ESMO E-Learning Diagnostic Work Up in NSCLC and the … · 2019-08-23 · Zheng D, et al....
53
DIAGNOSTIC WORK UP IN NSCLC AND THE IMPORTANCE OF OPTIMAL TISSUE MANAGEMENT IN THE ERA OF PRECISION MEDICINE Noemí Reguart, MD, PhD Hospital Clinic Barcelona, Barcelona, Spain Cristina Teixidó, MSc, PhD Hospital Clinic Barcelona, Barcelona, Spain
Transcript of ESMO E-Learning Diagnostic Work Up in NSCLC and the … · 2019-08-23 · Zheng D, et al....

DIAGNOSTIC WORK UP IN NSCLC AND THE IMPORTANCE OF OPTIMAL TISSUE MANAGEMENT IN THE ERA OF PRECISION MEDICINE
Noemí Reguart, MD, PhD
Hospital Clinic Barcelona, Barcelona, Spain
Cristina Teixidó, MSc, PhD
Hospital Clinic Barcelona, Barcelona, Spain

OUTLINE
◆ Advanced NSCLC: a need for personalised therapy
◆ Diagnostic workup of lung cancer:
⁃ Type of samples
⁃ Morphology and histology
⁃ Material for biomarker studies
◆ Overview of key genetic alterations in NSCLC
⁃ Techniques for diagnose
◆ Guidelines for genetic testing
◆ Summary / conclusions

OUTLINE
◆ Advanced NSCLC: a need for personalised therapy
◆ Diagnostic workup of lung cancer:
⁃ Type of samples
⁃ Morphology and histology
⁃ Material for biomarker studies
◆ Overview of key genetic alterations in NSCLC
⁃ Techniques for diagnose
◆ Guidelines for genetic testing
◆ Summary / conclusions

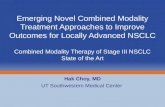
EVOLUTION OF LUNG CANCER DIAGNOSIS
Lung cancer classification has moved from histologic to molecular classification
H&E Molecular Testing
IHC
FISH
by 2000 2019
Genetic Testing Assays
FISH, fluorescent in situ hybridisation; H&E, hematoxylin and eosin stain; IHC, immunohistochemistry.
Images courtesy of Dr C Teixidó and Dr N Reguart

NOS, not otherwise specified. Adapted from Li T, et al. J Clin Oncol 2013;31:1039–49
NSCLC MOLECULAR CLASSIFICATION
NSCLC classification has moved from histologic to molecular subtyping
Molecular Testing: Adenocarcinoma and NSCLC-NOS histologies

DRIVER ONCOGENES IN LUNG ADENOCARCINOMA
BY ETHNICITY
USA/Europe East Asia
EGFR 5-15% 40-55%
KRAS 20-30% 8-10%
ALK 3-6% 3-5%
ROS1 1-2% 2-3%
BRAF 2-3% 0.5-1%
RET 1-2% 1-2%
MET 4% 1.3%
HER2 2-3% 2-3%
NTRK 1% <1%
More than 50% of all lung adenocarcinomas harbour driver oncogenes
Incidence of genomic driver is variable among ethnic populations
Kohno T, et al. Transl Lung Cancer Res 2015;4(2):156–64; Sehgal K, et al. Transl Cancer Res 2018; 7(Suppl 7):S779–S786;
Zheng D, et al. Oncotarget 2016;7(27):41691–702.

METASTATIC NSCLC: ESMO CLINICAL PRACTICE GUIDELINES
Stage IV Non-Squamous Cell Carcinoma
Molecular Tests Negative (PD-L1 expression)
Stage IV Squamous Cell Carcinoma
Molecular Tests Positive (ALK/BRAF/EGFR/ROS1)A BA B
LoE Levels of evidence (I-V); GoR nd grades of recommendation (A-E); TMB, tumour mutational burden.Planchard D, et al. Ann Oncol 2018;29(Supplement_4):iv192–iv237, by permission of Oxford University Press on behalf of the European Society for Medical Oncology.

