Epidemiology ofFine Particulate Air Pollutionand Human ......(usually daily) variations in health...
48
Epidemiology of Fine Particulate Air Pollution and Human Health: Biologic Mechanisms and Who's at Risk? C. Arden Pope Ill Brigham Young University, Provo, Utah, USA This article briefly summarizes the epidemiology of the health effects of fine particulate air pollution, provides an early, somewhat speculative, discussion of the contribution of epidemiology to evaluating biologic mechanisms, and evaluates who's at risk or is susceptible to adverse health effects. Based on preliminary epidemiologic evidence, it is speculated that a systemic response to fine particle-induced pulmonary inflammation, including cytokine release and altered cardiac autonomic function, may be part of the pathophysiologic mechanisms or pathways linking particulate pollution with cardiopulmonary disease. The elderly, infants, and persons with chronic cardiopulmonary disease, influenza, or asthma are most susceptible to mortality and serious morbidity effects from short-term acutely elevated exposures. Others are susceptible to less serious health effects such as transient increases in respiratory symptoms, decreased lung function, or other physiologic changes. Chronic exposure studies suggest relatively broad susceptibility to cumulative effects of long-term repeated exposure to fine particulate pollution, resulting in substantive estimates of population average loss of life expectancy in highly polluted environments. Additional knowledge is needed about the specific pollutants or mix of pollutants responsible for the adverse health effects and the biologic mechanisms involved. Key words: air pollution, cardiopulmonary disease, health effects, life expectancy, particulate pollution, review. - Environ Health Perspect 1 08(suppl 4):713-723 (2000). http.//ehpnetl.niehs. nih.gov/docs/2000/suppl-4/713-723pope/abstract.html It has long been known, or at least suspected, that there are adverse health effects associated with ambient air pollution (1). Extreme air pollution episodes in the 1930s-1950s were associated with dramatically elevated cardio- pulmonary morbidity and mortality. Evidence of serious health effects provided by these episodes spurred a growing concern about air pollution and in the United States during the 1950s through early 1970s, there was a series of legislative efforts related to try- ing to control air pollution. Current air pollu- tion legislation is based largely on the 1970 Clean Air Act and 1990 Amendments to this act (2). The amended Clean Air Act man- dated national ambient air quality standards for pollutants that are relatively common and widespread but may reasonably be anticipated to endanger public health. Six pollutants that met these basic criteria (criteria pollutants) were eventually selected, including particulate matter (PM), sulfur dioxide, nitrogen diox- ide, carbon monoxide, ozone, and lead. Since 1970 there have been hundreds of published studies that have evaluated the health effects of these air pollutants. A 1996 review of the health effects of these criteria pollutants (along with two other common pollutants) was prepared by the Committee of the Environmental and Occupational Health Assembly of the American Thoracic Society (ATS) (2). There have also been numerous recent reviews that have focused on health effects of particulate air pollution (3-14). This article does not attempt to replicate the excellent ATS review of all the criteria pollutants or previous general reviews of particulate air pollution. The overall plan of this article is to focus on three basic topics. First, the epidemiology of the health effects of fine particulate air pollution PM2.5 (particles < 2.5 pm) will be briefly summarized, although recent, more comprehensive reviews are available. This summary relies heavily on updates of several previous reviews by Dockery and Pope (6,8-11). Second, a some- what speculative discussion of the early but clearly incomplete contribution of epidemiol- ogy to evaluating the biologic mechanisms is provided. This discussion of biologic mecha- nisms is updated from papers originally pre- pared for presentation at international symposia (10,11). Finally, an original discus- sion of who risks adverse health effects due to exposure to fine particulate air pollution is presented. Characteristics of Fine Particles Particulate air pollution refers to an air- suspended mixture of solid and liquid particles that vary in size, composition, and origin. The size distribution of total suspended particles (TSPs) in the atmosphere is trimodal and includes coarse particles, fine particles, and ultrafine particles. Coarse particles (often defined as those with an aerodynamic diameter > 2.5 pm) are often naturally occurring and derived primarily from soil and other crustal materials. Fine particles (PM2,5) are derived chiefly from combustion processes in trans- portation, manufacturing, power generation, etc. Sulfate and nitrate particles are commonly generated by conversion from primary sulfur and nitrogen oxide emissions, and a varying portion of sulfate and nitrate particles may be acidic. Therefore, in most urban areas, PM2.5 mostly comprises primary combustion-source particles as well as secondary combustion particles including sulfates and nitrates. Ultrafine particles are often defined as parti- cles < 0.1 pm. These particles have relatively short residence times in the atmosphere because they accumulate or coagulate to form larger fine particles. Various physiologic and toxicologic considerations suggest that exposure to fine particles may be a health concern. Their size is such that they can be breathed most deeply in the lungs. They include sulfates, nitrates, acids, metals, and carbon particles with vari- ous chemicals adsorbed onto their surfaces. Relative to coarse particles, they more readily penetrate indoors, are transported over longer distances, and are somewhat uniform within communities, resulting in highly ubiquitous exposure. The initial reference method for meas- uring particle concentrations and establishing health standards in the United States was TSPs. In 1987 the U.S. Environmental Protection Agency (U.S. EPA) changed the reference method to include only inhalable particles. Inhalable particles refers to those particles that can penetrate the thoracic air- ways; for purposes of standard setting, inhal- able particles were specifically defined as particles < 10 pm in aerodynamic diameter (PM1o). In 1997 the U.S. EPA promulgated new standards (15) for an even finer cut of particulate air pollution-particles < 2.5 pm in aerodynamic diameter (PM2.5); however, in May 1999, a U.S. Court of Appeals blocked the implementation of these standards. Health Effects of Acute Exposure The large majority of epidemiologic studies of particulate air pollution have been acute exposure studies that evaluated short-term This article is part of the monograph on Environmental and Occupational Lung Diseases. Address correspondence to C. Arden Pope lil, 142 FOB, Brigham Young University, Provo, UT 84602 USA. Telephone: (801) 378-2157. Fax: (801) 378-2844. E-mail: [email protected] Received 24 May 1999; accepted 16 August 1999. Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 713
Transcript of Epidemiology ofFine Particulate Air Pollutionand Human ......(usually daily) variations in health...
-
Epidemiology of Fine Particulate Air Pollution and Human Health:Biologic Mechanisms and Who's at Risk?C. Arden Pope IllBrigham Young University, Provo, Utah, USA
This article briefly summarizes the epidemiology of the health effects of fine particulate airpollution, provides an early, somewhat speculative, discussion of the contribution of epidemiologyto evaluating biologic mechanisms, and evaluates who's at risk or is susceptible to adverse healtheffects. Based on preliminary epidemiologic evidence, it is speculated that a systemic responseto fine particle-induced pulmonary inflammation, including cytokine release and altered cardiacautonomic function, may be part of the pathophysiologic mechanisms or pathways linkingparticulate pollution with cardiopulmonary disease. The elderly, infants, and persons with chroniccardiopulmonary disease, influenza, or asthma are most susceptible to mortality and seriousmorbidity effects from short-term acutely elevated exposures. Others are susceptible to lessserious health effects such as transient increases in respiratory symptoms, decreased lungfunction, or other physiologic changes. Chronic exposure studies suggest relatively broadsusceptibility to cumulative effects of long-term repeated exposure to fine particulate pollution,resulting in substantive estimates of population average loss of life expectancy in highly pollutedenvironments. Additional knowledge is needed about the specific pollutants or mix of pollutantsresponsible for the adverse health effects and the biologic mechanisms involved. Key words: airpollution, cardiopulmonary disease, health effects, life expectancy, particulate pollution, review.- Environ Health Perspect 1 08(suppl 4):713-723 (2000).http.//ehpnetl.niehs. nih.gov/docs/2000/suppl-4/713-723pope/abstract.html
It has long been known, or at least suspected,that there are adverse health effects associatedwith ambient air pollution (1). Extreme airpollution episodes in the 1930s-1950s wereassociated with dramatically elevated cardio-pulmonary morbidity and mortality.Evidence of serious health effects provided bythese episodes spurred a growing concernabout air pollution and in the United Statesduring the 1950s through early 1970s, therewas a series of legislative efforts related to try-ing to control air pollution. Current air pollu-tion legislation is based largely on the 1970Clean Air Act and 1990 Amendments to thisact (2). The amended Clean Air Act man-dated national ambient air quality standardsfor pollutants that are relatively common andwidespread but may reasonably be anticipatedto endanger public health. Six pollutants thatmet these basic criteria (criteria pollutants)were eventually selected, including particulatematter (PM), sulfur dioxide, nitrogen diox-ide, carbon monoxide, ozone, and lead.
Since 1970 there have been hundreds ofpublished studies that have evaluated thehealth effects of these air pollutants. A 1996review of the health effects of these criteriapollutants (along with two other commonpollutants) was prepared by the Committee ofthe Environmental and Occupational HealthAssembly of the American Thoracic Society(ATS) (2). There have also been numerousrecent reviews that have focused on healtheffects of particulate air pollution (3-14).This article does not attempt to replicate theexcellent ATS review of all the criteria
pollutants or previous general reviews ofparticulate air pollution. The overall plan ofthis article is to focus on three basic topics.First, the epidemiology of the health effects offine particulate air pollution PM2.5 (particles< 2.5 pm) will be briefly summarized,although recent, more comprehensive reviewsare available. This summary relies heavily onupdates of several previous reviews byDockery and Pope (6,8-11). Second, a some-what speculative discussion of the early butclearly incomplete contribution of epidemiol-ogy to evaluating the biologic mechanisms isprovided. This discussion of biologic mecha-nisms is updated from papers originally pre-pared for presentation at internationalsymposia (10,11). Finally, an original discus-sion ofwho risks adverse health effects due toexposure to fine particulate air pollutionis presented.
Characteristics ofFine ParticlesParticulate air pollution refers to an air-suspended mixture of solid and liquid particlesthat vary in size, composition, and origin. Thesize distribution of total suspended particles(TSPs) in the atmosphere is trimodal andincludes coarse particles, fine particles, andultrafine particles. Coarse particles (oftendefined as those with an aerodynamic diameter> 2.5 pm) are often naturally occurring andderived primarily from soil and other crustalmaterials. Fine particles (PM2,5) are derivedchiefly from combustion processes in trans-portation, manufacturing, power generation,
etc. Sulfate and nitrate particles are commonlygenerated by conversion from primary sulfurand nitrogen oxide emissions, and a varyingportion of sulfate and nitrate particles may beacidic. Therefore, in most urban areas, PM2.5mostly comprises primary combustion-sourceparticles as well as secondary combustionparticles including sulfates and nitrates.Ultrafine particles are often defined as parti-cles < 0.1 pm. These particles have relativelyshort residence times in the atmospherebecause they accumulate or coagulate toform larger fine particles.
Various physiologic and toxicologicconsiderations suggest that exposure to fineparticles may be a health concern. Their sizeis such that they can be breathed most deeplyin the lungs. They include sulfates, nitrates,acids, metals, and carbon particles with vari-ous chemicals adsorbed onto their surfaces.Relative to coarse particles, they more readilypenetrate indoors, are transported over longerdistances, and are somewhat uniform withincommunities, resulting in highly ubiquitousexposure.
