
Ethical, Social, and Good Clinical Practice (GCP) Aspects Of Drug Development In Children And In...
38
Ethical, Social, and Good Clinical Practice (GCP) Aspects Of Drug Development In Children And In Paediatric Clinical Trials Klaus Rose, klausrose Consulting Pediatric Drug Development & More
-
Upload
arabella-parrish -
Category
Documents
-
view
220 -
download
0
Transcript of Ethical, Social, and Good Clinical Practice (GCP) Aspects Of Drug Development In Children And In...

Ethical, Social, and Good Clinical Practice (GCP) Aspects Of Drug Development In Children And In Paediatric Clinical Trials
Klaus Rose, klausrose Consulting Pediatric Drug Development & More [email protected]

Labels A Century Ago
918.
Source: www.wellcomecollection.org 2
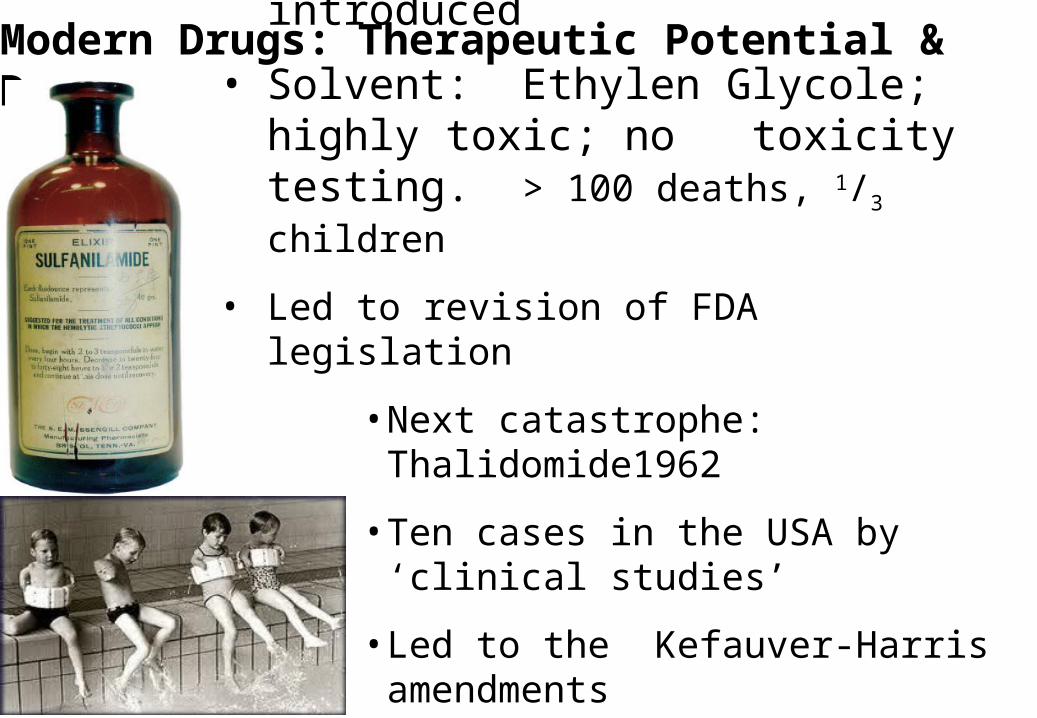
Modern Drugs: Therapeutic Potential & Dangers
• 1937 a liquid anibiotic was introduced
• Solvent: Ethylen Glycole; highly toxic; no toxicity testing. > 100 deaths, 1/3 children
• Led to revision of FDA legislation
• Next catastrophe: Thalidomide1962
• Ten cases in the USA by ‘clinical studies’
• Led to the Kefauver-Harris amendments
• Was the birth of modern labels
US Legislation Triggered Modern Drug Labels
• Date back to US legislation 1962: enforced proof of efficacy.
• Use in children mostly off-label since then.
• Voluntary Pediatric Exclusivity (PE): BPCA* 2007 after first laws 1997 & 2002. Biologics excluded.
• Mandatory ped development: PREA*** 2003. All age groups. Biologics included. Applies to same indication as in adults only.
• Re-authorized 2012 as FDASIA***
• BPCA &PREA resulted in multiple pediatric research on patented drugs. Both seen by FDA as major success
*BPCA Best Pharmaceuticals for Children Act
**PREA Pediatric Research Equity Act
***FDASIA FDA Safety & Innovation Act 4
klausrose Consulting - 6 -
EU Pediatric Regulation
• In force since January 2007
• Combines mandatory development with reward
• Pediatric Investigation Plan (PIP) mandatory end of human PK
• Without approved PIP Marketing Authorisation Application (MAA) is blocked
• PIP must cover all age groups
• Pediatric Committee (PDCO) assesses PIPs, waivers & deferrals
• Reward of six months SPC* prolongation
*SPC Supplementary Protection Certificate5
klausrose Consulting - 7 -