OUTLINE
◆ Advanced NSCLC: a need for personalised therapy
◆ Diagnostic workup of lung cancer:
⁃ Type of samples
⁃ Morphology and histology
⁃ Material for biomarker studies
◆ Overview of key genetic alterations in NSCLC
⁃ Techniques for diagnose
◆ Guidelines for genetic testing
◆ Summary / conclusions

Interventional
radiologist,
pulmonologist or
surgeon obtains
tissue for
diagnosis Lab or
pathologist
sends the
report to the
clinical care
team
Results within 10 working days (receipt of sample
by the lab to the clinical care team)
Oncologist
receives
results
SAMPLE JOURNEY FOR TESTING
Diagnose
and subtype
◆ Before starting, review relevant clinical information,
such as:
- Sample site
- Clinical suspicion on primary lung tumour or metastasis
- Reason for biopsy: diagnosis, molecular evaluation,
resistance
- Smoking history
◆ Then, stablish diagnostic work up:
⁃ FIRST→ Establish malignancy
⁃ SECOND → Define type of malignancy
⁃ THIRD→ Perform molecular testing as appropriate and
prioritise testing according to individual patients
1 2 3
Personalised
treatment
Sample
pre-analytics
Perform
Molecular testing
Adapted from Aisner DL, et al. Am J Clin Pathol. 2012;138:332–46 Adapted from Thunnissen E, et al. Lung Cancer 2012;76(1):1–18

NSCLC, non-small cell lung cancerImages courtesy of Dr C Teixidó and Dr N Reguart
THE HARSH REALITY OF TUMOUR SAMPLES
FOR DIAGNOSIS
Type of samples: cytology and formalin-fixed paraffin embedded (FFPE)
◆ Diagnostic material is generally scarce and it is essential to balance requirements for an accurate histologic diagnosis with the
need for molecular analyses
◆ When biopsy and cytology material from an individual patient are analysed by different professional (histopathologists and
cytologists), it is essential that they share information
◆ 40% NSCLC diagnosed by cytology
Ideal Sample SizeThe Reality Sample Size

1. IHC should not be performed unless necessary!!!!
2. In NSCLC-NOS, IHC reduces the number of
inconclusive diagnoses (rate <10%)
3. Limiting IHC between 2 and 4 markers seems
reasonable
HISTOLOGY: IMMUNOHISTOCHEMICAL MARKERS
Type of malignancy
TUMOUR TYPE IHC
Adenocarcinoma (ADC) CK7, TTF-1
Squamous cell carcinoma (SCC) P40 (P63, less specific)
Neuroendocrine (LCNEC, SCLC)CD56 (NSE, chromogranin,
synaptophysin)
◆ In NSCLC biopsy samples the following terminology
should be used:
⁃ ADC IHC not required if diagnostic morphology present
⁃ SCC IHC not required if diagnostic morphology present
⁃ Carcinomas lacking clear differentiation by morphology
and special stains are classified as NSCLC-NOS
⁃ NOS that stain with adenocarcinoma markers, classified
as NSCLC, favor adenocarcinoma
⁃ NOS that stain with squamous markers, classified as
NSCLC, favor squamous cell carcinoma
ADC, adenocarcinoma; LCNEC, large cell neuroendocrine carcinoma; NOS not otherwise specified; NSCLC, non-small cell lung cancer; SCC, squamous cell carcinoma;
SCLC, small-cell lung cancer.Travis WD, et al. WHO 4th ed. Lyon, France: IARC Press; 2015

HISTOLOGY: IMMUNOHISTOCHEMICAL MARKERS
Type of malignancy
Squamous cell carcinoma, P40 positiveLung adenocarcinoma, TTF1 positive
Images courtesy of Dr D. Martinez, Hospital Clinic Barcelona

TISSUE QUALITY CONTROL FOR MOLECULAR TESTING
Pathologist review H&E section and mark areas for analysis
The molecular specialist must evaluate whether the percentage of tumour in a given specimen reaches the detection
threshold of the specific molecular test or tests
H&E
SAMPLE
T
T
T
Assess tumour percentage and viability
Select ADC if mixed for testing
ADC, adenocarcinoma; H&E, haematoxylin and eosin stain; T, tumour. Images courtesy of Dr C Teixidó and Dr N Reguart

