
epubs.surrey.ac.ukepubs.surrey.ac.uk/849473/1/DPsych NK E-Thesis.doc · Web viewepubs.surrey.ac.uk
289
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC How Parents Understand Their Daughters Behaviour Before They Receive a Diagnosis of an Autism Spectrum Condition Natalie Kseib Submitted for the Degree of Doctor of Psychology (Clinical Psychology) School of Psychology Faculty of Health and Medical Sciences 1
Transcript of epubs.surrey.ac.ukepubs.surrey.ac.uk/849473/1/DPsych NK E-Thesis.doc · Web viewepubs.surrey.ac.uk
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
How Parents Understand Their Daughters Behaviour Before They Receive a Diagnosis
of an Autism Spectrum ConditionNatalie Kseib
Submitted for the Degree of
Doctor of Psychology(Clinical Psychology)
School of PsychologyFaculty of Health and Medical Sciences
University of SurreyGuildford, SurreyUnited KingdomSeptember 2018
© Natalie Kseib 2018
1
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Abstract
Introduction: Prevalence studies show that fewer girls are diagnosed with Autism Spectrum
Conditions (ASCs) than boys. This difference is particularly marked where there is no
cognitive impairment. Some suggest that ASCs present differently between males and
females, perhaps leading to delayed diagnosis in girls. A review of the literature exploring
sex/gender differences found that many studies have measured the severity of ASC symptoms
rather than the quality of difference. Limited research has considered the perspectives of
parents on the signs noticed in their daughters and the context in which difference is noticed.
Objective: This study sought to explore how parents make sense of their daughters’
behaviours and the processes by which behaviours are perceived as requiring intervention or
diagnosis. Participants: Five parents whose daughters (aged 9-12 years) had recently
received a diagnosis of an Autism Spectrum Condition without cognitive impairment were
invited to tell their stories of diagnosis. Design: Transcripts were analysed using a narrative
approach, focusing on how stories were told. Findings: Narrative themes were identified
across transcripts in relation to the process by which behaviours are made sense of. Themes
included: daughters only showing their ‘real self’ in safety; their distress peaking; parents
questioning normality; and parents feeling blamed and unheard. Conclusions: The findings
are discussed in relation to existing research and theory. Implications are discussed in relation
to education and health services and UK policies. Further research into parents’ experience of
judgement in relation to their child’s behaviour, and exploration of interventions for masking
in girls is needed.
2
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Acknowledgements
I would like to thank all of the tutors and staff on the course team for inspiring and supporting
me through the stressful but enriching experience of clinical training. Specifically, I want to
express my gratitude to my research supervisors, Dr Kate Gleeson and Dr Emma Williams
for their guidance, expertise and emotional support. I also wish to thank my clinical tutors, Dr
Eli Joubert, Dr Gemma Perman and Dr Zoe Clyde and all my placement supervisors
throughout my clinical placements, for helping me to develop my skills and challenge me to
reflect and continually learn more about myself.
I have had many challenging, enriching, stressful and happy experiences throughout training.
Thank you to everyone who has been part of the journey with me; to my past work colleagues
and fellow trainees.
Thank you finally to my wonderful friends and family; for being patient with me and
supporting me through the challenging times. Now this is in we can get celebrating!
3
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Contents
Part 1: Major Research Project Empirical Paper
Abstract
Introduction
Method
Results
Discussion
References
Empirical Paper Appendices
5
6
7
16
21
37
48
60
Part 2: Major Research Project Literature Review
Abstract
Introduction
Methods
Results
Discussion
References
Literature Review Appendix
113
115
116
121
137
151
160
173
Part 3: Summary of Clinical Experience 180
Part 4: Table of Assessments 183
4
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Part 1Major Research Project Empirical Paper
How Parents Understand Their Daughters Behaviour Before They Receive a Diagnosis of an Autism Spectrum Condition
Word Count: 9998
5
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Abstract
Introduction: Prevalence studies show that fewer girls are diagnosed with Autism Spectrum
Conditions (ASCs) than boys. This difference is particularly marked where there is no
cognitive impairment. Some suggest that ASCs present differently between males and
females, perhaps leading to delayed diagnosis in girls. A review of the literature exploring
sex/gender differences found that many studies have measured the severity of ASC symptoms
rather than the quality of difference. Limited research has considered the perspectives of
parents on the signs noticed in their daughters and the context in which difference is noticed.
Objective: This study sought to explore how parents make sense of their daughters’
behaviours and the processes by which behaviours are perceived as requiring intervention or
diagnosis. Participants: Five parents whose daughters (aged 9-12 years) had recently
received a diagnosis of an Autism Spectrum Condition without cognitive impairment were
invited to tell their stories of diagnosis. Design: Transcripts were analysed using a narrative
approach, focusing on how stories were told. Findings: Narrative themes were identified
across transcripts in relation to the process by which behaviours are made sense of. Themes
included: daughters only showing their ‘real self’ in safety; their distress peaking; parents
questioning normality; and parents feeling blamed and unheard. Conclusions: The findings
are discussed in relation to existing research and theory. Implications are discussed in relation
to education and health services and UK policies. Further research into parents’ experience of
judgement in relation to their child’s behaviour, and exploration of interventions for masking
in girls is needed.
Key Words: Autism, Diagnosis, Females, Gender, Girls, High Functioning
6
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Overview
A review of the literature showed that children and adolescents with a diagnosis of an
Autism Spectrum Condition (ASC)1 may show different signs and symptoms of the disorder
according to their sex/gender2. However, there is a lack of research that investigates the
context in which signs and symptoms of ASCs are noticed. An exploratory study was deemed
necessary in understanding this. This research aimed to analyse the stories of parents with
daughters diagnosed as having an ASC to explore how behaviours are made sense of before
diagnosis. In keeping with a narrative approach, I3 will firstly outline my influences for
conducting the research before summarising the literature demonstrating the rationale for the
study.
Influences for this Research
Personal significance
My interest in this research is informed by my curiosity about why people seek to
define difference given the often, negative connotations associated with it. I have observed, in
both my personal life and clinical work, the powerful impact that diagnosis can have on our
understandings of ourselves and others. This has sparked an interest in considering how our
1 In order to avoid implying a ‘disordered’ person (Baron-Cohen, Scott, Allison, Williams, Bolton et al., 2009) and to encourage less stigmatising terminology I will use the term Autism Spectrum Condition (ASC), rather than Autism Spectrum Disorder (ASD) throughout this paper. Where the term “autism” is used, this refers to the diagnostic label.2 In this paper “sex” refers to “the biological and physiological characteristics that define men and women,” whilst “gender” refers to “the socially constructed roles, behaviours, activities, and attributes that a given society considers appropriate for men and women.” (definitions adopted from the World Health Organization, 2015). However, because gendered socialization begins at birth, it is difficult to separate the effect of sex and gender. For this reason, unless “sex” or “gender” is specifically used as defined above, the term “sex/gender” will be used to acknowledge the inevitable overlap between them (Springer, Mager Stellman & Jordan-Young, 2012).3 ‘Honesty and transparency’ are regarded as important components of good quality qualitative research (Tracy, 2010). I have therefore chosen to narrate this thesis in both the first and third person to be open about my reflections.
7
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
stories shape our perceptions. Reflection on my own assumptions and values has been an
integral part of the research process.
Social significance
ASC diagnosis is complex and parents often experience difficulties and frustration
during the process. Additionally, parents of children with ASC are known to experience more
stress than parents of children with any other condition, perhaps due to challenges in social
relatedness and the parent–child relationship (Davis and Carter, 2008). In children without
Intellectual Disability, autism is believed to be mis- or under- diagnosed in girls in
comparison to boys (Giarelli, Wiggins, Rice, Levy, Kirby et al., 2010; Gillberg, 1993; Kim,
Leventhal, Koh, Fombonne, Laska et al., 2011; Mattila, Kielinen, Linna, Jussila, Ebeling et
al., 2011). By developing an improved understanding of the context of diagnosis for this
population, we could better support families by intervening earlier.
Understanding Autism Taking a Social Constructivist Approach
ASCs are predominantly understood within the medical model, and usually defined as
neurodevelopmental disorders. Medical and scientific literatures explicitly and implicitly
reflect this, representing autism as ontological, or a ‘truth’ that can be discovered (Timimi,
Gardner & McCabe, 2011). There is ongoing debate about what this ‘truth’ is. Autism is
usually assumed to be associated with genetic, neurological, biological or chemical
abnormality (Molloy & Vasil 2002; National Institute for Health and Care Excellence
[NICE], 2011) but the mechanism of causation remains unknown and to date, no specific
genes linked to ASC have been identified (NICE, 2011). The National Autistic Society states
that ‘Autism is a developmental condition affecting the way the brain processes information’
8
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
(National Autistic Society, 2016), representing ‘Autism’ as an agent that directly causes
neurological impairment.
Recently there has been some discussion about how autism can be regarded as a
‘social construct’, taking into account the social conditions in which ASCs first became and
are now labelled and recognised (Nadesan, 2013). These understandings do not necessitate
that there is no biogenic or psychogenic basis to ASC. Rather, they observe autism as a
diagnostic category that is shaped within a socio-cultural context of ‘normalness’ (Biklen,
2005; Molloy & Vasil 2002; Smukler, 2005; Timimi, 2004). That is, autism is understood as
a nominal category for grouping a greatly diverse group of people who share communication
practices that are significantly different from what is considered ‘normal’. In this way
society’s perceptions of normalcy are accounted for in the understanding of when and why
the diagnosis is given, and the impact of the diagnosis on both individuals who receive the
diagnosis and their networks. The theoretical understanding adopted in social constructivism
acknowledges the cultural and philosophical values and ideals that diagnosis is rooted in. It
also helps to explain the difficulty in defining autism, as it parallels the difficulty in defining
what is and is not ‘normal’ and critically considers the practice of formalising the label of
‘abnormal’ (Biklen, 2005; Nadesan, 2013; Smukler, 2005). This is important to consider in
the context of ASC research which predominantly implicitly assumes Autism as ontological.
The way in which this stance has impacted on the ASC literature and the relevance for
diagnosis between the sexes/genders is discussed in the following sections.
Diagnosing ASC: Relevance for Research
Diagnostic criteria define and characterise ASCs by two core features: impairment in
social communication and interaction and restricted/repetitive patterns of behaviour, interest
or activity (APA, 2013). Autism is defined as a ‘spectrum condition’ because the severity and
9
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
presentation of these symptoms show an extreme degree of variation. Symptoms of autism
are said to be present in early childhood and continue throughout the lifespan. In the first two
years of life, social deficits used to diagnose ASCs include a lack of joint attention, failure to
show interest towards others, lack of shared play and not responding when called (Ozonoff,
Williams, & Landa, 2005). In addition, children commonly present with a range of additional
symptoms, including sleep disorders, gastro-intestinal problems and anxiety and depression
(Mazzone & Vitiello, 2016).
The lack of a definitive cause, or marker for autism makes ASC diagnosis difficult.
Assessment relies on many sources of information and the diagnostic process includes
measures of parental report, child observation and interaction, and the use of clinical
judgment (Filipek, Accardo, Baranek, Cook, Dawson et al., 1999). Best practice measures
used include the Autism Diagnostic Interview‐Revised (ADI‐R; Lord, Rutter, & Le Couteur,
1994), a semi-structured interview conducted with parents and observational measures such
as the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord, Luyster,
Gotham & Guthrie, 2012). This and other ‘gold standard’ instruments depend on subjective
observations or experiences of caregivers and/or self and clinician observation and
assessment. Therefore, parent’s and professional’s experiences of ‘normal’ are inherent
within decisions, and are in turn likely influenced by cultural context. The predominance of
research investigating differences in autism presentation between girls and boys has mostly
overlooked this context (Kseib, 2018).
Prevalence of Autism Between the Sexes/Genders
Prevalence studies show that ASC without coexisting cognitive impairment (high
functioning ASC; HFASC) are diagnosed more commonly in males than females, with the
male:female ratio reported ranging from 6:1 to 16:1 (Baird, Simonoff, Pickles, Chandler,
10
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Loucas, et al., 2006; Fombonne 1999, 2002, 2003; Scott, Baron-Cohen, Bolton & Brayne,
2002; Volkmar, Szatmari, & Sparrow, 1993). Moreover, evidence suggests that females who
are diagnosed with HFASC are diagnosed significantly later than males with the same
diagnosis (Begeer, Mandell, Wijnker-Holmes, Venderbosch, Rem et al., 2013; Goin-Kochel,
Mackintosh, & Myers, 2006; Shattuck, Durkin, Maenner, Newschaffer, Mandell et al., 2009).
Studies also suggest that the age of first concern for individuals with HFASCs is significantly
later for females than for males, and that girls are brought to clinic later than boys (Begeer et
al., 2013; Rynkiewicz & Łucka, 2015).
There is a suggestion that such sex/gender discrepancies could be the result of
misdiagnosis and/or under-reporting by caregivers and parents (Giarelli et al., 2010; Gillberg,
1993; Kim et al., 2011; Mattila et al., 2011). It has been hypothesised that this results from a
difference in the way autism is expressed, or distinctive ‘phenotypes’ between sex/genders
(Rivet & Matson, 2011). A review of the literature was conducted to explore research on how
the differences in expression of HFASC between girls and boys is understood to date (Kseib,
2018).
ASC Presentation Differences Between the Sex/Genders
Existing evidence suggests that there are both similarities and differences between
males and females in symptoms on diagnostic measures; generally, no differences have been
found in overall scores on social communication (Frazier, Georgiades, Bishop & Hardan,
2014; Holtmann, Bölte & Poustka, 2007; Kumazaki, Muramatsu, Kosaka, Fujisawa, Iwata et
al., 2015; May, Cornish & Rinehart, 2014; Solomon, Miller, Taylor, Hinshaw & Carter,
2012; Supekar & Menon, 2015), but there were indications of difference between the
sexes/genders in subscales (Hiller, Young & Weber, 2014; May, Cornish & Rinehart, 2016).
Mostly, females with HFASC showed less severe Repetitive and Restricted Behaviours and
11
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Interests (RRBIs) compared to males (Frazier et al., 2014; Hiller et al., 2014; May et al.,
2016; Solomon et al., 2012; Supekar & Menon 2015; Wang, Deng, You, Chen, Li, et al.,
2017), and this pattern was found in typically developing (TD) populations too (May et al.,
2016). However, few studies measured the quality of impairments as opposed to the severity
of impairments.
One difficulty with the current research is that most studies investigated differences
by comparing male and female HFASC presentations using already established diagnostic
measures. These measures may have low validity in detecting the ‘female phenotype’ of ASC
and therefore may not be sensitive to possible differences between the males and females
(Rivet & Matson, 2011). Kopp and Gillberg (2011) suggest that diagnostic tools are moulded
around the male phenotype identified by Kanner (1943) and Asperger (1944), and thus lack a
sensitivity towards the subtle symptoms of autism that females may display (Yaull-Smith,
2008). Their revised screening tool (Autism Spectrum Screening Questionnaire; Ehlers,
Gillberg & Wing, 1999) showed that endorsement of certain items varied according to
sex/gender highlighting the deficient sensitivity of traditional measures for girls which are not
likely to detect more subtle differences. Additionally, it is likely that ASC female participants
used in current research fit the ‘male’ ASC profile and were diagnosed for this reason.
Furthermore, the measures rely on scores that are rated by clinicians and parents. By
comparing scores, most studies assume that ratings represent an objective record of observed
symptoms. However, where studies used other designs, consideration of contextual
information about perceptions of ‘symptoms’ was valuable in highlighting why signs of
autism may be more or less apparent and/or perceptible by others, according to the child’s
gender. For example, using observational data from a school playground, one qualitative
study reported that the way in which TD boys and girls play in contrast to HFASC boys and
girls may mean that social exclusion may be more obvious and observable by others for boys
12
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
in comparison to girls with HFASC (Dean Harwood & Kasari, 2017); girls with ASC tended
to stay in close proximity to social groups, perhaps masking social challenges from
onlookers. TD boys’ play tended to be structured making it easier to spot ASC boys, who
were often wandering alone apart from the game. This and other similar studies (Dean,
Kasari, Shih, Frankel, Whitney et al., 2014; Rynkiewicz, Schuller, Marchi, Piana, Camurri, et
al., 2016) highlight the lack of objectivity of diagnostic ratings that some studies assume.
They additionally show the value of qualitative studies in understanding why girls may not be
perceived as struggling in certain situations, or by certain people.
Many studies in the review used TD children as controls, and some found differences
between the sex/genders on ASC measures in TD populations. If we consider autism as a
deviation from ‘normal’ typical sex/gender differences should be accounted for. Faherty
(2006) highlights the significance of gendered expectations by suggesting that society expects
young girls to become engrossed in hobbies whilst rejecting more rigid interests in boys,
priming the autism ‘spotlight’ to land on boys rather than girls. Research suggests that the
saliency of symptoms is culturally shaped; Daley (2004) found that in India, qualities of
quietness, withheld emotion and keeping to oneself are interpreted as ‘good’ by parents, as it
means their children are ‘trouble-free’. Additionally, evidence suggests that we make
assumptions automatically and unconsciously, evaluating ourselves and others according to
cultural perceptions and stereotypes (Chatard, Guimond & Selimbegovic 2007). Therefore, a
purely biological understanding of proposed sex/gender differences is limited as it fails to
account for social constructions at play in our perceptions of ourselves and others.
In summary, it may be that, for females, some autistic symptoms are not noticed due
to a context which masks difficulties (Dean et al., 2017), or because they are seen as socially
acceptable in females. It is also likely, that we unconsciously account for gender expectations
and differences seen in neuro-typical populations, when we observe children. Diagnostic
13
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
ratings have been taken and used as observable and objective ‘truths’ in the research. This
emphasis on comparing males and females’ diagnostic scores means there is a need to
explore in depth the quality of how others perceive and make sense of children and
adolescent’s behaviours and expressed feelings before ASC diagnosis. Due to evidence that
girls are brought to clinic for assessment later than boys (Rynkiewicz & Łucka, 2015) and
that parents are usually the first people to start suspecting that a child has autism (Sicherman,
Loewenstein, Tavassoli & Buxbaum, 2018), a study that explores parent’s perceptions of
their daughters with HFASC is relevant.
Aim and Research Questions
To date, research measuring the severity of symptoms has dominated the literature in
an attempt to understand how males and females with HFASC differ in their presentation. As
yet, an understanding of how HFASC girl’s behaviours are made sense of by their parents,
and the role this plays in gaining diagnosis has not been established. In line with this, the aim
of the study presented is to explore parent’s personal narratives of their daughter’s diagnosis
in order to further our understanding of why HFASC girls are brought to clinic and diagnosed
later than HFASC boys. The following research questions will be addressed:
1) How do parents make sense of their daughters’ behaviours before diagnosis of an
Autism Spectrum Condition?
2) How do the daughters’ behaviours come to be perceived as being unusual or
requiring of diagnosis? And related to this;
3) Why is diagnosis sought at particular points in time?
In answering these questions, it is hoped that a contribution can be made to better
understanding parental decision making within their social context. In turn, this knowledge
might help professionals to know how to better support parents who notice ‘difference’ or
14
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
feel they need help. Overall, the study endeavours to contribute to the gap in research that
considers the role that parents play in perceiving their child’s behaviour as unusual or
requiring diagnosis and thus precipitating an eventual diagnosis. It is hoped that undertaking
a narrative analysis will allow for a more nuanced, culturally contextualised understanding
around the observed ‘signs’ of autism for girls.
Choice of Research Methodology
Qualitative methodology seeks to enhance understandings of the meanings individuals
bring to events and processes within their lives, and how their perceptions are shaped by the
social world around them (Miles & Huberman, 1994). Due to a gap in understanding of the
social and cultural landscape in which diagnosis is made, qualitative methodology was
identified as the most suitable way to explore the research questions.
The narrative approach is underpinned by the assumption that people organise life
events as stories and is concerned with understanding how events, values, past experiences
and future possibilities are made sense of and contribute to the way people view and
experience the world (Riley, Hawe & Shiell, 2005). A narrative analysis was selected because
this allowed for consideration of how participant stories were likely to have been influenced
by the context, which fits well with the focus of the research questions. Narrative analysis
assumes that story-telling serves a purpose in giving meaning to experiences within a broader
context of other stories and situations (Murray, 2003; Riessman, 2008). Therefore,
consideration is given to how a person’s story is influenced by those of other people, as well
as by broader narratives such as those about ability, gender and age. Again, this is relevant as
the research questions seek to enhance understanding of parents’ sense making in relation to
broader narratives such as those about gendered behaviour. The narrative frame is also
explicit in its recognition of co-construction between the narrator and researcher during the
15
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
story-telling and interpretation (Riessman, 2008) making it possible to consider my own
experience and interactions in the context of participants’ stories (Plummer, 2001).
Methods
Participants and Recruitment
Participants were recruited from ASC support groups on a social media website using
an online advert (Appendix B). Appendix C outlines detail on the recruitment process.
Inclusion Criteria:
Parent or primary caregiver of a girl with ASC (or equivalent)
ASC diagnosis was made within a year of recruitment
Parents/caregivers were able and willing to be interviewed
Daughter between the age of 8 and 18 years of age on date of diagnosis
Exclusion Criteria:
Daughter had a diagnosis of a learning or intellectual disability or signs of cognitive
impairment.
Children who had received a separate mental health diagnosis were included in the study
given that co-morbid difficulties are common.
Recruitment took place over a six-month period (July-December 2017); 54 parents
expressed interest. ASC diagnosis and other inclusion/exclusion criteria were then verified by
parental report over email. The exclusion criterion was checked by asking parents about any
known learning disability and their daughter’s place of education (i.e. mainstream or other).
Nine parents met the inclusion and exclusion criteria used for recruitment and were sent
further information (Appendix D). Five parents responded to this email confirming suitability
16
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
for the study and agreed to take part. The parents were then invited to meet for an interview
with the researcher either at the University of Surrey, a private community function room, or
participants’ homes. Due to distance, one of the participants was also given the option of
having their interview over Zoom, an online platform. Four interviews were held in
participant’s homes (one of which was held over Zoom) and one was held in a community
function room. Informed consent was obtained from all the five individual participants
included in the study (Appendix E).
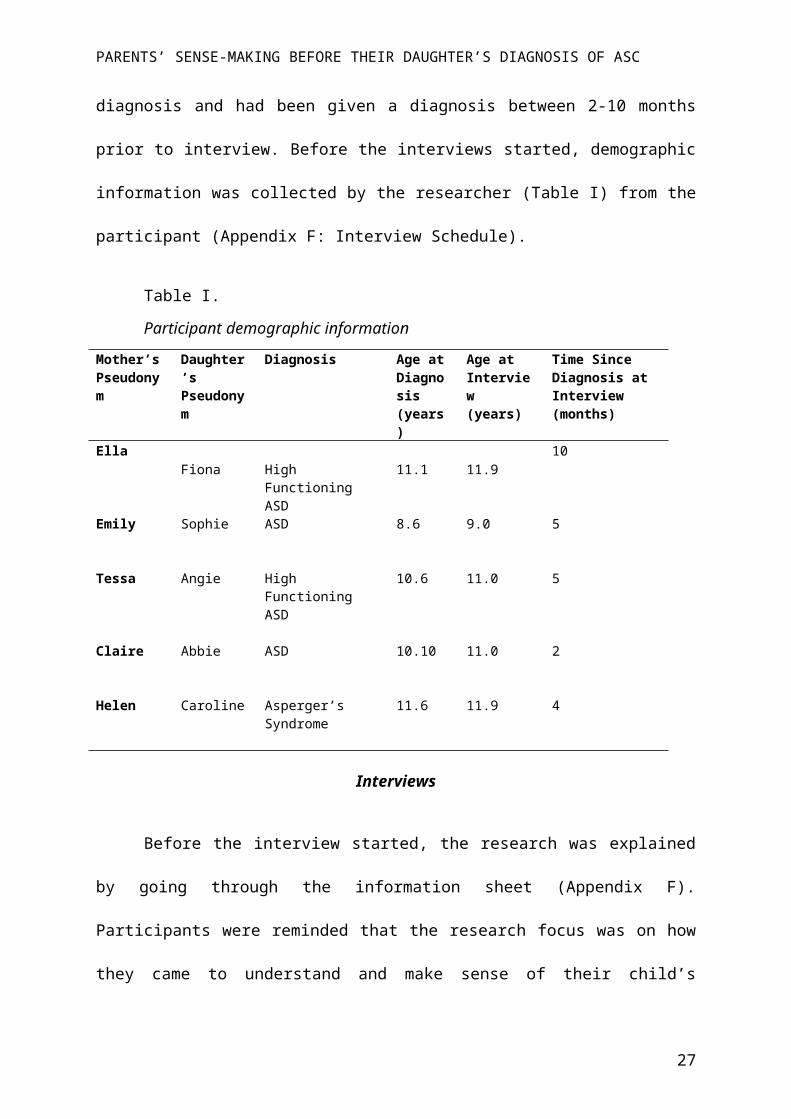
All participants were biological mothers of the child with autism. The children were
aged between 8.8–11.6 years at diagnosis and had been given a diagnosis between 2-10
months prior to interview. Before the interviews started, demographic information was
collected by the researcher (Table I) from the participant (Appendix F: Interview Schedule).
Table I.
Participant demographic information
Mother’s Pseudonym
Daughter’s Pseudonym
Diagnosis Age at Diagnosis (years)
Age at Interview (years)
Time Since Diagnosis at Interview (months)
EllaFiona High Functioning
ASD11.1 11.9
10
Emily Sophie ASD 8.6 9.0 5
Tessa Angie High Functioning ASD
10.6 11.0 5
Claire Abbie ASD 10.10 11.0 2
Helen Caroline Asperger’s Syndrome 11.6 11.9 4
Interviews
Before the interview started, the research was explained by going through the
information sheet (Appendix F). Participants were reminded that the research focus was on
17
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
how they came to understand and make sense of their child’s behaviours before diagnosis. An
interview schedule was created in order to encourage the detail of the story to be told, rather
than a question and answer approach (Riessman, 2008). The interview consisted of one main
question, which invited participants to ‘tell their story’, and additional prompt questions for
exploring areas of interest (Appendix F). I focused on actively listening in order to encourage
the process using verbal and non-verbal prompts, whilst reflecting on how my presence was
leading to a joint construction of the narrative (Crossley, 2000). Interviews lasted between
41-104 minutes (average 76 minutes) and each was digitally recorded and transcribed
verbatim. I reflected on my experience of each interview in a journal.
Analytic Procedure
I chose to use a structured process (Crossley, 2000) for analysis to allow for
transparency in the process (Tracy, 2010).
Step 1: Reading and familiarising
I transcribed the first two interviews but due to time limits had the following three
professionally transcribed. To capture the stories, it was considered sufficient to transcribe at
the level of the words and conversational characters (e.g. laughter). I familiarised myself
with the data by listening to the recordings and re-reading the transcripts multiple times in
order to get an overview of the content and structure. I began to code and make notes in
relation to general themes, patterns and language.
Step 2: Identifying narrative tone
Narrative tone is the manner in which a story is told. The plot of a narrative takes a
certain shape, which gives it a certain ‘emotional flavour’ (Murray, 2003). This also conveys
18
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
something to the audience about how they should interpret it (Andrews, Squire, Tamboukou,
1995). The shape or genre the narrative takes may be identifiable, for example as a romance,
tragedy or satire. I attended to the manner in which narratives were told to make sense of
events and assigned each narrative a genre. I also began creating summaries of each narrative.
Step 3: Identifying imagery and themes
I looked for and considered themes (summaries of the fundamental points) and images
(visual images evoked in the listener) across each narrative and how these changed as the
narrative progressed.
Step 4: Weaving a coherent story
I put each narrative back into a coherent story similar to creating a biography of the
participant’s story, remaining close to the data by using quotes.
Step 5: Cross-analysis
This involved looking for commonalities and differences across narratives by
synthesising salient themes and building a framework to summarise all narratives.
Epistemology
I took a social constructivism (relativist) position which broadly asserts that an
objective truth cannot be discovered, and that our language constructs versions of our reality
within social contexts (Willig, 2012). This contrasts a realist position which assumes
‘external reality’ and ‘truths’ that ‘exist’ and can be discovered (Harper, 2012). This stance
shares with narrative psychology an emphasis on language as a tool for forming identity
(Gergen, 1985). I believe that our interpretations of what is and is not autism are embedded in
socially constructed standards of what is and is not ‘normal’. These are rooted in cultural
values and practices, thereby contributing to the production and transformation of people
19
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
labelled with the disorder. By taking this stance I hope to build a more culturally
contextualised understanding of autism and give a voice to people that are not usually
considered ‘expert’ in their knowledge.
With regard to gender and sex, I take the position that the constructs of ‘male’ and
female’ are not solely reflections of naturally occurring differences in human beings but
bound up with the normative prescriptions of masculinity and femininity in culture (Burr,
2003 p.3). I believe that people experience and interpret other people’s behaviours in unique
ways, informed by their personal and social context and available social discourses.
Credibility
Allowing for consideration that narratives cannot be treated as an exact record or an
unveiled objective reality, to ensure credibility I observed Yardley’s (2000) principles of
quality qualitative research. Details about how these were observed can be found in Appendix
G.
Ethical Considerations
Ethical approval was sought and granted from the University of Surrey Faculty of
Health and Medical Sciences Ethics Committee (Appendix H). Potential participants were
sent an information sheet with no obligation to participate. Participants also went through this
with the researcher and were provided a space to ask questions to ensure consent was
informed. The main research question was open ended so participants could choose what
parts of their story they would like to tell, and were told that they could choose not to answer
any prompt questions. Participants could withdraw during the interview or any time up until
two weeks after the interview. Interviews were conducted in community locations that
permitted privacy and confidentiality. Recordings were stored on an encrypted device and
20
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
deleted following transcription. Participants were assigned pseudonyms and identifying
information was amended from transcripts to preserve anonymity. Additionally, only brief
examples of transcripts will be included in this report rather than full narratives.
Results
Overview
This section begins with summaries of the narratives; these are abridged versions free
from interpretation and keeping as close to the participant’s language as possible. Tone,
narrative impression, and key themes are presented providing a context for each participant in
which interpretations can be situated (Riessman, 2008). Extensive individual analyses cannot
be presented due to space limitations, however detailed examples can be found in the
appendix.
My interpretations of similarities and differences in genre and narrative technique are
then outlined. Following this I present themes that emerged from a narrative-thematic
analysis in relation to sense making in the diagnosis of autism. The analytic process sought to
notice patterns of beliefs or experience within the context of individual narratives, rather than
attempting to unearth a universal process or experience.
Narrative Introductions
Ella’s story about Fiona
21
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Ella described Fiona as a ‘really difficult baby’ who cried a lot and never slept ‘from
day one’. As Ella’s first baby, she did not know ‘what’s normal and what’s not’.
Academically, Fiona had ‘always been extremely clever’ whilst school said that ‘socially
she’s slightly below [her peers]’. At around the age of six or seven, Ella described that Fiona
had ‘anxiety around everything’. After Child and Adolescent Mental Health Services
(CAMHS) rejected a referral, Ella and Fiona ‘ended up going to see a private psychologist’.
Around the same time, Ella ‘mentioned the word meltdown’ on a Facebook group for parents
who have ‘children who are academically ahead’. A parent asked whether Ella’s daughter had
autism and sent her a link ‘to something around girls with autism’. Receiving this, Ella
remembers thinking ‘don’t be silly’, but then ‘started doing research on signs and symptoms
in girls’ and ‘found this checklist’. Ella said ‘it was just like somebody had written everything
about Fiona on there’ and that it was ‘uncannily scary’. The Clinical Psychologist seeing
Fiona ‘did not know’ if Fiona had autism, and wrote to Fiona’s GP recommending specialist
assessment. ‘CAMHS rejected it’ and recommended a ‘six-week anxiety management group’
for both Ella and Fiona whilst they waited to see a paediatrician. Before the group began, Ella
‘mentioned autism’ to the professionals and when the group ended Ella said that she was still
concerned about Fiona’s ‘negative thoughts’. They said that Fiona is ‘not autistic and if she’s
behaving this way still after having all these sessions you need to look at how you’re enabling
her behaviour’. Ella ‘stormed out’ feeling blamed and frustrated to be ‘told that it’s your
fault’. In the two year wait for diagnosis which Ella ‘put on the backburner’ Fiona’s ‘mental
health went downhill’ and she ‘started talking about wanting to kill herself’. She was
diagnosed with OCD following an emergency appointment with CAMHS. Fiona’s therapist
did not think she was autistic but advised they attend the assessment so that Ella could ‘cross
that off the list of the things that are wrong with her’. Fiona’s teachers also tried to reassure
Ella that ‘everything’s fine’. However, after ‘about six appointments’ and ‘almost two years
22
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
[from referral]’ Fiona was diagnosed with high functioning ASD in January 2017 at the age
of 11 years.
The tone of Ella’s story was thorough, matter of fact and methodical, taking the
listener through the journey in an ordered style, using ‘the checklist’ to describe the ‘signs
noticed’. A core theme of Ella’s story was ‘feeling blamed’ by professionals followed by a
shift in power to ‘becoming expert’.
Emily’s story about Sophie
Emily ‘always knew that something was different’ about Sophie. Sophie was ‘really
bright’, ‘talking in sentences by eighteen months’. She was ‘really chatty and really friendly’
and ‘seemed to get on well with adults’ but ‘less so with children’. Emily had a favourite toy
which ‘had to go everywhere’ and a favourite number. With hindsight, Emily perceives ‘all
these little things’ as ‘glaringly obvious [signs of autism]’. At the time, Emily thought these
were ‘weird quirks’ or ‘down to the hypermobility’. Each school year, Sophie had ‘difficulty
transitioning to the next year group’. In her first term of year two, when she was six, she
came home saying ‘I wish I was dead’. Emily went in to see the teacher and also went on a
‘hypermobility Facebook page’ asking ‘what this might mean’. On there, someone sent Emily
a web-link to Tania Marshall’s, Asperger’s Syndrome in Bright Young Girls. Emily described
disbelief and a ‘lightbulb moment’ because Sophie ‘ticked thirty out of forty’ traits listed.
Emily expressed concern to the GP about Sophie’s distress and her thoughts that ‘it might be
autism’. Whilst waiting for assessment, Emily went to a ‘support group’ and ‘went on a
course to help [Sophie]’. In this time Sophie’s school ‘denied that there were any issues’
saying, ‘there’s nothing wrong with her, she’s absolutely fine’. At 8 years-old, ‘nearly two
years’ after first referral, Sophie was diagnosed with ASD.
23
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
The tone of Emily’s story was dramatic and emotional as Emily recounted her
daughter’s distress. Her story conveyed frustration and anger towards Sophie’s school for
‘not believing her’. The tone became more positive when Sophie received a diagnosis which
she felt ‘explains everything’.
Tessa’s story about Angie
Tessa described Angie as an ‘awful baby’ that ‘didn’t sleep’ and ‘wouldn't even at
five weeks old, let anyone else hold her’ because ‘she'd scream and scream and scream’.
Angie was ‘early talking’ and ‘learn[ed] quickly apart from colours’. Watching a television
programme, Born Naughty on which a girl was diagnosed with Autism, Tessa recognised
‘one tiny thing’ [looking out the corner of her eye] that Angie did. Tessa started to research
autism and ‘it all clicked into place’. Five months later Tessa ‘plucked up to the courage’ to
say to a teacher, "I think there's something there"’. Tessa worried that school wouldn’t
‘believe’ her because ‘they don’t see what I see’. However, Angie’s teacher was
‘understanding’ and ‘got the Ed Psych [Educational Psychologist] to see her’. The contrast
between Tessa’s ‘report’ and the school’s ‘perfect pupil’ report ‘raised alarm bells’ for the
psychologist, who ‘made a referral’ for specialist assessment. After ‘nearly two years’ Angie
was diagnosed with High Functioning ASD, in a ‘twenty-minute’ appointment, at the age of
ten years.
