ESPEN Guidelines on Enteral Nutrition: Geriatricsespen.info/documents/ENGeriatrics.pdf · ESPEN...
31
Clinical Nutrition (2006) 25, 330–360 ESPEN GUIDELINES ESPEN Guidelines on Enteral Nutrition: Geriatrics $ D. Volkert a, ,1 , Y.N. Berner b , E. Berry c , T. Cederholm d , P. Coti Bertrand e , A. Milne f , J. Palmblad g , St. Schneider h , L. Sobotka i , Z. Stanga j , DGEM: $$ R. Lenzen-Grossimlinghaus, U. Krys, M. Pirlich, B. Herbst, T. Schu ¨tz, W. Schro¨er, W. Weinrebe, J. Ockenga, H. Lochs a Head Medical Science Division, Pfrimmer-Nutricia, Erlangen, Germany b Head Geriatric Department, Meir Hospital, Kfar Saba, Israel c Department of Human Nutrition & Metabolism, Hebrew University, Hadassah Med School, Jerusalem, Israel d Department of Public Health and Caring Science, Uppsala University, Uppsala, Sweden e Unite´ de Nutrition Clinique, CHUV, Lausanne, Switzerland f Health Services Research Unit, University of Aberdeen, Aberdeen, UK g Department of Medicine, Karolinska Institute, Huddinge University Hospital, Huddinge, Sweden h Gastroente´rologie et Nutrition Clinique, Hopital de l’Archet, Nice, France i Metabolic Care Unit, Department of Gerontology and Metabolic Care, Charles University, Faculty of Medicine, Hradec Kralove, Czech Republic j Internal Medicine and Clinical Nutrition, Inselspital/University Hospital, Bern, Switzerland Received 18 January 2006; accepted 19 January 2006 KEYWORDS Guideline; Clinical practice; Evidence-based; Recommendations; Summary Nutritional intake is often compromised in elderly, multimorbid patients. Enteral nutrition (EN) by means of oral nutritional supplements (ONS) and tube feeding (TF) offers the possibility to increase or to insure nutrient intake in case of insufficient oral food intake. The present guideline is intended to give evidence-based recommendations for the use of ONS and TF in geriatric patients. It was developed by an interdisciplinary expert group in accordance with officially accepted standards and is based on all ARTICLE IN PRESS http://intl.elsevierhealth.com/journals/clnu 0261-5614/$ - see front matter & 2006 European Society for Clinical Nutrition and Metabolism. All rights reserved. doi:10.1016/j.clnu.2006.01.012 Abbreviations: ADL, activities of daily living; BCM, body cell mass; BMI, body-mass index; CI, confidence interval; EN, enteral nutrition; FFM, fat-free mass; IADL, instrumental activities of daily living; MAC, mid-arm circumference; MAMC, mid-arm muscle circumference; NGT, nasogastric tube; ONS, oral nutritional supplement; OR, odds ratio; PEG, percutaneous endoscopic gastrostomy; RR, relative risk; SD, standard deviation; TF, tube feeding; TSF, triceps skin fold $ For further information on methodology see Schu ¨tz et al. 173 For further information on definition of terms see Lochs et al. 174 Corresponding author. Tel.: +49 9131 7782 31; fax: +49 9131 7782 86. E-mail address: [email protected] (D. Volkert). 1 Dorothee Volkert had been employed at the Department of Nutrition Science, University of Bonn, until May 31, 2005; she was not industry employed during the development of the guidelines. $$ The authors of the DGEM (German Society for Nutritional Medicine) guidelines on enteral nutrition in geriatrics are acknowledged for their contribution to this article.
Transcript of ESPEN Guidelines on Enteral Nutrition: Geriatricsespen.info/documents/ENGeriatrics.pdf · ESPEN...

ARTICLE IN PRESS
Clinical Nutrition (2006) 25, 330–360
0261-5614/$ - sdoi:10.1016/j.c
Abbreviationnutrition; FFM,circumference;RR, relative ris
$For further�CorrespondE-mail addr
1Dorothee Voindustry emplo
$$The autacknowledged
http://intl.elsevierhealth.com/journals/clnu
ESPEN GUIDELINES
ESPEN Guidelines on Enteral Nutrition: Geriatrics$
D. Volkerta,�,1, Y.N. Bernerb, E. Berryc, T. Cederholmd, P. Coti Bertrande,A. Milnef, J. Palmbladg, St. Schneiderh, L. Sobotkai, Z. Stangaj,DGEM:$$ R. Lenzen-Grossimlinghaus, U. Krys, M. Pirlich, B. Herbst,T. Schutz, W. Schroer, W. Weinrebe, J. Ockenga, H. Lochs
aHead Medical Science Division, Pfrimmer-Nutricia, Erlangen, GermanybHead Geriatric Department, Meir Hospital, Kfar Saba, IsraelcDepartment of Human Nutrition & Metabolism, Hebrew University, Hadassah Med School,Jerusalem, IsraeldDepartment of Public Health and Caring Science, Uppsala University, Uppsala, SwedeneUnite de Nutrition Clinique, CHUV, Lausanne, SwitzerlandfHealth Services Research Unit, University of Aberdeen, Aberdeen, UKgDepartment of Medicine, Karolinska Institute, Huddinge University Hospital, Huddinge, SwedenhGastroenterologie et Nutrition Clinique, Hopital de l’Archet, Nice, FranceiMetabolic Care Unit, Department of Gerontology and Metabolic Care, Charles University,Faculty of Medicine, Hradec Kralove, Czech RepublicjInternal Medicine and Clinical Nutrition, Inselspital/University Hospital, Bern, Switzerland
Received 18 January 2006; accepted 19 January 2006
KEYWORDSGuideline;Clinical practice;Evidence-based;Recommendations;
ee front matter & 2006lnu.2006.01.012
s: ADL, activities of dafat-free mass; IADL, inNGT, nasogastric tube;k; SD, standard deviatioinformation on method
ing author. Tel.: +49 913ess: d.volkert@nutricialkert had been employeyed during the develophors of the DGEM (Gefor their contribution to
Summary Nutritional intake is often compromised in elderly, multimorbidpatients. Enteral nutrition (EN) by means of oral nutritional supplements (ONS)and tube feeding (TF) offers the possibility to increase or to insure nutrient intake incase of insufficient oral food intake.
The present guideline is intended to give evidence-based recommendations forthe use of ONS and TF in geriatric patients. It was developed by an interdisciplinaryexpert group in accordance with officially accepted standards and is based on all
European Society for Clinical Nutrition and Metabolism. All rights reserved.
ily living; BCM, body cell mass; BMI, body-mass index; CI, confidence interval; EN, enteralstrumental activities of daily living; MAC, mid-arm circumference; MAMC, mid-arm muscleONS, oral nutritional supplement; OR, odds ratio; PEG, percutaneous endoscopic gastrostomy;n; TF, tube feeding; TSF, triceps skin foldology see Schutz et al.173 For further information on definition of terms see Lochs et al.174
1 7782 31; fax: +49 9131 7782 86..com (D. Volkert).d at the Department of Nutrition Science, University of Bonn, until May 31, 2005; she was notment of the guidelines.rman Society for Nutritional Medicine) guidelines on enteral nutrition in geriatrics arethis article.

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 331
Enteral nutrition;Oral nutritionalsupplements;Tube feeding;Geriatric patients;Undernutrition;Malnutrition;Elderly;Aged-80-and-over
relevant publications since 1985. The guideline was discussed and accepted in aconsensus conference.
EN by means of ONS is recommended for geriatric patients at nutritional risk, incase of multimorbidity and frailty, and following orthopaedic-surgical procedures. Inelderly people at risk of undernutrition ONS improve nutritional status and reducemortality. After orthopaedic-surgery ONS reduce unfavourable outcome. TF is clearlyindicated in patients with neurologic dysphagia. In contrast, TF is not indicated infinal disease states, including final dementia, and in order to facilitate patient care.Altogether, it is strongly recommended not to wait until severe undernutrition hasdeveloped, but to start EN therapy early, as soon as a nutritional risk becomesapparent.
The full version of this article is available at www.espen.org.& 2006 European Society for Clinical Nutrition and Metabolism. All rights reserved.
Summary of statements: Geriatrics
Subject
Recommendations Grade173 N umberIndications
In patients who are undernourished or at risk ofundernutrition use oral nutritional supplementation toincrease energy, protein and micronutrient intake,maintain or improve nutritional status, and improvesurvival.A 2
.1In frail elderly use oral nutritional supplements (ONS) toimprove or maintain nutritional status.
A 2
.2Frail elderly may benefit from TF as long as their generalcondition is stable (not in terminal phases of illness).
B 2
.2In geriatric patients with severe neurological dysphagiause enteral nutrition (EN) to ensure energy and nutrientsupply and, thus, to maintain or improve nutritionalstatus.
A 2
.3In geriatric patients after hip fracture and orthopaedicsurgery use ONS to reduce complications.
A 2
.4In depression use EN to overcome the phase of severeanorexia and loss of motivation.
C 2
.6In demented patients ONS or tube feeding (TF) may leadto an improvement of nutritional status.
2
.7In early and moderate dementia consider ONS—andoccasionally TF—to ensure adequate energy and nutrientsupply and to prevent undernutrition.
C 2
.7In patients with terminal dementia, tube feeding is notrecommended.
C 2
.7In patients with dysphagia the prevention of aspirationpneumonia with TF is not proven.
2
.9ONS, particularly with high protein content, can reducethe risk of developing pressure ulcers.
A 2
.10Based on positive clinical experience, EN is alsorecommended in order to improve healing of pressureulcers.
C 2
.10
ARTICLE IN PRESS
D. Volkert et al.332
Application
In case of nutritional risk (e.g. insufficient nutritionalintake, unintended weight loss 45% in 3 months or 410%in 6 months, body-mass index (BMI) o20 kg/m2) initiateoral nutritional supplementation and/or TF early.B 2
.1In geriatric patients with severe neurological dysphagiaEN has to be initiated as soon as possible.
C 2
.3In geriatric patients with neurological dysphagiaaccompany EN by intensive swallowing therapy until safeand sufficient oral intake is possible.
C 2
.3Initiate enteral nutrition 3 hours after PEG placement.
A 3 .2Route
In geriatric patients with neurological dysphagia preferpercutaneous endoscopic gastrostomy (PEG) tonasogastric tubes (NGT) for long-term nutritional support,since it is associated with less treatment failures andbetter nutritional status.A 2
.3Use a PEG tube if EN is anticipated for longer than 4weeks.
A 3
.1Type offormula
Dietary fibre can contribute to the normalisation of bowelfunctions in tube-fed elderly subjects.
A 3
.4Grade: Grade of recommendation; Number: refers to statement number within the text.
Terminology
Geriatric patient—a biologically elderly patient who is at acute risk of loss of independence due to acuteand/or chronic diseases (multiple pathology) with related limitations in physical, psychological, mentaland/or social functions. The abilities to perform the basic activities of independent daily living arejeopardised, diminished or lost. The person is in increased need of rehabilitative, physical, psychologicaland/or social care to avoid partial or complete loss of independence.
Elderly—a term used to describe a particular age group, i.e. over 65 years.Very old or very elderly—a term to describe those over 85 years of age.Frail elderly—Frail elderly are limited in their activities of daily living due to physical, mental,
psychological and/or social impairments as well as recurrent disease. They suffer from multiple pathologieswhich seriously impair their independence. They are therefore in particular need of help and/or care and arevulnerable to complications.
Reduced capacity for rehabilitation—This means that the older the patient, the more difficult it is torehabilitate that patient back to normal or to his/her previous state. Specifically, the restoration ofmuscle mass after illness requires much greater effort in terms of exercise and nutrition in the elderlycompared with the younger patient. It is also implicit that other functions, including mental, are similarlymore resistant to rehabilitation.
Functional status—This term is being used in a general sense to describe global function, e.g. the abilityto perform activities of daily living (ADL), or specific function, e.g. muscle strength or immune function.
Introduction
The risk of undernutrition is increased in elderlypatients due to their decreased lean body mass andto many other factors that may compromisenutrient and fluid intake. Consequently, an ade-quate intake of energy, protein and micronutrients
has to be ensured in each patient independently ofhis/her previous nutritional status. Since restorationof body cell mass (BCM) is more difficult than inyounger persons, preventive nutritional support hasto be considered.Nutritional care should be integrated appropri-
ately into the overall care plan, which takes into

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 333
account all aspects of the patient, personal, social,physical and psychological. A complete assessment ofthe patient should include that of nutritional status orrisk, followed by a nutritional programme reflectingethical as well as clinical considerations. In designingthe programme, it should be remembered that themajority of sick elderly patients require at least 1 gprotein/kg/day and around 30kcal/kg/day of energy,depending on their activity. Many elderly people alsosuffer from specific micronutrient deficiencies, whichshould be corrected by supplementation.
Oral nutritional therapy via assisted feeding anddietary supplements is often difficult, time-con-suming and demanding in elderly patients (due tomultimorbidity and slow responses). However,assisted oral feeding and supplements are able tosupport the physical and psychological rehabilita-tion of most elderly patients. Therefore, even intimes of declining financial and human resources, itis unacceptable to initiate tube feeding (TF) merelyin order to facilitate care or save time.
Decision making concerning TF in the elderly isoften difficult, and in many cases ethical questionsarise (see Guidelines ‘‘Ethical and legal aspectsin enteral nutrition’’). In each case, the followingquestions should be asked:
�
Does the patient suffer from a condition that islikely to benefit from enteral nutrition (EN)? � Will nutritional support improve outcome and/oraccelerate recovery?
� Does the patient suffer from an incurabledisease, but one in which quality of life andwellbeing can be maintained or improved by EN?
� Does the anticipated benefit outweigh thepotential risks?
� Does EN accord with the expressed or presumedwill of the patient, or in the case of incompetentpatients, of his/her legal representative?
� Are there sufficient resources available to manageEN properly? If long-term EN implies a differentliving situation (e.g. institution vs. home), will thechange benefit the patient overall?
Sedation of the patient for acceptance of thenutritional treatment is not justified.
The present guidelines are based on studies inelderly subjects or in those in whom the averageage of the study participants is 65 years or more.
1. What are the aims of EN therapy ingeriatrics?
�
Provision of sufficient amounts of energy,protein and micronutrients.�
Maintenance or improvement of nutritionalstatus. � Maintenance or improvement of function,activity and capacity for rehabilitation.
� Maintenance or improvement of quality oflife.
� Reduction in morbidity and mortality.Therapeutic aims for geriatric patients do notgenerally differ from those in younger patientsexcept in emphasis. While reducing morbidity andmortality is a priority in younger patients, ingeriatric patients maintenance of function andquality of life is often the most important aim.Considering the reduced adaptive and regenerativecapacity of the elderly, EN may be indicated earlierand for longer periods than in younger patients.
1.1. Can EN improve energy and nutrient intakein geriatric patients?
EN (oral nutritional supplement (ONS) and/or TF)increases energy and nutrient intake in geriatricpatients (Ia). Percutaneous endoscopic gastro-stomy (PEG) feeding is superior to nasogastricfeeding in this respect (Ia).
Comment: In a recent Cochrane analysis, ONS ledto an increase in energy and nutrient intake in 29out of the 33 analysed trials which had reportedintake. In three studies no difference in total intakewas found, since patients reduced their voluntaryfood consumption1 (Ia). The success of ONS issometimes limited by poor compliance due to lowpalatability, side effects such as nausea anddiarrhoea, and by cost.2–10 Variety and alterationin taste (different flavours, temperature andconsistency), encouragement and support by staff,as well as administration between the meals (andnot at meal times) are all important in order toachieve increased energy and nutrient intake.
Randomised controlled trials of TF in patientswith neurological dysphagia that compared naso-gastric (NG) with PEG feeding have shown that93–100% of the prescription was administered viathe PEG, versus 55–70% via a NG tube.11,12 In threestudies with supplemental overnight NG TF, be-tween 1000 and 1500 kcal were administered pernight in addition to daily food intake. Total energyand nutrient intake was, therefore, markedlyimproved.13–15
1.2. Can EN maintain or improve the nutritionalstatus of elderly patients?
ONS can maintain or improve nutritional status(Ia). Several studies have shown that TF also

