Portugal Inenglish 2004aw Motivating Lower Secundary Pupils to Read
Upload
ashlyn-youngCategory
view
227download
3
ESOPHAGUSESOPHAGUS


MOTILITY DISORDERSMOTILITY DISORDERS
SES SES LESLES Peristaltic wavesPeristaltic waves
PrimarPrimary – deglutitiony – deglutition SecundarSecundaryy – – GERDGERD TerTertiary – autonomic tiary – autonomic
muscle control muscle control independent of independent of deglutitiondeglutition

MOTILITY DISORDERSMOTILITY DISORDERS Primary motility disorders
Achalasia: cricopharingian, cardia Diffuse esophageal spasm LES and SES hypertonia
Secondary motility disorders sclerodermia diabetes Parkinson amiloidosis colagenosis miastenia gravis

ACHALAACHALASIASIA DefiniDefinitiontion
Lack of LES relaxationLack of LES relaxation + + loss of capacity loss of capacity to transmit peristaltic waves, replaced by to transmit peristaltic waves, replaced by incoordinated ocntractionsincoordinated ocntractions
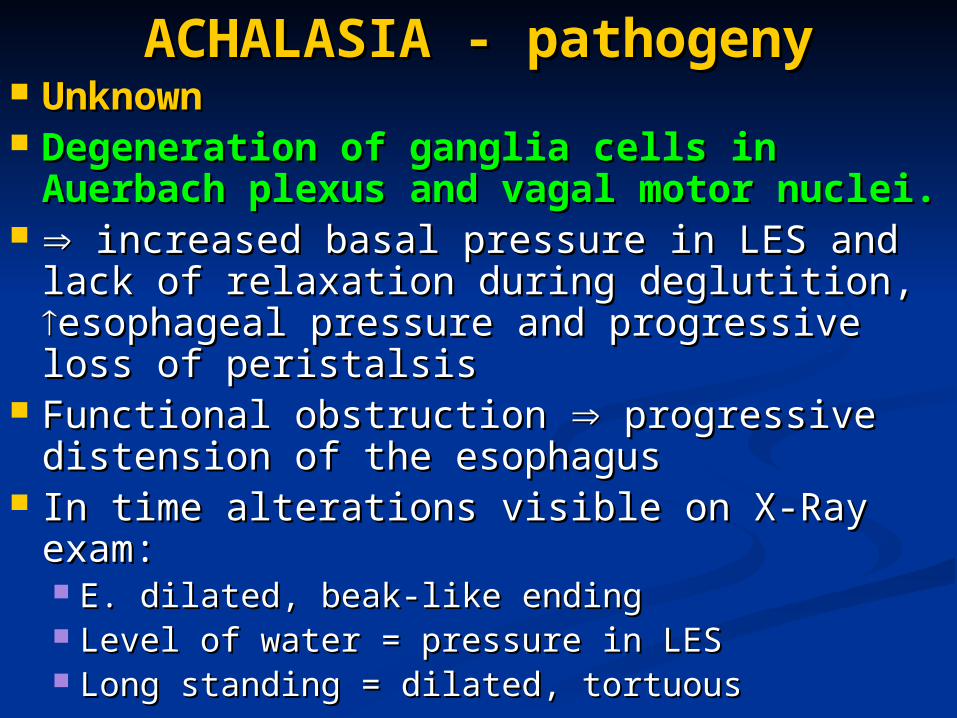
ACHALAACHALASIA - pathogenySIA - pathogeny UnknownUnknown Degeneration of ganglia cells in Degeneration of ganglia cells in
AuerbachAuerbach plexus and vagal motor plexus and vagal motor nuclei.nuclei.
increased basal pressure in LES and lack increased basal pressure in LES and lack of relaxation during deglutitionof relaxation during deglutition, , esophageal esophageal pressure and progressive loss of peristalsispressure and progressive loss of peristalsis
Functional obstruction Functional obstruction progressive progressive distension of the esophagusdistension of the esophagus
In time alterations visible on X-Ray examIn time alterations visible on X-Ray exam:: E. dilatE. dilateded, , beak-like endingbeak-like ending Level of water = pressure in LESLevel of water = pressure in LES Long standing = dilated, tortuousLong standing = dilated, tortuous

ACHALAACHALASIA - pathologySIA - pathology
MacroscopicMacroscopic dilatdilateded “ “botlebotle”, “”, “socketsocket”, ”, initially distal initially distal
end, followed by all esophagusend, followed by all esophagus Thick wallThick wall Esophagitis due to stasis and fermentationEsophagitis due to stasis and fermentation
uleration and bleedinguleration and bleeding MicroscopMicroscopyy
Low or absence of ganglia cells in the Low or absence of ganglia cells in the nervous plexus of Auernervous plexus of Auerbachbach

ACHALAACHALASIA clinical SIA clinical presentationpresentation
20 – 4020 – 40y subtle onsety subtle onset May be asymptomaticMay be asymptomatic THE ESOPHAGEAL SYNDROMETHE ESOPHAGEAL SYNDROME: :
DisDisphagia (intermitent, sometimes very phagia (intermitent, sometimes very acute, paradoxical!!)acute, paradoxical!!)
Pain (epigastric, thoracic) - radiates Pain (epigastric, thoracic) - radiates precordial, cervical, earprecordial, cervical, ear
Regurgitation (time after eating – Regurgitation (time after eating – depending on dilation of esophagus) – depending on dilation of esophagus) – may produce aspirationmay produce aspiration
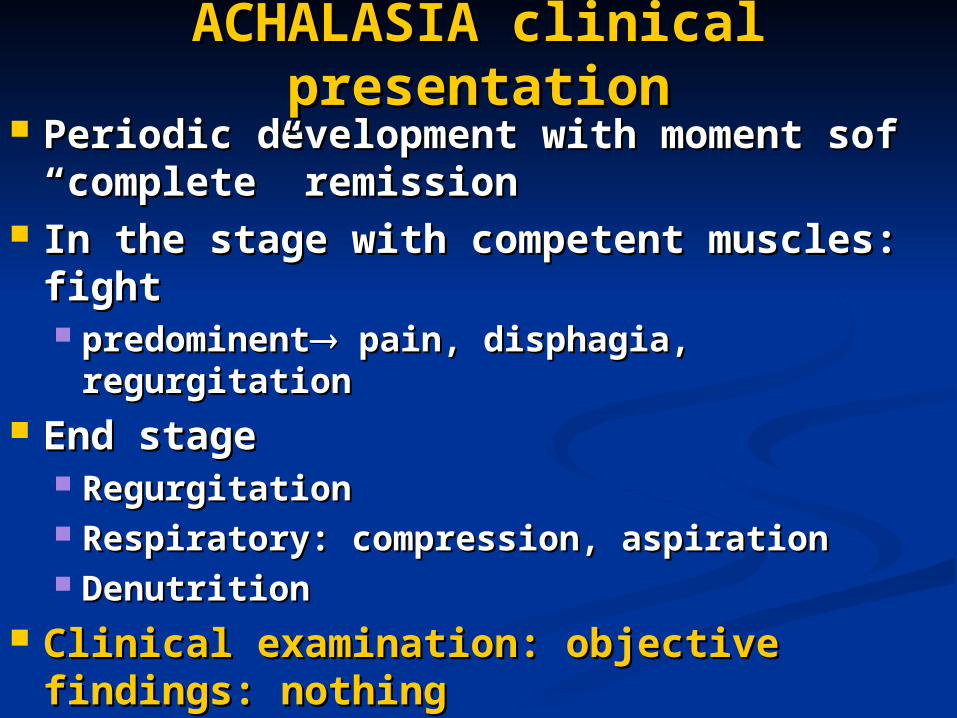
ACHALAACHALASIA clinical SIA clinical presentationpresentation
Periodic development with moment sof Periodic development with moment sof “complete” remission“complete” remission
In the stage with competent muscles: In the stage with competent muscles: fightfight predominpredominentent pain, disphagia, pain, disphagia,
regurgitationregurgitation End stageEnd stage
RegurgitationRegurgitation Respiratory: compression, aspiration Respiratory: compression, aspiration DenutritionDenutrition
Clinical examination: objective Clinical examination: objective findings: nothingfindings: nothing