MOLECULAR TECHNIQUES AVAILABLE IN
ROUTINE DIAGNOSIS
◆ IHC
Single-marker molecular tests Multiplex-marker molecular tests
Illumina NextSeq Qiagen GeneReaderIon Torrent S5Ion Torrent PGMIllumina MiSeq
◆ PCR ◆ FISH ◆ Multiplex test
◆ Massively parallel / NGS
FISH, fluorescent in situ hybridisation; IHC, immunohistochemistry; NGS, next generation sequencing; PCR, polymerase chain reaction. Images courtesy of Dr C Teixidó and Dr N Reguart

MOLECULAR TECHNIQUES AVAILABLE IN
ROUTINE DIAGNOSIS
Tissue requirements
H&E
SAMPLE
◆ IHC
◆ FISH
⌁50-100 cells*
Selection on tumour areas
⌁ 600-1000 cells*
◆ RT-PCR
◆ nCounter
◆ NGS
Whole tissue sections
*Numbers are approximations and tissue requirements depends on technique/ reagent/ platform
FISH, fluorescent in situ hybridisation; H&E, hematoxylin and eosin stain; IHC, immunohistochemistry; NGS, next generation sequencing;
RT-PCR, reverse transcription polymerase chain reactionImages courtesy of Dr C Teixidó and Dr N Reguart

STRATEGY TO MAXIMISE TISSUE FOR MOLECULAR TESTING
Molecular testing sections can be prepared:
Together with first H&E section
After initial H&E for histological diagnosis
H&E for histological diagnosis
Repeat
sectioning
For IHC
For Molecular Testing
H&E
◆ At the time of initial sectioning for morphologic diagnosis,
additional sections may be taken, in anticipation of IHC or
predictive markers analyses
⁃ Technicians should preserve as much tissue as
possible for further evaluations
◆ Using cytology samples, cell block preparation from clot
formed by remaining fluid should be obtained in
combination with smears to improve diagnostic information
H&E, haematoxylin and eosin stain; IHC, immunohistochemistryImages courtesy of Dr C Teixidó and Dr N Reguart

OUTLINE
◆ Advanced NSCLC: a need for personalised therapy
◆ Diagnostic Workup of lung cancer:
⁃ Type of samples
⁃ Morphology and Histology
⁃ Material for Biomarker Studies
◆ Overview of key genetic alterations in NSCLC
⁃ Techniques for diagnose
◆ Guidelines for genetic testing
◆ Summary / conclusions

EGFREpidermal Growth Factor Receptor

HOTSPOTS FOR EGFR GENE MUTATIONS
◆ Activating (and sensitising) EGFR mutations
are predictive for response to EGFR tyrosine
kinase inhibitors
◆ More common:
⁃ Never-smokers
⁃ Women
⁃ Adenocarcinoma subtype
◆ Alterations:
⁃ Insertions
⁃ Deletions
⁃ Point mutations
Reprinted by permission Springer]: Mod Pathol, Molecular pathology of lung cancer: key to personalized medicine, Cheng L, et al. Copyright 2012

EGFR MUTATION ASSAYS
Adapted from IASLC Textbook in Thoracic Oncology 2014
METHODTUMOUR DNA
REQUIRED (%)
Sanger direct sequencing 25
Real time/ TaqMan PCR 10
High Resolution melting analysis 5-10
Cobas 5-10
Pyrosequencing 5-10
SNaPshot PCR 1-10
MALDI-TOF MS-based genotyping 5
Cycleave PCR 5
Fragment lenght and RFLP analysis 5
Allelic specific PCR/ Scorpion ARMS 1
MassARRAY 1
PNA- LNA PCR clamp 1
Denaturing HPLC 1
Massively parallel/ NGS 0.1
Sen
siti
vity
AMP, Association for Molecular Pathology; ARMS, amplification refractory mutation system; CAP, College of American Pathologists; HPLC, high performance liquid chromatography; IASLC, International
Association for the Study of Lung Cancer; LNA, locked nucleic acid; NGS, next generation sequencing; PCR, polymerase chain reaction; PNA, peptide nucleic acid; RFLP, restriction fragment length polymorphism
CAP/IASLC/AMP recommended assays for EGFR
genotyping testing
PCR-based
methods
Non-squamous-cell NSCLC
Adenocarcinoma
Large-cell carcinoma
Other
Targeted
NGS
Lindeman N, et al. Arch Pathol Lab Med 2018;142(3):321–46