The initial reference method for meas-uring particle concentrations and establishinghealth standards in the United States wasTSPs. In 1987 the U.S. EnvironmentalProtection Agency (U.S. EPA) changed thereference method to include only inhalableparticles. Inhalable particles refers to thoseparticles that can penetrate the thoracic air-ways; for purposes of standard setting, inhal-able particles were specifically defined asparticles < 10 pm in aerodynamic diameter(PM1o). In 1997 the U.S. EPA promulgatednew standards (15) for an even finer cut ofparticulate air pollution-particles < 2.5 pmin aerodynamic diameter (PM2.5); however, inMay 1999, a U.S. Court of Appeals blockedthe implementation of these standards.
Health Effects ofAcute ExposureThe large majority of epidemiologic studies ofparticulate air pollution have been acuteexposure studies that evaluated short-term
This article is part of the monograph on Environmentaland Occupational Lung Diseases.
Address correspondence to C. Arden Pope lil, 142FOB, Brigham Young University, Provo, UT 84602USA. Telephone: (801) 378-2157. Fax: (801) 378-2844.E-mail: [email protected]
Received 24 May 1999; accepted 16 August 1999.
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 713
-
(usually daily) variations in health end pointssuch as mortality counts, hospitalizations,symptoms, and lung function associated withshort-term variations in levels of pollution. Abrief summary of the results of these acuteexposure studies is presented in Table 1.Unfortunately, until recently (following thepromulgation of the new PM2.5 standards),there has been very little daily monitoring offine partides, and most of the studies summa-rized in Table 1 used alternative measures ofparticulate concentrations.
Episode StudiesThe earliest and most methodologicallysimple epidemiologic studies are those thatevaluate air pollution episodes. These studiescompare mortality (and morbidity) before,during, and after pollution episodes. InDecember of 1930 in the Meuse Valley,Belgium, in October of 1948 in Donora,Pennsylvania, and in December of 1952 inLondon, England, stagnant air massesresulted in marked increases in the concentra-tions of air pollutants. Although the biologicmechanisms were not well understood, thelarge excess mortality and morbidity associ-ated with the extreme episodes clearly
demonstrated a link between mortality andmorbidity and air pollution. During theseepisodes of highly stagnant air conditions, thePM pollution would have been primarilyfrom combustion sources, and therefore PMmass would have been mostly fine particles.Two recent studies of less severe air pollutionepisodes (16,21) suggested smaller mortalityand morbidity effects associated with lessextreme pollution.
Mortality CountsMany recent daily time-series mortalitystudies have also observed changes in dailydeath counts associated with short-termchanges in particulate air pollution, even atrelatively low or moderate concentrations(Table 1). There have been more than 60 suchstudies conducted in at least 35 cities. The rel-ative risk of mortality increased monotonicallywith particulate concentrations, usually in alinear or near-linear fashion. These studies didnot observe a particulate pollution healtheffects threshold. In addition, these studiesoften observed a lead-lag relationship betweenAir nnliillinn incl mnrtAlitv- Thte rpf^RiiiR RlC-11 FVXtSVXul Cdlu *sSVt LtCLXy. A lie icgested that the increased mortalityconcurrently or within 1-5 days fol
Table 1. Summary of epidemiologic evidence of health effects of acute exposure to particulate air pollutiHealth end pointsEpisodes ofdeath andhospitalizationsMortality
Basic study designEvaluate changes in mortalityand morbidity before, during,and after pollution episodes.Population-based time-seriesstudies that include statisticaltime-series modeling to eval-uate potential associationswith daily mortality counts.
Hospitalization Population-based time-and other health- series studies that evaluatecare visits associations between
pollution and daily changesin hospitalization and relatedhealth-care end points.
Symptoms/ Panel-based time-serieslung function studies of symptom and/or
lung function datarepeatedly collected fromindividuals in well-definedpanels or cohorts.
Observed associations with PM
Elevated respiratory and cardiovascularmortality and hospitalizations.
Elevated daily respiratory and cardio-vascular mortality counts. Effects persistedwith various approaches to control fortime trends, seasonality, and weather.Near-linear associations with littleevidence of a threshold.Elevated hospitalizations, emergencyvisits, and clinic/outpatient visits forrespiratory and cardiovascular disease.Effects generally persisted with variousapproaches to control for time trends,seasonality, and weather.Increased occurrence of lower respiratorysymptoms, cough, and exacerbation of asthma.Only relatively weak associations withupper respiratory symptoms. Small,statistically significant declines in FEVo.75,FEV1, or PEF, and increased occurrence ofclinically significant declines in lung function.
Abbreviations: FEVoy75, forced expiratory volume in 0.75 sec; FEV1, forced expiratory volume in 1 sec; PEF, peak expiratory
Table 2. Overall estimates of daily mortality effects of an increase in exposure to particulate air polluticause-of-death categories.
Cause-specific percent PerceiPercent of increase per 50 pg/m3 deal
Cause of death total deathsa increase in PM2.5a PMAll causesb 100 7.0Respiratory 8 25.0Cardiovascular 45 11.0Other disease 47 0.4'Based on updated summary estimates from previous reviews (6,8, 10). bExcluding accidents, suicide, homicide, etc.
increase in air pollution. Because variousmeasurements of particulate pollution wereused in the different studies, and because vari-ous modeling strategies were used, precisecomparisons of effect estimates across all thestudies were difficult. However, changes indaily mortality associated with particulate airpollution were typically estimated at approxi-mately 0.5-1.5%/10 pg/m3 increase in PM1oconcentrations, or per about 5 or 6 pg/m3increase in PM2.5 concentrations.
Studies that provided a breakdown ofmortality by broad cause-of-death categoriesobserved that particulate air pollution gener-ally had the largest effect on respiratory andcardiovascular disease mortality. Estimates ofdaily mortality effects of an increase in expo-sure to particulate air pollution by broadcause-of-death categories are summarized inTable 2. The estimated cause-specificincrease in mortality risk is much larger forrespiratory than for cardiovascular disease.However, the percent of excess deaths attrib-utable to particulate exposure is mostly dueto cardiovascular disease.
occurred Hospitalizationslowing an Daily counts of hospital admissions can be
analyzed in a manner similar to the assess-ment of daily counts of mortality. More than50 daily time-series studies have reported
References associations between particulate air pollution
(16-21) and hospitalization or related health care endpoints (Table 1). Most of these studies haveevaluated associations between respiratory
(22-66) hospital admissions and air pollution. Severalstudies have also analyzed emergency depart-ment visits for asthma, chronic obstructivepulmonary disease, and other respiratory ail-ments, and observed associations with partic-
(67-114) ulate air pollution. More recent studies haveobserved associations between particulate airpollution and hospitalizations for cardio-vascular disease (73,74,87,98-100).
Symptoms/Lung Functon(115152) There are more than 40 published studies
evaluating associations between daily respira-tory symptoms and/or lung function and par-ticulate air pollution (Table 1). Althoughmany of these studies focused on asthmaticsand exacerbation of asthma, others followed
(flow. nonasthmatics and evaluated changes in acuterespiratory health status more generally.
ion by broad Small, often statistically insignificant, associa-tions between particulate pollution and upper
nt of excess respiratory symptoms were observed.ths due to Associations with lower respiratory symptomsexposure and cough, however, were typically larger and100 usually statistically significant. Exacerbation28 of asthma, based on recorded asthma attacks69 or increased bronchodilator use, were also3 associated with particulate air pollution.
Associations between more general measures
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000
POPE
714
-
FINE PARTICULATE AIR POLLUTION AND HUMAN HEALTH
of acute disease have been studied, includingevaluations of the timing of restricted activitydays of U.S. adult workers due to illness(131,132) and school absences in gradeschool children (141).
Measures of lung function have also beenused as an objective and potentially sensitiveindicator of acute response to air pollution.Various studies have taken repeated measure-ments of the lung function of panels of chil-dren and/or adults. These studies havetypically reported very small but often statisti-cally significant decreases in lung functionassociated with elevated levels of particulateair pollution concentrations. Lagged effects ofup to 7 days were observed.
Effects of Chronic ExposureThe previously discussed acute exposurestudies indicate that short-term exposures toelevated particulate air pollution are associ-ated with short-term changes in cardio-pulmonary health. These acute exposurestudies provide little information about howmuch life is shortened, how pollution affectslonger-term mortality rates, or pollution'spotential role in the process of inducingchronic disease that may or may not be lifethreatening. Chronic exposure studies evalu-ate health end points across communities orneighborhoods with different levels of averagepollution over longer time periods (usually 1year or more). Chronic exposure studiesattempt to evaluate the effects of low or mod-erate exposure that persists for long periods aswell as the cumulative effects of repeatedexposure to substantially elevated levels ofpollution. A brief summary of the results ofthe chronic exposure studies is provided inTable 3.
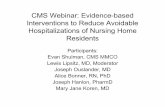
Mortality RatesSeveral population-based, cross-sectionalmortality studies have evaluated associationsbetween annual mortality rates and particu-late air pollution across U.S. metropolitanareas (Table 3). The basic conclusions fromthese population-based cross-sectional studieswere that mortality rates were associated withair pollution, and they were most stronglyassociated with fine or sulfate PM. Such asso-ciations are illustrated in Figure 1. Age, sex,and race-adjusted population-based mortalityrates for U.S. cities in 1980 are plotted overvarious indices of particulate air pollution[obtained from Lipfert et al. (158) and U.S.EPA (163)]. Although much apparently sto-chastic variability exists, adjusted mortalityrates are positively correlated with fine(PM2 5) and sulfate particles but not withTSPs. Multiple regression modeling tech-niques to evaluate cross-sectional differencesin air pollution and mortality and to controlfor other ecologic variables have been used.
Whereas the population-based cross-sectionalstudies from the United States dealt withtotal mortality, a study from the CzechRepublic focused on infant mortality (154).
Infant mortality, especially respiratory post-neonatal infant mortality, was strongly associ-ated with particulate air pollution. All ofthese population-based cross-sectional
Table 3. Summary of epidemiologic evidence of health effects of chronic exposure to particulate air pollution.
Health Observed associationsend points Basic study design with particulate pollution ReferencesMortality Population-based cross-sectional Higher mortality in areas with higher fine (153-160)rates analysis of mortality rates across particulate and/or sulfate pollution levels.
communities with different levels Pollution effect sensitive to modelof pollution. specification and choice of covariates
included in the analysis.Survival/life Cohort-based cross-sectional studies Increased risk of respiratory and cardio- (161-164)expectancy that link community-based air vascular mortality in adults, and respira-
pollution data with individual risk- tory and sudden infant death syndromefactor and survival data. mortality in infants, even after controlling
for individual differences in cigarettesmoking and various other risk factors.
Disease Cross-sectional studies of community Increased chronic cough, bronchitis, (165-170)air pollution with individual symptom/ and chest illness (but not asthma).disease data from surveys or collectedcohorts.
Lung Cross-sectional studies of community Particulate air pollution associated with (171-176)function ambient air pollution data with small but often statistically significant
individual lung function data from declines in various measures of lungnational surveys or collected cohorts. function in both children and adults.
Coa,C,
Co
Co
00
Co
E
cc
t
Cl:
0E
Co
o
U)
=
--
o°occ
0E
CO._
1,000 -
950 -
900 -
850 -
800 -
750 -
700 -
650 -
600 -
1,000 -
950 -
900 -
850 -
800-
750.