ACHALAACHALASIA SIA imagisticimagistic
RadiologRadiologyy funcţional funcţional
initialinitial Peristalsis OKPeristalsis OK Slow relaxation of cardiaSlow relaxation of cardia
advansedadvansed Upper Upper 1/3 1/3 peristalsisperistalsis CCabnormal, disorganised abnormal, disorganised
contraction that fail to contraction that fail to relax cardiarelax cardia
End stageEnd stage No peristalsisNo peristalsis
OOrganic rganic diameter of Ediameter of E length increased, bent,length increased, bent,
sinuosinuoss Lower extremity narrow: Lower extremity narrow:
“beak” or “candle” “beak” or “candle”
EndoscopEndoscopyy Narrow passageNarrow passage Does not open, Does not open,
BUTBUT easy passage easy passage cancercancer

ManomeManometrytry No harmonious peristalsis, tertiary wavesNo harmonious peristalsis, tertiary waves High pressure LES Incomplete relaxation of LES
ACHALAACHALASIA – differential SIA – differential dgdg
Cancer of lower esophagusCancer of lower esophagus Benign peptic stenosisBenign peptic stenosis Difuse esophageal sDifuse esophageal spasmul pasmul Ischemic heart diseasesIschemic heart diseases Respiratory problemsRespiratory problems ChagasChagas disease ( disease (Trypanosoma Trypanosoma
cruzicruzi) – damage to myenteric plexus ) – damage to myenteric plexus same clinical presentationsame clinical presentation

ACHALAACHALASIA progressSIA progress
Long, unpredictable Long, unpredictable over 20-30 yearsover 20-30 years
3 3 stagesstages DyDyssphphagiagiaa and and
regurgitationregurgitation Latent clinical stageLatent clinical stage MegaesophagusMegaesophagus
Progressive loss of Progressive loss of weight : malnutritionweight : malnutrition
CComplicaomplicationstions general general
denutridenutritiontion ca cachchexiexiaa regional regional
Mediastinal compressionMediastinal compression Aspiration: pulmonary Aspiration: pulmonary
complications complications TB decreased immune TB decreased immune
reaction: reactivationreaction: reactivation locallocal
EsofagitEsofagitisis UGI bleeding, ulcerUGI bleeding, ulcer Cancer Cancer Perforation + Perforation +
mediastinitismediastinitis
ACHALAACHALASIA treatmentSIA treatment
ConservatConservativeive avoidavoid
Very cold food, very hot food Very cold food, very hot food Rapid eating with large bulky swallows Rapid eating with large bulky swallows
Decrease LES tonus: nitrates, calcium chanle Decrease LES tonus: nitrates, calcium chanle blockers blockers
Mucosa protectionMucosa protection – Sucral – Sucralfat fat Little benefit in timeLittle benefit in time

Forcefull dilation – endoscopic Forcefull dilation – endoscopic Good initial approachGood initial approach 2 dila2 dilationstions NU NU surgerysurgery RISK: perforationRISK: perforation CICINDND: - : - long standing disease, tortuous esophagus, long standing disease, tortuous esophagus,
association with GERDassociation with GERD

Injection of Botulinum Injection of Botulinum toxine toxine
ACHALASIA - surgery ACHALASIA - surgery
IndicationsIndications Per primamPer primam Failure after dilationFailure after dilation
EExtramucosxtramucosalal Heller Heller myotomy myotomy 8-10 cm 8-10 cm incision of the muscular wall incision of the muscular wall
over the eso-gastric junction over the eso-gastric junction Abdominal/thoracic approach Abdominal/thoracic approach FundoplicatFundoplication n(antireflux ion n(antireflux
procedure)procedure)

ESOPHAGEAL ESOPHAGEAL DIVERTICULADIVERTICULA
Classification: - pharingo-esophageal – Zenker
junction between pharinx and esophagus;
- midd-esophageal close to trachea and bronchi;
- epiphrenic (supradiaphragmatic) last 10 cm of esophagus

Histology Histology
Structure of the wall: - true diverticula – all strata of the
esophageal wall; - false (pulsion) – only mucosa and
submucosa are present

PATHOGENYPATHOGENY
TYPE - pulsion diverticula due to high
pressure in the lumen + motility disorder
- traction diverticula – inflammatory processes in the vicinity with traction on the wall during scaring.

ZENKER diverticula
fals diverticula Pulsion type Weak area: posterior
aspect of the pharynx between the inferior constrictir and transversal situatated cricopharingeal = triangle of triunghiul Killian (only mucosa and some fibrotic tissue)

ZENKER diverticula
CLINICAL ASPECTCLINICAL ASPECT InitialInitial
Burning sensation, non-productive cough, sensation of foreign body in the neck
LateLate – – big diverticulabig diverticula DisDisphphagia agia RegurgitaRegurgitationtion Bead smellBead smell CompressionCompression

DIVERTICULUL ZENKER
IMAGISTICIMAGISTIC X-RayX-Ray EndoscopEndoscopyy
ZENKER DIVERTICULA
Complications Hemorhage Perforation Carcinoma Chronic pulmonary
infections

ZENKER DIVERTICULA
TRTREEATMENTATMENT SmallSmall
Nothing muchNothing much Big, symptomatic, complicationsBig, symptomatic, complications
Resection of the diverticula ± miotomy of SES
Endoscopic treatment

