
EPITHELIAL PATHOLOGY FROM A TO Z : What Every Clinician...
151
EPITHELIAL PATHOLOGY FROM A TO Z and Systemic Considerations: What Every Clinician Should Know Theresa Sullivan Gonzales, DMD, MS Colonel, United States Army Director, Orofacial Pain Management Tripler Army Medical Center Honolulu, Hawaii 96859 Diplomate, Oral and Maxillofacial Pathology
Transcript of EPITHELIAL PATHOLOGY FROM A TO Z : What Every Clinician...

EPITHELIAL PATHOLOGY
FROM A TO Z and Systemic
Considerations What Every
Clinician Should Know
Theresa Sullivan Gonzales DMD MS
Colonel United States Army
Director Orofacial Pain Management
Tripler Army Medical Center
Honolulu Hawaii 96859
Diplomate Oral and Maxillofacial Pathology
The 15 Most Common Oral Pathoses(Based on examination of 23616 US adults excludes caries amp periodontitis)
References Bouquot JE J Am Dent Assoc 1986 11250-57 wwworalpathcom
Diagnosis Rank
Number of Lesions per 1000 Adults
Males Females Both
Leukoplakia 1 425 131 237
Torus palatinus 2 132 217 187
Irritation fibroma 3 130 114 119
Fordyce granules 4 177 52 97
Torus mandibularis 5 96 79 85
Leaf-shaped fibroma (under denture) 6 04 129 67
Hemangioma 7 84 41 56
Inflammatory ulcer 8 54 51 52
Inflammatory erythema 9 45 48 47
Papilloma 10 53 42 46
Epulis fissuratum 11 34 44 40
Lingual varicosities 12 35 34 35
Fissured tongue 13 35 31 33
Geographic tongue 14 34 30 31
Papillary hyperplasia of palate 15 17 38 30
Differential DX
Deferential DX
Differential Diagnosis
M ndash Metabolic
I ndash Inflammatory
N ndash Neoplastic
D - Developmental
Developmental
Odontogenic
Mucosal
TeethPulpalPerio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oral and Maxillofacial Pathology
Categories
Clefts
Fordyce Granules
Fissured Tongue
Hairy Tongue
Tori
Dentigerous Cyst
OKCKOT
COC
Odontoma
Ameloblastoma
AOT
CEOT
Myxoma
ErosionAbfractionAbrasion
Amelogenesis Imperfecta
Dentinogenesis Imperfecta
GeminationFusion
PulpalPeriapical Dis
Periodontal Dis
Osteogenesis Imp
Cleidocranial Dysplasia
Pagetrsquos Disease
CGCG
BFOL
Osteoma
Osteosarcoma
Chondrosarcoma
Ewingrsquos Sarcoma
Rec Apthous Stomatitis
Sarcoidosis
Wegnerrsquos Granulomatosis
Angioedema
Contact StomatitisLichen Planus Pemphigus
Pemphigoid Erythema Multiforme
Erythema Migrans Lupus
Ectodermal Dysplasia Cowden Syndrome
Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
The 15 Most Common Oral Pathoses(Based on examination of 23616 US adults excludes caries amp periodontitis)
References Bouquot JE J Am Dent Assoc 1986 11250-57 wwworalpathcom
Diagnosis Rank
Number of Lesions per 1000 Adults
Males Females Both
Leukoplakia 1 425 131 237
Torus palatinus 2 132 217 187
Irritation fibroma 3 130 114 119
Fordyce granules 4 177 52 97
Torus mandibularis 5 96 79 85
Leaf-shaped fibroma (under denture) 6 04 129 67
Hemangioma 7 84 41 56
Inflammatory ulcer 8 54 51 52
Inflammatory erythema 9 45 48 47
Papilloma 10 53 42 46
Epulis fissuratum 11 34 44 40
Lingual varicosities 12 35 34 35
Fissured tongue 13 35 31 33
Geographic tongue 14 34 30 31
Papillary hyperplasia of palate 15 17 38 30
Differential DX
Deferential DX
Differential Diagnosis
M ndash Metabolic
I ndash Inflammatory
N ndash Neoplastic
D - Developmental
Developmental
Odontogenic
Mucosal
TeethPulpalPerio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oral and Maxillofacial Pathology
Categories
Clefts
Fordyce Granules
Fissured Tongue
Hairy Tongue
Tori
Dentigerous Cyst
OKCKOT
COC
Odontoma
Ameloblastoma
AOT
CEOT
Myxoma
ErosionAbfractionAbrasion
Amelogenesis Imperfecta
Dentinogenesis Imperfecta
GeminationFusion
PulpalPeriapical Dis
Periodontal Dis
Osteogenesis Imp
Cleidocranial Dysplasia
Pagetrsquos Disease
CGCG
BFOL
Osteoma
Osteosarcoma
Chondrosarcoma
Ewingrsquos Sarcoma
Rec Apthous Stomatitis
Sarcoidosis
Wegnerrsquos Granulomatosis
Angioedema
Contact StomatitisLichen Planus Pemphigus
Pemphigoid Erythema Multiforme
Erythema Migrans Lupus
Ectodermal Dysplasia Cowden Syndrome
Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Differential DX
Deferential DX
Differential Diagnosis
M ndash Metabolic
I ndash Inflammatory
N ndash Neoplastic
D - Developmental
Developmental
Odontogenic
Mucosal
TeethPulpalPerio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oral and Maxillofacial Pathology
Categories
Clefts
Fordyce Granules
Fissured Tongue
Hairy Tongue
Tori
Dentigerous Cyst
OKCKOT
COC
Odontoma
Ameloblastoma
AOT
CEOT
Myxoma
ErosionAbfractionAbrasion
Amelogenesis Imperfecta
Dentinogenesis Imperfecta
GeminationFusion
