ESP Nephropathology WG Slide Seminar (Krakow 2010) “D RUGS AND KIDNEY ” Case No. 6
23
ESP Nephropathology WG ESP Nephropathology WG Slide Seminar Slide Seminar (Krakow 2010) (Krakow 2010) “D “D RUGS AND KIDNEY RUGS AND KIDNEY ” ” Case No. Case No. 6 6 Dušan Ferluga Institute of Pathology, Faculty of Medicine University of Ljubljana, Ljubljana, Slovenia
description
ESP Nephropathology WG Slide Seminar (Krakow 2010) “D RUGS AND KIDNEY ” Case No. 6. Du š an Ferluga Institute of Pathology, Faculty of Medicine University of Ljubljana, Ljubljana, Slovenia. Medical history (I) of a 46-year-old woman. 1974 (age 13) - Juvenile rheumatoid arthritis - PowerPoint PPT Presentation
Transcript of ESP Nephropathology WG Slide Seminar (Krakow 2010) “D RUGS AND KIDNEY ” Case No. 6

ESP Nephropathology WG ESP Nephropathology WG Slide Seminar Slide Seminar (Krakow 2010)(Krakow 2010)
“D“DRUGS AND KIDNEYRUGS AND KIDNEY””Case No. Case No. 66
Dušan Ferluga
Institute of Pathology, Faculty of Medicine University of Ljubljana, Ljubljana, Slovenia

Medical history (I) Medical history (I) of a 46-year-old womanof a 46-year-old woman
1974 (age 13) - Juvenile rheumatoid arthritis1974-83 - Th: corticosteroids, gold, NSAID1983 (age 22) - Overlapping SLE (5 ARA: butterfly rash,
arthritis, ANA pos, a-dsDNA pos 0.98, proteinuria 1.1 g/d)
1st renal biopsy Class I, ID mes ++, sed +, sep+-/+1983-89 - Th: Cyclophosphamide pulses,
corticosteroids Remission of most symptoms, release of laboratory findings
Recurrent deep vein thrombosis assoc. IgG aCL in high titer Dg. APS Th warfarin

1st kidney biopsy in 1983 (age 22)1st kidney biopsy in 1983 (age 22)
Medulla and cortex with 9 glomeruli
ISN/RPS Class I (min mes lupus nephritis)
IA 0, IC 0
IF: »full-house« glom mes ID
EM: dense deposits mesangial/paramesangial ++,
sparse, segmental sed+, sep+-/+,
endothelial TRI myxovirus-like +,
no myelin-like cytoplasmic inclusions

1st kidney biopsy

1st kidney biopsy – EM

Medical history (II) Medical history (II) of a 46-year-old womanof a 46-year-old woman
1989 (age 30) - ANA pos, a-dsDNA low pos 0,452000 (age 41) - Positive skin biopsy band test by DIF
Urinalysis: norm2001 (age 42) - ANA pos 1:640, ENA pos HTE 1,
a-dsDNA pos 0.86, IgG aCL pos (>30) Th: cyclosporin (RR) replaced
methothrexate (side effects) replaced2001-2006 - Th: chloroquine 250 mg/d (cumul. 413 g)

Clinical / laboratory findings Clinical / laboratory findings at 2nd biopsyat 2nd biopsy
2006 (age 46) - Lab parameters of inflamm (SR, CRP) low
Reduced joint swelling and pain,
ARA criteria not fulfilled (SLE in remission?)
S-creatinine 150 µmol/L () Urinalysis: proteinuria 0.25-0.5 g/d,
mild erytrocyturia and leukocyturia
2nd renal biopsy

2nd kidney biopsy in 2006 (age 46)2nd kidney biopsy in 2006 (age 46)
Medulla and cortex with 14 glomeruli
LM: Widespread global (8/14) and segmental (1/14) glomerulosclerosisFocal (25%) interstitial fibrosis and tubular atrophyModerate arteriosclerosis and arteriolosclerosis
IF: Glom mesangial IgG, IgM and C3 in traces () EM: Traces of dissolved mesangial and subepithelial
deposits. No features of active lupus nephritis. A variety of cytoplasmic inclusions in renal cells
Dg.: 1. Class I lupus nephritis resolved (Class IVG (C)?) 2. FSGS, coincidental drug-induced?