EU Pediatric Regulation: Core Elements
6
• FDA started with looking for ‘some‘ pediatric data
• EU wants, as far as possible, full pediatric indication(s)
• Want the necessary data as soon as possible for marketed drugs and as early as possible for new drugs
• Expect each company to be knowledgeable + up to date
• EMEA / PDCO style: has evolved since 2007. Claim to be science-driven, but have developed a tough attitude
• Some requests can be perceived as exaggerated. Dictate clinical trials even if they do not make sense
klausrose Consulting - 9 -

Regulatory & Scientific Challenge: Earlier Inclusion of Children In Drug Developemnt
7
Entry into Man
Proof of Concept (PoC)
Patent-protected Market
Registration 1st Country
Phase II+III
Basic Research
Patent Expiry Generic Competition
FDA: Early dialogue recommended; Ped Plan mandatory at submission
EU Pediatric Investigation Plan (PIP): mandatory at end of human PK
klausrose Consulting - 10 -

8

Pediatric Homework
9
• Does the same indication exist in children?
• Diagnostics: which other diseases might be diagnosed?
• Drugs: which other pediatric diseases might be qualified as being within the ‘condition’ the drug is developed in?
• PDCO view: potential future use in children. May be different from future adult use.
• Which therapeutic alternatives exist in children?
• Risk/benefit assessment of ped development
klausrose Consulting

PIP Structure
10
Part A: Procedure for the assessment of the application
Part B: Overall Development Of The Drug & Target Disease
Part C: Product-Specific Waivers
Part D: Pediatric Investigation Plan
D1 Proposed ped dev: indication, age grups, existing data
D2 Quality (CMC, technical staff)
D3 Non-clinical aspects
D4 Clinical aspects: clinical strategy & individual studies
D5 Timeslines of proposesd measures
Part E Applications for Deferrals
b
klausrose Consulting

11
PDCO Oral Explanation: Room & Sitting
PDCO Members
PDCO Chairman
Applicant Representatives
15 m
Applicant‘s Speaker
EMA Representatives

Case Study Coronary Artery Disease (CAD)
• Nykomed requested a full waiver for a diagnostic agent for coronary artery disease (CAD), a disease listed on the class waiver list
• EMA: condition is “Visualisation of myocardial perfusion for diagnostic purposes”. Myocardial perfusion deficits exists in children (congenital heart defects, coronary anomalies, cardiomyopathies)
• Negative opinion 2008• Applicant took EMA to EU Court of Justice; 1st instance
backed EMA • US originator company negotiated a new PIP with EMA,
agreed 2011• Danish company continued law suit . EU General Court
backed EMA 2011: otherwise it would be too easy for companies to circumvent pediatric development.
•

EMA Decisions Perflubutane
• EMA decision of 28 November 2008 on the application for product specific waiver for perflubutane EMEA-000194-PIP01-08 in accordance with Regulation (EC) No 1901/2006 of the European Parliament and of the Council as amended. http://www.ema.europa.eu/docs/en_GB/document_library/PIP_decision/WC500005753.pdf
• EMA decision of 18 May 2011 on the agreement of a paediatric investigation plan and on the granting of a deferral and on the granting of a waiver for perflubutane (EMEA-000194-PIP03-10) http://www.ema.europa.eu/docs/en_GB/document_library/PIP_decision/WC500107411.pdf
13

EU Court of Justice Decisions
• Order of the President of the Court of First Instance of 24 April 2009 – Nycomed Danmark v EMEA (Case T-52/09 R). http://curia.europa.eu/juris/document/document.jsf?text=&docid=73453&pageIndex=0&doclang=EN&mode=lst&dir=&occ=first&part=1&cid=327397
• Judgment Of The General Court (Third Chamber) 14 December 2011. http://curia.europa.eu/juris/document/document.jsf?text=&docid=116583&pageIndex=0&doclang=EN&mode=doc&dir=&occ=first&part=1&cid=234507