MIDDLE ESOPHAGEAL DIVERTICULA
Traction type Middle thoracic Adjacent inflammatory
pathology ETHIOLOGY infections
Mediastinal TB (lymph nodes) Pleural infections Pericarditis
congenital

PATHOLOGY Traction type True diverticula Lateral wall of the
esophagus in the lateral wall
Large mouth to communicate with the esophageal lumen = no retention
Can also be pulsion type (not usual)

IMAGISTIC
DIAGNOSTICDIAGNOSTIC ClinicClinicalal
asasyymptomatmptomaticic disdisphagiaphagia
ComplicaComplicationstions HemorHemorrhagerhage PerforaPerforationtion CancerCancer
ImagisticImagistic X-RayX-Ray EEndoscopndoscopyy

TREATMENT
ConservatConservative (no ive (no clinical signs)clinical signs)
SurgerySurgery ExciExcisionsion Open or thoracoscopicOpen or thoracoscopic
EPIPHRENIC DIVERTICUL
A
Inferior esophagus PATHOGENY Associated with
motility disorders – achalasia, difuse esophageal spasm
Combines: high pressure + lack of relaxation
EPIPHRENIC DIVERTICULA
DIAGNOSTICDIAGNOSTIC Similar to thoracic typeSimilar to thoracic type +manometr+manometry for motility y for motility
disorderdisorder TRTREEATMENTATMENT
RezecRezectiontion + m + myyotomotomyy +tratament+tratament of associated of associated
diseasedisease

GERDGERD Physiologic refluxPhysiologic reflux
Normal in some instances, but quickly clearedNormal in some instances, but quickly cleared More often standing and while awakeMore often standing and while awake
LES tonus influenced by different factors:LES tonus influenced by different factors:
α stimulators, β blockers α blockers, β stimulators
gastrine, motiline colecistochinine, estrogen, progesteron, glucagon, somatostatin, secretine
antiacide medication, domperidol, PGF2
anticholinergics, barbiturics, calcium chanel blockers, cafeine, dopamine, teophiline, PGE1-2, diazepam
Pepermint, chiocolate, coffee, alchool, fatty food
GERDGERD
DiagnosticDiagnostic: : Presence of symptomsPresence of symptoms Endoscopic demonstration of Endoscopic demonstration of
esophagitisesophagitis LESLES

GERDGERD PATHOGENYPATHOGENY A. Mechanic failure of LESA. Mechanic failure of LES – valv – valve effecte effect
Inadequate Inadequate LES pressureLES pressure Inadequate length of LESInadequate length of LES Abnormal position of cardiaAbnormal position of cardia BrahiesophagusBrahiesophagus
B. B. Inefficient clearanceInefficient clearance – 4 factor – 4 factorss:: GGravitravityy Normal peristaltic movements of the esophagusNormal peristaltic movements of the esophagus Salivary gland productionSalivary gland production Positioning of distal esophagus in abdomenPositioning of distal esophagus in abdomen

GERD PATHOGENYGERD PATHOGENY C. Gastric reservoirC. Gastric reservoir
Gastric distentionGastric distention: : Decreases the length of LESDecreases the length of LES Causes: chewing gum, low saliva production Causes: chewing gum, low saliva production
(Sjogren), motility disorders. (Sjogren), motility disorders. High Gastric pressureHigh Gastric pressure
Outlet syndromeOutlet syndrome – – pyloric stenosis, pyloric stenosis, vagotomvagotomyy Diabetic gastroparesisDiabetic gastroparesis
Prolonged gastric stasisProlonged gastric stasis Miogenic causes (diabetes, neuromuscular Miogenic causes (diabetes, neuromuscular
problesm, anticholinergic medication, etc)problesm, anticholinergic medication, etc) Non-miogenic causes (vagotomy, antropyloric Non-miogenic causes (vagotomy, antropyloric
disfunctin, duodenal motility disorders, duodeno-disfunctin, duodenal motility disorders, duodeno-gastric reflux)gastric reflux)
Gastric hypersecretionGastric hypersecretion – – exposure to low pHexposure to low pH

GERD: E mucosa GERD: E mucosa aggressionaggression
Gastric juice:Gastric juice: Low pH – long term exposureLow pH – long term exposure Pepsine – proteolytic at pH<2Pepsine – proteolytic at pH<2
Duodenal reflux:Duodenal reflux: Billiary salts – E not used to deal with Billiary salts – E not used to deal with
high pHhigh pH Pancreatic enzymesPancreatic enzymes
DifferencesDifferences HCl, HCl, billiary acidsbilliary acids mucosal permeabilitymucosal permeability pepsinpepsinee, tripsin, tripsinee mucosal erosions mucosal erosions
Very Very little correlationlittle correlation between symptoms and between symptoms and endoscopic appearance of lesions. endoscopic appearance of lesions.
GERD complicationsGERD complications
ESOPHAGUSESOPHAGUS: prolonged exposure: prolonged exposure esofagitesofagitisis stricturstrictureses Barrett Barrett
RESPIRATORYRESPIRATORY: repeated aspiration : repeated aspiration pneumonia, pulmonary fibrosispneumonia, pulmonary fibrosis
Pathological seen lesion correlate withPathological seen lesion correlate with 1. 1. LES pressure (sphincter volume)LES pressure (sphincter volume) 2. 2. Acid + bile is more aggressive toward Acid + bile is more aggressive toward
mucosamucosa

GERD symptomsGERD symptoms DigestiveDigestive
Retrosternal burning pain Retrosternal burning pain pirozisulpirozisul
Regurgitations (according to Regurgitations (according to body position) body position)
Dysphagia (edema, stenosis, Dysphagia (edema, stenosis, damaged peristalsis) damaged peristalsis)
Respiratory Respiratory symptomssymptoms Chronic coghChronic cogh Senzation of lack of airSenzation of lack of air Horse voice (chronic laryngitis)Horse voice (chronic laryngitis) WWheezing heezing
Unusual symptomsUnusual symptoms Nausea, vomitingNausea, vomiting Full stomachFull stomach Atypical thoracic painAtypical thoracic pain
GERD imagisticGERD imagistic
Barium meal- Barium meal- esophagus, esophagus, stomach and stomach and duodenumduodenum
Reflux of bariumReflux of barium Hiatus herniaHiatus hernia StricturesStrictures Associated lesionsAssociated lesions