700-
650 -
600 -
1,000 -
950 -
900-
850 -
800 -
750 -
700 -
650 -
600
0
0*
0
8 10 12 14 16 18 20 22 24 26 28 30 32 34
Median PM2.5 for approximately 1980
0
0 *a %
0
0
4 6 8 10 12 14 16 18 20 22 24
Mean sulfate for approximately 1980
1,000 -
950 -
900 -
850 -
800 -
750 -
700 -
650 -
600 -
0
*S..
00a
0 00 0
0.0 0
0
0000
10 12 14 16 18 20 22 24 26 28 30 32 34
Mean PM2.5 for approximately 1980
0
0
@0
0. 00* 0
15 30 45 60 75 90 105 120 135 150 165
Mean TSP for approximately 1980Figure 1. Age-, sex-, and race-adjusted population-based mortality rates in U.S. cities for 1980 plotted over variousindices of particulate air pollution.
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000
1...~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
1 1 ---1~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
715
-
POPE
Table 4. Comparisons of mortality risk ratios (and 95% confidence interval) for air pollution from the Harvard Six-Cities, ACS, and postneonatal infant mortality studies.Particulate air pollution (range of pollution)
AHSMOG AHSMOGSix-Cities ACS ACS Infant (males) (females)
Cause of death (18.6 pg/M3 PM25) (24.5 pg/M3 PM25) (19.9 pg/M3 S04) (56.9 pg/M3 PM10) (24.1 pg/M3 PM10) (24.1 pg/M3 PM1O)All 1.26 (1.08-1.47) 1.17 (1.09-1.26) 1.15 (1.09-1.22) 1.25 (1.12-1.47) 1.11 (0.98-1.26) 0.94(0.84-1.04)Cardiopulmonary 1.37 (1.11-1.68) 1.31(1.17-1.46) 1.26 (1.16-1.37) 1.10 (0.94-1.30) 0.92 (0.80-1.05)Respiratory mentioneda - 1.23 (0.94-1.61) 1.10 (0.86-1.40)SIDS, NBW 1.91 (1.46-2.44)Lung cancer 1.37 (0.81-2.31) 1.03 (0.80-1.33) 1.36 (1.11-1.66) 3.36 (1.57-7.19) 1.33 (0.60-2.96)All others 1.01 (0.79-1.30) 1.07 (0.92-1.24) 1.01 (0.92-1.11) 1 00b (0.94-1.06)Abbreviations: NBW, normal birth weight; PM, particulate matter; SIDS, sudden infant death syndrome.'Any mention on the death certificate of nonmalignant respiratory disease as an underlying or contributing cause of death. hNBW.
mortality studies have severe limitations andhave been discounted for several reasons. Anoverriding concern is that they cannotdirectly control for individual differences inother important risk factors includingcigarette smoking.
SurivaL ExpectncySeveral cohort-based mortality studies haveevaluated effects of long-term pollution expo-sure. The first of these studies, often referredto as the Harvard Six-Cities study (162),involved a 14- to 16-year prospectivefollow-up of more than 8,000 adults living insix U.S. cities. It controlled for individual dif-ferences in age, sex, cigarette smoking, educa-tion levels, body mass index, and other riskfactors. Cardiopulmonary mortality was sig-nificantly associated with mean sulfate andfine particulate concentrations over the yearsof the study period.A second study, referred to as the ACS
study, linked individual risk factor data fromthe American Cancer Society, CancerPrevention Study II (CPS-II) with nationalambient air pollution data (163). The analy-sis used data for more than 500,000 personswho lived in up to 151 different U.S. metro-politan areas and who were followedprospectively from 1982 through 1989. Itcontrolled for individual differences in age,sex, race, cigarette smoking, and other riskfactors, and evaluated the association ofadjusted mortality with two indices of long-term exposure to combustion-source particu-late air pollution, mean sulfate, and medianfine particles. Both indices of combustion-source particulate air pollution were associ-ated with overall mortality and especiallywith cardiopulmonary mortality.
In both the Harvard Six-Cities study (162)and the ACS study (163), the positive associa-tion between combustion-related air pollutionand cardiopulmonary mortality was dominatedby cardiovascular disease deaths. However,because of concerns about cause-of-death cross-coding on the death certificates, respiratory andcardiovascular deaths were grouped togetherand analyzed as cardiopulmonary deaths.
A study of postneonatal infant mortalityin the U.S.-linked National Center forHealth Statistics birth and death records forinfants born between 1989 and 1991 withPM1o data from the U.S. EPA's AerometricDatabase (164). The full data set includedapproximately four million infants in 86 U.S.metropolitan areas. Because all infants in thestudy had PM1o exposure for at least part of2 months, the analysis compared postneona-tal infant mortality across different levels ofambient PMto concentrations during the2 months following birth. The analysis con-trolled for individual differences in maternalrace, maternal education, marital status,month of birth, maternal smoking duringpregnancy, and ambient temperatures.Particulate pollution exposure was associatedwith postneonatal infant mortality for allcauses, respiratory causes, and sudden infantdeath syndrome.
A final cohort study, known asthe Adventist Health Study of Smog(AHSMOG), related air pollution to1977-1992 mortality in more than 6,000nonsmoking adults living in California, pre-dominantly from the three metropolitan areasof San Diego, Los Angeles, and San Francisco(161). All natural cause mortalities, non-malignant respiratory mortalities, and lungcancer mortalities were significantly associ-ated with ambient PM1o concentrations inmales, but not in females. Cardiopulmonarydisease mortality was not significantly associ-ated with PM1o in either males or females.Unfortunately, this study did not have directmeasures of PM2.5 but relied on TSP andPM1o data. Furthermore, the cohort was rela-tively small and was predominantly from onlythree metropolitan areas, San Diego, LosAngeles, and San Francisco.
Comparisons of mortality risk ratios forair pollution from the Six-Cities, ACS, infantmortality, and AHSMOG studies are pre-sented in Table 4. The estimated overallexcess risk from the infant mortality study issimilar to those estimated for adults in theHarvard Six-Cities and ACS studies, eventhough the time frame of exposure for the
infants was clearly far shorter than for theadults. This observation suggests that the rele-vant time frame of exposure is short (a fewmonths vs years) and/or that infants are atgreater risk for exposure to air pollution.
Disea Lung FunctionThere have also been several studies evaluatingassociations between chronic exposure andparticulate air pollution and respiratorysymptoms and disease or lung function(Table 3). The effects of air pollution on res-piratory disease or symptoms were often esti-mated while adjusting for individualdifferences in various other risk factors.Significant associations between particulateair pollution and various respiratory symp-toms were often observed. Chronic cough,bronchitis, and chest illness (but not asthma)were associated with various measures of par-ticulate air pollution. Studies that evaluatedeffects of air pollution on lung functionadjusted for individual differences in age,race, sex, height, and weight, and controlledfor smoking or restricted the analysis tonever-smokers. These studies observed smallassociations between decreased lung functionand particulate air pollution that were oftenstatistically significant.
Stylizd Summary ofEffectsThe overall epidemiologic evidence isenhanced if adverse effects of exposure arereproducibly observed by different investiga-tors in different settings. That is, there shouldbe consistency of effects across independentstudies. The evidence is further strengthenedby a coherence of effects observed across acascade of related health outcomes. Figure 2presents a stylized summary of effect esti-mates of exposure to particulate air pollution.The effect estimates are not precise becausedifferent studies used various measures of pol-lution, different models, and differentlydefined health end points. In addition, therecent rapid growth of the literature in thisarea makes effect estimates a moving target.Figure 2, therefore, should be consideredstylized but illustrative. The estimates for the
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000716
-
FINE PARTICULATE AIR POLLUTION AND HUMAN HEALTH
acute time-series studies are revised fromrecent reviews (6,8). The effect estimates forthe cross-sectional and cohort studies arebased on selected studies that are reasonablyrepresentative. The population-based mortal-ity estimate is based on results presented byEvans et al. (155), Lipfert (157), Lipfert et al.(158), and Ozkaynak and Thurston (160).The cohort-based mortality estimates arebased on Dockery et al. (162), Pope et al.(163), and Woodruff et al. (164), respec-tively. Bronchitis, children's lung function,and adult lung function estimates are basedon results reported by Dockery et al. (167),Raizenne et al. (173), and Ackermann-Liebrich et al. (171), respectively.
As illustrated in Figure 2, a remarkablecascade of cardiopulmonary health end pointshas been observed. These include death fromcardiac and pulmonary disease, emergencyroom and physician office visits for asthmaand other cardiorespiratory disorders, hospi-tal admissions for cardiopulmonary disease,increased reported respiratory symptoms,and decreased measured lung function. Theoverall epidemiologic evidence indicates aprobable link between fine particulate airpollution and adverse effects on cardio-pulmonary health. Nevertheless, thereremains uncertainty about the role of chem-istry versus size of the particles, the role ofcopollutants, and the use of central-site airquality monitoring to estimate the effects onindividuals who spend most of their timeindoors. In addition, there remains substan-tial uncertainty with regard to the biologicplausibility of these associations.
What Are the BiologicMechanisms?Our knowledge about the underlying biologicmechanisms remains limited and requiresmuch additional study. The results of the epi-demiology outlined above, however, providea pattern of effects that may be biologicallygermane. Biologic plausibility is enhanced bythe observation of a coherent cascade ofcardiopulmonary health effects and by thefact that noncardiopulmonary health endpoints are not typically associated with thepollution. In addition, as summarized inTable 5, very recent epidemiologic studieshave attempted to look at specific physiologicend points, in addition to lung function, thatmay be part of the pathophysiologic pathwaylinking cardiopulmonary mortality andparticulate air pollution.
One hypothesized general pathwayincludes pollution-induced lung damage(potentially including oxidative lung damageand inflammation), declines in lung function,respiratory distress, and cardiovascular diseasepotentially related to hypoxemia (177).Evidence of pollution-related inflammation
10
9
CDc
0)
C.)4-
a_0)L)
7-
6
5
4
3
2
0
Effects of acute exposure
Mortality Hospitalizations/ Symptomsother health care
tiflrTTTt slbLung
functionv_
Effects of chronic exposure
Disease
Mortality risk/survival T
*b Lung function
t¶ *Adults
Figure 2. Stylized summary of observed health effects, presented as approximate percent changes in health endpoints per 5 pg/m3 increase in PM2.5. Abbreviations: COPD, chronic obstructive pulmonary disease; FVC, forced vitalcapacity; PEF, peak expiratory flow. Asterisk (*) indicates estimate based on very limited or inconsistent evidence.
Table 5. Brief summary of several recent epidemiologic studies of specific physiologic end points.
Physiologic Observed associations withend points elevated particulate matter exposure Authors/year (reference)
Lung function Small declines in lung function; large risk of substantial decrements Hoek et al. 1999 (125)Hypoxemia No clear associations with blood oxygen saturation Pope et al. 1999 1177)Plasma viscosity Increased risk of elevated blood plasma viscosity Peters et al. 1997 1178)Heart rate Increased mean HR and odds of a substantially elevated HR. Pope et al. 1999 (177)
Peters et al.1999 (179)Heart rate Changes in cardiac rhythm. Decrease in overall HRV. Liao et al. 1999(180)variability Pope et al. 1999)181)
Gold et al. 2000 (182)Pulmonary Elevated white blood cell counts, band cells expressed as percentage Tan et al. 2000 (183)inflammation of polymorphonuclear leukocytes, platelets, lymphocytes, and eosinophils Salvi et al. 1999 (184)a'This is actually a controlled human exposure study.
has been observed (183-185) and, as indicatedabove, several studies have reported declinesin lung function associated with elevated par-ticulate pollution exposures. However, astudy of potential PM-related hypoxemia didnot observe declines in blood oxygen satura-tion associated with elevated exposures toparticulate air pollution (177).
