
ESPEN Congress Prague 2007 · Nutrition support in obese patient. Claude Pichard. Nutrition...
43
Nutrition support in obese patient Claude Pichard Nutrition implication of obesity and Type II Diabetes ESPEN Congress Prague 2007
Transcript of ESPEN Congress Prague 2007 · Nutrition support in obese patient. Claude Pichard. Nutrition...

Nutrition support in obese patient
Claude Pichard
Nutrition implication of obesity and Type II Diabetes
ESPEN Congress Prague 2007

Nutrition Support in Obese Patients
Prague, 2007
C. Pichard, MD, PhD, Head Clinical Nutrition, University Hospital, Geneva, Switzerland

1. Protecting lean body mass
- Sarcopenic vs. active
2. Defining energy needs
- Predicting vs. Measuring energy expenditure
3. Defining protein needs
4. Micronutrients
- Well vs. malnourished
Nutrition in Obese Patients: Learning objectives

1. Protecting lean body mass
- Sarcopenic vs. active obese patients2. Defining energy needs
- Predicting vs. Measuring energy expenditure
3. Defining protein needs
4. Micronutrients
- Well vs. malnourished obese patients
Nutrition in Obese Patients: Learning objectives

INDICATIONS and CONTRAINDICATIONS :
About the same as for non-obese patients !
Nutrition SUPPORT in Obese Patients

Body composition measurements during wasting diseasesC. Pichard et al . Curr Op Clin Nutr 1998, 1: 357-61
Water 39.0 kg=55%
Protein 10.5 kg=15%
Fat16.8 kg=24%
Glycogen0.6%
Minerals=5%
Fat-Free Mass (FFM)
Fat Mass (FM)
70 kg

STRUCTURE AVAILABLEENERGY
70 kg kcal
800
Glycogen420 g = 0.6%
Water 39.0 kg=55%
Protein 10.5 kg=15%
Fat16.8 kg=24%
Minerals=5%24’000
120’000
7 kcal/g
60 % (4 kcal/g)
50% (4 kcal/g)

5 11.2 - 16.8
10 15.2 - 20.8
15 19.2 - 24.8
20 23.0 - 29.0
25 26.8 - 33.2______________________________________________
*95% confidence. Hill G.L. J Parent Enteral Nutr 16, 197-218, 1992
Body weight loss (%) Protein loss (%) *(in vivo neutron analysis)

Unvoluntary weight loss during disease is « Autocannibalism »

0%
20%
40%
60%
80%
100%
Normal FFMI& Normal FMI
Low FFMI& Normal FMI
Normal FFMI& High FMI
Low FFMI& High FMI
≥ 11 d
6-10 d
1-5 d
LOS
Prev
alen
ceIncreased length of hospital stay in underweight and
overweight patients at hospital admission:A controlled population study (1707 patients/1707 volunteers)
Kyle UG et al. Clin Nutr. 2005; 24: 133-142

Sarcopenicvs.
Active Obese patients

Fat Mass Lean Body Mass Total Mass
Dual X-ray Absorptiometry (DEXA)

Bioelectrical Impedance Analysis (BIA)