2nd kidney biopsy
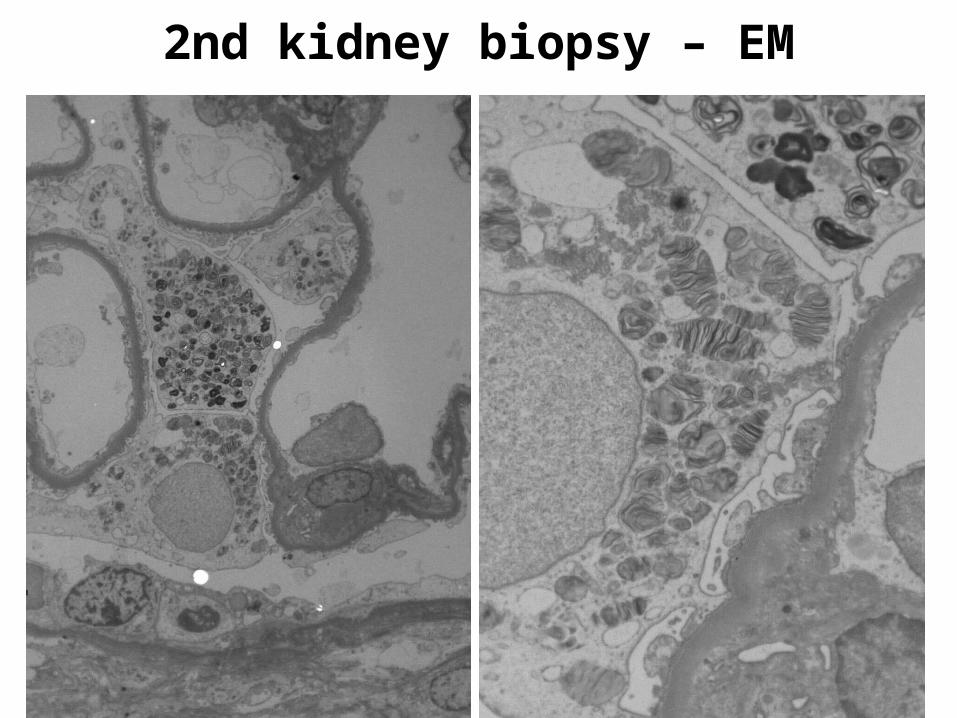
2nd kidney biopsy – EM

2nd kidney biopsy – EM

2nd kidney biopsy – EM

2nd kidney biopsy in 2006 (age 46) CONCLUSION
EM: Numerous myelin- and zebra-like lamellar cytoplasmic inclusions, irregularly distributed in variety of renal cells are ultrastructural features compatible with those of Fabry disease, particularly in heterozygous woman. However, additional findings of peculiar curvilinear bodies, convincibly demonstrated in vascular smooth muscle cells and one of the glomerular mesangial cells are highly suggestive of iatrogenic chloroquine-induced renal phospholipidosis.

Skin biopsy – EM

First skeletal muscle biopsy – EM

Second skeletal muscle biopsy – EM (6 months after chloroquine withdrawal)

Skin and skeletal muscle biopsies (age 46)
EM: Myelin-like and occasionally zebra-like lamellar cytoplasmic inclusions were demonstrated in the sarcoplasm of myofibers and in a variety of cells in the skin biopsy.
Associated curvilinear cytoplasmic bodies, present in abundance in the sarcoplasm of myofibers and to lesser extent in the vascular smooth muscle cells.
Complete clearance of lamellar inclusions but remnants of curvilinear bodies in follow-up skeletal muscle biopsy six months after chloroquine withdrawal.

Final diagnosis:
IATROGENIC CHLOROQUINE-INDUCED SYSTEMIC PHOSPHOLIPIDOSIS
mimicking Fabry disease

Arguments confirming final diagnosis:
Curvilinear cytoplasmic inclusions in addition to myeloid and zebra bodies
Slowly progressive renal insufficiency and biopsy proven nephrosclerosis could much easier be ascribed to chloroquine in cumulative dose of 413 g than to SLE being in remission
Considerable improvement of renal function and clearance of lamellar bodies from skeletal muscle after 6 months of discontinuation of chloroquine therapy
Absence of ultrastructural features of Fabry disease in the first renal biopsy
Lack of family history of Fabry disease Peripheral leukocyte testing for -galactosidase A
level within normal range and genetic analysis excluding mutation of -galactosidase A gene

Chloroquine side-effects in humans
retinopathy (1959), neuromyopathy (1963), cardiomyopathy (1977), nephropathy (2003) – iatrogenic phospholipidosis shared with more than 50 drugs with different therapeutic actions but all cationic, amphiphilic and lysosomotropic

Literature on chloroquine-induced phospholipidosis
Case reports
Underlying
Disease
Chloroquine Time Cumm
Lamellar bodies
Curvilin bodies
Prot (g/d)
S-Creat (mg/dL)
Müller-Hocher J et al, 2003
Sjögren syndrome
11 mo 51 g +++/+ + cell type?
0 1.0-2.1
Albay D et al, 2005
Rheum arthritis
18 mo 130 g +++/+ 0(muscle biopsy+)
traces 2.2
Bracamonte ER et al, 2006
Undefined autoimm disease
10 yrs intermitent
+++/+ 0 1.2 1.3
Wojwodt A et al, 2007
SLE Several years?
+++/+ 0 2 CCr
64ml/min

Tentative mechanisms involved in pathogenesis Tentative mechanisms involved in pathogenesis of chloroquine-induced phospholipidosisof chloroquine-induced phospholipidosis
• Adsorption to plasma membrane and accumulation in lysosomes
• Formation of amphiphilic cationic drug–polar lipid complexes resistant to digestion
• Inhibition of lysosomal enzyme activities through drug-induced increase of pH
• Direct drug induced strong but reversible inhibition of lysosomal phospholipases A and C and possibly other hydrolases

PatientsPatients (Kidney biopsy files 1987-2007)(Kidney biopsy files 1987-2007)
25 pts, mostly SLE, on chloroquine 250 mg/d (1day – 8yrs)
___________________________________________ Chloroquine treatment
Renal lipidosis
No. of
pts
Duration Cummulative Withdrawn before biopsy
Yes 6 (24%)
11 days – 4.5 yrs 5.3 – 413 g 0
Suspected 3 (12%)
37 days – 10 mo 11.7 – 79 g 0
No 2 (8%)
1 day – 2 days 0.5 – 1.0 g 0
No 14 (56%)
27 days – 5 yrs 9.3 – 460 g 3 mo – 8 yrs