The tone of the narrative was upbeat and comical. Many anecdotes from Angie’s life
were given but there were not many explicit links made with autism. The theme of Angie
needing safety to show her ‘real self’ stood out. Other core themes noted were, Angie as
inherently ‘good’ but ‘needing control’ and Angie ‘needing to understand’. The age of eight
was significant in enabling difficulties to be seen, due to increasing complexity of social
24
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
rules. Tessa also talked about the significance of Angie being her first child, in not suspecting
autism.
Claire’s story about Abbie
Abbie is Claire’s youngest child of four. Abbie’s brother Ed also has a diagnosis of
ASD. When Abbie was eight her teachers ‘were having problems with her behaviour’ and
‘wondered if she was bipolar’. Claire went to the doctor who thought Abbie was
‘overthinking things’ and referred her to a clinical psychologist. In the initial meeting, the
clinical psychologist asked whether Claire had ‘considered was she autistic? And then put her
on the autism pathway’. Claire reflected that she thought she would have been ‘more aware’
but that Abbie is ‘very different to how Ed is’. For Claire, meltdowns were ‘just a way of life’
and she had got ‘used to it’. She described Abbie as ‘difficult at school’ for example, trying
to run away. Eighteen months after being put on the ‘pathway’, Claire was diagnosed with
ASD at the age of 10-years-old.
Claire’s narrative was matter of fact in tone, injected with dry humour. Claire was
relatively passive before diagnosis. Like Tessa, anecdotes were given without explicit links
made to autism. The core themes in Claire’s narrative included: difference in son and
daughter’s presentation of autism; autism offering a useful alternative explanation to
naughtiness and; others seeing behaviours as problematic where Claire did not.
Helen’s story about Caroline
Helen has two children, ‘a boy and a girl’, both ‘on the spectrum’ and ‘really, really
different’ [from one another]. Helen described her older child John as ‘demanding’, having
‘challenging behaviour’ and ‘needing attention’ in comparison to Caroline as ‘extremely
calm, very friendly, very sociable, very outgoing’ and ‘much more loving and considerate’.
25
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
In reception class Caroline’s teacher, who had also taught John ‘took [Helen] aside’ and said
‘"Look, the brother was always obsessive about reading but this girl is obsessive about
drawing"’. Although she assured Helen that ‘it doesn't necessarily say that she is on the
spectrum’ it made Helen ‘watch things more’. Helen’s view of Caroline constantly changed;
‘one moment, you look at them and you'll see something what you think is spectrum, then the
next minute you see stuff that is completely not’. Because it had taken a long time for John to
‘go through the system’, Helen remembers thinking, even though it’s ‘little things’, ‘"I've got
to start her now or she won't get seen in time"’. Helen also went to support groups and learnt
about girls ‘on the spectrum’ and ‘started to really wonder because [Caroline] was starting to
have more and more problems at school’. Although Caroline was getting ‘support’ from
school, Helen asked school for a formal autism assessment. ‘Funding problems’ meant that
this was not possible, and Caroline’s father was also reluctant for Caroline to be assessed so
an ‘implant CAMHS worker’ helped to facilitate conversations about ‘whether Caroline
should be referred further’. Caroline’s parents reached agreement ‘that she could be seen’.
After sending ‘the paperwork off’, ‘they knocked it back completely’. A referral through the
GP also ‘got completely knocked back’. Helen was frustrated because the tests ‘are totally
geared to boys’ and felt that they had not ‘brought out her difficulties properly’. The ‘worker’
asked again for Caroline to be seen and suddenly, they were ‘seen within a week’. Caroline
was diagnosed with Asperger’s Syndrome at this appointment, when she was 11-years-old.
Helen’s narrative was detailed and descriptive with use of visual imagery creating a
cinematic feel. Though emotions were talked about, this was done with disconnection. The
tone of Helen’s narrative was one of empowerment through the expertise of having a child
with autism.
Cross Analysis: How Were Stories Told?
26
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
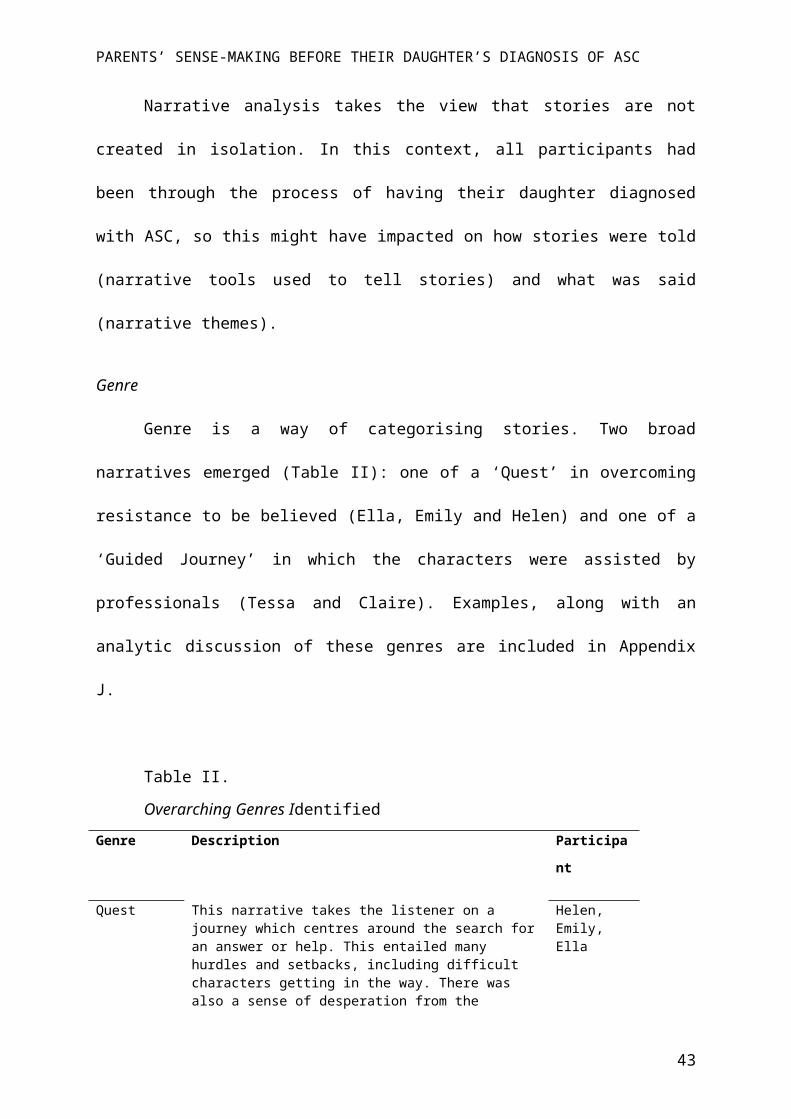
Narrative analysis takes the view that stories are not created in isolation. In this
context, all participants had been through the process of having their daughter diagnosed with
ASC, so this might have impacted on how stories were told (narrative tools used to tell
stories) and what was said (narrative themes).
Genre
Genre is a way of categorising stories. Two broad narratives emerged (Table II): one
of a ‘Quest’ in overcoming resistance to be believed (Ella, Emily and Helen) and one of a
‘Guided Journey’ in which the characters were assisted by professionals (Tessa and Claire).
Examples, along with an analytic discussion of these genres are included in Appendix J.
Table II.
Overarching Genres Identified
Genre Description Participant
Quest This narrative takes the listener on a journey which centres around the search for an answer or help. This entailed many hurdles and setbacks, including difficult characters getting in the way. There was also a sense of desperation from the parent. These narratives contained an important moment of insight that lead to a dramatic transformation in understanding of their child. These stories ended triumphantly with victory in diagnosis.
Helen, Emily, Ella
Guided Journey
These narratives were observational and used humour to enhance descriptions of difference from the norm. Although characters were helped in their journey towards diagnosis, dry humour was used to convey that others did not understand the whole ‘truth’ about their daughter and/or events, in this way placing knowledge more with parents than professionals.
Tessa, Claire
How is Autism Made Sense Of? Themes Across Narratives
In exploring the sense making process, superordinate themes of ‘Journey Towards
Diagnosis’ and ‘After Diagnosis’ emerged. Table III shows these and main emergent themes.
Due to limited space only the first superordinate theme, and related sub-themes will be
27
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
presented as these directly address the research questions. The ‘After Diagnosis’ sub-themes
are presented in an extended analysis (Appendix L).
Table III.
Superordinate and Emergent Themes
1.0 ‘Journey Towards Diagnosis’
1.1 A Safe Place To Show Herself1.2 The Tipping Point1.3 Questioning Normality 1.4 Feeling Judged and Blamed
2.0 ‘After Diagnosis’
2.1 Release from Responsibility2.2 Legitimacy and Validation2.3 Looking Through The Autism Lens
1.‘Journey Towards Diagnosis’
1.1‘A Safe Place To Show Herself’
All the participants talked about their daughters acting, conforming or being different
in public or with others in comparison to how they are in a safe place (specifically at home,
or with their mothers). Ella and Tessa talked about their daughters hiding parts of their
identity, by not being themselves, or acting due to a fear of the ‘real self’ being seen:
Ella: ‘[Fiona] says…“That's why I'm so good at acting, because I do it all day”’
Tessa: ‘She doesn't want to be herself. Because she doesn't want [friends] to see her,
so she's got this whole other person for her friends than she is at home.’.
Within the narratives parents describe their daughters as ‘hiding’ ‘their ‘real’ selves due to an
expectation of rejection. Shame may be inherent to the motivation to hide, as parents describe
their daughters as not liking or wanting to be themselves. The ‘real’ self is only shown when
the child perceives safety and unconditional acceptance from others. In doing this, the girls
28
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
show their assumptions that there are better ways of ‘being’ (hence putting on an act), and
that they know what will be acceptable to others. Tessa described Angie seeking privacy
when uncertain from a young age:
Tessa: ‘If it was a way she thought she couldn't behave, or she was unsure if it was a
way to behave, it would be done in private’.
Again, this shows a reluctance for Angie to show herself, when uncertain about how this will
be received. This suggests a strong concern for how she is viewed by others as well as
uncertainty about whether particular behaviours are acceptable to others or how they will be
received by others. In this way others are seen as potentially unsafe, whilst privacy is
perceived to be safe.
All participants described their daughters ‘holding in’ their emotions, wanting to be
seen as ‘good’ or to please others. Tessa said this happened from early on in Angie’s life.
This perhaps unveils the children’s assumptions that it is not acceptable to show some
emotions in public:
Tessa: ‘She'd always say she wants to go home whenever she was upset, and very
often not cry’
Emily: ‘That’s the problem. She has to hold it in because she’s been taught to be a
good girl and so she doesn’t want to show other adults that she actually wants
to let rip’
This was significant for some parents in meaning that there had to be a ‘fight’ to be believed
because of the difference in their child’s presentation at home and school.
Certainty of acceptance, love and safety were seen as central to the girls being able to
reveal their real feelings and/or selves:
29
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Emily: ‘She knows I’ll love her no matter what and so she can show me.’
Tessa: ‘I was like, “Why do you only behave like this for me?” And she was like,
“Because you'll always love me” [laughs]…I think that's her way of sort of
saying this is her safe place…she knows that me and her sister are sort of
accepting of it’.
The children were often portrayed as being pre-occupied or ‘overly aware’ of others in their
attempt to please. This meant stringently abiding by rules, in order not to be seen as
‘naughty’:
Tessa: ‘From nursery onwards she was just very, very conformist and very, sort of
like, she'd always be scared of being told off…she would follow all the rules’.
This ‘over-awareness’ was sometimes mentioned by many parents as not fitting with their
perceived ideas of autism, contributing to the delay in autism being raised as a ‘flag’.
1.2‘The Tipping Point’
Ella and Helen talked about their daughters’ levels of distress reaching a peak at the
age of nine years. Emily described this happening when Sophie was around seven:
Ella: ‘She just started screaming saying “can you put your knife away put the knife
away because I don’t know I’m going to go and get that knife and I don’t know
what I’m going to do with it”’
Emily: ‘She came home about November time. “I wish I was dead. Why don’t you just
shoot me”’
This tipping point led to, or accelerated the search for help. For Claire, Abbie’s school
30
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
became concerned when she started trying to run away. Being an overt behaviour, it makes
sense that this was noticed by school. Autism was described to suddenly become more
obvious. Emily and Ella hypothesised that this was due to increased social challenges:
Tessa: ‘When you're five or six, rules of play are really easy. You don't hit and you
share…It's a transition from really simple, let's throw a ball to each other to,
more complex. Sort of they're finding their place in the world’.
Here, Tessa indicates that an increase in social complexity is what she perceives as leading to
the increased visibility of her daughter’s difficulties.
1.3‘Questioning Normality’
All parents recounted a pivotal moment which initiated a nagging doubt or
questioning of normality. For Emily and Ella, this happened online, seeking help on social
media support forums, for Tessa watching a television programme, whilst for Helen and
Claire, this came from professionals:
Tessa: ‘And I start watching it and I was like, “Oh, Angie does that”’
Parents described a ‘backdrop’ of autism from which they started questioning:
Helen: ‘I think it kind of made me watch things more’
Ella: ‘But then it was just there in the back of my head’
Once the seed was planted, most participants researched autism and reached a moment of
realisation that perhaps things are not ‘normal’:
Ella: ‘I think that when you have all these things that you think are normal and then
you see them all written in a list, you start questioning whether things actually
are normal’
31
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Emily: ‘It listed about 40 different things and she ticked about thirty of them (gasps)’
Tessa: ‘And it, kind of all clicked into place.’
For these parents, reading and watching particular media sources shaped their perceptions of
‘normal’. This changed perceptions of behaviour that were previously seen as normal. For
some this resulted in a ‘light bulb’ moment of understanding.
All parents made comparisons both explicitly and implicitly when making sense of
their daughters and attempting to understand ‘normal’. Comparisons were continually made
in relation to; age; gender; common ideas of autism; their child at younger ages; peers;
siblings; themselves as a child; and autism checklists. For example:
Tessa: ‘I was just like, “What five-year-old thinks of that?”’
Helen: ‘No other child is doing that’
Helen and Tessa noticed differences in their daughter’s interests compared with peers:
Tessa: ‘She's really interested in all of that stuff, whereas, like I said, her friends are
like make-up and boys and Instagram’
Helen: ‘…they were talking about, it was boys…and Caroline was just zero interested
in that’
Comparisons both accelerated and decelerated diagnosis. Claire talked about meltdowns
being ‘normal’ in the home, meaning that she overlooked these, ‘I think because I have Ed
[Abbie’s brother] already that [laughs] meltdown it's just a way of life.’ Similarly, for Emily,
comparing Sophie’s difficulty in making friendships to her own, slowed down diagnosis, as
difficulties were not seen as unusual, ‘…but then I was the same’. These examples highlight
32
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
the importance of context and personal experience in parents’ perceptions of ‘normality’.
Tessa compared Angie’s behaviour to those of her peers who had started to seek separation
from their parents and push boundaries:
Tessa: ‘It's that rigidity, rigidness to the rules makes her stand out a little bit, because
11-year-old girls, they are a bit of rule breakers, aren't they?’
This example highlights Tessa’s perception of what the ‘norm’ is for an 11-year-old girl,
derived from her observations or experiences of what other girls of the same age do, or what
she hears of them doing. In other words, Tessa draws on the dominant stories and cultural
understandings of ‘normal’ particular to her cultural context. Parents also described how their
ideas of autism did not ‘fit’ with their daughters:
Ella: ‘I mean she was clever. She could talk and in my head autism was for children
who are developmentally delayed’
Helen: ‘You wouldn't expect autistic children to just speak so freely and so much to
strangers’.
The way in which comparisons were made by participants, brings to light the many factors
that impact on our judgements of what is and is not ‘normal’, based on our own ideas and
experiences, and those of the dominant culture we live in. The examples of comparison
highlight the way in which parents make sense of their children in relation to others, within
the context of age and gender and societal ideas of autism.
1.4‘Feeling Judged and Blamed’
Like their children, parents felt worried about how others (e.g. school, partners) would
33
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
perceive them in seeking diagnosis. Some assumed they would not be believed:
Tessa: ‘They're gonna think I'm like one of these mum’s that go, “I want some sort of
label for my child” and aren't gonna believe me’.
For Emily, Ella and Helen this became their reality. They did not feel supported or believed
by school and felt that others did not see, or refused to see their daughters in the same way
they did:
Ella: ‘I got the impression I was just being a paranoid mum’
[Describing school’s view] ‘She's absolutely fine. She's got friends. She's
doing well academically. There's nothing that we can see’
Helen: ‘[My ex-husband] was saying that I was making it all up’.
This suggests that in understanding difference, parents use the opinions of others as a
reference point to check their own perceptions against. Other people’s views are perceived to
be important in understanding their child’s behaviour as ‘different’. Thus, they appear to
make sense of their child in the context of both their own and other people’s views and this
becomes problematic when other’s views diverge from their own. Given their daughter’s
difference in behaviour at school and home, most parents found the reliance on behavioural
difficulties at school for diagnosis problematic. Emily described questioning herself:
Emily: ‘You know you do question yourself particularly when school are like don’t be
so silly. You know there’s nothing wrong with her, she’s absolutely fine’
Where there were discrepancies in perceptions (between parents and school) this resulted in
participants putting up a fight to be heard, making the journey emotionally difficult:
34
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Emily: ‘You just get angry when you’ve had two years of battling with school’
Emily also alluded to feeling that she was not seen as a credible source, ‘It’s not come from
us, it’s come from a professional’. There was an indication that some parents felt judged or to
blame for their daughter’s difficulties:
Ella: [Group facilitator] ‘said “…she’s not autistic erm and if she’s behaving this
way still after having all these sessions you need to look at how you’re
enabling her behaviour”…it’s really frustrating and then to be told that it’s
your fault.’
In the above example, there is an underlying message that ‘bad’ behaviour is either caused by
autism or parenting. Tessa also spoke about feeling embarrassed by Angie’s behaviour,
perhaps implying that she felt responsible for it:
Tessa: ‘It was shyness, but it was bordering on rude. And it would sort of embarrass
me’.
Interestingly, diagnosis meant some parents felt a release from this perceived blame about
their daughters’ behaviours. Diagnosis brought new perceptions about the locus of control of
behaviour, whereby parents and daughters were seen as not being able to change certain
behaviours. This is explored further, along with the other sub-themes, in the ‘After
Diagnosis’ extended analysis (Appendix L).
35
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Figure I. Proposed model of sense making for parents with a daughter with ASC
36
Questioning Normality
-Online information changing perceptions of normality
-Seeing through an autism backdrop-Making comparisons
Need for explanation
The Tipping Point
Build a case
Release from responsibility, blame and judgment
(Child and Parent)
Increasing social
demands
A Safe Place To Show Herself
-Sensitivity to safety -Acting or not showing ‘real’ self
-Not showing emotions
Diagnosis
Not feeling supported / understoodUncertainty
about what others want
Feeling Judged and Blamed
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Discussion
This study explored how parents made sense of their daughter’s behaviour before they
were diagnosed with autism. In presenting how stories were narrated and salient themes across
narratives, a tentative model (Figure I) was proposed to conceptualise ways in which behaviours
are understood and signs of autism are noticed and considered. The salient themes that emerged
centred around; girls ‘showing themselves’ only when feeling safe, their distress peaking, parents
questioning normality, and parents feeling blamed, unsupported and judged.
Parents described their daughters ‘acting’ differently at school and at home; at school
doing everything they could to ‘be good’ then showing their ‘real’ selves at home. Their
daughters’ competency in acting to ‘please’, sometimes meant that parents did not feel heard or
believed by professionals when seeking help; some felt disregarded and powerless. Being ‘good’
and fitting in became increasingly difficult for girls to manage. Parents thought that this was due
to a context of: increased social complexity within their daughter’s peer groups due to social
‘rules’ becoming less obvious and; peer’s interests (e.g. make-up and boys) not fitting their
daughter’s interests. This often led to a peak in distress characterised by meltdowns at home. The
diagnosis of autism offered parents relief from perceived judgement that their daughter’s
behaviour was ‘naughty’ and/or caused by bad parenting. Previous studies have shown that
diagnosis is sought when a child’s level of distress means that further support is needed
(Baghdadli, Pascal, Grisi & Aussilloux, 2003). This study found that for some parents, feeling
blamed, judged or unheard was also a central experience on their diagnosis journey. Where this
was the case, diagnosis led to relief from understanding the self as a ‘bad parent’, and offered
parents legitimacy and a ‘voice’. In the process of ‘questioning normality’, parents made various
social comparisons in reference to gender, age, diagnosis of autism and themselves, highlighting
37
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
socially and culturally shared ideas of what is, and is not ‘normal’. Parent’s perceptions of
behaviour also changed once autism was mentioned. Narrative theory suggests that scripts about
the self are continually redefined to make sense of experiences (Morgan, 2000). Participants
came to develop personal understandings of autism through sharing their stories with others on
online forums, doing research, and sharing stories with professionals. These findings may shed
new perspectives on understanding why it might take longer for girls to be diagnosed than boys.
Safety and Masking
Some suggest that females, ‘mask’ or ‘camouflage’ their difficulties during social
situations (Attwood, 2006) by either hiding behaviour that might be viewed as socially
unacceptable or ‘unnaturally’ performing behaviour deemed to be more ‘normal’ or socially
acceptable (Willey, 1999). It has been hypothesised that a girl’s level of social skill is just
enough to mask difficulties so that difficulties are not noticed until complexity increases
(Attwood, 2006). This study’s findings corroborated this but uniquely found that a sense of
safety was pivotal to the ‘whole self’ being shown. That is, girls might hide themselves and ‘act’
according to what they perceive others to want (including holding in ‘bad’ emotions), perhaps
due to shame or fear of rejection. This understanding assumes that girls are not necessarily
masking a specific difficulty, but rather they are extremely concerned about being seen as ‘bad’
and/or as different or not fitting in. This understanding of masking is slightly different to
previous understandings, as it functions to hide the self as a whole, as opposed to a specific
difficulty (i.e. lack of social skill). It also suggests the child is an active protagonist in the
situation; they attempt to act one way, rather than their abilities naturally masking difficulty. The
desire to hide the perceived ‘bad’ self, may relate to shame, which can be defined as a judgement
38
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
of the whole self, which leaves a person feeling worthless, vulnerable, visible and powerless
(Miller, 1996). Shame is often considered as stemming from a belief that the self is defective,
flawed or no good (Schimmenti, 2012).
Additionally, parents said explicitly and implicitly, that safety was pivotal to this
‘masking’; when their daughters felt safe, or unwavering love, the masking stopped and their
‘real’ self was shown. When the mask was metaphorically lifted in safety, distress was often
expressed. Parents described that their daughters were extremely sensitive to feeling safe; safety
was not found in other adults, children or situations, leading the children to hide perceived
unwanted or unpleasant behaviours and emotions much of the time. This preoccupation with
pleasing others made the girls ‘overly aware’ of others, which did not fit with parent’s
perceptions of autism, delaying the time in which autism was on the parent’s radar.
Why Seek Diagnosis? Changing Understandings
Recent research has evidenced that people with ASC are more likely to have been
diagnosed if they have co-occurring problems (Posserud, Hysing, Helland, Gillberg &
Lundervold, 2016). This fits with this study’s findings, where an expression of distress often
paralleled an approach to professionals. However, distress was not sufficient for parents to
‘question normality’; for three parents feeling judged and/or not supported by professionals
additionally motivated a need for diagnosis. For one parent, it was school who first instigated the
diagnosis, due to ‘mood swings’ and behaviour problems at school.
Moreover, the diagnosis itself was not necessary for gaining support; two parents gained
support before the diagnosis was given, whilst another expressed that she was satisfied with
support offered by school pre-diagnosis. Despite this, parents still felt a need for a diagnosis.
39
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Farrugia (2009) evidenced that a child’s ASC diagnosis was critical for parents to resist
stigmatisation. Similarly Russell and Norwich (2012) evidence that parents attempt to retain the
‘normal’ status of their child by either resisting ASC diagnosis, or through identification of ASC
and then trying to change society’s attitudes to de-stigmatise it. The present study similarly
showed that diagnosis offered relief from judgement, whether internal (self-criticism) or
external. Perhaps this was partly due to a perceived understanding of behaviour and emotion that
was previously inexplicable, and extremely upsetting (for example, suicidality).
Moreover, parents expressed that the diagnosis brought a greater understanding of why
their child behaved in certain ways. This exposes dominant cultural narratives whereby
diagnoses are seen as explanations in themselves, i.e. autism is causal to problems. Parents were
vague about how this new understanding was helpful (e.g. expressing that diagnosis meant
‘things could be put in place’). Some parents spoke about previous explanations of their
daughter’s behaviour and distress, expressing satisfaction of now knowing it was the autism
causing the distress. Thus, the autism explanation perhaps restricted understandings of why
behaviours were happening, and removed perceived choice about responding to these (i.e.
parents talked about having to parent in a certain way). Perhaps this relieved parents from
responsibility from socially dominant expectations that a child should be parented in a certain
way.
Narrative tone, as well as emergent themes, also suggested that diagnosis gave parents
legitimacy and a voice to assert their daughter’s needs, mostly at school. This might be needed
for parents of girls more than boys, given that ASC behaviour associated with boys is more
disruptive in school situations (Hiller et al., 2014), and so teachers may be more alerted to boy’s
40
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
needs without parents needing to assert these. Thus, rather than enabling access to practical
support, ASC diagnosis bolstered parents’ voices and perhaps helped them to feel less blamed.
Questioning ‘Normal’
The ambiguity of ASC as a label, and its construction by medical, media, cultural and
family discourses (Avdi, Griffin & Brough, 2000; Grinker & Cho, 2013; Huws & Jones, 2010)
allows for individuals with the diagnosis, and their families to interpret and construct its meaning
in different ways. Nadesan (2013) draws our attention to the socially constructed standards of
‘normalcy’ upon which the medical model stands and observes that before autism was
categorised as a disorder, associated social interactions may have been perceived as
‘eccentricities’ rather than ‘abnormalities’. The present study found that parents only started to
question normality when a person or situation raised the possibility of autism, rather than parents
noticing ‘abnormality’; it was only on looking back, through the lens of the present that signs
were noticed. This study also highlighted how checklists available online, shape understandings
of ‘normal’ and can be interpreted in many ways to fit with a child’s presentation.
Age was seen as an important factor by which signs became more obvious. Cridland and
colleagues (2014) evidence that a specific difficulty for girls with autism is the context in which
social interactions with other girls is more complex than those with boys. In this study, parents
also suggested that from the ages of seven to nine years old, their daughters found socialising
more difficult due to normal ‘rules’ of play being broken and challenged, becoming more
complex. This fits with previous suggestions that as girls transition into adolescence,
expectations from peers may be much higher than for boys, because typical female relationships
are characterised by complex relational skills, with interactions focused more on conversation,
41

PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
shared emotions and emotional support (Bauminger, Shulman & Agam, 2003; Hannah &
Murachver, 1999). Additionally, some parents thought their daughters did not have interests
similar to their female peers, for example boys and Instagram. These examples are particularly
relevant in terms of gender related norms and expectations and highlight how important these are
to account for more formally in assessment.
Parents also used others to check their perceptions of ‘normal’. Masking made this
difficult, especially where teachers did not perceive difficulty related to autism. This fits with
previous evidence that suggests that teachers do not rate ASC girl’s social difficulties as highly
on diagnostic measures compared to parents (Hiller et al., 2014). Hartung and Widiger (1998)
argue that individuals are more likely to be referred for assessment if they demonstrate social
inappropriateness or externalise distress. The current findings similarly show that if behaviour
was not disruptive or problematic at school, parents were not well supported in seeking
diagnosis.
Clinical Implications
These stories of diagnosis expose some challenges that schools and services need to meet
in terms of the support given both during assessment, and post-diagnosis. Policies have focused
on the length of the assessment process (NICE, 2011). Although participants waited for
approximately two years for their daughter’s diagnosis, this was not highlighted as problematic.
However, a lack of understanding and respect for parents, especially before diagnosis was
emphasised. The current research highlights the importance of families feeling heard and
understood and having their needs met, whether or not a diagnosis has been made. These needs
are undoubtedly varied and complex so a formulation driven approach which focuses on an
42
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
assessment of need rather than identification of symptoms would be useful when families are, or
would like to be, referred for assessment. This approach could also identify appropriate
interventions and consider other challenges and strengths within families that might otherwise be
missed when focus is unilaterally upon diagnosis. Formulation as part of a process of diagnosis
may help families to reflect on, and reach understandings that look past blame as an explanation.
A wider issue was also raised about some schools and professionals contributing to feelings of
blame; some parents felt that it was insinuated that parenting was causal to certain behaviours.
Working closely with our education colleagues and other professionals to help them to
understand behaviour and family’s experiences will be helpful so that diagnosis does not feel like
the only relief from judgement and blame. Additionally, the finding that parents experienced
some professionals as not sharing their concerns and labelled parents as over-anxious (a finding
also found in other research, e.g. Midence & O’Neill,1999) supports the recommendation made
by the National Autistic Society (NAS, 2003) that a team of skilled practitioners should be
developed with whom education and health professionals working with children can discuss
behaviours that they are concerned about (or that parents bring to them as a concern) along with
the same professionals receiving continuous ASC awareness training. The NAS also argue that
concerns about possible ASC at any age should lead to the triggering of a referral to the local
pathway. Perhaps not supporting children at an early stage means that their problems are further
compounded, which in turn can result in mental health difficulties and much distress for the child
and family.
Moreover, despite the wide range of interventions that could be helpful for families, this
study along with previous research (Wallace, Parr, & Hardy, 2013) has highlighted that this is
lacking after diagnosis. The practice of diagnosing without offering support or treatment raises
43
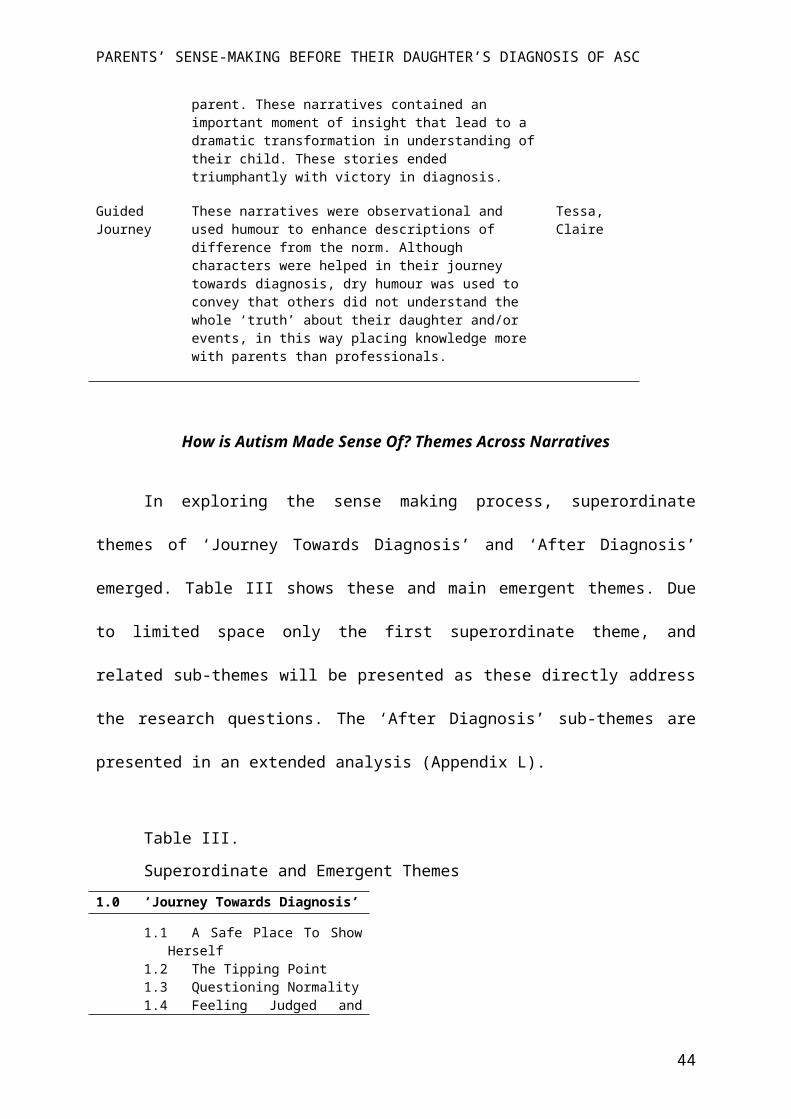
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
ethical questions. Parents also reported feeling that they had no choice in their parenting
responses to their daughters. The discourses that frame ASCs as genetic or biological may be
problematic, removing parent’s sense of agency. The way in which autism is talked about in
clinical settings is important; parents need to feel empowered to have agency in making changes
that may be helpful for their daughters, rather than feeling governed by autism. Moreover, if
autism is seen as causal, and therefore an explanation, this may inhibit our curiosity as
professionals about the detail of families’ experiences of distress (e.g. Why is safety only found
at home? What are the child’s experiences of school/separation/showing emotions?). Diagnosing
problems, without offering support might feed the narrative that ‘nothing can be changed’.
This study also highlights the challenges that parents and professionals face due to girls
hiding their distress at school. As professionals, in order to make better decisions diagnostically,
and to reduce feelings of blame, awareness and respect of the different contexts in which
difficulties arise is needed. For girls, reports of ‘no difficulties’ at school should be a ‘flag’ that
needs to be curiously explored.
Suggestions for Further Research
This research has attempted to address the context within which parents make sense of
their daughters’ behaviours before diagnosis of autism. These understandings are held tentatively
and are not transferable to other mothers of daughters with ASC without further research.
Findings from this study suggested that shame may be related to masking for autistic girls. It
would therefore be beneficial to explore further ASC girl’s: experience of shame; assumptions
that ‘difference’ will not be accepted and; perceived fears of showing the ‘real’ self. Perhaps
play-based studies could enable these experiences to be expressed. Parents saw the ‘holding in’
44
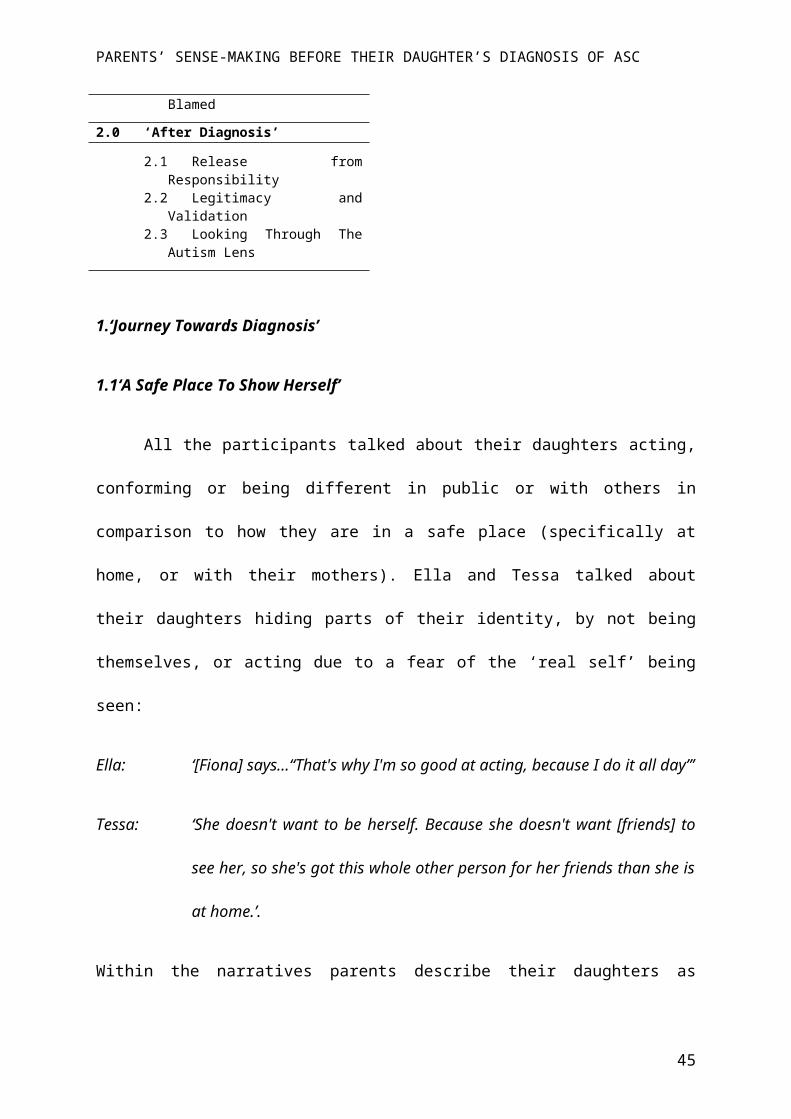
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
of the real self as significant to their daughter’s distress so a better understanding of masking
may help professionals to establish more helpful interventions. Acceptance, Commitment and
Compassion Focussed approaches have been found to be helpful in other contexts for addressing
shame (Gilbert & Irons, 2005; Luoma, Kohlenberg, Hayes & Fletcher, 2012), so further research
into adapted treatments for families is also warranted.
