ERRATA REPORT DNB CET REVIEW 3RD ED - Med Easy India · Modern surgical literature like schwartz,...
30
ERRATA REPORT DNB CET REVIEW 3RD ED Total number of questions in 2 volumes of DNB CET REVIEW 3rd ed = 4991 Total Number of Appendices in DNB CET REVIEW 3rd ed = 133 Total number of items in DNB CET REVIEW 3rd ed= 4991+133= 5124 Items Number of items Error percentage compared to 5124 items Change of explanation and answers 16 0.31% Misprints 33 0.64% New/Additional information 4 0.078% ERRATA DNB CET REVIEW 3RD EDITION UPTO 22 AUG 2013 2000 to 2008 Q1847 page 867 Volume 2 (1)Neurotransmitter which is implicated in both positive and negative symptoms in schizophrenia is? (2004) (A) Noradrenaline (B) Serotonin (C) Dopamine (D) All of the above ANSWER: (B) Serotonin REF: Kaplan and Sadocks 10th Edn Ch 13 EXPLANATION IS CORRECT December 2011 Q21 page 685 Volume 1 Removed from errata 2000 to 2008 Q1732 page 830 Volume 2 Vit D deficiency manifests as all EXCEPT: (2007) (A) Elevation of lower border of the ribs (B) Pigeon chest (C) Barrel chest (D) Funnel chest ANSWER: (C) Barrel chest REF: Nelson’s 18 th Ed Ch: 48, Radiology of Chest Diseases -Sebastian Lange, Geraldine Walsh (FRCR.)3rd ed Page 235 FUNNEL CHEST (Pectus excavatum ) occurs when there is a depression in the lower portion of the sternum with eversion of lower free border of ribs. This may compress the heart and great vessels, resulting in murmurs. Funnel chest may occur with rickets or Marfan's syndrome.
Transcript of ERRATA REPORT DNB CET REVIEW 3RD ED - Med Easy India · Modern surgical literature like schwartz,...
ERRATA REPORT DNB CET REVIEW 3RD ED Total number of questions in 2 volumes of DNB CET REVIEW 3rd ed = 4991
Total Number of Appendices in DNB CET REVIEW 3rd ed = 133
Total number of items in DNB CET REVIEW 3rd ed= 4991+133= 5124
Items Number of items
Error percentage compared to 5124 items
Change of explanation and answers 16 0.31%
Misprints 33 0.64%
New/Additional information 4 0.078%
ERRATA DNB CET REVIEW 3RD EDITION UPTO 22 AUG 2013
2000 to 2008 Q1847 page 867 Volume 2 (1)Neurotransmitter which is implicated in both positive and negative symptoms in
schizophrenia is? (2004)
(A) Noradrenaline
(B) Serotonin
(C) Dopamine
(D) All of the above
ANSWER: (B) Serotonin REF: Kaplan and Sadocks 10th Edn Ch 13 EXPLANATION IS CORRECT
December 2011 Q21 page 685 Volume 1 Removed from errata
2000 to 2008 Q1732 page 830 Volume 2 Vit D deficiency manifests as all EXCEPT: (2007)
(A) Elevation of lower border of the ribs
(B) Pigeon chest
(C) Barrel chest
(D) Funnel chest
ANSWER: (C) Barrel chest
REF: Nelson’s 18th Ed Ch: 48, Radiology of Chest Diseases -Sebastian Lange, Geraldine Walsh
(FRCR.)3rd ed Page 235
FUNNEL CHEST (Pectus excavatum ) occurs when there is a depression in the lower
portion of the sternum with eversion of lower free border of ribs. This may
compress the heart and great vessels, resulting in murmurs. Funnel chest may occur
with rickets or Marfan's syndrome.
PIGEON CHEST (Pectus Craniatum) occurs as displacement of sternum. There is an
increase in AP diameter. This may occur with Rickets, Marfan's syndrome or
Kyphoscoliosis.
BARREL CHEST occurs as a result of over inflation of lung. There is increased AP
diameter and increased intercostal space. It is seen in Emphysema and COPD.
2000 to 2008 Q1862 page 390 Volume 2 Defense mechanism in OCD is? (2003)
(A) Sublimation
(B) Projection
(C) Substitution
(D) Undoing
ANSWER: (D) Undoing REF: Kaplan and Sadock Psychiatry Synposis 10th Edn Page: 201-204, Ahuja Pshy 6th Edn
Page: 221, 223
2000 to 2008 Q1680 page 373 Volume 2 Congestive dysmenorrhoea is seen in? (2000)
(A) Endometriosis
(B) DUB
(C) Menarche
(D) Ovarian cyst
ANSWER: (A) Endometriosis REF: Dutta Gynaec 5th E. Pg No177, Shaws 6th Ed Pg 265
2000 to 2008 Q1096 page 650 Volume 2 Regarding spring catarrh, all of the following are true, EXCEPT: (2001) (A) Cobblestone appearance of conjunctiva (B) Common in spring months (C) Limbus conjunctival thickening (D) Sodium cromoglycate is a form of therapy ANSWER: (B) Common in spring months REF: AK Khurana Opthalmology 4th Edn Page 74
2000 to 2008 Q984 page 309 Volume 2

In a patient, Rinne's test positive in both ears, Webers lateralizes to the left. What does this signify? (2006) (A) Right Sensorineural Deafness (B) Left Sensorineural Deafness (C) Right Conductive Deafness (D) Left Conductive Deafness ANSWER: (A) Right Sensorineural deafness REF : Dhingra 4th Ed Pg 23,Diagnosis in Otorhinolaryngology: An Illustrated Guide By T.Metin Onerci Pg 8
2000 to 2008 Q756 page 288, 588 Volume 2 Bevelling of the skull is seen in the? (2004)
(A) Broad end of the entry point in bullet injury
(B) Narrow end of the entry point in bullet injury
(C) Outer table of Exit wound of bullet
(D) Depressed fracture of the skull
ANSWER: (C) Outer table of Exit wound of bullet REF: Parikh 5th Edn Page 250,289,393, Textbook Of Forensic Medicine and Toxicology: Principles and Practice, By Vij, page 324, http://www.forensicmed.co.uk/wounds/firearms/ See difference between entry and exit wound June 2010 (FMT) Note: Entry point and entry wound are two different terms. Both entry wound and exit wound have a entry and exit point.
The direction in which a bullet was traveling when it perforates a bone can be determined by the appearance of the wound in the bone. When a bullet perforates bone, it bevels out the bone in the direction in which it is traveling "When a bullet enters the skull it produces a "beveled-out" hole on the inner table (internal beveling). The exit defect will display "beveled-out" hole on the outer table (external beveling)" However in most of the cases the entry or exit of the bullet is not perpendicular to the skull bones and in these cases beveling is not seen in whole of the circumference. Gunshot Wounds Practical Aspects of Firearms, Ballistics and Forensic Techniques 2nd ed by Vincent J. M. DiMaio, M.D. page 105-107 A bullet striking the skull at a shallow angle may produce a keyhole wound of the bone. In the most common presentation, the bullet, impacting at a shallow angle, begins to punch out an entrance in the bone. Because of the stresses generated, part of the bullet shears off and travels a short distance beneath the scalp before either coming to rest or exiting. The bulk of the bullet enters the cranial cavity. This process results in a keyhole-shaped wound of bone. One end of this keyhole (Narrow end) wound will have the sharp edges typical of a
wound of entrance, whereas the other end (Broad end) will have the external beveling of a wound of exit. Summary: Beveling of the skull is seen in:
Broad end (or whole circumference when there are no broad or narrow ends)of
inner table (exit point) of entry wound
Broad end (or whole circumference when there are no broad or narrow ends)of
outer table (exit point) of exit wound
2000 to 2008 Q1244 page 701 Volume 2 All are the major criteria for diagnosing acute rheumatic fever, EXCEPT: (2005,2000)
(A) Rheumatic chorea
(B) Carditis
(C) Erythema nodosum
(D) Erythema marginatum
ANSWER: (C) Erythema nodosum REF: Harrisons Medicine 17th Edn, Page 2095, Table 315-1
2012 Session II page 196 Q344 Volume 1 All are seen after splenectomy EXCEPT:
(A) Thrombocytopenia
(B) Acute gastric dilation
(C) Sub diaphragmatic abscess
(D) Pulmonary complications
ANSWER: (A) Thrombocytopenia
REF: The Washington Manual of Surgery: Department of Surgery, Washington by Mary E.
Klingensmith, M.D. p :291, Schwartz 9th ed chapter 34,
Modern surgical literature like schwartz, sabiston etc have not mentioned gastric dilatation
as a complication but we found this text and some other literature supporting Gastric
dilatation as a complication of splenectomy:
"In the older surgical literature, the complication of acute gastric dilatation due to ligature
of the short gastric vessels., causing hemodynamic collapse, was seen not infrequently
following splenectomy"
REF: Gastrointestinal Surgery: Pathophysiology & Management by Haile T. Debas page 327
COMPLICATIONS OF SPLENECTOMY:
I. Intraoperative complications:
Pancreatic injury : upto 6% cases
Hemorrhage- The most common intraoperative complication is haemorrhage
Bowel injury : colon and stomach
Diaphragmatic injuries
II. Early post op complications:
Pulmonary : atelactasis , pleural effusion , pneumonitis
Sub phrenic abscess
Thrombocytosis
Thrombotic complications
Wound problems
Ileus
III. Late post op complications:
Overwhelming post splenectomy infection
Splenosis
Note:
Left lower lobe atelectasis is the most common complication after Open
splenectomy
Traumatic rupture of the spleen continues as the most common indication for Open
splenectomy
Regarding elective splenectomy, the most common indication in the past had been
staging for Hodgkin's disease.
