ce (C
MR)
- C
ompu
ted
Tom
ogra
phy
(CT)
- N
ucle
ar T
echn
ique
san
d th
en in
tegr
ate
the
resu
lts in
to
indi
vidu
al p
atie
nt c
are
Use
thes
e m
odal
ities
to m
easu
re
card
iac
stru
ctur
e an
d fu
nctio
n.-
Vent
ricul
ar c
ham
ber a
nd w
all
dim
ensio
ns-
Left
ven
tric
ular
(LV
) Mas
s-
Vent
ricul
ar v
olum
es-
Ejec
tion
/ reg
urgi
tatio
n fra
ctio
ns-
Regi
onal
wal
l mot
ion
abno
rmal
ities
- Es
timat
ion
of s
hunt
siz
e-
Cal
cula
tion
of v
alve
ste
nosis
- Es
timat
ion
of v
alvu
lar r
egur
gita
tion
- Es
timat
ion
of L
V d
iast
olic
func
tion
- C
alci
fi cat
ion
of c
oron
ary
arte
ries
- M
yoca
rdia
l per
fusio
n-
Myo
card
ial d
iseas
e-
Cor
onar
y A
rter
yD
iseas
e-
Peric
ardi
al d
iseas
e-
Car
diac
tum
ours
- C
onge
nita
l hea
rt d
iseas
e-
Non
-inva
sive
coro
nary
ang
iogr
am-
Aor
tic d
iseas
es-
Dise
ases
of t
he p
ulm
onar
y ci
rcul
atio
n
Skills
are
spe
cifi c
to e
ach
mod
ality
. Se
e be
low
.C
hoos
e th
e ap
prop
riate
imag
ing
tech
niqu
es fo
r spe
cifi c
clin
ical
situ
atio
ns,
incl
udin
g a
thor
ough
und
erst
andi
ng o
f th
e Ba
yesia
n ap
proa
chC
hoos
e im
agin
g te
chni
ques
, mod
aliti
es
and
prot
ocol
s in
a c
linic
ally
use
ful a
nd
cost
effe
ctiv
e w
ay, a
void
ing
over
and
un
der u
tilisa
tion
of te
sts,
kee
ping
in
min
d ra
diat
ion
expo
sure
, whe
re
appr
opria
teIn
tegr
ate
data
from
diff
eren
t non
-in
vasiv
e te
chni
ques
as
wel
l as
from
in
vasiv
e im
agin
g Re
mai
n cu
rren
t with
dev
elop
men
ts in
th
e fi e
ld o
f non
-inva
sive
imag
ing
•
•
5
ESC
Gu
idel
ines
• C
linic
al ro
le o
f car
diac
mag
netic
reso
nanc
e in
car
diov
ascu
lar d
iseas
e. (E
urop
ean
Hea
rt J
ourn
al 1
998;
19:
19-
39)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
No
n In
vasi
ve Im
agin
gEc
ho
card
iog
rap
hy,
CM
R, C
ard
iac
CT
and
Nu
clea
r te
chn
iqu
es
•• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Echo
card
iogr
aphy
Tech
niqu
es:
- M
-mod
e-
2-di
men
siona
l (2D
) mod
e-
Dop
pler
imag
ing
(blo
od fl
ow a
nd
tissu
e)-
Con
tras
t ech
ocar
diog
raph
yIn
dica
tions
:-
Eval
uatio
n of
sys
tolic
and
dia
stol
ic
func
tion
(incl
udin
g ej
ectio
n fra
ctio
n) o
f th
e le
ft v
entr
icle
- Re
gion
al w
all m
otio
n ab
norm
aliti
es-
LV m
ass
- C
ham
ber v
olum
es a
ndw
all d
imen
sions
- C
ardi
omyo
path
ies
- Va
lvul
ar m
orph
olog
y an
d fu
nctio
n,
incl
udin
g st
enos
is an
d re
gurg
itatio
n-
Righ
t ven
tric
ular
func
tion
- Sh
unt l
esio
ns-
Peric
ardi
al m
asse
s (tu
mor
s, th
rom
bi,
vege
tatio
ns)
- C
onge
nita
l hea
rt d
iseas
e-
Aor
tic d
iseas
eM
odal
ities
- Tr
anst
hora
cic
echo
- St
ress
test
- C
ontr
ast e
choc
ardi
ogra
phy
- 3D
ech
ocar
diog
raph
y
Perfo
rm a
nd in
terp
ret t
rans
thor
acic
(le
vel I
II co
mpe
tenc
e) a
nd
tran
soes
opha
geal
and
str
ess
echo
card
iogr
aphy
(lev
el II
com
pete
nce)
. A
doc
umen
ted
broa
d ex
perie
nce
is re
quire
d. (m
inim
um o
f 6 m
onth
s ex
perie
nce
in a
n ec
ho la
bora
tory
and
≥3
50 tr
anst
hora
cic
echo
card
iogr
ams)
Stre
ss te
stin
g
Reco
gnise
str
engt
hs a
nd w
eakn
esse
s of
ec
hoca
rdio
grap
hy in
a c
linic
al s
ituat
ion
Coo
pera
te w
ith in
terv
entio
nal
card
iolo
gist
s, e
lect
roph
ysio
logi
sts,
an
esth
esio
logi
sts
and
othe
r phy
sicia
ns
invo
lved
in e
mer
genc
y m
edic
ine
and
inte
nsiv
e ca
re, a
nd w
ith c
ardi
ac
surg
eons
Ex
plai
n to
pat
ient
s th
e im
plic
atio
ns o
f th
e re
sults
of t
he e
choc
ardi
ogra
phy
test
Car
diov
ascu
lar
Mag
netic
Res
onan
ce (C
MR)
Tech
niqu
es-
2D m
ode
- Pe
rfusio
n im
agin
g-
Late
enh
ance
men
tIn
dica
tion
- Vo
lum
es-
Ejec
tion
fract
ion
- LV
mas
s-
Shun
tM
odal
ities
- C
ine-
MR
- M
R an
giog
raph
y-
TI im
agin
g
Sele
ct th
e ap
prop
riate
CM
R in
dica
tions
fo
r pat
ient
s w
ith k
now
n or
sus
pect
ed
card
iova
scul
ar d
iseas
es a
nd e
valu
ate
CM
R ex
amin
atio
ns in
the
clin
ical
co
ntex
t. Le
vel I
I com
pete
nce
requ
ires
a do
cum
ente
d in
volv
emen
t in
50
case
s an
d a
sugg
este
d at
tach
men
t of
1 m
onth
con
sistin
g of
four
35
hour
w
eeks
sup
ervi
sed
by a
leve
l III
expe
rt.
Coo
pera
te w
ith ra
diol
ogist
s an
d C
MR
and
radi
olog
y te
chni
cian
s.
•
• •
(con
tinue
d)
• • •
••

6
ESC
Gu
idel
ines
• C
linic
al ro
le o
f car
diac
mag
netic
reso
nanc
e in
car
diov
ascu
lar d
iseas
e. (E
urop
ean
Hea
rt J
ourn
al 1
998;
19:
19-
39)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
No
n In
vasi
ve Im
agin
gEc
ho
card
iog
rap
hy,
CM
R, C
ard
iac
CT
and
Nu
clea
r te
chn
iqu
es
•• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Car
diac
Com
pute
d To
mog
raph
yTe
chni
ques
- 2D
- 3D
Indi
catio
ns-
Cal
cium
sco
re-
Cor
onar
y A
rter
y D
iseas
e (C
AD
) (in
clud
ing
graf
ts a
nd s
tent
s)M
odal
ities
- U
ltra-
fast
CT
- C
oron
ary
angi
ogra
m
Eval
uate
CT
exam
inat
ions
in th
e cl
inic
al
cont
ext (
a do
cum
ente
d in
dica
tive
num
ber b
eing
50
case
s an
d su
gges
ted
expo
sure
of 8
hal
f day
ses
sions
, to
achi
eve
leve
l II c
ompe
tenc
e).
Coo
pera
te w
ith ra
diol
ogist
s an
d ra
diol
ogy
tech
nici
ans.
A
sses
s th
e sid
e ef
fect
s of
con
tras
t m
edia
and
reco
gniz
e th
e ris
k of
ra
diat
ion
to p
atie
nt a
nd p
erso
nnel
Nuc
lear
Imag
ing
Tech
niqu
es-
Plan
ar a
ngio
grap
hy-
SPEC
T-
Gat
ed S
PEC
T-
Gat
ed b
lood
poo
l SPE
CT
- PE
TTr
acer
s-
Thal
lium
- Te
chne
tium
-labe
led
trac
ers
- Fl
uoro
deox
yglu
cose
Indi
catio
ns-
Myo
card
ial p
erfu
sion
- V
iabi
lity
- RV
and
LV
vol
umes
- Ej
ectio
n fra
ctio
n-
Dia
stol
ic fu
nctio
n-
Phas
e an
lysis
for c
ardi
ac a
sync
hron
ic-
Shun
tM
odal
ities
- Re
st m
etab
olism
- St
ress
pro
toco
ls (e
xerc
ise o
r ph
arm
acol
ogic
al)
Eval
uate
car
diac
nuc
lear
exa
min
atio
ns
in th
e cl
inic
al c
onte
xt a
nd w
ith
refe
renc
e to
oth
er n
onin
vasiv
e an
d in
vasiv
e ap
proa
ches
. Le
vel I
I co
mpe
tenc
e re
quire
s a
docu
men
ted
indi
cativ
e nu
mbe
r of 5
0 ca
ses
and
sugg
este
d ex
posu
re o
f 20
half
day
sess
ions
. St
ress
test
ing
Cho
ose
the
appr
opria
te s
tres
s m
odal
ity
for a
par
ticul
ar p
atie
ntC
oope
rate
with
nuc
lear
med
icin
e ph
ysic
ians
and
tech
nici
ans
Reco
gnise
the
risk
of io
nizi
ng ra
diat
ion
for p
atie
nt a
nd p
erso
nnel
•
(con
tinue
d)
• • • • •
• •
• • ••

7
4. In
vasi
ve Im
agin
g –
Car
dia
c C
ath
eter
isat
ion
an
d A
ng
iog
rap
hy
• • • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
C
oron
ary
and
left
ven
tricu
lar a
ngio
grap
hy:
To
be
able
to p
erfo
rm a
nd in
terp
ret n
ative
cor
onar
y an
d su
rgica
l con
duit
angi
ogra
ms
and
left
ven
tricu
lar a
ngio
gram
s
C
ardi
ac c
athe
teris
atio
n:
To b
e ab
le to
per
form
and
inte
rpre
t rig
ht
a
nd le
ft h
eart
cat
hete
risat
ion.
Des
crib
e th
e pr
incip
les
of fl
uoro
scop
ic im
agin
g, ra
diat
ion
phys
ics a
nd s
afet
y.D
escr
ibe
the
pote
ntia
l com
plica
tions
of
card
iac
cath
eter
isatio
n an
d an
giog
raph
y (in
cludi
ng h
ypot
ensio
n, h
eart
failu
re,
arrh
ythm
ias,
isch
emic
neur
olog
ic da
mag
e,
myo
card
ial is
chae
mia
, con
trast
reac
tion,
ch
oles
tero
l em
bolis
m, r
enal
failu
re,
vasc
ular
com
plica
tions
retro
perit
onea
l bl
eedi
ng, a
nd c
ardi
ac ta
mpo
nade
).O
utlin
e th
e ra
diol
ogica
l ana
tom
y of
the
hear
t, ao
rta,
larg
e ve
ssel
s an
d co
rona
ry
arte
ries,
as
wel
l as
that
of t
he fe
mor
al,
radi
al a
nd b
rach
ial a
rter
ies
used
for
vasc
ular
acc
ess
durin
g ca
thet
erisa
tion.
Reco
gnise
pre
ssur
e w
avef
orm
s ob
tain
ed
durin
g ca
rdia
c ca
thet
erisa
tion.
Des
crib
e th
e ro
utin
e co
llect
ion
of
haem
odyn
amic
and
oxym
etric
dat
a, a
nd
how
to c
alcu
late
car
diac
out
put,
vasc
ular
re
sista
nces
, val
ve a
reas
, and
AV
shun
ts
from
mea
sure
men
ts.
Des
crib
e th
e di
ffere
nt p
ercu
tane
ous
and
cut d
own
tech
niqu
es o
f cat
hete
risat
ion.
Des
crib
e th
e di
ffere
nt ty
pe o
f cat
hete
rs
used
in c
oron
ary
arte
riogr
aphy
and
ca
rdia
c ca
thet
erisa
tion.
Des
crib
e th
e eq
uipm
ent u
sed
and
the
tech
niqu
e of
tran
sept
al c
ardi
ac
cath
eter
isatio
n, a
nd d
iscus
s its
ap
plica
tions
.
Dem
onst
rate
kno
wle
dge
of
cath
eter
isatio
n la
b eq
uipm
ent
(phy
siolo
gica
l mon
itorin
g, tr
ansd
ucer
s,
bloo
d ga
s an
alys
ers,
pow
er in
ject
or).
Obt
ain
perc
utan
eous
art
eria
l acc
ess
(fem
oral
, rad
ial,
brac
hial
) and
ven
ous
acce
ss a
nd a
chie
ve h
aem
osta
sis a
fter
ca
thet
erisa
tion.
Perfo
rm le
ft h
eart
cat
hete
rizat
ion
incl
udin
g co
rona
ry a
ngio
grap
hy,
vent
ricul
ogra
phy,
and
ang
iogr
aphy
of
coro
nary
byp
ass
graf
ts; a
doc
umen
ted
min
imum
exp
erie
nce
is re
quire
d.Pe
rform
righ
t hea
rt c
athe
teris
atio
n at
th
e be
dsid
e in
clud
ing
mea
sure
men
t of
card
iac
outp
ut, p
ress
ure
mea
sure
men
t an
d ox
ymet
ry; a
doc
umen
ted
min
imum
ex
perie
nce
is re
quire
d.D
emon
stra
te p
rofi c
ienc
y in
man
agin
g lif
e-th
reat
enin
g ar
rhyt
hmia
s an
d ot
her
emer
genc
y sit
uatio
ns in
the
cath
lab,
in
clud
ing
resu
scita
tion
and
life
supp
ort
mea
sure
s.Ev
alua
te n
orm
al a
nd p
atho
logi
cal
coro
nary
ang
iogr
ams.
ven
tric
ulog
ram
s,
aort
ogra
ms,
and
pul
mon
ary
angi
ogra
ms.
To a
ssum
e re
spon
sibilit
y fo
r ord
erin
g,
perfo
rmin
g an
d in
terp
retin
g in
vasiv
e te
sts,
by
appr
opria
tely
wei
ghin
g up
the
risks
and
ben
efi ts
of t
hese
pro
cedu
res.
Sele
ct th
e ap
prop
riate
trea
tmen
t m
odal
ity (m
edic
al, p
ercu
tane
ous
or
surg
ical
) bas
ed o
n th
e da
ta g
ener
ated
by
car
diac
cat
hete
risat
ion,
taki
ng th
e cl
inic
al c
onte
xt in
to a
ccou
nt.
Reco
gnise
the
limita
tions
and
pot
entia
l ris
k of
inva
sive
proc
edur
es a
nd to
in
form
pat
ient
s ac
cord
ingl
y.Re
cogn
ise th
e ris
ks o
f ion
izin
g ra
diat
ion
for t
he p
atie
nt a
nd c
linic
al p
erso
nnel
.C
onsu
lt an
d lia
ise w
ith n
urse
and
te
chni
cian
per
sonn
el a
nd s
peci
aliz
ed
phys
icia
ns s
uch
as in
terv
entio
nalis
ts,
elec
trop
hysio
logi
sts
or p
aedi
atric
ca
rdio
logi
sts
as a
ppro
pria
te
• •
• • • • • •
• • • • •

8
ESC
Gu
idel
ines
• C
linic
al ro
le o
f car
diac
mag
netic
reso
nanc
e in
car
diov
ascu
lar d
iseas
e. (E
urop
ean
Hea
rt J
ourn
al 1
998;
19:
19-
39)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Inva
sive
Imag
ing
– C
ard
iac
Cat
het
eris
atio
n a
nd
An
gio
gra
ph
y
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Expl
ain
whe
n an
d ho
w to
per
form
car
diac
pa
cing
and
peric
ardi
ocen
tesis
, and
the
pote
ntia
l com
plica
tions
ass
ocia
ted
with
its
use
.U
nder
stan
d th
e ba
sic p
rincip
les
and
indi
catio
ns fo
r int
raco
rona
ry u
ltras
ound
, D
oppl
er a
nd p
ress
ure
asse
ssm
ent.
(con
tinue
d)