PIP Decisions • So far > 1000 PIPs have been submitted • The key elements are published, but not the details• Details are always confidential • Nevertheless, we can see trends in specific areas
Melanoma - Joint injuries - Vaccines - Drugs for preterm newborns - Drugs developed only for children - Rare diseases

Melanoma • Class waiver for melanoma was revoked • Justification: 1.7/ 100’000 15-19ys olds in US statistics Surveillance,
Epidemiology & End Results (SEER), www.seer.cancer.gov• 6 PIPs if you search with ‘melanoma’: Ipilimumab (2); MAGE-A3
recombinant protein; GSK1120212; GSK2118436; RO5185426 - Ipilimumab [BMS] conditions: melanoma (PIP 1) and solid
malignant tumours excluding melanoma (PIP 2) - Mage-A3 recombinant protein: Condition: melanoma- GSK1120212: Condition: Melanoma & malignant solid tumours
(excluding melanoma)- GSK2118436: Condition: Melanoma & malignant solid tumours
(excluding melanoma)- RO5185426: Condition: Melanoma

Ipilimumab (Yervoy)
• Condition: melanoma and non-melanoma solid tumors (2 PIPs)
• Studies for melanoma:
1. i.v. study of pre- and postnatal development in cynomolgus monkeys with a 6-month postnatal evaluation.
2. OL, dose escalation clinical trial of intravenously administered ipilimumab in children from 2 to less than 18 years (and in young adults to 21 years) with untreatable, refractory or relapsed solid malignant tumours.
3. OL multi-centre, single-arm i.v. ipilimumab in 12 to <18 y with untreated/ previously treated advanced/metastatic melanoma.
4. OL randomized active-controlled study: adjuvant ipilimumab anti-CTLA4 therapy vs. high-dose interferon α-2b in kids 12 - < 18 y (and adults) with resected high-risk melanoma.

Does This Make Sense? • Obviously, PDCO wants to do “something” for children with
melanoma. No doubt about their good intentions.
• It would be unethical to disallow adolescents or children with melanoma participation in adults trials.
• Once an adult melanoma drug is registered in adults, of course clinicians will use it in children as well. Too few patients for statistically significant results
• As companies have to commit to studies to be finished in a defined time horizon, the pediatric patients with melanoma are now blocked for PDCO-triggered clinical trials.
• Has started to affect e.g. US children with cancer, although the clinical community sees other priorities
• In consequence, danger of blocking promising treatments 18klausrose Consulting

Societal Impact of EU & US Pediatric Legislation • Increases cost of drug development
• For large companies costs are still marginal.
• Can be different for an individual small / medium company
• SME office @ EMA offers help, but PDCO treat all applicants equally
• Higher costs for pediatric medicines have not yet reached calculations of insurers / reimbursement institutions
• Takes decision power away from originating companies
• Does not contribute to pharmaceutical innovation in Europe
• Has increased the weight of academic pediatrics
• Many clinicians still have a generally positive view
• Assessment of relation of resources assigned to resulting clinical benefit for children almost impossible due to confidentiality
- 19 - 19
klausrose Consulting

Light at The End of The Tunnel? • EMA report to EU Commission emphasizes need for penalties
• EMA 5 years report July 2012 to EU Commission & EU Parliament: “Work is well advanced to promote less detailed PIP proposals, including the key elements in PIP opinions. The simplification of applications and subsequently of PDCO opinions should benefit early PIP applications …”
• First changes were presented by EMA at the EFGCP/DIA/EMA pediatric conference September 2012 in London, UK
• General revocation of class waivers in pediatric oncology was announced a few days ago
• Revision of pediatric regulation in 2018: reasonable modification of the regulation to be expected?

Conclusions • Drug development no longer possible without considering children• Increases cost & complexity of drug development• Mosaic of goodwill, scientific input, bureaucracy without checks &
balances, disproportionate use of resources, limited clinical benefit• PIP skills needed: intimate knowledge of PDCO, EMA & procedures • Potential for saving resources is highest during early PIP preparation • Aim for individual company: negotiate PIP that will serve child health in
the far future and lets company survive• Revision 2018: divergent proposals will be made• EU Council’s Lisbon strategy 2000: EU by 2010 “to become the most
competitive and dynamic knowledge-based economy in the world” • EU pediatric legislation should be seen in this framework. Is one of
many EU challenges. Good intentions are not enough• Legislation will stay no alternative than to continue the dialogue

