Epidemiology of Viral Hepatitis C -...
39
Seyed Moayed Alavian Professor of Gastroenterology and Hepatology Director of Middle East Liver Diseases Center Editor in-chief of Hepatitis Monthly E mail: [email protected] Epidemiology of Viral Hepatitis C Iran Countries of Middle East Eastern Mediterranean Region of WHO
Transcript of Epidemiology of Viral Hepatitis C -...

Seyed Moayed AlavianProfessor of Gastroenterology and HepatologyDirector of Middle East Liver Diseases CenterEditor in-chief of Hepatitis MonthlyE mail: [email protected]
Epidemiology of Viral Hepatitis C IranCountries of Middle East Eastern Mediterranean Region of WHO

Epidemiology of Viral Hepatitis
Hepatitis C Virus Infection
Overview

Natural History of HCV Infection
Epidemiology of Viral Hepatitis
HCV infection Chronic Infection
55-85%
Mild Fibrosis
Spontaneous
Resolution
15-45%
Cirrhosis
15-30%
Decompencated
Cirrhosis
Hepatocellular
Carcinoma(2-4% per year in
cirrhosis)
WHO Guideline. April 2016

Mortality Rates Due to HIV, HCV, and
HBV Infections in the US
Ly KN, et al. Ann Intern Med. 2012
7
6
5
4
3
2
1
0
Ra
te p
er
10
0,0
00
PY
*
Yr
Hepatitis B
Hepatitis C
HIV
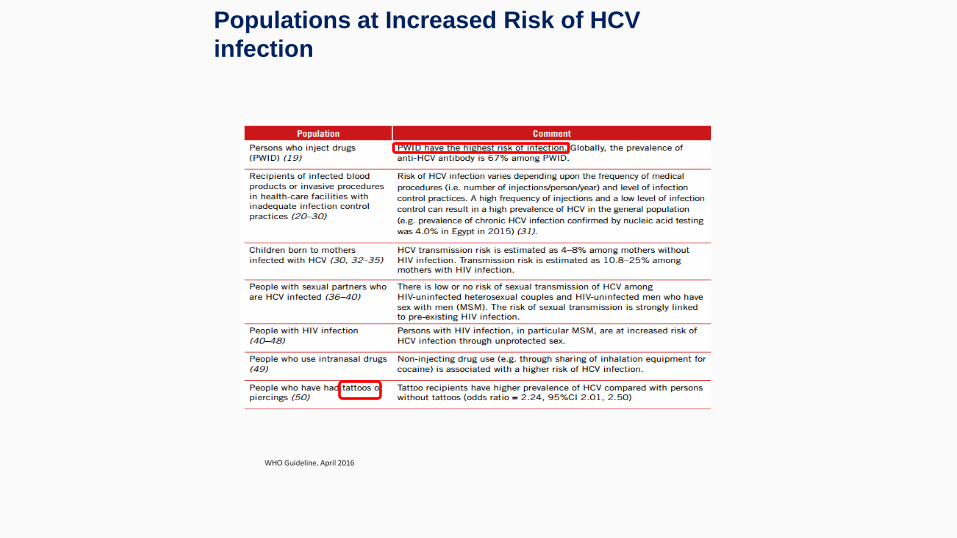
Populations at Increased Risk of HCV
infection
WHO Guideline. April 2016

Hepatitis C Virus Infection
Epidemiology of Viral Hepatitis
WHO Guideline. April 2016
Between 130-170 million people have HCV infectionworldwide.
HCV prevalence is highest in Egypt (>10%)
The most people with HCV infection are in china (29.8)
Asymptomatic nature of the disease lead to difficultdetection of Acute HCV infection

Global Distribution of Genotypes of HCV
Epidemiology of Viral Hepatitis
WHO Guideline. April 2016

