
EUnetHTA INTERIM REPORT - European...
227
EUnetHTA INTERIM REPORT YEAR 2006 The EUnetHTA-project is supported by a grant fr the European Commission om EUROPEAN NETWORK FOR HEALTH TECHNOLOGY ASSESSMENT
Transcript of EUnetHTA INTERIM REPORT - European...
E U n e t H T A INTERIM REPORT YEAR 2006 The EUnetHTA-project is supported by a grant fr the European Commission om
E U R O P E A N N E T W O R K F O R H E A L T H T E C H N O L O G Y A S S E S S M E N T

EUnetHTA
European network for Health Technology Assessment
TECHNICAL INTERIM REPORT
delivered by the main beneficiary
National Board of Health of Denmark Danish Centre for Health Technology Assessment (DACEHTA)
February 2007
ii
List of contents Abbreviations .............................................................................................................................................................. i Technical Fact Sheet .................................................................................................................................................iii 1 Introduction ............................................................................................................................................................. 1 2 Overview of the EUnetHTA project ......................................................................................................................... 2
2.1 Background ..................................................................................................................................................... 2 2.2 Objectives........................................................................................................................................................ 2
2.2.1 Strategic Objectives................................................................................................................................. 2 2.2.2 Specific Objectives .................................................................................................................................. 2
2.3 Commissioners................................................................................................................................................ 3 2.4 Project Coordination........................................................................................................................................ 3 2.5 Tasks and Deliverables ................................................................................................................................... 4 2.6 Time-table ....................................................................................................................................................... 6
3 Work Package 1: Coordination................................................................................................................................ 7 3.1 Overview ......................................................................................................................................................... 7 3.2 Tasks Performed ............................................................................................................................................. 8
3.2.1 Building network of partners within EUnetHTA........................................................................................ 8 3.2.2 Co-operation between WP1 members and EUnetHTA............................................................................ 8 3.2.3 Coordination face-to-face meetings ......................................................................................................... 8 3.2.3.1 WP1 Coordination Meeting in Copenhagen, January 27,2006 ............................................................. 9 3.2.3.2 Steering Committee meeting in Copenhagen ....................................................................................... 9 3.2.4 EUnetHTA Information Platform ............................................................................................................ 10 3.2.5 EUnetHTA web-conferencing/e-meeting ............................................................................................... 11 3.2.6 Cooperation with the external parties .................................................................................................... 12
3.3 Work Plan for the next period (2007)............................................................................................................. 12 3.3.1 WP1 coordinating meetings................................................................................................................... 12 3.3.2 Objectives, Milestones and Deliverables in 2007 .................................................................................. 12
4 Work Package 2: Communications ....................................................................................................................... 13 4.1 Overview ....................................................................................................................................................... 13 4.2 Tasks Performed ........................................................................................................................................... 14
4.2.1 External Project Launch January 31, 2006 ............................................................................................ 14 4.2.2 Internal Project Launch February 7, 2006.............................................................................................. 14 4.2.3. 3-year plan, Graphic Profile and Logotype ........................................................................................... 14 4.2.4 EUnetHTA Info Package........................................................................................................................ 14 4.2.5 EUnetHTA Website/Information Platform .............................................................................................. 15 4.2.5.1 The Public Website, www.eunethta.net .............................................................................................. 15 4.2.5.2 The Members-Only Site...................................................................................................................... 15 4.2.5.3 Eight Work Package extranets ........................................................................................................... 15 4.2.6 EUnetHTA Members Update – Internal e-newsletter............................................................................. 15 4.2.7 Communication to commissioning parties and stakeholders ................................................................. 16 4.2.8 Articles................................................................................................................................................... 17 4.2.9 Communication Strategy ....................................................................................................................... 17
4.3 Work Plan for the next period (2007)............................................................................................................. 18 4.3.1 HTAi Conference 2007 .......................................................................................................................... 18 4.3.2 Further development of the Information platform................................................................................... 18 4.3.3 Helping other WPs with the communication issues ............................................................................... 18 4.3.4 The EUnetHTA Conference, Paris November 2008 .............................................................................. 18
5 Work Package 3: Evaluation ................................................................................................................................. 19 5.1 Overview ....................................................................................................................................................... 19 5.2 Tasks Performed ........................................................................................................................................... 19
5.2.1 Participant survey .................................................................................................................................. 19 5.2.2 WP leader interviews ............................................................................................................................. 19 5.2.3 Meetings ................................................................................................................................................ 19
5.3 Work Plan for the next period (2007)............................................................................................................. 20 6 Work Package 4: Common Core HTA (ie, HTA Core Model)................................................................................ 21
6.1 Overview ....................................................................................................................................................... 21 6.2 Tasks performed ........................................................................................................................................... 22
6.2.1 Surveys.................................................................................................................................................. 22 6.2.2 Meetings organised by WP4.................................................................................................................. 22 6.2.3 Outcomes of actions .............................................................................................................................. 22 6.2.4 Adherence to the work plan during the reporting period ........................................................................ 22 6.2.5 Other communications with WP partners / external parties ................................................................... 23 6.2.6 WP4 Teams........................................................................................................................................... 23
6.3 Work Plan for the next period (2007)............................................................................................................. 25 7 Work Package 5: Adapting existing HTAs from one country to other settings ...................................................... 26
i
7.1 Overview ....................................................................................................................................................... 26 7.2 Tasks performed ........................................................................................................................................... 27
7.2.1 Meetings Held........................................................................................................................................ 31 7.2.2 Other Communications with WP5 partners............................................................................................ 31 7.2.3 Communication outside of EUnetHTA ................................................................................................... 31
7.3 Work Plan for the next period (2007)............................................................................................................. 31 7.3.1 Scheduled meetings for 2007..................................................................................................................... 32
8 Work Package 6: Transferability of HTA into Health Policy................................................................................... 33 8.1 Overview ....................................................................................................................................................... 33 8.2 Tasks performed ........................................................................................................................................... 34
8.2.1 Structure of policy study provided – (M4) April 2006 ............................................................................. 348.2.2 Questionnaire on HTA in health systems completed ............................................................................. 34 8.2.3 Stakeholder Forum under preparation – (M14) February 2007 ............................................................. 35 8.2.4 Workshop with policy makers under preparation (M15) – March 2007.................................................. 35 8.2.5 European HTA Parallel workshop at European Health Forum Gastein - October 2006......................... 35 8.2.6 Communication with WP partners ......................................................................................................... 36
8.3 Work Plan for the next period (2007)............................................................................................................. 36 9 Work Package 7: Monitoring development for emerging/new technologies and prioritisation for HTA.................. 37
9.1 Overview ....................................................................................................................................................... 37 9.2 Tasks performed ........................................................................................................................................... 38
9.2.1 Strand A................................................................................................................................................. 38 9.2.2 Strand B................................................................................................................................................. 39
9.3 Work plan for the next period (2007) ............................................................................................................. 40 9.3.1 Strand A................................................................................................................................................. 40 9.3.2 Strand B................................................................................................................................................. 40
10 Work Package 8: Systems to support HTA in MS with limited institutionalisation of HTA................................... 41 10.1 Overview ..................................................................................................................................................... 41 10.2 Tasks performed ......................................................................................................................................... 42
10.2.1 HTA organisation characteristics review.............................................................................................. 42 10.2.2 Survey on HTA organisations (cf. Annex WP8.2) ................................................................................ 43 10.2.3 Survey information needs .................................................................................................................... 44 10.2.4 Adherence to the work plan during the reporting period. ..................................................................... 44 10.2.5 Communication with WP partners (e-meetings, workshops..) ............................................................. 44
10.3 Work plan for the next period (2007) ........................................................................................................... 45 10.4 Additional material ....................................................................................................................................... 46
10.4.1 WP8 info letter ..................................................................................................................................... 46 10.4.2 Information about the EUnetHTA project and WP8 published in CAHTA’s newsletter in 2006............ 46
Annexes ................................................................................................................................................................... 47
ii

Abbreviations AETSA Agencia de Evaluación de Tecnologías Sanitarias de Andalucía, Spain AETS Agencia de Evaluación de Tecnologias Sanitarias, Spain AHRQ Agency for Healthcare Research and Quality, USA AHTAPol Agency for HTA in Poland ASR Agenzia Sanitaria Regionale, Emilia Romania, Italy AP Associated Partner (within the EUnetHTA project) AVALIA-T Galician Agency for Health Technology Assessment, Spain CADTH Canadian Agency for Drugs and Technologies in Health (former CCOHTA),
Canada CAHTA Catalan Agency for Health Technology Assessment and Research, Spain CAST Centre for Applied Health Services Research and Technology Assessment,
University of Southern Denmark, Denmark CEDIT Commitee for Evaluation and Diffusion of Innovative Technologies, Direction
de la Politique Médicale, France CEESTAHC Central and Eastern European Society for Technology Assessment in Health
Care CP Collaborating Partner (within the EUnetHTA project) CRD Centre for Reviews and Dissemination, University of York, United Kingdom CVZ College voor zorgverzekeringen, The Netherlands DACEHTA Danish Centre for Health Technology Assessment, Denmark DAHTA@DIMDI German Agency for Health Technology Assessment at the German Institute
for Medical Documentation and Information, Germany DSI Danish Institute for Health Services Research, Denmark EUCOMED European medical technology industry association EUnetHTA European network for Health Technology Assessment EUPHA European Public Health Association EuroScan The European Information Network on New and Changing Health
Technologies FinOHTA Finnish Office for Health Technology Assessment, Finland FIPRA Finsbury International Policy & Regulatory Advisers (senior Public
Policy and Regulatory Advisers network) HAS Haute Autorité de santé, France HPV Human Papilloma Virus HSS Horizon Scanning System HTA Health Technology Assessment HTAi Health Technology Assessment international HunHTA Unit of Health Economics and Health Technology Assessment, Corvinus
University of Budapest, Hungary ICTAHC Israeli Center for Technology Assessment in Health Care, Israel iHIQA Interim Health Information and Quality Authority, Ireland INAHTA International Network of Agencies for Health Technology Assessment IQWIG Institute for Quality and Efficiency in Health Care, Germany ISPOR International Society for Pharmacoeconomics and Outcomes Research IPHRS Institute for Public Health of Republic of Slovenia IUMPS Institut Universitaire de medicine sociale et préventive Lausanne, Switzerland KCE Belgian Health Care Knowledge Centre, Belgium LBI@HTA Ludwig Boltzmann Gesellschaft GmbH, Austria LP Lead Partner (within the EUnetHTA project, organisation responsible for
leading and managing work in a Work Package) MoH Ministry of Health MS Member State (of the European Union) MSAC Medical Services Advisory Committee, Australia NBoH National Board of Health NCCHTA National Coordinating Centre for Heath Technology Assessment, United
Kingdom NICE National Institute for Clinical Excellence, United Kingdom NOKC Norwegian Knowledge Centre for the Health Services, Norway OECD Organisation for Economic Co-operation and Development OSTEBA Basque Office for Health technology Assessment, Spain PHGEN Public Health Genomic European Network SBU Swedish Council on Technology Assessment in Health Care, Sweden SNHTA Swiss Network for Health Technology Assessment, Switzerland STAKES National Research and Development Centre for Welfare and Health, Finland TU Berlin Technische Univrsität Berlin, Germany UETS Unidad de Evaluación de Tecnologías Sanitarias, Spain
i
UCSC Università Cattolica del Sacro Cuore, Policlinico universitario “A. Gemelli”, Italy
WHO-HEN World Health Organisation, Health Evidence Network WP (1-8) Work Package (within the EUnetHTA project) ZonMw The Netherlands Organisation for Health Research and Development, The
Netherlands
ii

Technical Fact Sheet Project European network for Health Technology Assessment (EUnetHTA) Project No. 2005110(790621) Programme Public Health Programme 2003-2008; Health Information and knowledge
2005 Unit of DG Sanco Risk Assessment (from January 2007; previously – Health Information) Start Date of Project January 1, 2006 Duration 36 months Objectives The overall strategic objective of the network is to connect public
national/regional health technology assessment (HTA) agencies, research institutions and health ministries, enabling an effective exchange of information and support to policy decisions by Member States, thus
• reducing overlap and duplication of effort and hence promote more effective use of resources,
• increasing HTA input to decision-making in member states and the EU and hence increasing the impact of HTA,
• strengthening the link between HTA and health care policy making in the EU and its member states,
• supporting countries with limited experience with HTA Tasks/Work packages WP1 Coordination
WP2 Communications WP3 Evaluation WP4 Common Core HTA WP5 Adapting existing HTAs to new contexts WP6 Transferability to health policy WP7 Monitoring development for emerging/new technologies and prioritisation of HTAs WP8 Systems to support HTA in MS with limited institualisation of HTA
DG Sanco Representative Mr. Panagiotis Daskaleros (successor of Mr. Daniel Mann) EUnetHTA Project Leader Prof. Finn Børlum Kristensen Main Beneficiary National Board of Health of Denmark, Danish Centre for HTA
(DACEHTA) Associated Beneficiaries / Partners • Ludwig Boltzman Institute of Health Technology Assessment,
LBI@HTA, Austria • KCE - Belgian Health Care Knowledge Centre, Belgium • Ministry of Health, Cyprus • University of Southern Denmark, Center for Applied Research
and Technology Assessment, Denmark • DSI- Danish Institute for Health Services Research, Denmark • University of Tartu, Department of Public Health, Estonia • FinOHTA - Finnish Office for HTA (STAKES), Finland • HAS - Haute Autorité de santé / French National Authority for
Health, France • DAHTA@DIMDI- German Agency for HTA at the German
Institute for Medical Documentation and Information, Germany • Technische Universitaet Berlin, Germany • University of Bremen, Interdisciplinary Centre for HTA,
Germany • University of Lübeck, Institute for Social Medicine, Germany • HunHTA - Unit of Health Economics and Health Technology
Assessment, Corvinus University, Hungary • iHIQA - interim Health Information and Quality Authority, Ireland • ASR - Agenzia Sanitaria Regionale, Emilia Romagna, Italy • Università Cattolica del Sacro Cuore, Policlinico universitario “A.
Gemelli”, Health Technology Assessment Unit and Laboratory of Health Economics (Institute of Hygiene), Italy
• Regione Veneto, Italy • VSMTA - Health Statistics and Medical Technology State
Agency, Latvia
iii

• Ministry of Health, Republic of Lithuania • NOKC – Norwegian Knowledge Centre for the Health Services,
Norway • Institute of Public Health, Republic of Slovenia • AETS - Agencia de Evaluación de Tecnologias Sanitarias,
Spain • AETSA - Andalusian Agency for Health Technology
Assessment, Spain • AVALIA-t, Galician Agency for Health Technology Assessment,
Spain • CAHTA - Catalan Agency for Health Technology Assessment
and Research, Spain • OSTEBA - Basque Office for Health Technology Assessment,
Spain • Servicio Canario de la Salud, Spain • UETS - Unidad de Evaluación de Tecnologías Sanitarias,
Agencia Laín Entralgo, Spain • SBU - Swedish Council on Technology Assessment in Health
Care, Sweden • CVZ - College voor zorgverzekeringen, The Netherlands • ZonMw, Netherlands Organisation for Health Research and
Development, The Netherlands • NCCHTA - National Coordinating Centre for HTA, United
Kingdom • Cochrane Collaboration (Secretariat), United Kingdom
Collaborating Partners • MSAC - Medical Services Advisory Committee, Australia • Hauptverband der Österreichischen Sozialversicherungsträger,
Austria • CADTH (former CCOHTA) - Canadian Agency for Drugs and
Technologies in Health, Canada • HTA and Health Service Research, Center of Public Health,
Århus, Denmark • CEDIT - Commitee for Evaluation and Diffusion of Innovative
Technologies, Direction de la Politique Médicale, France • German HTA Association, Germany • IQWIG - Institute for Quality and Efficiency in Health Care,
Germany • Public Health Genomics European Network (PHGEN), German
Center for Public Health Genomics (DZPHG), Germany • University of Iceland, Faculty of Medicine, Iceland • ICTAHC - Israeli Center for Technology Assessment in Health
Care, Israel • Agency for HTA in Poland, AHTAPol, Poland • CEESTAHC - Central and Eastern European Society for
Technology Assessment in Health Care, Poland • Institute of Molecular Medicine, Portugal • SNHTA - Swiss Network for Health Technology Assessment,
Switzerland • CRD - Centre for Reviews and Dissemination, University of
York, United Kingdom • AHRQ - Agency for Healthcare Research and Quality, Center
for Outcomes & Evidence, USA
European/International Organisations:
• Council of Europe - Directorate General III - SOCIAL COHESION
• European Observatory on Health Systems and Policies • EuroScan - European Information Network on New and
Changing Health Technologies • G-I-N Executive - Guidelines International Network • HTAi - HTAi Secretariat • INAHTA - INAHTA Secretariat
iv

• OECD - Organisation for Economic Cooperation and Development
• WHO - Health Evidence Network (HEN)
Project Contacts • Ministry of Health, Czech Republic
• Ministry of Health, Greece • Ministry of Health, Luxembourg • Ministry of Health, Malta
v

1 Introduction This report is the first Interim Technical Report on Implementation of the European network for Health Technology Assessment project (EUnetHTA), delivered by the main beneficiary National Board of Health of Denmark (Danish Centre for Evaluation and HTA (DACEHTA) to the Directorate-General Health and Consumer Protection, Directorate C – Public and Risk Assessment, Unit C7 – Risk Assessment. The Interim Technical Report of EUnetHTA covers the period from January 1, 2006 (start of the project) to December 31, 2006. The project is co-funded by the National Board of Health of Denmark (Danish Centre for HTA (DACEHTA) and thirty-three Associated beneficiaries of the project. As stipulated in the Reporting Requirements (Annex III of the Grant Agreement 2005110 (790621), the Interim Technical Implementation Report
• provides information on the results obtained to date and • gives an outlook to the work programme to be performed.
The Interim Technical Report on Implementation of the EUnetHTA project was prepared by the main beneficiary in collaboration with the Lead Partners of the Work Packages (WPs) where the main beneficiary is not leading the work:
• WP2 (SBU, Sweden, and DAHTA@DIMDI, Germany), • WP3 (NOKC, Norway), • WP4 (FinOHTA, Finland), • WP5 (NCCHTA, United Kingdom), • WP7 (HAS, France and LBI@HTA, Austria), • WP8 (CAHTA, Spain)
According to Article I.5.2 of the Grant Agreement, the beneficiaries authorise the Commission to disseminate, communicate or publish the report concerning the action. The annexes indicated as having a restricted confidentiality level due to planned future publication and postponed public presentation of the preliminary results should not be made public until the end of the action (December 2008). Additionally, the main beneficiary has submitted a consolidated financial statement on the first period (January 1, 2006 – December 31, 2006).
1

2 Overview of the EUnetHTA project
2.1 Background Healthcare provision is increasingly subject to policy decisions and is more managed than it was in earlier times. Healthcare is also more and more international. Today health professions, research, and industry all work across borders. Thus, the challenges are two-fold: How best to serve unmet health needs with effective health interventions in complex health systems functioning under budget restraints. Thanks to research and innovation new technologies are continuously introduced to healthcare with the potential to improve health through more effective care. In order to optimise care within limited resources those technologies that have the highest proven effectiveness should be promoted while taking organisational, societal and ethical aspects into consideration. Many EU Member States have public agencies to evaluate health technologies and others plan to establish them. These bodies engage in HTA, Health Technology Assessment, a systematic, transparent process to summarize information on the medical, social, economic and ethical issues related to the use of a new or established health technology. HTA brings together scientific evidence to inform policy makers, clinicians, and the public on safety, effectiveness and cost of health technology. Currently there is substantial duplication of HTA work undertaken across the EU, yet many areas that would benefit from HTA are not assessed due to either limited resources to undertake the work or concerns about the timeliness of HTA input to policy decisions. Therefore, it has been considered of great need to connect public national/regional HTA agencies, research institutions, and health ministries to enable an effective exchange of information and support to policy decisions by Member States. The overall aim is to achieve rapid uptake and use of effective health technologies that will achieve major improvements in patient outcomes and promote wise investment of resources, both into HTA and health technology in general. The EUnetHTA project aims at avoiding duplication, creating a common understanding of what constitutes good and efficient practice in developing a scientific basis for decisions in health care irrespective of health care systems, and developing tools to strengthen the coordination and cooperation between European HTA organisations. Currently EUnetHTA is developing tools to facilitate a more effective use of HTA resources in the EU, e.g. a generic methodological HTA framework based on current best practices (Core HTA Structure, tools for systematically handling evidence), a toolkit for adapting core HTA information from existing HTA reports to other contexts, and tools to monitor the development of health technologies and to share data and results of this monitoring. These tools will enable the HTA organisations to build on each others’ work and to coordinate their efforts.
2.2 Objectives
2.2.1 Strategic Objectives The strategic objectives are:
• To reduce overlap and duplication of effort and hence promote more effective use of resources
• To increase HTA input to decision-making in member states and the EU and hence to increase the impact of HTA
• To strengthen the link between HTA and health care policy making in the EU and its member states
• To support countries with limited experience with HTA
2.2.2 Specific Objectives 1. To establish the organisational and structural framework for an effective and sustainable European
network for HTA with a supporting secretariat.
2. To develop and implement generic tools for adapting assessments made for one country to new contexts; including tools for producing a common core of HTA evidence on clinical effectiveness, basic economic data and models, and for identifying key social, cultural and ethical issues relevant to assessed technologies.
3. To develop and implement effective tools to transfer HTA results into applicable health policy advice in Member States and the EU – including systems for identification and prioritisation of topics for HTAs and assessment of impact of HTA advice.
2
4. To effectively disseminate and handle HTA results, information sharing and coordination of HTA activities through the development of elaborate communication strategies and clearinghouse activities.
5. Effective monitoring of emerging health technologies to identify those that will have greatest impact on health systems and patients.
6. To establish a support system to countries without institutionalised HTA activity.
2.3 Commissioners The EUnetHTA project is commissioned by the Directorate-General Health and Consumer Protection of the European Commission (furthermore DG Sanco) under the framework of the Public Health Programme 2003-2008. The National Board of Health of Denmark (Danish Centre for HTA (DACEHTA) as the main beneficiary and thirty-three associated beneficiaries (see Technical Fact Sheet for details), co-funding EUnetHTA, act as second commissioning parties.
2.4 Project Coordination The EUnetHTA project is a rather complex project involving a large number of diverse partners which requires a high level of commitment from all the parties involved and balanced delegation of management and coordination responsibilities to ensure adequate involvement and performance of each contributing party. The project is coordinated by the main beneficiary National Board of Health of Denmark (Danish Centre for HTA (DACEHTA) located in Copenhagen (Denmark) in cooperation with the nine Associated Partners that act as Lead Partners in the respective WPs: WP1 – Coordination: National Board of Health, Copenhagen Denmark WP2 – Communications: Lead Partner - SBU, Swedish Council on Technology Assessment in Health Care, Stockholm, Sweden; Co-Lead Partner (Clearinghouse strand) - DAHTA@DIMDI, German Agency for HTA at the German Institute for Medical Documentation and Information, Cologne, Germany WP3 – Evaluation: NOKC, Norwegian Knowledge Centre for the Health Services, Oslo, Norway WP4 – Common Core of HTA: Finnish Office for HTA/STAKES, Helsinki, Finland WP5 – Applying common core information and adapting existing HTAs into local/national settings: NCCHTA, National Coordinating Centre for HTA, Southampton, United Kingdom WP6 – Transferability of HTA into health policy: National Board of Health, Copenhagen, Denmark WP7 – Monitoring emerging/new technology development and prioritization of HTA: Lead Partner - HAS, Haute Autorité de santé / French National Authority for Health, Paris, France; Co-Lead Partner - LBI@HTA, Ludwig Boltzman Institute of Health Technology Assessment, Vienna, Austria WP8 – System for support of countries without institutionalized HTA: Catalan Agency for HTA and Research, Barcelona, Spain The main beneficiary acts as the Coordinating Secretariat for the whole of the project. Table 2.1 lists the DACEHTA staff contributed to the EUnetHTA project in 2006 (in 2007 two more experts are employed to join the coordinating team): Table 2.1 Overview – EunetHTA Coordinating team at DACEHTA
DACEHTA Coordinating team
Finn Børlum Kristensen (Project Leader) Julia Chamova (Project coordinator) Louise Hansen (Assistant Project coordinator) Camilla Palmhøj Nielsen (coordinator for WP6 – DACEHTA is WP6 Lead Partner) Karin Engel Rasmussen Jørgen Eriksen Mads Frellsen* Malene Fabricius Jensen* * involved in the work of various EUnetHTA WPs
Each LP is responsible for the coordination of the activities in their respective WP and timely delivery of the results (deliverables) that are due according to the contract’s time-table (cf. Table 2.2). The main beneficiary and the LPs constitute the Executive Committee of the project. All APs in the project constitute the Steering Committee of the project. The project governance and management structure as well as the guidelines on the administration and financial management of the project are described in the Standard Operations Procedures (SOP) Manual developed by the
3
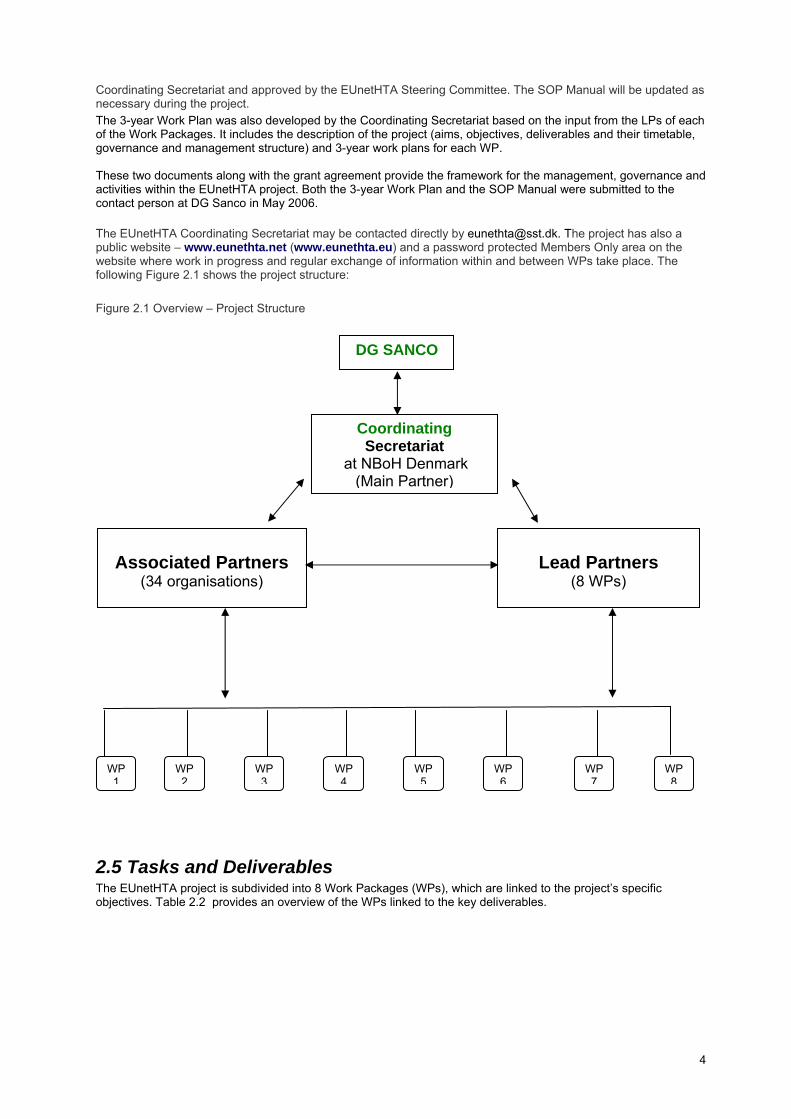
Coordinating Secretariat and approved by the EUnetHTA Steering Committee. The SOP Manual will be updated as necessary during the project. The 3-year Work Plan was also developed by the Coordinating Secretariat based on the input from the LPs of each of the Work Packages. It includes the description of the project (aims, objectives, deliverables and their timetable, governance and management structure) and 3-year work plans for each WP. These two documents along with the grant agreement provide the framework for the management, governance and activities within the EUnetHTA project. Both the 3-year Work Plan and the SOP Manual were submitted to the contact person at DG Sanco in May 2006. The EUnetHTA Coordinating Secretariat may be contacted directly by [email protected]. The project has also a public website – www.eunethta.net (www.eunethta.eu) and a password protected Members Only area on the website where work in progress and regular exchange of information within and between WPs take place. The following Figure 2.1 shows the project structure: Figure 2.1 Overview – Project Structure
2.5 Tasks and Deliverables The EUnetHTA project is subdivided into 8 Work Packages (WPs), which are linked to the project’s specific objectives. Table 2.2 provides an overview of the WPs linked to the key deliverables.
WP 1
Lead Partners
(8 WPs)
Associated Partners
(34 organisations)
Coordinating Secretariat
at NBoH Denmark (Main Partner)
WP 2
WP 3
WP 5
WP 4
WP 6
WP 8
WP 7
DG SANCO
4

Table 2.2: Overview – Objectives, WPs and deliverables Specific Objectives Deliverable No Work Package
To establish the organisational and
A organisational structure
nting the
structural framework for the network with a supporting secretariat
The EUnetHTincluding a supporting Secretariat Final report from the project EUnetHTA conference preseproject results
1 Coordination
To effectively disseminate and handle
f
ation platform
ity - detailed
TA conference presenting the
2 Communications HTA results, information sharing and coordination of HTA activities through the development and implementation oelaborate communication strategies and description of Clearinghouse functionality
Website/InformCommunication strategy A clearinghouse functionalidentification of the clearinghouse needsof different target groups and consecutive structure development to be ready for practical application after 3 years EUnetHproject results
tion of the project
3 Evaluation Internal evaluaFramework for external evaluation
To produce generic Core Models for
s well as
As for
4 Common core HTA HTAs on two essential categories of health technology questions: interventions and treatment, aCore HTAs on selected topics for each category
Core HTA structure/model 2 pilot examples of Core HTdifferent types of questions (e.g. diagnosis and treatment) A handbook on Core HTA.
To develop and implement generic tools A web based toolkit for adapting Core
ary
sting of core information
5 Adapting existing
settings
for adapting assessments made for one country to new contexts
HTA results from existing HTAs into other contexts including a HTA Glossof adaptation Applicability tefrom 2 existing HTA reports in various national environments using the toolkit
HTAs from one country into other
EUnetHTA Open Forum for stakeholders to exchange views and expectations/feedback oA book containing a systematic overvie
n HTA w
tems,
6 Transferability of cy
of the HTA & healthcare policy links in selected Member States & EU representing different health sysremuneration systems, etc
HTA to health poli
To develop and implement effective
the
and
ormation 7 Monitoring t
es
tools to transfer HTA results into applicable health policy advice in Member States and EU – including systems for identification and prioritisation of topics for HTAsassessment of impact of HTA advice
A prototype of a structured infservice on high volume, costly, rapidly developing, emerging technologies
developmenfor emerging new technologiand prioritisation of HTA
To develop effective monitoring of ntify
A set of monitoring tools for 7 Monitoring t for
logies
emerging health technologies to idethose that will have the greatest impact on health systems and patients
emerging/new technologies developmenemerging new technoand prioritisation of HTA
To establish a support system for TA
Handbook on HTA organisations. The 8 to support
d countries without institutionalised Hactivity
handbook will compile the results and information extracted from the review and the survey of HTA organisations
System HTA in Member States with limiteinstitutionalisation of HTA
5
In the following sections 3 to 10 each WP will be described in detail regarding its tasks and deliverables. Each section will
• give an overview of the WP (LP, APs and CPs involved, tasks, current status of deliverables, additional outcomes)
• describe the tasks performed and results obtained during the reporting period • present planned activities during the next reporting period
Deviations from the initial work programme outlined in the EUnetHTA grant agreement will be indicated. The EUnetHTA project coordination is pleased to report that additional tasks and spin-off activities have been performed than originally planned (eg, the network of the EUnetHTA partners have been enlarged by additional Collaborating Partners, and a cooperation on an HPV Vaccine HTA report currently performed by DACEHTA involves on an informal basis several EUneHTA members due to the sharing of protocols and information within the EUnetHTA project), which will be described in the respective sections on the individual WP reports.
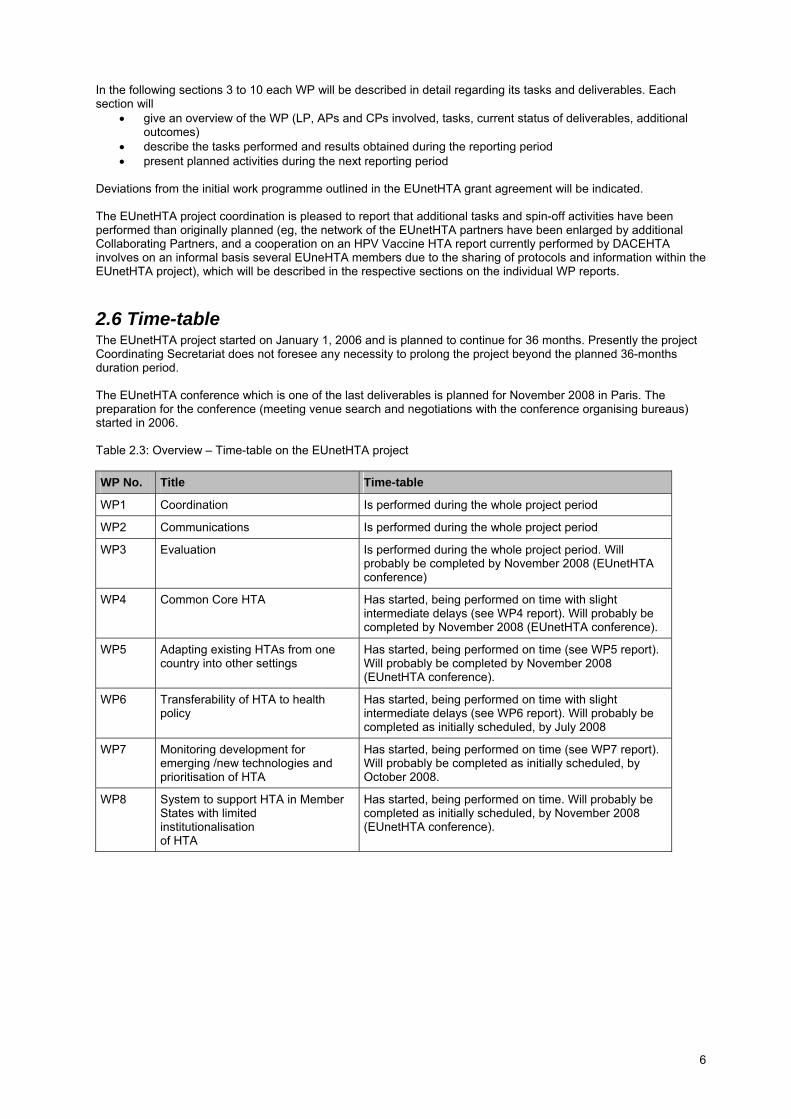
2.6 Time-table The EUnetHTA project started on January 1, 2006 and is planned to continue for 36 months. Presently the project Coordinating Secretariat does not foresee any necessity to prolong the project beyond the planned 36-months duration period. The EUnetHTA conference which is one of the last deliverables is planned for November 2008 in Paris. The preparation for the conference (meeting venue search and negotiations with the conference organising bureaus) started in 2006. Table 2.3: Overview – Time-table on the EUnetHTA project WP No. Title Time-table
WP1 Coordination Is performed during the whole project period
WP2 Communications Is performed during the whole project period
WP3 Evaluation Is performed during the whole project period. Will probably be completed by November 2008 (EUnetHTA conference)
WP4 Common Core HTA Has started, being performed on time with slight intermediate delays (see WP4 report). Will probably be completed by November 2008 (EUnetHTA conference).
WP5 Adapting existing HTAs from one country into other settings
Has started, being performed on time (see WP5 report). Will probably be completed by November 2008 (EUnetHTA conference).
WP6 Transferability of HTA to health policy
Has started, being performed on time with slight intermediate delays (see WP6 report). Will probably be completed as initially scheduled, by July 2008
WP7 Monitoring development for emerging /new technologies and prioritisation of HTA
Has started, being performed on time (see WP7 report). Will probably be completed as initially scheduled, by October 2008.
WP8 System to support HTA in Member States with limited institutionalisation of HTA
Has started, being performed on time. Will probably be completed as initially scheduled, by November 2008 (EUnetHTA conference).
6

3 Work Package 1: Coordination
3.1 Overview Work Package 1 Coordination Lead Partner (LP) Main Beneficiary: NBoH Denmark (Danish Centre for HTA (DACEHTA)
(LP in WP6)
Partners Involved
Associated Partners: LBI@HTA, Austria (Co-LP in WP7) DAHTA@DIMDI, Germany (Co-LP in WP2) FinOHTA (STAKES), Finland (LP in WP4) HAS, France (LP in WP7) NOKC, Norway (LP in WP3) CAHTA, Spain (LP in WP8) SBU, Sweden (LP in WP2) NCCHTA, United Kingdom (LP in WP5) Collaborating Partners: SNHTA, Switzerland WHO-HEN
Tasks
• Ensuring that the defined milestones and deliverables are
achieved according to the timetable and contract obligations • Acting as a contact point for DG Sanco, EUnetHTA APs and CPs
and for external parties • Ensuring a good communication and cooperation within the
project • Providing procedural, administrative and organisational support
during the project • Developing and maintaining SOP Manual up-to-date • Developing a 3-year EUnetHTA Work Plan • Preparing interim and final report for the project • Preparing and organising (in collaboration with WP2) EUnetHTA
conference at the end of the project • Developing the content of the EUnetHTA website
Current Status on Milestones and Deliverables
M5 (May 2006) Milestone – SOP Project manual to be approved by the Steering Committee – completed on time M6 (June 2006) Milestone – EUnetHTA website launch – completed on time M8 (August) Deliverable - An organisational structure for a European Network for HTA – including a supporting Secretariat – completed in advance (May 2006) to the deliverable date (part of the SOP Manual and the 3-year Work Plan developed by the Coordinating Secretariat and LPs) M14 (February 2007) Milestone – 1st Interim Report to the Commission – completed on time
Additional Outcomes/Activities
• Inclusion of additional relevant national and European institution
in the project • involvement of the EUnetHTA partners in the spin-off cross-
border collaborative activities in the actual HTA projects in the member institutions (HPV Vaccine HTA project)
• providing trainings in using new, Internet-based communication facilities (e-meetings) ensuring cost-effective use of limited project resources for communication
• participating in the Public Health Genomics (PHGEN) project (DG SANCO) to ensure relevant coordination with HTA through EUnetHTA
• participating (by way of DACEHTA, LBI@HTA , and Institute for Social Medicine, University of Lübeck) in the INNO-HTA project (DG Research, FP6)
• informing the Pharmaceutical Forum (DG Sanco, DG Enterprise) Working Group on Relative Effectiveness of Pharmaceuticals
7
about EUnetHTA activities on a continuous basis • establishing initial informal contacts with the stakeholder groups
not represented in the project membership to contribute in the development of the European HTA process responsive to the HTA-user needs
• contributing to the wider discussions on the future of the health services and health strategy in Europe
3.2 Tasks Performed
3.2.1 Building network of partners within EUnetHTA WP1 is linked to the strategic objective of connecting public national/regional HTA agencies, research institutions and health ministries, enabling an effective exchange of information and support to policy decisions by the Member States. The WP1 work is relevant throughout the whole project (cf. Table 2.3), with the work having started in winter 2004-2005. Already during the EUnetHTA proposal development, majority of the current EUnetHTA members committed themselves to participate in the project. Large part of the EUnetHTA membership consists of the HTA organisations that participated in the previous EU-supported projects on HTA. However, besides newcomer HTA organisations, quite a few EUnetHTA members represent additional stakeholder groups in the European HTA process (cf. Technical Fact Sheet), eg, Ministries of Health, research institutions, international/European supranational organisations, universities, third party payers that are new to being involved in the EU projects on HTA. During the first several months of the project several new collaborating partners joined the EUnetHTA partnership: Gesundheit Österreich GmbH (Austrian Health Institute), PHGEN project (Germany), Hauptverband der Österreichischen Sozialversicherungsträger (Germany), AHTAPol (Poland). At present WP8 is establishing working relationship with the Ministry of Health of Serbia. As of February 2007, 59 organisations from 24 EU Member States, 2 EEA countries (Norway and Iceland), Switzerland, and 4 countries outside Europe (Australia, Canada, Israel and USA) participate in the project. The WP1 consists of the EUnetHTA Associated Partners that assumed the role of the Lead Partners in the project. These organisations were initially involved in the development of the EUnetHTA project proposal in winter 2005 and committed themselves to lead work in the respective work packages (cf. 2 Overview of the EUnetHTA project). The Coordinating Secretariat and the LPs of the project developed the Standard Operations Procedures (SOP) Manual and the 3-year EUnetHTA Work Plan in spring 2006. Both documents were reviewed and approved by the EUnetHTA Steering Committee during the Steering Committee meeting in Copenhagen in May 2006 and submitted to the DG Sanco project contact at the time. The SOP Manual is updated as necessary. The Coordinating Secretariat is pleased to inform that a networking support provided by EUnetHTA (facilitated by the EUnetHTA webbased information platform) allowed to informally connect organizations-members of EUnetHTA in 9 countries to collaborate in an HPV Vaccine HTA project led by DACEHTA.
3.2.2 Co-operation between WP1 members and EUnetHTA To guarantee close cooperation and coordination of the activities within the project, WP1 holds monthly e-meetings with its members (cf. 3.2.5 EUnetHTA web-conferencing/e-meeting) in addition to extranet communication and regular (daily) exchange of information via email. Each LP also organises e-meetings within their respective WP individually based on the internal need to support their WP activities and involvement of their WP members. To facilitate the communication within and between the WPs the Internet-based EUnetHTA information platform has been set up (cf. 3.2.4 EUnetHTA Information Platform). In addition the Coordinating Secretariat produces regular (monthly) EUnetHTA Members Updates (e-mail based) with the information on the achievements, information requests, and upcoming activities/outcomes from the WPs. The Coordinating Secretariat holds regular coordinating team meetings at DACEHTA (on a fortnight basis).
3.2.3 Coordination face-to-face meetings For the EUnetHTA project, in addition to the e-meetings each WP has a number of planned face-to-face meetings. Table 3.1 shows the distribution of meetings between the work packages:
8

Table 3.1 EUnetHTA WP face-to-face meetings WP Location Number of meetings Schedule
DACEHTA, Copenhagen 2 1. January 27, 2006 2. May 11, 2006 (Steering Committee
meeting) CAHTA, Barcelona 1 • March 22-23, 2007 SBU, Stockholm 1 • October 2007
WP1
HAS, Paris 1 • April 2008 SBU, Stockholm 2 1. March 17-18, 2006
2. To be decided DAHTA@DIMDI, Cologne 2 1. December 7-8, 2006
2. To be decided
WP2
Ministry of Health of Cyprus, Nicosia
1 • May 12, 2007
NOKC, Oslo 1 • February 24, 2006 WP3 ASR, Bologna 1 • To be decided FinOHTA, Helsinki 3 1. September 19, 2006
2. January 18-19, 2007 (All APs to participate)
3. To be decided
WP4
University of Tartu, Estonia 1 • To be decided NCCHTA, London 1 • June 4-5, 2006 WP5 Regione Veneto, Venice 1 • September 27-28, 2007 DACEHTA, Copenhagen 1 • March 30, 2006 WP6 UCSC, Rome 1 • To be decided AETSA, Seville 1 • November 14-15, 2006 WP7 iHIQA, Dublin 1 • April 12-13, 2007 IPHRS, Ljubljana 1 • March 5-6, 2007 CAHTA, Barcelona 1 • June 2007
WP8
Galician Agency for HTA, Santiago di Compostella
1 • July 2008
DACEHTA, Copenhagen 1 • March 31, 2006 WPs 4-7 NCCHTA, London 1 • To be decided Due to close connection between the methodological developments of the work content in WP 4 to 7, it was deemed necessary to plan 2 face-to-face meetings between the LPs of these WPs to coordinate their content and activities’ schedule. The group has also organised an e-meeting on June 15 2006, and additional video conference between WP4 and WP5 LPs took place on August 21 (the minutes of the video conference is attached as annex to WP5 report). The list of participants, activities and outcomes of the first WPs 4-7 meeting (March 31, 2006) are described in the minutes of the meeting attached to this Interim Technical Implementation Report (cf. Annex WPI.3) The information from the WP2-8 meetings that took place in 2006 can be found in the reports of the respective WP (see following chapters).
3.2.3.1 WP1 Coordination Meeting in Copenhagen, January 27,2006 The WP1 members met in Copenhagen on January 27 2006. The main focus of the discussions was on preparation of the 3-year Project Work Plan and governance and management structure of the project. The summary of discussions including the list of participants and agenda is attached to this Interim Technical report (cf. Annex WPI.1)
3.2.3.2 Steering Committee meeting in Copenhagen The EUnetHTA Steering Committee meeting took place in Copenhagen on May 11, 2006. 42 persons, representing 36 institutions (including DG Sanco and the Ministry of Health of Denmark) participated in the meeting. The aim of the meeting was to provide opportunity for project participants to meet and get to know each other, thus strengthen the project dynamics. The agenda covered:
• presentation of the EUnetHTA project organisation and adoption of the SOP manual • presentation and endorsement of the EUnetHTA 3-year Work Plan • initial exchange of views on the opportunities and challenges of establishing a sustainable European
network for HTA The activities and outcomes of the Steering Committee meeting are described in detail in the minutes of the meeting attached to this Interim Technical Implementation Report (cf. Annex WPI.2)
9

3.2.4 EUnetHTA Information Platform To facilitate a good information flow between the EUnetHTA project and interested external parties as well as within the project, the Coordinating Secretariat has developed (in close cooperation with WP2) the EUnetHTA Information Platform. The public website was launched on June 31, 2006. The Information Platform is continuously developed further to become a well-known communication channel for the European HTA network beyond the project period. The Information Platform includes a public website (www.eunethta.net / www.eunethta.eu / www.eunethta.org) and a password-protected “Members Only” area that can be accessed through the public website. All EUnetHTA members have received log-in information. Please see below screenshots of a) the public EUnetHTA website and b) the Members Only area. a)
10

b)
The Members Only area is structured into the following sections:
• EUnetHTA information (subsections: eg, on the network members, deliverables, structure, 3-year work plan, administrative information including SOP an FAQ regarding financial management of the project)
• Definitions (within the project) • Work Packages (subsections: access to the individual WP• Communication (subsections: eg, publication guidelines, g
extranets) raphic profile, project calendar, access to the e-
ective WP extranets. A training session was provided to the LPs in ications).
The EUnetHTA members are encouraged to use the Members Only area and extranets for communication.
s its members with the internet based e-meeting facilities.
e Internet. It is live (information is conveyed according to an agenda, with a starting and ending time) and interactive, ie, information transmission is two-way between the audience and
uter anywhere in the world
That allows bringing together participants from different countries into a meeting in a live-simulated environment at a fra on ether in a face-to-face meeting.
In 20 t sessions to the EUnetHTA members in using the e-mee g
meeting facilities) • Contact (subsections: eg, searchable project contact database)
The Members Only area has also eight extranets for each Work Package. LPs are responsible for maintaining and placing up-to-date information in their respediting the contents of the extranets (cf. 4 Work Package 2 Commun
3.2.5 EUnetHTA web-conferencing/e-meeting To facilitate collaboration within Work Packages and also allow more effective and cost-effective interaction within the ongoing HTA projects in each Associated Partner organisation, EUnetHTA provide
E-meeting is a meeting conducted over th
presenter (both audio- and video-enabled). Each participant sits at his/her own compand connects to the meeting via Internet.
cti of the financial and organisational expenses of physically bringing people tog
06 he Coordinating Secretariat provided 17 trainingtin facilities.
11

The facil the inter-WP collaboration (please see individual WP reports). They were also used by the APs for their internal HTA collaboration efforts within the country and between the European
n with stakeholders in the European HTA process. T 6 the project started to establis older groups. The full list of meetin ere the EUnetHTA project was presen 2 Communications” section of these I ical Im lementation Report.
3 k Pl
3 1 coWP1 will hold 2 coo e Catalan Agency for earch (CAHTA) and on October 12, 2007 in Stockholm, Sweden (hosted by the S uncil on Board of Health, DACEHTA will assist in the organi
I egular of the work within the WPs and coord e activities i
3.3.2 ObjectiAccording to the 3- lowing objectives:
portin ating continuous content mana
engthe A network • Developin• Developin bers States’ MoH in EUnetHTA work • Strengthe ork and deliverables on
the Europ
Table 3.2 below shows the Milestones and Deliverables due in 2007. The deliverables due in 2007 will be submitted to the Commission according to the timetable below (ie, on the date of their availability)
Table 3.2: EUnetHTA Milestones and Deliverables 2007-02-11
ities were used by the LPs to support
countries – in total, 72 e-meetings took place as of December 31, 2006.
3.2.6 Cooperation with the external parties The EUnetHTA project aims at encouraging the closer cooperatio
hus, in 200gs wh
h contacts with relevant stakehted can be found in “4 WP
nterim Techn p
.3 Wor an for the next period (2007)
.3.1 WP ordinating meetings rdinating face-to-face meetings on March 22-23, 2007 in Barcelona, Spain (hosted by th HTA and Res
wedish Co technology Assessment in Health Care (SBU). The National ponsible for their contents. sation of the meetings and be fully res
n addition, r monthly e-meetings will be held to monitor the progressinating th n the project.
ves, Milestones and Deliverables in 2007 year WP1 Work Plan, the activities in 2007 will focus on the fol
• Sup g effective work within the WPs and facilitand
• Strgement coherence between WPs ning ties with identified partners external to EUnetHTg a long-term strategy for EUnetHTA g a sustainable mechanism for involving EU Memning the awareness about the EUnetHTA’s wean and international level
Date Milestone (Deliverable)
Year 2007
Month 13 WP2 (D2) – communication strategy (1 month delay from the initial date in 2006), WP4 (D5) – Core Model draft (2 months delay from the initial date in 2006), WP5 (D8) – Toolkit
Month 14 WP1: 1st Interim Report to the Commission WP7, Strand B (D13) - Prototype of a structured information service on the emerging technologies
Month 15 WP6 (D11) - Public Stakeholder Forum(website) established WP6 – Policy makers workshop
Month 17 WP4 (D6) – first pilot example of Core HTA Core HTA
Month 18 WP2 – Exhibition, Workshop at HTAI WP4 – meeting to discuss the results of the applicability testing and development needs WP8 - Survey a) HTA orgs, b) Info needs: results and report
Month 21 WP5: 1st applicability testing completed
Month 24 WP2 (D14): Clearinghouse functionality structure WP8 (D15): Handbook on HTA capacity building WP7 – Implementing and testing monitoring tool
Total EUnetHTA deliverables in 2007: 8
12

4 Work Package 2: Communications
4.1 Overview Work Package 2 Communications Lead Partner (LP) Co-Lead Partner
SBU, Sweden DAHTA@DIMDI, Germany (Clearinghouse strand)
Partners Involved
Associated Partners: ASR, Italy CAHTA, Spain Cochrane Collaboration, United Kingdom DACEHTA (NBoH Denmark), Denmark HAS, France HunHTA, Hungary KCE, Belgium MoH, Cyprus Regione Veneto, Italy UETS, Spain Collaborating Partners: AHRQ, USA AHTAPol, Poland CADTH, Canada CRD, United Kingdom EuroScan, United Kingdom G-I-N Executive, Germany INAHTA SNHTA (Winterthur Institute of Health Economics), Switzerland
Tasks • Facilitate coherent, effective and sustainable external and internal communication of the project, where its aims, objectives, work in progress, results and final products are known to all partners, identified stakeholders and target groups on the EU and national/regional levels. • Identify scientific literature databases of relevance to HTA and ways to provide access to support the work of the project members • Provide common data structures and common communication interoperability of information systems building on existing systems and databases such as INAHTA’s HTA Database. • Offer structures for semantic interoperability • Explore best solutions to providing a contemporary electronic publishing facility for results, methodological and scientific developments and public information of the network. • Provide structure for assuring the quality of the information produced by the network • Development of a model for the future operation of the Clearinghouse (including organisational, management, and financial aspects) in regard to the needs of members and external target groups • Development of a Clearinghouse prototype to describe the functionalities in preparation for the future implementation of a running Clearinghouse
Current Status on Milestones and Deliverables
M4 (April 2006) Milestone – Common logo/graphic profile, 3-year plan&info package – completed on time M6 (June 2006) Milestone – EUnetHTA website launch – completed on time M12 (December 2006) Deliverable – Communication strategy of the network – completed on Jan 19, 2007, delivered M18 (June 2007) Milestone –Seminar/open meeting at the HTAi
13

Conference 2007 – work in progress M24 (December 2007) Deliverable – Clearinghouse functionality – work in progress M35 (November 2008) Deliverable – EUnetHTA Conference (project results and future plans presented) – preparation work commenced M36 (December 2008) Deliverable – Final report from the project – due after completion of the project
Additional Outcomes/Activities
• Several presentations of the EUnetHTA project in international conferences
• Several articles about the project published • Publication and graphic guidelines were developed • EUnetHTA project is known to a wide group of relevant
stakeholders in MS • EUnetHTA project is referenced in the major European business
newspaper
4.2 Tasks Performed
4.2.1 External Project Launch January 31, 2006 A list of different target groups was compiled in due time before the project launch and a press release was sent electronically to identified selected specialised periodicals/mass media outlets, and associations for healthcare professionals, health care industry associations, patient associations at the EU and international level. The aim was to create awareness of the project and its aims. A temporary public website was developed within DACEHTA’s information platform and open for public access already several months prior to the project’s start.
4.2.2 Internal Project Launch February 7, 2006 To facilitate communications within the network a first temporary version of the Members-only-site was opened in time for the internal project launch. The website was developed within the CMS system hosted by SBU. A template text was prepared for the Ministers of Health and relevant health policy bodies informing about the project aims, objectives, and activities. The EUnetHTA partners took the responsibility to translate and adjust the text to local context and distribute to relevant healthcare policy bodies. Short text to create awareness of the project on the national/regional level was prepared and sent out for the members to put on their web sites, in e-newsletters, websites, etc To encourage EUnetHTA members to visit and get acquainted with the Members Only site, create a positive interest around EUnetHTA, and enhanced the traffic to the website a competition was arranged.
4.2.3. 3-year plan, Graphic Profile and Logotype 3-year WP2 Work Plan has been developed for inclusion for the EUnetHTA Project 3-year Work Plan. Developed early in the project, the EUnetHTA logo and graphic profile (includes colours, fonts, illustrations and photographs) was used in all communication on the web, in PowerPoint presentations, communication materials, etc. The EUnetHTA logo is a symbol of communication, cooperation, networking and energy. It has a distinct look and is easy to remember. The EUnetHTA logo makes it easier to gain and maintain recognition. A symbol has been created for each Work Package. The Work Packages have been assigned short names to be used on the websites and communication material together with the symbols. A Graphics Guide has been put together so that members can more easily use the graphic profile. The guide explains how to use the EUnetHTA logo, the EU logo, the Work Package Symbols, the pictures, etc.
4.2.4 EUnetHTA Info Package EUnetHTA is focusing on producing electronic communication material to be downloaded from the website. All communication material is produced in-house.PowerPoint templates with a variety of slides have been put together using the EUnetHTA graphic profile. Intended for external presentations, internal presentations and tables, they incorporate the logos of both EUnetHTA and the Partner organisations.
14