ARTICLE IN PRESS
D. Volkert et al.334
maintains or improves nutritional paramentersirrespective of the underlying diagnosis. Themetabolic consequences of ageing which can leadto sarcopenia and a severely reduced nutritionalstatus at the time of tube placement can impair oreven prevent successful nutritional therapy (III).
Comment: The administration of ONS has beenreported to have positive effects on nutritionalstatus irrespective of the main diagnosis. Weightloss, during acute illness and hospitalisation, can beprevented by the provision of food of high energyand protein density, combined with between mealsnacks, and by the use of ONS, when normal intakeis insufficient. Sometimes weight gain can even beachieved. Milne et al.1 analysed the percentageweight change in 34 randomised controlled trialswith 2484 elderly patients and showed a meanweight increase of 2.3% (pooled weighted meandifference; 95% confidence interval (CI) 1.9–2.7%)1
(Ia). Changes to anthropometric parameters areless consistent, but may reflect improvement ofnutritional status in general1 (Ia). Effects on bodycomposition have only occasionally been investi-gated. Increases in fat-free mass (FFM) (Ib)16,17
(IIa)18 and BCM (Ib)19 in supplemented patientshave been reported by some investigators whereasothers could not detect any change (Ib)20–22 (IIa)23.
Several observational studies exploring the ef-fect of TF in multimorbid geriatric patients haveshown improvements in nutritional status, e.g.maintenance of body weight24–27 (III) and eithermaintenance25,27 (III) or increase in albuminlevels24,26,28 (III). It should be emphasised, how-ever, that changes in albumin more usually reflectchanges in disease rather than nutritional sta-tus.29,30 In two studies of frail, mainly dementednursing home residents, weight gain has beenreported.31,32 Improvements in nutritional statushave also been described in patients with neurolo-gical dysphagia, in whom PEG feeding provedsuperior to nasogastric feeding (NGT)11,12 (Ib).The effects of nocturnal TF supplementary to dailyfood intake in elderly patients with hip fracture orfractured neck of femur, are inconsistent.13–15
Bastow et al.13 have reported the greatest benefitin undernourished patients (Compare 2.4).
The effectiveness of TF on nutritional status maybe limited by compliance with the tubes, and byside effects. The nutritional status of the frailelderly is often very reduced at the time of tubeplacement,24–26,33–38 and is accompanied by sarco-penia which is more difficult to reverse in the oldcompared with the young.39–41 Resistance training,if tolerated, may add to the effectiveness ofnutritional support.9,42 Many tube fed patients are
bedridden, and consequent immobility furtherenhances muscle wasting and prevents gain in leanmass. Weighing is also problematic in thesepatients.
1.3. Does EN maintain or improve functionalstatus or rehabilitative capacity?
Adequate nutrition is a prerequisite for anyfunctional improvement, although studies aretoo few and diverse to allow a general state-ment. Some studies have been positive and somenegative in this respect.
Comment: Available data concerning the effect ofONS on the functional capacity of elderly patientsare inconsistent, although several studies reportfunctional improvements. Thus, Gray-Donald et al.7
(Ib), observed a significantly lower frequency offalls in supplemented free-living frail elderlycompared with non-supplemented and Unossonet al.43 (Ib) describe a higher activity level inlong-term care residents after 8 weeks of ONS.Improvements in the ability to perform basicactivities of daily living (ADL) are reported in agroup of female patients after hip fracture byTidermark et al.44 (Ib), in a subgroup of severelyundernourished geriatric patients by Potter45 (Ib)and in a subgroup of patients with good acceptanceof a 6 months supplementation by Volkert et al.2
(Ib). Woo et al.46 (Ib) describe a significantlyimproved ADL status in patients during recoveryfrom chest infection after 3-months interventioncompared with the control group. Several studies,however, detected no difference between inter-vention and control groups with respect to inde-pendence in ADL (Ib)19,20,47–49 (IIa)6,50. Mobility wasalso unchanged in several studies (Ib)3,43,47 (IIa)6.Similarly, hand grip strength was unaltered in moststudies (Ib)3,6,7,17,21,51–53 (IIa)18 but this may be oflimited relevance as it only tests muscle function ofthe upper body. One randomised trial54 (IIa) as wellas two non-randomised23,55 and one uncontrolledtrial56 (IIb) report an improved hand grip strength insupplemented patients. In four trials, the effectson mental capacity were assessed and again nochanges were observed (Ib)20,43,52 (IIa)50.
At the time of tube placement, geriatric patientsare often in a significantly compromised generalcondition as well as severely functionally im-paired.24,27,36,57–59 Trials in nursing homes alsodescribe a high degree of frailty and dependencein PEG-fed residents32,36,60–63 (III).
Apart from the fractured femur studies withsupplementary overnight TF (Compare 2.4) onlya few, uncontrolled trials have reported theeffects of TF on either functional status or

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 335
rehabilitative capacity in other groups of elderlypatients.24,33,36,64,65 Callahan et al.24 evaluated 72PEG-fed patients with severe physical and mentalimpairments before and after PEG placement usingseveral ADL scales. Improvements in functionalstatus were only rarely observed (improvement ofinstrumental activities of daily living (IADL) in 6%,ADL 10%, upper body functions 18%, lower bodyfunctions 29%) (IIb). Kaw and Sekas,36 using theFunctional Independence Measure Scale (FIM), alsofailed to show significant improvements after 18months in functional status in tube-fed nursinghome residents who were in reduced generalcondition (52% demented, 48% completely ADLdependent) (III). Weaver et al.65 used a Quality ofLife Scale adapted from Spitzer, in which orienta-tion, communicative capacity, ability to self-care,and continence were assessed. In a mixed popula-tion of PEG-fed patients (median age 76 years), nosignificant change was detected after long-termEN. Relatives of the patients with the lowest valueon the scale tended to answer ‘‘no’’ to the questionwhether they would wish TF in a similar situationfor themselves (IIb). Nair et al.33 observed nochanges in function measured by the KarnovskyPerformance Scale after 6 months of PEG feeding in31 surviving patients aged 8478 years (IIa). OnlySanders et al.64 describe an improvement in ADL in25 stroke patients (mean age 80 years) with EN viaPEG. At the time of PEG placement 84% of thepatients had a Barthel index (0–100 points) of 0points (completely dependent; mean 0.5 points).After 6 months of EN a mean increase of 4.8 pointswas observed. Six patients (24%) showed a clearimprovement (Barthel index increase from 0.5 to 9points), in 10 patients (40%), however, no or only aminimal improvement was observed (IIa).
1.4. Does EN reduce length of hospital stay?
In geriatric patients, length of hospital stay isdetermined not only by nutritional status butalso by other factors. Available results concern-ing the effect of EN on length of hospital stay areconflicting.
Comment: Undernutrition increases the risk ofcomplications thereby increasing the length ofhospital stay in geriatric patients.66–69 Consequently,improvement in nutritional status using EN shouldresult in a reduced length of hospital stay. In geriatricpatients, however, length of hospital stay is not onlydetermined by nutritional status but also by otherfactors, e.g. the assurance of adequate care afterdischarge. In addition, in times of declining financialresources, length of hospital stay is only a poorreflection of the effects of EN.
Available study results about the impact of EN onlength of stay are conflicting. In 2002 Milne et al.70
analysed seven studies with 658 participants andreported a statistically significant benefit of ONSwith respect to hospital stay. Mean length of staywas 3.4 days shorter in the supplemented com-pared with the unsupplemented group (95% CI6.1–0.7 days) (Ia). The addition of three new trialsto the meta-analysis, however, shifted the resultsto non-significant effects.1 If patients with hip orfemoral neck fracture are regarded separately,several studies report significantly shorter length ofstay in supplemented patients71–74; this could nothowever be confirmed by others75 (Compare 2.4)
The effects of TF on length of hospital stay haveonly occasionally been measured11,13,15 and requirefurther study.
1.5. Does EN improve quality of life?
The effect of ONS and TF on quality of life isuncertain.
Comment: Although quality of life is crucial in theevaluation of therapeutic benefit in geriatrics, onlya few studies have examined the effect of EN uponit. Studies investigating the effect of ONS haveemployed different parameters, e.g: general well-being, subjective health, SF 36, EQ-5D, HospitalAnxiety and Depression Scale (HADS). Some reportimprovements (IIa)3,54,76, whereas others observeno changes7,22,51 (IIa). These few available data donot allow any firm conclusion about the effects ofONS on quality of life.
In patients requiring TF, impairments of cogni-tion, vigilance and speech can make assessingquality of life difficult. About 60% of the patientsin the trial of Callahan et al.24 were unable tocommunicate at the time of PEG placement, andthe majority of patients with preserved ability tocommunicate were cognitively impaired (IIb). Inthe cohort of 215 patients investigated by Banner-man et al.77 data on quality of life could only begathered in 30 patients (IIb). Verhoef and vanRosendaal78 used semi-structured interviews (witheither patients or their relatives), the KarnovskyPerformance Scale as well as the Quality of LifeIndex, in order to measure subjective quality of lifein patients after PEG placement (mean age 66718years). About 85% of the patients who were stillalive after one year and still fed via PEG (n ¼ 23)were not able to run a household, 67% weredependent in personal care and 19% were feelingvery ill. However, the majority of patients andcaregivers felt that it had been the right decision toagree to the PEG. All 10 patients who were aliveafter one year and could be asked, stated that they

ARTICLE IN PRESS
D. Volkert et al.336
would decide in favour of PEG again. The Karnovskyindex deteriorated in three of these 10 survivingpatients and improved in six (IIb). According to theauthors, these results do not necessarily imply aclear improvement in quality of life.78 Weaver etal.65 evaluated subjective quality of life by inter-view and observed a correlation between subjec-tive and objective quality of life (Compare 1.3).Significant changes in subjective quality of lifewere not detected (IIb). Abitbol et al.26 used both abehaviour scale and a depression scale in order toassess quality of life in 59 institutionalised patients(mean age 85 years) who received EN via a PEG.The patients were bedridden, their health statuswas reduced, and infections were present in 25%.After 3 months of EN via a PEG, quality of lifescores were unchanged, although the depressionscale tended to improve. However, 16 of thesurviving patients (27%) resumed full oral nutritionand six patients (10%), returned to their own homewith a functioning PEG tube (IIb). In a cohort of 38long-term home EN patients, quality of life waspoorer in elderly than in younger patients.79
All in all, these studies do not allow for anygeneral conclusions about effects of EN on qualityof life. TF may also have side effects that mayadversely affect quality of life, e.g. gastrointest-inal symptoms, aspiration, the discomfort of thetube, or the need to use restraints.
1.6. Does EN improve survival in geriatricpatients?
ONS improve average survival (Ia). In patientswho need TF due to the severity of disease, anincrease in survival is not proven.
Comment: Meta-analysis of the data from 32randomised controlled trials with 3017 partici-pants revealed a lower mortality risk in supple-mented elderly subjects than in controls (relativerisk (RR) 0.74; 95% CI 0.59–0.92)1 (Ia). Participantswere supplemented for at least 1 week andobserved for at least 2 weeks. A further meta-analysis from 12 randomised controlled trials(n ¼ 1146) and five non-randomised studies on theeffect of ONS in hospitalised geriatric patients withmixed diagnoses reached similar conclusions (RR0.58; 95% CI 0.4–0.83)80 (Ia). In contrast, a meta-analysis from five studies on the effect of proteinand energy supplementation, mainly in hip fracturepatients, showed no effect on mortality risk.75
Studies on supplementary overnight TF in hipfracture patients have produced similar results(Compare 2.4).
The effect of TF on the survival of elderlypatients without a hip fracture was investigated
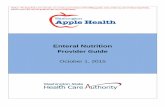
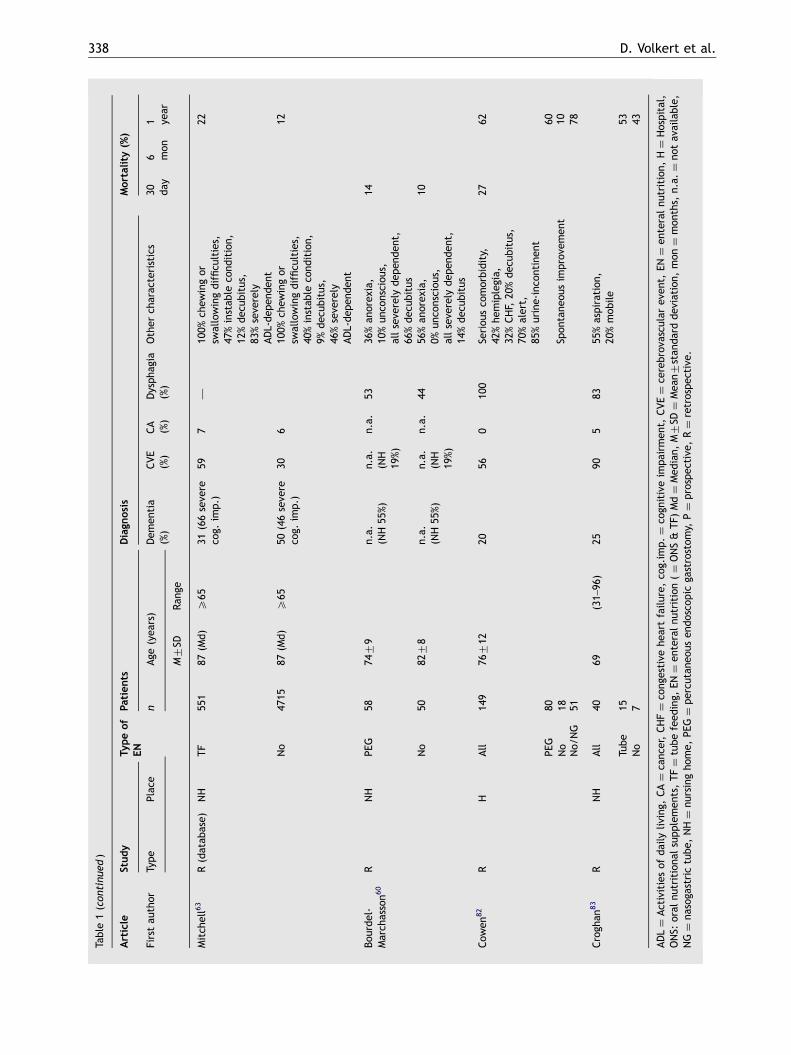
in nine non-randomised controlled studies (non-randomised for ethical reasons) (Table 1) and sev-eral uncontrolled observational studies (Table 2).
Four of the controlled studies were carried out inhospitals,33,81,82,84 five in nursing homes.60–63,83
Two of the studies were prospective,33,81 and theothers were retrospective comparisons of EN vs. noEN. In five studies, participants with advanceddementia were investigated.33,61,62,81,84 The mostrecent of these studies was retrospective anddescribes a mean survival of 59 and 60 days in 23severely demented dysphagic patients with PEGand in 18 patients without PEG.84 A databaseanalysis from Mitchell et al.62 in 1386 nursing homeresidents with severe cognitive impairment—where 135 were enterally fed—showed no increasein survival (III). Mortality rate after one year wassurprisingly low (15%). Meier et al.81 prospectivelystudied 99 acutely ill patients with advanceddementia, seventeen of whom were already beingfed by PEG at the time of hospital admission, 51had a PEG inserted in hospital, and the remaining31 consumed regular food orally. Half of all patientsdied during the following 6 months irrespective ofthe nutritional regimen. Nair et al.33 observed ahigher mortality rate in 55 severely dementedpatients with PEG after 6 months compared with acontrol group without a PEG (44% vs. 26%).According to the authors, the groups were com-parable regarding age, gender and comorbidity.PEG patients, however, suffered more often fromsevere hypoalbuminaemia (mean albumin con-centration 28.675 vs. 33.274 g/l in the controlgroup) suggesting more severe underlying inflam-matory disease. The only trial that detecteda significantly reduced mortality in nursing homeresidents with severe cognitive impairment isthe data base analysis from Rudberg et al.61
After 30 days, 15% had died in the group ofenterally fed patients compared with 30% in thecontrol group. After 1 year, the difference wasless distinct, but still statistically significant (50%vs. 61%). The control group was comparableregarding dementia, comorbidity, functional statusand BMI (III).
Two further non-randomised controlled studies innursing home patients with various diagnoses and alow percentage of demented patients also failed toshow prolonged survival in the enterally fedpatients.60,63 In the databank analysis from Mitchellet al.63 mortality in 551 tube-fed nursing homeresidents with chewing and swallowing difficultieswas even higher than in 4715 residents withoutnutritional therapy (III). Approximately half of theparticipants showed severe cognitive impairments(66% of tube-fed patients vs. 46% of the control