PulpalPeriapical Dis
Periodontal Dis
Osteogenesis Imp
Cleidocranial Dysplasia
Pagetrsquos Disease
CGCG
BFOL
Osteoma
Osteosarcoma
Chondrosarcoma
Ewingrsquos Sarcoma
Rec Apthous Stomatitis
Sarcoidosis
Wegnerrsquos Granulomatosis
Angioedema
Contact StomatitisLichen Planus Pemphigus
Pemphigoid Erythema Multiforme
Erythema Migrans Lupus
Ectodermal Dysplasia Cowden Syndrome
Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
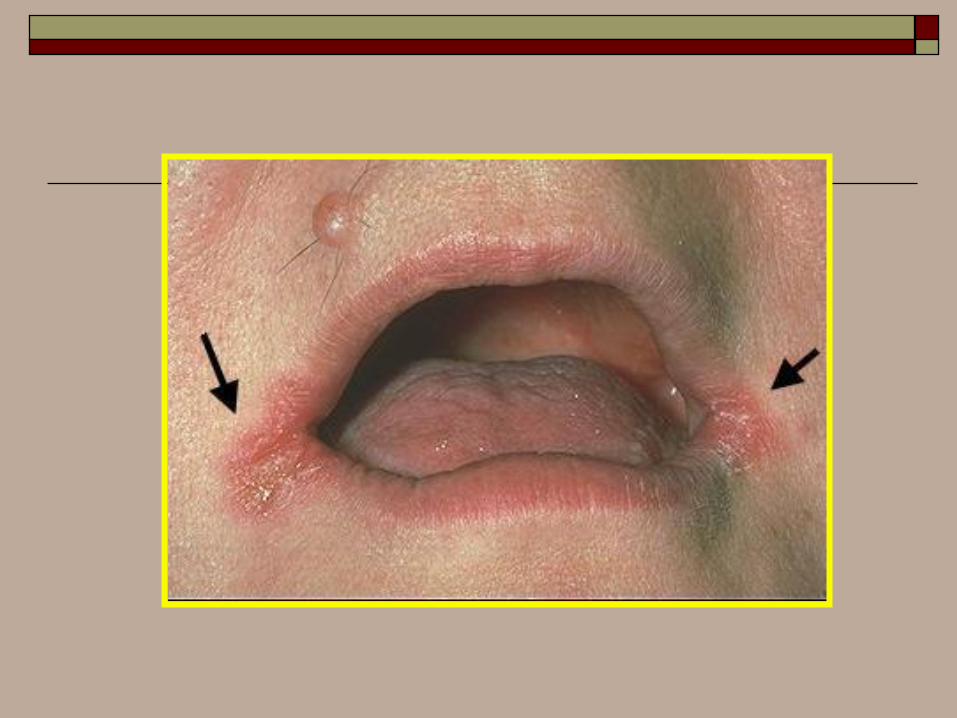
Differential Diagnosis
M ndash Metabolic
I ndash Inflammatory
N ndash Neoplastic
D - Developmental
Developmental
Odontogenic
Mucosal
TeethPulpalPerio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oral and Maxillofacial Pathology
Categories
Clefts
Fordyce Granules
Fissured Tongue
Hairy Tongue
Tori
Dentigerous Cyst
OKCKOT
COC
Odontoma
Ameloblastoma
AOT
CEOT
Myxoma
ErosionAbfractionAbrasion
Amelogenesis Imperfecta
Dentinogenesis Imperfecta
GeminationFusion
PulpalPeriapical Dis
Periodontal Dis
Osteogenesis Imp
Cleidocranial Dysplasia
Pagetrsquos Disease
CGCG
BFOL
Osteoma
Osteosarcoma
Chondrosarcoma
Ewingrsquos Sarcoma
Rec Apthous Stomatitis
Sarcoidosis
Wegnerrsquos Granulomatosis
Angioedema
Contact StomatitisLichen Planus Pemphigus
Pemphigoid Erythema Multiforme
Erythema Migrans Lupus
Ectodermal Dysplasia Cowden Syndrome
Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Developmental
Odontogenic
Mucosal
TeethPulpalPerio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oral and Maxillofacial Pathology
Categories
Clefts
Fordyce Granules
Fissured Tongue
Hairy Tongue
Tori
Dentigerous Cyst
OKCKOT
COC
Odontoma
Ameloblastoma
AOT
CEOT
Myxoma
ErosionAbfractionAbrasion
Amelogenesis Imperfecta
Dentinogenesis Imperfecta
GeminationFusion
PulpalPeriapical Dis
Periodontal Dis
Osteogenesis Imp
Cleidocranial Dysplasia
Pagetrsquos Disease
CGCG
BFOL
Osteoma
Osteosarcoma
Chondrosarcoma
Ewingrsquos Sarcoma
Rec Apthous Stomatitis
Sarcoidosis
Wegnerrsquos Granulomatosis
Angioedema
Contact StomatitisLichen Planus Pemphigus
Pemphigoid Erythema Multiforme
Erythema Migrans Lupus
Ectodermal Dysplasia Cowden Syndrome
Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Developmental
Odontogenic
Mucosal
Teethpulpal perio
Others
Infections
AllergyImmunologic
Bone
Heme DermatologicManifes of
Systemic Dis
Physical
ChemicalForensics
Salivary
Oromaxillofacial Pathology
Categories
Amyloidosis Vitamin Deficiency
Diabetes Hyperparathyroidism
Inborn Errors of Metabolism Addisonrsquos Disease
Crohnrsquos Disease Iron Def Anemia
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Papillary
Verruciform
Pigmented
Leurkoplakia
Erythroplakia
SCC
Verrucous C
Spindle Cell C
Basaloid SCC
Adenosquamos
BCC
Nasopharyngeal
Carc of Max Sin
Merkel Cell
Melanoma
Ephelis
Actinic Lentigo
Melasma
Oral Melanotic Macule
Melanoacanthoma
Smokerrsquos Melanosis
Nevi
Fibroma
3 Prsquos
Epulis Fissuratum
IPH
Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Oral Mucosal
Lesions
Epithelial Soft Tissue
Neoplastic Reactive Reactive Neoplastic
Benign
Malignant
Benign Malignant
Pre-malignant
SDK
Oral Submuc Fibrosis
Nicotine Stomatitis
Solar Keratosis
Actinic Cheilitis
Keratoacanthoma
PVL
Epithelial Dysplasia
Frictional Hyperkeratosis
Linea Alba
Morsicatio Buccarum
Morsicatio Linguarum
Cotton Roll Burn
Aspirin Burn
Radiation Mucositis
Sanguinaria-ass keratosis
Pyrophosphate-ass keratosis
Hyperplastic Candidiasis
Infectious
Physical
Chemical
Leukoplakia
Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Diagnosis ndash ldquothrough knowledgerdquo
hellipA solid knowledge of the basic principles of
the various disease processes is essential for
obtaining a good history As Goethe stated
The eyes see what the mind knows
Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Consider
Anatomical Location
Biological Plausibility
Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Patient History
Taking the patients history is traditionally
the first step in virtually every clinical
encounter
Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Other than that Mrs Lincoln how was the play
Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Prescription Drug Information for Consumers amp Professionals
Popular
Searches
Viagra
Cialis
Levitra
Lipitor
Zoloft
Hair Transplant
Health
Insurance
Healthy Diet
Lose Weight
Pain Relief
Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Multiplicity of Presentation
Systemic Disease
Syndromic Presentation
A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