One overall factsheet for the EUnetHTA project and one for each Work Package have been compiled. The factsheets are handed out at conferences, exhibitions, meetings, etc, where the EUnetHTA partners participate. PDF versions of the factsheets are available on the Members-only site so that they can be printed out by each Partner organisation. The Publication Guidelines for the project were developed. They include principles of publication, presentation and other public communication by EUnetHTA. The Publication Guidelines set the terms on which we agree to receive and provide information, striking the balance between transparency and confidentiality.
4.2.5 EUnetHTA Website/Information Platform The EUnetHTA information platform includes a public website with a Members-only section and eight extranets, one for each Work Package. The Members-only area has a login function, including a username and password. Users can upload information, participate in discussion forums and submit comments. Most EUnetHTA partners have established links to the EUnetHTA website. We have also registered the website at key web portals. The EUnetHTA website was developed using an Episerver Content Management System (CMS). The CMS makes the website easy to update regardless of programming skills. Development of the EUnetHTA website follows the Web Accessibility Initiative (WAI) Guidelines for universal accessibility. The guidelines have been recommended for all governmental agencies of EU Member States, and the European Commission co-finances the WAI project.
4.2.5.1 The Public Website, www.eunethta.net The content of the public website will be expanded during the project as information from the Work Packages is published and transferred from the Members-only site. The website includes information about EUnetHTA, its members, the results of the project, links to HTA organisations, important HTA sources and much more. Three domain names have been registered: www.eunethta.net, www.eunethta.org and www.eunethta.eu Some practical functions available on the EUnetHTA public website: • Subscription function: Visitors can sign up for the EUnetHTA Update, an e-newsletter that is sent to subscribers
and specified target groups.
• Search engine: The Members-only site includes a search engine.
• News function: News is listed automatically on the home page.
• Calendar Function is considered for development in 2007
4.2.5.2 The Members-Only Site The Members-only site is open to all EUnetHTA Members. There you will find minutes, work in progress, invitations to meetings, results of the project, etc. Some practical functions available on the Members-only site: • Members contact database: EUnetHTA Members have been entered into a contact database on the Members-
only site. The database, which is searchable, includes contact information for all EUnetHTA Members
• Search engine: The Members-only site includes a search engine.
• Group mail function: The group mail function makes it possible to e-mail all members of a Work Package or subgroup, whose addresses will be constantly updated
• Calendar: A calendar has been developed to keep track of conferences, meetings, etc
• Form template: The template makes it easy to create forms for surveys and the like.
4.2.5.3 Eight Work Package extranets Each Work Package has its own dedicated extranet that is accessible through the Members-Only site. The extranets contain working documents, minutes, meeting agendas, internal documents, financial information and other features. They will be updated by each Work Package Lead Partner. Relevant personnel from each Lead Partner organisation have been trained in Episerver.
4.2.6 EUnetHTA Members Update – Internal e-newsletter The EUnetHTA Members Update is sent to all EUnetHTA Partners once a month. The Secretariat, with help from WP 1, compiles and edits the information. WP 2 LP is responsible for developing the Members Update format. The
15

members are asked to forward the newsletter to their colleagues. The Members Update is planned to be published on the Members-only site.
4.2.7 Communication to commissioning parties and stakeholders The EUnetHTA project has been committed to a transparent communication to the commissioning parties (DG Sanco and Associated Partners) and to the stakeholder groups. The APs take responsibility for the communication on the national and regional level. A representative from the DG Sanco was present at the Steering Committee meeting in Copenhagen in May 2006. The login information to the Member-Only website and relevant email correspondence have been forwarded to the contact persons at DG Sanco. Table 4.1 gives an overview of the EUnetHTA project presentations held during 2006. Individual APs held presentations in their local institutions and held briefings at their respective D/MoH. Most of the presentations were held at the expense of the receiving institution or the presenting organisation. Table 4.1: Presentations of EUnetHTA in 2006
Date Place Audience Content of the presentation
Presenting Institution
01/2006 Trento, Italy Italian HTA Network Conference European HTA collaboration, EUnetHTA project
DACEHTA
02/2006 Bielefeld, Germany
PHGEN meeting EUnetHTA project, organisational aspects in HTA
DACEHTA
02/2006 Brussels, Belgium
Working Group on Relative Effectiveness Meeting
EUnetHTA project DACEHTA
02/2006 Luxembourg 6th meeting of the Network of Competent Authorities
EUnetHTA project DACEHTA
03/2006 Rome, Italy Meeting the Italian APs in the EUnetHTA project
Regional coordination of HTA in MS
DACEHTA
04/2006 Vienna, Austria
Meeting of Regulatory Bodies on Medical Devices
EUnetHTA project LBI@HTA
05/2006 Copenhagen, Denmark
Meeting with FIPRA EUnetHTA project DACEHTA
05/2006 Copenhagen, Denmark
Meeting with EUCOMED EUnetHTA project, involving stakeholders in the European HTA process
DACEHTA
05/2006 Paris, France Senior Management team at HAS
EUnetHTA project, European collaboration on HTA in individual MS
HAS/DACEHTA
06/2006 Brussels, Belgium
High Level Group Meeting Update on the EUnetHTA project
DACEHTA
06/2006 Manchester, United Kingdom
OECD Expert meeting on “The Evaluation of Clinical Validity and Clinical Utility of Genetic Tests”
EUnetHTA project HAS
07/2006 Adelaide, Australia
HTAi Annual Conference EUnetHTA project, Work in Progress
DACEHTA, HAS, LBI@HTA, NCCHTA, FinOHTA
08/2006 Seoul, Korea World Congress on Medical Physics and Biomedical Engineering 2006 “Imaging the Future Medicine
EUnetHTA presentation, abstract
MoH of Cyprus (in cooperation with the EUnetHTA Executive)
10/2006 Brussels, Belgium
Working Group on Relative Effectiveness Meeting
Update on the EUnetHTA project progress
DACEHTA
10/2006 Pavia, Italy Conference “HTA: Evaluazione e Diffusione in Italia”
EunetHTA project, international HTA
DACEHTA, UCSC
16

collaboration
10/2006 Copenhagen, Denmark
ISPOR, 9th Annual European Congress
EUnetHTA Project: Clearinghouse, emerging technologies and monitoring systems, Core HTA model Development, Adapting HTAs in various contexts
DACEHTA, DAHTA@DIMDI, FinOHTA, NCCHTA (HAS contributed)
10/2006 Bad Gastein, Austria
European Health Forum Gastein EUnetHTA project, European HTA activities, involvement of the stakeholders in the European HTA process
Diverse group of speakers; organized by DACEHTA (details can be seen on www.eunethta.eu)
11/2006 Montreaux, Swtzerland
EUPHA Annual Conference EUnetHTA project update DAHTA@DIMDI
11/2006 Seville, Spain
Spanish HTA Network Annual Conference
European HTA collaboration
DACEHTA, AETSA
12/2006 London, United Kingdom
1st Health Care Winter Symposium, Blenheim Palace
European HTA collaboration
DACEHTA
12/2006 Brussels, Belgium
Meeting with the representatives from DG Sanco, Unit C7-Risk Assessment
Progress of the EUnetHTA project
DACEHTA
12/2006 Luxembourg 7th meeting of the Working Party on Health Systems
Update on the EUnetHTA project
DACEHTA
12/2006 Brussels, Belgium
Seminar on Health Investments EUnetHTA project, role of TA in health investment decisions
KCE
12/2006 London, United Kingdom
HTA for Medical Devices across Europe, seminar
Core HTA of the drug eluting stents, EUnetHTA project update
FinOHTA
4.2.8 Articles The EUnetHTA project shall also be made public via articles in journals. A number of articles to create an awareness f the project has been published in 2006 (cf. Table 4.2), however, majority of the publications are planned by the end of the project when the project results can be presented. The published articles provided a general description of the project, its aims, objectives and organisation.
Table 4.2 – Articles on EUnetHTA in 2006
Date Journal Article Author 03/2006 Bundesgesundheitsblatt -
Gesundheitsforschung - Gesundheitsschutz
Toward a sustainable European Network for Health Technology Assessment
DACEHTA
04/2006 Eurohealth EUnetHTA and health policy-making in Europe
DACEHTA
05/2006 Journal of the European Association for Health Information and Libraries
EUnetHTA- The First European Network to Assess Health Technology
KCE
4.2.9 Communication Strategy The Communication Strategy is a project Deliverable and it has been published on the Members-only site and sent to the Commission in January 2007 (2 weeks delay of the initial date due to holiday season). The strategy is an internal living document to be developed and changed as the project progresses. All EUnetHTA Members will have an opportunity to comment on the document and discuss it further at future meetings. The strategy has been drawn up for the 3-year project. Once the network has become sustainable and continuous, the strategy will have to be adjusted accordingly. The purpose of the strategy is to identify how we must communicate to achieve the goals of EUnetHTA.
17

4.3 Work Plan for the next period (2007)
4.3.1 HTAi Conference 2007 EUnetHTA will hold a pre-conference session in Barcelona in June 2007. The focus will be on the proceedings from the WP4, 5 and 7. WP 1 is responsible for the session in collaboration with WP2. EUnetHTA will also consider other ways to be present at the HTAi Conference, eg, exhibition booth.
4.3.2 Further development of the Information platform The EUnetHTA website should eventually become more interactive. It should be possible to vote, take part in different discussion forums, submit comments and otherwise contribute. We must also listen to our members and visitors for ideas about how to improve the website. Once the running Clearinghouse has been launched, it will facilitate information sharing among various target groups. Analysis of the website statistics is planned. The following functions will be discussed within the group for inclusion:
• Bookmarks: This function makes it possible to save pages and information for future reference. You can create your own list of bookmarks in order to personalise the site and make it faster to navigate.
• RSS flows: Real Simple Syndication (RSS) flows allow you to automatically collect new content from a variety of websites and blogs so as to present it in a structured way.
• Podcasts: Podcast technology permits you to easily, quickly and inexpensively transmit audiovisual information from meetings and conferences.
• Wikipedia: A Wikipedia function makes it possible for anyone to write and modify text on a website. The function should be incorporated into the website and used when appropriate.
• Map of Europe: An interactive map of Europe will be designed to show information about EUnetHTA Partners, the healthcare systems of different countries and the like.
4.3.3 Helping other WPs with the communication issues During 2007 and 2008 WP2 will help with the following communication issues: Work Package 6: Develop dedicated part of the website for the EUnetHTA Open Stakeholder Forum: The first dedicated web pages will be launched in March 2007. They will include an open forum for stakeholders, including FAQ, and a discussion forum. One member from the Work Package 2 Communication group will assist with communication questions regarding the stakeholder groups. Work Package 5: Develop a web-based toolkit: Including a glossary for HTA report adaptation. Work Package 7: A Web-based form on which a partner can submit a request with different information (to be defined in 2007) and validate the page. The page would be sent to an e-mailbox (of the Lead Partner) for analysis and validation and a database of requests so that any Partner can read it (after validation by the Lead Partner)
4.3.4 The EUnetHTA Conference, Paris November 2008 The results of the 3-year EUnetHTA project will be presented at the EUnetHTA Conference in Paris on November 20, 2008. The title will be “Conference on European HTA Cooperation: Progress and Future”. WP 2 will organise the conference in collaboration with WP 1. The target is to attract 500 participants. The venue will be the “Scientific International Centre of the Pasteur Institute” in Paris. The invitation to the conference will be developed and possibly e-mailed and published on the EUnetHTA website by the end of 2007. The EUnetHTA Partners will be asked to pass along the invitation and publish it on their websites.
18

5 Work Package 3: Evaluation
5.1 Overview Work Package 3 Evaluation Lead Partner (LP)
NOKC, Norway
Partners Involved
Associated Partners: AETS, Spain ASR, Italy Cochrane Collaboration, United Kingdom DAHTA@DIMDI, Germany Regione Veneto, Italy SBU, Sweden VSMTA, Latvia Collaborating Partners: MSAC, Australia OECD Biotechnology Division, France SNHTA, Switzerland
Tasks • Carry out internal evaluation of the project • Prepare the framework for external evaluation
Current Status on Milestones and Deliverables
M4 (April 2006) Milestone - Establishing reporting routines from other work packages. Start prospective evaluation. Status: Completed. Results of first of five interviews of Work Package leaders and of first of three participant surveys are available M30 (June 2008) Deliverable – Framework for external evaluation. Status: is being prepared to be available in due time M34 (October 2008) Deliverable: Internal evaluation report. Status: is being prepared to be available in due time
Additional Outcomes/Activities
• The interim internal evaluation reports were developed to function as both the internal audit and coaching the activity during the project period.
5.2 Tasks Performed
5.2.1 Participant survey The participant survey questionnaire was developed to catch the impression of the participant ideas of domains of interest regarding the development of EUnetHTA and its future possibilities. The participants were also asked to give their experience and expectations for the work in the groups they had joined. The questionnaires underwent an iteration process among the WP3 members on the development of the questionnaire content. They were sent out as an attachment to an e-mail late in June 2006. The response was slow as the summer holiday varies across Europe. Lead Partner (LP) Manager for WP3 organized the collection of the questionnaire responses and made the report which the group reviewed. The results of the survey are published on the WP3 section of the members only of the EUnetHTA web-site.
5.2.2 WP leader interviews We sought to follow the WP leaders own view on the progress and any deviations to each WP plan every six month. This in order to catch their views and how they may alter as EUnetHTA is developing. The different stages may pose different challenges to the leaders. This evaluation was not one directed on detailed technical issues but one that should map their impressions of major issues as they saw it. In 2006 the leaders have been interviewed about the first six months of 2006. The interviews were short and were held by the WP3 LP Project Manager. The results of the interview are available on the WP3 section of the Members-Only site.
5.2.3 Meetings WP3 started its planning by holding a face-to-face meeting in Oslo, Norway, on February 24th 2006. In, addition, two telephone-meetings have been arranged. Minutes of the meetings are attached (cf. Annex WP3.1)
19

5.3 Work Plan for the next period (2007)
The following activities are planned: • Interviews with WP leaders no.2, January and 3, August • Participant Survey no.2, May-June • E-meeting /telephone-meeting in relation to the above activities
20

6 Work Package 4: Common Core HTA (ie, HTA Core Model)
6.1 Overview Work Package 4 Common Core HTA (ie, HTA Core Model) Lead Partner (LP)
FinOHTA, Finland
Partners Involved
Associated Partners: AETSA, Spain AVALIA-t, Spain Cochrane Collaboration, United Kingdom DACEHTA, Denmark DSI, Denmark KCE, Belgium MoH, Lithuania NCCHTA, United Kingdom NOKC, Norway OSTEBA, Spain SBU, Sweden TU Berlin, Germany University of Tartu, Estonia UCSC, Italy University of Lübeck, Germany ZonMW, the Netherlands Collaborating Partners: AHTAPol, Poland G-I-N Executive, Germany SNHTA, Switzerland University of Iceland, Iceland Gesundheit Österreich GmbH, Austria
Tasks • To produce examples of context-independent HTA topics (Core HTAs) for two different types of questions (e.g. diagnosis and treatment).
• Linked to the HTA production to develop a generic methodological HTA framework based on current best practices (Core HTA Structure).
• To support the adaptability testing of Core HTAs in various national HTA agencies (Adaptation, WP5) and to finalise the Core Structure after the testing.
• To participate in the development of models for policy transferability of national adaptations based on these Core HTAs (Transferability, WP6).
• To examine the need for developing additional types of Core Structures.
Current Status on Milestones and Deliverables
Milestones M9: September 2006, Workshop for evaluating Core Structure - Completed M10: October 2006, 1st Draft Core HTA Topic ready for applicability testing - In process, delayed until M14 M11: November 2006, Training meeting for APs testing Core Topics - Delayed until M13 (Jan 18-19) M18: June 2007, Meeting to discuss results of applicability testing & development needs - Scheduled for 2007 M33: September 2008, Second Core HTA finalised, Handbook on Core HTA development and use - Scheduled for 2008 Deliverables D 5: A generic methodological HTA framework based on current best practices (Core HTA Structure) - First draft ready, final draft delayed until M13 D 6: 2 pilot examples of Core HTAs for different types of questions (e.g. diagnosis and treatment) - First core topic (treatment) in process, draft ready for applicability testing in M14. Second topic (diagnostics) selected, work on actual report will commence in 2007.
21

6.2 Tasks performed
D 7: Handbook on Core HTA development and use -Scheduled for 2007-2008.
Additional Outcomes/Activities
• Consultation with stent manufacturer, see below. • The project was presented during the HTAi conference in
Adelaide, June 2-5, 2006 and at the 9th ISPOR Annual European Congress in Copenhagen, October 29, 2006.
• The project was presented in a seminar "Funding & reimbursement for Medical Devices" arranged by Informa Life Sciences in Brussels on 6 December 2006. Among the some 20 participants, health care managers and medical device industry were represented. It was a part of the EUnetHTA stakeholder involvement activities.
• The work being done in the WP4 was part of the presentations done on multiple occasions by the EUnetHTA Project Leader (see WP2 Communications).
6.2.1 Surveys Two surveys were conducted among the WP4 APs and CPs to select topics for the two assessments ("core HTAs") that are used for testing the two core models. Participants of the surveys first proposed topics that would be interesting from their point of view. The proposals were circulated and one most suitable and favoured topic was selected through a voting process. The first survey consisted of two rounds and resulted in selecting drug eluting stents to be the topic of the first core HTA. The second survey consisted of three rounds and resulted in selecting multi-slice CT angiography for the topic of the second core HTA.
6.2.2 Meetings organised by WP4 A workshop was organized to evaluate the first core model on the 19th of September in Helsinki. All APs and CPs that participate in the work package 4 were invited. Thirty persons participated, 19 of which were representatives of APs or CPs and 11 of FinOHTA. The minutes of the workshop are attached o this Interim Technical Implementation report as a separate file/document.
6.2.3 Outcomes of actions Work on the first core HTA structure, referred within the project also as the "core model", and the first core HTA on drug eluting stents has been divided to teams that consist of experts from partner organizations. Each team focuses on one domain of HTA, e.g. effectiveness, cost-effectiveness, ethics, or impact on health care organization. Teams are coordinated by representatives of FinOHTA. Full domain and team list are included at the end of this section.
The first draft of the first core model was produced for the September workshop. Based on discussions within the meeting and other feedback, a second draft is currently under construction and will be discussed in a WP4 meeting in January 2007. Work on the first core topic has also been initiated.
6.2.4 Adherence to the work plan during the reporting period Regarding the content, work has progressed as planned: drafts of core HTA structure (core model) and of a core HTA on drug eluting stents are under construction as a joint work of several European organizations. With respect to the original timeline, the work is slightly delayed. The deliverable D5 (draft of the core HTA structure) will be finalized by the end of M13 instead of M11*. A draft of the first core HTA on drug eluting stents (that is based on the core HTA structure) will be finalized by mid-February. These timelines have been agreed on with WP5 to prevent serious negative impact on their work. To facilitate common work with WP5, the most recent version of the core model was sent to WP5 during M12. The training meeting originally scheduled for M11 will be organized in M13.
We have identified three main reasons for delay in our work package. Firstly, the task of building a common core structure for HTA is very challenging per se. Despite earlier European collaborative projects, HTA is still perceived differently across Europe and the contents of HTA reports vary considerably. Hence extensive deliberation has been required to achieve common methodology and aims in building the core structure. Secondly, an active part of the activity in our work package took place during the summer months, which posed an extra difficulty. Summer vacation months vary in different parts of Europe (June-August), which made the collaborative work of various expert teams more difficult. Finally, the large size of the project consortium constitutes a problem for reaching
* The draft Core HTA model was delivered to the Commission DG Sanco on January 31. It is currently undergoing a review process within the EUnetHTA project and is requested not to be publicly distributed and kept them under the restricted confidentiality level until the scheduled public launch (June 17, 2007, HTAI pre-conference workshop, Barcelona, Spain)
22

agreements in practical things. WP4 has aimed to involve as many partner organizations as possible in the work, which in turn has required more time when waiting for responses.
6.2.5 Other communications with WP partners / external parties Frequent email communication with WP5, including a joint WP4/WP5 video-conference (5 participants) on the 21st of August, 2006.
WP4 organized on the the 7th of August, in collaboration with project lead partner DACEHTA, a meeting in Copenhagen to explore possible collaboration between the project and a major manufacturer of drug eluting stents, Johnson & Johnson and to hear manufacturer's views on assessment. Further consultations with other manufacturers are considered during the project.
WP4 participated in a WP6 meeting on the 30th of March (2 representatives) and on the 31st of March in a coordination meeting for WPs 4-7 (2 representatives). Both meetings took place in Copenhagen.
WP4 has participated in several e-meetings organized by WP1 to support coordination of the project.
The project was presented during the HTAi conference in Adelaide, June 2-5, 2006 and at the 9th ISPOR Annual European Congress in Copenhagen, October 29, 2006. The project was presented in a seminar "Funding & reimbursement for Medical Devices" arrance by Informa Life Sciences in Brussels on 6 December 2006. Among the some 20 participants, health care managers and medical device industry were represented.
6.2.6 WP4 Teams The work on different domains has been done as a collaborative effort of WP4 teams (cf.Table 6.1). Each team consists of investigators that are responsible for writing the sections of the report and reviewers whose task is to provide support and feedback to investigators in their team. Each team has also a coordinator on behalf of FinOHTA. 6.1 Table – WP4 Teams
DOMAIN
Coordinator Investigators Reviewers
Primary investigators for CM and CT in italics General design of the assessment
Kristian Lampe (CM) Marjukka Mäkelä (CT) [email protected]; [email protected]
Finn Børlum Kristensen, DACEHTA Inger Norderhaug, NOKC Alison Price, NCCHTA Alberto Ruano-Ravina, AVALIA-T Marcial Velasco Garrido, TU Berlin [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Irina Cleemput, KCE Chris De Laet, KCE Bo Freyschuss, SBU Marco Marchetti, UCSC Dagmar Lühmann, U Lübeck [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Current use of the technology (implementation level)
Marjukka Mäkelä [email protected]
Marcial Velasco Garrido (CM), TU Berlin Bo Freyschuss (CT), SBU Chris De Laet, KCE Marta Lopez de Argumedo, OSTEBA Monika Reesev, U Tartu Leonor Varela Lema, AVALIA-T [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Alberto Ruano-Ravina, AVALIA-T Nick Hicks, NCCHTA Marco Marchetti, UCSC Kersti Meiesaar, U Tartu [email protected]; [email protected]; [email protected]; [email protected]
Description and technical characteristics of technology
Marjukka Mäkelä (CM) [email protected]
Primary investigator for CT to be confirmed Pekka Kuukasjärvi, FinOHTA Antti Malmivaara, FinOHTA Marcial Velasco Garrido, TU Berlin [email protected]; [email protected]; [email protected]
Leonor Varela Lema, AVALIA-T Marta Lopez de Argumedo, OSTEBA Monika Reesev, U Tartu [email protected]; [email protected]; [email protected]
Safety Marjukka Mäkelä [email protected]
Nick Hicks (CM), NCCHTA Hans van Brabandt (CT), KCE Chris De Laet (CT), KCE Regina Kunz, SNHTA Pekka Kuukasjärvi, FinOHTA Antti Malmivaara, FinOHTA
Alberto Ruano-Ravina, AVALIA-T Leonor Varela Lema, AVALIA-T Marta Lopez de Argumedo, OSTEBA Inger Norderhaug, NOKC [email protected]; [email protected]; osteba5-
23

Alison Price, NCCHTA [email protected]; [email protected]@kenniscentrum.fgov.be; [email protected]; [email protected]; [email protected]; [email protected];
[email protected]; [email protected]
Effectiveness Marjukka Mäkelä [email protected]
Antti Malmivaara (CM), FinOHTA Regina Kunz (CT), SNHTA Chris De Laet, KCE Pekka Kuukasjärvi, FinOHTA Susanne Rasmussen, DSI Hans van Brabandt, KCE [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Alberto Ruano-Ravina, AVALIA-T Leonor Varela Lema, AVALIA-T Marta Lopez de Argumedo, OSTEBA Bo Freyschuss, SBU Marco Marchetti, UCSC Inger Norderhaug, NOKC Monika Reesev, U Tartu Kersti Meiesaar, U Tartu [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Costs, economic evaluation
Pirjo Räsänen (CT) [email protected]
Kersti Meiesaar (CM), U Tartu Matthias Bischof, SNHTA Irina Cleemput, KCE Henrik Hauschildt-Juhl, DSI Monika Reesev, U Tartu Harri Sintonen, FinOHTA [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Alberto Ruano-Ravina, AVALIA-T Marco Marchetti, UCSC Inger Norderhaug, NOKC Torbjørn Wisløff, NOKC [email protected]; [email protected]; [email protected]; [email protected]
Ethical aspects
Ilona Autti-Rämö (CM) [email protected]
Dagmar Lühmann (CT), U Lübeck Bjørn Hofmann, U Oslo Marco Marchetti, UCSC Inger Norderhaug, NOKC Samuli Saarni, FinOHTA [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Marta Lopez de Argumedo, OSTEBA Marcial Velasco Garrido, TU Berlin [email protected]; [email protected];
Organisational aspects
Päivi Reiman-Möttönen [email protected]
Ulla Saalasti-Koskinen (CM), FinOHTA Marco Marchetti (CT), UCSC Finn Børlum Kristensen, DACEHTA Nick Hicks, NCCHTA Juha Koivisto, FinSoc Pekka Kuukasjärvi, FinOHTA [email protected]; [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Irina Cleemput, KCE Marcial Velasco Garrido, TU Berlin Martti Kekomäki, FinOHTA Dagmar Lühmann, U Lübeck [email protected]; [email protected]; [email protected]; [email protected]
Societal aspects
Päivi Reiman-Möttönen [email protected]
Ilona Autti-Rämö (CM), FinOHTA Juha Koivisto (CT), FinSoc Heidi Anttila, FinOHTA Bjørn Hofmann, U Oslo Dagmar Lühmann, U Lübeck [email protected]; [email protected]; [email protected]; [email protected]; [email protected]
Marcial Velasco Garrido, TU Berlin Marco Marchetti, UCSC Markku Myllykangas, FinOHTA Alison Price, NCCHTA [email protected]; [email protected]; [email protected]; [email protected]
Legal aspects
Kristian Lampe [email protected];
Laura Walin (CM), FinOHTA Marco Marchetti (CT), UCSC Inger Norderhaug, NOKC [email protected];
Bjørn Hofmann, U Oslo Nick Royle, CC Sirpa Soini, FinOHTA to be confirmed [email protected];
24
[email protected]; [email protected];
[email protected]; [email protected]
6.3 Work Plan for the next period (2007) During year 2007, the following steps will be taken:
• A training meeting to support the use of the core model and core topics will be organized in January 2007
• The first core model and core topic will be sent to consultation to project partners and further refinements will be made.
• The applicability of the first core model will be tested in collaboration with WP5 in 2007.
• Work on the second core model and core topic will be initiated.
• A workshop to discuss further development of core models and topics will be organized in the summer for WP4 participants.
• Support will be given particularly to WP5 and WP6 as agreed in the contract.
• Public launch of the Core HTA Model, HTAi pre-conference workshop, June 17, Barcelona, Spain
25

7 Work Package 5: Adapting existing HTAs from one country to other settings
7.1 Overview Work Package 5 Adapting existing HTAs from one country to other settings Lead Partner (LP)
NCCHTA, United Kingdom
Partners Involved
Associated Partners: AETSA, Spain ASR, Italy Cochrane Collaboration, United Kingdom DACEHTA, Denmark DAHTA@DIMDI, Germany DSI, Denmark FinOHTA, Finland HAS, France LBI@HTA, Austria KCE, Belgium NOKC, Norway OSTEBA, Spain Servicio Canario de la Salud, Spain TU Berlin, Germany IPHRS, Slovenia Regione Veneto, Italy UCSC, Italy University of Tartu, Estonia ZonMW, the Netherlands Collaborating Partners: AHTAPol, Poland Austrian Health Institute, Austria Hauptverband der Österreichischen Sozialversicherungsträger, Austria Institute of Molecular Medicine, Portugal PHGEN, Germany SNHTA, Switzerland University of Iceland, Iceland
Tasks WP5’s objective is to ensure better use of existing HTA reports by developing a toolkit for adapting the “core” within assessments made for one country into advice appropriate to other contexts within which it may be implemented through policy. The intention is to enable the production of structured products based on work already done that can then be easily utilised in policy making in member states and the EU. Facilitating the use of existing HTAs will contribute to minimising the duplication of work. To this end, the following task are being undertaken:
1. A survey of current practice in Member States in adapting HTA reports from other countries.
2. The development of a toolkit for adapting core HTA information from existing HTA reports to other contexts.
3. The applicability testing of the adaptation of core information from 2 existing HTA reports in various national HTA environments using the toolkit.
Current Status on Milestones and Deliverables
Milestones M10 (October 2006) Draft glossary of HTA adaptation concepts and terms - Completed on time M12 (December 2006) Draft HTA adaptation toolkit document developed - Completed on time M21(September 2007) First applicability testing round - Planned to start M15 M30 (June 2008) Second applicability testing completed - Planned to start M22 Deliverables
• An HTA adaptation toolkit tailored for use by EU and Member States - Draft toolkit document currently under revision in
26
preparation for first round of applicability testing • Applicability testing of the adaptation of core information from 2
existing HTA reports in various national settings using the toolkit - Currently planning testing rounds
Additional Outcomes/Activities
Activities/Outcomes associated with the Toolkit - Preliminary survey of current practices of adaptation by WP
members - Literature search on methods and experience of adaptation - Delphi Questionnaire to WP5 member (3 rounds); to explore
initial ideas for the toolkit, to examine the role of the toolkit within stages of adaptation, and to comment on the draft toolkit.
- WP5 meeting in London June 2006 to discuss “adaptation of HTA” and the role of the toolkit.
- Individual members’ commentary work on toolkit content - Five e-meetings to discuss toolkit content - Review of toolkit ‘domains’ by WP5 members - One workshop and one e-meeting to discuss the development of
the interactive toolkit Activities/Outcomes associated with the Glossary
- Review of previous HTA glossaries. - Identification of potential glossary terms (via Delphi Questionnaire
Round 1 & WP5 Meeting). - E-mail consultation with WP5 members to develop a description
for ‘adaptation’. - Individual members’ work to develop descriptions for glossary
terms - Initial draft of glossary put on EUnetHTA website for review by
WP5 members. - Glossary put on EUnetHTA website for review by all EUnetHTA
members - Presentation at the HTAi Conference in Adelaide, June 2-5, 2006 - ISPOR conference presentation on toolkit and glossary
development (October 2006) - NCCHTA in-house presentation on the EUnetHTA project and
NCCHTA involvement (March 2006)
7.2 Tasks performed The main activities of WP5 to date have focused on the development of two deliverables:
1. An Adaptation Toolkit tailored for use by EU and Member States – delivered to the Commission in January 2007 and made available on the WP5 extranet. Public launch of the glossary is planned for the HTAi pre-conference workshop on June 17, 2007, Barcelona, Spain
2. A Glossary of HTA adaptation concepts and terms for EU member countries – delivered to the
Commission in January 2007 and made available on WP5 extranet. Public launch of the glossary is planned for the HTAi pre-conference workshop on June 17, 2007, Barcelona, Spain
Task Action Outcome
Time limited search of key papers on methods and experience of adaptation
Completed M3
Case studies of topics e.g. PET scanning where more than one European country have produced reports
To be undertaken (time permitting)
A preliminary survey of all WP5 APs and CPs to determine current and past practice of adapting HTA reports from other countries.
Completed M4
Delphi round 1 of all WP5 APs and CPs to help determine components for the toolkit. Aim of round 1 was for opinions on a proposed structure for the toolkit.
Completed M5
Discussion of Delphi round 1 results and issues relating to toolkit content at WP5 face to face meeting.
Completed M6
W5 members produced commentaries on areas of specific toolkit content (toolkit domains)
Completed M7 - M9
Adaptation Toolkit
(See Figure 1 below)
Delphi round 2 of all WP5 APs and CPs to agree Completed M7
27

structure and function of toolkit and role in adaptation E-meetings to discuss members’ commentary work. Completed M9 – M10 Members’ review of toolkit content (toolkit domains) Completed M11 Delphi round 3. Editorial round – comments on the draft toolkit document
Completed M12
Review previous glossaries e.g. those of INAHTA, CCRD, U.S. McMasters and CADTH, Cochrane Collaboration, EUPHA and EU Observatory on Health Care Systems.
Completed M4
Request ideas for glossary from WP5 members in the 1st round of Delphi and at the WP5 face-to-face meeting.
Completed M5/M6
Create a glossary of HTA ‘adaptation’ terms that complements previous glossaries. With focus on areas of misunderstanding e.g. assessment and appraisal.
Completed M7
Allocate 4/5 glossary terms to members requesting them to draft descriptions and examples of usage for each term.
Completed M9
Make glossary available on the web for comments from WP5 partners
Completed
Final collation and editing of Glossary, incorporating all descriptions and comments received from WP5 partners.
Completed M10
Preparation of a paper detailing the methods used in the development of the Glossary.
Completed M12
Glossary of HTA adaptation terms
(See Figure 2 below)
Make glossary and paper available on the web for comments from all EUnetHTA members, to enable continual evolution of the glossary terms and descriptions.
Currently underway
28

Figure 1 WP5 Adaptation toolkit: Sequence of activities
Stage 1Previous experience of
adaptation
WP5 Partners’ Review of toolkit domains
Literature search
Stage 2Initial ideas on toolkit structure
and content
Stage 3Toolkit function and role in
adaptation
Stage 4Toolkit content development
Stage 5Review & collation (NCCHTA)
ADAPTATION TOOLKIT
Delphi survey round 1
Proposed structure for toolkit
WP5 Partners’ commentary work on
toolkit ‘domains’
WP5 face to face
meeting
Stages yet to be completed:- Further revisions as result of review - Applicability testing - Review by all EUnetHTA partners
Delphi survey round 2
Toolkit content and role in adaptation
E-meetings with Partners on commentary work
Preliminary survey on adaptation
Delphi survey round 3
Review toolkit document
29

Figure 2 WP5 Glossary: Sequence of activities
Stage 1
Developing list of terms WP5 Meeting
Other HTA Glossaries
Delphi Round 1 Questionnaire
Stage 2
Gathering descriptions
Stage 3Collating the descriptions
(NCCHTA)
Stage 4
Comments on descriptions
Stage 5Final editing & collation
(NCCHTA)
GLOSSARY OF HTA ADAPTATION TERMS
11 WP5 partners asked to draft
descriptions on 3/4 terms (in style of
sample term)
All WP5 partners consulted on a draft of
the Glossary
NCCHTA drafts sample description of “adaptation”
WP5 partners consulted on description
Stages yet to be completed:- Review by WP5 partners - Review by all EUnetHTA partners
30
7.2.1 Meetings Held 1. WP 4,5,6, and 7 Coordinating meeting in Copenhagen, March 31, 2006 2. WP5 face to face meeting in London, UK June 5th and 6th 2006 (Minutes: cf. Annex WP5.1) 3. E-meetings with WP5 Partners to discuss toolkit domains (Minutes: cf. Annex WP5.1):
a. 21/09/06: Safety b. 21/09/06: Effectiveness c. 28/09/06: Technology Use d. 02/10/06: Economic Evaluation e. 02/10/06: Organisational Aspects
4. Interactive toolkit development e-meeting with WP2 Lead Partner 21/11/06 (Minutes: cf. Annex WP5.1)
5. Interactive toolkit development workshop with WP2 Lead Partner 14/12/06 6. WP4 and WP5 Lead Partners Videoconference 21/08/06 (Minutes: cf. Annex WP5.1)
7.2.2 Other Communications with WP5 partners E-mail requests to WP5 partners to aid in the development of the Toolkit and the Glossary. Toolkit:
• Preliminary survey of experience of adaptation. • Delphi round 1. • Delphi round 2. • Delphi round 3. • Review process.
Glossary:
• Consultation in the development of the description for “adaptation”. • Allocating 12 WP5 partners 3/4 terms to develop descriptions. • Draft glossary posted on web & WP5 partners contacted requesting comments.
Information and requests were also placed on the WP5 extranet site.
7.2.3 Communication outside of EUnetHTA • ISPOR conference presentation on toolkit and glossary development (October 2006)
• NCCHTA in-house presentation on the EUnetHTA project and NCCHTA involvement (March 2006)
7.3 Work Plan for the next period (2007) The next steps for WP5 are detailed below: Adaptation Toolkit
• Applicability testing of the adaptation of 2 Core HTAs in various national settings using the toolkit:
• Identify an existing HTA report for applicability testing • First round of applicability testing. Testing to be undertaken in a number of national HTA
environments using the toolkit • Refinement of toolkit guidance and glossary in light of applicability testing • Development of the web-based interactive toolkit • Second round of applicability test on existing HTA report and WP4 core topic • Feedback results of applicability testing to WP4 for refinement of core structure • Refinement of toolkit guidance and glossary in light of applicability testing • Integration of interactive adaptation toolkit and glossary into EUnetHTA website (subject to
discussion with WP2) • Report results to partners and stakeholders
Glossary of HTA adaptation terms
• Make glossary available to all EUnetHTA partners on the web. • Use the comments received to enable the continual evolution of the glossary terms and descriptions. • Incorporate final glossary into the toolkit.
Public launch of the Glossary at the HTAi Conference, June 17-20 2007, Barcelona, Spain.
31

7.3.1 Scheduled meetings for 2007 • Interactive toolkit development e-meeting with WP2 30/1/07 • WP4 and WP5 Lead Partners e-meeting to discuss testing rounds 14/2/07 • WP5 face to face meeting (Venice) 27/09/07 and 28/09/07
E-meetings with WP5 Partners involved in testing rounds will be scheduled throughout 2007.
32
8 Work Package 6: Transferability of HTA into Health Policy
8.1 Overview Work Package 6 Transferability of HTA into Health Policy Lead Partner (LP)
National Board of Health (DACEHTA), Denmark
Partners Involved
Associated Partners: TU Berlin, Germany AETS, Spain AVALIA-t, Spain CAST, Denmark Cochrane Collaboration, United Kingdom CVZ, the Netherlands DAHTA@DIMDI, Germany DSI, Denmark FinOHTA, Finland iHIQA, Ireland IPHRS, Slovenia KCE, Belgium NCCHTA, United Kingdom NOKC, Norway Servicio Canario de la Salud, Spain UCSC, Italy UETS, Spain University of Bremen, Germany University of Tartu, Estonia Collaborating Partners: AHRQ, USA CEDIT, France Council of Europe, Directorate General III Social Cohesion G-I-N Executive, Germany Hauptverband der Österreichischen Socialversicherungsträger, Austria HTAi Secretariat HTA and Health Services Research, Denmark IQWIG, Germany INAHTA Secretariat Institute of Molecular Medicine, Portugal OECD PHGEN, Germany SNHTA, Switzerland WHO - HEN University of Iceland, Iceland
Tasks • To get a systematic overview of the relations between HTA and healthcare policy making in selected Member States and the EU representing different health systems, remuneration systems etc., and to classify and analyse common characteristics of the relations
• To improve the responsiveness of HTA to the demands of the HTA consumers with the purpose of promoting HTA as policy input
• To show concrete use of HTA in policy making in Member States and the EU
• To position HTA in relation to other relevant sources of input to health policy making and to regulatory processes
• To support improved responsiveness by building a sustainable open forum for EUnetHTA to exchange views, expectations and feedback on HTA with HTA stakeholders.
The deliverables of WP6 are: • A book describing
o The policy structures and policy processes related to the production and use of HTAs in policy making in the
33

selected Member States and the EU o The demands to HTA from health care and clinical policy
members in the Member States and the EU o Possibly the actual handling of the EUnetHTA prototype
HTA in the Member States and in the EU, alternatively published separately
• The establishment of a EUnetHTA Stakeholder Forum Current Status on Milestones and Deliverables
M4 (April 2006) Milestone: Provide structure of policy study - Completed (cf. Annex WP6.1.a and Annex WP6.1.b) M14 (February 2007) Deliverable: EUnetHTA Stakeholder Forum established – ongoing, delayed 1 month (Draft – cf. Annex WP6.2) M15 (March 2007) Milestone: Workshop with researchers/book authors and policy makers - ongoing (cf. Annex WP6.3) M30 (June 2008) Deliverable: Book published and dissemination initiated - ongoing
Additional Outcomes/Activities
• Questionnaire on HTA in health systems (cf. Annex WP6.4) • European HTA Parallel Forum at European Health Forum
Gastein, October 2006 (cf. Annex WP6.5) • Information about the EUnetHTA project and WP6 published in
DACEHTA’s newsletter in 2006 (cf. Annex WP6.6) • Contribution to coordination of activities with The Pharmaceutical
Forum: the Working Group on Relative Effectiveness • Presentation of the work of WP6 at the HTAi Conference 2006 in
Adelaide and at the ISPOR Annual European Conference 2006 in Copenhagen.
8.2 Tasks performed The tasks and activities of WP6 which were planned to be done during this first year of the EUnetHTA project have been successful achieved (cf. Table 6.1). The following activities represent the major actions of 2006:
8.2.1 Structure of policy study provided – (M4) April 2006 By the end of March a draft structure of the policy study was provided for discussion during the meeting with all invited partners in Copenhagen (30.03.2006). After input from the partners at the meeting and a round of e-mail consultation a final structure of the policy study was distributed. The agreed-upon structure was finished in April, and a more detailed guideline for completion of the policy study and for distribution of the work was developed (cf. Annex WP6.1.a and Annex WP6.1.b).
The structure and the guideline for the policy study are now forming the basis for writing of 9 chapters which are all included in the policy study planned to be published in June 2008. First drafts of the chapters are expected in February 2007.
8.2.2 Questionnaire on HTA in health systems completed A questionnaire aimed at collecting information on the peculiarities of HTA in European health systems (not on individual organisations, but on the whole health system, the process and the impact of HTA in each country) was forwarded to all WP6 members (cf. Annex WP6.4). The purpose was to map the policy processes of HTA in the EU countries since these may take different forms in the same country/health care system. Different organisations might be doing and using HTA at different decision-levels, and differing in the breadth of aspects assessed.
The survey was constructed in order to supplement relevant information in the country profiles of the Health Care Systems in Transition (HiT) Series of the European Observatory on Health Systems and Policies with relevant HTA information. The purpose was to avoid duplication of already existing information and to compliment this with HTA process related knowledge.
The results of the survey are currently being analysed and will be used and reported in more chapters of the policy study. The survey was completed by the end of October 2006.
The results are also forming the basis of a general understanding of the relations between HTA and various stakeholders and will be useful in the work with the Stakeholder Forum.
34

8.2.3 Stakeholder Forum under preparation – (M14) February 2007 A Stakeholder Forum is currently under development (cf. Annex WP6.2) The Forum will focus on users of HTA, and five stakeholder groups are strategically selected: national/regional policymakers, institutional (hospital level) policymakers, patient organisations, health care professionals, and industry.
The aim of the Stakeholder Forum is to create an open environment which enables exchange of views, expectations and feedback on HTA between key stakeholders and EUnetHTA. The forum will function as a tool for receiving input from the selected stakeholder groups and providing output from EUnetHTA.
The first step is to create a stakeholder website (currently being developed). The further development of the forum is being planned and will be concretized by 5 working parties in WP6, but the existing plans include arranging face-to-face-meetings e.g. workshops with stakeholder groups (see policy maker workshop below), and encouraging position papers on HTA from key stakeholders or stakeholder groups.
The Stakeholder Forum is made public at the EUnetHTA website March 30, 2007.
8.2.4 Workshop with policy makers under preparation (M15) – March 2007 The workshop will be held in Berlin, 15th- 16th of March 2007. The aim of the workshop is to establish contact with central national/regional policymakers, to present work-in-progress from EUnetHTA and WP6 specifically, and not the least to exchange views, expectations and feedback on HTA (cf. Annex WP6.3)
The results of the workshop will both be reported in the EUnetHTA WP6 policy study and will be used in the work with the Stakeholder Forum.
8.2.5 European HTA Parallel workshop at European Health Forum Gastein - October 2006 EUnetHTA was presented and discussed at a European HTA parallel Forum. The purpose of this activity was: 1) to increase the knowledge of EUnetHTA in a forum engaging a broad range of stakeholders in the field of public health and health care and 2) to seek stakeholder involvement in the development of EUnetHTA in order to increase the responsiveness of HTA processes to stakeholder needs and expectations. The workshop was well-attended (around 70 people) and received a positive response from the European policymakers. EUnetHTA got a lot of valuable input from the stakeholders which will be used in the continuous work with establishing awareness and good relations with stakeholder groups, and with strengthening the openness and receptiveness of the HTA community. The content and outcomes of the workshop is reported in a program and a report with conclusions/recommendations (cf. Annex WP6.5) Table 6.1 - WP6 Work plan 2006 (January 2006 - December 2006)
Activities / Months 1 2 3 4 5 6 7 8 9 10 11 12 Deliverable 1 – Policy study (PS)
Structure for PS M Partners meeting in Copenhagen
Partners commenting on structure for PS
Detailed guideline for PS
Questionnaire on health systems
Policy study – chapter writing
Deliverable 2 - Stakeholder Forum (SF)
Early plan for SF Partners commenting on plan for SF
European Health Forum Gastein
Detailed plan for SF Preparation of policymaker workshop
M: milestone
35
8.2.6 Communication with WP partners The first partner’s meeting was held on March 30th in Copenhagen where the general outline of work in WP6 was discussed and agreed upon. Twenty-eight partners were represented at the meeting. During this meeting it was emphasised that in addition to e-mail contact it is possible to use e-meetings, phone meetings, and face-to-face meetings. During 2006 the main channel has been e-mail, but it has been the aim to start using the EUnetHTA members-only website for communication purposes as a supplement to e-mails. This effort will be intensified in 200. In addition a number of face-to-face meetings between partners have taken place in other situations (e.g. conferences, other WP meetings in EUnetHTA). These meetings have been used to plan and discuss the work of WP6. Finally a few telephone calls or meetings have taken place. In 2007 WP6 will focus on working in smaller groups focusing on either writing parts of the policy study or working with developing relations with different stakeholder groups. Communication in these smaller groups will first and foremost happen through e-meetings and e-mails
8.3 Work Plan for the next period (2007) Based on the achievements up to December 2006, the following are the next steps and major activities planned for next year 2007:
1. Finalising first draft of chapters for policy study (February 2007). Finalising second and third drafts. Peer review process initiated.
2. Policymaker workshop (Berlin, March 15th – 16th). The workshop will be organized so that policymakers
and WP6 partners meet and exchange views, and that the policymakers formulate their demands and expectations to HTA in future
3. Stakeholder Forum website made public. 4. Continued work with establishing stakeholder relations within the EUnetHTA Stakeholder Forum. In April
2007 each working group will provide detailed plans for establishing relations with each their stakeholder group.
Planned activities in 2008: Policy study finalised and followed up by dissemination activities. Continue developing a long-term strategy for Stakeholder involvement in HTA/EUnetHTA.
36

9 Work Package 7: Monitoring development for emerging/new technologies and prioritisation for HTA
9.1 Overview Work Package 7 Monitoring development for emerging/new technologies and
prioritisation for HTA Lead Partner (LP) Co-Lead Partner
HAS, France LBI@HTA, Austria
Partners Involved Associated Partners: AETS, Spain AETSA, Spain ASR, Italy AVALIA-t, Spain CAST, Denmark Cochrane Collaboration, United Kingdom CVZ, the Netherland DACEHTA, Denmark DAHTA@DIMDI, Germany iHIQA, Ireland IPHRS, Slovenia KCE, Belgium NOKC, Norway SBU, Sweden OSTEBA, Spain Regione Veneto, Italy UCSC, Italy University of Lübeck, Germany University of Tartu, Estonia Collaborating Partners: AHTAPol, Poland CEDIT, France European Observatory on Health Systems and Policies EuroScan ICTAHC, Israel OECD PHGEN, Germany SNHTA, Switzerland
Tasks Strand A: Models of Monitoring
• Provide overview of existing monitoring tools and technologies that are currently assessed with these tools.
• Build typology of tools used in technology assessment.
Strand B: Policy relevant information service on high volume, costly, rapidly developing, emerging technology.
• Develop structured information service on high volume technologies.
• Establish common criteria to determine which technologies should be the target for specific monitoring.
• Focus the information network on a limited number of technologies that represent a challenge for decision makers.
• Develop a procedure for prioritisation of topics. Current Status on Milestones and Deliverables
M12 (December 2006) Milestone: Overview on existing monitoring tools - completed. A full document with annexes is available. It will undergo revision in the first half of 2007 before publication.
Additional Outcomes/Activities
• Common definition of a monitoring system.
• Document (annex) on how new technologies are introduced in
37

the country of each WP7 partner.
• List of technologies for which partners would be interested in sharing existing data or in collecting new data.
9.2 Tasks performed
9.2.1 Strand A The Lead Partners conducted a survey of European experience and a review of the literature to meet the target of the first milestone. The end-product was an overview of existing monitoring systems for new technologies (cf. Annex WP7.1) which was presented at the September 26 e-meeting (cf. Annex WP7.2) and further discussed at the November 14-15 workshop in Seville (cf. Annex WP7.3 and Annex WP7.4). Survey of European experience
• HAS and LBI@HTA designed a questionnaire which was tested by the 8 CPs, revised, and then sent out to the 17 APs of WP7, 8 CPs of WP7, 2 LPs, 8 EUnetHTA members not WP7 partners (Finland, Belgium, Iceland, Cyprus, Portugal, Latvia, Hungary, Lithuania) and to 3 countries not members of EUnetHTA (Czech Republic, Luxembourg and Slovak Republic). A total of 38 questionnaires were sent; the minimum expected response rate was 17/38 (17 from the APs).
• HAS and LBI@HTA shared the responsibility of obtaining completed questionnaires from partners. HAS analysed responses.
• The questionnaire included a general introduction and two parts, each corresponding to an aim of WP7: o General introduction: respondent identity and description of the local context for introducing
emerging/new health technologies. o Part 1: description of current monitoring systems and tools for emerging/new health technologies
in the country/region. o Part 2: proposals for common monitoring tools for a given emerging/new health technology in
Europe and for a case study to test the tools in 2007-08.
• A total of 27/38 answers were received (23/27 WP7 partners responded to the survey). The response rate was 100% for APs and LPs, and 50% for CPs. There were 4/11 responses from non-WP7 partners. Responses came from 1 international collaboration, 14 HTA agencies, institutes or units from 18 countries, 3 universities, and 2 official bodies.
Literature review
• HAS carried out a literature review focusing on studies describing monitoring systems for emerging/new health technologies in different countries. The lack of keywords and MESH-terms for searching electronic databases proved to be a problem. Relevant information tended to be found in books and in the internal documents of HTA agencies or other healthcare structures. Documentation was reviewed using a grid based on the items of the survey of European experience.
• Further information was sought by: – searching the Internet sites of official public bodies or institutions (HTA agencies, health ministries,
regulatory bodies) for the United States, Canada and Australia; – contacting key people with experience in relevant monitoring systems.
o Professor Guy J. Maddern, Surgical Director ASERNIP-S, Royal Australasian College of Surgeons (for his experience in registers);
o Dr Leslie Levin, head, Senior Medical Adviser, Canada (for his knowledge on conditional coverage in the United States, Canada and Australia).
• Overall, 16 articles and 3 internet websites describing monitoring systems for emerging/new health technologies were selected for citation in the overview.
E-meeting, September 26, 2006
Two main issues were raised during the e-meeting (see Annex WP7.3): - How are strands A and B articulated? What is the position of strand A in relation to Euroscan? Monitoring (strand A)
concerns which stage in the life cycle of a health technology? - What are the concrete objectives of strand A in 2007 (main objective: “development and implementation of
shared monitoring tools”). Both these issues were further discussed at the Seville workshop.
38
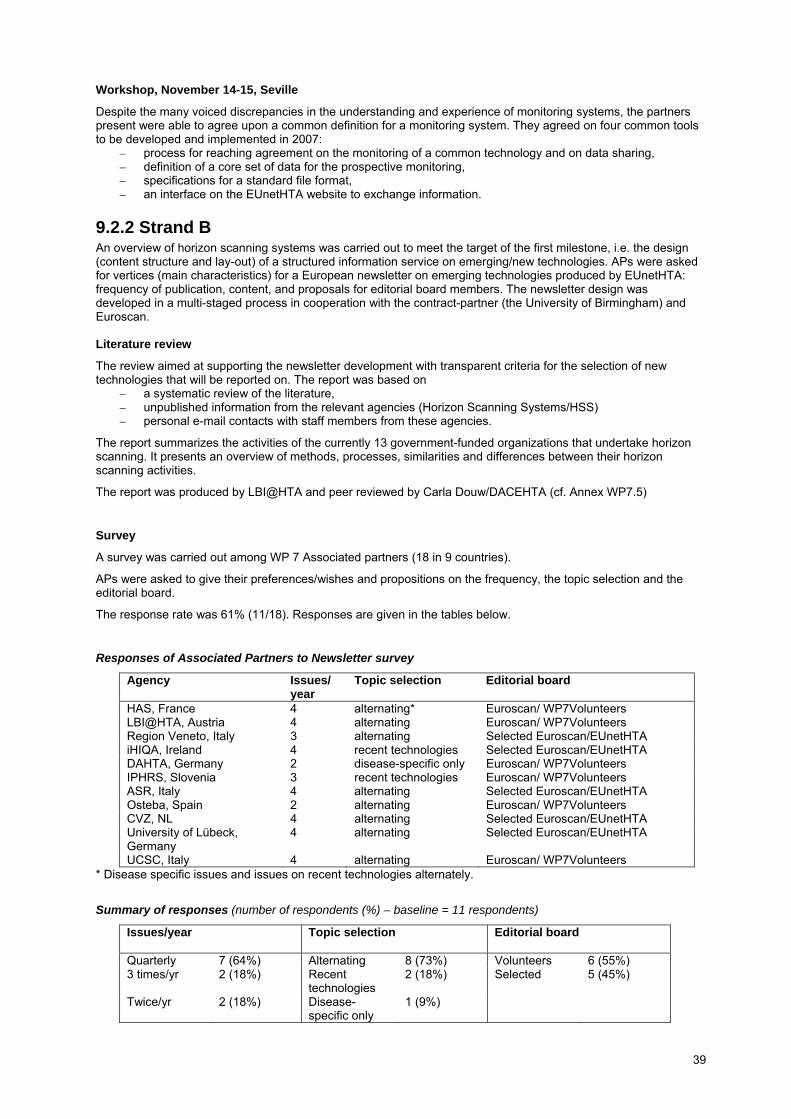
Workshop, November 14-15, Seville
Despite the many voiced discrepancies in the understanding and experience of monitoring systems, the partners present were able to agree upon a common definition for a monitoring system. They agreed on four common tools to be developed and implemented in 2007:
– process for reaching agreement on the monitoring of a common technology and on data sharing, – definition of a core set of data for the prospective monitoring, – specifications for a standard file format, – an interface on the EUnetHTA website to exchange information.
9.2.2 Strand B An overview of horizon scanning systems was carried out to meet the target of the first milestone, i.e. the design (content structure and lay-out) of a structured information service on emerging/new technologies. APs were asked for vertices (main characteristics) for a European newsletter on emerging technologies produced by EUnetHTA: frequency of publication, content, and proposals for editorial board members. The newsletter design was developed in a multi-staged process in cooperation with the contract-partner (the University of Birmingham) and Euroscan. Literature review
The review aimed at supporting the newsletter development with transparent criteria for the selection of new technologies that will be reported on. The report was based on
– a systematic review of the literature, – unpublished information from the relevant agencies (Horizon Scanning Systems/HSS) – personal e-mail contacts with staff members from these agencies.
The report summarizes the activities of the currently 13 government-funded organizations that undertake horizon scanning. It presents an overview of methods, processes, similarities and differences between their horizon scanning activities.
The report was produced by LBI@HTA and peer reviewed by Carla Douw/DACEHTA (cf. Annex WP7.5)
Survey
A survey was carried out among WP 7 Associated partners (18 in 9 countries).
APs were asked to give their preferences/wishes and propositions on the frequency, the topic selection and the editorial board.
The response rate was 61% (11/18). Responses are given in the tables below.
Responses of Associated Partners to Newsletter survey
Agency Issues/ year
Topic selection Editorial board
HAS, France 4 alternating* Euroscan/ WP7Volunteers LBI@HTA, Austria 4 alternating Euroscan/ WP7Volunteers Region Veneto, Italy 3 alternating Selected Euroscan/EUnetHTA iHIQA, Ireland 4 recent technologies Selected Euroscan/EUnetHTA DAHTA, Germany 2 disease-specific only Euroscan/ WP7Volunteers IPHRS, Slovenia 3 recent technologies Euroscan/ WP7Volunteers ASR, Italy 4 alternating Selected Euroscan/EUnetHTA Osteba, Spain 2 alternating Euroscan/ WP7Volunteers CVZ, NL 4 alternating Selected Euroscan/EUnetHTA University of Lübeck, Germany
4 alternating Selected Euroscan/EUnetHTA
UCSC, Italy 4 alternating Euroscan/ WP7Volunteers * Disease specific issues and issues on recent technologies alternately.
Summary of responses (number of respondents (%) – baseline = 11 respondents)
Issues/year
Topic selection Editorial board
Quarterly 7 (64%) Alternating 8 (73%) Volunteers 6 (55%) 3 times/yr 2 (18%) Recent
technologies 2 (18%) Selected 5 (45%)
Twice/yr 2 (18%) Disease-specific only
1 (9%)
39