Thank You For Your Attention!
- 22 - 22klausrose Consulting

Back-Ups
- 23 - 23klausrose Consulting

Better Medicines for Children or Better Use of Adult Medicines in Children?
• EU & US pediatric pharmaceutical legislation tries to close a gap - in the use of existing adult drugs in children
• So far, there is no industry that develops drugs for children
• Such an industry could exist if there would be a market
• There are enough rare diseases to keep thousands of researchers busy – but somebody has to pay
• Today, not even a straw facilitating intake of antibiotics is reimursed in Germany – formulation was abandoned
• We talk about two issues: (1) Handling additional pediatric requests in adult development, and (2) nice wording: ‘better medicines for children’
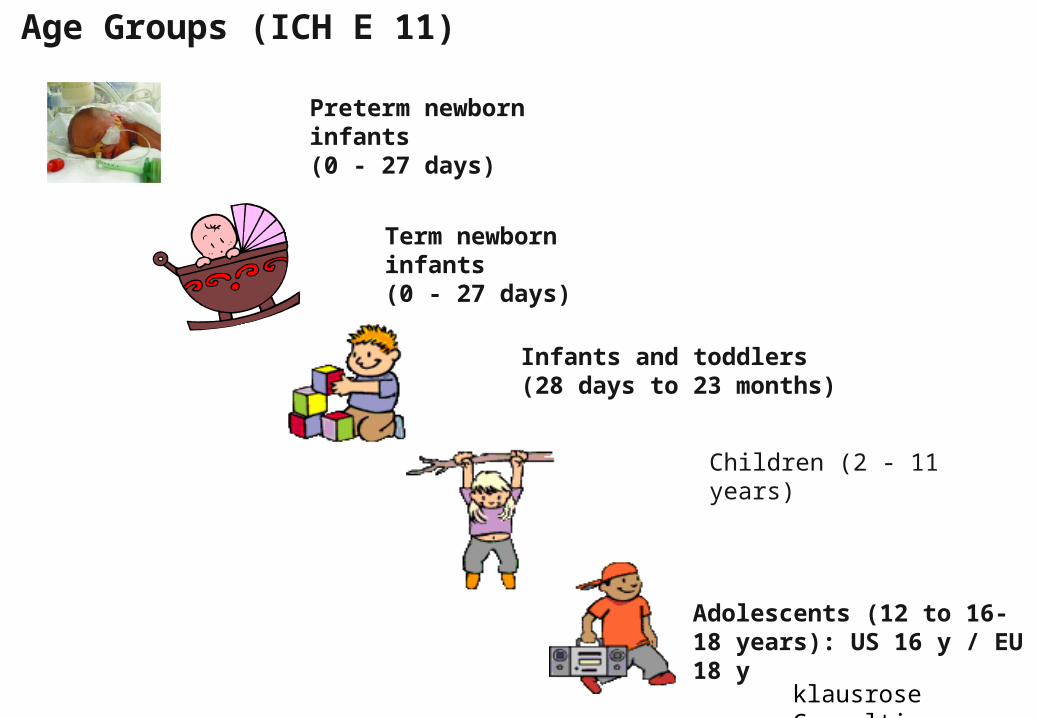
Age Groups (ICH E 11)
- 25 - 25
Term newborn infants(0 - 27 days)
Infants and toddlers(28 days to 23 months)
Children (2 - 11 years)
Adolescents (12 to 16-18 years): US 16 y / EU 18 y
Preterm newborn infants(0 - 27 days)
*ICH E 11
klausrose Consulting

26klausrose Consulting

Will be released May 2010
27klausrose Consulting
PDCO Summary Report Template D.1.b:
28
” The Regulation considers the need for data in the paediatric use. This can be based on the potential for off-label use in children. The Regulation does not require that the PIP is limited to the proposed wording of the adult indication, but it is assumed that there should be some relationship”
klausrose Consulting

EMA/ PDCO Feedbacks & Reports
• Requests for modification for validation
• Day 30 report: no action required from applicant
• Day 60 report: lists requested modifications: must be answered
• Day 90 report: lists requested last modifications
• Day 120: Showdown AND only chance for F2F Oral Explanation (OE)
29klausrose Consulting