Another area that could be explored further is the experience of blame and judgement for
parents during the process of, and after diagnosis. Interestingly, parents felt ASC diagnosis lifted
these feelings, though also reduced their perceived choice about how they could respond to their
daughters. It would be beneficial to examine how formulation versus diagnosis driven
approaches support families in reducing blame whilst also empowering parents to find helpful
ways of responding to their children.
The findings of this study indicated that mothers of daughters with ASC may make
decisions about what is right partly based on assumptions about gender (i.e. what a girl ‘should’
be like). Presently, diagnostic tools do not have clear guidelines about specific symptoms that are
observed in girls and boys. This study found that mothers noticed their daughter’s ‘difference’
when their daughters do not show gender-typical interests. An exploration of how clinicians
consider typical sex/gender differences, such as gender-specific interests using a qualitative
study would be useful. This might help to inform whether it would be possible to formalise these
considerations in diagnostic measures so as to enhance sensitivity and validity of the measures
for girls.
45
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appraisal of the Study
The current research contributes to the existing literature on the experiences and sense-
making process of parents seeking an autism diagnosis for their daughters. To date, research
considering the perspectives of parents has been limited. The use of a qualitative methodology is
a strength of the study because it enabled detailed and in-depth data to emerge. The narrative
approach allowed for stories to be told without constraint, from those who have an experience of
noticing and making sense of their daughter’s diagnosis of autism. This is valuable in a literature
that largely overlooks the context of autism diagnosis. Using open-ended questions from which
participants could tell their story was a strength in minimising researcher assumptions during the
interview. However, it is accepted that the researcher would have had an impact and that
personal assumptions were inevitable due to the co-creation of the narratives. Therefore, to
support credibility I adhered to Yardley’s (2000) principles by crosschecking transcripts in peer
supervision and with supervisors, and supporting ongoing reflexivity by attending peer-
supervision and keeping a research journal. Despite this, although acceptable, I also recognise
that it is possible to interpret one set of data in many ways (Ricoeur, 1976) and the
interpretations proposed are one, of many different but legitimate understandings of the data.
Participants were recruited mostly on online social media forums. It may be that these
mothers felt less supported because they were seeking support online. Moreover, mothers who
access these forums may identify and engage with autism in a particular way (e.g. perhaps
viewing autism as a larger part of their identity than other parents). This method of recruitment
may not be representative of parents who do not access these sorts of groups. However, it was
observed to be a fair way of accessing the community where 96-99% of adults aged 16-44 years
are on social networking sites (Office for National Statistics, 2018).
46
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
The research question set out to investigate how parents make sense of their daughter’s
behaviour before diagnosis of ASC. I acknowledge that because I chose to interview parents
whose daughters had already received a diagnosis, this would have coloured the lens through
which their memories are looked at. Additionally, the diagnosis itself might have impacted the
girls’ perceptions and behaviour, and their parents’ stories. All interviews took place within a
year of diagnosis in order to try and minimise this. Also, although it was not an inclusion criteria,
all participants were female. This is likely to have impacted on the findings, though also perhaps
reflects the fact that presently within the UK, women are more likely to take caring responsibility
for their children. It is important that future research examines the views of fathers because there
is evidence that suggest fathers have more difficulties accepting diagnosis than mothers and
employ different coping strategies (Evans, 2010), and feel neglected in the diagnostic process
(Potter, 2017).
Conclusion
This study explored how parents make sense of their daughters’ behaviours before
diagnosis of an ASC and how these experiences were narrated. In addressing the research
question, this study proposed a tentative model that outlines a process of sense making. Further
research is now needed to explore these processes to inform the ways in which diagnosis and
support is given for families.
47
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders
(DSM-5®) American Psychiatric Pub. Arlington, VA, US.
Andrews, M., Squire, C., & Tamboukou, M. (2013). Doing narrative research. California: Sage.
Asperger, H. (1944). Die „Autistischen psychopathen” im kindesalter. Archiv Für Psychiatrie
Und Nervenkrankheiten, 117(1), 76-136.
Attwood, T. (2006). The pattern of abilities and development of girls with Asperger’s syndrome.
Asperger’s and Girls, 1-7.
Avdi, E., Griffin, C., & Brough, S. (2000). Parents' constructions of the ‘problem’during
assessment and diagnosis of their child for an autistic spectrum disorder. Journal of Health
Psychology, 5(2), 241-254.
Baghdadli, A., Pascal, C., Grisi, S., & Aussilloux, C. (2003). Risk factors for self‐injurious
behaviours among 222 young children with autistic disorders. Journal of Intellectual
Disability Research, 47(8), 622-627.
Baird, G., Douglas, H. R., & Murphy, M. S. (2011). Recognising and diagnosing autism in
children and young people: Summary of NICE guidance. Bmj, 343(d6360), 10.1136.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., et al. (2006).
Prevalence of disorders of the autism spectrum in a population cohort of children in south
thames: The special needs and autism project (SNAP). The Lancet, 368(9531), 210-215.
48
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Baron-Cohen, S., Scott, F. J., Allison, C., Williams, J., Bolton, P., Matthews, F. E., et al. (2009).
Prevalence of autism-spectrum conditions: UK school-based population study. The British
Journal of Psychiatry, 194(6), 500-509.
Bauminger, N., Shulman, C., & Agam, G. (2003). Peer interaction and loneliness in high-
functioning children with autism. Journal of Autism and Developmental Disorders, 33(5),
489-507.
Begeer, S., Mandell, D., Wijnker-Holmes, B., Venderbosch, S., Rem, D., Stekelenburg, F., et al.
(2013). Sex differences in the timing of identification among children and adults with
autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(5), 1151-
1156.
Biklen, D. (2005). Autism and the myth of the person alone. New York, NY: NYU Press.
Brown, H. M. (1991). Shame and relapse issues with the chemically dependent
client. Alcoholism Treatment Quarterly, 8(3), 77-82.
Burr, V. (2003). Social constructionism, (2nd ed.). East Sussex: Routledge.
Chatard, A., Guimond, S., & Selimbegovic, L. (2007). “How good are you in math?” the effect
of gender stereotypes on students’ recollection of their school marks. Journal of
Experimental Social Psychology, 43(6), 1017-1024.
Cridland, E. K., Jones, S. C., Caputi, P., & Magee, C. A. (2014). Being a girl in a boys’ world:
Investigating the experiences of girls with autism spectrum disorders during
adolescence. Journal of Autism and Developmental Disorders, 44(6), 1261-1274.
Crossley, M. (2000). Introducing narrative psychology McGraw-Hill Education (UK).
49
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Daley, T. C. (2004). From symptom recognition to diagnosis: Children with autism in urban
india. Social Science & Medicine, 58(7), 1323-1335.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with
autism spectrum disorders: Associations with child characteristics. Journal of Autism and
Developmental Disorders, 38(7), 1278.
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: Gender differences in the
social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678-689.
Dean, M., Kasari, C., Shih, W., Frankel, F., Whitney, R., Landa, R., et al. (2014). The peer
relationships of girls with ASD at school: Comparison to boys and girls with and without
ASD. Journal of Child Psychology and Psychiatry, 55(11), 1218-1225.
Ehlers, S., Gillberg, C., & Wing, L. (1999). A screening questionnaire for Asperger syndrome
and other high-functioning autism spectrum disorders in school age children. Journal of
Autism and Developmental Disorders, 29(2), 129-141.
Evans, A. (2010). Parents’ Responses to their Child’s Diagnosis of Autism Spectrum Disorder
(ASD) Doctoral dissertation, University of Southampton.
Faherty, C. (2006). Asperger’s syndrome in women: A different set of challenges. Asperger’s
and Girls, , 9-14.
Farrugia, D. (2009). Exploring stigma: Medical knowledge and the stigmatisation of parents of
children diagnosed with autism spectrum disorder. Sociology of Health & Illness, 31(7),
1011-1027.
50
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Filipek, P. A., Accardo, P. J., Baranek, G. T., Cook, E. H., Dawson, G., Gordon, B., et al. (1999).
The screening and diagnosis of autistic spectrum disorders. Journal of Autism and
Developmental Disorders, 29(6), 439-484.
Flanigan, B. J. (1987). Shame. Alcoholism Treatment Quarterly, 4, 190-194.
Fombonne, E. (1999). The epidemiology of autism: A review. Psychological Medicine, 29(4),
769-786.
Fombonne, E. (2002). Epidemiological trends in rates of autism. Molecular Psychiatry, 7(S2),
S4.
Fombonne, E. (2003). Epidemiological surveys of autism and other pervasive developmental
disorders: An update. Journal of Autism and Developmental Disorders, 33(4), 365-382.
Frazier, T. W., Georgiades, S., Bishop, S. L., & Hardan, A. Y. (2014). Behavioral and cognitive
characteristics of females and males with autism in the Simons Simplex Collection. Journal
of the American Academy of Child & Adolescent Psychiatry, 53(3), 340. e3.
Gergen, K. J. (1985). Social constructionist inquiry: Context and implications. The social
construction of the person (pp. 3-18) Springer.
Giarelli, E., Wiggins, L. D., Rice, C. E., Levy, S. E., Kirby, R. S., Pinto-Martin, J., et al. (2010).
Sex differences in the evaluation and diagnosis of autism spectrum disorders among
children. Disability and Health Journal, 3(2), 107-116.
Gilbert, P., & Irons, C. (2005). Focused therapies and compassionate mind training for shame
and self-attacking. Compassion: Conceptualisations, Research and use in Psychotherapy, ,
263-325.
51
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Gillberg, C. (1993). Autism and related behaviours. Journal of Intellectual Disability
Research, 37(4), 343-372.
Goin-Kochel, R. P., Mackintosh, V. H., & Myers, B. J. (2006). How many doctors does it take to
make an autism spectrum diagnosis? Autism, 10(5), 439-451.
Grinker, R. R., & Cho, K. (2013). Border children: Interpreting autism spectrum disorder in
south korea. Ethos, 41(1), 46-74.
Hannah, A., & Murachver, T. (1999). Gender and conversational style as predictors of
conversational behavior. Journal of Language and Social Psychology, 18(2), 153-174.
Harper, D. J. (2012). Surveying qualitative research teaching on british clinical psychology
training programmes 1992–2006: A changing relationship? Qualitative Research in
Psychology, 9(1), 5-12.
Hartung, C. M., & Widiger, T. A. (1998). Gender differences in the diagnosis of mental
disorders: Conclusions and controversies of the DSM–IV. Psychological Bulletin, 123(3),
260.
Hiller, R. M., Young, R. L., & Weber, N. (2014). Sex differences in autism spectrum disorder
based on DSM-5 criteria: Evidence from clinician and teacher reporting. Journal of
Abnormal Child Psychology, 42(8), 1381-1393.
Holliday Willey, L. (1999). Pretending to be normal: Living with Asperger’s syndrome. London:
Jessica Kingsley.
52
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Holtmann, M., Bölte, S., & Poustka, F. (2007). Autism spectrum disorders: Sex differences in
autistic behaviour domains and coexisting psychopathology. Developmental Medicine &
Child Neurology, 49(5), 361-366.
Huws, J. C., & Jones, R. (2010). ‘They just seem to live their lives in their own little world’: Lay
perceptions of autism. Disability & Society, 25(3), 331-344.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2(3), 217-250.
Kim, Y. S., Leventhal, B. L., Koh, Y., Fombonne, E., Laska, E., Lim, E., et al. (2011).
Prevalence of autism spectrum disorders in a total population sample. American Journal of
Psychiatry, 168(9), 904-912.
Kopp, S., & Gillberg, C. (2011). The autism spectrum screening questionnaire (ASSQ)-revised
extended version (ASSQ-REV): An instrument for better capturing the autism phenotype in
girls? A preliminary study involving 191 clinical cases and community controls. Research
in Developmental Disabilities, 32(6), 2875-2888.
Kseib, N. A. (2018). A review of the differences in the presentation of girls and boys with autism
spectrum conditions without cognitive impairment. Unpublished manuscript, School of
Psychology, University of Surrey, Surrey, UK.
Kumazaki, H., Muramatsu, T., Kosaka, H., Fujisawa, T. X., Iwata, K., Tomoda, A., et al. (2015).
Sex differences in cognitive and symptom profiles in children with high functioning autism
spectrum disorders. Research in Autism Spectrum Disorders, 13, 1-7.
Lord, C., Luyster, R., Gotham, K., & Guthrie, W. (2012). Autism diagnostic observation
Schedule–Toddler module. Los Angeles: Western Psychological Services.
53
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised
version of a diagnostic interview for caregivers of individuals with possible pervasive
developmental disorders. Journal of Autism and Developmental Disorders, 24(5), 659-685.
Luoma, J. B., Kohlenberg, B. S., Hayes, S. C., & Fletcher, L. (2012). Slow and steady wins the
race: A randomized clinical trial of acceptance and commitment therapy targeting shame in
substance use disorders. Journal of Consulting and Clinical Psychology, 80(1), 43.
Mattila, M., Kielinen, M., Linna, S., Jussila, K., Ebeling, H., Bloigu, R., et al. (2011). Autism
spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: An
epidemiological study. Journal of the American Academy of Child & Adolescent
Psychiatry, 50(6), 592. e11.
May, T., Cornish, K., & Rinehart, N. (2014). Does gender matter? A one year follow-up of
autistic, attention and anxiety symptoms in high-functioning children with autism spectrum
disorder. Journal of Autism and Developmental Disorders, 44(5), 1077-1086.
May, T., Cornish, K., & Rinehart, N. J. (2016). Gender profiles of behavioral attention in
children with autism spectrum disorder. Journal of Attention Disorders, 20(7), 627-635.
Mazzone, L., & Vitiello, B. (Eds.). (2016). Psychiatric symptoms and comorbidities in autism
spectrum disorder. New York, NY: Springer.
Midence, K., & O’Neill, M. (1999). The experience of parents in the diagnosis of autism: A pilot
study. Autism, 3(3), 273-285.
Miles, M. B., Huberman, A. M., Huberman, M. A., & Huberman, M. (1994a). Qualitative data
analysis: An expanded sourcebook. California: Sage.
54
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Miller, S. (2013). Shame in context. New York, NY: Routledge.
Molloy, H., & Vasil, L. (2002). The social construction of Asperger syndrome: The
pathologising of difference? Disability & Society, 17(6), 659-669.
Morgan, A. (2000). What is narrative therapy?. Dulwich Centre Publications Adelaide.
Murray, M. (2003). Narrative psychology. Qualitative Psychology: A Practical Guide to
Research Methods, 111-131.
Nadesan, M. H. (2013). Constructing autism: Unravelling the'truth'and understanding the
social New York, NY: Routledge.
National Autistic Society (2016). What is autism? [online] Autism.org.uk. Retrieved from:
https://www.autism.org.uk/get-involved/media-centre/position-statements/causes.aspx
[Accessed 11 Jul. 2018].
National Collaborating Centre for Mental Health (UK. (2013). Autism: The management and
support of children and young people on the Autism Spectrum. British Psychological
Society. Chicago.
National Institute for Health and Care Excellence. (2011). Autism spectrum disorder in under
19s: recognition, referral and diagnosis (NICE Clinical guideline CG128). Retrieved from
https://www.nice.org.uk/guidance/qs39
Office for National Statistics. (2018, May 18). Statistical Bulletin: Internet users, UK: 2018
Internet use in the UK annual estimates by age, sex, disability and geographical. London:
Office for National Statistics. Retrieved from:
55
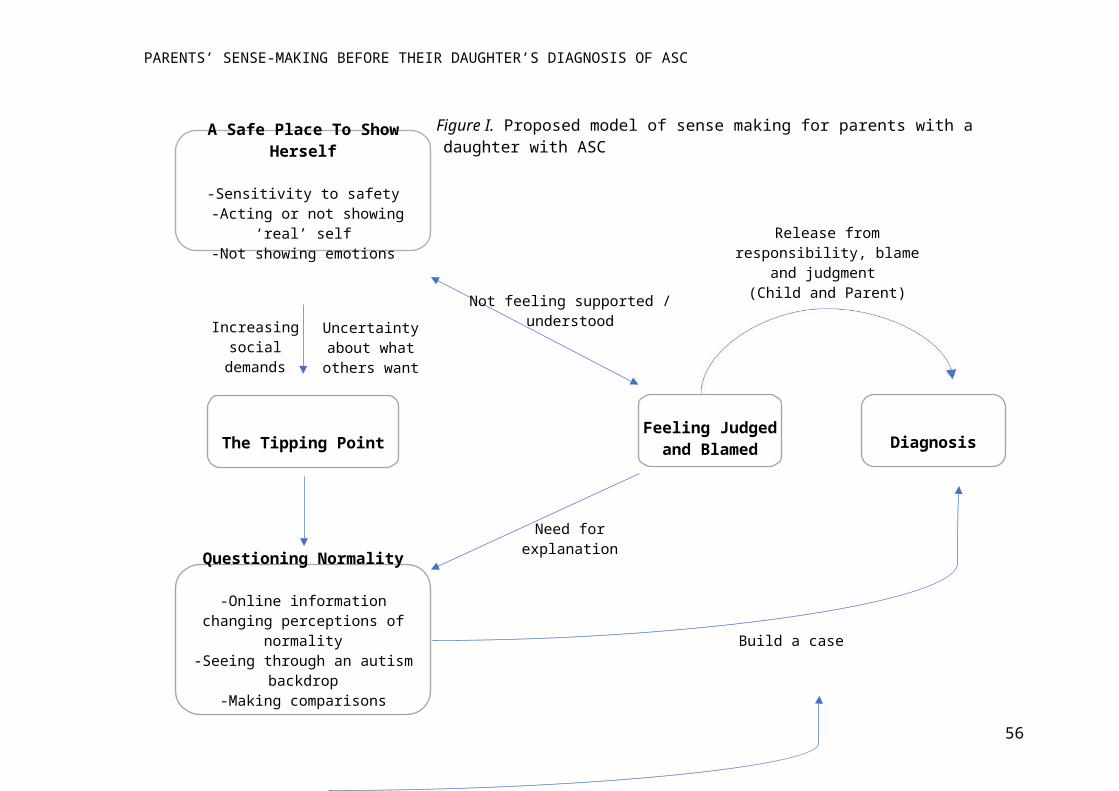
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
https://www.ons.gov.uk/businessindustryandtrade/itandinternetindustry/bulletins/
internetusers/2018 [Accessed 14 Jul. 2018].
Ozonoff, S., Williams, B. J., & Landa, R. (2005). Parental report of the early development of
children with regressive autism: The delays-plus-regression phenotype. Autism, 9(5), 461-
486.
Plummer, K. (2001). The call of life stories in ethnographic research. Handbook of
Ethnography, , 395-406.
Posserud, M., Hysing, M., Helland, W., Gillberg, C., & Lundervold, A. J. (2016). Autism traits:
The importance of “co-morbid” problems for impairment and contact with services. data
from the bergen child study. Research in Developmental Disabilities,
Potter, C. A. (2017). “I received a leaflet and that is all”: Father experiences of a diagnosis of
autism. British Journal of Learning Disabilities, 45(2), 95-105.
Ricoeur, P. (1976). Interpretation theory: Discourse and the surplus of meaning Texas: TCU
press.
Riessman, C. K. (2008). Narrative methods for the human sciences California: Sage.
Riley, T., Hawe, P., & Shiell, A. (2005). Contested ground: How should qualitative evidence
inform the conduct of a community intervention trial? Journal of Health Services Research
& Policy, 10(2), 103-110.
Rivet, T. T., & Matson, J. L. (2011). Review of gender differences in core symptomatology in
autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 957-976.
56
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Russell, G., & Norwich, B. (2012). Dilemmas, diagnosis and de-stigmatization: Parental
perspectives on the diagnosis of autism spectrum disorders. Clinical Child Psychology and
Psychiatry, 17(2), 229-245.
Rynkiewicz, A., & Łucka, I. (2015). Autism spectrum disorder (ASD) in girls. co-occurring
psychopathology. sex differences in clinical manifestation. Psychiatr.Pol. (31)
Rynkiewicz, A., Schuller, B., Marchi, E., Piana, S., Camurri, A., Lassalle, A., et al. (2016). An
investigation of the ‘female camouflage effect’in autism using a computerized ADOS-2 and
a test of sex/gender differences. Molecular Autism, 7(1), 10.
Schimmenti, A. (2012). Unveiling the hidden self: Developmental trauma and pathological
shame. Psychodynamic Practice, 18(2), 195-211.
Scott, F. J., Baron-Cohen, S., Bolton, P., & Brayne, C. (2002). Brief report prevalence of autism
spectrum conditions in children aged 5-11 years in Cambridgeshire, UK. Autism, 6(3), 231-
237.
Shattuck, P. T., Durkin, M., Maenner, M., Newschaffer, C., Mandell, D. S., Wiggins, L., et al.
(2009). Timing of identification among children with an autism spectrum disorder: Findings
from a population-based surveillance study. Journal of the American Academy of Child &
Adolescent Psychiatry, 48(5), 474-483.
Sicherman, N., Loewenstein, G., Tavassoli, T., & Buxbaum, J. D. (2018). Grandma knows best:
Family structure and age of diagnosis of autism spectrum disorder. Autism, 22(3), 368-376.
57
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Solomon, M., Miller, M., Taylor, S. L., Hinshaw, S. P., & Carter, C. S. (2012). Autism
symptoms and internalizing psychopathology in girls and boys with autism spectrum
disorders. Journal of Autism and Developmental Disorders, 42(1), 48-59.
Springer, K. W., Stellman, J. M., & Jordan-Young, R. M. (2012). Beyond a catalogue of
differences: A theoretical frame and good practice guidelines for researching sex/gender in
human health. Social Science & Medicine, 74(11), 1817-1824.
Supekar, K., & Menon, V. (2015). Sex differences in structural organization of motor systems
and their dissociable links with repetitive/restricted behaviors in children with
autism. Molecular Autism, 6(1), 50.
Timimi, S. (2004). Diagnosis of autism: Current epidemic has social context. BMJ: British
Medical Journal, 328(7433), 226.
Timimi, S., Gardner, N., & McCabe, B. (2011). The myth of autism: Medicalising men's and
boys' social and emotional competence Basingstoke, UK: Palgrave Macmillan.
Tracy, S. J. (2010). Qualitative quality: Eight “big-tent” criteria for excellent qualitative
research. Qualitative Inquiry, 16(10), 837-851.
Volkmar, F. R., Szatmari, P., & Sparrow, S. S. (1993). Sex differences in pervasive
developmental disorders. Journal of Autism and Developmental Disorders, 23(4), 579-591.
Wallace, S., Parr, J., & Hardy, A. (2013). One in a hundred: Putting families at the heart of
autism research. Autistica.Http://Autistica.Org.Uk/Document_downloads/Reports/Autistica-
1-100-Report.PDF [Accessed Apr 2015]
58
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Wang, S., Deng, H., You, C., Chen, K., Li, J., Tang, C., et al. (2017). Sex differences in
diagnosis and clinical phenotypes of Chinese children with autism spectrum
disorder. Neuroscience Bulletin, 33(2), 153-160.
Willig, C. (2012). Qualitative interpretation and analysis in psychology McGraw-Hill Education
(UK).
World Health Organization (2015) What do we mean by ‘sex’ and ‘gender’? World Health
Organization. http://www.who.int/gender/whatisgender/en/.
Yardley, L. (2000). Dilemmas in qualitative health research. Psychology and Health, 15(2), 215-
228.
Yaull-Smith, D. (2008). Girls on the spectrum. Communication. London: National Autistic
Society.
59
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Major Research Project Empirical Paper: Appendices
Appendix A: Guidelines for Authors: Journal of Autism and Developmental Disorders 61
Appendix B: Online Post for Internet Forums and Study Poster 79
Appendix C: Details of Recruitment Process 81
Appendix D: Participant Information Sheet 82
Appendix E: Consent Form 85
Appendix F: Interview Schedule 87
Appendix G: Criteria for Good Quality Qualitative Research 88
Appendix H: Evidence of Ethical Approval 90
Appendix I: Risk Assessment 91
Appendix J: Extended Analysis (How Were Stories Told? Genre) 95
Appendix K: Extended Analysis (How Were Stories Told? Imagery) 99
Appendix L: Extended Analysis (How is Autism Made Sense of? ‘After Diagnosis’) 101
Appendix M: Examples of Coded Transcript 106
Appendix N: Extracts from Reflective Journal 111
60
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix A: Guidelines for Authors: Journal of Autism and Developmental Disorders
EDITORIAL PROCEDURE
Double-Blind Peer Review
MANUSCRIPT FORMAT
All JADD manuscripts should be submitted to Editorial Manager in 12-point Times New Roman with standard 1-inch borders around the margins.
APA Style
Text must be double-spaced; APA Publication Manual standards must be followed.
As of January 20, 2011, the Journal has moved to a double-blind review process. Therefore, when submitting a new manuscript, DO NOT include any of your personal information (e.g., name, affiliation) anywhere within the manuscript. When you are ready to submit a manuscript to JADD, please be sure to upload these 3 separate files to the Editorial Manager site to ensure timely processing and review of your paper:
• A title page with the running head, manuscript title, and complete author information. Followed by (page break) the Abstract page with keywords and the corresponding author e-mail information.
• The blinded manuscript containing no author information (no name, no affiliation, and so forth).
• The Author Note
TYPES OF PAPERSArticles, Commentaries Brief Reports, Letters to the Editor← The preferred article length is 20-23 double-spaced manuscript pages long (not
including title page, abstract, tables, figures, addendums, etc.) Manuscripts of 40 double-spaced pages (references, tables and figures counted as pages) have been published. The reviewers or the editor for your review will advise you if a longer submission must be shortened.
← Special Issue Article: The Guest Editor may dictate the article length; maximum pages allowed will be based on the issue’s page allotment.
← Commentary: Approximately 20-25 double-spaced pages maximum, with fewer references and tables/figures than a full-length article.
← A Brief Report: About 8 double-spaced pages with shorter references and fewer tables/figures. May not meet the demands of scientific rigor required of a JADD article – can be preliminary findings.
← A Letter to the Editor is 6 or less double spaced pages with shorter references, tables and figures. Style sheet for Letter to the Editor:
61
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
← A title page with the running head, manuscript title, and complete author information including corresponding author e-mail information
← The blinded manuscript containing no author information (no name, no affiliation, and so forth):-- 6 or less double spaced pages with shorter references, tables and figures - Line 1: “Letter to the Editor” - Line 3: begin title (note: for “Case Reports start with “Case Report: Title”) - Line 6: Text begins; references and tables, figure caption sheet, and figures may follow (page break between each and see format rules)
REVIEW YOUR MANUSCRIPT FOR THESE ELEMENTS1. Order of manuscript pages
Title Page with all Author Contact Information & Abstract with keywords and the corresponding author e-mail information.
Blinded Manuscript without contact information and blinded Abstract, and References
Appendix
Figure Caption Sheet
Figures
Tables
Author Note
MANUSCRIPT SUBMISSION
Manuscript SubmissionSubmission of a manuscript implies: that the work described has not been published before; that it is not under consideration for publication anywhere else; that its publication has been approved by all co-authors, if any, as well as by the responsible authorities – tacitly or explicitly – at the institute where the work has been carried out. The publisher will not be held legally responsible should there be any claims for compensation.
PermissionsAuthors wishing to include figures, tables, or text passages that have already been published elsewhere are required to obtain permission from the copyright owner(s) for both the print and online format and to include evidence that such permission has been granted when submitting their papers. Any material received without such evidence will be assumed to originate from the authors.
Online SubmissionPlease follow the hyperlink “Submit online” on the right and upload all of your manuscript files following the instructions given on the screen.
62
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
TITLE PAGEThe title page should include:
← The name(s) of the author(s)← A concise and informative title← The affiliation(s) and address(es) of the author(s)← The e-mail address, telephone and fax numbers of the corresponding author
ABSTRACTPlease provide an abstract of 120 words or less. The abstract should not contain any undefined abbreviations or unspecified references.
KEYWORDSPlease provide 4 to 6 keywords which can be used for indexing purposes.
TEXT
Text FormattingManuscripts should be submitted in Word.
← Use a normal, plain font (e.g., 10-point Times Roman) for text.← Use italics for emphasis.← Use the automatic page numbering function to number the pages.← Do not use field functions.← Use tab stops or other commands for indents, not the space bar.← Use the table function, not spreadsheets, to make tables.← Use the equation editor or MathType for equations.← Save your file in docx format (Word 2007 or higher) or doc format (older Word
versions).
HeadingsPlease use no more than three levels of displayed headings.
AbbreviationsAbbreviations should be defined at first mention and used consistently thereafter.
FootnotesFootnotes can be used to give additional information, which may include the citation of a reference included in the reference list. They should not consist solely of a reference citation, and they should never include the bibliographic details of a reference. They should also not contain any figures or tables.
Footnotes to the text are numbered consecutively; those to tables should be indicated by superscript lower-case letters (or asterisks for significance values and other statistical data). Footnotes to the title or the authors of the article are not given reference symbols.
Always use footnotes instead of endnotes.
63
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
AcknowledgmentsAcknowledgments of people, grants, funds, etc. should be placed in a separate section on the title page. The names of funding organizations should be written in full.
BODY← The body of the manuscript should begin on a separate page. The manuscript page
header (if used) and page number should appear in the upper right corner. Type the title of the paper centered at the top of the page, add a hard return, and then begin the text using the format noted above. The body should contain:
← Introduction (The introduction has no label.)← Methods (Center the heading. Use un-centered subheadings such as: Participants,
Materials, Procedure.)← Results (Center the heading.)← Discussion (Center the heading)
HEADINGSPlease use no more than three levels of displayed headings.
Level 1: Centered
Level 2: Centered Italicized
Level 3: Flush left, Italicized
FOOTNOTESCenter the label “Footnotes” at the top of a separate page. Footnotes can be used to give additional information, which may include the citation of a reference included in the reference list. They should not consist solely of a reference citation, and they should never include the bibliographic details of a reference. They should also not contain any figures or tables.
Footnotes to the text are numbered consecutively; those to tables should be indicated by superscript lower-case letters (or asterisks for significance values and other statistical data). Footnotes to the title or the authors of the article are not given reference symbols.
Always use footnotes instead of endnotes. Type all content footnotes and copyright permission footnotes together, double-spaced, and numbered consecutively in the order they appear in the article. Indent the first line of each footnote 5-7 spaces. The number of the footnote should correspond to the number in the text. Superscript arabic numerals are used to indicate the text material being footnoted.
AUTHOR NOTEThe first paragraph contains a separate phrase for each author’s name and the affiliations of the authors at the time of the study (include region and country).
The second paragraph identifies any changes in the author affiliation subsequent to the time of
64
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
the study and includes region and country (wording: “authors name is now at affiliation”.)
The third paragraph is Acknowledgments. It identifies grants or other financial support and the source, if appropriate. It is also the place to acknowledge colleagues who assisted in the study and to mention any special circumstances such as the presentation of a version of the paper at a meeting, or its preparation from a doctoral dissertation, or the fact that it is based on an earlier study.
The fourth paragraph states, “Correspondence concerning this article should be addressed to…” and includes the full address, telephone number and email address of the corresponding author.
TERMINOLOGY← Please always use internationally accepted signs and symbols for units (SI units).←SCIENTIFIC STYLE← Generic names of drugs and pesticides are preferred; if trade names are used, the
generic name should be given at first mention.← Please use the standard mathematical notation for formulae, symbols etc.:Italic for
single letters that denote mathematical constants, variables, and unknown quantities Roman/upright for numerals, operators, and punctuation, and commonly defined functions or abbreviations, e.g., cos, det, e or exp, lim, log, max, min, sin, tan, d (for derivative) Bold for vectors, tensors, and matrices.
←REFERENCESCitationCite references in the text by name and year in parentheses. Some examples:
← Negotiation research spans many disciplines (Thompson 1990).← This result was later contradicted by Becker and Seligman (1996).← This effect has been widely studied (Abbott 1991; Barakat et al. 1995; Kelso and
Smith 1998; Medvec et al. 1999).
Reference listThe list of references should only include works that are cited in the text and that have been published or accepted for publication. Personal communications and unpublished works should only be mentioned in the text. Do not use footnotes or endnotes as a substitute for a reference list.
Reference list entries should be alphabetized by the last names of the first author of each work.
← Journal articleHarris, M., Karper, E., Stacks, G., Hoffman, D., DeNiro, R., Cruz, P., et al. (2001). Writing labs and the Hollywood connection. Journal of Film Writing, 44(3), 213–245.
← Article by DOI Slifka, M. K., & Whitton, J. L. (2000) Clinical implications of dysregulated cytokine production. Journal of Molecular Medicine, https://doi.org/10.1007/s001090000086
← BookCalfee, R. C., & Valencia, R. R. (1991). APA guide to preparing
65
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
manuscripts for journal publication. Washington, DC: American Psychological Association.
← Book chapterO’Neil, J. M., & Egan, J. (1992). Men’s and women’s gender role journeys: Metaphor for healing, transition, and transformation. In B. R. Wainrib (Ed.), Gender issues across the life cycle (pp. 107–123). New York: Springer.
← Online documentAbou-Allaban, Y., Dell, M. L., Greenberg, W., Lomax, J., Peteet, J., Torres, M., & Cowell, V. (2006). Religious/spiritual commitments and psychiatric practice. Resource document. American Psychiatric Association. http://www.psych.org/edu/other_res/lib_archives/archives/200604.pdf. Accessed 25 June 2007.
Journal names and book titles should be italicized.
For authors using EndNote, Springer provides an output style that supports the formatting of in-text citations and reference list.← EndNote style (zip, 3 kB)
TABLES← All tables are to be numbered using Arabic numerals.← Tables should always be cited in text in consecutive numerical order. ← For each table, please supply a table caption (title) explaining the components of
the table.← Identify any previously published material by giving the original source in the
form of a reference at the end of the table caption.← Footnotes to tables should be indicated by superscript lower-case letters (or
asterisks for significance values and other statistical data) and included beneath the table body.
Each table should be inserted on a separate page at the back of the manuscript in the order noted above. A call-out for the correct placement of each table should be included in brackets within the text immediately after the phrase in which it is first mentioned. Copyright permission footnotes for tables are typed as a table note.ARTWORK AND ILLUSTRATIONS GUIDELINES
Electronic Figure Submission← Supply all figures electronically.← Indicate what graphics program was used to create the artwork.← For vector graphics, the preferred format is EPS; for halftones, please use TIFF
format. MSOffice files are also acceptable.← Vector graphics containing fonts must have the fonts embedded in the files.← Name your figure files with "Fig" and the figure number, e.g., Fig1.eps.Line Art
66
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
← Definition: Black and white graphic with no shading.← Do not use faint lines and/or lettering and check that all lines and lettering within
the figures are legible at final size.← All lines should be at least 0.1 mm (0.3 pt) wide.← Scanned line drawings and line drawings in bitmap format should have a
minimum resolution of 1200 dpi.← Vector graphics containing fonts must have the fonts embedded in the files.
Halftone Art
← Definition: Photographs, drawings, or paintings with fine shading, etc.← If any magnification is used in the photographs, indicate this by using scale bars
within the figures themselves.← Halftones should have a minimum resolution of 300 dpi.←Combination Art
← Definition: a combination of halftone and line art, e.g., halftones containing line drawing, extensive lettering, color diagrams, etc.