Design of structured information service on emerging/new technologies
The WP7 lead partners met the contract-partners (University of Birmingham, Euroscan) on June 19 in Paris to discuss newsletter design and production. They drafted an agreement together on content, format, scope, the target audience, information gathering and selection process, the editorial board, and editorial control. WP2 (Susanna Allgurin-Neikter/SBU) developed a design for the newsletter.
9.3 Work plan for the next period (2007)
The milestones and deliverables of the WP7 work programme remain as agreed.
9.3.1 Strand A The work plan for January – May 2007 is modified in line with the conclusions of the first WP7 workshop. This is a deviation from the work programme outlined in the proposal.
Four groups will be constituted and each will be allocated a tool to develop: – January: allocation of tools to be developed to each of the four groups – March: e-meeting of each individual group to discuss development of these tools – April 12–13 (WP 7 workshop, Dublin, Ireland): submission of tools developed by the groups to all WP7
partners for comment and validation As planned in the programme outlined in the proposal: – the second half of 2007 will be devoted to the implementation of the tools and the identification of
performance indicators, – 2008 will be devoted to the evaluation of the tools.
9.3.2 Strand B January - March: Finalise formatting and design, develop criteria for prioritising technologies, develop electronic priority setting instrument, approach and set members for prioritisation and editorial board, identify, prioritize etc. production and distribution. April: Discussion of newsletter at WP7 workshop in Dublin.
40

10 Work Package 8: Systems to support HTA in MS with limited institutionalisation of HTA
10.1 Overview Work Package 8 Systems to support HTA in MS with limited institutionalisation of HTA Lead Partner (LP)
CAHTA, Spain
Partners Involved Associated Partners: AETS, Spain AVALIA-t, Spain CAST, Denmark Cochrane Collaboration, United Kingdom HunHTA, Hungary IPHRS, Slovenia MoH Cyprus NOKC, Norway UCSC, Italy University of Tartu, Estonia VSMTA, Latvia Collaborating Partners: AHTAPol, Poland CEESTAHC, Poland Council of Europe. Directorate General III Social Cohesion European Observatory on Health Systems and Policies EuroScan German HTA Association, Germany Hauptverband der Österreichischen, Austria HTAi Secretariat, IQWIG, Germany INAHTA Secretariat Institute of Molecular Medicine, Portugal PHGEN, Germany SNHTA, Switzerland University of Iceland, Iceland WHO - HEN
Tasks 1. To define minimum components related to the scope, structure, process and visibility of an HTA organisation
• Main characteristics of the specific setting defining different scopes and models of HTA organisations
• Key components within the scope of a new HTA organisation • The essential elements defining an HTA organisation, eg.
Structure, background professional profile, infrastructure resources, funding.
• Key aspects of organisational visibility 2. To develop tools for education support to institutions or healthcare systems in the process of evolving to/building HTA capacity and institutionalisation
3. To produce a handbook on building HTA capacity and institutionalisation
Current Status on Milestones and Deliverables
M6 (June 2006) Milestone: HTA organisation characteristics review – completed (cf. Annex WP8.1) M15(March 2007) Milestone: Report from survey of HTA user need. (cf.
41
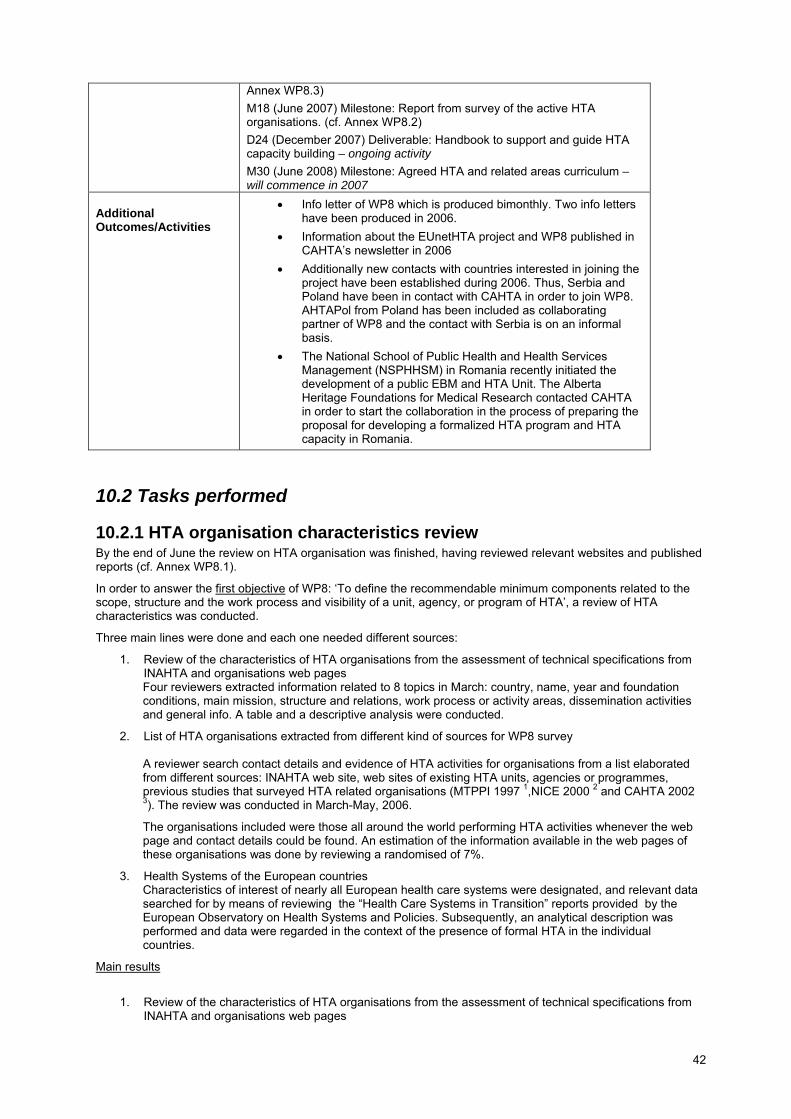
Annex WP8.3) M18 (June 2007) Milestone: Report from survey of the active HTA organisations. (cf. Annex WP8.2) D24 (December 2007) Deliverable: Handbook to support and guide HTA capacity building – ongoing activity M30 (June 2008) Milestone: Agreed HTA and related areas curriculum – will commence in 2007
Additional Outcomes/Activities
• Info letter of WP8 which is produced bimonthly. Two info letters have been produced in 2006.
• Information about the EUnetHTA project and WP8 published in CAHTA’s newsletter in 2006
• Additionally new contacts with countries interested in joining the project have been established during 2006. Thus, Serbia and Poland have been in contact with CAHTA in order to join WP8. AHTAPol from Poland has been included as collaborating partner of WP8 and the contact with Serbia is on an informal basis.
• The National School of Public Health and Health Services Management (NSPHHSM) in Romania recently initiated the development of a public EBM and HTA Unit. The Alberta Heritage Foundations for Medical Research contacted CAHTA in order to start the collaboration in the process of preparing the proposal for developing a formalized HTA program and HTA capacity in Romania.
10.2 Tasks performed
10.2.1 HTA organisation characteristics review By the end of June the review on HTA organisation was finished, having reviewed relevant websites and published reports (cf. Annex WP8.1).
In order to answer the first objective of WP8: ‘To define the recommendable minimum components related to the scope, structure and the work process and visibility of a unit, agency, or program of HTA’, a review of HTA characteristics was conducted.
Three main lines were done and each one needed different sources:
1. Review of the characteristics of HTA organisations from the assessment of technical specifications from INAHTA and organisations web pages Four reviewers extracted information related to 8 topics in March: country, name, year and foundation conditions, main mission, structure and relations, work process or activity areas, dissemination activities and general info. A table and a descriptive analysis were conducted.
2. List of HTA organisations extracted from different kind of sources for WP8 survey
A reviewer search contact details and evidence of HTA activities for organisations from a list elaborated from different sources: INAHTA web site, web sites of existing HTA units, agencies or programmes, previous studies that surveyed HTA related organisations (MTPPI 1997 1,NICE 2000 2 and CAHTA 2002 3). The review was conducted in March-May, 2006.
The organisations included were those all around the world performing HTA activities whenever the web page and contact details could be found. An estimation of the information available in the web pages of these organisations was done by reviewing a randomised of 7%.
3. Health Systems of the European countries Characteristics of interest of nearly all European health care systems were designated, and relevant data searched for by means of reviewing the “Health Care Systems in Transition” reports provided by the European Observatory on Health Systems and Policies. Subsequently, an analytical description was performed and data were regarded in the context of the presence of formal HTA in the individual countries.
Main results
1. Review of the characteristics of HTA organisations from the assessment of technical specifications from INAHTA and organisations web pages
42

Most of INAHTA organisations were established between 1994 and 1999, and under the auspices of the government. The main objectives for these organisations were to advise / assess policy makers or governments and to improve health services. The population served for them was mostly national. Most of the organisations informed about the development of systematic reviews and the most frequent dissemination strategies were their own web page and newsletters. There were great differences between organisations in relation to their structure, permanent staff, relations, consultants, and current HTA budget.
2. List of HTA organisations extracted from different kind of sources for the WP8 survey A preliminary list of 363 was elaborated merging information from different sources, 174 were eliminated because of different reasons: for 64 of them was not possible to find a web page, for 53 organisations were demonstrated they did not perform HTA, other 57 organisations were duplicated in different sources.
From the list of the 189 remaining organisations a randomised selection of 7% was done. In relation to the information topics, only contact details were found in almost all web pages, followed for establishment of the centre. Few organisations gave information about specific setting, aims and scope or structure. The topics which were less given were: work process and visibility of results.
3. Health Systems of the European countries: • Formal HTA is in place in 15 countries in Europe (from 37 countries considered). 13 countries with formal
HTA are members of the European Union. • Three countries of the Eastern and Central part of Europe introduced formal HTA. • Among those without formal HTA several have expressed their interest in the introduction of HTA and
sought for support. are several countries have commenced uncoordinated HTA activities • The health care systems of numerous countries are in enormous structural transition especially those in
the Eastern and Central part of Europe after the abolishment of the Semashko system.
As main conclusions:
There was a big variety in the information about the characteristics given by the organisations which makes difficult to establish comparison among them.
Information related to the work process, visibility of results, structure, scope and background of the organisations is not available in most of the web pages which have been reviewed
As a consequence of this, a survey is needed to obtain information from these topics in depth and in a comparable way.
There is a enormous need to promote the establishment of HTA across Europe since among 37 European countries that were considered in this study, formal HTA is in place in only about 40 % (15 countries) whereas the majority of them are EU member states (13 countries).
Particular support with respect to the introduction of formal HTA should be dedicated to Eastern and Central part of Europe as not more then three countries have introduced formal HTA..
The presence of formal HTA is neither associated with the health care services being financed predominantly through taxation nor by social insurance contributions. Both models are practically equally distributed among countries with formal HTA in place.
10.2.2 Survey on HTA organisations (cf. Annex WP8.2) A cross-sectional survey by means of a semi-structured questionnaire was conducted in order to achieve the above mentioned first objective of WP8.
The methodology took into account 2 main steps:
For the questionnaire design the following activities were planned: (Constitution of the working group of
experts (HTA, Information and documentation, and elaboration of surveys) and permanent review of questionnaire drafts; suggestions from the review of characteristics of HTA organisations (review report); review of surveys to HTA organisations of previous studies; pilot test survey to associated and collaborative partners of WP8 and the elaboration of the definitive version of WP8 survey). The design of the questionnaire was conducted in May-September, 2006.
The sampling procedure was based on a list elaborated from different sources: INAHTA, and the list of
participants of previous studies that have done surveys in the past. Specifically:
− − − −
−
EUnetHTA partners INAHTA (International Network of Agencies for HTA) website Websites of existing HTA units, agencies or programmes Report on overview of the implementation of activities related to evidence based practice in a broad representation of world health organization-collaborating centres, a survey conducted by the CAHTA (Catalan Agency for Health Technology Assessment and Research) in 2002 3 Project report on review of International Health Technology Assessment (IHTA). National Institute for Clinical Excellence 2000. 1
43

− The status of health technology assessment worldwide. Results of an international Survey. MTPPI 1997. 2
The inclusion criteria for the identified organisations, any HTA organisation performing HTA all around the world whenever their web page and contact details could be found. The search period for the previous sources was March-May 2006.
As main results:
The previous draft of the questionnaire identified 6 sections: Identification and establishment of the organisation, specific setting, aims and scope, structure, work process and visibility of results.
After the reviewing process by the working group of experts a final draft of the questionnaire with 47 questions was sent to 26 collaborative or associated partners of WP8 in a pilot test in August.
After e-mail and telephone reminders 61,5% of the organisations answered the questionnaire Fifteen comments or suggestions from this pilot test were introduced in the final questionnaire . The definitive questionnaire was sent to 126 organisations all around the world in November 2006. On
December 2006 13 organisations answered the questionnaire. A personal telephone reminder is planned to be done in January 2007.
10.2.3 Survey information needs A survey (cf. Annex WP8.3) to be answered for those HTA agencies/units which have been successful or try to be successful with the implementation of an information management policy and aimed at gathering data on their trained personnel, information resources, skills and competences in order to detect the information needs.
The survey on information needs will be sent in January 2007 in order to prepare the milestone (M15) for next year 2007
10.2.4 Adherence to the work plan during the reporting period. The objectives and tasks of WP8 which were planned to be done during this first year of the EUnetHTA project have been successful achieved. The adherence to the work plan during this firs period has been reached, not only the first milestone (M6) on this review on HTA organisations was finished in June but there were also other activities and tasks which were set up in 2006 (such as these surveys on HTA organisations and information needs and the WP8 info letter).
WP8 workplan 2006 (January 2006-December 2006)
Activities 1 2 3 4 5 6 7 8 9 10 11 12 Objective 1
Review HTA organizations
M
Survey HTA organizations
Report HTA organizations
Workshop (Slovenia) Handbook HTA organizat
Objective 2 Survey information needs
Compilation HTA Curricula
White Paper
M: milestone
10.2.5 Communication with WP partners (e-meetings, workshops..) The first e-meeting of WP8 was on 20th December in order to talk about the workgroup proposal for the workshop in Slovenia (cf. Annex WP8.4). The proposal was to divide the partners attending the workshop into some different
44

working groups according to the five main topics which were defined in the survey on HTA organisations. Few associated partners attended the e-meeting (cf. Annex WP8.5) and most of them agreed in the proposal. Additionally internal EUnetHTA meetings at CAHTA are scheduled monthly and the contact with the associated and collaborating partners of WP8 is mainly by email.
BIBLIOGRAPHY 1 Perry S, Gardner E, Thamer M. The status of health technology assessment worldwide. Results of an
international survey. Int J Technol Assess Health Care. 1997;13(1):81-98.
2 Mears R, Taylor R, Littlejohns P. Dillon A. Review of International Health Technology Assessment (IHTA). Project Report. London: National Institute for Clinical Excellence (NICE); 2000. Report no.:
3 Estrada MD, Serra-Sutton V. Rajmil L. Overview of the implementation of the health technology assessment activities in a broad representatio of world health organisation-collaborating centres [consulta técnica]. Barcelona: Agència d'Avaluació de Tecnologia i Recerca Mèdiques.Servei Català de la Salut.Departament de Sanitat i Seguretat Social.Generalitat de Catalunya; 20012. Report no.:
10.3 Work plan for the next period (2007) Based on the achievements up to December 2006, the next steps and major activities planned for next year 2007 will be the following ones:
1. Survey HTA organisations. The survey on HTA organisations will be finished by March 2007 2. 1st Workshop (Slovenia). The first WP8 face-to-face meeting will be in March 5-6, 2007. The
workshop will be organized in working groups in order to discuss and comment the results of the survey on HTA organisations.
3. Report on HTA organisations. The report on HTA organisations will include the results of the
survey on HTA organisation and will be submitted in June 2007.
4. Handbook HTA organisations. The handbook on HTA organisation is the first deliverable of WP8 which will be submitted in December 2007. (D24)
5. Survey on information needs: The survey on HTA organisations will be finished by March 2007
6. Report on information needs: The report on HTA organisations will be finished in June 2007.
7. 2nd Workshop (Barcelona) The second WP8 face-to-face meeting will be in June 2007. Other activities in 2007 and ongoing in 2008: Compilation HTA Curricula. White paper Elaboration of a “White Paper“ to know how to manage efficiently scientific and technical information that will be reviewed and agreed by different HTA information specialists.
This White Paper will highlight key factors in managing information and knowledge efficiently. It will help to identify, retrieve and manage information and to assist the introduction of information and communication technologies.
45

Table 8.1 WP8 workplan 2006 (January 2007-December 2007)
Activities 12 13 14 15 16 17 18 19 20 21 22 23 24 Objective 1
Survey HTA organizations 1st Workshop (Slovenia) W Report on HTA organizations M Handbook HTA organizations D
Objective 2 Survey information needs Report on information needs M Compilation HTA Curricula 2nd Workshop (Barcelona) W White Paper
10.4 Additional material
10.4.1 WP8 info letter The info letter idea is to send the latest news, the work in progress and other related info of WP8 to the associated and collaborative partners of this WP. This info letter will be produced bimonthly and made available for downloading in the extranet. Until now two info letters have been produced (cf. Annex WP8.6)
10.4.2 Information about the EUnetHTA project and WP8 published in CAHTA’s newsletter in 2006 (cf. Annex WP8.7)
M: milestone W: workshop D: deliverable
46
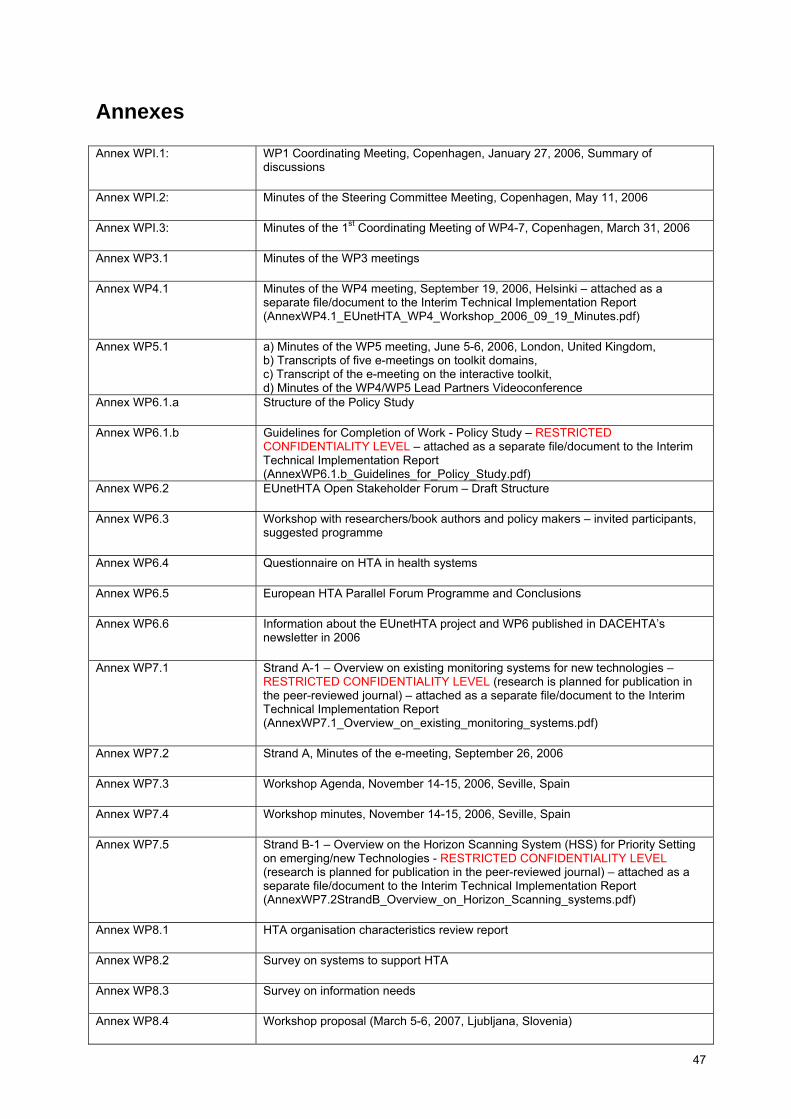
Annexes Annex WPI.1: WP1 Coordinating Meeting, Copenhagen, January 27, 2006, Summary of
discussions
Annex WPI.2: Minutes of the Steering Committee Meeting, Copenhagen, May 11, 2006
Annex WPI.3: Minutes of the 1st Coordinating Meeting of WP4-7, Copenhagen, March 31, 2006
Annex WP3.1 Minutes of the WP3 meetings
Annex WP4.1 Minutes of the WP4 meeting, September 19, 2006, Helsinki – attached as a separate file/document to the Interim Technical Implementation Report (AnnexWP4.1_EUnetHTA_WP4_Workshop_2006_09_19_Minutes.pdf)
Annex WP5.1 a) Minutes of the WP5 meeting, June 5-6, 2006, London, United Kingdom, b) Transcripts of five e-meetings on toolkit domains, c) Transcript of the e-meeting on the interactive toolkit, d) Minutes of the WP4/WP5 Lead Partners Videoconference
Annex WP6.1.a Structure of the Policy Study
Annex WP6.1.b Guidelines for Completion of Work - Policy Study – RESTRICTED CONFIDENTIALITY LEVEL – attached as a separate file/document to the Interim Technical Implementation Report (AnnexWP6.1.b_Guidelines_for_Policy_Study.pdf)
Annex WP6.2 EUnetHTA Open Stakeholder Forum – Draft Structure
Annex WP6.3 Workshop with researchers/book authors and policy makers – invited participants, suggested programme
Annex WP6.4 Questionnaire on HTA in health systems
Annex WP6.5 European HTA Parallel Forum Programme and Conclusions
Annex WP6.6 Information about the EUnetHTA project and WP6 published in DACEHTA’s newsletter in 2006
Annex WP7.1 Strand A-1 – Overview on existing monitoring systems for new technologies – RESTRICTED CONFIDENTIALITY LEVEL (research is planned for publication in the peer-reviewed journal) – attached as a separate file/document to the Interim Technical Implementation Report (AnnexWP7.1_Overview_on_existing_monitoring_systems.pdf)
Annex WP7.2 Strand A, Minutes of the e-meeting, September 26, 2006
Annex WP7.3 Workshop Agenda, November 14-15, 2006, Seville, Spain
Annex WP7.4 Workshop minutes, November 14-15, 2006, Seville, Spain
Annex WP7.5 Strand B-1 – Overview on the Horizon Scanning System (HSS) for Priority Setting on emerging/new Technologies - RESTRICTED CONFIDENTIALITY LEVEL (research is planned for publication in the peer-reviewed journal) – attached as a separate file/document to the Interim Technical Implementation Report (AnnexWP7.2StrandB_Overview_on_Horizon_Scanning_systems.pdf)
Annex WP8.1 HTA organisation characteristics review report
Annex WP8.2 Survey on systems to support HTA
Annex WP8.3 Survey on information needs
Annex WP8.4 Workshop proposal (March 5-6, 2007, Ljubljana, Slovenia)
47

Annex WP8.5 E-meeting report (December 20, 2006)
Annex WP8.6 WP8 Newsletter
Annex WP8.7 CAHTA Newsletter (EUnetHTA project presented)
48

Annex WPI.1 Work Package 1 Meeting January 27, 2006 8:30 – 16:00 DACEHTA, National Board of Health Tel +45 7222 7548 (secretary)
Participants
Prof. Nina Rehnqvist [email protected] Susanna Allgurin-Neikter [email protected]
SBU, Swedish Council on Technology Assessment in Health Care SWEDEN (Lead Partner WP2)
Dr. Alric Rüther [email protected] Dr. Hans-Peter Dauben [email protected]
DAHTA@DIMDI, German Agency for Health Technology Assessment at the German Institute for Medical Documentation and Information GERMANY (Co-Lead Partner, WP2)
Lise Lund-Håheim [email protected]
NOKC, Norwegian Knowledge Centre for the Health Services NORWAY (Lead Partner WP3)
Prof. Marjukka Mäkelä [email protected]
FinOHTA, Finnish Office for Health Technology Assessment FINLAND (Lead Partner, WP4)
Dr. Ruairidh Milne [email protected]
NCCHTA, National Coordinating Centre for Health Technology Assessment UK (Lead Partner, WP5)
Dr. Sun Hae Lee Robin [email protected]
HAS, French National Authority for Health FRANCE (Lead Partner WP7)
Dr. Claudia Wild [email protected]
ITA, HTA Unit of the Institute of Technology Assessment, Austrian Academy of Science AUSTRIA (Co-Lead Partner WP7)
Mireia Espallargues [email protected] Moharra [email protected]
CAHTA, Catalan Agency for Health Technology Assessment and Research SPAIN (Lead Partner WP8)
Christopher Künzli [email protected]
SNHTA, Swiss Network for Health Technology Assessment SWITZERLAND Collaborating Partner
Prof. Finn Børlum Kristensen [email protected] Camilla Palmhøj Nielsen [email protected] Niels Würgler Hansen [email protected] Staffan Stilven [email protected] Julia Chamova, [email protected]
DACEHTA, Danish Centre for Health Technology Assessment (Hosting the meeting) DENMARK Main Partner Lead Partner WP1, WP6
Agenda
1. Introduction 2. EUnetHTA organisation
49
a. Management structure b. Governance structure c. Financial mechanism
3. WP 2006 Work Plans presentations and discussions 4. EUnetHTA communication:
a. Policy and strategy (eg, publication rules), b. graphic profile/logotype, c. facilitation (members-only area and e-meetings arrangements)
5. Other issues a. Identifying key EUnetHTA stakeholders b. Involvement of the interested HTA organisations who are currently non-members of EUnetHTA
1. Introduction The overall project’s aim is a development of the operational, sustainable European HTA Network to inform health policy and decision-making in EU and member states. The idea behind the project is to develop and operate structures, frameworks and mechanisms that will be useful for policy makers at the EU and national policy level, ie the HTA user perspective has been the guiding principle in developing the project’s concrete work packages. The project is also aiming at developing stronger working relationships between the staff members of the European HTA institutions. Through the staffs’ engagement in the project’s work there is an expectation of developing a number of spin-off products useful in everyday HTA activities of the participating organisations. 2. EUnetHTA organisation
a. Management structure (Appendix 1)
The proposed management structure spans over the next 3 years of the project and is meant to facilitate an effective implementation of the project activities. The main role of the secretariat in the current structure is to support cooperation between partners during 2006-2008. The SOP of administration will become more detailed in the coming months. Developing the structure of the secretariat in DACEHTA will build on advice from APs.
b. Governance structure (Appendix 2)
Steering Committee should not go into details but decide on directions, should have sufficient information to enable them to promote the project and network to the “outside” world.
Lead partners should be able to make decisions, keep the Secretariat informed and when decisions have implication for other WPs the main partner and project leader should be involved in decision making. The role and functions of the Advisory group and its relationship to the Stakeholder will be clarified in the coming months. Advice will be sought from the DG Sanco and MoH representatives. The Role of the Forum is mainly to ensure close connection to stakeholders.
c. Financial structure (Appendix 3)
It was recommended to identify one person in each AP organisation who will be responsible for financials and will communicate directly with the project’s financial officer at DACEHTA, Staffan Stilvén ([email protected]). It was also recommended to keep copies of payments/receipts form the expenditure associated with the project.
3. WP 2006 Work Plans presentations and discussions The WPs Work Plans are available on line on the respective areas of the Members Only page of www.eunethta.net – please see for details.
WP1 plan Comments: The role of WP1 is to coordinate the work in the EUnetHTA project. Major activities in 2006 are to develop a SOP manual, a three year work plan, and effective communication routines.
WP2 Plan Comments: Conference in 2008 requires early lobbying efforts to attract attention and secure participation in the conference Structure/practicalities of the conference organisation will be taken care of by SBU
WP3 Plan Comments: • Evaluation of the project should not be a prospective evaluation study, since the impact of the project’s
results will be seen most likely in a few years after the implementation • Should not be a 360º evaluation
50
• A key focus for evaluating activities should be chosen for the project time frame of 3 years WP4 Plan Comments: Selection of topics being proposed for final selection will be done in collaboration with LPs in WP4,5,6 and 7. Final selection of topic will be done by APs in WP4. Besides effectiveness, WP4 plans to include cost modelling, organisational questions, ethical issues, equity, and social justice.
• Pharmaceuticals should not be discarded as possible topic for developing Core HTA for the
methodological, political and pragmatic reasons. • Intervention involving use of pharmaceuticals (eg, drug-eluting stents) can be a compromise solution • The choice of the topic will be influenced by the perspective taken and the decision making will be
influenced by the proposed governance structure in the project (might involve Executive Committee???)
WP5 Plan Questions to be clarified: • Adaptation of new ‘core’ or existing HTAs? - Both • Assessment or appraisal (by England and Wales Department of Health definitions)? – Not clear still, but
presumably focus on assessment – definitely not decisions or “guidance”, but definitely more than literature review
• HTAs to inform what kind of decision: regulatory, reimbursement, ‘informed choice’? - Reimbursement • ‘Evidence synthesis’ or new clinical research? – Evidence synthesis • Effectiveness, cost-effectiveness or what? – to be clarified with the WP partners
WP6 Plan Comments: • Policy analysis: screening cases should be included in the book
WP7 Plan: Comments: • Definition of emerging technologies (and the time-frame) should be clearly stated. Euroscan will be
involved in the work – issues of copyright and access to the proprietary information must be carefully discussed.
WP8 Plan: Comments: • 2 surveys, project-wide – must see ways of reducing the burden of survey-answering in the project (some
information is already available in other sources, eg, the ECHTA project report) • Analytical approach in WP8 work plan should be transferred to the practically applicable advice to new
HTA organisations • Needs of the users, ie, new HTA organisations should be secured in the WP working approach • Interviewing about challenges and difficulties in setting up HTA organisations would provide very valuable
info for new HTA organisationss
4 and 5. EUnetHTA communications and Other issues: The strategy for a sustainable European HTA network should be developed by the end of 2007. That would require support of the MoHs and other exterior involvement. EUnetHTA congress in 2008 should strengthen our position and produce a statement that would express support to form a sustainable network to be put in place without delay after the project is over. The preparation for the strategy development should start already now in considering how each organisation-partner in EUnetHTA, and especially LPs, can involve their MoH or relevant bodies. Balance in consideration should be placed toward the customer being the national health policy bodies , eg, MoH. However, the EUnetHTA partners’ staff should be also involved in the EUnetHTA project work to ensure an internal support for the project and EUnetHTA’s strategic direction. Issues:
• Surveys must be coordinated. Action: a WP calendar of surveys (who will be surveyed, when, deadline for response, purpose of the survey) Action: if the survey is intended for the whole of the project membership base, it should go through the Secretariat • Notify APs that the number of hours put into different WPs should be wisely distributed among the
packages as that will have budget implications • Results of the coordinating meeting between the Lead Partners in WP4,5,6,7 have implications for the
whole of EUnetHTA – report should be made available to all (deadline for first draft – April 10 (meeting will be held on March 31). WP2 would like to have this information reflected in the project brochure as well.
51
• WP3 should develop a list of requirements for information for their half-year reports and send these requirements to LPs.
• March 1 (10:00-11:00) and March 3 (14:30-15:30) (dates were adjusted after January 27 meeting) – e-
meeting facility tryout for LPs. Those unable to participate will have an opportunity later (date will be announced later).
• Publication rules and authorship issues: WP2 (under Nina Rehnqvist supervision) will develop a proposal.
• Presence at the conferences: template project poster should be developed (WP2), list of major
conferences where EUnetHTA should be presented (eg, Cochrane Colloquium, European health Association, ISPOR in Copenhagen (November)
• Logotype was approved. Slight adjustments can be made – Susanna Allgurin to implement
• E-meeting facilities: Secretariat to check how to handle possible security issues with firewalls in bigger
government organisations. Each participant must give his/her consent to being recorded during the sessions.
• EUnetHTA Forum aim should be clarified
• Criteria/policy for those non-EUnetHTA organisations who would like to join should be developed. Main
proposed criteria: public institutions, LPs should be consulted for their consent and willingness to accept the new member. Otherwise non-members can monitor the project progress through subscribing to EUnetHTA news updates.
• Partners are encouraged to publish articles promoting the project. It is useful to send copies to the
secretariat before publishing so that the secretariat can monitor publications (not control!) and advise on the publication sources those interested in learning more about EUnetHTA.
52

Annex WPI.2 EUnetHTA Steering Committee Meeting May 11, 2006 9:00 – 16:00
Copenhagen, Denmark
Meeting Summary Welcome Address and Introduction The Steering Committee members (Annex 1) were welcomed by Finn Børlum Kristensen (EUnetHTA Project Leader and Director of DACEHTA), John Erik Pedersen (Ministry of Health of Denmark), and Daniel Mann (DG SANCO, European Commission). A number of opportunities for EUnetHTA were mentioned during these addresses:
• the need to share the work between HTA-organisations rather than duplication of work • the need to show increased impact of HTA • the need to obtain synergies • the need to create tools for tailoring of reports • the need to create system support for countries without HTA experience • the need to create a financially sustainable cross-national network for HTA
The actions of Member States are becoming more interconnected than ever in the past. This is driven by many different factors, including movement of patients and professionals, the impact of Community law on health care, an increasingly shared culture creating common expectations, dissemination of new medical technologies and techniques, and the enlargement of the Union. Recent rulings from the European Court of Justice applying free movement rules to the health sector have added pressure for increased collaboration at European level and the Council recognised the need to strengthen cooperation on patient mobility and healthcare in its Conclusions of June 2002. A report in 2003 following the high level reflection process on patient mobility recognised the potential value of European cooperation in helping Member States to achieve their health objectives and the primary mechanism for taking work in this area was to establish a High Level Group on health services and medical care. The High Level Group included a Working Group on HTA which met twice to progress on establishing a network on health technology assessment as requested by the Council in 2003. The group found that health technology assessments are currently being done in many EU Member States on the same topics with an obvious overlap in activities. For example, more than ten countries have produced their own HTA reports on breast cancer screening. Similar research questions are often brought forward in different Member States at the same time. This calls for European wide collaboration. Prioritisation of the project promoting the cross-border cooperation, interconnectedness and sharing of culture and techniques underpinned by the development of the supporting practical tools were mentioned as the focus of the European Commission’s efforts in the healthcare field. Effective exchange of information leading to more useful HTA and raising common standards was acknowledged by the speakers as the leading objectives for the project. EUnetHTA project organisation – adoption of the SOP Manual Concerning the publication guidelines it was underlined that we are leaning on the Vancouver guidelines (http://www.icmje.org). It was questioned whether we need to acknowledge the EU in the way it was suggested in the presentation. Often it is only needed refer to the grant number. It was stressed that we need to make sure that the EU is not made responsible for our publications; however we can do it in small letters. The issue of conflict of interest was brought up. What is the standard for the major publications? One way is for the partners to declare conflict of interest every year; another is for authors to sign a form. It was stated that we should delegate the responsibility for overseeing this to the partners, and the partners should use the common standards from the leading medical journals. It was suggested that the SOP was adjusted when we write “authors for EUnetHTA” so that it includes a demand for a footnote stating that the content does not necessarily reflect the
53

opinion of the whole group. It was stressed that the coordinating secretariat should be sent a copy of all publications - preferably with an English abstract (at least a title in English should be always made available). It was suggested to develop a disclaimer stating that the publication by the members of EUnetHTA reflect the views of the authors and not of the project. Such a disclaimer will be used where appropriate and not universally. Following the discussion of the publications rules it was stressed that EUnetHTA is not primarily a research project. There will be intellectual contributions, but we should be aware not to think about publications first. Daniel Mann stressed that the question of ownership for the commission is only relevant in relation to final deliveries.
Concerning the suggested establishment of an Advisory Group it was expressed that the EU commission is a key actor. We should involve Ministries of Health, as we need their advice, however, we also need independence.
There will be posted a general presentation of EUnetHTA on the website. If any of the partners translate the presentation into their own language, it can be put on the EUnetHTA website too. The SOP manual was adopted. Suggested adjustments will be reflected in the final version which will be available on the Members only after the Steering Committee summary report is approved. EUnetHTA 3-year work plan The work plans were presented by the work package leaders. Specifically WP4 members identified the first core topic for development of the core model and framework – drug-eluting stents; the development and validation process will be done in dialogue and involvement of the WP4 members, the first workshop will be held in Helsinki on September 19, during the Finnish Presidency of the European Union. WP5 will hold its first WP meeting on June 5 in London to define common understanding of concepts; the main goal of developing a common adaptation terms glossary and toolkit is to reduce duplication in individual HTA agencies, promote efficiencies and spend less time searching databases, but instead work with informing policy making. Glossary will help make explicit how the terminology is used in different agencies. The work plan presentations generated a number of comments
• We need to be aware that the Ministries of Health are not necessarily the most important stakeholders in all countries. In the social security countries the health insurance bodies play a far bigger role.
• In relation to WP 5 it is important to be aware that in the area of guideline development there have been developed tools for adaptation. We are obliged to build on this work, but we should also be aware that adaptation of guidelines is not the same as adaptation of HTA.
• In relation to the work of WP 8 it could be useful to pair old and new HTA-organisations. Different stages of HTA organisation development should be taken into account when suggesting support tools. The newly established Agency for HTA in Poland (AHTAPol) offered to be a “pilot agency” where tools developed in WP8 could be applied.
• Concerning the planning and management it was asked whether it is possible to include ongoing initiatives from the partners in the work of e.g. WP 6. It was agreed that it is invited to include as many already ongoing initiatives in the promotion of EUnetHTA as possible.
• The changed title of WP 8 was discussed - what do we mean by limited resources and institutionalisation? • It was suggested that WP 1 coordinates the many questionnaires with overlapping issues so that we do
not spam people with overlapping questions. It was also suggested that we use telephone interview to get the information instead of just sending out questionnaires.
• Finally the importance of involving and informing the staff in the partner organisations – also those not directly involved in working in EUnetHTA – was stressed. It was suggested to arrange seminars in every partner organisation at the end of the project.
The 3-year work plan was endorsed.
Development of the sustainable European HTA Network (I+II) The discussions were introduced with a SWOT exercise performed by the Steering Committee members in pairs during the meeting (Annex 2). The results of the exercise will provide a starting point for the SWOT analysis to be done in WP6.
Communication of intermediate and final project results It was stressed that for the sustainability of the network and lobbying efforts it is important to inform about and involve the staff members of the participating organisations in the EUnetHTA work. Briefings about the project have been done in the majority of the participating organisations. The newsletter should be used to communicate progress of the project and to broadcast achievements/successes of EUnetHTA. Another suggestion is to develop a catchy phrase succinctly communicating the key message behind EUnetHTA to create awareness of EUnetHTA and promote our mission. It was expressed that we do not have a real message yet – it was suggested for the WP leaders to write a baseline article.
Another way of handling the communication strategy is to direct it towards citizens with special attention to societal subjects and democracy. More partners agreed that we should be more focused on the general public than on academics. There was a general agreement on the need to develop a communication strategy.
54

Stakeholder involvement EUnetHTA has come to being as a response to the demand expressed by the external parties (High Level Group/Ministries of Health, Commission) and therefore is highly client-oriented. It has many clients with many different interests. The types of involvement with different parties needs to be identified.. At the same time we need to be aware of competing or conflicting interests that may exist among the stakeholders. We need to develop different products to satisfy different stakeholders. The primary goal of our efforts in developing relationships with stakeholders is to facilitate sustainability beyond 3-year project time frame.
A central question is whether we see ourselves as a neutral platform or as a stakeholder. We need to be aware of the different kinds of partners – government funded organisations, university units etc. It is difficult to see ourselves as neutral brokers. The Stakeholder analysis (WP6 task) will help us navigate.
EUnetHTA is promoting a collective interest in furthering HTA as such and thus have a societal perspective, however, the core group of EUnetHTA is HTA doers with their own set of interests that should be facilitated. Such facilitation will not be sustainable in the long term without developing working relationships with other stakeholders in the HTA process.
HTA can be used at a societal level, an institutional level, and an individual level. It could be useful for each WP to reflect on which stakeholder groups that should be approached. It was agreed that individual members should take initiative to inform relevant and important (from the sustainability of the network point of view) stakeholders in their respective countries on the EUnetHTA objectives and progress. The Secretariat can facilitate but not substitute this work in the ways that are suitable in a particular situation. Collaboration with international organisations in the field of HTA We have to develop a clear EUnetHTA identity, acknowledge where others are better than we are, and develop cooperation in between. It is crucial that we are clear about our aims and strategies and know the aims and strategies of other international organisations.
It is important to focus on the starting point – securing long-term sustainability for our network. EUnetHTA strategic objectives and actions are to align with the demands, needs and possible funding sources for long-term activities of the network. That will determine our freedom in relation to the other organisations.
Structure of a future network To develop a structure, a core identity of the network should be identified and promoted. It was proposed to develop a form that will follow the function of the structure. The function is in turn determined by the level of stakeholders’ commitment and availability of resources to perform certain functions. A win-win situation for participants should be created, ie “getting out more than invested”.
It is important to stress the difference between EUnetHTA and INAHTA – there are large differences in work programmes. EUnetHTA could not be seen as a European branch of INAHTA, since EUnetHTA has been created as a response to an explicit demand from the European Commission and Ministries of Health to create a more effective European HTA network. A sustainable secretariat for the network is needed - it does not work with a volunteer basis. Thinking sustainability – we should extrapolate development (EU 2010). It is not enough with voluntary sharing. We need to develop real European products – also to match the industry that is organised at a European level. The network should provide an added value with its existence, eg, developing links with other European bodies (EMEA, DG Sanco, DG Enterprise, industry groups). True information sharing goes beyond sharing the final reports – other sources of information and data should be effectively exchanged within the network. Work on raising standards is important in this context as well as a possible procedure of mutual recognition based on eg, Core HTA model and framework.
The version presented was an alternative with a loose structure, the alternative with a more rigid structure would be an EU agency. The current alternative should be developed into a truly influential and structured approach to creating a sustainable network structure with common decision-making approaches, eg, core group of national/regional HTA agencies sharing the core HTA work that is consequently adapted to national/regional setting. One solution is for each HTA-organisation to set aside money for doing a number of core HTAs decided by the network. A clearinghouse would require extra funds. A mechanism for the topic selection and work distribution mechanism should be thought through. The arguments for setting aside national funds for the European network activities can include a necessity to produce a core HTA in English and to keep up the HTA methodology throughout Europe. A mechanism for outsourcing production of the systematic reviews and core HTAs can be also explored. Industry and other stakeholders could contribute valuable information, and perhaps provide some resources. Therefore it is important to involve them in the mechanism development in early stages.
55

The project has an obligation to deliver a practical solution in 3 years to those who expressed the need to put this network in place. Such a solution would require a strong commitment from all partners, especially the Associated Partners, as well as strategic approach to involving stakeholder groups and early solicitation of continuous support and involvement from the Ministries of Health and public health insurance bodies.
56

Annex 1 Main Partner / Coordinating Secretariat (Steering Committee member)
Member E-mail Organisation Country Work Package Affiliation
Finn Børlum Kristensen [email protected] DACEHTA Denmark
WP 1, 2, 4, 5, 6, 7
Julia Chamova [email protected]: +45 40 62 93 57
Niels Würgler Hansen
Camilla Palmhøj Nielsen
Karin Engel Rasmussen
Louise Hansen
Invited Speakers: Mr. John Erik Pedersen, Ministry of Health of Denmark Mr. Daniel Mann, Health Information Unit C2, SANCO - Health and Consumer Protection, European Commission Associated Partners (Steering Committee members)
Member E-mail Organisation Country Work Package Affiliation
Setefilla Luengo
AETS
Spain
WP 3, 6, 7, 8,
Eduardo Briones
AETSA
Spain
WP 4, 5, 7
Alessandro Liberati
ASR (Agenzia Sanitaria Regionale of Emilia Romagna)
Italy
WP 2, 3, 5, 7
Joan MV Pons
CAHTA (Catalan Agency for Health Technology Assessment and Research)
Spain
WP 1, 2, 8
Jan Sørensen
CAST (Center for Anvendt
Denmark WP 6, 8
57

Sundheds-tjeneste-forskning og Teknologi-vurdering)
Asbjørn Hrobjartsson
[email protected] Cochrane Collaboration
United Kingdom WP 2-8
Albert Boer
CVZ (College voor zorgverzekeringen)
The Netherlands
WP 6, 7
Alric Ruether
DAHTA@DIMDI (German Agency for Health Technology Assessment)
Germany
WP 1, 2, 3, 5, 6, 7
Henrik Hauschildt Juhl
DSI (Danish Institute for Health Services Research)
Denmark WP 4, 5, 6
Marjukka Mäkelä
FinOHTA/ STAKES Finland
WP 1, 4, 5, 6
Teresa Cerdá Mota
Galician Agency for Health Technology Assessment
Spain WP 4, 6, 8
Sun Hae Lee Robin
HAS (HAS - Haute Autorité de santé/ French National Authority for Health
France WP 1, 2, 5, 7
Michael Barry
iHIQA (Interim Health Information and Quality Authority)
Ireland WP 6, 7
Dagmar Lühmann
Institute for Social Medicine, University of Lübeck
Germany WP 4, 7
Eva Turk
[email protected] / [email protected]
Institute of Public Health
Slovenia WP 5,6,7,8
Claudia Wild
LBI@HTA Ludwig Boltzmann
Austria WP 1, 5, 7
58

Institute of Health Technology Assessment
Dirk Ramaekers
Dirk.Ramaekers@ kenniscentrum.fgov.be
KCE (Belgian Health Care Knowledge Centre)
Belgium
WP 2, 4, 5, 6
Stelios Christofides
Ministry of Health Cyprus WP 2, 8
Ruairidh Milne
NCCHTA (National Coordinating Centre for HTA)
United Kingdom
WP 1, 4, 5, 6
Nieves Sobradillo Ruiz
OSTEBA (Basque Office for Health Technology Assessment)
Spain WP 4, 5, 7
Nina Rehnqvist
SBU (Swedish Council on Technology Assessment in Health Care)
Sweden
WP 1, 2, 3, 4, 7
Susanna Allgurin Neikter
SBU (Swedish Council on Technology Assessment in Health Care)
Sweden WP 1, 2, 3, 4, 7
Reinhard Busse
Technische Universität Berlin, Dept. of Health Care Management
Germany WP 4, 5, 6
Lise Lund Håheim
NOKC (Norwegian Knowledge Centre for the Health Services)
Norway
WP 1, 3, 4, 5, 6, 7, 8
Juan Antonio Blasco
UETS (Agencia Laín Entralgo )
Spain WP 2, 6
László Gulácsi
Unit of Health Technology Assessment
Hungary WP 2, 8
59

60
Americo Cicchetti [email protected]
Universita Cattolica Del Sacro Cuore
Italy
WP 4, 5, 6, 7, 8
Monica Steinbach
University of Bremen Germany
WP 6, 7
Kersti Meiesaar
[email protected] University of Tartu Estonia
WP 4, 5, 6, 7, 8
Ilaria Passarani
Veneto Region
Italy
WP 2, 3, 5, 7
Igors Trofimovs
VSMTA (Health Statistics and Medical Technologies State Agency)
Latvia WP 3, 8
Jetty Hoeksema
[email protected] ZonMw
The Netherlands
WP 4, 5
Associated Partners Not Present: Ministry of Health (Lithuania), Gezondheidsraad - Health Council (the Netherlands), Servicio Canario de la Salud (Spain) Collaborating Partners
Member E-mail Organisation Country Work Package Affiliation
Norbert Wilk [email protected]
Agency for Health Technology Assessment
Poland WP 2, 4, 5, 7, 8
Christoph Künzli
SNHTA (Swiss Network for Health Technology Assessment)
Switzerland WP 1, 3, 4, 5, 6, 7, 8

Annex 2 SWOT Exercise Secretariat Introduction Internal Factors
Strengths • HTA expertise/skills • >10 years of European networking experience • Practical tools/deliverables
Weaknessess • Changing regional/national agendas of members • Staff involvement • Resources
External Factors
Opportunities • HTA is a recognised priority for Member States/Commission • Single EU HTA network initiative in Europe • Possibility to form strategic alliances with other relevant
established and developing European initiatives (Cochrane, EuroScan, etc)
Threats • Changing political agendas (EU, national, regional) • Being N1 and only one – target for constant close scrutiny on all fronts…
Steering Committee: Results of the work in pairs Internal Factors
Strengths • Multidisciplinarity • Enthusiasm • Commitment • Focus on win-win situation • Diversity of cultures • Many partners • Ability to identify research gaps • Good structure/project management • Well-organised project • Orientation on a contact to stakeholders
Weaknessess • Different backgrounds leading to possible misunderstandings • Wide involvement of stakeholders – risk of conflict of interest • Diversity of cultures • Many partners • Turnover of staff • Language • May become too academic • GOBSAT • Balance between management rigidity and flexibility
External Factors
Opportunities • External demand for HTA • Implementation plan for partners • EU-harmonisation • Facilitating of more HTA production • Quality • Show power/influence of HTA • Positive capacity building • Higher impact of HTA
Threats • Industry lobbying • Competing stakeholder interests • Confidentiality/data protection issues threatening transparency efforts • Different legal framework • Overload of information • DG Enterprise
61

62
• Less duplication Individual contributions: Homework (contributions which were not already mentioned in pair work results) Internal Factors
Strengths • Partners from all EU countries (2) • Involvement of different stakeholders at diff. institutional
levels • Structured and commonly shared information – resistance
to pressure groups • Shared methodology
Weaknessess • Quality and methodology variance • Disparity of objectives in partners (2) • Different stages of development in participating HTA organisations •
External Factors
Opportunities • Increased visibility of HTA, eg for general public (2) • Cross-border coordination necessity • Harmonisation of health benefit and coverage packages • Alliance with hospital management – bringing HTA into
practice •
Threats • Consumer lobbyism, not always guided by rational choice • Losing quality through adaptation (non-English language reports are lost • Innovation pressure – being competitive • Changes in the role of HTA and its priority within health system • Possibility of misunderstanding of the Associated Partner roles • New regulatory bodies not considering HTA • Perception of EUnetHTA by stakeholders • Possible competition with other HTA organisations (HEN, INAHTA, etc) • Expectations of decision-makers – expectations management might prove difficult • Credibility of different organisations in the same context • Long-term financial viability
Annex WPI.3 Notes from Work Package 4-5-6-7 Meeting March 31, 2006, Copenhagen 9:00 – 16:00 DACEHTA, National Board of Health Tel +45 7222 7548 (secretary) Mob +45 29 43 53 65 (Camilla Palmhøj Nielsen) Participants: Ilona Autti-Rämö, Kristian Lampe, Pirjo Räsänen and Heidi Anttila (FinOHTA) Ruairidh Milne, Nick Hicks and Debbie Chase (NCCHTA) Sun Hae Lee Robin and Céline Moty Monnereau (HAS) Finn Børlum Kristensen, Julia Chamova, Niels Würgler Hansen and Camilla Palmhøj Nielsen (DACEHTA). Detailed 2006 Work Plan content presentations Please see PP-slides (WP 7 oral presentation) WP links and how to operationalise the coordination In general WP4-5 provides structure and tools for HTA reporting, while WP6-7 provides information on what is happening after the report has been made. Strand B of the WP7 will however develop facilities to give information at different times of an HTA: - before an HTA report is made: the horizon scanning system - after a report is made on new/emergent technology : preliminary conclusions - during the process of monitoring new/emergent technologies : news on the existing monitoring systems, preliminary results... WP6 will use the results coming out of WP4, 5 & 7. Issue for WP4 and 5 – how do we report HTA results and process in Europe? Information on the methods used need to be transparent and available. WP2 Clearinghouse prototype is looking at the technical tools that can facilitate the access to this information. After developing common HTA structure with core and framework there will be a transitional phase in HTA reporting. What is the value of using common HTA structure with core and framework ?
- WP4 should identify and point out the incentives for using Core HTA in HTA reporting. It was agreed to involve all LPs in the final topic selection for WP pilot studies (2nd round before Easter), April 12-28, final topic selection. It was agreed that the “framework” term relates to the context-specific issues in developing HTA report. “Core HTA” as a term relates to the issues independent of the context, which can be shared from one country/context to another. WP5 glossary will expose/illuminate major concepts related to adaptation issues. The users of glossary and adaptation toolkit will be the HTA agencies and their contributors. Finn will check the progress of working groups with the INAHTA glossary Applicability testing scheduled in both WP4 and WP5 should be closely coordinated by both WP Leaders. The aim of the applicability testing in WP4 is to validate the developed common HTA structure with core and framework, while applicability testing in WP5 will be testing the usability of the developed adaptation toolkit. However, the applicability testing process can be organized so that it includes testing of both WP4 and WP5 products simultaneously. This needs further consideration on how it can be practically organized. Idea: when agencies start developing Core HTAs there should be a facility (e.g., database) to store the already-developed “Core HTAs” (extranet)– should be shared with WP2 Clearinghouse prototype strand

