Estudio prospectivo y randomizado de pacientes con ...€¦ · 2. Al menos un episodio de sincope...
12
Estudio prospectivo y randomizado de pacientes con síncope y trastorno de conducción intraventricular. Análisis de la utilidad del Holter implantable versus marcapasos Randomized prospective study of patients with syncope and bundel branch block. Analysis of the usefulness of implantable Holter versus pacemaker Hernández Madrid A., Nannini S., Limón L., Peng J., González Rebollo J. M., Marín Marín l., Bernal E., Escobar C. RESUMEN Introducción: En pacientes con síncope y bloqueo de rama, la etiología de los síncopes no siempre se debe a bradiarritmias. Hay disponibles muy pocos datos sobre el coste-efectividad en- tre el implante de marcapasos profiláctico o la monitorización prolongada con Holter implantable. Materiales y métodos: Cuarenta y siete pacientes se anali- zaron para ser incluídos en el estudio, por presentar síncope aso- ciado a bloqueo de rama. En todos se realizó historia clínica, examen físico y métodos complementarios, con estudio electro- fisiológico. Quince fueron excluídos por hallazgos patológicos que justificaban el síncope. Finalmente se randomizaron 32 pa- cientes, en los que no se encontró una causa objetiva. Resultados: Quince pacientes fueron randomizados a mar- capasos (grupo 1) y 17 a Holter implantable (grupo II) y segui- dos durante un promedio de 9 f 6 meses. No hubo mortalidad durante el seguimiento. En el grupo 1, un paciente recurrió con etiología vasovagal. En el grupo II, seis presentaron recurrencia sincopal, dos por bloqueo autículo-ventricular y se implantó mar- capasos, un tercero debido a taquicardia ventricular y tres pre- sentaron recurrencia sin alteraciones en el trazado. Conclusiones: En pacientes con trastorno de conducción y síncope, la utilización del Holter implantable reduce la tasa de implante de marcapasos en un 88% de los pacientes. Estudio prospectivo y randomizado de pacientes con síncope y trastorno de conducción intraventricular. Análisis de la utilidad del Holter implantable W)J~IS marcapasos Hernández Madrid A, Nannini S, Limón L, Peng J, González Rebollo J M, Marín Marín 1, Bernal E, Escobar C hwe.stigrrcidt~ C~rr~lio,~cr.scular, 2004; 7: 35-46 ABSTRACT Background: In patients with bundle branch block and syn- cope, bradydysrhythmias may not always be the cause underl- ying the latter. There are few data on the approach and cost-ef- fectiveness of the treatment strategy in these patients, involving empiric pacing versus implantable Holter. Material and metbods: Forty-seven patients were analyzed. Fifteen were discontinued due to pathological findings during the study. Thirty-two patients were randomized after the history, examination and complementary investigations, including elec- trophysiological study, failed to establish the cause of syncope. Results: Fifteen patients were randomized to pacemaker (group 1) and 17 to implantable Holter (group II). No mortality was recorded during a mean follow-up of 9 t 6 months. In group 1 only one patient showed recurrence, of vasovagal etiology. In group II there were six recurrences, two due to atrioventricular block, one due to ventricular tachycardia, and three without ab- normalities in the stored electrogram. Conclusions: In patients with bundle branch block and syn- cope of unknown origm, the use of implantable Holter allows us to reduce pacemaker implantation in 88% of cases. Key words: Svncope, pncemkrr. Randomized prospective study of patients with syncope and blundel branck block. Analysis of the usefulness of implantable Holter vrrsus pacemaker Hernández Madrid A, Nannini S, Limón L, Peng J, González Rebollo J M, Marín Marín 1, Bernal E, Escobar C Irwestigrrcio’n Crrrcliovrr.rcular, 2004; 7: 35-46 Correspondencia / correspondence: Antonio Hernández Madrid Servicio de Cardiología Unidad de Arritmias Hospital Ramón y Cajal Ctra. Colmenar Viejo, km. 9,100 28034 Madrid INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.” 1 35
Transcript of Estudio prospectivo y randomizado de pacientes con ...€¦ · 2. Al menos un episodio de sincope...

Estudio prospectivo y randomizado de pacientes con síncope y trastorno de conducción intraventricular. Análisis de la utilidad del Holter implantable versus marcapasos
Randomized prospective study of patients with syncope and bundel branch block. Analysis of the usefulness of implantable Holter versus pacemaker
Hernández Madrid A., Nannini S., Limón L., Peng J., González Rebollo J. M., Marín Marín l., Bernal E., Escobar C.
RESUMEN
Introducción: En pacientes con síncope y bloqueo de rama, la etiología de los síncopes no siempre se debe a bradiarritmias. Hay disponibles muy pocos datos sobre el coste-efectividad en- tre el implante de marcapasos profiláctico o la monitorización prolongada con Holter implantable.
Materiales y métodos: Cuarenta y siete pacientes se anali- zaron para ser incluídos en el estudio, por presentar síncope aso- ciado a bloqueo de rama. En todos se realizó historia clínica, examen físico y métodos complementarios, con estudio electro- fisiológico. Quince fueron excluídos por hallazgos patológicos que justificaban el síncope. Finalmente se randomizaron 32 pa- cientes, en los que no se encontró una causa objetiva.
Resultados: Quince pacientes fueron randomizados a mar- capasos (grupo 1) y 17 a Holter implantable (grupo II) y segui- dos durante un promedio de 9 f 6 meses. No hubo mortalidad durante el seguimiento. En el grupo 1, un paciente recurrió con etiología vasovagal. En el grupo II, seis presentaron recurrencia sincopal, dos por bloqueo autículo-ventricular y se implantó mar- capasos, un tercero debido a taquicardia ventricular y tres pre- sentaron recurrencia sin alteraciones en el trazado.