← Combination artwork should have a minimum resolution of 600 dpi.
Color Art← Color art is free of charge for online publication.← If black and white will be shown in the print version, make sure that the main
information will still be visible. Many colors are not distinguishable from one another when converted to black and white. A simple way to check this is to make a xerographic copy to see if the necessary distinctions between the different colors are still apparent.
← If the figures will be printed in black and white, do not refer to color in the
67
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
captions.← Color illustrations should be submitted as RGB (8 bits per channel).
Figure Lettering← To add lettering, it is best to use Helvetica or Arial (sans serif fonts).← Keep lettering consistently sized throughout your final-sized artwork, usually
about 2–3 mm (8–12 pt).← Variance of type size within an illustration should be minimal, e.g., do not use 8-
pt type on an axis and 20-pt type for the axis label.← Avoid effects such as shading, outline letters, etc.← Do not include titles or captions within your illustrations.
Figure Numbering← All figures are to be numbered using Arabic numerals.← Figures should always be cited in text in consecutive numerical order.← Figure parts should be denoted by lowercase letters (a, b, c, etc.).← If an appendix appears in your article and it contains one or more figures,
continue the consecutive numbering of the main text. Do not number the appendix figures,"A1, A2, A3, etc." Figures in online appendices (Electronic Supplementary Material) should, however, be numbered separately.
←Figure Captions← Each figure should have a concise caption describing accurately what the figure
depicts. Include the captions in the text file of the manuscript, not in the figure file.← Figure captions begin with the term Fig. in bold type, followed by the figure
number, also in bold type.← No punctuation is to be included after the number, nor is any punctuation to be
placed at the end of the caption.← Identify all elements found in the figure in the figure caption; and use boxes,
circles, etc., as coordinate points in graphs.← Identify previously published material by giving the original source in the form of
a reference citation at the end of the figure caption.←Figure Placement and Size← Figures should be submitted separately from the text, if possible.← When preparing your figures, size figures to fit in the column width.← For most journals the figures should be 39 mm, 84 mm, 129 mm, or 174 mm wide
and not higher than 234 mm.← For books and book-sized journals, the figures should be 80 mm or 122 mm wide
and not higher than 198 mm.←PermissionsIf you include figures that have already been published elsewhere, you must obtain permission from the copyright owner(s) for both the print and online format. Please be aware that some publishers do not grant electronic rights for free and that Springer will not be able to refund any costs that may have occurred to receive these permissions. In such cases, material from other
68
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
sources should be used.
AccessibilityIn order to give people of all abilities and disabilities access to the content of your figures, please make sure that
← All figures have descriptive captions (blind users could then use a text-to-speech software or a text-to-Braille hardware)
← Patterns are used instead of or in addition to colors for conveying information (colorblind users would then be able to distinguish the visual elements)
← Any figure lettering has a contrast ratio of at least 4.5:1
FIGURE CAPTION SHEETThe figure caption sheet contains a list of only the captions for all figures used. Center the label "Figure Captions" in uppercase and lowercase letters at the top of the page. Begin each caption entry flush left, and type the word "Figure", followed by the appropriate number and a period, all in italics. In the text of the caption (not italicized), capitalize only the first word and any proper nouns. If the caption is more than one line, double-space between the lines, and type the second and subsequent lines flush left. Table notes: Copyright permission footnotes for figures are typed as part of the figure caption.← Each figure should appear on a separate page. The page where the figure is found
should have the figure number and the word "top"[ie, Figure 1 top] typed above the figure. Figures or illustrations (photographs, drawings, diagrams, and charts) are to be numbered in one consecutive series of arabic numerals. Figures may be embedded in the text of a Word or Wordperfect document. Electronic artwork submitted on disk may be in the TIFF, EPS or Powerpoint format (best is 1200 dpi for line and 300 dpi for half-tones and gray-scale art). Color art should be in the CYMK color space. Assistance will be provided by the system administrator if you do not have electronic files for figures; originals of artwork may be sent to the system administrator to be uploaded. *** After first mention in the body of the manuscript, a call-out for the correct placement of each figure should be included in brackets on a separate line within the text.
ELECTRONIC SUPPLEMENTARY MATERIALSpringer accepts electronic multimedia files (animations, movies, audio, etc.) and other supplementary files to be published online along with an article or a book chapter. This feature can add dimension to the author's article, as certain information cannot be printed or is more convenient in electronic form.
Before submitting research datasets as electronic supplementary material, authors should read the journal’s Research data policy. We encourage research data to be archived in data repositories wherever possible.
Submission← Supply all supplementary material in standard file formats.← Please include in each file the following information: article title, journal name,
author names; affiliation and e-mail address of the corresponding author.← To accommodate user downloads, please keep in mind that larger-sized files may
69
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
require very long download times and that some users may experience other problems during downloading.
←Audio, Video, and Animations← Aspect ratio: 16:9 or 4:3← Maximum file size: 25 GB← Minimum video duration: 1 sec← Supported file formats: avi, wmv, mp4, mov, m2p, mp2, mpg, mpeg, flv, mxf,
mts, m4v, 3gp←Text and Presentations← Submit your material in PDF format; .doc or .ppt files are not suitable for long-
term viability.← A collection of figures may also be combined in a PDF file.←Spreadsheets← Spreadsheets should be submitted as .csv or .xlsx files (MS Excel).
Specialized Formats← Specialized format such as .pdb (chemical), .wrl (VRML), .nb (Mathematica
notebook), and .tex can also be supplied.
Collecting Multiple Files← It is possible to collect multiple files in a .zip or .gz file.
Numbering← If supplying any supplementary material, the text must make specific mention of
the material as a citation, similar to that of figures and tables.← Refer to the supplementary files as “Online Resource”, e.g., "... as shown in the
animation (Online Resource 3)", “... additional data are given in Online Resource 4”.← Name the files consecutively, e.g. “ESM_3.mpg”, “ESM_4.pdf”.←Captions← For each supplementary material, please supply a concise caption describing the
content of the file.
Processing of supplementary files← Electronic supplementary material will be published as received from the author
without any conversion, editing, or reformatting.←AccessibilityIn order to give people of all abilities and disabilities access to the content of your supplementary files, please make sure that
← The manuscript contains a descriptive caption for each supplementary material← Video files do not contain anything that flashes more than three times per second
70
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
(so that users prone to seizures caused by such effects are not put at risk)
ETHICAL RESPONSIBILITIES OF AUTHORSThis journal is committed to upholding the integrity of the scientific record. As a member of the Committee on Publication Ethics (COPE) the journal will follow the COPE guidelines on how to deal with potential acts of misconduct.
Authors should refrain from misrepresenting research results which could damage the trust in the journal, the professionalism of scientific authorship, and ultimately the entire scientific endeavour. Maintaining integrity of the research and its presentation can be achieved by following the rules of good scientific practice, which include:
← The manuscript has not been submitted to more than one journal for simultaneous consideration.
← The manuscript has not been published previously (partly or in full), unless the new work concerns an expansion of previous work (please provide transparency on the re-use of material to avoid the hint of text-recycling (“self-plagiarism”)).
← A single study is not split up into several parts to increase the quantity of submissions and submitted to various journals or to one journal over time (e.g. “salami-publishing”).
← No data have been fabricated or manipulated (including images) to support your conclusions
← No data, text, or theories by others are presented as if they were the author’s own (“plagiarism”). Proper acknowledgements to other works must be given (this includes material that is closely copied (near verbatim), summarized and/or paraphrased), quotation marks are used for verbatim copying of material, and permissions are secured for material that is copyrighted. Important note: the journal may use software to screen for plagiarism.
← Consent to submit has been received explicitly from all co-authors, as well as from the responsible authorities - tacitly or explicitly - at the institute/organization where the work has been carried out, before the work is submitted.
← Authors whose names appear on the submission have contributed sufficiently to the scientific work and therefore share collective responsibility and accountability for the results.
← Authors are strongly advised to ensure the correct author group, corresponding author, and order of authors at submission. Changes of authorship or in the order of authors are not accepted after acceptance of a manuscript.
← Adding and/or deleting authors and/or changing the order of authors at revision stage may be justifiably warranted. A letter must accompany the revised manuscript to explain the reason for the change(s) and the contribution role(s) of the added and/or deleted author(s). Further documentation may be required to support your request.
← Requests for addition or removal of authors as a result of authorship disputes after acceptance are honored after formal notification by the institute or independent body and/or when there is agreement between all authors.
← Upon request authors should be prepared to send relevant documentation or data in order to verify the validity of the results. This could be in the form of raw data, samples, records, etc. Sensitive information in the form of confidential proprietary data is
71
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
excluded.
If there is a suspicion of misconduct, the journal will carry out an investigation following the COPE guidelines. If, after investigation, the allegation seems to raise valid concerns, the accused author will be contacted and given an opportunity to address the issue. If misconduct has been established beyond reasonable doubt, this may result in the Editor-in-Chief’s implementation of the following measures, including, but not limited to:← If the article is still under consideration, it may be rejected and returned to the
author.← If the article has already been published online, depending on the nature and
severity of the infraction, either an erratum will be placed with the article or in severe cases complete retraction of the article will occur. The reason must be given in the published erratum or retraction note. Please note that retraction means that the paper is maintained on the platform, watermarked "retracted" and explanation for the retraction is provided in a note linked to the watermarked article.
← The author’s institution may be informed.←COMPLIANCE WITH ETHICAL STANDARDS
To ensure objectivity and transparency in research and to ensure that accepted principles of ethical and professional conduct have been followed, authors should include information regarding sources of funding, potential conflicts of interest (financial or non-financial), informed consent if the research involved human participants, and a statement on welfare of animals if the research involved animals.
Authors should include the following statements (if applicable) in a separate section entitled “Compliance with Ethical Standards” when submitting a paper:
← Disclosure of potential conflicts of interest← Research involving Human Participants and/or Animals← Informed consent
Please note that standards could vary slightly per journal dependent on their peer review policies (i.e. single or double blind peer review) as well as per journal subject discipline. Before submitting your article check the instructions following this section carefully.
The corresponding author should be prepared to collect documentation of compliance with ethical standards and send if requested during peer review or after publication.
The Editors reserve the right to reject manuscripts that do not comply with the above-mentioned guidelines. The author will be held responsible for false statements or failure to fulfill the above-mentioned guidelines.
DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST
72

PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Authors must disclose all relationships or interests that could influence or bias the work. Although an author may not feel there are conflicts, disclosure of relationships and interests affords a more transparent process, leading to an accurate and objective assessment of the work. Awareness of real or perceived conflicts of interests is a perspective to which the readers are entitled and is not meant to imply that a financial relationship with an organization that sponsored the research or compensation for consultancy work is inappropriate. Examples of potential conflicts of interests that are directly or indirectly related to the research may include but are not limited to the following:
← Research grants from funding agencies (please give the research funder and the grant number)
← Honoraria for speaking at symposia← Financial support for attending symposia← Financial support for educational programs← Employment or consultation← Support from a project sponsor← Position on advisory board or board of directors or other type of management
relationships← Multiple affiliations← Financial relationships, for example equity ownership or investment interest← Intellectual property rights (e.g. patents, copyrights and royalties from such
rights)← Holdings of spouse and/or children that may have financial interest in the work
In addition, interests that go beyond financial interests and compensation (non-financial interests) that may be important to readers should be disclosed. These may include but are not limited to personal relationships or competing interests directly or indirectly tied to this research, or professional interests or personal beliefs that may influence your research.
The corresponding author collects the conflict of interest disclosure forms from all authors. In author collaborations where formal agreements for representation allow it, it is sufficient for the corresponding author to sign the disclosure form on behalf of all authors. Examples of forms can be found← here:
The corresponding author will include a summary statement on the title page that is separate from their manuscript, that reflects what is recorded in the potential conflict of interest disclosure form(s).
See below examples of disclosures:
Funding: This study was funded by X (grant number X).
Conflict of Interest: Author A has received research grants from Company A. Author B has received a speaker honorarium from Company X and owns stock in Company Y. Author C is a
73
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
member of committee Z.
If no conflict exists, the authors should state:
Conflict of Interest: The authors declare that they have no conflict of interest.
RESEARCH INVOLVING HUMAN PARTICIPANTS AND/OR ANIMALS
1) Statement of human rightsWhen reporting studies that involve human participants, authors should include a statement that the studies have been approved by the appropriate institutional and/or national research ethics committee and have been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
If doubt exists whether the research was conducted in accordance with the 1964 Helsinki Declaration or comparable standards, the authors must explain the reasons for their approach, and demonstrate that the independent ethics committee or institutional review board explicitly approved the doubtful aspects of the study.
The following statements should be included in the text before the References section:
Ethical approval: “All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.”
For retrospective studies, please add the following sentence:
“For this type of study formal consent is not required.”
2) Statement on the welfare of animalsThe welfare of animals used for research must be respected. When reporting experiments on animals, authors should indicate whether the international, national, and/or institutional guidelines for the care and use of animals have been followed, and that the studies have been approved by a research ethics committee at the institution or practice at which the studies were conducted (where such a committee exists).
For studies with animals, the following statement should be included in the text before the References section:
Ethical approval: “All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.”
If applicable (where such a committee exists): “All procedures performed in studies involving animals were in accordance with the ethical standards of the institution or practice at which the studies were conducted.”
74
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
If articles do not contain studies with human participants or animals by any of the authors, please select one of the following statements:
“This article does not contain any studies with human participants performed by any of the authors.”
“This article does not contain any studies with animals performed by any of the authors.”
“This article does not contain any studies with human participants or animals performed by any of the authors.”
INFORMED CONSENT
All individuals have individual rights that are not to be infringed. Individual participants in studies have, for example, the right to decide what happens to the (identifiable) personal data gathered, to what they have said during a study or an interview, as well as to any photograph that was taken. Hence it is important that all participants gave their informed consent in writing prior to inclusion in the study. Identifying details (names, dates of birth, identity numbers and other information) of the participants that were studied should not be published in written descriptions, photographs, and genetic profiles unless the information is essential for scientific purposes and the participant (or parent or guardian if the participant is incapable) gave written informed consent for publication. Complete anonymity is difficult to achieve in some cases, and informed consent should be obtained if there is any doubt. For example, masking the eye region in photographs of participants is inadequate protection of anonymity. If identifying characteristics are altered to protect anonymity, such as in genetic profiles, authors should provide assurance that alterations do not distort scientific meaning.
The following statement should be included:
Informed consent: “Informed consent was obtained from all individual participants included in the study.”
If identifying information about participants is available in the article, the following statement should be included:
“Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.”
ENGLISH LANGUAGE EDITINGFor editors and reviewers to accurately assess the work presented in your manuscript you need to ensure the English language is of sufficient quality to be understood. If you need help with writing in English you should consider:
← Asking a colleague who is a native English speaker to review your manuscript for clarity.
75
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
← Visiting the English language tutorial which covers the common mistakes when writing in English.
← Using a professional language editing service where editors will improve the English to ensure that your meaning is clear and identify problems that require your review. Two such services are provided by our affiliates Nature Research Editing Service and American Journal Experts. Springer authors are entitled to a 10% discount on their first submission to either of these services, simply follow the links below.
← English language tutorial← Nature Research Editing Service← American Journal Experts
Please note that the use of a language editing service is not a requirement for publication in this journal and does not imply or guarantee that the article will be selected for peer review or accepted.
If your manuscript is accepted it will be checked by our copyeditors for spelling and formal style before publication.
RESEARCH DATA POLICYThe journal encourages authors, where possible and applicable, to deposit data that support the findings of their research in a public repository. Authors and editors who do not have a preferred repository should consult Springer Nature’s list of repositories and research data policy.← List of Repositories← Research Data Policy
General repositories - for all types of research data - such as figshare and Dryad may also be used.
Datasets that are assigned digital object identifiers (DOIs) by a data repository may be cited in the reference list. Data citations should include the minimum information recommended by DataCite: authors, title, publisher (repository name), identifier.← DataCite
Springer Nature provides a research data policy support service for authors and editors, which can be contacted at [email protected] service provides advice on research data policy compliance and on finding research data repositories. It is independent of journal, book and conference proceedings editorial offices and does not advise on specific manuscripts.← Helpdesk
AFTER ACCEPTANCEUpon acceptance of your article you will receive a link to the special Author Query Application at Springer’s web page where you can sign the Copyright Transfer Statement online and indicate whether you wish to order OpenChoice, offprints, or printing of figures in color.
Once the Author Query Application has been completed, your article will be processed and you will receive the proofs.
76
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Copyright transferAuthors will be asked to transfer copyright of the article to the Publisher (or grant the Publisher exclusive publication and dissemination rights). This will ensure the widest possible protection and dissemination of information under copyright laws.
← Creative Commons Attribution-NonCommercial 4.0 International License
OffprintsOffprints can be ordered by the corresponding author.
Color illustrationsOnline publication of color illustrations is free of charge. For color in the print version, authors will be expected to make a contribution towards the extra costs.
Proof readingThe purpose of the proof is to check for typesetting or conversion errors and the completeness and accuracy of the text, tables and figures. Substantial changes in content, e.g., new results, corrected values, title and authorship, are not allowed without the approval of the Editor.
After online publication, further changes can only be made in the form of an Erratum, which will be hyperlinked to the article.
Online FirstThe article will be published online after receipt of the corrected proofs. This is the official first publication citable with the DOI. After release of the printed version, the paper can also be cited by issue and page numbers.
OPEN CHOICEIn addition to the normal publication process (whereby an article is submitted to the journal and access to that article is granted to customers who have purchased a subscription), Springer provides an alternative publishing option: Springer Open Choice. A Springer Open Choice article receives all the benefits of a regular subscription-based article, but in addition is made available publicly through Springer’s online platform SpringerLink.
Copyright and license term – CC BYOpen Choice articles do not require transfer of copyright as the copyright remains with the author. In opting for open access, the author(s) agree to publish the article under the Creative Commons Attribution License.← Find more about the license agreement
AUTHORS' CONTRIBUTIONSTo give appropriate credit to each author of a paper, the individual contributions of authors to the manuscript should be specified in this section.
An "author" is generally considered to be someone who has made substantive intellectual
77
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
contributions to a published study. To qualify as an author one should 1) have made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) have been involved in drafting the manuscript or revising it critically for important intellectual content; and 3) have given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. Acquisition of funding, collection of data, or general supervision of the research group, alone, does not justify authorship.
We suggest the following kind of format (please use initials to refer to each author's contribution): AB conceived of the study, participated in its design and coordination and drafted the manuscript; JY participated in the design and interpretation of the data; MT participated in the design and coordination of the study and performed the measurement; ES participated in the design of the study and performed the statistical analysis; FG conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
All contributors who do not meet the criteria for authorship should be listed in an acknowledgements section. Examples of those who might be acknowledged include a person who provided purely technical help, writing assistance, or a department chair who provided only general support.
NOTE: Because the Journal of Autism and Developmental Disorders operates double-blind peer review, the Authors' contributions section should be uploaded as part of the acknowledgment file, and not included in the main manuscript file.
Retrieved from http://www.springer.com/psychology/child+%26+school+psychology/journal/10803?print_view=true&detailsPage=pltci_3161162
78
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix B: Online Post for Internet Forums and Study Poster
Post for online forums:
I am a trainee clinical psychologist at the University of Surrey looking for parents of girls with an Autistic Spectrum Disorder (ASD) to take part in a study. I’m interested in understanding why it takes longer for girls to receive a diagnosis of ASD than boys, by exploring parent’s thoughts and stories about the ‘lead up’ to their daughter’s first clinic visit.
Please let me know if you are interested in my study by contacting me by email on [email protected]
I have attached a copy of the flyer and would be happy to answer any questions.
This study has been reviewed and received a favourable ethical opinion from the University of Surrey FHMS Ethics Committee.
79
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
80
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix C: Details of Recruitment Process
The researcher searched on Facebook for local ASC support groups such as those
affiliated with the National Autistic Society and posted the advert on these support group pages.
The researcher also shared the study on their Facebook profile and encouraged others to share
the post. The post was shared by friends of the researcher and onwards by friends of friends. The
study was also advertised on the National Autistic Society research webpage, however all the
participants who took part in the study said that they found the advert on Facebook. All
participants who took part in the study lived in the United Kingdom.
81
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
/Appendix D: Participant Information Sheet
Participant Information Sheet[November 2017, Version 2]
PROJECT TITLE: How do parents come to understand that their daughter has an autistic spectrum condition?
IntroductionI am a Trainee Clinical Psychologist from the University of Surrey and I am conducting a research study as part of my clinical doctorate qualification. I will describe the study for you so that you can decide if you would like to take part. Please ask as many questions as you need to make sure you understand what is involved.
What is the purpose of the study?There is very little research exploring how parents come to understand that their daughter might have an autistic spectrum condition (sometimes called Autism). We would like to understand when and how they begin to notice that their child may not be like typical children, and how they come to seek advice and have their child assessed.
Why have I been invited to take part in the study?You have been invited to take part in this study because you have a daughter who has a diagnosis of ASD without cognitive impairment (sometimes called learning disability) and I am interested in hearing your personal story in relation to your daughter before her diagnosis. Between five and eight participants will take part in this study.
Do I have to take part?No, you do not have to participate and it is your choice if you want to be involved. If you agree to take part, you can chose not to answer all of the questions in the interview. You are also free to withdraw without giving a reason, either during the interview or at any time after it up until two weeks have passed. At that time I will have already begun to analyse the interview.
What will my involvement require?If you agree to take part, you will take part in an interview with me. This interview will take place at a convenient location for you. If we are unable to meet face to face, it may be possible for us to conduct the interview over Skype, Zoom or FaceTime. You will be asked to sign a consent form before the interview starts. If we are doing the interview online, you will be required to email or mail me this consent form before the interview.
During the interview you will be asked questions which will give you the opportunity to tell your story about how you came to realise that your daughter may not be like typical children and how you came to seek advice and have her assessed, including the very first things that you noticed. The interview could last any length of time, depending on how long you want to talk for. It is imagined that the interview will last about an hour, however it may go on longer than this if you wish.
Page 1 of 3
82
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Will my taking part in the study be kept confidential?Yes. Your interview (the ‘data’) will be stored securely in accordance with the UK Data Protection Act (1998). This means that all information that is collected including information from the interviews will be kept confidential. Personal identifiable information (such as your name and any other information that make it possible to identify you) will be changed or “anonymised”. The recordings will be stored securely until they have been anonymised. Anonymised transcripts may be included within my final thesis and retained for 10 years in line with university policy.
Information would only be shared in an instance where I believe that you or another person could be at significant risk of harm.
What will happen to information that I provide?The interview will be recorded on a digital audio recorder so that I can transcribe (write down) what you have said and analyse it after the interview. A professional transcriber may be used if you provide consent for this. All names will be changed and identifying information will be removed from these written versions. The professional transcriber will be required to sign a confidentiality agreement to ensure information in the recording remains confidential. Once transcription is completed the professional transcriber will be required to delete their copies of the written transcription and the audio-recording file. The transcriber will be required to act in accordance with Data Protection Act 1998, maintain confidentiality and store data securely and anonymously. Only myself, my supervisors and other researchers supporting the research will have access to the audio-recordings and written interviews after transcription. Your recordings will be copied on to an encrypted hard drive within 24 hours of the interview.
With your consent, to make the most of your participation and support efficient advancements in science, your anonymised interviews could also be used for future research. We cannot tell you at this moment in time what this research will entail or what analyses will be carried out but we can assure you that all appropriate legal, ethical and other approvals will be in place. For practical reasons your consent would not be sought again. Your data will not be used for commercial purposes.
Will I be paid my expenses?You will be reimbursed for reasonable travel expenses you incur to attend the interview. These will be paid on production of a receipt or a reasonable mileage given, and paid at a standard mileage rate.
What are the possible disadvantages or risks of taking part?Conversations about family members may sometimes bring up emotions that may make you upset during the interview. Your welfare is our priority and therefore if you become distressed the interview can be stopped. I will also make sure that you have details of how to access support if you would like these.
What are the possible benefits of taking part?Some people think that the process of telling their story can be therapeutic, so it is possible that the interview could be a helpful experience for you.
Page 2 of 3
83
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
/It is hoped that the research will help us to understand any differences between boys and girls in getting a diagnosis. Early diagnosis and intervention is known to have a positive impact on those diagnosed with ASD and their families.
What happens when the research study stops?The study will be running between July and November 2017 so that lots of people have an opportunity to participate. Once the study stops, all the data will be analysed and written up as part of my doctoral thesis. If you take part, you can ask me to inform you of the results once it’s completed in 2018.
What if there is a problem?If you have any concerns or complaints about the way in which you have been treated during the research you can contact me or my supervisor:
Natalie Kseib (Principle Investigator): [email protected] Kate Gleeson (Supervisor): [email protected] .
School of Psychology AD BuildingUniversity of SurreyGuildfordGU2 7XH
Telephone: 01483689436
Below is a list of organisations that can also provide you with further support:
National Autistic SocietyHelpline for Advice and support Tel: 0808 800 4104Website: http://www.autism.org.uk/
Carers UKAdvice line and local group meetingsTel: 0808 808 7777Website: https://www.carersuk.org
In addition to the organisations listed above, you can contact your GP for further advice and support.
Who has reviewed the project?This research has been looked at by an independent group of people, called an Ethics Committee, to protect your interests. This study has been reviewed by and received a Favourable Ethical Opinion from University of Surrey Faculty of Health and Medical Sciences Ethics Committee.
Thank you for taking the time to read this Information Sheet
Page 3 of 3
84
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix E: Consent Form
Consent Form[November 2017, Version 2]
Please initial each box
I have read and understood the Information Sheet provided (Version 2, March 2017). I have been given a full explanation by the investigator of the nature, purpose, location and likely duration of the study, and of what I will be expected to do.
I have been given the opportunity to ask questions on all aspects of the study and have understood the advice and information given as a result.
I agree for my anonymised data (as outlined in the accompanying information sheet) to be used for this study
I give consent to the interview to be audio recorded
I give consent to anonymous verbatim (exactly your words) quotations being used in reports
I understand that all data is held and processed in the strictest confidence and in accordance with the UK Data Protection Act (1998). I understand that confidentiality will only be broken in the event of a significant risk and that this would be discussed with me.
I understand that I am free to withdraw from the study at any time without needing to justify my decision, without prejudice.
/I confirm that I have read and understood the above and freely consent to participating in this study. I have been given adequate time to consider my participation.
/I understand and agree that the recording will be transcribed into a written copy by a professional transcriber and all information will be recorded anonymously. The professional transcriber will be required to sign a non-disclosure agreement to ensure the information in your recording remains confidential. The transcriber will delete all written copies of the transcription and the audio-recording file when transcription is completed.
Optional
//I agree for my anonymised data to be used for future research that will have received all relevant legal, professional and ethical approvals.
Name of participant (BLOCK CAPITALS) .............................................
Signed ...............................................
Date ...............................................
University of Surrey – RIGO v.10 - 14 July 2015
Page 1 of 2When completed: 1 for participant; 1 for researcher site file.
85
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Name of researcher taking consent ……......................................(BLOCK CAPITALS)
Signed ...........................................
Date ...........................................
University of Surrey – RIGO v.10 - 14 July 2015
Page 2 of 2When completed: 1 for participant; 1 for researcher site file.
86
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix F: Interview Schedule
Interview Guide
Thank you for agreeing to take part in this interview today. As we have discussed, I am completing this research as part of my Doctorate in Clinical Psychology at the University of Surrey. This interview is being recorded and will be later transcribed; any personal or identifiable information in these transcriptions will be changed. I would like to remind you that you can stop the interview at any point if you don’t wish to continue. If you want to withdraw your interview data, you can contact me within two weeks of the interview and I will destroy the recording and the transcript. If there are any questions that you would prefer not to answer, please say so.
Demographic information:Daughter’s date of birth:Date of autism diagnosis:Others living at home:Other children:
In a moment I will be asking you to tell your journey of coming to recognise your daughter’s behaviour as unusual or requiring attention by professionals. There will also be a series of prompt questions that I may use throughout the interview to guide the process.
Question:I would like you to start by telling me about your personal story of how you came to realise that X may not be like typical children, including the very first things that you noticed and how you came to seek advice and have X assessed. Please feel free to tell your story in whatever way you wish and begin the story when you feel comfortable.
Areas that I will be sensitised to: Comparisons – whether, how and between who are they made? Behaviours – why and when seen as unusual Ideas of concept of Autism Who talked to How things are explained/ made sense of Expectations (especially in relation to gender) Others involved
Prompt questions to elaborate: You mentioned… Can you tell me about that? Your experience of … sounds really interesting, would you mind expanding on that? Could you give me an example? What happened next? Can you tell me about what X is like?
87
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix G: Criteria for Good Quality Qualitative Research
1. Sensitivity to context: The research question was developed after a review of the
literature, prior to the study commencing. A reflective diary was kept throughout the
process to ensure that context and wider societal narratives were considered in line with
the epistemological position. I used the diary to explore and reflect on my relationship
with the research (including the impact of it on my beliefs about autism), the process of
carrying out the research, and the participants and their stories.
2. Commitment and rigour: A process was followed in relation to data collection and
analysis over a ten-month period in order to fully engage with the data and reflect
between each stage. Time restraints meant that a professional transcriber was used for
three transcripts but I made sure that I listened to these, as well as the two that were
personally transcribed, whilst reading and checking the transcripts several times. This
listening and re-reading of each transcript allowed for an immersion in the data. I took a
methodical stepped approach to the analysis to demonstrate academic rigour. All
transcripts and analysis were reviewed by supervisors and discussed, before being
reanalysed. Furthermore, peer supervision was attended as a space to reflect on the
research.
3. Transparency and coherence: Extracts from transcripts and analysis and the reflective
journal are included in the appendix to enhance transparency by allowing the reader to
discern and identify patterns. Quotes from the interviews are provided to evidence
interpretations. I attended supervision with two experienced qualitative researchers, one
88
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
of whose area of expertise is in autism as well as peer supervision with a group of fellow
Trainee Clinical Psychologists using qualitative methodology. In peer group supervision,
we reflected on the process of using qualitative analysis and explored the impact of our
beliefs and values on the collection and analysis of data. A fellow member of this group
also analysed an extract of a transcript and similarities and differences in our analyses
and interpretations were discussed. Myself and my peer observed similar themes in the
data, with some differences which were understood by the impact of reading the
transcript for the first time versus having conducted and transcribed the interview.
4. Impact and importance: A gap in our current knowledge was identified and the study
aims to contribute a unique understanding of our interpretations of behaviour. It is also
hoped that findings will be disseminated to other professionals in the field through
publication.
89
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix H: Evidence of Ethical Approval
/
90
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix I: Risk Assessment
Risk Assessment for Study : What are the processes by which parents and caregivers of females with Autistic Spectrum Disorder (ASD) without cognitive impairment come to understand their child’s behaviours as requiring intervention?Version: 1 Date: 13/03/2017Relevant Local SOPs and local risk assessments (add all relevant SOPs and risk assessments that apply to your study)
1. SOP/risk assessment ref #: 1. Title and Expiry date: dd/mm/yyyy
Consideration Person at Risk
Scale of Risk Existing Protocols/SOPs/risk assessments
Additional Mechanisms (specific
to the study)
State the risk, e.g .lone working, data storage, confidentiality …
Participant and / or Researcher
Low / Medium / High
What is currently in place to mitigate this risk?
Is there anything in addition to the existing protocols that can be done to mitigate this risk?
Lone working. Safety of the researcher when conducting interviews alone in community locations such as the participant’s home.
Researcher Low
University of Surrey Health & Safety policies (lone working). I will share my schedule of appointments and contact addresses with my supervisors. I will also inform someone of my whereabouts before going to an interview and will agree to call that person following the interview to confirm that I am safe. I will also carry my mobile and establish a call in procedure with that person if a situation arises in which I feel unsafe.
Participant becoming distressed during the interview. Conversations about family members could elicit difficult feelings.
Participant LowParticipants will be briefed before taking part in the study and any concerns that the participant has will be discussed. The interview has been designed to be as sensitive as possible and I will be alert to any potential distress during the interview. Participants will be reminded that they can refuse to answer questions and that the interview can be stopped at any time. I will also signpost participants for support (e.g. National Autistic
91
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Risk Assessment for Study : What are the processes by which parents and caregivers of females with Autistic Spectrum Disorder (ASD) without cognitive impairment come to understand their child’s behaviours as requiring intervention?Version: 1 Date: 13/03/2017Relevant Local SOPs and local risk assessments (add all relevant SOPs and risk assessments that apply to your study)
1. SOP/risk assessment ref #: 1. Title and Expiry date: dd/mm/yyyy
Consideration Person at Risk
Scale of Risk Existing Protocols/SOPs/risk assessments
Additional Mechanisms (specific
to the study)Society, carer groups) if they would like this.
Participant disclosing information which could indicate that harm could come to them or another person.
Participant and or others Low
The participant will be informed of confidentiality and its limits before taking part in the interview. If concerned about this risk during the interview, I would inform the participant of my concern and remind the participant of my duty to share the relevant information. I will be supervised throughout the process and any concerns will be discussed in supervision.
University of Surrey - Ethicsv.6 - December 2016
Please note: If you refer to a policy or a standard operating procedure (SOP) in your risk assessment, you will need to refer to this in your submission (e.g. include SOP reference number). Researchers should ensure that all guidance is removed from the template before submitting a completed risk assessment to the University Ethics Committee.
92
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Guidance: You will need to demonstrate awareness of all relevant SOPs and risk assessments that apply to your study and include their title, reference numbers and expiry dates. As part of your research proposal you need to assess any significant risks arising out of your proposed research. The scope of your risk assessment needs to consider the risk of harm to yourself or others as well as the risk to the research process e.g. loss of data, breach of confidentiality or loss of University reputation.SOP: A standard operating procedure (SOP) is a set of step-by-step instructions to be followed routinely for the performance of designated operations or activities.Researcher: consideration needs to be given to any significant risks to the researchers own health and wellbeing that could arise from the research project. Such risks could be due to the nature of the project e.g. distress, tiredness etc. Or as a direct result of working with certain types of equipment e.g. risks from machinery, sharps or exposure to hazardous agents such as radiation, noise etc. Having identified these risks, suitable control measures need to be taken to effectively mitigate the risk to an acceptable level in order that the work can proceed without detriment to either the researcher or the participants.Travel: research may involve travel to locations where the risk to individuals is adjudged to be higher than that in the UK. The University offers general health & safety and security advice to travellers in its travel guidance document. The most up to date travel security information from around the world can be obtained from the FCO (Foreign and Commonwealth Office) website. This information should be used to inform your assessment of the risk of travel to your proposed destination. The University uses a booking agent (Key Travel) to arrange flights and accommodation for business travellers, as part of the Key Travel service additional support is available should an emergency situation arise. The University Insurance website contains detailed information relating to insurance cover for business travellers. It is the individual’s responsibility to ensure sufficient insurance cover is in place before departure. The University Occupational Health service at the Robens Centre provides advice on the health risks associated with International travel.Lone working: researchers may be working alone in situations that pose additional risks e.g. conducting interviews in a participant’s home. These risks need to be mitigated with additional measures taken to safeguard the researcher. Such measures may include; sharing your schedule of appointments and contact addresses with a colleague, carrying a mobile phone with programmed speed dial numbers, established call in procedures, escalation process in the event of a failure to call in at an agreed time etc.Vulnerable groups: research can often involve the study of vulnerable groups, in which case the risk assessment would need to identify the protocols used to safeguard the researcher and the study group. Issues such as the consent process for vulnerable individuals, maintaining confidentiality of participants, the style of interview / questioning being used, if enhanced DBS checks are required for the researcher etc. need to be considered as part of the risk assessment. The researcher would also need to demonstrate an understanding of safeguarding in terms of the protocols governing their conduct during the research project.Participants Wellbeing: it is important to identify within the assessment any risks that the research may pose to the participants’ physical or mental wellbeing. As part of our duty of care to participants, it is important to have adequate controls in place to address foreseeable risks arising as a direct result of participation in the research study. Data Protection: the research process should provide adequate control over the integrity of the data gathered during the research project. There are however risks associated with the storage and use of research data that should be considered as part of the risk assessment process. Issues such as the loss or theft of data held
University of Surrey - Ethicsv.6 - December 2016
on a mobile storage device, corruption of data files, control of data transfer via open networks (the cloud), sharing data with research collaborators / private businesses and data protection should all be considered as part of the overall assessment.