More recent data suggest that ITP is now the most frequent indication for elective
splenectomy.
ERRATA DNB CET REVIEW 3RD EDITION UPTO 16 AUG 2013
2000 to 2008 Q515 page 539 Volume 2 Commonest Type of Intracranial Tumour is? (2004, 2000)
(A) Astrocytoma (B) Medulloblastoma (C) Meningioma (D) Secondaries ANSWER: (D) Secondaries REF: Robbins 8th Ed Page 1330,1333
Commonest brain tumour Secondaries
Most common origin of brain metastases Lung
Commonest primary brain tumour Gliomas (include astrocytomas, oligodendrogliomas, and ependymomas)
Commonest Gliomas Infiltrating Astrocytomas
Commonest adult primary brain tumors Infiltrating Astrocytomas
most common childhood brain tumor Pilocytic astrocytoma
Commonest paediatric brain tumour Medultoblastoma, cerebellum
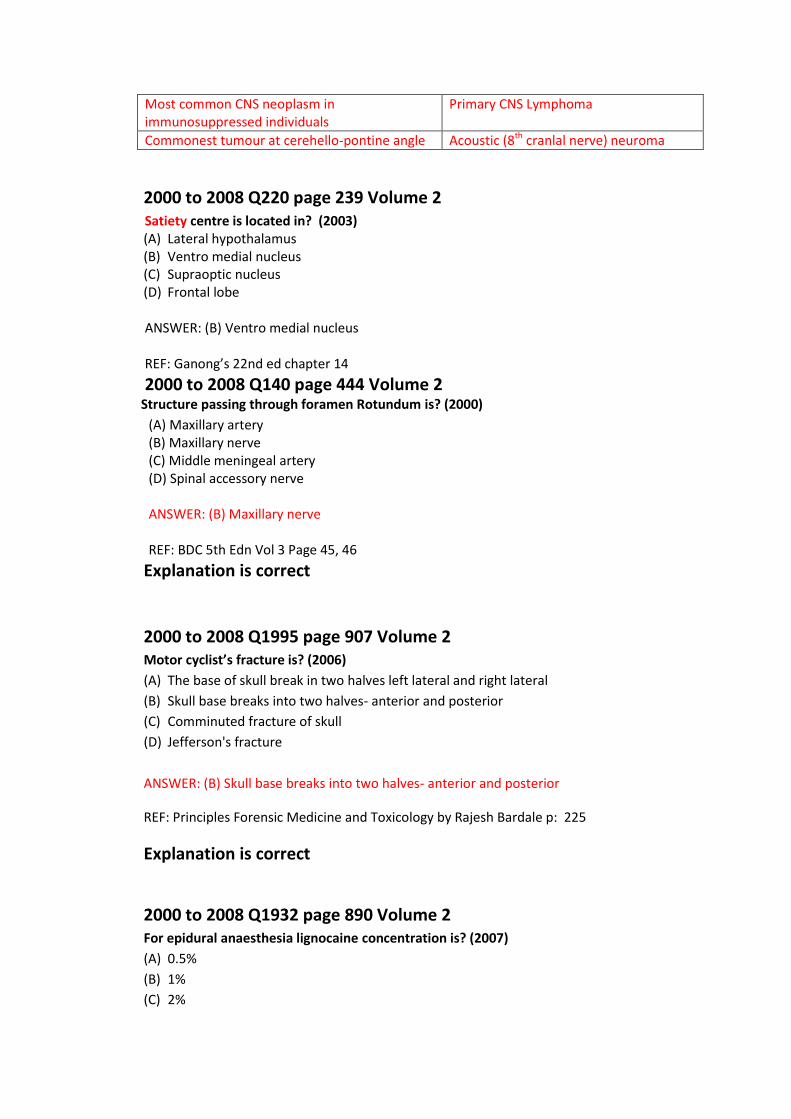
Most common CNS neoplasm in immunosuppressed individuals
Primary CNS Lymphoma
Commonest tumour at cerehello-pontine angle Acoustic (8th cranlal nerve) neuroma
2000 to 2008 Q220 page 239 Volume 2 Satiety centre is located in? (2003) (A) Lateral hypothalamus (B) Ventro medial nucleus (C) Supraoptic nucleus (D) Frontal lobe
ANSWER: (B) Ventro medial nucleus REF: Ganong’s 22nd ed chapter 14
2000 to 2008 Q140 page 444 Volume 2
Structure passing through foramen Rotundum is? (2000)
(A) Maxillary artery (B) Maxillary nerve (C) Middle meningeal artery (D) Spinal accessory nerve ANSWER: (B) Maxillary nerve REF: BDC 5th Edn Vol 3 Page 45, 46
Explanation is correct
2000 to 2008 Q1995 page 907 Volume 2 Motor cyclist’s fracture is? (2006)
(A) The base of skull break in two halves left lateral and right lateral
(B) Skull base breaks into two halves- anterior and posterior
(C) Comminuted fracture of skull
(D) Jefferson's fracture
ANSWER: (B) Skull base breaks into two halves- anterior and posterior
REF: Principles Forensic Medicine and Toxicology by Rajesh Bardale p: 225
Explanation is correct
2000 to 2008 Q1932 page 890 Volume 2 For epidural anaesthesia lignocaine concentration is? (2007)
(A) 0.5%
(B) 1%
(C) 2%
(D) 4%
ANSWER: (C) 2 %
REF: Morgan’s Anaesthesia 4/e p.270
See table of 2012 Session I, June 2011 for Lignocaine concentrations
Explanation is correct
2000 to 2008 Q1984 OBG page 903 Volume 2 Bony ankylosis occurs in all EXCEPT: (2008)
(A) Septic arthritis
(B) Tuberculosis of joints
(C) Arthrogryposis
(D) Rheumatoid arthritis
ANSWER: (C) Arthrogryposis
Misprint, Explanation is correct
2012 Session 2 Q183 page 374 Volume 1 What is the chance of an offspring being affected with an affected mother and normal
father, in an X linked recessive condition? (A) 50% of daughters are carriers
(B) 50% of sons are asymptomatic carriers
(C) 50% of the off springs are carriers
(D) Males will never be affected
ANSWER: (C) 50% of the off springs are carriers
REF: BRS Genetics by Ronald W. Dude page 31-33
In an x linked recessive condition, when mother is affected, 100% of sons will be affected
and 100% of daughters will be carriers, i.e. 50% of off springs are carrier.
Rest of the explanation is correct
2012 Session I page 503, Q484 Volume 1
Blood glucose levels in children > 2months with hypoglycaemia is?
(A) <40 mg/dL
(B) <45 mg/dL
(C) <50 mg/dL
(D) <54 mg/dL
ANSWER: (C) <50 mg/dL
2000 to 2008 Q1790 page 383, 849 Volume 2
Scarring alopecia is caused by all EXCEPT (2007)
(A) Discoid lupus
(B) Androgenic alopecia
(C) Tinea capitis
(D) Traction
ANSWER: (B) Androgenic alopecia
REF: Rook’s 7th ed 66.40
Explanation is correct
ERRATA DNB CET REVIEW 3RD EDITION UPTO 13 AUG 2013
2012 Session II page 3 Q1 Volume 1 Secondary spermatocyte is?
(A) Haploid (n) and 2N
(B) Haploid (2n) and 2N
(C) Diploid (2n) and N
(D) Diploid (n) and 2N
ANSWER: (A) Haploid (n) and 2N
Explanation is correct
2012 Session II page 82 Q 68 Volume 1 Left shift in arneth index indicates?
(A) Anemia
(B) Neutrophilia
(C) Spleenomegaly
(D) Hyperactive bone marrow
ANSWER: (B) Neutrophilia & (C) Hyperactive bone marrow
REF: Wintrobe's clinical Hematology page 183, Textbook of Medical Physiology by Khurana
page 178, Textbook Of Practical Physiology - 2nd ed By G.K. & Pal, Pal, Pravati page 81-82
COOK ARNETH COUNT OR ARNETH COUNT:
Arneth count is the determination of percentage distribution of different types of
neutrophils on the basis of their number of nuclear lobes. Arenth a German physiologist
classified neutrophils into 5 stages according to number of lobes in their nuclei.