GERD endoscopyGERD endoscopy Every patient with dysphagia - compulsoryEvery patient with dysphagia - compulsory EsophagitisEsophagitis
gr I – gr I – congestion of mucosa, no ulcerationscongestion of mucosa, no ulcerations gr II – gr II – linear ulcerations bordered by granulation tissue that bleeds on linear ulcerations bordered by granulation tissue that bleeds on
touchtouch gr III – gr III – confluent ulcerations with isles of normal mucosa confluent ulcerations with isles of normal mucosa gr IV - stenogr IV - stenosissis
GERD – Barrett esophagusGERD – Barrett esophagus Epitelial metapasis:Epitelial metapasis:
Normal squamos cell epithelium – into gastric Normal squamos cell epithelium – into gastric columnar epitheliumcolumnar epithelium
Biopsy: metaplasia, displasia, adenocarcinomaBiopsy: metaplasia, displasia, adenocarcinoma

GERD and hiatus herniaGERD and hiatus hernia HH often associated with GERD (main symptom) HH often associated with GERD (main symptom)
SlidingSliding Rolling – not often associated with reflux (cardia Rolling – not often associated with reflux (cardia
normal) normal) CombinedCombined
GERD - manometryGERD - manometry
Stationary Stationary manometrymanometry
Evaluation of LES Evaluation of LES pressure<6mmHgpressure<6mmHg Total length in abdomen < Total length in abdomen <
1cm1cm Total LES <2cmTotal LES <2cm
Sphincter area volumeSphincter area volume Primary motility Primary motility
disordersdisorders (ac (achhalaalassia, ia, difuse spasm) difuse spasm)
GERD induced motility GERD induced motility disorders disorders RGERGEafect afect SEI/ peristaltica E/ SEI/ peristaltica E/ amplitudinea amplitudinea contracţiilor contracţiilor

GERD manometryGERD manometry 2424 hours ambulatory manometry hours ambulatory manometry
Better diagnostic of motor dysfunctinBetter diagnostic of motor dysfunctin In non-obstructive dysphagia: non In non-obstructive dysphagia: non
coordinated muscle function coordinated muscle function Scintigrapic evaluation of esophageal Scintigrapic evaluation of esophageal
transittransit 10 ml water with 10 ml water with Tc99Tc99 Non specificNon specific Quantification of esophageal transit timeQuantification of esophageal transit time Prolonged time in achalasia, sclerodermia, Prolonged time in achalasia, sclerodermia,
difuse spasm, nutcracker syndromedifuse spasm, nutcracker syndrome
GERD pH monitoringGERD pH monitoring Quantification Quantification
time with pH<4time with pH<4 Total time of pH<4 Total time of pH<4
exposureexposure Frequency of Frequency of
exposureexposure Duration of epsiodes Duration of epsiodes
>5 minutes>5 minutes Longest period of Longest period of
refluxreflux Association with Association with
eventsevents Acid relfux: pH<4Acid relfux: pH<4 Alkaline reflux pH>7Alkaline reflux pH>7 Pletismography: Pletismography:
quantification of quantification of billiary refluxbilliary reflux

GERD differential diagnsticGERD differential diagnstic
Achalasia –dysphagia + lack of esophageal empting (Rx + endoscopy)
Esophageal cancer: dysphagia (endoscopy)
Hiatus hernia: may be clinical silent Esophageal diverticula motility
disorders, regurgitation (Rx, endoscopy)
UGI pathology Ischemic heart disease Pneumonia and other respiratory
problems

GERD treatment GERD treatment MedicalMedical – first step (no evaluation) – first step (no evaluation) Minor changes in habitsMinor changes in habits
Raised position in bedRaised position in bed Avoid very tight clothingAvoid very tight clothing Small frequent mealsSmall frequent meals Dine before 6pm and small quantityDine before 6pm and small quantity Loose weightLoose weight Avoid alcohol, smoking, coffeeAvoid alcohol, smoking, coffeeee, tea, pepermint, , tea, pepermint,
chocolate, fatchocolate, fat Protective tratement for mucosa (Protective tratement for mucosa (alginalginat – at –
creates a barrier)creates a barrier) + antacides (may relieve + antacides (may relieve symptoms but rebound)symptoms but rebound)
Promotilic medicationPromotilic medication

REFLUXUL REFLUXUL GASTROESOFAGIANGASTROESOFAGIAN
Step II persistent symptoms)Step II persistent symptoms) Endoscopy +/- Rx studies for complications; Endoscopy +/- Rx studies for complications;
manometrymanometry PPI – decrease gastric acid output (high PPI – decrease gastric acid output (high
recurrence when stop) – continuous recurrence when stop) – continuous medication with periods without. Long term: medication with periods without. Long term: increases risk of hyperplastic gastric polypsincreases risk of hyperplastic gastric polyps
Persistent symptoms: aggressive Persistent symptoms: aggressive exploration exploration
TREATMENT: aggressiveTREATMENT: aggressive MedicalMedical Surgical Surgical

GERD surgeryGERD surgery
IndicationsIndications Persistence of endoscopic lesions in Persistence of endoscopic lesions in
spite of aggressive medicationspite of aggressive medication Young patients – long term treatmentYoung patients – long term treatment No response to treatmentNo response to treatment
FUNDOPLICAFUNDOPLICATIONTION
LOGIC – rebuild LOGIC – rebuild competence of LEScompetence of LES
1. 1. Restore Restore LES pressureLES pressure 2x 2x over gastric over gastric pressure over >3cm: fundoplicationpressure over >3cm: fundoplication
2. 2. Restore the Restore the length of intraabdominal length of intraabdominal esophagusesophagus (positive pressure) – 2 cm (positive pressure) – 2 cm
3. Allow for a 3. Allow for a normal swallownormal swallow: gastric : gastric fundus used in wrap arround LES + avoid fundus used in wrap arround LES + avoid vagus nerve injury + loose wrapvagus nerve injury + loose wrap
4. 4. Degree of fundoplicationDegree of fundoplication: according : according to diameter and degree of motility to diameter and degree of motility disorder disorder
5. 5. Intraabdomina position of the Intraabdomina position of the fundoplicationfundoplication : Collis gastroplasty : Collis gastroplasty

BARRETT esophagusBARRETT esophagus Acquired problem in 10% of GERD patients – end stageAcquired problem in 10% of GERD patients – end stage GERDGERD mucosa destructionmucosa destruction replaced with columnar replaced with columnar
epithelium more resistant to acid aggressionepithelium more resistant to acid aggression It impliesIt implies
Major deficiency in LES functionMajor deficiency in LES function Major deficiens in esophageal clearanceMajor deficiens in esophageal clearance Long term exposure to acidLong term exposure to acid

BARRETTBARRETT COMPLICATIONSCOMPLICATIONS
Ulcer formation (very similar with Ulcer formation (very similar with gastric ulcer) – same complicationsgastric ulcer) – same complications
Stricture formationStricture formation Displasia – metaplasia - cancerDisplasia – metaplasia - cancer

BARRETT - diagnosticBARRETT - diagnostic Rx - indirectRx - indirect
BrachiesopagusBrachiesopagus UlcerUlcer StrictureStricture
EndoscopEndoscopY - BIOPSYY - BIOPSY PrePresence and degree of metaplasiasence and degree of metaplasia