93
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Research Samples: research is often supported by the taking and subsequent analysis of samples. These can range from physical samples of material through to biological samples taken from humans or animals. Samples that carry a risk of infection would require additional controls such as vaccinations and the use of Personal Protective Equipment (PPE) to be robustly implemented. Legislative controls e.g. HTA (Human Tissue Act) are in place that tightly control the taking and use of biological samples. Further controls exist to restrict the transportation of materials e.g. transport of dangerous goods legislation (ADR). Import / Export control licence restrictions may also apply to some categories of material being brought into the UK. Failure to adhere to any of these controls would not only jeopardise the research project but may also result in the prosecution of the University.
University of Surrey - Ethicsv.6 - December 2016
94
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix J: Extended Analysis
How Were Stories Told?
Genre
Two broad narratives emerged: one of a ‘Quest’ in overcoming resistance to be
believed (Ella, Emily and Helen) and one of a ‘Guided Journey’ in which the characters were
assisted by professionals (Tessa and Claire).
The ‘Quest’ narrative often included a moment of realisation, where signs come
together to ‘make sense’ as autism:
Emily: ‘I looked at the list and it was like a lightbulb moment where I ticked thirty out
of the forty things it just described her to a tee (sniffs)’
I chose this as a genre because there was a strong sense that once ‘seen’ the meaning
of behaviours could not be separated from the autism:
Emily: ‘Weird quirks become glaringly obvious signs’
The ‘seeing’ was followed by an emotional quest for the ‘truth’ in the form of a formal
diagnosis and to be legitimatised by others. Helen’s story took the listener through a timeline
of significant events, ending triumphantly with the ‘truth’ being found:
Helen: ‘It's really great that she was diagnosed now because she can now go forward
in secondary school with people understanding her true situation’.
Ella’s story was also identified within the ‘Quest’ narrative. There was an undertone
of desperation on her quest, for example in the acceptance of Obsessive Compulsive Disorder
diagnosis for Fiona, in order to obtain support:
95
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Ella: ‘…because they agreed to see her. I just thought well we’ll go with it’.
In this narrative Ella describes a battle to be held by Child and Adolescent Mental Health
Services:
Ella: ‘I didn’t want her discharged so we had this battle going on’.
And disbelief at the lack of care for her daughter, where professionals were framed as the
obstacles in the quest for support:
Ella: ‘I said “how bad does it have to get before you see her” and of course they
won’t tell you’.
The ‘Guided Journey’ narratives had a lighter tone. Claire and Tessa narrated
humorous scenes, inviting the listener to laugh:
Claire: ‘A teacher once said to her, "Abbie, I've got better things to do than stand here
while you go in the toilet and locking the door." And she says, "Well, just go
do them."’
Tessa: ‘I had watched Super Nanny, I know what I'm doing, I put her back in bed,
don't talk to her, don't make eye contact just put her back in bed and she'll be
fine. And every single thing - we had a baby-gate at the top of the stairs so she
couldn't come down the stairs -- every single thing out of her bedroom came
over the stairs, including her mattress. And she sat with all at the bottom of
the stairs, I was like, "This never happened to the Super Nanny."’
This observational humour perhaps allowed for their daughter’s differences to be expressed,
without blame being assigned to themselves, or their daughters. Claire’s humour was wry. It
mainly centred around other’s advice and judgement about parenting not fitting her own more
96
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
expert knowledge of her daughter:
Claire: [school said] " She needs to find something to do that's not destructive...
“Hmm, we'll try." [laughs]
In this way, perhaps this positioned her in a more powerful ‘knowing’ position than
professionals.
Discussion ~ Constructing a Diagnosis Narrative
By analysing how participants told their stories I considered how tools were used to
convey a message. Participants used a range of genres. All the narratives conveyed the autism
as something which inherently exists within the child. This was especially the case in the
‘Quest’ narratives in which the autism was ‘unveiled’ or searched for.
It may be that the ‘Guided Journey’ stories helped the narrators to externalise blame
and distress and whilst also defining ‘difference’ in their experiences from the norm. In doing
this, the narrator controlled how difficult experiences or painful emotions were presented.
After the interviews with the participants who used this genre, I observed that I felt more
convinced by the inherent ‘existence’ of autism and more empathetic towards the narrators.
Brown (2012) proposed that when we feel empathy from another person, we feel accepted
rather than judged. As well as eliciting acceptance and reducing judgement, perhaps humour
functioned in curtailing the ‘questioning’ parts of the listener. This may have functioned in
helping the narrator to overcome any threat of feeling blamed.
Within the ‘Quest’ narratives, blame was similarly externalised blame from the self to
the ‘door shutting’ professionals who were portrayed as unwilling to help, no matter how
difficult things were. White and Epston (1990) suggest that externalising emotions removes
blame from the individual and makes the emotional aspect of a story less important. Again, it
could be interpreted that minimising emotions associated with a story by externalising blame,
97
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
could make experiences easier to talk about, without feeling judged.
98
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix K: Extended Analysis
How Were Stories Told?
In addition to the analysis presented in the main paper, imagery was recognised as
narrative tool is presented here as an extended part of the analysis.
Imagery
The creation of visual images was interpreted as a narrative tool because this helped
the listener to visualise the participant’s ideas of ASC. All participants took realist
perspectives on autism. This was reflected in the images evoked by the stories, two of which
dominated: ‘Uncovering the Truth’ and, ‘The Degenerative Illness’.
‘Uncovering the Truth’
Within some narratives, autism was portrayed as a truth and diagnosis was portrayed
as the uncovering of this truth:
Helen: ‘She can now go forward in secondary school with people understanding her
true situation’.
This image reflects a broader narrative relating to a realist perspective, that there is a ‘truth’
out there to be identified.
‘The Degenerative Illness’
Autism was often depicted as an illness that might worsen if not identified:
Helen: ‘So many of the mothers, report really, really, really shocking behaviour and
99
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
shocking distress in their daughters cos they haven't got picked up in time’.
It was also described as having a sudden onset, in the way in which signs and symptoms
showed:
Helen: ‘Right, nine. Maybe nine and a half. And I suddenly was like, "Ah, this is
suddenly happening." And I was like-- I was just like taken aback because it
had never happened before’.
This example could show how the conceptualisation of autism as an ‘illness’ is used as a tool
of persuasion to convince the listener of the ‘reality’ of autism. Helen had come up against
much difficulty in getting a diagnosis. It may be that this context fed into the way in which
Helen tells her story in order to persuade the listener that it was specifically autism causing
these difficulties, and not something else. Similarly, many participants eluded to the autism
being hereditary:
Tessa: ‘I think their dad’s got it’.
Again, this reflects dominant narratives of autism as biological and/or genetic.
100
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix L: Extended Analysis
How is Autism Made Sense Of? Themes Across Narratives
2. ‘After Diagnosis’
Although this was not specifically part of the research question, parents’ stories about
after diagnosis shed light on how they had felt before diagnosis.
2.1 ‘Release from Responsibility’
For many parents, diagnosis changed their understandings of their daughter’s
behaviours. One theme was that blame about their daughter behaviour was removed, both
from themselves and from their daughter. In this way, the perception of control of behaviour
changed, whereby parent and child were seen as not being able to change certain behaviours.
Moreover, parents talked about not having choice in their parenting practices:
Emily: ‘If you have a different kind of child everything changes and the way you deal
with them is just completely different…all you parenting principles go out of
the window (laughs)…we have to do an awful lot of bribery to get her to do
anything…’
Tessa: ‘So in the end, it kind of had to be a different strategy’
Some parents insinuated that they would have preferred to parent in a different way, and
perhaps that there are ‘right’ ways to parent:
Emily: ‘I would have never have been one to sort of fall in to the trap of bribery’
Claire: ‘I know you shouldn't but I tend to treat her differently now’
101
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Despite the diagnosis limiting perceptions of choice in the ways to parent, diagnosis helped to
shift blame away from behaviour being caused by a ‘bad parent’, offering relief:
Emily: ‘So to be able to know what it is. Honestly. It’s such a big relief. Yeah explains
everything.’
Similarly, diagnosis helped to shift blame away from the child, and naughtiness was
externalised to the autism, changing the way in which behaviours are viewed. The child was
no longer viewed as ‘naughty’ because they could not control their behaviour:
Emily: ‘It’s very unlikely that Sophie got shouted at much herself because she’s a
good kid I think she got shouted at for being slow and that’s something she
can’t help’
Claire: ‘It is better now we have a diagnosis cos we can say she's not being naughty.
But this is the problem’
Tessa: ‘What she was doing wasn't actually naughty anyway, it was just a reaction I
think’
Ella: ‘She just wouldn’t or actually couldn’t looking back on it’
Some understandings seemed to be limited by the diagnosis whereby behaviours,
emotions, strengths and weaknesses were seen as symptoms of, or caused by autism, rather
than understood in the context of the situation or experiences:
Emily: ‘I think partly the initial being really upset was because the teacher was
shouty and it was noise’
102
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Ella: [talking about Fiona talking in ‘proper sentences’ at 16 months] ‘it was
probably due to autism’
Perhaps this allowed for extremely distressing experiences that were previously
difficult to make sense of, to be explained:
Emily: ‘She wishes she was dead (sniffs) and it’s not right. Erm we think it might be
autism’.
However, some participants talked about this impacting their daughter’s perception of
themselves and sense of self-efficacy in their achievements:
Ella: ‘She thinks that she is as clever as she is and as good at acting and singing as
she is, because of autism and therefore she feels that she's cheating’.
2.2 ‘Legitimacy and Validation’
Especially where parents had previously felt blamed, diagnosis helped to bring a
sense of legitimacy, validation and credibility. Helen, eluded to safety in the diagnosis, even
though it did not necessarily mean that there was further support, whilst Ella and Emily felt
more believed and supported by their daughter’s schools:
Ella: ‘They (school) obviously believe me cos I've got a diagnosis for her’
Emily: ‘School have been much more supportive since we got the diagnosis’
Some parents’ narratives also eluded to feelings of empowerment in their knowledge about
autism:
103
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Ella: ‘This school tell me things that even I don’t know about autism’.
There was a sense from Emily that it might feel threatening for this knowledge to be
challenged:
Emily: ‘No matter what anybody says I know she’s autistic’.
These examples of empowerment through diagnosis, highlight how school and healthcare
systems may feed into a need for people to have a diagnosis, by not offering help or listening
without a diagnosis. In their daughter’s receiving a diagnosis, participants came to develop an
understanding of themselves as a ‘good’ and mastered parent empowered by their knowledge
of their child and knowing best about how to parent them.
2.3 ‘Looking Through The Autism Lens’
Many parents’ narratives reconstructed the past with knowledge from the present.
Behaviours that were previously seen as part of their daughter’s personality are now seen as
caused by Autism:
Emily: ‘She always had a very vivid imagination so we just thought you’re just a bit
quirky. You’re just a bit different you know but it’s cute’
Ella: ‘I just put it down to her love of reading, her love of books and didn't really
think any more of it’
Other diagnoses were also overshadowed by the autism:
Claire: ‘I just thought she was just having separation anxiety. But I think maybe that
is the autism now, that then was causing the problems and issues.’
104
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
All parents talked about ‘signs’ of autism becoming obvious looking back:
Emily: ‘There’s loads of other stuff that when we look back we go ow my god how
stupid were we (laughs) well we didn’t know that’s the thing’.
These examples show how after diagnosis, autism was construed as causal to
behaviour and personality encompassing both ‘negative’ and ‘positive’ parts of this. Parents
externalised blame and naughtiness, but also more positive attributes from their child into the
autism. This understanding also seemed to have been absorbed by children; some parents
spoke about their children no longer feeling proud of their strengths or achievements, because
the child saw them as part of the autism and therefore not their ‘doing’ or responsibility. In
this way, it seemed that for some parents, and some children, the diagnosis of ASC overrode
other explanations and narratives of distress, strength and weakness of the individual’s
identity. The diagnosis enabled a reframing, showing how relocating certain ‘traits’ or
behaviours in language shifts understanding.
Appendix M: Examples of Coded Transcripts
105
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Participant 4: ‘Claire’Descriptive
level
Record playing over and over
Separation anxiety
Impact on parenting- no choice
99. C: Yeah, when-when she used to go nursery when she
was
100.two year old even, on the car journey, she would upset,
101.we'd have to have the Ede record on again and again.
And
102. they said that she had separation anxiety, because at the
103. nursery, they always had to give her a special toy and sit
104. her in a baby chair for many hours, because she just
105. wouldn't come out of it, and at-at the time, I just thought
106. she was just having separation anxiety. But I think maybe
107. that is the autism now, that then was causing the problems
108. and issues.
109. In the end I gave up working away from the house because
110. she was just too difficult to leave, and she still is even
and-and she's 11 in a couple of days. She's still very hard
111. to leave for a short time. Um, so I think- and then at
112.school, they have to lock the - we have to go in through a
different entrance and then lock the door behind her
113. because she would just run out of school. Um, and it
was
114. just seen as being naughty. Like she was just naughty and
115. she was arguing. She never had any awareness of it, of
116. authority. They had a teacher once said to her, "Abbie,
117. I've got better things to do than stand here while you go
Items of interest, comments, images, emerging themes, tone, interpretations
Specific routine – separation anxiety
Autism causal – other explanations not valid
106
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Would want to run off
Seen as being naughtyarguingawareness of authority
Doesn’t understand expressions
Tricky to understand what people mean with sayings first time
Grandparents struggle – think cheekyWants to please
118. in the toilet and locking the door." Andd she says,
119."Well, just go do them." (laughs)
120.She just speaks and she just speaks the way, and
121. somebody else said she's making a mountain out of a
122. molehill and these things, these expressions, like 'pulling
123. your socks up', she just doesn't get them. We'll explain
124. them to her now, and she-she-she will. She understands
125. what people are saying to her now, but, if somebody uses
126. something new, that new expression, it's very tricky for
127. her to understand what's going on.
128.And then, grandparents struggle with her because they
129. don't get her. They just think she's cheeky, but she's not
130. really. All she wants to do is please you. But sometimes,
131.the way she comes across is as being back-chatting and-
132. 'cause it's got to be right, it's got to be Abbie- if Abbie
133.has a rule, that's the way it is. And if I've said something
134. to one person, that rule should apply across. [Laughs]
135. She's tricky. [Laughs] It is better now we have a
136. diagnosis 'cause we can say she's not being naughty. But
this is the problem.
Naughtiness now seen as autism
Others perceive her as rude?
Wants to please you
107
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Has to follow rules. Rules need to be fair. No exceptions
Diagnosis saves reputation
ASD the cause of problems
More flexible parenting
Wants to make people happy
When being difficult, get her on your side
Diagnosis useful as an explanation for others - not a ‘naughty child’(or ‘bad parent’?)ASD cause of problems
Participant 3: ‘Tessa’
108
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
109
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
110
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix N: Extracts from Reflective Journal
14th November 2017
Having just completed my second interview, I’ve reflected more on the first, and
realised how much more compelled I had felt to ask questions in the first interview. Having
set up both of the interviews in a very similar way, I felt that the first participant wanted more
for me to be more a part of the conversation. I felt more compelled to ask questions, and was
very conscious that I almost felt like I was being pulled into a clinician role, to ‘assess’ rather
than to listen to her story. This could have been perhaps partly due to my own anxiety in
being my first interview and perhaps not leaving as much space for the participant. However,
on reflection I also wonder if it was also something about her relationship with ‘knowledge’:
an assumption that a parent’s experience may not be as valuable as what we know from ‘hard
science’ that meant that she did not feel comfortable as the storyteller, and so looked to me to
take the lead, because I would ‘know’ what I am looking for? In line with this ‘Ella’ (the first
participant) drew much more ‘information’ from a checklist, almost scaffolding her
knowledge around this. I wonder if this is a reflection of how professionals make parents feel,
and it is assumed that ‘the checklist’ which is more relevant than experience and stories of
individuals. This could have also been used as a tool to persuade the listener of the validity of
the diagnosis and I wonder if this may have been used after many ‘rejections’ from mental
health professionals.
The participant today was fluent in her story, and I felt that I had to do less to
enabling the story to come through. I had time to think about what she was saying and felt
drawn into and convinced by the idea of autism being ‘present’. This surprised me, and I
wonder whether it was something about the way the story was told and the emotion that it
was told with. In some ways it was very comical, but this had a pain and ‘darkness’ to it too. I
also wondered about the fluency of the story and how connected this woman seemed to be
111
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
with an identity of a mother of autistic children. Although this parent spoke with a lot of pain,
it also seemed that this gave her an identity that she seemed very confident with.
9th February 2018
One of the findings that I think is interesting is how parents look back at their
children’s behaviour and ‘see’ things that relate to autism. I have reflected on the parallel
process of my ‘lens’ when looking at the data, that will have been coloured by my personal
experiences and assumptions about what I will find. Now that I am well into my analysis, and
starting to draw out themes I have decided to look back in my journal and see how, what I
think I have found, compares to what I thought I would find around four months ago. One of
my expectations, was that I thought that I would find that ‘signs’ that stand out for parents are
those that do not fit with gender stereotypes for girls e.g. lacking social ability or too much
energy. Mostly however I have found that parents are saying these things did not stand out,
but that only looking back that they can ‘see’ that things weren’t quite right. Another of my
expectations was that parents might feel blamed or stigmatised for their child’s differences
and I wondered whether I would find that diagnosis offers a relief from this. This is
something that I think that I have found in the data. In sharing this with my supervisors, I am
now going to look back over the data and see whether blame and relief from blame is
explicitly or implicitly mentioned. Where it is implicitly mentioned I will think about why I
have interpreted it in this way. I have also decided that I will use quotes for every point in my
results section to be sure that my interpretations are grounded in the data.
112
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Part 2Major Research Project Literature Review
A Review of the Differences in the Presentation of Girls and Boys with Autism Spectrum Conditions Without Cognitive Impairment
Word Count: 7997
113
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Statement of Journal Choice
This literature review is written with the view of submitting to a peer-reviewed journal. The
journal of choice for this review is The Journal of Autism and Developmental Disorders. This
journal has an impact factor of 3.3 and is published monthly. It accepts manuscripts on all
aspects of autism spectrum disorders and related developmental disabilities including
diagnosis advancements and also publishes literature reviews making it an appropriate
journal choice.
114
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Abstract
Estimates from epidemiological research show that Autism Spectrum Conditions (ASCs) are
diagnosed more commonly in males than females. The extent of this disparity is higher
amongst individuals who do not have cognitive impairment. There have also been claims that
girls may be misdiagnosed or underdiagnosed due to a difference in expression or
manifestation of symptoms. The DSM-V (American Psychiatric Association, 2013)
recognises this but does not state what these sex/gender differences look like. This paper
reviews the literature on sex/gender differences in the presentation of children and
adolescents with ASC without cognitive impairment. A systematic search strategy was
conducted which led to 36 papers being identified for the review. Many different aspects of
Autism were reported on and results showed a complex picture with inconsistent findings.
The majority of research has focussed on comparing symptoms on established diagnostic
profiles of ASC and found few differences in broad Social Communication criteria and some
suggestion that girls show less severe Restricted and Repetitive Behaviours and Interests. In
experimental paradigms, females showed better skill in communication, whilst no differences
were found in motor skill, or general adaptive functioning. Typically, females had more
difficulty with symptoms of depression, anxiety and sensory sensitivity, and fewer symptoms
of hyperactivity. However, few studies measured the quality of impairments as opposed to
the severity of impairments. A recommendation is made for qualitative research that
contextualises the existing predominantly quantitative evidence in order to enrich our
understanding of personal experience in perceiving signs of autism, and inform diagnosis.
Key Words: Autism, Females, Gender, Girls, High Functioning
115
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Introduction
There have been many suggestions that people with Autism present with different
symptoms according to their sex/gender4 (Gould & Ashton-Smith, 2011). As there is no clear
picture of how, or even if, males and females present differently, this review will evaluate the
empirical research that has investigated these differences.
Defining Autism Spectrum Disorders
First described by Kanner (1943) in his essay “Autistic disturbances of affective
content”, Autism is currently most widely understood as a neurodevelopmental disorder
involving impaired social communication alongside restricted or repetitive patterns of
behaviour or interest (American Psychiatric Association, 2013). The term “Autism Spectrum
Disorder” or “ASD” (Wing, 1988) is now generally used to represent individuals with
Autistic Disorder, Asperger's Syndrome and Pervasive Developmental Disorder-Not
Otherwise Specified (PDD-NOS). Prevalence studies indicate that ASD is diagnosed in
approximately 1.1% of the UK population (Baird, Simonoff, Pickles, Chandler, Loucas et al.,
2006; Brugha, McManus, Meltzer, Smith, Scott et al., 2009).
In 2013 the DSM-V (APA, 2013) revised the way in which ASD is diagnosed.
Previously ASD was a collective term for a group of Pervasive Developmental Disorders
characterised by deficits and impairment in three areas of development: reciprocal social
interaction, communication, and the presence of stereotyped or restricted behaviours,
interests, and activities (APA, 2000). Distinct diagnoses of Autistic Disorder, Asperger’s
Syndrome and PDD-NOS would have been given according to specific presentation and
need. Now, clinicians provide a single label of ASD and distinctions of individual need are
4 In this paper “sex” refers to “the biological and physiological characteristics that define men and women” whilst “gender” refers to “the socially constructed roles, behaviours, activities, and attributes that a given society considers appropriate for men and women.” (definitions adopted from the World Health Organization, 2015). However, because gendered socialization begins at birth, it is difficult to separate the effect of sex and gender. For this reason, unless “sex” or “gender” is specifically used as defined above, the term “sex/gender” will be used to acknowledge the inevitable overlap between them (Springer, Mager Stellman & Jordan-Young, 2012).
116
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
specified by three severity levels of the two broad criteria: impairment in social
communication and interaction as well as restricted and repetitive patterns of behaviour and
interests (RRBI; APA, 2013). In order to avoid implying a ‘disordered’ person (Baron-
Cohen, Scott, Allison, Williams, Bolton et al., 2009) and to encourage less stigmatising
terminology I will use the term Autism Spectrum Condition (ASC) or autism5 throughout this
paper.
ASCs are diagnosed behaviourally where a collection of behavioural symptoms is
assumed to signify the presence of an underlying impairment (Rutter, 1978). Currently,
diagnosis relies on observations of behaviour according to signs and symptoms that vary with
age (APA, 2013). The instruments used in best practice in diagnosis include a standardised
clinical interview (Autism Diagnostic Interview-Revised, ADI-R; Lord, Rutter & Le Couteur,
1994) and an observation of set activities (Autism Diagnostic Observation Schedule, ADOS;
Lord, Rutter, Goode, Heemsbergen, Jordan et al., 1989). These instruments rely on subjective
observations or experiences of parents, caregivers, or self and clinician observation and
assessment. The ASC phenotype is thought to also encompass a range of associated features
in the cognitive, behavioural, emotional, motor and sensory domains.
Sex/Gender Disparity in Prevalence Studies
Estimates from epidemiological research show that ASCs are diagnosed more
commonly in males than females though the extent of this sex/gender difference is variable.
Some studies have suggested a male:female ratio of around 4:1 when people of all levels of
intellectual functioning are included (Fombonne, 2003, 2005). This ratio declines to around
2:1 in studies researching individuals with lower intellectual functioning (Fombonne 2003,
2005, 2009). The sex/gender disparity is much higher for individuals without co-occurring
Intellectual Disability (ID) ranging from 6:1 to 16:1 (Baird et al., 2006; Fombonne 1999,
5 The term ‘autism’ is used here to refer to the diagnostic label.
117
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
2002, 2003; Scott, Baron-Cohen, Bolton & Brayne, 2002; Volkmar, Volkmar, Szatmari &
Sparrow, 1993).
There is evidence to show that females who are diagnosed with ASC without ID or
cognitive impairment (high functioning ASC; HFASC), are diagnosed significantly later than
males with the same diagnosis (Begeer, Mandell, Wijnker-Holmes, Venderbosch, Rem et al.,
2013; Goin-Kochel, Mackintosh, & Myers, 2006; Shattuck, Durkin, Maenner, Newschaffer,
Mandell et al., 2009). Additionally, some studies suggest that the age of first concern for
HFASC females is significantly later than for HFASC males (Begeer et al., 2013;
Rynkiewicz & Łucka, 2015).
Explanations for the Sex/Gender Disparity
Several hypotheses have been proposed in an attempt to explain these sex/gender
prevalence differences. These can be summarised under two frameworks; the first is that the
disparity exists due to a ‘real’ difference in the prevalence in males and females, i.e. that
autism impacts fewer females than males (Baron-Cohen, 2005; Wing, 1981a); the second is
that autism is expressed differently in females and thus remains ‘undetected’. These dominant
narratives explaining the disparity also reflect the dominant narrative in which autism is
conceptualised as an ontological truth in that it exists as an observable and essential entity in
itself that can be discovered (Timimi, Gardner & McCabe, 2011).
An ‘Essential Difference’
Baron-Cohen’s ‘Extreme Male Brain Hypothesis’ (Baron-Cohen, 2002; Baron-Cohen,
Knickmeyer & Belmonte, 2005) posits that there is an essential difference between the
neurobiology of the male and female brains, and autism is conceptualised as an extreme
‘male’ brain at the cognitive and biological level. This theory proposes that the gender ratio is
biased towards males because a male brain is more likely to become more ‘male-like’ than a
118
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
female brain. The extreme male brain theory of autism was first informally suggested by
Asperger in 1944 who wrote, ‘The autistic personality is an extreme variant of male
intelligence. Even within the normal variation, we find typical sex differences in
intelligence...In the autistic individual, the male pattern is exaggerated to the extreme’
(Asperger, 1944; Frith, 1991, pp.84–85). This theory predicts that women will cognitively
present as more 'male like', and that typical sex differences found in the general population
will not be found in individuals with ASCs. The theory is supported by evidence that there
are limited differences in symptomology between male and female populations with autism
(Van Wijngaarden-Cremers, van Eeten, Groen, Van Deurzen, Oosterling et al., 2014).
Mis- or Under-diagnosis
Some studies have suggested that discrepancies between male and female HFASC
prevalence could be the result of misdiagnosis and/or under-reporting by caregivers and
parents (Giarelli, Wiggins, Rice, Levy, Kirby et al., 2010; Gillberg, 1993; Kim, Leventhal,
Koh, Fombonne, Laska et al., 2011; Mattila, Kielinen, Linna, Jussila, Ebeling et al., 2011). A
large population study investigating symptoms in undiagnosed populations in South Korea
found larger proportions of females in general education settings that met criteria for ASC
than in special educational needs settings, perhaps raising the possibility that girls may be
‘undiagnosed’ or less likely to be referred for evaluation (Kim et al., 2011). Similarly, in a
twin study, researchers found that girls needed to have either more behavioural problems or
ID, or both, to be diagnosed (Dworzynski, Ronald, Bolton & Happé, 2012).
Similarly, some suggest that a difference in expression or manifestation of symptoms
between the sex/genders alongside a dominance of research in males with autism may mean
that the ‘female phenotype’ of ASCs is not widely recognised by parents or professionals.
Additionally, current assessment tools detecting ASC may have low validity for girls
(Dworzynski et al., 2012; Rivet & Matson, 2011). Correspondingly, the DSM-5 (APA 2013)
119
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
states that ‘females without ID may go unrecognised due to subtler manifestation of
symptoms’. However, it does not indicate what these might look like.
Taking a biosocial perspective, Goldman (2013) proposes that children are socialised
according to their gender, impacting symptom expression of autism, and perhaps allowing for
a basic level of social skill that means difficulties are ‘masked’ in girls. Others have similarly
suggested that females ‘camouflage’ their difficulties during social situations (Attwood,
2006) by either hiding socially unacceptable behaviour or ‘unnaturally’ performing behaviour
deemed to be more ‘normal’ or socially acceptable (Holliday-Willey, 1999).
What do we know about Gender and the Diagnostic Features of ASC?
Many studies have reported similar clinical profiles between male and female children
with ASC (Amr, Raddad, El-Mehesh, Mahmoud & El-Gilany, 2011; Andersson, Gillberg &
Miniscalo, 2013; Mayes & Calhoun 2011). A review and meta-analysis of the literature on
sex/gender differences in ASC found no differences in the domain of social behaviour and
communication (Van Wijngaarden-Cremers et al., 2014). The only difference found was that
boys showed more repetitive and stereotyped behaviours after the age of six. However,
evidence that females with ASC are more likely to have ID are important in interpreting these
results. ASC might be identified more in girls with ID in comparison to those without ID,
perhaps due to more obvious symptom expression, or inability to camouflage symptoms
(Wing 1981b). Cognitive ability (Lord, Schopler & Revicki, 1982; Mayes & Calhoun 2011;
Park, Cho, Cho, Kim, Kim et al., 2012; Sipes, Matson, Worley & Kozlowski, 2011; Volkmar
et al., 1993), and age (Carter, Black, Tewani, Connolly, Kadlec et al., 2007; Mayes &
Calhoun 2011; McLennan, Lord, & Schopler, 1993) are most often suggested to be the
greatest mediating factors influencing the symptomatology and sex/gender differences
observed in ASC clinical presentation. More recently, studies have focussed on investigating
sex/gender differences between individuals with high functioning ASC (e.g. Dean, Harwood
120
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
& Kasari, 2017), but these studies have not been reviewed before.
Rationale
Overall, in comparison to males, evidence suggests that females without ID are: taken
for assessment later; take longer to be diagnosed; are more likely to be misdiagnosed, and;
are less likely to receive a diagnosis of ASC despite showing symptoms. Emerging from an
interest in understanding why females are less likely to be diagnosed as early as boys, this
paper aims to review the literature that has explored sex/gender differences in the
presentation of children and adolescents (0-18 years) with HFASC. It is recognised that ASC
symptoms and presentation change with age but it is beyond the scope of the review to
identify these differences in adults too. The review aims to answer the following research
question by systematically searching the literature:
What does the research tell us about sex/gender differences in the presentation of children
and adolescents with HFASC without ID or cognitive impairment?
Method
Database Searching
An initial scoping of the literature was conducted. This revealed that searching for
‘ASD and "gender or sex" differences’ returned too broad an array of results. Results were
narrowed by adding age and cognitive impairment restrictions to the search terms. After some
trial and error, the following finalised key search terms were used to narrow the results, but
not so much that relevant papers were missed; ‘‘"autism spectrum disorder" OR ASD OR
"pervasive development disorder" OR PDD OR Asperger* OR autism OR "autistic spectrum
condition" OR ASC’ AND ‘"gender difference*" OR "sex difference*"’ AND ‘child* OR
adolescent*’ AND ‘"high functioning" OR "average intelligence"’.
Five databases were searched; Web of Science, Embase, PsycINFO, Medline and
121
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Scopus. The key words were searched for in all fields in Embase and PyscNET, title, subject,
abstract and keywords in Medline, title, abstract and keywords in Scopus and title and topic
in Web of Science. The last search was carried out on the 11 th February 2018 and no limits
were put on the time period of the search.
Inclusion Criteria
All search results were exported into bibliographic software (ProQuest RefWorks)
where duplicate records were removed leaving 346 potentially eligible records. The title and
abstract of these records were inspected based upon the following inclusion criteria:
1. Must allude to ASD and behaviour, symptom or profile of ASD
2. A child or young person (0-18 years) population sample should be used
3. Sample used must not have ID or cognitive impairments
4. Intervention studies not included
5. Opinion papers and book chapters excluded
6. Written in English
If all of the inclusion criteria were not identified in the abstract, papers were included
providing the first inclusion point was met. It was decided to be over-inclusive to enable a
thorough reading to take place.
One-hundred-and-seven articles were found to meet this criteria at screening. The
reference lists of these articles were hand-searched, revealing another four further potential
records. Following this, the 111 articles were accessed in full. Figure 1 shows the reasons for
exclusions at this stage, and the process of searching. Thirty-six papers were included in the
review.
122
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Quality Assessment
The 36 papers were assessed for quality using the Health Technology Assessment
(HTA) framework (Kmet, Lee & Cook, 2004). This tool was used as a guide to consider
quality, but papers were not excluded based on this. The HTA is endorsed by the National
Institute for Health Research (NIHR) and assesses quantitative and qualitative research. This
was beneficial because the qualitative papers included were not detailed enough to use a
specific qualitative assessment tool.
The HTA framework assesses quality in terms of the extent to which papers minimise
errors and biases and was designed for considering diverse study designs (Kmet et al., 2004).
Each criterion is scored as; 2=met in full, 1=partially met criteria, 0=failed to meet criteria or
not applicable. Maximum scores are 28 for quantitative papers and 20 for qualitative papers.
Each paper was scored and given a percentage quality mark. Some papers were discussed
with supervisors to check consistent use of the tool, but this was not possible for every paper
due to time limitations.
The range of quality was 64%-95%, with an average quality score of 85%. Kmet et al.
(2004) consider 75% to be a ‘conservative’ cut-off and 55% to be a ‘liberal’ cut off.
Therefore, the quality ranges from ‘modest’ to ‘very good’. Thirty-four papers were
considered good quality (above 75%); two papers fell below the conservative cut-off but no
paper fell below the less stringent quality criterion (above 55%). A summary of the findings,
including detail of quality is outlined in Table I.
123
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Figure 1. Flow chart of search methodology
124
Exclusion of duplicate records using bibliographic software N= 152
Potentially eligible records N= 346
Excluded - did not meet screening criteria N= 239
Full text articles assessed and read further to assess for eligibility N= 111
Potentially eligible records identified through database searches N=498
Web of Science N= 166Embase N= 63Scopus N= 74PsycINFO N= 46Medline N= 148The Cochrane Collaboration Register N=1
Exclusions after reading N=75
Reasons:
Book chapters, theses, commentaries, letters (not peer reviewed) N=9
Not a child/adolescent sample N=6
Sex/gender differences not reported N=37
Not only ASD sample N= 2
Sample included individuals with ID N=19
Intervention study N=1
Did not measure cognition or behaviour N=1
Additional potentially relevant records N= 4
Final papers included in the literature review N=36
Quality criteria applied to remaining
articles using Health Technology
Assessment Tool
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Table I.
Summary of papers included in the review
Paper Quality Rating6
Country Method, Design and Measure(s) Sample Summary of Relevant Findings
Baron-Cohen, Hoekstra, Knickmeyer & Wheelwright (2006)
The autism-spectrum quotient (AQ)—adolescent version.
19/2286%
UK Quantitative. Cross-sectional design.
Overall ASC symptoms measured using Autism Spectrum Quotient (AQ)
N=152 (aged 9.8–15.4 years)
ASC females, n=14;ASC males, n=38;TD females, n=50;TD males, n=50.
No significant difference in overall scores in ASC symptoms between boys and girls with ASC (p> .09).
Among the controls, boys scored significantly higher than girls (p= .002).
Cridland, Jones, Caputi & Magee (2014)
Being a girl in a boys’ world: investigating the experiences of girls with autism spectrum disorders during adolescence.
17/2085%
Australia Qualitative. Interpretative Phenomenological Analysis.
Five semi-structured interviews with three mother–daughter dyads and two additional mothers.
N=5 (aged 12–17 years)
ASC females, n=3;ASC female’s mothers, n=5.
Girls with ASC experience challenges similar to those experienced by boys during adolescence such as: challenges of transitioning to and coping with high school and; importance of learning personal boundaries in interactions with others. Other issues of particular relevance to adolescent ASC girls such as difficulties socialising with typically developing girls.
6 See Appendix A for main strengths and limitations of each study.
125
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Dean, Harwood & Kasari, (2017)
The art of camouflage: Gender differences in the social behaviours of girls and boys with autism spectrum disorder.
20/2291%
USA Mixed methods.
Qualitative descriptions of the social behaviour recorded and Playground Observation of Peer Engagement (POPE) used to rate play.