A
Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Recurrent Aphthous Stomatitis
ldquoaphthous ulcerationsrdquo
ldquocanker soresrdquo
Prevalence in the general population 5
to 66 with a mean of 20
Mucosal destruction ndash T-cell mediated
immunologic reaction
Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Etiologic Factors
Allergies
Genetic predisposition
Nutritional deficiencies ndash B12 B6 Fe ++
Hematological abnormalities
Hormonal influences
Infectious agents
Trauma
Stress
Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Four
Principal Categories
Primary immunodysregulation
Decrease of the mucosal barrier
Increase in antigenic exposure
Genetic predisposition HLA-12 HLA
- B51 and Cw7
Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Systemic Disorders Associated with
Recurrent Aphthous Stomatitis
Behcetrsquos syndrome
Celiac disease
Cyclic neutropenia
Nutritional deficiencies
IgA deficiency
Immunoincompetence
Inflammatory bowel disease
Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Three Clinical Variations
Minor
Major ndash Suttonrsquos disease or PMNR
(periadenitis mucosa necrotica
recurrens)
Herpetiform
Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Minor Aphthous Ulcerations
Non-keratinized mucosa
Prodromal symptoms ndash burning itching
stinging
Erythematous macule ndash fibrinopurulent
membrane with a erythematous halo
except in immunocompromised
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Major Aphthous Ulcerations
Larger - 1 to 3 cm
Deeper
Clinically persistent
Develop post pubertal
Recurrences for up to 20 years or more
Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Herpetiform Aphthous
Ulcerations
Greatest number of lesions
Increased frequency of occurrence
Superficial resemblance to herpes
simplex viral infection
Any mucosal surface may be involved
Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Behcetrsquos Syndrome
ldquothe silk routerdquo
Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Behcetrsquos Syndrome
1937 ndash Turkish dermatologist ndashHulusi
Behcet described this condition
Ocular Inflammation
Orogenital Inflammation
Multisystem Disorder
Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Behcetrsquos Disease
Highest Prevalence ndash Middle East and
Japan
Oral Involvement ndash primary
manifestation in 25 to 75 of the
cases
All three forms of aphthous stomatitis
may be seen
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Behcetrsquos Disease
Genital lesions are clinically similar to
oral lesions
75 of the patients demonstrate the
genital lesions
Genital lesions are generally more
symptomatic in males
Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Behcetrsquos Disease
Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Criteria for the Diagnosis of Behcetrsquos
Disease (International Study Group)
Recurrent oral ulceration
Plus two of the following
Recurrent genital ulcerations
Eye lesions ndashanteriorposterior uveitis
Skin lesions
+ pathergy ndash read by 24-48 hours
Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Behcetrsquos Disease
Treament
Topical or intralesional corticosteriods
Oral colchicine
Thalidomide
Low-dose methotrexate
Systemic corticosteriods
Cyclosporine
Interferon alpha2A
Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment
Triamcinolone 01 in Orabase (Kenalog
in Orabase) Apply to dried ulcer two to
four times daily until healed
Randomized controlled studies show decreased
pain
Dexamethasone elixir 05 mg per 5 ml
Swish and spit with 5 mL every 6 hours
As above
B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

B
Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Burning Mouth Syndrome
About 13 million American adults mostly
postmenopausal women are afflicted with
Burning Mouth Syndrome a chronic often
debilitating condition whose cause remains a
medical mystery
Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Burning Mouth Syndrome
The main symptom of burning mouth
syndrome is a burning sensation involving the
tongue lips gums palate throat or
widespread areas of the whole mouth People
with the syndrome may describe the sensation
in the affected areas as hot or scalded as if
they had been burned with a hot liquid
Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Burning Mouth Syndrome
Dry mouth
Sore mouth
A tingling or numb sensation in your mouth
or on the tip of your tongue
A bitter or metallic taste
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Causes
Dry mouth (xerostomia)
Nutritional deficiencies
Allergies
Psychological factors
Nerve disturbance or damage
(neuropathy)
Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatments
Potentially efficacious medicines include
tricyclic antidepressants (like amitriptyline -brand name Elavil)
benzodiazepines (like clonazepam - brand name Klonopin or
chlordiazepoxide brand name - Librium)
even anticonvulsants have proven effective in some cases
BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

BMS Treatment
Tricyclic antidepressants
Amitriptyline (Elavil)10 to 150 mg per day
10 mg at bedtime increase dosage by 10 mg
every 4 to 7 days until oral burning is relieved
or side effects occur
BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