BARRETT - treatmentBARRETT - treatment MedicalMedical
No metaplasia: treatment of GERD – No metaplasia: treatment of GERD – surveilancesurveilance
Dysplasia: destruction: radiofrequency Dysplasia: destruction: radiofrequency ablation, photodynamic ablationablation, photodynamic ablation
SurgicalSurgical Antireflux surgeryAntireflux surgery High risk dysplasia: esophagectomyHigh risk dysplasia: esophagectomy

Esophageal peptic strictureEsophageal peptic stricture Stenosis developing as a result of long standing Stenosis developing as a result of long standing
refluxreflux Dg: need to exclude a malingnant stenosisDg: need to exclude a malingnant stenosis Essential in deciding upon therapyEssential in deciding upon therapy
1. 1. response to dilatationresponse to dilatation 2. 2. length of staneosis and length of esophaguslength of staneosis and length of esophagus 3. 3. nromal vs abnormal motilitynromal vs abnormal motility
TTrreeatamentatament Dilatation + treatment of GERDDilatation + treatment of GERD

HIATUS HERNIAHIATUS HERNIA DefiniDefinition: herniation of the stomach tion: herniation of the stomach
through the esophageal hiatusthrough the esophageal hiatus
HIATUS HERNIA HIATUS HERNIA classificationclassification Tip I - Tip I - slidingsliding
90-95%90-95% Cardia positioned in the thoraxCardia positioned in the thorax

HIATUS HERNIA HIATUS HERNIA classificationclassification Tip II - Tip II - paraesophageal or rolling paraesophageal or rolling
5-10%5-10% Cardia within abdominal cavityCardia within abdominal cavity
HIATUS HERNIA HIATUS HERNIA classificationclassification Tip IIITip III - - combinedcombined
brachyesophagusbrachyesophagus - 1-2% - 1-2% Congenital or aquired due to GERDCongenital or aquired due to GERD

HIATUS HERNIA HIATUS HERNIA pathogenypathogeny
Mechanism Mechanism - - failure of the mechansim failure of the mechansim that fix the eso-cardial complexthat fix the eso-cardial complex
HIATUS HERNIA - HIATUS HERNIA - causescauses 1. 1. age: changes in strcutures with ageage: changes in strcutures with age
2. 2. obesity: infiltration with fat lowers resistanceobesity: infiltration with fat lowers resistance 3. 3. high abdominal pressure (pregnancy, high abdominal pressure (pregnancy,
constipation, chronic cough, prostatic problems, constipation, chronic cough, prostatic problems, chronic effort, etc)chronic effort, etc)
4. 4. anomalies of the rachis (anomalies of the rachis (scolioscoliosis, cifosis) sis, cifosis) change in the diaphragmatic pillars change in the diaphragmatic pillars
5. 5. traumatrauma 6. 6. iatrogenic – dissection in area for other iatrogenic – dissection in area for other
pathologies pathologies 8. 8. asociateasociated problems d problems – – billiary stones and diverticula billiary stones and diverticula
of colon of colon ((sdr Saintsdr Saint )) = = muscular hipertonicity (colics) + muscular hipertonicity (colics) + increased in abdominal pressureincreased in abdominal pressure
9. 9. Gastric problemsGastric problems Peptic ulcer disease: pyloric spasmPeptic ulcer disease: pyloric spasm → ↑ → ↑ gastric gastric pres pressuresure Gastric outlet syndrome (organic or functional)Gastric outlet syndrome (organic or functional)

HIATUS HERNIA pathogenyHIATUS HERNIA pathogeny
GERD with all symptoms associated GERD with all symptoms associated wioth refluxwioth reflux
Mechanic effects of gastric herniation Mechanic effects of gastric herniation Gastric wall lesions (compression, acidity Gastric wall lesions (compression, acidity
in the puch)in the puch) Ulcerations, edema – UGI bleeding Ulcerations, edema – UGI bleeding Strangulation – gangrene and paerforationStrangulation – gangrene and paerforation
Respiratory and cardiac problemsRespiratory and cardiac problems DispnDispnoea and irritative coughoea and irritative cough Tachycardia, abnormal heart beats, mimics Tachycardia, abnormal heart beats, mimics
angina angina Develop after eating or aggravated, in Develop after eating or aggravated, in
decubitus and may dissapear in ortostatismdecubitus and may dissapear in ortostatism

HIATUS HERNIA HIATUS HERNIA symptomssymptoms
A. A. GERD symptomsGERD symptoms Epigastric pain Epigastric pain 50% 50% Anterior thoraci burning painAnterior thoraci burning pain 67% 67% RRegurgitaegurgitationstions - - 40% 40%
After meal and bending downAfter meal and bending down NocturnalNocturnal tracheal aspiration, pneumoniatracheal aspiration, pneumonia
DyDyssphphagia agia intermitent intermitent - - spasmspasm permanent – permanent – stenosis stenosis

HIATUS HERNIA HIATUS HERNIA symptomssymptoms
B. B. Volume of hernia Volume of hernia Respiratory problemsRespiratory problems
DispnDispnoea, coughingoea, coughing After large meals + positionsAfter large meals + positions
Cardiac problemsCardiac problems - palpita - palpitationtion, , extrasistolextrasistolic heart beatsic heart beats, , angina-likeangina-like
Hickups Hickups

HIATUS HERNIA HIATUS HERNIA symptomssymptoms
C. C. ComplicationsComplications UGI bleeding versus occult bleeding and UGI bleeding versus occult bleeding and
anemiaanemia Gastric puch discomfort: meteorism, belching, Gastric puch discomfort: meteorism, belching,
lack of airlack of air stenoza esofagiană sau/ şi cancerul esofagianstenoza esofagiană sau/ şi cancerul esofagian Strangulation + perforationStrangulation + perforation Stenosis (+/- malignancy)Stenosis (+/- malignancy)
HIATUS HERNIA HIATUS HERNIA imagisticimagistic
RadiologyRadiology All positions: All positions: orto-, orto-,
clinostatism, lateral, clinostatism, lateral, TrendelemburgTrendelemburg
Presence of the Presence of the gastric puch with gastric puch with mucosal folds mucosal folds
Position of cardiaPosition of cardia E - lE - long and curved ong and curved
or straight and short or straight and short (brachyesophagus) (brachyesophagus)

HIATUS HERNIA HIATUS HERNIA imagisticimagistic
ENDOSCOPYENDOSCOPY See the herniaSee the hernia Free reflux (bulk) Free reflux (bulk) Associated Associated
esophagitisesophagitis Essential for Essential for
stenosis and ulcerstenosis and ulcer BiopsyBiopsy

