
ETIOPATOGENIA EXISTE BASE GENETICA? PORQUE RESPONDE AL OH? QUE ESTRUCTURAS CAUSAN EL TEMBLOR? CUAL...
32
ETIOPATOGENIA • EXISTE BASE GENETICA? • PORQUE RESPONDE AL OH? • QUE ESTRUCTURAS CAUSAN EL TEMBLOR? • CUAL ES EL NT MAS IMPORTANTE? • EXISTE DETERIORO COGNITIVO? • MORTALIDAD ESTA AUMENTADA? • CUAL ES LA BASE NEUROPATOLOGICA? • INFLUYEN FACTORES DIETETICOS- METABOLICOS? • OVERLAP CON OTRAS ENTIDADES • EXPERIMENTACION ANIMAL • NEUROIMAGEN FUNCIONAL • NEUROCIRUGIA FUNCIONAL
-
Upload
makenzie-prowse -
Category
Documents
-
view
214 -
download
0
Transcript of ETIOPATOGENIA EXISTE BASE GENETICA? PORQUE RESPONDE AL OH? QUE ESTRUCTURAS CAUSAN EL TEMBLOR? CUAL...

ETIOPATOGENIA• EXISTE BASE GENETICA?• PORQUE RESPONDE AL OH?• QUE ESTRUCTURAS CAUSAN EL TEMBLOR?• CUAL ES EL NT MAS IMPORTANTE?• EXISTE DETERIORO COGNITIVO?• MORTALIDAD ESTA AUMENTADA?• CUAL ES LA BASE NEUROPATOLOGICA?• INFLUYEN FACTORES DIETETICOS-METABOLICOS?• OVERLAP CON OTRAS ENTIDADES• EXPERIMENTACION ANIMAL• NEUROIMAGEN FUNCIONAL• NEUROCIRUGIA FUNCIONAL

¿EXISTE BASE GENETICA?• 50 % AF – AD (65 %) POLIGENICA. PENETRANCIA COMPLETA A LOS 65. • DETECCION EN FAMILIAS DE GENES INVOLUCRADOS :
Cr. 4P;
3Q13 (ETM 1); (D3)
2P22-25(ETM2)
6p23
ASOCIACIONES: EP – D – M- CMT

¿QUE ESTRUCTURA CAUSA EL TEMBLOR?
PETHemisferios CerebelososVia dento-rubro-talamica- cortical Oscilador talámico Oscilador olivar Aceleración ritmo descarga MNI Oscilador central origina; periferia modula; influencia somatosensitiva.
*Hiperfunción via cerebelo talamica (Glutamato), reversible c/OH
Estudios de Coherencia (sincronía EMG – NI áreas cer.): varios osciladores según topografía del temblor.
NEUROCIRUGIA FUNCIONAL: NVINEUROPATOLOGÍA: celulas torpedo (Pk), CL, atrofia dentado. ESTIMULACION MAGNETICA TRANSCRANEANA CEREBELO
TEMBLOR EN LAS HEREDOATAXIASDISFUNCIONES OME EN TE
A positron emission tomography study of essential tremor: Evidence for overactivity of cerebellar connections
• Dr. I. H. Jenkins, MRCP 1 *, P. G. Bain, MRCP 2, J. G. Colebatch, FRACP 1, P. D. Thompson, PhD. 2, L. J. Findley, MD 2, R. S. J. Frackowiak, MD 1, C. D. Marsden, DSc 2, D. J. Brooks, MD 1
• 1Medical Research Council (MRC) Cyclotron Unit, Hammersmith Hospital, London, United Kingdom2MRC Human Movement and Balance Unit, National Hospital for Neurology and Neurosurgery, London, United Kingdom
• *Correspondence to I. H. Jenkins, MRC Cyclotron Unit, Hammersmith Hospital, DuCane Road, London W12 OHS, UK
• ABSTRACT• The origin of essential tremor is unknown. Animal models have suggested that the inferior olivary
nucleus may act as a tremor generator. We used positron emission tomography to study changes in regional cerebral blood flow associated with involuntary postural tremor and passive wrist oscillation in patients with essential tremor. Activation due to voluntary wrist oscillation and arm extension without tremor was studied in normal control subjects. The essential tremor group had bilaterally increased cerebellar blood flow at rest (without tremor) compared with the control group. Involuntary postural tremor was associated with further bilateral cerebellar activation, and also contralateral striatal, thalamic, and sensorimotor cortex activation. Voluntary wrist oscillation, maintained arm extension without tremor, and passive wrist oscillation were all associated with significant ipsilateral rather than bilateral cerebellar activation. We conclude that essential tremor is associated with increased bilateral cerebellar activity both at rest and during tremor.
• Received: 24 August 1992; Revised: 27 January 1993; Accepted: 11 February 1993