N=96 (aged 6-8 years)
ASC females, n=24;ASC males, n=24;TD females, n=24;TD males, n=24.
Qualitative and quantitative results showed that girls with ASC stayed in close proximity to peers and wove in and out of activities, which masked their social challenges. Comparatively, the ‘male landscape’ made it easier to detect the social challenges of boys with ASC; TD boys tended to play organized games whilst boys with ASC tended to play alone (boys with ASC spent significantly more time in ‘solitary’ than all other groups).
Dean, Kasari, Shih, Frankel, Whitney, Landa, Lord, Orlich, King & Harwood (2014).
The peer relationships of girls with ASD at school: comparison to boys and girls with and without ASD.
18/2282%
USA Mixed-methods. Cross-sectional design.
Friendships Survey (Cairns & Cairns, 1994) used to measure social acceptance, social preference, social connections, social salience, reciprocal friendship, and rejection.
N=100 (aged 6-8 years)
ASC females, n=25;ASC males, n=25;TD females, n=25;TD males, n=25.
Quantitative findings: Both TD and ASC children of both genders preferred and primarily socialised with same gender friends. Girls with ASC receive significantly fewer friendship nominations than the typically developing girls (p= .03) whilst boys with ASC were not significantly different from the typically developing boys. With significantly fewer nominations and social relationships, girls and boys with ASC appear more socially similar to each other than their TD peers. Boys with ASC were more overtly socially excluded compared to girls with ASC who were overlooked rather than rejected.
Frazier, Georgiades, Bishop, & Hardan (2014).
Behavioural and cognitive characteristics of females and males with autism in the Simons Simplex Collection.
18/2282%
USA Quantitative. Cross-sectional design (analysis of existing data sets).
ADOS; ADI-R; SRS; RBS; CBCL; Aberrant Behaviour Checklist; Developmental Coordination Questionnaire; Comprehensive Test of Phonological Processing; Peabody Picture Vocabulary Test.
N=2418 subjects (304 females, 2114 males)
ASC females, n=304; ASC males, n= 2114
(Females IQ >80, n=135; Males IQ>80, not reported)
ASC females had significantly lower levels of restricted interests than ASC males, independent of IQ.
ASC females showed greater irritability than ASC males, independent of IQ.
ASC females did not show a verbal/ nonverbal discrepancy, whilst ASC males were more likely to show a discrepancy in favour of non-verbal IQ.
Fulton, Paynter & 18/22 Australia Quantitative. Cross-sectional N= 116 (aged 29-74 No significant differences in overall scores in
126
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Trembath (2017).
Gender comparisons in children with ASD entering early intervention.
82% design.
VABS; SCQ; Preschool Language Scale; ADI-R.
months)
ASC females, n=22; ASC males, n= 94
adaptive functioning, cognition, or ASC symptoms between boys and girls with ASC.
Goddard, Dritschel, & Howlin (2014)
A preliminary study of gender differences in autobiographical memory in children with an autism spectrum disorder.
20/2291%
UK Mixed methods. Quantitative data including number of memories and references to emotion and Verbal Fluency.
Autobiographical Memory Cueing Task; Recent and Remote Memory Task; Verbal Fluency Tasks; SCQ.
N=48 (aged 8-16 years)ASC females, n= 12; ASC males, n= 12; TD females, n=12; TD males, n=12.
Females scored significantly lower than males (p=.01) on overall SCQ score.
Deficit in specific memory retrieval was more characteristic of ASC males than ASC females. Females in both the TD and ASC groups generated significantly more detailed and emotional memories than males. They also demonstrated significantly superior verbal fluency scores.
Head, McGillivray & Stokes (2014)
Gender differences in emotionality and sociability in children with autism spectrum disorders.
20/2291%
Australia Quantitative. Cross-sectional correlation design.Friendship Questionnaire
N=101 (aged 10-16 years)ASC females, n = 25; ASC males, n = 25; TD females, n = 25; TD males, n = 26.
Females with ASC significantly have more developed social skills than males with ASC (parent-rated). Females also scored significantly higher than males independent of diagnosis.
Hiller, Young & Weber (2014)
Sex differences in autism spectrum disorder based on DSM-5 criteria: evidence from clinician and teacher reporting.
20/2291%
UK Quantitative. Cross-sectional design. Autism Detection in Early Childhood; CARS; ADI-R; ADOS.
N= 138 (mean ages 8-9 years old)ASC females, n = 69; ASC males, n = 69; TD females, n = 25; TD males, n = 26
No significant sex/gender differences found on broad social criteria. Teachers reported significantly fewer concerns for ASC girls than boys regarding their social skill and externalising behaviours (p< .001).
No significant differences found on overall peer relationships (p= .34) and social-emotional reciprocity (p= .99) criteria. However, ASC girls significantly more likely to show ability to integrate non-verbal and verbal behaviours, maintain a reciprocal conversation and initiate, but
127

PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
not maintain friendships. ASC girls appeared to present with a significantly greater ability to engage in reciprocal conversation, use non-verbal language, and share interests and achievements.
ASC girls presented with both significantly fewer and different restricted interests.
128
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Holtmann, Bölte & Poustka (2007).
Autism spectrum disorders: Sex differences in autistic behaviour domains and coexisting psychopathology.
19/2286%
Germany Quantitative. Cross-sectional design.
ADI-R; ADOS; CBCL- parent report
N= 46 (aged 5- 20).
ASC females, n= 23; ASC males, n= 23.
No significant differences found between males and females on the core triad of impairment.
Parent reports revealed significantly more symptoms related to psychopathology in females than males particularly: social (p<.01), attention (p<.01) and thought problems(p<.01).
Howe, O’Rourke, Yatchmink, Viscidi, Jones, & Morrow (2015).
Female autism phenotypes investigated at different levels of language and developmental abilities.
20/2291%
USA Quantitative. Cross-sectional design. Analysis of existing data sets (AGRE, AC, ATN & SSC)
ADOS; SRS; CBCL; VABS.
N= 5723 (aged 6-14 years)
ASC females, n=872; ASC males, n= 4851
Verbally fluent ASC females had similar or better adaptive and social abilities than ASC males. For example, females showed significantly better social skills on the VABS in the AGRE (p= .05) dataset and the AC (p=.005) dataset.
Hurtig, Kuusikko, Mattila, Haapsamo, Ebeling, Jussila,.& Moilanen (2009).
Multi-informant reports of psychiatric symptoms among high-functioning adolescents with Asperger syndrome or autism.
21/2295%
Finland Quantitative. Cross-sectional analysis.
Youth Self-Report (self-report); CBCL (parent report); Teacher Report Form (teacher report)
N=275 (aged 11 – 17 years)
ASC females, n= 11; ASC males, n= 32; TD females, n=132; TD males, n=85
Self- report: Both sex/genders with ASC reported significantly more problems in ‘withdrawal’ and ‘social problems’ than TD girls. ASC girls reported significantly more ‘thought and attention problems’ than TD girls and ASC boys.
Parent report: The same patterns were found.
129
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Jamison, Bishop, Huerta, & Halladay (2017).
The clinician perspective on sex differences in autism spectrum disorders.
16/2080%
UK Mixed Methods. Online Survey.Respondents asked to consider sex differences across specific DSM-5 ASD criteria and comorbid conditions as well as qualitative information about their experiences of evaluating female children and adults.
106 clinicians who are actively engaged in the assessmentand diagnosis of ASC and related disorders
Clinicians perceived significantly more sex-related differences in restricted and repetitive behaviours (females were less likely to present with ‘restricted and fixated interests’ and fewer differences for social communication features. Significant differences were most commonly observed in school age and adolescence.
Kauschke, van der Beek, & Kamp-Becker (2016).
Narratives of girls and boys with autism spectrum disorders: gender differences in narrative competence and internal state language.
20/2291%
Germany Quantitative. Experimental design. Cross-sectional analysis.
Narrative competence and Internal State Language (ISL) was investigated using narrations elicited by a wordless picture book.
N=33 (aged 8-19).
ASC females, n= 11; ASC males, n= 11; TD females, n=11.
Girls with ASC produced significantly more words for internal states and explained the causes and consequences of internal states significantly more often than boys with ASC. Both boys and girls with ASC fell behind TD girls in production of affective words.
Kim, Rosenthal, Gwaltney, Jarrold, Hatt, McIntyre, Swain, Solomon & Mundy (2015)
A virtual joy-stick study of emotional responses and social motivation in children with autism spectrum disorder.
17/2285%
USA Quantitative. Experimental.
Virtual-reality emotion sensitivity test measure for emotion recognition and interpersonal distance called the virtual-reality emotion sensitivity test.
N=42 (aged 8-16 years)
ASC females, n= 6; ASC males, n= 13; TD females, n=7; TD males, n=16.
No significant effects of participant sex/gender were observed on accuracy of affect recognition or Interpersonal Distance.
There was little evidence of disturbance of affect recognition among children with ASC.
Kopp & Gillberg (2011)
The Autism Spectrum Screening Questionnaire (ASSQ)-Revised
20/2291%
Sweden Quantitative. Validation of measure. Cross-sectional analysis.18 items added to the ASSQ (ASSQ-GIRL).
N=105 (aged 6-16 years)
ASC females, n=27; ASC males, n= 20; TD
Certain ASSQ-GIRL items were much more typical of girls than of boys with ASC ("avoids demands", "very determined", "careless with physical appearance and dress", "interacts mostly with younger children", “has a difference
130
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Extended Version: an instrument for better capturing the autism phenotype in girls?
females, n=58. voice/speech” and “difficulties completing simple daily activities”). ‘‘Lacks best friends’’ item was significantly more typical of boys than of girls with ASC.
Koyama, Kamio, Inada & Kurita (2009)
Sex Differences in WISC-III profiles of children with high-functioning pervasive developmental disorders.
17/2277%
Japan Quantitative. Cross-sectional design.Japanese version of the WISC.
N= 142
ASC females, n=26 (mean age 8.2 years); ASC males, n= 116 (mean age 9.0 years).
ASC girls scored significantly higher on the Processing Speed Index, Coding and Symbol Search, and significantly lower on Block Design than ASC boys. Both groups showed weakness on Comprehension.
Girls' profiles were relatively even and different from the boys', which were characterized by a peak on Block Design.
Kumazaki, Muramatsu, Kosaka, Fujisawa, Iwata, Tomoda, Tsuchiya & Mimura (2015)
Sex differences in cognitive and symptom profiles in children with high functioning autism spectrum disorders.
17/2277%
Japan Quantitative. Cross-sectional design.WISC (Japanese version); CARS – Tokyo Version.
N= 46 (aged 5–9) ASC females, n=28; ASC males, n= 28.
ASC girls and ASC boys shared similar cognitive profiles on the WISC-III.
ASC boys more ‘abnormal’ in “Object Use”, “Activity Level” and “fear or nervousness” and ASC girls more abnormal in “Taste, Smell, and Touch Response and Use”.
ASC boys generally had more ‘unusual interests’ than ASC girls.
Lohr, Daniels, Wiemken, Williams, Kelley, Kuravackel & Sears (2017)
The screen for child emotional disorders is sensitive but not specific in identifying anxiety in children with HF-ASD.
19/22
86%USA
Quantitative. Cross-sectional correlation design.
Screen for Child Anxiety-Related Emotional Disorders (SCARED); Achenbach System of Empirically Based Assessment; CBCL; Youth Self-Report for subjects > 11 years.
N= 100 (aged 8-18 years)
ASC females n= 12; ASC males n= 88
Significant differences in self and parent reports suggest that parents interpret externalizing behaviours as signs of anxiety in children with ASC, whereas youth may describe internalized symptoms as anxiety.
Parents and females with ASC agree more closely in their reports of anxiety.
Girls with ASC may self-report more anxiety than males.
131
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
May, Cornish & Rinehart (2014)
Does gender matter? A one year follow-up of autistic, attention and anxiety symptoms in high-functioning children with autism spectrum disorder.
21/22
95%
Australia Quantitative. Cross-sectional correlation design
WISC; WASI; SRS (parent rated); CCC; RBQ.
N=100 (aged 7-12)
ASC females, n= 28; ASC males, n= 28; TD females, n=22; TD males, n=22
No significant sex/gender differences in ASC symptoms.
Males were significantly more hyperactive. Females were significantly more socially anxious.
Similar gender profiles were present across two time points (one year follow up).
May, Cornish & Rinehart (2016)
Gender profiles of behavioural attention in children with autism spectrum disorder.
21/22
95%
Australia Quantitative. Cross-sectional design.
SRS; CCC; RBQ (parent reported).
N=124 (aged 7-12 years)
ASC females, n=32, ASC males, n=32, TD females, n=30; TD males, n=30.
No significant sex/gender differences in social difficulties found in children with ASC.
Significantly more repetitive motor movements (p= .006), communication difficulties, and inattention (p= .041), reported in boys than girls, regardless of whether they had a diagnosis. ASC boys made significantly more (p= .033), ‘inappropriate initiations’ (talking repetitively about things that no one is interested in) and had more ‘unusual interests’ (p= .004), than ASC girls. Younger boys with ASC had significantly more elevated levels of hyperactivity-impulsivity than younger girls with ASC.
132
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
May, Rinehart, Wilding & Cornish (2013)
The role of attention in the academic attainment of children with autism spectrum disorder
21/2295%
Australia Quantitative. Cross-sectional design.
Parent-reported attention symptoms; attention tasks; school mathematics and reading attainment.
N=124 (7–12 years)
ASC females, n=32; ASC males, n=32; TD females, n=30; TD males, n=30
No significant sex/gender differences on the sustained attention or attention switching tasks.
No significant differences in reading and mathematics performance between boys and girls with ASC.
Noterdaeme, Mildenberger, Minow & Amorosa (2002)
Evaluation of neuromotor deficits in children with autism and children with a specific speech and language disorder.
17/2277%
Germany Quantitative. Cross-sectional design.
Standardised neurological examination. Measures of performance time for the domains of fine motor skills, coordination and balance.
N=22 (mean ages 8-9 years old)
ASC females, n= 3; ASC males, n= 8; TD females, n=1; TD males, n=10
No significant differences between boys and girls on any of the five motor domains for the ASC group or the TD groups.
Children with ASC had significantly more motor problems than TD children on: fine motor, oral, coordination, balance and gross motor neurological subsystems.
Oswald, Winter-Messiers, Gibson, Schmidt, Herr, & Solomon (2016)
Sex differences in internalizing problems during adolescence in autism spectrum disorder
20/2291%
USA Quantitative. Cross-sectional design.
Revised Children's Anxiety and Depression Scale (parent rated); Multidimensional Anxiety Scale for Children.
N=64 (aged 12-18 years)
ASC females, n=14; ASC males, n=18; TD females, n=;14 TD males, n= 18
ASC females exhibited significantly greater depressive symptoms than ASC males and TD females particularly during early adolescence.
Parish-Morris, Liberman, Cieri, Herrington, Yerys, Bateman, Donaher, Ferguson, Pandey & Schultz (2017)
Linguistic camouflage in girls with autism spectrum disorder.
20/2291%
USA Experimental. Logistic regression models assessed effects of age, IQ, sex, and ASD symptoms on total ‘um’ total ‘uh’and ‘um to uh’ ratios.
Participant IQ was estimated using the DAS-II; ADI-R; VABS; SCQ; ADOS speech segments transcribed.
N=82 (aged 6-17 years)
ASC females, n= 16; ASC males, n= 49; TD females, n=9; TD males, n=8.
TD and ASC girls exhibited significantly higher UM ratios than boys with ASC. Girls in both groups suppressed UH relative to their male peers.
Filled pause differences in boys and girls with ASC were not attributable to increased social pragmatic ability in girls, as girls and boys in had equivalent social communication skills and comparable ASC symptom severity.
133
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Pathak, Bennett & Shui (2017)
Correlates of adaptive behavior profiles in a large cohort of children with autism: the autism speaks Autism Treatment Network registry data.
17/2277%
USA Quantitative. Cross-sectional design. Analysis of existing data set (ATN registry)
IQ and VABS scores.
N= 2538 (aged 5 to 17 years)
Grouped by IQ: Borderline IQ = 70-85; Average IQ > 85) and age (5-10 and 11-17 years), and gender.
Females with IQ > 85 had significantly higher adaptive and communication scores than males.
Pisula, Pudło, Słowińska, Kawa, Strząska, Banasiak & Wolańczyk (2017).
Behavioral and emotional problems in high-functioning girls and boys with autism spectrum disorders: Parents’ reports and adolescents’ self-reports.
19/2286%
Poland Quantitative. Cross-sectional design. Correlations between parents’ and adolescents’ ratings also measured.
CBCL (parent reported), Youth Self-Report
N=118 (aged 11-18 years)
ASC females, n= 35; ASC males, n= 35; TD females, n=24; TD males, n=24.
ASC adolescents presented higher levels of behavioural and emotional problems than TD adolescents, according to both parent and the adolescent self-reports. No significant sex/gender differences were found.
Adolescents with ASC see their problems as less severe compared to their parents, while the reverse is true of TD adolescents.
Ross, Del Bene, Molholm, Frey & Foxe (2015)
Sex differences in multisensory speech processing in both typically developing children and those on the autism spectrum.
19/2286%
USA Quantitative. Experimental. Independent measures design.
Responses on audio-visual integration task.
N= 175 (aged 5-17)
ASC females, n=15; ASC males, n = 58; TD females, n = 47; TD males, n = 55.
Both TD and ASC females were significantly superior in their ability to recognize words under audio-visual listening conditions compared than TD and ASC males.
Development of audio-visual integration is delayed in male relative to female children, both in TD and ASC children.
134
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Rynkiewicz & Łucka (2015)
Autism spectrum disorder (ASD) in girls. Co-occurring psychopathology. Sex differences in clinical manifestation.
14/2264%
Poland Quantitative. Cross-sectional design.
ADOS (polish version); AQ (parent-reported whilst older adolescents completed self-report version); Australian Scale for Asperger Syndrome; Girls’ Questionnaire for Autism Spectrum Conditions)
N=31 (aged 10 – 20 years)
ASC females n=15; ASC males, n= 16.
Girls communication, both verbal and gestures was significantly better than boys.
Girls presented with significantly more abnormalities in sensory profile. Girls significantly greater risk for developing anxiety, depression, suicidal ideation and psychiatric hospitalisation. Boys significantly greater risk for co-occurring ADHD, OCD and tics.
Rynkiewicz, Schuller, Marchi, Piana, Camurri, Lassalle & Baron-Cohen (2016)
An investigation of the ‘female camouflage effect’ in autism using a computerized ADOS-2 and a test of sex/gender differences.
15/2268%
Poland Quantitative. Experimental independent measures design and cross-sectional survey.
The ‘Faces Test’ and the ‘Eyes Test’.
N=33 (aged 5-10 years)
ASC females, n = 16; ASC males, n = 17.
Females found to use significantly more gestures and more 'vividly' than males. Females made significantly more mistakes on emotion recognition.
Parents of ASC boys rated their current communication skills significantly better than did parents of ASC girls.
Solomon, Miller, Taylor, Hinshaw & Carter (2012)
Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders.
20/2291%
USA Quantitative. Cross-sectional design.
WASI; ADOS; SCQ; SRS; CCC; RBS; The Behaviour Assessment System for Children; Children's Depression Inventory.
N= 76 (aged 8-18 years)
ASC females, n=20; ASC males, n = 20; TD females, n = 19; TD males, n = 17.
ASC symptom profiles were similar in boys and girls with ASC.
Adolescent girls with ASC evidenced significant internalizing symptoms compared to boys with ASC and TD girls.
ASC boys presented with more pronounced (marginally significant) restricted interests, than ASC girls.
135
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Stern, Gadgil, Blakeley-Smith, Reaven & Hepburn, (2014)
Psychometric properties of the SCARED in youth with autism spectrum disorder.
19/2286%
USA Quantitative. Cross-sectional design.
Structured clinical interview.ADIS; ADOS; SCQ; SCARED.
Children N=83 (aged 7-14 years):ASC females, n=11; ASC males= 72.
Adolescents N= 36 (aged 13-18 years): ASC females, n=11; ASC males= 25.
No significant sex/gender differences in child-reported anxiety symptoms. Parent-reported social anxiety scores were significantly higher for female children than for male children (p=.008).
Supekar & Menon (2015)
Sex differences in structural organization of motor systems and their dissociable links with repetitive/ restricted behaviours in children with autism.
19/2286%
USA Quantitative. Cross-sectional analysis of existing data sets (NDAR and ABIDE)
ADI-R: social, communication and repetitive/restricted behaviours (RRB) domains.
N=792 (aged 7-13 years)
All with ASC diagnosis(i) NDAR dataset: Females, n=128; males, n= 614 (ii)ABIDE dataset: Females, n=25; males, n=25.
No significant sex/gender differences in scores on the social domain (p = .28) or the communication domain (p = .12) of the ADI-R. ASC girls showed less severe RRB as measured by the ADI-R, compared to ASC boys (p<.01). This pattern was shown across both datasets.
Wakabayashi, Baron-Cohen, Uchiyama, Yoshida, Tojo, Kuroda & Wheelwright (2007)
The autism-spectrum quotient (AQ) children’s version in Japan: a cross-cultural comparison.
19/2286%
Japan Quantitative.Cross-sectional analysis.
AQ (Japanese version)
N = 475 (aged 6-15 years)
ASC females, n=30; ASC males, n = 73; TD females, n =184; TD males, n = 188.
No significant sex/gender differences were found in ASC groups on any domain measuring ASC symptoms. The groups of children with HFASC scored significantly higher than controls.
Wang, Deng, You, Chen, Li, Tang, Ceng, Zou, Zou (2017)
Sex differences in diagnosis and clinical phenotypes of Chinese
18/2282%
China Quantitative.Cross-sectional analysis.
ADI-R; ADOS.
N= 597(24-83 months old)
Verbal group:ASC females, n=134; ASC males, n=463.
Girls showed significantly greater socio-emotional reciprocity (use of the body to communicate, offering comfort, quality of expression of social interest, appropriate facial expressions, appropriateness of social response) than boys (p=.049).
136
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Children with autism spectrum disorder
Girls also showed significantly fewer RRBs than boys (p<.001 on ADI-R, p=.006 on ADOS), and the type of RRBs in girls differ from those in boys. The ADI-R was found to be less sensitive in girls, particularly for assessment in the RRBs domain.
Zarokanellou, Kolaitis, Vlassopoulos & Papanikolaou (2017)
Brief report: A pilot study of the validity and reliability of the Greek version of the Social Communication Questionnaire.
17/2277%
Greece Quantitative.Cross-sectional correlation design.
SCQ (Greek translated)
N=103 (aged 7-10 years)
ASC females, n=7; ASC males, n = 19; TD females, n = 38; TD males, n = 39.
No significant difference between girls and boys in the ASC group or TD group in overall score on SCQ.
ABIDE Autism Brain Imaging Data ExchangeAC Autism ConsortiumADI-R Autism Diagnostic Interview–RevisedADIS Anxiety Disorders Interview Schedule-Parent VersionADOS Autism Diagnostic Observation ScheduleAGRE Autism Genetics Resource ExchangeASC Autism Spectrum ConditionATN Autism Treatment NetworkAQ Autism QuotientASSQ Autism Spectrum Screening QuestionnaireCARS Childhood Autism Rating ScaleCCC Children's Communication ChecklistCBCL Child Behaviour ChecklistDAS-II Differential Ability Scales-IIDSM-5 Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition)IQ Intelligence quotientNDAR National Database for Autism ResearchRBS Repetitive Behaviours ScaleRBQ Repetitive Behaviour QuestionnaireSCAREDScreen for Child Anxiety-Related Emotional DisordersSCQ Social Communication QuestionnaireSRS Social Responsiveness ScaleSSC Simons Simplex ComplexVABS Vineland Adaptive Behaviour ScaleWASI Wechsler Abbreviated Scale of IntelligenceWISC Wechsler Intelligence Scale for Children
137
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Results
The included studies used a range of methodological approaches, outcomes and
focussed on varied aspects of ASC presentation. One study used primarily qualitative
methodology (Cridland et al., 2014) whilst three used mixed-methodologies (Dean et al.,
2017; Goddard et al., 2014; Jamison et al., 2017). The remaining 32 studies used quantitative
methodologies, almost all of which employed a cross-sectional design, either collecting
questionnaire measures at a single time point or analysing existing data and comparing
outcomes according to sex/gender. Five studies adopted an experimental design to assess
participants’ abilities on tasks (Kauschke et al., 2016; Kim et al., 2015; Parish-Morris et al.,
2017; Ross et al., 2015; Rynkiewicz et al., 2016).
The results have been organised according to the broad aspect of ASC presentation
examined; Social Communication; RRBIs; Adaption, Emotional and Behavioural
Difficulties; Cognitive and Motor Functions; and Other Traits. Design, sample
characteristics, findings and quality ratings of the studies are summarised in Table I.
Participants
The total number of participants with ASC across the 36 studies was 13,740. Of these
participants, 81.8% (11,238) were male. This means that at 18.2%, women were under-
represented in the samples. The range of ages sampled across the studies covers most of
childhood and adolescence (24 months- to 18 years-old). Most studies were conducted in
Western populations, including Europe (Germany, Greece, Finland, Poland, Sweden and the
UK), USA, and Australia. Three of the studies were conducted in China and Japan.
138
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Measures
A variety of screening and diagnostic ASC measures, psychological wellbeing and
adaptive functioning measures were used in the studies. The measures most commonly used
in the studies are summarised in Table II.
Table II.
Descriptions of the most commonly used diagnostic measures in the literature
Measure Description
Autism Diagnostic Observation Schedule (ADOS; Lord et al., 1989)
A semi-structured, standardised assessment of communication, social interaction, imaginative play and restricted and repetitive behaviours. Presents various activities that elicit behaviours directly related to diagnosis of ASCs.
The Autism Diagnostic Interview-Revised (ADI-R; Rutter, Le Couteur & Lord, 2003)
A caregiver-report semi-structured interview, covering early development, verbal and non-verbal communication, social development and stereotypic interests and behaviours. Three domain scores (social interaction, communication, and restrictive and repetitive behaviour) can be calculated.
Autism Spectrum Screening Questionnaire (ASSQ; Ehlers, Gillberg & Wing, 1999)
A 27-item parent or teacher-report questionnaire for children or adolescents (6 to 17 years of age). Designed as an initial screen for HFASCs.
The Children's Communication Checklist-2 (CCC; Bishop 2003).
70-item parent-report questionnaire which assesses communication abilities.
Social Communication Questionnaire (SCQ; Rutter et al. 2003).
A 40-item questionnaire version of the ADI-R.
Repetitive Behaviours Scale-Revised (RBS-R; Lam & Aman, 2007)
A 44-item caregiver-report questionnaire that is used to measure the breadth of repetitive behaviour in children and adolescents (aged 6-17 years) with ASCs.
The Repetitive Behaviour Questionnaire-II (RBQ-II; Leekam et al 2007).
Determines the presence of repetitive behaviours in children based on the ICD-10 criteria for autism.
Social Responsiveness Scale (SRS; Constantino 2002, Constantino et al 2003).
A 65-item parent-report questionnaire to assess social awareness, social information processing, reciprocal social communication, social anxiety/avoidance, autistic preoccupations and traits.
139
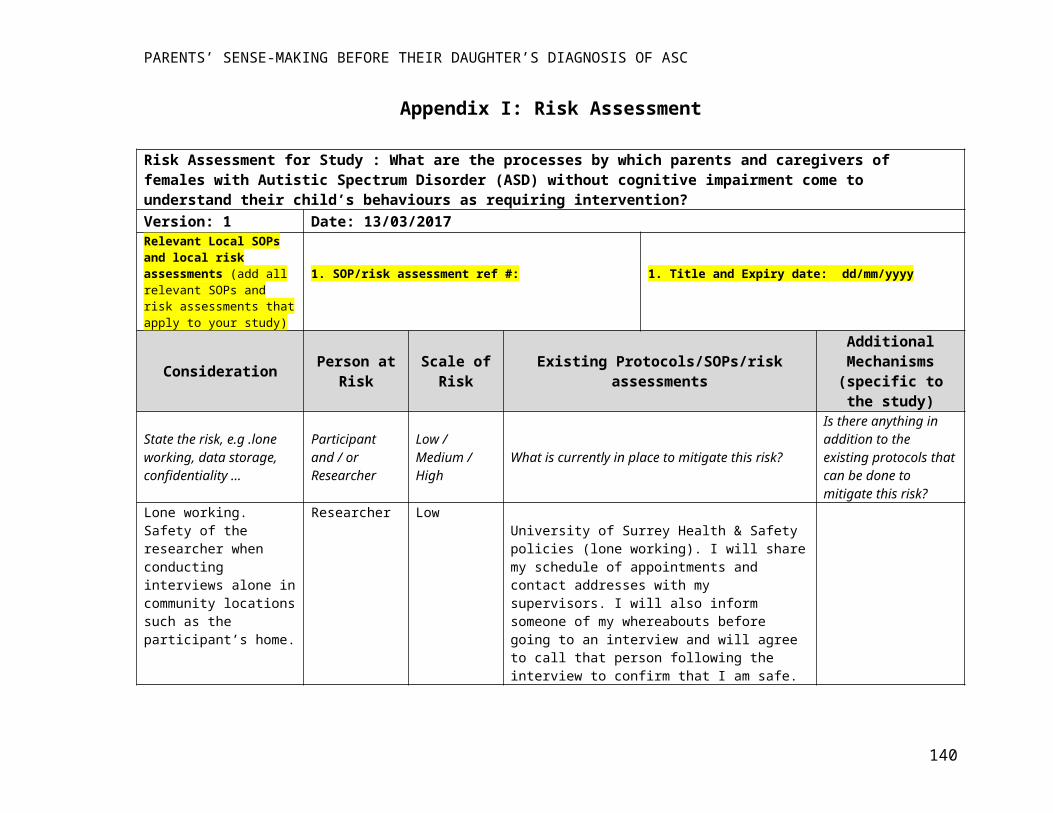
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
1. Clinical and Diagnostic Features of ASC
The studies reporting on overall differences on diagnostic measures are summarised
first. The studies that reported on separate constructs of diagnostic features are summarised
subsequently.
1.1 Overall Diagnostic Scores
Ten studies reported on overall differences between male and female children
diagnosed with ASC using scores from a variety of diagnostic measures and screening tools
(ADOS, ADI-R, AQ, ASSQ and SCQ). These studies all reported no differences between the
sex/genders on overall ASC scores (Baron-Cohen et al., 2006; Fulton, et al., 2017; Hiller et
al., 2014; Holtmann et al., 2007; Kopp & Gillberg, 2011; May et al., 2014; Parish-Morris et
al., 2017; Solomon et al., 2012; Wakabayashi et al., 2007; Zarokanellou et al., 2017). The
studies reported on children as young as 29 months (Fulton et al., 2017) to 18 years.
Some studies also reported on TD children’s scores on the same measures and found
that TD boys scored significantly higher than TD girls (Baron-Cohen et al., 2006;
Wakabayashi et al., 2007).
1.2 Social Communication
The construct of social communication has many facets including empathy for others,
use of gestures and emotion recognition. Twenty-two of the studies reviewed reported on
these different features, and/or on the overall construct. Overall findings from diagnostic
measures and clinician ratings are summarised first, followed by more particular aspects of
social ability and communication.
140
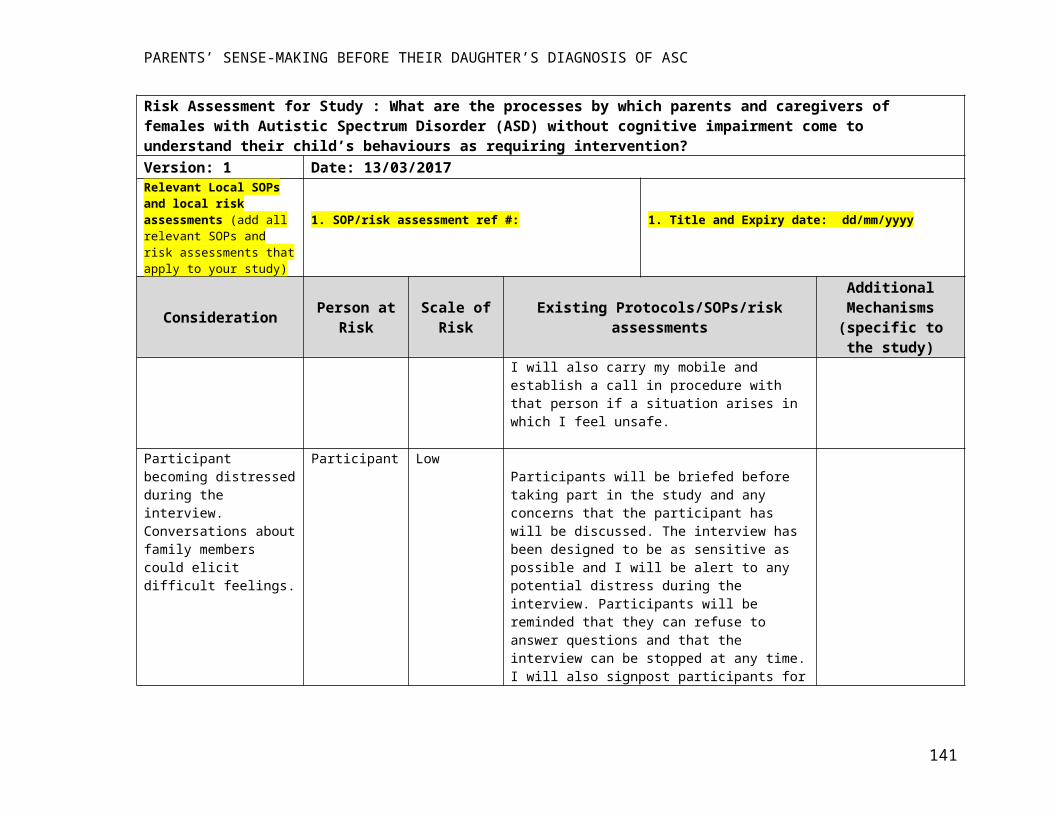
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
1.2.1 Overall Diagnostic Scores
Ten studies reviewed parent-reported measures of social communication from clinical
samples (Frazier et al., 2014; Head et al., 2014; Holtmann et al 2007; Howe et al., 2015;
Kumazaki et al., 2015; May et al., 2016; May et al., 2014; Parish-Morris et al., 2017;
Rynkiewicz, et al, 2016; Supekar & Menon, 2015). The majority of these studies found no
differences between sex/genders with regard to social ability and communication (Frazier et
al., 2014; Holtmann et al., 2007; Kumazaki et al., 2015; May et al., 2014; Solomon et al.,
2012; Supekar & Menon, 2015). Additionally, May and colleagues (2014) showed that
symptom severity stayed stable after a one year follow-up. Unsurprisingly, ASC groups
showed more social and communication difficulties than typically developing (TD) groups
(Solomon et al., 2012; May et al., 2016). Jamison and colleagues’ (2017) qualitative study
asking clinicians to reflect and comment on their perceptions and experiences of gender
differences in ASCs, also revealed no differences between the sex/genders on social
communication features.