9
5. G
enet
ics
•• • • •
• • • • •
• • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rsTo
be
able
to p
erfo
rm g
ener
al
card
iolo
gica
l ass
essm
ent a
nd tr
eatm
ent
of p
atie
nts
with
inhe
rited
or f
amilia
l ca
rdio
vasc
ular
dise
ase.
Des
crib
e th
e in
ciden
ce a
nd p
reva
lenc
e of
in
herit
ed c
ardi
ovas
cula
r diso
rder
s in
the
loca
l com
mun
ity.
Stat
e th
e ba
sic k
now
ledg
e of
car
diac
em
bryo
logy
and
maj
or g
ene
fam
ilies
invo
lved
in c
ardi
ogen
esis.
D
escr
ibe
the
prin
ciple
s of
Men
delia
n in
herit
ance
.D
escr
ibe
the
prin
ciple
s of
pol
ygen
ic ca
rdio
vasc
ular
dise
ases
(suc
h as
hyp
erte
nsio
n, d
iabe
tes
and
dysli
pida
emia
s)Re
call
know
ledg
e of
maj
or
mon
ogen
ic ca
rdio
vasc
ular
dise
ases
; hy
pert
roph
ic ca
rdio
myo
path
y, fa
milia
l ao
rtop
athi
es s
uch
as th
e M
arfa
n sy
ndro
me,
Ehl
ers
Dan
los
synd
rom
e,
and
Willi
am’s
syn
drom
e; fa
milia
l di
late
d ca
rdio
myo
path
ies;
fam
ilial
chan
nelo
path
ies;
fam
ilial d
isord
ers
of
sept
atio
n; fa
milia
l bas
is of
con
otru
ncal
an
omal
ies;
triso
mie
s in
par
ticul
ar tr
isom
y 21
; fam
ilial d
yslip
idae
mia
s in
par
ticul
ar
diso
rder
s of
the
low
den
sity
lipop
rote
in
rece
ptor
.Ex
plai
n th
e fa
milia
l bas
is of
inhe
rited
ca
rdia
c tu
mou
rs
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion.
Eval
uate
rele
vant
fam
ily h
istor
y an
d co
nstr
uct a
fam
ily p
edig
ree.
D
istin
guish
aut
osom
al d
omin
ant,
auto
som
al re
cess
ive,
X-li
nked
, and
m
itoch
ondr
ial p
atte
rns
of in
herit
ance
.D
emon
stra
te h
ow to
cou
nsel
inde
x ca
ses,
fam
ily m
embe
rs a
t risk
on
the
prob
abilit
y of
bei
ng a
ffect
ed b
y a
gene
tic c
ardi
ovas
cula
r diso
rder
.Re
cogn
ise p
robl
ems
with
ped
igre
e in
terp
reta
tion
such
as
inco
mpl
ete
pene
tran
ce, v
aria
ble
expr
essiv
ity, a
nd
age
rela
ted
patt
erns
of e
xpre
ssiv
ity.
Coo
pera
te w
ith c
linic
al g
enet
icist
sD
evel
op a
sys
tem
atic
met
hod
of
appr
oach
ing
a fa
mily
with
a p
oten
tially
in
herit
ed c
ardi
ovas
cula
r dise
ase.
Ado
pt a
ppro
pria
te c
ouns
elin
g sk
ills to
ex
plai
n, e
duca
te a
nd in
form
pat
ient
s fu
lly o
f the
nat
ure
of th
eir d
iseas
e,
the
diag
nost
ic te
sts
used
to m
ake
a di
agno
sis a
nd th
e in
here
nt s
tren
gths
an
d w
eakn
esse
s of
suc
h di
agno
stic
te
sts
in in
divi
dual
s at
risk
. C
onsu
lt w
ith p
atie
nts
and
thei
r fam
ily
mem
bers
impr
ovin
g re
cogn
ition
and
m
anag
emen
t of f
amilia
l car
diov
ascu
lar
dise
ase
Con
sult
with
med
ical
pro
fess
iona
ls of
oth
er s
peci
altie
s on
pat
ient
s w
ith
gene
tic d
isord
ers

10ES
C G
uid
elin
es•
Exp
ert
cons
ensu
s do
cum
ent
on t
he u
se o
f ant
ipla
tele
t ag
ents
. (Eu
rope
an H
eart
Jou
rnal
200
4; 2
5: 1
66-1
81)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
6. C
linic
al P
har
mac
olo
gy
• • • •
• • • • • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To m
aste
r the
theo
ry a
nd p
ract
ice
of s
tate
of t
he a
rt p
harm
acol
ogic
al
trea
tmen
t of c
ardi
ovas
cula
r diso
rder
s
Reco
gnise
the
class
ifi cat
ion
and
mod
e of
act
ion
of d
rugs
(with
em
phas
is on
an
giot
ensin
-con
vert
ing
enzy
me
inhi
bito
rs,
angi
oten
sin-re
cept
or b
lock
ers,
ald
oste
rone
an
tago
nist
s, a
ntia
rrhyt
hmic
drug
s, b
eta-
bloc
kers
, cal
cium
ant
agon
ists,
diu
retic
s,
lipid
-low
erin
g dr
ugs,
ant
ipla
tele
t age
nts,
an
ticoa
gula
nts,
inot
rope
s, d
igita
lis, n
itrat
es,
othe
r vas
odila
tatin
g dr
ugs,
dru
gs w
ith
card
iac
toxic
ity a
nd o
ther
dru
gs w
ith n
ovel
m
echa
nism
s of
act
ion
like
reni
n-in
hibi
tors
or
pota
ssiu
m c
hann
el b
lock
ers)
Reco
gnise
for t
he d
rugs
liste
d ab
ove:
- Pha
rmac
okin
etics
(abs
orpt
ion,
bi
oava
ilabi
lity,
dist
ribut
ion,
bi
otra
nsfo
rmat
ion,
exc
retio
n)- P
harm
acod
ynam
ics- P
harm
acog
enet
ics- I
ndica
tions
.- C
ontra
indi
catio
ns- I
nter
actio
ns- A
dver
se e
ffect
s an
d to
xicity
.Pe
rform
and
inte
rpre
t dia
gnos
tic te
sts
to
asse
ss d
rug
effi c
acy
and
safe
ty (l
abor
ator
y te
sts,
ECG
and
hae
mod
ynam
ic m
onito
ring,
Ec
ho).
Des
crib
e ba
sic k
now
ledg
e of
rand
omise
d cli
nica
l tria
ls an
d ev
iden
ce b
ased
med
icine
.
Take
a re
leva
nt h
istor
y of
a p
atie
nt’s
m
edic
atio
n re
gim
e, in
clud
ing
purc
hase
of
ove
r the
cou
nter
med
icin
esA
sses
s th
e ris
ks a
nd b
enefi
ts o
f pr
escr
ibin
g an
indi
vidu
aliz
ed d
rug
trea
tmen
t reg
imen
for a
giv
en
card
iova
scul
ar c
ondi
tion.
Mon
itor t
he d
esire
d ef
fect
s of
a
patie
nt’s
dru
g th
erap
y an
d al
so th
e sid
e ef
fect
s. F
rom
this,
be
able
to
mak
e ap
prop
riate
mod
ifi ca
tions
to th
e tr
eatm
ent r
egim
en.
Reco
gnise
and
man
age
poss
ible
dru
g in
tera
ctio
ns (i
nclu
ding
trea
tmen
ts o
f co
ncom
itant
dise
ases
).Ev
alua
te th
e de
sign
and
resu
lts o
f pu
blish
ed c
linic
al tr
ials.
Iden
tify
and
inco
rpor
ate
the
impo
rtan
ce
of h
erba
l rem
edie
s ta
ken
by p
atie
nts.
Inco
rpor
ate
the
prin
cipl
es o
f evi
denc
e ba
sed
ther
apy
and
cur
rent
Gui
delin
es
into
clin
ical
pra
ctic
e.C
omm
unic
ate
with
pat
ient
s an
d th
eir
fam
ily m
embe
rs to
impr
ove
trea
tmen
t co
mpl
ianc
e, a
nd to
ens
ure
early
re
cogn
ition
of p
ossib
le a
dver
se e
ffect
s.C
onsid
er c
ost-
effe
ctiv
enes
s an
d fe
asib
ility
of th
e pr
escr
ibed
trea
tmen
t re
gim
en.
•

11
7. C
ard
iova
scu
lar
Dis
ease
Pre
ven
tion
–
Ris
k Fa
cto
rs, A
sses
smen
t an
d M
anag
emen
t
• • • • • • • •
• • • • • •
• • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To a
sses
s an
d tr
eat p
atie
nts
with
risk
fa
ctor
s fo
r car
diov
ascu
lar d
iseas
e.To
be
able
to e
valu
ate
how
diff
eren
t pr
even
tion
met
hods
wor
k.To
des
crib
e ca
rdio
vasc
ular
dise
ase
and
risk
fact
ors
in th
e lo
cal c
omm
unity
.To
con
trib
ute
to th
e gl
obal
effo
rts
in
redu
cing
Car
diov
ascu
lar m
orbi
dity
an
d m
orta
lity
by c
omm
unic
atin
g th
e pr
even
tion
mes
sage
to th
e pu
blic
.To
app
roac
h ris
k pr
even
tion
in a
hol
istic
w
ay, u
nder
stan
ding
the
pote
ntia
tion
of
card
iova
scul
ar ri
sk b
y cl
uste
ring
of ri
sk
fact
ors.
Defi
ne
epid
emio
logy
of c
ardi
ovas
cula
r di
seas
e in
the
loca
l com
mun
ity:
inci
denc
e, p
reva
lenc
e, s
urvi
val
Defi
ne
risk
fact
ors
and
desc
ribe
dist
ribut
ion
and
frequ
ency
of h
igh
risk
cond
ition
s in
the
loca
l com
mun
ityEx
plai
n ris
k as
sess
men
t in
prim
ary
prev
entio
n, m
ultif
acto
rial r
isk
inte
ract
ion:
risk
sco
ring
char
ts.
Expl
ain
diet
and
nut
ritio
n in
rela
tion
to
card
iova
scul
ar ri
sk m
anag
emen
t.D
escr
ibe
spec
ial t
reat
men
t/pr
even
tion
stra
tegi
es fo
r sm
okin
g, d
yslip
idae
mia
, di
abet
es m
ellit
us, h
yper
tens
ion,
ph
ysic
al in
activ
ity, l
eft v
entr
icul
ar
hype
rtro
phy
(LV
H),
obes
ity, m
etab
olic
sy
ndro
me,
psy
chos
ocia
l fac
tors
.Re
cogn
ise th
at ri
sk fa
ctor
s of
ten
clus
ter
and
requ
ire a
com
preh
ensiv
e ap
proa
ch.
Expl
ain
risk
asse
ssm
ent i
n se
cond
ary
prev
entio
n in
clud
ing
drug
ther
apy.
Reco
gnise
the
com
plic
atio
ns a
nd
cons
eque
nces
of s
peci
fi c ri
sk fa
ctor
s.
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion.
Eval
uate
CV
D ri
sk a
nd a
sses
s gl
obal
CV
D ri
sk a
t ind
ivid
ual l
evel
(H
eart
SCO
RE).
Eval
uate
CV
D ri
sk a
t pop
ulat
ion
leve
l (m
orta
lity,
mor
bidi
ty, d
isabi
lity)
Eval
uate
the
bene
fi t o
f pre
vent
ion
at
indi
vidu
al a
nd p
opul
atio
n le
vels
Man
age
risk
fact
ors
appr
opria
tely
and
co
mm
unic
ate
thei
r im
port
ance
to
patie
nts,
thei
r fam
ilies
and
the
wid
er
com
mun
ity.
Eval
uate
the
risk
of C
VD
for a
n in
divi
dual
pat
ient
.Ev
alua
te th
e be
nefi t
of r
isk fa
ctor
in
terv
entio
n fo
r the
indi
vidu
al p
atie
nt.
App
reci
ate
the
impo
rtan
ce o
f risk
fact
or
man
agem
ent.
App
reci
ate
varia
tion
in C
VD
risk
s ac
ross
po
pula
tion,
soc
ioec
onom
ic, g
ende
r, an
d ra
cial
gro
ups.
Thro
ugh
patie
nt e
duca
tion,
en
cour
age
a he
alth
ier l
ifest
yle
with
sp
ecifi
c em
phas
is on
risk
fact
ors
and
mai
nten
ance
of f
avou
rabl
e ris
k pr
ofi le
ov
er li
fetim
e.O
ffer a
dvic
e an
d su
ppor
t to
fam
ily
mem
bers
with
inhe
rited
CV
D.
Coo
pera
te w
ith o
ther
spe
cial
ists
such
as
diet
icia
ns, d
iabe
tolo
gist
s an
d sp
ecia
list n
urse
s.To
par
ticip
ate
activ
ely
at C
VD
pr
even
tion
prog
ram
s ( c
hild
ren,
adu
lts
and
elde
rly)..
To c
onsid
er c
ost-
effe
ctiv
enes
s of
the
pres
crib
ed tr
eatm
ent r
egim
en.
• • • • •

12
Car
dio
vasc
ula
r D
isea
se P
reve
ntio
n –
Risk
Fac
tors
, Ass
essm
ent
and
Man
agem
ent
• • • • • • • • • • • •
• • • • •
• • •
• • • • • • • • •
• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Hyp
erte
nsio
n
To d
iagn
ose
and
trea
t diff
eren
t for
ms
of
arte
rial h
yper
tens
ion.
To a
sses
smen
t car
diac
and
oth
er e
nd-
orga
n co
mpl
icat
ions
in p
atie
nts
with
ar
teria
l hyp
erte
nsio
n.
Defi
ne
the
epid
emio
logy
aet
iolo
gy
and
path
ophy
siolo
gy o
f Ess
entia
l H
yper
tens
ion.
Des
crib
e th
e co
mpl
icat
ions
an
d co
nseq
uenc
es o
f ess
entia
l hy
pert
ensio
n.D
escr
ibe
the
diag
nosis
and
ass
essm
ent
of e
ssen
tial h
yper
tens
ion;
- Bl
ood
pres
sure
mea
sure
men
t, in
clud
ing
ambu
lato
ry b
lood
pre
ssur
e m
onito
ring
- Sy
mpt
oms
and
signs
of t
arge
t org
an
dam
age
- D
iagn
ostic
pro
cedu
res
Elab
orat
e th
e m
anag
emen
t of e
ssen
tial
hype
rten
sion.
Defi
ne
seco
ndar
y hy
pert
ensio
n an
d re
call
its v
ario
us c
ause
s-
Reno
vasc
ular
hyp
erte
nsio
n-
Bila
tera
l ren
al p
aren
chym
al d
iseas
e-
Hyp
erte
nsio
n in
duce
d by
hor
mon
al
cont
race
ptiv
es a
nd c
onju
gate
d oe
stro
gens
- O
ther
form
s of
sec
onda
ry
hype
rten
sion.
Out
line
the
cell
biol
ogy
of le
ft
vent
ricul
ar h
yper
trop
hy
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion.
Ass
ess
bloo
d pr
essu
re u
sing
the
corre
ct
met
hods
for d
iagn
osis
and
trea
tmen
t co
ntro
l in
hype
rten
sion,
incl
udin
g am
bula
tory
blo
od p
ress
ure
mon
itorin
g.A
dvise
pat
ient
s on
life
styl
e m
anag
emen
t an
d tr
eatm
ent c
ompl
ianc
e.A
dvise
pat
ient
s on
mea
surin
g th
eir o
wn
bloo
d pr
essu
re.
Perfo
rm c
ost e
ffi ci
ent s
cree
ning
for
seco
ndar
y hy
pert
ensio
n.Se
lect
ade
quat
e tr
eatm
ent f
or lo
wer
ing
Bloo
d Pr
essu
re to
targ
et v
alue
s an
d pr
even
t/tr
eat e
nd-o
rgan
dam
age.
Sele
ct a
ppro
pria
te p
aram
eter
s in
ord
er to
de
scrib
e th
e ris
k pr
ofi le
in a
n in
divi
dual
pa
tient
with
hyp
erte
nsio
n.Id
entif
y se
cond
ary
orga
n da
mag
e (in
pa
rtic
ular
car
diac
, neu
rolo
gica
l, re
nal a
nd
athe
rosc
lero
tic v
ascu
lar d
iseas
e) c
ause
d by
hyp
erte
nsio
n.M
anag
e m
ulti-
drug
trea
tmen
t reg
imes
ac
cord
ing
to a
pat
ient
’s c
o-m
orbi
ditie
s an
d po
ssib
le s
ide
effe
cts.
Reco
gnise
that
the
diag
nosis
and
tr
eatm
ent o
f hyp
erte
nsio
n ne
ed a
m
ultid
iscip
linar
y ap
proa
ch.
Be a
ble
to m
otiv
ate
the
patie
nt to
m
aint
ain
long
term
com
plia
nce
with
an
tihyp
erte
nsiv
e th
erap
y.A
ppre
ciat
e th
at h
yper
tens
ion
itsel
f is
ofte
n un
der d
iagn
osed
and
und
er
-tre
ated
.Re
cogn
ise th
e cl
uste
ring
of ri
sk fa
ctor
s th
at in
clud
e hy
pert
ensio
n in
ord
er to
fo
rmul
ate
a ho
listic
app
roac
h to
pat
ient
m
anag
emen
t
Dys
lipid
emia
To d
iagn
ose
and
trea
t diff
eren
t for
ms
of
dysli
pide
mia
.To
ass
ess
card
iac
and
extr
a-ca
rdia
c co
mpl
icat
ions
of d
yslip
idem
ia.
Defi
ne
the
epid
emio
logy
, aet
iolo
gy a
nd
path
ophy
siolo
gy o
f dys
lipid
emia
Des
crib
e th
e co
mpl
icat
ions
and
co
nseq
uenc
es o
f dys
lipid
emia
Des
crib
e th
e di
agno
sis a
nd a
sses
smen
t of
dys
lipid
emia
.El
abor
ate
the
man
agem
ent o
f dy
slipi
dem
ia.
Out
line
the
cell
biol
ogy
of
athe
rosc
lero
sis.
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion.
Ass
ess
dysli
pide
mia
usin
g th
e co
rrect
m
etho
ds fo
r dia
gnos
is an
d th
erap
eutic
co
ntro
l.A
dvise
pat
ient
s on
life
styl
e m
anag
emen
t an
d tr
eatm
ent c
ompl
ianc
e.A
dvise
pat
ient
s on
mea
surin
g th
eir l
ipid
s.Se
lect
ade
quat
e tr
eatm
ent f
or lo
wer
ing
bloo
d pr
essu
re to
targ
et v
alue
s an
d pr
even
t/tr
eat i
ts c
onse
quen
ces
Reco
gnise
that
the
diag
nosis
and
tr
eatm
ent o
f dys
lipid
emia
som
etim
es
need
a m
ultid
iscip
linar
y ap
proa
ch.
Be a
ble
to m
otiv
ate
the
patie
nt to
m
aint
ain
long
-ter
m c
ompl
ianc
e w
ith
antih
yper
tens
ive
lipid
low
erin
g th
erap
y Re
cogn
ise th
e cl
uste
ring
of ri
sk fa
ctor
s th
at in
clud
e dy
slipi
dem
ia in
ord
er to
fo
rmul
ate
an in
tegr
ated
app
roac
h to
pa
tient
man
agem
ent.
• • • •
(con
tinue
d)