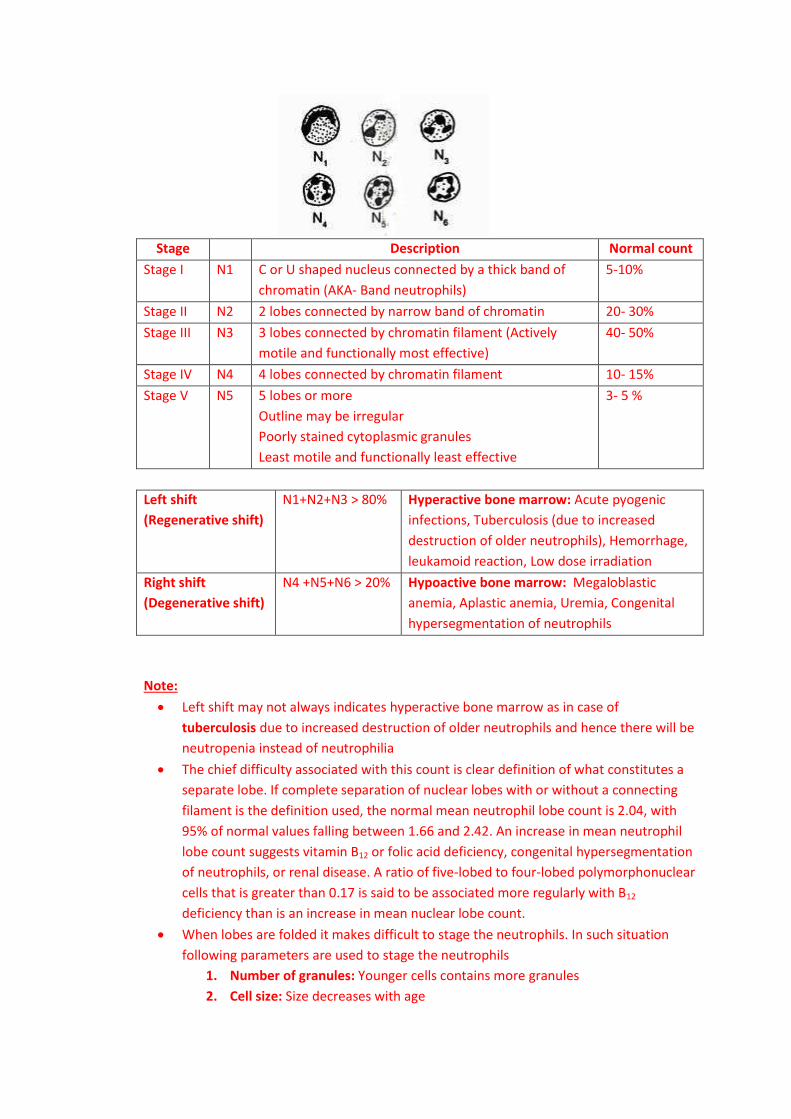
Stage Description Normal count
Stage I N1 C or U shaped nucleus connected by a thick band of
chromatin (AKA- Band neutrophils)
5-10%
Stage II N2 2 lobes connected by narrow band of chromatin 20- 30%
Stage III N3 3 lobes connected by chromatin filament (Actively
motile and functionally most effective)
40- 50%
Stage IV N4 4 lobes connected by chromatin filament 10- 15%
Stage V N5 5 lobes or more
Outline may be irregular
Poorly stained cytoplasmic granules
Least motile and functionally least effective
3- 5 %
Left shift
(Regenerative shift)
N1+N2+N3 > 80% Hyperactive bone marrow: Acute pyogenic
infections, Tuberculosis (due to increased
destruction of older neutrophils), Hemorrhage,
leukamoid reaction, Low dose irradiation
Right shift
(Degenerative shift)
N4 +N5+N6 > 20% Hypoactive bone marrow: Megaloblastic
anemia, Aplastic anemia, Uremia, Congenital
hypersegmentation of neutrophils
Note:
Left shift may not always indicates hyperactive bone marrow as in case of
tuberculosis due to increased destruction of older neutrophils and hence there will be
neutropenia instead of neutrophilia
The chief difficulty associated with this count is clear definition of what constitutes a
separate lobe. If complete separation of nuclear lobes with or without a connecting
filament is the definition used, the normal mean neutrophil lobe count is 2.04, with
95% of normal values falling between 1.66 and 2.42. An increase in mean neutrophil
lobe count suggests vitamin B12 or folic acid deficiency, congenital hypersegmentation
of neutrophils, or renal disease. A ratio of five-lobed to four-lobed polymorphonuclear
cells that is greater than 0.17 is said to be associated more regularly with B12
deficiency than is an increase in mean nuclear lobe count.
When lobes are folded it makes difficult to stage the neutrophils. In such situation
following parameters are used to stage the neutrophils
1. Number of granules: Younger cells contains more granules
2. Cell size: Size decreases with age
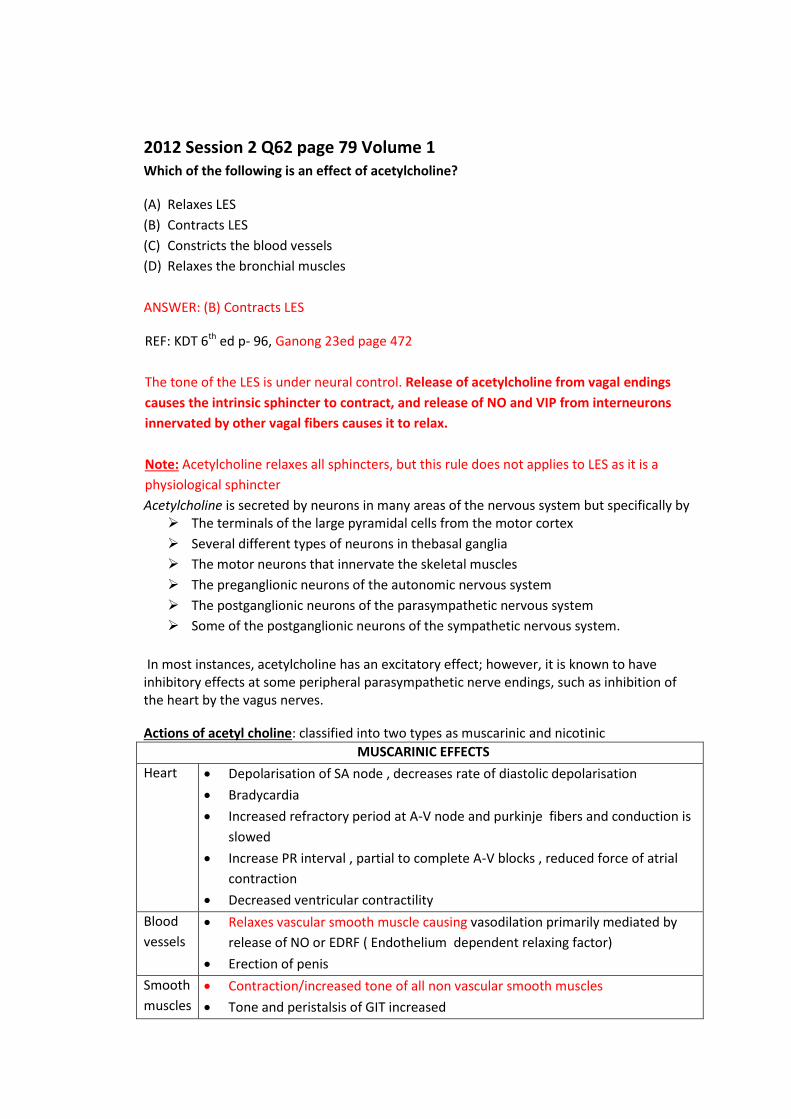
2012 Session 2 Q62 page 79 Volume 1 Which of the following is an effect of acetylcholine?
(A) Relaxes LES
(B) Contracts LES
(C) Constricts the blood vessels
(D) Relaxes the bronchial muscles
ANSWER: (B) Contracts LES
REF: KDT 6th ed p- 96, Ganong 23ed page 472
The tone of the LES is under neural control. Release of acetylcholine from vagal endings
causes the intrinsic sphincter to contract, and release of NO and VIP from interneurons
innervated by other vagal fibers causes it to relax.
Note: Acetylcholine relaxes all sphincters, but this rule does not applies to LES as it is a
physiological sphincter
Acetylcholine is secreted by neurons in many areas of the nervous system but specifically by The terminals of the large pyramidal cells from the motor cortex
Several different types of neurons in thebasal ganglia
The motor neurons that innervate the skeletal muscles
The preganglionic neurons of the autonomic nervous system
The postganglionic neurons of the parasympathetic nervous system
Some of the postganglionic neurons of the sympathetic nervous system.
In most instances, acetylcholine has an excitatory effect; however, it is known to have inhibitory effects at some peripheral parasympathetic nerve endings, such as inhibition of the heart by the vagus nerves.
Actions of acetyl choline: classified into two types as muscarinic and nicotinic
MUSCARINIC EFFECTS
Heart Depolarisation of SA node , decreases rate of diastolic depolarisation
Bradycardia
Increased refractory period at A-V node and purkinje fibers and conduction is
slowed
Increase PR interval , partial to complete A-V blocks , reduced force of atrial
contraction
Decreased ventricular contractility
Blood
vessels
Relaxes vascular smooth muscle causing vasodilation primarily mediated by
release of NO or EDRF ( Endothelium dependent relaxing factor)
Erection of penis
Smooth
muscles
Contraction/increased tone of all non vascular smooth muscles
Tone and peristalsis of GIT increased
Relaxation of sphincters
Increased ureteric persitalsis
Contraction of detrusor , relaxation of trigone and sphincters
Constriction of bronchial muscles
Glands Increased secretion, salivation, sweating , lacrimation. Trachea bronchial and
