Equinoxe fracture technique 7-11 - University of...
18
A Great Day in the O.R. SM 352-377-1140 1-800-EXACTECH www.exac.com #718-00-33 REV A 0705 ©2005 EXACTECH, INC. ISO 13485 CERTIFIED Operative Technique Fracture Stem ANATOMICAL. REDEFINED. Equinoxe Fracture Stem • Operative Technique
Transcript of Equinoxe fracture technique 7-11 - University of...

A Great Day in the O.R. SM
352-377-11401-800-EXACTECHwww.exac.com
#718-00-33 REV A 0705
©2005 EXACTECH, INC. ISO 13485 CERTIFIED
Operative Technique
Fracture Stem
ANATOMICAL.REDEFINED.
Equin
oxe Fractu
re Stem
• Operative Tech
niq
ue

TABLE OF CONTENTS
INTRODUCTION ........................................................................... 1
SYSTEM SPECIFICATIONS .......................................................... 2
OVERVIEW TECHNIQUE FOR RIGHT SHOULDER ..................... 3
DETAILED OPERATIVE TECHNIQUE ............................................ 6
SPECIAL CONSIDERATIONS ....................................................... 6
PRE-OPERATIVE EVALUATION.................................................... 6
PATIENT POSITIONING ................................................................ 6
SURGICAL APPROACH................................................................. 7
HUMERAL PREPARATION............................................................ 8
FRACTURE STEM TRIALING ........................................................ 8
Retroversion when the distal bicipital groove is visible....... 8
Retroversion when the distal bicipital groove is not visible 8
Humeral Stem Height .............................................................. 9
Tips for Establishing Height Intra-Operatively ..................... 9
Humeral Head Trial ................................................................... 9
TRIAL REDUCTION ....................................................................... 10
CEMENTING THE FRACTURE STEM ........................................... 10
TUBEROSITY FIXATION ............................................................... 11
Tuberosity Reattachment.......................................................... 11
SUTURING TECHNIQUE FOR RIGHT SHOULDER ..................... 12
TYING THE SUTURES .................................................................. 14
FINAL STABLE RECONSTRUCTION ........................................... 16
POST-OPERATIVE REHABILITATION ........................................... 17
EQUINOXE IMPLANT SCOPE ..................................................... 18
EQUINOXE INSTRUMENT SCOPE ............................................. 18
EQUINOXE SHOULDER SYSTEM DESIGN TEAM
Pierre-Henri Flurin, M.D. Surgical Clinic of Bordeaux, Merignac (France)
Thomas W. Wright, M.D. University of Florida
Joseph D. Zuckerman, M.D. NYU - Hospital for Joint Diseases
The Equinoxe Shoulder System redefines “anatomical.” Theprimary stem allows independent adjustability of all fouranatomic parameters in situ. The fracture stem’s offsetanterior-lateral fin and asymmetric tuberosity beds define thenext generation in complex fracture reconstruction.
INTRODUCTION
Throughout the development process, our team has collaborated onevery facet of the Equinoxe Shoulder System including this surgicaltechnique. We decided to take a comprehensive approach to thetechnique, discussing the surgery from pre-operative planning to post-operative rehabilitation, since many shoulder replacements areperformed by surgeons who may only do two to three per year.Obviously, there are myriad approaches to each step of shoulderarthroplasty and the surgeon should feel free to employ those withwhich he is most comfortable. The Equinoxe-specific techniques, though,should be respected to help ensure a safe and successful surgery.
We began the product development process by identifying concerns ourteam had with shoulder replacements for complex fractures of theproximal humerus. Our goal was to develop solutions to those concernsand we believe the Equinoxe System significantly improves thesurgeon's ability to secure the tuberosities. The asymmetric beds act asa scaffold for the stable reconstruction of the fractured fragments. Theoffset anterior-lateral fin, when placed in the distal bicipital groove,assists the surgeon in correctly establishing retroversion.
We've decided to offer the surgical technique in two different formats.The first is a high level overview intended as a refresher before surgeryor as a guide for the surgeon's support staff. The detailed narrativeversion is intended for an in-depth understanding of the step-by-stepapproach that our team has endorsed and should be read at least oncebefore using the Equinoxe Shoulder System.
We hope that our work, both the technique and the EquinoxeShoulder System, will facilitate “A Great Day in the OR” for thesurgeon and the staff.
Respectfully,
Pierre-Henri Flurin, M.D.Surgical Clinic of Bordeaux-Merignac (France)
Thomas W. Wright, M.D.University of Florida
Joseph D. Zuckerman, M.D.NYU - Hospital for Joint Diseases
Left Right