13
[1] E
SC G
uide
lines
on
the
Four
th J
oint
Eur
opea
n So
ciet
ies’
Tas
k Fo
rce
on c
ardi
ovas
cula
r dise
ase
prev
entio
n in
clin
ical
pra
ctic
e. E
xecu
tive
Sum
mar
y (E
urop
ean
Hea
rt J
ourn
al 2
007;
28:2
375-
2414
) and
Ful
l tex
t (Eu
rope
an J
ourn
al o
f C
ardi
ovas
cula
r Pre
vent
ion
and
Reha
bilit
atio
n 20
07; 1
4(su
ppl 2
):S1-
S113
)
Car
dio
vasc
ula
r D
isea
se P
reve
ntio
n –
Risk
Fac
tors
, Ass
essm
ent
and
Man
agem
ent
• • • • •
• • • • •
• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Sele
ct a
ppro
pria
te p
aram
eter
s to
de
scrib
e th
e ris
k pr
ofi le
in a
n in
divi
dual
pa
tient
with
dys
lipid
emia
Iden
tify
othe
r vas
cula
r are
as a
ffect
ed
by a
ther
oscl
eros
ic v
ascu
lar d
iseas
eM
anag
e m
ultid
rug
trea
tmen
t reg
imen
s ac
cord
ing
to a
pat
ient
’s c
omor
bidi
ties
and
poss
ible
sid
e ef
fect
s.
Dia
betic
hea
rt d
iseas
e
Dia
gnos
e an
d tr
eat c
ardi
ovas
cula
r co
mpl
icat
ions
in th
e di
abet
ic p
atie
nt,
appr
ecia
ting
the
cont
inuu
m ra
ngin
g fro
m im
paire
d fa
stin
g gl
ucos
e to
in
sulin
dep
ende
nt d
iabe
tes
and
its
com
plic
atio
ns.
Defi
ne
Dia
bete
s M
ellit
usD
escr
ibe
the
role
of d
iabe
tes
in
Cor
onar
y he
art d
iseas
e in
the
follo
win
g ar
eas
- Ep
idem
iolo
gy -
Pat
hoph
ysio
logy
of c
ardi
ovas
cula
r co
mpl
icat
ions
- Ro
le o
f risk
fact
or in
terv
entio
n-
scre
enin
g fo
r CA
D in
dia
betic
s-
scre
enin
g fo
r dia
bete
s in
CA
D (o
ral
gluc
ose
test
ing)
Des
crib
e th
e pa
thop
hysio
logy
of
dia
bete
s an
d its
non
-car
diac
an
d ca
rdia
c co
mpl
icat
ions
(CA
D,
diab
etic
car
diom
yopa
thy,
aut
onom
ic
neur
opat
hy a
nd it
s ca
rdio
vasc
ular
af
fect
s).
Out
line
trea
tmen
ts in
clud
ing
diet
, ex
erci
se, h
ypog
lyca
emic
dru
gs a
nd
insu
linEx
plai
n cu
rren
t thi
nkin
g re
gard
ing
the
conc
ept o
f the
met
abol
ic s
yndr
ome
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Man
age
the
prev
entio
n, d
iagn
osis
and
trea
tmen
t of d
iabe
tes
and
its a
ssoc
iate
d ca
rdio
vasc
ular
com
plic
atio
ns.
Act
ivel
y pa
rtic
ipat
e in
a m
ultid
iscip
linar
y ne
twor
k of
phy
sicia
ns a
nd a
ssist
ant
med
ical
per
sonn
el in
ord
er to
trea
t pa
tient
s w
ith d
iabe
tes
adeq
uate
ly
acco
rdin
g to
dise
ase
stat
e an
d co
mpl
icat
ions
.
Und
erst
and
the
mul
tidisc
iplin
ary
appr
oach
to th
e pa
tient
with
dia
bete
s.Be
aw
are
of th
e im
port
ance
of
reco
gnisi
ng th
e co
ntin
uum
that
ex
tend
s fro
m p
rimar
y pr
even
tion
to
trea
tmen
t of e
nd o
rgan
dam
age.
App
reci
ate
the
impo
rtan
ce o
f tre
atin
g as
ympt
omat
ic p
atie
nts
in o
rder
to
impr
ove
prog
nosis
.Re
cogn
ise th
e cl
uste
ring
of ri
sk fa
ctor
s th
at in
clud
e di
abet
es in
ord
er to
fo
rmul
ate
a ho
listic
app
roac
h to
pat
ient
m
anag
emen
t
•
(con
tinue
d)

14
8. A
cute
Co
ron
ary
Syn
dro
mes
(A
CS)
• • • • • •
• • • • • • • • • •
• • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith a
cute
cor
onar
y sy
ndro
mes
in
clud
ing
- ST
EMI (
ST s
egm
ent e
leva
tion
myo
card
ial i
nfar
ctio
n)-
Non
-STE
MI
- U
nsta
ble
angi
na
Out
line
the
mai
n as
pect
s of
the
path
ophy
siolo
gy o
f acu
te c
oron
ary
synd
rom
es; M
yoca
rdia
l isc
haem
ia,
Ath
eros
cler
osis
of th
e ep
icar
dial
co
rona
ry a
rter
ies,
Eve
nts
that
pr
ecip
itate
AC
S, N
on-a
ther
omat
ous
CA
DD
escr
ibe
the
dom
inan
t clin
ical
feat
ures
of
AC
S; C
ardi
ac is
chae
mic
che
st p
ain,
ex
amin
atio
n of
CV
sys
tem
in A
CS,
Sile
nt
ischa
emia
and
infa
rctio
nD
escr
ibe
the
diag
nost
ic p
roce
ss i
n un
stab
le a
ngin
a an
d no
n-ST
ele
vatio
n M
I - a
naly
sis o
f sym
ptom
s an
d cl
inic
al
diffe
rent
ial d
iagn
osis,
12-
lead
EC
G,
Labo
rato
ry s
tudi
es, I
mag
ing
mod
aliti
esD
escr
ibe
the
diag
nost
ic p
roce
dure
s in
A
MI -
ana
lysis
of s
ympt
oms
and
clin
ical
di
ffere
ntia
l dia
gnos
is, 1
2-le
ad E
CG
, La
bora
tory
stu
dies
, Im
agin
g m
odal
ities
Des
crib
e th
e po
tent
ial c
ompl
icat
ions
of
AM
I; M
yoca
rdia
l Is
chem
ia, A
rrhy
thm
ias
and
Mec
hani
cal c
ompl
icat
ions
Des
crib
e tr
eatm
ent o
ptio
ns fo
r A
MI;
Pre-
hosp
ital a
nd e
arly
-hos
pita
l ad
junc
tive
phar
mac
olog
ical
ther
apy,
pe
rcut
aneo
us c
oron
ary
inte
rven
tion
(PC
I), C
oron
ary
bypa
ss g
raft
ing
(CA
BG),
early
in-h
ospi
tal.
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
App
reci
ate
the
role
of r
isk fa
ctor
s,
the
clin
ical
cha
ract
erist
ics
of c
oron
ary
occl
usio
n, a
nd s
ubse
quen
t clin
ical
co
urse
.In
terp
ret b
ioch
emic
al m
arke
rs o
f m
yoca
rdia
l dam
age.
Inte
rpre
t EC
G a
nd im
agin
g te
chni
ques
to
det
ect a
nd lo
cate
isch
aem
ia a
nd/o
r in
farc
tion.
U
nder
stan
d th
e im
port
ance
of
mon
itorin
g pa
tient
s w
ith A
CS.
Prov
ide
appr
opria
te p
harm
acol
ogic
al
trea
tmen
t inc
ludi
ng a
nalg
esic
, an
tipla
tele
t, an
d an
tithr
ombo
tic a
nd
anti-
ischa
emic
ther
apy.
Und
erst
and
indi
catio
ns a
nd
cont
rain
dica
tions
for a
cute
repe
rfusio
n tr
eatm
ent a
nd m
ake
appr
opria
te
deci
sions
.D
emon
stra
te p
rofi c
ienc
y in
sel
ectin
g ca
rdia
c ca
thet
erisa
tion
in th
e co
ntex
t of
AC
S.D
emon
stra
te p
rofi c
ienc
y in
trea
ting
patie
nts
with
hea
rt fa
ilure
and
ca
rdio
geni
c sh
ock,
incl
udin
g in
vasiv
e ha
emod
ynam
ic m
onito
ring.
Dem
onst
rate
kno
wle
dge
of a
dvan
ced
CPR
tech
niqu
es a
nd m
anag
emen
t of
life
thre
aten
ing
arrh
ythm
ias.
Reco
gnise
the
urge
ncy
of o
rgan
ised
team
wor
k re
quire
d fo
r the
opt
imal
m
anag
emen
t of p
atie
nts
with
AC
S.Re
cogn
ise th
e ur
genc
y of
mak
ing
rapi
d de
cisio
ns re
gard
ing
patie
nts
with
AC
S,
from
the
time
of th
eir a
rriv
al in
the
emer
genc
y de
part
men
t unt
il de
fi niti
ve
ther
apy
is es
tabl
ished
(for
exa
mpl
e m
inim
ising
doo
r-to-
ballo
on/n
eedl
e tim
e).
App
reci
ate
the
dist
ress
that
une
xpec
ted
and
serio
us il
lnes
s ca
uses
bot
h to
the
patie
nt a
nd th
eir r
elat
ives
.Re
cogn
ise w
hen
to tr
ansf
er th
e pa
tient
to
ano
ther
hos
pita
l for
inte
rven
tiona
l or
surg
ical
reva
scul
arisa
tion.
Con
trib
ute
to im
prov
ing
publ
ic
awar
enes
s of
the
signi
fi can
ce o
f ch
est p
ain
and
enco
urag
ing
early
pr
esen
tatio
n.
•

15
ESC
Gu
idel
ines
• G
uide
lines
on
the
Man
agem
ent
of N
on-S
T Se
gmen
t El
evat
ion
Acu
te C
oron
ary
Synd
rom
es (E
urop
ean
Hea
rt J
ourn
al, 2
007;
28
(13)
: 159
8-16
60).
• G
uide
lines
for P
ercu
tane
ous
Cor
onar
y In
terv
ensio
ns (P
CI)
(Eur
opea
n H
eart
Jou
rnal
, 200
5; 2
6 (8
): 80
4-84
7).
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Acu
te C
oro
nar
y Sy
nd
rom
es (
AC
S)
• • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To u
nder
stan
d in
dica
tions
, tec
hniq
ues,
ty
pica
l acu
te a
nd lo
ng-t
erm
pro
blem
s,
limita
tions
, com
plic
atio
ns, a
ltern
ativ
es,
and
adju
nctiv
e ph
arm
acot
hera
py o
f PC
I
Know
mec
hani
sms
of a
ctio
n of
mai
n PC
I tec
hniq
ues
(bal
loon
ang
iopl
asty
, st
ent i
mpl
anta
tion,
rota
blat
ion)
.U
nder
stan
d fu
ndam
enta
l cha
ract
erist
ics
of b
allo
ons
and
sten
ts, i
nclu
ding
typi
cal
leng
ths
and
diam
eter
s, a
ntip
rolif
erat
ive
drug
coa
ting.
Und
erst
and
the
prob
lem
of r
este
nosis
, ac
ute
and
suba
cute
ste
nt th
rom
bosis
, an
d ap
prop
riate
ly w
eigh
risk
s an
d be
nefi t
s of
inte
rven
tiona
l tec
hniq
ues.
Reco
gniz
e th
e ad
ded
risk
from
dia
bete
s an
d re
nal i
mpa
irmen
t;Be
aw
are
of a
cute
and
chr
onic
co
mpl
icat
ions
of P
CI.
Know
cur
rent
diff
eren
tial i
ndic
atio
ns
for s
urgi
cal a
nd in
terv
entio
nal
reva
scul
ariz
atio
n as
wel
l as
cons
erva
tive
trea
tmen
t of C
AD
with
resp
ect t
o an
atom
y, e
xten
t of d
iseas
e, ro
le o
f lef
t ve
ntric
ular
func
tion
both
in th
e se
ttin
g of
AC
S an
d of
chr
onic
CA
D.
Know
adj
uvan
t dru
g th
erap
y, in
pa
rtic
ular
ant
icoa
gula
tion
regi
mes
an
d pl
atel
et-in
hibi
tors
(asp
irin,
th
ieno
pyrid
ines
, gly
copr
otei
n IIb
/IIIa
-in
hibi
tors
).
To a
ppro
pria
tely
sel
ect A
CS
patie
nts
who
are
can
dida
tes
for u
rgen
t an
giog
raph
y an
d PC
ITo
app
ropr
iate
ly s
elec
t chr
onic
CA
D
patie
nts
who
are
can
dida
tes
for
angi
ogra
phy
and
PCI.
To a
dapt
pha
rmac
othe
rapy
, esp
ecia
lly
antic
oagu
latio
n an
d an
tiagg
rega
tory
m
edic
atio
n, b
efor
e an
d af
ter P
CI t
o cl
inic
al n
eeds
.To
be
resp
onsiv
e to
pot
entia
l haz
ards
su
ch a
s co
ntra
st n
ephr
opat
hy, a
rter
ial
acce
ss c
ompl
icat
ions
(hem
atom
a), d
rug
com
plia
nce
issue
s, d
rug
resis
tanc
e,
non-
card
iac
dise
ases
or i
nter
vent
ions
w
ith b
leed
ing
risks
whi
le th
e pa
tient
is
on th
ieno
pyrid
ine
and
aspi
rin
med
icat
ion.
Expl
ain
risk,
ben
efi ts
and
alte
rnat
ives
in
a c
ompa
ssio
nate
way
to th
e pa
tient
and
be
resp
onsiv
e to
his
fear
s an
d w
orrie
s; ta
ke p
atie
nt’s
wish
es,
co-m
orbi
ditie
s an
d so
cial
situ
atio
n in
to a
ccou
nt w
hen
mak
ing
med
ical
de
cisio
nsIn
tera
ct a
nd c
oope
rate
pro
fess
iona
lly
with
inte
rven
tiona
l car
diol
ogist
s, h
eart
su
rgeo
ns, a
nd s
uppo
rtin
g m
edic
al
pers
onne
l
•
(con
tinue
d)
• • • • • • •
Perc
uta
neo
us
coro
nar
y in
terv
entio
n

16
9. C
hro
nic
Isch
aem
ic H
eart
Dis
ease
• • • • • • •
• • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith c
hron
ic Is
chae
mic
Hea
rt D
iseas
e (IH
D)
To e
valu
ate
patie
nts
and
inte
rpre
t the
re
sults
of d
iagn
ostic
pro
cedu
res
To s
elec
t and
man
age
appr
opria
te
ther
apie
s
Des
crib
e th
e ep
idem
iolo
gy o
f chr
onic
IH
D a
nd it
s ris
k fa
ctor
sEx
plai
n th
e m
olec
ular
and
cel
lula
r bi
olog
y of
IHD
, its
pat
holo
gy a
nd
deve
lopm
ent,
and
the
effe
cts
of
ischa
emia
on
the
card
iac
myo
cyte
Des
crib
e ev
ents
that
pre
cipi
tate
a
clin
ical
ang
ina
atta
ckO
utlin
e th
e pr
ogno
sis o
f chr
onic
IHD
Des
crib
e th
e cl
inic
al a
sses
smen
t of
know
n or
sus
pect
ed c
hron
ic IH
D,
incl
udin
g ev
alua
tion
of c
hest
pai
n,
othe
r sym
ptom
s an
d sig
ns, a
nd
diag
nost
ic p
roce
dure
sD
escr
ibe
the
man
agem
ent o
f chr
onic
IH
D, i
nclu
ding
life
styl
e m
easu
res,
ph
arm
acol
ogic
al m
anag
emen
t -
- di
seas
e m
odify
ing
drug
s-
sym
ptom
con
trol
ling
drug
sEx
plai
n th
e ro
le a
nd re
lativ
e m
erits
of
med
ical
ther
apy
and
reva
scul
arisa
tion
(per
cuta
neou
s co
rona
ry in
terv
entio
n or
co
rona
ry a
rter
y by
pass
sur
gery
) in
the
patie
nt w
ith IH
D
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion.
Dem
onst
rate
the
abilit
y to
risk
str
atify
in
divi
dual
pat
ient
s an
d to
sel
ect a
n ap
prop
riate
man
agem
ent s
trat
egy.
Sele
ct, u
se a
nd in
terp
ret n
on-in
vasiv
e an
d in
vasiv
e di
agno
stic
tool
s fo
r the
ev
alua
tion
of is
chae
mia
, via
bilit
y, le
ft
vent
ricul
ar s
truc
ture
and
func
tion
and
coro
nary
ana
tom
y.Id
entif
y an
d tr
eat r
isk fa
ctor
s fo
r chr
onic
IH
D.
Reco
gnise
the
impo
rtan
ce o
f risk
fa
ctor
man
agem
ent a
nd s
econ
dary
pr
even
tion.
Con
sult
with
spe
cial
ists
such
as
inte
rven
tiona
l car
diol
ogist
s, c
ardi
ac
surg
eons
, die
ticia
ns a
nd d
iabe
tolo
gist
s in
ord
er to
dev
ise a
n ap
prop
riate
m
anag
emen
t pla
n fo
r ind
ivid
ual
patie
nts
• • •