Lesión o (+) NVI tálamo (eferencia cerebelosa) mejora temblor: normaliza
oscilación celular anómala en Hemisferios Cerebelosos

Benito-León J and Louis ED (2006) Essential tremor: emerging views of a common disorderNat Clin Pract Neurol 2: 666–678 10.1038/ncpneuro0347
Figure 1 Section of cerebellar folium from a patient with essential tremor, showing two torpedoes (arrows)
Permission obtained from American Medical Association © Louis ED et al. (2006) Arch Neurol 63: 1189–1193.

Benito- León J and Louis ED (2006) Essential tremor: emerging views of a common disorderNat Clin Pract Neurol 2: 666–678 10.1038/ncpneuro0347
Figure 2 Section of the dentate nucleus from an individual with essential tremor, showing neuronal loss
Permission obtained from American Medical Association © Louis ED et al. (2006) Arch Neurol 63: 1189–1193.

Benito-León J and Louis ED (2006) Essential tremor: emerging views of a common disorderNat Clin Pract Neurol 2: 666–678 10.1038/ncpneuro0347
Figure 3 Multiple Lewy bodies (arrows) are seen in a section of the locus ceruleus from a patient with essential tremor
Permission obtained from AAN Enterprises, Inc. © Louis ED et al. (2006) Neurology 66: 1756–1759.

OH 50 %
¿POR QUÉ? ETANOL MODULA (-) GLUTAMATO A
TRAVES DE RECEPTOR NMDA, VIA HIPERACTIVADA EN EL TEMBLOR ESENCIAL.
Eur J Neurol. 2008 Jul;15(7):697-705. Epub 2008 May 15. Links
A possible mechanism for the beneficial effect of ethanol in essential tremor.
• Manto M, Laute MA.• Laboratoire de Neurologie Expérimentale, ULB-Erasme, Bruxelles, Belgium. [email protected]
• BACKGROUND: Essential tremor is one of the most common movement disorders in elderly people. The hypothesis of a disregulation of N-methyl-D-aspartate (NMDA) pathways has been suggested. It was shown experimentally that infusion of NMDA in cerebellar nuclei down-regulates glutamate release. METHODS: We assessed the effects of intranuclear administration of harmaline on the NMDA-mediated regulation of glutamate in rats using reverse dialysis. We hypothesized that ethanol, which improves essential tremor in the clinic, antagonizes the effect of harmaline upon glutamatergic transmission. We tested the interaction of ethanol and harmaline upon glycerol (a marker of membrane turn-over), lactate, and pyruvate concentrations. RESULTS: Harmaline increased the concentrations of glutamate and impaired the NMDA-mediated regulation of glutamate. Ethanol decreased the concentrations of glutamate during NMDA stimulation in case of pre-administration with harmaline. Concentrations of glycerol rose with harmaline. Glycerol levels markedly decreased during NMDA infusion when inhibitors of nitric oxide synthase, alpha-amino-3-hydroxy-5-methylisoxazole-4-propionate antagonists or NMDA antagonists were administered. Harmaline increased lactate/pyruvate ratios during NMDA infusion but these ratios returned to normal values in presence of ethanol. DISCUSSION: We provide a possible mechanism for the beneficial effect of ethanol on essential tremor. The concept of glutamatergic disregulation underlying essential tremor is highlighted. Consequences for our understanding of essential tremor are discussed.
• PMID: 18445025 [PubMed - indexed for MEDLINE]

Neurology 2006;66;69-74


Ann Neurol. 1985 Apr;17(4):329-33.Association between essential tremor and
Parkinson's disease.Geraghty JJ, Jankovic J, Zetusky WJ.
To examine a possible relationship of essential tremor to Parkinson's disease (PD), 130 patients with essential tremor were studied. Twenty-five patients had both essential tremor and PD. These 25 patients were matched for age and duration of PD symptoms with 25 patients who had idiopathic PD. Bradykinesia, postural instability, and gait difficulty were more severe in the patients with idiopathic PD. Degree of tremor, rigidity, and functional disability did not differ in the two groups. The prevalence of PD in the population with
essential tremor was 24 times greater than expected. This study suggests that some patients with essential tremor have a genetically increased risk for PD.
PMID: 4004153 [PubMed - indexed for MEDLINE]


