esophageal atresia
26
ESOPHAGEAL ATRESIA LAMYAA ANWAR ALGHAFLI
-
Upload
- -
Category
Health & Medicine
-
view
296 -
download
0
Transcript of esophageal atresia

ESOPHAGEAL ATRESIALAMYAA ANWAR ALGHAFLI

OBJECTIVES
Embryology of esophagus and trachea. Incidence and epidemiology of tracheoesophageal atresia. Classification of tracheoesophageal atresia. Associated anomalies. Diagnosis and treatment “Antenatal VS postnatal”.

EMBRYOLOGY

INCIDENCE AND EPIDEMIOLOGY
The birth incidence of varies between 1 in 2500 to 3000 live births. There is a slight male preponderance of 1.26 : 1. Environmental factors: 1-Thalidomide exposure OR use of methimazole in early pregnancy. 2-Prolonged use of contraceptive pills OR progesterone and estrogen exposure. 3-Maternal diabetes.
31,32 Chromosomal anomalies are found in 6–10% of the patients. The total number of trisomy 18 cases exceeds the total number of trisomy 21
cases. Three genes have been associated: MYCN, CHD7, and SOX2. It may occasionally seen in: 1-Fetal alcohol syndrome. 2-Maternal phenylketonuria. 3-Fanconi anemia. 4-Others.
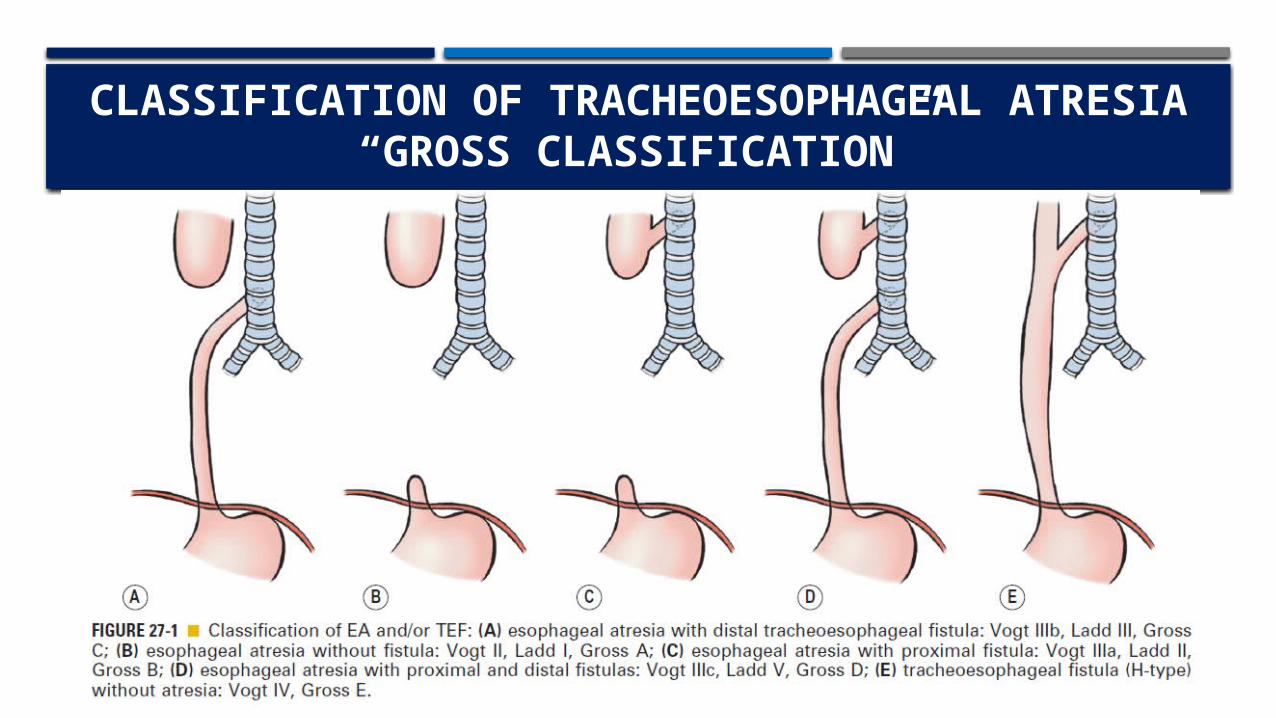
CLASSIFICATION OF TRACHEOESOPHAGEAL ATRESIA
“GROSS CLASSIFICATION”
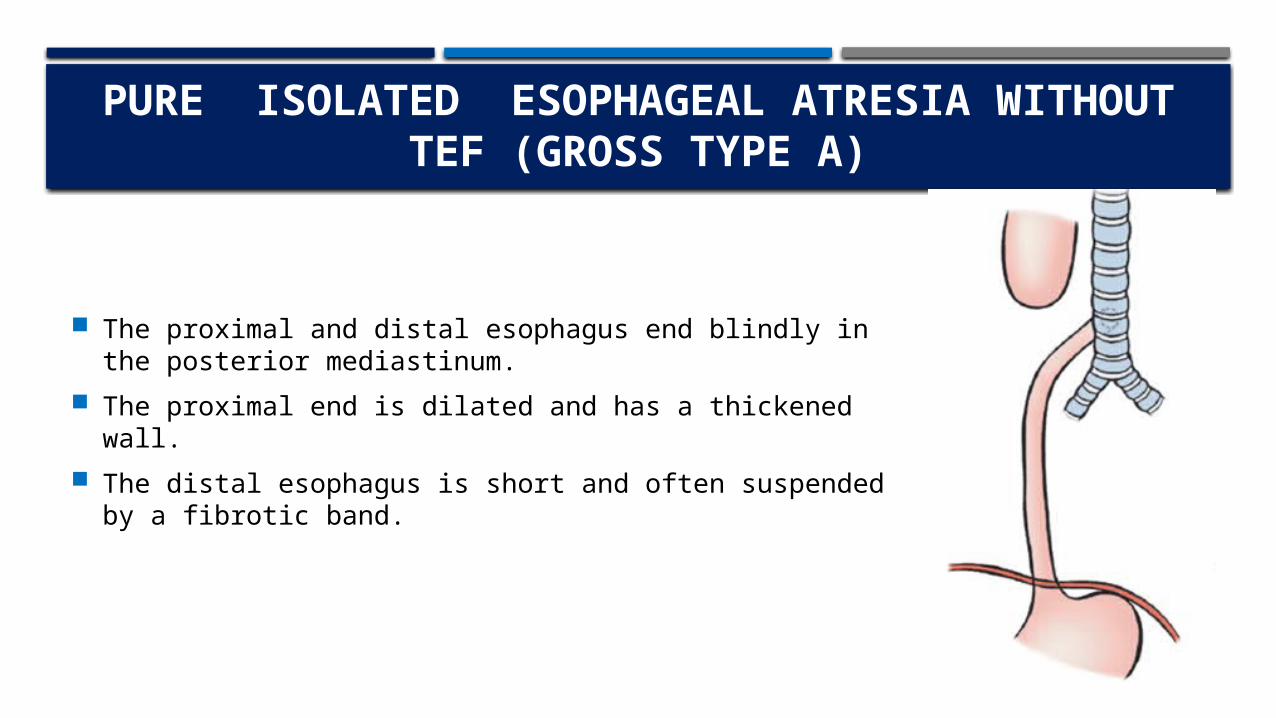
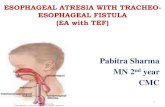
PURE” ISOLATED” ESOPHAGEAL ATRESIA WITHOUT TEF (GROSS TYPE A)
The proximal and distal esophagus end blindly in the posterior mediastinum.