HIATUS HERNIA HIATUS HERNIA evaluationevaluation
Functional testsFunctional tests:: manometrmanometryy
Evaluation of LESEvaluation of LES Motility disordersMotility disorders
24 24 hours pH monitoringhours pH monitoring Time with pH<4Time with pH<4
HIATUS HERNIA HIATUS HERNIA treatmenttreatment
MedicalMedical – – any HH with GERD symptoms any HH with GERD symptoms medical treatment for a minimum of 6 monthsmedical treatment for a minimum of 6 months Change in posture after meal and during sleepChange in posture after meal and during sleep Changes in eating habits Changes in eating habits
Small meals, more frequentSmall meals, more frequent No large meals in the eveningNo large meals in the evening Avoid alcohol, spices, carbonated drinks Avoid alcohol, spices, carbonated drinks
Decrease abdominal pressureDecrease abdominal pressure Loose weight (obese patients)Loose weight (obese patients) Avoid constipation and major effortsAvoid constipation and major efforts
IndicationsIndications: : gr. I – IIgr. I – II esophagitis: avoid and operation esophagitis: avoid and operation Gr. III-IV esophagitis: prepare for an operation Gr. III-IV esophagitis: prepare for an operation
CIND: old people, comorbidities +/- CIND: old people, comorbidities +/- laparoscopy laparoscopy

HIATUS HERNIA HIATUS HERNIA treatmenttreatment
MedicationMedication Lower acid secretion PPI, H2 blockersLower acid secretion PPI, H2 blockers SedativeSedatives?s? PromotilicsPromotilics
EndoscopicEndoscopic Induce sclerosis: cautery applications Induce sclerosis: cautery applications Dilation in cases of stenosisDilation in cases of stenosis Endoluminal mucosal plicature – Endoluminal mucosal plicature –
antireflux procedureantireflux procedure

HIATUS HERNIA HIATUS HERNIA treatmenttreatment
SurgicalSurgical IndicaIndicationstions:: No response to medical treatmentNo response to medical treatment Large HH with respiratory, cardiac Large HH with respiratory, cardiac
symptoms or UGI bleeding risksymptoms or UGI bleeding risk ComplicationsComplications
gr. III-IVgr. III-IV esophagitis esophagitis UGI bleeding, stenosis, brachyesophagusUGI bleeding, stenosis, brachyesophagus
Rolling type hernia- risk of strangulationRolling type hernia- risk of strangulation HH in new born children HH in new born children

HIATUS HERNIA HIATUS HERNIA treatmenttreatment
PrincipPrinciplesles Reposition the stomach in abdomen and Reposition the stomach in abdomen and
fix it therefix it there CalibraCalibration of the hiatustion of the hiatus Closure of the angle ofClosure of the angle of Hiss Hiss ReconstructReconstruct gastro- gastro-phphrenicrenic ligament ligament PrevePrevent reflux (wrap formation) nt reflux (wrap formation)

HIATUS HIATUS HERNIAHERNIA
TehnicTehnicss:: gastropexgastropexyy FundoplicaFundoplication tion
(270-360 degree (270-360 degree wrap)wrap)
ESOPHAGUS - CANCERESOPHAGUS - CANCER
7% of all digestive cancer; 7% of all digestive cancer; 2% of all2% of all
M > FM > F 60-7060-70yy AsiaAsia (China, Iran, Japonia) (China, Iran, Japonia), ,
South Afrika, USA South Afrika, USA 66thth cause of detah related to cause of detah related to
cancercancer
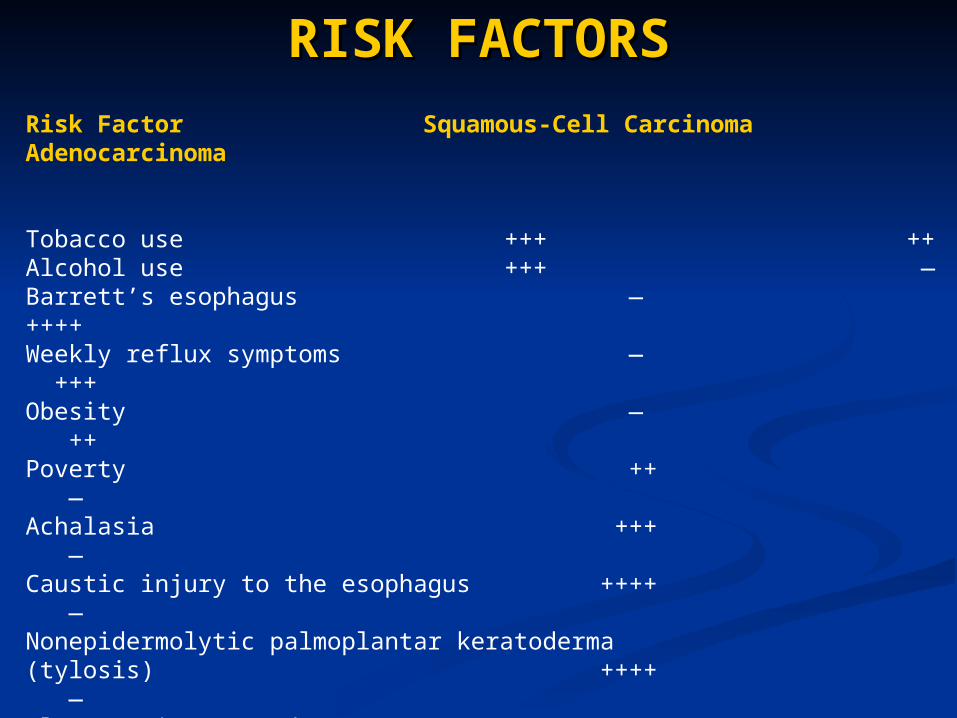
RISK FACTORSRISK FACTORSRisk Factor Squamous-Cell Carcinoma Adenocarcinoma
Tobacco use +++ ++Alcohol use +++ —Barrett’s esophagus — ++++Weekly reflux symptoms — +++Obesity — ++Poverty ++ —Achalasia +++ —Caustic injury to the esophagus ++++ —Nonepidermolytic palmoplantar keratoderma(tylosis) ++++ —Plummer–Vinson syndrome ++++ —History of head and neck cancer ++++ —History of breast cancer treated with radiotherapy +++
+++Frequent consumption of extremely hot beverages +
—Prior use of beta-blockers, anticholinergic agents,or aminophor aminophyllines — ±

