ESMO MAGNITUDE OF CLINICAL BENEFIT SCALE...Grade 4 Mark with X if relevant HR 0.70 AND Gain 9 months...
40
ESMO MAGNITUDE OF CLINICAL BENEFIT SCALE Rolf Stahel University Hospital Zürich Mexico 21.4..2018
Transcript of ESMO MAGNITUDE OF CLINICAL BENEFIT SCALE...Grade 4 Mark with X if relevant HR 0.70 AND Gain 9 months...

ESMO MAGNITUDE OF CLINICAL BENEFIT SCALE
Rolf Stahel
University Hospital Zürich
Mexico 21.4..2018

BACKGROUND
Differences between countries in:
– drug related health care expenditures
– drug prices
– access time to drugs after approval by EMA
Sometimes lack of drug supply in “countries with cheaper drugs” due to parallel import to “countries where the drug is more expensive”.
Unequal access within some countries:
– sometimes (co)-payment of the drug costs by patients required
Differences in access to relevant new anticancer drugs in
Europe

BACKGROUND
• Committed
to promote high-quality, rational, responsible & affordable cancer care
• Recognises
the need for clear and unbiased statements regarding the magnitude of clinical benefit from new therapeutic approaches
• Wants to
highlight treatments which bring substantial improvements to the duration of survival and/or the QoL of cancer patients
use the scale for accelerated reimbursement evaluation
ESMO position

ESMO MCBS
• Cure takes precedence over deferral of death
• Direct endpoints such as survival and QoL take precedence over surrogates* such as PFS or RR
• DFS in curative disease is a more valid surrogate than PFS or RR in non-curative disease
• Interpretation of the evidence for benefit derived from surrogate outcomes (such as PFS) may be influenced by secondary outcome data
Underlaying premises
* EMA recognizes PFS and valid endpoint

Factors taken into account for ESMO-MCBS
Magnitude of Clinically Benefit
Overall survival,
Progression free survival
Toxicity
Costs
Prognosis of the
condition
Quality of Life
HR,Long term survival,
RR
Not analyzed in view of significant “Heterogeneity”across Europe

Definition ESMO-MCBS substantial improvements
• Curative setting A & B or non-curative setting 5 & 4
Curative Non-curative
5
4
3
2
1
A
B
C

ESMO-MCBS v1.0developed by task force, field testing & simulation scenarios
v1.0
Patients


ESMO MCBS V1.1
Reasons to develop an updated version
• The ESMO-MCBS is a dynamic tool
• v1.0 only scored comparative studies need grade single arm studies
• Further reasons for revision
– Experience field testing and scoring recent studies
– Input/queries from clinicians and industry
– Active internal peer review
• Detailed discussions & field testing
• ESMO-MCBS v1.1: Annals of Oncol, Cherny et al. September 2017


FORMS ESMO-MCBS V1.1
Curative Setting → Evaluation form 1
A, B, C
Non-curative setting → Evaluation form 2a
5, 4, 3, 2, 1
Evaluation form 2b
4, 3, 2, 1
Evaluation form 2c
4, 3, 2, 1
Non-curative setting → Evaluation form 3
Single arm studies 4, 3, 2, 1

Evaluation form 1: for new approaches to adjuvant therapy or new potentially curative therapies
Grade AMark with X if
relevant
>5% improvement of survival at ≥3 years follow-up
Improvements in DFS alone (primary endpoint) (HR <0.65) in studies
without mature survival data
≥ 3% but ≤ 5% improvement at ≥3 years follow-up
Improvement in DFS alone (primary endpoint) (HR 0.65 - 0.8) without
mature survival data
Non-inferior OS or DFS with reduced treatment toxicity or improved
Quality of Life (with validated scales)
Non-inferior OS or DFS with reduced treatment cost as reported study
outcome (with equivalent outcomes and risks)
<3% improvement of survival at ≥ 3 years follow-up
Improvement in DFS alone (primary endpoint) (HR >0.8) in studies
without mature survival data
Improvements in pCR alone (primary endpoint) by >30% relative AND
>15% absolute gain in studies without mature survival data
Grade B
Grade C

Trastuzumab after Adjuvant Chemotherapyin HER2-Positive Breast Cancer
Picart, NEJM 2005