The proximal end is dilated and has a thickened wall. The distal esophagus is short and often suspended by a
fibrotic band.
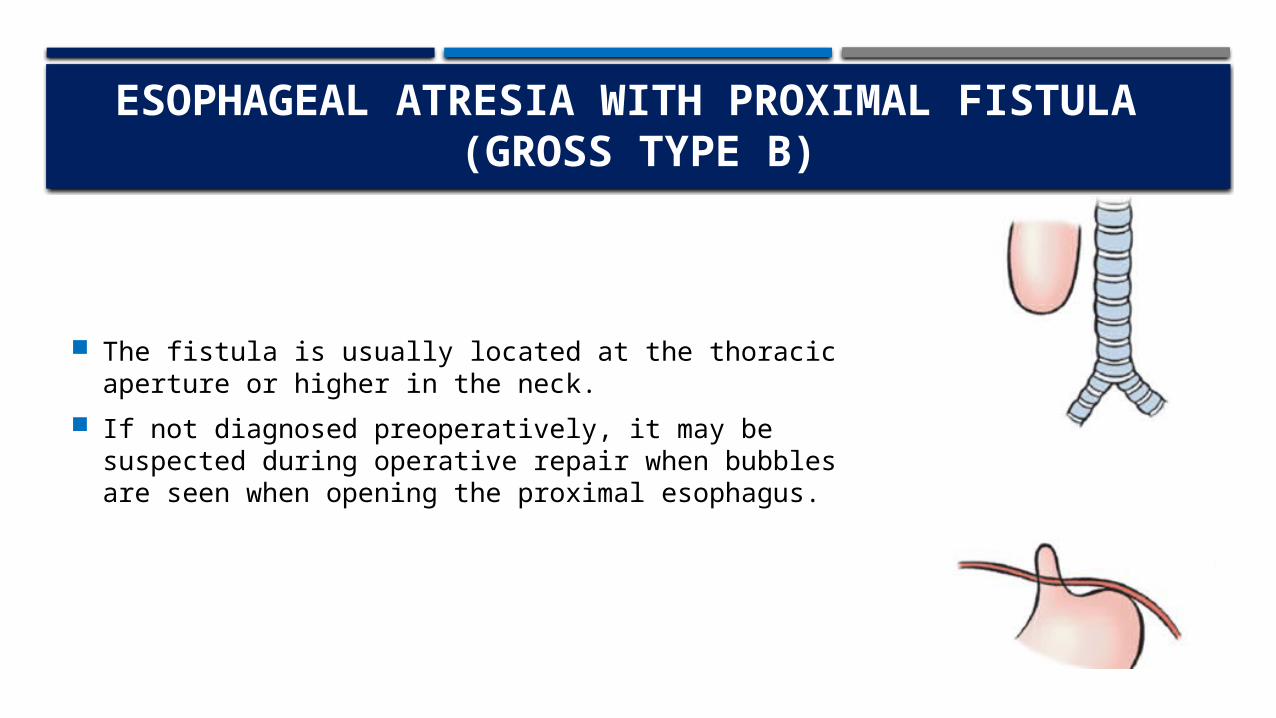
ESOPHAGEAL ATRESIA WITH PROXIMAL FISTULA
(GROSS TYPE B)
The fistula is usually located at the thoracic aperture or higher in the neck.
If not diagnosed preoperatively, it may be suspected during operative repair when bubbles are seen when opening the proximal esophagus.
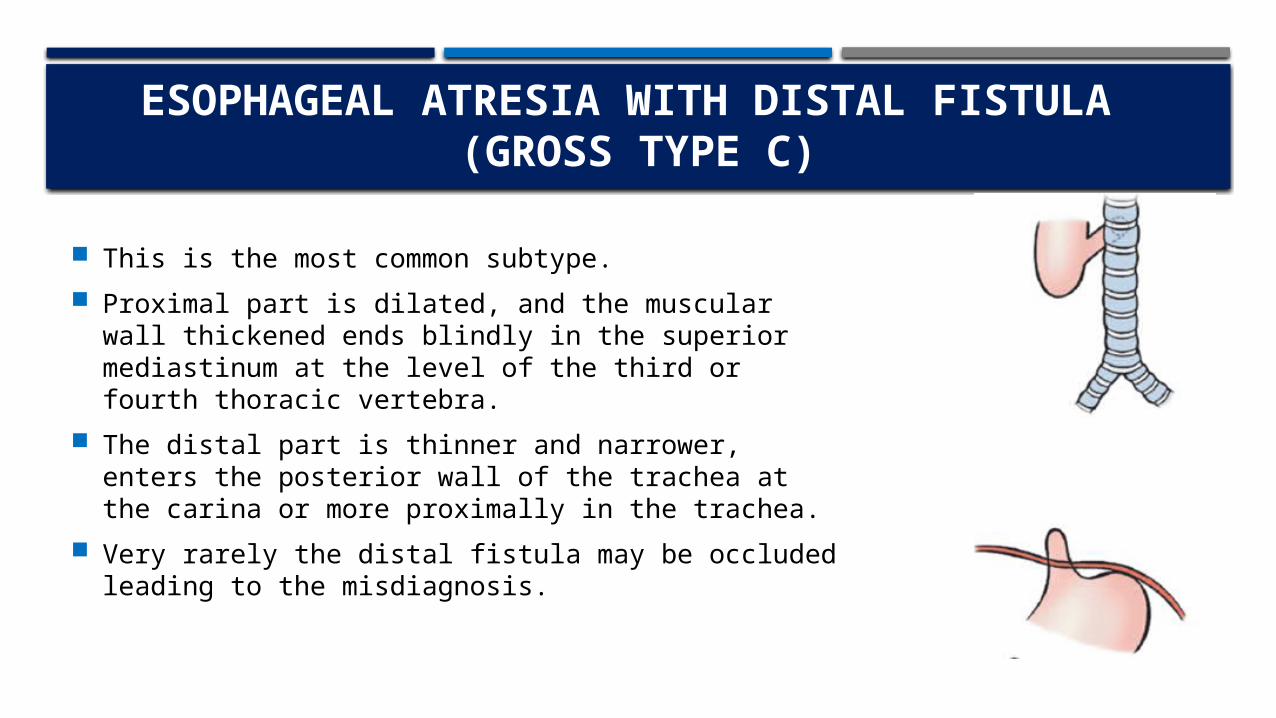
ESOPHAGEAL ATRESIA WITH DISTAL FISTULA (GROSS TYPE C)
This is the most common subtype. Proximal part is dilated, and the muscular wall
thickened ends blindly in the superior mediastinum at the level of the third or fourth thoracic vertebra.