gastric secretion increases
No marked effect on pancreas or intestinal glands
Secretion of milk and bile not affected
Eye Miosis
CNS Complex pattern of stimulation and depression
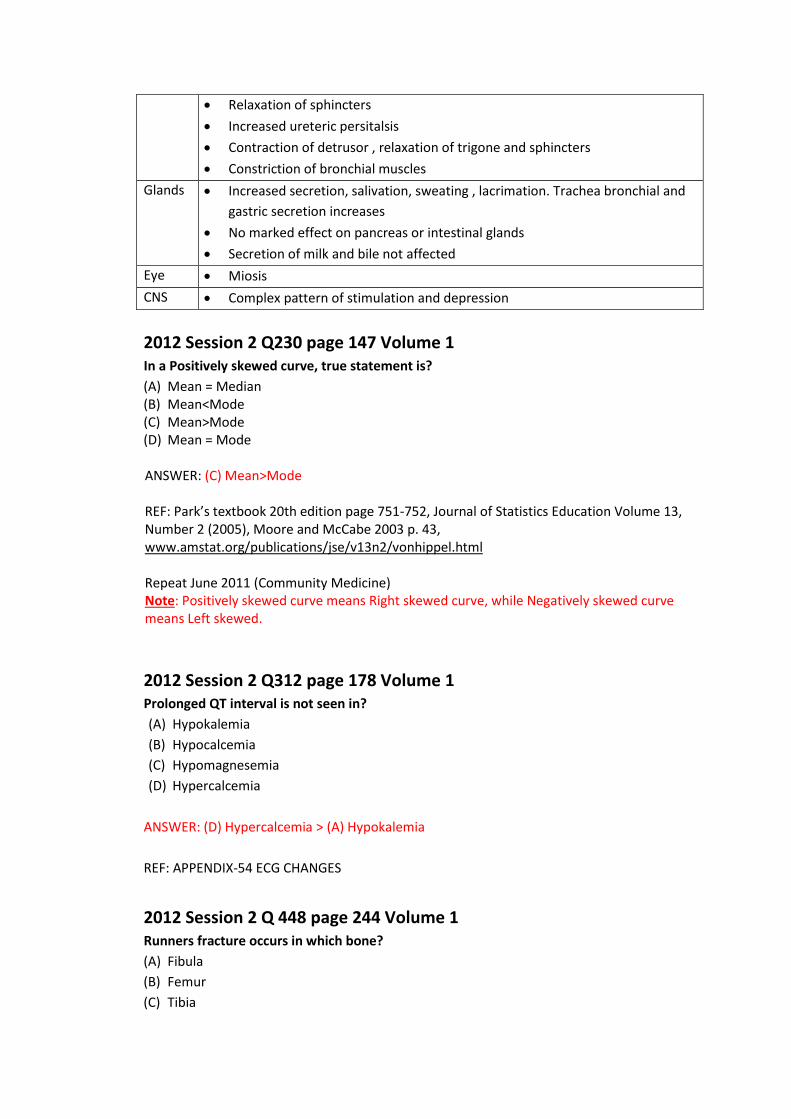
2012 Session 2 Q230 page 147 Volume 1 In a Positively skewed curve, true statement is?
(A) Mean = Median (B) Mean<Mode (C) Mean>Mode (D) Mean = Mode ANSWER: (C) Mean>Mode REF: Park’s textbook 20th edition page 751-752, Journal of Statistics Education Volume 13, Number 2 (2005), Moore and McCabe 2003 p. 43, www.amstat.org/publications/jse/v13n2/vonhippel.html Repeat June 2011 (Community Medicine) Note: Positively skewed curve means Right skewed curve, while Negatively skewed curve means Left skewed.
2012 Session 2 Q312 page 178 Volume 1 Prolonged QT interval is not seen in?
(A) Hypokalemia
(B) Hypocalcemia
(C) Hypomagnesemia
(D) Hypercalcemia
ANSWER: (D) Hypercalcemia > (A) Hypokalemia
REF: APPENDIX-54 ECG CHANGES
2012 Session 2 Q 448 page 244 Volume 1 Runners fracture occurs in which bone?
(A) Fibula
(B) Femur
(C) Tibia
(D) All of The Above
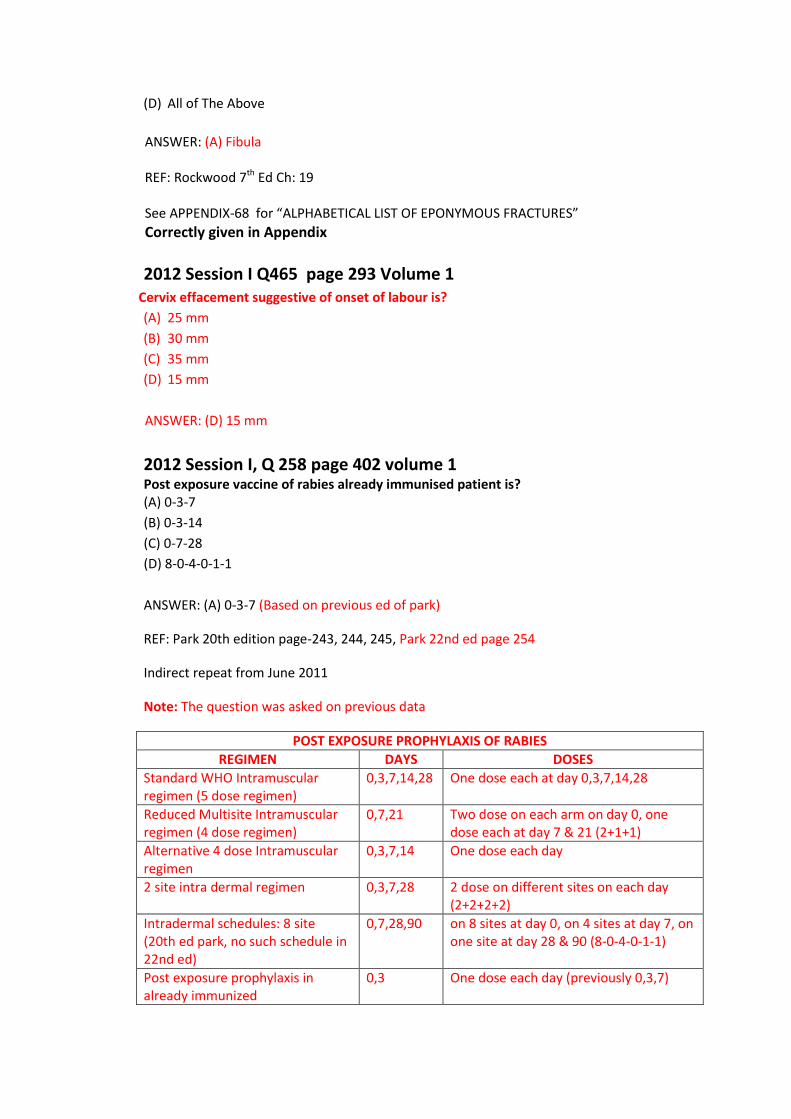
ANSWER: (A) Fibula REF: Rockwood 7th Ed Ch: 19 See APPENDIX-68 for “ALPHABETICAL LIST OF EPONYMOUS FRACTURES”
Correctly given in Appendix
2012 Session I Q465 page 293 Volume 1 Cervix effacement suggestive of onset of labour is?
(A) 25 mm
(B) 30 mm
(C) 35 mm
(D) 15 mm
ANSWER: (D) 15 mm
2012 Session I, Q 258 page 402 volume 1 Post exposure vaccine of rabies already immunised patient is? (A) 0-3-7
(B) 0-3-14
(C) 0-7-28
(D) 8-0-4-0-1-1
ANSWER: (A) 0-3-7 (Based on previous ed of park)
REF: Park 20th edition page-243, 244, 245, Park 22nd ed page 254
Indirect repeat from June 2011
Note: The question was asked on previous data
POST EXPOSURE PROPHYLAXIS OF RABIES
REGIMEN DAYS DOSES
Standard WHO Intramuscular regimen (5 dose regimen)
0,3,7,14,28 One dose each at day 0,3,7,14,28
Reduced Multisite Intramuscular regimen (4 dose regimen)
0,7,21 Two dose on each arm on day 0, one dose each at day 7 & 21 (2+1+1)
Alternative 4 dose Intramuscular regimen
0,3,7,14 One dose each day
2 site intra dermal regimen 0,3,7,28 2 dose on different sites on each day (2+2+2+2)
Intradermal schedules: 8 site (20th ed park, no such schedule in 22nd ed)
0,7,28,90 on 8 sites at day 0, on 4 sites at day 7, on one site at day 28 & 90 (8-0-4-0-1-1)
Post exposure prophylaxis in already immunized
0,3 One dose each day (previously 0,3,7)
(Intramuscular)
Alternative Post exposure prophylaxis in already immunized (Intradermal)
0 4 doses equally distributed on right and left deltoid or thigh on day 0
2012 Session I Q 294 page 416 Volume 1 Degree of Eustachian tube from horizontal line in adults is?
(A) 35 degree
(B) 45 degree
(C) 55 degree
(D) 65 degree
ANSWER: (B) 45 degree
REF: Gray’s anatomy 40th ed ch: 36, Head & Neck Surgery: Otolaryngology Byron J. Bailey,
Jonas T. Johnson, Shawn D Newlands 4th ed Page 1254
Grays anatomy says eustachian tube is approximately 45° with the sagittal plane and 30°
with the horizontal (these angles increase with age and elongation of the skull base).
But Grays anatomy has most probably wrongly stated here as the angle between horizontal
and vertical plane is always 90o , the sum of angles of eutachian tube from horozontal and
vertical planes should be 90o. However 45 + 30 is 75o.
Also all ENT texts particularly mentions that "In adults, the eustachian tube lies at an angle
of 45 degrees in relation to thehorizontal plane. In infants, this inclination is only
10 degrees"
The pharyngotympanic tube or Eustachian tube connects the tympanic cavity to the
nasopharynx and allows the passage of air between these spaces in order to equalize the air
pressure on both aspects of the tympanic membrane.
It is about 36 mm long and is formed partly by cartilage and fibrous tissue and partly
by bone.
The cartilaginous part, which is approximately 24 mm long, The bony part,
approximately 12 mm long, is oblong in transverse section, with its greater
dimension in the horizontal plane
At birth the pharyngotympanic tube is about half its adult length, it is more horizontal
and its bony part is relatively shorter but much wider. The pharyngeal orifice is a
narrow slit, level with the palate and without a tubal elevation.