2 3
Fracture StemSurface Finish Inherent Anterior
Distal Length Sides Material Tuberosity Remainder Suture Posterior OffsetDiameter (mm) Beds of Stem Holes Offset (mm) of Fin (mm)
(mm)7.09.5 14012.0
Humeral Heads
Height (mm)Diameter Short Tall Expanded Offset Material
(mm) (mm)38 16 19 041 16 20 044 17 21 1.5
Co-Cr47 18 22 26 1.550 19 23 27 1.553 20 24 28 1.5
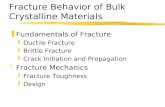
A. Incision and exposure B. Reaming the humeral shaft C. Inserting the trial fracture stem
D. Establishing/maintaining the height E. Trial reduction F. Preparing shaft for cement
Rights& Lefts
Ti-6Al-4V 16 grade
Satin finishgrit blast
Rounded toavoid
breakage
SYSTEM SPECIFICATIONS OVERVIEW TECHNIQUEFOR RIGHT SHOULDER
1.8 6.01.8 7.51.8 7.5
• Contralateral X-ray with templateoverlays to approximate height(use fin holes as reference)
• Pull down test — With trial headin place, pull arm distally and thetop of the head should be at the topof the glenoid
• Finger test — One finger shouldfit between the greater tuberosityand the acromion
• Piece back the tuberosities tosnugly fit under the humeral head
• If medial bone is intact, use as areference to determine height
• Once height is established,maintain with fracture stempositioning device

4 5
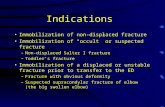
M. Tie LT vertical suture
N. Tie GT vertical suture O. Tie final cerclage I. Place LT horizontal sutures (LTH)
J. Place final cerclage (FC) K. Tie horizontal sutures
L. Place and tie cuff interval suture (RCI)
H. Place GT horizontal sutures (GTH)
G. Cementing final stem
GreaterTuberosity Lesser
Tuberosity