Review of principles & methods.
Clin Nutr 200423: 1226-1243
Utilisation in clinical practice.Clin Nutr 2004
23: 1430-1453
ESPEN GUIDELINESBioelectrical impedance analysis
www.espen.org/education
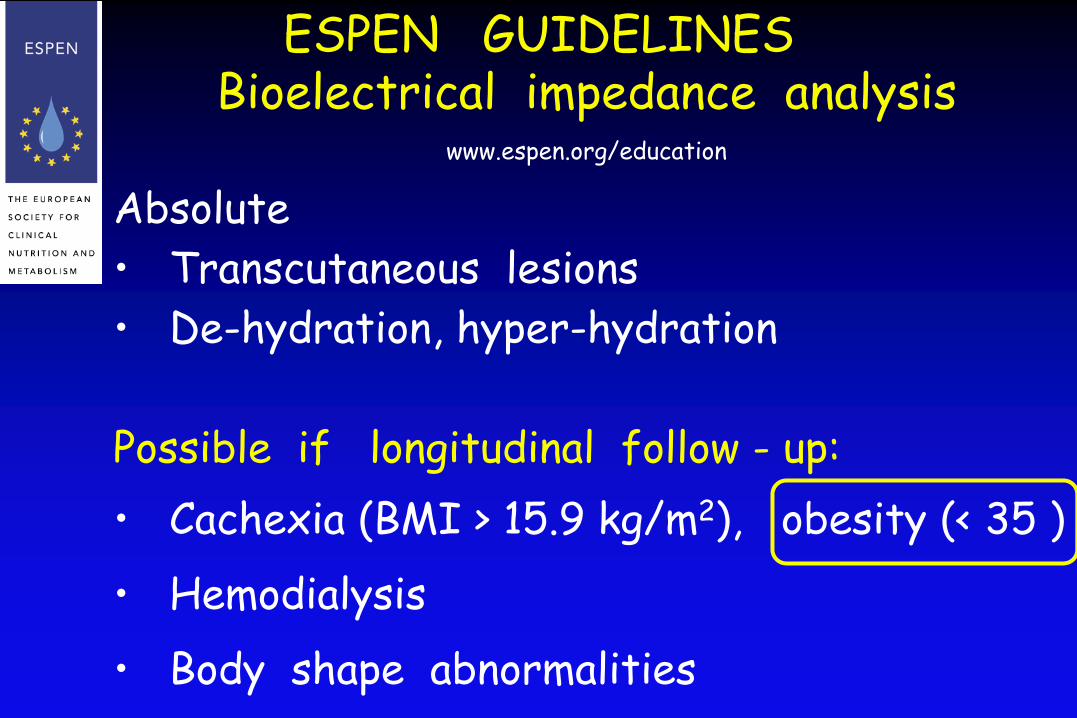
Absolute• Transcutaneous lesions• De-hydration, hyper-hydration
Possible if longitudinal follow - up:• Cachexia (BMI > 15.9 kg/m2), obesity (< 35 )• Hemodialysis• Body shape abnormalities
ESPEN GUIDELINESBioelectrical impedance analysis
www.espen.org/education

1. Protecting lean body mass
- Sarcopenic vs. active obese patients
2. Defining energy needs
- Predicting vs. Measuring energy expenditure3. Defining protein needs
4. Micronutrients
- Well vs. malnourished obese patients
Nutrition in Obese Patients: Learning objectives

69 yrs, 156 cm, Pneumonia, no chronic diseaseUsual BW : ? (72 kg nine years ago)Estimated : 115-118 kg Measured :104 kg

Predicting EE in Extremely Obese WomenDobratz JR. JPEN 2007, 31: 217-227
N= 14, BMI 49.8 6.2, 49 +- 10 yrs
- EE : indirect calorimetry
- EQUATIONS:
Harris-Benedict (actual BW)
Cunningham
Mifflin-St Jeor
Owen
World Health Organization
Bernstein

Predicting EE in Extremely Obese WomenDobratz JR. JPEN 2007, 31: 217-227
« The Mifflin-St Jeor equation was most accurate »
Harris-Benedict:Women: 665.09 + (9.56 × wt) + (1.84 × ht) - (4.67 × age)
-> 2045 +/- 215 kcal/d
Mifflin-St Jeor :Women: -161 + (9.99 × wt) + (6.25×ht) - (4.92 x age)
-> 2005 +/- 240 kcal/d