Hepatitis C Virus
Infection In Iran

Content
Epidemiology of Viral Hepatitis
Gower E, Global epidemiology and genotype distribution of the hepatitis C virus infection. Journal of hepatology. 2014;61(1 Suppl):S45-57.
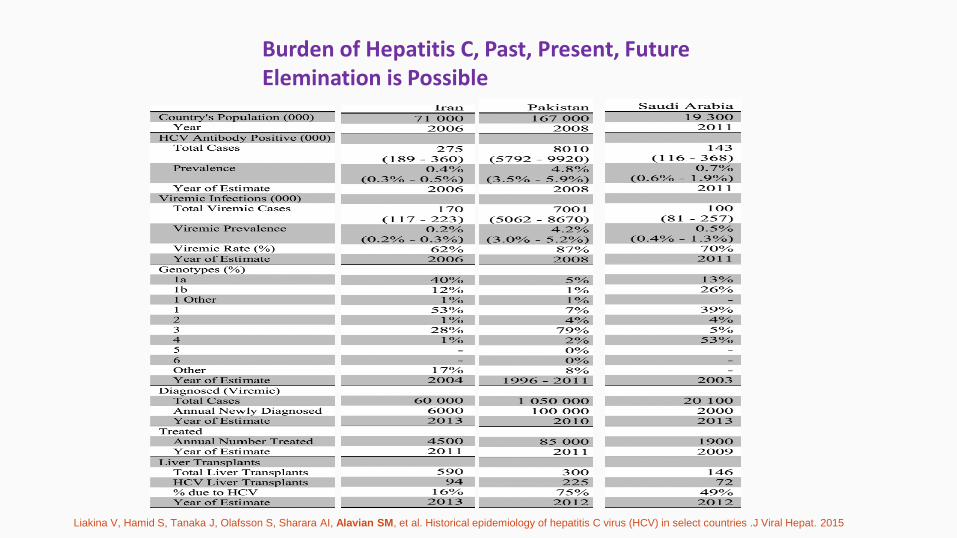
Liakina V, Hamid S, Tanaka J, Olafsson S, Sharara AI, Alavian SM, et al. Historical epidemiology of hepatitis C virus (HCV) in select countries .J Viral Hepat. 2015
Burden of Hepatitis C, Past, Present, FutureElemination is Possible
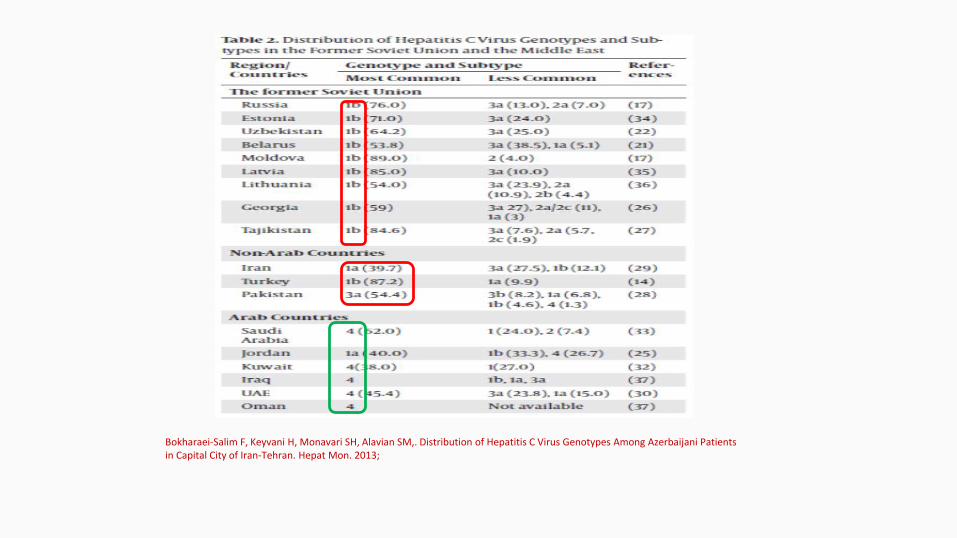
Bokharaei-Salim F, Keyvani H, Monavari SH, Alavian SM,. Distribution of Hepatitis C Virus Genotypes Among Azerbaijani Patients in Capital City of Iran-Tehran. Hepat Mon. 2013;

Distribution of Genotypes of HCV in the Region
Epidemiology of Viral Hepatitis
Sadeghi F. Prevalence of Hepatitis C Virus Genotypes Among Patients in Countries of the Eastern Mediterranean Regional Office of WHO (EMRO): A Systematic Review and Meta-Analysis. Hepat Mon. 2016