Leader (DAHTA) How long should it take to use the toolkit?
- 1 week max, it should be a quick process of examining for adaptability. It is not a critical quality appraisal tool of each other’s reports, but critical appraisal of the information to identify information possible for adaptation in another setting.
Suggestion: we should avoid judgment terminology such as “quality assurance” since it can create confusion and rejection. WP6: Core HTA will be described in a chapter in the WP6 book – FinOHTA agreed to lead this. WP7, Strand A – objective is to develop a structure for a common monitoring tool collecting information on emerging new technologies and elaborate a prototype of the system that makes it feasible and useful to monitor emerging technologies on a EU level. WP 2 is relevant here and roles and relations to EuroScan should be clear. Strand B – web based information service on rapidly changing, high volume, etc technologies targeted at decision and policy makers. This service can include updates and information about the developments in Strand A. Editorial control of the content in the information service should be a part of the development activities in Strand B, since highly sensitive information can be presented and it can potentially have a great influence on the decision making on the national/regional level. Disclaimer should be put protecting the interests of EUnetHTA. How to show concrete results during EUnetHTA 3-year project period This is considered important and should be discussed at the Steering Committee meeting and later during the project. Discussion of stakeholder involvement in relation to WP 4-7 See PP-slide presentation from Sun Hae Lee Robin. When meeting with stakeholders (eg, industry representatives) in relation to EUnetHTA activities, the Executive will be informed. There is a need for stakeholder analysis from the perspective of each work package. This will be included in the work of WP6. Action points: Early June – e-meeting with the LPs in WP4-7 (possibly WP2 Clearinghouse strand).
64
Annex WP3.1
Minutes from WP3-meeting Date: 24.February 2006
9.00-16.00.
At: Norwegian Knowledge Centre for the Health Service (NOKC), Universitetsgaten 7, Oslo, Norway
AP Contact Persons present:
Igors Trofimovs, VSMTVA, Latvia Helena Dhlgren, SBU, Sweden Hans-Peter Dauben, DIMDI, Germany Berit Mørland, NOKC, Norway Lise Lund Håheim, NOKC, Norway; Project leader In addition: Morten Bjørklund, NOKC, Norway; assistant
AP Contact Persons not present:
Alric Rüther, DIMDI, Germany Alessandro Liberati, Cochrane and ASR, Italy José Maria Amate Blanco, AETS, Spain Giampetro Rupolo, Regione Veneto, Italy
CC of AP: Roberto Grilli, ASR, Italy Antonio Sarria-Santamera, AETS, Spain Jesús Gonzáles-Enriquez, AETS, Spain Inaki Imaz-Iglesia, AETS, Spain Carmen Bouza-Alvarez, AETS, Spain Carmen Garcia-Comin, AETS, Spain Constantino Gallo, Regione Veneto, Italy Ialria Passarani, Regione Veneto, Italy Nina Rehnqvist, SBU, Sweden Juliette Säwe, SBU, Sweden
CP Stephen Blamey, MSAC, Australia Iain Gillespie, OECD, France Marlène Laeubli, Swiss Network for Health Technology Assessment, Switzerland Christoph Künzli, Swiss Network for Health Technology Assessment, Switzerland
Agenda Welcome a) Brief presentation of participants. Helena, Igor and Hans-Peter were only external participants. Unfortunately, others could not come.
65

b) About evaluation Lise presented information on evaluation to start the discussion. The plan for the meeting was to start with the general plan of the evaluation before making detailed plans. Overall planning a) General plan of activities: What and when The main activity will be to get information through questionnaires. These will form the basis for five biannual reports. The last six months will not have a separate report. In this manner we hope to record the project progress and any changes during the project. The purpose of our reports was discussed in terms of the reports being only for internal audit or if they, in addition, should have a function of coaching the activity during the project development. We suggest that the reports serve both purposes. In this manner we hope our evaluation will give some useful guidance to us all during the process of establishing EUnetHTA. b) Content of activities It was decided to make one questionnaire to register activity in work packages that is to be sent to work package leaders and one asking about the participant experience of taking part in WP, Steering Committee, Executive Committee, Coordinating Secretariat and Advisory. The content of activities is of course open for discussion and group member comments and suggestions about how to best do the evaluation, will be collected and circulated for a discussion among group members. Only one more face-to-face meeting is budgeted. However, E-meetings will be organized and will allow us to discuss the activities in the project. All drafts will be sent as e-mail and be open for comments before we have E-meetings to finalize eg. questionnaires and reports. It is advisable to practice for the E-meeting, if you are not familiar with E-meetings, by taking a training session “First Course in Centra”. Information is found on EUnetHTA homepage. Detailed planning a) Making required questionnaires for evaluation The two questionnaires were discussed and developed. Copies are enclosed and are open for comments. The format you see them in know is an adjusted version by Lise. Time did not permit to find a suitable format in the meeting. However, the content is the one that was decided on in the meeting. Concern was raised in the meeting about differences regarding language, the way questions are asked and the usefulness of questions in view of different countries/cultures. There are differences in how one expresses oneself and members are encouraged to give suggestions for alternatives as seen necessary. Please read the questionnaires carefully and send comments to Lise. All comments will be included in a new version that will be returned for further comments. If we then are near an agreement, the final discussion will be in an E-meeting. b) Specific content of interim reports and final report
66

The interim reports and final report will be very much based on the results of the questionnaires, milestones and deliverables. No detailed planning was done at this meeting as time was running short. We suggest the reports are made available on the EunetHTA member homepage. c) Other issues. i) A 3-year work plan has to be ready by March 15th. ii) We need the final work plan from all work packages to get the reference points of the registration for our evaluation. iii) A EUnetHTA forum will be organized and we may wish to make a separate questionnaire to those participants. iv) Deadlines:
1. 12th March : Comments on 3-year work plan
2. 19th March: Comments on questionnaires and activity plan as in minutes Documents enclosed: Draft of questionnaires 1 and 2 Draft for 3-year work plan
Minutes from WP3-telephone meeting Date: 27.April 2006
13.45 – 15.45
At: Telephone meeting arranged by Norwegian Knowledge Centre for the Health Service (NOKC),
AP and CP Contact Persons present:
Igors Trofimovs, VSMTVA, Latvia Helena Dahlgren, SBU, Sweden Hans-Peter Dauben, DIMDI, Germany Alessandro Liberati, Cochrane and ASR, Italy Inaki Imaz-Iglesia, AETS, Spain Ilaria Passarani, Regione Veneto, Italy Marlène Laeubli, Swiss Network for Health Technology Assessment, Switzerland Antonio Sarria-Santamera, AETS, Spain Berit Mørland, NOKC, Norway Lise Lund Håheim, NOKC, Norway; Project leader
AP Contact Persons not present:
Alric Rüther, DIMDI, Germany José Maria Amate Blanco, AETS, Spain Gampietro Rupolo, Regione Veneto, Italy
67

CC of AP: Roberto Grilli, ASR, Italy Jesús Gonzáles-Enriquez, AETS, Spain Carmen Bouza-Alvarez, AETS, Spain Carmen Garcia-Comin, AETS, Spain Constantino Gallo, Regione Veneto, Italy Teresa Gasparetto, Regione Veneto, Italy Nina Rehnqvist, SBU, Sweden Juliette Säwe, SBU, Sweden
CP Stephen Blamey, MSAC, Australia Iain Gillespie, OECD, France Christoph Künzli, Swiss Network for Health Technology Assessment, Switzerland
Agenda 1) Discuss the content and outline of the questionnaires 1 and 2 for the evaluation. Questionnaire 1 on WP-leader information on work package progress was discussed first. The discussion concentrated on the format of this survey. The participants argued for a change from questionnaire to personal interviews by Lund Håheim structured according to questionnaire 1. They saw this as the most feasible approach to gain the interest and necessary response by busy WP-leaders. The interviews will be carried out biannually. The way the questionnaires are outlined opens for a wide approach to comments on the progress of the different work packages. From this information certain issues will emerge and be reported. With this approach it is possible that the first round of interviews can be considered as a pilot. This remains to be decided on when the results of the first round of interviews has been analyzed. Questionnaire 2 was then discussed. It will be sent to all participants taking part in the EUnetHTA project. This survey is to be repeated every year. The questionnaire was reviewed in detail. Main points were: The introduction must emphasize more clearly for whom and why the questionnaire is sent. The questions in the table on Challenges for the network were reorganized and made more specific. The answer option of Do not know was deleted. The questions on WP work were reconsidered by rephrasing, content altered or deleted. The questions on EUnetHTA were included. Lund Håheim shall modify the questions. The questionnaires will be adjusted according to the advice by the group and be returned for review by the group members. 2) 3-year work plan WP3 member participation during the project was raised. No decisions were made to work distribution at this moment. The members are free to now or later to flag their interest in certain tasks they would like to take part in and follow through the project period. 3) Other issues. No other issues were raised
68

Documents enclosed: Draft of questionnaires 1 and 2
Minutes from WP3-telephone meeting Date: October 9th 2006
14.00 – 14.30 (15.00)
At: Telephone meeting arranged by Norwegian Knowledge Centre for the Health Service (NOKC),
Present: Helena Dahlgren, SBU, Sweden
Lise Lund Håheim, NOKC, Norway; Project leader
Absent: Alric Rüther, DIMDI, Germany Marlène Laeubli, Swiss Network for Health Technology Assessment, Switzerland
Not able to attend or no response to invitation:
Igors Trofimovs, VSMTVA, Latvia José Maria Amate Blanco, AETS, Spain Gampietro Rupolo, Regione Veneto, Italy Alessandro Liberati, Cochrane and ASR, Italy Constantino Gallo, Regione Veneto, Italy Berit Mørland, NOKC, Norway Stephen Blamey, MSAC, Australia Iain Gillespie, OECD, France
Agenda 1) Results of the first round of WP-leader interviews No changes were put forward. It was suggested that this report is sent to all those being interviewed and to be presented at the WP1 E-meeting on November 8th. WP3-members are asked to comment to this issue as soon as possible. 2) Results of the first participant survey The format of the report was discussed. Helena and Lise will go through the text questions and categorize the answers. They have planned a telephone meeting for Tuesday October 17th to coordinate this work. The report is then distributed to the WP3-group for comments. The report is suggested to be put out on the EUnetHTA intranet.
69

Annex WP5.1 a) Notes from Work Package 5 Meeting June 5th and 6th, 2006 Melia White House Hotel Regents Park London
Participants Finn Børlum Kristensen, Camilla Palmhøj Nielsen (DACEHTA), Elena Berti (ASR), Eduardo Briones (AETSA), Bernard Burnand (IUMSP), Marina Cerbo (Italian HTA network), Mike Clarke (UK Cochrane Collaboration), Hans-Peter Dauben (DAHTA@DIMDI), Teresa Gasparetto (Region Veneto), Jessika van Kammen (ZonMw), Jakob Kjellberg (DSI), Sun Hae Lee Robin, Céline Moty Monnereau (HAS), Mark Leys (KCE), Julio López Bastida (Servicio Canario de la Salud), Marjukka Mäkelä (FinOHTA), Kersti Meiesaar (University of Tartu), Ruairidh Milne, Nick Hicks, Debbie Chase (NCCHTA), Rosa Rico (OSTEBA), Tobias Schulte in den Bäumen (PHGEN), Marcial Velasco Garrido (TU Berlin), Norbert Wilk, Jadwiga Czeczot (AHTAPol), Ingrid Zechmeister (LBI@HTA) Slides and papers P-P slides and papers detailing the methods and results of the WP5 preliminary survey and round 1 Delphi survey will be made available on the WP5 extranet at the end of June. EUnetHTA overview The structure of the sustainable network will be proposed by DACEHTA in August 2006 in a process paper for further discussion. WP5 and adaptation Distinction between adaptation and adoption. There is a spectrum ranging from the creation of a completely new report, adaptation to varying degrees and complete adoption of another country’s report (with possible language translation). A description of the stages of adaptation is required. There is no formalised process of adaptation. There are different types of HTA reports e.g. mini HTA reports. What types of HTA reports are members producing? An understanding of the needs of agencies and users is required. There was consensus that applicability testing will not produce ‘adapted reports’ but ‘adaptation material’. WP5 should always start from an existing HTA. Coordination (architecture) is the realm of WP4. Thoughts on toolkit Toolkit should consider relevance, reliability (quality assessment) and transferability. It should include a checklist of prompts to local context issues for consideration. It should be very practical and useable.
70
We must be aware of different types of users e.g. those who haven’t adapted a report before, no agency/large agency, information for specialists and generalists. Should consider issue of dealing with multiple HTA reports May need more than 5 headings. Not all sub-headings are relevant for the 5 headings. Toolkit will develop and change over years 2 and 3 of this project. It will start simple and become more sophisticated over time. Guidance on use will be developed but the toolkit will, eventually, be software based. A practical exercise would be useful. Using an HTA report as a template and using the toolkit on this i.e. applicability testing. Thoughts on glossary Ensure close working with developers of the INAHTA glossary to inform them of our work and for future links. Issues raised at the meeting for other work packages? Development of a Clearing House meta-search engine for searching for HTA reports. This facility would search the INAHTA database and agencies’ websites for reports. Provide a standard data extraction sheet and format for an HTA report. Have a meta-database of literature within HTA reports e.g. efficacy data Attendees felt there was a need for contact information in future HTA reports to identify additional information and provide access to economic models Need for instructions to agencies on how to write HTA reports in ways that make these reports easier to use/adapt Actions Mini round of e-mails to enable convergence on definition of adaptation. To send out 19/06/06 for comments by 26/06/06. E-mail members who did not attend meeting. Suggest e-meeting to help understanding of our objectives, work plan, their input. Revisions of toolkit and glossary descriptions. Second round of Delphi – further developed toolkit. Proposed send out beginning of July. Two week deadline. Full results from preliminary survey and 1st round Delphi survey to be made available on Episerver. End of June/early July. Allocation of commentaries to members. Early July. Deadline early September. Allocation of glossary terms and definitions. Early July. Deadline early September.
71

b) E-meetings on toolkit domains Transcript type notes from Safety Toolkit Commentary Work E-Meeting, 10am Thursday 21st September 2006 Lead: Nick Hicks, Debbie Chase, Celia Davidson, NCCHTA, England Participants: Celine Moty-Monnereau and Najoua MLIKA-CABANNE, HAS, France Rosa Rico and Nieves Sobradillo, OSTEBA, Spain Assistance: Julia Chamova, DACEHTA, Denmark Slide 6-10 Reliability questions Rosa: Need to integrate the issues suggested by all commentary workers. Nick: Will integrate responses after the e-meeting. Rosa: In my proposal we talked about data coming from contextual database. Data are heavily linked to contextual setting. Celine’s co-worker: Our proposals are based on in house experience. We have lots of experience of adapting guidelines. These are produced for stakeholders and decision makers. The proposals are in-depth questions used for adapting guidelines. We may not wish to utilise all these questions in the WP5 toolkit. Debbie: The safety domain within the toolkit could have two sections. The first would include key safety reliability and transferability questions. The second would include more comprehensive questions that could be utilised when necessary. It is important that we assess reliability before transferability. What is your experience of using these questions to assess reliability? Celine’s co-worker: Experienced for 3 topics in guidelines area. Have used in depth. Examples are: Initiating labour for women. Syncope, stroke. Propose that these examples are sent to Debbie for consideration. Rosa: Happy to use HAS checklist in WP5 toolkit with integration of OSTEBA questions. Slides 11 – 15 Transferability questions and conclusions Nick: Looking at the HAS checklist, there is a match between the points and those suggested by Rome Group: 1+2 HAS. 2nd point from Rome also in HAS. Rosa: I agree that they are complementary. Rosa: Important to add the training aspect to the HAS transferability checklist. Also important to consider evidence from medical incident report systems/ questionnaires in the health services. Nick: This isn’t always emphasised enough in reports or guidance in writing HTA reports. Debbie: Which methods are better for reporting safety? How could we address this in the toolkit? Rosa: Don’t know about incident report systems. In HTA, usually work with local context with this kind of data because usually no conducted trials re safety but difficult for transferability. Need to known how to read and use other countries’ context specific data. It is a necessity. Celine’s co-worker: Need to talk to ADAPTE group: http://www.adapte.org/index.html (Bernard Burnand a member). Criteria already there for adaptation: consistent, but no validation undertaken. They are comfortable with it, but not tested. Debbie: Bernard will be part of the group reviewing these safety checklists.
72

Are there any specific questions relating to certain types of health technologies that we should include in the toolkit? Nick: Let’s talk internally about this. Slide 16: Speedy sifting Debbie: Speedy sifting. Reminder of questions. Can you think of any relevant questions in relation to safety? Now/later? Rosa: Descriptive questions. Safety [is connected to?] effectiveness question, too. So – perhaps better to do it later? Celine’s co-worker: 5. Be aware that if author is from a well-known organisation still need to check reliability. Be careful with authorship. Slide 17: Future work. Debbie: Next stage - review by members who have not worked on this domain, then on WP5 extranet for comments from all WP5 members Julia: Important to record methods used for development of toolkit – choice of members for work etc. Debbie: There has been no recording for this e-meeting session. Notes/transcript will be sent to all participants.
73
Transcript type notes: Effectiveness domain e-meeting 12.00-13.00 Thursday 21st September 2006 Lead: Nick Hicks, Debbie Chase, Celia Davidson, NCCHTA, England Participants: Kristian Lampe FinOHTA, Finland Inger Natvig Norderhaug NOKC, Norway Assistance: Julia Chamova, DACEHTA, Denmark Apologies: Mike Clarke, Cochrane UK Comments on Mike’s commentary work suggestions (12 reliability and one transferability questions): Kristian: Questions 1 and 2 are from the Overview Quality Assessment Questionnaire (OQAQ) checklist and therefore fine. Question 3 is a new question, and a good idea. Should we be specific that the search should include the HTA database? Inger: Good ideas – agree with Kristian: relevance for filtering as not only the quality dimension: consider early or late in the toolkit? Need to consider if intervention is relevant in local context. Inger, Kristian, Debbie: Questions 5-8. Agreed, should be included in the toolkit. Inger: Questions 9-13. Need to reconsider the wording of question 12 i.e. relevance. Inger: These are all important questions to include in the toolkit. It is important that we consider relevance. Kristian: Important that our standards are connected to some international standards. All questions in toolkit should relate to existing work. Oxman and Guyatt checklist developed to assess the quality of systematic reviews. Debbie: Do you think that this checklist adequately deals with effectiveness issues – as much as efficacy? Are there further questions we need to add to this checklist relating to effectiveness issues? Inger: Thinking on quality assessment of effectiveness data is too premature yet to include in the toolkit. We could add this in the future. Comments on Kristian’s commentary work suggestions regarding transferability: List of factors Kristian: Proposed list of factors for consideration comes from a colleague and was published recently. Inger: Some of the items listed relate to validity of the study rather than transferability. Transferability issues – regarding population, intervention and comparator. Analysis part – more on reliability. Kristian: Agree, some of these issues would fit within the reliability checklist. Transferability questions Inger: Agree with the transferability questions proposed by Kristian. Would like to test the toolkit in-house using the agreed checklists.
74

Economic evaluation e-meeting 2/10/06 Lead: Debbie Chase, Hilary Bunce, Ruairidh Mine, Andrew Cook, NCCHTA, England Participants: Jakob Kjellberg, DSI, Denmark Ingrid Zechmeister, LBI@HTA, Austria Teresa Gasparetto, Regione Veneto, Italy
Slide 6 - OBIG (Ingrid Rosian-Schikuta) Drummond checklist should be used for assessing economic evaluation data reliability Ingrid: Reference 4 from slide 6, used same for our commentary. This is a German publication. Useful for assessing reliability, quality and transferability. All other references considered for this commentary apart from reference 5. Slide 7 - Servicio Canario de la Salud, Spain (Julio Lopez Bastida) Aspects to be followed up later Supports use of Drummond checklist for assessment of reliability Jakob: Checklist questions proposed for transferability very similar to questions proposed in the other commentaries. Slides 8, 9 - Regian Veneto (Teresa) Reliability – though no definition of what reliability means in this context Possibly benefits from report -> source of bias So much benefit -> Bias. When should the report be excluded? Slides 10, 11, 12 – LBI@HTA (Ingrid Zechmeister) Information from personal experience Reliability -> Drummond, but possibly leave out some questions (would be dealt with in speedy sifting part of toolkit) Transferability -> Welte & Leidl checklist for transferability translated into English W& L have published in English themselves. These criteria are easy to operationalise when dealing with transferability. The checklist has been validated. Exel based algorithm needs more consideration/investigation. Ingrid has not used this algorithm. It is linked to table 1. However, Ingrid has used the list of factors in table 2 to help with adapting reports from other settings. Slides 13, 14 - Danish Institute for Health Service Research (Jakob) All guidelines develop from Drummond & Canadian guidelines, ?Philips Little to choose between them – unless there is an advanced decision-analytic model in which case Philips may be superior. Some guidelines have better structure. No special preference as to which we chose to include in the toolkit. Questions must guide assessor where to look in a model – which may have hidden depths in spreadsheets or a computer programme. These are easy to miss for assessors lacking health economics experience -> checklist must be very detailed and comprehensive to guide inexperienced assessors. Drummond therefore will not be detailed enough. The CCOHTA checklist is a more practical tool, more detailed and helpful for inexperienced assessors. Issue regarding whether an economic evaluation violates national/regional guidelines on economic evaluation. Important to take account of national economic guidance. For example, in Denmark, equity issues are very important. There are specific guidelines for dealing with cost and CBAs. In relation to transferability, there are organisational issues here. For example, the English health system is not that different from the Danish health system but, in transferring information from a NICE report, we need to be aware of differences in treatment patterns. The way the treatment is organised is very important and has a big impact on cost. Proposed way forward
75
Participants agreed that we should include the Drummond checklist (plus additional questions from CCOHTA) in the toolkit and also include the transferability questions and issues raised by all participants (including the list of factors highlighted in Ingrid’s commentary). It was agreed that flagging the issue of national economic guidance would be an important addition to the checklists. Questions and issues regarding reliability and transferability will be collated in-house and e-mailed to members who produced economic evaluation commentaries. Once agreed, these will be sent for review by other WP5 members. Organisational aspects e-meeting 2/10/06 Lead: Nick Hicks, Debbie Chase, Hilary Bunce, NCCHTA, England Participants: Mark Leys, KCE, Belgium Camilla Palmhøj Nielsen, DACEHTA, Denmark Finn Børlum Kristensen, DACEHTA, Denmark Hans-Peter Dauben, DAHTA@DIMDI, Germany
Agreement from participants that ’organisational impact’ should be changed to ’organisational aspects’.
Slide 6 – KCE (Mark Leys) Has a background in Sociology. Technology not an external factor to organization. Need to understand how it is shaping the organization. Specific context is important – legal/political/cultural. For example, in Sweden there is a stronger focus on primary care than in Germany or France. Need to take account of inter-organisational issues or relationships between organizations. We focus too much on intra-. In assessing organizational issues, qualitative research, changes/processes important. There are different approaches but no one checklist to assess reliability. Ideas from system theory. Slide 7 – DACEHTA (Camilla) Very brief descriptions on organisational aspects in previous European projects. WP4 already have ideas on how to take this forward. Qualitative data important. Checklists already mentioned, however these only look at transparency of data and not theoretical basis of data. What do we mean by transfer of data on organizational aspects? Is this the conclusions? Hans-Peter: From German experience, problem is, what do you want to do with these data from another context? Slide 8 – TU Berlin (presented by Debbie) Consideration of dimensions and how HTs can induce changes in dimensions. This domain one of the most context dependent aspects in HTA. Results unlikely to be transferable, the methods used in the assessment might be transferred to other situations. Slide 9 – ZonMW (presented by Debbie) Important that organizational aspects are dealt with as a distinct subject and also implicit in other toolkit domains. Organisational aspects not routinely incorporated into HTA reports - likely reason why there are no checklists or tools for assessing reliability. Transfer sensible for the kind of issues on organizational aspects and the kind of data, but not the data themselves. Methodologies might also be transferable. Camilla: Use of different methods, relates to Mark’s comment on organizational aspects. Important to consider at different organizational levels. General discussion Mark: Need to clearly distinguish all levels of organizational issues – department, direct user…. With a focus on inter-departmental issues. Nick: Need for a matrix/3-D table that takes account of the different levels and impact on organizations? Debbie: Does anyone have any examples of adapting information/methods etc. relating to organizational aspects from one report to another?
76

Hans-Peter: Tried to adapt some HTA reports to different settings. Have tried to develop a model for transferring information into the German setting. For the C-virus HTA report, this was adapted into the Canadian setting. To accomplish this, ?the author, was part of a Working Group that adapted the report to the new setting. (Hans-Peter please could you check that I have understood this correctly) Camilla: In Denmark, we often adapt more local, Danish, reports. Therefore, not from one country to another. Always include organizational aspects, but don’t usually find this in other reports. Mark: At the descriptive level, HTA reports should include information on organizational aspects. What is the impact on personnel? On relationship? No examples exist. Hans-Peter: There is a need for more organizational aspects information within the report to be adapted to help transfer information. Finn: We should look to the WP4 handbook for assistance. Way forward Debbie: What should we include in the toolkit? (1) A high-level checklist dealing with issues and methods in this area, (2) nothing – given that few reports include this domain and assessment ideas are at an early stage of development or (3) something else? Camilla: Try to go with checklist, co-ordinate closely with WP4 and take time to describe issues and problems. Mark: Thinking in this area has not moved on since 1990s. We need to include this in toolkit. But keep it at a basic level at the moment. Hans-Peter: Toolkit needs to include information in general about organizational aspects (less checklist). INAHTA working group have been in discussions regarding checklists – difficult, too many different types of topics. Not practicable. Mark: We are not writing a HIT report. A basic classification is needed. Not too complex. Basic matrix, can locate which level we are dealing with. Matrix: Content (human resources/logistics…) against levels of analysis. We don’t need to understand other contexts to do this. Look at transferring issues for certain levels/settings. Notes from technology use and background e-meeting 28/09/06 Lead: Debbie Chase, Hilary Bunce, Andrew Cook, NCCHTA, England Participants: Kersti Meiesaar Uni of Tartu, Estonia, Elena Berti ASR, Italy Eva Turk, Slovenia University of Tartu (Kersti) Technology background information Should this stuff be at the beginning of the toolkit? – assessment of relevance rather than reliability (Important to relate to WP4 work – recent meeting in Helsinki) Were conditions appropriately defined? Paper from ?? international journal ?? in 2002 Technology use Need to tackle reliability? (of the technology?) (of a report to be converted?) ASR, Italy (Elena) Information taken from Valesco Textbook?? Professional Journal of HTA Background Definition of policy and research question No need to be strict about method of evaluation Institute of Public Health, Slovenia (Eva) Based on commentary from other partners
Why has the assessment been made – who ordered the work? Mainly the ‘political thing’
77

General Discussion Does information on technology use and development affect adaptation? Just a feeling from participants that it is important to include reliability questions on background information,. Do we need a small section to consider the quality of the information in an HTA? Might this fit under question 4 or 7 of Debbie’s 8 relevance questions i.e. speedy sifting questions? Relevance questions deal with most of the questions/issues proposed on technology use and development. Do we need a separate section in the toolkit that addresses technology use and background information? Or can all the issues be addressed in the speedy sifting part and under each of the other sections e.g. issues relating technology use and development to safety outcomes would be dealt with in the safety section of the toolkit.
78

c) E-meeting on the interactive toolkit
Web-based toolkit E-meeting
21st November 2006 Attendees: Representing WP5 Representing WP2 Ruairidh Milne (Chair) Alric Rüther, DAHTA@DIMDI, Germany Neil Adams Hans-Peter Dauben, DAHTA@DIMDI, Hilary Bunce Debbie Chase Purpose of meeting
1. To understand what WP2 and WP5 are doing 2. To agree on possible collaboration
WP2 plans for the Clearinghouse Purpose of Clearinghouse: to bring together information from different areas to help users prepare or read an HTA report. The Clearinghouse will include a database of information. Its aim is to reduce duplication of effort. It will have a ‘public’ and ‘closed’ area. EUnetHTA and INAHTA toolkits can be brought together within the Clearinghouse. Clearinghouse facility will not be completely ‘up and running’ by the end of the EUnetHTA project period. However, prototypes will be developed using WP4 and WP5 products by the end of 2008. The facility will be a ‘portal’. Users would be led through this portal by the questions. It will have an electronic format, linking to websites and a main database. There will be input boxes for data and tables. It is likely to be a Java based system. WP2 are also setting up a communications strategy for EUnetHTA. The next WP2 meeting in December WP5 update on the Toolkit The first version of the toolkit is currently out for review (by WP5 members). It is in the form of a guidance document. We would like the toolkit to be available both as a guidance document and a user-friendly practical tool. WP5 members provided their thoughts on what a user-friendly toolkit would look like through the Delphi round 2 survey. A summary of their responses was presented at the meeting. Mike Clarke, Cochrane Collaboration, made a useful distinction at the WP5 June meeting, that a handbook is a static resource e.g. a pdf file and a toolkit is more like a series of web pages with possible link to a database. At NCCHTA, we are considering the spectrum of what this user-friendly toolkit would look like and achieve i.e. from a simple set of web-pages to a series of web-forms linked to a database. We need to consider the costs and benefits of different approaches, and decide on what we can achieve within the project period, given the available resources. Possibilities for Collaboration What could be achieved in 2007? An interactive tool could be developed within 6 months after the toolkit is finalised. A less sophisticated tool i.e. not linked to a database, could be achieved in 2 to 3 months. The content, questions and language of the toolkit will be continually developed over the next couple of years through applicability testing rounds and review from EUnetHTA members.
79

It would be difficult to integrate the toolkit into the Clearinghouse at a much later date. We will need to develop the interactive toolkit alongside the development of toolkit contents. There is a need for flexibility to make changes to the interactive version. Initially, we need to consider the graphical user interface and principles for development. Then, determine a ‘freezing point’ i.e. timepoint in the project period when the interactive toolkit structure is finalised and not developed further. Next steps Goal for WP5 would be to test the interactive toolkit in the 2nd round of our applicability testing (September 2007). However, if feasible, e-meeting participants were keen to test the interactive version in our first round (March 2007).
1. Schedule a workshop to agree on a graphical user interface, development of the toolkit and planning workload. Date fixed for 14th December 2006, Southampton, England
2. Inform WP2 of our initial plans regarding an interactive toolkit at the WP2 meeting 3. Include information about collaboration with WP2 and initial planning ideas for the interactive
toolkit within the WP5 technical report
80

d) WP4 and WP5 Lead Partners Videoconference
WP4 and WP5 videoconference 21st August 2006 Attendees NCCHTA: Ruairidh Milne, Nick Hicks and Debbie Chase FinOHTA: Kristian Lampe and Ilona Autti-Rämö Key points (i) WP4 are defining 'core' as some part of the product of importance and transferability (rather than the intersection of importance and transferability); and will describe their process for agreeing on core before doing the work (ii) WP5 will decide on whether to call them domains/aspects/facets; WP4 and WP5 will then use the same term For future reference – it was discussed that in using this structure we may miss important issues relating to parameters that fall across domains e.g. quality of life Final decision after much consideration(!): Domains (iii) It will be very useful for WP5 to reflect more closely on the overlaps between WP5 and WP4 processes, once their processes are more clearly defined. For example – information on quality assessment and transferability issues on WP4 cards (each one is about a critical issue relating to the core) will be directly relevant to guidance in the WP5 toolkit (iv) WP4 will involve WP5 in some yet to be defined way in deciding on the transferability (but not perhaps the importance) of the domains (eg effectiveness) and/or the topics (eg mortality) (v) WP4 will also involve WP5 in some yet to be defined way in deciding on final status of particular domains and sub-domains. (final status meaning whether something is in the core or not) (vi) WP4 will call their testing 'validation/validity testing' (and not 'applicability testing') (vii) WP4 and WP5 need to ensure that we are using the same terms to describe the same things (as in ii). This will be done by ensuring that we each have access to each others reports as early as possible. After meeting thought – most importantly, WP5 will provide WP4 with the draft glossary (at the same time as WP5 members) before M10 deadline
81
Annex WP6.1.a Structure for policy study on HTA (EUnetHTA WP6 “Transferability to health policy”2) Lead partners: DACEHTA and TU Berlin/ Observatory Lead scientists/ editors: Prof. Reinhard Busse and Prof. Finn Børlum Kristensen Objectives
1. To get a systematic overview of the links / relations between HTA and health care policy making in (selected) Member States and the EU representing different health systems, remuneration systems etc., and to classify and analyse common characteristics of the relations
2. To improve the responsiveness of HTA to the demands of the HTA consumers with the purpose of improving the effectiveness of HTA as policy input
3. To show concrete use of HTAs in policy making in member states and the EU 4. To position HTA in relation to other relevant sources of input to health policy making such as
regulatory processes of pharmaceuticals and devices by EMEA and technology pricing processes.
Rationale Health technology assessment (HTA) is concerned with the evaluation of the impact of interventions on health and on the health care system including cost-effectiveness (efficiency) considerations. In respect to the improvement of health care quality, the role of HTA is dual. On one hand it supports the decision-making process related to the formulation of best practice standards by providing information on which interventions (preventive, diagnostic, therapeutic incl. drugs, organisational etc.) might work and how they should be delivered to maximize effectiveness. On the other hand, the impact of quality improvement initiatives on the health care system can also be assessed by means of HTA.3 Both directions should contribute to the policy basis by allowing timely and appropriate access by users to existing and innovative technologies with a significant contribution to health outcomes. However, as with all potentially quality-enhancing interventions, HTA can only achieve its potential if it is applied to the right actors at the right time. We will therefore review, comprehensively, the contribution of HTA and related initiatives and networks across EU Member States, candidate countries and EEA/EFTA countries providing an analytical overview of the impact of HTA and related initiatives on health care planning and policy, and effectiveness and responsiveness of health care systems. The book will analyse how research evidence can be better “translated / tailored / transferred” to improve policy- and decision-making about (new) health technologies, e.g. how to include research evidence/ HTAs in the basis of decisions about e.g. the benefit basket, how to guide providers to employ them appropriately (i.e. for the right patients at the right time), thereby reducing practice variations and ultimately improving population health. This should in turn allow for tools and models of good practice to be identified – and implemented at a later stage.
Contents (subject to final agreement by partners) The book is structured into three parts as follows.
Part I: The conceptual and policy environment for HTA 1. Policy framing: This chapter introduces HTA as input to policy making from a policy process
perspective. This general framing will provide a short general introduction to HTA and more specifically an introduction of the possible contribution to health policy making. Responsible: lead partners
2 Even though the WP is termed „transferability“, the WP is about both sides of the „HTA bridge“, i.e. how HTA doers can/ should increase the transferability of their products to policy-makers (or how to “tailor” them according to the policy-makers’ demands and expectations) as well as how policy-makers can/ should increase their “HTA literacy” in order to use assessments for their decision-making. 3 Organisational, financial or regulatory interventions can also be considered as health technologies. As defined by the EPOC Group (Effective Practice and Organisation of Care Review Group, within the Cochrane Collaboration), different types of interventions, such as professional (e.g. educational program on prescription), financial (e.g. co-payment), organisational (e.g. changes in medical record system) and regulatory (e.g. licensure) are included here.
82

2. Conceptual framing: This chapter will map the way by outlining how HTA fits together with other structural quality measures such as licensing, certification and accreditation; process-oriented activities such as evidence based medicine, protocols, and clinical practice guidelines; management oriented quality improvement measures including audit; and outcome-oriented activities such as benchmarking, “league tables” etc. within a European context. Responsible: lead partners
3. Health system/ policy/ regulation: This chapter (possibly split into two) will summarise the Member States’ experience with the various approaches taken to implement and utilise HTA (and related) structures and activities to understand relevant regulatory and policy processes in the Member States as well as on the EU level. The chapter will be based on available information (from the Observatory’s “Health Care Systems in Transition” profiles, previous and ongoing European projects on HTA etc.) as well as questionnaires filled out by EUnetHTA project partners for each country (e.g. identifying relevant legislation and actors), and consultation with relevant EU authorities and stakeholders. Responsible: lead partners, co-authors from other WP6 partner(s), all WP6 partners for providing information
Part II: The contribution of HTA to policy-making and population health 4. What is HTA? How should it be done? The process of HTA (from identification and prioritization [input
from WP7] to doing and dissemination). This chapter will be based on the relevant ECHTA reports but will incorporate new developments as arising from WP4 and WP5. Responsible: lead partners, co-authors from other WP4, WP5, WP6 and WP7 partner(s)
5. Review of the demands and expectations to HTA from health care policy-makers in member countries and EU and the concrete handling of HTA including (but not limited to) HTA produced by EUnetHTA (in WP 4 and 5) in Member States and the EU. The chapter will be based on a systematic literature review on the topic (incl. results from similar projects, e.g. policy-makers view on economic evaluations) as well as on the discussions during the workshop (month 15) with relevant policy-makers from selected Member States. Responsible: lead partners, co-authors from other WP6 partner(s) + OBS
6. Reviewing, comprehensively, the contribution of HTA and related initiatives and networks across EU Member States and EEA/EFTA countries providing an analytical overview of the (potential and actual) impact of interventions on governance, effectiveness and responsiveness of health care systems and ultimately health. This chapter will be based on a systematic review of the literature. Responsible: lead partners, co-authors from other WP6 partner(s)
Part III: Improving the impact of HTA 7. Impact (possibly split into more chapters): This chapter will explore factors which in practice facilitate
and hinder the impact of HTA reports through decision-makers. It will be based on national and regional case studies supplied by the project partners as well as on the experience of WP4 (i.e. the trans-national common core HTAs with context-based national adaptations) and WP5 (i.e. the adaptation of national HTA reports through other countries) . Responsible: co-authors from other partner(s), WP6 partners with interesting case studies, WP4 leader, WP5 leader.
8. Conclusions: Analysis of how research evidence in the form of HTAs can be better “translated/ tailored/ transferred” to improve policy- and decision-making about (new) health technologies and how policy-making/ makers can become susceptible to HTAs (e.g. necessary regulatory framework, division of labour between HTA doers and decision-makers, formulation of policy-relevant questions, observing context for decisions, training courses). Responsible: lead partners.
83

Annex WP6.2 Preliminary draft 2006
Work Package 6 Stakeholder Forum
The Stakeholder Forum: This paper describes considerations on the establishment of the EUnetHTA Stakeholder Forum. The Forum is planned to be an open and changeable environment, depending on the situation and the needs of the EUnetHTA project, and not a closed permanent group of people. The Stakeholder Forum is a deliverable for Work Package 6, but is at the same time closely connected to the whole EUnetHTA project. Overall aim: The aim is to establish links to exchange views, expectations and feedback on HTA with key stakeholders in order to ensure support among these to establish a sustainable European network for HTA. The Stakeholder Forum will function as a tool for receiving input from selected stakeholder groups and providing output from EUnetHTA to these stakeholders. Objectives: To achieve the overall aim a number of subordinate objectives need to be met. First of all the relevant stakeholders should be identified. The partners in WP 6 have selected five key stakeholder groups:
• Policymakers at national/regional level • Policymakers at institutional (hospital) level • Industry • Health care professionals • Patient organisations
Specific (European/national) stakeholders within these groups have to be identified and approached to establish links between these and EUnetHTA. A second objective is to create tools/channels to ensure sharing of experiences with the stakeholders. One main entry point should be established to enhance the visibility and quality of dialogue between European HTA and relevant stakeholder groups. Activities: A number of activities are currently in preparation Identification and analysis of key stakeholders at European and national level In order to provide the basic information on the stakeholders a general stakeholder identification and analysis is being prepared. Work Package 6 members are expected to take an active part in the stakeholder analysis in their own country. It is suggested that we develop standardized templates to make a common framework for the analysis. The stakeholder analysis provides a time limited overview of the stakeholder field, and in the longer run it should be regularly updated or if necessary repeated. Website A special Stakeholder Forum will be established on the public EUnetHTA website and it will contain both general information on the links between HTA and the selected stakeholder groups and specific information on the development of the EUnetHTA project. The main objective is to enable interested stakeholders to engage in on-line dialogue with the EUnetHTA project. The material that will be presented on the Stakeholder Forum website could, e.g., be:
• Progress reports from the EUnetHTA WPs • Information on existing links between the organisations involved in EUnetHTA and the selected
stakeholder groups • Research Papers/grey literature on relations between HTA and stakeholders • Discussion papers from key stakeholders on future structure for stakeholder involvement in
European HTA Furthermore a discussion forum could be established to insure the possibility of input to EUnetHTA from interested stakeholders.
84

It is important that we do not duplicate the other fora for stakeholders that already exist (e.g., HTAi Forum, ISPOR, etc). We will build on what already exists and will stay informed on their developments. We will feed on and contribute to the general discussions on the stakeholder involvement issues that the other fora concentrate on. However, our focus is on the European HTA process where we look at the needs and issues pertinent to the existing and developing HTA entities in Europe and stakeholder needs in the European environment. We need to be aware of possible barriers related to web based communication. It is a challenge to engage and activate stakeholders on-line. One way of promoting the forum and to engage stakeholders could be to make very short questionnaires with responses from stakeholders and to publish it on the website. Other possible ways of promoting the site should be developed. Face-to-face contact In addition to the web based contact, we need to establish face-to-face contact with stakeholders. In the short run we will meet stakeholders at the European Health Forum, Gastein, where the Stakeholder Forum will be introduced, and at a policy workshop in March, 2007 with a special focus on political and administrative stakeholders. Furthermore, a number of meetings have been and will be held with specific stakeholders during the project. However, it is most likely necessary to develop more systematic face-to-face contact in the longer run. One possible solution is to work towards establishing an annual EUnetHTA stakeholder meeting, perhaps with changing focus on different stakeholder groups.
85

Annex WP6.3 Suggested participants – policymakers: Country Decision-Level Type of Institution Person Position Invite? CH Macro /National Federeal Office Public
Health (gov)
Peter Indra Vice-Director (Head of Sickness and Accident Directorate)
yes
CH Meso/Regional University Hospital Andreas Tobler Medical Director Univ. Hospital Bern
2. (NGO-Foundation)
England National and Local NICE (gov)
Ken Stein Vice-Chair NICE Appraisal Committee
yes
England National and Regional Public Health Office (gov)
Mike Gill Regional Director of Public Health
yes
England National and Local HTA Edmund Jessop Chair of National Specialist Commissioning Advisory Group (Disease Prevention)
2. (gov)
Italy Macro/ Local Regional Health Services (gov)
Carlo Favaretti Director Trento Health Services Enterprise
yes
Italy Macro /National Ministry of Health (gov)
Alessandro Ghirardini
Professor yes
Italy Macro /Regional Regional Health Services
Roberto Grilli Director Emilia-Romagna Regional Health Enterprise
2.
(gov) Estonia Macro /National Ministry Social Affairs
(gov) Peter Laasik Deputy Minister yes
Estonia Macro /National Health Insurance (sickness fund)
Hannes Danilov Chairman Management Board
yes
Estonia Macro /National Parliament Urmo Kööbi MP, Member of Social Committee
2.
DK Central Gov. Ministry of Health Steffen Egesborg Hansen
Head of Dpt. yes
DK Central Gov. Ministry of Health John Erik Pedersen
Head of Dpt. 2.
DK Regional Gov. Copenhagen Capital Region
Helle Ulrichsen Managing Director yes
DK Regional Gov. Copenhagen Capital Region
Leif Vestergaard Pedersen
Health Director 2.
DK Regional Gov. Copenhagen Capital Region
Jens Elkaer Health Director 2.
DK International WHO Jens Kristian Götrik
Medical Direcotr Chairman of the Board WHO-Europe
NO
FIN Macro/National non-for-profit, self-governing
Liisa-Maria Voipio-Pulkki
Ass Prof, senior medical adviser
yes
Belgium Macro / National National Health Insurance Board (Government)
Jo De Cock CEO (administrateur general)
2.
Belgium Macro / National Ministry of Health Prof. Karel Vermeyen
Ministerial adviser yes
Belgium Macro / National not-for-profit: (largest mutuality in Belgium)
Rob Van Den Oever
Director yes
Belgium Macro / National National Health Insurance Board (Government)
Ri De Ridder Director general yes
Belgium Macro / National non-for profit: Socialist Mutuality
Patrick Galloo Director 2.
Spain Meso / Local Hospital Jorge Gómez Zamora
Hospital manager/Director 2.
Spain Macro / Regional non-for-profit, Miguel Angel Director yes
86
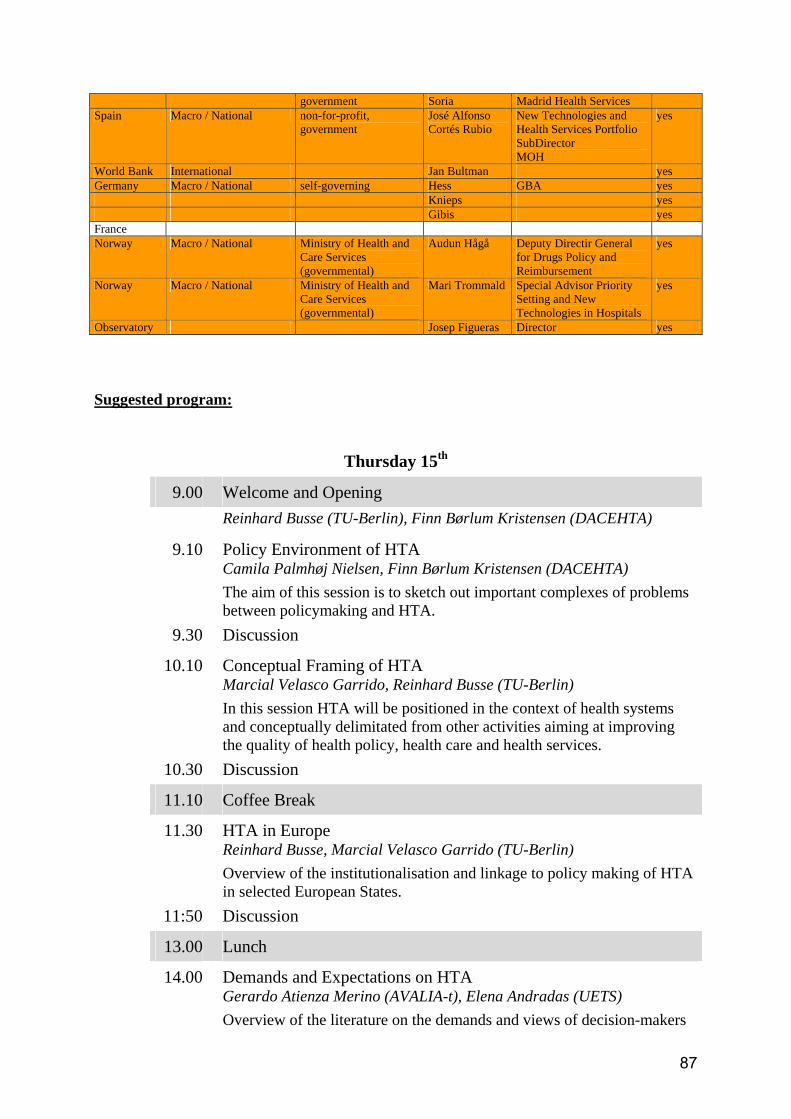
government Soria Madrid Health Services Spain Macro / National non-for-profit,
government José Alfonso Cortés Rubio
New Technologies and Health Services Portfolio SubDirector MOH
yes
World Bank International Jan Bultman yes Germany Macro / National self-governing Hess GBA yes Knieps yes Gibis yes France Norway Macro / National Ministry of Health and
Care Services (governmental)
Audun Hågå Deputy Directir General for Drugs Policy and Reimbursement
yes
Norway Macro / National Ministry of Health and Care Services (governmental)
Mari Trommald Special Advisor Priority Setting and New Technologies in Hospitals
yes
Observatory Josep Figueras Director yes Suggested program:
Thursday 15th
9.00 Welcome and Opening Reinhard Busse (TU-Berlin), Finn Børlum Kristensen (DACEHTA)
9.10 Policy Environment of HTA Camila Palmhøj Nielsen, Finn Børlum Kristensen (DACEHTA) The aim of this session is to sketch out important complexes of problems between policymaking and HTA.
9.30 Discussion
10.10 Conceptual Framing of HTA Marcial Velasco Garrido, Reinhard Busse (TU-Berlin) In this session HTA will be positioned in the context of health systems and conceptually delimitated from other activities aiming at improving the quality of health policy, health care and health services.
10.30 Discussion
11.10 Coffee Break
11.30 HTA in Europe Reinhard Busse, Marcial Velasco Garrido (TU-Berlin) Overview of the institutionalisation and linkage to policy making of HTA in selected European States.
11:50 Discussion
13.00 Lunch
14.00 Demands and Expectations on HTA Gerardo Atienza Merino (AVALIA-t), Elena Andradas (UETS) Overview of the literature on the demands and views of decision-makers
87

on HTA and evidence reports. 15.00 Structured Discussion „Needs of Decision Makers“
How can HTA better respond to the demands of decision makers?
17.00 Closing
19:30 Dinner
Friday 16th
9.00 Opening Reinhard Busse (TU-Berlin), Finn Børlum Kristensen (DACEHTA)
9.10 Contribution of HTA Ansgar Gerhardus (University of Bielefeld) A systematic review of studies which have assessed the contribution of
HTA to the process of health care policy and ultimately to population’s
health.
9.30 Discussion
10.10 Bringing Evidence into Policy Antonio Sarriá Santamera (AETS) What can be learnt from experiences outside the area of HTA and from theoretical developments in the field of knowledge transfer?
10.30 Discussion
11.10 Coffee Break
11.30 Future Challenges John Arne Røtingen (NOKC) This session will explore the broader policy related factors which in practice facilitate and hinder the impact of HTA reports in future.
11:50 Discussion
13.30 Lunch
14.30 Last Words, Time Schedule of Project
15.30 Closing
88
Annex WP6.4
Work Package 6 Policymaker workshop
Berlin and Copenhagen 01.09.2006
Dear Colleagues,
In order to get now really started (after our workshop this March in Copenhagen), we enclose
the following material to facilitate the progress of the project in the next months:
1. A questionnaire to be completed by all partners in order to gather information on the
way HTA is utilised in the various countries. It serves as information for preparing
the book (mainly chapters 3 and 8). The questionnaire should be returned at the latest
on the 20th October to: [email protected] AND [email protected]
Thank you very much for your co-operation,
Camilla Palmhøj Nielsen Marcial Velasco-Garrido
Finn Børlum Kristensen Reinhard Busse
89

WP 6 – Questionnaire on HTA in health systems
This questionnaire aims at collecting information on the peculiarities of HTA in
European health systems (not on individual organisations). For this reason we need that
from each of the countries taking part in the project a single answer if possible. The
questionnaire will be forwarded to all institutions for general information, but only one
institution per country will be asked to coordinate the answer (i.e. to the institution
representing the country in this Work-Package; in case of more than one to the
institution with the broader mandate). For countries represented by more than one
institution in the project it would be desirable that the institution taking the lead in the
answering of the questionnaire gets feedback from the other national participants and
that a consensuated single answer is delivered.
We are aware that some of you will also be answering a questionnaire from WP-8 and
have been worried about duplication of work. After reviewing the questionnaire of WP-
8 we came to the conclusion that this is aiming at identifying charachteristics of the
organisations involved in doing HTA. The emphasis of WP-6 i.e. of this questionnaire–
lays in the whole health system, the process and the impact of HTA in each country.
Thus, despite the possibility of some overlapping, both questionnaires address different
issues.
For some of the countries there is already some information available in the respective
country profiles of the Health Care Systems in Transition (HiT) Series of the European
Observatory on Health Systems and Policies. We encourage participants to take this
information as a starting point to answer the following questionnaire. For the purpose of
WP-6, it is however important to update and expand the description contained in the
HiT. HiTs are freely available at the Observatory’s webpage
(http://www.euro.who.int/observatory/Hits/TopPage).
The questionnaire has four parts:
• First we ask for the contact details of the person responsible for the answers, for
the case that further information is required.
• The second part aims at describing the decision-making environment relevant to
HTA in the health care system as provided by the regulatory framework.
• In the third part you are asked to provide a description of the system of HTA in
place.
• The fourth part asks you to choose some real cases in order to illustrate the
process of HTA in your country. The parts II, III, and IV are open questions.
Consider that the questionnaire does not refer to a/ your single institution/ organisation
doing HTA but to the whole system of HTA in your country. We assume that HTA –
the structured analysis of health technology with the purpose of informing the policy-
making process– may be met in different forms in the same country. Different
organisations might be doing and using HTA at different decision-levels, and differing
in the breadth of aspects assessed.
If you have any questions regarding the questions, the desired structure of answers etc,
please contact [email protected].
The answers to the questionnaire should be delivered by the 20th October 2006. The
extension of the answers should not exceed 1500 words. Please return your answers to
both [email protected] and [email protected]
2

I - Contact Details
Country
Name of person responsible for the
answers
Institution:
Telephone:
e-mail:
3