The distal part is thinner and narrower, enters the posterior wall of the trachea at the carina or more proximally in the trachea.
Very rarely the distal fistula may be occluded leading to the misdiagnosis.
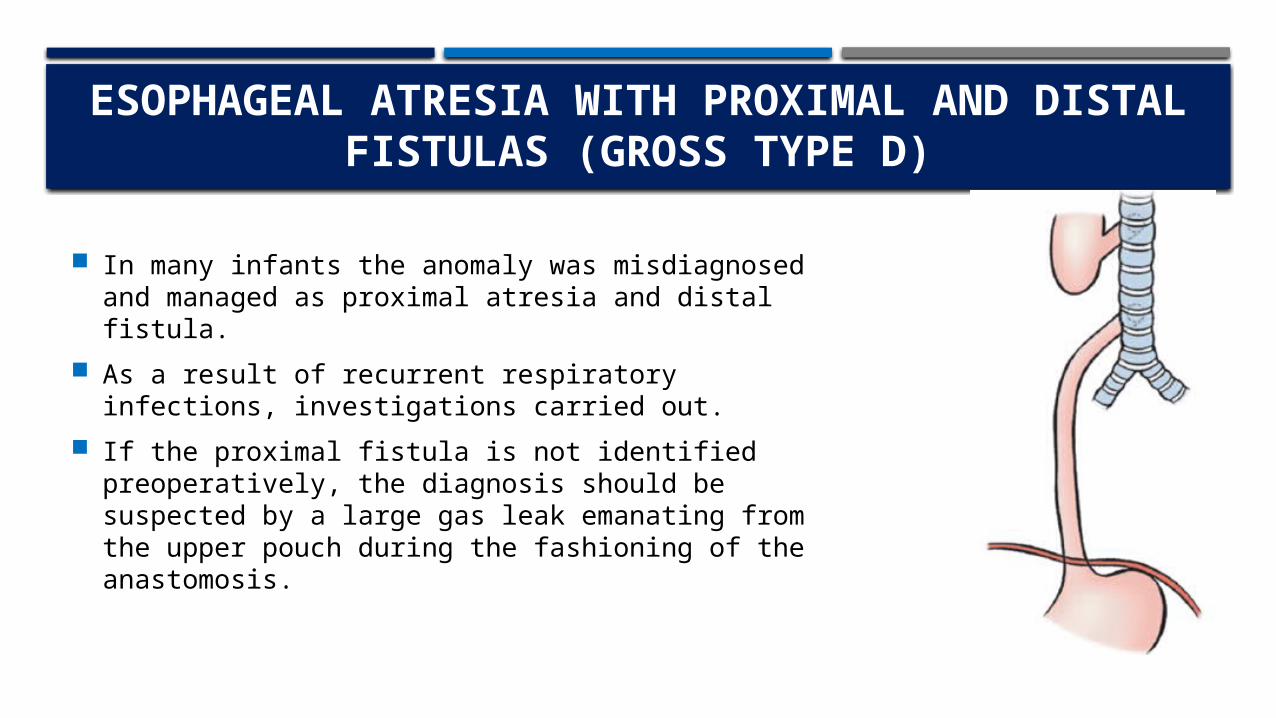
ESOPHAGEAL ATRESIA WITH PROXIMAL AND DISTAL FISTULAS (GROSS TYPE D)
In many infants the anomaly was misdiagnosed and managed as proximal atresia and distal fistula.
As a result of recurrent respiratory infections, investigations carried out.
If the proximal fistula is not identified preoperatively, the diagnosis should be suspected by a large gas leak emanating from the upper pouch during the fashioning of the anastomosis.