Younger HCV infected patients in Iran
Liakina V, Hamid S, Tanaka J, Olafsson S, Sharara AI, Alavian SM, et al. Historical epidemiology of hepatitis C virus (HCV) in select countries .J Viral Hepat. 2015
Iran has one of thelowest rates of HCVprevalence in the MiddleEast. Under the currenttreatment paradigm, HCVinfections will increase inIran.
Less than 0.4% in general population
Epidemiology of Viral Hepatitis
Hepatitis C Virus Infection
Prevalence in Hemodialysis Patients

HCV infection in Hemodialysis Patients in EMRO
Epidemiology of Viral Hepatitis
Alavian SM, et al. Epidemiology and risk factors of HCV infection among hemodialysis patients in countries of the Eastern Mediterranean
Regional Office of WHO (EMRO): a quantitative review of literature. J Public Health (Oxf). 2011.

HCV infection in Hemodialysis Patients in Iran
Epidemiology of Viral Hepatitis
Alavian SM, et al. Epidemiology and risk factors of HCV infection among hemodialysis patients in countries of the Eastern Mediterranean
Regional Office of WHO (EMRO): a quantitative review of literature. J Public Health (Oxf). 2011.

Preventive Strategies
• Strict adherence to universal infectioncontrol precautions seems to be the mostimportant approach to control diseasespread in HD units.
• Designing and implementation an onlinenetwork to link the dialysis centers forsurveillance system
• Therapy of infected patients ASAP
• HCV infected should be placed in thepriority of renal transplantation
Alavian SM. Hepatitis C, Chronic Renal Failure, Control Is Possible! Hepat Mon. 2006
• Prevalence of positive HBS Ag and HCV Abs in patients on hemodialysis
decreased from 3.8% and 14.4% in 1999 to 2.6% and 4.5% in 2006,
respectively.
Alavian SM, et al. Hepatitis B and C in dialysis units in Iran: Changing the epidemiology. Hemodial Int. 2008
HBV and HCV Infection in hepatocellular Carcinoma
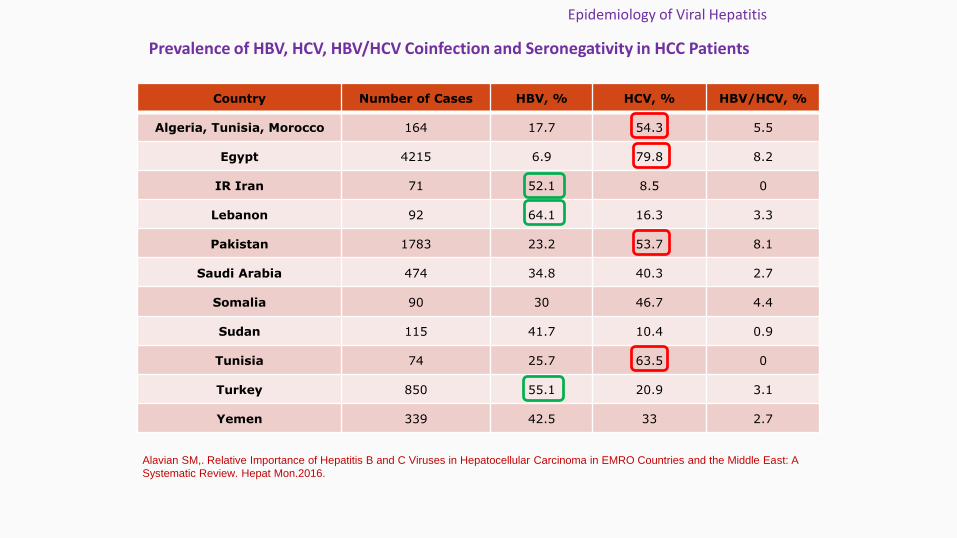
Prevalence of HBV, HCV, HBV/HCV Coinfection and Seronegativity in HCC Patients
Epidemiology of Viral Hepatitis
Country Number of Cases HBV, % HCV, % HBV/HCV, %
Algeria, Tunisia, Morocco 164 17.7 54.3 5.5
Egypt 4215 6.9 79.8 8.2
IR Iran 71 52.1 8.5 0
Lebanon 92 64.1 16.3 3.3
Pakistan 1783 23.2 53.7 8.1
Saudi Arabia 474 34.8 40.3 2.7
Somalia 90 30 46.7 4.4
Sudan 115 41.7 10.4 0.9
Tunisia 74 25.7 63.5 0
Turkey 850 55.1 20.9 3.1
Yemen 339 42.5 33 2.7
Alavian SM,. Relative Importance of Hepatitis B and C Viruses in Hepatocellular Carcinoma in EMRO Countries and the Middle East: A
Systematic Review. Hepat Mon.2016.