Conclusiones: En pacientes con trastorno de conducción y síncope, la utilización del Holter implantable reduce la tasa de implante de marcapasos en un 88% de los pacientes.
Estudio prospectivo y randomizado de pacientes con síncope y trastorno de conducción intraventricular. Análisis de la utilidad del Holter implantable W)J~IS marcapasos Hernández Madrid A, Nannini S, Limón L, Peng J, González Rebollo J M, Marín Marín 1, Bernal E, Escobar C hwe.stigrrcidt~ C~rr~lio,~cr.scular, 2004; 7: 35-46
ABSTRACT
Background: In patients with bundle branch block and syn- cope, bradydysrhythmias may not always be the cause underl- ying the latter. There are few data on the approach and cost-ef- fectiveness of the treatment strategy in these patients, involving empiric pacing versus implantable Holter.
Material and metbods: Forty-seven patients were analyzed. Fifteen were discontinued due to pathological findings during the study. Thirty-two patients were randomized after the history, examination and complementary investigations, including elec- trophysiological study, failed to establish the cause of syncope.
Results: Fifteen patients were randomized to pacemaker (group 1) and 17 to implantable Holter (group II). No mortality was recorded during a mean follow-up of 9 t 6 months. In group 1 only one patient showed recurrence, of vasovagal etiology. In group II there were six recurrences, two due to atrioventricular block, one due to ventricular tachycardia, and three without ab- normalities in the stored electrogram.
Conclusions: In patients with bundle branch block and syn- cope of unknown origm, the use of implantable Holter allows us to reduce pacemaker implantation in 88% of cases.
Key words: Svncope, pncemkrr.
Randomized prospective study of patients with syncope and blundel branck block. Analysis of the usefulness of implantable Holter vrrsus pacemaker Hernández Madrid A, Nannini S, Limón L, Peng J, González Rebollo J M, Marín Marín 1, Bernal E, Escobar C Irwestigrrcio’n Crrrcliovrr.rcular, 2004; 7: 35-46
Correspondencia / correspondence: Antonio Hernández Madrid Servicio de Cardiología Unidad de Arritmias Hospital Ramón y Cajal Ctra. Colmenar Viejo, km. 9,100 28034 Madrid
INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.” 1 35

A. Hernández, S Nannini, L. Limón, et al.
INTRODUCCIÓN INTRODUCTION
El síncope es un síntoma muy frecuente, pue- de representar hasta un 3% de las urgencias y un 6% de las consultas ambulatorias (1). Debido a la necesidad de un diagnóstico lo más preciso posi- ble, para definir tanto el pronóstico como el trata- miento se han definido distintas metodologías de estudio, a pesar de las cuales muchos episodios quedan sin diagnóstico. Para mejorar el rendimien- to diagnóstico actualmente tenemos disponible el Holter implantable, habiendo sido confirmada su utilidad en estudios previos (2-6).
En pacientes con bloqueo de rama, síncope y hallazgos objetivos en prueba complementarias o estudio electrofisiológico patológico la actitud a seguir no suele presentar problemas. Sin embar- go, en este tipo de pacientes en los que no se en- cuentra ningún hallazgo patológico, con estudio electrofisiológico negativo, la estrategia terapéuti- ca no está bien definida. Distintas series han in- formado el desarrollo de bloqueo aurículo-ventri- cular (AV) durante el seguimiento (7-131, y en un estudio reciente se observo que este tipo de pa- cientes tiene una tasa de recurrencia del 42%, cu- yo mecanismo predominante son pausas prolon- gadas, generalmente dadas por bloqueo AV paroxístico (14).
En el presente estudio, tras la evaluacirjn com- pleta de pacientes con síncope y bloqueo de ra- ma, analizamos dos estrategias terapéuticas: el im- plante de marcapasos profiláctico o el implante de un Holter implantable.
MATERIAL Y MÉTODOS
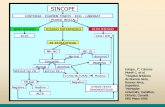
El estudio se realizó de forma randomizada y prospectiva. Se incluyeron pacientes con síncope de origen no filiado asociado a trastornos de la conducción intraventricular. Los pacientes siguie- ron el esquema diagnóstico-terapéutico de la Figura 1. Para ser randomizados, debieron cum- plir los siguientes criterios de inclusión:
1. Hombre o mujer mayor de 18 años. 2. Al menos un episodio de sincope no filiado
en los últimos seis meses. 3. Presencia de bloqueo de rama o trastorno
de conducción intraventricular. 4. Firmar consentimiento informado.
Syncope is a very common condition that may account for up to 3% of all emergency visits and 6% of global outpatient consultations (11. Maximum diagnostic accuracy is required in such situations in order to define the prognosis and treatment approach. Different study methodologies have been developed in this sense, though man y syncopal episodes remain undiagnosed. Implantable Holter systems are currently available for improving diagnostic performance, and their usefulness has been confirmed in earlier studies (2-6).
In patients with bundle block, syncope and objective findings in complementary tests, or a pathological electroph ysiological study, the indicated management approach is usually clear. However, in the case of syncopal patients without pathological findings and with a negative electroph ysiological study, the therapeutic strategy is not well defined. Different authors have descríbed the development of atrioventricular (VA) block during follow-up /7- 131, and a recent study has repotted a 42% recurrence rate in patients of this kind - the predominant mechanism involved being prolonged pauses, generally attributable to paroxysmal AV block (14).
In the present study patients with syncope and bundle block were thoroughly evaluated, with an analysis of two therapeutic strategies: empiric pacing (proph ylactic pacemaker implantation) versus implantable Holter monitorization.