cfDNA, cell-free DNA; TKI, tyrosine-kinase inhibitorLindeman N, et al. Arch Pathol Lab Med 2018;142(3):321-346;
Planchard D, et al. Ann Oncol 2018;29(Supplement_4):iv192-iv237, by permission of Oxford University Press on behalf of the European Society for Medical Oncology
EGFR TESTING IN CELL-FREE PLASMA DNA
The dynamic nature of EGFR resistance mechanisms can be monitored in cfDNA
◆ Insufficient evidence to support the use of cfDNA for
the diagnosis of primary lung adenocarcinoma
◆ When tissue is limited and/or insufficient for molecular
testing, physicians may use a cfDNA assay to identify
EGFR mutations as an alternative
◆ Physicians may use cfDNA methods to identify EGFR
T790M mutations in lung adenocarcinoma patients
with progression or secondary clinical resistance to
EGFR-targeted TKI
◆ Testing of the tumour sample is recommended if cfDNA
result is negative

ALKAnaplastic Lymphoma Kinase

NOS, not otherwise specified Soda M, et al. Nature 2007;448:561–66; Takeuchi K, et al. Clin Cancer Res 2009;15:3143–9; Zhang X, et al. Mol Cancer 2010;9:188;
Rodig SJ, et al. Clin Cancer Res 2009;15:5216–23; Shaw AT, et al. J Clin Oncol 2009;27:4247–53
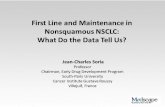
ALK FUSION GENE
◆ ALK fusion gene results in formation of cytoplasmic
chimeric proteins with constitutive kinase activity
◆ The ALK fusion gene appears to be a distinct NSCLC
molecular subset susceptible to targeted inhibition
◆ Tends to be mutually exclusive with EGFR and
KRAS mutations
◆ More common:
⁃ Never or light smokers
⁃ Younger age
⁃ Adenocarcinoma subtype Pfizer, data on file

ALK FUSION GENE
Exon A20
Variants
of the -fusion protein
ALKEML4
ALKEML4
ALKEML4
ALKEML4
ALKEML4
ALKEML4
ALKEML4
ALKEML4
ALKKIF5B
ALKTFG
ALKKLC1
ALKPTPN3
ALKSTRN
Fusion protein Variant
Frequency
in ALK+
NSCLC
E13;A20 (V1) 33%
E6a/b;A20 (V3a/b) 29%
E20;A20 (V2) 9%
E14;A20 (V4) 3%
E18;A20 (V5) 2%
E14;A20 (V7) 2%
E2a/b;A20 (V5a/b) 2%
E17;A20 (V8) 1%
0.5%
Unknown %
Most common partner EML4 (90%)
Breakpoint within EML4 differ: 21 variants
EML4
136 14 15 2017 182Breakpoints
Breakpoints within EML4
Breakpoint within ALK always at exon 20
Produces oncogenic EML4-ALK-fusion protein
Protein activation by partner-provided
coiled-coil dimerisation domain
Gridelli C, et al. Cancer Treat Rev 2014;40(2):300–6; D‘Arcangelo M, et al. Curr Opin Oncol 2013;25(2):121–9; Hallberg B, et al. Nat Rev Cancer 2013;13(10):685-700;
Ou SI, et al. Oncologist 2012;893:179–87.

FFPE, formalin-fixed paraffin embedded; FISH, fluorescent in situ hybridisation; IHC, immunohistochemistryLindeman N, et al. Arch Pathol Lab Med 2018;142(3):321–46
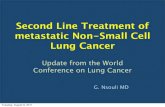
TESTING FOR ALK GENE FUSION
ALK fusion variants in NSCLC
TECHNIQUES
Fluorescent in-situ hybridisation (FISH)
Immunohistochemistry (IHC)
Reverse transcription polymerase chain reaction (RT-PCR)
nCounter
Next Generation Sequencing (NGS)
◆ The ALK break-apart FISH assay detects ALK fusions in FFPE NSCLC tissue specimens
◆ Considered ALK positive if >15% cell with break-apart
◆ The centromeric (green) and telomeric (red) probes flank the ALK locus
⁃ Splitting probes of the red and green signals indicates ALK fusion
⁃ A yellow signal indicates no ALK fusion
◆ ALK IHC (D5F3, Ventana or 5A4, Novocastra) may be used as a screening test