Waivers
• Waivers are given for all children or specific age groups
• Age classifcation based on ICH E 11
• Waivers only for 3 conditions:– Drug probably ineffective or unsafe– Disease doesn‘t exist in children– No significant therapeutic benefit
- 30 - 30klausrose Consulting
• Allows company to perform pediatric measures (studies, technical development etc.) at a later defined time point
• Only concrete measures can be deferred
• Basic framework outlined in ICH E 11: – Will for most new drugs be granted as long as there are not
sufficient safety & efficacy data in adults– Will for marketed drugs with off-label pediatric use be very
difficult to obtain
- 31 - 31
Deferrals
klausrose Consulting

Melanoma PIP Considerations
• Classification as adolescent disease refers to US data 15-19ys olds. Ovarial carcinoma, 1.4/100’000 in 15-19y: class waiver stays.
• Deducing 2/5 from 1.7 (18/ 19 y old are adults) & 2/5 of 1.4 lower limit 1.02 - 0.84/ 100’000 as limit for ultra rare disease? Not official
• Melanom ist rare < 18; most are detected without metastases. With these case numbers no statistically significant results possible
→ Separate clin studies in adolescent melanoma ethically questionable• Adolescents should have the right to participate at adult studies, but • No PIPs for more frequent pediatric cancer types – because they
don’t exist in adults & hence no business case for drug development • Starts to negatively impact pediatric cancer research worldwide as
PDCO decisions block pediatric patients

Cartilage Disorders• ACT (autologous chondrocyte transplantation) routine in treating
cartilage injuries. Belated registration required by German law PIP. • Two published chondrocyte PIPs:
Autologous cartilage derived cultured chondrocytes (Genzyme) Culture expanded autologous chondrocytes (Fidia, Italy)
• Genzyme: Retrospective investigation of S and prospective investigation of S&E data in ped patients treated for cartilage defects with autologous cartilage derived cultured chondrocytes. Pediatric population from closure of femoral epiphyseal growth plate to <18 y.
• Fidia: Randomized MC S&E study of Hyalograft autologous chondrocyte implantation compared to microfracture in 16-17y olds
• An adolescent‘s knee is biologically the same as a young adult‘s one
• PDCO uses legal age to order medically & ethically questionable trials

More Examples
• Vaccines: were developed for decades without PDCO• Drugs for preterm newborns: development team’s competence is
sufficient to develop drug from research to registration – for which CHMP is responsible. Addition ‘input’ from PDCO not helpful.
• Drugs developed only for children: there are a few companies who dare. Addition ‘input’ from PDCO not helpful.
• Rare diseases starting in childhood. Drug development requires very special knowledge. MAA is discussed with CHMP. Mandatory additional PDCO discussion perceived as waist of time & resources by industry

Dosing In Adolescents
- 35 -
• In an FDA hearing 2012 12 of 13 clinicians voted for the routine acceptance of adult doses in adolescents
• Was based on an FDA report on adolescent PK Studies • Discussion is ongoing in the pediatric scientific press • FDA publications and massive advances in pediatric dosing in
pharmaceutical companies

EU Ombudsman
- 36 -
• Two companies complained against EMA/PDCO @ EU ombudsman• The EU ombudsman concluded that in contrast to EMA’s position
the complaint fell within the scope of ‘maladministration’ and hence, under his mandate.
• The enquiry resulted in recommending, inter alia,EMA guidelines to assist PDCO to follow a coherent structure of analysis in future cases.
• We will later today hear more directly from a representative of the EU ombudsman’s office!
• alia, EMA guidelines to assist PDCO to follow a coherent structure of analysis in future cases

Resources
• Big companies: PIP is one of many many challenges
• SMEs: limited resources. Additional PIP challenge is usually much more time consuming than originally thought
• Estimated consulting dimensions: • Regulatory PIP consulting: 200-300 hours• Clinical input should come from the sponsoring company• Deep clinical consulting can increase the effort by factor
3 to 5• This does not include additional internal costs by the
sponsor and not the costs of PIP execution• Even best external consulting will not allow the sponsoring
company to just forget pediatrics
37klausrose Consulting

PIP Execution
• Ca. 20 – 30‘000 € / costs per patient Study 100 adults ~ 2-3 Mio €
• Multiply with factor P for pediatric studies
• More patients higher costs
• Additional costs: juvenile animal studies, pediatric formulation, establish a registry, etc.
• BD&L rough estimate if you buy a product where pediatric homework has not been done: ~ 20 Mio € (including study execution, provided your MAA is not blocked
• A part of this money must be invested before MAA, a part thereafter
38klausrose Consulting


















