ESPEN Congress Copenhagen 2016 · ESPEN Congress Copenhagen 2016 BUILDING EVIDENCE IN CLINICAL...
15
SURROGATE MEASURES FOR CLINICAL OUTCOME J.R. Andersen (DK) ESPEN Congress Copenhagen 2016 BUILDING EVIDENCE IN CLINICAL NUTRITION- HOW TO DO WITHOUT RANDOMIZED CONTROLLED TRIALS
Transcript of ESPEN Congress Copenhagen 2016 · ESPEN Congress Copenhagen 2016 BUILDING EVIDENCE IN CLINICAL...
SURROGATE MEASURES FOR CLINICAL OUTCOME
J.R. Andersen (DK)
ESPEN Congress Copenhagen 2016BUILDING EVIDENCE IN CLINICAL NUTRITION- HOW TO DO WITHOUT RANDOMIZED CONTROLLED TRIALS
Jens Rikardt Andersen
Department of Nutrition, Exercise and
Sports
University of Copenhagen, Denmark
27/09/2016 1
A surrogate outcome measure is
A laboratory measurement
A physical sign
Another intermediate substitute, that is able to
predict an interventions effect on a clinically
meaningful outcome
A clinical outcome detects how a patient feels,
functions or survives
27-09-2016 2
We know surrogate measures from the area of
cardio-vascular diseases – plasma cholesterol
and blood pressure as well known examples
These measurements are correlated to
survival, risk of myocardial infarction, stroke
etc as the correspondent clinical outcome
The changes in the surrogate measure is much
faster than the correspondent clinical, and
much easier to use in practice
These surrogates have predictive value
27-09-2016 3
A surrogate outcome measure occurs
faster or more often,
is cheaper
and/or less invasively achieved than the clinicaloutcome
In practice validation of a surrogate outcome is surprisingly often overlooked, especially if a biological plausible rationale is proposed
Surrogate outcomes must be validated before usein the ideal world – but in clinical practice, we have to find ways until such validations are documented
27-09-2016 4
First step: correlation between surrogate and
clinical outcome?
Second step: do the interventions effect on the
surrogate outcome predict the interventions effect
on the clinical outcome?
Third step: is the surrogate meausure valid for
groups or individuals (to which extent can you use
the measure in the treatment of the individual
patient?
To my knowledge no surrogate measure fulfills all
these demands, so what do we do in clinical
practice?
27-09-2016 5
Traditionally weight (weight-loss) has been the dominating variable used to predict clinicaloutcomes as mortality, risk of infectiouscomplications, risk of thrombosis during hospital stay etc
Now we know that body-composition is veryimportant, so weight is often substituted with LBM (lean body mass)
On the other hand we know, that a lot of confounders emerge: hydration in the acutephase, deposition of fat in the long run
We have major problems in finding practical solutions for these problems
27-09-2016 6
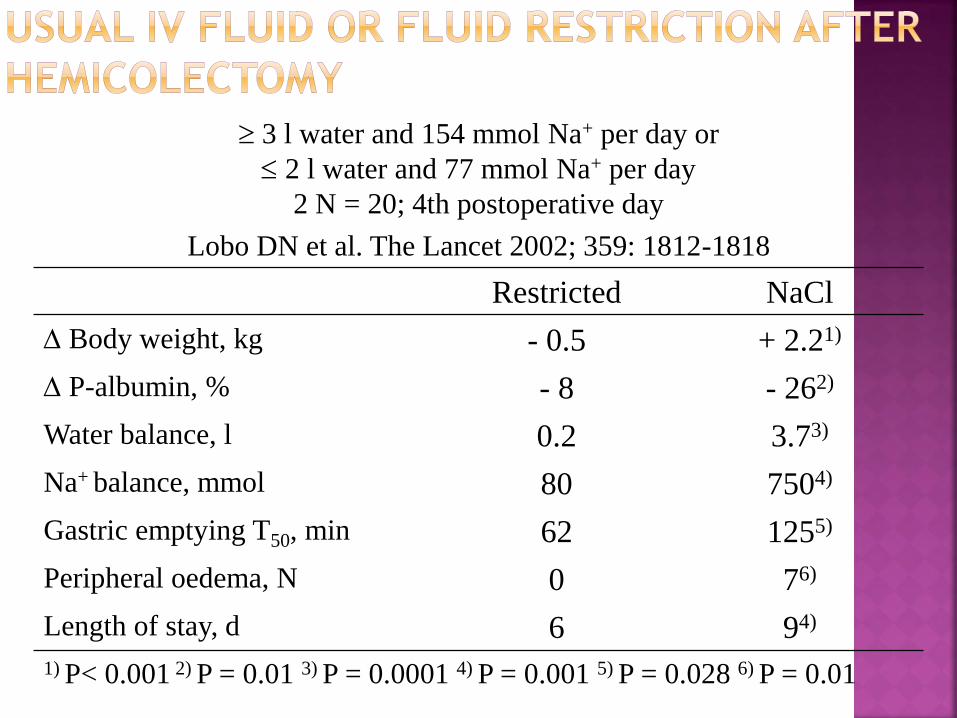
3 l water and 154 mmol Na+ per day or
2 l water and 77 mmol Na+ per day
2 N = 20; 4th postoperative day
Lobo DN et al. The Lancet 2002; 359: 1812-1818
Restricted NaCl
Body weight, kg - 0.5 + 2.21)
P-albumin, % - 8 - 262)
Water balance, l 0.2 3.73)
Na+ balance, mmol 80 7504)
Gastric emptying T50, min 62 1255)
Peripheral oedema, N 0 76)
Length of stay, d 6 94)
1) P< 0.001 2) P = 0.01 3) P = 0.0001 4) P = 0.001 5) P = 0.028 6) P = 0.01