The Most Prevalent Cause of Hepatocellular Carcinoma (HCC) and Their Share in Causing HCC
Epidemiology of Viral Hepatitis
Alavian SM,. Relative Importance of Hepatitis B and C Viruses in Hepatocellular Carcinoma in EMRO Countries and the Middle East: A
Systematic Review. Hepat Mon.2016.

Specific Problems in the Region
Epidemiology of Viral Hepatitis
Specific Problems in the Region
Population of 355 million and the vast majority of people
living in middle-income countries including a young and
educated population
Syria, Iraq, Libya and Yemen are in civil war, causing untolddamage to human lives and physical infrastructure.
Fifteen million people have fled their homes, many to fragile oreconomically strapped countries such as Jordan, Lebanon,Djibouti and Tunisia, giving rise to the biggest refugee crisissince World War II
http://www.worldbank.org/en/region/mena/overview#1

Hemophilia on HCV
• Prevalence among this group is one of the highest among all
known at risk groups and estimated to be between 70%-95%.
1- Being exposed to repeated infections of different HCV strains
2- Multiple viral infections, specially HBV and HIV
3- Low activity and obesity
4- Habits, like alcohol and smoking
Alavian SM, Aalaei-Andabili, S. H. Big Gap Knowledge about Hepatitis C Infection Rate among Inherited Coagulation Disorders Patients in EMRO Countries 2011
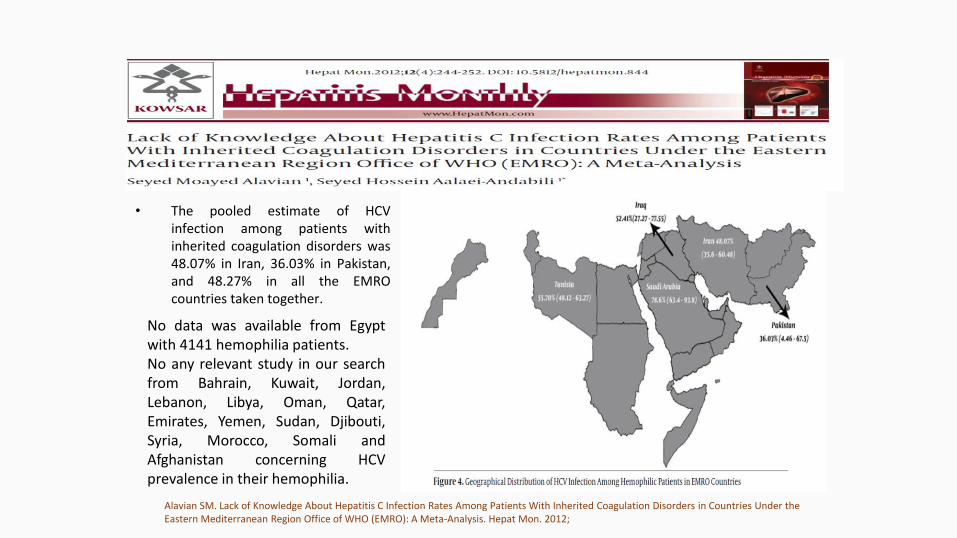
• The pooled estimate of HCV infection among patients with inherited coagulation disorders was 48.07% in Iran, 36.03% in Pakistan, and 48.27% in all the EMRO countries taken together.
No data was available from Egyptwith 4141 hemophilia patients.No any relevant study in our searchfrom Bahrain, Kuwait, Jordan,Lebanon, Libya, Oman, Qatar,Emirates, Yemen, Sudan, Djibouti,Syria, Morocco, Somali andAfghanistan concerning HCVprevalence in their hemophilia.
Alavian SM. Lack of Knowledge About Hepatitis C Infection Rates Among Patients With Inherited Coagulation Disorders in Countries Under the Eastern Mediterranean Region Office of WHO (EMRO): A Meta-Analysis. Hepat Mon. 2012;
Two hundred and twenty-five subjects (61%) achieved SVR,66 patients relapsed and 30 subjects did not respond andnine patients developed breakthrough during treatment.
In a multivariate logistic regression model, age<24 oddsratio (OR) = 1.8, genotype non-1 OR= 1.8, BMI<25 OR= 2.1and HCV RNA<600 000 IU/ml OR= 1.7 were independentpredictors of SVR.
Alavian SM, et al. Peginterferon alpha-2a and ribavirin treatment of patients with haemophilia and hepatitis C virus infection: a single-centre study of 367 cases. Liver Int. 2010