2012 Session I, Q 362 page 440 volume 1 Acute endocarditis with abscess is most commonly associated with? (A) Listeria
(B) Staphylococcus

(C) Streptococcus
(D) Enterococcus
ANSWER: (B) Staphylococcus
REF: Harrison’s 18th ed chapter 124 , Braunwald's Heart Disease: A Textbook of
Cardiovascular Medicine 18th ed chapter 63
Most textbooks including braunwald’s agree that cardiac abscess is more common in
infective endocarditis of the prosthetic valves.
Brauwald characteristically mentions that staphylococcus aureus is associated with cardiac
abscess
Remember according to Brunwald 18th ed
M.c cause of community acquired native valve endocarditis in neonate is
Staphylococcus aureus
M.c cause of community acquired native valve endocarditis (overall and age >2
months) is streptococci
M.c cause of native valve endocarditis in health care associated patients :
Staphylococcus aureus
M.c cause of infective endocarditis in prosthetic valve endocarditis
<2 months and 2-12 months: coagulase negative staphylococcus
> 12 months: Streptococcus (They say it is similar to native valve
endocarditis)
M.c cause of infective endocarditis in IV drug users:
Over all: Staph. Aureus
Right side: Staph. Aureus
Left side: Enterococcus > Staph. Aureus (Marginally)
2012 Session I Q378 Page 452 Volume 1 The signs and symptoms of CRF are seen when the renal function deteriorates by?
(A) 40 %
(B) > 50 %
(C) > 60 %
(D) > 70 %
ANSWER: (D) > 70% REF: Harrison’s 18th ed chapter 280 Repeat December 2011
Misprint, Explanation is correct
Post diploma Q98 page 599 Volume 1 Most common primary site for congenital tuberculosis is?
(A) Lungs
(B) Lymph nodes
(C) Liver
(D) Skin
ANSWER: (C) Liver > (A) Lung
REF: Textbook of Pulmonary Medicine volume 1 by 2nd edition D. Behera page 495
Misprint, Explanation is correct
December 2011 Q82 page 713 Volume 1 Paraneoplastic syndrome not seen in renal cell cancer is? (A) Acanthosis nigricans (B) Amyloidosis (C) Polycythemia (D) Sweet syndrome
ANSWER: (A) Acanthosis nigricans REF: Harrison’s 18th ed chapter 100, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1475999/ See APPENDIX- 125 for “PARANEOPLASTIC SYNDROMES ASSOCIATED WITH COMMON CANCERS”
June 2011 Q88 Page 825 Volume 1 Valproic acid causes all EXCEPT:
(A) It is an enzyme inhibitor
(B) It causes obesity
(C) It causes Hirsutism
(D) It causes neural tube defects
ANSWER: (C) It causes Hirsutism
REF: KDT 7th ed p- 408
Explanation is correct
June 2011 Q127 Page 829 Volume 1 RDA of calcium in normal adult male is?
(A) 100 mg
(B) 400 mg
(C) 600 mg

(D) 800 mg
ANSWER: (C) 600 mg
REF: Park 20th ed p-552, Park 22nd edition page 615
See APPENDIX- 127 for "INDIAN REFERENCE, RECOMMENDED DIETARY ALLOWANCE &
BALANCED DIET"
Note: Previously in 20th edition of park it was 400 mg but latest (22nd edition) of park has
changed values of RDA
Answer & Explanation is correct
December 2010 Q276 Page 968 Volume 1 Daily dose of folic acid for women of child bearing age is? (A) 40 micro gm (B) 4 milli gm (C) 0.5 mg (D) 0.4 mg
ANSWER: (D) 0.4 mg REF: Novak’s gynecology 13th edition page 85, Katzung 9th ed page 536
Misprint, Explanation is correct
December 2010 Q178 page 1051 Volume 1 Yellow Fever certificate of vaccination is valid for? (A) 6 years, starting from 6 days after vaccination (B) 10 years, starting from 10 days after vaccination (C) 10 years, starting from 6 days after vaccination (D) 6 years, starting from 10 days after vaccination ANSWER: (B) 10 years, starting from 10 days after vaccination
Misprint, Explanation is correct
December 2009 Q71 Page 9, 45 Volume 2 All about warfarin are true EXCEPT:
(A) Half-life is 36 hours
(B) Crosses placenta
(C) Not contraindicated in hepatic failure
(D) Inhibits all vitamin K dependent clotting factors

ANSWER: (C) Not contraindicated in hepatic failure REF: Goodman and Gillman’s 11TH edition, page 955-956 Warfarin:
Therapeutic doses of warfarin decrease by 30–50% the total amount of each vitamin
K–dependent coagulation factor made by the liver
The usual adult dose of warfarin (COUMADIN) is 5 mg/day for 2–4 days, followed by
2–10 mg/day as indicated by measurements of the INR
The bioavailability of warfarin is nearly complete when the drug is administered
orally, intravenously, or rectally.
Warfarin is almost completely (99%) bound to plasma proteins, principally albumin,
and the drug distributes rapidly into a volume equivalent to the albumin space
Warfarin is metabolised in the liver, and liver disease may result in dangerous levels
of warfarin.
The t1/2 ranges from 25 to 60 hours (mean= 40 hours); the duration of action of
warfarin is 2–5 days.
Bleeding is the major toxicity of oral anticoagulant drugs.
Crosses placenta and causes fetal malformations and abortion if given during
pregnancy (see APPENDIX-32)
December 2009 Q57 Page 41 Volume 2 A patient is having deficiency of Von Willebrand factor. What abnormalities he will present with? (A) Increased PTT, increased PT (B) Decreased PT, Increased PTT (C) Normal PT , Normal PTT (D) Normal PT & Increased PTT
ANSWER: (D) Normal PT & Increased PTT
Misprint, Explanation is correct
June 2009 Q193 Page 122 Volume 2 True statements regarding acute attack of gouty arthritis is all EXCEPT:
(A) Joint aspirate reveals negative birefringent crystals
(B) Allopurinol should be started immediately
(C) Colchicine is known to provide relief
(D) Serum Uric acid levels may be absolutely normal
Misprint, Explanation is correct
June 2009 Q194 Page 191 Volume 2
Correct but additional information Male patient suffering from headache, proffuse sweating, palpitations and BP-160/110.
Drug which will be most useful is?
(A) Nifedipine
(B) Labetalol
(C) Prazosin
(D) Phenxybenzamine
ANSWER: (B) Labetalol
REF: Harrison 17th ed table 241, Swanson's Family Medicine Review: A Problem Oriented
Approach by Richard W. Swanson, Alfred F. Tallia, Joseph E. Scherger, Nancy Dickey page 123
This is a case of hypertensive crisis. Both hypertensive emergency and hypertensive urgency
are included in hypertensive crisis. The key to successful management of severe
hypertension is to differentiate hypertensive crises from hypertensive urgencies. The degree
of target organ damage, rather than the level of blood pressure alone, determines the
rapidity with which blood pressure should be lowered. Tables 241-9 list a number of
hypertension-related emergencies and recommended therapies.