ARTICLE IN PRESS
Table
1Mortality
intube-fedelderly
subjects(con
trolled,no
n-rand
omised
stud
ies).
Article
Study
Typeof
EN
Patients
Diagn
osis
Mortality(%
)
Firstau
thor
Type
Place
nAge
(yea
rs)
Dem
entia
(%)
CVE
(%)
CA
(%)
Dyspha
gia
(%)
Other
charac
teristics
306
1
M7SD
Ran
geday
mon
year
Mitch
ell62
R(datab
ase)
NH
TF
135
87(M
d)(65–
107)
100seve
re47
6—
63%instab
leco
ndition,
30%dec
ubitus,
33%seve
reADL-de
pen
den
t,84
%ch
ewingor
swallowingproblems
o5
ca.15
No
1251
87(M
d)(65–
107)
100seve
re27
7—
52%instab
leco
ndition,
15%dec
ubitus,
45%seve
reADL-
dep
ende
nt,
61%ch
ewingor
swallowingproblems
o5
ca.15
Meier
81
PH
68PEG
,31
no99
84.8
(63–
100)
100ad
vanc
ed0
0—
Allac
utelyill,
56%dec
ubitus,
62%infections
ca.20
5065
Nair3
3P
HPEG
5583
710
100ad
vanc
ed0
0—
NoCA,CVE,
seve
redisea
se,EN
due
tolow
oral
intake
44
No
3380
78
100ad
vanc
ed0
0—
NoCA,CVE,
seve
redisea
se26
Rud
berg6
1R(datab
ase)
NH
NG
353
8577
X65
93co
g.im
p.
(63seve
re)
——
100
100%
dyspha
gia&
eating
dep
ende
nce,
96%dep
ende
ntin
6ADL
1550
No
1192
8677
X65
93co
g.im
p.
(64seve
re)
——
100
100%
dyspha
gia&
eating
dep
ende
nce,
96%dep
ende
ntin
6ADL
3061
ESPEN Guidelines on Enteral Nutrition 337
ARTICLE IN PRESS
Table
1(con
tinu
ed)
Article
Study
Typeof
EN
Patients
Diagn
osis
Mortality(%
)
Firstau
thor
Type
Place
nAge
(yea
rs)
Dem
entia
(%)
CVE
(%)
CA
(%)
Dysph
agia
(%)
Other
charac
teristics
306
1
M7SD
Ran
geday
mon
year
Mitch
ell63
R(datab
ase)
NH
TF
551
87(M
d)
X65
31(66seve
reco
g.im
p.)
597
—10
0%ch
ewingor
swallowingdifficu
lties,
47%instab
leco
ndition,
12%dec
ubitus,
83%seve
rely
ADL-dep
ende
nt
22
No
4715
87(M
d)
X65
50(46seve
reco
g.im
p.)
306
100%
chew
ingor
swallowingdifficu
lties,
40%instab
leco
ndition,
9%dec
ubitus,
46%seve
rely
ADL-dep
ende
nt
12
Bou
rdel-
March
asson6
0R
NH
PEG
5874
79
n.a.
(NH55
%)
n.a.
(NH
19%)
n.a.
5336
%an
orex
ia,
10%un
consciou
s,allseve
rely
dep
enden
t,66
%dec
ubitus
14
No
5082
78
n.a.
(NH55
%)
n.a.
(NH
19%)
n.a.
4456
%an
orex
ia,
0%un
consciou
s,allseve
rely
dep
enden
t,14
%dec
ubitus
10
Cow
en82
RH
All
149
76712
2056
010
0Se
riou
sco
morbidity,
42%he
miplegia,
32%CHF,
20%dec
ubitus,
70%alert,
85%urine-inco
ntinen
t
2762
PEG
8060
Spon
tane
ousim
prove
men
t10
No
1878
No/
NG
51
Crogh
an83
RNH
All
4069
(31–
96)
2590
583
55%aspiration,
20%mob
ile
Tube
1553
No
743
ADL¼
Activitiesof
daily
living
,CA¼
canc
er,CHF¼
cong
estive
heartfailure,
cog.im
p.¼
cogn
itiveim
pairm
ent,
CVE¼
cerebrova
scular
even
t,EN¼
enteralnu
trition,
H¼
Hospital,
ONS:
oral
nutritiona
lsupplem
ents,TF¼
tubefeed
ing,
EN¼
enteralnu
trition(¼
ONS&
TF)
Md¼
Med
ian,
M7SD¼
Mea
n7stan
darddev
iation
,mon¼
mon
ths,
n.a.¼
notav
ailable,
NG¼
nasoga
strictube,
NH¼
nursingho
me,
PEG¼
percu
tane
ousen
dosco
pic
gastrostom
y,P¼
prospec
tive
,R¼
retrospe
ctive.
D. Volkert et al.338

ARTICLE IN PRESS
Table
2Mortality
intube-fedelderly
subjects(observationa
lstud
ieswitho
utco
ntrolgrou
p).
Article
Study
type
Typeof
EN
Patients
Diagn
osis
Mortality
Firstau
thor
nAge
(yr)
(Ran
ge)
Dem
entia
CVE
CA
Dyspha
gia
Other
charac
teristics
30day
3mon
6mon
1ye
arM7SD
(%)
(%)
(%)
(%)
(%)
(%)
(%)
(%)
Nursing
homeresiden
tsGolden
32
RPEG
102
8976
(71–
104)
89seve
re20
010
0Pe
rsistent
dyspha
gia,
low
intake
,75
%co
mpl.
ADL-dep
enden
t,stab
leco
ndition,
noterm
inal
stag
e,LE
atleast1mon
1224
38
Abuk
sis5
7R
PEG
4784
711
(44–
100)
8749
0—
94%desoriented
,96
%bed
ridden
4Kaw
36
RPEG
4674
(19–
96)
5224
7—
48%co
mpletely
ADL-
dep
enden
t,on
ly4%
could
dec
idein
favo
urof
PEG
them
selves,poo
rge
neral
cond
ition
2050
70%470
Geriatric
patien
ts(all465yr
ormea
nage
465yr)
Lind
eman
n85
PPEG
3683
(X65
)10
00
011
84%low
intake
(53%
chron,
31%ac
ute),
6%beh
avioural
disorder
2542
Sand
ers5
9R
PEG
103
77—
100
00
100
allseve
rely
ADL-dep
enden
t(BI0-5P)
5478
8190
Dwolatzky8
6P
PEG
3285
76
(X65
)84
533
2872
%refusalto
eat
545
NG
9082
79
(X65
)68
432
3763
%refusalto
eat
2080
Abuk
sis5
7R
PEG
6780
716
(26–
103)
5230
1031
79%bed
ridden
,11
%un
consciou
s29
Paillaud
35
RPEG
7383
79
(X65
)45
—4
4549
%an
orex
ia,30
%infection
44%reduc
edmob
ility,
44%dec
ubitus
3252
63
Fay2
7R
PEG
8070
.2—
3252
2379
31%dec
ubitus,
91%in
need
ofassistan
cein
ADL,
76%faec
al-,
90%urine-inco
ntinen
t
1755
70
NG
2969
.8—
1341
2841
21%dec
ubitus,
86%in
need
ofassistan
cein
ADL,
66%faec
al-,
82%urine-inco
ntinen
t
2845
70
Callaha
n24
PPEG
9979
79
(60–
98)
3541
13—
35%ne
uro-deg
enerative
disorder,seve
rephy
sica
lan
dmen
talim
pairm
ent
2250
Cioco
n25
PNG
7082
(65–
95)
34—
—47
50%refusalto
eat,
3%oe
sopha
gus-ob
struction,
multiple
&ad
vanc
eddisea
se
541
Quill87
RNG/G
554
70(X
70)
3149
27—
69%inco
mpeten
tAbitbol
26
PPEG
5983
77
50%485
30—
242
31%MNwitho
utdys,
25%refusalto
eat
54%dec
ubitus,49
%pulmon
ary
infection
25
Bussone
88
RPEG
155
84(70–
98)
24—
3—
35%ne
urol,
38%dep
ression
16
Bussone
89
PPEG
101
83.6
(70–
98)
2236
4—
38%dep
ression
14Markgraf9
0R/P
PEG
5487
(65–
94)
——
24—
72%ne
urol,multimorbid
33Rah
a91
?PEG
161
79(53–
99)
—81
—88
12%MN
2039
Finu
cane
92
PPEG
2882
(68–
99)
—93
—10
07%
Parkinson;
NG-intoleran
t8
ESPEN Guidelines on Enteral Nutrition 339

ARTICLE IN PRESS
Table
2(con
tinu
ed)
Article
Study
type
Typeof
EN
Patients
Diagn
osis
Mortality
Firstau
thor
nAge
(yr)
(Ran
ge)
Dem
entia
CVE
CA
Dyspha
gia
Other
charac
teristics
30day
3mon
6mon
1ye
arM7SD
(%)
(%)
(%)
(%)
(%)
(%)
(%)
(%)
James
93
RPEG
126
80(M
d)
(53–
94)
—10
0—
100
aspirationrisk
2338
4653
Wan
klyn
94
RPEG
3774
(48–
89)
—10
0—
—92
%he
miplegia
68Wijdicks
95
RPEG
6374
(Md)
(41–
98)
0 adva
nced
100
0—
noterm
inal
stag
es;
63%he
miplegia,
21%ap
hasia,
35%reduc
edco
nsciou
sness
14 (2wks)
Mixed
coho
rtswithhigh
perce
ntage
ofelderly
Clarkston
96
RPEG
4271
.4(33–
99)
——
24—
67%ne
urol,9%
MN
2648
Frieden
berg9
7P
PEG
6476
(39–
97)
——
20—
80%seve
rene
urol.dysfunc
tion
,38
%respiratoryproblems,
seve
reco
gnitiveim
pairm
ent
33
Horton98
RPEG
224
75(20–
103)
670
15—
—8
Kohli99
RPEG
100
82(47–
102)
4—
238
48%MN
16La
rson
100
RPEG
314
n.a.
(3–92
)—
—1
—75
%ne
urol,
13%orop
haryng
eal
1666
%460
Ligh
t101
RPEG
416
75(18–
103)
1130
9—
19%MN;-
23Llan
eza1
02
RPEG
7367
(30–
96)
——
19—
34%ne
urol,18
%AP
26Markgraf1
03
RPEG
8469
714
(35–
98)
——
39—
59%ne
urol,polym
orbid
3165
%X65
Nicho
lson
104
RPEG
168
70(16–
96)
—58
—18
15%ne
urol,9%
obstruction
9.5
Rab
enec
k105
RPEG
7368
68.1
(18–
102)
—19
30—
29%ne
urol
5926
%475
Rim
on106
PPEG
339
71.3
(14–
96)
——
11—
82%ne
urol
19.5
Sali107
RPEG
3275
(38–
88)
—53
1310
016
%pseud
obulbar
paralysis
16Sand
ers5
9R
PEG
361
68.5
—29
3318
100
20%misce
llan
eous
diagn
oses
2844
5263
Skelly
58
PPEG
7469
(Md)
(28–
90)
—42
2623
%ch
ron.
neurol;
seve
refunc
tion
ally
impaired
(38%
BI0,
Md1point)
1935
42
Stua
rt108
RPEG
4870
(Md)
——
—17
—66
%ne
urol,13
%COPD
31Stua
rt108
Rop
.G.
5565
(Md)
——
—29
—64
%ne
urol,7%
COPD
24Tan1
09
RPEG
4465
(14–
94)
—39
3610
059
%ne
urol,7%
Parkinson
Taylor
110
RPEG
9776
.5(o
1–97
)—
555
25%othe
rCNS-disea
ses,
55%im
pairedvigilanc
e,87
%assistan
cein
toilet
&tran
sfer
2253
Wolfsen
111
R/P
PEG
/PEJ
201
66716
(X18
)—
—36
—64
%ben
igndisea
se,
esp.ne
urol
50
Hom
een
tera
lnu
tritionpatien
tsElia
112
BANS
HEN
1230
—(65–
75)
—10
0—
41%bed
ridden
,31
%ho
use-bou
nd25
2970
—(X
75)
—10
0—
47%bed
ridden
,30
%ho
use-bou
nd36
How
ard113
RHEN
787
7978
(X65
)10
0ne
urom
uscu
lardyspha
gia
53Sand
ers1
14
PPEG
8774
(35–
88)
——
—PEG
-com
plica
tion
sat
home
17Schn
eider
115
PHEN
5486
(Md)
(60–
101)
100
00
010
0%low
intake
4680
148
75(M
d)
(1–97
)0
57
097
3%low
intake
(asindication),
20%ALS
1759
6465
(Md)
(40–
92)
00
100
100
0%low
intake
(asindication)
1263
3275
(Md)
(1–94
)0
00
010
0%low
intake
due
todep
ressionor
disea
serelated
stress
1944
ADL¼
activities
ofdaily
living
,ALS¼
amyo
trop
hic
lateral
sclerosis,
AP¼
aspiration
pne
umon
ia,
BANS¼
British
Artificial
Nutrition
Survey,
BI¼
Barthel
Index
,CA¼
canc
er,
chron¼
chronic,
compl.¼
completely,COPD¼
chronicob
structive
pulmon
arydisea
se,CVE¼
cerebrova
scular
even
t,Dys¼
Dyspha
gia,
EN¼
enteralnu
trition,
G¼
Gastrostomy,
HEN¼
home
enteralnu
trition,
LE¼
life
expec
tanc
y,Md¼
med
ian,
MN¼
malnu
trition,
M7SD¼
mea
n7stan
dard
dev
iation
,mon¼
mon
ths,
n.a.¼
notav
ailable,NG¼
nasoga
stric
tube,
neurol¼
neurolog
ical,op
.G.¼
operative
gastrostom
y,P¼
prospec
tive
,PEG¼
percu
tane
ousen
dosco
pic
gastrostom
y,PEJ¼
percu
tane
ousen
dosco
pic
jejuno
stom
y,R¼
retrospec
tive
.
D. Volkert et al.340

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 341
group) and 83% and 46%, respectively, wereseverely dependent in basic ADLs. The mortalityrate after one year was comparably low in bothgroups (22% and 12%, respectively). Bourdel-March-asson et al.60 (III) reported in a mixed population of108 severely dependent nursing home residents amortality rate of 14% in the PEG group vs. 10% inthe group without nutritional support. Gastroin-testinal and pulmonary complications were also notsignificantly different. The prevalence of dementiain the nursing home was reported to be 55% and ofstroke 19%. Specific prevalence data for the studygroup, however, are not given.
Two trials in dysphagic patients reach differentconclusions. Croghan et al.83 report no differencein mortality between 15 tube-fed and seven orallyfed nursing home residents suffering from aspira-tion, who underwent videofluoroscopic swallowingevaluation mainly because of stroke. Cowen et al.82
(III) recruited 149 severely ill hospital patients withdysphagia and compared the mortality of threesubgroups after one year: Death had occurred in60% of 80 patients who had received a PEG, in 10%of 18 patients who did not receive a PEG becausetheir clinical situation had improved in hospital,and in 78% of 51 patients who did not receive a PEGfor other reasons (28 had refused EN, 12 had diedbefore PEG placement, one patient was transferredto another hospital and 10 patients were fed via aNGT).
The study by Cowen et al.82 is an example of thedifficulty of all non-randomised controlled studies,i.e. there is a lack of comparability between theintervention and control group. The enterally fedpatients from almost all studies described aboveare probably not comparable with the patients inthe control group. The only exception is the studyfrom Rudberg et al.61 In the studies from Meieret al.81 and Murphy and Lipman84 the groups are notproperly described. In the non-randomised studies,the enterally fed patients obviously differed fromthose patients who did not receive EN—for avariety of reasons. The decision not to use EN isprobably linked to the status of the patients insome respects. Moreover, the heterogeneity ofgeriatric patient populations provides a multitudeof factors which may influence outcome, e.g. maindiagnosis, comorbidity, nutritional status and gen-eral condition, mood, various functional para-meters including cognition, vigilance, self-careability, mobility and continence which are presentat the same time in different combinations and to avarying extent.
Observational studies reporting mortality ofenterally fed elderly subjects focus on mortalityafter 30 days or after 1 year (Table 2). However,
comparisons between studies are generally difficultdue to the heterogeneous populations involved thatare often not properly characterised. In most of thestudies, between 10% and 30% of the participantsdied after 30 days. Lower mortality rates arereported by Abuksis et al.57 and Dwolatzkyet al.86 mainly in the demented elderly, byFinucane et al.92 and Horton et al.98 in geriatricpatients with predominantly cerebrovascularevents, and by Ciocon et al.25 in a mixed populationof elderly patients. Extremely high 30 day mortalityrates of 46% and 54% are described by Schneideret al.115 and Sanders et al.59 in the dementedelderly. One year after initiation of EN, mortalityrates between 15% and 90% are reported (Table 2).The highest as well as the lowest mortality rate isreported in demented patients59,62 (Compare 2.7).
Mitchell et al. who performed a meta-analysis ofseven controlled studies on mortality with orwithout PEG, draw the conclusion that the impactof TF on survival ‘‘is not known because the level ofevidence is limited’’.116 Further studies are neededin groups in whom nutrition may further reasonablybe expected to influence mortality.
2. EN in specific diagnostic groups
2.1. Is EN indicated in patients with under-nutrition?
Undernutrition and risk of undernutrition repre-sent essential and independent indications forEN in geriatric patients. ONS is recommended inorder to increase energy, protein and micronu-trient intake, maintain or improve nutritionalstatus, and improve survival in patients who areundernourished or at risk of undernutrition (A).ONS and/or TF are recommended early inpatients at nutritional risk (e.g. insufficientnutritional intake, unintended weight loss 45%in 3 months or 410% in 6 months, BMIo20 kg/m2) (B).
Comment: Undernutrition in geriatric patients isassociated with poor outcome. Essential signs ofundernutrition in the elderly are unintended weightloss 45% in 3 months or 410% in 6 months as wellas a BMI below 20 kg/m2. Risk of undernutrition isindicated by loss of appetite, reduced oral intakeand stress (physical as well as psychological).
In a Cochrane analysis of 49 studies including4790 randomised elderly patients with manifestundernutrition or risk of undernutrition, positiveeffects of ONS have been shown: there is increasein energy and nutrient intake, maintenance orimprovement of nutritional status and reduction of