H-TYPE FISTULA WITHOUT ESOPHAGEAL ATRESIA
(GROSS TYPE E)
It may be part of the VACTERL association. The fistula starts from the membranous trachea and runs
caudad to enter the esophagus. Normally it is short. The fistula is usually situated at the thoracic aperture or
higher in the neck.

ASSOCIATED ANOMALIES EA divided clinically into: 1-Isolated EA. 2-Syndromic EA. The most frequent associated malformations encountered in syndromic EA are:• Cardiac (13–34%).• Vertebral (6–21%).• Limb (5–19%).• Anorectal (10–16%).• Renal (5–14%).
VACTERL association CHARGE association Vertebral Coloboma Anorectal Heart defects Cardiac Atresia of the choanae Tracheo-esophageal Developmental retardation Renal Genital hypoplasia Limb abnormalities Ear deformities

DIAGNOSIS AND TREATMENT
Prenatal Diagnosis two nonspecific signs on ultrasound scan performed after the 18th week of
gestation: 1-polyhydramnios. 2-Absent or small stomach bubble. The combination of a small stomach together with a dilated cervical esophagus
(the pouch sign) has been confirmed to be diagnostic for pure EA in a number of patients.
Postnatal Diagnosis Excessive salivation requiring repeated suctioning. A catheter passed into the esophagus and do x-ray for the chest and abdomen, the
tip arrested in the superior mediastinum while gas in the stomach and intestine signifies the presence of a distal tracheooesophageal fistula.
The absence of gastrointestinal gas is indicative of an isolated atresia.

Radiographs may reveal associated anomalies such as vertebral and rib anomalies, or duodenal atresia.
Mediastinal ultrasound, CT and MRI could be helpful. Bronchoscopy perform prior to exploration to assess the distal fistula and upper
pouch fistula. Echocardiography should be performed prior to operation to reveal cardiac and/or
aortic arch anomalies. Renal ultrasound and spine radiographs should be obtained as well.

MANAGEMENT
Preoperative A suction catheter is placed to prevent aspiration. The child is positioned head-up and on his\her side, Intravenous access and the
vital signs are monitored. If the child is in respiratory distress, endotracheal intubation and ventilation may
be needed. Forceful ventilation will over distend the stomach, causing diaphragmatic splinting
and gastric rupture. Gentle low-pressure ventilation is therefore essential.