The EquinoxeTM Fracture Shoulder System is indicated to relieve pain and restorefunction in skeletally mature individuals with three- and four-part fractures of theproximal humerus and humeral head fracture with displacement of thetuberosities. For a more detailed description of the indications and the listing ofcontraindications, please refer to the package insert.
Special ConsiderationsThe decision to proceed with proximal humeral replacement should reflect acareful consideration of both injury and patient factors. An important injury factoris the degree of tuberosity displacement; it indicates the degree of soft-tissueinjury and is associated with an increased risk of osteonecrosis. The degree ofcomminution and bone quality are also important factors that may prevent optimalfixation.
Important patient factors include the age and functional needs of the patient.Additionally, the presence of pre-existing functional deficits in the involvedextremity must be considered in the decision to proceed with a reconstructiveprocedure. Patients must be able to participate in a structured post-operativerehabilitative program, which is essential for a successful outcome.
Pre-operative EvaluationEstablishing the appropriate humeral head heightand humeral length is a challenge inreconstructing four-part proximal fractures. Themost common pre-operative method to evaluatehumeral head height in the fractured shoulder isby comparison to the contralateral humerus in anAP radiograph.
Once the appropriate head height is established,mark the AP radiograph with the anticipatedlocation of the humeral head using the Equinoxesurgical templates. (Figure 1) Define the heightlevel of the humeral stem relative to the fractureline. The graduated markings on the templateshould be used to match those on the stem trial toestablish the final height. Additionally, assess theappropriate stem diameter relative to the canaldiameter; each stem has a 1mm circumferentialcement mantle.
Patient PositioningThe patient should be placed on an operatingtable in a supine position. The head of theoperating table should be elevated approximately30° in a modified beach chair position. A small
bolster is placed behind the involved scapula. The patient should be moved to theside of the table so that the upper extremity can be placed into maximumextension without obstruction by the operating table. Alternatively, a captain’schair or similar positioning device can be used for proper patient positioning. Thepatient should be secured to the operating table to minimize any changes in positionintra-operatively. The entire upper extremity should be prepped and draped to allowfull mobility during the procedure.
Surgical ApproachA straight deltopectoral incision is made beginning just lateral to the tip of thecoracoid process and extending distally and laterally to the insertion of the deltoid.The subcutaneous tissues are divided and medial and lateral flaps are elevated toexpose the deeper muscular layers.
The deltopectoral interval is identified by localization of the cephalic vein. Thecephalic vein is usually retracted laterally with the deltoid muscle. In someinstances the cephalic vein is more easily retracted medially with the pectoralismajor. In either case, care should be taken to preserve the cephalic veinthroughout the procedure.
The subdeltoid space is mobilized, as is the pectoralis major. The conjoined tendonmuscles are identified and the clavipectoral fascia is divided at the medial edge ofthe conjoined tendon muscles. The fracture hematoma is usually evident afterdividing the clavipectoral fascia. The conjoined tendon muscles and the pectoralismajor are retracted medially and the deltoid is retracted laterally. This can be mosteasily accomplished with the use of a self-retaining type of retractor. After thefracture hematoma has been evacuated, the deeper structures can be visualized.The biceps tendon should be identified and tagged with a suture. The bicepstendon provides an orientation to the greater and lesser tuberosities.
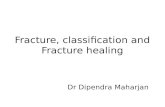
The lesser tuberosity is located medial to thebiceps tendon and the greater tuberosity islocated superiorly and laterally. Each tuberosityshould be tagged with a #2 suture for easiermobilization. These sutures should be placed atthe tendon insertion site because this isgenerally the most secure area: placement of thesutures through the tuberosity itself can result infragmentation. The lesser tuberosity is mobilizedand retracted medially while the greatertuberosity is retracted laterally and superiorly toallow visualization of the articular segment.(Figure 2)
In four-part fractures, the articular segment isgenerally devoid of soft-tissue attachments andis easily removed. The coracoacromial ligamentshould be identified at its coracoid attachmentand followed to its acromial attachment. Whenpossible, preserve the ligament because of itspotential contribution to anterior-superior stability.
With the articular segment removed and the tuberosities retracted, the glenoidarticular surface should be inspected. In most situations, the articular surface of theglenoid is intact. It should be visualized to confirm the absence of pre-existingdegenerative changes or acute injury. The axillary nerve can usually be palpated atthe anterior-inferior aspect of the glenoid. Continuity of the axillary nerve can beconfirmed by the "tug test" which consists of palpation of the nerve as it comesaround the humeral neck on the underside of the deltoid and as it passes inferiorto the glenoid. A gentle back and forth "tugging" motion confirms its continuity. Atthis point the humerus should be placed in extension to expose the proximalportion of the humeral shaft.
6 7
DDEETTAAIILLEEDD OOPPEERRAATTIIVVEE TTEECCHHNNIIQQUUEE
Figure 1 Determining height pre-operatively using
Equinoxe Surgical Templates
Figure 2 Tuberosity
Identification and Mobilization
Left Right