Thalassemia Patients are special patients
Special patient populations require special care

• Patients with thalassemia or otherhemoglobinopathies were atgreater risk of acquiring HCVinfection as a consequence ofrepeated transfusions of blood,respectively, before theintroduction of blood donorscreening for hepatitis C.
0
4
Introduction
Previously Thalassemia patients died as
consequences of cardiovascular diseases and
infections and because of low life expectancy liver
diseases caused by iron overload or HCV/HBV
infection did not get the chance to manifest itself.
However today, longer life expectancy are turning liver diseases to the third cause of morbidity and mortality in thalassemia patients.

Epidemiology of HCV in Thalassemia
Iran
EMRO
In Iran, blood donors screening for HCV infection started in 1996. The pooled OR of HCV
infection rate for patients transfused before that date was OR=7.6 and this implies an increase
in blood safety and more attention to health precautions in Iran
Hepatitis C in thalassemia in IranHepatitis C in thalassemia in EMRO
In Iran from a total of 5229 thalassemia subjects
Its Seroepidemiology ranged
from 2 to 32%.
Pooled HCV infection rate was 18%
Pooled HCV infection rate
was:
45% in Pakistan
63% in Saudi Arabia
69% in Egypt
Alavian SM, et al.. Epidemiology of HCV Infection among Thalassemia Patients in eastern Mediterranean Countries: a Quantitative Review of Literature. Iran Red Cres Med J. 2010
Nosocomial Transmission of Hepatitis C at
Iranian Thalassemia Centers
• Strains in seven clades were from nine patients infected between 1999and 2005 and similar to strains from eight patients infected before 1996,indicating ongoing transmission at the centers.
• Further epidemiological investigation revealed that 28 patients infectedwith strains within the same clade had frequently been transfused at thesame shift sitting on the same bed.
• An additional eight patients with related strains had frequently beentransfused simultaneously in the same room.
• Nosocomial transmission at these thalassemia centers both before andafter the introduction of blood screening. Further training of staff andstrict adherence to preventive measures are thus essential to reduce theincidence of new HCV and TREATMENT OF ALL PATINETS WITH NEWDRUGS
Samimi-Rad K, Alavian, S. M., et al. Patient-to-Patient Transmission of Hepatitis C at Iranian Thalassemia Centers Shown by Genetic Characterization of Viral Strains. Hepat Mon. 2013
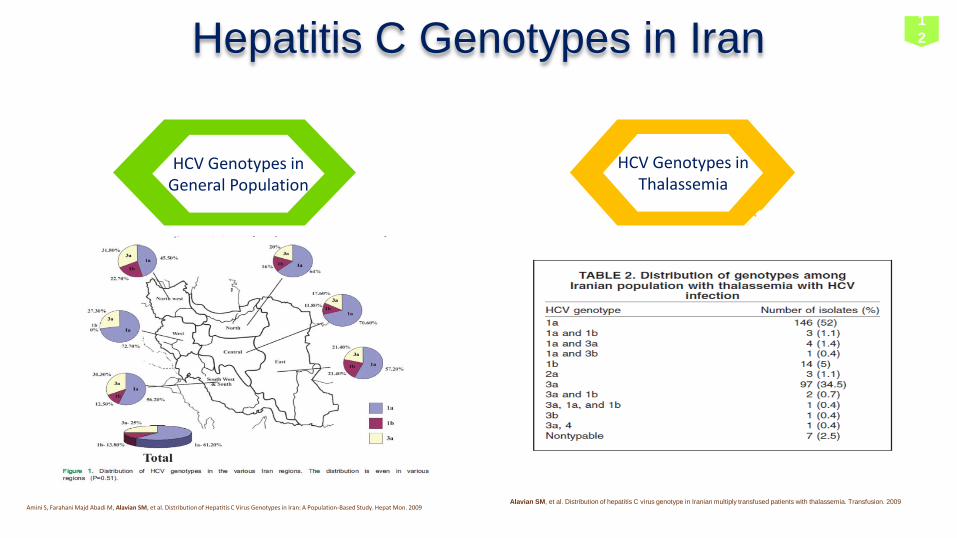
HCV Genotypes in General Population
HCV Genotypes in Thalassemia
Hepatitis C Genotypes in Iran
Alavian SM, et al. Distribution of hepatitis C virus genotype in Iranian multiply transfused patients with thalassemia. Transfusion. 2009Amini S, Farahani Majd Abadi M, Alavian SM, et al. Distribution of Hepatitis C Virus Genotypes in Iran: A Population-Based Study. Hepat Mon. 2009
1
2