II- HTA in the Health Care System
Based on previous research, we know that not all health technologies –drugs, services, devices, etc.– will
be reimbursed/covered/ offered within/ by the public payers (NHS or sickness funds) in the health care
system. This implies that a policy-process (i.e. a decision-making process) concerning what is “in” and
what is “out” of the scope of the system (i.e. what care should be delivered and what not) does exist in
each country.
Additionally a decision-making process concerning how the system is managed (i.e. which organisational
interventions/technologies –e.g. co-payments, “integrated care”– will be implemented or not implemented
/ will be applied or not applied to the system) will exist.
We refer here to the actors/ institutions making the decisions, while HTA institutions (as “doers”) are
approached in part III.
Concerning the interventions to be delivered as part of the health services:
1- Which institutions are involved in the decision-making process? Are they governmental/ non-
governmental institutions? Are they local/ regional/ national? Do their decisions apply to all
sectors/ only one sector (i.e. primary health care, ambulatory care, public health, hospital…)?
2- Are there any explicit criteria (e.g. stated by law) to be taken into account in the decision-making
process? If so which are these criteria (e.g. “medically necessary”, “cost-effective”)?
3- Do the institutions have the obligation/ possibility to commission assessments/ research in order
to assess the fulfilment of decision-criteria?
4- Do the institutions conduct themselves assessments –i.e. do the decision-making institutions
have their own HTA-institution/unit as part of them)?
Concerning the interventions to be applied to the health system (i.e. organisation/ management/
financing):
1- Which institutions are involved in the decision-making process? Are they governmental/ non-
governmental institutions? Are they local/ regional/ national?
2- Are there any explicit criteria (e.g. stated by law) to be taken into account in the decision-making
process? If so which are these criteria?
3- Do the institutions have the obligation/ possibility to commission assessments/ research in order
to assess the fulfilment of decision-criteria?
4- Do the institutions conduct themselves assessments –i.e. do the decision-making institutions
have their own HTA-institution/unit as part of them)?
For a start, please have a look at the “benefits” and, if existing, “health technology assessment” sections
of the “HiT” profile of the European Observatory. You may wish to copy paragraphs and update them –
or write new ones. A desirable addition to this part of the questionnaire would be to construct a table
(especially if several institutions are involved in decision-making) to provide an overview.
(continues next page)
4

We propose (answers are examples only):
Institution A … Institution X
Status (Gov/Non-Gov) Gov Non-Gov
Area of Influence (Local/ Regional/National) National Local
Sector of influence (PHC, Ambulatory, Hospital,
Rehabilitation)
All Hospital
Explicit criteria to be accounted for Cost-
effectiveness
Budget impact,
medical necessity
Link to HTA (optional, mandated) Mandated Optional
Own HTA unit/institution Yes no
5

III – System of HTA
Assuming that in the same country several organisations might be doing HTA, please do not focus only
on one organisation but try to provide an overview of the different institutions. Please try to map the
distribution of HTA-organisations and activites across different levels of the health system.
1- Are there any institutions/ organisations whose principal mandate is to evaluate technologies
with the aim of informing the policy process?
2- If such institutions exist, please characterize them according to their:
a. area of influence (single organisation/local, regional, national)
b. type of funding (public, private) and orientation (for-profit, non-for-profit)
c. location within the health system (belonging to governmental or state-institutions,
belonging to NHS as purchaser, other public purchaser, private purchaser, provider,
self-governing institutions)
d. relation to decision-making institution as described in part II (dependent/ independent)
e. links to policy-process (formally/explicitly linked to policy-processs –explaining to
what kind of decision i.e. benefit basket, organisation of services, etc. – not
formally/explicitly linked) and level of policy process to which is linked (micro, meso,
macro –explaining details)
f. initiative to work (i.e. only commissioned work, own initiative)
g. “kind” of HTA they perform (primary research, review of literature) and aspects
covered (safety, clinical effectiveness, economic/ cost-effectiveness, organisational,
etc.)
h. type of HTA products delivered (public/confidential, extensive HTA reports, mini
HTA-reports, recommendations, informations sheets, other).
i. functions other than doing HTA (i.e. surveillance, health plan elaboration, education,
etc.)
3- If such organisations do not exist, do any other organisations/ institutions undertake
assessments? Are there any possibilites for policy-makers to commission HTA work to
someone? Under which circumstances?
4- If such organisations do not exist, are there any planned?
5- Please provide a brief description of the development of HTA in your country: are there any
trends worth mentioning (i.e. increasing number of institutions, widening of mandate, etc.)?
6

IV – Case Studies
Please provide a set of two or three cases which illustrate the peculiarities of HTA in your country. The
description of the cases should not extend too much on the explanation of the technology but focus on the analysis
of the aspects listed in questions 1 to 6 below.
We argue that the following situations are possible concerning the use of HTA in decision-making (see cross-
table below). Please provide cases from different cells.
HTA-Report exists
Technology “positive” conclusion
(i.e. technology effective) “negative” conclusion
(i.e. technology ineffective)
no HTA-report
introduced/adopted/ purchased
not introduced/abandoned/ not purchased
1- What was the policy question? What kind of decision was to be taken? At which level within the health
system?
2- Did the policy question lead to a formal assessment (HTA-Report, no matter how extensive)?
a. If yes, how did the transfer between policy-question and research-questions worked? Which
organisation/institution undertook the assessment? Was there any contact between decision-
makers and researchers (HTA-doers)? Did the assessement focus on the aspects required by the
decision-makers? Did the assessment formulate any clear recommendations?
b. If not, was there an informal contact/feedback between policy-makers and researchers? Did
HTA-doers forward research evidence? Did HTA-doers formulate any recommendations?
3- Was the decision in accordance to the recommendations (if any) formulated by HTA-doers? Do HTA-
doers consider that the decision was in accordance to the findings of the assessment/ the informal
feedback?
4- Which aspects took the greatest weight in the decision (e.g. effectiveness, budget impact, equity, other)?
Were these aspects part of a formal assessment and content of an HTA-report?
5- If neither an assessement nor an informal knowledge transfer was done, were the arguments on which the
decision was founded made public? If so which aspects were mentioned?
6- Beside decision-makers and HTA-doers, were other actors involved in the decision-making process (i.e.
did other actors informed/influenced the process)?
If possible, please also provide weblinks or references to reports and papers documenting the information
available during the decision-making process and/or the decision itself – even if this information will usually be
only available in the country’s language.
7

Annex WP6.5 European HTA Parallel Forum at European Health Forum Gastein Program:
October 4, 2006, 15:30-18:30
A. HTA in health care planning and policy – experience from Member States
15:30 Chair’s introduction to the session 15:35 HTA as input to NICE guidance in England and Wales Sara Garner, Technical Advisor, NICE, UK 15:45 How to insure the policy relevance of HTA – views from the government perspective Kari Harno, Ministry of Health, Finland
15:55 From evidence to policy in a decentralised healthcare system Peter Sawicki, Director, Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWIG), Germany 16:05 HTA in regional healthcare planning Giancarlo Ruscitti, Veneto Region, Italy 16:15 Questions/comments from the audience
B. Stakeholder perspective in the HTA process 16:30 HTA in hospital management Americo Cicchetti, Director of research, HTA Unit, “A Gemelli” University Hospital, Italy 16:40 HTA: a tool to improve patient access to innovation – an industry perspective Andrea Rappagliosi, Vice-Chair Board of Directors, EuropaBio 16:50 HTA as input to reimbursement decisions Gotfried Endel, Hauptverband der Österreicheschen Sozialversicherungsträger, Austria 17:00 Questions/comments from the audience 17:15 20 minute BREAK
C. European network for HTA - EUnetHTA 17:35 European network for HTA – why a priority for the European Commission? Bernard Merkel, Head of Health Strategy Unit, DG Sanco, European Commission 17:45 EUnetHTA – what is it all about? Finn Børlum Kristensen, Director Danish Centre for Evaluation and HTA, National Board of Health, Denmark 17:55 How can new Member States benefit from a sustainable European HTA Network?
8
Norbert Wilk, Deputy Director for HTA and International Collaboration, Agency for HTA in Poland (AHTAPol), Poland 18:05 General discussion and concluding remarks October 5, 9:00-12:00 D. From innovation to healthcare practice 9:00 Session will be opened by Chair introducing the panel topics for the day and providing a brief summary of Thursday’s session. (10 minutes) 9:10 HTA seen from an industry perspective Maurice Wagner, Director General, Eucomed 9:25 Keeping track of rapidly developing technologies – the French experience Lise Rochaix, Board Member, Haute Autorité de Santé (HAS), France 9:40 Pricing and reimbursement for new health technologies – the role of HTA Stefaan van der Spiegel, Directorate General Enterprise and Industry, European Commission 9:55 Questions/comments from the audience 10:15 20 minutes BREAK E. HTA and public health 10:35 HTA and public health challenges Tit Albreht, Adviser to the Director, Institute of Public Health of the Republic of Slovenia 10:50 Quality of health care and HTA Jan Bultman, Lead Health Specialist, World Bank, Europe and Central Asia Region 11:05 Q&A/General discussion 11:45 Concluding remarks for the Forum Report: Parallel Forum F3 European HTA: From research to policy – Health Technology Assessment as a bridge October 4-5, 2006 Bad Hofgastein, Austria General view, framework Health systems over the globe face ever increasing competition for resources at the same time as technological innovation accelerates and citizens live longer. Citizen participation in decision-making cannot ignore the necessity to prioritise scarce resources across competing priorities. Knowledge transfer across borders and disciplines intensify and require integrated approaches that allow decision-makers at different levels to successfully deal with the complex pressures they face. HTA was developed as an effective tool to assist in informing healthcare planning and decision-making on complex issues based on research. HTA is an interdisciplinary process that brings together the clinical expertise of professions and systematic and rigorous assessment of the research base with organisational
9

and health economic analysis, and assessment of wider consequences for the individual and society. It takes in evidence multidisciplinarity, pragmatism, and policy orientation - and recognises that results of research are necessary yet not sufficient to inform decisions. The aim to inform decision-making necessitates the early involvement of various stakeholders’ perspectives from the very start and throughout the HTA process. The European network for Health Technology Assessment, EUnetHTA, will seek HTA stakeholders’ involvement to increase responsiveness of the HTA process to their needs. General Recommendations/Conclusions: 1. HTA is a tool to inform the formulation of safe, effective and efficient health policies, investment
decisions and quality health services that are patient focused, seek to achieve best value, and promote patient access to innovative and effective health technologies.
2. A focal point, for sharing knowledge and supporting coordinated HTA from the Members States respecting national and regional differences should be established on a permanent basis.
3. The stakeholder groups contributing to production or use of HTA reports should actively interact with those entities establishing the European HTA network and provide their views and constructive comments fostering responsiveness and transparency of HTA processes in Member States.
4. The European network for HTA (EUnetHTA) should contribute to the development of the high quality of HTA methodology and practical tools with increased general applicability across European borders, including New Member States.
5. EU and Member States should invest in the development of a permanent European HTA collaboration mechanism beyond 3-year project period (2006-2008).
Closing remarks Health policy planning operating under budgetary constraints requires structured, transparent and research based input generated by several disciplines. The European Health Technology Assessment Forum that gathered wide spectrum of stakeholders confirmed the potential of health technology assessment to deal with complex issues faced by decision makers in health care. Introduction of technologies simultaneously in several countries and knowledge transfer across borders highlight the need for European solutions. Maturity of HTA methods at a European level has reached the point that it is deemed possible to answer needs expressed by Member States and EU Commission to transform existing cross-border collaboration into a sustainable network. Stakeholders agreed that to ensure responsiveness and effectiveness of the European HTA process EU and Member States should support a permanent and sustainable European HTA collaboration mechanism after the end of the project period. Such mechanism should also offer avenues for supporting non member states in Europe.
10

Annex WP6.6
11
Annex WP7.2 First E-meeting WP7 - strand A Tuesday 26 September, 10.00-11.30 Minutes Present: Elena Berti, Sophie Blanchard, Julia Chamova, Karla Douw, Mads Frellsen, Teresa Gasparetto, Setefilla Luengo-Matos, Sun Hae Lee Robin, Francesco Martelli, Kersti Meiesaar, Celine Moty-Monnereau, Esther Pensado, Fabienne Quentin, Eva Turk The presentation (power-point) and the survey questions (asked during the E-meeting) are available on
the WP7 Extranet.
Two main issues were raised during the E-meeting and will be discussed further during the workshop
1. How are strands A and B articulated? What is the position of strand A in relation to Euroscan? Monitoring (strand A) deals with which stage of the life cycle of a health technology? These points will be clarified and discussed further during the workshop. For WP7 leaders, strand B focuses on a stage in the life cycle of a health technology that is upstream
from strand A. Strand B deals with identifying new/emerging technologies and establishing priorities.
The work is carried out in collaboration with the University of Birmingham (the member of Euroscan
hosting the Euroscan secretariat).
Strand A focuses on new health technologies after their introduction into the healthcare system (i.e. after market authorization and/or decision to reimburse). 2. What are the concrete objectives of strand A in 2007 (main objective : “development and implementation of shared monitoring tools”) To set up a common monitoring study in the space of just one year may be too ambitious. It may not
be possible to obtain the legal authorizations required to exchange data on individual patients within
this space of time.
It may be preferable to concentrate on identifying ways of sharing resources and information, including on existing monitoring systems.
Common tools could be developed as well as a common database on the EUnetHTA website.
Technologies already monitored in some countries could be chosen as case studies to test common tools developed by WP7 partners.
12

Annex WP7.3
13
Annex WP7.3
WP7 meeting: Focus on Strand A
14-15 November 2006 Hotel Husa los Seises, Sevilla
Agenda
13

Tuesday 14th November
11.00 – 12.30 Registration
12.30 – 13.30 Lunch at Hotel Restaurant
13.30 – 14.00 Welcome
Welcome speech
Sun Hae Lee-Robin
Agenda Céline Moty-Monnereau
14.00 – 15.30
Developing a common understanding of Strand A (WP7)
Overview of WP7 Céline Moty-Monnereau
Principles underlying Strand A Sun Hae Lee-Robin
Monitoring systems for new technologies in Europe Fabienne Quentin
Group work: Learning from others
15.30 – 15.50 Coffee break
Feedback from group work
Work in pairs: Agreement on final definitions
Final debriefing; schedule for the next day Sun Hae Lee-Robin
17.30
End of session
14
Wednesday 15th November
8.30 Proposals for common tools
More results from partners on a common tool Fabienne Quentin
Group work: Work on tools
Feedback from group work
10.20 – 10.40 Coffee break
Choice of technologies to test the common tools Fabienne Quentin / Céline Moty-Monnereau
Improvement of the strand A overview (document) All
WP7 strand B: Work in progress Claudia Wild
Next steps Strand A Sun Hae Lee-Robin Next steps Strand B Claudia Wild
12.30
Lunch
15
EUnetHTA - WP7 meeting 14-15 November 2006 Hotel Husa los Seises, Sevilla List of participants Name
Agency, Country
Partner
Sun Hae Lee-Robin Céline Moty-Monnereau Fabienne Quentin Sophie Blanchard
HAS, France LP (strand A)
Claudia Wild Rosemarie Felder
LBI-HTA, Austria LP (strand B)
Finn Borlum Kristensen
DACEHTA Project Leader
Anne-Florence Fay
CEDIT CP
Dagmar Luehmann
Institute for Social Medicine, Luebeck AP
Eduardo Briones
AETSA, Spain AP
Elena Berti
ASR, Italia AP
Emma Gutiérrez de Mesa
IPTS-SAFH Invited
Eva Turk
Institute of Public Health, Slovenia AP
Gaizca Benguria
OSTEBA Invited
Iga Lipska
AHTAPol CP
Inaki Guierrez-Ibarluzea
OSTEBA, Spain AP
Inger Natvig Norderhaug
NOKC, Norway AP
Kathrin Peter
SNHTA, Switzerland CP
Kersti Meiesaar
University of Tartu, Estonia AP
Leonor Varela Lema
Galician HTA agency CP
Mads Frellsen
DACEHTA, Denmark AP
Mairin RYAN
IHIQA, Ireland AP
Michael Barry
IHIQA, Ireland AP
Setefilla Luengo-Matos
AETS, Spain AP
Teresa Gasparetto
Regione Veneto, Italia AP
Tobias Schulte in den Bäumen
DZPHG (PHGEN) CP
Victor Sarmiento AETSA, Spain AP
16

Annex WP7.4
Notes from Work Package 7 Meeting November 14th and 15th, 2006 Hotel Los Seises Seville
Participants Elena Berti (ASR Italy), Eduardo Briones, Victor Sarmiento, Leda Ojeda Florido (AETSA Spain), Setefilla Luengo-Matos (AETS Spain), Iga Lipska (AHTAPol Poland), Leonor Varela Lema (Avalia-t Spain), Anne-Florence FAY (CEDIT France), Finn Børlum Kristensen, Mads Frellsen (DACEHTA Denmark) Hans-Peter Dauben (DAHTA@DIMDI Germany) Tobias Schulte in den Bäumen (DZPHG,PHGEN Germany), Sun Hae Lee Robin, Céline Moty-Monnereau, Fabienne Quentin, Sophie Blanchard (HAS France), Eva Turk (Institute of Public Health Slovenia), Dagmar Luehmann (Institute for Social Medicine, Luebeck Germany), Claudia Wild, Rosemarie Felder (LBI-HTA Austria), Inger Natvig Norderhaug (NOKC Norway), Iňaki Gutiérrez-Ibarluzea (OSTEBA Spain), Kathrin Peter (SNHTA Switzerland), Kersti Meiesaar (University of Tartu Estonia) Guests Emma Gutierrez de Mesa (IPTS-SAFH Spain), Gaizca Benguria (OSTEBA Spain) Slides and papers P-P slides and papers are available on the WP7 extranet. Developing a common understanding of strand A (WP7) Overview of WP7 The strand A will focus on the diffusion (rather than the development) of new (rather than emerging) technologies. On the contrary, the strand B will focus on the development of emerging technologies. Learning from others It appeared to all that there are many differences and few similarities between countries as far as the understanding and experience of monitoring systems are concerned. Some suggested to have a common understanding of the purposes of the monitoring system rather than of the definition itself. The question of the inclusion of vigilance systems in the WP7 definition of a monitoring system did not lead to a consensus. Based on the discussion, the leaders decided to give a large definition of a monitoring system and to precise the purposes (as far as the WP7 is concerned):
17

Definition Set of tools for generating and collecting data on health technologies for their assessment from the stage of introduction into the healthcare system until the stage of broader diffusion
Purposes
- To collect more evidence on effectiveness (eg for a decision on Coverage) - Description of the real life use (eg : to check the utilisation of the
technology under the approved conditions of use : indications, environment, learning curve, volumes, …)
Methods For both purposes, the method can be either sharing existing data or collecting new data prospectively. Towards common tools What can we share ? For the work in group discussions it appeared that :
- It is necessary to establish a core set of data which are not context related and could be collected and exchanged. The WP4 could be contacted to identify the data that are not context related thus would be easily usable by others.
- Depending on the countries : aggregated data or results (analysed data) could be exchangeable thus allowing countries to use unpublished data.
Which common tools ? For the work in group discussions it appeared that :
- The partners agreed on four common tools: - process on agreement on monitoring a common technology and on sharing data, - definition of a core set of data for the prospective monitoring , - specifications on the standard format of the files - and an interface on the EUnetHTA website to exchange information.
- Some partners suggested that we share information on the difficulties we met while setting up a monitoring system in our country.
Choice of technologies Partners were invited to give names of technology for which - either they could give data that they already have to other partners - or they would like to set up a monitoring system to collect new data based on the same core protocol. At the end of the “post-it activity”, it appears that four technologies could be identified with 2 to 3 partners being interested in collecting new data : Coronary CT scanning, Kyphoplasty, Anti-cancer drugs and Drug eluting stents. As some partners answered that they had data for two of these, the leaders choose to propose these technologies for sharing data : Anti-cancer drugs, Drug eluting stents. Please see the Excell files. A round Delphi will be done after the workshop to check and precise the partners’ answers and collect additional names of technologies if necessary.
18

Strand B The strand B had to wait for the discussions in the Euroscan meeting in Birmingham (November 20th 2006). Euroscan members decided that Euroscan will participate () in the next steps of developing the pilot of a EU-wide Emerging Tech Newsletter within the EUnetHTA project. Now a copyright expert has been asked to "reflect" upon shared editorship and disclosure statements. During the workshop, the partners were asked to choose between three drafts of newsletter. The result was in favor of the layout with the image. Next steps: signing of the contract with University of Birmingham (2006) and development of pilot newsletter (early 2007) that will be sent to APs for evaluation. Issues raised at the meeting linked with other work packages WP4 : for the identification of the core set of data WP2 : for the specifications on the standard format of the files for the development of an interface on the Intranet to exchange data and information Next steps Mini round of e-mails to enable convergence on the choice of technologies for the pilot phase. To send out 15/12/06 – 1 week deadline. E-mail members who did not attend the meeting. Information of the WP2 and WP4 about our developments and demands. Revisions of the new version of the strand A overview (including the annexes) : questions sent out by Fabienne Quentin week of the 18th of December : deadline for members ideas and corrections : January 15th 2007. Mid-January : allocation of the tools and indicators (to be developed) to group of members – 2 weeks deadline E-meetings in February to discuss on the developed tools within each group. March : tools sent out to all partners for comments and identification of indicators for the evaluation – 2 weeks deadline Workshop : 12/13 April 2006 in Ireland Proposed agenda for the strand A : final validation of the tools and indicators before testing
19

20
Annex WP8.1
WP8. Systems to support Health Technology
Assessment (HTA) in member states with limited institutionalisation
Review on HTA organisations
Catalan Agency for Health Technology Assessment and Research (CAHTA)

INDEX 1. INTRODUCTION .................................................................................................. 22 2. OBJECTIVES ....................................................................................................... 25 3. METHODOLOGY.................................................................................................. 26
3.1 To describe the characteristics of HTA organizations the main information sources were: ........................................................................................................... 26 3.2 To elaborate a list of HTA organizations and to realise a pilot test with a 7% of them about the information that could be collected from their web pages:............... 26 3.3 To summarize the Health Systems of the European countries, information included were:........................................................................................................... 26
4. RESULTS ............................................................................................................. 29
4.1 Characteristics of INAHTA members review ...................................................... 29 4.2 HTA organisations identification and review of their web pages................... 33 4.3 HTA in the Context of Health Care Systems in the European Region................ 35
5. ANNEXES............................................................................................................. 38
ANNEX 1.- Collaborative organisations in different WP ........................................... 38 ANNEX 2.- Main objectives of the eight work packages of EUnetHTA project......... 40 ANNEX 3.- Main characteristics of the HTA agencies. Data extracted from the technical specification of INAHTA members............................................................. 41 ANNEX 4. List of the HTA organisations identified in the search ............................. 64 ANNEX 5. Characteristics of European Health Care Systems ................................. 67 ANNEX 6. BIBLIOGRAPHY...................................................................................... 69
21

1. INTRODUCTION
Health technology assessment (HTA) 1 seeks to inform health policy makers by using the best scientific evidence on the medical, social, economic and ethical implications of investments in health care. Technology is broadly defined to include the drugs, devices, medical and surgical procedures used in health care, as well as measures for prevention and rehabilitation of disease, and the organisational and support systems in which health care is provided. With regard to the type of evaluated technology health procedures are most assessed, following medical devices and pharmaceuticals 2 whereas preventive and health promotion interventions are still under-represented. Assessment includes:
1. Identifying evidence, or lack of evidence, on the benefits and costs of health interventions 2. Synthesising health research findings about the effectiveness of different health interventions 3. Evaluating the economic implications and analysing cost and cost-effectiveness 4. Appraising social and ethical implications of the diffusion and use of health technologies as well
as their organisational implications.
The main purpose of HTA is to facilitate efficient and equitable allocation of resources. Emerging new technologies as well as currently used technologies need to be properly assessed in order to ensure effectiveness, patient safety, promotion of public health, as well as optimal use of resources. Patients should be protected from ineffective health interventions. HTA is a valuable tool in this context that has been used for more than 25 years but during the past years the extent is growing 2 The significance of HTA has been also affirmed by the World Health Organisation. HTA organisations has been involved in the development of a network for “Health Evidence”. This network is the answer of the World Health Organisation of the growing need to get timely information for decision-making. Several HTA organisations are functioning currently as technical members in this network. It could be concluded that the impact of HTA on both clinical practice as well as policy making in healthcare can be significant. However, a recent study by 3 revealed that even in countries with well established HTA practice, as for instance Sweden, England Wales, France or Netherlands, the influence of HTA on policy making is still marginal and need to be promoted. Besides this, when new technologies emerge they need to be properly assessed. HTAs are currently undertaken in many EU Member States, often on the same topics and thus there is obvious overlap in activities. Similar research questions are often brought forward in different Member States at the same time. For this reason, more coordinated approaches to HTA could reduce duplication and waste and will increase the impact of HTA. Better coordination of HTA activities, and collaborative approaches to transfer of core HTA into health policy and guidance could achieve significant improvements in the health of EU citizens while helping to contain costs of health services and achieve greater value for money. The EU is in a strong position to foster and enable greater collaboration, and to formalise links Among member states and their respective HTA programmes.
Recently, the EU Commission initiated a High Level Group on Health Services and Medical Care as a means to take recommendations of the report on patient mobility reflection process further. One of the areas of their focus is HTA and it was concluded, that HTA has become “a political priority and there is an urgent need for establishing a sustainable European network on HTA”. Many EU Member States have national HTA agencies and others plan to establish them. In this situation a collaborative European network could help to provide reliable, timely and transparent information to underpin policy decisions.
Current HTA situation in European countries A review of the European current situation about HTA is summarised in table 1. Most of the European countries still don’t have formal HTA units or agencies. Among the EU members, only 13 of 25 countries count with formal HTA agencies or units. None of the applicant countries to the EU (4), and only Norway and Switzerland from the other 15 European countries count with a formal HTA unit or agency.
22
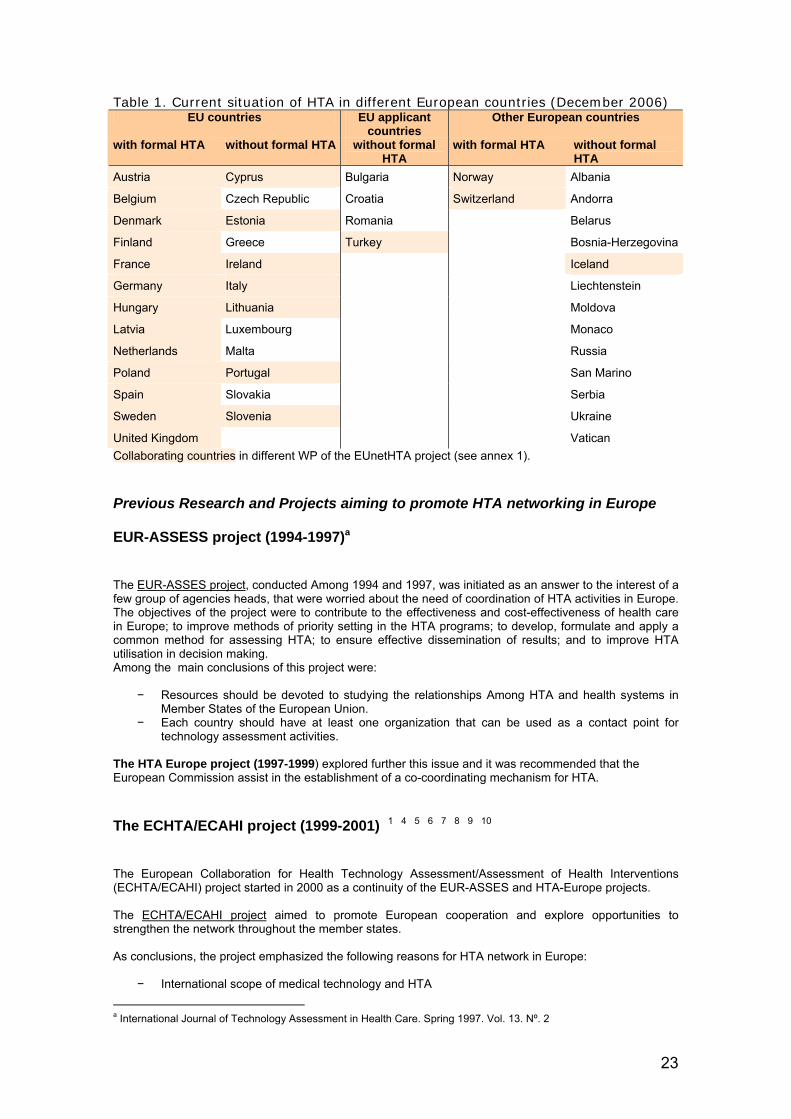
Table 1. Current situation of HTA in different European countries (December 2006) EU countries EU applicant
countries Other European countries
with formal HTA without formal HTA without formal HTA
with formal HTA without formal HTA
Austria Cyprus Bulgaria Norway Albania
Belgium Czech Republic Croatia Switzerland Andorra
Denmark Estonia Romania Belarus
Finland Greece Turkey Bosnia-Herzegovina
France Ireland Iceland
Germany Italy Liechtenstein
Hungary Lithuania Moldova
Latvia Luxembourg Monaco
Netherlands Malta Russia
Poland Portugal San Marino
Spain Slovakia Serbia
Sweden Slovenia Ukraine
United Kingdom Vatican Collaborating countries in different WP of the EUnetHTA project (see annex 1). Previous Research and Projects aiming to promote HTA networking in Europe EUR-ASSESS project (1994-1997)a
The EUR-ASSES project, conducted Among 1994 and 1997, was initiated as an answer to the interest of a few group of agencies heads, that were worried about the need of coordination of HTA activities in Europe. The objectives of the project were to contribute to the effectiveness and cost-effectiveness of health care in Europe; to improve methods of priority setting in the HTA programs; to develop, formulate and apply a common method for assessing HTA; to ensure effective dissemination of results; and to improve HTA utilisation in decision making. Among the main conclusions of this project were:
− Resources should be devoted to studying the relationships Among HTA and health systems in
Member States of the European Union. − Each country should have at least one organization that can be used as a contact point for
technology assessment activities. The HTA Europe project (1997-1999) explored further this issue and it was recommended that the European Commission assist in the establishment of a co-coordinating mechanism for HTA.
The ECHTA/ECAHI project (1999-2001) 1 4 5 6 7 8 9 10
The European Collaboration for Health Technology Assessment/Assessment of Health Interventions (ECHTA/ECAHI) project started in 2000 as a continuity of the EUR-ASSES and HTA-Europe projects. The ECHTA/ECAHI project aimed to promote European cooperation and explore opportunities to strengthen the network throughout the member states. As conclusions, the project emphasized the following reasons for HTA network in Europe:
− International scope of medical technology and HTA
a International Journal of Technology Assessment in Health Care. Spring 1997. Vol. 13. Nº. 2
23

− Use of same sources to compile evidence − Although every state must address the evidence into consideration with governmental priorities,
ethical and social implications of technology and issues of cost-effectiveness; evidence is the same for all countries.
As Eur-assess concluded, each country should have at least one organization that can be used as a contact point for technology assessment activities. In spite of this, after ten years of the formulation of this recommendation, 16 European countries still doesn’t count with formal HTA units. Networking in HTA in Europe should focus, Among other aims, in helping all the European countries to develop their own HTA organisation. Therefore, it’s important to work for make easier the building of new HTA organisations by providing them useful tools (establish the minimum components related to the scope, background, structure, process of work and visibility) and a education support.
The EUnetHTA project EUnetHTA builds on this previous EU supported HTA projects. Therefore, the EUnetHTA project wants to develop and implement tools to provide reliable, timely, transparent and transferable information on the effectiveness of health technologies as input to decision-making in Member States and in the EU.
EUnetHTA will facilitate transferability of reports among Member States by establishing “core” information about the effectiveness of technologies that can be shared among Member States, thus avoiding duplication of effort; outlining the cultural, economic, social and ethical issues to be considered in national contexts, and supporting and assessing the adaptation of national HTA report to other contexts. A clearinghouse facility will promote effective exchange and use of evidence based information. The project will include development of tools to improve the responsiveness of HTA to its consumers (a sustainable open EUnetHTA Forum with participation of main stakeholders will be established), pilot projects for different types of technologies and an evaluation of the network. The network will monitor emerging health technologies to identify those that will have greatest impact on health systems and patients and will support countries without institutionalised HTA activity. Thus, EUnetHTA includes eight work packages to achieve coordinated, rapid, influential HTA work informing health policy in all Member States. The main objectives of the eight WP of EunetHTA project can be consulted in annex 2.
Specifically, WP8, regarding the gap of HTA units or agencies in all the European countries, wants to study more in depth which are the most important characteristics an emerging HTA unit should take into account in order to establish itself. The knowledge of the main aspects related to the structure, scope, background, work and visibility of the HTA organisations will allow WP8 define the minimum components an HTA organisation needs and to conclude recommendations and the elaboration of tools to education support to institutions or healthcare systems in the process of evolving to/building an HTA organisation / capacity.
24

2. OBJECTIVES
1. To define the recommendable minimum components related to the scope, structure and the work process and visibility of a unit, agency, or program of HTA.
1.1 To conceptualise the main characteristics of the specific setting (healthcare system, sociocultural context, links with academia and healthcare decision makers, collaborations -past or current- with other countries as well as organization characteristics) which define different scopes and models of the HTA organizations 1.2 To identify and specify key components when defining the scope of a new agency, unit or program by means of the strategic and business plan, lines of activity, products/services portfolio and target stakeholders. 1.3 To characterize those essential elements defining an HTA organization in relation to the structure, background human profile (research, technician, assistant, etc. in different areas of expertise), infrastructure resources and funding.
1.4 To define key aspects of organizational visibility related to information and dissemination management strategies of the HTA products and services.
25
3. METHODOLOGY
In order to achieve the first objective of WP8 two strategies were decided:
− To carry out a review of HTA organisations at international level − To elaborate a survey of the active or in process of being an European HTA unit, agency or programme.
The report on the survey can be consulted in appendix 2. This report is focused on the review on HTA organisations Sampling frame (inclusion/exclusion criteria) Selections criteria for HTA agencies or units, gathering initial information were:
To belong to HTA networks (INAHTA members) Public organizations:
o Non for profit o Public funding > 50% budget o Relationship with local, regional or national government o Performing HTA
USA, Oceania; Europe, Asia, Canada and Russia. Information source:
3.1 To describe the characteristics of HTA organizations the main information sources were:
− INAHTA members − HTA organization web pages
3.2 To elaborate a list of HTA organizations and to realise a pilot test with a 7% of them about the information that could be collected from their web pages:
− INAHTA (International Network of Agencies for HTA) website − Websites of existing HTA units, agencies or programmes − Report on overview of the implementation of activities related to evidence based practice
in a broad representation of world health organization-collaborating centres, a survey conducted by the CAHTA (Catalan Agency for Health Technology Assessment and Research) in 2002 11
− Project report on review of International Health Technology Assessment (IHTA). National Institute for Clinical Excellence 2000. 12
− The status of health technology assessment worldwide. Results of an international Survey. MTPPI 1997. 13
− Other publications or reports describing the abovementioned characteristics of HTA units, agencies or programmes
3.3 To summarize the Health Systems of the European countries, information included were:
− financing of the system, − health care delivery, − organisational structure, − Health care model (Beveridge or Bismarckian)
The period of search, for the first two points, was between March and May of 2006 and for point 1.3 were from the year 1999 up to 2006, the latest.
26

Variables included
I. To describe the characteristics of HTA organizations the main information extracted o reviewed were:
− Country, name, year and foundation conditions, main mission, structure and relations, work process or activity areas, dissemination activities and general info (population served, current HTA budget, permanent staff and consultants).
II To elaborate a list of HTA organizations and to realise a pilot test with a 7% of them about the information that could be collected from their web pages:
− For the list: Organization name, country, web page, e-mail and telephone of contact and evidence of they were performing HTA activities.
− For the pilot test about the information available in the web pages: Contact details, Establishment of the centre (date, initiative, reasons, barriers and solutions), Specific setting of the organisation (for-profit / non-for-profit, profile, collaborations and collaborators, HTA supporting policy), Aims and scope of the organisation (Level of work, statuts and strategic plan, Main line of activity, Type of HTA and products, level of recommendations distribution, target groups for recommendations), Structure (government, nomination of governance members, staff –contractual situation and background-, sponsors, private funding, facilities and equipment), Work process (Priorities –who set them, criteria and process, advisory mechanisms-, barriers and solutions, aspects of HTA, frequency & criteria to assess impact, options on impact), Visibility of the results of the organisation (dissemination strategy & methods, Intenders users of results).
III Characteristics of Health Systems of European countries
To summarize the characteristics of Health Systems of European countries, information included were:
− Financing of the system, − Health care delivery, − Organisational structure, − Health care model (Beveridge or Bismarckian)
Analysis Information was collected in tables and a descriptive analysis of this data was conducted.
For the point 1.3 different classifications of health systems from previous approaches were taken into account:
Prior, within the framework of the EUR-ASSESS Project 4 (1997) health care systems of European countries were considered in the context of HTA. Within these studies eight, mainly Western European countries, were considered in the perspective of their principle models for arranging the benefit provision.
4 Jonsson E. International Journal of Technology Assessment in Health Care, 1997, 13 (2). Cambridge University Press.
27

Health care provision can be organised according:
a) the reimbursement model, b) the integrated model, and c) the contract model.
The models will be described as following: “The patient reimbursement model is characterised by the presence of a (…) compulsory or voluntary health insurance involving cash reimbursement of patients for all or part of the cost of medical care received” 5. A health care system in accordance to the integrated model involves a “compulsory or voluntary health insurance or third-party funding in which both the insurance and provision of health care is supplied by the same organization in a vertically integrated system” 6. In contrast to the contract model, which implies according the WHO (1998a) a “system of health service provision which involves contracts between three separate parties: a) the beneficiaries; or patients; b) the fund-holders or purchasers acting on behalf of the beneficiaries; and c) the providers of services” 7.
Another model regarding HTA, especially decision making in HTA, in the perspective of the health system environment was introduced by the OECD in 2005 14. According to that model two dimensions play a major role that should be considered while evaluating the environment for HTA. First, the level of regulation in the health care market, which can rank from highly regulated to free-market activity. Moreover, the involvement of the government in the health care system. On the one site of the scale it can be limited to purchasing the health care services and on the other end the government can be engaged directly in services provision.
Both of these models were taken as a basis for the selection of health system characteristics with relevance for the country’s commitment in HTA. These characteristics concern the financing of the system, the health care delivery, and its organisational structure, which involves also the Beveridge8 or the Bismarckian9 model.
Due to the extensive approach in terms of the geographical scope of this project, this analysis sought to include nearly all countries in the European region, which can be found also in table 1 in the introduction of this report10 . Not considered were Belarus, Serbia, and Ireland because either no report were available from the European Observatory on Health Systems and Policies about these countries or the population seize were regard as to be too small as in case of Andorra, Vatican, San Marino, Monaco and Liechtenstein. 37 countries of the European region were considered and separated in those with formal HTA in place (15) and those without (22). The classification in EU countries and EU candidate countries as well as other countries in the European regions aimed to identify further associations.
5 According OECD (1992), cited in the glossary of the European Observatory on Health Systems and Policies”, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07. 6 According OECD (1992), cited in the glossary of the European Observatory on Health Systems and Policies”, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07. 7 According WHO (1998), cited in the glossary of the European Observatory on Health Systems and Policies”, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07. 8 A health care system organized according the Beveridge model implies a “system of social security and health services arising out of the Beveridge report in England and Wales, first published in 1943 this report recommended provision of health car for all people through central taxation and other compulsory financial contributions and that a system of universal benefits should give support during unemployment or sickness and after disability and retirement. The national Health Service act of 1946 established the provision of services, free-of-charge, for the prevention, diagnosis and treatment of disease” (According WHO, 1998a, cited in the glossary of the European Observatory on Health Systems and Policies”, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07). 9 Health care systems according Bismarck is defined as “A system of national social security and health insurance introduced in the 19th century German empire under the then Chancellor Bismarck. This system is a legally mandatory system for the majority or the whole population to obtain health insurance with a designated (statutory) third-party payer through non-risk related contributions which are kept separate from taxes or other legally mandated payments” (Glossary of the European Observatory on Health Systems and Policies, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07). 10 Austria, Belgium, Denmark, Finland, France, Germany, Hungary, Latvia, Netherlands, Poland, Spain, Sweden, UK, Norway, Switzerland, Cyprus, Czech Republic, Estonia, Greece, (Ireland), Italy, Lithuania, Luxembourg, Malta, Portugal, Slovakia, Slovenia, Bulgaria, Croatia, Romania, Turkey, Albania, Bosnia- Herzegovina, Iceland, Moldova, Russia, Ukraine
28

4. RESULTS
4.1 Characteristics of INAHTA members review
INAHTA (International Network of Agencies for Health Technology Assessment) was established in 1993 with a main mission: to provide a forum for the identification and pursuit of interests common to health technology assessment agencies. The membership is open to those agencies or organisations that provide the following conditions:
− Assesses technology in health care − Is a non-profit organization − Relates to a regional or national government − Is funded at least 50% by public sources − Provide free access to their reports upon request
The available information of all the INAHTA members, in the period of search, were reviewed. Specifically, data of 39 agencies from 19 countries was collected as table 1 summarises. Table 1. Number of agencies being member of INAHTA for each country (May 2006)
CO
UN
TRY
Arg
entin
a
Aus
tral
ia
Aus
tria
Bel
gium
Can
ada
Den
mar
k
Finl
and
Ger
man
y
Hun
gary
Isra
el
Latv
ia
Net
herla
nds
New
Zea
land
Nor
way
Spai
n
Swed
en
Switz
erla
nd
UK
USA
Agencies number
1
3
1
1
5
2
1
1
1
1
1
3
1
1
6
2
1
5
2
A big variety in the year of establishment of the reviewed organisations was found. The reviewed agencies were founded Among 1902 and 2004, but most of them were established Among 1984 and 1999, specially in the first 10 years. Figure 1 shows the numbers of agencies established by years. The history and establishment of the organisations was also collected. Most of the agencies were founded under the auspices of the government. Nineteen of them declared itself as a governmental organisations in its establishment. Eleven more declared to be independent organisations at the current time. Two other state their semi-governmental condition, two more agencies declared to be academic organisations, and two more state themselves as governmental-academic organisations. About the mission/s of the organisations, in agreement with the previous outcome, 24 organisations state as its mission to advice / assess policy makers, or governments or stakeholders. Thirteen agencies defined their mission to improve health services, by looking for efficacy, equity, etc. For six organisations, to promote research and to educate and train professionals was their mission. Two organisations declared as their mission to develop Evidence Based Medicine (EBM). An agency, consider to maintain the public awareness in the efficacy of health technology.
29
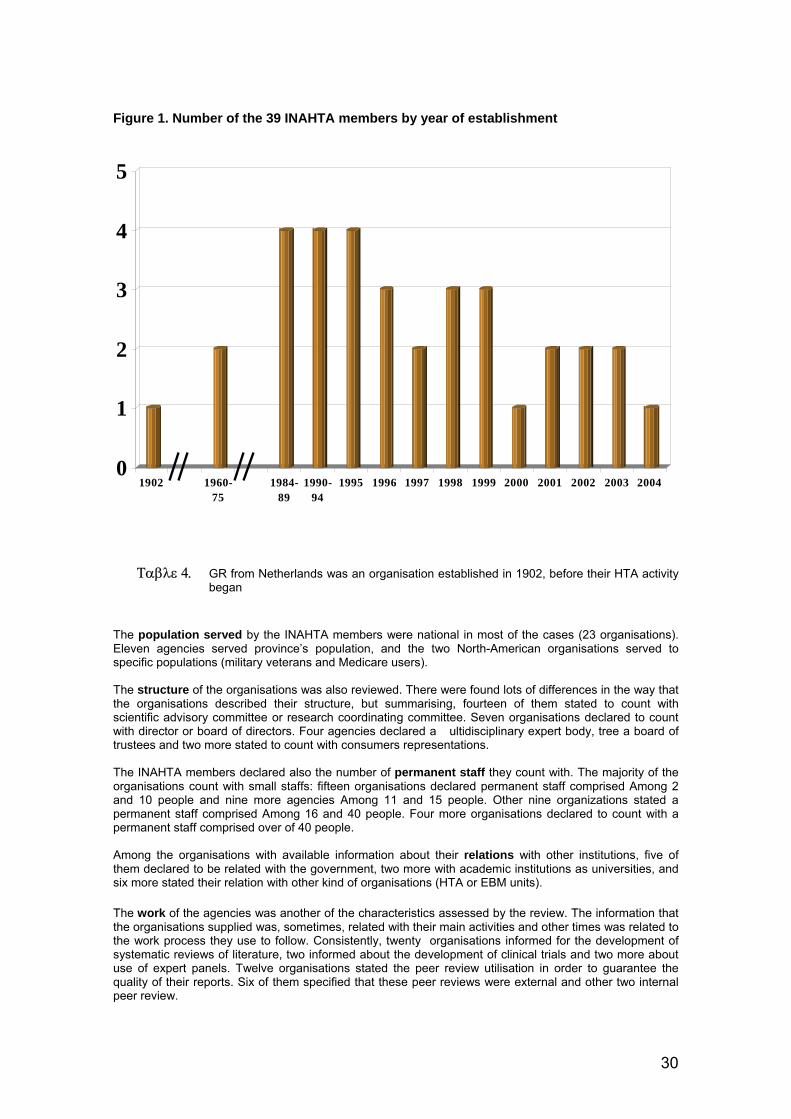
30
Figure 1. Number of the 39 INAHTA members by year of establishment
Ταβλε 4. GR from Netherlands was an organisation established in 1902, before their HTA activity
began The population served by the INAHTA members were national in most of the cases (23 organisations). Eleven agencies served province’s population, and the two North-American organisations served to specific populations (military veterans and Medicare users). The structure of the organisations was also reviewed. There were found lots of differences in the way that the organisations described their structure, but summarising, fourteen of them stated to count with scientific advisory committee or research coordinating committee. Seven organisations declared to count with director or board of directors. Four agencies declared a �ultidisciplinary expert body, tree a board of trustees and two more stated to count with consumers representations. The INAHTA members declared also the number of permanent staff they count with. The majority of the organisations count with small staffs: fifteen organisations declared permanent staff comprised Among 2 and 10 people and nine more agencies Among 11 and 15 people. Other nine organizations stated a permanent staff comprised Among 16 and 40 people. Four more organisations declared to count with a permanent staff comprised over of 40 people. Among the organisations with available information about their relations with other institutions, five of them declared to be related with the government, two more with academic institutions as universities, and six more stated their relation with other kind of organisations (HTA or EBM units). The work of the agencies was another of the characteristics assessed by the review. The information that the organisations supplied was, sometimes, related with their main activities and other times was related to the work process they use to follow. Consistently, twenty organisations informed for the development of systematic reviews of literature, two informed about the development of clinical trials and two more about use of expert panels. Twelve organisations stated the peer review utilisation in order to guarantee the quality of their reports. Six of them specified that these peer reviews were external and other two internal peer review.
0
1
2
3
4
5
1902 1960-75
1984-89
1990-94
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
31
As the main activities, Horizon scanning (4 agencies), guidelines (3 organisations), quick response (4 agencies), briefs reports (4 organisations), education and training (4 agencies), commissioned research (2 organizations) were reported. The number of consultants stated was very variable from 2 to 300. Among the dissemination strategies the most frequently mentioned was the use of their own web page (35 agencies). Newsletters (19 agencies), participation in seminars / congress (13 organisations), and printed reports (11 agencies) were, also, strategies frequently used for the INAHTA members. Seven organisations stated to publish their reports in journals, five declared to organise or attend meetings, tree stated to use the media, and two else to use INAHTA web page. An organisation declared to use on-line events to disseminate their results. The current HTA budget declared for the organisations was comprised Among 0,005 and 21,6 mil USD. Fifteen of the agencies declared budgets under 1,1 mil USD. Eleven organisations stated budgets Among 1,1 and 4 mil USD. Four more organisations declared budgets Among 4,1 and 17 mil USD. Another organisation stated a budget of 21,6 mil USD.
Panel remarks
The extraction of information was made in March of 2006, from then on is possible that the information of other new members could be incorporated on the INAHTA web page. Since INAHTA only accept those organisations which comply with their membership conditions, this review does not collect information about private agencies or those for-profit. The technical specification of the INAHTA members allows to consult rich information in relation with their main characteristics. Nevertheless, in the extent that this information was given by the organisations in an open answer, there were big differences Among the kind and extension of this data. Sometimes, the answer gave by agencies were referred to different nuances or, even, different ideas. Therefore, for example, when agencies answered the INAHTA question ‘How your organisation works?’ most of them gave an answer related to the main activities their organisation use to develop, and others gave information about the work process they follow to develop their work. All the information was not always available for all the agencies. For example, some of them explain their structure and relation with others organisations, conditions of their establishment, current budget, dissemination activities, but others didn’t do it. The information available on the INAHTA web page is just a summary and doesn’t reflect all the characteristics from their organisation members. The missing information was not always available in the web-page of these agencies.
Conclusions
− Since each organisation answered an open category, there was a big variety in the information about
the characteristics given by the organisations on the INAHTA web page − The variety in the information given for HTA organisations makes difficult to establish comparisons
Among them. − Data collected was not always clear enough to understand the characteristics of the organisations.
For example, most of the organisations talked about their activities whereas others explain their work process
− More information about the structure, scope, background, work process and activities, visibility, etc. is needed in order to study the characteristics of HTA organisations
− A list of possible questions for the WP8 survey was elaborated coming from the information given by the organisations and other sources (see survey report). These questions are summarised in table 2.
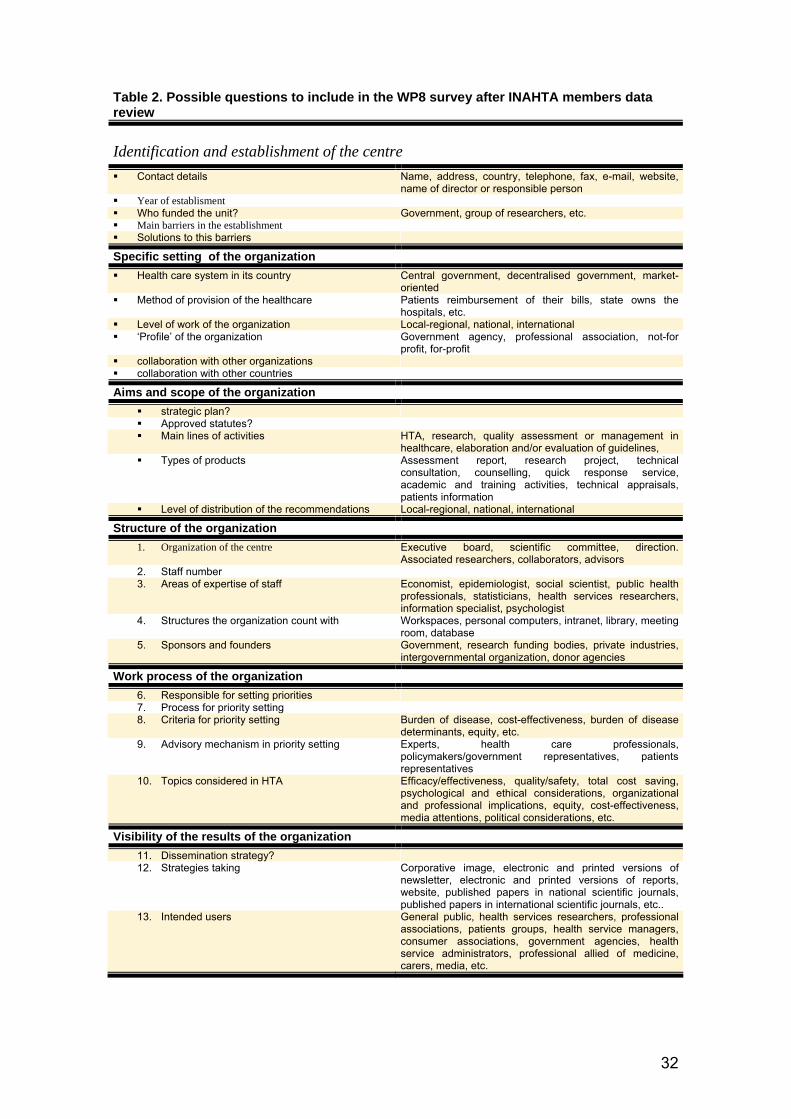
32
Table 2. Possible questions to include in the WP8 survey after INAHTA members data review
Identification and establishment of the centre Contact details Name, address, country, telephone, fax, e-mail, website,
name of director or responsible person Year of establisment Who funded the unit? Government, group of researchers, etc. Main barriers in the establishment Solutions to this barriers
Specific setting of the organization
Health care system in its country Central government, decentralised government, market-oriented
Method of provision of the healthcare Patients reimbursement of their bills, state owns the hospitals, etc.
Level of work of the organization Local-regional, national, international ‘Profile’ of the organization Government agency, professional association, not-for
profit, for-profit collaboration with other organizations collaboration with other countries
Aims and scope of the organization
strategic plan? Approved statutes? Main lines of activities HTA, research, quality assessment or management in
healthcare, elaboration and/or evaluation of guidelines, Types of products Assessment report, research project, technical
consultation, counselling, quick response service, academic and training activities, technical appraisals, patients information
Level of distribution of the recommendations Local-regional, national, international
Structure of the organization
1. Organization of the centre Executive board, scientific committee, direction. Associated researchers, collaborators, advisors
2. Staff number 3. Areas of expertise of staff Economist, epidemiologist, social scientist, public health
professionals, statisticians, health services researchers, information specialist, psychologist
4. Structures the organization count with Workspaces, personal computers, intranet, library, meeting room, database
5. Sponsors and founders Government, research funding bodies, private industries, intergovernmental organization, donor agencies
Work process of the organization
6. Responsible for setting priorities 7. Process for priority setting 8. Criteria for priority setting Burden of disease, cost-effectiveness, burden of disease
determinants, equity, etc. 9. Advisory mechanism in priority setting Experts, health care professionals,
policymakers/government representatives, patients representatives
10. Topics considered in HTA Efficacy/effectiveness, quality/safety, total cost saving, psychological and ethical considerations, organizational and professional implications, equity, cost-effectiveness, media attentions, political considerations, etc.
Visibility of the results of the organization
11. Dissemination strategy? 12. Strategies taking Corporative image, electronic and printed versions of
newsletter, electronic and printed versions of reports, website, published papers in national scientific journals, published papers in international scientific journals, etc..
13. Intended users General public, health services researchers, professional associations, patients groups, health service managers, consumer associations, government agencies, health service administrators, professional allied of medicine, carers, media, etc.