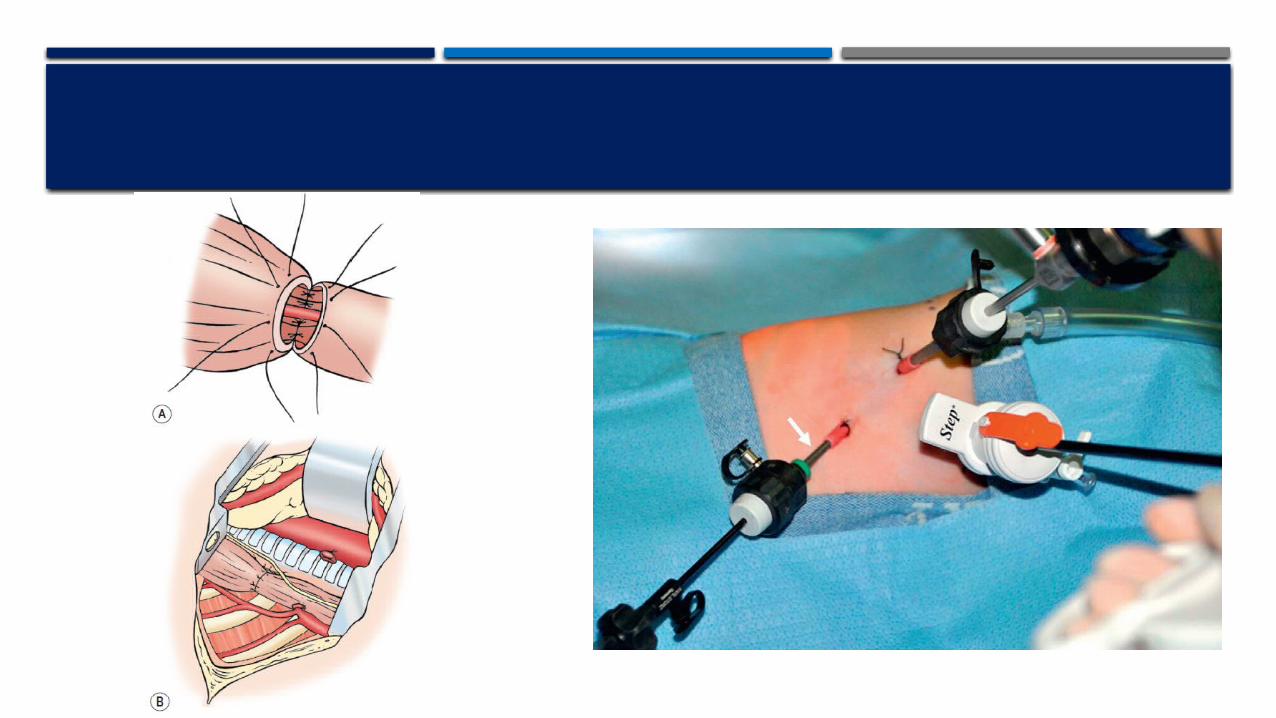
Under general anesthesia. With adequate venous access. Pulse oximeter. End tidal CO2 monitor. Thoracotomy or using a thoracoscopic approach. The side of entrance into the chest is opposite the turn of the aortic arch.


Make incision in the baby chest, usually in the right side. Through the incision, gently move the lung to aside to view the trachea and
esophagus. After identifying the tracheoesophageal fistula, slowly close the fistulas connection
to the trachea with sutures then cut the connection away from the trachea. The fistulas connection to the esophagus will also be cut and the fistula will be
removed. Make an incision at the end of the upper esophagus to open it. Then the upper and the lower esophagus will be connected with sutures. Finally, insert a surgical drain in the chest and close the incision with sutures.

AFTER THE PROCEDURE
The baby will continue to use the breathing tube until they have healed enough to breath on their own.
The baby will taken to neonatal intensive care unit for monitoring. Pain medication will be given. The baby may continue to receive antibiotics through the IV. Babies are released from the hospital when they were able to eat enough to
maintain their weight which may be after two weeks or longer.


RECOURSE
ASHCRAFT'S Pediatric Surgery book Bailey & Love's short practice surgery book Spitz, L. (2007). Oesophageal atresia. Orphanet journal of rare diseases, 2(1), 1. Teich, S., Barton, D. P., Ginn-Pease, M. E., & King, D. R. (1997). Prognostic classification for
esophageal atresia and tracheoesophageal fistula: Waterston versus Montreal. Journal of pediatric surgery, 32(7), 1075-1080.

THANK YOU FOR LISTENING