Alternatively, the autonomic nervoussystem may play an important role in thepathophysiologic pathway between particu-late exposure and cardiopulmonary disease.Seaton et al. (186) hypothesized that fineparticulate air pollution may provoke alveolarinflammation, resulting in the release ofpotentially harmful cytokines and increasedblood coagulability. Autonomic nervoussystem-activated changes in blood viscosity,heart rate (HR), and heart rate variability(HRV) may increase the likelihood of cardiacdeath (187). A few recent epidemiologicstudies (177-183) have evaluated such auto-nomic nervous system-related physiologic
measures and air pollution, although theyhave been extremely limited and mostlyexploratory pilot studies.
Peters et al. (178) evaluated blood plasmaviscosity from a random sample of men andwomen living in Augsburg, Germany, duringthe winter of 1984-1985. Between January 4and 7, 1985, there was a pollution episodewith marked increases in sulfur oxide andparticulate pollution concentrations. Duringthis episode a significant increase in the riskof elevated plasma viscosity was observed.The odds ratios (and 95% confidence inter-vals [CIs]) for plasma viscosity were above the95th percentile of the sample distribution;they were 3.6 (1.6-8.1) and 2.3 (1.0-5.3) formen and women, respectively.
A daily time-series panel study of elderlysubjects with repeated measures of bloodoxygenation did not observe pollution-relatedhypoxemia but did observe that elevated par-ticulate air pollution levels were associatedwith increased pulse rate (177). A 100-mg/m3
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 717
-
POPE
increase in PM1o on the previous 1-5 dayswas associated with an average increase in thepulse rate of 0.8 beats/min and a 29% and95% increase in the odds of the pulse ratebeing elevated by 5 or 10 beats/min, respec-tively.
In a related study (181), repeated 24-hrambulatory electrocardiograph (ECG) moni-toring was conducted on seven subjects for atotal of 29 days during episodes of high pol-lution and during periods of relatively lowpollution. HR was positively associated withparticulate air pollution. Additionally, beat-to-beat (R-R) HRV was analyzed to assesscardiac autonomic control. Particulate airpollution was associated with changes inHRV including: reduced 24-hr SDNN (thestandard deviation of all normal R-R inter-vals and an estimate of overall HRV);reduced SDANN (standard deviation of theaverages of R-R intervals in all 5-min seg-ments of the 24-hr ECG recording and anestimate of long-term components of HRV);and increased r-MSSD (the square root ofthe mean of squared differences betweenadjacent R-R intervals and an estimate of theshort-term components of HRV). The asso-ciations between HRV and particulate pollu-tion persisted even after controlling for meanHR, suggesting a possible link between ele-vated exposure to PM and lower cardiacautonomic control.A prospective study ofHRV and mortality
in subjects with chronic heart failure wasrecently reported (187). Survival analysisconducted in this study included a CoxProportional Hazards regression model tocontrol for multiple risk factors. Based on thismodel the estimated risk ratio for a 41.2-msdecrease in SDNN (from 24-hr ambulatoryECG monitoring) was 1.62 (95% CI,1.16-2.44). As an interesting but highly spec-ulative look at plausibility, the 24-hr SDNNmortality relationship from this study can becombined with the decline in 24-hr SDNNassociated with PM1o from the above HRVstudy (181). The expected increase in mortal-ity risk can then be estimated and comparedwith the PM-related cardiovascular mortalityrisk directly estimated from the PM mortalityepidemiology studies. For example, the esti-mated decline in 24-hr SDNN associatedwith 100 pg/m3 PM1o was approximately18 ms (SE = 4.9). Using the coefficientsreported in these two studies (181,187), theestimated mortality risk ratio of an 18-msdecline in 24-hr SDNN can be calculated as1.23 (e[l8*(lnl.62)/4.2]). This risk ratio seemssomewhat plausible. It is larger than risk ratiosfor total or cardiovascular disease mortalitythat are generally estimated from daily time-series studies but smaller than risk ratios esti-mated from the prospective cohort mortalitystudies oflong-term chronic exposure.
Two additional studies have also recentlyevaluated associations between particulate airpollution and HRV. One of these studiesexplored daily changes in HRV associatedwith daily changes in fine particulate air pol-lution with a panel of elderly subjects livingin metropolitan Baltimore (180). Daily ECGmonitoring was conducted with resting,supine, 6-min R-R interval data collectedeach day. The second study involved subjects53-87 years of age living in Boston,Massachusetts (182). Weekly ECG monitor-ing was conducted using ambulatory (Holter)monitors continuously for 25 min, including5 min of rest, 5 min of standing, 5 min ofoutdoor exercise, 5 min of recovery, and 20cycles of slow breathing. Although the pollu-tion levels were relatively low during thestudy periods in both of these studies, lowerHRV was associated with elevated concentra-tions of fine particulate pollution, and theassociation was stronger for subjects withpre-existing cardiovascular conditions.
In the three currently available studiesof particulate air pollution and HRV(180-182), a negative association with par-ticulate exposure and overall HRV wasobserved. The results, however, are notentirely consistent, especially with measuresof the short-term (or high-frequency) compo-nents of HRV. To what degree these incon-sistencies across studies can be explained bydifferences in ECG monitoring time frames,make-up of subjects, differences in pollutionlevels, or other differences needs to beexplored.A study of rabbits found that alveolar
macrophage phagocytosis of small carbon par-ticles < 10 pm in aerodynamic diameterresulted in the release of cytokines that led tostimulation of the bone marrow to releaseyoung polymorphonuclear leukocytes(PMNs). The authors postulated that thesePMNs caused the health effects noted in epi-demiologic studies (188). A follow-up studywas conducted of an air pollution episode dueto fires in Southeast Asia in 1997 (183). Bloodsamples from 30 healthy male military person-nel were collected during and after the episode.The pollution episode was associated with sig-nificant increases in total white blood cellcounts, band cells expressed as a percentage ofPMNs, platelets, lymphocytes, and eosino-phils. The authors suggest that these resultsimply a systemic response to PM-related pul-monary inflammation. A recent controlledhuman study of exposure to diesel exhaust alsoobserved a well-defined and marked systemicand pulmonary inflammatory response inhealthy human volunteers (184).
The physiologic relevance of no PM-related hypoxemia but PM-related changes inblood plasma viscosity, HR, HRV, and pul-monary inflammation is not well understood.
Recent animal studies have observed some-what complementary results (188-194), butthe epidemiologic observations are prelimi-nary and based on only a few studies, most ofwhich were exploratory pilot studies. Thesechanges may reflect PM-induced pulmonaryinflammation, cytokine release, and alteredcardiac autonomic function as part of thepathophysiologic mechanisms or pathwayslinking PM and cardiovascular mortality. Ingeneral, it is speculated that interactionsbetween inflammation, abnormal hemostaticfunction, and altered cardiac rhythm mayplay an important role in the pathogenesis ofcardiopulmonary diseases related to air pollu-tion. An adequate understanding of theserelationships clearly requires further research.
Who's at Risk?The question of who is at risk or who issusceptible to adverse health effects of finePM pollution does not have an easy answer.It seems evident that the elderly, young chil-dren, and persons with chronic cardio-pulmonary disease, influenza, and asthma aremost likely to be susceptible. However, thisanswer is far too simplistic. For example,assume a large population of nonsmokers.Require all in the population to smoke a packof cigarettes for a day and then stop. Whowill be susceptible to this relatively short-termexposure to cigarette smoking? Mortality andserious morbidity effects would most likelyaffect the very old, young, and those withasthma or chronic cardiopulmonary disease.This does not mean that others are un-affected. For healthy, middle-aged adults, theeffects are unlikely to be immediately lifethreatening, but short-term adverse effectssuch as coughing, throat and eye irritation, oreven mild or moderate cigarette smoke-induced pulmonary inflammation may beexperienced. Further suppose smoking doesnot stop after 1 day but continues throughoutthe lives of all in the population. Now who issusceptible to exposure to cigarette smoke?Over a lifetime, the chronic exposure has thepotential to eventually effect all. Although theexposures and effects for active cigarettesmoking are much larger, cigarette smokinghas been associated with a spectrum of car-diopulmonary diseases similar to those associ-ated with fine PM. Interestingly, a decrease inHR and an increase in HRV have also beenobserved following smoking cessation (195).Clearly, the answer to the question of who issusceptible is not simple but is dependent onthe health effects being evaluated and thelevel and length of exposure.
At Risk fiom Short-Term,Acute ExposureA summary of who may be susceptible tovarious adverse health effects from PM
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000718
-
FINE PARTICULATE AIR POLLUTION AND HUMAN HEALTH
exposure and overall health relevance ispresented in Table 6. With respect to acutelyelevated exposures, reflected by day-to-daychanges in PM, those susceptible to dying arethe elderly, the very young, and persons withchronic cardiopulmonary disease, influenza,or asthma. During the London episode of1952, for example, approximately 80-90% ofthe excess deaths were in adults with respira-tory and/or cardiovascular disease that wasgenerally chronic in nature. There was also anapproximate doubling of deaths in childrenless than 1 year of age (20). As summarizedin Table 2, more recent daily time-seriesstudies also observe that most of the excessmortality from PM exposure is from respira-tory and cardiovascular disease deaths.
How much life shortening is due toacutely elevated levels of PM and how muchof the mortality is due to short-term mortalitydisplacement (harvesting) remains uncertain.If the increased mortality is only in the mostfrail persons with little remaining lifeexpectancy, then death may be advanced byonly a few days or weeks. However, recentresearch using data from Philadelphia,Pennsylvania observed that the increase inmortality was inconsistent with only short-term mortality displacement and suggests thatmortality for many may be substantiallyadvanced (196). These results also suggestthat those who are susceptible to increasedrisk of mortality from acutely elevated PMmay include more than just the most old andfrail who are already very near death.
On any given day, the number dying dueto PM exposure is extremely small. Based onthe 1996 average death rate for the UnitedStates (8.8/1000/year) and the summary esti-mates presented in Table 2, a 50-,ug/m3increase in PM2.5 would result in an averageof only 1.7 deaths per day per one million
people (compared to an expected rate ofapproximately 24/day). This minimal excessdeaths per day reflects the fact that theincreased risk of mortality due to acutely ele-vated PM exposure is small, and on any givenday there may only be a very small fraction ofthe population at serious risk of dying due tothis acute exposure.
As summarized in Table 6, the number ofthose susceptible to being hospitalizedbecause of acute PM exposure is probablyalso quite limited and similar to the numberof those at risk of dying. However, the num-ber of those susceptible to less serious healtheffects such as increased respiratory symp-toms, decreased lung function, or other phys-iologic changes may be quite broad. For mostpeople, these effects are likely small, transient,and maybe even unnoticed. For a few, thedecline in lung function may be clinically rel-evant (125), or the effects may be result inshort-term absence from work (131,132) orschool (141).