Elimination of HCV infection in Iran will be in 2030 but in thalassemia is possible in 2020!
Solution
Work together
More support for therapy
More attention to blood safety
More education the nurses in thalassemia centers
Increase the thalassemia patients awareness regarding the
issue.
25

Amini S, Farahani Majd Abadi M, Alavian SM, Joulaie M, Ahmadipour MH. Distribution of Hepatitis C Virus Genotypes in Iran: A Population-Based Study. Hepat Mon. 2009
Neonatal Blood Exchange and HCV Infection in Iran
• For finding the situation before screening of HCV in blooddonors?
• Between 2000-2002, questionnaire to 47227 parents ofstudents, eight different part of Tehran, randomly selected,
• Do you have children between 9-11 years ( screening startedin 1995)?
• 465 children with history of blood exchange
• Two were HCV Ab positive and only one case with HCV RNApositive and genotype 1a
• Risk of HCV infection among transfused neonate isuncommon, but it is critical to find them
Nikbin M, Alavian SM, Tavangar HR. Hep Mon 2006
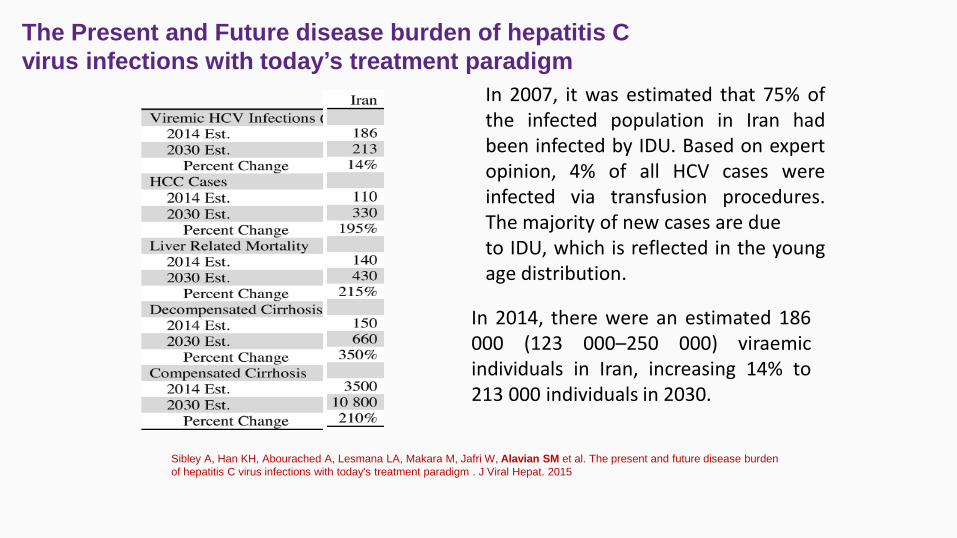
The Present and Future disease burden of hepatitis C
virus infections with today’s treatment paradigm
Sibley A, Han KH, Abourached A, Lesmana LA, Makara M, Jafri W, Alavian SM et al. The present and future disease burden
of hepatitis C virus infections with today's treatment paradigm . J Viral Hepat. 2015
In 2007, it was estimated that 75% ofthe infected population in Iran hadbeen infected by IDU. Based on expertopinion, 4% of all HCV cases wereinfected via transfusion procedures.The majority of new cases are dueto IDU, which is reflected in the youngage distribution.
In 2014, there were an estimated 186000 (123 000–250 000) viraemicindividuals in Iran, increasing 14% to213 000 individuals in 2030.