1.2.2 Social Ability - Diagnostic Scores
The majority of studies found no sex/gender differences on overall parent-reported
scores measuring social skill (Hiller et al., 2014; Howe et al., 2015; May et al., 2016; Supekar
& Menon, 2015). However, Wang and colleagues (2017) found that parents rated their ASC
girls as having better social skill than their ASC boys on measures of socio-emotional
reciprocity and social skill. This study’s participants were younger (aged 24-83 months) than
the other studies. This could suggest that before they reach their sixth birthday, ASC girls’
social difficulties are either; not present, or as apparent to parents as the social difficulties
found among ASC boys. Interestingly, Hiller and colleagues found that teachers reported
fewer concerns for girls than boys regarding their social skill, whilst there were no overall
141
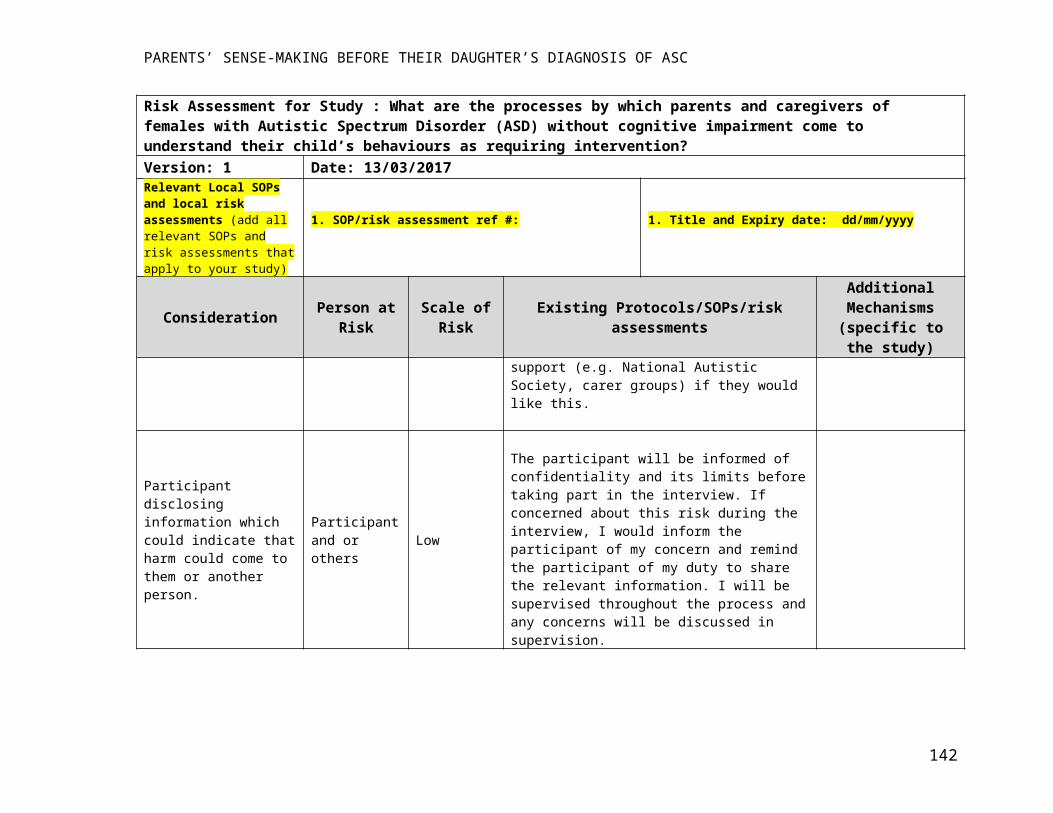
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
sex/gender differences on overall peer relationships and social-emotional reciprocity criteria
on diagnostic measures (Hiller et al., 2014). Perhaps this shows a discrepancy between
teacher’s perceptions of social skill, and those of clinicians and parents (i.e. that teachers
perceive autistic girls as more socially able than autistic boys in comparison to parents, who
might see more difficulty at home). Additionally, the different ratings by teachers and parents
could suggest that in the context of school, autistic girls’ social difficulties are less
perceptible than autistic boys’.
Where no sex/gender differences were found overall, two studies that examined
diagnostic criteria in more detail found more nuanced differences in how they were met
(Hiller et al., 2014; May et al., 2016). Examining existing data, Hiller and colleagues (2014)
found that girls presented with better use of social gestures, whilst their ability to understand
and interpret other people’s nonverbal gestures was not significantly different to boys. This
perhaps suggests an ability to act socially without understanding others’ social behaviour.
Additionally, the type of impairments on the ‘social-emotional reciprocity’ criterion was
different; girls were rated as more able to engage in reciprocal conversation, share interests
and achievements with others, and had better and more ‘normal’ imaginative play than boys.
Friendship difficulties also manifested in different ways; girls were found to be more able to
initiate friendships but had trouble maintaining them due to a need to have control over play.
Girls were also more able to regulate and manage their behaviour in public (e.g. monitoring
volume of voice, avoiding socially inappropriate comments and externalising behaviour).
These observations fit with the findings that teachers perceive girls as more socially able than
autistic boys.
142
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
1.2.3 Communication - Diagnostic Scores
Many aspects of communication were reported on, making findings challenging to
bring together. However, the studies that reported on ‘communication’ generally, either found
no sex/gender differences (Supekar & Menon, 2015) or found that communication difficulties
were more evident for boys, sometimes irrespective of ASC diagnosis (Hiller et al., 2014;
May et al., 2016; Pathak et al., 2017; Rynkiewicz & Łucka, 2015). Again, some differences
were found on more specific aspects of the communication construct, generally showing
more communication skill in girls than boys. For example, boys generally made more
‘inappropriate initiations’, talking repetitively about things that no-one is interested in (May
et al., 2016). Hiller and colleagues (2014) found that the abilities to integrate nonverbal and
verbal gestures and use pragmatic language was significantly predictive of being female.
Only in one study, (Rynkiewicz et al., 2016) were boys rated by their parents as having better
communication skills than girls on the SCQ. This study’s participants were 5-10 years-old
whilst the other studies’ participants were mostly around 10-18 years-old. One reason for this
study’s outlying results could be that girls who have already been diagnosed in this age group
may have had more obvious communication difficulties than girls with more subtle
symptoms that are not diagnosed until later.
1.2.4 Soc ial Communication – Other Measures/ Designs
Generally, experimental studies found that girls with ASC had better expressive and
receptive communication than boys whilst few sex/gender differences were found in studies
that measured emotion recognition and/or social motivation. Studies observing friendship
patterns, reported that the social challenges of girls with ASC look different and are perhaps
less obvious, than those of boys with ASC.
143
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Receptive and Expressive Communication
Using an “objective computerised technique” to measure gestures during two ADOS-
2 tasks, Rynkiewicz and colleagues (2016) found that ASC girls used gestures more
frequently and more “vividly” than ASC boys. Whilst this study is robust in controlling
report bias, it is not clear whether more vivid use of gestures is indicative of better body
language use in communication (i.e. there was no interpretation of the relevance of the
gestures to the message conveyed, or whether gestures enhanced or hindered
communication). Interpretation of gestures according to context may have proved useful, but
perhaps would come at the cost of introducing observer bias. These findings are similar to
those found by Hiller and colleagues (2014) on teacher-reported measures, that females are
more able in their use of social gestures and ability to integrate nonverbal and verbal gestures.
Kauschke and colleagues (2016) analysed children’s discourses telling a story from a
wordless picture book. They found that ASC girls acknowledged internal states (e.g.
physiological sensations and modality of events) more than ASC boys, though this did not
extend to emotional terms. The evidence about sex/gender differences in the use of internal
state language in neuro-typical children is inconclusive: some studies have found that girls
use a greater proportion of internal state terms than boys (e.g. Hughes and Dunn, 1998) whilst
some have found no differences (e.g. Peterson & Biggs, 2001). Parish-Morris and colleagues
(2017) found that both ASC and TD females use ‘pragmatic language-markers’ such as ‘um’
better than their male peers. They suggest that this may normalize the way ASC girls sound
relative to other children, serving as “linguistic camouflage”.
Investigating children’s abilities to integrate auditory and speech signals, Ross and
colleagues (2015) found that females, both TD and with ASC, performed significantly better
at recognising words than boys.
144
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Emotion Recognition and Social Motivation
Kim and colleagues (2015) observed no sex/gender differences in ASC or TD groups
on a computerised emotion recognition task. Interestingly, they also found no differences
between ASC and TD groups on affect recognition tasks. However, the study had few
participants, and subtle differences may not have reached significance. Another study using
computerised emotion recognition tests found that ASC girls made significantly more
mistakes than ASC boys (Rynkiewicz et al., 2016) This is surprising given that in TD
populations, a subtle female advantage for facial emotion recognition has been evidenced
(Lawrence, Campbell & Skuse, 2015; Montirosso, Peverelli, Frigerio, Crespi, & Borgatti,
2010).
Using avatars in a video game, Kim and colleagues (2015) also measured children’s
preference for interpersonal closeness/distance or ‘social motivation’ and observed no
sex/gender differences in the ASC or TD groups.
Friendship
In a playground observation of 6 to 8 year-old children, Dean and colleagues (2017)
suggest that social challenges of ASC boys look different, and are more obvious, than those
of ASC girls. ASC girls tended to stay in close proximity to social groups, perhaps masking
social challenges from onlookers whilst TD boys’ play tended to be physically active or
structured making it relatively easy to spot ASC boys, who were often wandering alone apart
from the game. Investigating the perspectives of children using the ‘Friendships Survey’
(Cairns & Cairns, 1994), Dean and colleagues (2014) found that boys with ASC were more
overtly socially excluded, compared to girls with ASC who were ‘overlooked’, i.e. not put
down on their peer’s friend lists.
145
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Head and colleagues (2014) found that regardless of diagnosis, girls and their parents’
ratings on the Friendship Questionnaire (Baron-Cohen & Wheelwright, 2003) were higher
than boys’, indicating higher levels of sociability, emotionality and friendship. The largest
difference between parent and child reports on social difficulty was found between ASC
females and their parents, perhaps suggesting that parents are less aware of their daughter’s
challenges, compared to parents of ASC boys.
Analysing interviews with mother-daughter dyads about their experiences of ASC,
Cridland and colleagues (2014) found that some challenges were similar to those of boys, for
example, transitioning to and coping with high school and learning about personal
boundaries. Adolescent girls with ASC expressed specific difficulty with socialising with TD
girls. These were difficulties with following conversations because of the length of time
needed to process information, and difficulty fitting in due to disinterest in fashion.
Altogether, these studies suggest that although friendship difficulties exist for both
girls and boys with ASC, these may look different according to a child’s sex/gender and are
perhaps less obviously observable for girls than boys.
1.3 Restricted and Repetitive Behaviours and Interests
Nine studies compared the severity and/or type of RRBIs between girls and boys with
HFASC using parent-reported measures and qualitative methodology (Jamison et al., 2017).
Except for two studies that reported no differences between males and females (Holtmann et
al., 2007; May et al., 2014), ASC females showed significantly fewer RRBIs compared with
ASC males (Frazier et al., 2014; Hiller et al., 2014; May et al., 2016; Solomon et al., 2012;
Supekar & Menon 2015; Wang et al., 2017). In general, studies that had larger sample sizes,
for example those using existing datasets, were more likely to report sex/gender differences
on RRBIs, perhaps suggesting that differences are subtle and require large samples to reach
146
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
significance. Some researchers reported more RRBI symptoms in boys regardless of presence
of ASC diagnosis (e.g. repetitive motor movements; May et al., 2016) whilst others reported
no differences between the sex/genders in TD children (e.g. Solomon et al., 2012).
Four studies reported on various domains of RRBI (Hiller et al., 2014; Jamison et al.,
2017; Rynkiewicz & Łucka, 2015; Solomon et al., 2012). No sex/gender differences were
reported in any of the following domains: stereotyped behaviour, self-injurious behaviour,
compulsive behaviour, ritualistic behaviour, sameness behaviour, routine adherence,
stereotyped movement and preoccupation with parts of objects. However, females were less
likely to present with ‘restricted and fixated interests’ (Jamison et al., 2017; Solomon et al.,
2012) and ‘stereotyped use of objects’ such as lining up or sorting behaviour (Hiller et al.,
2014).
Hiller and colleagues (2014) reported on differences in the type of RRBIs. They found
that girls had more restricted interests in the ‘seemingly random’ category (e.g. rocks,
stickers, pens) whilst boys were more likely to have fixations with screen time, such as
obsessive gaming. Conversely, however, in two studies ASC boys were more likely to be
rated as having ‘unusual interests’ than ASC girls (Kumazaki et al., 2015; May et al., 2016)
though the nature of these interests were not reported on. This highlights an issue around the
subjectivity of what is and is not ‘unusual’ which will be considered further in the discussion.
1.4 Adaption, Emotional and Behavioural Difficulties
Twelve studies reported on various aspects of the emotional and behavioural
tendencies of children with ASC. Some of these commented broadly on emotional and
behavioural problems. These are summarised first, followed by studies that commented on
constructs of depression, anxiety, sensory difficulty, adaption and hyperactivity. Although the
picture was complex, in general, females were reported to have more difficulty with
147
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
symptoms of depression, anxiety and sensory sensitivity, whilst males were more likely to
present with symptoms of hyperactivity. Generally, females were rated by their parents as
having similar adaptive daily living skills to males.
1.4.1 Emotional and Behavioural Problems
Reporting broadly on behavioural and emotional difficulties, studies found that both
sex/genders with ASC presented with more difficulty on self- and parent-report measures
than their TD peers (Holtmann et al., 2007; Hurtig et al., 2009). Pisula and colleagues (2017)
found no differences between the sex/genders for adolescents with ASC, both on the parent-
reported Child Behaviour Checklist (CBCL; Achenbach and Rescorla, 2001) and self-
reported Youth Self-Report (Achenbach, 1991). In contrast, other studies found more
‘coexisting psychopathology’ for girls than boys, for example, social, attention and thought
problems rated by parents (Holtmann et al., 2007) and ‘thought problems’ both parent and
child rated (Hurtig et al., 2009).
Internalising and Externalising
There were mixed findings regarding patterns of internalising and externalising
problems between the studies. This could be due to a range of factors such as: lacking
consistency in conceptualisation and measurement; the range of perspectives reported on (i.e.
parent, self, teacher); and the broad age range of participants (5-18 years-old). However,
generally, adolescent ASC females were found to score more highly on internalising
symptoms than ASC males, whilst the opposite pattern was found for externalising
symptoms.
Internalising. Solomon and colleagues (2012) found no sex/gender differences on
‘internalising psychopathology’ or depression measured by the parent-rated Behaviour
148
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Assessment System for Children (Reynolds & Kamphaus, 2004) and the self-rated Children’s
Depression Inventory (Kovacs, 1992) for TD or ASC children. They found that both
sex/genders with ASC had higher depression scores than their TD peers. However, analysing
adolescents alone, ASC females had significantly higher internalising scores than ASC males
and TD females, whilst ASC boys had similar internalising scores to their TD peers.
Generally, female children and adolescents with ASC exhibited more depressive
symptoms (Oswald et al., 2016; Rynkiewicz & Łucka, 2015), showed greater irritability
(Frazier et al., 2014) and were more at risk of developing suicidal ideation and of psychiatric
hospitalisation (Rynkiewicz & Łucka, 2015) than ASC males and TD females. Oswald and
colleagues (2016) found that depressive symptoms are particularly severe for females during
early adolescence.
Additionally, ASC females exhibited greater anxiety symptoms on both parent and
self-reported measures than ASC males (Fulton et al., 2017; Hiller et al., 2014; Rynkiewicz &
Łucka, 2015; Lohr, 2017; Solomon et al., 2012), and TD females (Solomon et al., 2012).
Social anxiety symptoms were consistently higher for ASC females than ASC males (Fulton
et al., 2017; Hiller et al., 2014; Kopp & Gillberg, 2011; May et al., 2014; when rated by
parents Stern et al., 2014), a pattern found in TD children too (May et al., 2014). However,
there were some exceptions to this pattern. No differences between the sex/genders were
found for ASC groups in; self-ratings of separation anxiety, or panic in late adolescence
(Oswald et al., 2016) and self-reported anxiety symptoms (Stern et al., 2014). Lohr and
colleagues (2017) found that girls with ASC and their parents may agree more closely in their
reports of anxiety than parents of boys with ASC. This raises questions about the validity of
parent-report measures for mood disorders which may explain some of the differences in
findings.
149
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Externalising. Hiller and colleagues (2014) found that teachers reported substantially fewer
concerns about ASC females compared to ASC males for ‘externalising behaviours’. May
and colleagues (2014) found no differences between the sex/genders in parent-reported
ratings of ‘oppositional behaviours’ despite having more prevalence in boys than girls in TD
populations. This highlights differences in perspective based on context (i.e. school versus
home). Several studies found that, like TD children, ASC males were more likely to present
with more hyperactivity, hyperactivity-impulsivity, or have a diagnosis of ADHD than
females (Hiller et al., 2014; Kumazaki et al 2015; May et al., 2016; May et al., 2014;
Rynkiewicz & Łucka, 2015).
1.4.2 Sensory
Two studies reported on sensory profiles and both found females to have more
difficulty in their sensory responses to stimulation than males, e.g. seeking/avoiding certain
sensations (Kumazaki et al., 2015; Rynkiewicz & Łucka 2015).
1.4.3 Adaptive Functioning
Generally, ASC females were rated by their parents as having similar (Fulton et al.,
2017; Pathak et al., 2017) or better (Howe et al., 2015) adaptive daily living skills than ASC
males.
1.5 Cognitive and Motor Functions
Six studies reported on sex/gender differences in relation to some facet of cognitive
functioning. Two of these investigated cognitive profiles using the Wechsler Intelligence
Scale for Children-Japanese version (Koyama et al., 2009; Kumazaki et al., 2015).
Comparing 5 to 9 year-olds, Kumazaki and colleagues (2015) reported no significant
150
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
sex/gender differences on any of the subtests or composites and found a relative weakness on
‘Comprehension’ and strength in Block Design for both sexes. In contrast, comparing six to
twelve-year-olds, Koyama and colleagues (2009) found that girls' subtest profiles were
relatively even and significantly different from the boys', which were characterized by a peak
on Block Design.
Investigating children’s (8-16 years) autobiographical memory and verbal-fluency
ability, Goddard and colleagues (2014) found that irrespective of ASC diagnosis presence,
females produce more detailed and emotional memories and demonstrate superior verbal-
fluency compared to boys. Similarly, Frazier and colleagues (2014) found ASC males more
likely to show a discrepancy in favour of non-verbal IQ, whilst ASC females do not show a
verbal-nonverbal discrepancy.
Measuring various motor skills (fine-motor, gross-motor, coordination, balance and
oral), Noterdaeme and colleagues (2002) found no significant differences between the sexes
on neurological examination or timed tasks in both ASC and TD children. All ASC children
had more motor problems than TD children. May and colleagues (2013) found no sex/gender
differences on sustained attention, attention switching tasks or parent-reported reading or
mathematics performance.
1.6 Other Traits
In establishing a diagnostic measure sensitive for girls with ASC (‘ASSQ-GIRL’)
Kopp and Gillberg (2011) reported on ‘other’ traits associated with ASC. They found that
certain items on their diagnostic measure were more typical of girls than boys with ASC.
These included: "avoids demands", "very determined", "careless with physical appearance
and dress", "interacts mostly with younger children", "different voice/speech" and
"difficulties completing simple daily activities". Subtle distinctions were found that
151
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
differentiated girls from boys: girls scored higher on "different voice" whilst boys scored
higher on "robot-like language"; girls scored higher on "insists on no change" whilst boys
scored higher on "plays with other children only on own terms". It could be that these subtle
differences are impacted by gender expectations, or the way in which we frame and describe
a difficulty according to gender.
Discussion
The results from the review show a complex picture with inconsistent findings for
most of the constructs explored. Generally, on diagnostic measures differences between the
sex/genders were not found in overall scores on social communication, but there were
indications of differences in subscales and in how scores were reached. Mostly, females with
ASC showed less severe RRBIs compared to males, a pattern also found in TD populations.
No sex/gender differences were found in motor skills, or generally in adaptive functioning.
Typically, females had more difficulty with symptoms of depression, anxiety and sensory
sensitivity, whilst males were more likely to present with symptoms of hyperactivity. Few
studies measured the quality of impairments as opposed to the severity of impairments. The
studies that looked past established diagnostic measures found that ASC girls may present
with a surface-level 'look' different from the classic ASC presentation (Dean et al., 2014;
Dean et al., 2017; Parish-Morris et al., 2017; Rynkiewicz et al., 2016). Although the research
shows patterns of difference and similarity between the sex/genders, there are also
contradictions within these findings, which may be due to methodological issues. These are
explored further here.
The literature has so far focused on finding differences between girls and boys in
relation to the established diagnostic profiles or psychopathological symptoms. The findings
that, for example, there are no differences between boys and girls in overall ratings of social
152
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
skill is not surprising given that the studies used children who have already been diagnosed,
using measures that involve assessment of social skill. Most of the studies used diagnostic
measures which were developed as diagnostic measures, and so may not be reliable or valid
as metrics of symptom severity. Moreover, the tools may have low validity in detecting the
‘female phenotype’ of ASC and may not detect subtle differences in characteristics between
the sexes (Dworzynski et al., 2012).
Additionally, the participants used would have received their diagnosis using the same
or similar instruments. Knowledge about ASCs has largely been based on observations of
males. Consequently, the instruments used in diagnosis, such as the ADI-R, may be biased
towards detection of ‘male-like’ symptoms as they have been developed using predominantly
male samples (Constantino, Zhang, Frazier, Abbacchi, & Law, 2010). By already having an
ASC diagnosis, it is possible that female participants present with signs and symptoms that
are more similar to the male phenotype of ASC. If indeed there is a ‘missed’ population of
girls as several researchers have suggested (Attwood, 2006; Giarelli et al., 2010; Gillberg,
1993; Kim et al. 2011; Mattila et al. 2011), these girls may present differently from those
with a diagnosis. In summary, the diagnostic measures may not be sensitive enough to detect
ASC symptoms in females. To develop sex/gender specific behavioural measures of ASC,
more of an understanding around the subtleties of difference in symptoms and how these
intersect with cultural expectations related to gender will need to be established.
Social Context: Perspectives and Expectations
The majority of the studies reviewed did not consider the child’s social context. For
example, the studies included participants that had already been diagnosed which in itself
may impact on other’s perceptions of the child and/or the child’s view of themselves and
therefore their behaviour. That is, parents and children may rate behaviour and emotion in the
153
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
context that they know about the autism, perhaps noticing signs and symptoms that they may
be sensitised to through having the diagnosis.
Additionally, parent-, clinician- and teacher-reported measures are likely to be
impacted by interpreting bias, whereby decisions about what is ‘normal’ are informed by
previous experiences and gendered socio-cultural expectations. Previous evidence indicates
that parents expect more socially desired behaviour from their daughters than sons (Arliss,
1991). This might explain some of the differences found between experimental methods
where computers were used to rate ability compared to human-rated measures. For instance,
the studies using computers to rate expressive and receptive communication abilities,
consistently rated females as having greater skill (Kauschke et al., 2016; Parish-Morris et al.,
2017; Ross et al., 2015; Rynkiewicz et al., 2016), whilst in one of the same studies using the
same children, parents rated their ASC sons as having better communication skills than their
daughters on the SCQ (Rynkiewicz et al., 2016). It may be that ASC symptoms are rated as
more severe on diagnostic instruments for girls due to these higher social expectations.
Likewise, other findings from the reviewed studies may be coloured by these
gendered behavioural standards. The findings from the review that females present less with
‘restricted and fixated interests’ (Jamison et al., 2017) and ‘stereotyped use of objects’ such
as lining up or sorting behaviour (Hiller et al., 2014) may simply reflect a cultural
acceptability and/or gendered expectation that girls like organising. Evidence suggests that in
childhood, shyness is socially acceptable and even encouraged for girls but is not tolerated in
boys (Doey, Coplan & Kingsbury, 2014). Attwood (2006) suggests that ‘unusual behaviour’
displayed by a female may be more likely to be perceived as character traits acceptable for
females, such as ‘shyness’ or ‘passivity’. Parent reports, even when measured by standardised
instruments, inherently contain bias impacted by cultural and socialised understandings of
what a boy and a girl ‘should’ be like, and consequently what is expected and unusual.
154
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Clinicians and teachers may have different expectations and be influenced in their decision
making by their own contexts, both professionally and personally. This is further
complicated by evidence that girls may be more likely to mask certain behaviours in public
settings in order to fit in. Thus, further exploration of the context in which ASC symptoms
present and are perceived, and how parents’, teachers’ and clinicians’ expectations are
accounted for in diagnosis is needed.
Differentiating Constructs
Perhaps a challenge of the culturally prevailing medical model is that symptoms of
ASC and other difficulties are assumed to be independent, not only from the context in which
they are shaped and observed but also from one another. For example, in one of the studies
reviewed, Holtmann and colleagues (2007) reported that ASC females showed more social
impairment, social immaturity and social dependency and more inattentive, impulsive and
hyperactive as well as compulsive and bizarre behaviours on parent-rated ‘psychopathology’
ratings. However, in the same study, no differences between the sex/genders were found on
the core triad of ASC impairment as rated on the ADI-R. This highlights the difficulty in
discriminating between what is perceived to be autism and what is perceived to be part of a
similarly defined difficulty. Given the uncertainty around the aetiology of ASCs, and the fact
that they are behaviourally diagnosed, it is very difficult to decipher what is, and is not, part
of autism based on measures that are designed to detect ‘abnormality’. In psychiatric settings,
evidence shows that doctors attribute different meaning to identical symptoms according to
the patient’s gender (Malterud & Okkes, 1998) and are more likely to attribute women’s
illness to psychiatric disorders than men’s (World Health Organization, 1998). Using
Holtmann and colleague’s study as an example, although the symptoms are similar, it may be
that we understand them under the constructs of ‘emotionality’ for a girl, and ‘autism’ for a
155
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
boy, perhaps because our social contexts make these differentiations more likely. Linked to
this, Lohr and colleagues (2017) evidenced that parents interpret girl’s ‘externalising
behaviours’ as anxiety whilst Stern and colleague’s (2014) found a difference in parents’ and
adolescents’ perceptions of anxiety. This highlights that diagnostic instruments measure
interpretations of behaviour and emotion, rather than an objective reality. Additionally, none
of the studies measuring diagnostic ratings reported on the sex/gender of the person
completing the measure. It would be interesting to explore further whether ratings are
impacted by the sex/gender of the observer.
Additionally, the studies mostly did not consider how other emotions might impact on
the presentation of autism. For example, Kim and colleagues’ (2015) study using a video
game to measure emotion recognition, may have reduced social anxieties in participants by
minimising the ‘realness’ of the situation. Interestingly, they found no sex/gender differences
in emotion recognition, and no differences between ASC and TD groups. This could indicate
that anxiety is one context which impacts on particular ASC symptoms. These interactions
warrant further exploration.
Social Context: Age and Gender
Many aspects of social functioning in TD populations are known to vary as a function
of age and gender. For example, there is evidence to suggest that before the age of 5 years-
old, girls are slightly ahead of boys in verbal skills (Bornstein, Hahn & Haynes, 2004). A
limitation of many of the studies reviewed was the nature of the between-group comparison
of males and females with ASC, sometimes not controlling for gender differences in TD
populations. The research literature suggests that parent’s perceptions, play practices and
styles of interaction differ according to their child’s sex/gender (Stern & Karraker, 1989) and
that socialisation strategies used with females provide an environment more supportive of
156
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
social communication development than is the case for males (Bussey & Bandura, 1999;
Huttenlocher, Haight, Bryk, Seltzer & Lyons, 1991; Leaper, Anderson & Sanders, 1998;
Malatesta & Haviland, 1982). For example, TD infant girls hear more language, receive more
eye contact, and have more opportunities to engage in social-emotional interaction than infant
boys (Christensen, Bilder, Zahorodny, Pettygrove, Durkin et al., 2016). This could contribute
to observed sex/gender differences in typical development and serve as a protective factor
against social communication difficulties for females. Some studies found significant
sex/gender differences in the ability of children with ASC and TD children (e.g. in
understanding language, Ross et al, 2015; May et al., 2016). Using between-group designs we
may risk interpreting differences as showing a behavioural phenotype of ASC, when they
may simply represent a restatement of sex differences in typical development and gender
socialisation patterns.
This again, raises the question about how difference and difficulty is perceived,
according to the context within which the judgement is made. Hartung and Widiger (1998)
observed that when the expression of symptoms of a disorder differs by gender, the
development of diagnostic criteria is biased toward the gender that externalises distress and
exhibits ‘socially unacceptable’ behaviour. They propose that individuals are more likely to
be referred for assessment if they demonstrate social inappropriateness, which in turn may be
determined by the social and cultural context of the individual. TD boys showed more
externalising emotions than TD girls at toddler/preschool and middle childhood and fewer
externalising emotions than TD girls in adolescence. Similarly, ASC presentation may
change and/or be more noticeable for girls in adolescence. Boys therefore may pose more of a
challenge for others at younger ages, whilst girls may show their distress at a later point.
Accounting for these patterns in typically developing children is important for making
157
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
interpretations of ‘abnormality’ as well as understanding why girls may not be ‘picked up’ so
early on.
Similarly, boys and girls may show their emotional distress in ways that are more
socially acceptable according to gender norms. Lohr and colleagues (2017) found that girls
with ASC and their parents agree more closely in their reports of anxiety, than boys with
ASC and their parents. This may highlight a context in which it is more socially acceptable
for girls to express anxiety than it is for boys. In one of the qualitative studies reviewed,
which explored the experience of girls with ASC, Cridland and colleagues (2014) suggest a
specific difficulty for girls may be in the context of interactions between girls being more
socio-emotionally complex than boys in adolescence. It may be that at this point distress is
noticed and becomes apparent (i.e. as the girls can no longer contain their difficulties under
increasing social and emotional pressures) where it has been camouflaged sufficiently before
this point. These aspects of experience that the qualitative literature bring, can provide a more
detailed frame to the quantitative literature’s findings and assumptions and highlight the
significance of environment, relationships and socially constructed gendered roles in shaping
presentation and experience.
The Next Steps in Understanding ASC and Gender: Future Research
Whilst there is use and value in measurement and using experimental paradigms to
explore sex/gender difference in ASCs, this review found a lack of research that was able to
locate these findings within context. Some of the studies made claims that a certain difference
between the sexes in the presentation of autism meant that girls are more likely to be missed.
However, this understanding does not account for the broader picture of how and why certain
behaviours and emotions are noticed or become distressing. It is likely that it is not the
expectations of ‘normalness’ that brings children to clinic, but the point at which the
158
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
behaviours and/or emotions are perceived as problematic, for the person themselves or for the
people around them. An exploration of the first-hand, lived experiences of children and
adolescents and their families would help to reveal more nuanced understanding of
difference, not only in the presentation of autism according to sex/gender, but how signs and
symptoms of autism are noticed, perceived and acted upon by others.
Limitations
In the past twenty years, quantitative research has dominated the social sciences
literature. This review reflects this, showing a lack of in-depth research that explores the
subjective experience of autism in relation to gender and sex. However, it is acknowledged
that in this review, because ‘difference’ was used as a search term, that qualitative research
that included only one sex would have been overlooked. However, following initial searches
the search terms were developed to be reasonably broad and qualitative studies comparing the
experiences of boys and girls, and qualitative meta-syntheses are lacking. It is also hoped that
by checking additional literature cited in papers the risk of missing important papers was
minimised. Still, the review did not consider autobiographical literature available on the
experience of having a diagnosis of an ASC, of which there is an abundance. An interesting
area of future research might be to review this literature to identify any differences in
experience between the genders.
Summary and Conclusions
This literature review has examined what we know about the differences between
girls’ and boys’ presentation of ASCs. The majority of research has focussed on comparing
symptoms on established diagnostic profiles of ASC and found few differences in broad
social communication criteria and some suggestion that girls show less severe RRBIs.
159
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
However, few studies have measured the quality of impairments or considered the context in
which these measurements are made.
The present focus on what the basic differences between ASC ‘symptoms’ in males
and females are, leaves unanswered the question of how the people around a child make sense
of their behaviour as typical or not and why help is sought. A recommendation is made for
qualitative research that contextualises the existing predominantly quantitative evidence in
order to enrich our understanding of personal experience and inform diagnosis.
160
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
References
Achenbach, T. M. (1991). Manual for the youth self-report and 1991 profile Department of
Psychiatry, University of Vermont Burlington, VT.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms &
profiles. Burlington: Research Centre for Children, Youth and Families, University of
Vermont Burlington, VT.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (DSM-5®) American Psychiatric Pub.
Amr, M., Raddad, D., El-Mehesh, F., Mahmoud, E., & El-Gilany, A. (2011). Sex differences
in Arab children with autism spectrum disorders. Research in Autism Spectrum
Disorders, 5(4), 1343-1350.
Andersson, G. W., Gillberg, C., & Miniscalco, C. (2013). Pre-school children with suspected
autism spectrum disorders: Do girls and boys have the same profiles? Research in
Developmental Disabilities, 34(1), 413-422.
Arliss, L. P. (1991). Gender communication. Englewood Cliffs, NJ: Prentice Hall.
Asperger, H. (1944). Die “Autistischen psychopathen” im kindesalter. Archiv Für Psychiatrie
Und Nervenkrankheiten, 117(1), 76-136.
Attwood, T. (2006). The pattern of abilities and development of girls with Asperger’s
syndrome. Asperger’s and Girls, 1-7.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., et al. (2006).
Prevalence of disorders of the autism spectrum in a population cohort of children in
161
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
south thames: The special needs and autism project (SNAP). The Lancet, 368(9531),
210-215.
Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in Cognitive
Sciences, 6(6), 248-254.
Baron-Cohen, S. (2005). The empathizing system. Origins of the Social Mind: Evolutionary
Psychology and Child Development, 468-492.
Baron-Cohen, S., Hoekstra, R. A., Knickmeyer, R., & Wheelwright, S. (2006). The autism-
spectrum quotient (AQ)—adolescent version. Journal of Autism and Developmental
Disorders, 36(3), 343.
Baron-Cohen, S., Knickmeyer, R. C., & Belmonte, M. K. (2005). Sex differences in the
brain: Implications for explaining autism. Science, 310(5749), 819-823.
Baron-Cohen, S., Scott, F. J., Allison, C., Williams, J., Bolton, P., Matthews, F. E., et al.
(2009). Prevalence of autism-spectrum conditions: UK school-based population
study. The British Journal of Psychiatry, 194(6), 500-509.
Begeer, S., Mandell, D., Wijnker-Holmes, B., Venderbosch, S., Rem, D., Stekelenburg, F., et
al. (2013). Sex differences in the timing of identification among children and adults with
autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(5),
1151-1156.
Bornstein, M. H., Hahn, C., & Haynes, O. M. (2004). Specific and general language
performance across early childhood: Stability and gender considerations. First
Language, 24(3), 267-304.
Brugha, T., McManus, S., Meltzer, H., Smith, J., Scott, F. J., Purdon, S., et al. (2009). Autism
spectrum disorders in adults living in households throughout england: Report from the
162
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
adult psychiatric morbidity survey 2007. Leeds: The NHS Information Centre for Health
and Social Care.
Bussey, K., & Bandura, A. (1999). Social cognitive theory of gender development and
differentiation. Psychological Review, 106(4), 676.
Cairns, R. B., & Cairns, B. D. (1994). Lifelines and risks: Pathways of youth in our time.
Cambridge University Press.
Carter, A. S., Black, D. O., Tewani, S., Connolly, C. E., Kadlec, M. B., & Tager-Flusberg, H.
(2007). Sex differences in toddlers with autism spectrum disorders. Journal of Autism
and Developmental Disorders, 37(1), 86-97.
Christensen, D. L., Bilder, D. A., Zahorodny, W., Pettygrove, S., Durkin, M. S., Fitzgerald,
R. T., et al. (2016). Prevalence and characteristics of autism spectrum disorder among 4-
year-old children in the autism and developmental disabilities monitoring
network. Journal of Developmental & Behavioral Pediatrics, 37(1), 1-8.
Constantino, J. N., Zhang, Y. I., Frazier, T., Abbacchi, A. M., & Law, P. (2010). Sibling
recurrence and the genetic epidemiology of autism. American Journal of
Psychiatry, 167(11), 1349-1356.
Cridland, E. K., Jones, S. C., Caputi, P., & Magee, C. A. (2014). Being a girl in a boys’
world: Investigating the experiences of girls with autism spectrum disorders during
adolescence. Journal of Autism and Developmental Disorders, 44(6), 1261-1274.
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: Gender differences in
the social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678-
689.
163
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Dean, M., Kasari, C., Shih, W., Frankel, F., Whitney, R., Landa, R., et al. (2014). The peer
relationships of girls with ASD at school: Comparison to boys and girls with and without
ASD. Journal of Child Psychology and Psychiatry, 55(11), 1218-1225.