0
400
800
1200
1600
Males(n=64)
Females(n=55)
Total(n=119)
Measured RMR compared to estimated RMR
* Significant difference between measured and estimated RMR (p<0.05)
* *
* * * *
RMR
mea
sure
d
Har
ris B
ened
ict
WH
O/F
AO/U
NU
RMR
mea
sure
d
RMR
mea
sure
d
Har
ris B
ened
ict
Har
ris B
ened
ict
WH
O/F
AO/U
NU
WH
O/F
AO/U
NU
Comparison of equations for estimating resting metabolic rate in healthy subject over 70 years of age
Melzer K et al. Clin Nutr 2007, 26: 498 - 5005
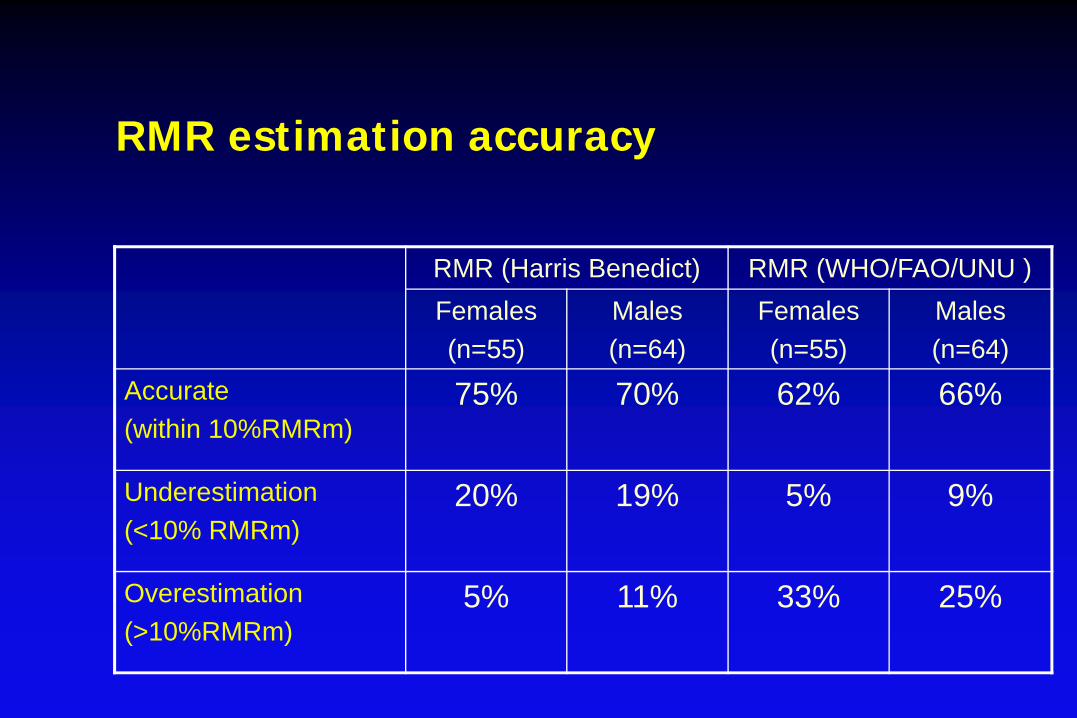
RMR (Harris Benedict) RMR (WHO/FAO/UNU )Females (n=55)
Males(n=64)
Females(n=55)
Males(n=64)
Accurate(within 10%RMRm)
75% 70% 62% 66%
Underestimation(<10% RMRm)
20% 19% 5% 9%
Overestimation(>10%RMRm)
5% 11% 33% 25%
RMR estimation accuracy

Agreement between RMRm and RMRe(Bland and Altman)
200018001600140012001000800
(RMR(Harris Benedict) + RMRm)/2
500
250
0
-250
-500
RM
R(H
arris
Ben
edic
t) -R
MR
m femalesmalesSex
+2 SD
Mean
-2 SD