MATERIAL AND METHODS
A randomized prospective study was designed, including patients with syncope of undetermíned origin associated with intraventricular conduction disorders. The diagnostic and therapeutic approach is shown in Figure 1. The randomized patients were required to meet the following inclusion criteria:
1. Males or females over 18 years of age. 2. At least one syncopal episode of
undetermined origin in the previous six months. 3. Bundle block or intraventricular
conduction disorders. No debieron tener ninguno de los siguientes
criterios de exclusión:
1. Embarazo o lactancia.
4. The signing of informed consent.
Included patients were required to meet none of the following exclusion criteria:
36 INVESTIGACIÓN CARDIOVASCULAR, 2004, val. 7, n ’ 1

Síncope y bloqueo de rama. Estudio randomizado Syncope and bundle block. Randomized study
SíNCOPE
a BLOQUEO RAMNA
QRS > 120 mseg TCIV
n EEF NEGATIVO
SYNCOPE
a BUNDLE BLOCK
0% > 120 msec, WC7
a NEGATIVE ELECTROPHYSIOLOGICAL STUDY
Se considerará positivo si: 1. Disfunción sinusal, con bradicardia sinusal y
TRNS > 1.500 mseg. 2.- HV basal > 70 mseg, bloqueo de segundo o tercer
grado durante estimulación auricular o bloqueo del His Purkinje de alto grado durante la administración de pro- cainamida (> 100 mseg).
3. Inducción de taquicardia ventricular monomorfa sos- tenida.
4. Inducción de arritmias supraventriculares, que pro- duzcan hipotensión arterial o reproduzcan los síntomas.
Pos~bv~ty IS defined by: 7. Smus dysfuncbon, wth WJUS bradycardla and SI-
nus node recovely time z 1,500 msec. 2.. Basebne HV > 70 msec, second- or thlrd-degree
blcck duting atnal panng, or highdegree H/s-Putkqe bund- le block during procalnamide adm/nistratlon (> 100 msec.).
3. Inducbon of sustamed monomorphlc ventricular tachycardia.
4. lnductlon of supraventncular dysrhythmlas causmng artenal hypotensron or the reproduction of symptoms.
n a HOLTER IMPLANTE MARCAPASOS
Figura 1. Dise60 del estudio.
n n IMPLANTABLE HOLTER PACEMAKER
Figure 1. Study design.
2. Etiología de síncope definida por la evalua- ción inicial.
3. Estudio electrofisiológico positivo. 4. Enfermedad vascular periférica significa-
tiva. 5. Trastorno severo de la conducción AV, o
cualquier otra condición de indicación de marca- pasos definitivo.
6. Disfunción autonómica demostrada. 7. Enfermedad neoplásica o psiquiátrica. 8. Abuso de drogas o alcohol.
1. Pregnancy or nursing. 2. Syncope etiology defined at initial
evaluation. 3. A positive electroph ysiological study. 4. Significant peripheral vascular disease. 5. Severe AV conduction alterations or any
other condition requiring definitive pacemaker implantation.
6. Demonstrated autonomous dysfunction. 7. Neoplastic or psychiatric disease. 8. Drug or alcohol abuse.
Protocolo de estudio Study protocol
Se realizó una historia clínica completa con los siguientes datos: edad, sexo, talla, peso, fecha de nacimiento, profesión, datos patológicos: cardio- patía estructural, antecedentes personales y fami- liares, anamnesis de los episodios sincopales te- niendo en cuenta el tiempo de evolución (en meses) desde el primer episodio, número de epi- sodios, sintomatología asociada y previa (náuse- as, diaforesis, visión borrosa, malestar gástrico), posición en que se producen (decúbito, sedesta- ción, bipedestación), reposo o esfuerzo, desenca- denantes (ninguno, dolor, emoción, micción, de- fecación, etilismo agudo), enfermedades asociadas, medicación previa.
The medical history comprised patient age, sex, height, weight, date of birth, profession, and disease state: structural heart disease, personal and family antecedents, anamnesis of the syncopal episodes taking into account the time elapsed (in months) from the first episode, the number of episodes, associated and previous symptoms (nausea, diaphoresis, blurry vision, gastric discomfort), the position in which syncope occurs fdecubitus, seated or standing), appearance at rest or in response to exertion, triggering factors (none, pain, emotions, micturition, defecation, acute ethylism), associated diseases and prior medication.
INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.’ 1

A. Hernández, S Nannini, L. Limón, et al.
Se obtuvo un examen físico completo inclu- yendo masaje del seno carotídeo, y exploracio- nes complementarias con analítica, ECG, ecocar- diograma, Holter de 24 horas y test de mesa basculante. Posteriormente, si no se había halla- do una etiología evidente se realizó un estudio electrofisiológico, con medición de tiempos de conducción AH, HV en forma basal y posterior a la administración de procainamida intravenosa a dosis de 1 mg/kg. Se realizó la medición del pun- to Wenckebach anterógrado, del tiempo de recu- peración del nodo sinusal y, posteriormente, se realizó estimulación ventricular programada con uno, dos y tres extraestímulos, desde dos puntos distintos del ventrículo derecho a frecuencia es- pontánea, a 400 y 600 mseg, y luego sobreesti- mulación.
Se consideró el estudio negativo en ausencia de:
1. Bradicardia sinusal y tiempo de recupera- ción del nodo sinusal alterado.
2. Intervalo HV basal de más de 70 mseg, blo- queo aurícula-ventricular de segundo o tercero du- rante estimulación auricular otras administración de procainamida intravenosa.
3. Inducción de taquicardia ventricular mono- motfa sostenida.
4. Inducción de taquiarritmia supraventricular rápida con descompensación hemodinámica o que reproduce los síntomas espontáneos.
A los pacientes randomizados a marcapasos se les canalizó bajo anestesia local la vena sub- clavia izquierda, se les realizó un bolsillo subfacial en la región infraclavicular izquierda, el implante de electrodo/s con medición de umbrales y resis- tencia, el implante del generador de impulsos y posteriormente se les suturó la herida por planos. A los pacientes randomizados al Holter Reveal, se les colocó a nivel paraesternal izquierdo, posterior al mapeo, el dispositivo Holter Revea1 (Medtro- nic) en plano subcutáneo. La programación del modo de registrar los eventos se realizó según la clínica del paciente. Luego se informó al pacien- te y a los familiares el manejo del activador ma- nual tras experimentar síncopes 0 presíncopes. Ambos procedimientos se realizaron sin compli- caciones.