BMS Treatment
Benzodiazepines
Clonazepam (Klonopin)025 to 2 mg per
day025 mg at bedtime increase dosage by
025 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken as full dose or
in three divided doses
BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

BMS Treatment
Anticonvulsants
Gabapentin (Neurontin) 300 to 1600 mg per
day100 mg at bedtime increase dosage by
100 mg every 4 to 7 days until oral burning is
relieved or side effects occur as dosage
increases medication is taken in three divided
doses
C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

C
Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Candidiasis
Oral thrush and other Candida infections
occur when your immune system is
weakened by disease or drugs such as
prednisone or when antibiotics disturb the
natural balance of microorganisms in the
body
Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Predisposing factors for infection
Infancy or old age
Serious underlying disease such as cancer or infection with HIV
Dry mouth due to disease of the salivary glands or medications eg antihistamines diuretics
Dentures (especially if they are not regularly cleaned or fit badly)
Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Predisposing factors for infection
Smoking
Injury to the mouth
Nutritional deficiency eg iron ampor B-vitamin deficiency
Inhaled corticosteroids used to treat asthma eg beclometasone budesonide fluticasone Drink water after inhalation to reduce this complication
Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Clinical features
Acute pseudomembranous candidiasis There are
white patches on gums tongue amp inside the mouth
that can be peeled off leaving a raw area
Acute atrophic candidiasis There are smooth red
shiny patches on the tongue The mouth is very sore
Chronic atrophic candidiasis This is common in
those with dentures The underlying mucosa is red
and swollen
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Clinical features
Angular cheilitis There are sore red splits at each side of the mouth more likely if there is overhang of the upper lip over the lower lip causing a moist deep furrow Angular cheilitis due to candida andor Staphylococcus aureus arises frequently in those taking the medication isotretinoin for acne this medication dries the lips
Chronic hyperplastic candidiasis This is a type of oral leukoplakia (white patch) inside the cheeks or on the tongue with persistent nodules or lumps It usually affects smokers and is pre-malignant Red patches (erythroplakia) as well as white patches may indicate malignant change
Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Clinical features
Chronic mucocutaneous candidiasis presents
as a chronic pseudomembranous infection
The skin and nails are also affected
Median rhomboid glossitis - there is diamond-
shaped inflammation at the back of the
tongue
Severe infections may extend down the throat
(esophageal infection)
Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Rationale for Treatment Topical vs
Systemic Drugs
Topical antifungals are usually the drug of
choice for uncomplicated localized
candidiasis in patients with normal immune
function
Systemic antifungals are usually indicated in
cases of disseminated disease andor in
immunocompromised patients
Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Suggested Medications for the
Treatment of Candidiasis
Rx
Clotrimazole troches 10 mg
Disp 70 troches
Sig Let 1 troche dissolve in mouth 5 times
per day for 14 days Do not chew NPO 12
hour
Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Suggested Systemic Medications for
the Treatment of Candidiasis Rx
Ketoconazole tablets 200 mgDisp 14 tabletsSig Take 1 tab qd with a meal or orange juice for 14 days
RxFluconazole tablets 100 mgDisp 15 tabletsSig Take 2 tablets stat then 1 tablet qd for 14 days
RxItraconazole tablets 100 mgDisp 28 tabletsSig Take 1 tablet bid with a meal or orange juice for 14 days
CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

CA
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Head and Neck Cancer
Squamous Cell Carcinoma
Intraoral Melanoma
Lymphoma
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Intraoral Melanoma
The five year survival rate for oral melanoma
is less than 20 as compared to 75 for
Cutaneous melanomas The average time of
first local recurrence for oral melanoma is less
than one year and metastatic disease is usually
diagnosed within three months of the
recurrence The average survival rate after
metastasis is typically less than 6 months
Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Extranodal Lymphoma
Extranodal lymphomas usually develop as a
rapidly growing mass of the palate or
posterior tongue (area of Waldeyerrsquos ring)
Pain may or may not be a presenting sign
Clinically the lesion may present as an
erythematous mass with a boggy consistency
The average survival rate for AIDS patients
with an intraoral lymphoma is eight months
Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Squamous Cell Carcinoma
Second primary ndash field cancerization
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
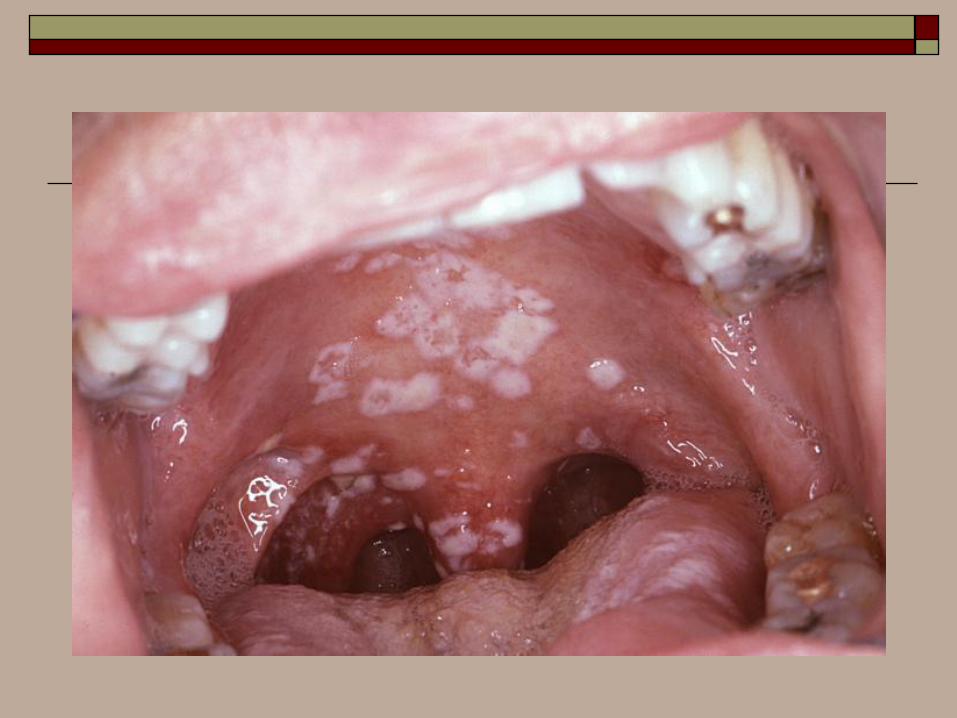
Incidence amp Mortality HampN Ca
41000 new cases annually
13000 affected will die of disease
Rates constant over last 20yrs
lt 5 of neoplasias US
Highest incidence southeastern amp south-
central Asia
Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Disease in Women
Prior to 1940 malefemale ratio - 101
1980s ratio 31
Reason tobacco use among women in early
decades of the century
Habits have stabilized ndash malefemale
incidence normalized
Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Tobacco Use
1956 Wynder et al HampN Ca 10-fold
increase among smokers
Most studies 5-fold to 25-fold increase
intensity and duration of tobacco
consumption
80-90 of HampN Ca patients use tobacco
Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Alcohol
Odds ratio increases 3- to 15-fold for HampN
Ca after adjusting for tobacco use with
consumption of alcohol
Multiplicative effect with tobacco and
alcohol
Location of cancer ndash oral
pharyngeal(topical mechanism)
Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Alcohol
Promotional effects independent of
initiation
-prostaglandin synthesis lipid peroxidation
free radical oxygen enhance cell turnover
Enhances cell permeability
Defective repair mechanisms
Depressed immunity
Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Dz
RISK FACTORS (RF)
1 RF
2 RF
3 RF
4 RF
The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