ESMO-MCBS distinctions v1.1: for treatment with non-curative intent
PFS or TTP
Primary endpoint
OS
Median with
standard therapy
≤ 1 year > 1-2 years
Median with
standard therapy
≤ 6 months > 6 months
Other than
OS or PFS
> 2 years

Evaluation form 2a: for therapies that are not likely to be curative with primary endpoint OS
IF median OS with the standard treatment <12 months
Grade 4Mark with X
if relevant
HR ≤0.65 AND Gain ≥3 months
Increase in 2 year survival alone ≥10%
HR ≤0.65 AND Gain >2.0 - <3 months
HR ≤0.65 AND Gain >1.5 - <2 months
HR >0.65-0.70 AND Gain >1.5 months
HR > 0.70 OR Gain <1.5 months
Grade 3
Grade 2
Grade 1

Evaluation form 2a: for therapies that are
not likely to be curative with primary endpoint OS
4 3 2 1
Preliminary magnitude of clinical benefit grade
Assessment QoL & grade 3-4 toxicities
Final adjusted magnitude of clinical benefit grade
5 4 3 2 1
Upgrade 1 level if improved QoL or toxicity is shown
Step 1
Step 2
Step 3
If there is a long term plateau in the survival curve, and OS advantage continues to be observed at 5/7 year, also score according to Form 1 (treatments with curative potential) and present both scores i.e. A/4
Does secondary endpoint quality of life show improvement
Are there statistically significantly less grade 3-4 toxicities
impacting on daily well-being*

Nivolumab versus docetaxel in advanced squamous cell NSCLC
Brahmer, NEJM 2015

Less toxicity with immune checkpoint inhibitors in second line comparative studies
18 |
ToxicityGade
% of patients
Check-mate 17 Checkmate 57 KEYNOTE 10
N Doc N Doc P2 P10 Doc
All 59 87 69 88 63 66 35
3-5 8 60 10 54 13 16 79

Gemcitabine and cisplatin with or without necitumumab in squamous cell lungcancer
Thatcher, Lancet Oncol 2015

Docetaxel taxel plus ramucirumab (REVEL) versus docetaxel plus placebo for 2nd line treatment of stage IV NSCLC
20 |
OS 10.5 vs 9.1 months
Garon, Lancet Oncol 2014

Evaluation form 2a: for therapies that are not likely to be curative with primary endpoint OS
IF median OS with the standard treatment > 12 months <24 months
Grade 4Mark with X
if relevant
HR ≤0.70 AND Gain ≥5 months
Increase in 3 year survival alone ≥10%
HR ≤0.70 AND Gain >3-<5 months
HR ≤0.70 AND Gain >1.5-<3 months
HR >0.70-0.75 AND Gain >1.5 months
HR > 0.75 OR Gain <1.5 months
Grade 3
Grade 2
Grade 1

Evaluation form 2a: for therapies that are not likely to be curative with primary endpoint OS
IF median OS with the standard treatment >24 months
Grade 4Mark with X
if relevant
HR ≤0.70 AND Gain ≥9 months
Increase in 5 year survival alone ≥10%
HR ≤0.70 AND Gain >6 - <9 months
HR ≤0.70 AND Gain >4 - <6 months
HR >0.70-0.75 AND Gain >4 months
HR >0.75 OR Gain <4 months
Grade 3
Grade 2
Grade 1

Studies with median PFS with standard treatment <6 months
Grade 3Mark with X
if relevant
HR ≤0.65 AND Gain >1.5 months
HR <0.65 BUT Gain <1.5 months
HR >0.65
Grade 2
Grade 1
Evaluation form 2b: for therapies that are
not likely to be curative with primary endpoint PFS

Studies with median PFS with standard treatment >6 months
Grade 3Mark with X
if relevant
HR ≤0.65 AND Gain > 3 months
HR <0.65 BUT Gain < 3 months
HR >0.65
Grade 2
Grade 1
Evaluation form 2b: for therapies that are not likely to be curative with primary
endpoint PFS