Note:
Drug of choice for prevention and treatment of Pheochromocytoma is
Phenxybenzamine
Drug of choice for adrenergic crisis of Pheochromocytoma is Phentolamine
Drug of choice for hypertensive crisis in general is Nitroprusside
Also see APPENDIX- 88 for “ANTIHYPERTENSIVE MEDICATIONS”
Harrison 17th ed table 241-1 Blood Pressure Classification
Blood Pressure Classification Systolic, mmHg Diastolic, mmHg
Normal <120 and <80
Prehypertension 120–139 or 80–89
Stage 1 hypertension 140–159 or 90–99
Stage 2 hypertension >160 or >100
Isolated systolic hypertension >140 and <90
Harrison says “In addition to pheochromocytoma, an adrenergic crisis due to
catecholamine excess may be related to cocaine or amphetamine overdose, clonidine
withdrawal, acute spinal cord injuries, and an interaction of tyramine-containing
compounds with monamine oxidase inhibitors. These patients may be treated with
phentolamine or nitroprusside”
Table 241-9 Preferred Parenteral Drugs for Selected Hypertensive Emergencies
Hypertensive encephalopathy Nitroprusside, nicardipine, labetalol
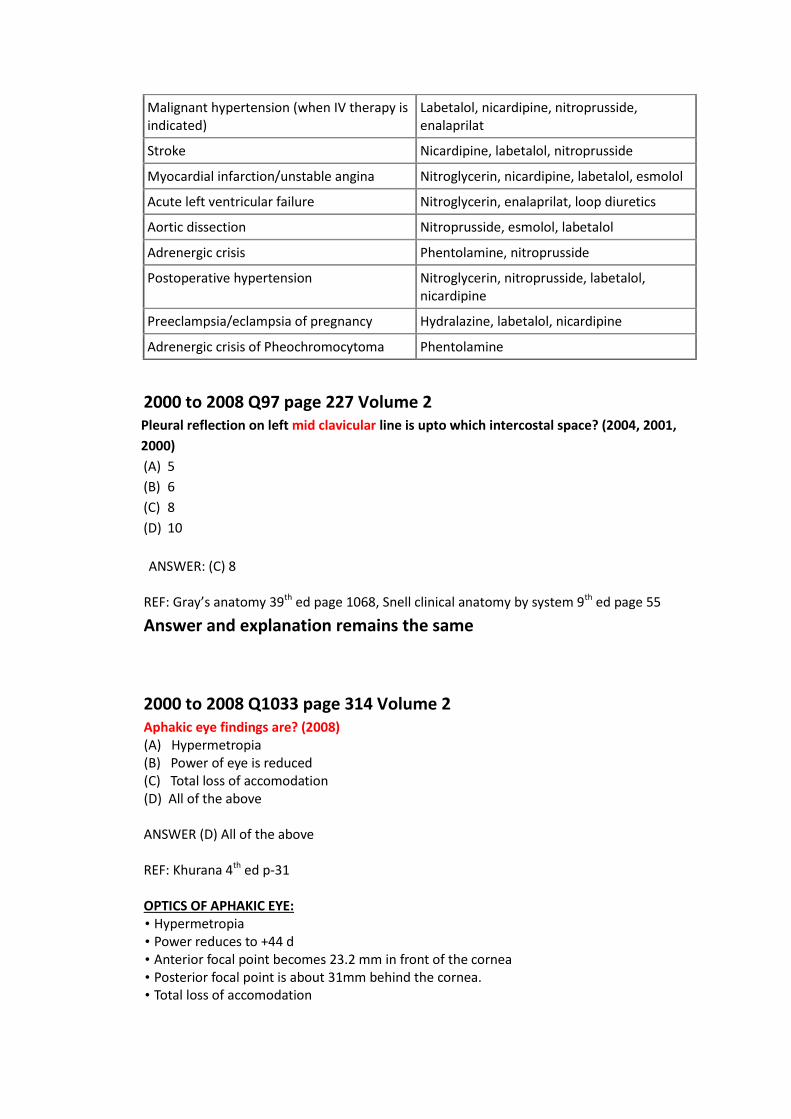
Malignant hypertension (when IV therapy is indicated)
Labetalol, nicardipine, nitroprusside, enalaprilat
Stroke Nicardipine, labetalol, nitroprusside
Myocardial infarction/unstable angina Nitroglycerin, nicardipine, labetalol, esmolol
Acute left ventricular failure Nitroglycerin, enalaprilat, loop diuretics
Aortic dissection Nitroprusside, esmolol, labetalol
Adrenergic crisis Phentolamine, nitroprusside
Postoperative hypertension Nitroglycerin, nitroprusside, labetalol, nicardipine
Preeclampsia/eclampsia of pregnancy Hydralazine, labetalol, nicardipine
Adrenergic crisis of Pheochromocytoma Phentolamine
2000 to 2008 Q97 page 227 Volume 2 Pleural reflection on left mid clavicular line is upto which intercostal space? (2004, 2001,
2000)
(A) 5
(B) 6
(C) 8
(D) 10
ANSWER: (C) 8
REF: Gray’s anatomy 39th ed page 1068, Snell clinical anatomy by system 9th ed page 55
Answer and explanation remains the same
2000 to 2008 Q1033 page 314 Volume 2 Aphakic eye findings are? (2008) (A) Hypermetropia (B) Power of eye is reduced (C) Total loss of accomodation (D) All of the above
ANSWER (D) All of the above REF: Khurana 4th ed p-31 OPTICS OF APHAKIC EYE: • Hypermetropia • Power reduces to +44 d • Anterior focal point becomes 23.2 mm in front of the cornea • Posterior focal point is about 31mm behind the cornea. • Total loss of accomodation
2000 to 2008 Q1180 page 327 & 676 Volume 2 Methaemoglobinaemia may result from exposure to? (2007,2006,2004)
(A) Carbon monoxide
(B) Aniline
(C) Sodium chlorate
(D) Both (B) & (C)
ANSWER: Both (B) & (C) REF: Harrisons Medicine 18th Edn Page 857, 858, Cecil Medicine 19th Edn, CMDT 2011
Misprint, Explanation is correct
2000 to 2008 Q1312 page 339 Volume 2 Which of the following is not used in treatment of status epilepticus? (2000) (A) Lorazepam (B) Clonazepam (C) Propofol (D) Gabapentin ANSWER: (D) Gabapentin REF: Harrisons 18th Edn Page 3268
Misprint, Explanation is correct
2000 to 2008 Q1851 page 389 & 867 Volume 2 Treatment of choice in acute Bipolar depression is? (2004) (A) Valproate (B) Lamotrigine (C) Lithium (D) All of the above ANSWER: (B) Lamotrigine
REF: Kaplan and Sadock's 9th Edn Page: 568-72, Neeraj Ahuja 5th Edn Page: 75-80 First line of treatment of acute bipolar depression is SSRI with mood stabliser. Lamotrigine may be used if response is not obtained. ECT may also be used. Lithium, valproate, carbamezapine is used in maintenance.
2000 to 2008 Q273 page 487 Volume 2 Purine metabolism end product in non primates is? (2007)
(A) Uric acid
(B) Ammonia
(C) Allantoin
(D) Both A & B
ANSWER: (C) Allantoin
REF: Biochemistry 3rd edition by S C Rastogi page 366
See PD June 2012 (Biochemistry) for explanation
Explanation is correct
2000 to 2008 Q749 page 589 Volume 2 Obturator foramen in female is? (1990)
(A) Oval
(B) Triangular
(C) Square
(D) Rounded
ANSWER: (B) Triangular
Explanation is correct
2000 to 2008 Q760 page 589 Volume 2 Cyanides acts by binding to? (2007,2004,2002)
(A) Cytochrome oxidase (B) Acetylcholinesterase (C) Beta 2 adrenergic receptors (D) Histamine ANSWER: (A) Cytochrome oxidase REF: Parikh 6th Edn, Page 6.38, 11.26 Repeat 2012 Session II
2000 to 2008 Q793 page 594 Volume 2 Temperature of the body rises up for the first 2 hrs after death. The probable condition
includes the following, EXCEPT (1989)

(A) Sun stroke
(B) Frost bite
(C) Septicemia
(D) Tetanus
ANSWER: (C) Frost bite REF: Parikh 6th Ed Pg 3.9
Explanation is correct
2000 to 2008 Q1006 page 631 Volume 2 Lateral sinus thrombosis is associated with all EXCEPT: (2003)
(A) Greisinger sign
(B) Gradenigo sign
(C) Lily crowe sign
(D) Tobey Ayer test
ANSWER : (B) Gradenigo sign
REF: P.L. Dhingra 3rd Edn Page: 110, 78, 83,84 Indirect Repeat 2012 Session I, December 2011 Note: Lily Crowe sign is the same as Crowe Beck sign
2000 to 2008 Q1193 page 682 Volume 2 Decrease vasomotor tone & increase pooling of blood seen in shock due to? (2007)
(A) Neurogenic shock
(B) Pulmonary embolism
(C) Cardiac shock
(D) Hypolvemia
ANSWER : (A) Neurogenic shock REF: Harrison’s 17th Ed Ch 264
Misprint, Explanation is correct
2000 to 2008 Q1196 page 683 Volume 2 Notching of the ribs is seen in? (2007,2006,2004) (A) TR (B) TOF
(C) Coarctation of aorta (D) PDA ANSWER: (C) Coarctation of aorta REF: Harrison Medicine 17th Edn Page 1462, OP Ghai 6th Edn Page 419, BD Chaurasia , Repeat December 2009 (Medicine)
Misprint, Explanation is correct
2000 to 2008 Q1418 page 761 Volume 2 Linitis plastica is a type of? (2005,2001)
(A) Gastric ulcer
(B) Carcinoma stomach
(C) Duodenal ulcer
(D) None
ANSWER: (B) Carcinoma stomach
Misprint, Explanation is correct
2000 to 2008 Q1445 page 767 Volume 2
A foreign body usually gets arrested in which part of the oesophagus? (2003) (A) Cardiac part of the oesophagus (B) In the middle third of the oesophagus (C) Below the cricopharynx (D) Above the cricopharynx ANSWER: (C) Below the cricopharynx REF: Schwartz 9th Edn Page 2738, P L Dhingra, 4th edition, page 64, Keith L. Moore 4th edition page 109 Indirect repeat June 2010 (anatomy), see constrictions of esophagus NOTE: Most of the text books mentions the most common site of foreign body in esophagus as "at the level of cricopharynx". Going by logic it should be just above the cricopharynx constriction, However some of the ENT books have particularly mentioned as "Just below the cricopharynx". On searching Journals we found this text: "Most of the foreign bodies were arrested at a distance of an inch below the cricopharyngeal sphincter. An explanation forwarded by Nandi and Ong for this phenomenon is that the strong propulsive pharyngeal muscles force an object this far while the less active oesophageal musculature cannot carry it further"
REF: Nandi, P. and Ong, G. B.: Foreign bodies in the oesophagus: Review of 2394 cases. Brit. J. Surg., 65: 5-9, 1978.
The most common foreign body found in adults was bone and in children it was a coin.
Foreign bodies in the esophagus typically impact at physiologic or pathologic areas of narrowing with the most common site being the cervical inlet followed by the middle esophagus, and least likely the lower esophagus.
The first constriction where the esophagus commences at the cricopharyngeal sphincter; this is the narrowest portion of the esophagus and is the most common site of foreign body
The most common site of oesophageal impaction is at the thoracic inlet. Defined as the area between the clavicles on chest radiograph, this is the site of anatomical change from the skeletal muscle to the smooth muscle of the oesophagus. The cricopharyngeus sling at C6 is also at this level and may "catch" a foreign body. About 70% of blunt foreign bodies that lodge in the oesophagus do so at this location.
Another 15% become lodged at the mid oesophagus, in the region where the aortic
arch and carina overlap the oesophagus on chest radiograph. (T4)
The remaining 15% become lodged at the lower oesophageal sphincter (LES) at the
gastroesophageal junction. (T11)
2000 to 2008 Q1461 page 772 Volume 2
Which of the following is not an indication for liver transplantation? (2002)
(A) Fatty liver
(B) HIV
(C) Wilson's disease
(D) Primary hyperoxaluria
ANSWER: (B) HIV REF: Harrison 17th Edn Page 1984 table 304-1, Washington Manual of Surgery 5th Edition page 406 table 23-6
Misprint, Explanation is correct
2000 to 2008 Q1584 page 800 Volume 2
ADDITIONAL INFORMATION High risk of trophoblastic disease is in which one of the following? (2007)
(A) Normal term delivery
(B) Abortion
(C) H.mole
(D) Eclampsia
ANSWER: (A) Normal term pregnancy
REF: Novak's 15 ed Pg 1591
RISK FACTORS OF GESTATIONAL TROPHOBLASTIC DISEASE: 1. Areas with a high incidence of molar pregnancy also have a high frequency of vitamin A
deficiency.