Los pacientes fueron citados a los 6, 12, 18, 24, 30 y 38 meses. También fueron examinados in- mediatamente tras cualquier evento. Durante la visita se realizó una historia clínica, en el que se hizo hincapié en la recurrencia del síncope, carac- terísticas de los episodios, medicación preventi- va, desarrollo de nuevas enfermedades; examen físico completo, ECG y analítica. Luego se llevó
A complete physical examination was made, including carotid sinus massage and complementary studies involving laboratory tests, electrocardiogram, echocardiography, 24-hour Holter monitorization and tilting table test. Posteriorly, in the event no clear cause was identified, an electrophysiological study was carried out, with measurement of the AH and HV conduction times both at baseline and after intravenous procainamide administration (1 mg/kg). The anterograde Wenckebach point was measured, along with the sinus node recovery time, followed by programmed ventricular pacing with one, two and three extrastimuli, from two different points of the right ventricle at spontaneous frequency, and al 400 and 600 msec, followed by overpacing.
A negative study was defined by the absence Of
1. Sinus bradycardia and an altered sinus node recovery time.
2. Baseline HV interval>70 msec, second- or third-degree AV block during atrial pacing or after intravenous procainamide dosing.
3. Induction of sustaíned monomorphic ventricular tachycardia.
4. Induction of rapid supraventricular tachydysrhythmia with hemodynamic decompensation or reproduction of the spontaneous symptoms.
The patíents randomized to pacemaker were subjected to catheterization of the left subclavian vein under local anesthesia, with the preparation of a subfascial pouch in the left infraclavicular region. The electrode was positíoned, with measurement of the corresponding thresholds and resistance, and the pulse generator was implanted followed by layered wound suturing. The patients randomized to Holter were in turn subjected to subcutaneous implantation of a Holter Revea1 (Medtronic) at left parasternal level, after due mapping. The event registry mode was programmed according to the clinical condition of the patient. The patient and relatives were then instructed on the use of the manual activator following syncope or presyncope. Both procedures were completed without complications.
The patients were programmed for visits after 6, 12, 18,24,30 and 38 months. They were also examined immediately after any event. During the visits the clinical history was recorded, with emphasis on the recurrence of syncope, the characteristics of the episodes, preventive medication, and the development of new
38 INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.’ 1

Síncope y bloqueo de rama. Estudio randomizado Syncope and bundle block. Randomized study
a cabo la interrogación de los dispositivos y la impresión y análisis de los registros almacena- dos.
illnesses. A complete ph ysical examination was also carried out, together with an electrocardiographic study and laboratory tests. The devices were then evaluated, and the stored registries were printed and analyzed.
Objetivos Objectives
El objetivo de nuestro estudio fue evaluar en pacientes con bloqueo de rama y síncopes de etio- logía no filiada la utilidad del Holter implantable versus el implante de marcapasos definitivo.
Los objetivos secundarios fueron analizar la re- lación coste-beneficio, la evolución de los pacien- tes de ambos grupos, y el análisis de los trazados de ambos tipos de dispositivos ante la persisten- cia de los síntomas.
The primary objective of the study was to evaluate the usefulness of an implantable Holter versus a definitive pacemaker in patients with bundle block and syncope of undetermined origin.
The secondary objectives were a cost-benefit analysis, the study of patient evolution in both groups, and an analysis of the recordings of both types of device in the event of persistent symptoms.
Análisis estadístico Statistical analysis
Las variables cuantitativas son presentadas co- mo media + desviación estándar. La comparación de las variables cualitativas como las característi- cas clínicas, electrocardiográficas y electrofisioló- gicas entre ambas poblaciones, se realizaron me- diante la utilización del Chi cuadrado, mientras que las variables cuantitativas fueron comparadas me- diante el test de la t student. Se consideró signifi- cativo una p < 0,05.
RESULTADOS
Características clínicas se los pacientes
Desde junio de 2000 hasta agosto de 2003 se incluyeron un total de 47 pacientes, de los cuales 17 pacientes se randomizaron al implante de Hol- ter Reveal, y 15 pacientes al implante de marca- pasos definitivo. Los 15 pacientes restantes fue- ron excluidos 13 por HV prolongado (más de 70 ms), uno por la inducción de arritmia ventricular maligna y cardiopatía estructural y el último por enfermedad del nodo sinusal. Un paciente sin an- tecedentes de cardiopatía estructural y randomi- zado al implante de marcapasos, presentó in- ducción de fibrilación ventricular durante la estimulación ventricular programada requiriendo desfibrilación, siendo esto considerado como res- puesta inespecífica. Las características clínicas, electrocardiográficas y electrofisiológicas son mos- tradas en la Tabla 1.
Quantitative variables were recorded as the mean 2 standard deviation (SD). Comparison of the qualitative variables, e.g., clinical, electrocardiographic and electroph ysiological characteristics, between the two groups was made usíng the chi-square test, while the quantitatíve variables were contrasted by means of the Student t-test. Statistical significance was considered for p < 0.05.
RESULTS
Clinical characteristics of the patients
From June 2000 to August 2003 a total of 47 patients were recruited. Of these, 17 were andomized to Holter Revea1 implantation and 15 to definitive pacemaker implantation. The remaining 15 patients were discontinued: 13 due to prolonged HV conduction f> 70 msec.); one because of the induction of malignant ventricular dysrhythmia and the presente of structural heart disease; and another due to sinus node disease. One patient without a history of structural heart disease and randomized to pacemaker suffered ventricular fibrillation during programmed ventricular pacing that required defibrillation; this was regarded as a nonspecific response. The clinical, electrocardiographic and electroph ysiological characteristics are shown ín Table 1.
INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, m” 1 39

A. Hernández, S Nannini, L. Limón, et al.
TABLA 1. Características clínicas de los pacientes / TABLE 1. Clinical characterisitics of the patients
Marcapasos / Holter implantable / Pacemaker Implantable Holter
N.” de pacientes 15 17 No. of patients Edad, (años) 70 + 6 70 2 7 NS Age (yearsl Varones, N (%) 12 (80%) ll (65%) NS Males (%) Cardiopatía estructural, N (%) 8 (53%) 9 (52%) NS Structural heart diseases, N (%)
lsquémica 3 4 NS Ischemic Hipertensiva 3 2 NS Hypertensive Valvular 0 1 NS Valvular Dilatada 2 2 NS Dilatory
FE, % 572 10 58 * 9 NS EF, % HV (ms) 6Ok 8 59 2 5 NS HV (msec) N.” de episodios sincopales 2.1 2 0.9 2.4 + 0.75 NS No. of syncopal episodes Traumatismos 3 4 NS Traumatisms Pródromos 8 9 NS Prodromic manifestations
FE: fracción de eyección ventricular izquierda. EI? left ventricle eiection fraction.
Seguimiento clínico
Los pacientes fueron seguidos entre 2 a 38 me- ses con un promedio de 9 f 6 meses, y el fin del seguimiento se debió a el cumplimiento del obje- tivo principal, el agotamiento de la batería del Hol- ter, la pérdida del paciente (debido a abandono, pérdida de contacto telefónico, mudanza a otra ciudad, otros) o la finalización del estudio. Durante el seguimiento no hubo mortalidad en ninguno de los pacientes.
Se implantaron 15 marcapasos, de éstos, do- ce fueron bicamerales, dos VDD y un sistema de resincronización ventricular en un paciente porta- dor de miocardiopatía dilatada e insuficiencia car- díaca congestiva. Sólo un paciente presentó co- mo complicación la infección del bolsillo del marcapasos por lo que el dispositivo fue explan- tado. En el otro grupo se realizó el implante de Holter Revea1 en 17 pacientes, con una progra- mación de activación de eventos automáticos o manuales y definición de frecuencias a sensar in- dividualizada a cada situación. Sólo un paciente presentó agotamiento prematuro del dispositivo, por lo que fue reemplazado por otro.
Hubo ocho recurrencias con un tiempo medio desde la randomización hasta el evento de 3,8 f 3 meses. De los pacientes randomizados a mar- capasos, hubo sólo una recurrencia de presíncope similar a los episodios previos, que fue cataloga- do como disaufonomía diabética. De los pacien- tes randomizados a Holter Revea1 hubo seis recu-
40
Clinical follow-up
The patients were followed-up on for 2 to 38 months, with an average of 9 2 6 months. Follow-up ended when the primary objective was reached, the Holter battery ran out, the patient was lost to follow-up (dropout, loss of telephone contact, change of residency, or other causes), or the study was completed. No deaths were recorded during follow-up.
Fifteen pacemakers were implanted (12 bicameral, two VDD, and one ventricular resynchronization system in a patient with dilated m yocardiopath y and congestive heart failurel. Only one patient presented complications in the form of pacemaker pouch infection, as a result of which the device was explanted. In the other group, Holter Revea1 monitors were implanted in 17 patients, with automatic or manual event activation programming and sensing frequency definitions adapted to each situation. Only one patient showed early exhaustion of the device, which was replaced by another unit.
There were eight recurrences, with an average time from randomization to the event of 3.8 ? 3 months. The pacemaker group presented a single presyncope recurrence similar to the previous episodes (classified as a diabetic autonomic alteration). In the Holter group there were 6 recurrences, comprising two syncopal complete AV blocks (Figure 2) requiring
INVESTIGACIÓN CARDIOVASCULAR, 2004; WI. 7, n.’ 1

Síncope y bloqueo de rama. Estudio randomizado Syncope and bundle block. Randomized study
rrencias, dos bloqueos aurícula-ventriculares com- pletos sincopales (Figura 21, que requirieron el im- plante de marcapasos definitivo, una taquicardia ventricular monomotfa sostenida sintomática en una paciente con disfunción severa ventricular iz- quierda (Figura 3). Los tres casos restantes no pre- sentaron alteraciones significativas en los regis- tros del dispositivo durante los síntomas, siendo considerados de etiología vasovagal. En otro pa- ciente con antecedente de cardiopatía isquémica se objetivo durante una crisis de angor el supra- desnivel transitorio del segmento ST en el regis- tro (Figura 4). De los pacientes excluídos, a los que se le implantó un marcapasos, hubo uno con re- currencia de mareos, también siéndole atribuido a neuropatía diabética y disautonomía. El resto de
definitive pacemaker implantation, and one symptomatic sustained monomorphic ventricular tachycardia episode in a patient with severe left ventricular dysfunction (Figure 3). The remaining three cases showed no significant alterations of the device recordings during the symptomatic episode, and were considered to be of vasovagal origin. Another patient with a histoty of ischemic heart disease showed transient ST-segment displacement on the recording during an angina1 episode (Figure 4). Regarding the excluded patients in whom a pacemaker was implanted, one presented recurrence of dizziness that was likewise attributed to diabetic neuropathy and autonomic dysfunction. The rest of the patients
Figura 2. Registro del Revea1 de un paciente de 70 años portador de bloqueo de rama derecha con eje del QRS desvia- do a la izquierda durante un episodio de Stokes-Adams. Se observa el bloqueo aurículoventricular completo con ritmo de escape de QRS ancho. La velocidad de registro es de 25 mm/seg.
Figure 2. Holter Revea/ recording in a 70-year-old male with right bundle block and left deviation of the QRS axis during a Stokes-Adam episode. Complete AV block with a broad QRS escape rhythm is observed. The recording velocity was 25 mm/se-c.