8 9
Figure 3 Straight Reamer Scale
Figure 4Establish version by aligning
the anterior-lateral fin with thedistal bicipital groove.
HUMERAL PREPARATION
Sequentially ream the intramedullary canalbeginning with the 8mm reamer, untilendosteal cortical contact is achieved. (Figure3) To avoid over reaming, keep in mind theanticipated stem diameter based on pre-operative templating. The canal should bereamed to the depth specified by the laseretching, which corresponds to the heightestablished during the templating.
The use of a cement restrictor is based onpersonal preference; however, anappropriately sized cement restrictor willimprove distribution. If a cement restrictor willbe used, it is advantageous to place the cementrestrictor in the humeral canal after reamingand before the fracture stem positioning deviceis attached to the humerus to avoid interferencewith the K-wires.
Note: Reaming to the 115mm laser mark willensure adequate depth if desired height wasdifficult to determine pre-operatively.
Fracture Stem Trialing
Select the trial stem based on the last reamerused. Ensure that the appropriate stem side ischosen (e.g. “Right” or “Left”).
Retroversion when the distal portion ofbicipital groove is visible
Retroversion is established by aligning theanterior-lateral fin of the trial stem with theposterior aspect of the distal bicipital groove.(Figure 4) Computational analysis of data fromour anatomic study of cadaveric humeridemonstrated that placing the fin in theposterior aspect of the distal bicipital grooveestablished retroversion as accurately as thetraditional technique of using a pre-selectedfixed angle relative to the epicondylar axis.
Retroversion when the distal portion ofbicipital groove is not visible
Typically, the distal portion of the bicipitalgroove is visible but in cases when it is not, thestandard technique of retroverting the implantat 20° relative to the forearm should be used. Inthis case, the surgeon must attach the stemimpactor to the trial and screw in theretroversion guide as shown in the figure to theright. By aligning the retroversion guide withthe forearm, the stem will be placed in 20° ofretroversion. (Figure 5) A mark should beplaced on the humeral cortex that correspondsto the anterior-lateral fin of the implant tomaintain 20° of retroversion duringimplantation.
Humeral Stem Height
Place the trial stem into the intramedullarycanal at the desired height as determined pre-operatively (e.g. templating contralateralshoulder) or based on the surgeon's intra-operative judgment (see “Tips for EstablishingHeight Intra-operatively”). Select the fracturestem positioning device that corresponds tothe size of the stem and slide the two pinsthrough the top and bottom suture holes in theanterior-lateral fin of the stem. Then place twoK-wires (0.062mm) into the humeral shaft tostabilize the fracture stem positioning deviceto the bone. The goal is to secure the K-wires in the cortical bone so choose the widest holes that still align with the humerus. Selecting a middle row allows the surgeon to make +/- 4mm height adjustments during the trial reduction by sliding the fracture stem positioning device off the K-wires andrepositioning it.
Tips for Establishing Height Intra-operatively
• PULL DOWN TEST — With trial head in place, pull arm distally and the top of the head should be at the top of the glenoid
• FINGER TEST — One finger should fit between the greater tuberosity and the acromion
• Piece back the tuberosities to snugly fit under the humeral head
• If there is no medial bone comminution and no metaphyseal bone on the head fragment then the calcar of the humeral stem can be placed directly on this medial bone which will then determine head height.
Humeral Head Trial
As a starting point, choose a humeral head trialbased on the size of the patient's anatomichumeral head. The eccentric position of themodular humeral head should be chosenbased on the anatomy and/or soft tissuetension as assessed during trial reduction ofthe tuberosities.
Figure 5As a visual check of version,the retroversion guide can be
aligned with the forearm toplace the humeral stem in 20°
of retroversion.
Figure 6The fracture stempositioning device
maintains the surgeon'sdesired stem height
during trial reduction.