2. Maternal age older than 35 years has consistently been shown to be a risk factor for
complete mole. In one study, the risk for complete mole was increased 2.0-fold for
women older than 35 years and 7.5-fold for women older than 40 years
3. Previous history of Hydatiform mole (5-40 times)
4. Limited information is available concerning risk factors for partial molar pregnancy.
However, the epidemiologic characteristics of complete and partial mole may differ.
There is no association between maternal age and the risk for partial mole.
5. The risk for partial mole has been reported to be associated with the use of oral
contraceptives and a history of irregular menstruation, but not with dietary factors
INCIDENCE OF GESTATIONAL TROPHOBLASTIC TUMOR Gestational trophoblastic neoplasia almost always develops with or follows some form of pregnancy.
Approximately half of cases follow a hydatidiform mole
25 percent follow an abortion
25 percent develop after an apparently normal pregnancy.
RISK FACTORS FOR GESTATIONAL TRIOPHOBLASTIC TUMOR:
1. hCG level >100,000 mIU/ml
2. Excessive uterine enlargement
3. Theca lutein cysts 6 cm in diameter.
4. Older patients are also at increased risk of developing postmolar GTT. One study
reported that persistent tumor developed after a complete molar pregnancy in 37% of
women older than 40 years, whereas in another study this finding occurred in 56% of
women older than 50 years
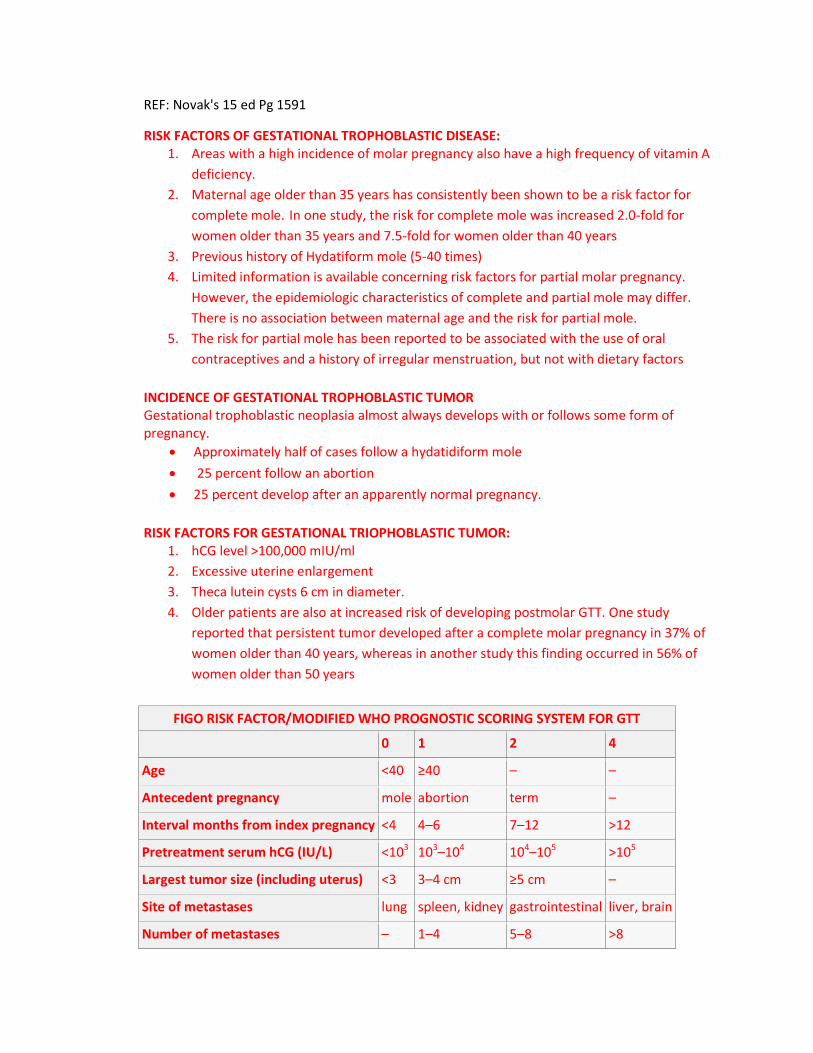
FIGO RISK FACTOR/MODIFIED WHO PROGNOSTIC SCORING SYSTEM FOR GTT
0 1 2 4
Age <40 ≥40 – –
Antecedent pregnancy mole abortion term –
Interval months from index pregnancy <4 4–6 7–12 >12
Pretreatment serum hCG (IU/L) <103 103–104 104–105 >105
Largest tumor size (including uterus) <3 3–4 cm ≥5 cm –
Site of metastases lung spleen, kidney gastrointestinal liver, brain
Number of metastases – 1–4 5–8 >8
Previous failed chemotherapy – – single drug ≥2 drugs
Women with a score of 6 or less are at low risk and tend to have a good outlook
regardless of how far the cancer has spread. The tumor(s) will usually respond well to
chemotherapy.
Women with a score of 7 or more are at high risk, and their tumors tend to respond less
well to chemotherapy, even if they haven't spread much. They may require more
intensive chemotherapy.
NOTE: From the above text it is clear that although GTT are more common in H.Mole, but are High risk
in Normal term pregnancies (See table)
2000 to 2008 Q1599 page 802 Volume 2 'Peg cells' are seen in? (2006,2000)
(A) Vagina
(B) Vulva
(C) Ovary
(D) Fallopian Tubes
ANSWER: (D) Fallopian tubes REF: Shaws 14th Edn Page 9, Oxford Desk Reference: Obstetrics and Gynaecology edited by Sabaratnam Arulkumaran, Lesley Regan, Aris Papageorghiou, Ash Monga, David Farquharso page 472
"Peg cells are nonciliated secretory epithelial cells that are found in increasing numbers from the infundibulum to the isthmus in the oviduct and serves to produce fluid rich in nutrient for the ova, spermatozoa and zygote. Peg cells are particularly well developed and easy to see at day 14 of menstrual cycle around the time of ovulation" The mucosa of oviduct (Fallopian tubes) have three different cell types.
Columnar ciliated epithelial cells 25%
Non ciliated columnar cells 60% (Most prominent in Isthmus)
Peg cells between secretory and ciliated cells 15%
2000 to 2008 Q1627 page 808 Volume 2 Uterus with two uterine cavities and single cervix is? (2004) (A) Uterus bicornis unicolis (B) Uterus unicornis (C) Uterus bicornis bicolis (D) Uterus didelphys
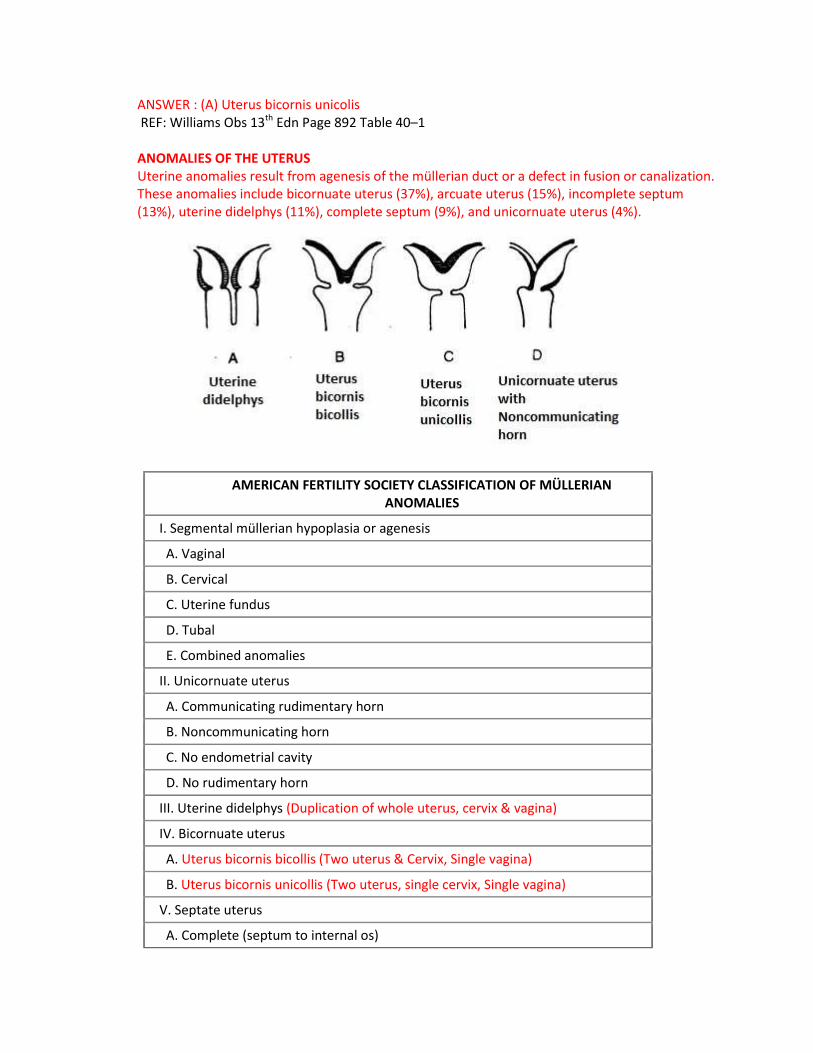
ANSWER : (A) Uterus bicornis unicolis REF: Williams Obs 13th Edn Page 892 Table 40–1 ANOMALIES OF THE UTERUS Uterine anomalies result from agenesis of the müllerian duct or a defect in fusion or canalization. These anomalies include bicornuate uterus (37%), arcuate uterus (15%), incomplete septum (13%), uterine didelphys (11%), complete septum (9%), and unicornuate uterus (4%).