ARTICLE IN PRESS
D. Volkert et al.342
mortality risk1 (Ia) (Compare 1.1, 1.2 and 1.6).ONS are, therefore, clearly recommended (A).Effects on functionality and quality of life are,however, uncertain (Compare 1.3 and 1.5).
The effects of TF in undernourished elderlypatients are unclear due to limited data. Veryoften TF is not initiated until advanced under-nutrition has developed, which is a clear impedi-ment to the success of nutritional therapy(Compare 1.2). Results from several studies how-ever, indicate maintenance or improvement ofnutritional parameters in undernourished elderlypatients after TF24–26 (III). Effects on functionalstatus and quality of life are uncertain (Compare1.3 and 1.5).
It is highly recommended to initiate nutritionalsupport, not only in manifest undernutrition, but assoon as there are indications of nutritional risk, andas long as physical activity is possible, EN—
together with rehabilitative exercise—can help tomaintain muscle mass (C). Early routine nutritionalscreening is mandatory. Several tools (e.g. ESPENguidelines,117 MNA118) are available for this pur-pose.
2.2. Is EN indicated in frail elderly?
In frail elderly, ONS are recommended in order toimprove or maintain nutritional status (A).
Frail elderly may benefit from TF as long as theirgeneral condition is stable (not in terminalphases of illness). TF is therefore recommendedearly in case of nutritional risk (B), wherenormal food intake is insufficient.
Comment: Frail elderly are limited in their ADL dueto physical, mental, psychological and/or socialimpairments a well as recurrent disease. Theysuffer from multiple pathology which seriouslyimpairs their independence. Therefore they are inparticular need of help and care and are vulnerableto complications. An inadequate intake of fluidsand nutrients is a common problem in thesesubjects. Frail elderly therefore are at high risk ofundernutrition and its serious consequences. Ex-perience has shown that the ability to eat sufficientamounts orally is inversely associated with theextent of frailty. Decreasing oral intake maytherefore be an indication of the progress orseverity of disease or frailty.
ONS lead to a significant increase in energy andnutrient intake as well as to a stabilisation orimprovement of nutritional status in mixed samplesof multimorbid elderly with acute and/or chronicdiseases, at home as well as in nursing homes andhospitals (Table 3). Effects on functional status andquality of life are uncertain due to limited data.
Effects on length of hospital stay and mortalityhave been investigated only occasionally. Potter etal.127 found a reduced length of hospital stay onlyin a subgroup of patients with adequate initialnutritional status. Data on mortality are contro-versial in frail elderly.8,127
Clinical experience shows that frail elderly, atnutritional risk, may benefit from TF as long as theirgeneral condition is stable. Observational studiesindicate a relatively good prognosis in tube-fed frailelderly nursing home residents with good healthstatus32,57 (III) (Table 2). Although data are scarce,it is recommended that nutritional support beinitiated early, as soon as there are indications ofnutritional risk and as long as physical activity ispossible since EN—together with rehabilitativeexercise—can help to maintain muscle mass (C).Nutritional screening has to be implemented as amatter of routine for early detection of risk ofundernutrition. Several tools (e.g. ESPEN guide-lines,117 MNA118) are available for this purpose.
TF is not recommended in frail elderly who haveprogressed to an irreversible final stage, e.g. withextreme frailty and advanced disease (irreversiblydependent in ADL, immobile, unable to commu-nicate, as well as high risk of death) (IV).
2.3. Is EN indicated in geriatric patients withneurological dysphagia?
In geriatric patients with severe neurologicaldysphagia, EN is recommended in order toensure energy and nutrient supply and, thus, tomaintain or improve nutritional status (A). Forlong-term nutritional support PEG should bepreferred to NGT, since it is associated with lesstreatment failures, better nutritional status (A),and it may also be more convenient for thepatient. In patients with severe neurologicaldysphagia TF has to be initiated as soon aspossible (C). EN should accompany intensiveswallowing therapy until safe and sufficient oralintake from a normal diet is possible (C).
Comment: In neurological dysphagia, nutritionaltherapy depends on the type and extent of theswallowing disorder. Nutritional therapy may rangefrom normal food, to mushy meals (modifiedconsistency), thickened liquids of different consis-tencies or total EN delivered via NGT or PEG.Nutritional therapy and swallowing therapy have tobe closely coordinated. Typical complications ofneurological dysphagia are aspiration with bronch-opulmonary infections136–139 and undernutrition,causing extended length of hospital stay andrecurrent hospitalisations.139–141 Mortality due todysphagia is significantly enhanced.139 Patients

ARTICLE IN PRESS
Table
3Oralsupplemen
tation
inmixed
coho
rtsof
frailelderly.
Article
Study
type
Patients
Supplements
Resu
lts
Firstau
thor
nAge
(yr)
Nutrition
alPlace
Energy
Protein
Duration
Intake
Nutrition
alstatus
Func
tion
alstatus
Qua
lity
oflife
M7SD
(ran
ge)
status
(kca
l/d)
(g/d
)
EProt
Cha
ndra
119
RCT
30(70–
84)
MN
Atho
me
Individ.
n.a.
4wks
n.a.
n.a.
Weigh
t+TSF+
Alb,PA
+im
mun
erespon
se+
n.a.
n.a.
Gray-Don
ald7
RCT
5078
BMI19
73
Atho
me
500–
700
17–26
12wks
(+)
n.a.
Weigh
t+skinfolds¼
AMC,CC¼
Han
dgrip¼
falls+
Well-
being¼
subjective
health¼
(460
)
Paye
tte3
RCT
8380
77
BMI20
73
Atho
me
500–
700
17–26
16wks
+(+)
Weigh
t+skinfolds¼
AMC,CC¼
Han
dgrip¼
mob
ility¼
days
inbed
+
‘‘Em
otiona
lrole
func
tion
ing’’+
(465
)
Volkert2
RCT
4685
MN
Atho
me
250
15.0
6mon
n.a.
n.a.
Weigh
t¼
ADL+
(inco
mplian
tsubgrou
p)
n.a.
(75–
98)
BMI19
72
Woo
46
RCT
8173
BMI20
75
Atho
me
500
17.0
1mon
++
Weigh
t+(m
)fatmass+
FFM+(m)
ADL+
activity+
men
talfunc
tion¼
appetite¼
slee
p+
n.a.
(465
)
Wou
ters
22
RCT
6882
BMI24
72
Nursing
home
250
8.8
6mon
++
weigh
t+
FFM,FM
,CC¼
Alb,PA¼
Han
dgrip¼
ADL¼
mob
ility¼
slee
p+
¼
(X65
)
Wou
ters
120
RCT
5583
BMI24
72
Nursing
home
250
8.8
6mon
n.a.
n.a.
Vit.C,E,
Cysteine+
Antiox.
capac
ity+
n.a.
n.a.
(X65
)
Ban
erjee1
21,122
RCT
6381
n.a.
Nursing
home
265
18.6
14wks
¼+
TSF+
Alb,Trf,
PA¼
%T-Lympho
cytes¼
Com
plemen
tC3¼
Skin
problems+
n.a.
(60–
98)
Bec
k123
RCT
1685
BMI20
(M)
Nursing
home
380
5.0
2mon
¼n.a.
weigh
t¼
n.a.
n.a.
(65–
96)
MNA17
–23
,5
Ek124
RCT
482
8028
.5%MN
Nursing
home
400
16.0
26wks
n.a.
n.a.
Skin
test+
n.a.
n.a.
Fiataron
e20
RCT
5088
71
BMI
25.5
(M)
Nursing
home
360
15.0
10wks
¼n.a.
Weigh
t+FF
M¼
FM(+)
Alb,Fe
,HDL¼
Vit.D,E,
Folate¼
ADL¼
depression¼
men
talfunc
tion¼
n.a.
(470
)
Han
key1
25
RCT
1481
72
weigh
t45
kg,Alb
33g/
L
Nursing
home
680
n.a.
8wks
+n.a.
weigh
t(+)
TSF,AMC
+Album
in¼
n.a.
n.a.
(475
)
ESPEN Guidelines on Enteral Nutrition 343

ARTICLE IN PRESS
Table
3(con
tinu
ed)
Article
Study
type
Patients
Supplements
Resu
lts
Firstau
thor
nAge
(yr)
Nutrition
alPlace
Energy
Protein
Duration
Intake
Nutrition
alstatus
Func
tion
alstatus
Qua
lity
oflife
M7SD
(ran
ge)
status
(kca
l/d)
(g/d
)
EProt
Larsson8
RCT
435
8029
%MN
Nursing
home
400
16.0
26wks
n.a.
n.a.
n.a.
n.a.
Lauq
ue53
RCT
3585
BMI22
71
Nursing
home
300–
500
20–30
60day
s+
+Weigh
t+Han
dgrip¼
MNA+
n.a.
(465
)MNA
17-23.5
Uno
sson
43
RCT
430
8026
%MN
Nursing
home
400
16.0
26wks
n.a.
n.a.
n.a.
Activity+
,mob
ility¼
men
talfunc
tion¼
gene
ralwell-being¼
n.a.
Hub
sch1
9RCT
7286
MN
Hospital
500
30.0
3wks
++
Weigh
t¼
FFM¼
BCM+
Alb,Trf,
RBP¼
Vit.B1,
C+
ADL(+)
n.a.
(75–
99)
McE
voy1
26
RCT
51n.a.
MN
Hospital
644
36.4
4wks
n.a.
n.a.
Weigh
t+TSF+,
AMC¼
Alb¼
n.a.
n.a.
Potter
127
RCT
381
83(M
d)
Non
-obese
hospital
540
22.5
Hospital
(Md17
day
s)+
n.a.
Weigh
t+AMC(+)
ADL+
(MN)
n.a.
(61–
99)
Bun
ker1
28
NRT
5880
BMI
24.4
(M);
Atho
me
200(in
under-
weigh
tpatients
300)
20.0
12wks
n.a.
n.a.
Alb,PA¼
,RBP+
Fe,Zn
,Se
+lympho
cyte-pop
ulations¼
skin
test
(+)
n.a.
n.a.
(70–
85)
19%o20
Ced
erho
lm55
NRT
2374
71
MN
Atho
me
400
40.0
3mon
n.a.
n.a.
Weigh
t+TSF,
AMC+
Alb,Orosomuc
oid¼
skin
test+
Han
dgrip+
pea
kflow¼
n.a.
BMI17
(M)
Bos
18
NRT
2379
MN
Hospital
400
30.0
10day
s+
+Weigh
t+FF
M+
Alb,Trf,
PA¼
CRP,
IGF-I¼
Immun
glob
ulin¼
Com
plemen
tC3¼
Han
dgrip
(+)
n.a.
(69–
90)
BMI
2173
Bou
rdel-M
.129
NRT
672
83Alb
3275
Hospital
400
30.0
15day
s+
+n.a.
Dec
ubitus
(+)
n.a.
(465
)
D. Volkert et al.344

ARTICLE IN PRESS
Cha
ndra
130
UCT
21460
MN
Atho
me
500
17.5
8wks
n.a.
n.a.
Alb,PA
,Trf,
RBP+
Zn+,
Ferritin¼
skin
test+
lympho
cyte
pop
ulations+
n.a.
n.a.
Gray-Don
ald131
UCT
1479
76
MN
Atho
me
500
KA
12wks
++
Alb
(+),
RBP,
Hb¼
lympho
cyte
coun
t+
Han
dgrip¼
Well-
being
+(4
60)
Lipschitz
132
UCT
1275
‘‘Highrisk’’
Atho
me
1050
39.0
16wks
++
Weigh
t+Alb,TIBC,Vit.+
Hb,metals¼
lympho
cyte
coun
t¼
skin
test¼
n.a.
n.a.
Harrill133
UCT
1889
(Md)
n.a.
Nursing
home
355
13,0
30day
s(+)
(+)
Vit.A,C,B1,
B2+
Alb,Hb,Ht,
Fe¼
n.a.
n.a.
Welch
134
UCT
1581
Alb
32g/
LNursing
home
n.a.
n.a.
6mon
++
Weigh
t+Alb,Hb,Ht+
Fe,TIBC,Trf¼
Dec
ubitus+
n.a.
Bou
rdel-M
.23
UCT
1187
MN
Hospital
400
30.0
4wks
¼¼
Weigh
t+musclemass¼
Alb+
Han
dgrip+
n.a.
BMI18
73
Joosten1
35
UCT
5083
76
BMI24
.574
Hospital
600
19.0
1376day
s+
n.a.
n.a.
n.a.
n.a.
Alb
3676g/
L
Katak
ity5
6UCT
12(71–
84)
n.a.
n.a.
204
9.0
12wks
n.a.
n.a.
Hb¼
Vit.C,D,B1
Han
dgrip+
men
talfunc
tion¼
dark
adap
tion¼
n.a.
ADL¼
activities
ofdaily
living
,Alb¼
album
in,AMC¼
arm
muscle
circum
ferenc
e,Antiox.¼
antiox
idative,
BCM¼
bod
yce
llmass,
BMI¼
bod
y-massindex
[Kg/
m2],
CC¼
calf
circum
ferenc
e,CRP¼
C-rea
ctiveprotein,E¼
energy,Fe¼
iron
,FF
M¼
fatfree
mass,FM¼
fatmass,Hb¼
hemog
lobin,
Ht¼
hematoc
rit,n.a.¼
notav
ailable,M¼
Mea
n,(m
)¼
male
participan
ts,Md¼
med
ian,
MN¼
malnu
trition,
MNA¼
MiniNutrition
alAssessm
ent,
mon¼
mon
ths,
NRT¼
non-rand
omised
trial,PA¼
prealbum
in,Prot¼
protein,RCT¼rand
omised
controlled
trial,
RBP¼
Retino
lbindingprotein,Re
f.¼
referenc
e,SD¼
stan
darddev
iation
,Se¼
Selen,
TIBC¼
totaliron
bindingca
pac
ity,
TSF¼
Tricep
sskinfold,Trf¼
Tran
sferrin,
UCT¼un
controlled
trial,Vit.¼
vitamin,wks¼
wee
ks,Zn¼
Zinc
.+improv
emen
tin
supplem
entedgrou
p(SG)co
mpared
toco
ntrolgrou
p(CG).
(+)tren
dtowardsim
prove
men
t,no
tsign
ifica
nt;¼
nodifferenc
eSG
–CG.
ESPEN Guidelines on Enteral Nutrition 345

