ESPEN Congress Florence · PDF fileESPEN Congress Florence 2008 ... NCP 21:438, 2006. Trace...
38
ESPEN Congress Florence 2008 The long-term ICU patient Micronutrient requirements of the long-term ICU patient Mette M. Berger (Switzerland)
Transcript of ESPEN Congress Florence · PDF fileESPEN Congress Florence 2008 ... NCP 21:438, 2006. Trace...

ESPEN Congress Florence 2008
The long-term ICU patient
Micronutrient requirements of the long-term ICU
patient
Mette M. Berger (Switzerland)

Micronutrient requirements of the long-term ICU patient
Mette M. Berger Dpt of Intensive Care Medicine & Burns
CHUV – Lausanne - Switzerland
25

« Long-term » ICU patient
ICU treatment > 7 days? > 14 days ?
Persistent organ failure
What about the gut?
Organ failure by SOFA score
Cardio / resp / renal / liver (bili) / hemato / neuro
What about the gut?

Essential MicronutrientsTrace elements (10) Vitamins (13)
Cu Copper A Retinol
Se Selenium D Cholecalciferol
Zn Zinc E Alpha-tocopherol
Fe Iron K Phyloquinone
Mn Manganese B1 Thiamin
Mo Molybdenum B2 Riboflavin
Cr Chromium B3 Niacin(PP)
F Fluoride B5 Pantothenic acid
I Iodide B6 Pyridoxine
Co Cobalt B8 Biotine(H)
B9 Folic acid
B12 Cobalamin
+ 4 Ni, Si, Sn, V C Ascorbic acid

Micronutrients FunctionsNutrition + Prevention of deficiencies: Anabolism enzyme cofactors of carbohydrate,
lipid and protein metabolism
Immunity Humoral: immunoglobulin production
Cellular: macrophages, neutrophil, lymphocytes
Regulation Gene expression
AOX defence Confine free radicals in defined spaces and [ ]
Modulation of the extension of acute diseases
Prevention of chronic diseases

The argument for selenium intake in EuropeRayman MP, Proceedings of the Nutrition Society 61: 203
2002
Recent mean levels of serum or plasma Se in Europe compared with (---),
bottom tertile in Nutritional Prevention of Cancer (NPC) trial of Clark et al.
(1996); (·····), level required for optimal plasma GPx activity

Monitoring micronutrients – why ?
Some pathologies are associated with altered
absorption (pernicious anaemia, bariatric surgery,
inflammatory bowel diseases, celiac disease)
Some conditions losses: inflammatory bowel
disease, fistulae, burns, haemorrhage
Some of our therapies directly deplete the
patients of hydrosoluble micronutrients such as
renal replacement therapies, drains
Status is unpredictable Hyper- & Hypo- both deleterious

Chronic conditions – bariatric surgeryInflammatory bowel diseasesFluid resuscitation
Absorption issues

Nutritional follow up after gastric bypassGasteyer et Giusti, Rev Med Suisse, 2:844, 2006
0
20
40
60
80
100
3 6 12 18 24
Time after bypass (months)
% substitutionMicronutrient
Bariatric surgery

Impact of fluid resuscitation on visceral edemaKinsky MP et al, J Trauma, 49: 844 2000
Tissue water content for
colon, ileum, kidney,
liver, pancreas, and
skeletal muscle.
Mean ± SEM from 9 to
12 animals per group.
Asterisk indicates p < 0.05,
HSD (7.5% NaCl/6% dextran
70) versus LR; [psi], p < 0.05,
HSD vs nonburned skin;
[delta], p < 0.05, LR vs
nonburned skin.

The ICU patient
Impact on micronutrient status
Oxidative stress
Inflammation
Organ failure

Trace elementsAcute phase response
Shenkin, Nutrition 11:100, 1995
0
5
10
15
20
25
µm
ol /
L
-16 -8 0 8 16 24 32 40 48
Time (hours)
Incision
Cu
Fe
Zn

Oxidative stress and metallothionein expression - liver of rats with severe thermal injury Ding et al Burns, 28:215, 2002
Effects of severe thermal injury on the zinc concentrations both in the serum
and in the liver. mean±sem, n=5. *P<0.001, **P<0.01 and # P<0.05 vs. the
corresponding normal control