INVESTIGACION CARDIOVASCULAR, 2004, val. 7, n.O 1 41

A. Hernández, S Nannini, L. Limón, et al.
Figura 3. Registro del Revea1 que muestra taquicardia ventricular monomorfa sostenida posterior a ritmo sinusal, en una paciente de 68 años portadora de miocardiopatía dilatada con depresión de la fracción de eyección, bloqueo de rama iz- quierda y estudio electrofisiológico negativo. La velocidad de registro es de 25 mm/seg.
Figure 3. Holter Revea/ recordíng showing sustained monomorphic ventricular tachycardia posterior to sinus rhythm in a 68-year-old woman with dilated myocardiopathy and reduced ejection fraction, left bundle block and a negative elec- trophysiological study. The recording velocity was 25 mm/se-c.
Figura 4. Registro del Revea1 que muestra onda de lesión transitoria en un paciente de 58 años portador de cardiopatía isquémica durante una crisis de angor. La velocidad de registro es de 25 mm/seg.
r
Figure 4. Holter Revea/ recording showing a transient lesion wave in a 58-year-old male with ischemíc heart disease in the course of an angina/ episode. The recording velocity was 25 mm/se-c.
los pacientes no habían tenido nuevos eventos al had suffered no new events at the end of final del seguimiento. follow-up.
DISCUSIÓN
Ante un paciente con síncope, la secuencia de estudios diagnósticos varía de acuerdo al núme-
DISCUSSION
When dealing with patients presenting syncope, the diagnostic sequence varies
42 INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.’ 1

Síncope y bloqueo de rama. Estudio randomizado Syncope and bundle block. Randomized study
ro de eventos, formas de presentación y a la sos- pecha clínica. En un extremo están los pacientes sin cardiopatía ni trastornos de la conducción in- traventricular y con alta probabilidad de etiología vasovagal con buena evolución en el seguimien- to pero muchas veces con síntomas recurrentes y refractarios al tratamiento médico. Por otra parte están los pacientes con sospecha de etiología arrít- mica, en los cuales se recomienda el estudio pre- coz y completo de los mismos, incluyendo el es- tudio electrofisiológico.
La utilidad del estudio electrofisiológico en el diagnóstico del síncope ha sido ampliamente in- vestigada (16, 17). Sin embargo, es conocido el hecho de que el estudio electrofisiológico normal en pacientes con bloqueo de rama en el electro- cardiograma, no descarta el bloqueo aurículo-ven- tricular paroxístico ya ha sido descrito previamente (7, 8). Además también ha habido publicaciones sobre la recurrencia de los eventos y mortalidad de hasta un 30% al año, fundamentalmente a ex- pensas de taquicardia ventricular en pacientes con disfunción ventricular izquierda y estudios elec- trofisiológicos negativos (18).
Debido a estas dificultades en el diagnóstico etiológico de los eventos sincopales, y a la difícil relación entre los hallazgos de los estudios com- plementarios con el síntoma, surge el Holter im- plantable como una herramienta adicional de diag- nóstico potencialmente útil en muchos de estos pacientes.
Después de revisar la literatura no hemos en- contrado ningún estudio publicado de las carac- terísticas del presente. Sí hemos hallado estudios como el ISSUE, que evaluó un subgrupo de pa- cientes con síncopes y bloqueo de rama (141, pe- ro que se focalizaba en definir cual era el meca- nismo de los episodios y la tasa de recurrencia de los mismos sin comparar directamente la eficien- cia de estas dos estrategias terapéuticas. Según este grupo de investigadores y otros autores, en los pacientes con síncope y bloqueo de rama, el bloqueo AV paroxístico es la causa más frecuen- te, aunque no la única de los eventos sincopales (12, 14).
Debido a la dificultad para encontrar variables predictoras del mecanismo del síncope y, por lo tanto, de la necesidad de implante de marcapasos (151, pensamos que comparar estas dos alternati- vas es importante ya que el coste asociado a ca- da una es distinto.
A diferencia de algunos estudios clínicos (19- 211, y en concordancia con otros (3, ll, 141, el prin- cipal hallazgo de este estudio es que durante el seguimiento realizado la mortalidad de los pa- cientes fue nula asociado a baja morbilidad. Esto
according to the number of events, the forms of presentation and the clinical clues. Syncopal patients range from individuals wíthout heat-t disease or intraventricular conduction problems, where the likely cause is vasovagal and the course is favorable -though often with recurrent symptoms that are refractory to medical treatment - to patients with a suspected dysrhythmic etiology where early and complete evaluation is indicated, including an electroph ysiological study.
The usefulness of electroph ysiological evaluation in diagnosing syncope has been extensively investigated (76, 17). However, it is known that a normal electroph ysiological study in patients presenting bundle block on the electrocardiogram does not discard possible paroxysmal A V block (7,s). Moreover, a number of studies have reported recurrences of the events and mortal@ reaching 30% after one year - fundamentally due to ventricular tach ycardia in patients wíth left ventricle dysfunction and negative electroph ysiological findings (18).
In view of these difficulties in establishing an etiologic diagnosis of syncopal events, and the complications for correlatíng the findings of complementay studies to the symptomatology, the implantable Holter monitor appears as a potentially useful diagnostic tool in sch patients.
A review of the literature failed to revea1 any previous studies similar to our own. A number of investigations, such as the ISSUE study, were found that evaluated a subgroup of patients with syncope and bundle block (14), though emphasis in this case was placed on defining the mechanism underlying the episodes and their recurrence rate - without directly contrasting the effectíveness of the two therapeutic strategies considered. According to these and other authors, in patients with s yncope and bundle block, paroxysmal A V block is the most frequent cause of syncope - though not the only one (12, 14).