17
(For
PC
I, se
e ch
apte
r 8.)
ESC
Gu
idel
ines
• E
urop
ean
guid
elin
es o
n ca
rdio
vasc
ular
dise
ase
prev
entio
n in
clin
ical
pra
ctic
e –
Exec
utiv
e Su
mm
ary.
(Eur
opea
n H
eart
Jou
rnal
200
7; d
oi: b
is.10
93/e
urhe
artj/
ehm
316)
• M
anag
emen
t of
sta
ble
angi
na p
ecto
ris. (
Euro
pean
Hea
rt J
ourn
al 2
006;
27:
134
1-13
81)
• G
uide
lines
on
univ
ersa
l myo
card
ial i
nfar
ctio
n re
defi n
ition
(Eur
opea
n H
eart
Jou
rnal
200
7; d
oi: b
is.10
93/e
urhe
artj/
ehm
355)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Ch
ron
ic Is
chae
mic
Hea
rt D
isea
se
• • • •
• •
•
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
exe
rcise
or
phar
mac
olog
ical
str
ess
test
ing
alon
e,
or in
con
junc
tion
with
, an
imag
ing
mod
ality
Out
line
the
basic
prin
cipl
es o
f cor
onar
y ph
ysio
logy
Des
crib
e th
e pr
inci
ples
of e
xerc
ise
phys
iolo
gyD
escr
ibe
the
mec
hani
sms
of a
ctio
n of
va
sodi
lato
rs a
nd in
otro
pic
dru
gs u
sed
for s
tres
s te
stin
gA
ppre
ciat
ing
the
indi
catio
n of
str
ess
test
ing
in o
ther
car
diac
diso
rder
s (in
clud
ing
valv
ular
dise
ase,
arr
hyth
mia
s an
d he
art f
ailu
re)
Be a
ble
to in
terp
ret t
he E
CG
to d
etec
t isc
haem
ia a
nd/o
r arr
hyth
mia
sM
anag
ing
life-
thre
aten
ing
arrh
ythm
ias,
isc
haem
ia, o
r oth
er e
mer
genc
y sit
uatio
ns, i
nclu
ding
AC
LS, d
urin
g th
e te
st
Sele
ct th
e ap
prop
riate
str
ess
mod
ality
fo
r a p
artic
ular
pat
ient
and
inte
rpre
t ac
cord
ing
to B
ayes
ian
prin
cipl
es ta
king
in
to a
ccou
nt s
peci
fi c s
tren
gths
and
w
eakn
esse
s of
a g
iven
test
mod
ality
in
a g
iven
pat
ient
(e.g
., fre
quen
t fal
se
posit
ive
stre
ss E
CG
in w
omen
)
•Stre
ss T
estin
g
(con
tinue
d)

18
ESC
Gu
idel
ines
• C
linic
al e
xper
t co
nsen
sus
docu
men
t on
hyp
ertr
ophi
c ca
rdio
myo
path
y (E
urop
ean
Hea
rt J
ourn
al 2
003;
24:
196
5-19
91)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
10. M
yoca
rdia
l Dis
ease
• • • • • • •
• • • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith c
ardi
omyo
path
y an
d m
yoca
rditi
s.
Defi
ne
and
desc
ribe
the
epid
emio
logy
of
dila
ted,
hyp
ertr
ophi
c, re
stric
tive,
in
fi ltr
ativ
e ca
rdio
myo
path
ies
and
oblit
erat
ive
endo
myo
card
ial d
iseas
eD
escr
ibe
the
path
ophy
siolo
gy in
clud
ing
gene
tics,
clin
ical
feat
ures
and
dia
gnos
tic
crite
ria o
f car
diom
yopa
thie
sEl
abor
ate
the
med
ical
and
inva
sive
(sur
gica
l, el
ectr
ophy
siolo
gica
l and
in
terv
entio
nal)
man
agem
ent o
f ca
rdio
myo
path
ies:
indi
catio
ns,
cont
rain
dica
tions
, pos
sible
adv
erse
ef
fect
sId
entif
y pr
ogno
stic
fact
ors
Myo
card
itis
Defi
ne
myo
card
itis
and
desc
ribe
its
aetio
logy
D
escr
ibe
the
clin
ical
feat
ures
, pat
holo
gy
and
diag
nost
ic c
riter
ia o
f inf
ectiv
e an
d no
n-in
fect
ive
myo
card
itis,
in p
artic
ular
th
e ty
pica
l fea
ture
s of
diff
eren
t for
ms
of m
yoca
rditi
s on
mag
netic
reso
nanc
e im
agin
gRe
call
the
trea
tmen
t of p
atie
nts
with
m
yoca
rditi
s an
d its
com
plic
atio
ns
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
To b
e ab
le to
inte
rpre
t di
agno
stic
da
ta (E
CG
, am
bula
tory
EC
G, E
cho,
ex
erci
se te
stin
g, c
hest
X-r
ay, c
ardi
ac
cath
eter
isatio
n, c
oron
ary
angi
ogra
phy,
m
agne
tic re
sona
nce
and
radi
onuc
lide
imag
ing,
end
omyo
card
ial b
iops
y,
gene
tic a
sses
smen
t)To
be
able
to s
elec
t app
ropr
iate
tr
eatm
ent a
nd s
uppo
rt m
odal
ities
(m
edic
al, i
nter
vent
iona
l, su
rgic
al, I
CD
/C
RT, a
ssist
dev
ices
, bal
loon
pum
ping
or
othe
r tre
atm
ent)
To b
e ab
le to
ass
ess
indi
vidu
al
prog
nosis
in re
latio
n to
the
need
for
tran
spla
ntat
ion.
Eval
uate
pat
ient
s fo
r end
omyo
card
ial
biop
sy re
cogn
izin
g di
agno
stic
yie
ld a
nd
pote
ntia
l risk
of t
his
proc
edur
e.
To e
stab
lish
coop
erat
ion
with
med
ical
pr
ofes
siona
ls in
oth
er s
peci
altie
s (im
mun
olog
y, b
acte
riolo
gy, g
enet
ics,
ca
rdia
c su
rger
y, i
nter
vent
iona
l ca
rdio
logy
, im
agin
g) fo
r tim
ely
diffe
rent
ial d
iagn
osis
of m
yoca
rdia
l di
seas
e an
d fu
rthe
r tre
atm
ent
To b
e ab
le to
cou
nsel
pat
ient
s w
ith
card
iom
yopa
thie
s an
d th
eir r
elat
ives
ab
out a
ssoc
iate
d ris
ks.
•

19
ESC
Gu
idel
ines
• G
uide
lines
on
the
diag
nosis
and
man
agem
ent
of p
eric
ardi
al d
iseas
es. (
Euro
pean
Hea
rt J
ourn
al 2
004;
25:
587
-610
)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
11. P
eric
ard
ial D
isea
se
• • • • • •
• • • • • • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith p
eric
ardi
al d
iseas
es
Cla
ssify
and
defi
ne
- A
cute
per
icar
ditis
(inf
ectiv
e, id
iopa
thic
or
neo
plas
tic)
- C
hron
ic p
eric
ardi
tis-
Con
stric
tive
peric
ardi
tisD
escr
ibe
for e
ach
the
epid
emio
logy
, pa
thop
hysio
logy
, and
aet
iolo
gy
(incl
udin
g in
fect
ive,
infl a
mm
ator
y an
d ne
opla
stic
diso
rder
s)D
escr
ibe
rele
vant
inve
stig
atio
ns: n
on-
inva
sive
and
inva
sive.
Expl
ain
and
outli
ne th
e di
ffere
ntia
l di
agno
sis o
f con
stric
tive
peric
ardi
tis
from
rest
rictiv
e ca
rdio
myo
path
yD
escr
ibe
the
man
agem
ent o
f pe
ricar
ditis
Reca
ll re
late
d co
mpl
icat
ions
; per
icar
dial
ef
fusio
n, c
ardi
ac ta
mpo
nade
and
co
nstr
ictio
n.
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Dem
onst
rate
s kn
owle
dge
of th
e EC
G
abno
rmal
ities
in a
cute
per
icar
ditis
Sele
ct a
nd u
se th
e di
ffere
nt n
on-
inva
sive
imag
ing
mod
aliti
es: e
cho,
C
MR,
CT
as w
ell a
s in
vasiv
e pr
essu
re
mea
sure
men
ts to
dia
gnos
e pe
ricar
dial
di
seas
e.Ev
alua
te h
aem
odyn
amic
sta
tus;
D
eter
min
e th
e ae
tiolo
gy o
f per
icar
dial
ef
fusio
n B
e ab
le to
clin
ical
ly d
iffer
entia
te
peric
ardi
tis fr
om m
yoca
rdia
l isc
haem
ia.
Ass
ist in
and
idea
lly p
erfo
rm
peric
ardi
ocen
tesis
on
appr
opria
tely
se
lect
ed p
atie
nts
Con
sider
per
icar
dial
dise
ases
with
in
the
diffe
rent
ial d
iagn
osis
of a
pat
ient
pr
esen
ting
with
car
diov
ascu
lar d
iseas
eBe
aw
are
of th
e di
ffere
nt d
iagn
ostic
an
d th
erap
eutic
str
ateg
ies
requ
ired
for
each
indi
vidu
al c
ase
To w
ork
clos
ely
with
radi
olog
ists,
ca
rdia
c su
rgeo
ns a
nd o
ncol
ogist
s.
•

20
12. C
ard
iac
Tum
ou
rs • • • • •
• • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith c
ardi
ac tu
mou
rs
Cla
ssify
and
des
crib
e th
e ep
idem
iolo
gy,
path
ophy
siolo
gy, p
atho
logy
and
cl
inic
al m
anife
stat
ions
of p
rimar
y ca
rdia
c tu
mou
rs a
nd m
etas
tatic
car
diac
tu
mou
rs, i
nclu
ding
lym
phom
aD
escr
ibe
effe
ct o
f tum
our s
ize
and
loca
tion
Out
line
clin
ical
feat
ures
incl
udin
g-
Impa
irmen
t of c
ardi
ac fu
nctio
n-
Syst
emic
man
ifest
atio
ns-
Syst
emic
and
pul
mon
ary
embo
li-
Sign
s of
phy
sical
obs
truc
tion
to b
lood
fl o
w (e
.g. a
tria
l myx
oma)
- Pe
ricar
dial
invo
lvem
ent-
cons
tric
tion
and
tam
pona
deId
entif
y ap
prop
riate
dia
gnos
tic
proc
edur
es-
echo
card
iogr
aphy
, com
pute
d to
mog
raph
y, m
agne
tic re
sona
nce
imag
ing
Des
crib
e op
erat
ive
man
agem
ent
(tum
our r
emov
al, h
eart
tran
spla
ntat
ion,
pa
lliativ
e m
anag
emen
t)
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Sele
ct a
nd u
se a
ppro
pria
te im
agin
g m
odal
ities
Con
sider
a d
iffer
entia
l dia
gnos
is of
pr
imar
y or
sec
onda
ry n
eopl
astic
in
volv
emen
t of t
he h
eart
Re
cogn
ise o
ther
car
diac
mas
ses
incl
udin
g th
rom
bi o
r veg
etat
ions
Col
labo
rate
effe
ctiv
ely
with
ca
rdio
vasc
ular
sur
geon
s an
d w
ith o
ther
sp
ecia
lists
dea
ling
with
neo
plas
tic
dise
ase
Und
erst
and
the
impo
rtan
ce o
f sup
port
an
d co
unse
lling
for t
he p
atie
nt a
nd
fam
ily
•

21
13. C
on
gen
ital H
eart
Dis
ease
in A
du
lt P
atie
nts
• • • •
• • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
ass
ess,
man
age
and
appr
opria
tely
refe
r adu
lt pa
tient
s w
ith
cong
enita
l hea
rt d
iseas
e in
clud
ing
thos
e pa
tient
s w
ho h
ave
unde
rgon
e pr
evio
us c
ardi
ac s
urge
ry
Des
crib
e th
e ep
idem
iolo
gy, a
etio
logy
, pr
even
tion,
pat
hoph
ysio
logy
, no
men
clat
ure,
and
foet
al a
nd
tran
sitio
nal c
ircul
atio
nsD
escr
ibe
diag
nosis
and
ass
essm
ent
Out
line
prin
cipl
es o
f man
agem
ent
Iden
tify
path
olog
y, d
iagn
osis
and
man
agem
ent o
f spe
cifi c
con
ditio
ns-
Atr
ial s
epta
l def
ect
- A
trio
vent
ricul
ar s
epta
l def
ects
- Ve
ntric
ular
sep
tal d
efec
ts-
Ano
mal
ous
pulm
onar
y ve
nous
co
nnec
tions
- Pu
lmon
ary
sten
osis
- A
ortic
ste
nosis
- Pa
tent
duc
tus
arte
riosu
s-
Coa
rcta
tion
of th
e ao
rta
- Tr
icus
pid
atre
sia-
Ebst
ein’
s an
omal
y of
the
tric
uspi
d va
lve
- A
bnor
mal
ities
of t
he le
ft
atrio
vent
ricul
ar ju
nctio
n-
Tetr
alog
y of
Fal
lot
- D
oubl
e-ou
tlet r
ight
ven
tric
le-
Com
plet
e tr
ansp
ositi
on o
f the
gre
at
arte
ries
- C
onge
nita
lly c
orre
cted
tran
spos
ition
of
the
grea
t art
erie
s-
Dou
ble
outle
t lef
t ven
tric
le-
Com
mon
art
eria
l tru
nk
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Sele
ct im
agin
g te
chni
ques
and
whe
re
appr
opria
te u
se in
vasiv
e pr
oced
ures
for
diag
nosis
and
trea
tmen
t.Fo
llow
ing
diag
nosis
and
initi
al
trea
tmen
t pro
vide
long
term
follo
w
up, i
nclu
ding
pat
ient
mon
itorin
g an
d lif
esty
le a
dvic
e.
Und
erst
and
the
impo
rtan
ce o
f ref
errin
g pa
tient
s fo
r a s
peci
alist
opi
nion
.A
ppre
ciat
e th
e im
port
ance
of g
enet
ic
coun
sellin
g.A
ppre
ciat
e th
e so
cial
and
em
otio
nal
diffi
culti
es e
ncou
nter
ed b
y ad
ult
patie
nts
with
con
geni
tal h
eart
dise
ase
•