Negative balances – the causes in critically illBerger, NCP 21:438, 2006
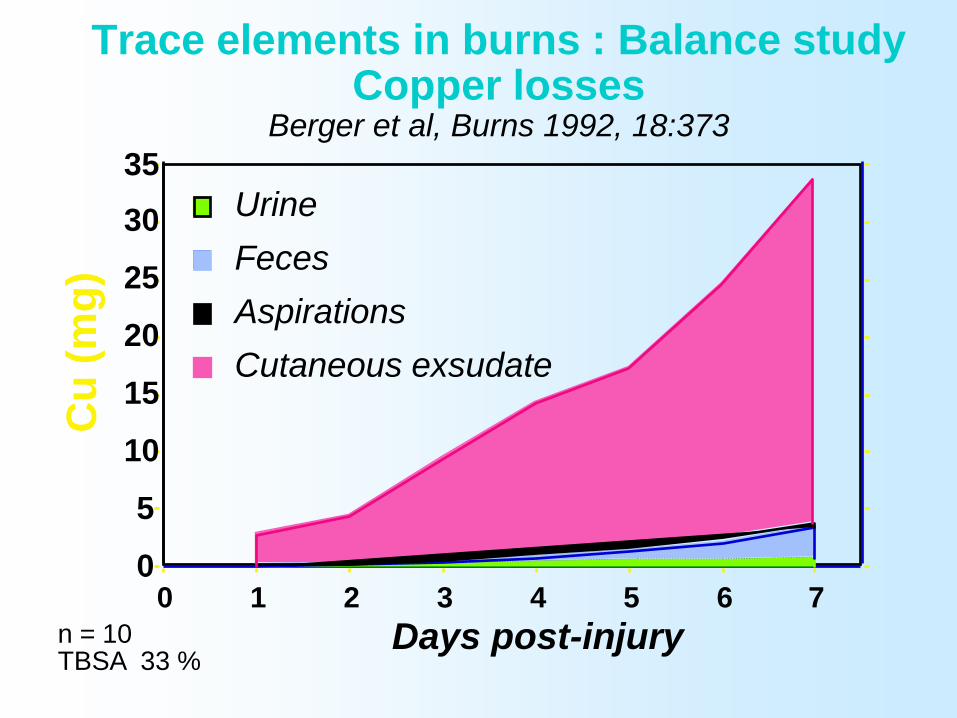
Trace elements in burns : Balance study Copper losses
Berger et al, Burns 1992, 18:373
n = 10TBSA 33 %
0
5
10
15
20
25
30
35
Cu
(m
g)
0 1 2 3 4 5 6 7
Days post-injury
Cutaneous exsudate
Aspirations
Feces
Urine

Se balances after major trauma Berger MM et al, J Trauma, 40:103, 1996
-100
-75
-50
-25
0
25
µg
/ 2
4h
0 1 2 3 4 5 6 7
Days post-injury
Selenium
n = 11x ± sd

Micronutrient losses during CVVHBerger MM et al, Amer J Clin Nutr, 410, 2004
Plasma Cu, Se, Zn, and thiamine in effluents from patients with acute renal failure under
CRRT with either Na-bicarbonate (Bic group; Full) or Na- lactate (Lac group; )

Trace Elements RequirementsChanging paradigms
Controversies regarding how to establish recommended intakes
Making universal recommendations among the different ecologic, anthropologic, and geographic settings appears futile
Lower than normal body stores may be adaptiveGaps in our knowledge regarding the bases of
nutrient requirementsTE are inorganic: potential for accumulation (Cu,
Fe, Mn) and toxicityScientists must produce new evidences
Solomons & Ruz, 1998

New integrative concept Dietary Reference Intakes (DRI)
Set of 4 reference values:
Estimated Average Requirements (EAR)
Recommended Dietary Allowances (RDA)
Adequate Intakes (AI)
Tolerable Upper Intake Levels (UL)

Antioxidants - Synergisms
ROOH, ROH Tocopheryl Ascorbate GSSG NADPHradical
Vitamin E Vitamin C
ROO-, RO
- Tocopherol Dehydro- GSH NADP Ascorbate

Malnutrition and InfectionAlternative model - Beck MA 1999
Malnutrition
Micronutrient deficiency
Immunity virus virulence Susceptibility to pathogens
(viral, bacteria, fungi)
Infections
Oxidative stress

Critically ill
Requirements
Supplementation Trials

Micronutrient supplementation – AimsBerger & Shenkin, Curr Opin Clin NutMC,
9:711,2006
Nutritional effect (intermediate metabolism)
Substituting for losses = restore normal status
and enzyme activity
Providing supranormal status = pharmacological
AOX action
Decrease and shorten the inflammatory response

Can oxidative damage be treated nutritionally?
Berger MM Clin Nutr, 2005
Nutritional
AOX intake
AOX defence
Qu
an
tity
Oxidative
damage
Normal
range
Time (minutes years)
Injury – Acute disease
1
2

Trace element in Burns – Plasma TE, GSHPx
Berger et al, 2006, submitted
Higher plasma Se &
Gshpx
concentrations in
TE group
from day 5.