AMERICAN FERTILITY SOCIETY CLASSIFICATION OF MÜLLERIAN ANOMALIES
I. Segmental müllerian hypoplasia or agenesis
A. Vaginal
B. Cervical
C. Uterine fundus
D. Tubal
E. Combined anomalies
II. Unicornuate uterus
A. Communicating rudimentary horn
B. Noncommunicating horn
C. No endometrial cavity
D. No rudimentary horn
III. Uterine didelphys (Duplication of whole uterus, cervix & vagina)
IV. Bicornuate uterus
A. Uterus bicornis bicollis (Two uterus & Cervix, Single vagina)
B. Uterus bicornis unicollis (Two uterus, single cervix, Single vagina)
V. Septate uterus
A. Complete (septum to internal os)

B. Partial
VI. Arcuate
VII. Diethylstilbestrol related
APPENDIX-54 page 1040 Volume 2
ECG CHANGES
DIGOXIN INTOXICATION (Hypokaliemia, hypomagnesaemia and hypercalcemia aggravate digitalis toxicity)
Oddly shaped ST-depression (Salvador
Dali's mustache appearance) T wave flat, negative or
biphasic Short QT interval Increased u-wave amplitude Prolonged PR-interval Bradyarrhythmias: Sinus
bradycardia, AV block. Including complete AV
block and Wenckebach. Tachyarrhythmia’s: Junctional
tachycardia, Atrial tachycardia Ventricular ectopia, bigemini, monomorphic ventricular
tachycardia, bidirectional ventricular
tachycardia
HYPOTHERMIA
Sinus bradycardia Prolonged QT-interval ST depression Osborne-waves/ J Wave
(temperature <32 C)
HYPERKALEMIA
Broad based, Tall T waves (T wave tenting,
Thorn like T wave-Earliest change)
Poor p-waves (Flat, even absent in severe
hyperkalemia) Prolonged PR interval Wide QRS widening
(nonspecific intraventricular conduction
defect) Slurred QRS complex which
blends sinuously with the tall T wave
into a "sine" wave pattern At concentrations > 7.5
mmol/L, atrial and ventricular fibrillation can
occur.
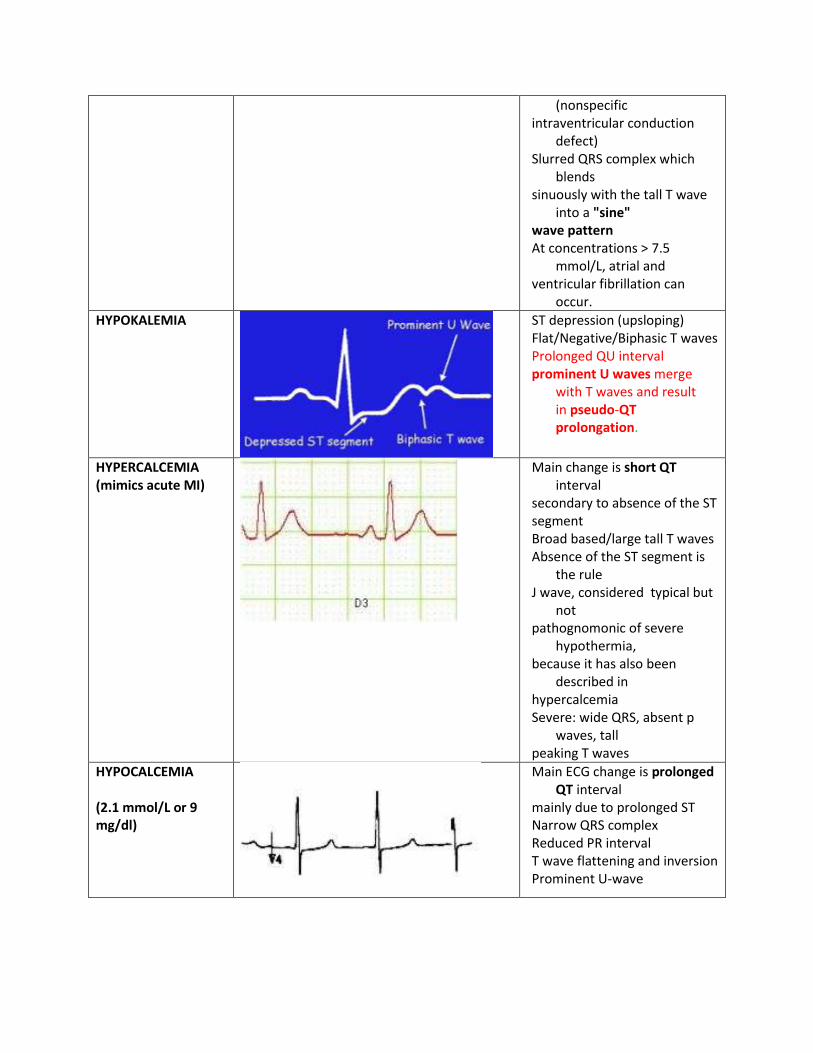
HYPOKALEMIA
ST depression (upsloping) Flat/Negative/Biphasic T waves Prolonged QU interval prominent U waves merge
with T waves and result in pseudo-QT prolongation.
HYPERCALCEMIA (mimics acute MI)
Main change is short QT interval
secondary to absence of the ST segment Broad based/large tall T waves Absence of the ST segment is
the rule J wave, considered typical but
not pathognomonic of severe
hypothermia, because it has also been
described in hypercalcemia Severe: wide QRS, absent p
waves, tall peaking T waves
HYPOCALCEMIA (2.1 mmol/L or 9 mg/dl)
Main ECG change is prolonged QT interval
mainly due to prolonged ST Narrow QRS complex Reduced PR interval T wave flattening and inversion Prominent U-wave
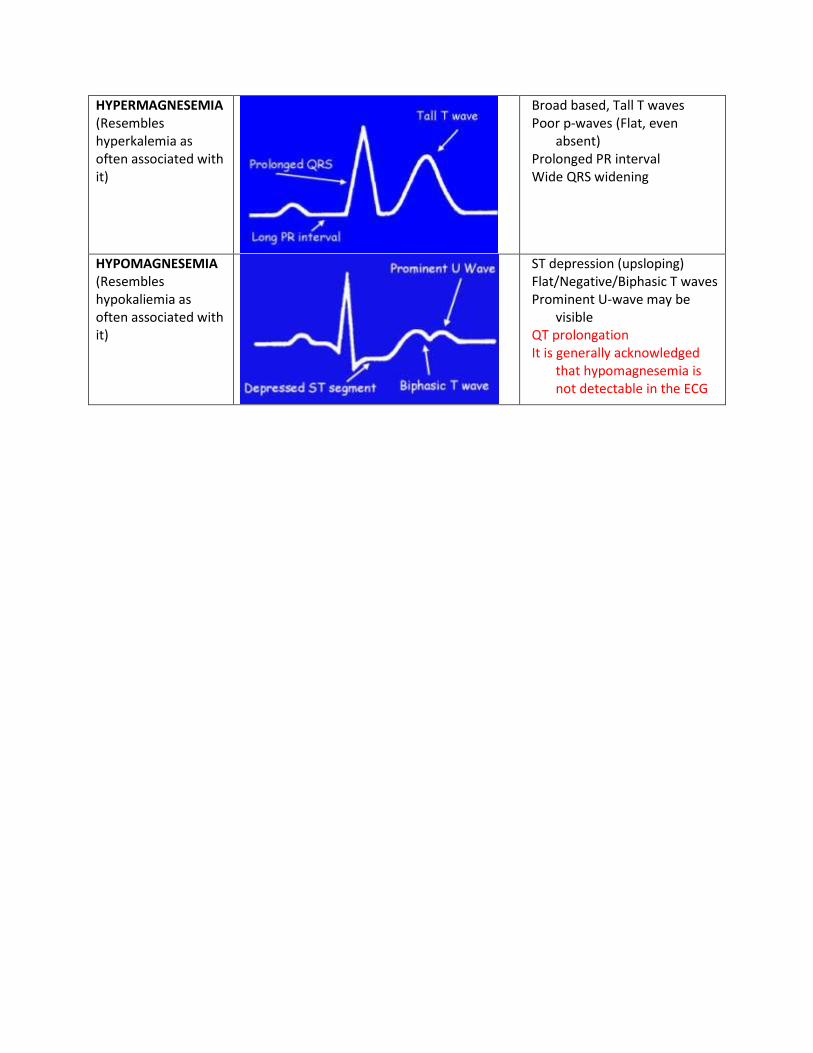
HYPERMAGNESEMIA (Resembles hyperkalemia as often associated with it)
Broad based, Tall T waves Poor p-waves (Flat, even
absent) Prolonged PR interval Wide QRS widening
HYPOMAGNESEMIA (Resembles hypokaliemia as often associated with it)
ST depression (upsloping) Flat/Negative/Biphasic T waves Prominent U-wave may be
visible QT prolongation It is generally acknowledged
that hypomagnesemia is not detectable in the ECG