22
ESC
Gu
idel
ines
• G
uide
lines
for t
he in
terp
reta
tion
of t
he n
eona
tal e
lect
roca
rdio
gram
. (Eu
rope
an H
eart
Jou
rnal
200
2; 2
3: 1
329-
1344
)•
Man
agem
ent
of g
row
n up
con
geni
tal h
eart
dise
ase.
(Eur
opea
n H
eart
Jou
rnal
200
3; 2
4: 1
035-
1084
)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Co
ng
enita
l Hea
rt D
isea
se in
Ad
ult
Pat
ien
ts
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
- Pu
lmon
ary
atre
sia-
Con
geni
tal m
alfo
rmat
ions
of c
oron
ary
arte
ries
- C
onge
nita
l mal
form
atio
ns o
f pu
lmon
ary
arte
ries
- A
ortic
arc
h an
omal
ies
- A
rter
iove
nous
mal
form
atio
ns
(con
tinue
d)
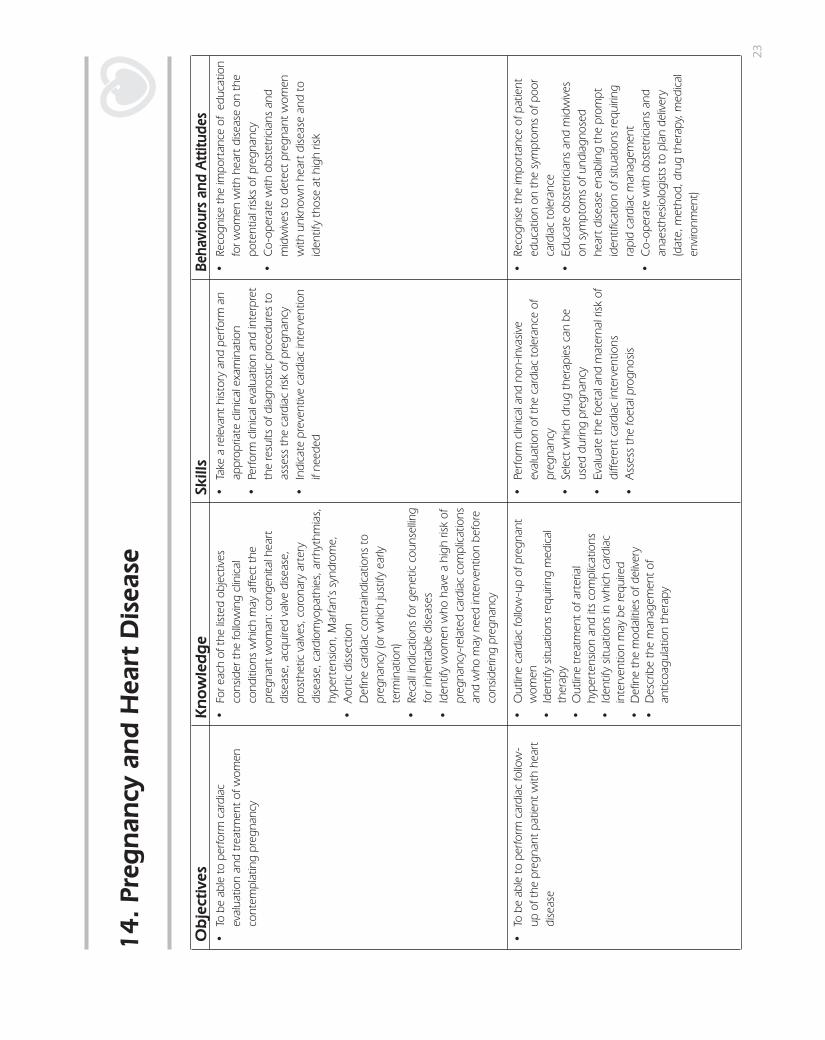
23
14. P
reg
nan
cy a
nd
Hea
rt D
isea
se
• • • •
• • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
car
diac
ev
alua
tion
and
trea
tmen
t of w
omen
co
ntem
plat
ing
preg
nanc
y
For e
ach
of th
e lis
ted
obje
ctiv
es
cons
ider
the
follo
win
g cl
inic
al
cond
ition
s w
hich
may
affe
ct th
e pr
egna
nt w
oman
: con
geni
tal h
eart
di
seas
e, a
cqui
red
valv
e di
seas
e,
pros
thet
ic v
alve
s, c
oron
ary
arte
ry
dise
ase,
car
diom
yopa
thie
s, a
rrhy
thm
ias,
hy
pert
ensio
n, M
arfa
n’s
synd
rom
e,
Aor
tic d
issec
tion
Defi
ne
card
iac
cont
rain
dica
tions
to
preg
nanc
y (o
r whi
ch ju
stify
ear
ly
term
inat
ion)
Reca
ll in
dica
tions
for g
enet
ic c
ouns
ellin
g fo
r inh
erita
ble
dise
ases
Iden
tify
wom
en w
ho h
ave
a hi
gh ri
sk o
f pr
egna
ncy-
rela
ted
card
iac
com
plic
atio
ns
and
who
may
nee
d in
terv
entio
n be
fore
co
nsid
erin
g pr
egna
ncy
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Perfo
rm c
linic
al e
valu
atio
n an
d in
terp
ret
the
resu
lts o
f dia
gnos
tic p
roce
dure
s to
as
sess
the
card
iac
risk
of p
regn
ancy
Indi
cate
pre
vent
ive
card
iac
inte
rven
tion
if ne
eded
Reco
gnise
the
impo
rtan
ce o
f ed
ucat
ion
for w
omen
with
hea
rt d
iseas
e on
the
pote
ntia
l risk
s of
pre
gnan
cyC
o-op
erat
e w
ith o
bste
tric
ians
and
m
idw
ives
to d
etec
t pre
gnan
t wom
en
with
unk
now
n he
art d
iseas
e an
d to
id
entif
y th
ose
at h
igh
risk
To b
e ab
le to
per
form
car
diac
follo
w-
up o
f the
pre
gnan
t pat
ient
with
hea
rt
dise
ase
Out
line
card
iac
follo
w-u
p of
pre
gnan
t w
omen
Id
entif
y sit
uatio
ns re
quiri
ng m
edic
al
ther
apy
Out
line
trea
tmen
t of a
rter
ial
hype
rten
sion
and
its c
ompl
icat
ions
Iden
tify
situa
tions
in w
hich
car
diac
in
terv
entio
n m
ay b
e re
quire
dD
efi n
e th
e m
odal
ities
of d
eliv
ery
Des
crib
e th
e m
anag
emen
t of
antic
oagu
latio
n th
erap
y
Perfo
rm c
linic
al a
nd n
on-in
vasiv
e ev
alua
tion
of th
e ca
rdia
c to
lera
nce
of
preg
nanc
ySe
lect
whi
ch d
rug
ther
apie
s ca
n be
us
ed d
urin
g pr
egna
ncy
Eval
uate
the
foet
al a
nd m
ater
nal r
isk o
f di
ffere
nt c
ardi
ac in
terv
entio
ns
Ass
ess
the
foet
al p
rogn
osis
Reco
gnise
the
impo
rtan
ce o
f pat
ient
ed
ucat
ion
on th
e sy
mpt
oms
of p
oor
card
iac
tole
ranc
eEd
ucat
e ob
stet
ricia
ns a
nd m
idw
ives
on
sym
ptom
s of
und
iagn
osed
he
art d
iseas
e en
ablin
g th
e pr
ompt
id
entifi
cat
ion
of s
ituat
ions
requ
iring
ra
pid
card
iac
man
agem
ent
Co-
oper
ate
with
obs
tetr
icia
ns a
nd
anae
sthe
siolo
gist
s to
pla
n de
liver
y (d
ate,
met
hod,
dru
g th
erap
y, m
edic
al
envi
ronm
ent)
•
• • • • • •
• • • •
• • •
•

24
ESC
Gu
idel
ines
• E
xper
t co
nsen
sus
docu
men
t on
man
agem
ent
of c
ardi
ovas
cula
r dise
ases
dur
ing
preg
nanc
y. (E
urop
ean
Hea
rt J
ourn
al 2
003;
24:
761
-781
)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Preg
nan
cy a
nd
Hea
rt D
isea
se
• •
• •
•
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f car
diac
pa
tient
s af
ter p
regn
ancy
Des
crib
e fo
llow
-up
mod
aliti
es d
urin
g th
e po
st-p
artu
m p
erio
dD
iagn
ose
and
trea
t pos
t-pa
rtum
ca
rdio
myo
path
y
Ana
lyse
car
diac
con
ditio
n af
ter
preg
nanc
yA
sses
s th
e ca
rdia
c ris
k of
sub
sequ
ent
preg
nanc
ies
Info
rm o
bste
tric
ians
and
mid
wiv
es o
n th
e ris
k of
wor
seni
ng o
f car
diac
sta
tus
durin
g th
e ea
rly p
ost-
part
um p
erio
d
Reca
ll ef
fi cac
y, ri
sks,
and
co
ntra
indi
catio
ns to
the
vario
us
cont
race
ptiv
e m
etho
ds a
ccor
ding
to
type
of h
eart
dise
ase
Co-
oper
ate
with
gyn
aeco
logi
sts
an
d ob
stet
ricia
ns w
ith re
gard
to
reco
mm
enda
tions
on
cont
race
ptio
n
•
••
(con
tinue
d)

25
ESC
Gu
idel
ines
• G
uide
lines
on
the
Man
agem
ent
of V
alvu
lar H
eart
Dise
ase
(Eur
opea
n H
eart
Jou
nral
200
7; 2
8: 2
30-2
68)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
15. V
alvu
lar
Hea
rt D
isea
se
• • • • • • •
• • • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
per
form
a s
peci
alist
as
sess
men
t and
trea
tmen
t of p
atie
nts
with
the
follo
win
g va
lvul
ar p
atho
logi
es:
- A
ortic
ste
nosis
- A
ortic
regu
rgita
tion
- M
itral
val
ve s
teno
sis-
Mitr
al v
alve
regu
rgita
tion
- Tr
icus
pid
sten
osis
- Tr
icus
pid
regu
rgita
tion
- Pu
lmon
ary
valv
e di
seas
e
Expl
ain
path
olog
y an
d pa
thop
hysio
logy
Reca
ll na
tura
l hist
ory
and
prog
ress
ion.
Expl
ain
stre
ngth
s an
d lim
itatio
ns o
f di
agno
stic
tech
niqu
es, i
n pa
rtic
ular
ec
hoca
rdio
grap
hy, a
nd re
cogn
ize
the
valu
e of
add
ition
al te
chni
ques
suc
h as
m
agne
tic re
sona
nce
imag
ing
or a
nd
inva
sive
hem
odyn
amic
s in
cas
es o
f di
scre
pant
fi nd
ings
Reca
ll th
e in
dica
tions
, ben
efi ts
, and
ris
ks o
f med
ical
ther
apy,
and
sur
gica
l or
perc
utan
eous
inte
rven
tions
App
reci
ate
the
indi
catio
ns fo
r and
m
anag
emen
t of a
ntic
oagu
latio
n Kn
ow th
e ro
le o
f con
com
itant
cor
onar
y he
art d
iseas
e in
val
vula
r hea
rt d
iseas
e an
d its
impa
ct o
n su
rgic
al m
anag
emen
tO
utlin
e po
st o
pera
tive
care
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Sele
ct th
e ap
prop
riate
use
of i
nvas
ive
or
non-
inva
sive
diag
nost
ic te
chni
ques
Inte
rpre
t res
ults
of d
iagn
ostic
pr
oced
ures
Be
abl
e to
dec
ide
whe
ther
to in
dica
te
surg
ery
and
appr
opria
te ti
min
g
Co-
oper
ate
with
car
diov
ascu
lar
surg
eons
, int
erve
ntio
nal c
ardi
olog
ists,
an
d ra
diol
ogist
s Re
cogn
ise im
port
ance
of p
atie
nt
educ
atio
n, w
ith re
spec
t to
the
natu
ral
hist
ory
of v
alvu
lar h
eart
dise
ase,
m
anag
emen
t of a
ntic
oagu
latio
n,
prop
hyla
xis
of b
acte
rial e
ndoc
ardi
tis
and
choi
ce o
f val
ve p
rost
hesis
whe
n ap
prop
riate
Con
vey
to th
e pa
tient
the
impo
rtan
ce
of m
onito
ring
of s
ympt
oms
and
signs
of
val
vula
r hea
rt d
iseas
e an
d of
per
iodi
c fo
llow
-up
by th
e ca
rdio
logi
st
To b
e ab
le to
per
form
follo
w u
p af
ter v
alve
sur
gery
or p
ercu
tane
ous
inte
rven
tion,
incl
udin
g im
med
iate
po
st-o
pera
tive
care
and
long
term
m
anag
emen
t of p
atie
nts
with
pr
osth
etic
val
ves
Und
erst
and
post
oper
ativ
e pa
thop
hysio
logy
Po
stop
erat
ive
man
agem
ent o
f an
ticoa
gula
nts,
diu
retic
s an
d ot
her
drug
s, p
roph
ylax
is ag
ains
t inf
ectiv
e en
doca
rditi
s, m
anag
emen
t of
preg
nanc
y an
d no
n-ca
rdia
c su
rger
y in
th
e pa
tient
with
pro
sthe
tic v
alve
s
Reco
gnise
and
man
age
the
com
plic
atio
ns w
hich
may
occ
ur in
pa
tient
s w
ith p
rost
hetic
val
ves
or a
fter
va
lvul
ar in
terv
entio
ns
Co-
oper
ate
with
car
diac
sur
geon
s an
d an
aest
hetis
tsRe
cogn
ise th
e ap
prop
riate
freq
uenc
y of
fo
llow
up
with
spe
cifi c
refe
renc
e to
the
clin
ical
con
ditio
n fo
llow
ing
surg
ery
or
inte
rven
tion.
•
• •
•• •
•

26
ESC
Gu
idel
ines
• G
uide
lines
on
the
prev
entio
n, d
iagn
osis
and
trea
tmen
t of
infe
ctiv
e en
doca
rditi
s –
Exec
utiv
e Su
mm
ary.
(Eur
opea
n H
eart
Jou
rnal
200
4; 2
5: 2
67-2
76)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
16. I
nfe
ctiv
e En
do
card
itis
• • • • • • • • •
• • • • • •
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Ass
ess,
dia
gnos
e an
d tr
eat p
atie
nts
with
infe
ctiv
e en
doca
rditi
s (o
f nat
ive
and
pros
thet
ic v
alve
s a
s w
ell a
s du
e to
in
dwel
ling
devi
ces
such
as
pace
mak
ers
and
cath
eter
s)
Des
crib
e ep
idem
iolo
gy,
path
olog
y,
path
ogen
esis
and
mic
robi
olog
y o
f in
fect
ive
endo
card
itis
Reco
gnise
the
clin
ical
feat
ures
Des
crib
e la
bora
tory
inve
stig
atio
ns
incl
udin
g m
icro
biol
ogic
al r
esul
ts
Des
crib
e th
e us
e of
car
diac
imag
ing
and
the
impo
rtan
ce o
f tra
nsoe
soph
agea
l ec
hoca
rdio
grap
hy to
det
ect
com
plic
atio
ns s
uch
as a
bsce
sses
Ex
plai
n th
e se
lect
ion
and
man
agem
ent
of a
ntib
iotic
ther
apy
Des
crib
e th
e ro
le o
f val
ve s
urge
ry in
pa
tient
s w
ith e
ndoc
ardi
tisD
escr
ibe
the
man
agem
ent o
f co
mpl
icat
ions
Reco
gnise
hig
h-ris
k pa
tient
s an
d sit
uatio
ns
Iden
tify
indi
catio
ns fo
r ant
ibio
tic
prop
hyla
xis
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Sele
ct th
e ap
prop
riate
use
of
labo
rato
ry in
vest
igat
ions
and
di
agno
stic
pro
cedu
res,
in p
artic
ular
ec
hoca
rdio
grap
hy
Sele
ct a
ppro
pria
te a
ntib
iotic
regi
men
Be a
ble
to d
eter
min
e th
e ne
ed fo
r, an
d tim
ing
of s
urge
ryM
anag
e co
mpl
icat
ions
Pres
crib
e ap
prop
riate
ant
ibio
tic a
gent
s fo
r pro
phyl
axis
Dev
elop
a m
ultid
iscip
linar
y ap
proa
ch
with
car
diac
sur
geon
s, a
nd
mic
robi
olog
ists
for d
iagn
osis
and
man
agem
ent
Reco
gnise
the
impo
rtan
ce o
f pat
ient
an
d ph
ysic
ian
educ
atio
n on
pro
phyl
axis
•