At Risk from Long-TermChronic posureLong-term, repeated PM exposure has beenassociated with increased population-basedmortality rates (155-160) as well as increasedrisk of mortality in broad-based cohorts orsamples of adults (162,163) and children(164) (Table 4). Chronic exposure studies ofPM suggest rather broad susceptibility tocumulative effects of long-term repeatedexposure. There is no evidence that increasedmortality risk is unique to any well-definedsusceptible subgroup. All who are chronicallyexposed may ultimately be affected. However,because the relative risk is small, the long-term cumulative effects are most likely to beobserved in older age groups with relativelyhigher baseline risks of mortality.
To illustrate the potential cumulativemortality effects of PM, survival curves and lifeexpectancies have been estimated under six dif-ferent scenarios illustrated in Figure 3. The firstcurve is a baseline survival curve based on pro-jected U.S. life tables prepared by the Office ofthe Chief Actuary in the Social SecurityAdministration and obtained from the BerkeleyMortality Database (197). Although a survivalcurve for never-smokers and for persons notexposed to urban air pollution was not directlycalculated, this projected baseline curve is usedto represent a reasonable baseline estimate forthe total U.S. population. The life expectancyof this baseline curve is equal to 76.4 years.
The second, third, and fourth survivalcurves are calculated from the baseline curveassuming an additional relative risk of mortal-ity from PM exposure equal to 1.25. This isapproximately the relative risk estimated inboth the Harvard Six-Cities study (162) andthe postneonatal infant mortality study (164)for the relevant range of PM air pollutionthat exists in U.S. urban areas (Table 4). Theonly difference between the second, third,and fourth curves is the age at which peoplebegin to be susceptible to the effects of pollu-tion. Curves two, three, and four assume thatsusceptibility begins at age 45 years, age 1year, and at birth, respectively. As can be seenin Figure 3, these three survival curves appearto be nearly identical. The close concurrencebetween these three curves is because thebaseline mortality risk for infants, children,and young adults is so low compared to thebaseline mortality risks for older adults. Theestimated life expectancy for curves two,three, and four equal 73.9, 73.5, and 73.4years, respectively. This suggests an averageloss of life expectancy equal to 2.5, 2.9, and3.1 years, respectively. Obviously, earlieronset ages of susceptibility result in greater
Table 6. Summary of who's susceptible to adverse health effects from PM exposure and overall health relevance.
Health effects Who's susceptible? Overall health relevanceAcute exposure
Mortality Elderly, infants, persons with chronic Obviously relevant. How much life shortening is involved and how muchcardiopulmonary disease, influenza, or asthma is due to short-term mortality displacement (harvesting) is uncertain.
Hospitalization/ other Elderly, infants, persons with chronic cardiopulmonary Reflects substantive health impacts in terms of illness, discomfort,health care visits disease, pneumonia, influenza, or asthma treatment costs, work or school time lost, etc.
Increased respiratory Most consistently observed in people with asthma Mostly transient effects with minimal overall health consequence,symptoms and children although for a few there may be short-term absence from work or
school due to illness.Decreased lung function Observed in both children and adults For most, effects seem to be small and transient. For a few, lung function
losses may be clinically relevant.Plasma viscosity, heart rate, Observed in both healthy and unhealthy adults. No Effects seem to be small and transient. Overall health relevanceheart rate variability, studies of children is unclear, but may be part of pathophysiologic pathway linkingpulmonary inflammation PM with cardiopulmonary mortality.
Chronic exposureIncreased mortality rates, Observed in broad-based cohorts or samples of Long-term, repeated exposure appears to increase the risk of cardio-reduced survival times, chronic adults and children (including infants). All pulmonary disease and mortality. May result in lower lung function.cardiopulmonary disease, chronically exposed potentially are affected Population average loss of life expectancy in highly polluted citiesreduced lung function may be as much as a few years.
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 719
-
POPE
100
90 l
80
70
60 -
-. o U40-
340-
-- - e - Baseline survival curve; life expectancy = 76.4 years20 - 0 - 1.25 RR from pollution; ages
-
FINE PARTICULATE AIR POLLUTION AND HUMAN HEALTH
Seoul and Ulsan, Korea. Environ Health Perspect 107:149-154(1999).
35. loomis D, Castillejos M, Gold DR, McDonnell W, Borja-AburtoVH. Air pollution and infant mortality in Mexico City.Epidemiology 10:118-123 (1999).
36. Michelozzi P, Forastiere F, Fusco D, Perucci CA, Ostro B, AnconaC, Pallotti G. Air pollution and daily mortality in Rome, Italy.Occup Environ Med 55:605-610 (1998).
37. Moolgavkar SH, Leubeck EG, Hall TA, Anderson EL. Air pollutionand daily mortality in Philadelphia. Epidemiology 6:476-484(1995).
38. Moolgavkar SH, Leubeck EG, Hall TA, Anderson EL. Particulateair pollution, sulfur dioxide and daily mortality: a reanalysis ofthe Steubenville data. Inhal Toxicol 7:35-4 (1995).
39. Morgan G, Corbett S, Wlodarczyk J, Lewis P. Air pollution anddaily mortality in Sydney, Australia, 1989 through 1993. Am JPublic Health 88:759-764 (1998).
40. Ostro B. Fine particulate air pollution and mortality in twoSouthern California counties. Environ Res 70:98-104 (1995).
41. Ostro BD, Sanchez JM, Aranda C, Eskeland GS. Air pollutionand mortality: results from a study of Santiago, Chile. J ExposAnal Environ Epidemiol 6:97-114 (1996).
42. Ponka A, Savela M, Virtanen M. Mortality and air pollution inHelsinki. Arch Environ Health 53:281-286 (1998).
43. Pope CA Ill, Kalkstein LS. Synoptic weather modeling and esti-mates of the exposure-response relationship between dailymortality and particulate air pollution. Environ Health Perspect104:414-420 (1996).
44. Pope CA Ill, Schwartz J, Ransom MR. Daily mortality and PM 10pollution in Utah Valley. Arch Environ Health 47:211-217(1992).
45. Rahlenbeck SI, Kahl H. Air pollution and mortality in East Berlinduring the winters of 1981-1989. Int J Epidemiol 25:1220-1226(1996).
46. Saldiva PHN, Pope CA Ill, Schwartz J, Dockery OW, LichtenfelsAJ, Salge JM, Barone I, Bohm GM. Air pollution and mortalityin elderly people: a time series study in Sao Paulo, Brazil. ArchEnviron Health 50:159-163 (1995).
47. Samet JM, Zeger SL, Berhane K. The association of mortalityand particulate air pollution. In: Particulate Air Pollution andDaily Mortality: Replication and Validation of Selected Studies.The Phase Report of the Particle Epidemiology EvaluationProject. Cambridge, MA:Health Effects Institute, 1995.
48. Samet JM, Zeger SL, Kelsall JE, Xu J, Kalkstein LS. Doesweather confound or modify the association of particulate airpollution with mortality? An analysis of the Philadelphia data1973-1980. Environ Res 77:9-19 (1998).
49. Schwartz J. Particulate air pollution and daily mortality inDetroit. Environ Res 56:204-213 (1991).
50. Schwartz J. Air pollution and daily mortality in Birmingham,Alabama. Am J Epidemiol 137:1136-1147 (1993).
51. Schwartz J. Total suspended particulate matter and daily mor-tality in Cincinnati, Ohio. Environ Health Perspect 102:186-189(1994).
52. Schwartz J. What are people dying of on high air pollutiondays? Environ Res 64:26-35 (1994).
53. Schwartz J, Dockery DW. Particulate air pollution and daily mor-tality in Steubenville, Ohio. Am J Epidemiol 135:12-19 (1992).
54. Schwartz J, Dockery DW. Increased mortality in Philadelphiaassociated with daily air pollution concentrations. Am RevRespir Dis 145:600-604 (1992).
55. Schwartz J, Dockery DW, Neas LM. Is daily mortality associ-ated specifically with fine particles? J Air Waste Manage Assoc46:927-939 (1996).
56. Schwartz J, Marcus A. Mortality and air pollution in London: atime series analysis. Am J Epidemiol 131:185-194 (1990).
57. Simpson RW, Williams G, Petroeschevsky A, Morgan G,Rutherford S. Associations between outdoor air pollution anddaily mortality in Brisbane, Australia. Arch Environ Health52:442-454 (1997).
58. Spix C, Heinrich J, Dockery D, Schwartz J, Volksch G,Schwinkowski K, Collen C, Wichmann HE. Air pollution anddaily mortality in Erfurt, East Germany, 1980-1989. EnvironHealth Perspect 101:518-526 (1993).
59. Spix C, Wichmann HE. Daily mortality and air pollutants: find-ings from KoIn, Germany. J Epidemiol Comm Health 50(suppi1 ):S52-S58 (1996).
60. Sunyer J, Castellsague J, Saez M, Tobias A, Anto JM. Air pollu-tion and mortality in Barcelona. J Epidemiol Comm Health50(suppl 1):S76-S80 (1996).
61. Thurston GD, Ito K, Lippmann M, Hayes C. Reexamination ofLondon, England, mortality in relation to exposure to acidicaerosols during 1963-1 972 winters. Environ Health Perspect79:73-82 (1989).
62. Touloumi G, Pockock SJ, Katsouyanni K, Trichopoulos D.Short-term effects of air pollution on daily mortality in Athens:a time-series analysis. lnt J Epidemiol 23:957-961 (1994).
63. Verhoeff AP, Hoek G, Schwartz J, van Wijnen JH. Air pollutionand daily mortality in Amsterdam. Epidemiology 7:225-230(1996).
64. Wietlisbach V, Pope CA Ill, Ackermann-Liebrich U. Air pollutionand daily mortality in three Swiss urban areas. SozPraventivmed 41:107-115 (1996).
65. Xu X, Gao J, Dockery DW, Chen Y. Air pollution and daily mor-tality in residential areas of Beijing, China. Arch Environ Health49:216-222 (1994).
66. Zmirou D, Schwartz J, Saez M, Zanobetti A, Wojtyniak B,Touloumi G, Spix C, Ponce de Leon AA, Le Moullec Y,Bacharova L, et al. Time-series analysis of air pollution andcause-specific mortality. Epidemiology 9:495-503 (1998).
67. Anderson HR, Spix C, Medina S, Schouten JP, Castellsague J,Rossi G, Zmirou D, Touloumi G, Wojtyniak B, Ponka A, et al. Airpollution and daily admissions for chronic obstructive pul-monary disease in 6 European cities: results from the APHEAproject. Eur RespirJ 10:1064-1071 (1997).
68. Atkinson RW, Anderson HR, Strachan DP, Bland JM, BremnerSA, Ponce de Leon A. Short-term associations between outdoorair pollution and visits to accident and emergency departmentsin London for respiratory complaints. Eur Respir J 13:257-265(1999).
69. Bates DV, Baker-Anderson M, Sizto R. Asthma attack periodic-ity: a study of hospital emergency visits in Vancouver. EnvironRes 51:51-70 (1990).
70. Bates DV, Sizto R. The Ontario air pollution study: identificationof the causative agent. Environ Health Perspect 79:69-72(1989).
71. Burnett RT, Brook JR, Yung WT, Dales RE, Krewski D.Association between ozone and hospitalization for respiratorydisease in 16 Canadian cities. Environ Res 72:24-31 (1997).
72. Burnett RT, Dales RE, Raizenne ME, Krewski D, Summers PW,Roberts GR, Raad-Young M, Dann T, Brook J. Effects of lowambient levels of ozone and sulfates on the frequency of respi-ratory admissions to Ontario hospitals. Environ Res 65:172-194(1994).