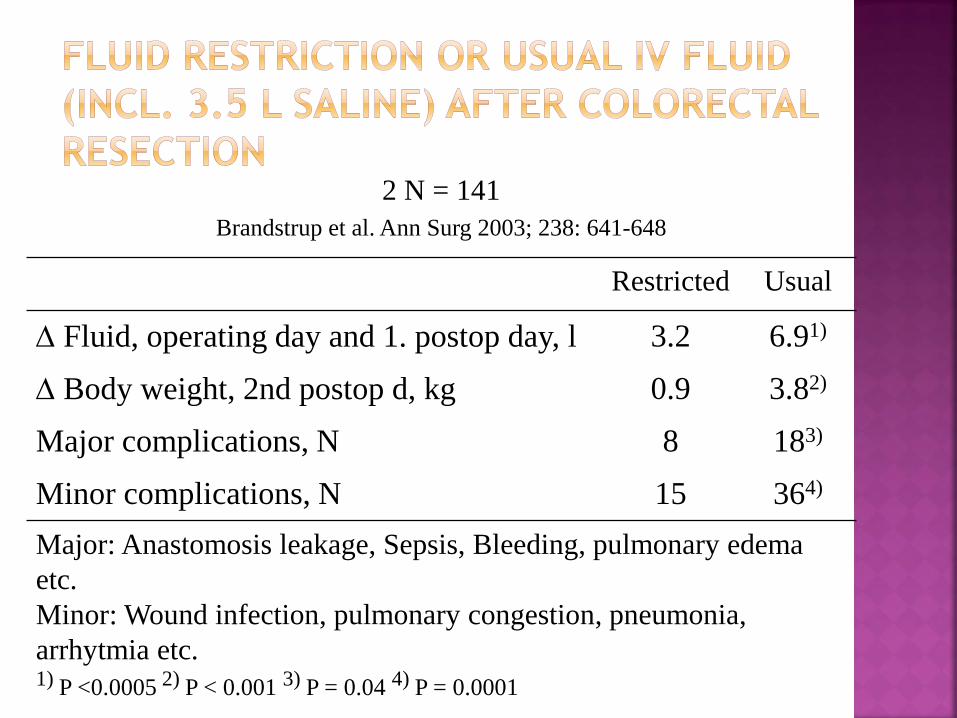
2 N = 141
Brandstrup et al. Ann Surg 2003; 238: 641-648
Restricted Usual
Fluid, operating day and 1. postop day, l 3.2 6.91)
Body weight, 2nd postop d, kg 0.9 3.82)
Major complications, N 8 183)
Minor complications, N 15 364)
Major: Anastomosis leakage, Sepsis, Bleeding, pulmonary edema
etc.
Minor: Wound infection, pulmonary congestion, pneumonia,
arrhytmia etc.1) P <0.0005 2) P < 0.001 3) P = 0.04 4) P = 0.0001
The hypothesis is that nutrients (glucose) feed
the mitochondrium and increase muscle cell
contraction (myosine shortness in the sarcomer)
Is that the only factor involved?
Perfusion of the muscle? Physical training
Motivation? Psychological fitnes, no concentration
Pain in the arm or hand?
27-09-2016 9
It is now well established, that p-albumine is not a good estimate of the nutritional state
P-albumine is affected by hydration
P-pre-albumine is used by some to get an estimateof albumine production
Albumine synthesis is decreased when the synthesis of acute phase reactants are increasedand gluconeogenesis is accellerating (i.e. stress-metabolism)
May be p-albumine is valuable in describingextreme malnutrition in refugee camps, but probably only in steady-state conditions (noinfection)
27-09-2016 10
Energy and protein intake in relation to estimatedneeds
N-balance
P-tranferrin
Anthropometric measurements
Skin test for delayed hypersensitivity
Lymphocyte count
An investigation of the concordance (allthoughbased on underpowered trials) between thesemeasurements and valid clinical outcomes (so-called ”hard endpoints”) – NO CONCORDANCE
(Koretz. Proc Nutr Soc 2005;64:277-84)
27-09-2016 11
ADL - Activities of Daily Living (multiple questionaires and
Time to ability to resume habitual activities (work, hobby)
Quality of life (multiple questionaires)
Muscle strenght (remember, that strenght without muscle
co-ordination is rarely usefull)
Estimates of LBM:
Frequent DXA-scans are probably not possible inless new
technologies are developed
BIA has its pitfalls, but the technology is under fast
improvement
Blood-tests: Hardly usefull in general, but may be in
selected patients
27-09-2016 12
Unless the nutritional problem is one of shortage
of micro- or macronutrients the clinical outcomes
depend on nutrition in combination with other
kinds of therapies (surgery, antibiotics, drugs etc)
We have to accept that and choose a combined
clinical outcome (and may be a suurogate for that
particular outcome)
Follow-up is therefore essential for nutritional
therapy as well as other kinds of therapy
Clinical Nutrition is a discipline for co-operation
with other disciplines – but also an important one
27-09-2016 13
Does the patient improve in a reasonable manner?
Is the improvement important for the patient´slife (or merely a measurement, that satisfies the therapeutic system)?
Is the improvement a real improvement or a slower development of expected problems?
Can problems in any way be related to metabolism(nutrients, the oxydation or excretion)?
Is the patient compliant to advices given? (If no –change the therapy instead of the patient)
At which time-point is follow-up not necessary anylonger?
27-09-2016 14