Antioxidants TE in major burnsMDA with trace element
supplementsBerger & Chiolero, Burns, 21: 507, 1995
Design: PCT
11 patients
(5 / 6)
BSA 42 / 43 %
- control: ø
- TE: Cu,Se,Zn
Urine:
24 hr collection
p < 0.030
50
100
150
200
1 2 3 4 5 6 7 10 15 20 Days
MDA (µmol/24hr)
Group C
Group TE
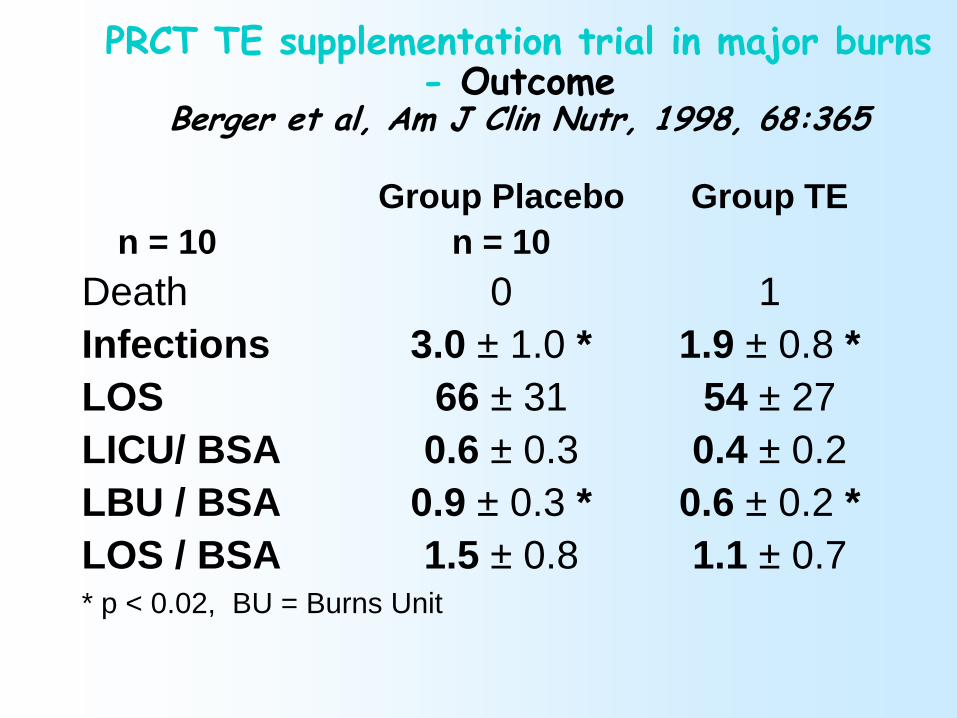
PRCT TE supplementation trial in major burns- Outcome
Berger et al, Am J Clin Nutr, 1998, 68:365
Group Placebo Group TE
n = 10 n = 10
Death 0 1
Infections 3.0 ± 1.0 * 1.9 ± 0.8 *
LOS 66 ± 31 54 ± 27
LICU/ BSA 0.6 ± 0.3 0.4 ± 0.2
LBU / BSA 0.9 ± 0.3 * 0.6 ± 0.2 *
LOS / BSA 1.5 ± 0.8 1.1 ± 0.7* p < 0.02, BU = Burns Unit

Trace element in Burns – Tissue Se, Zn & GSH…Berger et al, 2006, submitted
p < 0.01
p < 0.02

Time to first
Nosocomial
Pneumonia
N = 41
Burns 45% BSA
p=0.002 by
stratified
Log rank test
Trace element in burns – Nosocomial pneumoniaBerger et al, Critical Care 2006 in press

Selenium in ICU SIRS-sepsis patients – PRCTAngstwurm et al- CCM 2006 in press
249 patients in severe sepsis or septic shock: 1000 mcg Se or placebo daily for 2 weeks after a loading dose
Kaplan -Meier survival curves in patients by intention to treat analysis. Difference between groups by log rank test.
The estimated mean survival time was 19.7 days in Se1 patients (bold line) versus 16.4 days in the Se0 group (dotted line) (p = 0.0476).