73. Burnett RT, Dales R, Krewski D, Vincent R, Dann T, Brook JR.Associations between ambient particulate sulfate and admis-sions to Ontario hospitals for cardiac and respiratory diseases.Am J Epidemiol 142:15-22 (1995).
74. Burnett RT, Smith-Doiron M, Stieb D, Cakmak S, Brook JR.Effects of particulate and gaseous air pollution on cardiorespi-ratory hospitalizations. Arch Environ Health 54:130-139 (1999).
75. Castellsague J, Sunyer J, Saez M, Anto JM. Short-term associ-ation between air pollution and emergency room visits forasthma in Barcelona. Thorax 50:1051-1056 (1995).
76. Choudhury AH, Gordian ME, Morris SS. Associations betweenrespiratory illness and PM10 air pollution. Arch Environ Health52:113-117 (1997).
77. Delfino RJ, Becklake MR, Hanley JA, Singh B. Estimation ofunmeasured particulate air pollution data for an epidemiologi-cal study of daily respiratory morbidity. Environ Res 67:20-38(1994).
78. Delfino RJ, Murphy-Moulton AM, Burnett RT, Brook JR,Becklake MR. Effects of air pollution on emergency room visitsfor respiratory illnesses in Montreal, Quebec. Am J Respir CritCare Med 155:568-576 (1997).
79. Gordian ME, Ozkaynak H, Xue J, Morris SS, Spengler JD.Particulate air pollution and respiratory disease in Anchorage,Alaska. Environ Health Perspect 104:290-297 (1996).
80. lipfert FW, Hammerstorm T. Temporal patterns in air pollutionand hospital admissions. Environ Res 59:374-399 (1992).
81. Lipsett M, Hurley S, Ostro B. Air pollution and emergency roomvisits for asthma in Santa Clara County, California. EnvironHealth Perspect 105:216-222 (1997).
82. Lutz LJ. Health effects of air pollution measured by outpatientvisits. J Fam Pract 16:307-313 (1983).
83. Moolgavkar SH, Luebeck EG, Anderson EL. Air pollution andhospital admissions for respiratory causes in Minneapolis-St.Paul and Birmingham. Epidemiology 8:364-370 (1997).
84. Morgan G, Corbett S, Wlodarczyk J. Air pollution and hospitaladmissions in Sydney, Australia, 1990 to 1994. Am J PublicHealth 88:1761-1766 (1998).
85. Ostro BD, Eskeland GS, Sanchez JM, Feyzioglu T. Air pollutionand health effects: a study of medical visits among children inSantiago, Chile. Environ Health Perspect 107:69-73 (1999).
86. Pantazopoulou A, Katsouyanni K, Kourea-Kremastinou J,Trichopoulos 0. Short-term effects of air pollution on hospitalemergency outpatient visits and admissions in the GreaterAthens, Greece area. Environ Res 69:31-36 (1995).
87. Poloniecki JD, Atkinson RW, Ponce de leon A, Anderson HR.Daily time series for cardiovascular hospital admissions andprevious day's air pollution in London, UK. Occup Environ Med54:535-540 (1997).
88. Ponce de Leon A, Anderson HR, Bland JM, Strachan DP, BowerJ. Effects of air pollution on daily hospital admissions for respi-ratory disease in London between 1987-88 and 1991-92. JEpidemiol Comm Health 50(suppl 1:S63-S70 (1996).
89. Ponka A. Asthma and low level air pollution in Helsinki. ArchEnviron Health 46:262-270 (1991).
90. Pope CA Ill. Respiratory disease associated with community airpollution and a steel mill, Utah Valley. Am J Public Health79:623-628 (1989).
91. Pope CA Ill. Respiratory hospital admissions associated withPM10 pollution in Utah, Salt Lake, and Cache Valleys. ArchEnviron Health 46:90-97 (1991).
92. Samet JM, Speizer FE, BishopY, Spengler JD, Ferris BG Jr. Therelationship between air pollution and emergency room visits inan industrial community. J Air Pollut Control Assoc 31:236-240(1981).
93. Schwartz J. Air pollution and hospital admissions for the elderlyin Birmingham, Alabama. Am J Epidemiol 139:589-598 (1994).
94. Schwartz J. Air pollution and hospital admissions for the elderlyin Detroit, Michigan. Am J Respir Crit Care Med 150:648-655(1994).
95. Schwartz J. PM10, ozone, and hospital admissions for theelderly in Minneapolis-St. Paul, Minnesota. Arch Environ Health49:366-373 (1994).
96. Schwartz J. Short term fluctuations in air pollution and hospitaladmissions of the elderly for respiratory diseases. Thorax50:531-538 (1995).
97. Schwartz J. Air pollution and hospital admissions for respira-tory disease. Epidemiology7:20-28 (1996).
98. Schwartz J. Air pollution and hospital admissions for cardiovas-cular disease in Tucson. Epidemiology 8:371-377 (1997).
99. Schwartz J. Air pollution and hospital admissions for heart dis-ease in eight U.S. counties. Epidemiology 10:17-22 (1999).
100. Schwartz J, Morris R. Air pollution and hospital admissions forcardiovascular disease in Detroit, Michigan. Am J Epidemiol142:23-35 (1995).
101. Schwartz J, Slater D, Larson TV, Pierson WE, Koenig JO.Particulate air pollution and hospital emergency room visits forasthma in Seattle. Am Rev Respir Dis 147:826-831 (1993).
102. Schwartz J, Spix C, Wichmann HE, Malin E. Air pollution andacute respiratory illness in five German communities. EnvironRes 56:1-14 (1991).
103. Sheppard L, Levy D, Norris G, Larson TV, Koenig JO. Effects ofambient air pollution on nonelderly asthma hospital admissionsin Seattle, Washington, 1987-1994. Epidemiology 10:23-30(1999).
104. Smith MA, Jalaludin B, Byles JE, Lim L, Leeder SR. Asthma pre-sentations to emergency departments in western Sydney duringthe January 1994 bushfires. Int J Epidemiol 25:1227-1236(1996).
105. Spix C, Anderson HR, Schwartz J, Vigotti MA, LeTertre A, VonkJM, Touloumi G, Balducci F, Piekarski T, Bacharova L, et al.Short-term effects of air pollution on hospital admissions ofrespiratory diseases in Europe: a quantitative summary ofAPHEA study results. Air pollution and health: a Europeanapproach. Arch Environ Health 53:54-64 (1998).
106. Sunyer J, Saez M, Murillo C, Castellsague J, Martinez F, AntoJM. Air pollution and emergency room admissions for chronicobstructive pulmonary disease: a 5 year study. Am J Epidemiol137:701-705 (1993).
107. Sunyer J, Anto J, Murillo C, Saez M. Effects of urban air pollu-tion on emergency room admissions for chronic obstructive pul-monary disease. Am J Epidemiol 134:277-286 (1991).
108. Tenias JM, Ballester F, Rivera ML. Association between hospi-tal emergency visits for asthma and air pollution in Valencia,Spain. Occup Environ Med 55:541-547 (1998).
109. Thurston GD, Ito K, Kinney PL, Lippmann M. A multi-year studyof air pollution and respiratory hospital admissions in threeNew York State metropolitan areas: results for 1988 and 1989summers. J Expos Anal Environ Epidemiol 2:429-450 (1992).
110. Thurston GD, Ito K, Hayes CG, Bates DV, Lippmann M.Respiratory hospital admissions and summertime haze air pollu-tion in Toronto, Ontario: consideration of the role of acidaerosols. Environ Res 65:271-290 (1994).
111. Wordley J, Walters S, Ayres JG. Short term variations in hospi-tal admissions and mortality and particulate air pollution. OccupEnviron Med 54:108-116 (1997).
112. Xu X, Dockery OW, Christiani DC, Li B, Huang H. Association ofair pollution with hospital outpatient visits in Beijing. ArchEnviron Health 50:214-220 (1995).
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 721
-
POPE
113. Xu X, Li B Huang H. Air pollution and unscheduled hospital out-patient and emergency room visits. Environ Health Perspect103:286-289 (1995).
114. Yang W, Jennison BL, Omaye ST. Cardiovascular disease hospi-talization and ambient levels of carbon monoxide. J ToxicolEnviron Health 55:185-196 (1998).
115. Boezen M, Schouten J, Rijcken B, Vonk J, Gerritsen J, van derZee S, Hoek G, Brunekreff B, Postma D. Peak expiratory flowvariability, bronchial responsiveness, and susceptibility to ambi-ent air pollution in adults. Am J Respir Crit Care Med158:1848-1854 (1998).
116. Braun-Fahrlander C, Ackermann-Liebrich U, Schwartz J,Gnehm HP, Rutishauser M, Wanner HU. Air pollution and res-piratory symptoms in preschool children. Am Rev Respir Dis145:42-47 (1992).
117. Brunekreef B, Kinney PL, Ware JH, Dockery DW, Speizer FE,Spengler JD, Ferris BG Jr. Sensitive subgroups and normal vari-ation in pulmonary function response to air pollution episodes.Environ Health Perspect 90:189-193 (1991).
118. Dassen W, Brunekreef B, Hoek G, Hofschreuder P, Staatsen B,deGroot H, Schoutan E, Biersteker K. Decline in children's pul-monary function during an air pollution episode. J Air PollutControl Assoc 36:1223-1227 (1986).
119. Dockery DW, Ware JH, Ferris BJ, Speizer FE, Cook NR,Herman SM. Change in pulmonary function in children associ-ated with air pollution episodes. J Air Pollut Control Assoc32:937-942 (1982).
120. Dusseldorp A, Kruize H, Brunekreef B, Hofschreuder P DeMeerG, Oudvorst AB. Associations of PM10 and airborne iron withrespiratory health of adults living near a steel factory. Am JRespir Crit Care Med 152:1932-1939 (1995).
121. Gold DR, Damokosh Al, Pope CA Ill, Dockery DW, McDonnellWF, Serrano P, Retama A, Castillejos M. Particulate and ozonepollutant effects on the respiratory function of children insouthwest Mexico City. Epidemiology 10:6-16 (1999).
122. Hoek G, Brunekreef B. Effects of low level winter air pollutionconcentrations on respiratory health of Dutch children. EnvironRes 64:136-150 (1994).
123. Hoek G, Brunekreef B. Effect of photochemical air pollution onacute respiratory symptoms in children. Am J Respir Crit CareMed 151:27-32 (1995).
124. Hoek G, Brunekreef B. Acute effects of a winter air pollutionepisode on pulmonary function and respiratory symptoms ofchildren. Arch Environ Health 48:328-335 (1993).
125. Hoek G, Dockery DW, Pope CA Ill, Neas L, Roemer W,Brunekreff B. Association between PM10 and decrements inpeak expiratory flow rates in children: reanalysis of data fromfive panel studies. Eur RespirJ 11:1307-1311 (1998).
126. Johnson KG, Gideon RA, Loftsgaarden D0. Montana air pollutionstudy: children's health effects. J Off Stat 5:391-408 (1990).
127. Johnson KG, Loftsgaarden DO, Gideon RA. The effects of Mt.St. Helens volcanic ash on the pulmonary function of 120 ele-mentary school children. Am Rev Respir Dis 126:1066-1069(1982).
128. Koenig JQ, Larson TV, Hanley OS, Rebolledo V, Dumler K,Checkoway H, Wang SZ, Lin D, Pierson WE. Pulmonary functionchanges in children associated with fine particulate matter.Environ Res 63:26-38 (1993).