Evaluation form 2b: for therapies with PFS improval without an OS benefit that are
not likely to be curative
3 2 1
Preliminary magnitude of clinical benefit grade (highest grade scored)
Step 1
Step 2
Early stopping or crossover
Did the study have an early stopping rule based on interim analysis of
survival?
Was there early crossover because or early stopping or crossover based
on detection of survival advantage at interim analysis
(If the answer to both is “yes”, then see adjustment “a” below)

Evaluation form 2b: for therapies with PFS improval without an OS benefit that are
not likely to be curative
Step 3Toxicity and QoL adjustment when only a PFS improvement
Is the new treatment associated with a statistically significant incremental
rate of:
Mark with X
if relevant
«toxic» death >2%
Cardiovascular ischemia >2%
Hospitalization for «toxicity» >10%
Excess rate of severe CHF >4%
Grade 3 neurotoxicity >10%
Severe other irreversible or long lasting toxicity >2% please specify:
Toxicity assessment
(Incremental rate refers to the comparison versus standard therapy in the control arm)

Evaluation form 2b: for therapies with PFS improval without an OS benefit that are not
likely to be curative Assessment QoL & grade 3-4 toxicities
Highest grade that can be achieved grade 4
Step 3
a) When OS as 2nd endpoint is improved, it prevails, score according to form 2a
b) Downgrade 1 level if ≥ 1 of above incremental toxicities
c) Downgrade 1 level if the drug ONLY leads to improved PFS (mature data shows no OS advantage) and
QoL assessment does not demonstrate improved QoL
d) Upgrade 1 level if > QoL or if less grade 3-4 toxicities that bother patients
e) Upgrade 1 level if study had early crossover because of early stopping or crossover based on detection
of survival advantage at interim analysis
f) Upgrade 1 level if there is a long term plateau in the PFS curve, and there is >10% improvement in PFS
at 1/2 year
Final, toxicity and QoL adjusted, magnitude clinical benefit grade
Step 4
Was quality of life (QoL) evaluated as secondary outcome?
Does secondary endpoint quality of life show improvement
Are there statistically significantly less grade 3-4 toxicities impacting on
daily well-being*
4 3 2 1

EGFR-mutated advanced NSCLC: Erlotinib with bevacizumab in frist-line
JO25567: Ph2, randomized, Japanese multicenter, open-label trial
Seto, Lancet Oncol 2014

Erlotinib alone or with bevacizumab as first-line therapy in advancedNSCLC harbouring EGFR mutations (JO25567)
29 |Seto. Lancet Oncol 2014

Evaluation form 2c: for therapies that arenot likely to be curative with primary endpoint other than
OS or PFS and or equivalence studies
Primary outcome is Toxicity or Quality of life AND Non-inferiority Studies
Grade 4
Mark with X
if relevant
Reduced toxicity or improved QoL (using validated scale) with evidence
for statistical non-inferiority or superiority in PFS/OS
Improvement in some symptoms (using a validated scale) BUT without
evidence of improved overall QoL
RR is increased >20% but no improvement in toxicity/QoL/PFS/OS
RR is increased <20% but no improvement in toxicity/QoL/PFS/OS
Grade 2
Grade 1
Grade 3

Evaluation form 3: for single-arm studies in “orphan diseases” and for diseases with “high unmet need” when primary
outcome is PFS or ORR
Grade 3Mark with X
if relevant
PFS >6 months
ORR (PR+CR) >60%
ORR (PR+CR) >20, <60% AND Duration of response >9 months
PFS >3-<6 months
ORR (PR+CR) >40, <60%
ORR (PR+CR) >20, <40% AND Duration of response >6 months <9 months
PFS 2-<3 months
ORR (PR+CR) >20, <40% AND Duration of response <6 months
ORR (PR+CR) >10, <20% AND Duration of response >6 months
Grade 2
Grade 1

Preliminary magnitude of clinical benefit grade
Final adjusted magnitude of clinical benefit grade
Step 1
Step 2
Step 3
Adjustments 1. Downgrade 1 level if there are > 30% grade 3-4 toxicities impacting
on daily well being2. Upgrade 1 level if improved QoL 3. Upgrade 1 level for confirmatory, adequately sized, phase 4
experience
Evaluation form 3: for single-arm studies in “orphan diseases” and for diseases with “high unmet need” when primary outcome is PFS or ORR
3 2 1
4 3 2 1