27
17. H
eart
Fai
lure
(H
F)
• • • • • • • • • • • • •
• • • • •
• • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To re
cogn
ise th
e im
pact
of h
eart
failu
re
on m
orbi
dity
and
mor
talit
y in
the
loca
l an
d ge
nera
l pop
ulat
ion
To b
e ab
le to
reco
gnise
the
diffe
rent
un
derly
ing
caus
es o
f hea
rt fa
ilure
To b
e ab
le to
per
form
spe
cial
ist
asse
ssm
ent a
nd tr
eatm
ent o
f pat
ient
s w
ith h
eart
failu
re
Des
crib
e th
e ep
idem
iolo
gy,
path
ophy
siolo
gy a
nd p
rogn
osis
of h
eart
fa
ilure
Reco
gnise
com
plic
atio
nsRe
call
the
inte
rnat
iona
l cla
ssifi
catio
ns
of fu
nctio
nal l
imita
tion
( for
exa
mpl
e N
YHA
cla
sses
)O
utlin
e th
e di
agno
stic
pro
cedu
res
in
the
patie
nt w
ith k
now
n or
sus
pect
ed
HF
incl
udin
g N
atiu
retic
pep
tides
, Ech
o,
ECG
, am
bula
tory
EC
G, s
tres
s te
stin
g,
card
iac
cath
eter
isatio
nD
escr
ibe
the
med
ical
man
agem
ent o
f ac
ute
HF
Des
crib
e th
e m
edic
al m
anag
emen
t of
chro
nic
HF
(neu
rohu
mor
al b
lock
ade)
Out
line
devi
ce m
anag
emen
t of H
F:
Car
diac
Res
ynch
roni
satio
n Th
erap
y, IC
DEx
plai
n th
e ro
le o
f car
diac
sur
gery
in
clud
ing
tran
spla
ntat
ion
Iden
tify
the
role
of e
xerc
ise tr
aini
ng
prog
ram
s in
HF
patie
nts
Reco
gnise
the
impo
rtan
ce o
f m
ultid
iscip
linar
y ca
re, i
nclu
ding
hom
e ba
sed
nurs
ing
in H
FId
entif
y th
e co
mpl
icat
ions
of H
F-pa
tient
s D
eter
min
e th
e ap
prop
riate
follo
w u
p of
H
F-pa
tient
s Re
cogn
ise th
e im
port
ance
of t
he
vole
mic
sta
tus
and
the
eval
uatio
n of
re
nal f
unct
ion
and
elec
trol
ytes
in H
F pa
tient
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Be a
ble
to s
elec
t and
use
dia
gnos
tic
tech
niqu
es to
diff
eren
tiate
the
unde
rlyin
g ca
uses
of H
FBe
abl
e to
del
iver
life
styl
e ad
vice
and
ho
me
base
d tr
eatm
ent s
trat
egy
to
patie
nts
Be a
ble
to ri
sk s
trat
ify H
F pa
tient
s an
d se
lect
app
ropr
iate
dru
g an
d ot
her t
hera
pies
(Im
plan
tabl
e C
ardi
ac D
efi b
rilla
tor (
ICD
), C
ardi
ac
Resy
nchr
onisa
tion
ther
apy
(CRT
), su
rger
y)To
eva
luat
e H
F pa
tient
s du
ring
follo
w
up a
nd a
ppro
pria
tely
and
con
tinuo
usly
ad
just
the
trea
tmen
t pla
n.
Emph
asise
the
impo
rtan
ce o
f life
styl
e,
exer
cise
and
wei
ght l
oss.
Hel
p pa
tient
s to
und
erst
and
the
need
for l
ong-
term
co
mpl
ex d
rug
ther
apy
App
reci
ate
the
impo
rtan
ce o
f re
habi
litat
ion
Dev
elop
and
sus
tain
sup
port
ive
rela
tions
hips
with
pat
ient
s w
ith c
hron
ic
hear
t fai
lure
Teac
h pa
tient
s, re
lativ
es a
nd s
peci
al
nurs
es in
HF
trea
tmen
t.Re
cogn
ise th
e a
dvan
tage
s an
d lim
itatio
ns o
f spe
cifi c
hea
rt fa
ilure
th
erap
ies
Expl
ain,
neg
otia
te a
nd o
verc
ome
the
barr
iers
to c
ompl
ianc
e w
ith h
eart
failu
re
trea
tmen
tsRe
cogn
ise th
e im
port
ance
of s
uppo
rtiv
e an
d pa
lliativ
e ca
re in
the
hear
t fai
lure
po
pula
tion
• • •
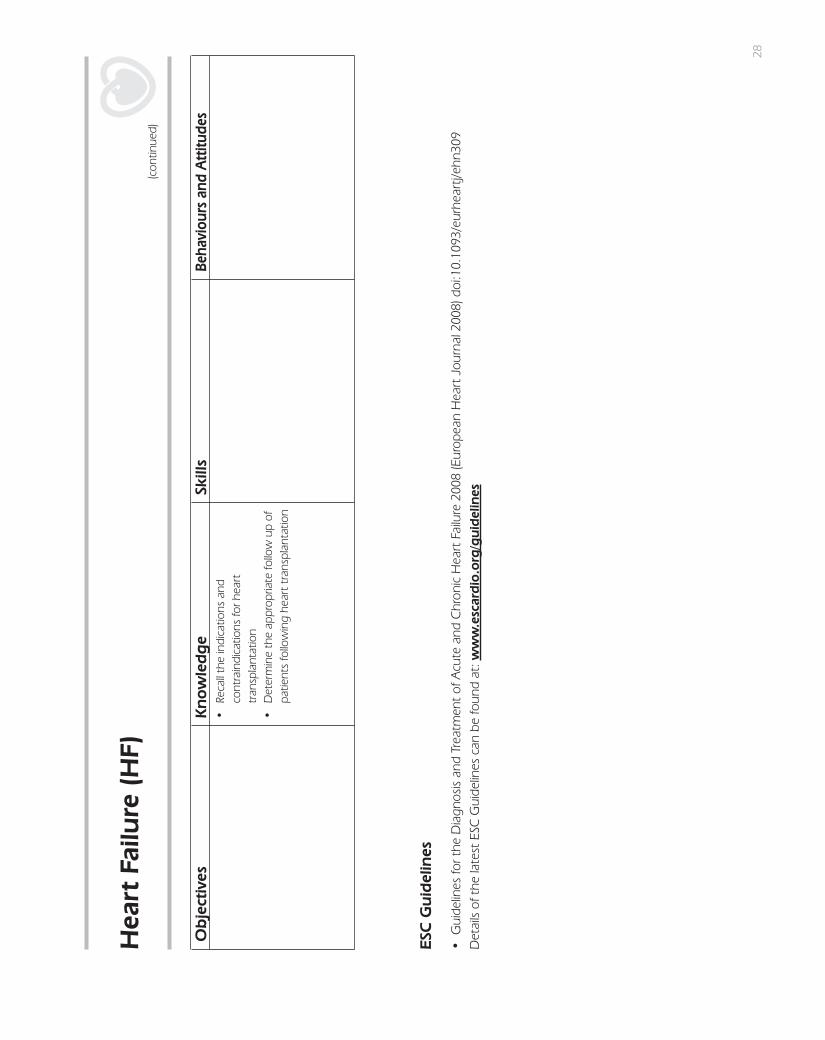
28
ESC
Gu
idel
ines
• G
uide
lines
for t
he D
iagn
osis
and
Trea
tmen
t of
Acu
te a
nd C
hron
ic H
eart
Fai
lure
200
8 (E
urop
ean
Hea
rt J
ourn
al 2
008)
doi
:10.
1093
/eur
hear
tj/eh
n309
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Hea
rt F
ailu
re (
HF)
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Reca
ll th
e in
dica
tions
and
co
ntra
indi
catio
ns fo
r hea
rt
tran
spla
ntat
ion
Det
erm
ine
the
appr
opria
te fo
llow
up
of
patie
nts
follo
win
g he
art t
rans
plan
tatio
n
(con
tinue
d)

29
ESC
Gu
idel
ines
• G
uide
lines
for t
he D
iagn
osis
and
Trea
tmen
t of
Acu
te a
nd C
hron
ic H
eart
Fai
lure
200
8 (E
urop
ean
Hea
rt J
ourn
al 2
008)
doi
:10.
1093
/eur
hear
tj/eh
n309
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
18. P
ulm
onar
y A
rter
ial H
yper
tens
ion
• • • • • • •
• • • • • •
• • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
dia
gnos
e pu
lmon
ary
arte
rial h
yper
tens
ion
(PA
H)
To b
e ab
le to
pro
vide
opt
imal
m
anag
emen
t for
pat
ient
s w
ith P
AH
To b
e ab
le to
dist
ingu
ish b
etw
een
the
diffe
rent
cau
ses
of p
ulm
onar
y hy
pert
ensio
n
Defi
ne
pulm
onar
y hy
pert
ensio
n an
d its
fu
nctio
nal c
lass
ifi ca
tion
Des
crib
e th
e ep
idem
iolo
gy o
f PA
H
(inci
denc
e, p
reva
lenc
e, a
etio
logy
, ge
netic
s, h
igh-
risk
grou
ps)
Des
crib
e th
e pa
thol
ogy
and
path
ophy
siolo
gy o
f PA
HD
escr
ibe
the
clin
ical
feat
ures
of P
AH
Out
line
the
diag
nost
ic c
riter
ia o
f PA
HId
entif
y pr
ogno
stic
mar
kers
Des
crib
e m
anag
emen
t of P
AH
(med
ical
, su
rgic
al a
nd in
terv
entio
nal i
nclu
ding
ba
lloon
atr
ial s
epto
stom
y, in
dica
tions
, co
ntra
indi
catio
ns a
nd p
ossib
le a
dver
se
effe
cts)
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Reco
gnise
clin
ical
sig
ns s
ugge
stiv
e of
PA
HD
iffer
entia
te b
etw
een
pulm
onar
y hy
pert
ensio
n an
d ot
her d
iseas
es w
ith
simila
r sym
ptom
sPe
rform
and
inte
rpre
t acc
urat
e m
edic
al a
sses
smen
t (us
ing
labo
rato
ry
anal
yses
incl
udin
g ar
teria
l blo
od
gase
s, c
ardi
ac b
iom
arke
rs; p
ulm
onar
y fu
nctio
n te
st, E
CG
, Ech
ocar
diog
raph
y,
card
iopu
lmon
ary
stre
ss-t
estin
g,
vent
ilatio
n-pe
rfusio
n lu
ng s
can,
spi
ral
CT,
mag
netic
reso
nanc
e im
agin
g,
card
iac
cath
eter
isatio
n an
d pu
lmon
ary
an
giog
raph
y, lu
ng b
iops
y)Pr
escr
ibe
appr
opria
te m
edic
al o
r inv
asiv
e (s
urgi
cal o
r int
erve
ntio
nal)
man
agem
ent
Eval
uate
clin
ical
and
hae
mod
ynam
ic
prog
nost
ic m
arke
rs
Esta
blish
coo
pera
tion
with
fam
ily
phys
icia
ns a
nd o
ther
hea
lth c
are
prof
essio
nals
for e
arly
reco
gniti
on o
f pr
imar
y pu
lmon
ary
hype
rten
sion;
Effe
ctiv
ely
colla
bora
te w
ith o
ther
m
edic
al s
peci
alist
s (fa
mily
med
icin
e,
thor
acic
sur
gery
, inv
asiv
e ca
rdio
logy
, im
agin
g) fo
r diff
eren
tial d
iagn
osis
of
pulm
onar
y hy
pert
ensio
n an
d tim
ely
refe
rral
to s
urgi
cal t
reat
men
tPr
ovid
e ge
netic
cou
nsel
ing
to fa
milie
s af
fect
ed b
y fa
milia
l PA
HM
aint
ain
long
-ter
m in
volv
emen
t of
patie
nts
and
thei
r fam
ily m
embe
rs in
su
ppor
tive
activ
ities
for h
ealth
y lif
e-st
yle
adhe
renc
e an
d tr
eatm
ent c
ompl
ianc
eA
ppre
ciat
e th
e in
crea
sed
prev
alen
ce o
f PA
H in
oth
er m
edic
al c
ondi
tions
, suc
h as
scl
erod
erm
aRe
fer t
o Sp
ecia
lists
in P
AH
whe
n ap
prop
riate
• • •

30
19. R
ehab
ilita
tion
an
d E
xerc
ise
Phys
iolo
gy
• • • • • • •
• • • • •
• • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
pro
vide
app
ropr
iate
re
habi
litat
ion
and
seco
ndar
y pr
even
tion
serv
ices
to p
atie
nts
with
car
diov
ascu
lar
dise
ase,
spe
cifi c
ally
acu
te c
oron
ary
synd
rom
es, a
fter
reva
scul
arisa
tion,
with
st
able
ang
ina
pect
oris,
pat
ient
s w
ith
high
car
diov
ascu
lar r
isk, h
eart
failu
re,
diab
etes
, and
oth
ers
To b
e ab
le to
eva
luat
e th
e ca
rdio
vasc
ular
risk
and
the
exer
cise
ca
paci
ty o
f the
pat
ient
s To
be
able
to e
valu
ate
“ath
lete
s he
art”
ch
arac
teris
tics
Defi
ne
reha
bilit
atio
n an
d se
cond
ary
prev
entio
n as
inte
grat
ed c
ompo
nent
s of
car
diac
car
eD
efi n
e ta
rget
pop
ulat
ions
and
risk
st
ratifi
cat
ion
of p
atie
nts
Und
erst
and
base
line
asse
ssm
ent,
exer
cise
test
ing,
exe
rcise
trai
ning
, pa
tient
edu
catio
n, li
fest
yle
inte
rven
tion,
ris
k fa
ctor
man
agem
ent,
psyc
hoso
cial
an
d vo
catio
nal s
uppo
rtU
nder
stan
d ex
erci
se a
nd s
port
s ph
ysio
logy
, an
d be
nefi t
s of
exe
rcise
tr
aini
ng, r
ecog
nize
saf
ety
issue
s Re
cogn
ise p
sych
olog
ical
asp
ects
of
reha
bilit
atio
n U
nder
stan
d sp
ecifi
c po
pula
tion
chal
leng
es
Des
crib
e pr
ogra
mm
es fo
r spe
cifi c
po
pula
tions
in a
ppro
pria
te s
ettin
gs
Take
a re
leva
nt h
istor
y an
d pe
rform
an
app
ropr
iate
clin
ical
exa
min
atio
n as
par
t of a
com
preh
ensiv
e ba
selin
e as
sess
men
tPe
rform
and
inte
rpre
t risk
str
atifi
catio
n,
usin
g an
d/or
per
form
ing
nam
ely
the
CPX
or t
he c
onve
ntio
nal e
xerc
ise te
st,
the
echo
card
iogr
am o
r oth
er te
sts
as
indi
cate
dPr
escr
ibe
exer
cise
pro
gram
mes
, in
term
s of
mod
e, in
tens
ity, d
urat
ion
and
prog
ress
ion,
and
oth
er li
fest
yle
inte
rven
tions
Pres
crib
e ca
rdio
vasc
ular
pre
vent
ive
med
icat
ions
acc
ordi
ng to
bes
t pra
ctic
e gu
idel
ines
Reco
gniz
e “a
thle
ts h
eart
” ch
arac
teris
tics
(EC
G, e
cho)
and
use
the
ESC
re
com
men
datio
n fo
r elig
ibilli
ty.
Reco
gnise
reha
bilit
atio
n an
d se
cond
ary
prev
entio
n as
an
inte
grat
ed c
ompo
nent
of
car
diac
car
eRe
cogn
ise th
e im
port
ance
of
reha
bilit
atio
n an
d se
cond
ary
prev
entio
n fo
r pro
fess
iona
l (w
ork)
, per
sona
l (in
clud
ing
driv
ing,
trav
ellin
g, le
isure
and
se
x) a
nd s
ocia
l life
am
ong
patie
nts
with
he
art d
iseas
eRe
cogn
ise th
e in
terp
lay
of p
hysic
al a
nd
psyc
holo
gica
l asp
ects
of h
eart
dise
ase
Reco
gnise
the
impo
rtan
ce o
f pat
ient
s an
d pa
rtne
rs/fa
milie
s ed
ucat
ion
Reco
gnise
the
role
of o
ther
pr
ofes
siona
ls in
clud
ing
nurs
e sp
ecia
lists
, ph
ysio
ther
apist
s, p
sych
olog
ists,
di
etic
ians
and
gen
eral
pra
ctiti
oner
s in
re
habi
litat
ion
and
seco
ndar
y pr
even
tion
Reco
gnise
the
role
of s
port
s in
C
ardi
olog
y
• • •

31
20. A
rrh
yth
mia
s
• • • • • •
• • • • • • • • • • • • •
• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
ass
ess
and
trea
t pat
ient
s w
ith a
rrhy
thm
ias
Elec
trop
hys
iolo
gy
To h
ave
a go
od u
nder
stan
ding
of
dia
gnos
tic a
nd th
erap
eutic
el
ectr
ophy
siolo
gy in
rela
tion
to p
atie
nts
with
arr
hyth
mia
s
Paci
ng
To b
e ab
le to
ass
ess
patie
nts
for p
acin
g.
Be a
ble
to p
ace
patie
nts
inde
pend
ently
an
d sa
fely
Imp
lan
tab
le C
ard
iove
rter
Defi
bril
lato
r (IC
D)
To b
e ab
le to
ass
ess
patie
nts
who
re
quire
ICD
impl
anta
tion
Cla
ssify
and
defi
ne
Brad
ycar
dias
Tach
ycar
dias
- S
upra
vent
ricul
ar a
rrhy
thm
ias
- V
entr
icul
ar a
rrhy
thm
ias
Des
crib
e th
e ep
idem
iolo
gy,
path
ophy
siolo
gy, g
enet
ics,
dia
gnos
is an
d cl
inic
al fe
atur
es o
f arr
hyth
mia
sId
entif
y pr
ogno
sis in
clud
ing
risk
eval
uatio
nD
escr
ibe
the
prin
cipl
es o
f el
ectr
ocar
diog
raph
y an
d el
ectr
ophy
siolo
gy a
nd re
leva
nt fi
ndin
gs
in d
iffer
ent a
rrhy
thm
ias,
incl
udin
g hi
gh
risk
feat
ures
in th
e re
stin
g EC
G s
uch
as lo
ng Q
T, s
hort
QT,
and
Bru
gada
sy
ndro
me
Des
crib
e th
e ph
arm
acol
ogy
of a
ntia
rrhy
thm
ic d
rug
ther
apy
Out
line
the
prin
cipl
es o
f inv
asiv
e an
d de
vice
man
agem
ent o
f arr
thm
ias,
in
clud
ing
- ca
thet
er a
blat
ion
- Pa
cem
aker
ther
apy
(tem
pora
ry a
nd
perm
anen
t)-
ICD
ther
apy
- Su
rgic
al th
erap
y
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Be c
ompe
tent
in c
ardi
o-pu
lmon
ary
resu
scita
tion
Cla
ssify
arr
hyth
mia
s by
sta
ndar
d el
ectr
ocar
diog
ram
M
anag
e ac
ute
arrh
ythm
ias
with
dru
gsM
anag
e ac
ute
arrh
ythm
ias
with
ca
rdio
vers
ion
Pres
crib
e ap
prop
riate
pre
vent
ativ
e ph
arm
acol
ogic
al th
erap
yPe
rform
and
inte
rpre
t el
ectr
ocar
diog
raph
ic m
onito
ring.
Inte
rpre
t ele
ctro
phys
iolo
gica
l stu
dyRe
fer p
atie
nts
for c
athe
ter a
blat
ion
and
perfo
rm fo
llow
-up
afte
r cat
hete
r ab
latio
nPa
cing
& IC
DIn
sert
tem
pora
ry p
acin
g el
ectr
odes
,Im
plan
tatio
n of
per
man
ent s
ingl
e ch
ambe
r, du
al c
ham
ber p
acem
aker
s (a
doc
umen
ted
indi
cativ
e nu
mbe
r be
ing
50 c
ases
to a
chie
ve le
vel I
I co
mpe
tenc
e).
App
ropr
iate
ly s
elec
t and
refe
r pat
ient
s fo
r biv
entr
icul
ar p
acin
g M
anag
e th
e fo
llow
up
of p
atie
nts
with
pa
cem
aker
s in
clud
ing
inte
rroga
tion
and
prog
ram
min
g of
the
devi
ce
App
reci
ate
the
anxi
ety
suffe
red
by
patie
nts
with
arr
hyth
mia
s an
d w
ith
som
e m
etho
ds o
f man
agem
ent,
e.g.
ca
thet
er a
blat
ion,
pac
ing
and
ICD
App
reci
ate
the
impo
rtan
ce o
f coe
xist
ing
stru
ctur
al h
eart
dise
ases
, inc
ludi
ng
coro
nary
art
ery
dise
ase
in re
latio
n to
th
e ou
tcom
e an
d m
anag
emen
t of
arrh
ythm
ias
App
reci
ate
the
limita
tions
and
pot
entia
l ris
ks o
f ant
i-arr
hyth
mic
dru
g th
erap
y A
ppre
ciat
e th
e pa
lliativ
e na
ture
and
po
tent
ial a
dver
se e
ffect
s of
non
-ph
arm
acol
ogic
al th
erap
ies
• • • •