• Large discrepencies exist between EE predicting formula.
• HB formula performs best.
• Develop more accurate formula including body composition markers
Comparison of equations for estimating resting metabolic rate
In healthy subjects over 70 years of age
Melzer K et al. Clin Nutr 2007, 26: 498 - 5005
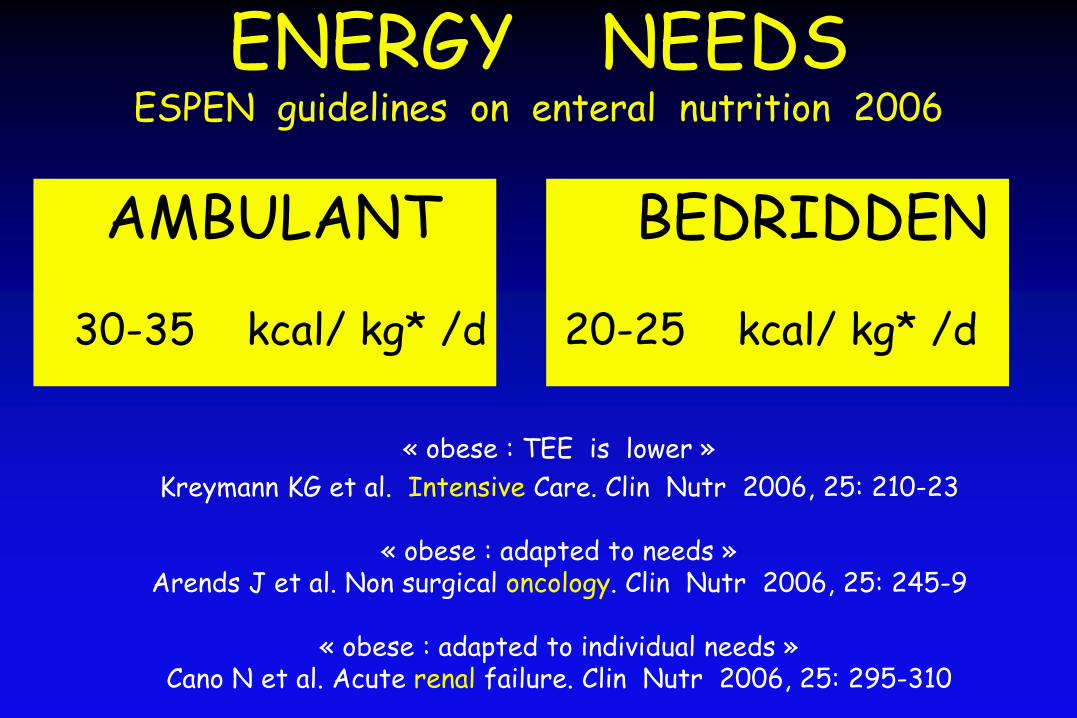
ENERGY NEEDSESPEN guidelines on enteral nutrition 2006
AMBULANT BEDRIDDEN
30-35 kcal/ kg* /d 20-25 kcal/ kg* /d
« obese : TEE is lower »Kreymann KG et al. Intensive Care. Clin Nutr 2006, 25: 210-23
« obese : adapted to needs »Arends J et al. Non surgical oncology. Clin Nutr 2006, 25: 245-9
« obese : adapted to individual needs »Cano N et al. Acute renal failure. Clin Nutr 2006, 25: 295-310

ENERGY NEEDS in OBESE Patients
« Geneva »
30-35 kcal/ kg* / d
* Ideal body weight
If « ambulant »:IBW + 20% for
increased Fat-free mass

Calorimetry required if « chronic acute » care or sarcopenia

1. Protecting lean body mass
- Sarcopenic vs. active obese patients
2. Defining energy needs
- Predicting vs. Measuring energy expenditure
3. Defining protein needs4. Micronutrients
- Well vs. malnourished obese patients
Nutrition in Obese Patients: Learning objectives

+10
0
-10
-20
-2 0 +2 +4 +6
NitrogenBalance
(mg/kg/d)
Protein Utilization Depends on Energy Availability
Estimated Energy Balance (kcal/kg/d)
Rombeau J.L. In Clinical Nutrition. Enteral & Tube Feeding. 1990

Protein Needs1.2 – 1.5 g / kg* / d
* Ideal body weight
If « active »:IBW + 20% for increased Fat-free mass
+ compensate in case of severe losses

1. Protecting lean body mass
- Sarcopenic vs. active obese patients
2. Defining energy needs
- Predicting vs. Measuring energy expenditure
3. Defining protein needs
4. Micronutrients
- Well vs. malnourished obese patients
Nutrition in Obese Patients: Learning objectives

Why is malnutrition underrecognized ?

Malnutrition
• Financial• Social• « Practical »• Medical….
(Bariatric surgery)
« Obesity does not protect you frommicronutrients deficiencies »

Conclusion

PROACTIVE NUTRITION
« to prevent adverse effectsrelated to poor nutritional status
among high - risk populations »
August DA. JPEN 1996, 20: 394-400

1. Feeding obese patients : same indications & contra-indications
than in non-obese
2. Protecting lean body mass : prevent loss -> be proactive !
3. Defining energy needs : HB or 30-35 kcal /kg (IBW)/ d
Calorimetry required if « chronic acute » care or sarcopenia
4. Defining protein needs: 1.2-1.5 g /kg (IBW)/ d
5. Detecting micronutrients deficits: energy excess = balanced
intakes
Nutrition in Obese Patients: Learning objectives