The concept of
TUMOR
local
regional
systemic
local T
N
M
INFECTION PAIN
INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

INFECTION NEOPLASM
CERVICAL LYMPH NODE ENLARGEMENT
bullbacterial
bullviral (local systemic)
bullfungal
bullpostinfect fibrosed node
bulllt 40 yrs lymphoma
bullgt 40 yrs metastatic SCC
OTHERS
bullleukemia
bullconnective tissue diseases (eg lupus)
bullsarcoidosis
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Importance of early diagnosis of squamous cell carcinoma
60
stage III amp IV
23 recurrence lt 2 yrs
lt 13 survive 3 yrs
40
stage I amp II
80-90 cure
Second primary tumor in successfully treated patients within 5-7
years up to 40 Follow-up important
Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Squamous Cell Carcinoma
Mortality (8000) deaths per year
Mortality by Site
Tongue 432
Salivary 130
Floor of mouth 950
Lip 24
Other 319
Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Premalignant Lesions
Leukoplakia
Erythroplakia
Erythroplasia
Carcinoma in situ
Verrucous Leukoplakia
Tobacco patch keratosis
Actinic cheilosis
Mouth wash (Viadent) dysplasia
Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Leukoplakia
Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Erythroplakia
Defined as a red patch that can not be
clinically or pathologically diagnosed as any
other condition
Almost all erythroleukoplakia demonstrate
dysplasia or CIS
Etiology is similar to oral SCC
May occur in conjunction with leukoplakia
Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Erythroplakia
Risk of malignant transformation in
erythroleukoplakia about 4x greater than
homogenous leukoplakia
Predominately disease of older men with peak
prevalence of 65 to 74 years
Floor of mouth tongue and soft palate are
most common sites of involvement
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Erythroplakia
The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