4.2 HTA organisations identification and review of their web pages In order to include information about the characteristics of interest (structure, work process, scope, visibility, etc.) of any type of HTA organisations at international level, besides of the INAHTA members review, a search of HTA units was conducted through different sources. At a first stage, a definitive list of HTA organisations was elaborated by merging the information from the different sources. It was necessary to improve this list because of the duplication of organisations and for the co-existing old and new names of a same HTA organisation. An excel document was elaborated. A search in internet was done in order to identify web pages, e-mails and telephone contacts of the HTA organisations and to find out if they were really performing HTA activities. From the 363 HTA organisations found, 174 were eliminated because different circumstances: for 64 of them was not possible to find a web page, for 53 organisations was demonstrated they didn’t perform HTA, other 57 organisations were duplicated in the different sources. The remaining 189 organisations can be consulted in annex 4. Once the list was finished, and in order to assess the information obtained from the HTA organisations web pages, a 7% of the organisations were selected by a randomised method. Thirteen web page organisations were reviewed in order to obtain all the information we wanted to collect with the last questionnaire draft. Table 3 summarises the results of this extraction of information. The 13 organisations selected were found in different sources. Five of them come from a international journal report (1997), 3 came from the NICE report, 2 from the WHO report, 2 from EUnetHTA list of partners and 1 from the INAHTA membership. Almost all the organisations gave information about their contact details. The second topic with more information available was the establishment of the centre, specially in relation with the date an initiative of establishment. None of the organisations explain their barriers in the building of the organisation. Just a few of the organisations gave information about their specific setting (organisation’s profile, collaborations, etc.) or about their aims and scope (statutes, target groups for their recommendations, customers, type of HTA and products, etc.). In relation with the structure half of the organisations gave information regarding their governance, and few about the nomination of the members of governance. Practically, none of the organisations gave information about their staff (contractual situation and background), funding, facilities & equipment The work process and the visibility of results of the organisations were the two topics with the poorest information available on web pages. Related to the work process, none of the organisations gave information about their priorization process, the strategies to guarantee the quality of their products, or the frequency and criteria used to assess the impact of their recommendations. About the visibility of their results, none of the organisations gave any information about their dissemination strategy and methods or about the intenders users of their results.
33

Table 3. Information available in the web pages of a randomised sample of the organisations identified Concept
N. of centres
Classification by source Contact details: 12 Establishment of the centre:
- Date establishment: 10 (1 EUnetHTA & 1 WHO not) - Initiative: 7 (2 IJ97, 1 EUnetHTA , 1 WHO & 1 INAHTA not) - Reasons establishment: 1 (1 IJ97)
- Barriers and solutions: 0 ______
Specific setting of the organization: - For profit/not-for-profit: 4 (2 NICE, 1IJ97 & 1 WHO)
- Organization’s profile: 5 (1 IJ97; 2 NICE & 1 WHO)
- Collaborations & collaborators: 2 (1 NICE & 1 INAHTA)
- HTA supporting policy: 0 ______
Aims and scope of the organization: - Level* of work 5 (2 IJ97, 1 NICE, 1 WHO & 1 EUnetHTA)
- Statutes or strategic plan: 0 ______
- Main line of activity: 3 (2 NICE & 1 INAHTA)
- Type of HTA: 3 (2 IJ97 & 1 INAHTA)
- Type of products: 4 (2 IJ97, 1 WHO & 1 INAHTA)
- Customers: 3 (2 IJ97 & 1 NICE)
- Level* recommendations distribution: 3 (2 IJ97 & 1 INAHTA)
- Target groups recommendations: 2 (2 IJ97)
Structure of the organization: - Governance organization: 7 (3 IJ97, 2 NICE, 1 EUnetHTA & 1 INAHTA)
- Nomination of members governance: 3 (2 IJ97 & 1 NICE)
- Staff, contractual situation & background: 1 (1 INAHTA)
- Sponsors, private funding: 0 ______
- Facilities & equipment: 0 ______
Work process of the organization: - Who set priorities: 0 ______
o Criteria: 1 (1 IJ97) o Process, advisory mechanisms: 0 ______
- Barriers & solutions: 0 ______
- Aspect for HTA: 1 (1 IJ97)
- Quality of products: 0 ______
- Frequency & criteria to asses impact: 0 ______
- Opinions on impact: 0 ______
Visibility of the results of the organization: - Dissemination strategy & methods: 0 ______
- Intended users of results: 0 ______ * Level.- (national, local, etc.) Conclusions − The information obtained from the web pages of HTA organisations is very variable among them, so
some times it’s not possible to make comparisons to analyse the information − Nevertheless, information about work process, visibility of results, structure, scope and background of
the organisations is not available in most of the web pages reviewed − Since HTA organisation’s web pages don not explain much about the important and necessary
information to achieve WP8 objectives and the available information will probably difficult the comparison, web pages don’t seem to be a good source for extracting this information
− WP8 survey seems to be the better option to obtain good information about the characteristics of HTA organisations
− It is easier to find information about contact details and history of the establishment of the organisations in organisation’s web pages, so web pages are a nice source to obtain information about contact people and e-mail address for WP8 survey.
34

4.3 HTA in the Context of Health Care Systems in the European Region Countries with formal HTA Even though the type and level of activity are varying immensely, evidence of high quality evaluation activity can be found in all EU countries 15. However, formal Health Technology Assessment are currently in place in not more than 15 countries in the European Region with 13 of them being a member of the European Union. Well established formal HTA can be found across Scandinavia and Western European countries and furthermore, in a very small number in the Eastern European part (Hungary, Latvia, Poland). Among those with formal HTA, seven countries finance their health care system predominantly through taxation (Denmark, Finland, Latvia, Spain, Sweden, UK, Norway), eight by means of mandatory health insurances (Austria, Belgium, France, Germany, Hungary, Netherlands, Poland, Switzerland). Consequently, both the Beveridge as well as the Bismarckian systems is in virtually equal shares in place in such countries. Likewise the distribution in terms of the supply of health care services. In about half of these countries the state plays a dominant role in health care with respect to the service provision.
Among the Eastern European countries Hungary and very recently Poland have introduced formal HTA. Both of these countries have undergone efforts to decentralise their system. Moreover, purchasing and provision were separated. Both countries reverted to a health care system following the Bismarckian principle, which were already in place before the Second World War. A national health insurance fund was introduced and contracted as a third party payer with providers. Latvia as another example of an Eastern European country formerly organised according the Semashko11 model has introduced formal HTA. Latvia established in 1998 a State Compulsory Health Insurance Agency, even though the health care budget continues to be financed through taxation. However, Latvia has adopted the contract model and has strived for a decentralized health care system12 Countries without formal HTA Countries that haven’t introduced formal HTA yet are predominantly Central and Eastern European countries, South-Eastern European countries respectively, as well as Greece, Ireland, Italy, Malta and Portugal. The majority of the Eastern and Central European countries are in a phase of transition after the abolishment of the former centrally-organized Semashko-modelled system with its determined responsibilities. The bulk of countries of such countries tend to develop rather towards a decentralised and contract model of social health insurance. Even though they are approaching the Bismarckian system in terms of characteristics as the payer-provider split and consequently, the existence of third party payers, they have been evolved in their particular context and differ though from Bismarckian systems of Western European countries . However, in both groups, countries with or without formal HTA, hospitals are mostly under the ownership and guidance of the state. In many cases the state functions as the main service provider.
EU countries without formal HTA Among the countries that are pertaining to the European Union are Cyprus, Czech Republic, Estonia, Greece, Ireland, Italy, Lithuania, Luxembourg, Malta, Portugal, Slovenia and Slovakia that haven’t established formal HTA. However, there are some countries showing increasingly interest in HTA. In particular Portugal were a formal HTA agency is being planned 13, but also Luxembourg, and recentlySlovenia and Italy are becoming more aware that HTA may help to be better informed about the consequences of the application of health technologies.
The Portuguese health system is predominantly funded through taxation. Additionally, in Portugal are, besides private insurance schemes, health subsystems in existence that cover about 25% of the population and are mainly funded by employers and employees14. The public sector has a predominant role in terms of service provisions by hospitals and general practitioners. Decentralization efforts have been undergone but not achieved its targets yet 14
11 “A uniform model of organizing health services introduced in CEE/CIS countries after the Second World War, and abolished in the early 1990s. Financing of health services is entirely through the state budget, with publicly owned health care facilities and publicly provided services. Different levels of state administration—central, regional, and local—were responsible for planning, allocation of resources and managing capital expenditures” (According Saltman et al., 1998, cited in the glossary of the European Observatory on Health Systems and Policies”, http://www.euro.who.int/observatory/Glossary/TopPage, last accessed 09.01.07). 12 Karaskevica J, Tragakes E. Health Care systems in Transition. European Observatory on Health Care Systems, 2003.
13 R. Busse, (2005) “HTA in Europa: Verhaeltnis zur Politik, Verankerung, Impact”, Presentation in Bad Nenndorf 11.10.2005, http://www.mig.tu-berlin.de/files/2005.lectures/2005.10.11rb_BadNenndorf.pdf, last accessed 10.01.07. 14 Allin S et al. Snapshots of health systems. European Observatory on Health Systems, 2005
35

Another example of an EU country without formal Health Technology Assessment but growing interest in HTA is Luxembourg. The health system of the smallest member state of the European Union is financed by a health insurance that is compulsory for all employees and self-employed residents. Luxembourg has a technology resource centre called SANTEC, which conducts HTA studies based on specific requests from the Ministry of Health Department of Curative Medicine and the Department of Radioprotection 15 . Italy has established assessments units (embedded in academic institutions) in as for instance in Venezia but the amount of HTA related research differs greatly across the country 15. That could be explained with the fact that in Italy a great deal of responsibility for public health care lies within the regions and even lower-level purchaser and provider organisations enjoy more autonomy due to the process of decentralisation of the National Healthcare System. Italy’s health care system is half tax funded with third party payers making up the reminder. Moreover, as also presented in the annex, some Italian units are engaged also in the EUnetHTA project. The former Yugoslavian country Slovenia has demonstrated great interest in the establishment of formal HTA since is actively collaborating with the European project EunetHTA. The Slovenian health care system, remains still relatively centralized although it is transforming towards a system according Bismarckian lines. It is predominantly financed through the statutory health insurance, which covers virtually the entire population 11. EU applicant countries without formal HTA Three of the four countries (Bulgaria, Croatia, Romania) that are applying for the membership to the European Union have organised their health care system with tendency towards a Bismarckian system and adopted the contract model. Among the applicant countries only Turkey’s health care system is characterized by an integrative organisation.
Another country that recently expressed high interest in establishing formal HTA through seeking actively support from other HTA agencies is Romania. Romania’s health system had transformed from a former tax-based and centralized health system according Semashko lines into a decentralized and pluralistic social health insurance system, with contractual relationships between health insurance funds as purchasers and health care providers 16.
The following graphic aims to give an overview of the characteristics of European countries that are relevant concerning the countries` commitment in HTA. The graphic is based on data summarised in a table (see annex 5).
15 Wagener R. Health Technology Assessment in Luxembourg. International Journal of Technology Assessment in Health Care, 16:2 (2000):475-84.
36

Figure 2. HTA in the Context of European Health Care Systems
02468
1012141618
With formal HTA Without formalHTA
Tax funded
Third party payer
State is main serviceproviderContract Model
Integrated Model
Reimbursement Model
With respect to this graphic it must be mentioned that the compilation of the overview posed some problems regarding the classification. One reason is that the greater part of the countries is in structural transition. Regardless the fact, that is was not always possible to find concrete data allowing to allocate strictly the country to one of the pertaining characteristic, these data are not complete, additionally, overlapping was not fully avoidable. Nonetheless, since numerous of countries were involved, a summary of the detailed data appeared to be indispensable for providing an overview.
Conclusions
− There is a enormous need to promote the establishment of HTA across Europe since among 37 European countries that were considered in this study, formal HTA is in place in only about 40 % (15 countries) whereas the majority of them are EU member states (13 countries).
− Particular support with respect to the introduction of formal HTA should be dedicated to Eastern and Central part of Europe as not more then three countries have introduced formal HTA..
− The presence of formal HTA is neither associated with the health care services being financed predominantly through taxation nor by social insurance contributions. Both models are practically equally distributed among countries with formal HTA in place.
− Health care systems of numerous countries are in enormous structural transition involving the introduction of the payer-provider split with elements of a market driven health care. Due to this fact the need for of cost-containment and quality assurance arises which can be an incentive for introducing HTA
− Those countries in the Eastern and Central part of Europe that are in transition after the abolishment of the Semashko system have a special support need since this organisation didn’t demand any attentiveness to effective health care provision.
37

5. ANNEXES
ANNEX 1.- Collaborative organisations in different WP
Country Organisation WP Austrian Academy of Sciences-Institut für Technikfolgen-Abschätzung (ITA) 1.5.7
Austrian Health Institute 4,5
Austria
Hauptverband der Ósterreichischen Sozialversicherungsträger 5,6,8,
Belgium Health Care Knowledge Centre (KCE) 2,4,5,6
Cyprus Ministry of Cyprus 2,8
Centre for Applied Health Services Research and Technology Assessment, University of Southern Denmark (CAST)
6,8
Danish Institute for Health Services Research (DSI) 4,5,6
Danish Centre for Evaluation and HTA (DACEHTA) 1,2,4,5,6,7
Denmark
HTA Unit, Aarhus University Hospital 5,6,8
Estonia University of Tartu, Department of Health 4,5,6,7,8
Finland Finnish Office for HTA (FinOHTA) 1,4,5,6
Haute Autorité de Santé 1,2,5,7 France
Assistance Publique-Hôpitaux de Paris, Direction de la Politique Médicale, Comité d’évaluation et de diffusion des innovations technologies
6,7
German Agency for HTA at the German Institute for Medical Documentation and Information (DAHTA@DIMDI)
1,2,3,5,6
Institute for Social Medicine, Medical University Luebeck 4,7
Technische Universität Berlin, Department Health Care Management 4,5,6
Centre of competence for clinical studies Bremen 6,7
Gernan HTA Association (CP) 8
Institute for Quality and Efficiency in Health Care (IQWIG) 6,8
Germany
German Centre for Public Health Genetics (DZPHG) 5,6,8
Hungary Centre for Public Affairs Studies Foundation. Corvinus University of Budapest.
2,8
Iceland University of Iceland 4,5,6,8
Ireland Interim Health Information and Quality Authority 6,7
Agenzia Sanitaria Regionale, Emilia Romagna 2,3,5,7
Università Cattolica del Sacro Cuore, Policlinico universitario “A Gemelli”. 4,5,6,7,8
Italy
Regione Veneto 2,3,5,7
Latvia Health Statistics and Medical Technology State Agency 3,8
Lithuania Ministry of Health 4
CVZ College vor zorverzekeringen 6,7
Health Council of the Netherlands 7
Netherlands
The Netherlands Organisation for Health Research and Development 4,5
Norway Norwegian Health Services Research Centre 1,3,4,5,6,7,8
38

Country Organisation WP Central and Eastern European Society for Technology Assessment in Health Care (CEESTAHC)
8 Poland
Polish Agency for Health Technology Assessment 2,4,5,7
Portugal Institute of Molecular Medicine 4,5,6,8
Slovenia Institut za varovanje zdravja Republike Slovenije 5,6,7,8
Spain Instituto de Salud Carlos III 3,6,7,8
Agencia de Evaluación de Tecnologías Sanitarias de Andalucía 4,5,7
Catalan Agency for Health Technology Assessment and Research 1,2,8
Galician Agency for HTA 4,6,8
Basque Office for HTA 4,5,7
Servicio Canario de la Salud 5,6
Unidad Evaluación Tecnologías Sanitarias 2,6
Sweden Swedish Council for Technology Assessment in Health Care 1,2,3,4,7
Switzerland Swiss Network for HTA 1,2,3,4,5,6,7,8
National Coordinating Centre for HTA (NCCHTA) 1,4,5,6 United Kingdom
Centre for Reviews and Dissemination. University of York 2
39
40
ANNEX 2.- Main objectives of the eight work packages of EUnetHTA project WP1. Coordination of the Project Objective: To establish the organisational and structural framework for an effective and sustainable European Network for HTA with a supporting secretariat.
WP2. EUnetHTA Communications
Objective: Effective dissemination and handling of HTA results, information sharing and coordination of HTA activities through the development and implementation of elaborate communication strategies and clearinghouse activities”.
WP3. Evaluation of the Project Objective: To monitor and provide an internal audit function for EUnetHTA to achieve the objectives and produce the deliverables in the WPs
WP4. Common core of health technology assessment –HTA.
Objective: To develop a generic methodological HTA framework based on current best practices (Core HTA Structure).
WP5. Adapting existing HTAs from one country to other settings.
Objective: To ensure better use of existing HTA reports by developing a toolkit for adapting the “core” within assessments made for one country into advice appropriate to other contexts (social, political, economic and health system).
WP6. Transferability to health policy. Objective: To get a systematic overview of the relations Among HTA and healthcare policy making
WP7. Monitoring development for emerging/new technologies and prioritization of HTAs.
Objective: To provide tools to monitor the development of health technologies and to share data and results of this monitoring.
WP8. Systems to support HTA in member states with limited institutionalisation of HTA. Objective: To define minimum components related to the scope, structure, process and visibility of an HTA organisation and to develop tools for education support to institutions or healthcare systems in the process of evolving to/building an HTA organisation / capacity

ANNEX 3.- Main characteristics of the HTA agencies. Data extracted from the technical specification of INAHTA members
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Argentina
IECS Independent and non-profit
To improve efficiency, equity, quality, and sustainability of healthcare systems and policies.
Publications are subject to an internal peer review process and to an external process in the case of peer-reviewed journal article submissions or scientific meeting presentations. For internal documents, external experts in the peer review process and feedback are involved. The reports are based on systematic literature searches and classification and synthesis of the evidence. Quick Response Reports Brief Technical Reports are preliminary evaluations of a particular health technology.
Website:
www.iecs.org.arPublications are available in electronic and printed formats. Reports are disseminated via web page. Developing an electronic newsletter that will also inform readers about the HTA reports.
Population served: (mil): 36 (National) Current HTA budget (mil USD): 0,450 Permanent staff: 12 Consultants: 8
Australia
AHTA (unit) (Without INAHTA profile)
To provide a rational basis for health care decision-making
- Located within the Department of Public Health, University of Adelaide. - Contracted work for Department of Health and Ageing, on behalf of the MSAC, PBAC; NICS and the NHMRC - Write brief appraisals (horizon scanning) on behalf of the Health Policy Advisory Committee on Technology which reports to Australian Health Minister’s Advisory Council and the MSAC
- Identify and appraise effectiveness of health services using evidence-based (EB) methods. - Conduct systematic reviews on a wide range of health care topics. - Horizon Scanning on new and emerging HT/procedures - Develop EB guidelines for clinical practice and program implementation. - Collaborate with specialties and policy-makers in production of reports. - Produce reports, publications and other forms of media.
Staff: 12 (1 director, 1 manager, 5 senior research, 4 research officer and 1 administration officer).
41

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Australia
ASERNIP-S (programme)
1996 Funded by Commonwealth Government of Australia, Department of Health and Ageing
To provide quality and timely assessments of a new and emerging surgical technologies and techniques.
- Programme of the Royal Australasian College of Surgeons. - Overseen by a Management Committee of surgeons (endorsed each review before dissemination activities) and representatives of both professional bodies and consumer groups. - Managed by a Surgical Director and a Programme Manager.
- Systematic reviews of the peer-reviewed literature. - Establishment and facilitation of clinical audits or trials - Identification of emerging technologies by horizon scanning. - The production of clinical practice guidelines. - Surgical speciality groups, government and consumer bodies, other organizations and individuals suggest procedures for assessment to ASERNIP-S. After that, Management Committee ratified them. - Review groups (surgeons and other experts) for each procedure advise and direct the researchers conducting the reviews. - Data on safety and efficacy is collected. - Reviews are usually completed within 6 months.
to: surgical community, government, hospital credentialing committees and consumers. - journals, newsletters and the ASERNIP-S website. - Each review is published in full, along with executive and consumer summaries on the ASERNIP-S website. - Executive summary is circulated in a newsletter to all fellows of the College, and an article is prepared for a national or international peer-reviewed journal. - Review information is disseminated via government and consumer publications, and a press release may be forwarded to the media.
Population served: national Population served (mil) 20.0 Current HTA budget (mil USD): 0.6 - Permanent staff (14): 4 administrative and 11 researchers with expertise in information management, computer and database programming, epidemiology, biostatistics, critical analysis of literature and scientific editing. - Consultants: variable.
Australia
MSAC 1998 Funded by the Australian Government
To advice the Australian Government on the strength of evidence available on new MT and procedures in terms of their safety, effectiveness and cost-effectiveness.
- Multidisciplinary expert body comprising 21 members drawn disciplines such as pathology, surgery, internal medicine and general practice, clinical epidemiology, and health economics. - Also has a consumer representative, a representative from the Commonwealth Government, and a member representing the State Territory Governments. - Establish Supporting Committees to assist in work program. - Diagnostics and Technology Branch of the Commonwealth Department of Health and Ageing provides a secretariat and project support to MSAC.
- Makes independent, EB evaluations of MT and procedures based on scientific and clinical grounds. - All new medical procedures and technologies are evaluated by MSAC before being admitted to the Medicare Benefits Schedule. - Adopts an EB approach, undertaking systematic reviews of the scientific literature, ant other information sources. - Also consults widely providers, users, and funders of health care
- Advice the Commonwealth and State/Territory Governments, the health professions, and the community. - Activities and findings are disseminated widely among its stakeholders. Through MSAC web site and mailouts of its reports and newsletters to professional medical colleges and organisations, State and Commonwealth health authorities, hospitals and to other interested parties.
Population served: national Current HTA budget (mil USD): 2.3 - Permanent staff: 12. - Consultants: 6
42

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Austria
ITA 1988 Small interdisciplinary public-funded research unit at the Academy of Sciences.
To create public awareness on HTA as a tool to secure the equal access to effective health care Assess technologies related to telecommunications, the environment, medicine, genetics, and biotechnology.
To gather and disseminate information on assessments of healthcare interventions carried out internationally. To coordinate and support networks of decision-makers To assess health technologies (projects) HTA topics are identified in discussions with experts, and relevant decision makers (health insurers & hospital management) Nearly all projects are funded by those decision-makers (reimbursement) All projects engage an interdisciplinary team including a sociologist, an economist, and a specialist in the medical field. Projects are presented and critically reviewed at internal seminars and undergo an external review process.
http://www.oeaw.ac.at/ita/htaReports are disseminated free-of-charge via the webpage, A monthly newsletter (500 recipients), monthly public seminars (attended regularly by 20-30 "mediators)
Current HTA budget (mil USD): 0.75 (National) Permanent staff: 2 Consultants: variable
Belgium
kCE 2002 Semi-governmental
To advice policy makers about the possibilities to obtain an efficient allocation of scarce health care resources that optimizes the quality and accessibility of health care
One general director and one vice-general director. Board of Directors. Scientific advisory committee.
Research topics are planned and prioritized in collaboration with the Board of Directors. Topic proposals can be submitted throughout the year by anyone from the Belgian population and are evaluated once a year. Research projects are performed by internal experts or in commissioned to an external partner (university or another research organization).
Website
www.kenniscentrum.fgov.be. Reports published on the websie in English (executive summary in Dutch & French) Press releases on the web-site in order to disseminate the message to the general public. weekly seminars
Population served: (mil):10.3 (National) Current HTA budget (mil USD): 3.06 Permanent staff: 29 Consultants: variable
43

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Canada
MAS A unit within the Ontario Ministry of Health and Long-Term Care.
- To provide EB policy advice on the coordinated uptake of new health technologies and health services in Ontario to the Ministry, other government agencies, and the Ontario healthcare system. - To ensure that residents of Ontario have access to the best available new health technologies that will improve patient outcomes.
- The Secretariat is led by the Senior Medical Advisor and managed by a director who provides liaison with other entities. - Eight clinical epidemiologists perform health technology policy analyses (HTPAs). - MAS also employs 3 health policy analysts and 2 administrative staff. - We also contract with a medical editor and a medical information science consultant. - MAS collaborates with governmental and non-governmental organizations to evaluate promising health technologies for which there is insufficient evidence of effectiveness or of how the technology will function in Ontario. - MAS works with external resources to test patient and provider safety for new health technologies and provides evidence based practice guidelines for recommended technologies. - Our reviews encompass medical methods used at any point in healthcare delivery. However, we do not examine pharmaceutical products or information systems in isolation.
- Technology review: a brief description of the technology, current options, scientific literature, current use, and the possible issue for the HTPA. In diagnostics, we also determine preliminary evidence of specificity and sensitivity. - For HTPAs, MAS systematically reviews the scientific literature, collaborates with relevant governmental partners, and consults with clinical and other external experts. We attempt to include all relevant research. - MAS evaluates the methodological quality of each study and identifies biases that might affect validity. - Economic analysis is performed only when there is evidence of effectiveness. - An external expert, preferably in Ontario, reviews the HTPA. The reviewer sees the systematic review, but not the implications/policy analysis or the recommendations from OHTAC. - MAS performs several "dry runs" with staff to obtain peer reviews prior to presenting the findings to OHTAC. - HTPAs are completed within 12 weeks. - OHTAC uses the HTPA to make EB recommendations to the Deputy Minister of Health. The Ministry responds within 60 days of receiving the OHTAC recommendation. The entire process takes 16 weeks. - MAS shares information with government officials from other Canadian and international jurisdictions.
- Summaries and full PDF versions of MAS health technology reports and OHTAC technology recommendations are posted on the respective websites. - The public has full access to the sites and may comment to the Secretariat via a dedicated e-mail address. - A monthly E-Bulletin informs healthcare providers and government officials of findings from recent MAS reviews and recommendations from OHTAC. MAS is also a leading participant in the Health Technology Policy Forum, an intergovernmental exchange on policy development in Canadian provinces dealing with pressures to introduce new health technologies.
Population served: Provincial Population served (mil): 12.4 Current HTA budget (mil USD): 1275 Permanent staff: 14 Consultants: 2 (Various staff, eg, health economists, from other areas of the Ministry are called in at times)
44

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Canada
CCOHTA 1989 Established by Canada’s federal, provincial and territorial Health Ministers. - A non-government body, working at arms-length decision-makers, CCOHTA is accountable to the federal, provincial and territorial Conference of Deputy Ministers of Health (CDM) through the CCOHTA Boards of Directors. - Receives all of its funding from the federal, provincial and territorial Ministries of Health. - In October 2004, with the approval of the Canadian Health Technology Strategy, CCOHTA became the national HT agency for Canada.
- A comprehensive Canadian source for impartial EB information on drugs, devices and health systems. - From an initial focus on assessing medical devices, CCOHTA’s role has expanded to include providing expert guidance with respect to publicly funded drug plan formulary decisions to becoming a centre for best practices resources with respect to drug prescribing and use. - Now supports informed decisions and policy through 3 programs: HTA program, Common Drug Review (CDR) program (for assessing new drugs for potential coverage by publicly funded federal, provincial and territorial drug benefit plans in Canada, except Quebec) and COMPUS program (for promoting best practices in drug prescribing and use among health care providers and patients/consumers). - 2004: To facilitate the appropriate and effective utilization of HT within the health care systems in Canada.- To provide timely, relevant, and rigorously derived EB information to decision-makers and support for the decision-making processes.
- Advisory Committees: 5 advisor bodies, which report to the CCOHT Board of Directors: - A national scientific advisory panel provided strategic direction on HTA methodologies and other scientific advances. - The Advisory Committee on Pharmaceuticals (ACP) provides advice on pharmaceutical issues and priorities. - The Devices and Systems Advisory Committee provides advice on medical device and health system issues and priorities. - The Canadian Experts Drug Advisory Committee is a national independent body established as part of the CDR program to provide EB drug formulary listing recommendations to publicly funded drug plans. - The COMPUS Advisory Committee is the liaison Among CCOHTA’s COMPUS program and federal, provincial and territorial jurisdictions. - Through its Liaison Program, CCOHTA is hiring a staff member in each province and territory to increase two-way communication Among the jurisdictions and CCHOTA. - CCOHTA’s Liaison Officers convey unique jurisdictional needs to CCOHTA and provide an effective channel for delivering information to stakeholders within each jurisdiction.
- CCOHTA provides a range of services to support the effective uptake and use of information generated through these programs, including outreach and communications, Knowledge transfer and support for operational linkages. - CCOHTA provides EB information on HT to Canadian health Care decision makers. - HTA program assesses technologies at various stages of their lifecycle. Assessment are conducted internally, commissioned to researchers across Canada, or performed in collaboration with other organizations. Assessments are reviewed by external experts and by the CCOHTA Scientific Advisory Panel. - CDR program provides a review of the best available clinical evidence and a critique of manufacturer-submitted pharmacoeconomic analyses for new drugs after they have been approved for sale in Canada by Health Canada. - COMPUS program is the Canadian centre for information and education on best practices in drug prescribing and utilizations.
- EB information produced by CCOHTA is readily available at no cost through its website. - Results are also published as detailed technical reports, overviews, bulletins, alerts and articles in peer-reviewed journals. - CCOHTA researchers present their work at national and international academic conferences and workshops and have been involved in the development of national consensus guidelines.
Population served: National Population served (mil): 32.8 Current HTA budget (mil USD): 16.9 - Permanent staff: 139. - Consultants: variable.
45

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Canada
AHFMR (Program/ Unit)
1995 - Has been established under an agreement with the Alberta Health Ministry. - HTA functions were transferred to AHFMR from Alberta
- Maintains a HTA network within the province, and establishers links with organizations in Canada and other countries. - Future plans: To further an ethos of HTA in Alberta, including support for HTA initiatives by regional health authorities.
- The program is assisted by a HTA Advisory Committee - Supports a community of researchers who generate knowledge that improves the health and quality of life of Albertants and people throughout the world. - Undertakes assessments in response to requests from organizations and individuals, related to HT likely to be of significance to Alberta. - Alberta Health and regional health authorities are important sources of requests. - The Unit also initiates assessments when it becomes aware of important health technology issues.
- in-house activities at the Foundation - Encourages development of HTA activities by other organizations in the province, through provision of advice and through collaborative projects.
- HTA reports. - Short summaries of these reports for more general audiences, and a newsletter are distributed widely throughout the province and elsewhere. - Knowledge of individual products and the HTA program has been increased through involvement of healthcare professionals in the development of projects, contact with key players with health authorities, and use of the mass media. - Details of HTA reports are given on the Foundation’s website. - A closer alliance with the Alberta Research Transfer Network provides the opportunity to develop and implement strategies to enhance the uptake of research produced by the HTA Unit.
Population served: Province of Alberta Population served (mil): 3.5 Current HTA budget (thousand USD): 600.000 - Permanent staff: 6 - Consultants: variable
Canada
IHE (Without INAHTA profile)
1995. - An independent public-private partnership, not-for-profit organization. - The Institute receives funding from different organizations (universities, industry, etc.).
- To deliver outstanding health economics, health outcomes and health policy research and related services to governments, health care providers, the health industry and universities for the betterment of society.
- Board of Directors, Research coordinating Committee, Research Fellows (33) and Staff (20)
- IHE has produced a significant amount of research describing pharmaceutical issues in Canada and other countries, and on measuring the economic, clinical and human consequences of those policies. - health economics and health technology assessment expertise, our diabetes outcomes and policy research, and our health care costing studies. - A centre of excellence in pharmaceutical policy research. - A source of information and information exchange for health care professionals, academics and policy markers. - Interdisciplinary collaboration. - We undertake both short and long-term research projects, from reviewing and analysing bodies of work to responding to specific research requests from our fellows, membership, and clients. - The IHE creates placement opportunities for Masters, PhD, and post-doctoral students as well as training practicing physicians in health care research skills.
- Shares knowledge by releasing publications, all available online and sponsoring events such as lectures, conferences, courses, and workshops for government, academic, and industry participants. - Research papers focusing on these issues are listed below and are available free of charge through our Publications page.
46
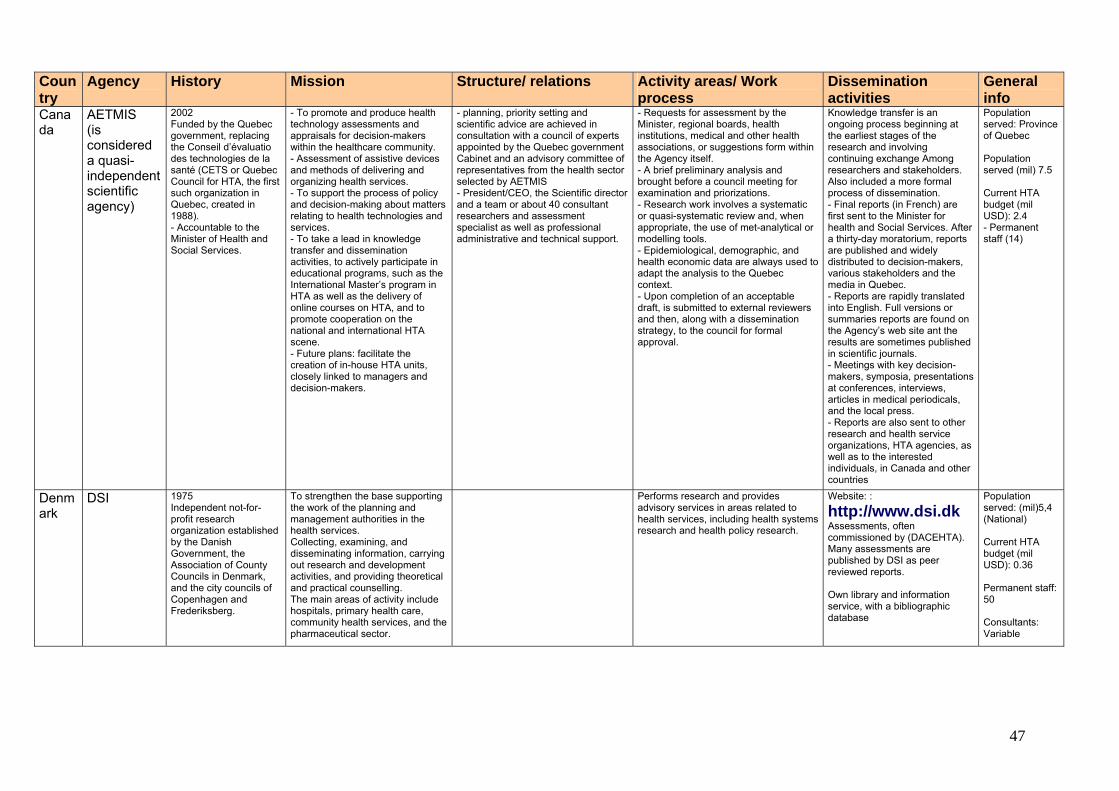
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Canada
AETMIS (is considered a quasi-independent scientific agency)
2002 Funded by the Quebec government, replacing the Conseil d’évaluatio des technologies de la santé (CETS or Quebec Council for HTA, the first such organization in Quebec, created in 1988). - Accountable to the Minister of Health and Social Services.
- To promote and produce health technology assessments and appraisals for decision-makers within the healthcare community. - Assessment of assistive devices and methods of delivering and organizing health services. - To support the process of policy and decision-making about matters relating to health technologies and services. - To take a lead in knowledge transfer and dissemination activities, to actively participate in educational programs, such as the International Master’s program in HTA as well as the delivery of online courses on HTA, and to promote cooperation on the national and international HTA scene. - Future plans: facilitate the creation of in-house HTA units, closely linked to managers and decision-makers.
- planning, priority setting and scientific advice are achieved in consultation with a council of experts appointed by the Quebec government Cabinet and an advisory committee of representatives from the health sector selected by AETMIS - President/CEO, the Scientific director and a team or about 40 consultant researchers and assessment specialist as well as professional administrative and technical support.
- Requests for assessment by the Minister, regional boards, health institutions, medical and other health associations, or suggestions form within the Agency itself. - A brief preliminary analysis and brought before a council meeting for examination and priorizations. - Research work involves a systematic or quasi-systematic review and, when appropriate, the use of met-analytical or modelling tools. - Epidemiological, demographic, and health economic data are always used to adapt the analysis to the Quebec context. - Upon completion of an acceptable draft, is submitted to external reviewers and then, along with a dissemination strategy, to the council for formal approval.
Knowledge transfer is an ongoing process beginning at the earliest stages of the research and involving continuing exchange Among researchers and stakeholders. Also included a more formal process of dissemination. - Final reports (in French) are first sent to the Minister for health and Social Services. After a thirty-day moratorium, reports are published and widely distributed to decision-makers, various stakeholders and the media in Quebec. - Reports are rapidly translated into English. Full versions or summaries reports are found on the Agency’s web site ant the results are sometimes published in scientific journals. - Meetings with key decision-makers, symposia, presentations at conferences, interviews, articles in medical periodicals, and the local press. - Reports are also sent to other research and health service organizations, HTA agencies, as well as to the interested individuals, in Canada and other countries
Population served: Province of Quebec Population served (mil) 7.5 Current HTA budget (mil USD): 2.4 - Permanent staff (14)
Denmark
DSI 1975 Independent not-for-profit research organization established by the Danish Government, the Association of County Councils in Denmark, and the city councils of Copenhagen and Frederiksberg.
To strengthen the base supporting the work of the planning and management authorities in the health services. Collecting, examining, and disseminating information, carrying out research and development activities, and providing theoretical and practical counselling. The main areas of activity include hospitals, primary health care, community health services, and the pharmaceutical sector.
Performs research and provides advisory services in areas related to health services, including health systems research and health policy research.
Website: :
http://www.dsi.dkAssessments, often commissioned by (DACEHTA). Many assessments are published by DSI as peer reviewed reports. Own library and information service, with a bibliographic database
Population served: (mil)5,4 (National) Current HTA budget (mil USD): 0.36 Permanent staff: 50 Consultants: Variable
47

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Denmark
DACEHTA 1997 Established by the Ministry of Health Independent, state-financed
To implement the National Strategy for Health Technology Assessment. The principal objective is to establish HTA as a solid and comprehensive basis for decision-making and to integrate the principles of HTA at all levels of health care.
Scientific advisory board. DACEHTA hosts the Danish Guideline Secretariat and the Unit for Documentation of Health Care Prevention
Broad approach to HTA - focusing on organisational and social aspects as well as on clinical and economic effectiveness. Participation and contribution to the national, regional and local "policy - HTA - policy" loops. Strategic and activity plans are discussed with the National Board of Health and the scientific advisory board and act as guidelines for priority setting in day-to-day operations. DACEHTA uses ad hoc expert groups, Peer review is incorporated to assure quality of draft reports.
Newsletters The "Health Technology Assessment Handbook" Publications database
Population served: (MIL):5,4 (National) Current HTA budget (mil USD): 4.5 Permanent staff: 22 Consultants: variable
Finland
FinOHTA 1995 Established within the National Research and Development Centre for Welfare and Health (STAKES). STAKES is subordinated to and financed by the Ministry of Social Affairs and Health
To promote the effectiveness of Finnish health care. concentrating on technologies that deal with major health problems or are of economic importance for the country.
Scientific committee (10 people) Advisory Board ( 28-members) Expert Network ( 60 members)
National clearinghouse for healthcare technology assessments (international and domestic). Promotes national HTA research by funding studies which meet "good assessment" criteria. Close co-operation with the healthcare profession and different organizational entities in the healthcare sector and related sectors
Website: http://www.stakes.fi/finohta/Newsletter called "Impakti" and has a website www.stakes.fi/finohta. Dissemination of foreign assessment abstracts as leaflets called (Assessment Brief)".
Population served: (mil) 5,1 (Nacional) Current HTA budget (mil USD): 2.0 Permanent staff: 17 Consultants: 65
Germany
DAHTA@DIMDI
1999
To extend the literature databases To support interest groups (politicians, decision makers, medical professionals and patients) by providing information about HTA. To support scientific applications and methods in health technology assessment by financing HTA reports. To provide a stage for the different scientific faculties to discuss and reduce "interfaculty language bias".
Scientific Advisory Board Board of Trustees
To identify new technologies that are of interest from an HTA perspective
Website:
http://www.dimdi.de/Meetings at both the national and the international levels Newsletter (found on the Internet or delivered by post e-mail. Workshops and courses for clinicians
Population served: (mil):80 (National) Current HTA budget (mil USD): 1.5 Permanent staff: 130 (10) Consultants: variable
48

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Hungary
HunHTA 2001 Universitarian Part of the department of public policy and management, Budapest University of Economic sciences and Public administration.
To provide education to students and to offer training in health economics and health technology assessment to professionals in the Hungarian healthcare system. To invest in HTA yields good returns, both monetary and non-monetary
International scientific advisory committee Board of trustees
Education and training: HunHTA, in collaboration with ISAC, aims to establish education and training programs for healthcare professionals to remedy the short supply of HTA specialists in Hungary. Developing local competence is the crucial next step. International collaboration: Joining the mainstream of HTA, sharing results, using what is already available, and working as part of INAHTA are the most costeffective ways of doing HTA. Two-way transfer of knowledge and learning offer a way forward. Working with colleagues: HTAs will only be as useful as decision-makers, professionals, and the public value them. HunHTA aims to establish proper cooperation with each of these groups. Engaging with, and changing the culture of, health care is the focus of our activity.
Strategy under construction Website:
http://hecon.uni-corvinus.huNewsletters Conferences and workshops working for and with professional societies and governmental and non-governmental agencies
Current HTA budget: (mil SD): 0.005 Permanent staff: 11 Consultants: 80
Israel ICTAHC 1998 Established at the Gertner Institute for Epidemiology and Health Policy Research. - An independent research center, and one of its major tasks is to advise the Israel Ministry of Health on national policy in technology management. - The foundations for the Center were set by the Medical Technology Assessment Unit which has been operating since 1992. - The Center is a multidisciplinary unit,
- To serve as a research center for medical technology assessment; - To act as a national center for health technology management and to assist the Ministry of Health, public hospitals, private clinics, and the health funds to develop systematic processes to introduce new technologies; - To identify health priorities at a national level; - To serve as an educational center for students and policy makers within the universities in Israel; - To maintain working relations with overseas counterparts while adapting information to Israel's cultural, social, and ethical values as well as its economic environment. - To organize consensus conferences on national health issues.
- The Center comprised of physicians, nurses, pharmacists, economists, and other professionals.
- ICTAHC organizes special task forces in response to requests for systematic reviews made by the Ministry of Health and the major health funds.
- CTAHC provides university courses in the departments of medicine and administration. -The Center plans to expand HTA training to healthcare professionals in hospitals and the health funds.
Description of population served: National Population served (mil): Current HTA budget (mil USD): 0.75 Permanent staff: 8 Consultants: variable
49

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Latvia HSMTA 1995
To improve the quality of health care in Latvia, mainly by furthering the safety, effectiveness, and cost-effectiveness of health services To provide evidence-based information for decision making (government, institutions, authorities, professionals, and patients)..
Includes the following departments: Health Statistics Registry Monitoring Conformity Assessment (certification) Medical Technologies Project Appraisal Master Planning
For approval of a health technology: The key factor is scientific evidence regarding the safety and effectiveness (or at least efficacy) of the technology Medical, economic, ethical, and political issues are also discussed with relevant experts before recommending approval of a technology Technologies of national economic importance are assessed at the request of the Ministry. The assessments rely mainly on evidence of effectiveness from international HTAs and economic evaluations interpreted in a national context. Multidisciplinary teams of health professionals are involved in the assessment process.
Website:
http:/www.vsmta.lvPlaning to produce HTA reports targeted to different populations Consensus conference
Population served: National Permanent staff: 8 Consultants: variable
Netherlands
GR 1902 The Council is funded by the Government.
The Health Council advises the Government on current scientific knowledge with respect to questions of health care and public health. This includes the early warning of emerging technologies and other developments which are relevant to government policy making. The Council's recommendations are based first and foremost on scientific evidence. In addition to topics directly related to health care, the Council deals with such issues as prevention and health protection issues related to food and nutrition, Occupational hygiene and topics related to health and the environment, including ecology and ecotoxicology questions.
independent body of experts which is consulted by the government on various public health and healthcare matters. Its present legal base dates back to the 1956 Health Act, and its members (approx. 170) are appointed exclusively on the basis of their expertise. The full Council never meets; rather, members serve on ad hoc and/or standing committees.
Reports are sent to numerous institutions and individuals, depending on the topic. A press communiqué is usually issued, often resulting in coverage by the media. All reports in Dutch carry an Executive Summary in English. Collected Executive Summaries are published once a year. An increasing number of reports are fully translated into English. The Council publishes an information bulletin (Graadmeter) for its Dutch readership and a newsletter in English (Network) for its international audience. Both address new activities and publications, and update published reports.
Pobl. 16.600.000 USD.- 3.500.000 Staff.- 25 Col.- 200
50

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Netherlands
CVZ CVZ's program is approved by the Minister of Health, Welfare, and Sports.
supervise, coordinate, and improve the health insurance and financing system, and to guarantee accessible and appropriate health services. A natural element of this mission is to stimulate HTA of both new and established technologies
? CVZ formulates advices to the minister concerning the question which new health care technologies should be included in the package of benefits of the legal health insurance system. The CVZ advice is maximally supported by all available HTA results; CVZ makes use of existing HTA projects but also commissions new HTA projects. The phase of approval of the available evidence is executed by the staff of CVZ itself. Most experiences are in the field of Pharmacy, but the approval and advice on other areas of health care is developing rapidly. HTA Program - Started in the year 2001 this HTA program is managed byZonMW. CVZ is involved in assessing the importance for policy of new proposals sent to ZonMW from a health-insurance perspective. The ongoing projects (started before 2001) are still managed by CVZ. Farmacoeconomic research - To improve the quality of HTA-research and to use results when making decisions regarding the reimbursement of drugs, CVZ formulated the Dutch guidelines for farmacoeconomic research. The responsibility for carrying out financing this research into new drugs lies with the manufacturer. The guideline is published in 1999 and will be evaluated and adjusted when necessary. Related topics - Similar efforts are going on for other topics. For the recommendations for appropriate diagnostic procedures, prescribing medical aids, drugs and other technologies and organisational questions we use the results of (HTA)-research. If there are additional policy questions there's the possibility to fund research through the different committees.
These activities include the diffusion of reports on finished projects to appropriate institutions, including medical unions, the medical profession, and health insurance companies. Dissemination also takes place via the Internet, through INAHTA, and by annually publishing collected findings from different projects. Short summaries of reports are published in a leading Dutch medical journal, and press releases are issued, depending on the topic.
Pobl. 16.000.000 USD.- 10.300.000 Staff.- 4 Col.- 5
51

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Netherlands
ZonMW 2001 The Health Research and Development Council and the Council for Medical and Health Research from the Netherlands Organization for Scientific Research have integrated to form a new organization: the Netherlands Organization for Health Research and Development ZonMw.
ZonMw is a national organization that promotes quality and innovation in the field of health research and health care, initiating and fostering new developments. In the same line ZonMw actively promotes knowledge transfer and implementation. This means that knowledge is exchanged Among all relevant stakeholders (for example health researchers, health professionals, patients/consumers and the general public), not only for transfer, but also for structured implementation of newly developed knowledge into the health care system and of emerging health care questions into the research agenda. In short, one of the basic challenges of ZonMw is to enable mutual exchange of innovation and inspiration Among the various stakeholders of the same 'knowledge' continuum: from basic, strategic and applied research to daily health services. ZonMw fulfils the role of intermediary organization Among policy, research and practice. Evidence-based medicine, relevance-based science, information-based policy: it is ZonMw's firm believes that only through an active exchange of ideas, knowledge and experience the innovation cycle is able to flourish and to contribute to an up-to-date society.
The main assigning bodies of ZonMw are the Ministry of Health, Welfare and Sports (VWS) and the Netherlands Organization for Scientific Research (Dutch acronym NWO). VWS, as governmental department, holds its main perspective in the contribution to public health including prevention and health services. NWO is the non-governmental organization in the area of fundamental and strategic research and plays - as the national research council - a key role in the development of science, technology and culture in the Netherlands. With respect to health research and development - and thereby its mandate to ZonMw - NWO holds its main interest in the contribution to cure, care and prevention through a better understanding of the (molecular basis and epidemiology of) disease and research related to medical or health technology assessment.
One of the main programs of ZonMw is a research program on the efficiency of health care, the Health Care Efficiency Research Program. This program is financed by the Ministry of Health, Welfare and Sports (Dutch acronym VWS).
Dissemination activities will include the publications of annual reports, TA-reports and research findings through various media, including newsletters, website and peer-reviewed literature. There is an active policy to achieve implementation of the results of the projects. The importance of implementation is recognized both on the level of the program as on the level of the separate projects.
Pobl. 16.000.000 USD.- 13.500.000 Staff.- 7,3 Col.- variable
New Zealand
NZHTA 1997 The Transitional Health Authority (National Funding Agency) along with the New Zealand Ministry of Health awarded a three-year contract to the University of Otago to establish a health outcomes and health technology assessment clearing house.
- To assist New Zealand health and disability services through the production and dissemination of evidence-based information for decisions on health policy and purchasing, service management, and clinical practice.
- A Governance Board heads NZHTA, which is responsible for establishing and ensuring achievement of NZHTA's Mission and Objectives through effective policy development management.
- The main function of NZHTA is to identify effective health care interventions and technologies and thereby facilitate EB policy making and purchasing by the New Zealand funder of health and disability services (the Ministry of Health). - The work of NZHTA is closely tied to the priorities of its two contract partners (the New Zealand Ministry of Health and the Medical Services Advisory Committee of the Australian Department of Health and Aged Care) who are responsible for determining the content of its work programme. - NZHTA provides four levels of review,
- NZHTA's outputs and reports are disseminated to their contract partners and other target groups (clinicians, administrators, and INAHTA members). - NZHTA's outputs are also available through the Internet
Description of population served: National Population served (mil): 4 Current HTA budget (mil USD): NR Permanent staff: 14 Consultants: variable
52

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
which offers the flexibility to accommodate a variety of requests within a diverse range of different topics and budgets.
Norway
NOCK 2004
To gather and disseminate evidence about the effect and quality of methods and interventions within all parts of the health services. The uptake of this evidence by the health services
Based upon a merger of the following organizations: The Norwegian Centre for Health Technology Assessment (SMM), parts of the Division for Knowledge Management in The Directorate for Health and Social Affairs, and the Foundation for Health Services Research (HELTEF).
Among the central tasks of NOKC are: - HTA reports - Systematic reviews (Cochrane and others) - Overviews of overviews - Early warnings - Surveys - Informed Choice Research. The Centre will also be assigned important tasks when it comes to monitoring of clinical practice: - Clinical registries - Outcome indicators. .
Website: http:/www.nock.no Reports disseminated to defined target groups - clinicians, health policy makers, administrators, media and the general public.. Workshops and seminars for target groups and teaching newsletter is being planned
Description of population served: National, Population served (mil): 4,5 Current HTA budget (mil USD): 4,0 Permanent staff: 30 Consultants: 100
Spain OSTEBA 1992 Funded from the Health Department budget. .
To contribute to the appropriate use of existing and future health technology. To provide information on safety, efficacy, effectiveness, accessibility, and equity about different technologies, as required by decision makers in the Basque Country.
Advisory committees.
Work conducted in-house by the expert panels and external professionals from the Ministry of Health, universities, the public health system, and private practices. Systematic overviews and cost analyses expert panels to develop consensus statements. Commissioned research projects
Website:
http://www.euskadi.net/sanidad/ostebaReports, technical documents, brief reports. Newsletter disseminated by direct mailing. Courses and lectures to clinicians and policy makers, and collaborates. Coordination of activities on the methodology of health services assessment and research.
Population served: 2.1 (Basque Region) Current HTA budget (mil USD): 0.3 Permanent staff: 5 Consultants: 40+
Spain AETS 1994 Governmental Branch of the Instituto de Salud Carlos III which gives scientific and technical support to the Ministry of Health and to the National Health System.
To assess different health technologies as a basis for formulating policies on technology selection and implementation in the NHS To promote the appropriate use of existing technologies.
Reports reviewed by an independent panel of experts Identification of specific issues to assess on a national scale was initiated by The Consejo Interterritorial de Salud del SNS IS - Interregional Council of the NHS). Teaching and training programs. National and international cooperation.
Website:
http://www.isciii.esInternal reports Public reports by AETS are disseminated through selective mailing. Participation in meetings of scientific and professional societies. Short-term training courses for healthcare managers and clinicians.
Current HTA budget: (mil SD): 0.6 Permanent staff: 11 Consultants: 80
53