ARTICLE IN PRESS
D. Volkert et al.346
with acute stroke and dysphagia often alreadyexhibit a poor nutritional status on hospital admis-sion, which negatively impacts on outcome andcosts: length of hospital stay is extended, rehabi-litation is delayed and survival is reduced.141–143
These results are confirmed by the current inter-national FOOD study.144
Controlled trials studying the effects of EN afterdysphagic stroke are not available, since controlgroups without nutritional support would be un-ethical. It is common sense, however, that energyand nutrient supply has to be ensured in thesepatients in order to maintain nutritional status andto avoid the development of undernutrition. Due tothe strong physiological plausibility based on thefact that patients with severe neurological dysphy-gia are not able to sustain their life withoutnutritional support, this recommendation wasrated at the highest level.
Nutritional status: In a Cochrane analysis ofinterventions for dysphagia in acute stroke ENdelivered via PEG was associated with a greaterimprovement of nutritional status when comparedto EN delivered via NGT.145 These results are basedon a randomised controlled trial conducted byNorton et al.11 (Ib) in 30 patients and on unpub-lished data from the authors of the Cochraneanalysis from 19 further patients. In anotherrandomised controlled trial in 40 patients withneurological dysphagia (mean age 60 years), thegroup receiving PEG also exhibited weight gain aswell as an increase in mean serum albumin andtransferrin. Due to a high drop out rate noevaluation was undertaken in the NGT group12 (Ib).
Functional status: Sanders et al.64 reported animprovement in ADL in 25 stroke patients (meanage 80 years) with EN via PEG (PEG placement onaverage 14 days after stroke). At the time of PEGplacement Barthel index was 0 points (completelydependent) in 84% of patients (mean 0.5 points).After 6 months of EN a mean increase of 4.8 pointswas observed. Six patients (24%) showed a clearimprovement (Barthel index increase from 0.5 to 9points). In 10 patients (40%), however, no or only aminimal improvement was observed (IIa).
Resuming oral nutrition: Dysphagia may bereversible in stroke patients.146 In various studiesbetween 4% and 29% of patients resumed full oralnutrition after 4–31 months11,92,93,95,112,115 (III)(Table 4). In the British Artificial Nutrition Survey(BANS) no difference between 65- and 75-year oldelderly people and younger adults (16–64 years)was found, although resumption of oral nutritionwas slightly reduced in the elderly above the age of75 years112 (Table 4). Schneider et al.115 report therate of resuming oral nutrition in different diag-
nostic groups of tube-fed patients at home. Among148 neurological patients with dysphagia (mean age75 years), 24% regained the ability to eat sufficientamounts orally within the study period of 2427494days.
Mortality: Clear statements about the effect ofEN on overall mortality after dysphagic stroke arenot possible since the investigated groups are tooheterogeneous, and control groups without nutri-tional support would be unethical (Compare 1.6).In the study of Norton et al.11 mortality after 6weeks was significantly lower in the PEG group thanin the group fed by NGT (12% vs. 57%), due probablyto the lower percentage of the prescribed intakereached in the latter. In the recent multicentreFOOD trial147 no difference in 6-month mortalitywas found between 162 dysphagic stroke patientswith PEG and 159 patients with NGT. However,these results are of limited value since only thosepatients were enrolled in whom the responsibleclinician was uncertain of the best feeding practice.Furthermore the duration of the intervention isunclear and there was a greater delay to first TF inthe PEG group than in the nasogastic group. Becauseof these methodological problems, results of theFOOD trial have to be interpreted with caution.
Timing of tube placement: In patients withsevere neurological dysphagia, TF has to beensured immediately unless there are compellingreasons against it. Studies investigating the role ofearly TF after acute cerebrovascular events in age-mixed samples have shown that early TF is feasiblealso in elderly patients148,149 and has a positiveimpact on survival148 and length of hospital stay144
(III). In a retrospective analysis of stroke patients(19% of patients 465 years) by Nyswonger andHelmchen,149 the group receiving TF within 72 hafter the cerebrovascular event had a reducedhospital stay compared to patients that received TFafter 72 h (III). Taylor148 found that patients, whohad spent less than 5 days without nutrient supply,had a lower mortality than patients who had morethan 5 days without nutrition. Interestingly, thisdifference was statistically significant only inpatients aged 465 years and was less distinct inyounger patients. The authors conclude that olderpatients react more sensitively to food deprivationthan younger patients and that TF should beinitiated as early as possible in this group (III).
In the recent multicentre FOOD trial147 nodifference in outcome was found between dyspha-gic stroke patients who received EN via a PEGwithin 7 days of hospital admission and anothergroup in whom TF was avoided for at least 7 days.Again, these results are of limited value because ofmethodological problems (see above).

ARTICLE IN PRESS
Table
4Re
sumingoral
nutritionafteren
teralnu
tritionin
elderly
patients.
Article
Study
Patients
TypeofEN
Proportion
resu
mingfull
oralnutrition(%
)
Tim
eperiod
Firstau
thor
Type
Place
nAge
(yr)
Prop
ortion
ofelderly
M7SD
(Ran
ge)
Neu
rologicdys
pha
gia
Finu
cane
92
PHospital
2882
(68–
99)
PEG
4%6mon
ths
Elia
112
PAtho
me
2970
—(X
75)
EN10
%12
mon
ths
Elia
112
PAtho
me
1230
—(65–
75)
EN15
%12
mon
ths
Norton1
1P
Hospital
1676
—PEG
19%
6mon
ths
Schn
eider
115
PAtho
me
148
75(M
d)
(1–97
)EN
24%
4mon
ths(M
)Wijdicks
95
RHospital
6374
(Md)
(41–
98)
PEG
28%
2–36
mon
ths
(Md4mon
ths)
James
93
RHospital
126
80(M
d)
(53–
94)
PEG
29%
4–71
mon
ths
Mixed
coho
rts
(Md31
mon
ths)
Quill87
RHospital
55470
(X70
)51
%480
yrNG
4%—
Clarkston
96
RHospital
4271
.4(33–
99)
PEG
7%2mon
ths
Dwolatzky8
6P
Hospital
122
—(X
65)
PEG
/NG
8%3mon
ths
Markg
raf1
03
RHospital
8469
714
(35–
98)
65%X65
yrPEG
12%
14–22
9day
s(M
108day
s)Markg
raf9
0R/P
Hospital
5487
(65–
94)
PEG
13%
14–22
9day
s(M
133day
s)Bussone
88
RHospital
155
84(70–
98)
PEG
14%
—
Larson
100
RHospital
314
—(3
–92
)66
%460
yrPEG
14%
—
Skelly
58
PHospital
7469
(Md)
(28–
90)
PEG
15%
6mon
ths
Tan1
09
RHospital
4465
(14–
94)
PEG
16%
1–44
mon
ths
How
ard113
RAtho
me
887
7978
(X65
)EN
17%
12mon
ths
Nicho
lson
104
RHospital
168
70(M
d)
(16–
96)
PEG
21%
4mon
ths(M
d)
Wolfsen
111
R/P
Hospital
201
66716
—PEG
/PEJ
21%
2757
353day
s(M
d14
4day
s)
Sali107
RHospital
3275
(38–
88)
PEG
22%
2–8mon
ths
Mitch
ell63
RAtho
me
551
87(M
d)
(65–
107)
TF
25%
12mon
ths
Taylor
110
PHospital
9776
.5(o
1–97
)PEG
25%
1day
–7yr
(Md32
7day
s)Abitbol
26
PHospital
5983
77
—50
%485
yrPEG
27%
12mon
ths
Verhoe
f78
PHospital
7166
718
(17–
89)
PEG
28%
12mon
ths
EN¼
enteralnu
trition,
M¼
mea
n,Md¼
Med
ian,
NG¼
nasoga
strictube,
P¼
prospec
tive
,PEG¼
percu
tane
ousen
dosco
pic
gastrostom
y,PEJ¼
percu
tane
ousen
dosco
pic
jejuno
stom
y,R¼
retrospec
tive
,SD¼
stan
darddev
iation
,TF¼
tube
feed
ing,
yr¼
years.
ESPEN Guidelines on Enteral Nutrition 347

ARTICLE IN PRESS
Table
5Su
pplemen
tary
overnigh
ttubefeed
ingin
elderly
frac
ture
patients.
Article
Patients
Supplement
Resu
lts
Firstau
thor
nAge�
(yr)
Diagn
osis
Energy
and
protein/d
ayDuration
Intake
Nutrition
alstatus
Clinica
lco
urse
Bastow13
58CG
80Fe
mur
neck
+100
0kcal
16–39
day
sTotalintake
mAnthrop
ometry
mADL¼
64SG
81frac
ture
&malnu
trition
+28gprot
Md26
day
sFo
odintake¼
Proteins
mLO
Rk
LOSk
Mortality
(k)
Hartgrink
14
67CG
8378
Hip
frac
ture
&risk
ofpressuresores
+150
0kcal
7an
d14
day
s,resp.
mDespitelow
toleranc
eIntend
edto
feed
:Alb,TP¼
Pressure
sores¼
only
40%tolerated
tube41wk
62SG
8477
+60gprot
Actua
llyfed:
Alb
m,TPm
Sullivan
15
10CG
7776
Hip
frac
ture
&go
odnu
tritiona
lstatus
+138
3kcal
1676day
sm
Alb,
tran
sferrin¼
Com
plica
tion
s¼
8SG
7572
+86gprot
ADL¼
LOS¼
In-hospital
mortality¼
6-mon
thsmortalityk
ADL¼
activities
ofdaily
living
,Alb¼
album
in,CG¼
controlgrou
p,LO
R¼
leng
thof
reha
bilitation
,LO
S¼
leng
thof
stay,Md¼
med
ian,
prot¼
protein,SG¼
Supplemen
tedgrou
p,
TP¼
totalprotein,yr¼
years.
mincrea
se,k
dec
rease(orim
prove
men
tin
thesupplmen
tedgrou
pco
mpared
totheco
ntrolgrou
p);¼
nodifferenc
ebetwee
nthegrou
ps.
�Mea
nor
mea
n7stan
dard
dev
iation
.
D. Volkert et al.348

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 349
In earlier studies, long periods of 44–63 daysbetween the acute event and PEG placement arenoticeable.91,93,107 Three studies on the naturalcourse of dysphagia after stroke show that sponta-neous remission of the swallowing difficulty occurs7–14 days after the acute event in 73–86%.150–152
Based on clinical experience, prognosis of dyspha-gia seems to be better in medial cerebral infarctthan in brain stem infarct (IV). If severe dysphagiapersists longer than 14 days after the acute event,a PEG should be placed immediately. Controlledtrials on the ideal timing and length of TF inneurological dysphagia, that also consider thevarying kinds and extents of swallowing disorders,are still not available.
2.4. Is EN indicated after orthopaedic surgery ingeriatric patients?
ONS are recommended in geriatric patients afterhip fracture and orthopaedic surgery in order toreduce complications (A).
Comment: Voluntary oral intake is often insuffi-cient to meet the enhanced requirements ofenergy, protein and micronutrients after orthopae-dic surgery. Rapid deterioration in nutritionalstatus, and impaired recovery and rehabilitationare common.
The results of several randomised studies of ENafter hip fracture are summarised in a Cochraneanalysis75 that includes eight trials testing supple-mentary overnight TF, five trials with ONS and threestudies regarding the effects of supplementary oralprotein. The quality of most of the studies and theavailability of outcome data were considered poorby the authors of the Cochrane analysis.75 Inaddition, a recent randomised controlled study153
and two non-randomised trials with ONS areavailable.4,6,154
Energy and nutrient intake: Administration ofONS leads to a significant increase in energy andnutrient intake.75 However, several trials71,74,155
have shown that the daily requirements for energyand protein are still not met. This may be due topoor compliance of less than 20%,7 to intolerance ofsupplements by some patients,155 and to require-ments being markedly increased.
Supplementary overnight TF enables the admin-istration of larger amounts of enteral formu-lae,13–15 but is of limited tolerance in practice. Inthe trial of Hartgrink et al.14 only 40% tolerated thisintervention longer than 1 week and only one-quarter for the whole study period of 2 weeks.
Nutritional status: Information about the effectsof ONS on nutritional status is sparse and incon-sistent. Delmi et al.71 observed a larger increase in
albumin and transferrin levels in supplementedpatients than in the unsupplemented control group(Ib), whereas Lawson et al.154 and Williams et al.6
detected no difference with respect to serumalbumin (IIa). In the study of Lawson et al.154 BMIand mid-arm muscle circumference (MAMC) werealso unaffected, however transferrin and haemo-globin decreased less than in the unsupplementedgroup. Williams et al.6 reported a positive effect ontriceps skinfold thickness (TSF) and MAMC in thesupplemented group. In contrast Tidermark et al.44
registered weight loss, and Brown and Seabrock74
observed decreases in body weight, mid-armcircumference (MAC) and TSF in the supplementedas well as in the control group.
Positive effects of protein supplementation onbone density and parameters of bone metabolismwere described by Tkatch et al.72 and Schurchet al.73 (Ib). A 6-month administration of protein-enriched supplements led to a significant attenua-tion of loss of bone mineral density when comparedto the control group. Even short-term supplemen-tation (o40 days) was accompanied by a smallerdecrease in proximal femur bone mineral densitythan in the unsupplemented group. However, otherskeletal sites were unaffected. Moreover, proteinrepletion was shown to be associated with anincrease in serum osteocalcin72 and insulin-likegrowth factor-I,73 both of which are importantmediators of bone metabolism.
The effect of supplementary overnight TF onnutritional status of elderly patients with eitherhip or femoral neck fracture was investigated inthree randomised controlled studies13–15 (Ia)(Table 5). Initial nutritional status as well as resultswere inconsistent. Clear improvements were re-ported by Bastow et al.13 who divided theirpatients into ‘‘thin’’ and ‘‘very thin’’ according toanthropometric measurements. In both interven-tion groups (‘‘thin’’ and ‘‘very thin’’), anthropo-metric parameters (body weight, TSF, MAC)and postoperative prealbumin increased during16–39 days. ‘‘Very thin’’ patients had the greatestbenefit from the nutritional therapy. No change inserum albumin was observed in the study ofHartgrink et al.14 in 62 patients intended to receivesupplementary TF. An evaluation of the actuallytube-fed patients however (n ¼ 25 after 1 week,n ¼ 16 after 2 weeks), revealed increased serumconcentrations of albumin and total protein. Noeffects on plasma proteins were reported in thestudy of Sullivan et al.15 who examined patientswith a relatively good nutritional status (BMI24.1 kg/m2, albumin 32 and 35 g/l, respectively),with respect to albumin, transferrin and cholester-ol values.

ARTICLE IN PRESS
D. Volkert et al.350
Length of hospital stay: Data concerning thelength of hospital stay are inconsistent. Delmi etal.71 found a significantly shorter length of hospitalstay (including rehabilitation) in patients receivingONS (median 24 days) compared to control patients(median 40 days) (Ib). Protein administration in thetrials of Tkatch et al.72 and Schurch et al.73 wasalso associated with a significantly reduced lengthof stay (30 and 21 days, respectively). In five otherstudies, however, the observed differences werenot significant.44,75
A positive impact of supplementary overnight TFon the length of hospital stay of geriatric patientsafter hip or femur neck fracture cannot be firmlyconcluded from the data available.13–15
Functional status: Data regarding functionalstatus are heterogeneous and unsatisfactory. TheCochrane analysis of Avenell and Handoll75 refers tofour studies investigating this aspect. Only one ofthem showed positive effects of ONS on ADL-functions after 6 months.44 The non-randomisedtrial of Williams et al.6 showed a trend towardsimproved mobility and greater independence athospital discharge in supplemented patients. Oralsupplementation of calcium, protein and vitaminsin the study of Espaulella et al.47 showed nosignificant changes in mobilisation, ADL status anduse of walking aids when compared to the controlgroup receiving an isocaloric placebo as well.
Bastow et al.13 assessed the time between thepatient0s operation and the achievement of phy-siotherapy goals (e.g. recovering independent mobi-lity). Thin patients (according to anthropometricmeasurements; see above) receiving supplementaryovernight TF, achieved independent mobility in 10days, while thin control patients did so in 12 days.Very thin patients from the intervention groupreached this goal after 16 days whereas very thincontrol patients needed 23 days to regain indepen-dent mobility (Po0:05) (IIa). ADL status at discharge,however, was not affected by the intervention.13
Postoperative complications and mortality: ONShave a positive impact on the rate of postoperativecomplications. Thus, Lawson et al.154 in theirrecent non-randomised study found a significantlylower rate of complications in post-operativelysupplemented orthopaedic patients than in thoseunsupplemented (IIa). In the study of Tkatch etal.72 the complication rate in protein supplementedpatients was significantly lower during hospitalstay, as well as 7 months later, compared to thecontrol group with isocaloric placebo. The pooledanalysis of five randomised studies in the meta-analysis of Avenell and Handoll75 revealed aborderline reduction of the risk of complicationsin supplemented patients (RR 0.61, 95% CI
0.36–1.03). When risks for mortality and complica-tions were combined in these five studies, thechances of an unfavourable outcome were reducedin supplemented patients (RR 0.52, 95% CI0.32–0.84)72 (Ia).
If mortality was considered separately in themeta-analysis of five studies with ONS, no reductionin mortality risk was found.75 The same was true inthe study of Espaulella et al.47 Combining mortalityoutcome of all the studies with supplementaryovernight TF did not produce a significant riskreduction either (RR 0.99; 95% CI 0.5–1.97).75 Thepooled analysis of studies using ONS or overnight TFin geriatric patients with either hip or femoral neckfracture also did not show a significant reduction ofmortality risk in the enterally fed patients whencompared to controls (RR 0.94; 95% CI 0.59–1.50).75
2.5. Is EN indicated in the perioperative phase ofmajor surgery in geriatric patients?
There is no evidence that nutritional therapy inelderly patients undergoing major surgery (e.g.pancreatic surgery, head and neck surgery)should be different from that in younger pa-tients. We therefore refer to the Guidelines.‘‘Surgery and transplantation’’.
It is generally recognised, however, that elderlyare at higher risk of being undernourished thanyounger patients and restoration of BCM is moredifficult. Therefore, preventive nutritional supporthas to be considered.
2.6. Is EN indicated in elderly patients withdepression?
EN is recommended in depression in order toovercome the phase of severe anorexia and lossof motivation (C).
Comment: Depression is common in elderly pa-tients, but often not recognised due to thedifficulty of discriminating it from other symptomsof old age. Anorexia and refusal to eat are integralsymptoms of this disease, and depression is there-fore regarded as a major cause of undernutrition inthe elderly.156 Undernutrition may itself contributeto the depressive states often seen in theelderly.157 Depression can be treated by severalmethods, especially by drugs, although this maytake some time to be effective. Based on positiveclinical experience and expert opinion, EN isrecommended in the elderly suffering from depres-sion in order to support the patient during the earlyphase of severe anorexia and loss of motivation,thereby preventing the development of under-nutrition with its serious consequences (C).