The Management of Head and
Neck Cancer
Major advances
Conservative or partial resections
Micro vascular free-tissue transfer in
reconstruction
Better definition of the roles of chemotherapy
and radiotherapy
Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Despite these advances the treatment of loco
regional recurrence remains a major challenge
success rates for salvage therapy are poor
Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment
Surgery
Radiotherapy
Chemotherapy
Immunotherapy
at present the role of immunotherapy remains investigational
Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Chemotherapy
Several randomized and non-randomized trial have evaluated chemotherapy for the treatment of head and neck cancer
Various agents have been shown to produce a response
No agents either alone or in combination have demonstrated an improvement in survival
cisplatin and 5 - FU
Uses
Inoperable tumors
Salvage therapy for recurrent tumors
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Treatment
The main treatment modalities for head and neck
cancer remain surgery and radiotherapy
Patient factors that merit consideration
Impact on the quality of life
Medical condition ndash ldquoco - morbiditiesrdquo
Patient preference
Treatment cost and convenience
Compliance
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
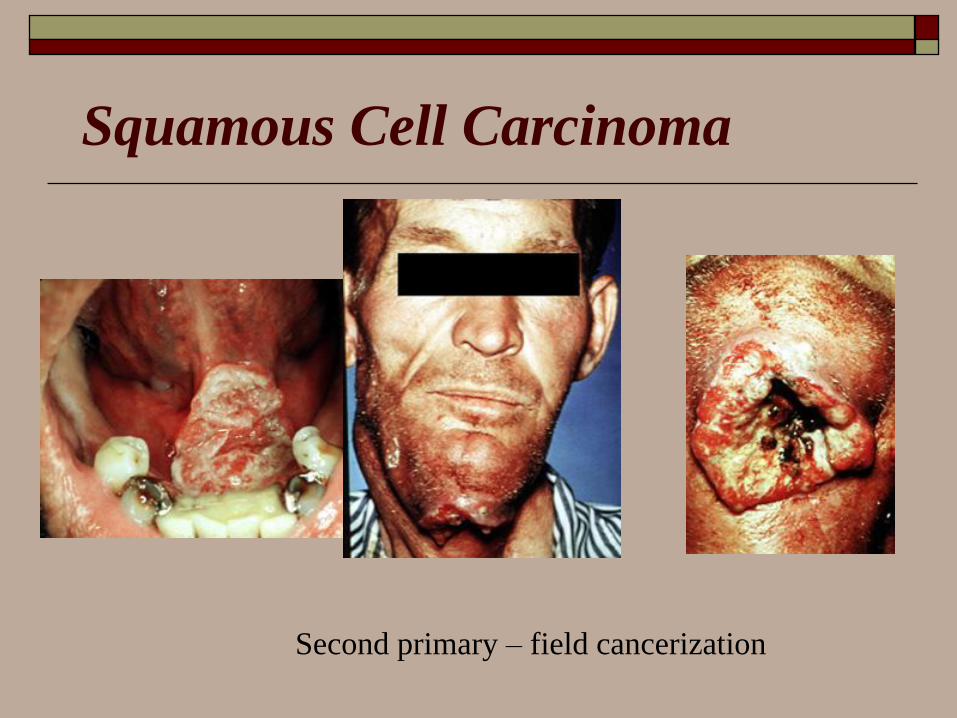
Treatment
Early stage disease (stage I and II) can be treated with either surgery or radiotherapy with equivalent control rates
Small lesions of the oral cavity wide local excision is preferred over radiotherapy
Radiotherapy can be delivered to a site generally only once
Reserve this modality for less operable lesions
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
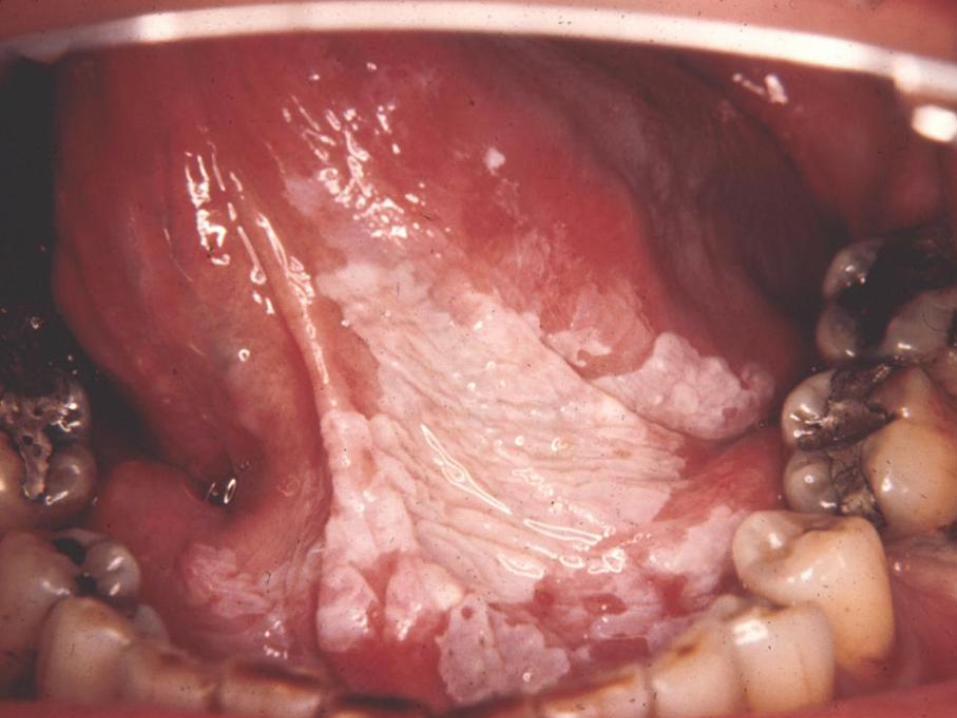
Treatment Combined Modality
Surgery and RadiotherapyIndications for post operative radiotherapy
Primary Tumor
Advance T stage
High histologic grade
Positive surgical resection margins
Lymphatic permeation
Vascular invasion
Perineural spread
Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Radiotherapy
Daily dose of 180 cGy to 200 cGy
5000 cGy over a five week period
T1 ndash 6000 to 6600 cGy
T2 - 6600 to 7000 cGy
T3T4 - gt 7000 cGy
ldquoshrinking field techniquerdquo
hyperfractionation technique 200 cGy per day for 25 days followed by 400 cGy per day for 5 days
D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