10 11
Trial Reduction
Trial reduction is a critical part of the procedurebecause it defines the parameters needed toobtain a stable construct. After the humeralhead is reduced onto the glenoid, the greaterand lesser tuberosities are pulled into position.The biceps tendon is allowed to fall betweenthe tuberosities. Traction on the tuberositysutures not only maintains the tuberosities inposition but also provides a more accurateassessment of stability. Self-retainingretractors should be relaxed when assessingsoft-tissue tension.
Assessment of posterior, inferior, and anteriorstability should be performed by translatingthe humeral head in each direction. Up to 50%of posterior and inferior translation of thehumeral head on the glenoid is acceptable;however, anterior translation should notexceed 25%. If translation is greater, theposition of the stem should be re-evaluated toconfirm that it has not subsided or rotatedwithin the canal.
Varying the thickness of the modular humeralhead provides the ability to optimize stabilityand range of motion. (Figure 7) If soft-tissuelaxity is excessive, a taller humeral head maybe needed. Conversely, if soft-tissue tension isexcessive, a shorter humeral head is chosen. Ineither situation, repeat assessment of stabilityis required to confirm that the propercomponents and position have been chosen.When the proper position and component sizeare confirmed, the trial prosthesis should beremoved.
Cementing the Fracture Prosthesis
To remove the stem, leave the fracture stempositioning device attached to the humerusand slide the holding pins out of the sutureholes in the anterior-lateral fin.
Two drill holes are placed through the humeralcortex into the intramedullary canal. Theseholes should be placed approximately 1.5 to 2cm distal to the level of the surgical neck, andadjacent to the bicipital groove. Two #5 non-absorbable sutures are passed through onedrill hole into the intramedullary canal and thenout through the second drill hole. (Figure 8)These vertical sutures are used for tuberosityfixation. The canal is then irrigated copiouslyand any loose cancellous bone removed.
Formal cement pressurization is avoided todecrease the possibility of humeral shaftfracture. The intramedullary canal should bepacked with a sponge to obtain adequatedrying before cementing. Cement is mixed andinjected into the canal with a cement gun.
Insert the final prosthesis into the canal andinsert the fracture stem positioning device'stwo holding pins through the top and bottomholes of the stem's anterior-lateral fin. (Figure9) Ensure the two sutures in the humeral shaftremain mobile and that no cement hardens inthe posterior suture handle. This will ensurethat the prosthesis is inserted at the sameheight and version as the trial.
When the cement is hardened, make certainthe taper is dry and free of any debris. The finalhumeral head component is placed on thestem in the same orientation established in thetrialing phase. Impact the humeral head usingthe impactor directly in line with the taper toensure proper engagement of the Morse taper.
Alternatively, the surgeon may want to passthe sutures through the greater tuberosity thenthe posterior bar and lateral fin prior to placingthe head as this gives easier access.
Tuberosity Fixation
Fixation of the tuberosities to the prosthesisand the shaft is critical to the success of theprocedure. Proper tuberosity reattachment andsecure fixation will enhance the probability of asuccessful outcome in terms of pain relief,range of motion, and overall function.
A grafting window is provided in the anterior-lateral fin to allow tuberosity apposition. Applycancellous bone from the humeral headbetween the shaft and the tuberosities andbetween the tuberosities to facilitate healingand a more anatomic reconstruction.
Tuberosity Reattachment
The principles of tuberosity fixation include: (1)two horizontal sutures around each tuberosityto pull the tuberosities to the stem (Figure 10);2) placement of one longitudinal suture fromthe shaft to each tuberosity to bring thetuberosities into a position below theprosthetic articular surface and into contactwith the humeral shaft; and 3) one finalcerclage suture, which cinches the tuberositiestogether and to the stem for added stability.
To secure the tuberosities to the stem, werecommend heavy (#5) non-absorbablesutures. Tuberosity reattachment should beperformed with the arm in approximately 20degrees of abduction and neutral flexion.
Head Diameter (mm)
38 41 44 47 50 53
Short 16 16 17 18 19 20
Tall 19 20 21 22 23 24
Expanded 26 27 28
Hei
gh
t (m
m)
Figure 8Prepared humerus shaft
Figure 7Humeral Head Scope
Figure 9The fracture stem positioning device enables the final
prosthesis to be positioned at the same height determinedduring trialing and maintains the desired height during
cement polymerization.
Figure 10Tuberosity reattachment

12 13
SUTURING TECHNIQUEFOR RIGHT SHOULDER

1a: To reattach the greater tuberosity, pass twohorizontal sutures between the greatertuberosity and humeral stem. Pass the firstsuture (First Horizontal suture for the GreaterTuberosity, GTH1) through the lower portion ofthe infraspinatus tendon where it inserts intothe greater tuberosity, through the posteriorhandle and through an inferior lateral suturehole of the anterior-lateral fin. Pass the secondsuture (Second Horizontal suture for the GreaterTuberosity, GTH2) through the upper portion ofthe infraspinatus tendon where it inserts intothe greater tuberosity, through the posteriorhandle and through a superior lateral suturehole of the anterior-lateral fin.
Anterior

Posterior
1b: To reattach the lesser tuberosity, pass twohorizontal sutures between the lesser tuberosityand the humeral stem. Pass the first suture(First Horizontal suture for the Lesser TuberosityLTH1) through the lower portion of thesubscapularis tendon where it inserts into thelesser tuberosity, through the anterior handleand through an inferior lateral suture hole of theanterior-lateral fin. Pass the second suture(Second Horizontal suture for the LesserTuberosity LTH2) through the upper portion ofthe subscapularis tendon where it inserts intothe lesser tuberosity, through the anteriorhandle and through a superior lateral suturehole of the anterior-lateral fin.

1c: Next, pass the finalcerclage (FC) through themiddle of the infraspinatustendon, through the posteriorhandle and around the medialportion of the stem. Next,pass the final cerclage (FC)through the anterior handleand through the middle of thesubscapularis tendon.

14 15
2: It is important to balance the applied-tensionwhen tying off each suture so as not to displace thetuberosities. First, tie the horizontal sutures for thegreater tuberosity when the arm is slightlyexternally rotated. Second, tie the horizontalsutures for the lesser tuberosity when the arm isplaced in neutral rotation.
TYING THE SUTURES

2a: Closure includes repair of therotator interval with #2 non-absorbable sutures. This repair isperformed with the humerus inexternal rotation to decrease thepossibility that rotator intervalclosure will restrict rotation.