Doey, L., Coplan, R. J., & Kingsbury, M. (2014). Bashful boys and coy girls: A review of
gender differences in childhood shyness. Sex Roles, 70(7-8), 255-266.
DSM-IV-TR, A. (2000). Diagnostic and statistical manual of mental disorders, text
revision. Washington, DC: American Psychiatric Association.
Dworzynski, K., Ronald, A., Bolton, P., & Happé, F. (2012). How different are girls and boys
above and below the diagnostic threshold for autism spectrum disorders? Journal of the
American Academy of Child & Adolescent Psychiatry, 51(8), 788-797.
Fombonne, E. (1999). The epidemiology of autism: A review. Psychological
Medicine, 29(4), 769-786.
Fombonne, E. (2002). Epidemiological trends in rates of autism. Molecular
Psychiatry, 7(S2), S4.
Fombonne, E. (2003). Epidemiological surveys of autism and other pervasive developmental
disorders: An update. Journal of Autism and Developmental Disorders, 33(4), 365-382.
Fombonne, E. (2005). The changing epidemiology of autism. Journal of Applied Research in
Intellectual Disabilities, 18(4), 281-294.
Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatric
Research, 65(6), 591.
Frazier, T. W., Georgiades, S., Bishop, S. L., & Hardan, A. Y. (2014). Behavioral and
cognitive characteristics of females and males with autism in the simons simplex
164

PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
collection. Journal of the American Academy of Child & Adolescent Psychiatry, 53(3),
340. e3.
Frith, U. (1991). Asperger and his syndrome. Autism and Asperger Syndrome, 14, 1-36.
Fulton, A. M., Paynter, J. M., & Trembath, D. (2017). Gender comparisons in children with
ASD entering early intervention. Research in Developmental Disabilities, 68, 27-34.
Giarelli, E., Wiggins, L. D., Rice, C. E., Levy, S. E., Kirby, R. S., Pinto-Martin, J., et al.
(2010). Sex differences in the evaluation and diagnosis of autism spectrum disorders
among children. Disability and Health Journal, 3(2), 107-116.
Gillberg, C. (1993). Autism and related behaviours. Journal of Intellectual Disability
Research, 37(4), 343-372.
Goddard, L., Dritschel, B., & Howlin, P. (2014). A preliminary study of gender differences in
autobiographical memory in children with an autism spectrum disorder. Journal of
Autism and Developmental Disorders, 44(9), 2087-2095.
Goin-Kochel, R. P., Mackintosh, V. H., & Myers, B. J. (2006). How many doctors does it
take to make an autism spectrum diagnosis? Autism, 10(5), 439-451.
Goldman, S. (2013). Opinion: Sex, gender and the diagnosis of autism—A biosocial view of
the male preponderance. Research in Autism Spectrum Disorders, 7(6), 675-679.
Gould, J., & Ashton-Smith, J. (2011). Missed diagnosis or misdiagnosis? Girls and women
on the autism spectrum. Good Autism Practice (GAP), 12(1), 34-41.
Hartung, C. M., & Widiger, T. A. (1998). Gender differences in the diagnosis of mental
disorders: Conclusions and controversies of the DSM–IV. Psychological
Bulletin, 123(3), 260.
165
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Head, A. M., McGillivray, J. A., & Stokes, M. A. (2014). Gender differences in emotionality
and sociability in children with autism spectrum disorders. Molecular Autism, 5(1), 19.
Hiller, R. M., Young, R. L., & Weber, N. (2014). Sex differences in autism spectrum disorder
based on DSM-5 criteria: Evidence from clinician and teacher reporting. Journal of
Abnormal Child Psychology, 42(8), 1381-1393.
Holliday Willey, L. (1999). Pretending to be normal: Living with Asperger’s
syndrome. London: Jessica Kingsley,
Holtmann, M., Bölte, S., & Poustka, F. (2007). Autism spectrum disorders: Sex differences in
autistic behaviour domains and coexisting psychopathology. Developmental Medicine &
Child Neurology, 49(5), 361-366.
Howe, Y. J., O’Rourke, J. A., Yatchmink, Y., Viscidi, E. W., Jones, R. N., & Morrow, E. M.
(2015). Female autism phenotypes investigated at different levels of language and
developmental abilities. Journal of Autism and Developmental Disorders, 45(11), 3537-
3549.
Hurtig, T., Kuusikko, S., Mattila, M., Haapsamo, H., Ebeling, H., Jussila, K., et al. (2009).
Multi-informant reports of psychiatric symptoms among high-functioning adolescents
with Asperger Syndrome or autism. Autism, 13(6), 583-598.
Huttenlocher, J., Haight, W., Bryk, A., Seltzer, M., & Lyons, T. (1991). Early vocabulary
growth: Relation to language input and gender. Developmental Psychology, 27(2), 236.
Jamison, R., Bishop, S. L., Huerta, M., & Halladay, A. K. (2017). The clinician perspective
on sex differences in autism spectrum disorders. Autism, 21(6), 772-784.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2(3), 217-250.
166
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Kauschke, C., van der Beek, B., & Kamp-Becker, I. (2016). Narratives of girls and boys with
autism spectrum disorders: Gender differences in narrative competence and internal state
language. Journal of Autism and Developmental Disorders, 46(3), 840-852.
Kim, K., Rosenthal, M. Z., Gwaltney, M., Jarrold, W., Hatt, N., McIntyre, N., et al. (2015). A
virtual joy-stick study of emotional responses and social motivation in children with
autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12),
3891-3899.
Kim, Y. S., Leventhal, B. L., Koh, Y., Fombonne, E., Laska, E., Lim, E., et al. (2011).
Prevalence of autism spectrum disorders in a total population sample. American Journal
of Psychiatry, 168(9), 904-912.
Kmet, L. M., Cook, L. S., & Lee, R. C. (2004). Standard quality assessment criteria for
evaluating primary research papers from a variety of fields.
Kopp, S., & Gillberg, C. (2011). The autism spectrum screening questionnaire (ASSQ)-
revised extended version (ASSQ-REV): An instrument for better capturing the autism
phenotype in girls? A preliminary study involving 191 clinical cases and community
controls. Research in Developmental Disabilities, 32(6), 2875-2888.
Kovacs, M. (1992). Children's depression inventory Multi-Health Systems North
Tonawanda, NY.
Koyama, T., Kamio, Y., Inada, N., & Kurita, H. (2009). Sex differences in WISC-III profiles
of children with high-functioning pervasive developmental disorders. Journal of Autism
and Developmental Disorders, 39(1), 135.
Kumazaki, H., Muramatsu, T., Kosaka, H., Fujisawa, T. X., Iwata, K., Tomoda, A., et al.
(2015). Sex differences in cognitive and symptom profiles in children with high
167
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 13, 1-
7.
Lawrence, K., Campbell, R., & Skuse, D. (2015). Age, gender, and puberty influence the
development of facial emotion recognition. Frontiers in Psychology, 6, 761.
Leaper, C., Anderson, K. J., & Sanders, P. (1998). Moderators of gender effects on parents'
talk to their children: A meta-analysis. Developmental Psychology, 34(1), 3.
Lohr, W. D., Daniels, K., Wiemken, T., Williams, P. G., Kelley, R. R., Kuravackel, G., et al.
(2017). The screen for child anxiety-related emotional disorders is sensitive but not
specific in identifying anxiety in children with high-functioning autism spectrum
disorder: A pilot comparison to the achenbach system of empirically based assessment
scales. Frontiers in Psychiatry, 8, 138.
Lord, C., Rutter, M. L., Goode, S., Heemsbergen, J., Jordan, H., Mawhood, L., et al. (1989).
Autism diagnostic observation schedule: A standardized observation of communicative
and social behavior. Journal of Autism and Developmental Disorders, 19(2), 185-212.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A
revised version of a diagnostic interview for caregivers of individuals with possible
pervasive developmental disorders. Journal of Autism and Developmental
Disorders, 24(5), 659-685.
Lord, C., Schopler, E., & Revicki, D. (1982). Sex differences in autism. Journal of Autism
and Developmental Disorders, 12(4), 317-330.
Malatesta, C. Z., & Haviland, J. M. (1982). Learning display rules: The socialization of
emotion expression in infancy. Child Development, 991-1003.
168
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Malterud, K., & Okkes, I. (1998). Gender differences in general practice consultations:
Methodological challenges in epidemiological research. Family Practice, 15(5), 404-
410.
Mattila, M., Kielinen, M., Linna, S., Jussila, K., Ebeling, H., Bloigu, R., et al. (2011). Autism
spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria:
An epidemiological study. Journal of the American Academy of Child & Adolescent
Psychiatry, 50(6), 592. e11.
May, T., Cornish, K., & Rinehart, N. (2014). Does gender matter? A one year follow-up of
autistic, attention and anxiety symptoms in high-functioning children with autism
spectrum disorder. Journal of Autism and Developmental Disorders, 44(5), 1077-1086.
May, T., Cornish, K., & Rinehart, N. J. (2016). Gender profiles of behavioral attention in
children with autism spectrum disorder. Journal of Attention Disorders, 20(7), 627-635.
May, T., Rinehart, N., Wilding, J., & Cornish, K. (2013). The role of attention in the
academic attainment of children with autism spectrum disorder. Journal of Autism and
Developmental Disorders, 43(9), 2147-2158.
Mayes, S. D., & Calhoun, S. L. (2011). Impact of IQ, age, SES, gender, and race on autistic
symptoms. Research in Autism Spectrum Disorders, 5(2), 749-757.
McLennan, J. D., Lord, C., & Schopler, E. (1993). Sex differences in higher functioning
people with autism. Journal of Autism and Developmental Disorders, 23(2), 217-227.
Montirosso, R., Peverelli, M., Frigerio, E., Crespi, M., & Borgatti, R. (2010). The
development of dynamic facial expression recognition at different intensities in 4‐to 18‐
year‐olds. Social Development, 19(1), 71-92.
169
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Noterdaeme, M., Mildenberger, K., Minow, F., & Amorosa, H. (2002). Evaluation of
neuromotor deficits in children with autism and children with a specific speech and
language disorder. European Child & Adolescent Psychiatry, 11(5), 219-225.
Oswald, T. M., Winter-Messiers, M. A., Gibson, B., Schmidt, A. M., Herr, C. M., &
Solomon, M. (2016). Sex differences in internalizing problems during adolescence in
autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(2), 624-
636.
Parish-Morris, J., Liberman, M. Y., Cieri, C., Herrington, J. D., Yerys, B. E., Bateman, L., et
al. (2017). Linguistic camouflage in girls with autism spectrum disorder. Molecular
Autism, 8(1), 48.
Park, S., Cho, S., Cho, I. H., Kim, B., Kim, J., Shin, M., et al. (2012). Sex differences in
children with autism spectrum disorders compared with their unaffected siblings and
typically developing children. Research in Autism Spectrum Disorders, 6(2), 861-870.
Pathak, M., Bennett, A., & Shui, A. M. (2017). Correlates of adaptive behavior profiles in a
large cohort of children with autism: The autism speaks autism treatment network
registry data. Autism, 1362361317733113.
Pisula, E., Pudło, M., Słowińska, M., Kawa, R., Strząska, M., Banasiak, A., et al. (2017).
Behavioral and emotional problems in high-functioning girls and boys with autism
spectrum disorders: Parents’ reports and adolescents’ self-reports. Autism, 21(6), 738-
748.
Reynolds, C., & Kamphaus, R. (2004). Behavior assessment system for children, (BASC-2)
handout. AGS Publishing, 4201, 55014-51796.
170
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Rivet, T. T., & Matson, J. L. (2011). Review of gender differences in core symptomatology
in autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 957-976.
Ross, L. A., Del Bene, V. A., Molholm, S., Frey, H., & Foxe, J. J. (2015). Sex differences in
multisensory speech processing in both typically developing children and those on the
autism spectrum. Frontiers in Neuroscience, 9, 185.
Rutter, M. (1978). Diagnosis and definition of childhood autism. Journal of Autism and
Childhood Schizophrenia, 8(2), 139-161.
Rynkiewicz, A., & Łucka, I. (2015). Autism spectrum disorder (ASD) in girls. co-occurring
psychopathology. sex differences in clinical manifestation. Psychiatr. Pol. (31)
Rynkiewicz, A., Schuller, B., Marchi, E., Piana, S., Camurri, A., Lassalle, A., et al. (2016).
An investigation of the ‘female camouflage effect’ in autism using a computerized
ADOS-2 and a test of sex/gender differences. Molecular Autism, 7(1), 10.
Scott, F. J., Baron-Cohen, S., Bolton, P., & Brayne, C. (2002). Brief report prevalence of
autism spectrum conditions in children aged 5-11 years in Cambridgeshire,
UK. Autism, 6(3), 231-237.
Shattuck, P. T., Durkin, M., Maenner, M., Newschaffer, C., Mandell, D. S., Wiggins, L., et
al. (2009). Timing of identification among children with an autism spectrum disorder:
Findings from a population-based surveillance study. Journal of the American Academy
of Child & Adolescent Psychiatry, 48(5), 474-483.
Sipes, M., Matson, J. L., Worley, J. A., & Kozlowski, A. M. (2011). Gender differences in
symptoms of autism spectrum disorders in toddlers. Research in Autism Spectrum
Disorders, 5(4), 1465-1470.
171
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Solomon, M., Miller, M., Taylor, S. L., Hinshaw, S. P., & Carter, C. S. (2012). Autism
symptoms and internalizing psychopathology in girls and boys with autism spectrum
disorders. Journal of Autism and Developmental Disorders, 42(1), 48-59.
Springer, K. W., Stellman, J. M., & Jordan-Young, R. M. (2012). Beyond a catalogue of
differences: A theoretical frame and good practice guidelines for researching sex/gender
in human health. Social Science & Medicine, 74(11), 1817-1824.
Stern, J. A., Gadgil, M. S., Blakeley-Smith, A., Reaven, J. A., & Hepburn, S. L. (2014).
Psychometric properties of the SCARED in youth with autism spectrum
disorder. Research in Autism Spectrum Disorders, 8(9), 1225-1234.
Stern, M., & Karraker, K. H. (1989). Sex stereotyping of infants: A review of gender
labelling studies. Sex Roles, 20(9-10), 501-522.
Supekar, K., & Menon, V. (2015). Sex differences in structural organization of motor
systems and their dissociable links with repetitive/restricted behaviors in children with
autism. Molecular Autism, 6(1), 50.
Timimi, S., Gardner, N., & McCabe, B. (2011). The myth of autism: Medicalising men's and
boys' social and emotional competence Palgrave Macmillan Basingstoke.
Van Wijngaarden-Cremers, P. J., van Eeten, E., Groen, W. B., Van Deurzen, P. A.,
Oosterling, I. J., & Van der Gaag, Rutger Jan. (2014). Gender and age differences in the
core triad of impairments in autism spectrum disorders: A systematic review and meta-
analysis. Journal of Autism and Developmental Disorders, 44(3), 627-635.
Volkmar, F. R., Szatmari, P., & Sparrow, S. S. (1993). Sex differences in pervasive
developmental disorders. Journal of Autism and Developmental Disorders, 23(4), 579-
591.
172
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Wakabayashi, A., Baron-Cohen, S., Uchiyama, T., Yoshida, Y., Tojo, Y., Kuroda, M., et al.
(2007). The autism-spectrum quotient (AQ) children’s version in japan: A cross-cultural
comparison. Journal of Autism and Developmental Disorders, 37(3), 491-500.
Wang, S., Deng, H., You, C., Chen, K., Li, J., Tang, C., et al. (2017). Sex differences in
diagnosis and clinical phenotypes of Chinese children with autism spectrum
disorder. Neuroscience Bulletin, 33(2), 153-160.
Wing, L. (1981a). Asperger's syndrome: A clinical account. Psychological Medicine, 11(1),
115-129.
Wing, L. (1981b). Sex ratios in early childhood autism and related conditions. Psychiatry
Research, 5(2), 129-137.
Wing, L. (1988). The continuum of autistic characteristics. In Diagnosis and assessment in
autism (pp. 91-110) Springer. Boston, MA.
World Health Organization (1998) Gender and health: technical paper. Geneva: World
Health Organization; Report no.: WHO/FRH/WHD/98.16.
World Health Organization (2015) What do we mean by ‘sex’ and ‘gender’? World Health
Organization. http://www.who.int/gender/whatisgender/en/.
Zarokanellou, V., Kolaitis, G., Vlassopoulos, M., & Papanikolaou, K. (2017). Brief report: A
pilot study of the validity and reliability of the greek version of the social
communication questionnaire. Research in Autism Spectrum Disorders, 38, 1-5.
173
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Appendix A: Table III Showing Strengths and Limitations of Reviewed Studies
Table III.
Summary strengths and limitations of papers included in the review
Paper Quality Rating
Strengths and Limitations
Baron-Cohen, Hoekstra, Knickmeyer & Wheelwright (2006)
The autism-spectrum quotient (AQ)—adolescent version.
19/2286%
- Assumes ASC construct known and measurable by parent report.- Measure not validated for adolescents before this study.- Assumes that the gender disparity is present due to essential difference. i.e. if there
are ‘missed’ populations of girl’s, these traits are not considered in discussion.- Significance of sex/gender differences on subscale scores not reported.- Adequate sample size
Cridland, Jones, Caputi & Magee (2014)
Being a girl in a boys’ world: investigating the experiences of girls with autism spectrum disorders during adolescence.
17/2085%
- Design and analysis unique in contextualising sex/gender differences.- Focus on female experience which is underrepresented in the literature.- Open-ended interview format allowed for perspectives of girls with ASC and their
families to be put first, minimising researcher control over the discussion.- Reflexivity only partially demonstrated.- Recruitment process /sampling strategy not covered in detail.
Dean, Harwood & Kasari, (2017)
The art of camouflage: Gender differences in the social behaviours of girls and boys with autism spectrum disorder.
20/2291%
- Study used TD children with ‘positive social skills’ as nominated by teachers which may have impacted on social interactions.
- Unique study design which allowed consideration of context.- Study does not capture the ongoing nature of relationships i.e. observation only
made at one point in time.- ‘Solitary time’ may have been due to children wanting this, rather than lacking skills
to engage.
174
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Dean, Kasari, Shih, Frankel, Whitney, Landa, Lord, Orlich, King & Harwood (2014).
The peer relationships of girls with ASD at school: comparison to boys and girls with and without ASD.
18/2282%
- IQ of the children with ASC about 10 points below the normative average (however ASC sample recruited from mainstream school so perhaps this is representative)
- Unique study design taking into account children’s perspectives of one another socially.
- Challenging to draw conclusions from results with certainty.- Questionable ecological validity of the questionnaire (perceptions of friendship may
be impacted by many other factors e.g. self-esteem)
Frazier, Georgiades, Bishop, & Hardan (2014).
Behavioural and cognitive characteristics of females and males with autism in the Simons Simplex Collection.
18/2282%
- No TD control group- Unable to get information regarding ‘strict’ inclusion criteria for SSC database. If
criteria were very strict, some cases (and perhaps more likely female cases) may have been missed.
- Rater biases (e.g. socialised gender expectations) not considered- Risk of type 1 errors with large sample size.- ADOS becomes increasingly less sensitive and specific for higher functioning
individuals, particularly females (Van Wijngaarden-Cremers et al., 2014)
Fulton, Paynter & Trembath (2017).
Gender comparisons in children with ASD entering early intervention.
18/2282%
- Sample size not sufficiently sensitive to more subtle gender differences (i.e. on subscales)
- Females diagnosed early may not be representative to females who are not diagnosed at this point (symptoms may be more obvious behaviourally or more severe).
- No TD control group used.- Significance of each finding between male and female HFASC groups were not
reported.
Goddard, Dritschel, & Howlin (2014)
A preliminary study of gender differences in autobiographical memory in children with an autism spectrum disorder.
20/2291%
- Small sample size.- Difference in experimental autobiographical memory and children’s ability to
spontaneously remember in real life/ natural environment (validity)?- Novel study investigating memory and verbal fluency.-
Head, McGillivray & Stokes (2014)
Gender differences in emotionality and sociability in children with autism spectrum disorders.
20/2291%
- Aim to measure friendship quality. Study measured social skill rather feelings of connectedness.
- Questionnaire originally designed as a self-report measure however children were interviewed. Possibility of biasing or impacting results?
- Strength that the study considered both parent’s and children’s perspectives-
175
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Hiller, Young & Weber (2014)
Sex differences in autism spectrum disorder based on DSM-5 criteria: evidence from clinician and teacher reporting.
20/2291%
- Strength that the study differentiated between parent, clinician and teacher reports from diagnostic assessments.
- Behaviours that were not seen under the conceptualisation of ASC might have been missed.
- Social and cultural sex/gender expectations are inherent in every rating. Strength that the discussion considered this.
-Holtmann, Bölte & Poustka (2007).
Autism spectrum disorders: Sex differences in autistic behaviour domains and coexisting psychopathology.
19/2286%
- Participants matched for ASD diagnosis, chronological age and full-scale IQ.- Broad age range of participants may have meant that some differences were missed
or overstated- Strength included critique of potential crossover between psychopathology and ASC
Howe, O’Rourke, Yatchmink, Viscidi, Jones, & Morrow (2015).
Female autism phenotypes investigated at different levels of language and developmental abilities.
20/2291%
- Large sample size.- ADOS may not be sensitive to females with ASC with higher IQ as these females
may be able to imitate appropriate social skills and mask any weaknesses (Lai et al. 2011). Females with more subtle ASC symptomatology that is not detected by ADOS may have been excluded.
-Hurtig, Kuusikko, Mattila, Haapsamo, Ebeling, Jussila,.& Moilanen (2009).
Multi-informant reports of psychiatric symptoms among high-functioning adolescents with Asperger syndrome or autism.
21/2295%
- Small sample size.- Strength that the study included parent, self and teacher reports
Jamison, Bishop, Huerta, & Halladay (2017).
The clinician perspective on sex differences in autism spectrum disorders.
16/2080%
- Mixed method approach could have obtained more in-depth ‘picture’ however study focussed on severity of impairment rather than quality of impairment which can be investigated through diagnostic measures.
- How the clinicians make their judgement of ‘expected’ was not considered.- Strength in critique of limitations of study.-
176
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Kauschke, van der Beek, & Kamp-Becker (2016).
Narratives of girls and boys with autism spectrum disorders: gender differences in narrative competence and internal state language.
20/2291%
- Small sample with large age range. - Lack of TD boys control group.- Age and IQ matched samples- Novel design that focussed on one characteristic of ASC allowed for more in-depth
data and novel findings.-
Kim, Rosenthal, Gwaltney, Jarrold, Hatt, McIntyre, Swain, Solomon & Mundy (2015)
A virtual joy-stick study of emotional responses and social motivation in children with autism spectrum disorder.
17/2285%
- Novel experimental design- Observer bias/expectation removed due to video game design. However, also maybe
not as valid due to the ‘realness’ being minimised e.g. questionable validity of using interpersonal distance in computer game in measuring ‘social motivation’.
- Interesting way of reducing anxiety of ‘realness’ of situation by using video game- Few participants, subtle differences may not have reached significance
Kopp & Gillberg (2011)
The Autism Spectrum Screening Questionnaire (ASSQ)-Revised Extended Version: an instrument for better capturing the autism phenotype in girls?
20/2291%
- Sample size relatively small.- Bias inherent in parent ratings. Strength that this was acknowledged.- TD groups matched for IQ and age.
Koyama, Kamio, Inada & Kurita (2009)
Sex Differences in WISC-III Profiles of Children with High-functioning Pervasive Developmental Disorders.
17/2277%
- ASC girls sample size relatively small.- Information about the clinics that participants were recruited from not detailed.
Uncertain whether results can be generalised to ASC children not accessing specialist clinics.
- Age range not reported (means only).
Kumazaki, Muramatsu, Kosaka, Fujisawa, Iwata, Tomoda, Tsuchiya & Mimura (2015)
Sex differences in cognitive and symptom profiles in children with high functioning autism spectrum disorders.
17/2277%
- Sample size small. - Results not reported in detail.- No TD controls.-
Lohr, Daniels, Wiemken, Williams, Kelley, Kuravackel & Sears (2017)
The screen for child emotional disorders is sensitive but not specific in identifying anxiety in children with HF-ASD.
19/2286%
- Small sample size of ASC girls especially given the wide age range.- No control group used.- Strength is that the study considers teacher, child and parent perspectives of anxiety.-
177
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
May, Cornish & Rinehart (2014)
Does gender matter? A one year follow-up of autistic, attention and anxiety symptoms in high-functioning children with autism spectrum disorder.
21/2295%
- Cannot be generalised to ASC children not accessing specialist clinics.- Relatively small sample size.
May, Cornish & Rinehart (2016)
Gender profiles of behavioural attention in children with autism spectrum disorder.
21/2295%
- Relatively small sample size -subtle differences may not have been detected.--
May, Rinehart, Wilding & Cornish (2013)
The Role of Attention in the Academic Attainment of Children with Autism Spectrum Disorder
21/2295%
- Relatively small sample size.
Noterdaeme, Mildenberger, Minow & Amorosa (2002)
Evaluation of neuromotor deficits in children with autism and children with a specific speech and language disorder.
17/2277%
- Very small sample size. Subtle differences may not have reached significance.- Conclusion perhaps stating lack of differences with too much confidence given
sample size.- Control children were matched as closely as possible to the clinical groups with
respect to age and non-verbal IQ.
Oswald, Winter-Messiers, Gibson, Schmidt, Herr, & Solomon (2016)
Sex differences in internalizing problems during adolescence in Autism Spectrum Disorder
20/2291%
- Small sample size. Subtle differences may not have reached significance.- Some of the scales have low reliability.- Strength that participants with ASC were one-to-one matched to control participants
on both IQ and sex.- Community sample used.
Parish-Morris, Liberman, Cieri, Herrington, Yerys, Bateman, Donaher, Ferguson, Pandey & Schultz (2017)
Linguistic camouflage in girls with autism spectrum disorder.
20/2291%
- Linguistic markers measurable without observer bias/ expectation. - Only small sample of TD control participants included
178
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Pathak, Bennett & Shui (2017)
Correlates of adaptive behavior profiles in a large cohort of children with autism: The autism speaks Autism Treatment Network registry data.
17/2277%
- Participants used were diagnosed using ADOS which may not be sensitive to females with ASC with higher IQ as these females may be able to imitate appropriate social skills and mask any weaknesses (Lai et al. 2011). Females with more subtle ASC symptomatology that is not detected by ADOS may have been excluded.
- No control used to investigate differences in TD children.
Pisula, Pudło, Słowińska, Kawa, Strząska, Banasiak & Wolańczyk (2017).
Behavioral and emotional problems in high-functioning girls and boys with autism spectrum disorders: Parents’ reports and adolescents’ self-reports.
19/2286%
- Small sample size and unrepresentative sample of community girls with ASC.- Age and IQ matched samples- Multiple perspectives measured (parent and self-report measures)- Validity of measures not reported.
Ross, Del Bene, Molholm, Frey & Foxe (2015)
Sex differences in multisensory speech processing in both typically developing children and those on the autism spectrum.
19/2286%
- In depth analysis of social communication using design which controls for rater bias- Ability to read visual speech cues and integrate them very specific ability and a
small component of social communication (validity).
Rynkiewicz & Łucka (2015)
Autism spectrum disorder (ASD) in girls. Co-occurring psychopathology. Sex differences in clinical manifestation.
14/2264%
- Small sample with large age range. - No TD control group.- Research has shown parent reports of ‘psychopathology’ not to be consistent with
adolescent reports (e.g. Stern et al., 2014).
Rynkiewicz, Schuller, Marchi, Piana, Camurri, Lassalle & Baron-Cohen (2016)
An investigation of the ‘female camouflage effect’ in autism using a computerized ADOS-2 and a test of sex/gender differences.
15/2268%
- Small sample with large age range. - No TD control group.- Using gestures more frequently and vividly assumed to be better use of
communication.
179
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Solomon, Miller, Taylor, Hinshaw & Carter (2012)
Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders.
20/2291%
- Relatively small sample size. Possibility of type II errors.- Measures not validated for ASC children/adolescents.
Stern, Gadgil, Blakeley-Smith, Reaven & Hepburn, (2014)
Psychometric properties of the SCARED in youth with autism spectrum disorder.
19/2286%
- No TD control group.- Small female ASC sample- Measure not validated. Anxiety Disorders Interview Schedule (ADIS) used as ‘gold
standard’ for anxiety diagnosis although reliability not been established in ASC populations.
Supekar & Menon (2015)
Sex differences in structural organization of motor systems and their dissociable links with repetitive/ restricted behaviours in children with autism.
19/2286%
- Females with more subtle ASC symptomatology that is not detected by ADI-R may have been excluded.
- No TD controls.
Wakabayashi, Baron-Cohen, Uchiyama, Yoshida, Tojo, Kuroda & Wheelwright (2007)
The autism-spectrum quotient (AQ) children’s version in Japan: a cross-cultural comparison.
19/2286%
- Females with more subtle ASC symptomatology may have not been included in this study.
- TD controls were not IQ or age matched.
Wang, Deng, You, Chen, Li, Tang, Ceng, Zou, Zou (2017)
Sex Differences in Diagnosis and Clinical Phenotypes of Chinese Children with Autism Spectrum Disorder
18/2282%
- Females with more subtle ASC symptomatology may have not been included in this study.
- Females who have been diagnosed at a young age may be showing different/more severe or obvious traits than girls not diagnosed at this age.
Zarokanellou, Kolaitis, Vlassopoulos & Papanikolaou (2017)
Brief report: A pilot study of the validity and reliability of the Greek version of the Social Communication Questionnaire.
17/2277%
- Not much information about where participants were recruited from.- Samples not matched age or IQ matched. - Small sample size means subtle differences may not have reached significance.
180
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Part 3: Clinical Experience on Training
Year 1
Adult Placement (12 months)
I spent my first year of clinical training working within a community adult recovery and support team. My main role was conducting psychological assessments, formulation and interventions and I gained experience of delivering evidence based psychological interventions, primarily Cognitive Behavioural Therapy (CBT) with adults presenting with a range of complex problems. Client’s difficulties ranged in severity and were varied in terms of psychiatric diagnoses, including obsessive compulsive disorder, panic disorder and acrophobia, bipolar affective disorder, depression, psychosis and bulimia nervosa binge eating disorder. I also worked closely alongside my multi-disciplinary team (MDT) colleagues in order to formulate and deliver interventions. I also co-facilitated a CBT group for people diagnosed with attention deficit hyperactivity disorder with another clinical psychologist.
In addition to therapeutic interventions I undertook psychometric and neuropsychological assessments. I provided informal consultation to the MDT as well as delivering training to the team on attachment and structured clinical management. Whilst I was on placement I evaluated the therapy outcomes of two of the recovery and support teams and wrote this up for my service evaluation project.
Year 2
Learning Disability Placement (6 months)
On my learning disability placement I worked within a community service which was a joint health and social care team. I delivered 1:1 therapy, which was adapted in order to make it accessible and used a range of approaches including CBT, positive behaviour support PBS, mindfulness and systemic approaches for clients with anger, low mood and anxiety. Approaches were flexible in order to make therapy as accessible and meaningful as possible. I also co-facilitated a bereavement group with my supervisor in a supported living home. I completed psychometric and neuropsychological assessments as part of assessments for a diagnosis of a learning disability, as well as using adapted measures to assess dementia. In addition to formal reports I wrote client accessible reports. I was often asked to work with the team to manage issues of capacity and consent and completed an assessment related to the capacity to consent to sexual relationships. I offered systemic consultations to families and
181
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
residential care homes for managing challenging behaviour and would use integrative assessments and observations to develop Positive Behavioural Support (PBS) plans. I also delivered some joint training for bus drivers with my supervisor on Autism Spectrum Disorders.
Child Placement (6 months)
My child placement was in a community Child and Adolescent Mental Health Team (CAMHS). My main role was to provide assessment, formulation and focussed interventions to young people with mild to moderate mental health problems. I had opportunity to work with young people with a range of difficulties including separation anxiety, depression and Autism Spectrum Conditions, drawing upon CBT, systemic, interpersonal psychotherapy, narrative and psychodynamic approaches.
I also completed two cognitive assessments using the Wechsler Intelligence Scale for Children (WISC) and carried out a school observation as part of this. I co-facilitated a CBT group for parents of children with anxiety with an assistant psychologist colleague. I also had the opportunity to be part of a reflecting team using a one-way screen, as well as observing and reflecting on an art psychotherapy group for children with anxiety. I also helped to deliver training to multi-agency professionals on ‘depression in adolescence'.
Year 3
Older Adult Placement (6 months)
My older adult placement was split between a memory assessment clinic, older adult community mental health team and community dementia support service. I had a role in completing dementia assessments using a comprehensive battery of neuropsychological tests, observations and family interviews.
I also carried out psychological assessments, formulation and interventions. These focussed on a range of difficulties including anxiety, depression and adjusting to dementia using systemic and psychodynamic approaches. I co-facilitated a psychosocial peer group programme, the Living Well With Dementia group, with my supervisor for people with a recently diagnosed dementia with my supervisor. I also delivered a Dementia Information Group for people with a recent diagnosis of dementia and their families, using a psychoeducational approach with an occupational therapist colleague. I was also involved in carrying out assessment and consultation to residential cares homes to help staff with managing behaviour that challenges.
182
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Specialist Placement (6 months) Adult Oncology (Family)
My final and specialist placement was based within a specialist cancer hospital. I worked with adults diagnosed with cancer, and their families. My main role was to provide assessment, formulation and interventions for people with a diagnosis of cancer who had dependent children. I also worked with young adults with cancer and their families. I used systemic approaches to help people with a variety of challenges and questions around adjustment including: communicating with and meeting their children’s attachment needs; coping with change and uncertainty of health; existential questions; low mood and anxiety. Some of the work was carried out 1-1 however work was often with more than one family member. I developed and co-facilitated a narrative therapy Tree of Life group with a trainee clinical psychologist for young people who had recently had a specific bone marrow treatments.
I co-delivered training to nurse colleagues on the psychosocial impact of cancer on children, with my supervisor. I was also involved in initiating a team around a patient meeting for a patient with potential risk issues and consulted regularly at weekly palliative care MDT meetings.
183
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Part 4: Table of Assessments Completed During Training
Year I AssessmentsASSESSMENT TITLE
WAIS WAIS Interpretation (online assessment)
Practice Report of Clinical Activity
Cognitive Behavioural Therapy with a man in his fifties presenting with symptoms of depression, panic and delusions
Audio Recording of Clinical Activity with Critical Appraisal
Critical appraisal of an audio recording of clinical activity with a male client in his 60s presenting with OCD and depression.
Report of Clinical Activity N=1
Cognitive Behavioural Therapy with a woman in her thirties presenting with symptoms of panic disorder with agoraphobia
Major Research Project Literature Survey
Is contemplation of your own death good for you? A review of the effects of the ‘death reflection’ manipulation
Major Research Project Proposal
What are the processes by which parents and caregivers of females with an Autism Spectrum Disorder (ASD) without cognitive impairment come to understand their child’s behaviours as requiring intervention?
Service-Related Project An evaluation of psychological therapy outcomes in two community adult recovery and support teams
Year II AssessmentsASSESSMENT TITLE
Report of Clinical Activity – Formal Assessment
A learning disability assessment for a man in his early twenties
PPLD Process Account Reflections from my experiences of the first two years of Personal and Professional Learning Discussion Group
Year III Assessments ASSESSMENT TITLE
Presentation of Clinical Activity
Resilience building with a five year old girl using an integrative approach: Attachment Narrative Therapy
Major Research Project Literature Review
A review of the differences in the presentation of girls and boys with Autism Spectrum Conditions without cognitive impairment
Major Research Project How parents understand their daughters behaviour before
184
PARENTS’ SENSE-MAKING BEFORE THEIR DAUGHTER’S DIAGNOSIS OF ASC
Empirical Paper they receive a diagnosis of an Autism Spectrum Condition
Report of Clinical Activity
A Couple’s Intervention to Adjust to Dementia
Final Reflective Account
On becoming a clinical psychologist: A retrospective, developmental, reflective account of the experience of training
185


