ARTICLE IN PRESS
Table
6Prev
alen
ceof
aspirationpne
umon
iain
tube-fedelderly
patients.
First
author
Studytype
Patients
Aspirationpneumonia
(AP)
nAge�
(yea
rs)
Diagn
oses
Before
After
Timeperiod
Patel160
P24
72CVE,
CA,dem
entia
58%
14/2
4(58%
)(all)
UntilAPor
dea
th12
/14(86%
)(w
ithAP)
Paillaud
35
R73
8379
Mixed
15%
53%
2,6,
12mon
ths
Sali107
P32
75Mixed
9%— 3/
5(60%
)dea
thsdue
toAP
2–48
8day
s
Abitbol
26
P59
8377
Nursing
homeresiden
ts49
%51
%
30day
s
Bae
ten1
61
P90
72CA,ne
urolog
ical
disea
se—
6%
12mon
ths
Wijdicks
95
P63
74Apop
lex
—16
%
Hospital
stay
Peschl
151
P33
76Cereb
raldysfunc
tion
s—
18%
2–36
mon
ths
Kaw
36
R46
74Neu
rologica
ldisea
se,dem
entia
—22
%6mon
ths
Stua
rt108
R12
570
CA,dem
entia,
cach
exia
—28
%12
,18
mon
ths
Bou
rdel-M
arch
asson6
0R
4681
79
Mixed
—39
%30
day
s
Fay2
7R
8070
Apop
lex,
dem
entia,
PEG
—6%
/32%
14/1
92day
s
2970
Parkinson
NG
—24
%/4
6%14
/141
day
s
Golden
32
R10
289
76
dem
entia
—51
%6mon
ths
AP¼
aspirationpne
umon
ia,CA¼
carcinom
a,CVE¼
cerebrova
scular
even
t,NG¼
nasoga
strictube,
P¼
prospec
tive
,R¼
retrospe
ctive.
�Mea
nor
mea
n7stan
dard
dev
iation
.
ESPEN Guidelines on Enteral Nutrition 351

ARTICLE IN PRESS
D. Volkert et al.352
2.7. Is EN indicated in dementia?
ONS or TF may lead to an improvement innutritional status in demented patients. In earlyand moderate dementia ONS—and occasionallyTF—may contribute to ensuring an adequateenergy and nutrient supply and to preventingundernutrition from developing; they are there-fore recommended (C). In those with terminaldementia, TF is not recommended (C). Thedecision in each case must be made on anindividual basis.
Comment: An indequate intake of energy andnutrients is a common problem in dementedpatients. Undernutrition may be caused by severalfactors including anorexia (common cause: poly-pharmaco-therapy), insufficient oral intake (for-getting to eat), depression, apraxia of eating or,less often, enhanced energy requirement due tohyperactivity (constant pacing).158 In advancedstages of dementia, dysphagia may develop andmight be an indication for EN in a few cases.
Some studies with ONS have shown improve-ments in body weight (Ib)49,159 (IIa)50. In tube-feddemented elderly patients, two studies reportedweight gain31,32 (III), but two others reported nochange (III)24 (IIb)86. Available trials regarding theeffects of ONS (Ib)49 (IIa)50 or TF24,33,36 onfunctional status, report no improvement (Com-pare 1.5). In terms of survival most studies show nobenefit.33,81,84,94 On the other hand, Rudberg etal.61 described lower mortality, compared to con-trols, at 30 days and 1 year in enterally fed patientswith severe cognitive impairment (IIb). Very lowmortality rates have been reported in PEG-feddemented nursing home residents.32,57,62 On theother hand, in one retrospective study comparingmortality rates in different diagnostic groups,outcome was worst among the demented59 (III).
In conclusion, tube-fed demented patients varyconsiderably with respect to their prognosis. Out-come and also the success of nutritional therapy indemented patients are strongly influenced by theseverity of disease, the kind and extent ofcomorbidities and by their general condition. It istherefore recommended that adequate and highquality nutrition is ensured, especially in the earlyand middle stages of dementia, in order to preventundernutrition developing and to help maintain astable general condition (C).
TF may be useful in some demented patients.The following aspects have to be considered indecision-making:
�
presumed or previously expressed wishes of thepatient with respect to TF;�
severity of the disease; � the individual prognosis and life expectancy ofthe demented patient;
� the anticipated quality of life of the patient withor without TF;
� the anticipated complications and impairmentsdue to TF;
� the mobility of the patient.The decision for or against TF has always to bemade individually and together with relativesand care givers, legal custodian, family doctorand therapists, and in case of doubt, with legaladvice.
For patients with terminal dementia (irreversi-ble, immobile, unable to communicate, completelydependent, lack of physical resources) TF is notrecommended (C).
2.8. Is EN indicated in geriatric patients withcancer?
In principal, nutritional therapy in geriatricpatients with cancer does not differ from young-er cancer patients (see Guidelines on ‘‘Non-surgical oncology’’).
Comment: It is generally recognised, however, thatelderly are at higher risk of being undernourishedthan younger patients and restoration of BCM ismore difficult. Therefore, preventive nutritionalsupport has to be considered.
2.9. In patients with dysphagia does TF preventaspiration pneumonia by improving functionalstatus?
Due to the heterogeneity of the studies, and lackof data on prevalence before the TF, firmconclusions can not be drawn.
Comment: Dysphagia may enhance aspiration frompharyngeal contents, but, on the other hand, TFmay enhance reflux and aspiration of gastriccontents. Several studies have reported the pre-valence of aspiration pneumonia in tube-fedelderly patients (Table 6). Due to the heterogeneityof patient groups and lack of data on theprevalence of aspiration before TF, it is difficultto draw any firm conclusion whether bypassingdysphagia, using a NG tube or PEG helps to reducethe incidence of pneumonia. It certainly has thepotential to increase reflux and aspiration. Dataabout the incidence of aspiration pneumonia duringnutritional support via PEG compared to NGT arecontroversial.12,27,86,161 It is also not proven thatsurgical or endoscopic jejunostomy prevents thiscomplication.

ARTICLE IN PRESS
Table
7PEG
versus
nasoga
strictubefeed
ingin
elderly
patients.
First
author
Study
type
nAge�
(years)
Diagn
oses(place
)Duration
Treatment
failure
Intake
Nutritional
status
Aspiration
Other
complica
tions
Mortality
LOS
Bae
ten1
61
P44
PEG
72710
Mixed
(hospital)
18720
day
sk
n.a.
n.a.
¼n.a.
n.a.
n.a.
RCT
46NG
Norton1
1P
16PEG
76Apop
lexia
(hospital)
6wks
km
mn.a.
n.a.
kk
RCT
14NG
79
Park
12
P20
PEG
5675
Neu
rolog.
dyspha
gia
(hospital)
4wks
km
m¼
/m¼
/mn.a.
n.a.
RCT
20NG
6573
Dwolatzky8
6P
32PEG
85Chron
ic,
mixed
(hom
e)
4wks/1
2wks
kn.a.
¼/m
k¼
kn.a.
NRT
90NG
82
Fay2
7R
80PEG
70.2
Mixed
(hospital)
1427
192
day
sk
n.a.
¼k
¼¼
n.a.
NRT
29NG
68.8
LOS¼
leng
thof
stay,n.a.¼
notav
ailable,NG¼
nasoga
strictube,
NRT¼
non-rand
omised
trial,
PEG¼
percu
tane
ousen
dosco
pic
gastrostom
y,P¼
prospec
tive
,R¼
retrospec
tive
,RCT¼rand
omised
controlled
trial,Re
f.¼
referenc
e,wks¼
wee
ksm
increa
se,k
dec
rease(improv
emen
tin
thePEG
-group
compared
totheNG-group
);¼
nodifferenc
ebetwee
nPEG
andNG.
�Mea
nor
mea
n7stan
dard
dev
iation
.
ESPEN Guidelines on Enteral Nutrition 353

ARTICLE IN PRESS
D. Volkert et al.354
2.10. Can EN prevent or improve pressure ulcersin geriatric patients?
ONS, particular high protein ONS, can reduce therisk of developing pressure ulcers (A). Based onpositive clinical experience, EN is also recom-mended in order to improve healing of pressureulcers (C).
Comment: Adequate nutrition is a prerequisite forpreventing and healing pressure ulcers. Studiesaddressing this topic are difficult to conductbecause of the multifactorial origin of pressureulcers, various uncontrollable factors affecting thedevelopment of pressure ulcers and the necessarilylong observational periods. Only few trials areavailable examining the effects of EN on preventionor healing of decubitus ulcers. These trials varygreatly with respect to study design, patientpopulation and reported outcome variables.
A recent meta-analysis of four randomised con-trolled trials showed that oral nutritional supple-mentation was associated with a significantly lowerincidence of pressure ulcer development in at-riskpatients compared to routine care (odds ratio (OR)0.75; 95% CI 0.62–0.89)162 (Ia). Three of the fourstudies used high protein ONS (30 energy percent).Three other studies, which were not meta-analy-sable, showed a trend towards improved healing ofexisting pressure ulcers in patients receivingONS.162
Available studies on the effect of TF do not showsignificant effects, neither on healing nor onprevention of decubitus ulcers,14,26,31,60,62 how-ever, overall quality of the studies is poor.
The importance of protein in pressure sorehealing was suggested in an 8-week non-rando-mised study in 28 undernourished nursing homeresidents with decubitus ulcers.163 The administra-tion of a TF formula with 61 g protein per litre (24energy percent) was more successful in decreasingtotal pressure ulcer surface area than a TF formulawith 37 g protein per litre (14 energy percent).
Clinical experience suggests that wound healingin elderly patients may be improved by theadministration of supplements containingprotein and micronutrients that are involved inwound healing (zinc, arginine, carotenoids, vita-mins A, C and E). Crucial for the effect of thesenutrients is the local circulation in the pressureulcer area, which determines effective nutrienttransport and local metabolism as well as removalof toxic cell products. Besides the correction ofnutrient deficiencies, the correct positioning of thepatient to allow optimal blood circulation to thepressure area and to minimise further tissuedamage is crucial.
3. Special practical aspects of EN in
geriatric patients3.1. How should EN be delivered: by PEG or byNGT?
In elderly patients in whom EN is anticipated forlonger than 4 weeks, placement of a PEG tube isrecommended (A).
Comment: Five studies (four prospective, threerandomised) comparing PEG with NGT, show thesuperiority of PEG (Table 7) in allowing the admin-istration of greater amounts of energy and nutrientsover longer periods, resulting in better nutritionalstatus (Ib)11,12 (IIa)86 The use of NGT is associatedwith more tube displacements86 (IIa) and more re-insertions (Ib)12,161 (III)27. Less treatment failureswith PEG are reported in all studies (Ib)11,12,161
(IIa)86 (III)27. Moreover, fewer fixations are necessaryin PEG patients, and the management is easier bothfor patients and nursing staff161 (Ib).
Improved survival in PEG-fed patients was ob-served in one randomised controlled trial and onenon-randomised trial (Ib)11 (IIa)86. In their retro-spective study, however, Fay et al.27 found nodifference in mortality between PEG- and NGT-fedpatients. Dwolatzky et al.86 (IIa) and Fay et al.27
(III) reported a lower incidence of aspiration inpatients fed by PEG than by NGT. However, Parket al.12 and Baeten and Hoefnagels161 found nodifference in aspiration rates in their randomisedstudies. In geriatric patients the frequent combina-tion of neurological swallowing difficulties withcognitive impairment (dementia, Parkinson’s dis-ease, recurrent cerebrovascular events) is asso-ciated with a higher risk of aspiration. In thesesituations, early PEG placement compared to NGTmight be advantageous.
An important aspect of PEG in patients withneurological dysphagia is that it allows moreeffective swallowing therapy without interferenceby NGT. As swallowing improves, TF can be reducedas oral intake increases, and in many cases it can becompletely abandoned.
3.2. When should TF be initiated after PEGplacement?
TF can be initiated 3 h after PEG placement ingeriatric patients (A).
Comment: In three randomised prospective studiesthat included elderly patients, early feeding (3–4 hafter PEG placement) vs. delayed feeding (24 hafter PEG placement) was studied164–166 (Ib).Tolerance and safety were equal whether nutritionwas initiated 3 or 24 h after PEG placement.164,165

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 355
Another study comparing initiation of nutrition 4vs. 24 h after PEG placement, also found nosignificant differences between the two groups.166
These results confirm early feeding after PEGplacement as a safe and effective procedure inelderly patients.
3.3. Is EN in geriatric patients associated withspecific complications?
Complications of EN are similar to those in otherage groups. There is no information availableabout the prevalence of specific complications indifferent age groups.
3.4. Is dietary fibre beneficial for enterally fedgeriatric patients?
Available studies suggest that dietary fibre cancontribute to the normalisation of bowel func-tions in elderly tube-fed subjects (B).
With respect to ONS no studies are available.
Comment: Elderly patients often suffer fromgastrointestinal problems, including constipationand diarrhoea. The effect of dietary fibre in ONS onbowel function has not been studied. Since dietaryfibre intake from food is usually low in geriatricpatients, fibre-containing products are generallyrecommended.
Few studies of the effects of fibre-containingenteral formulae on bowel function in elderlysubjects are available.167–172 Despite great differ-ences in study populations, gastrointestinal pro-blems and the type and amount of fibre used, thesestudies all report that fibre helps to normalisebowel functions during TF.
In a randomised cross-over study design with 10long-term tube-fed elderly patients recoveringfrom stroke without diarrhoea the administrationof 28.8 g soy/oat fibre per day (14.4 g/l) signifi-cantly increased the number of bowel movementsper day (0.970.4 vs. 0.570.2, Po0:05) and faecalweights (57731 vs. 32725 g/d, Po0:05)167 (Ib). Arandomised pilot study with seven immobile long-term care residents on long-term TF also reportedmore stools with a softer consistency168 (III).
In long-term care patients with diarrhoea ENwith 12.8 g soy fibre/1000 kcal resulted in signifi-cantly fewer reports of diarrhoea (6 vs. 26,Po0:01) and markedly improved bowel functioncompared with the control group without fibre169
(Ib). In a prospective observational study with 20elderly bedridden patients (mean age 7975 years)with diarrhoea, receiving EN due to cerebrovascu-lar events, Nakao et al.170 demonstrated thatsoluble fibre decreased the frequency of daily
bowel movements significantly and simultaneouslyimproved faecal features in the course of 4 weekswith gradually increasing fibre administration from7 to 28 g/d (III). A retrospective chart review in 50long-term care patients with mixed diagnoses (age28–83 yr, median age 71 yr) who received EN with14 g soy polysaccharides/l for at least 3 weeks alsoresulted in fewer loose stools and diarrhoea than inpatients given a fibre-free solution171 (III). Homannet al.172 investigated the effects of 20 g partiallyhydrolised guar gum/l in a prospective, randomisedcontrolled trial with 100 surgical and medicalpatients. About 30 patients (mean age 60 years,mainly gastric or oesophageal resection) receivedtotal EN and 70 patients (mean age 69 years, mainlymetastatic malignancies) received supplementaryEN. In patients receiving total EN with fibre and inthe whole group receiving fibre the incidence ofdiarrhoea was significantly lower than in patientsreceiving the standard diet without fibre.
In order to increase tolerance and avoid gastro-intestinal side-effects such as bloating and flatu-lence, the mode of administration (rate,temperature) is important. In subjects not used todietary fibre intake, fibre fortified feedings shouldbe added gradually.
Since different kinds of fibre may have dissimilareffects in different clinical situations, furtherstudies are necessary to elucidate the role ofspecific types of dietary fibre in enterally fedgeriatric patients.
References
1. Milne AC, Potter J, Avenell A. Protein and energysupplementation in elderly people at risk from malnutri-tion. Cochrane Database Syst Rev 2005; Issue 1. Art. No.:CD003288.pub2. DOI:10.1002/14651858.
2. Volkert D, Hubsch S, Oster P, Schlierf G. Nutritional supportand functional status in undernourished geriatric patientsduring hospitalization and 6-month follow-up. Aging ClinExp Res 1996;8:386–95.
3. Payette H, Boutier V, Coulombe C, Gray-Donald K. Benefitsof nutritional supplementation in free-living, frail, under-nourished elderly people: a prospective randomized com-munity trial. J Am Diet Assoc 2002;102:1088–95.
4. Lawson RM, Doshi MK, Ingoe LE, Colligan JM, Barton JR,Cobden I. Compliance of orthopaedic patients with post-operative oral nutritional supplementation. Clin Nutr2000;19:171–5.
5. Roebothan BV, Chandra RK. Relationship between nutri-tional status and immune function of elderly people. AgeAgeing 1994;23:49–53.
6. Williams CM, Driver LT, Older J, Dickerson JWT. A controlledtrial of sip-feed supplements in elderly orthopaedicpatients. Eur J Clin Nutr 1989;43:267–74.
7. Gray-Donald K, Payette H, Boutier V. Randomized clinicaltrial of nutritional supplementation shows little effect on