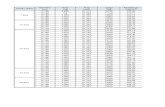
EMA APPROVED SINCE 2016 SCORED WITH ESMO-MCBS
Tumor type Medicine ESMO-MCBS score
NSCLC 2L Nivolumab 5
NSCLC 2L Pembrolizumab 5 in PD-1 > 50%
NSCLC 2L Pembrolizumab 3 in PD-L1 > 1%
NSCLC (EGFR mutated together with erlotinib) Bevacizumab 2
NSCLC 2L Ramucirumab 2
NSCLC 2L Squamous Afatinib 1
NSCLC 1L Squamous Necitumumab 1
NSCLC change to existing indication (2L non-mutated)
Erlotinib 1

New EMA approval after Jan
1st, 2016
a. ESMO Guideline staff
b. Guideline SE + Author
E-Update MCBS WG
Final E-Update approved by ESMO
GL-SC and Presidents
Exec Board
Arbitration only
ESMO-MCBS included in ESMO Guidelines

ESMO guidelines
• In 2016 and 2017 there were over 1 million unique page views* of ESMO Guidelines pages on the ESMO.org website
• These totals represent ~22% of all unique page views on the ESMO.org website
2011 2012 2013 2014 2015 2016 2017
Total 89 530 100 738 394 889 734 150 892 540 1 052 185 1 377 993
*Unique Page views: the number of visits during which a page was viewed one or more times

1 NCCN 2 NICE 3 ESMO 4 ASCO
Primary purpose Providers, patients & other stakeholders in treatment decision
Produce guidance:Public healthClinical practiceHealth technologies
Inform public policy, clinical guidelines, clinical practice
Shared decision making, patients/MDs
Treatment modalities Systemic therapies in all major cancer types
Medicines, treatments and procedures
Drugs for solid tumors Drugs for solid &hematologic malignancies
Data source informing framework
Clinical trials & expert consensus
Clinical trials, experts,service users, carers & public
Clinical trials Clinical trials
Scoring/Grading
Evidence blocks Score: 5-1 Clinical benefit, health benefit,
A-C: curative disease5-1: adv disease
Net Health Benefit score
Cost Affordability scale (1-5) Costs, cost effectiveness (QALY)
Not addressed Cost/month (Advdisease), Cost/course (Adjdisease)
Updating Yearly, changes as impact of therapies change
Dynamic Dynamic Dynamic
Modified from Schnipper et al. Oncologist 2016

Clinical benefit of 37 anticancer drugs approved by the FDA from 2000 to 2015
Vivot, Ann Oncol 2017

No relation between price and clinical benefit of 37 FDA approved anticancer drugs 2000-2015
Vivot, Ann Oncol 2017

MAGNITUDE OF CLINICAL BENEFIT OF CANCER DRUG APPROVED BY FDA 2006-2015
• 63 individual drugs for 118 indications
• 135 studies, among which were 105 RCTs for which ESMO-MCBS could beapplied
• Over time, there has been an increase in the number of trials meeting the ESMO-MCBS threshold (Ptrend = .04)
• However, fewer than half of RCTs supporting FDA approval meet thethreshold for clinically meaningfulbenefit
Tibau, JNCI 2018

Tumor type Drug ESMO-MCBS score
NSCLC Nivolumab 5
NSCLC Pembrolizumab 5 in PD-1 > 50%
Renal cell carcinoma Nivolumab 5
Melanoma Nivolumab 4 nivolumab alone
Renal cell carcinoma Lenvatinib 4
Soft tissue sarcoma Olaratumab 4 olaratumab + doxorubicin
Breast cancer Palbociclib 4 palbociclib + fulvestrant
3 palbociclib + letrozole
NSCLC Pembrolizumab 3 in PD-L1 > 1%
Colorectal cancer Ramucirumab 3
Neuroendocrine tumor Everolimus 3
Renal cell carcinoma Cabozantinib 3
NSCLC Bevacizumab 2
NSCLC Ramucirumab 2
Colorectal cancer Trifluridine/tipiracil 2
Melanoma Nivolumab 2 nivolumab + ipilimumab
NSCLC Afatinib 1
NSCLC Necitumumab 1
NSCLC change to existing indication Erlotinib 1
EMA approved since 2016 scored with ESMO-MCBS