Muscle Nerve. 1993 Sep;16(9):904-10. Links Hereditary motor-sensory neuropathy and
movement disorders.Cardoso FE, Jankovic J.Department of Neurology, Parkinson's Disease Center and Movement Disorders Clinic, Baylor College of Medicine, Houston, Texas 77030.
To explore the relationship between hereditary motor and sensory neuropathy (HMSN) and movement disorders, we examined 7 patients with HMSN referred to our Movement Disorders Clinic and surveyed members of the Charcot-Marie-Tooth association. The following movement disorders were observed in the index patients: postural tremor in 6, rest tremor in 3, and Parkinsonism and dystonia in 2. Tremor, present in 40% of the 201 patients who responded to the survey, was first noted at a mean age of 36 years, and mostly involved the hands. Family history of tremor was more frequent in the tremor group (P < 0.005), which also had a significantly worse writing score
than the nontremor group (P < 0.001). The overlap in clinical features between HMSN-associated tremor and essential tremor (ET), the high frequency of family history of tremor, and the lack of a relationship between the severity of tremor and of peripheral neuropathy suggest that the tremor in HMSN is pathogenically related to ET.
PMID: 8355721 [PubMed - indexed for MEDLINE]

E. D. Louis, W. Zheng, X. Mao, and D. C. ShunguBlood harmane is correlated with cerebellar metabolism in essential tremor: A pilot studyNeurology, August 7, 2007; 69(6): 515 - 520.
Mov Disord. 2005 Mar;20(3):298-305. Links
Harmaline-induced tremor as a potential preclinical screening method for essential tremor medications.Martin FC, Thu Le A, Handforth A.Research Service, Veterans Affairs Greater Los Angeles Healthcare System, Los Angeles, California 90073, USA. [email protected] preclinical method to evaluate potential new medications for essential tremor (ET) is available currently.
NEUROLOGY 2005;65:391-396© 2005 American Academy of Neurology
Blood harmane concentrations and dietary protein consumption in essential tremor E. D. Louis, MD, MS, W. Zheng, PhD, L. Applegate, BA, L. Shi, MS and P. Factor-Litvak, PhD
Conclusions: The similarity between patients and controls in daily animal protein consumption and the absence of the normal
correlation between daily animal protein consumption and logHA in patients suggests that another factor (e.g., a metabolic defect) may be increasing blood harmane concentration in patients.

Benito- León J and Louis ED (2006) Essential tremor: emerging views of a common disorderNat Clin Pract Neurol 2: 666–678 10.1038/ncpneuro0347
Figure 4 Archimedean spirals drawn by individuals with and without essential tremor
TRATAMIENTO

• IDENTIFICAR CAUSAS: INTERROGAR - TSH• EXPLICAR Q NO PADECE EP• NO TRATAR SI NO INTERF. FUNCIONALIDAD• IDENTIFICAR y FAVORECER CONDUCTAS (-)• EL TRATAMIENTO ES SINTOMATICO • LARGO PLAZO• A MENUDO MAL TOLERADO • CONTRAINDICACIONES