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Spain CAHTA 1994 Non-profit public agency affiliated to the Catalan Health Service.
To promote research oriented to health and healthcare services needs of the population and to knowledge needs of the healthcare system itself. To encourage the introduction, adoption, diffusion and utilization of health technologies according to proven scientific knowledge and the criteria of efficacy, safety, effectiveness, and efficiency.
Executive Committee Scientific Committee
Combination of different study methodologies in its assessments. Primary data, secondary data, and data synthesis . Activities requested or by own initiative- take place within the public Catalan healthcare system, industry, insurance companies, research units, and users in Catalonia, Spain, and abroad. Collaborating centre of the World Health Organization (WHO), developing various support tasks on HTA and promoting use of proper health technologies. Quick response service.
Website :
http://www.aatrm.netQuarterly newsletter. Annual report, assessment reports, scientific journal articles, a collection of report abstracts and technical informative notes are published in Catalan, Spanish and some in English. Teaching activities are developed at under-and postgraduate level and in ongoing training
Population served: 7 (Catalonia Region) Current HTA budget (mil USD): 2.4 Permanent staff: 30 Consultants: 150
Spain AETSA 1996 Governmental Supported by the Regional Ministry of Health.
To help decision-makers and to facilitate information to health professionals on the more efficient use of clinical resources. To develop a strategic plan to enhance the quality of care in Hospitals and Primary Health Care Centres, by incorporating scientific evidence into clinical practice.
Scientific Advisory Committee (15 members)
Assessments projects from a list of projects selected by health authorities, the Scientific Advisory Committee, and qualified professionals. Systematic reviews of international scientific literature. Courses for researchers and clinical leaders.
Website http://www.juntadeandalucia.es/salud/aetsa/Newsletter (NETS), distributed to policy makers, health care professionals, consumers, libraries and medical journals, and other INAHTA members. Reviews and reports and scientific information are disseminated. Organization of meetings and conferences for health professionals.
Population served: 7.5 (Andalusian Region) Current HTA budget (mil USD): 0.9 Permanent staff: 15 Consultants: variable
Spain AVALIA 1999 Governmental (established by the Galician Regional Government).
To contribute improving the health of the Galician population. Support to the decision-making process by providing the best available evidence on the efficacy, effectiveness, safety, and equity of specific health technologies.
Clinical practice guidelines for the Public Galician Health Care System. Systematic reviews requested by directive entities of the Galician Department of Health. Reports for their own initiative, for other entities, or for private organizations. Support to primary studies and systematic reviews on health technologies at the national level. All HTA reports include internal and external reviews and are always based on the best available scientific evidence. .
Website http://avalia-t.sergas.esReports are sent by e-mail to all professionals associated with the technology assessed and also to the managers of health services. Some of the reports are published in scientific journals or institutional publications.
Population served:2.7 (Galician Region) Current HTA budget (mil USD): 0.35 Permanent staff: 7 Consultants: Variable
54
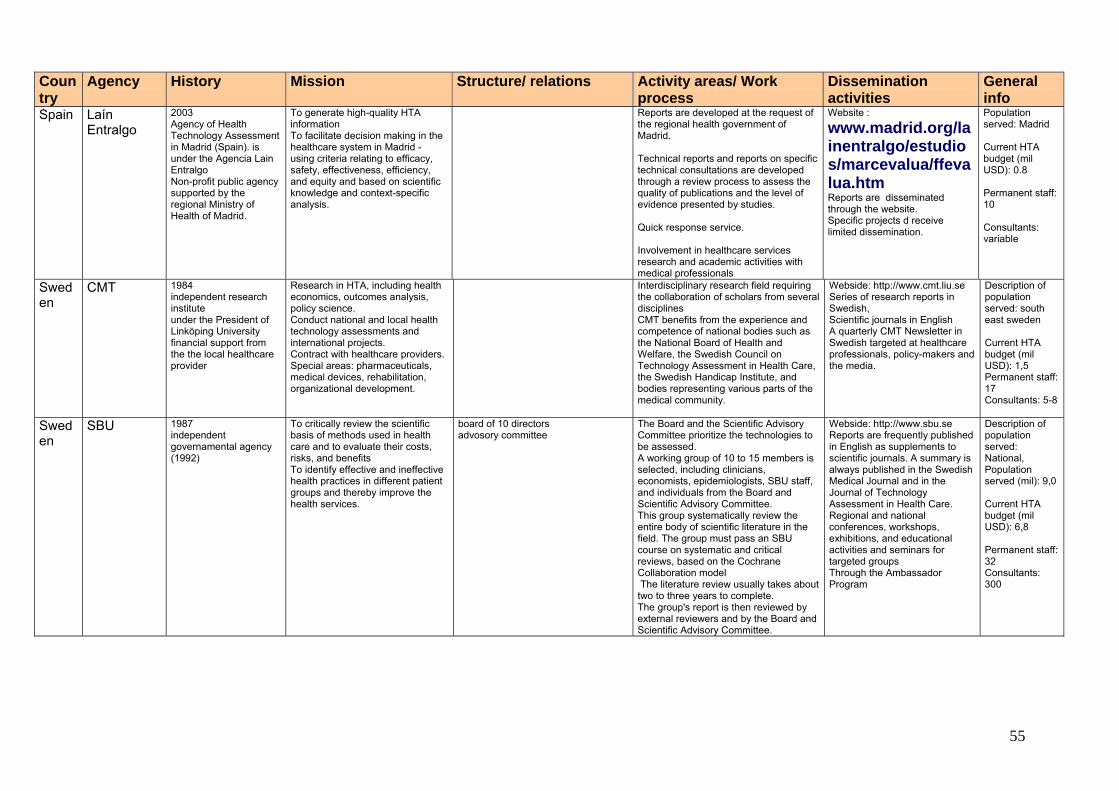
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Spain Laín Entralgo
2003 Agency of Health Technology Assessment in Madrid (Spain). is under the Agencia Lain Entralgo Non-profit public agency supported by the regional Ministry of Health of Madrid.
To generate high-quality HTA information To facilitate decision making in the healthcare system in Madrid - using criteria relating to efficacy, safety, effectiveness, efficiency, and equity and based on scientific knowledge and context-specific analysis.
Reports are developed at the request of the regional health government of Madrid. Technical reports and reports on specific technical consultations are developed through a review process to assess the quality of publications and the level of evidence presented by studies. Quick response service. Involvement in healthcare services research and academic activities with medical professionals
Website :
www.madrid.org/lainentralgo/estudios/marcevalua/ffevalua.htm Reports are disseminated through the website. Specific projects d receive limited dissemination.
Population served: Madrid Current HTA budget (mil USD): 0.8 Permanent staff: 10 Consultants: variable
Sweden
CMT 1984 independent research institute under the President of Linköping University financial support from the the local healthcare provider
Research in HTA, including health economics, outcomes analysis, policy science. Conduct national and local health technology assessments and international projects. Contract with healthcare providers. Special areas: pharmaceuticals, medical devices, rehabilitation, organizational development.
Interdisciplinary research field requiring the collaboration of scholars from several disciplines CMT benefits from the experience and competence of national bodies such as the National Board of Health and Welfare, the Swedish Council on Technology Assessment in Health Care, the Swedish Handicap Institute, and bodies representing various parts of the medical community.
Webside: http://www.cmt.liu.se Series of research reports in Swedish, Scientific journals in English A quarterly CMT Newsletter in Swedish targeted at healthcare professionals, policy-makers and the media.
Description of population served: south east sweden Current HTA budget (mil USD): 1,5 Permanent staff: 17 Consultants: 5-8
Sweden
SBU 1987 independent governamental agency (1992)
To critically review the scientific basis of methods used in health care and to evaluate their costs, risks, and benefits To identify effective and ineffective health practices in different patient groups and thereby improve the health services.
board of 10 directors advosory committee
The Board and the Scientific Advisory Committee prioritize the technologies to be assessed. A working group of 10 to 15 members is selected, including clinicians, economists, epidemiologists, SBU staff, and individuals from the Board and Scientific Advisory Committee. This group systematically review the entire body of scientific literature in the field. The group must pass an SBU course on systematic and critical reviews, based on the Cochrane Collaboration model The literature review usually takes about two to three years to complete. The group's report is then reviewed by external reviewers and by the Board and Scientific Advisory Committee.
Webside: http://www.sbu.se Reports are frequently published in English as supplements to scientific journals. A summary is always published in the Swedish Medical Journal and in the Journal of Technology Assessment in Health Care. Regional and national conferences, workshops, exhibitions, and educational activities and seminars for targeted groups Through the Ambassador Program
Description of population served: National, Population served (mil): 9,0 Current HTA budget (mil USD): 6,8 Permanent staff: 32 Consultants: 300
55

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Switzerland
MTU-SFOPH
1960
Reviews of procedures which have been "contested or are controversial" as to their effectiveness, appropriateness, and/or cost-effectiveness. Responsible for the assessment of these technologies for the Swiss Federal Coverage Committee.
"Manual for the Standardization of Clinical and Economic Evaluation"
Website:
http://www.snhta.chDistribution of the "Manual for the Standardization of Clinical and Economic Evaluation of Medical Technologies" (in German, French, and English).
Population served: National Permanent staff: 6 Consultants: 60
56
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
UK NCCHTA 1996 Launched to support the NHS Health Technology Assessment Programme funded since 1993 by the Department of Health's Research and Development Directorate
The programme's mission is to help provide high quality evidence to inform NHS decision making. To achieve this goal, NCCHTA coordinates and manages the NHS HTA Programme. This involves assisting in the identification of knowledge gaps; providing scientific support for the prioritizing of research questions; assisting in the management of the research commissioning process; and making the results available to decision makers in the health service. The HTA programme has two key characteristics: it is needs-led and it is science-added. By 'needs-led' we mean that the NHS HTA programme is driven by the information needs of those who use, manage, provide care in and develop policy for the NHS. Systems understanding those information needs are therefore central to the programme. By 'science-added', we mean that the HTA programme adds knowledge value at every stage of its processes, ensuring that researchers meet the information needs of the NHS
The NHS HTA Programme is the largest single activity funded though the NHS Research and Development Programme. NCCHTA supports the work of the HTA Programme in identifying and commissioning relevant technology assessment research.
Commissioned HTA. NCCHTA runs a cycle that begins with identifying the areas of need by consultation throughout the health service and scrutinizing the recommendations of previous research. Topics identified in this way are then prioritized by expert panels. Research based on primary or secondary data sources is commissioned from health service or academic research organizations under each of the priority areas. Responsive HTA. In 2006 the HTA programme launched a new responsive stream which funds research on topics proposed by researchers: 1) funding for pragmatic clinical trials of the sort already funded by the HTA programme, with researchers invited to submit outline primary research proposals on an ongoing basis; and 2) funding for research (primary, methodological or evidence synthesis) in specific themed areas, with calls for outline proposals on a biennial basis. The first themed call for proposals took place in 2005, in the area of Medicines for Children. Call-off contract. This is a stream to support NICE guidance (both Technology Appraisal Reports and the new Single Technology Appraisals). NCCHTA commissions reports from seven contracted academic departments in the UK that provide the independent evidence base for NICE guidance. NCCHTA encourages high quality research through a process of active monitoring of on-going projects and rigorous peer view.
NCCHTA has produced a monograph series (ISSN 13366-5278) to publicize and disseminate the results of research from the HTA Programme. Executive summaries and reports are available by direct mail, in printed format, on CD-Rom, and through the Internet at www.hta.ac.uk
Pobl. 59.200.000 USD.- 21.600.000 Staff.- 36 Col.- variable
57

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
UK NHSC 1998 Funded by the Research and Development Directorate of the Department of Health for England. The Centre is based in the Department of Public Health and Epidemiology at the University of Birmingham. The NHSC developed from work initially undertaken within the National Coordinating Centre for Health Technology Assessment (NCCHTA).
The National Horizon Scanning Centre aims to provide advance notice to the Department of Health and the wider National Health Service of new and emerging technologies (including changing applications and uses of existing technologies) that need urgent evaluation, consideration of clinical and cost impact or modification of clinical guidelines or guidance.
? The NHSC undertakes a wide ranging identification process including scanning and contacting primary sources including industry; secondary sources including expert groups, the media and the Internet; and tertiary sources such as EuroScan and other horizon scanners. Once identified, new and emerging technologies pass through a multi-stage filtration and selection process to identify those that would benefit from further evaluation. After collection of relevant information, an estimate of a technology's potential for impact is made with regard to health benefit, service impact, associated costs, likely speed of diffusion, and whether current clinical guidance or guidelines will need revision.The NHSC produces technology briefings for the Department of Health, the National Institute for Health and Clinical Excellence (NICE), and for other evaluation and national policy-making bodies including the Centre for Evidence-Based Purchasing and the National Steering Committee. The NHSC is host to the Secretariat of EuroScan: The European Information Network on New and Changing Health Technologies.
The NHSC undertakes to place all our technology briefings onto our website and on the EuroScan and HTA-databases.
Pobl. 52.000.000 USD.- 10.300.000 Staff.- 6,5 Col.- variable
58

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
UK IAHS 1999 Formed by incorporating the Health Economics Research Unit (HERU), the Health Services Research Unit (HSRU), the Dept of Public Health, the Dept of Primary Care and General Practice, and others.
To provide a service to the UK National Health Service via NICE and the HTA programme To undertake and publish high-quality HTAs, both systematic reviews and primary research, both incorporating economic evaluations To consider the methodologies of HTA, especially "rapid reviews" such as TARs and pragmatic trials of non-drug technologies.
HERU and HSRU are core funded by the Scottish Government, but receive additional grants, eg, from the UK Health Technology Assessment Programme. Since 2000, IAHS has produced technology assessment reports (TARs) for NICE. HSRU runs several HTA trials and is part of a "Review Body" for the NICE Interventional Procedures Programme. IAHS is the editorial home of the Cochrane Incontinence Group and co-convenes the Cochrane Economics Methods Group. IAHS members contribute to the Cochrane Metabolic and Endocrine Disorders Group and other Cochrane reviews. Key academic interests in HTA include non-pharmacological interventions, diabetes care, and screening.
IAHS incorporates a wide range of disciplines and skills. TARs are performed by small, core teams representing information science, systematic reviews, epidemiology/public health, health economics, and statistics. The teams are supplemented on an ad hoc basis according to the needs of individual reviews, eg, from relevant clinical specialties. Advisory panels of clinical experts, methodologists, and patient representatives are convened for each review. All reviews are peer reviewed. The trials are coordinated from a formal trials service.
TARs can be disseminated for NICE in at least five ways: 1) the reports are released by NICE as part of their consultation process, eg, via their website; 2) they are published as HTA monographs by the NCCHTA, both on paper and electronically; 3) short versions are often submitted for publication in medical journals; 4) they are listed in the HTA database in the Cochrane Library and some TARs, or parts of them, are converted to Cochrane reviews; and 5) the reports may be presented at conferences eg, HTAi.
Pobl. ? USD.- 400.000 Staff.- 10 Col.- Variable
59
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
UK NHS QIS 2000 The Health Technology Board for Scotland (HTBS) was established as a special health board to provide a single source of authoritative advice to NHSScotland on new and existing health technologies. In January 2003 HTBS merged with several other organizations to form NHS Quality Improvement Scotland (NHS QIS). Undertaking health technology assessment is one of the key tasks of NHS QIS.
The role of NHS QIS is to lead in improving the quality of healthcare that NHSScotland delivers to patients. We achieve this by looking at scientific evidence, listening to the needs and preferences of patients and careers and learning from the experiences of healthcare professionals. NHS QIS informs local and national decisions by providing advice on the clinical and cost effectiveness of new and existing health technologies. HTA consider the medical, social, ethical and economic implications of the development, diffusion and use of health technology. Their theme is making evidence work for a healthier Scotland by providing a bridge Among the scientific evidence, the judgement of health professionals, the views of patients and the general public, and the needs of policy-makers. In providing advice about value for money and the resources required for implementing HTA recommendations, NHS QIS is keen to shape HTA to make them rigorous, but also timely and of practical use to decision makers at all levels.
NHS QIS works closely with the Scottish Intercollegiate Guidelines Network (SIGN), the Scottish Medicines Consortium (SMC) and the Scottish Health Council (SHC).
NHS QIS demonstrates its independence by choosing its own work program, reaching its own conclusions based on the best available evidence and publishing its findings. Its processes have been developed in partnership with NHSScotland staff and all aspects of its work involve liaison with healthcare professionals. To promote openness and transparency and to gain an understanding of the needs and preferences of patients and stakeholders, NHS QIS involves the public in its work. As part of its work program, NHS QIS produces Evidence Notes (short 1-2 page summaries of health interventions) and is piloting the development of different types of HTAs. NHS QIS uses the INAHTA definition of HTA, ie a multi-disciplinary policy analysis that studies the medical, social, ethical and economic implications of development, diffusion and use of health technology. Systematic literature searching is undertaken and manufacturers, patients and professional groups are invited to submit evidence. Focus groups are undertaken where appropriate to ascertain the views of patients. In order to allow robust economic modeling and detailed budget impact calculations, many discussions are required with health professionals to understand the details of a patient journey and the associated benefits and resources. A multi-disciplinary group of experts (including patient representatives) help to interpret the evidence for the Scottish setting. The process incorporates statistical and economic analysis, peer review, dialogue with those who submit evidence and open consultation.
The NHS QIS website www.nhshealthquality.org is a key tool for disseminating information and capturing ideas and feedback. The site includes the work program, processes, consultation papers and publications. NHS QIS uses a direct mailing list and networks to disseminate its advice. It also participates in educational initiatives and facilitates workshops and seminars on methodological developments.
Pobl. 5.600.000 USD.- 680.000 Staff.- 10 Col.- variable
60

Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
UK CRD English NHS R&D Programme, to provide the NHS with important information on the effectiveness of treatments and the delivery and organization of health care.
To carry out credible, rigorous evidence syntheses (including systematic reviews) of research findings on the effectiveness and cost effectiveness of health and social care relevant to the NHS. To improve the accessibility of these and other research reviews by maintaining and updating an international register of research reviews and providing a single access point to this information for enquirers in the NHS. To provide simple and effective mechanisms by which the results of systematic reviews on the clinical effectiveness, cost-effectiveness, and acceptability of health service interventions can be communicated rapidly to relevant audiences.
Commissioned by the English NHS R&D Programme, It is the sibling organization of the UK Cochrane Centre.
Systematic reviews are carried out by a research team comprised of two reviewers and a member of the Information Team, using established methodological guidelines. A panel of experts is recruited for each review to advise and to help ensure accuracy and relevance to the NHS. The CRD Information Service is available to health professionals, researchers, managers, and information workers. It answers enquiries about reviews and economic evaluations relating to health care, and acts as a helpdesk for the CRD databases.
Most of the CRD's dissemination activity focuses on raising awareness of key messages from research, and providing key research intelligence in easily accessible and usable forms. The core dissemination products include CRD reports, summaries, journal articles, and research findings summarized for the lay and professional media. Three databases have been produced by CRD and are publicly available: the Database of Abstracts of Reviews of Effects (DARE), the NHS Economic Evaluation Database and the Health Technology Assessment (HTA) database. The HTA database is of particular relevance to technology assessment agencies as it contains records of ongoing and completed projects and publications of HTA agencies around the world. All CRD databases are available free of charge and can be accessed via the Internet: (www.york.ac.uk/inst/crd/crddatabases.htm) and as part of the Cochrane Library.
Pobl. 52.000.000 USD.- 4.000.000 Staff.- 53 Col.- variable
61
Country
Agency
History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
USA VA TAP 1994 Originally formed within the research arm of the Veterans Health Administration (VA), VATAP formally aligned with VA clinical services within the Office of Patient Care Services in 2000. As a small program, VATAP views its membership to INAHTA since 1995 as a central resource for HTA products, expertise and critical review to support VA evidence-based policy.
VATAP's charge is to enhance the health of veterans and the nation by providing and fostering HTA for evidence-based health care.
? VATAP's clients are VA senior managers in Central Office and in the field. Clients may request VATAP services through the Chief Officer of Patient Care Services. VATAP applies Cochrane Collaboration methods and standards to generate qualitative systematic reviews of the medical literature. VATAP commissions or conducts descriptive research or meta-analyses, as needed. All VATAP systematic reviews are peer-reviewed by content and methods experts. Focusing on the needs of a wide range of clients, VATAP produces a variety of products and services for VA clinicians, managers and patients. Products range from brief overviews of existing high quality reviews and primary research, to concise systematic reviews called Short Reports produced within two to three months, to comprehensive systematic reviews produced over several months that may include primary data collection. VATAP's information service conducts rapid retrieval of bibliographic lists with quality filtering. Executive summaries, one-page summaries, and patient-focused pieces presented in a question and answer format are available for most reports.
Oral presentations and electronic media are VATAP's primary methods of dissemination. VATAP targets scientific venues and VA forums to promote its services. VATAP's web pages on the Internet (www.va.gov/vatap) and VA Intranet (vaww.va.gov/vatap) provide easy access to all program products, activities and related HTA links. Electronic mail is used for targeted dissemination to internal and external audiences. VATAP distributes Tech Watch, a quarterly electronic mail bulletin of selected INAHTA reports and HTA topics, to VA managers and clinicians and limited audiences outside VA.
Pobl. 7.200.000 USD.- 500.000 Staff.- 4,5 Col.- variable
62
63
y History Mission Structure/ relations Activity areas/ Work process
Dissemination activities
General info
Country
Agenc
USA AHRQ 2003 The Center for Outcomes and Evidence serves as a single point of contact for organizations searching for comprehensive evidence reviews on health conditions, treatments, and technologies. The Center is one of five research centers in AHRQ that conduct and support research to enhance the quality, appropriateness, and effectiveness of health services in the United States. AHRQ is a "science partner" with private and public organizations in their efforts to improve the quality, effectiveness, and appropriateness of clinical practice by improving the evidence base that serves as its foundation.
AHRQ's mission is to conduct and support studies of the outcomes and effectiveness of diagnostic, therapeutic and preventive health care services and procedures.
? 13 Evidence-based practice Centers (EPCs) throughout North America, which develop evidence reports and technology assessments on clinical topics that are common, expensive, and/or significant for the Medicare population. National Guideline Clearinghouse (NGC), a comprehensive, Internet-based source for clinical practice guidelines in partnership with American Association of Health Plans (AAHP) and the American Medical Association (AMA). The US Preventive Services Task Force (USPSTF), an expert panel whose members evaluate the scientific evidence for effectiveness of a range of clinical preventative services and produce recommendations for services to be included in the periodic health examination. The technology assessment program at the Agency for Healthcare Research and Quality (AHRQ) provides technology assessments for the Centers for Medicare & Medicaid Services (CMS). These technology assessments are used by CMS to inform its national coverage decisions for the Medicare program as well as provide information to Medicare carriers. AHRQ's technology assessment program uses state-of-the-art methodologies for assessing the clinical utility of medical interventions. Technology assessments are based on a systematic review of the literature, along with appropriate qualitative and quantitative methods of synthesizing data from multiple studies. Technology assessments may be done in-house by AHRQ staff, or they may be done in collaboration with one of our Evidence-based Practice Centers. When available, technology assessment topics are linked to corresponding information on the CMS Web site.
A list of completed reports and work in progress are available on the AHRQ website (www.ahrq.gov). Reports may be obtained by contacting the technology assessment program at [email protected].
Pobl. 40.000.000 USD.- 1.500.000 Staff.- 4 Col.- those who are needed
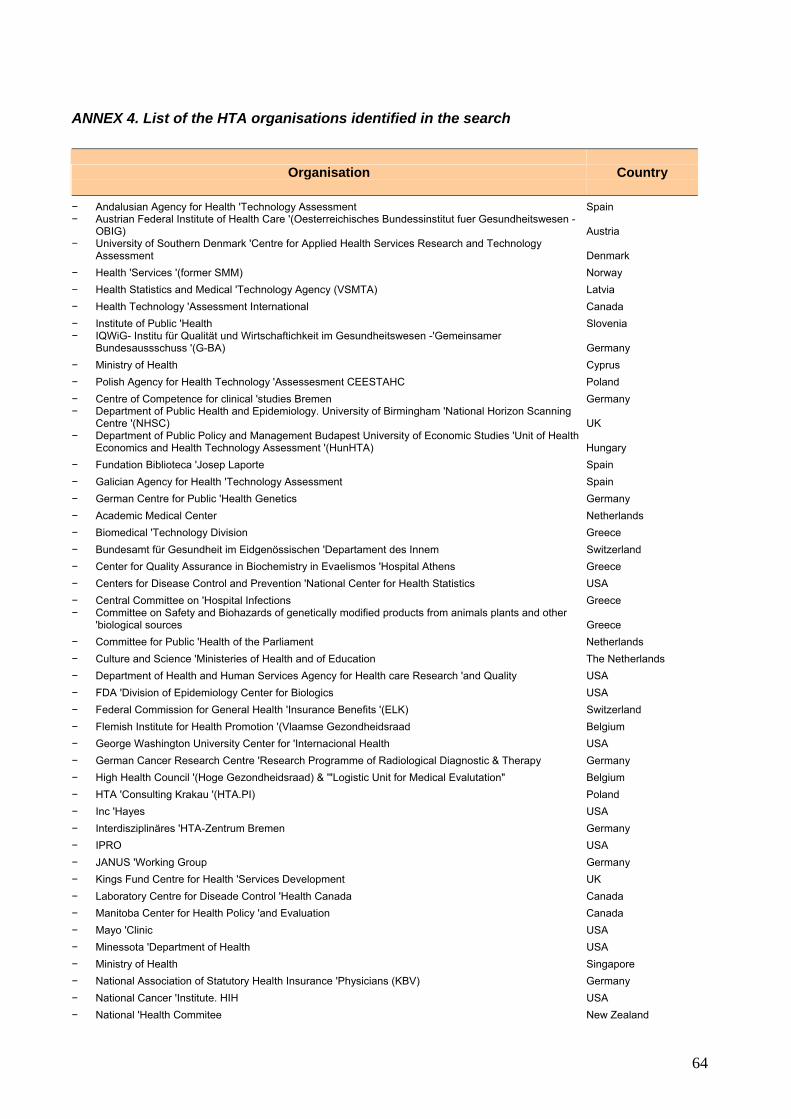
ANNEX 4. List of the HTA organisations identified in the search
Organisation
Country
− Andalusian Agency for Health 'Technology Assessment Spain − Austrian Federal Institute of Health Care '(Oesterreichisches Bundessinstitut fuer Gesundheitswesen -
OBIG) Austria − University of Southern Denmark 'Centre for Applied Health Services Research and Technology
Assessment Denmark − Health 'Services '(former SMM) Norway − Health Statistics and Medical 'Technology Agency (VSMTA) Latvia − Health Technology 'Assessment International Canada − Institute of Public 'Health Slovenia − IQWiG- Institu für Qualität und Wirtschaftichkeit im Gesundheitswesen -'Gemeinsamer
Bundesaussschuss '(G-BA) Germany − Ministry of Health Cyprus − Polish Agency for Health Technology 'Assessesment CEESTAHC Poland − Centre of Competence for clinical 'studies Bremen Germany − Department of Public Health and Epidemiology. University of Birmingham 'National Horizon Scanning
Centre '(NHSC) UK − Department of Public Policy and Management Budapest University of Economic Studies 'Unit of Health
Economics and Health Technology Assessment '(HunHTA) Hungary − Fundation Biblioteca 'Josep Laporte Spain − Galician Agency for Health 'Technology Assessment Spain − German Centre for Public 'Health Genetics Germany − Academic Medical Center Netherlands − Biomedical 'Technology Division Greece − Bundesamt für Gesundheit im Eidgenössischen 'Departament des Innem Switzerland − Center for Quality Assurance in Biochemistry in Evaelismos 'Hospital Athens Greece − Centers for Disease Control and Prevention 'National Center for Health Statistics USA − Central Committee on 'Hospital Infections Greece − Committee on Safety and Biohazards of genetically modified products from animals plants and other
'biological sources Greece − Committee for Public 'Health of the Parliament Netherlands − Culture and Science 'Ministeries of Health and of Education The Netherlands − Department of Health and Human Services Agency for Health care Research 'and Quality USA − FDA 'Division of Epidemiology Center for Biologics USA − Federal Commission for General Health 'Insurance Benefits '(ELK) Switzerland − Flemish Institute for Health Promotion '(Vlaamse Gezondheidsraad Belgium − George Washington University Center for 'Internacional Health USA − German Cancer Research Centre 'Research Programme of Radiological Diagnostic & Therapy Germany − High Health Council '(Hoge Gezondheidsraad) & '"Logistic Unit for Medical Evalutation" Belgium − HTA 'Consulting Krakau '(HTA.PI) Poland − Inc 'Hayes USA − Interdisziplinäres 'HTA-Zentrum Bremen Germany − IPRO USA − JANUS 'Working Group Germany − Kings Fund Centre for Health 'Services Development UK − Laboratory Centre for Diseade Control 'Health Canada Canada − Manitoba Center for Health Policy 'and Evaluation Canada − Mayo 'Clinic USA − Minessota 'Department of Health USA − Ministry of Health Singapore − National Association of Statutory Health Insurance 'Physicians (KBV) Germany − National Cancer 'Institute. HIH USA − National 'Health Commitee New Zealand
64

Organisation
Country
− National Institute for 'Clinical Excellence '(NICE) UK − National Institute for Health and Evionmental 'Hygiene PRIVM The Netherlands − National Technical University of Athens 'Department of Biomedical Technology Greece − Portugal 'Medical Association Portugal − Potsdam Institute of Pharmacoepidemiology and Technology Assessment '(PIPTA) Germany − Quebec Agency for Health Services and 'Technology Assessment Canada − Regional Directorate for Hospital and 'Ambulatory Services Italy − Standing Group on 'Health Technology '(SGHT) − Suzuka University of Medical Science 'and Technology Japan − Swiss Federal Office of Social Security/ Medical 'Technology Section '(MTS) Swiss − U. S. Food and 'Drug Administration USA − Utrecht 'National Organization for Quality Assurance in Hospitals Netherlands − VA Tecnology 'Assessment Program '(VATAP) USA − 'Canadian Agency for Drugs and Technologies in Health ('former CCOHTA) CADTH Canada − 'Israel Center for Technology Assessment in Health Care '(ICTAHC)' Gerther Institute Israel − Adelaide Health Technology Assessment AHTA Australia − AETMIS -Agence 'd'ëvaluation des Technologies et des Modes d'Intervention en Santé Canada − Agencia Lain Entralgo Spain − Agency for Healthcare Research and Quality Center 'for Outcome & Evidence '(AHRQ) Canada − Agency for Quality 'in Medicine '(German Agency for Quality in Medicine-AEZQ) Germany − Agency for Regional 'Health Services Italy − American 'College of Cardiology USA − American College of Obstetricians 'and Gynecologists USA − College voor Zorgverzekeringen/Health Care 'Insurance Board Netherlands − Australia and New Zealand Horizon 'Health Policy 'Scanning Network '(ANZHSN) Australia − Australian Safety and Efficat Register of New 'Interventional Pocedures-Surgical ASERNIP-S Australia − Austrian 'Academy of Sciences Austria − Department Health Care Management 'Technische Unviersität Berlin Germany − Austrian Health 'Institute OEBIG Austria − Battele Centers for Public 'Health Research USA − Belgian Health Care 'Knowledge Centre '(KCE) Belgium − Berlin 'Institut für Gesundheits und Sozialforschung '(IGES) (Häussler) Germany − Blue Cross / Blues Shield Association Technology 'Evaluation Center '(TEC) USA − Boehringer 'Ingelheim Corp Germany − British Columbia Office of Health 'Technology Assessment Canada − Büro für Technikfolgen-Abschätzung beim Deutschen 'Bundestag (TAB) '(Office of Technology
Assessment at the German Bundestag) Germany − Campus Essen Alfreid Krupp von Bohien Und Halbach-Stiftungslehrstuhis für Medizinmanagement
'Universität Duisburg Essen '(Wasem) Germany − Catalan Agency for Health Technology Assessment 'and Research '(CAHTA) Spain − CEDIT - Comité d'Evaluation et de 'Diffusion des Innovations Tecnologiques (Assistance Publique
Hôpitaux de Paris) Commitee for Evaluation and Diffusion of Innovative Technologies France − Center for Health Policy Research and Education 'Duke University USA − Center for Medical Technology Assessment (CMT) 'Linkoping University Sweden − Central and Eastem European Society for Technology Assessment in 'Health Care Poland − Emilia Romagna 'Agenzia Sanitaria Regionale Italy − Finnish Office for Health Care 'Technology Assessment '(FinOHTA) Finland − Consejeria 'de Sanidad del Gobierno de Canarias Spain − Council for 'Health Research '(RGO-Raad voor Gezondheidsonderzoek) Netherlands − Danish 'Board of Technology '(DBT) Denmark − Danish Center for Evaluation and Health 'Technology Assessment '(DACEHTA) Denmark − Danish 'Council of Etnics Denmark − Danish Institute for Health 'Service Research '(DSI) Denmark
65

Organisation
Country
− DECIT-CGATS Department of Science 'Technology-Brazilian Health Brazil − German Institute for Medical Documentation 'and Information '(DIMDI) Germany − Department of Development and Planning. 'Aalborg University Denmark − Department of Facility Sciences National 'Institute of Public Health '(HIPH) Japan − Department of Health 'and Children '(An Roinn Sláinte agus Leanai) Ireland − Department of Health Research and 'Development Directorate UK − Department of Microbiology 'Medion Group Belgium − ECRI Technology 'Assessment Program USA − Institute of Social 'Medicine: − Erasmus University Rotterdam 'Institute for Medical Technology Assessment '(iMTA) The Netherlands − Fachhochschule 'KMUB Germany − Fraunhofer Institute for Systems and 'Innovation Research '(ISI) Germany − Fritz Beske Institut für 'Gesundheits-System-Forschung Kiel Germany − Ludwig Boltzmann Institute for 'Medical Sociology '(Ludwig Boltzmann-Institu für Health Technology
Assessment) Austria − German Scientific Working Group of Technology Assessment in 'Health Care Germany − Glaxo Research and 'Development Limited UK − Hauptverband 'der Österreichischen Sozialversicherrungsträger Austria − Health Care Technology Assessment Agency 'Instituo Carlos 'III Spain − Health 'Council of the Netherlands '(Gezondheitdsraad GR) The Netherlands − Health 'Research Board '(HRB) '(ASSRR) Ireland − Health Services Research and Development Services 'U. S. Veterans Administration USA − Health Technology Assessment Unit Medical Development Division Malaysia 'Ministry of Health Malaysia − Health Technology Board for Scotland (HTBS) - NHS Quality 'Improvement Scotland '(NHS QIS) United Kingdom − HTA -Programm- Institute of Health Economics 'Alberta Heritage Foundation for Medical Research
'(AHFMR) (IHE) Canada − Inc 'Medical Technology and Practice Patterns Institute '(MTPPI) USA − Ind 'ABT Associates − Institue for Standardization & Documentation in the Medical Laboratory (INSTAND e.v.) Germany − Institut für Versicherungsbetriebsiehre 'Universität Hannover '(von der Schulendburg) Germany − Institute for Clinical Effectivenss and Health Policy Argentina − Institute for Clinical 'Evaluative Sciences Canada − Institute 'for Clinical Systems Integrations USA − Institute for Medical 'Outcomes Research '(IMOR) Germany − Institute of Applied Health Sciences. University of Aberdeen. 'Department of Public Health United Kingdom − Institute of Biomedical 'Technology '(INBIT) Greece − Institute of Health 'Economics '(IHE) Canada − Institute of Public-Health 'Radiation Hygiene Laboratrory Romania − Medical & Health Research 'Council of the Netherlands '(ZonMW) The Netherlands − Institute of Social Medicine at the University of Graz Austria − Institute of Social Medicine 'University of Viena Austria − Medical Services 'Advisory Commitee '(MSAC) Australia − Jefferson Ultrasound Research & Education Institute Thomas 'Jefferson University USA − Karlstad University 'Public Health Science Sweden − London School of Hygiene & Tropical Medicien 'European Centre on Health of Societies in Transition
'(ECOHOST) (LSHTM) United Kingdom − Medical University Luebeck 'Institute for Social Medicine Germany − Lung and Blood Institute HIH 'National Heart USA − Mario 'Negri Institute Italy − Ministry of Health of the Republic of Lithuania Lithuania − Medical 'Department of the RIZIV Belgium − Medical 'Research Council South Africa − Regione 'Veneto Italy
66

67
Organisation
Country
− Medication Use 'Management Services Canada − Medizinischer 'Dienst der Spitzenverbände der Krankenkassen '(MDS) Germany − Mexican Institute of Social Security-Health 'Systems Division Mexico − Ministry of Health and Long-Term Care Ontario 'MAS -Medical Advisory Secretariat Canada − Swedish Council on Technology Assessment in 'Health Care '(SBU) Sweden − National Center for Health Technology Excellence (CENETEC) Centro Nacional de Excelencia
Tecnológica en Salud Mexico − National Health Reserarch and Development Program 'Helath Canada Canada − National Organization 'for Medicine '(EOF) Greece − National School of Public Health Portugal − Netherland Institute of Mental Health 'and Addiction '(Trimbos instituut) Netherlands − Netherlands Institute of Primary 'Health Care '(NIVEL) Netherlands − New Zealand Health Technology '- Assessment '(NZHTA) New Zealand − New 'Zealand Ministry of Health New Zealand − NHS Quality Improvement Scotland Health Services Research & Assessment 'Unit Glasgow United Kingdom − NWO (Nederlandse Organisatie voor Wetenschappelijik Onderzoek) - Netherlands Organisation for
'Scientific Research Netherlands − Oregon Health 'Resources Commission USA − Osteba 'Basque Office for Health Technology Assessment Spain − Peking Union Medical 'College Hospital China − Pharmaceutical Benefits 'Advisory Commitee Australia − RAND 'Health USA − Univertiy of Southhampton 'National Coordinating Centre for HTA '(NCCHTA) UK − Research Centre on Technology Assessment 'on Biotechnology '(BIOGUM) Germany − Saskatchewan 'Health Canada − Semashko Scientific Research Institute of Social Hygiene & Academy of Medical Science 'Department
of Public Health Statistics Russia − Shanghai 'Blood Centre China − Swiss 'Medical Association Switzerland − SwissHTA / Swiss Netword 'for HTA Switzerland − Technische Universität Wien 'Institute of Technology and Society '(ITG) Austria − Technology Assessment Program. Office of Patient 'Care Services USA − TNO -Netherlands Organization for Applied 'Scientific Research Netherlands − TNO Prevention 'and Health Netherlands − Unidad 'de Evaluación de Tecnologías de Salud. Ministerio de Salud de Chile '(ETESA) Chile − Universität Hannover Institut für 'Versicheurengsbetriebsl ehre '(von der Schulenburg) Germany − Universitätsklinikum Schleswing-Holstein Campus Lübeck Institut 'für Sozialmedizin '(Raspe) Germany − University of Athens 'Center for Management and Evaluation Department of Nursing '(CHESME) Greece − University of Leuven Belgium − University of Oxford 'National Perinatal Epidemiology Unit UK − University of Patras 'Departmen of Medical Physics and Biomedical Engineering Greece − University of Pennsylvania 'Leonard Davis Institute of Health Economics USA − University of Sheffield 'Sheffield Centre for Health and Health Related Research UK − University of Tromso Norway − University of York 'Centre for Health Economics UK
ANNEX 5. Characteristics of European Health Care Systems (next page)
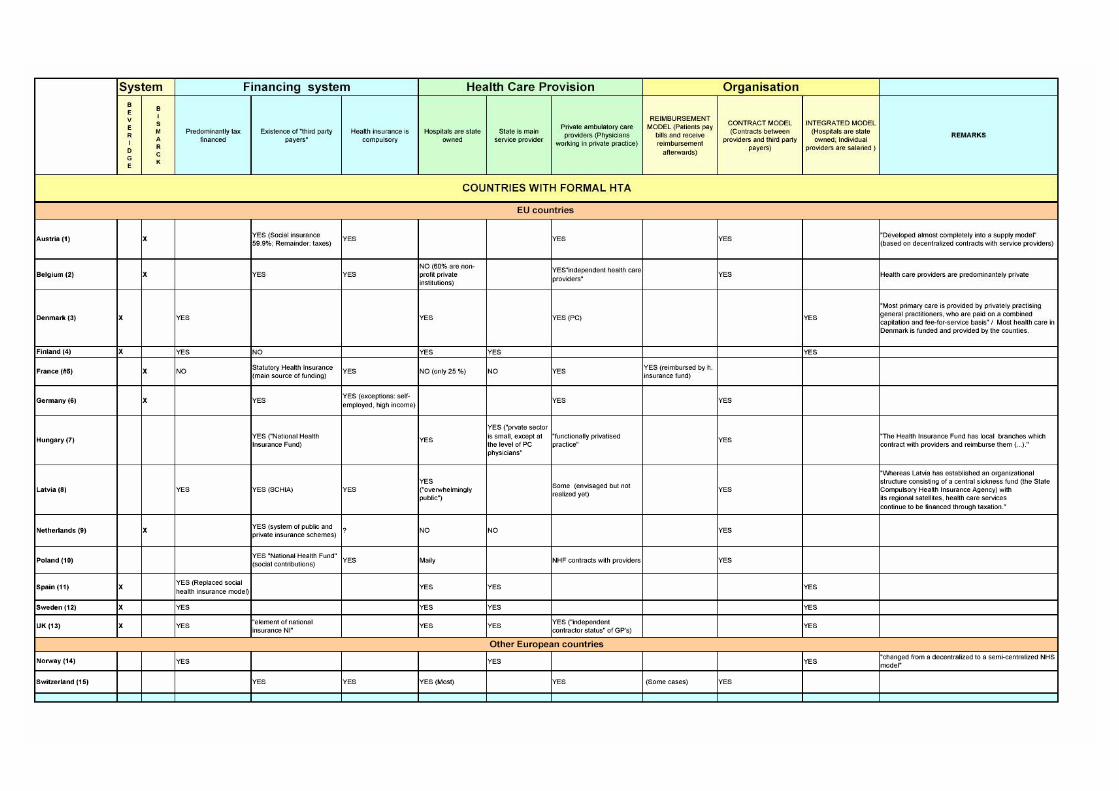
68

69

BIBLIOGRAPHY 1 Hofmarcher MM, Rack HM. Health care systems in transition: Austria
[monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006:8(3). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E89021.pdf.
2 Health care systems in transition. HiT Summary: Austria [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E89021sum.pdf.
3 Health care systems in transition: Belgium [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2000. [16 gen 2007]. Available from: http://www.euro.who.int/document/e71203.pdf.
4 Vallgarda S, Krasnik A, Vrangbaek K. Health care systems in transition: Denmark [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2001:3(7). [16 gen 2007]. Available from: http://www.euro.who.int/document/e72967.pdf.
5 Health care systems in transition. HiT Summary: Denmark [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002. [16 gen 2007]. Available from: http://www.euro.who.int/document/Obs/DENsum110802.pdf.
6 Järvellin J. Health care systems in transition: Finland [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002:4(1). [16 gen 2007]. Available from: http://www.euro.who.int/document/e74071.pdf.
7 Health care systems in transition. HiT Summary: Finland [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002. [16 gen 2007]. Available from: http://www.euro.who.int/Document/Obs/FINsum112002.pdf.
8 Sandier S, Paris V, Polton D. Health care systems in transition: France [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(2). [16 gen 2007]. Available from: http://www.euro.who.int/document/e83126.pdf.
1

9 Health care systems in transition. HiT Summary: France [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/document/e83126sum.pdf.
10 Busse R, Riesberg A. Health care systems in transition: Germany [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(9). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85472.pdf.
11 Health care systems in transition. HiT Summary: Germany [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85472sum.pdf.
12 Gaál P. Health care systems in transition: Hungary [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(4). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84926.pdf.
13 Health care systems in transition. HiT Summary: Hungary [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84926sum.pdf.
14 Health care systems in transition: Latvia [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2001. [16 gen 2007]. Available from: http://www.euro.who.int/document/e72467.pdf.
15 den Exter A, Hermans H, Dosljak M, Busse R. Health care systems in transition: Netherlands [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(6). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84949.pdf.
16 Health care systems in transition. HiT Summary: Netherlands [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84949sum.pdf.
17 Kuszewski K, Gericke C. Health care systems in transition: Poland [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005:7(5). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88670.pdf.
2
18 Health care systems in transition. HiT Summary: Poland [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88670sum.pdf.
19 Durán A, Lara JL, van Waveren M. Health care systems in transition: Spain [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006:8(4). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E89491.pdf.
20 Health care systems in transition. HiT Summary: Spain [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E89491sum.pdf.
21 Glenngard AH, Hjalte F, Svensson M, Anell A, Bankauskaite V. Health care systems in transition: Sweden [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005:7(4). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88669.pdf.
22 Health care systems in transition. HiT Summary: Sweden [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88669sum.pdf.
23 Health care systems in transition: United Kingdom [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 1999. [16 gen 2007]. Available from: http://www.euro.who.int/document/e68283.pdf.
24 Johnsen JR. Health care systems in transition: Norway [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006:8(1). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88821.pdf.
25 Health care systems in transition. HiT Summary: Norway [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2006. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E88821sum.pdf.
26 Health care systems in transition: Switzerland [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2000. [16 gen 2007]. Available from: http://www.euro.who.int/document/e68670.pdf.
3

27 Golna C, Pashardes P, Allin S, Theodorou M, Merkur S, Mossialos E. Health care systems in transition: Cyprus [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(5). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85255.pdf.
28 Health care systems in transition. HiT Summary: Cyprus [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85255sum.pdf.
29 Rokosová M, Háva P. Health care systems in transition: Czech Republic [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005:7(1). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E86823.pdf.
30 Health care systems in transition. HiT Summary: Czech Republic [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E86823sum.pdf.
31 Jesse M, Habicht J, Aaviksoo A, Koppel A, Irs A, Thomson S. Health care systems in transition: Estonia [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(11). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85516.pdf.
32 Health care systems in transition. HiT Summary: Estonia [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85516sum.pdf.
33 Health care systems in transition: Greece [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 1996. [16 gen 2007]. Available from: http://www.euro.who.int/document/e72454.pdf.
34 Espallargues M, Gallo P, Pons JMV. Sampietro-Colom L. Situació i abordatge de les llistes d'espera a Europa. Barcelona: Agència d'Avaluació de Tecnologia i Recerca Mèdiques.Servei Català de la Salut.Departament de Sanitat i Seguretat Social.Generalitat de Catalunya; 2000. Report no.: IN04/2000.
35 Donatini A, Rico A, D'Ambrosio MG, Lo Scalzo A, Orzella L, Cicchetti A et al. Health care systems in transition: Italy [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2001:3(4). [16 gen 2007]. Available from: http://www.euro.who.int/document/e73096.pdf.
4

36 Health care systems in transition. HiT Summary: Italy [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2001. [16 gen 2007]. Available from: http://www.euro.who.int/document/E73096sum.pdf.
37 Health care systems in transition: Lithuania [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2000. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E69920.pdf.
38 Health care systems in transition: Luxembourg [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 1999. [16 gen 2007]. Available from: http://www.euro.who.int/document/e67498.pdf.
39 Health care systems in transition: Malta [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 1999. [16 gen 2007]. Available from: http://www.euro.who.int/document/e67140.pdf.
40 Bentes M, Dias CM, Sakellarides C, Bankauskaite V. Health care systems in transition: Portugal [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(1). [16 gen 2007]. Available from: http://www.euro.who.int/document/e82937.pdf.
41 Health care systems in transition. HiT Summary: Portugal [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/document/E82937sum.pdf.
42 Hlavacka S, Wágner R, Riesberg A. Health care systems in transition: Slovakia [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(10). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85396.pdf.
43 Health care systems in transition. HiT Summary: Slovakia [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E85396sum.pdf.
44 Albreht T, Cessen M, Hindle D, Jakubowski E, Kramberger B, Kerstin Petric V et al. Health care systems in transition: Slovenia [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the
5
European Observatory on Health Systems and Policies; 2002:4(3). [16 gen 2007]. Available from: http://www.euro.who.int/document/E76966.pdf.
45 Health care systems in transition. HiT Summary: Slovenia [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002. [16 gen 2007]. Available from: http://www.euro.who.int/document/Obs/SVNsum122002.pdf.
46 Koulaksazov S, Todorova S, Tragakes E, Hristova S. Health care systems in transition: Bulgaria [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003:5(2). [16 gen 2007]. Available from: http://www.euro.who.int/document/e81760.pdf.
47 Health care systems in transition. HiT Summary: Bulgaria [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003. [16 gen 2007]. Available from: http://www.euro.who.int/document/e81760sum.pdf.
48 Health care systems in transition: Croatia [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 1999. [16 gen 2007]. Available from: http://www.euro.who.int/document/e68394.pdf.
49 Health care systems in transition: Romania [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2000. [16 gen 2007]. Available from: http://www.euro.who.int/document/e71423.pdf.
50 Health care systems in transition. HiT Summary: Romania [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002. [16 gen 2007]. Available from: http://www.euro.who.int/document/Obs/ROMsum122002.pdf.
51 Serdar Savas B, Karahan Ö, Ömer Saka R. Health care systems in transition: Turkey [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002:4(4). [16 gen 2007]. Available from: http://www.euro.who.int/document/E79838.pdf.
52 Health care systems in transition. HiT Summary: Turkey [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/document/E79838sum.pdf.
6

53 Nuri B. Health care systems in transition: Albania [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002:4(6). [16 gen 2007]. Available from: http://www.euro.who.int/document/E80089.pdf.
54 Health care systems in transition. HiT Summary: Albania [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003. [16 gen 2007]. Available from: http://www.euro.who.int/Document/Obs/albsum092003.pdf.
55 Cain J, Duran A, Fortis A, Jakubowski E. Health care systems in transition: Bosnia and Herzegovina [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002:4(7). [16 gen 2007]. Available from: http://www.euro.who.int/document/E78673.pdf.
56 Halldorsson M. Health care systems in transition: Iceland [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003:5(4). [16 gen 2007]. Available from: http://www.euro.who.int/document/e82881.pdf.
57 Health care systems in transition. HiT Summary: Iceland [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/document/e82881sum.pdf.
58 MacLehose L. Health care systems in transition: Republic of Moldova [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2002:4(5). [16 gen 2007]. Available from: http://www.euro.who.int/document/e81265.pdf.
59 Health care systems in transition. HiT Summary: Republic of Moldova [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004. [16 gen 2007]. Available from: http://www.euro.who.int/document/E81265sum.pdf.
60 Tragakes E, Lessof S. Health care systems in transition: Russian Federation [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003:5(3). [16 gen 2007]. Available from: http://www.euro.who.int/document/e81966.pdf.
61 Health care systems in transition. HiT Summary: Russian Federation [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2003. [16 gen 2007]. Available from: http://www.euro.who.int/document/Obs/russum.pdf.
7

62 Lehkan V, Rudiy V, Nolte E. Health care systems in transition: Ukraine [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2004:6(7). [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84927.pdf.
63 Health care systems in transition. HiT Summary: Ukraine [resum]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2005. [16 gen 2007]. Available from: http://www.euro.who.int/Document/E84927sum.pdf.
8

ANNEX 6. BIBLIOGRAPHY 1 Jonsson E, Banta HD, Henshall C, Sampietro-Colom L. Executive Summary of
the ECHTA/ECAHI project. Int J Technol Assess Health Care. 2002;18(2):213-7.
2 Draborg E, Gyrd-Hansen D. Time-trends in health technology assessments: an analysis of developments in composition of international health technology assessments from 1989 to 2002. Int J Technol Assess Health Care. 2005;21(4):492-8.
3 Oliver A, Mossialos E, Robinson R. Health technology assessment and its influence on health-care priority setting. Int J Technol Assess Health Care. 2004;20(1):1-10.
4 Jonsson E, Banta HD, Henshall C, Sampietro-Colom L. Summary report of the ECHTA/ECAHI project. European Collaboration for Health Technology Assessment/Assessment of Health Interventions. Int J Technol Assess Health Care. 2002;18(2):218-37.
5 Dauben HP, Forde OH, Loud ML, Isacsson SO, Paccaud F, Sanchez E et al. Health promotion and disease prevention as a complement to community health indicators. Working group 1. Int J Technol Assess Health Care. 2002;18(2):238-72.
6 Hagenfeldt K, Asua J, Bellucci S, Jensen MF, Morland B, Oortwijn W et al. Systems for routine information sharing in HTA. Working group 2 report. Int J Technol Assess Health Care. 2002;18(2):273-320.
7 Estrada MD, Asplund K, Barrington R, Faisst K, Kahan JP, Kjonniksen I et al. European joint assessments and coordination of findings and resources. Working group 3 report. Int J Technol Assess Health Care. 2002;18(2):321-60.
8 Velasco M, Perleth M, Drummond M, Gurtner F, Jorgensen T, Jovell A et al. Best practice in undertaking and reporting health technology assessments. Working group 4 report. Int J Technol Assess Health Care. 2002;18(2):361-422.
9 Antes G, Briones E, Britton M, Burnand B, Engel G, Gallo P et al. Education and support networks for assessment of health interventions. Working group 5 report. Int J Technol Assess Health Care. 2002;18(2):423-46.
10 von Below GC, Boer A, Conde-Olasagasti JL, Dillon A, Gibis B, Grilli R et al. Health technology assessment in policy and practice. Working group 6 report. Int J Technol Assess Health Care. 2002;18(2):447-55.
11 Estrada MD, Serra-Sutton V. Rajmil L. Overview of the implementation of the health technology assessment activities in a broad representatio of world health organisation-collaborating centres [consulta técnica]. Barcelona: Agència d'Avaluació de Tecnologia i Recerca Mèdiques.Servei Català de la Salut. Departament de Sanitat i Seguretat Social.Generalitat de Catalunya; 20012. Report no.:
12 Mears R, Taylor R, Littlejohns P. Dillon A. Review of International Health Technology Assessment (IHTA). Project Report. London: National Institute for Clinical Excellence (NICE); 2000. Report no.:
9

13 Perry S, Gardner E, Thamer M. The status of health technology assessment worldwide. Results of an international survey. Int J Technol Assess Health Care. 1997;13(1):81-98.
14 Health technologies and decision making. Paris (France): Orgnisation for Economic Co-operation and Development (OECD); 2006.
15 Chew DP. Cost-effectiveness of drug-eluting stents: if only all things were equal! Med J Aust. 2006;182(8):376-7.
16 Health care systems in transition: Romania [monografia a internet]. Copenhagen (Denmark): WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies; 2000. [16 gen 2007]. Available from: http://www.euro.who.int/document/e71423.pdf.
10

Annex WP8.2
Characteristics of HTA organizations at international level
Survey’s elaboration
Catalan Agency for Health Technology Assessment and Research CAHTA
11

INDEX 1.INTRODUCTION ....................................................................................................... 13 2. METHODOLOGY ..................................................................................................... 14 3.RESULTS .................................................................................................................. 15
3.1 Survey design ..................................................................................................... 15 3.2 Pilot test .............................................................................................................. 18 3.3 Sampling frame................................................................................................... 20 3.4 Distribution of the survey .................................................................................... 21
4. ANNEXES............................................................................................................. 22
ANNEX 1.Collaborative organisations in different WP ............................................. 22 ANNEX 2.Comparison among the questionnaires of previous studies, INHATA information and WP8 project protocol....................................................................... 24 ANNEX 3.List of associated and collaborative partners to whom the pilot test survey was sent.................................................................................................................... 25 ANNEX 4.List of the HTA organisations surveyed in November 2006 ..................... 26 Annex 5.Final version of the questionnaire............................................................... 29 ANNEX 6.BIBLIOGRAPHY....................................................................................... 48
12

1.INTRODUCTION
In order to achieve the first objective of WP8 two strategies were decided:
− To carry out a review of HTA organisations at international level − To elaborate a survey of the active or in process of being a European HTA unit, agency or programme. The introduction and the first objective of WP8 can be consulted in the review report (appendix 1 of the technical report). This report is focused on the survey.
13

2. METHODOLOGY
Design
A cross-sectional survey by means of a semi-structured questionnaire.
Sampling The sampling procedure was based on a list elaborated from different sources: INAHTA, and the list of participants of previous studies that had done surveys in the past. Specifically:
− EUnetHTA partners − INAHTA (International Network of Agencies for HTA) website − Websites of existing HTA units, agencies or programmes − Report on overview of the implementation of activities related to evidence based practice in a
broad representation of world health organization-collaborating centres, a survey conducted by the CAHTA (Catalan Agency for Health Technology Assessment and Research) in 2002 1
− Project report on review of International Health Technology Assessment (IHTA). National Institute for Clinical Excellence 2000. 2
− The status of health technology assessment worldwide. Results of an international Survey. MTPPI 1997. 3
The inclusion criteria for the identified organisations were: any HTA organisation performing HTA all around the world that their web page and contact details could be found.
The search period for the previous sources was March-May of 2006. Pilot test The last version of the questionnaire was send on August 2006 to the collaborative and associated partners of WP8. E-mail and telephone reminders were conducted in September. Suggestions from responders were introduced in the questionnaire. Workplan of the questionnaire design:
- Constitution of the survey elaboration group of experts (HTA, Information and documentation) and permanent review of questionnaire drafts
- Suggestions from the review of characteristics of HTA organisations (review report) - Review of surveys of HTA organisations of previous studies - Pilot test survey was sent to associated and collaborative partners of WP8 - Final version of WP8 survey
14