FFPE, formalin-fixed paraffin embedded; FISH, fluorescent in situ hybridisation; IHC, immunohistochemistryLindeman N, et al. Arch Pathol Lab Med 2018;142(3):321–46
TESTING FOR ALK GENE FUSION
Diagnostic algorithm that uses IHC as the primary test for ALK identification
ALK IHC
Negative
Score 0/1+Equivocal
Score 2+Positive
Score 3+
Reported as ALK NEGATIVE
ALK FISH
PositiveNegative
Reported as ALK POSITIVE
◆ Considered ALK IHC positive if strong granular
cytoplasmic staining with/without membrane
accentuation
◆ Occasional cases may be difficult to interpret
because of heterogeneous fixation/preservation
and/or nonspecific staining artefacts (e.g.,
staining in alveolar macrophages, neural cells,
extracellular mucin, necrosis). In these settings,
these cases should also be tested by a
validated method (e.g., ALK FISH)

TESTING FOR ALK GENE FUSION
IHC 5A4 NovocastraIHC D5F3 VentanaFISH BAP Menarini
Split
signal
Non-split
signal
Non-split
signal
BAP, break-apart probe; FISH, fluorescent in situ hybridisation; IHC, immunohistochemistry Images courtesy of Dr C Teixidó and Dr N Reguart
Fernandez-Martínez A, et al. Cancer Treatment Communications 2016;6:4–7

ROS1c-ROS Oncogene 1

◆ The ROS1 fusion gene appears to be a distinct NSCLC
molecular subset susceptible to targeted inhibition
◆ Tends to be mutually exclusive with EGFR, KRAS,
ALK alterations
◆ More common:
⁃ Never or light smokers
⁃ Younger age
⁃ Adenocarcinoma subtype
◆ The mechanism by which the ROS1 fusion protein is
activated remains unclear
Bergethon K, et al. J Clin Oncol 2012;30(8):863–70; Shaw AT, et al. N Engl J Med 2014;371(21):1963–71;
Rossi G, et al. Lung Cancer Targets and Therapy 2017:8 45–55. Images available under Non Commercial (unported, v3.0) License. Available at: http://creativecommons.org/licenses/by-nc/3.0/. Accessed Jun 2019.
ROS1 FUSION GENE

ROS1 FUSION GENE
Many partners, most common CD74 (30%)
ROS1
32 3534Breakpoints
Breakpoints within ROS1
Breakpoint sites vary exons 32, 34, 35
Produces oncogenic ROS1 kinase protein
ROS1Partner
Unknown mechanism of protein activation (no coiled-coil
dimerisation domain provided)
KinaseDimerisation domain
Shaw AT, et al. N Engl J Med 2014;371(21):1963–71; Takeuchi K, et al. Nat Med 2012;18(3):378–81;
Republished with permission of Pioneer Bioscience Publishing Company, from Transl Lung Cancer Res, Kohno T, et al. 4(2), 2015; permission conveyed through Copyright Clearance Center, Inc.

FISH, fluorescent in situ hybridisation; IHC, immunohistochemistryLindeman N, et al. Arch Pathol Lab Med 2018;142(3):321–46
TESTING FOR ROS1 GENE FUSION
TECHNIQUES
Fluorescent in-situ hybridisation (FISH)
Immunohistochemistry (IHC)
Reverse transcription polymerase chain
reaction (RT-PCR)
nCounter
Next Generation Sequencing (NGS)
◆ FISH is the trial-validated standard. The ROS1 FISH
testing should be performed with a break-apart probe
design given the multiple fusion partners described
◆ Considered ROS1 positive if >15% cell with break-apart
◆ ROS1 IHC (D4D6, Cell Signalling Technology) may be
used as a screening test in lung adenocarcinoma
patients; however, positive ROS1 IHC results should be
confirmed by an orthogonal method - cytogenetic method
(FISH) or molecular