2b: Next, pass and tie the verticalsuture (LTV1) through the topupper portion of the subscapularistendon near the rotator intervalwhere it inserts into the lessertuberosity.

2c: Finally, pass and tie the verticalsuture (GTV1) through thesupraspinatus tendon where itinserts into the greater tuberosity.

2d: Once completed, tie the finalcerclage.

16 17
Post-operative Rehabilitation
It is recommended to initiate the rehabilitationprogram on the same day as surgery or on post-operative day one. All patients begin activerange of motion of the elbow, wrists and hand,and passive range of motion of the shoulder.External rotation should be limited based uponthe intra-operative evaluation; internal rotationis allowed to the chest. This is important to avoidany excess stress on the tuberosity repair thatcould compromise healing.
Exercises are continued for six to eight weeks.Radiographs are obtained approximately twoweeks following surgery to confirm theposition of the tuberosities. Additionalradiographs are obtained at six to eight weeksfollowing surgery to assess the degree oftuberosity healing. If tuberosity healing issufficient, the sling is discontinued and anactive range-of-motion program is begun. Thepatient is encouraged to use the upperextremity for activities of daily living. Passiverange-of-motion is continued with gentlestretching to increase overall range. At eightweeks following surgery, isometric deltoid andinternal and external rotator strengtheningexercises are begun. Vigorous strengtheningexercises are not allowed until active forwardelevation of at least 90° is obtained. Mostpatients can expect continued improvementduring the first year following surgery,although most recovery will occur during thefirst six months.
Final Stable Reconstruction
When the tuberosity fixation is completed, thestability of the fixation should be carefullyassessed. Range of motion in forwardelevation, external rotation, internal rotation,and abduction should be performed todetermine the specific limits of motion that willbe allowed in the post-operative rehabilitationprogram.
Depending on surgeon preference, a drain maybe placed deep into the deltopectoral intervaland brought out through the skin distally andlaterally. The deltopectoral interval is repairedwith an absorbable suture, as is thesubcutaneous tissue. Skin closure can beperformed with either sutures or staples. Asterile dressing is applied and the upperextremity is placed in a sling.
Radiographs in the operating room arestrongly recommended. These should includean AP view of the shoulder with the humerus ininternal rotation (on the chest) and maximumexternal rotation as defined by the intra-operative assessment. An axillary view is alsoobtained. These radiographs provide excellentvisualization of the position of the prosthesisas well as the position of the tuberosities.

18
EQUINOXE IMPLANT SCOPE
Fracture Stems304-01-07 Equinoxe, humeral stem, fracture, left. 7mm304-01-10 Equinoxe, humeral stem, fracture, left, 9.5mm304-01-12 Equinoxe, humeral stem, fracture, left, 12mm304-02-07 Equinoxe, humeral stem, fracture, right, 7mm304-02-10 Equinoxe, humeral stem, fracture, right, 9.5mm304-02-12 Equinoxe, humeral stem, fracture, right, 12mm
Short Heads310-01-38 Equinoxe, humeral head, short, 38mm310-01-41 Equinoxe, humeral head, short, 41mm310-01-44 Equinoxe, humeral head, short, 44mm310-01-47 Equinoxe, humeral head, short, 47mm310-01-50 Equinoxe, humeral head, short, 50mm310-01-53 Equinoxe, humeral head, short, 53mm
Tall Heads310-02-38 Equinoxe, humeral head, tall, 38mm310-02-41 Equinoxe, humeral head, tall, 41mm310-02-44 Equinoxe, humeral head, tall, 44mm310-02-47 Equinoxe, humeral head, tall, 47mm310-02-50 Equinoxe, humeral head, tall, 50mm310-02-53 Equinoxe, humeral head, tall, 53mm
Expanded Heads310-03-47 Equinoxe, humeral head, expanded, 47mm310-03-50 Equinoxe, humeral head, expanded, 50mm310-03-53 Equinoxe, humeral head, expanded, 53mm
Stem Trials
Multiple sizes
Straight reamer
Multiple sizes
Fracture stem inserter/extractor305-07-10
Head trials
Multiple sizes
Mallet301-07-01
Head removal tool311-05-01
Impactor311-07-05
Humeral Head Impactor Tip311-07-07
Fracture Stem Positioning Device
Multiple sizes
EQUINOXE INSTRUMENT SCOPE