ARTICLE IN PRESS
D. Volkert et al.356
functional status among free-living frail elderly. J Nutr1995;125:2965–71.
8. Larsson J, Unosson M, Ek A-C, Nilsson L, Thorslund S,Bjurulf P. Effects of dietary supplement on nutritionalstatus and clinical outcome in 501 geriatric patients—arandomized study. Clin Nutr 1990;9:179–84.
9. Fiatarone MA, O’Neill EF, Ryan ND, et al. Exercise trainingand nutritional supplementation for physical frailty in veryelderly people. N Engl J Med 1994;330:1769–75.
10. Ovesen L. The effect of a supplement which is nutrient densecompared to standard concentration on the total nutritionalintake of anorectic patients. Clin Nutr 1992;11:154–7.
11. Norton B, Homer-Ward M, Donnelly MT, Long RG, HolmesGK. A randomised prospective comparison of percutaneousendoscopic gastrostomy and nasogastric tube feeding afteracute dysphagic stroke. Br Med J 1996;312:13–6.
12. Park RH, Allison MC, Lang J, et al. Randomised comparisonof percutaneous endoscopic gastrostomy and nasogastrictube feeding in patients with persisting neurologicaldysphagia. Br Med J 1992;304:1406–9.
13. Bastow MD, Rawlings J, Allison SP. Benefits of supplemen-tary tube feeding after fractured neck of femur: arandomised controlled trial. Br Med J 1983;287:1589–92.
14. Hartgrink HH, Wille J, Konig P, Hermans J, Breslau PJ.Pressure sores and tube feeding in patients with a fractureof the hip: a randomized clinical trial. Clin Nutr 1998;17:287–92.
15. Sullivan DH, Nelson CL, Bopp MM, Puskarich-May CL, WallsRC. Nightly enteral nutrition support of elderly hip fracturepatients: a phase I trial. J Am Coll Nutr 1998;17:155–61.
16. Norregaard O, Tottrup A, Saaek A, Hessov I. Effects of oralsupplements to adults with chronic obstructive pulmonarydisease (abstract). Clin Resp Physiol 1987;23:388s.
17. Jensen MB, Hessov I. Dietary supplementation at homeimproves the regain of lean body mass after surgery.Nutrition 1997;13:422–30.
18. Bos C, Benamouzig R, Bruhat A, et al. Nutritional statusafter short-term dietary supplementation in hospitalizedmalnourished geriatric patients. Clin Nutr 2001;20:225–33.
19. Hubsch S, Volkert D, Oster P, Schlierf G. Moglichkeiten undGrenzen der Anwendung flussiger Nahrstoffkonzentrate inder Therapie der Mangelernahrung geriatrischer Patienten.Akt Ernahr -Med 1994;19:109–14.
20. Fiatarone Singh MA, Bernstein MA, Ryan AD, O’Neill EF,Clements KM, Evans WJ. The effect of oral nutritionalsupplements on habitual dietary quality and quantity infrail elders. J Nutr Health Aging 2000;4:5–12.
21. Meredith CN, Frontera WR, O’Reilly KP, Evans WJ. Bodycomposition in elderly men: Effect of dietary modificationduring strength training. J Am Geriatr Soc 1992;40:155–62.
22. Wouters-Wesseling W, Van Hooijdonk C, Wagenaar L, BindelsJ, de Groot L, van Staveren W. The effect of a liquid nutritionsupplement on body composition and physical functioning inelderly people. Clin Nutr 2003;22:371–7.
23. Bourdel-Marchasson I, Joseph PA, Dehail P, et al. Functionaland metabolic early changes in calf muscle occurringduring nutritional repletion in malnourished elderly pa-tients. Am J Clin Nutr 2001;73:832–8.
24. Callahan CM, Haag KM, Weinberger M, et al. Outcomes ofpercutaneous endoscopic gastrostomy among older adultsin a community setting. J Am Geriatr Soc 2000;48:1048–54.
25. Ciocon JO, Silverstone FA, Graver LM, Foley CJ. Tubefeedings in elderly patients. Indications, benefits, andcomplications. Arch Intern Med 1988;148:429–33.
26. Abitbol V, Selinger-Leneman H, Gallais Y, et al. Percuta-neous endoscopic gastrostomy in elderly patients. A
prospective study in a geriatric hospital. GastroenterolClin Biol 2002;26:448–53.
27. Fay DE, Poplausky M, Gruber M, Lance P. Long-term enteralfeeding: a retrospective comparison of delivery viapercutaneous endoscopic gastrostomy and nasoenterictubes. Am J Gastroenterol 1991;86:1604–9.
28. Vetta F, Gianni W, Ronzoni S, et al. Role of aging inmalnutrition and in restitution of nutritional parameters bytube feeding. Arch Gerontol Geriatr 1996(Suppl. 5):599–604.
29. Friedman PJ, Campbell AJ, Caradoc-Davies TH. Hypoalbu-minemia in the elderly is due to disease not malnutrition.J Clin Exp Gerontol 1985;7:191–203.
30. Franch-Arcas G. The meaning of hypoalbuminaemia inclinical practice. Clin Nutr 2001;20:265–9.
31. Peck A, Cohen CE, Mulvihill MN. Long-term enteral feedingof aged demented nursing home patients. J Am Geriatr Soc1990;38:1195–8.
32. Golden A, Beber C, Weber R, Kumar V, Musson N, SilvermanM. Long-term survival of elderly nursing home residentsafter percutaneous endoscopic gastrostomy for nutritionalsupport. Nurs Home Med 1997;5:382–9.
33. Nair S, Hertan H, Pitchumoni CS. Hypoalbuminemia is apoor predictor of survival after percutaneous endoscopicgastrostomy in elderly patients with dementia. Am JGastroenterol 2000;95:133–6.
34. Okada K, Yamagami H, Sawada S. The nutritional status ofelderly bed-ridden patients receiving tube feeding. J NutrSci Vitaminol 2001;47:236–41.
35. Paillaud E, Bories PN, Merlier I, Richardet JP, Jeanfaivre V,Campillo B. Prognosis factors of short and long-termsurvival in elderly hospitalized patients after percutaneousendoscopic gastrostomy. Gastroenterol Clin Biol 2002;26:443–7.
36. Kaw M, Sekas G. Long-term follow-up of consequences ofpercutaneous endoscopic gastrostomy (PEG) tubes innursing home patients. Dig Dis Sci 1994;39:738–43.
37. Panos MZ, Reilly H, Moran A, et al. Percutaneousendoscopic gastrostomy in a general hospital: prospectiveevaluation of indications, outcome, and randomisedcomparison of two tube designs. Gut 1994;35:1551–6.
38. Sitzmann JV. Nutritional support of the dysphagic patient:methods, risks, and complications of therapy. J ParenterEnteral Nutr 1990;14:60–3.
39. Hebuterne X, Schneider S, Peroux J-L, Rampal P. Effects ofrefeeding by cyclic enteral nutrition on body composition:comparative study of elderly and younger patients. ClinNutr 1997;16:283–9.
40. Schneider SM, Al-Jaouni R, Pivot X, Braulio VB, Rampal P,Hebuterne X. Lack of adaptation to severe malnutrition inelderly patients. Clin Nutr 2002;21:499–504.
41. Shizgal HM, Martin MF, Gimmon Z. The effect of age on thecaloric requirement of malnourished individuals. Am J ClinNutr 1992;55:783–9.
42. Fiatarone MA, O’Neill EF, Doyle N, et al. The Boston FISCITStudy: The effects of resistance training and nutritionalsupplementation on physical fraility in the oldest old. J AmGeriatr Soc 1993;41:333–7.
43. Unosson M, Larsson J, Ek A-C, Bjurulf P. Effects of dietrysupplement on functional condition and clinical outcomemeasured with a modified Norton scale. Clin Nutr 1992;11:134–9.
44. Tidermark J, Ponzer S, Carlsson P, et al. Effects of protein-rich supplementation and nandrolone in lean elderlywomen with femoral neck fractures. Clin Nutr 2004;23:587–96.

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 357
45. Potter JM. Oral supplements in the elderly. Curr Opin ClinNutr Metab Care 2001;4:21–8.
46. Woo J, Ho SC, Mak YT, Law LK, Cheung A. Nutritional statusof elderly patients during recovery from chest infectionand the role of nutritional supplementation assessed by aprospective trial. Age Ageing 1994;23:40–8.
47. Espaulella J, Guyer H, Diaz-Escriu F, Mellado-Navas JA,Castells M, Pladevall M. Nutritional supplementation ofelderly hip fracture patients. A randomized, double-blind,placebo-controlled trial. Age Ageing 2000;29:425–31.
48. Gariballa SE, Parker SG, Taub N, Castleden CM. Arandomized, controlled, single-blind trial of nutritionalsupplementation after acute stroke. J Parenter EnteralNutr 1998;22:315–9.
49. Wouters-Wesseling W, Wouters AE, Kleijer CN, Bindels JG,de Groot CP, van Staveren WA. Study of the effect of aliquid nutrition supplement on the nutritional status ofpsycho-geriatric nursing home patients. Eur J Clin Nutr2002;56:245–51.
50. Faxen-Irving G, Andren-Olsson B, af Geijerstam A, Basun H,Cederholm T. The effect of nutritional intervention inelderly subjects residing in group-living for the demented.Eur J Clin Nutr 2002;56:221–7.
51. Saudny-Unterberger H, Martin JG, Gray-Donald K. Impactof nutritional support on functional status during an acuteexacerbation of chronic obstructive pulmonary disease. AmJ Respir Crit Care Med 1997;156:794–9.
52. Kwok T, Woo J, Kwan M. Does low lactose milk powderimprove the nutritional intake and nutritional status of frailolder Chinese people living in nursing homes? J Nutr HealthAging 2001;5:17–21.
53. Lauque S, Arnaud-Battandier F, Mansourian R, Guigoz Y.Protein-energy oral supplementation in malnourished nur-sing-home residents. A controlled trial. Age Ageing 2000;29:51–6.
54. Efthimiou J, Fleming J, Gomes C, Spiro SG. The effect ofsupplementary oral nutrition in poorly nourished patientswith chronic obstructive pulmonary disease. Am Rev RespirDis 1988;137:1075–82.
55. Cederholm TE, Hellstrom KH. Reversibiliy of protein-energymalnutrition in a group of chronically ill elderly out-patients. Clin Nutr 1995;14:81–7.
56. Katakity M, Webb JF, Dickerson JWT. Some effects of a foodsupplement in elderly hospital patients: a longitudinalstudy. Hum Nutr Appl Nutr 1983;37A:85–93.
57. Abuksis G, Mor M, Segal N, et al. Percutaneous endoscopicgastrostomy: high mortality rates in hospitalized patients.Am J Gastroenterol 2000;95:128–32.
58. Skelly RH, Kupfer RM, Metcalfe ME, et al. Percutaneousendoscopic gastrostomy (PEG): change in practice since1988. Clin Nutr 2002;21:389–94.
59. Sanders DS, Carter MJ, D’Silva J, James G, Bolton RP,Bardhan KD. Survival analysis in percutaneous endoscopicgastrostomy feeding: a worse outcome in patients withdementia. Am J Gastroenterol 2000;95:1472–5.
60. Bourdel-Marchasson I, Dumas F, Pinganaud G, Emeriau J-P,Decamps A. Audit of percutaneous endoscopic gastrostomyin long-term enteral feeding in a nursing home. Int J QualHealth Care 1997;9:297–302.
61. Rudberg MA, Egleston BL, Grant MD, Brody JA. Effectivenessof feeding tubes in nursing home residents with swallowingdisorders. J Parenter Enteral Nutr 2000;24:97–102.
62. Mitchell SL, Kiely DK, Lipsitz LA. The risk factors andimpact on survival of feeding tube placement in nursinghome residents with severe cognitive impairment. ArchIntern Med 1997;157:327–32.
63. Mitchell SL, Kiely DK, Lipsitz LA. Does artificial enteralnutrition prolong the survival of institutionalized elderswith chewing and swallowing problems? J Geront Biol SciMed Sci 1998;53:M207–13.
64. Sanders H, Newall S, Norton B, Holmes GT. Gastrostomyfeeding in the elderly after acute dysphasgic stroke. J NutrHealth Aging 2000;4:58–60.
65. Weaver JP, Odell P, Nelson C. Evaluation of the benefits ofgastric tube feeding in an elderly population. Arch FamMed 1993;2:953–6.
66. Sullivan DH, Walls RC. Impact of nutritional status onmorbidity in a population of geriatric rehabilitationpatients. J Am Geriatr Soc 1994;42:471–7.
67. Lumbers M, Driver LT, Howland RJ, Older MWJ, Williams CM.Nutritional status and clinical outcome in elderly femalesurgical orthopaedic patients. Clin Nutr 1996;15:101–7.
68. Incalzi RA, Landi F, Cipriani L, et al. Nutritional assessment:A primary component of multidimensional geriatric as-semssment in the acute care setting. J Am Geriatr Soc1996;44:166–74.
69. Davalos A, Ricart W, Gonzalez-Huix F, et al. Effect ofmalnutrition after acute stroke on clinical outcome. Stroke1996;27:1028–32.
70. Milne AC, Potter J, Avenell A. Protein and energysupplementation in elderly people at risk from malnutri-tion. Cochrane Database Syst Rev 2002; CD003288.
71. Delmi M, Rapin C-H, Benoga JM, Delmas PD, Vasey H.Dietary supplementation in elderly patients with fracturedneck of femur. Lancet 1990;335:1013–6.
72. Tkatch L, Rapin C-H, Rizzoli R, et al. Benefits of oralprotein supplementation in elderly patients with fractureof the proximal femur. J Am Coll Nutr 1992;11:519–25.
73. Schurch MA, Rizzoli R, Slosman D, Vadas L, Vergnaud P,Bonjour JP. Protein supplements increase serum insulin-likegrowth factor-I levels and attenuate proximal femur bone lossin patients with recent hip frature. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1998;128:801–9.
74. Brown KM, Seabrock NA. Nutritional influences on recoveryand length of hospital stay in elderly women followingfemoral fracture. Proc Nutr Soc 1992;51:132A.
75. Avenell A, Handoll HH. Nutritional supplementation for hipfracture aftercare in the elderly. Cochrane Database SystRev 2005; Issue 2. CD001880. pub3.
76. Krondl M, Coleman PH, Bradley CL, Lau D, Ryan N.Subjectively healthy elderly consuming a a liquid nutritionsupplement maintained body mass index and improvedsome nutritional parameters and perceived well-being. JAm Diet Assoc 1999;99:1542–8.
77. Bannerman E, Pendlebury J, Phillips F, Ghosh S. A cross-sectional and longitudinal study of health-related qualityof life after percutaneous gastrostomy. Eur J GastroenterolHepatol 2000;12:1101–9.
78. Verhoef MJ, van Rosendaal GM. Patient outcomes related topercutaneous endoscopic gastrostomy placement. J ClinGastroenterol 2001;32:49–53.
79. Schneider SM, Pouget I, Staccini P, Rampal P, Hebuterne X.Quality of life in long-term home enteral nutrition patients.Clin Nutr 2000;19:23–8.
80. Stratton RJ, Green CJ, Elia M. Disease-related malnutri-tion: an evidence-based approach to treatment. Oxon, UK:CABI Publishing; 2003.
81. Meier DE, Ahronheim JC, Morris J, Baskin-Lyons S, MorrisonRS. High short-term mortality in hospitalized patients withadvanced dementia: lack of benefit of tube feeding. ArchIntern Med 2001;161:594–9.