Alfaleh FZ, Nugrahini N, Maticic M, Tolmane I, Alzaabi M, Hajarizadeh B, Alavian SM et al. Strategies to manage hepatitis C virus
infection disease burden - volume . J Viral Hepat. 2015
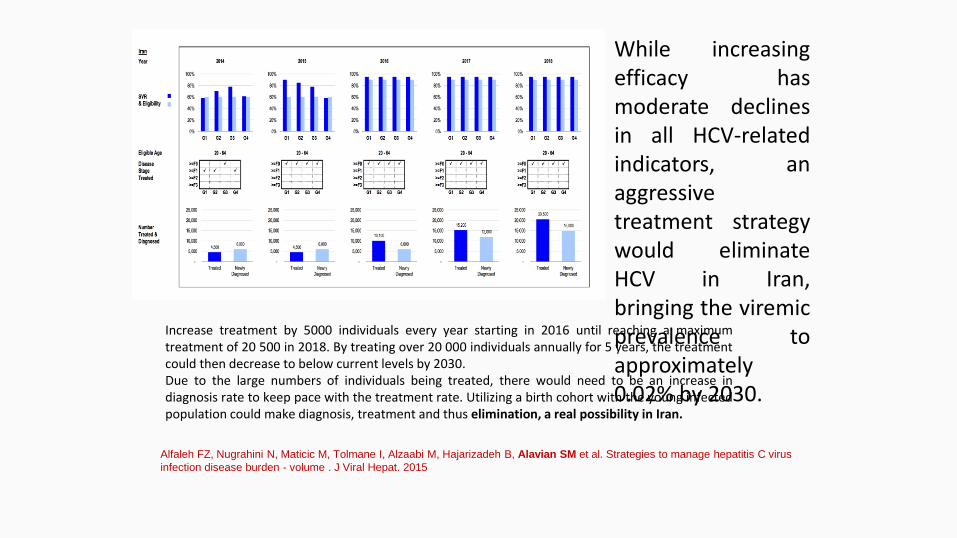
While increasingefficacy hasmoderate declinesin all HCV-relatedindicators, anaggressivetreatment strategywould eliminateHCV in Iran,bringing the viremicprevalence toapproximately0.02% by 2030.
Increase treatment by 5000 individuals every year starting in 2016 until reaching a maximumtreatment of 20 500 in 2018. By treating over 20 000 individuals annually for 5 years, the treatmentcould then decrease to below current levels by 2030.Due to the large numbers of individuals being treated, there would need to be an increase indiagnosis rate to keep pace with the treatment rate. Utilizing a birth cohort with the young infectedpopulation could make diagnosis, treatment and thus elimination, a real possibility in Iran.

Hepatitis C Virus Infection
Patients Findings with Consideration of Direct Acting
Antivirals
Special Screening Program for high Risk Groups Risk-based screening strategies can identify about 86% of patients with HCV
in the US The Necessity of Mass Screening The feasibility of such an approach is highly dependent on the economic
situation of a given country.
Hesamizadeh K,. Next Steps for Eradication of Hepatitis C in the Era of Direct Acting Antivirals. Hepat Mon.2016
Peer-based Approaches
• Peers are likely to be nonjudgmental and supportive; participants tend to feelmore comfortable and those they trustful for the patients.
• Peers are also the best placed people to engage other drug users on hepatitis Crisk and prevention, since they are often present when people are injecting.
• Educating IDUs by peers is very informative and efficient. Encouraging the IDUs tobe clean and to learn more from each other is effective, too.