D
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Desquamative gingivitis is a clinical term to describe red painful glazed and friable gingivae which may be a manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Clinical features of desquamative
gingivitis
Fiery red friable gingiva
Painful desquamates easily
Buccal aspect of anterior attached gingiva
affected
Marginal gingiva spared
Not significantly improved by oral hygiene
measures alone
Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Differential Diagnosis Erosive Lichen Planus
Immune-mediated blistering diseases
Intra-epithelial
Pemphigus
Subepithelial
Pemphigoid
Linear IgA disease
Dermatitis herpetiformis
Epidermolysis bullosa
Erythema multiforme
Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment Topical Corticosteroids Recurrent aphthous ulcers
bull Oral manifestations of Behccedilets disease Reiters syndrome acute
vulvar ulcer MAGIC syndrome PFAPA syndrome ulcerative colitis
Crohns disease Melkersson-Rosenthal syndrome Sweets
syndrome among others
bull Drug-induced ulcerations mediated by an immune mechanism
bull Lichen planus
bull Cicatricial pemphigoid
bull Mucous membrane pemphigoid
bull Bullous pemphigoid
bull Erythema multiforme
bull Linear IgA dermatosis
bull Pemphigus vulgaris
Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Topicals Temovate cream 005 Clobetasol propionate
Halog cream 01 Halcinonide
Lidex cream 005 Fluocinonide
Topicort cream 025 Desoximethasone
Lidex gel 005 Fluocinonide
Aristocort cream H-P 05 Triamcinolone acetinode
Diprosone cream 005 Betamethasone dipropionate
Florone cream 005 Diflorasone diacetate
Maxiflor cream 005 Diflorasone diacetate
Synalar cream H-P 02 Fluocinolone acetonide
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
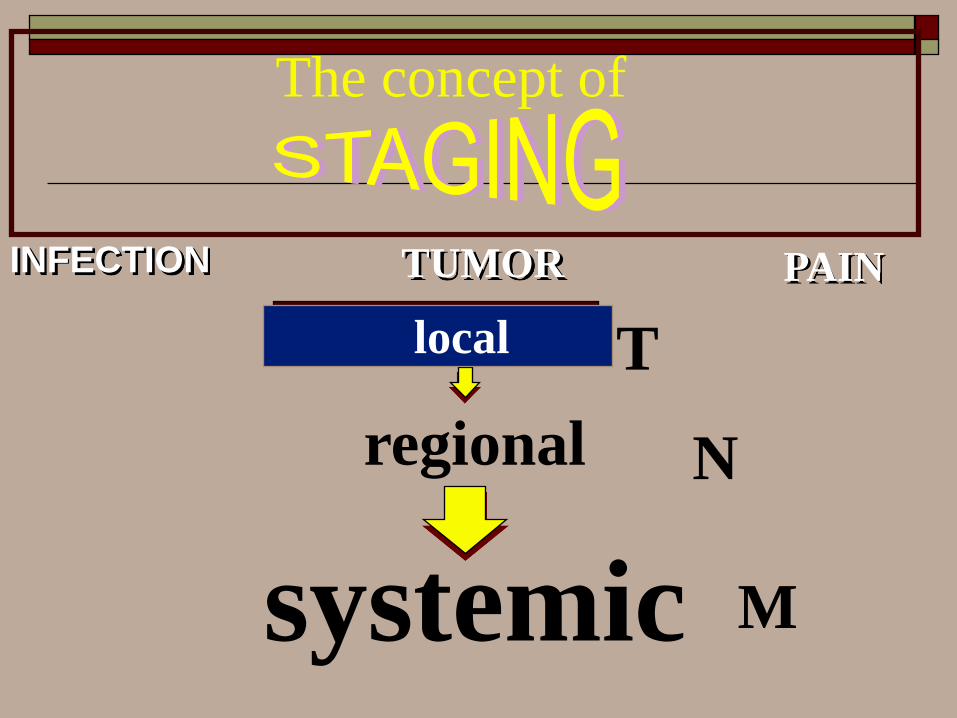
Topicals Tropicort-LP cream 005 Desoxymethasone
Benisone cream 0025 Betamethasone benzoate
Cordran cream 0025 Flurandenolide
Kenalog cream 01 Triamcinolone acetonide
Locoid cream 01 Hydrocortisone butyrate
Synalar cream 0025 Fluocinolone acetonide
Valisone cream 01 Betamethasone valerate
Tridesilon cream 005 Desonide
Locorten cream 003 Flumetasone pivalate
1 Hydrocortisone
Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Topical Corticosteroids
Used to treat oral lesions
Clobetasol (Temovate) -- Suppresses mitosis and increases synthesis of proteins that decrease inflammation and cause vasoconstriction Class I superpotent topical steroid useful in treating oral lesions Topical corticosteroids commonly are used intraorally for oral manifestations of autoimmune blistering skin diseases Since these diseases are chronic inflammatory in nature topical corticosteroids are very useful as an adjunct treatment Patients with disease confined to the gingiva should see a dentist to have a custom-made soft tray to carry the medication
H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

H
How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

How does herpes simplex develop
overexposure to sunlight
overexposure to wind
colds influenza and similar infections
heavy alcohol use
fever from any cause
the menstrual period
physical stress
emotional stress
Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Symptoms
Primary (Initial) HSV I Fever
Adenopathy
Ulcers deep in mouth
Secondary (Later) HSV I (Recurrent labial lesions) Fever Blisters form on outer vermillion border
Cold Sores form on inner lip Initial Vesicle
Next Crust
Last Healing in 10-14 days
Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Differential Diagnosis
Differs from Aphthous Ulcers in that
Found on keratinized (bound-down) intraoral
mucosa
Vesicles rupture into coalescing ulcers
HSV lesions are anterior compared with
Herpangina
Hand Foot and Mouth Disease
Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Specific antiviral drugs Herpes
Oral acyclovir (Zovirax) or the recently
developed drugs valacyclovir (Valtrex) or
famciclovir (Famvir) lessen the symptoms
and frequency of fever blister recurrences for
some patients These drugs prevent HSV from
multiplying and are effective when taken in
pill form prior to an outbreak of the virus
Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Systemic Antivirals
Acyclovir
Dose 15 mgkg (max 200 mg) PO 5xday for 7 days
Shortens first HSV infection by 6 days in children
Famciclovir
Shortens healing time by 2 days in UV-induced cases
Spruance (1999) J Infect Dis 179303-10
Valacyclovir (FDA approved for age 12 and older)
Adult dose 2 g PO bid for one day
Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Specific antiviral drugs Herpes
Topical antiviral creams containing acyclovir
(Zovirax) or penciclovir (Denavir) may also
help in limiting the extent or duration of
lesions if applied promptly to affected areas
Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Topical Treatments
Penciclovir (Denavir) heals HSV-1 sores on average about half a day faster than without treatment stops viral shedding and reduces the duration of the pain Ideally the patient should apply the cream within the first hour of symptoms although benefits have also been noted with later application It is continued for four consecutive days and should be reapplied every two hours while awake
Docosanol cream (Abreva) is an over-the-counter agent for oral-facial herpes It helps resist infection by inhibiting the ability of the virus to become fully active after it has attached itself to the host cell It is applied five times a day beginning at the first sign of tingling or pain Studies have been mixed on it benefits
Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Topical Treatments
Acyclovir cream (Zovirax) has been approved It may speed healing of oral herpes lesions and lessen the duration of pain particularly if it is applied early on (at the first sign of pain or tingling)
Lidex is a gel that contains a fluocinonide as corticosteroid Corticosteroids commonly called steroids are anti-inflammatory agents and not ordinarily used for herpes Some evidence suggests it may be effective in combination with oral famciclovir
Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Topical Treatments
Over-the-counter topical anesthetics may provide
modest relief They include Anbesol gel Blistex lip
ointment Campho-phenique Herpecin-L
Viractin and Zilactin In one study Viractin
reduced the duration of the attack compared to
placebo by two days It also relieved itching but had
little effect on other symptoms In general however
few studies have been conducted on any of these
products
X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