BRAFB-raf Proto-Oncogene

◆ Activating mutations in BRAF, especially p.V600E, lead to
oncogenic signaling through MAPK
◆ BRAF V600E mutations appear to be a distinct NSCLC
molecular subset susceptible to targeted inhibition:
BRAF/MEK inhibitors
◆ Typically mutually exclusive of other oncogenic drivers
◆ It is appropriate to include BRAF as either part of larger
testing panels performed initially or when routine EGFR,
ALK, and ROS1 testing are negative
HOTSPOTS FOR BRAF GENE MUTATIONS
Lindeman N et al. Arch Pathol Lab Med 2018; 142(3):321-346
Planchard D et al. Ann Oncol 2018 1;29(Supplement_4):iv192-iv237From files of Teixidó C, Reguart N
N, N-terminal; C, C-terminal; RBD, RAS-binding domain; PL, P-loop; αC, alpha C hélix motif ; DF, dimerization interface; CL, catalytic loop; AS, activation site; aa, amino acid
CN
BRAF Kinase Domain
ASRBD PL ⍺C DF CL
717 766aa0 457
K601G596
V600
D594N581G466
G464
G469
DFG

RETREarranged during Transfection

RET FUSION GENE
Not currently indicated as routine stand-alone test outside the context of a clinical trial
◆ The RET fusion gene appears to be a distinct NSCLC
molecular subset susceptible to targeted inhibition
◆ Tends to be mutually exclusive with other oncogenic
drivers
◆ More common:
⁃ Never or light smokers
⁃ Younger age
⁃ Adenocarcinoma subtype
◆ To date, no RET-directed targeted therapeutic has
received regulatory approval for RET-mutant or RET-
rearranged solid tumours
Ju YS, et al Genome Res 2012;22:436–45;
Ferrara R, et al. J Thorac Oncol. 2018;13(1):27–45. Image available under the terms of the Creative Commons Attribution-NonCommercial-No Derivatives License (CC BY NC ND) Available at
https://creativecommons.org/licenses/by-nc-nd/4.0/ Accessed June 2019.

RET FUSION GENE
KinaseDimerisation domain
Six partners, most common KIF5B (30%)
RET
1211Breakpoints
Breakpoints within RET
Breakpoint sites vary exons 11, 12
Produces oncogenic RET kinase protein
Protein activation by partner-provided
coiled-coil dimerisation domain
RETPartner
Takeuchi K, et al. Nat Med 2012; Figure republished with permission of Pioneer Bioscience Publishing Company, from Transl Lung Cancer Res, Kohno T, et al. 4(2), 2015;
permission conveyed through Copyright Clearance Center, Inc.

TESTING FOR RET GENE FUSION
TECHNIQUES
Fluorescent in-situ hybridisation (FISH)
Reverse transcription polymerase chain
reaction (RT-PCR)
nCounter
Next Generation Sequencing (NGS)
◆ The RET FISH testing should be performed with a break-apart probe design given the multiple fusion partners described
◆ Considered RET positive if >15% cell with break-apart
◆ RET fusion genes cannot be adequately detected by IHC
Not currently indicated as routine stand-alone test outside the context of a clinical trial
IHC, immunohistochemistry; FISH, fluorescent in situ hybridisationLindeman N, et al. Arch Pathol Lab Med 2018; 142(3):321-346; Ferrara R, et al. J Thorac Oncol 2018;13(1):27–45
Ferrara R, et al. J Thorac Oncol 2018;13(1):27–45. Available under NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) licence. Available at https://creativecommons.org/licenses/by-nc-nd/4.0/,
accessed June 2019.

NTRKNeurotrophic tyrosine kinase

NTRK FUSION GENE
Family of neurotrophin receptors (NTRK 1-3)
NTRK fusion gene appears to be a distinct NSCLC
molecular subset susceptible to targeted inhibition
◆ Tends to be mutually exclusive with other
oncogenic drivers
◆ Prevalence in unselected population
⁃ Occur across age and smoking status
⁃ No gender preference
◆ To date, no NTRK-directed targeted therapeutic
has an approval for NTRK-gene fusion
Farago AF, et al. J Thorac Oncol 2015;10(12):1670–4. Available under NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) licence. Available at https://creativecommons.org/licenses/by-nc-nd/4.0/,
accessed June 2019;
Farago AF, et al J Thorac Oncol 2015;10(12):1670–4; Farago AF, et al. JCO Precis Oncol 2018; DOI: 10.1200/PO.18.00037

NTRK FUSION GENE
FISH
FISH
NTRK1
1412Breakpoints
Breakpoints within NTRK1
Breakpoint sites vary exons 12, 14
Oncogenic constitutive activation of TRKA
KinaseDimerisation domain
Most common partners CD74 and MPRIP
Neurotrophic receptors: NTRK1, NTRK2, NTRK3
Transmembrane proteins: TRKA, TRKB and TRKC
Most common fusion in lung NTRK1
Unknown mechanism of protein activation
(no coiled-coil dimerisation domain provided)
NTRKPartner
Vaishnavi A, et al. Nat Med 2013;19(11):1469–72; David Hyman, 2017 ASCO Annual Meeting. By permission of Dr D. Hyman.