5
10
15
20
25
30
35
40
45
50
15-24 25-34 35-44 45-54 55-64 65-74 75-84 >85
Women
Age (years)
95th90th
75th
50th
25th10th5th
Percentiles of Fat Mass in 5225 VolunteersKyle U. et al. Nutrition 2001, 17:534-541
Women
KgKG

8070605040302010030
34
38
42
46
50
54
hommefemme
DEPENSE ENERGETIQUE
ans
kcal
/ m2/
heu
re
Fleisch A. Helv Med Acta 1951;1:23-44
Energy requirements alter with advancing age due to1:
• reduction in the intensity and frequency of physical activity• loss of fat-free mass• decline in Na+-K+- ATPase activity• decrease in muscle protein turnover, and • alteration in mitochondrial membrane proton permeability
1 Wilson MM, Morley JE. Invited review: aging and energy balance. J Appl Physiol 2003;95:1728-36.
Accurate estimation of individual energy requirements is necessaryfor establishing adequate caloric prescriptions.

Agreement between RMRm and RMRe (Bland and Altman)
200018001600140012001000800(RMR(WHO/FAO/UNU) + RMRm)/2
500
250
0
-250
-500
RM
R(W
HO
/FA
O/U
NU
) -R
MR
m femalesmalesSex
+ 2SD
Mean
-2SD
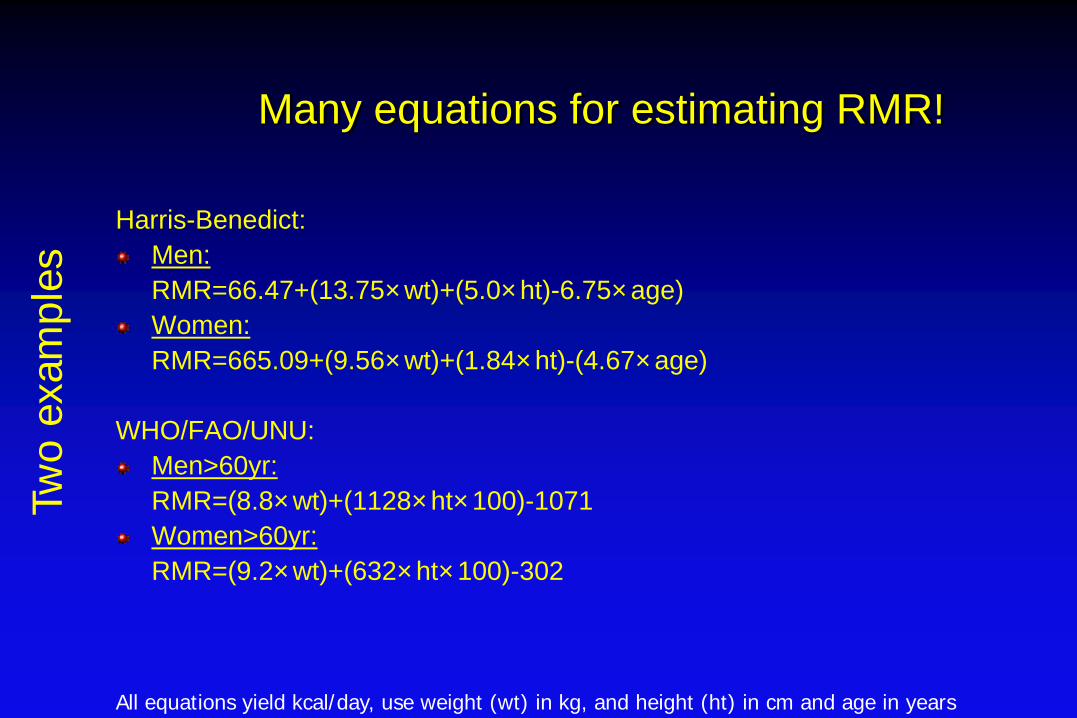
Many equations for estimating RMR!
Harris-Benedict:Men:RMR=66.47+(13.75×wt)+(5.0×ht)-6.75×age)Women:RMR=665.09+(9.56×wt)+(1.84×ht)-(4.67×age)
WHO/FAO/UNU:Men>60yr:RMR=(8.8×wt)+(1128×ht×100)-1071Women>60yr:RMR=(9.2×wt)+(632×ht×100)-302
All equations yield kcal/day, use weight (wt) in kg, and height (ht) in cm and age in years
Two
exam
ples


