3.RESULTS
3.1 Survey design
For the elaboration of the WP8 questionnaire, the CAHTA team for WP8 set a working group. The expertise of working group members came from different fields (HTA, Information and documentation, and elaboration of surveys). The working group assessed periodically the questionnaire draft, in order to guarantee that the WP8 questionnaire was collecting the relevant information for WP8 objectives.
The working group for the elaboration of the questionnaire decided to review more in depth the contents of previous surveys of HTA organisations in order not to overlap work and as a guide to establish the contents of interest for the WP8 survey. The previous studies selected were:
• Review of International Health Technology Assessment (IHTA). NICE 2000 3 • The status of health technology assessment worldwide. Results of an international survey. Medical Technology
and Practice Patterns Institute (MTPPI). 1997 2 • Overview of the implementation of the health technology assessment activities in a broad representation of world
health organization-collaborating centres (WHO). CAHTA 2002 1
The HTA organisations surveyed in each study were different depending on the inclusion criteria taken into account for each of them. As is shown in table 1, there were different broads on the inclusion criteria. The NICE 2000 study only surveyed non-for-profit HTA organisations, while WHO 2002, surveyed any WHO collaborating centre working in anything related with HTA. MTPPI 1997, surveyed every institution with active HTA programmes, being public or private funded.
The surveys elaborated for the NICE and the WHO studies were reviewed in order to assess their contents. It was not possible to obtain the MTPPI survey. The table in annex 2 summarises the comparison among the contents of these surveys, INAHTA member’s information and the sections proposed in WP8 project protocol. Both had different objectives and those were different from the WP8 ones, the NICE study was more focused on ‘Health Policy Decisions’ specifically on HTA and Guidelines activities, whereas the WHO study was more broad and descriptive. However, this comparison was very useful for the elaboration of the questionnaire. INAHTA information, as the review report explains, was very variable since each organisation answered an open question, however the main contents given by the organisations were summarised in the table.
All the approaches, or almost all, took into account the information related to the scope of the organisation, objectives, funding, main activities, staff, and strategies of results dissemination, but sometimes this information was located in different sections. Other information was collected only by one or two of the approaches: work process, history (establishment) and health policy decisions.
15

Table 1. Inclusion criteria for the previous studies surveying HTA organisations NICE 2000 MTPPI 1997 WHO 2002
Incl
usio
n cr
iteria
‘not-for-profit’ organizations
Health Technology Policy organization.- those whose outputs impact upon the health care decision making process.
Organizations with active HTA programs, were HTA is:
HTA.- any study or inquiry the objective of which is to provide information regarding the effects of a technology designed to maintain or improve health or to be used as a part of an intervention for such purposes, whether or not the study evaluate the effects.
HTA organization could be a professional, trade, or other association, university or other not-for-profit entity, government agency, or for-profit corporation.
An ongoing HTA program could be a structure or process within a given organization, if not the entire organization, that assess medical technologies and generates assessment reports.
1. Being a WHO collaborating centre 2. Being ascribed to any of the who programmes falling in what was considered ‘Health technology’ or ‘health intervention assessment’: Health policy and management Health system research and
development National health systems and policies Organization and management of
health systems based on primary health care
Health in socio-economic development Health, science and public policy Epidemiology, statistics, trend
assessment and country health information
National health policies and programmes development and management
Research policy and strategy co-ordination
Quality of care and health technology Technology for health care
The first draft of the questionnaire was elaborated on the bases of these comparisons and considering the specific objectives of WP8. The information collected from the different sources (INAHTA members information and surveys of previous studies) and from the specific interest of the project were organised into 6 sections:
Identification and establishment of the centre. Contact details were considered as relevant information for the organisation of the survey and further consultations. Information about the establishment of the organisation (initiative of foundation, year, etc.), main barriers and solutions were considered interesting for the project.
Specific setting. In this first draft, to gate information about the health care system, provision of healthcare, scope of the organisations work, profile of the organisation and collaborations was considered of relevance.
Aims and scope. For this section, to collect information about having a Strategic plan or approved statutes, the main line of activities and types of products and the distribution of the recommendations was considered relevant.
Structure. It was considered important to gate information about the organization, staff, sponsors and funders and the material resources the organisation counts with.
Work process. In this first draft, the information considered as relevant was related to the priority setting and the topics considered in HTA.
Visibility of results. In relation with this section, the information considered for the first draft was the strategies took and the intended users.
Table 2 summarises the main information that was considered of interest to be collected by the survey.
16

Table 2. Possible questions to include in the WP8 survey after INAHTA members data review
Identification and establishment of the centre Contact details Name, address, country, telephone, fax, e-mail, website,
name of director or responsible person Year of establisment Who founded the unit? Government, group of researchers, etc. Main barriers in the establishment Solutions to this barriers
Specific setting of the organization
Health care system in its country Central government, decentralised government, market-oriented
Method of provision of the healthcare Patients reimbursement of their bills, state owns the hospitals, etc.
Level of work of the organization Local-regional, national, international ‘Profile’ of the organization Government agency, professional association, not-for
profit, for-profit collaboration with other organizations collaboration with other countries
Aims and scope of the organization
strategic plan? Approved statutes? Main lines of activities HTA, research, quality assessment or management in
healthcare, elaboration and/or evaluation of guidelines, Types of products Assessment report, research project, technical
consultation, counselling, quick response service, academic and training activities, technical appraisals, patients information
Level of distribution of the recommendations Local-regional, national, international
Structure of the organization
4. Organization of the centre Executive board, scientific committee, direction. Associated researchers, collaborators, advisors
5. Staff number 6. Areas of expertise of staff Economist, epidemiologist, social scientist, public health
professionals, statisticians, health services researchers, information specialist, psychologist
7. Structures the organization count with Workspaces, personal computers, intranet, library, meeting room, database
8. Sponsors and funders Government, research funding bodies, private industries, intergovernmental organization, donor agencies
Work process of the organization
9. Responsible for setting priorities 10. Process for priority setting 11. Criteria for priority setting Burden of disease, cost-effectiveness, burden of disease
determinants, equity, etc. 12. Advisory mechanism in priority setting Experts, health care professionals,
policymakers/government representatives, patients representatives
13. Topics considered in HTA Efficacy/effectiveness, quality/safety, total cost saving, psychological and ethical considerations, organizational and professional implications, equity, cost-effectiveness, media attentions, political considerations, etc.
Visibility of the results of the organization
14. Dissemination strategy? 15. Strategies took Corporative image, electronic and printed versions of
newsletter, electronic and printed versions of reports, website, published papers in national scientific journals, published papers in international scientific journals, etc..
16. Intended users General public, health services researchers, professional associations, patients groups, health service managers, consumer associations, government agencies, health service administrators, professional allied of medicine, carers, media, etc.
17
The review of this first draft made by the working group raised up some suggestions that were added in order to improve the questionnaire. On several meetings the working group decided a list of modifications:
1. Generals suggestions. To reduce as open questions as possible. To introduce clear definitions for each concept, in order to improve the comparability of the
answer of the different organisations To introduce a first filter question (with definitions) in order to avoid that organisations not actually
developing HTA could answer the questionnaire To specify that all the questions are related only to HTA units, if it is into a biggest organisation
2. Contact details To ask for the name and position of the person who is answering the questionnaire To distinguish among micro and mesolevel decision-makers
3. Specific setting To ask in different questions about the profile of the organisation and if it is for-profit or not-for-
profit Not to ask about the health Care system or the provision of healthcare of the organisation’s
country since this information is available from other sources To add a question about the possibility that the government enacted a HTA supporting policy or
act. 4. Aims and Scope
To add a question about the main types of health technology that the organisation use to asses To ask about the main ‘customers’ the organisation have To ask about to whom does the organisation address its recommendations
5. Structure To add a question to gate information about the nomination of the executive board and scientific
/advisory committee To ask about the contractual situation and category of the staff To ask more in depth about the private funding the organisation receives
6. Work process To define criteria for setting priorities in a closed question To ask about the main barriers and solutions the organisation finds in their daily work To ask about the way the organisations ensure the quality of their products To ask about the assessment of impact of the organisation recommendations (how often they do
it, inclusion of indicators to evaluate it in their reports, the criteria used, and their opinion about the most important strategies to reach a high impact)
7. Visibility of results Not to add more questions since there should be a second specific questionnaire for information
needs of the organisations
All these considerations were take by the working group for the elaboration of the last draft of the questionnaire that was sent to the associated and collaborative partners of WP8 in a pilot test (26 organisations).
3.2 Pilot test
The pilot test survey was conducted in August 2006 in order to know if the questionnaire was understandable for the organisations surveyed and to improve it with their suggestions and comments. The pilot test, also, was a way to learn more about the time needed to answer the questionnaire and to ask WP8 partners their opinion about the questionnaire and if they were finding any important missing topic. E-mail and telephone reminders were done in September and October in order to increase the response rate. We obtained answers from 61,5% of the overall interviewed agencies and units. Exactly, nine out of the 11 associated partners answered the questionnaire, 4 of them declared no HTA activity. Seven out of 15 collaborative partners, returned us the fulfilled questionnaire. Two of them declared no HTA activity.
Table 3. Main outcomes of the pilot test of W8 questionnaire Quest.
Comments/Observations
18

General Make more clear that questions should be answered only for the HTA unit, if this is located into a biggest organisation
General ‘Too heavy’ questionnaire.- try to compact/reduce questions General Correction of English General When more than an option is possible, indicate it to responders (questions 4, 8, 27, 35 & 46)
New Q Is the organisation part of a regional/national/international network with other organisations’ New Q When establishing a new agency, it is important to have?
- A clear mission - Good anchoring and network - Engaged staff - Funding - Opportunities of education - A director with a good reputation
1 To change the answer format? 4 & 5 Include the ‘no barriers’ category option 6 & 7 Merge them
15 Disagreement with categories answer 16 Others: main biomedical equipments; Disagreement with the inclusion of ‘early warning’ 17 2 questions for products & services.
Add: quick response, consultation & training 18 Include as category answer: private sector (industry); Difficult question to understand 21 Just ask for organisational structure 25 Add another professionals profiles: graphics, students, pharmacist, advocacy, engineers on
biotechnology, public relations, electronic engineer, biomedical engineer, health policy & HTA 26 Is it necessary to ask for this question? 33 Make it before question 32; Before Q 30; if not go to Q 35 36 Change the question: ‘How are you trying to solve these limitations?’ 37 Add: educational, cultural & equity implications/aspects 39 If the organisations doesn’t make recommendations go to question 45 41 Include examples 43 Suggest categories answer; This is a difficult item to answer 44 ‘High readability of products/reports’ for ‘Narrative appropriateness’
The time needed for responders to answer the questionnaire was among 40 and 300 minutes. The average was 122 minutes, 5 of the responders spent 60 or less minutes; 2 responders spent 80 and 90 minutes (respectively) and 4 responders among 160 and 300 minutes. It was observed that those responders with high knowledge of the organisation had spent less time in filling in the questionnaire (directors, heads of units, etc.)
The 11 fulfilled questionnaires were analysed and comments and suggestions were collected from them. The main comments related to W8 questionnaire are shown in table 3. These comments were discussed by the working group. Some of the suggestions were turned down for different reasons. For example, suggestions to reroute responders if their organisation is not responsible for setting priorities was actually included in the draft of the questionnaire. Also, comments related to the extend of the questionnaire were took into account, but the team conclude that the objective of the questionnaire was to collect all this information in order to gather new information not collected before by other previous studies. Most of the comments and suggestions were included resulting in the following changes:
- A remark about the needs to answer the questionnaire taking into account only the HTA unit, if the organisation was undertaking other kinds of activities, was included in the first page of the questionnaire
- The space to answer question 1 was reduced - A ‘No barriers’ option was included in question 4, rerouting responders to question 6 if this option
was selected. - The category answer ‘ Horizon scanning system / Early warning / Emerging technologies’, from
question 16, was reduced to ‘Emerging technologies’ - A ‘Public Health Intervention’ category answer was included in question 16 - Question 33 was moved before question 31 - Question 36 was changed for ‘How is your organisation trying to resolve these barriers?’ - In question 37, equity option was included as a category answer, and ‘social’ option was changed
for ‘Social / Cultural’
19
- For the open question 43, a 4 category answer was included (high, moderate, few and none) asking responders to justify their answer
- The category answer ‘narrative appropriateness’ was changed for ‘High readability of products/reports’ in question 44
- A new question was included:
48. Which of the following aspects do you consider important in the establishment of a new agency?
Please, select the three more relevant
Clear mission
Engaged staff
Funding
Good anchoring and network
Education opportunities
Director with a good reputation
Political opportunity
Involvement system stakeholders
Lack of conflict of interest
Others. Please specify:
- The English was reviewed for an English speaker - Two versions of the questionnaire (access file and a word document) were developed in order to
make easier to answer it.
The final version of the questionnaire can be consulted in annex 4 .
3.3 Sampling frame
The definitive list of HTA organisations to be surveyed was elaborated by merging the information from the different sources:
− EUnetHTA partners − INAHTA (International Network of Agencies for HTA) website − Websites of existing HTA units, agencies or programmes − Report on overview of the implementation of activities related to evidence based practice in a
broad representation of world health organization-collaborating centres, a survey conducted by the CAHTA (Catalan Agency for Health Technology Assessment and Research) in 2002 1
− Project report on review of International Health Technology Assessment (IHTA). National Institute for Clinical Excellence 2000. 2
− The status of health technology assessment worldwide. Results of an international Survey. 1997. 3
It was necessary to improve this list because of the duplication of organisations and for the co-existing old and new names of the same HTA organisation. An excel document was elaborated. A search in internet was done in order to identify web pages, e-mails and telephone contacts of the HTA organisations and to find out if they were really performing HTA activities.
From the 363 HTA organisations found, 174 were eliminated because different reasons: for 64 of them was not possible to find a web page, for 53 organisations was demonstrated they did not perform HTA, other 57 organisations were duplicated in the different sources. Also, all the organisations without personalised e-mail address, were eliminated. Finally, 126 organisations complied with all this criteria. The definitive list can be consulted in annex 5.
20

3.4 Distribution of the survey
The questionnaire was sent via internet to the 126 organisations identified in November 2006. Thirteen questionnaire were received before 31 of December. E-mail reminders had been conducted and telephone reminders are planed in January 2007, in order to improve the response rate.
21
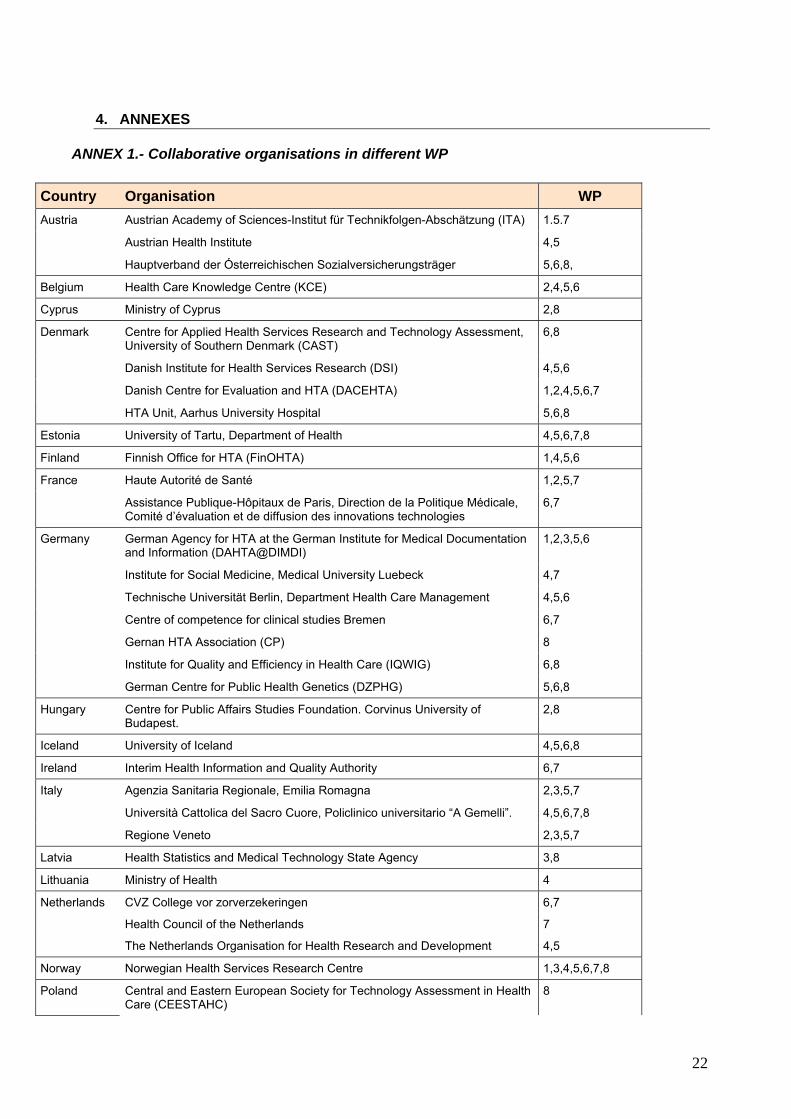
4. ANNEXES
ANNEX 1.- Collaborative organisations in different WP
Country Organisation WP Austrian Academy of Sciences-Institut für Technikfolgen-Abschätzung (ITA) 1.5.7
Austrian Health Institute 4,5
Austria
Hauptverband der Ósterreichischen Sozialversicherungsträger 5,6,8,
Belgium Health Care Knowledge Centre (KCE) 2,4,5,6
Cyprus Ministry of Cyprus 2,8
Centre for Applied Health Services Research and Technology Assessment, University of Southern Denmark (CAST)
6,8
Danish Institute for Health Services Research (DSI) 4,5,6
Danish Centre for Evaluation and HTA (DACEHTA) 1,2,4,5,6,7
Denmark
HTA Unit, Aarhus University Hospital 5,6,8
Estonia University of Tartu, Department of Health 4,5,6,7,8
Finland Finnish Office for HTA (FinOHTA) 1,4,5,6
Haute Autorité de Santé 1,2,5,7 France
Assistance Publique-Hôpitaux de Paris, Direction de la Politique Médicale, Comité d’évaluation et de diffusion des innovations technologies
6,7
German Agency for HTA at the German Institute for Medical Documentation and Information (DAHTA@DIMDI)
1,2,3,5,6
Institute for Social Medicine, Medical University Luebeck 4,7
Technische Universität Berlin, Department Health Care Management 4,5,6
Centre of competence for clinical studies Bremen 6,7
Gernan HTA Association (CP) 8
Institute for Quality and Efficiency in Health Care (IQWIG) 6,8
Germany
German Centre for Public Health Genetics (DZPHG) 5,6,8
Hungary Centre for Public Affairs Studies Foundation. Corvinus University of Budapest.
2,8
Iceland University of Iceland 4,5,6,8
Ireland Interim Health Information and Quality Authority 6,7
Agenzia Sanitaria Regionale, Emilia Romagna 2,3,5,7
Università Cattolica del Sacro Cuore, Policlinico universitario “A Gemelli”. 4,5,6,7,8
Italy
Regione Veneto 2,3,5,7
Latvia Health Statistics and Medical Technology State Agency 3,8
Lithuania Ministry of Health 4
CVZ College vor zorverzekeringen 6,7
Health Council of the Netherlands 7
Netherlands
The Netherlands Organisation for Health Research and Development 4,5
Norway Norwegian Health Services Research Centre 1,3,4,5,6,7,8
Poland Central and Eastern European Society for Technology Assessment in Health Care (CEESTAHC)
8
22
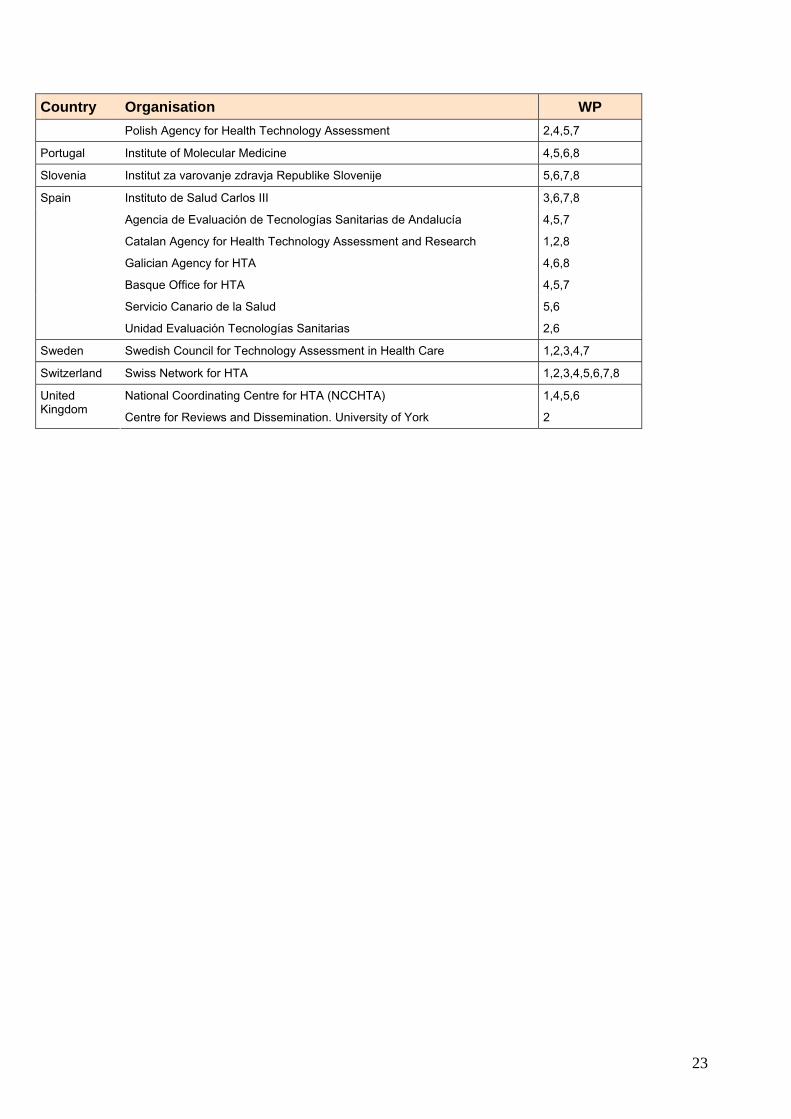
23
Country
Portuga
Sloven
Spain
Sweden
Switze
UnitedKingdom
Organisation WP Polish Agency for Health Technology Assessment 2,4,5,7
l Institute of Molecular Medicine 4,5,6,8
ia Institut za varovanje zdravja Republike Slovenije 5,6,7,8
Instituto de Salud Carlos III 3,6,7,8
Agencia de Evaluación de Tecnologías Sanitarias de Andalucía 4,5,7
Catalan Agency for Health Technology Assessment and Research 1,2,8
Galician Agency for HTA 4,6,8
Basque Office for HTA 4,5,7
Servicio Canario de la Salud 5,6
Unidad Evaluación Tecnologías Sanitarias 2,6
Swedish Council for Technology Assessment in Health Care 1,2,3,4,7
rland Swiss Network for HTA 1,2,3,4,5,6,7,8
National Coordinating Centre for HTA (NCCHTA) 1,4,5,6
Centre for Reviews and Dissemination. University of York 2

24
ANNEX 2. Comparison among the questionnaires of previous studies, INHATA information and WP8 project protocol Project protocol INAHTA information WHO Questionnaire NICE Questionnaire
•
• • Scope
StrategiLines of aProductsTarget stakeholder
• StructBackgroundInfrasfunding
• Work proce
• History Year establishment
Kind establishment (new, fusion existing units, from a existing group)
Who ask for establishment
• Identification items Name, address, contact details WHO’s collaborating program WHO’s collaborating description
• Identification items Name, address, contact details Establishment date
• Objectives/mission • Objectives • Objectives : c and business plan
ctivity /services portfolio
• Influence area (local, national, international)
Structure Funding Staff Annual budget
• Structure Funding Background human profile Are they composed by different subgroups? Are they into a biggest structure? Annual budget Annual projects Population served Description population served Staff Consultants
• Structure and funding Funding (public, private industry, research, non for profit organizations, others. Full time staff Staff’s work areas
ure: human profile
tructure resources
• Work areas New technologies GPC up date Cost-effect evaluations Research management Quality evaluation Etc
• Evidence-based production Centre’s activities
List of HTA in last 12 months Current HTA’s HTA programmed for next year
• Information about activities Who priorises work?
ss: • How works Who ask for the evaluations, reports, etc.?
Do they priorise topics to evaluate? How they priorise them? Work methodology (qualitative, quantitative) Who participles in evaluations?
HTA External help HTA specifications Kind of intervention evaluated Information’s sources used HTA’s Internal teams
GuidelinesSpecific area? Assessment’s mechanisms Output (professionals, patients, reports) Up date strategies Up date teams?
• Visibility: Information and dissemination management strategies of the HTA products and services
• Dissemination activities Web Electronical / conventional mailings Conference, etc. Peer review journals Bulletins Annual reports Teaching
• Result Dissemination and users relation
• Results dissemination Output users?
Publications, web, reports List of outputs Dissemination strategy?
• Health policy decisions Process?
Kind of health policy (equipment, health services, services payment, others)

ANNEX 3. List of associated and collaborative partners to whom the pilot test survey was sent
Associated partners (n=11) Country OrganisationSpain Cochrane
Italy Università Cattolica del Sacro Coure, Policlinico universitario "A. Gemelli"
Spain Avalia
Cyprus Ministry of Health Cyprus
Estonia University of Tartu - Department of Public Health
Spain Agència de Evaluación de Tecnologías Sanitarias - Instituto de Salud "Carlos III"
Slovenia Institute of Public Health of the Republic of Slovenia
Hungary Unit of Health Economics/Health Technology Assessment - Corvinus University of Budapest
Denmark CAST - University of Southern Denmark, Center for Applied Research and Technology Assessment
Norway NOKC Norwegian Knowledge Center for the Health Services
Latvia VSMTA - Health Statistics and Medical Technology Agency
Collaborative partners (n=15) Country OrganisationDenmark WHO Health Evidence Network (HEN)
Switzerland Swiss Network for Health Technology Assessment
Poland CEESTAHC
UK EuroScan - European Information Network on New and Changing Health Technologies
Poland Agency for Health Technology Assessment
Germany German HTA Association
Portugal Institute of Molecular Medicine
Sweden INAHTA Secretariat
Germany Public Health Genetics European Network (PHGEN)
Austria Hayotverband der Österriechischen
Belgium European Observatory on Health Systems
Canada HTAi
France Council of Europe
Germany IQWIG. Institute for Quality and Efficiency in Health Care
Island University of Iceland, Faculty of Medicine
25

ANNEX 4. List of the HTA organisations surveyed in November 2006
Organisation
Country
1. Adelaide Health Technology Assessment AHTA Australia 2. AETMIS -Agence d'ëvaluation des Technologies et des Modes
d'Intervention en Santé Canada
3. Agencia Lain Entralgo Spain 4. Agency for Healthcare Research and Quality Center for Outcome &
Evidence (AHRQ) Canada
5. Agency for Quality in Medicine (German Agency for Quality in Medicine-AEZQ)
Germany
6. Agency for Regional Health Services (ASSRR) Italy 7. American College of Cardiology USA 8. American College of Obstetricians and Gynecologists USA 9. Andalusian Agency for Health Technology Assessment Spain 10. Australia and New Zealand Horizon Scanning Networkk (ANZHSN) Australia 11. Australian Safety and Efficacy Register of New Interventional Pocedures-
Surgical ASERNIP-S Australia
12. Austrian Academy of Sciences Austria 13. Austrian Federal Institute of Health Care (Oesterreichisches
Bundessinstitut fuer Gesundheitswesen - OBIG) Austria
14. Austrian Health Institute OEBIG Austria 15. Battele Centers for Public Health Research USA 16. Belgian Health Care Knowledge Centre (KCE) Belgium 17. Berlin Institut für Gesundheits und Sozialforschung (IGES) (Häussler) Germany 18. Blue Cross / Blues Shield Association Technology Evaluation Center
(TEC) USA
19. Boehringer Ingelheim Corp Germany 20. British Columbia Office of Health Technology Assessment Canada 21. Büro für Technikfolgen-Abschätzung beim Deutschen Bundestag (TAB)
(Office of Technology Assessment at the German Bundestag) Germany
22. Campus Essen Alfreid Krupp von Bohien Und Halbach-Stiftungslehrstuhis für Medizinmanagement Universität Duisburg Essen (Wasem)
Germany
23. CEDIT - Comité d'Evaluation et de Diffusion des Innovations Tecnologiques (Assistance Publique Hôpitaux de Paris) Commitee for Evaluation and Diffusion of Innovative Technologies
France
24. Center for Health Policy Research and Education Duke University USA 25. Center for Medical Technology Assessment (CMT) Linkoping University Sweden 26. Centre of Competence for clinical studies Bremen Germany 27. College voor Zorgverzekeringen/ Health Care Insurance Board Netherlands 28. Consejeria de Sanidad del Gobierno de Canarias Spain 29. Council for Health Research (RGO-Raad voor Gezondheidsonderzoek) Netherlands 30. Danish Board of Technology (DBT) Denmark 31. Danish Council of Etnics Denmark 32. Danish Institute for Health Service Research (DSI) Denmark 33. DECIT-CGATS Department of Science Technology-Brazilian Health Brazil 34. Department Health Care Management Technische Unviersität Berlin Germany 35. Department of Development and Planning. Aalborg University Denmark 36. Department of Facility Sciences National Institute of Public Health (HIPH) Japan 37. Department of Health and Children (An Roinn Sláinte agus Leanai) Ireland 38. Department of Health Research and Development Directorate UK 39. Department of Microbiology Medion Group Belgium 40. Department of Public Policy and Management Budapest University of Hungary
26

Organisation
Country
Economic Studies Unit of Health Economics and Health Technology Assessment (HunHTA
41. ECRI Technology Assessment Program USA 42. Emilia Romagna Agenzia Sanitaria Regionale Italy 43. Erasmus University Rotterdam Institute for Medical Technology
Assessment (iMTA) Fachhochschule KMUB Netherlands
44. Finnish Office for Health Care Technology Assessment (FinOHTA) Finland 45. Canadian Agency for Drugs and Technologies in Health (former
CCOHTA) CADTH Canada
46. Fraunhofer Institute for Systems and Innovation Research (ISI) Germany 47. Fritz Beske Institut für Gesundheits-System-Forschung Kiel Germany 48. German Centre for Public Health Genetics Germany 49. German Institute for Medical Documentation and Information (DIMDI) Germany 50. German Scientific Working Group of Technology Assessment in Health
Care Germany
51. Hauptverband der Österreichischen Sozialversicherrungsträger Austria 52. Health Council of the Netherlands (Gezondheitdsraad GR) Netherlands 53. Health Research Board (HRB) Ireland 54. Health Services Research and Development Services U. S. Veterans
Administration USA
55. Health Technology Assessment International Canada 56. Health Technology Assessment Unit Medical Development Division
Malaysia Ministry of Health Malaysia
57. HTA -Programme- Institute of Health Economics Alberta Heritage Foundation for Medical Research (AHFMR) (IHE)
Canada
58. Inc Medical Technology and Practice Patterns Institute (MTPPI) USA 59. Ind ABT Associates 60. Institut für Versicherungsbetriebsiehre Universität Hannover (von der
Schulendburg) Germany
61. Institute for Clinical Effectiveness and Health Policy Argentina 62. Institute for Clinical Evaluative Sciences Canada 63. Institute for Clinical Systems Integrations USA 64. Institute for Medical Outcomes Research (IMOR) Germany 65. Institute of Applied Health Sciences. University of Aberdeen. Department
of Public Health UK
66. Institute of Biomedical Technology (INBIT) Greece 67. Institute of Health Economics (IHE) Canada 68. Institute of Public-Health Radiation Hygiene Laboratory Romania 69. Institute of Social Medicine 70. IQWiG- Institu für Qualität und Wirtschaftichkeit im Gesundheitswesen -
Gemeinsamer Bundesaussschuss (G-BA) Germany
71. Jefferson Ultrasound Research & Education Institute Thomas Jefferson University
USA
72. Karlstad University Public Health Science Sweden 73. Lisbon National School of Public Health Portugal 74. London School of Hygiene & Tropical Medicien European Centre on
Health of Societies in Transition (ECOHOST) (LSHTM) UK
75. Ludwin Boltzmann Institute for Medical Sociology (Ludwing Boltzmann-Institu für Health Technology Assessment)
Austria
76. Lung and Blood Institute HIH National Heart USA 77. Mario Negri Institute Italy 78. Medical & Health Research Council of the Netherlands (ZonMW) Netherlands 79. Medical Department of the RIZIV Belgium 80. Medical Laboratory (INSTAND e.v.) 81. Medical Research Council South Africa 82. Medical Services Advisory Committee (MSAC) Australia
27

Organisation
Country
83. Medical University Luebeck Institute for Social Medicine Germany 84. Medication Use Management Services Canada 85. Medizinischer Dienst der Spitzenverbände der Krankenkassen (MDS) Germany 86. Mexican Institute of Social Security-Health Systems Division Mexico 87. Mexico National Center for Health Technology Excellence (CENETEC)
Centro Nacional de Excelencia Tecnológica en Salud México
88. Ministry of Health and Long-Term Care Ontario MAS -Medical Advisory Secretariat
Canada
89. Ministry of Health 90. National Health Research and Development Program Health Canada Canada 91. National Organization for Medicine (EOF) Greece 92. Netherlands Institute of Mental Health and Addiction (Trimbos instituut) Netherlands 93. Netherlands Institute of Primary Health Care (NIVEL) Netherlands 94. New Zealand Health Technology - Assessment (NZHTA) New Zealand 95. New Zealand Ministry of Health New Zealand 96. NHS Quality Improvement Scotland Health Services Research &
Assessment Unit Glasgow UK
97. NWO (Nederlandse Organisatie voor Wetenschappelijik Onderzoek) - Netherlands Organisation for Scientific Research
Netherlands
98. Oregon Health Resources Commission USA 99. Osteba Basque Office for Health Technology Assessment Spain 100. Peking Union Medical College Hospital China 101. Pharmaceutical Benefits Advisory Committee Australia 102. RAND Health USA 103. Regione Veneto Italy 104. Research Centre on Technology Assessment on Biotechnology
(BIOGUM) Germany
105. Saskatchewan Health Canada 106. Semashko Scientific Research Institute of Social Hygiene & Academy of
Medical Science Department of Public Health Russia
107. Shanghai Blood Centre China 108. Swedish Council on Technology Assessment in Health Care (SBU) Sweden 109. Swiss Medical Association Switzerland 110. SwissHTA / Swiss Netword for HTA Switzerland 111. Technische Universität Wien Institute of Technology and Society (ITG) Austria 112. Technology Assessment Program. Office of Patient Care Services USA 113. The Gerther Institute Israel Center for Technology Assessment in Health
Care (ICTAHC) Israel
114. TNO -Netherlands Organization for Applied Scientific Research Netherlands 115. TNO Prevention and Health Netherlands 116. Universität Hannover Institut für Versicheurengsbetriebsl ehre (von der
Schulenburg) Germany
117. Universitätsklinikum Schleswing-Holstein Campus Lübeck Institut für Sozialmedizin (Raspe)
Germany
118. University of Athens Center for Management and Evaluation Department of Nursing (CHESME)
Greece
119. University of Graz 120. University of Leuven UK 121. University of Oxford National Perinatal Epidemiology Unit UK 122. University of Patras Department of Medical Physics and Biomedical
Engineering Greece
123. University of Pennsylvania Leonard Davis Institute of Health Economics USA 124. University of Sheffield Sheffield Centre for Health and Health Related
Research UK
125. University of Tromso Norway 126. University of York Centre for Health Economics UK
28

Annex 5. Final version of the questionnaire
29

30
31
32

33
34

35

36
37

38
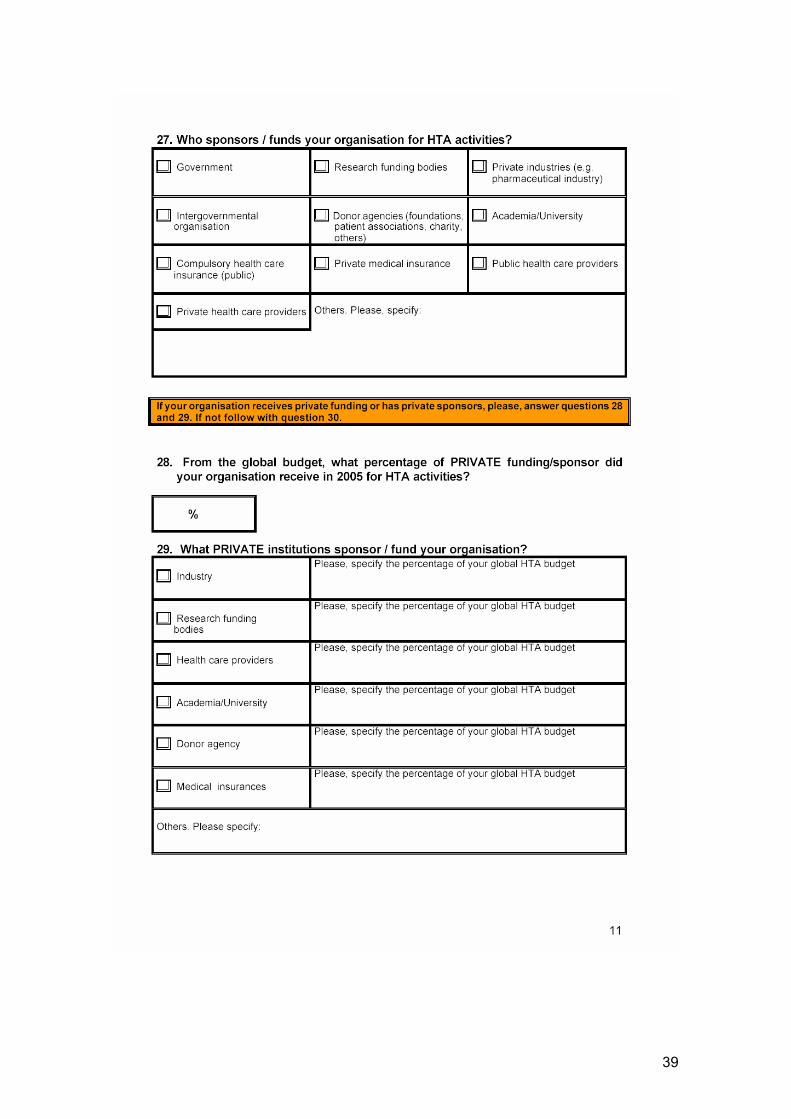
39
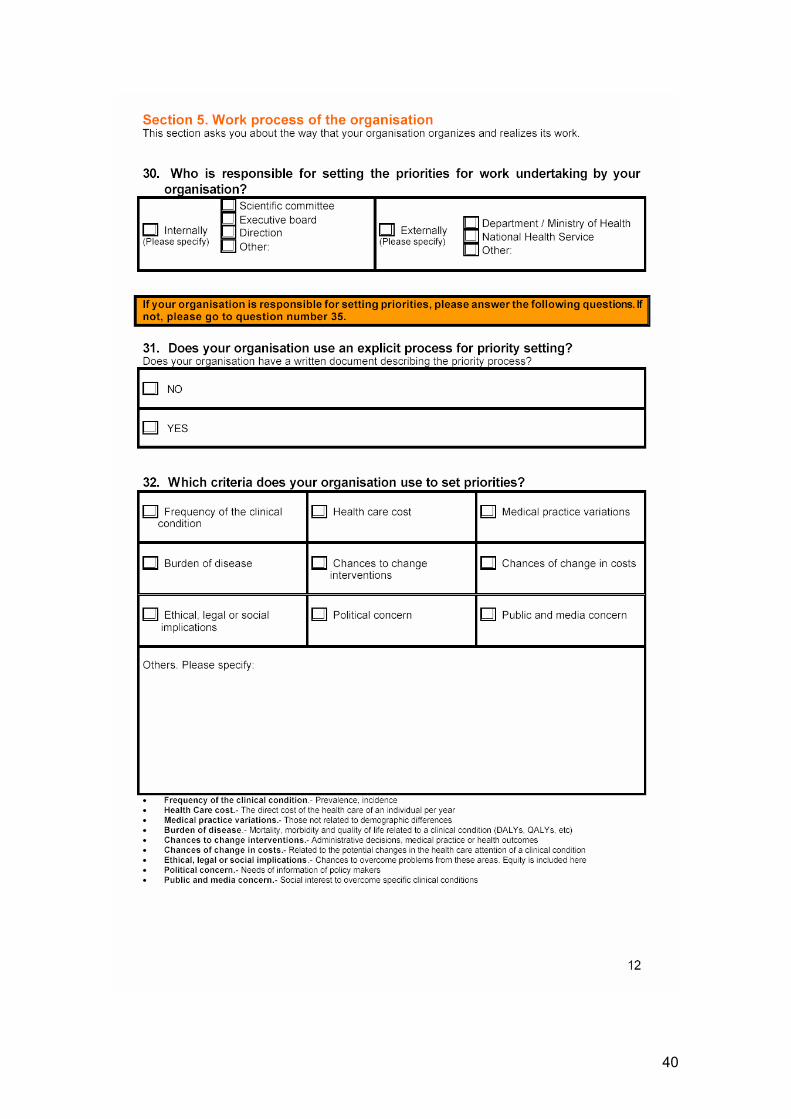
40

41
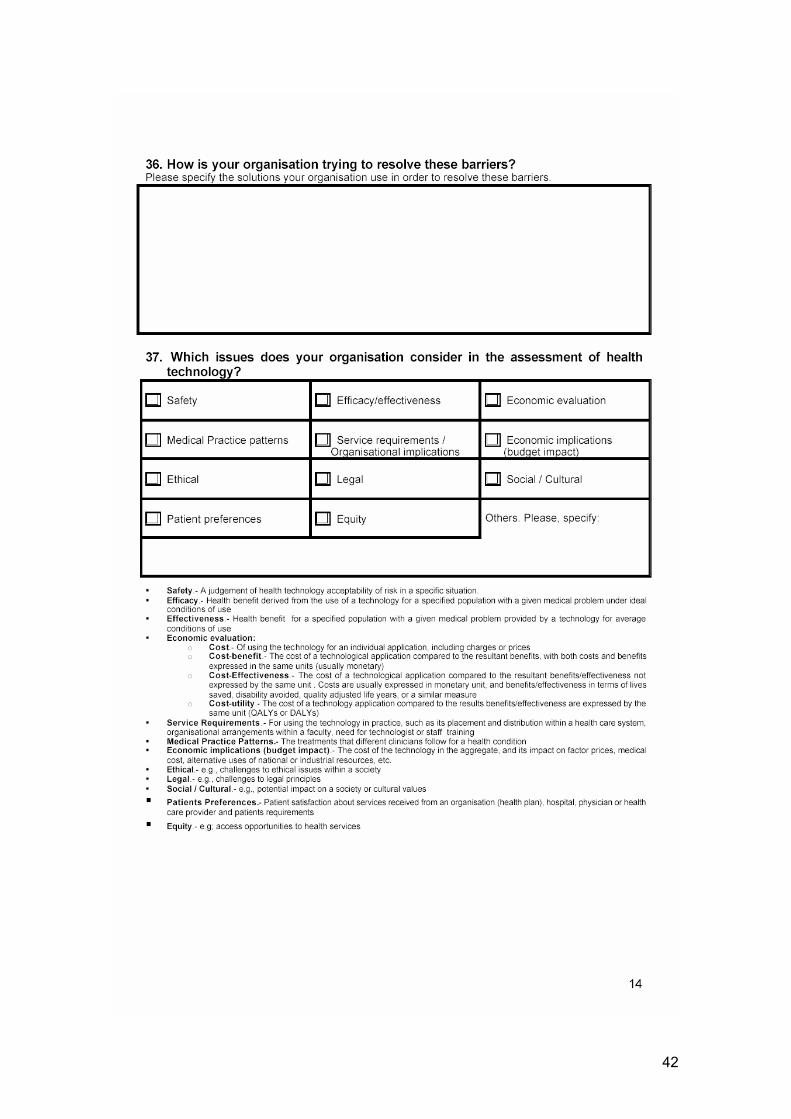
42

43

44

45
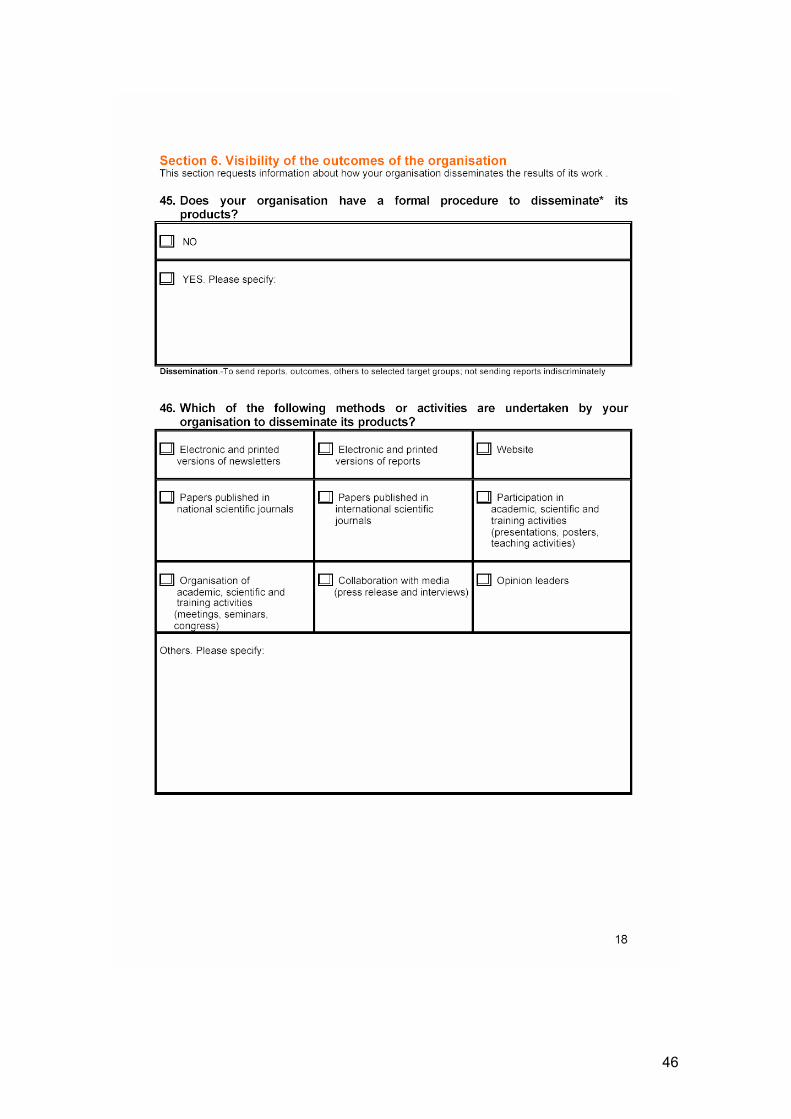
46
47
ANNEX 6. BIBLIOGRAPHY 1 Estrada MD, Serra-Sutton V. Rajmil L. Overview of the implementation of the health technology
assessment activities in a broad representatio of world health organisation-collaborating centres [consulta técnica]. Barcelona: Agència d'Avaluació de Tecnologia i Recerca Mèdiques.Servei Català de la Salut.Departament de Sanitat i Seguretat Social.Generalitat de Catalunya; 20012. Report no.:
2 Perry S, Gardner E, Thamer M. The status of health technology assessment worldwide. Results of an international survey. Int J Technol Assess Health Care. 1997;13(1):81-98.
3 Mears R, Taylor R, Littlejohns P. Dillon A. Review of International Health Technology Assessment (IHTA). Project Report. London: National Institute for Clinical Excellence (NICE); 2000. Report no.:
48

49
Annex WP8.4
WORKSHOP PROPOSAL
WP8. Systems to support Health Technology Assessment (HTA) in member states with limited institutionalisation of HTA
December 2006
WP8 proposal refers to a specific participation of associative and collaborative partners.
The idea consist in giving information to collaborative and associated partners, involved in the workshop in Ljubljana, of different kinds –a review abstract and the preliminary outcomes of WP8 survey- Also, they will be asked about how they interpret these outcomes and possible suggestions to study more in depth.
Workshop in Slovenia: March 2007 Workshop in Ljubljana could be a milestone to obtain a partial product. Five main areas which are the main key components for a
new HTA agency have been defined according to the WP8 survey’s sections:
- Scope - Background - Structures - Work process - Visibility of outcomes
This proposal divides the partners into three working groups in order to work more in depth each of the previous topics (see annex 1). Participants will be able to choose the working group they want to participate in. An e-meeting organised in December 2006 took place to discuss this proposal with the project partners and decisions were took into account. If there are enough participants in each group (2 or 3 participants for each group) the information and documentation will be sent to you in January 2007 (after Christmas holidays). Another e-meeting could be organised in February 2007 in order to coordinate and speed up the work in each area. There should be an e-meeting for each working group. The e-meetings materials to discuss and to work could be:
1. Questionnaire main outcomes presentation of each area and individual proposal of work for the next e-meeting 2. Review report abstract 3. Presentation of the individual work and group discussion. Consensus.
Each group could present their outcomes in Ljubljana workshop and reach a general consensus with the questionnaire outcomes for each work group. Workshop program could include the following agenda:
- General presentation of the questionnaire outcomes - Presentation of the work methodology of each topic - Presentation of the main outcomes of each work group - General group discussion
The methodology to follow up in each e-meeting group could be similar to the ‘discussion group’, and should be lead by WP8 team. The work with little groups should make easier to call together partners and to coordinate the e-meetings.
50

Annex WP8.5
WP8 e-Meeting Summary
December 20, 2006
10:00-11:30 am
E-meeting
Organised by CAHTA
Participants:
Marta Aymerich, CAHTA, Spain
Marina Cerbo, Università Cattolica del Sacro Cuore, Italy
Teresa Cerdá Mota, Galician Agency for Health Technology Assessment, Spain.
Mònica Cortés, CAHTA, Spain.
Stelios Cristofides, Ministry of Health of Cyprus. Cyprus.
Joan Pons, CAHTA, Spain
Eva Turk, Institute of Public Health. Slovenia.
Hindrik Vondeling, CAST, Denmark.
Apologies:
Lise Lund, NOKC, Norway.
Piotr Mierzewski, Council of Europe, Directorate General III - SOCIAL COHESION, France.
Antonio Sarría, Agencia de Evaluación de Tecnologías Sanitarias, Spain.
Martin Raab, SNHTA, Switzerland.
1. New Director at CAHTA. Marta Aymerich Marta Aymerich, Director of the Catalan Agency for Health Technology Assessment and Research (CAHTA), Catalonia,
Barcelona.
Marta Aymerich is currently the Director of the CAHTA where she has been developing her professional career as a researcher since 1995. From 2004 to 2006 she was appointed as the Director of the Interministerial Council for Research and Technological Innovation by the Government of Catalonia. She holds a PhD in Medicine and Surgery (2002), an MD degreee (1993), and a Master in Health Services Assessment and Management (2000) from the Autonomous University of Barcelona. Marta also holds a Master of Public Health (MPH) from Harvard University (1999).
2. Workplan of WP8. Overview
2.1. Review on HTA organisations
The review of the HTA organisations report was finished by the end of June as planned, having reviewed the following sources: relevant websites and published reports (for example, Perry, Gardner and Thamer. Worldwide review of the HTA status published in the HTAi Journal). The report on this review will be prepared and submitted to the coordinating centre by Jan 15th, 2007.
2.2. 2.2 Survey on HTA organisations
Pilot phase of survey: The first pilot version of WP8 about: Systems to support Health Technology Assessment (HTA) in member states with limited institutionalisation of HTA was sent in August to the collaborative and associated partners of WP8. The
51

questionnaire version was sent to 26 organisations. E-mail and telephone reminders were done in September and October in order to increase the response rate. The final version of the questionnaire is placed on the WP8 extranet.
Report on the results of the pilot phase questionnaire: The responses of this first pilot phase are collected in a document which is placed on the WP8 extranet. The final version of the questionnaire was sent in November to a large number of organisations (about 120). The responses are now being collected.
Upcoming events: 1. First e-meeting session December 20th, 2006. The main topic will be the organisation of the first face-to-face meeting in Slovenia. 2. Organisation of the workshop in Slovenia. WP8 has been in contact with the Institute of Public Health in Slovenia in order to organise the workshop. 3. The technical report of WP8 is being prepared and will be sent to the coordinating centre by January 15th, 2007.
3. Collaboration of associated and collaborating partners
WP 8 has produced an info letter which is sent bimonthly telling the AP which AP and CP have done during that period. Two info letters have been produced so far from June to October.
4. Workshop in Slovenia: 5-6 March 2007, first face-to-face e-meeting WP8 workshop proposal refers to a specific participation of associated and collaborative partners. The idea is to divide the partners that will attend the workshop in three or four work groups in order to work more in depth specific topics. Participants will be able to choose in which group they prefer to participate. If there are enough participants in each group (2 or 3) the information and documents will be sent to you in January 2007 (after Christmas holidays). Some other e-meetings will be organised in February 2007 in order to coordinate and speed up the work in each topic. There should be an e-meeting for each work group. The e-meetings materials to discuss and to work could be: 1.Questionnaire main outcomes. Presentation of each area and individual work proposal for the next e-meeting2.Report on HTA organisations review3. Presentation of the individual work and group discussion. Consensus. Five main topics which are the main key components for a new HTA agency have been defined according to the WP8 survey’s sections: 1. Scope
2. Background 3. Structures 4. Work process 5. Visibility of outcomes
These 5 main topics could be divided into 3 in order to create three work groups:
1. Scope, background and structures2. Work process3. Visibility of outcomes 1.Scope, Background & StructureCharacteristics of the organization: Area of influence, Statutes, Strategic plan, profit/non-for-profit, profile organisation…Activities of the organizations: lines of activity, types of HT, type of productsUsers of services and products: main costumers, target users of recommendationsBackground: supporting policy, political opportunity, involvement system stakeholders, Structure: management, executive board nomination, contractual situation of staff, professionals background, engaged staff, facilities & equipment, funding for HTA activities 2. Work process Priorities setting (responsible, process, criteria, advisory mechanisms) Barriers & solutions in daily work Issues considered in HTA Strategies to ensure quality Assessment of impact (attitude, frequency of assessment, use of indicators 3. Visibility of Outcomes Formal procedure to disseminate products Activities used Target users of productsNext e-meetings (dates to be set) January 2007 February 2007
52
Annex 1. Working group proposal
Three working groups 1. Scope, Background & Structure
a) Characteristics of the organization (Area of influence, Statutes, Strategic plan, For profit/Non-for-profit, Profile organisation, Collaborations (national and international)
b) Activities of the organizations (Lines of activity, Types of HT, Types of products) c) Users of services and products (Main costumers, Target users of recommendations) d) Background (Supporting policy?, Political opportunity, Involvement system stakeholders, Management reputation, Anchoring
and network, Conflict of interest?) e) Structure (Management, Executive board nomination, Contractual situation of staff, Professionals background, Engaged
staff, Facilities & equipment, Funding for HTA activities
2. Work process o Priorities setting (responsible, process, criteria, advisory mechanisms, etc.) o Barriers & solutions in daily work o Issues considered in HTA o Strategies to ensure quality o Assessment of impact (attitude, frequency of assessment, use of indicators?, criteria to assess it, strategies to reach it)
3. Visibility of Outcomes
o Formal procedure to disseminate products? o Activities used o Target users of products?
53
Annex WP8.7
54
55

56

57

58
59
Annex WP8.7

60


