129. Neas LM, Dockery DW, Koutrakis P, Tollerud DJ, Speizer FE.The association of ambient air pollution with twice daily peakexpiratory flow rate measurements in children. Am J Epidemiol141:111-122 (1995).
130. Neas LM, Dockery DW, Burge H, Koutrakis P, Speizer FE.Fungus spores, air pollutants, and other determinants of peakexpiratory flow rate in children. Am J Epidemiol 143:797-807(1996).
131. Ostro BD. Associations between morbidity and alternative mea-sures of particulate matter. Risk Anal 10:421-427 (1990).
132. Ostro BD, Rothschild S. Air pollution and acute respiratory mor-bidity: an observational study of multiple pollutants. EnvironRes 50:238-247 (1989).
133. Ostro BD, Lipsett MJ, Wiener MB, Pharm D, Selner JC.Asthmatic responses to airborne acid aerosols. Am J PublicHealth 81:694-702 (1991).
134. Ostro BD, Lipsett MJ, Mann JK, Krupnick A, Harrington W. Airpollution and respiratory morbidity among adults in SouthernCalifornia. Am J Epidemiol 137:691-700 (1993).
135. Peters A, Dockery DW, Heinrich J, Wichmann HE. Short-termeffects of particulate air pollution on respiratory morbidity inasthmatic children. Eur Respir J 10:872-879 (1997).
136. Peters A, Dockery DW, Heinrich J, Wichmann HE. Medicationuse modifies the health effects of particulate sulfate air pollu-tion in children with asthma. Environ Health Perspect105:430-435(11997).
137. Peters A, Wichmann HE, Tuch T, Heinrich J, Heyder J.Respiratory effects are associated with the number of ultrafineparticles. Am J Respir Crit Care Med 155:1376-1383 (1997).
138. Pope CA Ill, Dockery DW, Spengler JD, Raizenne ME.Respiratory health and PM10 pollution: a daily time seriesanalysis. Am Rev Respir Dis 144:668-674 (1991).
139. Pope CA Ill, Dockery DW. Acute health effects of PM10 pollu-tion on symptomatic and asymptomatic children. Am Rev RespirDis 145:1123-1128 (1992).
140. Pope CA Ill, Kanner RE. Acute effects of PM10 pollution on pul-monary function of smokers with mild to moderate chronicobstructive pulmonary disease. Am Rev Respir Dis147:1336-1340(1993).
141. Ransom MR, Pope CA Ill. Elementary school absences andPM10 pollution in Utah Valley. Environ Res 58:204-219(1992).
142. Roemer W, Hoek G, Brunekreef B. Effect of ambient winter airpollution on respiratory health of children with chronic respira-tory symptoms. Am Rev Respir Dis 147:118-124(1993).
143. Roemer W, Hoek G, Brunekreff B, Haluszka J, Kalandidi A,Pekkanen J. Daily variations in air pollution and respiratory healthin a multicentre study: the PEACE project. Pollution effects onasthmatic children in Europe. Eur Respir J 12:1354-1361 (1998).
144. Romieu I, Meneses F, Ruiz S, Sienra JJ, Huerta J, White MC,Etzel RA. Effects of air pollution on the respiratory health ofasthmatic children living in Mexico City. Am J Respir Crit CareMed 154:300-307 (1996).
145. Scarlett JF, Abbott KJ, Peacock JL, Strachan DP, Anderson HR.Acute effects of summer air pollution on respiratory function inprimary school children in Southern England. Thorax51:1109-1114(1996).
146. Schwartz J, Dockery DW, Neas LM, Wypij D, Ware JH,Spengler JD, Koutrakis P, Speizer FE, Ferris BG. Acute effects ofsummer air pollution on respiratory symptom reporting in chil-dren. Am J Respir Crit Care Med 150:1234-1242 (1994).
147. Timonen KL, Pekkanen J. Air pollution and respiratory healthamong children with asthmatic or cough symptoms. Am JRespir Crit Care Med 156:546-552 (1997).
148. Vedal S, Petkau J, White R, Blair J. Acute effects of ambientinhalable particles in asthmatic and nonasthmatic children. AmJ Respir Crit Care Med 157:1034-1043 (1998).
149. Vedal S, Schenker MB, Munoz A, Samet JM, Batterman S,Speizer FE. Daily air pollution effects on children's respiratorysymptoms and peak expiratory flow. Am J Public Health77:694-698 (1987).
150. von Mutius E, Sherrill DL, Fritzsch C, Martinez FD, Lebowitz MD.Air pollution and upper respiratory symptoms in children fromEast Germany. Eur Respir J 8:723-728 (1995).
151. Whittemore AS, Korn EL. Asthma and air pollution in the LosAngeles area. Am J Public Health 70:687-696 (1980).
152. Xu X, Wang L. Synergistic effects of air pollution and personalsmoking on adult pulmonary function. Arch Environ Health53:44-53 (1998).
153. Archer VE. Air pollution and fatal lung disease in three Utahcounties. Arch Environ Health 45:325-334 (1990).
154. Bobak M, Leon DA. Air pollution and infant mortality in theCzech Republic, 1986-1988. Lancet 340:1010-1014 (1992).
155. Evans JS, Tosteson T, Kinney PL. Cross-sectional mortalitystudies and air pollution risk assessment. Environ Int 10:55-83(1984).
156. Lave LB, Seskin EP. Air pollution and human health. Science169:723-733 (1970).
157. Lipfert FW. Air pollution and mortality: specification searchesusing SMSA-based data. J Environ Econ Manage 11:208-243(1984).
158. Lipfert FW, Malone RG, Daum ML, Mendell NR, Yang CC. A sta-tistical study of the macroepidemiology of air pollution andtotal mortality. Rep no BNL 52112. Upton, NY:BrookhavenNational Laboratory, 1988.
159. Mendelsohn R, Orcutt G. An empirical analysis of air pollutiondose-response curves. J Environ Econ Manage 6:85-106 (1979).
160. Ozkaynak H, Thurston GD. Associations between 1980 U.S.mortality rates and altemate measures of airborne particle con-centrations. Risk Anal 7:449-461 (1987).
161. Abbey DE, Nishino N, McDonnell WF, Burchette RJ, KnutsenSF, Beeson WL, Yang JX. Long-term inhalable particles andother air pollutants related to mortality in nonsmokers. Am JResp Crit Care Med 159:373-382119991.
162. Dockery DW, Pope CA Ill, Xu X, Spengler JD, Ware JH, Fay ME,Ferris BG, Speizer FA. An association between air pollution andmortality in six U.S. cities. N EngI J Med 329:1753-1759 (1993).
163. Pope CA Ill, Thun MJ, Namboodiri MM, Dockery DW, Evans JS,Speizer FE, Heath JCW. Particulate air pollution as a predictorof mortality in a prospective study of U.S. adults. Am J RespirCrit Care Med 151:669-674 (1995).
164. Woodruff TJ, Grillo J, Schoendorf KC. The relationship betweenselected causes of postneonatal infant mortality and particulateair pollution in the United States. Environ Health Perspect105:608-612 (1997).
165. Abbey DE, Hwang BL, Burchette RL, Vancuren T, Mills PK.Estimated long-term ambient concentrations of PM10 anddevelopment of respiratory symptoms in a nonsmoking popula-tion. Arch Environ Health 50:139-152(1995).
166. Dockery DW, Cunningham J, Damokosh Al, Neas LM, SpenglerJD, Koutrakis P, Ware JH, Raizenne M, Speizer FE. Healtheffects of acid aerosols on North American children: respiratorysymptoms. Environ Health Perspect 104:500-505(1996).
167. Dockery DW, Speizer FE, Stram DO, Ware JH, Spengler JD,Ferris BG. Effects of inhalable particles on respiratory health ofchildren. Am Rev Respir Dis 139:587-594(1989).
168. Peters JM, Avol E, Navidi W, London SJ, Gauderman WJ,Lurmann F, Linn WS, Margolis H, Rappaport E, Gong H, et al. Astudy of twelve Southern California communities with differinglevels and types of air pollution. I: Prevalence of respiratorymorbidity. Am J Respir Crit Care Med 159:760-767 (1999).
169. Portney PR, Mullahy J. Urban air quality and chronic respiratorydisease. Regional Sci Urban Econ 20:407-418 (1990).
170. Schwartz J. Particulate air pollution and chronic respiratory dis-ease. Environ Res 62:7-13 (1993).
171. Ackermann-Liebrich U, Leuenberger P, Schwartz J, Schindler C,Monn C, Bolognini G, Bongard JP, Brandli 0, Domenighetti G,Elsasser S, et al. Lung function and long term exposure to airpollutants in Switzerland. Am J Respir Crit Care Med155:122-129 (1997).
172. Chestnut LG, Schwartz J, Savitz DA, Burchfiel CM. Pulmonaryfunction and ambient particulate matter: epidemiological evi-dence from NHANES I. Arch Environ Health 46:135-144(1991).
173. Raizenne ME, Neas LM, Damokosh Al, Dockery DW, SpenglerJD, Koutrakis P, Ware JH, Speizer FE. Health effects of acidaerosols on North American children: pulmonary function.Environ Health Perspect 104:506-514 (1996).
174. Schwartz J. Lung function and chronic exposure to air pollution:a cross-sectional analysis of NHANES II. Environ Res50:309-321 (1989).
175. Tashkin DP, Detels R, Simmons M, Liu H, Coulson AH, Sayre J,Rokaw S. The UCLA population studies of chronic obstructiverespiratory disease: Xl: Impact of air pollution and smoking onannual change in forced expiratory volume in one second. Am JRespir Crit Care Med 149:1209-1217(1994).
176. Wang B, Peng Z, Zhang X, Xu Y, Wang H, Allen G, Wang L, XuX. Particulate matter, sulfur dioxide, and pulmonary function innever-smoking adults in Chongqing, China. Int J Occup EnvironHealth 5:14-19 (1999).
177. Pope CA Ill, Dockery DW, Kanner RE, Villegas GM, Schwartz J.Oxygen saturation, pulse rate, and particulate air pollution: adaily time-series panel study. Am J Respir Crit Care Med159:365-372 (1999).
178. Peters A, Doring A, Wichmann HE, Koenig W. Increased plasmaviscosity during the 1985 air pollution episode: a link to mortal-ity? Lancet 349:1582-1587 (1997).
179. Peters A, Perz S, Doring A, Stieber J, Koenig W, Wichmann E.Increases in heart rate during an air pollution episode. Am JEpidemiol 150(10):1094-1098 (1999).
180. Liao D, Creason J, Shy C, Williams R, Watts R, Zweidinger R.Daily variation of particulate air pollution and poor cardiacautonomic control in the elderly. Environ Health Perspect107:521-525 (1999).
181. Pope CA Ill, Verrier RL, Lovett EG, Larson AC, Raizenne ME,Kanner RE, Schwartz J, Villegas GM, Gold DR, Dockery DW.Heart rate variability associated with particulate air pollution.Am Heart J 138:890-899 (1999).
182. Gold DR, Litonjua A, Schwartz J. Ambient air pollution andheart rate variability. Circulation 10(1l):1267-1273 (2000).
183. Tan WC, Qiu D, Liam BL, Ng TP, Lee SH, van Eeden S,D'Yachkova Y, Hogg JC. The human bone marrow response toacute air pollution caused by forest fires. Am J Respir Crit CareMed 161(4 pt 1):1213-1217 (2000).