In view of the diffículty of defining variables capable of predicting the mechanism of syncope and therefore the need for pacemaker implantation (15), we consider it impottant to contrast these two management alternatives, since the cost associated to each is different.
Unlike some clinical studíes (19-21), and in concordante with others (3, 11, 14), the main finding ín this study was that patient mortal@ was zero and morbidity low in the course of follow-up. This may be due to the different patient selection criteria involved as
INVESTIGACdN CARDIOVASCULAR, 2004; val. 7, n.” 1 43

A. Hernández, S Nannini, L. Limón, et al.
posiblemente se deba a la distinta selección de pa- cientes en lo que se refiere a la prevalencia de car- diopatía estructural fundamentalmente con dis- función ventricular izquierda e insuficiencia cardíaca (14) y al incluir pacientes con múltiples explora- ciones complementarias y estudio electrofisioló- gico normal (7, 8).
Debido posiblemente al escaso número de la muestra, el presente estudio no ha encontrado nin- gún determinante clínico ni electrocardiográfico predictor del desarrollo de bloqueo aurículo-ven-
El diagnóstico de bradiarritmia severa como
tricular establecido o intermitente durante el se-
causa más común del síncope también concuer- da con otras publicaciones previamente citadas (14, 151, en las cuales mediante la estrategia del
guimiento. El hallazgo de la alteración de la repo-
Holter implantable un 44% recibió tratamiento con marcapasos. En el presente estudio se implantó
larización con la apariencia de supradesnivel del
marcapasos sólo en un 12% de los pacientes ran- domizados al grupo Holter, durante el seguimien-
ST en un paciente coronario durante una crisis de
to efectuado (Figura 5).
angina demuestra una nueva utilidad de este tipo de dispositivos de grabación.
En resumen, a pesar que se han reportado se- ries con disminución de las recurrencias de los epi- sodios sincopales posterior al implante empírico de marcapasos (211, nuestro estudio también des- taca la utilidad del Holter implantable en este tipo de pacientes, ya que sólo se necesitó el implante de marcapasos definitivo en un 12% de los pa- cientes randomizados a la estrategia de monitori- zación prolongada. Por lo tanto, en pacientes con
regards the prevalence of structural heart disease -fundamental@ with left ventricle dysfunction and heart failure (14)- and to the fact that patients with multiple complementary explorations and normal electrophysiological findings were included (7, 8).
Possibly as a result of the limited sample size, we identified no clinical or electrocardiographic predictor of the
The diagnosis of severe bradydysrhythmia as the most common cause of syncope also
development of established or intermittent AV
coincides with the observations of the aforementioned studies (14, 151, where 44% of
block during follow-up. The observatíon of
the subjects subjected to implantable Holter
altered repolarization with apparent ST-segment
monitorization received a pacemaker. In the present study pacemakers were only implanted in 12% of the patients randomized to
displacement in a patient with coronary disease
the Holter group in the course of follow-up
during an angina1 episode suggests a new and
(Figure 51.
useful application for this type of Holter recording s ystem.
To summarize, despite reports in the literature of reductions in syncope recurrence after empirical pacemaker implantation (Zl), our study stresses the usefulness of implantable Holter monitorization in such patients, since the implantation of a definitive pacemaker only proved necessary in 12% of the subjects randomly assigned to the prolonged monitorization strategy. There fore, in patients
Figura 5. Represen- tación gráfica de la etiología de las recu- rrencia de eventos en los pacientes ran- domizados al Holter Reveal.
50
Recurrencias en el grupo Revea1 / Recurrences ,in the Holter Reval Group
0 Vasovagall Vasovagal 0 TVMS / SMVT
0 Bloqueo AV l AV block
Figure 5. Graphic re- presentatíon of the recurrence of events in patients randomly assigned to Holter Revea1 monitoriza- Con.
44 INVESTIGACIÓN CARDIOVASCULAR, 2004, val 7, II.’ 1

Síncope y bloqueo de rama. Estudio randomizado
trastornos de la conducción intraventricular y sín- copes de origen no filiado, el uso del Holter im- plantable es una estrategia segura, eficaz y con una buena relación coste-eficacia.
CONCLUSIONES
Syncope and bundle block. Randomized study
with intraventricular conduction alterations and syncope of undetermined origin, the implantable Holter offers a safe effective management strategy, with a good cost-effectiveness ratio.
CONCLUSIONS
1. La mortalidad en estos pacientes durante el seguimiento fue nula y la morbilidad fue baja, in- dependientemente de ser tratados con marcapa- sos o recibir un sistema de monitorización de lar- ga duración.
2. Durante el seguimiento efectuado (2-38 me- ses), la necesidad de implante de marcapasos en el grupo de pacientes con Holter implantable fue de un 12%, que es razonablemente bajo.
3. En el grupo Reveal, si bien sólo el 33% re- currió en forma de bloqueo AV completo, no po- demos inferir que el resto de los pacientes no ne- cesiten un marcapasos en el futuro.
4. La eficiencia y relación coste-efectividad del sistema de Holter implantable fue muy alta en nuestro grupo de pacientes, al permitir ahorrar du- rante el seguimiento efectuado un 88% de im- plantes de marcapasos, con nula morbimortali- dad.
5. El hallazgo de la posible onda de lesión tran- sitoria en el registro del Holter implantable (tenien- do en cuenta que es sólo una derivación electro- cardiográfica) nos alienta a investigar una nueva metodología de estudio con fines diagnósticos y pronósticos en pacientes con angina variante, 0 isquemia silente en coronarios de alto riego.
6. Los pacientes asignados al grupo marca- pasos tienen un bajo índice de recurrencias sin- copales.
1. Mortal@ in our series during follow-up was zero, and the morbidity was low, regardless of whether a pacemaker was implanted ora Holter monitor was used.
2. During follow-up (2-38 months), pacemaker implantation proved necessary in the Holter group in 12% of patients - this figure being reasonably low.