PATHOLOGYPATHOLOGY SQUAMOS CELL CARCINOMASQUAMOS CELL CARCINOMA
Most frequentMost frequent Frequent multicentricFrequent multicentric Upper part of esophagusUpper part of esophagus Narrow anatomy: rapid invasion in bronchi and Narrow anatomy: rapid invasion in bronchi and
trachea, aorta, pleura, left recurrent nerve. trachea, aorta, pleura, left recurrent nerve. AdenocarcinomAdenocarcinomaa
Cardia and distal esophagusCardia and distal esophagus Origin:Origin:
Submucosal glands of esophagusSubmucosal glands of esophagus Cylindric epithelium of distal esophagusCylindric epithelium of distal esophagus Cylindric epithelium of BarrettCylindric epithelium of Barrett
Frequent extension (submucosal proximal and Frequent extension (submucosal proximal and subserosal distal)subserosal distal)
Larger mediastinum – late invasion in adjacent Larger mediastinum – late invasion in adjacent structuresstructures

ESOPHAGUS - CANCERESOPHAGUS - CANCER Macroscopy: Macroscopy:
squamos cell squamos cell carcinomacarcinoma

CANCERUL ESOFAGIANCANCERUL ESOFAGIAN
MACROSCOPY: adenocarcinomaMACROSCOPY: adenocarcinoma

MicroscopyMicroscopy
Most typical Most typical form = form = squamas cell squamas cell carcinomacarcinoma Often MTSOften MTS Radiosensibile Radiosensibile
MicroscopyMicroscopy AdenocarcinAdenocarcin
omaoma Esophageal or Esophageal or
gastric origin?gastric origin? Not responding Not responding
well to well to radiotherapyradiotherapy
CANCER - invasionCANCER - invasion
Local invasionLocal invasion Adjacent organsAdjacent organs
LymphaticsLymphatics – – regional LNregional LN 1/3 inf – 1/3 inf – mediastinum – abdomen (celiac mediastinum – abdomen (celiac
trunk)trunk) 1/3 m1/3 middleiddle – – trachea bifurcation - trachea bifurcation -
mediastinummediastinum 1/3 sup – 1/3 sup – recurrent – supraclavicular – recurrent – supraclavicular –
cervicalcervical Blood born metastasisBlood born metastasis
Liver, lungs, scheleton, etcLiver, lungs, scheleton, etc

STAGINGSTAGING T:T:
T1 – laminT1 – laminaa propriapropria//submucossubmucosaa
T2 – muscT2 – muscularisularis propria propria T3 – T3 – adventiciaadventicia T4 – T4 – neighbor organsneighbor organs
N:N: N0 – N0 – no LN no LN N1 –N1 – invasion in invasion in
regional LNregional LN M: M:
M0 – M0 – no MTSno MTS M1 – M1 – distant MTSdistant MTS
StaStagesges:: I: T1N0M0I: T1N0M0 IIa: T2N0M0 IIa: T2N0M0 oror
T3N0M0T3N0M0 IIb: T1N1M0 IIb: T1N1M0 oror
T2N1M0T2N1M0 III: T3N1M0 III: T3N1M0 oror
T4N0-1M0T4N0-1M0 IV: IV: anyany T T anyany N M1 N M1

SYMPTOMSSYMPTOMS Always with malnutritionAlways with malnutrition Late – very late presentationLate – very late presentation DDYSPHYSPHAGIAAGIA
First and dominant symptom inFirst and dominant symptom in 90 % 90 % of casesof cases ((esophageal lumen diminised withesophageal lumen diminised with ≈ 90 % ≈ 90 %))
progressiveprogressive Sometimes sudden onset (large piece of food Sometimes sudden onset (large piece of food
impacted)impacted) PAINPAIN
Retrosternal and back irradiation – not very often Retrosternal and back irradiation – not very often and can have significance in diagnostic and can have significance in diagnostic
MASSIVE WEIGHT LOSSMASSIVE WEIGHT LOSS Major symptomMajor symptom Not able to eat; late cachexia due to advanced Not able to eat; late cachexia due to advanced
neoplasianeoplasia

SYMPTOMSSYMPTOMS
RegurgitationRegurgitation – – late symptomlate symptom
HyHypersalivapersalivationtion Non-specific UGI Non-specific UGI
symptomssymptoms Low grade feverLow grade fever UGI bleeding – UGI bleeding –
usually occultusually occult
Changes in voice Changes in voice qualityquality
Cough and Cough and respiratory respiratory symtomssymtoms
Signs of aero-Signs of aero-digetsive fistuladigetsive fistula
CLINICAL EVALUATIONCLINICAL EVALUATION GGeneral eneral
Loss of weight (massive), dehydration Loss of weight (massive), dehydration AAbdominal bdominal
EpigastrumEpigastrum → → low development of low development of tumor may be palpabletumor may be palpable
LiverLiver→ → MTSMTS Cervical – LNCervical – LN RespiratoryRespiratory
fistulafistula
IMAGISTICIMAGISTIC
Barium mealBarium meal

IMAGISTICIMAGISTIC

CT - MRICT - MRI

ENDOSCOPIC ENDOSCOPIC ULTRASOUNDULTRASOUND

EVALUATIONEVALUATION Brush cytologyBrush cytology – early lesions – early lesions LaringoscopLaringoscopyy + Bron + Broncchoscophoscopyy
Invasion in bronchi or tracheaInvasion in bronchi or trachea CompressionCompression Fistula formationFistula formation
LaparoscopLaparoscopyy Liver MTSLiver MTS Abdominal LN evaluationAbdominal LN evaluation
Respiratory evaluationRespiratory evaluation VEMS < 1 = CIVEMS < 1 = CIND for operationsND for operations
Lab Lab Non specificNon specific

TREATMENTTREATMENT Pathologic typePathologic type
SSqquamocelular – uamocelular – RXT + surgeryRXT + surgery AdenocarcinomAdenocarcinomaa - - surgerysurgery
StStageage RezecRezectable?table? CurativCurative versus e versus paliativpaliativee
General status: can he survive an General status: can he survive an operation? operation?

PROGNOSTICPROGNOSTIC
CurativCurative intente intent In countries without screeningIn countries without screening ≈ 10- ≈ 10-
20 %20 % CHT-RXT versus CHT-RXT + SurgeryCHT-RXT versus CHT-RXT + Surgery Goal: resect the T with negative Goal: resect the T with negative
margins + ALL regional LNmargins + ALL regional LN 10 cm away from macroscopic margin10 cm away from macroscopic margin Often total esophagectomyOften total esophagectomy

Mucosal resectionMucosal resection

PALIATIVE PALIATIVE TREATMENTTREATMENT
Treat dysphagiaTreat dysphagia Stoma for artifical feedingStoma for artifical feeding Restore the lumen of the esophagus Restore the lumen of the esophagus
LaserLaser Alcohol sclerotherapyAlcohol sclerotherapy Photodynamic therapy Photodynamic therapy BrahytherapyBrahytherapy StentsStents