TESTING FOR NTRK GENE FUSION
TECHNIQUES
Fluorescent in-situ hybridization (FISH)
Immunohistochemistry (IHC)
Reverse transcription polymerase chain
reaction (RT-PCR)
nCounter
Next Generation Sequencing (NGS)
◆ TRK protein testing can be considered as part of broad immunohistochemistry testing
◆ TRK IHC may be used as a screening test
◆ A TRK positive test should then be confirmed with NGS
NCCN Clinical Practice Guidelines in Oncology, Version 2.2019. Reprinted by permission from Springer Nature, Mod Pathol, Molecular characterization of cancers with NTRK gene fusions. Gatalica Z, et al. 32(1):147–53,
Copyright 2019.
IHC, immunohistochemistry; NGS, next generation sequencing

METMET Proto-Oncogene

TESTING FOR MET GENE AMPLIFICATION
Not currently indicated as routine stand-alone test outside the context of a clinical trial
◆ FISH is the trial-standard technique but there is no guideline for cut-off
of MET positivity
◆ High polysomy occurs when there are multiple copies of chromosome 7
(CEP7) in tumour cells (>5)
◆ MET amplification may be classified by using MET:CEP7 Ratio as low
(≥1.8 to 2.2≤), intermediate (>2.2 to <5), and high (≥5)
◆ Low–intermediate levels can occur synchronously with other oncogenic
mutations and gene rearrangements up to 63% of lung carcinomas
TECHNIQUES
Fluorescent in-situ hybridisation (FISH)
Immunohistochemistry (IHC)
Real time polymerase chain reaction (qRT-PCR)
nCounter
Next Generation Sequencing (NGS)
Noonan SA, et al. J Thorac Oncol 2016;11(12):2253–8; Drilon A, et al. J Thorac Oncol 2017;12(1):15–26
Image courtesy of Dr C Teixidó and Dr N Reguart

TESTING FOR MET EXON 14 SKIPPING MUTATIONS
Not currently indicated as routine stand-alone test outside the context of a clinical trial
Schematic illustration of some MET△14
◆ MET△14 mutations exhibit a highly diverse sequence composition
(insertions, deletions, SNV)
TECHNIQUES
In-situ hybridisation (ISH)
Direct Sequencing
Reverse transcription polymerase chain reaction
(RT-PCR)
nCounter
Next Generation Sequencing (NGS)
SNV, single nucleotide variationReprinted from Cancer Discov 2015, 5(8):842–9, Paik PK, et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping, with permission from AACR.

PD-L1Programmed Cell Death Ligand-1

IHC, immunohistochemistryImages courtesy of Dr C Teixidó and Dr N Reguart
PD-L1 TESTING FOR IMMUNOTHERAPY
Standard Detection by IHC
◆ PD-L1 expression has been detected on tumour cells and
tumour-infiltrating immune cells
◆ PD-L1 on tumour cells may lead to the inhibition of
activated T-cells
◆ To enrich for those patients more likely to benefit from
anti-PD-1 or anti-PD-L1 therapy
◆ IHC to identify PD-L1 expression at the appropriate level
and on the appropriate cell population(s) as determined by
the intended drug and line of therapy
TPS <1%
TPS 1–49%
TPS ≥50%

PD-L1 IHC ASSAYS IN LUNG CANCER
Summary of PD-L1 antibodies and technical aspects for evaluation in NSCLC
mAb cloneAb host
speciesPlatform
PD-L1
scoringCut-offs
22C3 Mouse Dako TCTC ≥1% or
TC ≥50%
28-8 Rabbit Dako TC TC ≥1%
SP142 Rabbit Ventana TC, IC TC ≥50% or IC
≥10%
SP263 Rabbit Ventana TC TC ≥25%
73-10 Rabbit Dako TC TC ≥1%
Blueprint Phase 2a
22C3, 28-8 and SP263 assays are
comparable when used to determine
PD-L1 status of patient’s tumour (TPS),
SP142 detects less, while 73-10 stains
more PD-L1 positive tumour cells
TC, tumour cells; IC, immune cells; TPS, tumour proportion scoreAdapted from Teixidó C, et al. Ther Adv Med Oncol 2018;10:1–17
Tsao MS, et al. J Thorac Oncol. 2018 Sep;13(9):1302-1311