32
ESC
Gu
idel
ines
• G
uide
lines
on
Car
diac
Pac
ing
and
Car
diac
Res
ynch
roni
zatio
n Th
erap
y (E
urop
ean
Hea
rt J
ourn
al 2
007
- do
i: 10
.109
3/eu
rhea
rtj/e
hm30
5)•
AC
C/A
HA/
ESC
gui
delin
es fo
r the
man
agem
ent o
f pat
ient
s w
ith V
entri
cula
r Arrh
ythm
ias
and
the
Prev
entio
n of
Sud
den
Car
diac
Dea
th –
Exe
cutiv
e Su
mm
ary.
(E
urop
ean
Hea
rt J
ourn
al 2
006;
27:
209
9-21
40) a
nd F
ull T
ext (
Euro
pace
200
6)•
AC
C/A
HA
/ESC
Gui
delin
es fo
r the
Man
agem
ent o
f Pat
ient
s w
ith A
tria
l Fib
rilla
tion,
Exe
cutiv
e Su
mm
ary
(Eur
opea
n H
eart
Jou
rnal
, 200
6; 2
7: 1
979-
2030
) and
Ful
l Tex
t
(Eur
opac
e 20
06 d
oi: 1
0.10
93/e
urop
ace/
eul0
97)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Arr
hyt
hm
ias
•
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Use
hist
ory,
exa
min
atio
n an
d ca
rdia
c im
agin
g to
det
erm
ine
whi
ch p
atie
nts
requ
ire a
n IC
D.
(con
tinue
d)

33
ESC
Gu
idel
ines
• A
CC/A
HA/
ESC
guid
elin
es o
n th
e m
anag
emen
t of p
atie
nts
with
atri
al fi
brilla
tion
- Exe
cutiv
e Su
mm
ary.
(Eur
opea
n H
eart
Jou
rnal
200
6; 2
7: 1
979-
2030
). Eu
ropa
ce 2
006
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
21. A
tria
l Fib
rilla
tion • • • • • • •
• • • • • • •
• • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
car
ry o
ut s
peci
alist
as
sess
men
t and
trea
tmen
t of p
atie
nts
with
Atr
ial F
ibril
latio
n (A
F)
Des
crib
e th
e ep
idem
iolo
gy, p
rogn
osis,
an
d pa
thop
hysio
logy
of a
tria
l fi b
rilla
tion
Cla
ssify
atr
ial fi
bril
latio
nD
escr
ibe
the
diag
nosis
, clin
ical
feat
ures
an
d im
pact
on
qual
ity o
f life
Iden
tify
asso
ciat
ed c
ondi
tions
Out
line
diag
nost
ic p
roce
dure
s:-
Min
imum
eva
luat
ion
- A
dditi
onal
Inve
stig
atio
nRe
call
embo
lic c
ompl
icat
ions
Des
crib
e m
anag
emen
t:-
antic
oagu
lant
ther
apy
- rh
ythm
vs.
rate
con
trol
- co
nver
sion
to s
inus
rhyt
hm-
prev
entio
n of
recu
rren
ces
- co
ntro
l of v
entr
icul
ar ra
te-
pace
mak
er-d
efi b
rilla
tor t
hera
py-
cath
eter
abl
atio
n-
surg
ery
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Perfo
rm o
r int
erpr
et:
- el
ectr
ocar
diog
ram
- ec
hoca
rdio
gram
- tr
anso
esop
hage
al e
choc
ardi
ogra
phy
- pr
olon
ged
ECG
mon
itorin
g (e
.g.H
olte
r m
onito
ring)
- ex
erci
se te
stin
g
Man
agem
ent
Dev
elop
app
ropr
iate
ant
i-thr
ombo
tic
stra
tegi
es fo
r pre
vent
ion
of is
chem
ic
stro
ke a
nd s
yste
mic
em
bolis
mSe
lect
pat
ient
s ap
prop
riate
ly fo
r ca
rdio
vers
ion
and
perfo
rm c
ompe
tent
ly:
phar
mac
olog
ical
el
ectr
ical
Perfo
rm rh
ythm
con
trol
ther
apy:
phar
mac
olog
ical
Pe
rform
rate
con
trol
ther
apy:
phar
mac
olog
ical
Se
lect
and
refe
r pat
ient
s fo
r-
elec
trop
hysio
logi
cal s
tudi
es-
atria
l cat
hete
r abl
atio
n-
surg
ical
abl
atio
n- p
acem
aker
and
defi
bril
lato
r im
plan
tatio
n-
AV ju
nctio
n ab
latio
n an
d pa
cing
App
reci
ate
the
anxi
ety
patie
nts
suffe
r w
ith A
F, pa
rtic
ular
ly in
cas
e of
cer
tain
m
etho
ds o
f man
agem
ent,
e.g.
cat
hete
r ab
latio
n an
d pa
cing
Reco
gnise
the
impo
rtan
ce o
f coe
xist
ing
stru
ctur
al h
eart
dise
ases
for t
he
outc
ome
and
man
agem
ent o
f AF
App
reci
ate
the
limita
tions
and
pot
entia
l ris
ks o
f ant
iarr
hyth
mic
dru
g th
erap
y of
A
FA
ppre
ciat
e th
e im
port
ance
of
antic
oagu
lant
ther
apy
App
reci
ate
the
pallia
tive
natu
re a
nd
pote
ntia
l adv
erse
effe
cts
of n
on-
phar
mac
olog
ical
ther
apie
sA
ppre
ciat
e ne
wer
met
hods
for t
reat
ing
Atr
ial F
ibril
latio
n an
d ho
w to
refe
r pa
tient
s fo
r spe
cial
ist tr
eatm
ent w
hen
appr
opria
te, s
uch
as p
ercu
tane
ous
or
surg
ical
abl
atio
n.
•

34
22. S
ynco
pe
• • • • • •
• • • •
• • • • • • • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To d
efi n
e sy
ncop
eTo
diff
eren
tiate
syn
cope
from
the
othe
r ca
uses
of l
oss
of c
onsc
ious
ness
To a
sses
s an
d tr
eat o
f pat
ient
s w
ith
sync
ope
Des
crib
e th
e ep
idem
iolo
gy a
nd
unde
rsta
nd p
reva
lenc
e of
diff
eren
t ca
uses
of s
ynco
peD
escr
ibe
its p
atho
phys
iolo
gyC
lass
ify c
ause
s of
loss
of c
onsc
ious
ness
(e
.g. N
eura
lly-m
edia
ted
refl e
x sy
ncop
e,
Stok
es A
dam
s at
tack
, ort
host
atic
hy
pote
nsio
n,
Iden
tify
prog
nosis
Des
crib
e di
agno
stic
eva
luat
ion
- St
rate
gy o
f eva
luat
ion
- In
itial
eva
luat
ion
(hist
ory,
phy
sical
-
exam
inat
ion,
bas
elin
e EC
G)
- Ec
hoca
rdio
gram
- Ex
erci
se s
tres
s te
stin
g-
Tilt
test
ing
- El
ectr
ocar
diog
raph
ic m
onito
ring
(Lon
g te
rm E
CG
, ext
erna
l and
impl
anta
ble
loop
reco
rder
s)-
Elec
trop
hysio
logi
cal t
estin
gD
escr
ibe
trea
tmen
ts: d
evic
e ba
sed
or
phar
mac
olog
ical
for
- N
eura
lly-m
edia
ted
(refl e
x) s
ynco
pe-
Ort
host
atic
hyp
oten
sion
- C
ardi
ac a
rrhy
thm
ias
as p
rimar
y ca
use
- St
ruct
ural
car
diac
or c
ardi
opul
mon
ary
dise
ase
Dia
gn
osis
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Perfo
rm o
r int
erpr
et:
- el
ectr
ocar
diog
ram
- ec
hoca
rdio
gram
- ca
rotid
sin
us m
assa
ge-
tilt t
estin
g-
elec
troc
ardi
ogra
phic
mon
itorin
g (L
ong
term
EC
G, e
xter
nal a
nd im
plan
tabl
e lo
op re
cord
er)
- el
ectr
ophy
siolo
gica
l tes
t-
exer
cise
str
ess
test
ing
- ca
rdia
c ca
thet
eriz
atio
n an
d co
rona
ry
angi
ogra
phy
Perfo
rm ri
sk s
trat
ifi ca
tion
Trea
tmen
tSe
lect
app
ropr
iate
trea
tmen
t:
- Ed
ucat
ion
and
reas
sura
nce
- Ph
ysic
al m
anoe
uvre
s-
Dru
g th
erap
y-
Dev
ice
impl
anta
tion
App
reci
ate
the
impa
ct o
f syn
cope
on
the
patie
nts
lifes
tyle
App
reci
ate
that
syn
cope
is a
tran
sient
sy
mpt
om a
nd n
ot a
dise
ase
Con
sult
with
oth
er s
peci
alist
s.Re
cogn
ise th
e di
agno
stic
crit
eria
for t
he
caus
es o
f syn
cope
Reco
gnise
app
ropr
iate
inve
stig
atio
ns in
th
e va
rious
sub
grou
ps o
f pat
ient
s w
ith
sync
ope
Reco
gnise
how
pat
ient
s w
ith s
ynco
pe
shou
ld b
e ris
k st
ratifi
ed
App
reci
ate
how
pat
ient
s w
ith s
ynco
pe
shou
ld b
e ho
spita
lized
. Re
cogn
ise tr
eatm
ents
that
are
like
ly
to b
e ef
fect
ive
in p
reve
ntin
g sy
ncop
al
recu
rren
ces
Dia
gn
osis
App
reci
ate
that
the
diag
nosis
of
sync
ope
is of
ten
pres
umpt
ive
App
reci
ate
that
the
diag
nost
ic v
alue
(s
ensit
ivity
and
spe
cifi c
ity) o
f tes
ts fo
r sy
ncop
e is
impe
rfect
App
reci
ate
that
obs
erva
tions
dur
ing
the
even
t are
of k
ey im
port
ance
App
reci
ate
that
the
diag
nost
ic
yiel
d of
the
test
s de
pend
s on
thei
r ap
prop
riate
ness
of t
heir
sele
ctio
n (p
re-
test
pro
babi
lity)
• • •

35
ESC
Gu
idel
ines
• G
uide
lines
on
Man
agem
ent
(dia
gnos
is an
d tr
eatm
ent)
of s
ynco
pe -
upd
ate
2004
, Exe
cutiv
e Su
mm
ary.
(E
urop
ean
Hea
rt J
ourn
al 2
004;
25:
205
4-20
72) a
nd fu
ll te
xt (E
urop
ace
2004
; 6: 4
67-5
37)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Syn
cop
e
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Ther
apy
Reco
gnise
that
mos
t pat
ient
s do
not
ne
ed a
ny s
peci
fi c tr
eatm
ent a
part
from
ed
ucat
ion
and
reas
sura
nce
Reco
gnise
that
dru
g th
erap
ies
are
ofte
n in
effe
ctiv
eRe
cogn
ise th
e ris
k-be
nefi t
and
the
cost
-ef
fi cac
y of
pac
emak
er, I
CD
and
cat
hete
r ab
latio
n th
erap
y (con
tinue
d)

36
ESC
Gu
idel
ines
• G
uide
lines
on
sudd
en c
ardi
ac d
eath
– E
xecu
tive
Sum
mar
y. (E
urop
ace
2002
; 4: 3
-18)
• A
CC/A
HA/
ESC
upda
ted
guid
elin
es o
n Ve
ntric
ular
Arrh
ythm
ias
and
Prev
entio
n of
Sud
den
Card
iac
deat
h –
Exec
utive
Sum
mar
y. (E
urop
ean
Hea
rt J
ourn
al 2
006;
27:
209
9-21
40)
an
d Fu
ll Te
xt (E
urop
ace
2006
)D
etai
ls of
the
late
st E
SC G
uide
lines
can
be
foun
d at
: ww
w.e
scar
dio
.org
/gu
idel
ines
23. S
ud
den
Car
dia
c D
eath
(SC
D)
and
Res
usc
itatio
n
• • • • • • •
• • • • • • • • • •
• • • • • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Sud
den
Car
dia
c D
eath
To m
anag
e pa
tient
s w
ith th
reat
ened
or
abo
rted
SC
D, i
nclu
ding
risk
st
ratifi
cat
ion,
inve
stig
atio
n an
d tr
eatm
ent
Resu
scita
tion
To b
e ab
le to
car
ry o
ut b
asic
and
ad
vanc
ed c
ardi
ac li
fe s
uppo
rt
Sud
den
Car
dia
c D
eath
Defi
ne
SCD
and
kno
w a
nd u
nder
stan
d th
e ep
idem
iolo
gy, a
etio
logy
, pat
holo
gy,
path
ophy
siolo
gy a
nd c
linic
al
pres
enta
tion
of th
e di
ffere
nt c
ondi
tions
w
hich
may
lead
to S
CD
Defi
ne
the
prin
cipl
es o
f acu
te
man
agem
ent o
f pat
ient
s w
ith S
CD
Defi
ne
the
prin
cipl
es o
f dia
gnos
tic w
ork
up a
nd ri
sk s
trat
ifi ca
tion
of s
urvi
vors
; in
par
ticul
ar, r
ecog
nize
EC
G s
igns
in
dica
tive
of h
igh
SCD
risk
(e.g
., lo
ng
QT,
sho
rt Q
T, B
ruga
da s
yndr
ome
etc.
) an
d kn
ow h
ow to
furt
her e
valu
ate
patie
nts
with
thes
e sig
ns a
nd th
eir
fam
ilies
Sele
ct a
ppro
pria
te lo
ng te
rm
ther
apeu
tic o
ptio
nsRe
call
the
curr
ent r
ecom
men
datio
ns
for s
econ
dary
pre
vent
ion
of S
CD
(e
.g.,
indi
catio
ns fo
r pre
vent
ive
ICD
im
plan
tatio
n in
pat
ient
s w
ith is
chem
ic
card
iom
yopa
thy)
Iden
tify,
risk
str
atify
and
man
age
indi
vidu
als
at e
leva
ted
risk,
incl
udin
g fa
mily
mem
bers
of S
CD
pat
ient
s
Resu
scita
tion
Expl
ain
the
met
hods
and
gui
delin
es
of b
asic
and
adv
ance
d lif
e su
ppor
t in
clud
ing
airw
ay m
anag
emen
t, ap
prop
riate
dru
g us
e, d
efi b
rilla
tion
and
paci
ng
Sud
den
Car
dia
c D
eath
Perfo
rm re
susc
itatio
n (s
ee b
elow
)Ta
ke a
rele
vant
hist
ory
and
perfo
rm a
n ap
prop
riate
clin
ical
exa
min
atio
n In
terp
ret p
rodr
omal
sym
ptom
s,
unde
rlyin
g ca
uses
and
pro
gnos
is of
a
SCD
-Sur
vivo
r Pe
rform
and
inte
rpre
t risk
str
atifi
catio
n us
ing
the
follo
win
g te
chni
ques
(Hol
ter-
ECG
, LV
func
tion,
Ech
o, C
ath,
EP,
hear
t ra
te v
aria
bilit
y)
Follo
w u
p SC
D-S
urvi
vors
Resu
scita
tion
Iden
tify
the
caus
e of
col
laps
ePe
rform
BLS
(CPR
) and
AC
LS in
clud
ing
diffe
rent
ski
lls.
Lead
and
coo
rdin
ate
the
actio
ns o
f an
AC
LS-T
eam
Te
ach
basic
life
sup
port
(BLS
)
Sud
den
Car
dia
c D
eath
Reco
gnise
the
urge
ncy
of th
e m
anag
emen
t of c
ardi
ac a
rres
t, Re
cogn
ise th
e im
port
ance
of p
rodr
omal
sy
mpt
oms.
App
reci
ate
patie
nt a
nd fa
mily
anx
ietie
sA
ppre
ciat
e th
e im
port
ance
of p
atie
nt
educ
atio
n an
d se
cond
ary
prev
entio
nU
nder
stan
d th
e m
edic
al, p
sych
olog
ical
, an
d so
cial
pro
blem
s ar
ising
in p
atie
nts
with
end
-sta
ge h
eart
failu
re a
nd
frequ
ent I
CD
act
ivat
ion
Resu
scita
tion
App
reci
ate
the
impo
rtan
ce o
f wor
king
in
a te
am w
ith la
yper
sons
, par
amed
ics
and
othe
r med
ical
per
sonn
el d
urin
g re
susc
itatio
n (B
LS a
nd A
CLS
).U
nder
stan
d th
e im
port
ance
of r
egul
ar
audi
t of t
he b
asic
and
adv
ance
d lif
e su
ppor
t pro
gram
me.
• •