ARTICLE IN PRESS
D. Volkert et al.358
82. Cowen ME, Simpson SL, Vettese TE. Survival estimates forpatients with abnormal swallowing studies. J Gen InternMed 1997;12:88–94.
83. Croghan JE, Burke EM, Caplan S, Denman S. Pilot study of12-month outcomes of nursing home patients with aspira-tion on videofluoroscopy. Dysphagia 1994;9:141–6.
84. Murphy LM, Lipman TO. Percutaneous endoscopic gastro-stomy does not prolong survival in patients with dementia.Arch Intern Med 2003;163:1351–3.
85. Lindemann B, Nikolaus PT. Outcomes of percutaneousendoscopic gastrostomy in dementia patients. J Am GeriatrSoc 2001;49:838–9.
86. Dwolatzky T, Berezovski S, Friedmann R, et al. Aprospective comparison of the use of nasogastric andpercutaneous endoscopic gastrostomy tubes for long-termenteral feeding in older people. Clin Nutr 2001;20:535–40.
87. Quill TE. Utilization of nasogastric feeding tubes in a groupof chronically ill, elderly patients in a community hospital.Arch Intern Med 1989;149:1937–41.
88. Bussone M, Meaune S. Percutaneous endoscopic gastro-stomy in old age patients. Age and Nutrition 1992;3:110–1.
89. Bussone M, Lalo M, Piette F, Hirsch JF, Senecal P.Percutaneous endoscopic gastrostomy: its value in assistedalimentation in malnutrition in elderly patients. Apropos of101 consecutive cases in patients over 70 years of age.Annales de Chirurgie 1992;46:59–66.
90. Markgraf R, Geitmann K, Pientka L, Scholten T. Ernahrunguber perkutane endoskopische Gastrostomie. Langzeiter-gebnisse bei polymorbiden geriatrischen Patienten. Geria-trische Forschung 1994;4:123–9.
91. Raha SK, Woodhouse K. The use of percutaneous endo-scopic gastrostomy (PEG) in 161 consecutive elderlypatients. Age Ageing 1994;23:162–3.
92. Finucane P, Aslan SM, Duncan D. Percutaneous endoscopicgastrostomy in elderly patients. Postgrad Med J 1991;67:371–3.
93. James A, Kapur K, Hawthorne AB. Long-term outcome ofpercutaneous endoscopic gastrostomy feeding in patientswith dysphagic stroke. Age Ageing 1998;27:671–6.
94. Wanklyn P, Cox N, Belfield P. Outcome in patients who requirea gastrostomy after stroke. Age Ageing 1995;24:510–4.
95. Wijdicks EF, McMahon MM. Percutaneous endoscopic gastro-stomy after acute stroke: complications and outcome.Cerebrovascular Diseases 1999;9:109–11.
96. Clarkston WK, Smith OJ, Walden JM. Percutaneous endo-scopic gastrostomy and early mortality. South Med J1990;83:1433–6.
97. Friedenberg F, Jensen G, Gujral N, Braitman LE, Levine GM.Serum albumin is predictive of 30-day survival afterpercutaneous endoscopic gastrostomy. J Parenter EnteralNutr 1997;21:72–4.
98. Horton WL, Colwell DL, Burlon DT. Experience withpercutaneous endoscopic gastrotomy in a communityhospital. Am J Gastroenterol 1991;86:168–70.
99. Kohli H, Bloch R. Percutaneous endoscopic gastrostomy: acommunity hospital experience. Am Surg 1995;61:191–4.
100. Larson DE, Burton DD, Schroeder KW, DiMagno EP.Percutaneous endoscopic gastrostomy. Indications, suc-cess, complications, and mortality in 314 consecutivepatients. Gastroenterology 1987;93:48–52.
101. Light VL, Slezak FA, Porter JA, Gerson LW, McCord G.Predictive factors for early mortality after percutaneousendoscopic gastrostomy. Gastrointest Endosc 1995;42:330–5.
102. Llaneza PP, Menendez AM, Roberts R, Dunn GD. Percuta-neous endoscopic gastrostomy: clinical experience andfollow-up. South Med J 1988;81:321–4.
103. Markgraf R, Geitmann K, Pientka L, Scholten T. Long-termresults of enteral nutrition by percutaneous endoscopicgastrostomy in multi-morbid internal medicine patients. ZGastroenterol 1993;31(Suppl. 5):21–3.
104. Nicholson FB, Korman MG, Richardson MA. Percutaneousendoscopic gastrostomy: a review of indications, complica-tions and outcome. J Gastroenterol Hepatol 2000;15:21–5.
105. Rabeneck L, Wray NP, Petersen NJ. Long-term outcomes ofpatients receiving percutaneous endoscopic gastrostomytubes. J Gen Intern Med 1996;11:287–93.
106. Rimon E. The safety and feasibility of percutaneousendoscopic gastrostomy placement by a single physician.Endoscopy 2001;33:241–4.
107. Sali A, Wong PT, Read A, McQuillan T, Conboy D. Percutaneousendoscopic gastrostomy: the Heidelberg Repatriation Hospitalexperience. Aust NZ J Surg 1993;63:545–50.
108. Stuart SP, Tiley EH, Boland JP. Feeding gastrostomy: acritical review of its indications and mortality rate. SouthMed J 1993;86:169–72.
109. Tan W, Rajnakova A, Kum CK, Alponat A, Goh PM. Evaluationof percutaneous endoscopic gastrostomy in a universityhospital. Hepato-Gastroenterology 1998;45:2060–3.
110. Taylor CA, Larson DE, Ballard DJ, et al. Predictors ofoutcome after percutaneous endoscopic gastrostomy: acommunity-based study. Mayo Clin Proc 1992;67:1042–9.
111. Wolfsen HC, Kozarek RA, Ball TJ, et al. Long-term survival inpatients undergoing percutaneous endoscopic gastrostomyand jejunostomy. Am J Gastroenterol 1990;85:1120–2.
112. Elia M, Stratton RJ, Holden C, et al. Home enteral tubefeeding following cerebrovascular accident. Clin Nutr2001;20:27–30.
113. Howard L, Malone M. Clinical outcome of geriatric patientsin the United States receiving home parenteral and enteralnutrition. Am J Clin Nutr 1997;66:1364–70.
114. Sanders DS, Carter MJ, D’Silva J, McAlindon ME, WillemsePJ, Bardham KD. Percutaneous endoscopic gastrostomy: aprospective analysis of hospital support required andcomplications following discharge to the community. EurJ Clin Nutr 2001;55:610–4.
115. Schneider SM, Raina C, Pugliese P, Pouget I, Rampal P,Hebuterne X. Outcome of patients treated with homeenteral nutrition. J Parent Ent Nutr 2001;25:203–9.
116. Mitchell SL, Tetroe JM. Survival after percutaneous endo-scopic gastrostomy placement in older persons. J GerontolBiol Sci Med Sci 2000;55:M735–9.
117. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. ESPENguidelines for nutrition screening 2002. Clin Nutr 2003;22:415–21.
118. Vellas B, Guigoz Y, Garry PJ, et al. The Mini NutritionalAssessment (MNA) and its use in grading the nutritionalstate of elderly patients. Nutrition 1999;15:116–22.
119. Chandra RK, Puri S. Nutritional support improves antibodyresponse to influenza virus vaccine in the elderly. Br Med J1985;291:705–6.
120. Wouters-Wesseling W, Wagenaar LW, de Groot LC, BindelsJG, van Staveren WA. Biochemical antioxidant levelsrespond to supplementation with an enriched drink in frailelderly people. J Am Coll Nutr 2003;22:232–8.
121. Banerjee AK, Brocklehurst JC, Wainwright H, Swindell R.Nutritional status of long-stay geriatric in-patients: effectsof a food supplement (Complain). Age and Ageing 1978;7:237–43.
122. Banerjee AK, Brocklehurst JC, Swindell R. Protein status inlong-stay geriatric in-patients. Gerontology 1981;27:161–6.
123. Beck AM, Ovesen L, Schroll M. Home-made oral supplementas nutritional support of old nursing home residents, who

ARTICLE IN PRESS
ESPEN Guidelines on Enteral Nutrition 359
are undernourished or at risk of undernutrition based onthe MNA. A pilot trial. Aging Clin Exp Res 2002;14:212–5.
124. Ek A-C, Larsson J, von Schenck H, Thorslund S, Unosson M,Bjurulf P. The correlation between anergy, malnutritionand clinical outcome in an elderly hospital population. ClinNutr 1990;9:185–9.
125. Hankey CR, Summerbell J, Wynne HA. The effect of dietarysupplementation in continuing-care people: nutritional,anthropometric and biochemical parameters. J Hum NutrDiet 1993;6:317–22.
126. McEvoy AW, James OFW. The effect of a dietary supplement(Build-up) on nutritional status in hospitalized elderlypatients. Hum Nutr Appl Nutr 1982;36A:374–6.
127. Potter JM, Roberts MA, McColl JH, Reilly JJ. Proteinenergy supplements in unwell elderly patients—a rando-mized controlled trial. J Parenter Enteral Nutr 2001;25:323–9.
128. Bunker VW, Stansfield MF, Deacon-Smith R, Marzil RA,Hounslow A, Clayton BE. Dietary supplementation andimmunocompetence in housebound elderly subjects. Br JBiomed Sci 1994;51:128–35.
129. Bourdel-Marchasson I, Barateau M, Rondeau V, et al. Amulti-center trial of the effects of oral nutritionalsupplementation in critically ill older inpatients. Nutrition2000;16:1–5.
130. Chandra RK, Joshi P, Au B, Woodford G. Nutrition andimmunocompetence of the elderly: effect of short-termnutritional supplementation on cell-mediated immunityand lymphocyte subsets. Nutr Res 1982;2:223–32.
131. Gray-Donald K, Payette H, Boutier V, Page S. Evaluation ofthe dietary intake of homebound elderly and the feasibilityof dietary supplementation. J Am Coll Nutr 1994;13:277–84.
132. Lipschitz DA, Mitchell CO, Steele RW, Milton KY. Nutritionalevaluation and supplementation of elderly subjects parti-cipating in a ‘‘meals-on-wheals’’ program. J ParenterEnteral Nutr 1985;9:343–7.
133. Harrill I, Kunz M, Kylen A. Dietary supplementation andnutritional status in elderly women. J Nutr Elder 1981;1:3–13.
134. Welch PK, Dowson M, Endres JM. The effect of nutrientsupplements on high risk long term care residents receivingpureed diets. J Nutr Elderly 1991;10:49–62.
135. Joosten E, Vander Elst B. Does nutritional supplementationinfluence the voluntary dietary intake in an acute geriatrichospitalized population? Aging (Milano) 2001;13:391–4.
136. Brin MF, Younger D. Neurologic disorders and aspiration.Orolaryngol Clin North Am 1988;21:691–9.
137. Daniels SK, Brailey K, Priestly DH, Herrington LR, WeisbergLA, Foundas AL. Aspiration in patients with acute stroke.Arch Phys Med Rehabil 1998;79:14–9.
138. Teasell RW, McRae M, Marchuk Y, Finestone HM. Pneumoniaassociated with aspiration following stroke. Arch Phys MedRehabil 1996;77:707–9.
139. Smithard DG, O’Neill PA, Park C, Morris J, Wyatt R, EnglandR, Martin DF. Complications and outcome after acutestroke—does dysphagia matter? Stroke 1996;27:1200–4.
140. Odderson IR, Keaton JC, McKenna BS. Swallow managementin patients on an acute stroke pathway: quality is costeffective. Arch Phys Med Rehabil 1995;76:1130–3.
141. Smithard DG, Kenwick D, Martin D, O0Neill P. Chestinfection following acute stroke: does aspiration matter?Age Ageing 1993;22(Suppl. 3):24–9.
142. Axelsson K, Asplund K, Norberg A, Eriksson S. Eating problemsand nutritional status during hospital stay of patients withsevere stroke. J Am Diet Assoc 1989;89:1092–6.
143. Gariballa SE, Parker SG, Taub N, Castleden M. Nutritionalstatus of hospitalized acute stroke patients. Br J Nutr1998;79:481–7.
144. FOOD Trial Collaboration. Poor nutritional status onadmission predicts poor outcomes after stroke: observa-tional data from the FOOD trial. Stroke 2003;34:1450–6.
145. Bath PM, Bath FJ, Smithard DG. Interventions for dysphagiain acute stroke. Cochrane Database Syst Rev 2000;CD000323.
146. Broadley S, Croser D, Cottrell J, et al. Predictors ofprolonged dysphagia following acute stroke. J Clin Neurosci2003;10:300–5.
147. FOOD trial collaboration. Effect of timing and method ofenteral tube feeding for dysphagic stroke patients (FOOD):a multicentre randomised controlled trial. Lancet 2005;365:764–72.
148. Taylor SJ. Audit of nasogastric feeding practice at twoacute hospitals: is early enteral feeding associated withreduced mortality and hospital stay? J Hum Nutr Diet1993;6:477–89.
149. Nyswonger GD, Helmchen RH. Early enteral nutrition andlength of stay in stroke patients. J Neurosci Nurs1992;24:220–3.
150. Smithard DG, O’Neill PA, England RE, et al. The naturalhistory of dysphagia following a stroke. Dysphagia 1997;12:188–93.
151. Peschl L, Zeilinger M, Munda W, Prem H, Schragel D.Percutaneous endoscopic gastrostomy—a possibility forenteral feeding of patients with severe cerebral dysfunc-tions. Wiener Klin Wschr 1988;100:314–8.
152. Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke.Br Med J (Clin Res Ed) 1987;295:411–4.
153. Houwing RH, Rozendaal M, Wouters-Wesseling W, BeulensJW, Buskens E, Haalboom JR. A randomised, double-blindassessment of the effect of nutritional supplementation onthe prevention of pressure ulcers in hip-fracture patients.Clin Nutr 2003;22:401–5.
154. Lawson RM, Doshi MK, Barton JR, Cobden I. The effect ofunselected post-operative nutritional supplementation onnutritional status and clinical outcome of orthopaedicpatients. Clin Nutr 2003;22:39–46.
155. Stableforth PG. Supplement feed and nitrogen and caloriebalance following femoral neck fracture. Br J Surg 1986;73:651–5.
156. Morley JE, Kraenzle D. Causes of weight loss in acommunity nursing home. J Am Geriatr Soc 1994;42:583–5.
157. Brozek J. Effects of generalized malnutrition on person-ality. Nutrition 1990;6:389–95.
158. Marcus EL, Berry EM. Refusal to eat in the elderly. Nutr Rev1998;56:163–71.
159. Carver AD, Dobson AM. Effects of dietary supplementationof elderly demented hospital residents. J Hum Nutr Diet1995;8:389–94.
160. Patel PH, Thomas E. Risk factors for pneumonia afterpercutaneous endoscopic gastrostomy. J Clin Gastroenterol1990;12:389–92.
161. Baeten C, Hoefnagels J. Feeding via nasogastric tube orpercutaneous endoscopic gastrostomy. A comparison.Scand J Gastroenterol 1992;194:95–8.
162. Stratton RJ, Ek A-C, Engfer M, et al. Enteral nutritionalsupport in prevention and treatment of pressure ulcers: asystematic review and meta-analysis. Ageing Res Rev2005;4:422–50.
163. Breslow RA, Hallfrisch J, Guy DG, Crawley B, Goldbert AP.The importance of dietary protein in healing pressureulcers. J Am Geriatr Soc 1993;41:357–62.

ARTICLE IN PRESS
D. Volkert et al.360
164. Brown DN, Miedema BW, King PD, Marshall JB. Safety ofearly feeding after percutaneous endoscopic gastrostomy. JClin Gastroenterol 1995;21:330–1.
165. Choudhry U, Barde CJ, Markert R, Gopalswamy N.Percutaneous endoscopic gastrostomy: a randomized pro-spective comparison of early and delayed feeding. Gastro-intest Endosc 1996;44:164–7.
166. McCarter TL, Condon SC, Aguilar RC, Gibson DJ, Chen YK.Randomized prospective trial of early versus delayedfeeding after percutaneous endoscopic gastrostomy place-ment. Am J Gastroenterol 1998;93:419–21.
167. Zarling EJ, Edison T, Berger S, Leya J, DeMeo M. Effect ofdietary oat and soy fiber on bowel function and clinicaltolerance in a tube feeding dependent population. J AmColl Nutr 1994;13:565–8.
168. Grant LP, Wanger LI, Neill KM. Fiber-fortified feedings inimmobile patients. Clin Nurs Res 1994;3:166–72.
169. Shankardass K, Chuchmach S, Chelswick K, et al. Bowelfunction of long-term tube-fed patients consuming for-
mulae with and without dietary fiber. J Parenter EnteralNutr 1990;14:508–12.
170. Nakao M, Ogura Y, Satake S, et al. Usefulness of solubledietary fiber for the treatment of diarrhea during enteralnutrition in elderly patients. Nutrition 2002;18:35–9.
171. Bass DJ, Forman LP, Abrams SE, Hsueh AM. The effect ofdietary fiber in tube-fed elderly patients. J Gerontol Nurs1996;22:37–44.
172. Homann HH, Kemen M, Fuessenich C, Senkal M, Zumtobel V.Reduction in diarrhea incidence by soluble fiber in patientsreceiving total or supplemental enteral nutrition.J Parenter Enteral Nutr 1994;18:486–90.
173. Schutz T, Herbst B, Koller M. Methodology for thedevelopment of the ESPEN Guidelines on Enteral Nutrition.Clin Nutr 2006;25(2):203–9.
174. Lochs H, Allison SP, Meier R, Pirlich M, Kondrup J, SchneiderSt., van den Berghe G, Pichard C. Introductory to the ESPENGuidelines on Enteral Nutrition: Terminology, Definitionsand General Topics. Clin Nutr 2006;25(2): 180–6.