OUTLINE
◆ Advanced NSCLC: a need for personalised therapy
◆ Diagnostic workup of lung cancer:
⁃ Type of samples
⁃ Morphology and histology
⁃ Material for biomarker studies
◆ Overview of key genetic alterations in NSCLC
⁃ Techniques for diagnose
◆ Guidelines for genetic testing
◆ Summary / conclusions

1
ALK
2
ROS1
KRAS
RET HER2MET
NSCLC Recommendations
ESMO Guidelines
‘Must-test’
‘Should-test’
BRAFEGFR PD-L1
◆ Testing for EGFR mutation status [LoE, GoR: I, A],
ALK rearrangement [I, A], ROS1 rearrangement [II,
A], BRAF V600 mutation status [II, A] and PD-L1
expression by IHC [I, A] should be systematically
analysed in advanced NSCLC
◆ Molecular EGFR and ALK testing are not
recommended in patients with a confident
diagnosis of squamous, except in unusual cases,
eg, never/former light smokers or long-time
ex-smokers [IV, A]
METASTATIC NSCLC: ESMO CLINICAL PRACTICE
Molecular pathology/biology recommendations
LoE, levels of evidence (I–V); GoR, grades of recommendation (A–E); NSCLC, non-small cell lung cancer; IHC, immunohistochemistry; FISH, fluorescent in situ hybridisationPlanchard D, et al. Ann Oncol 2018;29(Supplement_4):iv192-iv237, by permission of Oxford University Press on behalf of the European Society for Medical Oncology.

METASTATIC NSCLC: ESMO CLINICAL PRACTICE
Molecular pathology/biology recommendations
◆ EGFR mutation testing should have adequate coverage of mutations in exons 18–21, including those
associated with resistance to some therapies [LoE, GoR: III, B]
◆ Detection of the ALK translocation by FISH remains a standard, but IHC with high-performance ALK
antibodies and validated assays may be used for screening [III, A] and have recently been accepted as
an equivalent alternative to FISH for ALK testing
◆ Detection of the ROS1 translocation by FISH remains a standard; IHC may be used as a screening
approach [IV, A]
◆ If available, multiplex platforms (NGS) for molecular testing are preferable [III, A]. Whatever testing
modality is used, it is mandatory that adequate internal validation and quality control measures are in
place and that laboratories participate in, and perform adequately in, external quality assurance schemes
for each biomarker test [III, A]
FISH, fluorescent in situ hybridisation; GoR, grades of recommendation (A–E); IHC, immunohistochemistry; LoE, levels of evidence (I–V); NGS, next generation sequencing.Planchard D, et al. Ann Oncol 2018;29(Supplement_4):iv192-iv237

METASTATIC NSCLC: ESMO CLINICAL PRACTICE
Biomarker testing
FISH, fluorescent in situ hybridisation; GoR, grades of recommendation (A–E); IHC, immunohistochemistry; LoE, levels of evidence (I–V); MEK, mitogen-activated protein kinase
kinase; NGS, next generation sequencing; TKI, tyrosine-kinase inhibitorPlanchard D, et al. Ann Oncol 2018;29(Supplement_4):iv192-iv237, by permission of Oxford University Press on behalf of the European Society for Medical Oncology.

SUMMARY / CONCLUSIONS
◆ In NSCLC, the determination of histologic subtype and molecular predictive markers are
standard of care
◆Determination of EGFR, ALK, ROS1, BRAF and PD-L1 status in tumour specimens is
currently standard of care in advanced NSCLC patients
◆ In lung cancer, optimal management of biopsy specimens are needed to avoid repeat biopsies
⁃Pathologists have a key role in treatment decisions
⁃Closed interaction between pulmonologists, pathologists, biologists, and oncologists is
required
◆ In the era of personalised therapy, professionals involved in lung cancer diagnosis/
management should develop their own multidisciplinary tissue management strategy to obtain
specimens and process them