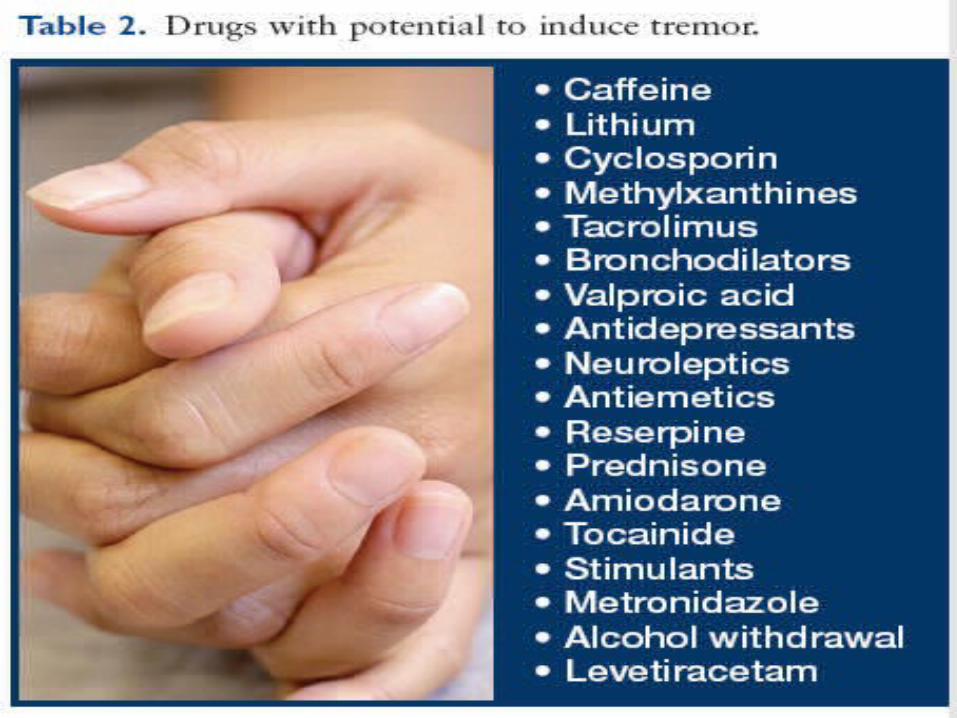
CAUSAS DE TEMBLOR• EMOCIONES: ANSIEDAD STRESS MIEDO• FATIGA• HIPOGLICEMIA• HIPERTIROIDISMO• FEOCROMOCITOMA• FARMACOS

ALCOHOL• NIVEL de EVIDENCIA II-B• 1 – 2 TRAGOS ALCOHOL ETILICO• REDUCE 75 % el TEMBLOR EN 50-90 % de los
PACIENTES• TRANSITORIO: 45 – 60 MINUTOS• PUEDE DESARROLLARSE TOLERANCIA• ADVERTIR EVITAR ABUSO• EL RIESGO DE ADICCION ES BAJO

ALPRAZOLAM
0,25 – 1 mgs. v/o HORAS ANTES DE UN EVENTO

Neurology 2005;64;2008-2020; originally published online Jun 22, 2005; This information is current as of August 20, 2008

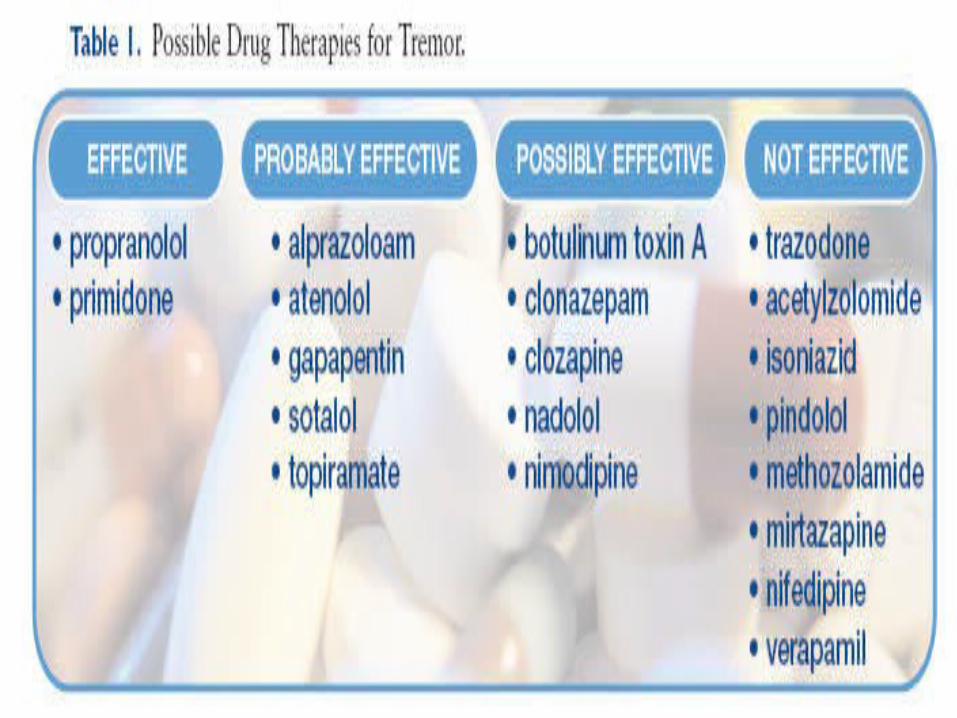
Abstract—Background: Essential tremor (ET) is one of the most common tremor disorders in adults and is characterized by kinetic and postural tremor. To develop this practice parameter, the authors reviewed available evidence regardinginitiation of pharmacologic and surgical therapies, duration of their effect, their relative benefits and risks, and thestrength of evidence supporting their use. Methods: A literature review using MEDLINE, EMBASE, Science CitationIndex, and CINAHL was performed to identify clinical trials in patients with ET published between 1966 and August2004. Articles were classified according to a four-tiered level of evidence scheme and recommendations were based on the
level of evidence. Results and Conclusions: Propranolol and primidone reduce limb tremor (Level A). Alprazolam, atenolol,gabapentin (monotherapy), sotalol, and topiramate are probably effective in reducing limb tremor (Level B). Limitedstudies suggest that propranolol reduces head tremor (Level B). Clonazepam, clozapine, nadolol, and nimodipine possibly reduce limb tremor (Level C). Botulinum toxin A may reduce hand tremor but is associated with dose-dependent hand weakness (Level C). Botulinum toxin A may reduce head tremor (Level C) and voice tremor (Level C), but breathiness,hoarseness, and swallowing difficulties may occur in the treatment of voice tremor. Chronic deep brain stimulation (DBS) (Level C) and thalamotomy (Level C) are highly efficacious in reducing tremor. Each procedure carries a small risk of major complications. Some adverse events from DBS may resolve with time or with adjustment of stimulator settings. There is insufficient evidence regarding the surgical treatment of head and voice tremor and the use of gamma knife thalamotomy (Level U). Additional prospective, double-blind, placebo-controlled trials are needed to better determine theefficacy and side effects of pharmacologic and surgical treatments of ET.NEUROLOGY 2005;64:2008–2020