COROSIVE ESOPHAGITIS COROSIVE ESOPHAGITIS AND STENOSIS OF THE AND STENOSIS OF THE
ESOPHAGUSESOPHAGUS

PATHOGENYPATHOGENY
AGENTAGENT acute injury acute injury + chronic sequels + chronic sequels
MattersMatters: type, : type, concentration, quantity, concentration, quantity, time of contact time of contact ACID: dry necrosis ACID: dry necrosis ALCALINE: necrosis and ALCALINE: necrosis and
liquefactionliquefaction Location of maximum Location of maximum
injuryinjury Mouth to pylorusMouth to pylorus Natural narrow placesNatural narrow places Alcaline: little effect on Alcaline: little effect on
stomachstomach
3 3 Stages of developmentStages of development:: AcutAcute necrosis: 1-4 dayse necrosis: 1-4 days
Protein coagulation = Protein coagulation = necrosisnecrosis
Inflammation fallowsInflammation fallows Ulceration and granulation Ulceration and granulation
10-12 days10-12 days Necrotic membrane is Necrotic membrane is
eliminated eliminated Large ulcerated raw surface Large ulcerated raw surface
filled by granulation tissuefilled by granulation tissue Esophageal wall very friable Esophageal wall very friable
Scar formation Scar formation From 3From 3rdrd week week Fibrosis leads to stenosisFibrosis leads to stenosis Treatment tries to prevent Treatment tries to prevent
fibrosis fibrosis
DIAGNOSTICDIAGNOSTIC SymptomsSymptoms
3 stages3 stages Early presentation: shock, acidosis, renal failureEarly presentation: shock, acidosis, renal failure Respiratory: laryngeal spasm, edema of larynx, Respiratory: laryngeal spasm, edema of larynx,
pulmonary edemapulmonary edema Clinical evaluationClinical evaluation lesions of the lips and mouth lesions of the lips and mouth
Early endoscopy Early endoscopy
1.1. mucosal edema mucosal edema 2. 2. bleeding, exudat, ulcerations and pseudomembranesbleeding, exudat, ulcerations and pseudomembranes 3. 3. ulcers, massive bleeding, obstructions (edema) and ulcers, massive bleeding, obstructions (edema) and
perforationsperforations X-RayX-Ray –strictur –strictureses
farinfarinxx EsoEsophagusphagus StomachStomach

TREATMENTTREATMENT A. A. Immediate (on site)Immediate (on site)
Find the bottleFind the bottle Check airways freedomCheck airways freedom Venous accessVenous access
NNO attempt to neutralize the O attempt to neutralize the substance substance There is no antidoteThere is no antidote Favors diffusion of toxicFavors diffusion of toxic Burns due to antidoteBurns due to antidote
NNOO - - do not induce vomiting do not induce vomiting Promotes burns in the respiratory tractPromotes burns in the respiratory tract Inhales toxic Inhales toxic
NNOO - - nasogastric tube nasogastric tube Induces Induces refluxreflux VomitingVomiting PerforationPerforation

TREATMENTTREATMENT
TRANSPORTATIONTRANSPORTATION: : hospital + hospital + carecare
ICUICU Endoscopy +/- bronchoscopyEndoscopy +/- bronchoscopy Specialized surgerySpecialized surgery Toxicology determinations Toxicology determinations

In hospital treatmentIn hospital treatment A. – A. – Treat respiratory failuresTreat respiratory failures
O2O2 CortisoneCortisone Intubation +/- tracheostomy Intubation +/- tracheostomy Treat soc and acidosis Treat soc and acidosis
B. B. EndoscopyEndoscopy grade lesionsgrade lesions
C. C. BronchoscopyBronchoscopy – – respiratory respiratory lesions lesions

TREATMENT PROTOCOLTREATMENT PROTOCOL gr. IIIgr. III burns burns Surgery immediate Surgery immediate Endoscopic aspect essential:Endoscopic aspect essential:
Difuse necrosis eophagus and stomach: Difuse necrosis eophagus and stomach: high chances of mediastinitis and high chances of mediastinitis and perforationperforation
Early operation Early operation Esogastrectomy: stripping + jejunostomyEsogastrectomy: stripping + jejunostomy Late reconstruction Late reconstruction Difuse necrosis only esophagusDifuse necrosis only esophagus: :
esophagectomy (stripping) + esophagectomy (stripping) + reconstruction later reconstruction later
Difuse gastric necrosisDifuse gastric necrosis: total gastrectomy : total gastrectomy and reconstructionand reconstruction
TREATMENT PROTOCOLTREATMENT PROTOCOL gr. IIgr. II medical treatment medical treatment
Nothing per mouth ~20 daysNothing per mouth ~20 days +/- jejunostomy/gastrostomy+/- jejunostomy/gastrostomy
PrognosticPrognostic No complications no sequeleNo complications no sequele Complications: bleeding, perforation, stenosisComplications: bleeding, perforation, stenosis
STENOSIS: STENOSIS: Dilatation (risk of perforation)Dilatation (risk of perforation) Construction of a neo-esophagusConstruction of a neo-esophagus (stomach, (stomach,
colon, jejunum)colon, jejunum)
gr. Igr. I moderate lesions moderate lesions Healing without sequelsHealing without sequels Short surveilance (3 days) Short surveilance (3 days)
TREATMENT PROTOCOLTREATMENT PROTOCOL
BENIGN TUMORSBENIGN TUMORS
<1% of all E tumors<1% of all E tumors LeiomiomLeiomiomaa
Develops inside the wallDevelops inside the wall Can be visible within the lumenCan be visible within the lumen TTrreeatment atment
Endoscopic removal if pediculated Endoscopic removal if pediculated Surgical rezectin + reconstruction of neo-Surgical rezectin + reconstruction of neo-
esophagusesophagus EnucleationEnucleation

OTHER BENIGN TUMORSOTHER BENIGN TUMORS FibromaFibroma SSchwannomchwannom Branchial development cystsBranchial development cysts HHemangioamemangioamaa Adenomatous polypAdenomatous polyp
Originates in submucosal gland or ectopic Originates in submucosal gland or ectopic mucosamucosa
PPapiloapilomama Squamos cell epitheliumSquamos cell epithelium
MMixomixomaa
BENIGN TUMORSBENIGN TUMORS CAUSECAUSE
unknownunknown Inflammatory strictures may be a cause Inflammatory strictures may be a cause
that favorsthat favors DiagnosticDiagnostic
clinicclinicalal Esophageal syndrome or nothingEsophageal syndrome or nothing Complications: bleeding, compressionComplications: bleeding, compression
imagisticimagistic Barium swallow, endoscopy, CR, MRIBarium swallow, endoscopy, CR, MRI,,
endoscopic USendoscopic US
Tratament Tratament conservatconservativiv DilataDilatation +/-tion +/- Surgical removalSurgical removal RXT for hemangioma RXT for hemangioma