X
Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Xerostomia
Xerostomia is not a disease but can be a symptom
of certain diseases It can produce serious
negative effects on the patients quality of life
affecting dietary habits nutritional status
speech taste tolerance to dental prosthesis and
increases susceptibility to dental caries The
increase in dental caries can be devastating in
many patients and therefore special care must be
made to control this condition
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Causes for Xerostomia include
-Medications - Several hundred current medications
can cause xerostomia antihypertensives
antidepressants analgesics tranquilizers diuretics
and antihistamines c
-Cancer Therapy - Chemotherapeutic drugs can
change the flow and composition of the saliva
Radiation treatment that is focused on or near the
salivary gland can temporarily or permanently
damage the salivary glands
-Sjogrens syndrome - An autoimmune disease causes
xerostomia and dry eyes
Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Causes for Xerostomia include
-Other conditions -such as bone marrow transplants endocrine disorders stress anxiety depression and nutritional deficiencies may cause xerostomia
-Nerve Damage - Trauma to the head and neck area from surgery or wounds can damage the nerves that supply sensation to the mouth While the salivary glands may be left intact they cannot function normally without the nerves that signal them to produce saliva
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Treatment
Identify the xerostomic condition and the
cause Some of the causes may be
ameliorated and this will aid therapy But
in many situations it will be difficult to
eliminate the causes Thus it will be
necessary for the Dentist to control the
results of xerostomia This is especially
true about the increase in dental caries
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid
Treatment -pilocarpine (Salagen) 5mg qid prescription required
-special food preparation - blended and moist foods are easier to swallow
artificial saliva (available over-the-counter)
-sipping plain water is usually preferred over artificial saliva by most patients
-Biotene brand over-the-counter dry mouth products (toothpaste alcohol- free mouth rinse and Oralbalance lubricating gel)
-avoidance of alcohol-based mouth rinses
-use of water and glycerin mixed in a small aerosol spray bottle
RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

RX
Contains sorbitol sodium
carboxymethlcellulose and
methylparaben in a
pleasantly flavored
solution
120 mL (406 fl oz)
Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Z
Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment
Acyclovir (Zovirax)dagger800 mg orally five times
daily for 7 to 10 days
10 mg per kg IV every 8 hours for 7 to 10
daysDagger
$174 to 248 (129 to 200)
Famciclovir (Famvir)dagger500 mg orally three
times daily for 7 days
$140
Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment
Valacyclovir (Valtrex)dagger1000 mg orally three
times daily for 7 days
$84
Prednisone (Deltasone)30 mg orally twice
daily on days 1 through 7 then 15 mg twice
daily on days 8 through 14 then 75 mg twice
daily on days 15 through 21
Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Treatment
Lotions containing calamine (eg Caladryl)
may be used on open lesions to reduce pain
and pruritus
Once the lesions have crusted over capsaicin
cream (Zostrix) may be applied
Topically administered lidocaine (Xylocaine)
and nerve blocks have also been reported to
be effective in reducing pain
Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Postherpetic Neuralgia
Amitriptyline (Elavil) -- By inhibiting reuptake of serotonin andor norepinephrine by presynaptic neuronal membrane may increase synaptic concentration in CNS Useful as analgesic for certain types of chronic and neuropathic pain
Adult DoseEarly in course of HZ 25 mgd PO hs to prevent PHNAfter PHN develops 30-100 mg PO qhs
Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Postherpetic Neuralgia
Capsaicin cream (Dolorac Capsin Zostrix) --Natural chemical derived from plants of Solanaceae family By depleting and preventing reaccumulation of substance P in peripheral sensory neurons may render skin and joints insensitive to pain Substance P thought to be chemomediator of pain transmission from periphery to CNS
Adult DoseCream Apply to skin tidqid for 3-4 consecutive wk and evaluate efficacy not to exceed 4 applicationsd
Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Postherpetic Neuralgia
Lidocaine (DermaFlex gel Lidoderm 5 patch) --Several recent studies have advocated topical administration of lidocaine as treatment of PHN Lidocaine gel (5) in placebo-controlled study showed significant relief in 23 patients studied Lidocaine tape also decreases severity of pain
Adult DoseGel (5) Apply to affected area prnPatch (5) Apply to most painful area up to 3 patches per application patch may remain in place for up to 12 h in any 24 h period
Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid

Postherpetic Neuralgia Gabapentin (Neurontin) -- This medication has been
approved by the FDA for the treatment of PHN Has properties common to other anticonvulsants and antineuralgic effects Exact mechanism of action is not known Structurally gabapentin is related to GABA but it does not interact with GABA receptors Believed to have a binding site at the alpha 2-delta protein an auxiliary subunit of voltage-gaited calcium channels In the rat brain binding is localized on neuronal dendritic areas Relevance of these observations to treatment of PHN is not known
Adult Dose100 mg PO tid titrate dose prn recommended dose is 900-1800 mg PO qd not to exceed 900 mg PO qid









![Skin Inflammation, [Acute, Suppurative, Chronic, Chronic ... · Skin – Inflammation, [Acute, Suppurative, Chronic, Chronic Active, Granulomatous] presence of mononuclear cells (lymphocytes,](https://static.fdocuments.net/doc/165x107/5f0eb0c97e708231d44075f1/skin-inflammation-acute-suppurative-chronic-chronic-skin-a-inflammation.jpg)