184. Salvi S, Blomberg A, Rudell B, Kelly F, Sandstrom T, Holgate ST,Frew A. Acute inflammatory responses in the airways andperipheral blood after short-term exposure to diesel exhaust inhealthy human volunteers. Am J Respir Crit Care Med159:702-709(1999).
185. Souza MB, Saldiva PHN, Pope CA Ill, Capelozzi VL. Respiratorychanges due to long-term exposure to urban levels of air pollu-tion: a histopathologic study in humans. Chest 113:1312-1318(1998).
186. Seaton A, MacNee W, Donaldson K, Godden D. Particulate airpollution and acute health effects. Lancet 345:176-178 (1995).
722 Environmental Health Perspectives - Vol 108, Supplement 4 * August 2000
-
FINE PARTICULATE AIR POLLUTION AND HUMAN HEALTH
187. Nolan J, Batin PD, Andrews R. Prospective study of heart ratevariability and mortality in chronic heart failure. Circulation98:1510-1516 (1998).
188. Terashima T, Wiggs B, English D, Hogg JC, vanEeden SF.Phagocytosis of small carbon particles (PM10) by alveolarmacrophages stimulates the release of polymorphonuclearleukocytes from bone marrow. Am J Respir Crit Care Med155:1441-1447 (1997).
189. Becker S, Soukup JM, Gilmour Ml, Deviin RB. Stimulation ofhuman and rat alveolar macrophages by urban air particles:effects on oxidant radical generation and cytokine production.Toxicol AppI Pharmacol 141:637-648 (1996).
190. Dreher KL, Jaskot RH, Lehmann JR, Richards JH, McGee JK,Ghio AJ, Costa Dl. Soluable transition metals mediate residualoil fly ash induced acute lung injury. J Toxicol Environ Health
50:285-305(1997).191. Godleski JJ, Sioutas C, Verrier RL. Inhalation exposure of
canines to concentrated ambient air particles. Am J Respir DisCrit Care Med 155:A246 (1997).
192. Godleski JJ, Sioutas C, Katler M, Koutrakis P. Death frominhalation of concentrated air particles in animal models of pul-monary disease. Am J Respir Crit Care Med 153:A15 (1996).
193. Nadziejko C, Chen LC, Zelikoff IT, Gordon T. Hematological andcardiovascular effects of acute exposure to ambient particulatematter (PM). Am J Respir Crit Care Med 155:A24 (1997).
194. Watkinson WP, Campen MJ, Costa DL. Cardiac arrhythmiainduction after exposure to residual oil fly ash particles in arodent model of pulmonary hypertension. Toxicol Sci41:209-216 (1998).
195. Yotsukura M, Koide Y, Fujii K, Tomono Y, Katayama A, Ando H,
Suzuki J, Ishikawa K. Heart rate variability during the firstmonth of smoking cessation. Am Heart J 135:1004-1009(1998).
196. Zeger SL, Dominici F, Samet J. Harvesting-resistant estimatesof air pollution effects on mortality. Epidemiology 10:171-175(1999).
197. The Berkeley Mortality Database (BMD). Department ofDemography, University of California, Berkeley. Available:http.//demog.berkeley.edu/wilmoth/mortality [cited 15 March1999].
198. Nevalainen J, Pekkanen J. The effect of particulate air pollutionon life expectancy. Sci Total Environ 217:137-141 (1998).
199. Brunekreef B. Air pollution and life expectancy: is there a rela-tion? Occup Environ Med 54:781-784(1997).
Environmental Health Perspectives * Vol 108, Supplement 4 * August 2000 723
-
Human health effects of air pollution
Marilena Kampa, Elias Castanas*
Laboratory of Experimental Endocrinology, University of Crete, School of Medicine, P.O. Box 2208, Heraklion, 71003, Greece
Received 4 June 2007; accepted 10 June 2007
The effect of air pollutants on human health and underlying mechanisms of cellular action are discussed.
Abstract
Hazardous chemicals escape to the environment by a number of natural and/or anthropogenic activities and may cause adverse effects onhuman health and the environment. Increased combustion of fossil fuels in the last century is responsible for the progressive change in the at-mospheric composition. Air pollutants, such as carbon monoxide (CO), sulfur dioxide (SO2), nitrogen oxides (NOx), volatile organic compounds(VOCs), ozone (O3), heavy metals, and respirable particulate matter (PM2.5 and PM10), differ in their chemical composition, reaction proper-ties, emission, time of disintegration and ability to diffuse in long or short distances. Air pollution has both acute and chronic effects on humanhealth, affecting a number of different systems and organs. It ranges from minor upper respiratory irritation to chronic respiratory and heartdisease, lung cancer, acute respiratory infections in children and chronic bronchitis in adults, aggravating pre-existing heart and lung disease,or asthmatic attacks. In addition, short- and long-term exposures have also been linked with premature mortality and reduced life expectancy.These effects of air pollutants on human health and their mechanism of action are briefly discussed.� 2007 Elsevier Ltd. All rights reserved.
Keywords: Air pollutant; Human health; Cellular actions; Detoxification
1. Introduction
Although a number of physical activities (volcanoes, fire,etc.) may release different pollutants in the environment,anthropogenic activities are the major cause of environmentalair pollution. Hazardous chemicals can escape to the environ-ment by accident, but a number of air pollutants are releasedfrom industrial facilities and other activities and may cause ad-verse effects on human health and the environment. By defini-tion, an air pollutant is any substance which may harmhumans, animals, vegetation or material. As far as humansare concerned an air pollutant may cause or contribute to anincrease in mortality or serious illness or may pose a presentor potential hazard to human health. The determination ofwhether or not a substance poses a health risk to humans is
based on clinical, epidemiological, and/or animal studieswhich demonstrate that exposure to a substance is associatedwith health effects. In the context of human health, ‘‘risk’’ isthe probability that a noxious health effects may occur.
2. Pollutant categories
The main change in the atmospheric composition is primar-ily due to the combustion of fossil fuels, used for the genera-tion of energy and transportation. Variant air pollutants havebeen reported, differing in their chemical composition, reac-tion properties, emission, persistence in the environment, abil-ity to be transported in long or short distances and theireventual impacts on human and/or animal health. However,they share some similarities and they can be grouped to fourcategories:
1. Gaseous pollutants (e.g. SO2, NOx, CO, ozone, VolatileOrganic Compounds).
* Corresponding author. Tel.: þ30 28 1039 4580; fax: þ30 28 1039 4581.E-mail addresses: [email protected] (M. Kampa), [email protected]
(E. Castanas).
0269-7491/$ - see front matter � 2007 Elsevier Ltd. All rights reserved.doi:10.1016/j.envpol.2007.06.012
Available online at www.sciencedirect.com
Environmental Pollution 151 (2008) 362e367www.elsevier.com/locate/envpol
mailto:[email protected]:[email protected]://www.elsevier.com/locate/envpol
-
2. Persistent organic pollutants (e.g. dioxins).3. Heavy metals (e.g. lead, mercury).4. Particulate Matter.
Gaseous pollutants contribute to a great extent in composi-tion variations of the atmosphere and are mainly due to com-bustion of fossil fuels (Katsouyanni, 2003). Nitrogen oxidesare emitted as NO which rapidly reacts with ozone or radicalsin the atmosphere forming NO2. The main anthropogenic sour-ces are mobile and stationary combustion sources. Moreover,ozone in the lower atmospheric layers is formed by a seriesof reactions involving NO2 and volatile organic compounds,a process initiated by sun light. CO, on the other hand, isa product of incomplete combustion. Its major source is roadtransport too. While the anthropogenic SO2 results from thecombustion of sulphur-containing fossil fuels (principallycoal and heavy oils) and the smelting of sulphur containingores, volcanoes and oceans are its major natural sources.The latter contribute only ~2% of the total emissions. Finallya major class of compounds that fuel combustion and espe-cially combustion processes for energy production and roadtransport are the major source of emission are the so calledvolatile organic compounds (VOCs). This is a class of com-pounds, which includes chemical species of organic naturesuch as benzene. Even though the majority of gaseous pollut-ants are inhaled and mainly affect the respiratory system theycan also induce haematological problems (CO, benzene) andcancer.
Persistent organic pollutants form a toxic group of chemi-cals. They persist in the environment for long periods oftime, and their effects are magnified as they move up throughthe food chain (bio-magnification). They include pesticides, aswell as dioxins, furans and PCBs. Generally, the generic term‘‘dioxins’’ is used to cover polychlorinated dibenzo-dioxins(PCDDs) and polychlorinated dibenzo-furans (PCDFs) whilepolychlorinated biphenyls (PCB) are called ‘‘dioxin likecompounds’’ and can act similarly in terms of dioxin-typetoxicity (Schecter et al., 2006). Dioxins are formed during in-complete combustion and whenever materials containingchlorine (e.g. plastics) are burned. Emitted in the atmosphere,dioxins tend to deposit on soil and water but, being water-insoluble, they do not contaminate ground water sources.Most dioxins in plants come from air and dust or pesticidesand enter the food chain where they bio-accumulate due totheir ability to be stably bound to lipids.
Heavy metals include basic metal elements such as lead,mercury, cadmium silver nickel, vanadium, chromium andmanganese. They are natural components of the earth’s crust;they cannot be degraded or destroyed, and can be transportedby air, and enter water and human food supply. In addition,they enter the environment through a wide variety of sources,including combustion, waste water discharges and manufactur-ing facilities. To a small extent they enter human bodieswhere, as trace elements, they are essential to maintain thenormal metabolic reactions. However, at higher (although rel-atively low) concentrations they can become toxic (Jarup,2003). Most heavy metals are dangerous because they tend
to bio-accumulate in the human body. Bioaccumulationmeans an increase in the concentration of a chemical in a bi-ological organism over time, compared to the chemical’sconcentration in the environment. Compounds accumulatein organisms any time they are taken in and stored fasterthan they are broken down (metabolized) or excreted.
Particulate matter (PM) is the generic term used for a typeof air pollutants, consisting of complex and varying mixturesof particles suspended in the breathing air, which vary insize and composition, and are produced by a wide variety ofnatural and anthropogenic activities (Poschl, 2005). Majorsources of particulate pollution are factories, power plants, re-fuse incinerators, motor vehicles, construction activity, fires,and natural windblown dust. The size of the particles varies(PM2.5 and PM10 for aerodynamic diameter smaller than2.5 mm and 10 mm respectively) and different categorieshave been defined: Ultrafine particles, smaller than 0.1 mmin aerodynamic diameter, Fine particles, smaller than 1 mm,and Coarse particles, larger than 1 mm. The size of the parti-cles determines the site in the respiratory tract that they willdeposit: PM10 particles deposit mainly in the upper respiratorytract while fine and ultra fine particles are able to reach lungalveoli. So far, no single component has been identified thatcould explain most of the PM effects. Among the parametersthat play an important role for eliciting health effects are thesize and surface of particles, their number and their composi-tion. The composition of PM varies, as they can absorb andtransfer a multitude of pollutants. However, their major com-ponents are metals, organic compounds, material of biologicorigin, ions, reactive gases, and the particle carbon core. Thereis strong evidence to support that ultra fine and fine particlesare more hazardous than larger ones (coarse particles), interms of mortality and cardiovascular and respiratory effects.In addition, the metal content, the presence of PAHs and othero