B-BLOQUEANTES• PROPANOLOL (OTROS: TIMOLOL NADOLOL
SOTALOL METOPROLOL)• NIVEL DE EVIDENCIA I-A (DE ELECCION)• (-) REC. B2 PERIFERICOS, TB. PROBABLE CENTRAL
B1• CONTRAINDICACIONES: INS. CARD (II-III); DM,
ASMA, EPOC, AOC, BAV 2-3.• EFECTOS SECUNDARIOS: FATIGA, IMPOTENCIA,
DEPRESION, HIPOTENSION, ARRITMIAS.

PROPANOLOL• DOSIS INDIVIDUALIZADA• EFECTO NO ES DOSIS DEPENDIENTE• 40 mg 1 VEZ AL DIA POR 3 DIAS• AUMENTAR 40 mg CADA 3 DIAS HASTA 120 (EN 3
TOMAS O PREPARADOS DE ACCION PROLONGADA)
• SI NO HAY RESPUESTA AUMENTAR A 160 mg/dia. SI NO RESPONDE RETIRAR GRADUALMENTE (AUNQUE HASTA 320 PUEDE HABER RESPUESTA)
• CONTROLA EL TEMBLOR EN UN 50%, S/T MANOS, EN 50 – 70% DE LOS PACIENTES, ALGUNOS RESPUESTA NOTABLE, OTROS NO RESPONDEN

PRIMIDONA• REDUCE 40- 50 % TEMBLOR EN 50 – 70 % DE LOS PACIENTES,
S/T MANOS. EVIDENCIA I-A• BARBITURICO METABOLIZA A FENOBARBITAL, PERO SU
ACCION ANTITEMBLOR ES INDEPENDIENTE, PROBABLEMENTE CENTRAL
• INICIAR EN DOSIS BAJAS 62,5 mg. (1/4 comp. 250) *NO HAY COMP DE 50 o 60*. DE NOCHE. CADA 3 DIAS PASAR A ½ COMP., LUEGO ¾, LUEGO 1. SI NO BASTA DOSIS UNICA NOCTURNA DE 250 mg, AGREGAR 1 o 2 tomas mas de ½ COMP (125) EN LA M y la T.
• FRECUENTE INTOLERANCIA 25 % (VARIABLE, FARMACOGENETICA): HIPERSOMNIA, MAREOS, VERTIGOS, NAUSEAS, OBNUBILACION, COMA, RASH. 24 – 72 % SE ALIVIA.


Zesiewicz, T. A. et al. Neurology 2005;64:2008-2020

Benito- León J and Louis ED (2006) Essential tremor: emerging views of a common disorderNat Clin Pract Neurol 2: 666–678 10.1038/ncpneuro0347
Table 1 Pharmacological agents for the treatment of essential tremor

Zesiewicz, T. A. et al. Neurology 2005;64:2008-2020


