37
ESC
Gu
idel
ines
• D
iagn
osis
and
man
agem
ent
of a
ortic
diss
ectio
n. (E
urop
ean
Hea
rt J
ourn
al 2
001;
22:
164
2-16
81)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
24. D
isea
ses
of
the
Ao
rta
and
Tra
um
a to
th
e
Ao
rta
and
Hea
rt
• • •
• • •
• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
ass
ess
dise
ases
of t
he
Aor
ta, a
nd tr
aum
a to
the
aort
a an
d he
art
To b
e ab
le to
impl
emen
t the
ap
prop
riate
med
ical
, int
erve
ntio
nal o
r su
rgic
al tr
eatm
ent r
egim
e
Und
erst
and
the
epid
emio
logy
, ae
tiolo
gy, p
atho
logy
, gen
etic
s,
path
ophy
siolo
gy a
nd c
linic
al
pres
enta
tion
of a
ortic
dise
ase,
aor
tic
root
dise
ase,
and
trau
ma
to th
e ao
rta
and
hear
t inc
ludi
ng:
- A
cute
aor
tic s
yndr
omes
:
- A
ortic
diss
ectio
n-
Intr
amur
al h
aem
atom
a-
Trau
mat
ic a
ortic
tran
sect
ion
- C
hron
ic a
ortic
diss
ectio
n-
Ane
urys
m o
f the
thor
acic
aor
ta-
Aor
tic a
ther
omat
ous
dise
ase
- A
ortit
is-
Trau
ma
of th
e he
art (
incl
udin
g m
yoca
rdia
l con
tusio
n)Re
cogn
ise s
tren
gths
and
lim
itatio
ns o
f di
ffere
nt im
agin
g m
odal
ities
D
escr
ibe
the
appr
opria
te m
edic
al,
inte
rven
tiona
l or s
urgi
cal m
anag
emen
t st
rate
gy
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Cho
ose,
per
form
and
inte
rpre
t th
e ap
prop
riate
imag
ing
stud
ies
(tran
stho
raci
c an
d tr
anso
esop
hage
al
echo
card
iogr
aphy
, mag
netic
reso
nanc
e,
com
pute
d to
mog
raph
y, u
ltras
ound
(s
urfa
ce a
nd in
trav
ascu
lar)
and
angi
ogra
phy
of th
e ao
rta
and
of th
e he
art t
o as
sess
aor
tic d
iseas
e an
d tr
aum
atic
lesio
nsTo
man
age
diffe
rent
aor
tic c
ondi
tions
w
ith th
e ap
prop
riate
trea
tmen
t m
odal
ity in
a ti
mel
y m
anne
r
Coo
pera
te w
ith c
ardi
ovas
cula
r su
rgeo
ns a
nd in
terv
entio
nal
card
iolo
gist
s as
wel
l as
radi
olog
ists
for
diag
nosis
and
trea
tmen
tRe
cogn
ise th
e po
tent
ial u
rgen
cy
requ
ired
in m
anag
ing
patie
nts
with
di
seas
es o
f the
aor
ta a
nd c
ardi
ac
trau
ma
Reco
gniz
e an
d or
gani
ze fa
mily
sc
reen
ing
whe
re a
ppro
pria
teRe
cogn
ize
the
need
for a
nd u
nder
take
lo
ng te
rm fo
llow
-up
of p
atie
nts
with
ch
roni
c ao
rtic
dise
ase
• •

38
25. P
erip
her
al A
rter
ial V
ascu
lar
Dis
ease
s
• • • • • •
• • •
• • • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
ass
ess
and
trea
t pat
ient
s w
ith p
erip
hera
l art
eria
l vas
cula
r dise
ase
Des
crib
e ep
idem
iolo
gy a
nd p
atho
logy
Des
crib
e di
agno
sis a
nd a
sses
smen
tD
escr
ibe
med
ical
and
inva
sive
(inte
rven
tiona
l and
sur
gica
l) in
terv
entio
nal m
anag
emen
t and
thei
r re
lativ
e m
erit
in d
iffer
ent s
ituat
ions
Iden
tify
prog
nosis
Reca
ll th
e as
soci
atio
n of
per
iphe
ral
vasc
ular
dise
ase
with
vas
cula
r dise
ase
in
othe
r ter
ritor
ies
in p
artic
ular
car
otid
and
re
nal a
rter
ies
Reco
gnise
the
caus
es o
f acu
te li
mb
ischa
emia
and
the
urge
ncy
of it
s m
anag
emen
t
Take
a re
leva
nt h
istor
y an
d pe
rform
an
app
ropr
iate
phy
sical
exa
min
atio
n,
espe
cial
ly th
e ex
amin
atio
n of
per
iphe
ral
pulse
sId
entif
y th
e ris
k fa
ctor
s an
d se
lect
ap
prop
riate
ly th
e m
anag
emen
t str
ateg
y ke
epin
g in
min
d th
at p
erip
hera
l vas
cula
r di
seas
e is
a m
anife
stat
ion
of g
ener
alise
d at
hero
scle
rosis
Sele
ct, u
se a
nd in
terp
ret d
iagn
ostic
to
ols
appr
opria
tely
incl
udin
g:-
Ultr
asou
nd (d
uple
x sc
anni
ng a
nd
othe
r Dop
pler
mod
aliti
es, i
nclu
ding
an
kle
brac
hial
inde
x)
- M
R an
giog
raph
y-
CT
angi
ogra
phy
- A
ngio
grap
hy
App
reci
ate
the
syst
emic
nat
ure
of
athe
rosc
lero
sis a
nd it
s im
plic
atio
n fo
r a
patie
nt w
ith d
iseas
e m
anife
sted
w
ithin
a
give
n te
rrito
ryRe
cogn
ise th
e im
port
ance
of r
isk fa
ctor
m
odifi
catio
n in
pre
vent
ion.
Enco
urag
e pa
tient
s to
ado
pt a
hea
lthie
r lif
esty
le w
ith s
peci
fi c e
mph
asis
on ri
sk
fact
ors
Col
labo
rate
with
spe
cial
ists
such
as
inte
rven
tiona
l car
diol
ogist
s, ra
diol
ogist
s,
vasc
ular
sur
geon
s an
d di
abet
olog
ists.
•

26. T
hro
mb
oem
bo
lic V
eno
us
Dis
ease
• • • • •
• • • • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To b
e ab
le to
dia
gnos
e, tr
eat a
nd
prev
ent:
- de
ep v
enou
s th
rom
bosis
- pu
lmon
ary
embo
lism
Des
crib
e th
e ep
idem
iolo
gy a
nd ri
sk
fact
ors
for d
eep
veno
us th
rom
bosis
in
the
clin
ical
set
tings
of:
reco
very
from
maj
or s
urge
ry o
r tra
uma,
pro
long
ed
imm
obilit
y, o
ral c
ontr
acep
tive
pill
use,
preg
nanc
y an
d ai
r tra
vel
Expl
ain
incr
ease
d pu
lmon
ary
vasc
ular
resis
tanc
e an
d ve
ntila
tion
perfu
sion
mism
atch
Des
crib
e th
e cl
inic
al p
rese
ntat
ion
of d
eep
veno
us th
rom
bosis
and
pulm
onar
y em
bolis
m
Out
line
the
diag
nosis
by:
- Bi
omar
kers
: D-d
imer
and
trop
onin
s
- EC
G
- Ec
hoca
rdio
grap
hy
- U
ltras
ound
and
Dop
pler
of l
eg a
nd
pelv
is ve
ins
- M
DC
T
- Ve
ntila
tion-
perfu
sion
scan
- M
R-an
giog
raph
y
- Pu
lmon
ary
angi
ogra
phy
Des
crib
e tr
eatm
ent:
Hep
arin
s, V
itam
in
K an
tago
nist
s, N
ew a
ntic
oagu
lant
s,
Thro
mbo
lysis
, Em
bole
ctom
y an
d
fragm
enta
tion
Take
a re
leva
nt h
istor
y an
d pe
rform
an
appr
opria
te c
linic
al e
xam
inat
ion
Inte
rpre
t EC
G, e
choc
ardi
ogra
phy,
spi
ral
CT,
ven
tilat
ion-
perfu
sion
scan
ning
sig
ns o
f pul
mon
ary
hype
rten
sion
or
pulm
onar
y th
rom
boem
bolis
mSe
lect
app
ropr
iate
ther
apy
for a
cute
pu
lmon
ary
embo
lism
Dia
gnos
e an
d m
anag
e ac
ute
and
chro
nic
deep
ven
ous
thro
mbo
sisD
ecid
e up
on th
e du
ratio
n of
an
ticoa
gula
tion
ther
apy
for p
atie
nts
with
thro
mbo
embo
lic v
enou
s di
seas
e
App
reci
ate
the
diffi
culti
es in
dia
gnos
ing
pulm
onar
y em
bolis
m o
n th
e ba
sis o
f sy
mpt
oms
and
signs
Col
labo
rate
with
oth
er im
agin
g sp
ecia
lists
incl
udin
g ra
diol
ogist
s an
d nu
clea
r im
agin
g sp
ecia
lists
Ensu
re p
atie
nt u
nder
stan
ding
of t
he
dise
ase,
the
impo
rtan
ce o
f com
plia
nce
and
appr
opria
te p
reca
utio
ns re
quire
d du
ring
long
term
ant
icoa
gula
nt th
erap
y
•
39

ESC
Gu
idel
ines
• G
uide
lines
on
the
diag
nosis
and
man
agem
ent
of a
cute
pul
mon
ary
embo
lism
. (Eu
rope
an H
eart
Jou
rnal
200
8) d
oi:1
0.10
93/e
urhe
artj/
ehn3
10•
Exp
ert
cons
ensu
s do
cum
ent
on t
he u
se o
f ant
ipla
tele
t ag
ents
. (Eu
rope
an H
eart
Jou
rnal
200
4; 2
5: 1
66-1
81)
Det
ails
of t
he la
test
ESC
Gui
delin
es c
an b
e fo
und
at: w
ww
.esc
ard
io.o
rg/g
uid
elin
es
Thro
mb
oem
bo
lic V
eno
us
Dis
ease
• •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Des
crib
e pr
even
tive
mea
sure
s:
Com
pres
sion
stoc
king
s, h
epar
ins
Des
crib
e m
anag
emen
t of c
hron
ic
pulm
onar
y hy
pert
ensio
n, in
clud
ing
thro
mbe
ndar
tere
ctom
y
(con
tinue
d)
40

27. T
he
card
iac
con
sult
• •
• • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
To s
elec
t app
ropr
iate
pre
oper
ativ
e im
agin
g te
chni
ques
from
the
follo
win
g fo
ur im
agin
g m
odal
ities
for c
ardi
ac ri
sk
eval
uatio
n.£ Re
stin
g/st
ress
ech
ocar
diog
raph
y£ Re
stin
g/st
ress
nuc
lear
per
fusio
n im
agin
g£ C
ardi
ac c
ompu
ted
tom
ogra
phy
(CT)
£ C
ardi
ovas
cula
r mag
netic
reso
nanc
e (C
MR)
To in
tegr
ate
info
rmat
ion
rega
rdin
g th
e es
timat
ed e
ffect
s of
sur
gica
l str
ess
durin
g op
erat
ion.
To in
tegr
ate
info
rmat
ion
on th
e lo
ng-
term
impa
ct o
f car
diac
dise
ase
on
outc
ome
in p
atie
nts
shou
ld th
ey li
ve
long
eno
ugh
to e
njoy
the
bene
fi ts
of
surg
ery.
Und
erst
and
that
pre
oper
ativ
e te
sts
shou
ld o
nly
be d
one
if th
ey w
ill
infl u
ence
per
iope
rativ
e or
long
-
term
car
diac
trea
tmen
t and
risk
man
agem
ent,
with
out d
elay
ing
surg
ery
if te
st re
sults
will
not c
hang
e
man
agem
ent
App
ly th
e im
agin
g te
chni
ques
to a
sses
s
£ Le
ft v
entr
icul
ar e
ject
ion
fract
ion
at re
st
£ Va
lve
abno
rmal
ities
(ste
nosis
/
insu
ffi ci
ency
)
£ C
alcu
latio
n of
val
ve s
teno
sis g
radi
ent.
£ Es
timat
ion
of v
alvu
lar r
egur
gita
tion
fract
ion.
£ C
oron
ary
arte
ry d
iseas
e, n
ew w
all
mot
ion
abno
rmal
ities
dur
ing
stre
ss. T
he
seve
rity,
ext
ent a
nd is
chem
ic h
eart
rate
thre
shol
d du
ring
stre
ss te
stin
g.
£ In
trao
pera
tive
card
iac
mon
itorin
g fo
r
volu
me
and
ische
mia
sta
tus.
£ N
on-in
vasiv
e co
rona
ry a
ngio
gram
Con
sider
hea
rt v
alve
repl
acem
ent i
n pa
tient
s w
ith s
ever
e st
enos
is pr
ior t
o su
rger
y.C
onsid
er c
oron
ary
reva
scul
ariz
atio
n in
se
lect
ed p
atie
nts
with
ext
ensiv
e st
ress
in
duce
d isc
hem
ia p
rior t
o su
rger
y.
Con
sider
imm
edia
te c
oron
ary
reva
scul
ariz
atio
n in
pat
ient
s w
ith
intr
aope
rativ
e he
mod
ynam
ic in
stab
ility,
ST
-seg
men
t cha
nges
and
new
wal
l m
otio
n ab
norm
aliti
es.
Com
mun
icat
e to
pat
ient
s th
e im
plic
atio
ns o
f the
resu
lts o
f pr
eope
rativ
e te
sts
on p
erio
pera
tive
man
agem
ent.
Indi
cate
the
pote
ntia
l co
mpl
icat
ions
of d
elay
ing
the
inde
x su
rgic
al p
roce
dure
and
the
bene
fi t o
f ad
ditio
nal (
inva
sive)
car
diac
ther
apy.
Com
mun
icat
e w
ith o
ther
spe
cial
ties
invo
lved
in p
erio
pera
tive
care
(a
nest
hesio
logi
st, s
urge
on, a
nd
inte
nsiv
ist) t
o in
divi
dual
ize
patie
nt c
are.
Re
cogn
ize
stre
ngth
s an
d lim
itatio
ns o
f ea
ch im
agin
g m
odal
ity.
• • •
41
Peri-
oper
ativ
e ca
rdia
c co
nsul
t for
non
-ca
rdia
c su
rger
y

The
card
iac
con
sult • • •
• • •
• • •
Ob
ject
ives
Kno
wle
dg
eSk
ills
Beha
viou
rs a
nd A
ttitu
des
Sear
ch fo
r pot
entia
l sou
rces
of
card
iac
embo
lism
, and
adv
ise p
rope
r m
anag
emen
tSe
arch
for o
ther
car
diov
ascu
lar
man
ifest
atio
ns o
f ath
eros
cler
osis,
in
part
icul
ar c
oron
ary
hear
t dise
ase
and
perip
hera
l art
eria
l dise
ase,
and
adv
ise
prop
er m
anag
emen
t
Und
erst
and
the
mec
hani
sm, l
ikel
ihoo
d,
and
pote
ntia
l tre
atm
ent o
ptio
ns o
f ca
rdia
c an
d ao
rtic
sou
rces
of e
mbo
lism
Be a
war
e of
the
frequ
ency
of
conc
omita
nt c
oron
ary
and
othe
r art
eria
l di
seas
e in
the
pres
ence
of i
sche
mic
ne
urol
ogic
dise
ase
Use
ech
ocar
diog
raph
y, in
clud
ing
tran
soes
opha
geal
ech
ocar
diog
raph
y,
and
othe
r tec
hniq
ues
to s
earc
h fo
r po
tent
ial s
ourc
es o
f em
bolis
mPr
opos
e a
diag
nost
ic w
ork-
up o
f th
e pa
tient
for o
ther
ath
eros
cler
otic
m
anife
stat
ions
, and
dev
ise p
rope
r th
erap
y an
d ris
k m
anag
emen
t
App
reci
ate
that
pot
entia
l sou
rces
of
em
bolis
m a
re fr
eque
ntly
of l
ow
prob
abilit
y (in
par
ticul
ar, p
aten
t for
amen
ov
ale)
and
com
mon
tly c
o-ex
istU
nder
stan
d th
e im
port
ance
of
diag
nosin
g an
d tr
eatin
g co
-exi
stin
g ca
rdio
vasc
ular
ath
eros
cler
otic
dise
ase
Real
ize
the
frequ
ency
of c
ardi
ac
sym
ptom
s, p
robl
ems
and
cons
ider
atio
ns in
oth
er d
iseas
es, (
e.g.
pu
lmon
ary
dise
ase,
con
nect
ive
tissu
e di
sord
ers)
and
be
able
to p
rovi
de p
rope
r m
anag
emen
t adv
ice
Ant
icip
ate
card
iova
scul
ar p
robl
ems
acco
mpa
nyin
g pr
imar
ily n
on-c
ardi
ac
dise
ases
Coo
pera
te c
lose
ly w
ith o
ther
disc
iplin
es
and
offe
r pro
mpt
sup
port
for t
heir
need
s an
d qu
estio
ns
• •
(con
tinue
d)
42
Car
diac
con
sult
in th
e pa
tient
with
isc
haem
ic n
euro
logi
c sy
mpt
oms
Car
diac
con
sult
in o
ther
situ
atio
ns

Co
re Curriculum
for th
e Gen
eral Card
iolo
gist
EUROPEANSOCIETY OFCARDIOLOGY ®
EUROPEAN SOCIETY OF CARDIOLOGY2035, ROUTE DES COLLES
LES TEMPLIERS - BP 17906903 SOPHIA ANTIPOLIS CEDEX - FRANCE
PHONE: +33 (0)4 92 94 76 00 FAX: +33 (0)4 92 94 76 01E-mail: [email protected]
Update 2008