EN enriched with carotenoids normalizes the carotenoid status and oxidative stress in long-
term enterally fed patientsVaisman N et al, Clin Nutr 2006, 25:897
PRCT : 2 x 25 patients: Mean serum carotenoid levels (ng/ml)
and CI; low dose carotenoid mixture (3 mg/1500 kcal: Nutrison® Nutricia)

EN enriched with carotenoids normalizes the carotenoid status and oxidative stress in long-
term enterally fed patientsVaisman N et al, Clin Nutr 2006, 25:897
NFkB and MDA evolution
More is not always better !
Vitamins: lack of a salutary effect consistently for various doses (Vit E 50-800 IU) of vitamins in diverse populations Vivekananthan DP et al Lancet.
2003;361:2017
High-dosage vit. E supplements may increase all-cause mortality Miller RD et al Ann Intern Med, 2005 142:37
Specific forms of tocopherol in excess may be toxic (tocotrienols). Warrants strategic investment into the lesser known forms of vitamin ESen et al, Life Sci, 2006;78(18):2088

Dose response curveB
iolo
gic
ca
l activity
A+B+C deficieny, D suboptimal, E optimal, G toxicity, H lethal

Effect of excessive micronutrient intakes
Chromium >3mg Spinal / joint degeneration,
immunity problems
Copper > 5mg behavioural problems, vascular
defects, infections, anemia, Wilson’s d
Iron vomiting, diarrhoea, metabolic acidosis,
hyperglycemia
Manganese neuro: extrapyramidal symptoms
Selenium > 750 mcg/d Deiodination, hair + nail discoloration
Zinc > 50 mcg/d immunity
Vitamin C > 1 g/d oxalosis, acute RF
Vitamin E > 150 mg/d mortality
Micronutrients - Why monitor?
Status is unpredictable
Absorption uncertain with bowel oedema
Hypo-status deleterious
–Deficiency associated with altered immune and
AOX defences
Hyper-status deleterious too: toxicity
You can do something about the status
Targets can be defined for some micronutrients:
plasma levels/activities
Helps defining length of supplementation
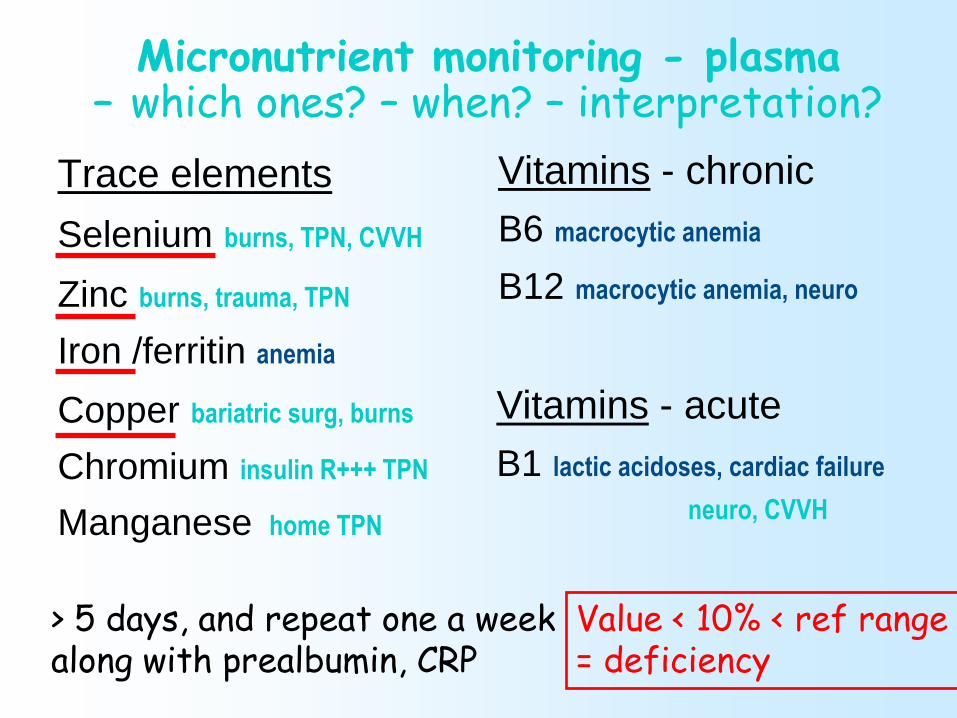
Micronutrient monitoring - plasma– which ones? – when? – interpretation?
Trace elements
Selenium burns, TPN, CVVH
Zinc burns, trauma, TPN
Iron /ferritin anemia
Copper bariatric surg, burns
Chromium insulin R+++ TPN
Manganese home TPN
Vitamins - chronic
B6 macrocytic anemia
B12 macrocytic anemia, neuro
Vitamins - acute
B1 lactic acidoses, cardiac failure
neuro, CVVH
> 5 days, and repeat one a weekalong with prealbumin, CRP
Value < 10% < ref range= deficiency

Micronutrient requirements of the long-term ICU patient
Conclusions
Oxidative stress present in most acute conditions and persist with long stay
Critically ill have an altered micronutrient status, with
of circulating levels acute phase response losses
Several micronutrients (Se, Zn, carotenoids, vit C, vit E) are essential for AOX defence which can be restored by supplements
Monitoring weekly: burns, supplemented, long stays