3. In the Holter Revea1 group, while only 33% showed recurrence in the form of complete AV block, it cannot be postulated that the rest of the patients will not require a pacemaker in future.
4. The effectiveness and cost-benefit ratio of the implantable Holter system was vety high in our series, affording an 88% reduction in pacemaker implantations during follow-up, with no associated morbidity-mortal@.
5. The finding of the possible transient lesion wave in the implantable Holter registty (taking into account that it constitutes a single electrocardiographic leadl encourages us to evaluate a new investigational method for diagnostic and prognostic purposes in patients with variant angina or silent ischemia in high-risk coronary patients.
6. The patients randomized to the pacemaker group showed a low incidence of s yncopal recurrence.
BIBLIOGRAFíA / REFERENCES
1. DAY S C, COOK E F, FUNKENSTEIN H, GOLDMAN L. Evaluation and outcome of emergency room patients with transient loss of conciousness. Am J Med. 1982; 72: 15-23.
2. KRAHN A D, KLEIN G J, YEE R, MANDA V. The high cost of syncope: cost implications of a new insertable loop recorder in the investigation of recurrent synco- pe. Am Heart J. 1999; 137 (5): 870-871.
3. KRAHN A, KLEIN G J, YEE R, SKANES A C. Randomi- zed assessment of syncope trial. Conventional diag- nostic testing versus a prolonged monitoring strategy. Circulation. 2001; 104: 46-51.
4. KRAHN A D, KLEIN G J, YEE R, TAKLE-NEWHOUSE T, NORRIS C. Use of an extended monitoring strategy
in patients with problematic syncope, Revea1 Investi- gators. Circulation. 1999; 26; 99: 406-410.
5. SEIDL K, RAMEKEN M, BREUNUNG S, SENGES J, JUNG W, ANDRESEN D, VAN TOOR A, et al. Diagnos- tic assessment of recurrent unexplained syncope with a new subcutaneously implantable loop recorder. Reveal-lnvestigators. Europace. 2000; 2 (3): 256-262.
6. ASHBY D T, CEHIC D A, DISNEY P J, MAHAR L J, YOUNG G D. A retrospective case study to assess the value of the implantable loop recorder for the investi- gation of undiagnosed syncope. f’acing CIin Electro- physiol. 2002; 25 (8): 1200-1205.
7. KUSHNER J A, KON W H, KADISH A H, MORADY F. Natural history of patients with unexplained syncope
INVESTIGACION CARDIOVASCULAR, 2004, val. 7, n o 1 45

A. Hernández, S Nannini, L. Limón, el al.
and a non-diagnostic electrophysiologic study. J Am Coll Cardiol. 1989; 14: 391-396.
8. LINK M, KIM K M, HOMOUD M, ESTES III M, WANG P. Long term outcome of patients with syncope as- sociated with coronary artery disease and a non-diag- nostic electrophysiological evaluation. Am J Cardiology. 1999; 83: 1334-1337.
9. GAGGIOLI G, BOnONI N, BRIGNOLI M, et al. Progres- sion to second or third degree atrioventricular block in patients electrostimulated for bundle branch block: a long-term study. G Ita/ Cardiol. 1994; 24: 409-416.
10. KAPOOR W N. Evaluation and outcome of patients with syncope. Medecine. 1990; 69: 160-175.
11. DONATEO P, BRIGNOLE M, ALBONI P, MENOZZI C, RABIELE A, DEL ROSSO A, et al. A standardized con- ventional evaluation of the mechanism of syncope in patients with bundle branch block. Europace. 2002; 4 (4): 357-360.
12. KRAHN A D, KLEIN G J, NORRIS C, et al. The etiology of syncope in patients with negative tilt table an elec- trophysiological testing. Circularion. 1995; 92: 1819- 1824.
13. MENOZZI C, BRIGNOLE M, GARCíA-CIVERA R, MOYA A, BOTO GIANLUCA, TERCEDOR L, et al. Mechanism of syncope in patients with heart disease and negati- ve electrophysiologic test. Circulation. 2002; 105: 2741. 2745.
14. BRIGNOLE M; MENOZZI C, MOYA A, GARCíA-CIVERA R. MONT L. ALVAREZ M, et al. Mechanism of synco-
pe in patients with bundle branch block and negative electrophysiological test. ISSUE Investigators. Circula- tion. 2001; 104: 2045-2050.
15. KRAHN A D, KLEIN G J, FITZPATRICK A, SEIDL K, ZAIDI A, SKANES A, YEE R. Predicting the outcome of patients with unexplained syncope undergoing pro- longed monitoring. PACE. 2002; 25: 37-41.
16. KLEIN G J, GERSH B J, YEE R. Electrophysiological testing. The final court of appeal for diagnosis of syn- cope? Circulation. 1995; 92: 1332-1335.
17. BASS E B, ELSON J J, FOGOROS R N, et al. Long-term prognosis of patients undergoing electrophysiologic studies for syncope of unknown origin. Am J Cardiol. 1988; 62: 1186-1191.
18. KAPOOR W M, HANUSA B. Is a syncope a risk factor for poor outcomes?. Comparison of patients with and without syncope. Am J Med. 1996; 100: 646-655.
19. SOTERIADES E S, EVANS J C, LARSON M G, HUI CHEN M, CHEN L, BENJAMIN E J, et al. Incidence and prognosis of syncope. N Engl J Med. 2002; 347 (12): 878-885.
20. KAPOOR W N, KARPF M, WIEAND S, PETERSON J R, LEVEY G S. A prospective evaluation and follow-up of patients with syncope. N fngl J Med. 1983; 309: 197- 204.
21. RATTES M F, KLEIN G J, SHARMA A D, et al. Efficacy of empirical cardiac pacing in syncope of unknown cause. CMAJ. 1989; 140: 381-385.
INVESTIGACIÓN CARDIOVASCULAR, 2004; val. 7, n.” 1