醫師公會 slide1.ppt [相容模式]2009/6/28 1 骨質疏鬆 最新治療趨勢 振興醫院...
18
2009/6/28 1 骨質疏鬆 最新治療趨勢 振興醫院 過敏免疫風濕科 李信興主任 骨質疏鬆 Normal Moderate Osteoporosis Severe Osteoporosis 什麼是骨質疏鬆症 • 一種全身性骨量降低,使骨骼微細結構 發生破壞的疾病,會導致骨骼的脆弱, 結果使發生骨折的危險性增加。 •英文字義 多孔的骨骼 •英文字義=多孔的骨骼 世界衛生組織對骨鬆的定義 ‧WHO 對骨質疏鬆的定義: 骨質密度與年輕族群比較低於2.5的標準偏差 Osteoporosis is Serious M th D ht M th D ht Mother Daughter Mother Daughter N Engl J Med 2008 May 29;358;2388 骨質重塑 造骨細胞 破骨細胞 骨質再吸收 骨合成 人體的骨骼如同其他的細胞一樣,隨時都在進行新陳 代謝,目的是修補傷害或因應體能活動而重塑新的骨 架,這個過程稱之為骨骼重塑,體內同時有 好幾百萬個部位進行這樣的工作
Transcript of 醫師公會 slide1.ppt [相容模式]2009/6/28 1 骨質疏鬆 最新治療趨勢 振興醫院...
-
2009/6/28
1
骨質疏鬆最新治療趨勢
振興醫院
過敏免疫風濕科
李信興主任
骨質疏鬆
Normal ModerateOsteoporosis
SevereOsteoporosis
什麼是骨質疏鬆症
• 一種全身性骨量降低,使骨骼微細結構發生破壞的疾病,會導致骨骼的脆弱,結果使發生骨折的危險性增加。
•英文字義 多孔的骨骼•英文字義=多孔的骨骼
世界衛生組織對骨鬆的定義
‧WHO 對骨質疏鬆的定義:骨質密度與年輕族群比較低於2.5的標準偏差
Osteoporosis is Serious
M th D ht M th D htMother Daughter Mother Daughter
N Engl J Med 2008 May 29;358;2388
骨質重塑
造骨細胞破骨細胞
骨質再吸收
骨合成
人體的骨骼如同其他的細胞一樣,隨時都在進行新陳代謝,目的是修補傷害或因應體能活動而重塑新的骨架,這個過程稱之為骨骼重塑,體內同時有好幾百萬個部位進行這樣的工作
-
2009/6/28
2
The Dynamic of OsteoporosisNormal Bone Osteoporosis
骨質疏鬆症的危險性
‧骨折
‧疼痛
‧活動性降低
肌肉衰弱‧肌肉衰弱
‧外觀變形(駝背,脊柱側彎,身高變矮)
‧行動不變造成與社會疏離
‧喪失獨立自主的能力
‧高死亡率(與乳癌末期死亡率相當)
易發生骨折的部位
• 脊椎 Spine– 壓迫型/楔狀/魚尾狀
– Kyphosis/Iordosis/dowager’s hump
• 腕部 Wrist or Colles’
• 髖部 Hip – 股骨頸/股骨頭/股骨幹
依健保紀錄,台灣髖部骨折一年內的死亡率男性為22 %,女性為15 %。死因以長期臥床引發之感染為主。
髖部骨折台灣每年醫療耗費急性住院期:10 億台幣復健:11.3 億台幣
骨質疏鬆症所帶來的經濟負擔
共 21.3 億台幣
間接耗費醫療器材、居家設備、看護、失業等共 68 億台幣
蔡益堅, 何彥瑤:台灣地區老年髖骨骨折罹病天數及經濟成本台中:台灣省家庭計劃研究所, 1994
-
2009/6/28
3
Women With Osteoporotic Fractures Often Go Undiagnosed and Untreated
708090
100
ents
Patients Admitted with Osteoporotic Fractures
Data from Hajcsar EE, et al. CMAJ. 2000;163:819-822.
100
2030405060
% o
f pat
ie
BMDbefore
fracture
15%BMDafter
fracture
22%
Osteoporosisdiagnosis
18%
32%
Calciumprescribed
Vitamin Dprescribed
15%
Bisphosphonateprescribed
8%
# Fractures
Pers
on-Y
ears
Num
ber
Fracture RateBMD Distribution
40
50
60
300
350
400
450OsteoporosisOsteopenia
許多骨折也會發生在Osteopenia骨質缺乏的病人
骨質密度 T-scores
Frac
ture
Rat
e pe
r 100
0 of Fractures
>1.01.0 to 0.5
0.5 to 0.00.0 to –0.5
–0.5 to –1.0–1.0 to –1.5
–1.5 to –2.0–2.0 to –2.5
–2.5 to –3.0–3.0 to –3.5
< –3.5
Adapted from Siris ES, et al. JAMA. 2001;286:2815-22.
0
10
20
30
0
50
100
150
200
250
20
30
40AgeAge
6060
70708080
tic F
ract
ure
Ris
ktic
Fra
ctur
e R
isk
年齡與骨折風險的關係
高骨折風險
如果年齡較高病患,即使判定為骨質缺乏(osteopenia) ,仍可能為高風險而建議治療
0
10
20
−3 −2.5 −2 −1.5 −1 -0.5 0 0.5 1
BMD T-Score
5050
Ost
eopo
rot
Ost
eopo
rot
Core data from Kanis JA, et al. Core data from Kanis JA, et al. Osteoporosis Int.Osteoporosis Int. 2001;12:9892001;12:989––995995McClung MR. McClung MR. BoneBone 2005;38:S132005;38:S13--S17S17
骨質疏鬆 骨質缺乏
骨質密度
2008 NOF治療規範
停經後婦女和超過(含)五十歲男性
髖部或 骨質缺乏骨質疏鬆 骨質缺乏
National Osteoporosis Foundation, 2008National Osteoporosis Foundation, 2008
TreatTreat
髖部或脊椎骨折
其他部位骨折
骨質缺乏--2.5
-
2009/6/28
4
Bone Remodeling in BMUs (Basic Multicellular Units)
19From Canalis et al, NEJM, 357: 905-916, 2007
Antiresorptives vs Anabolic Agents
Bone resorption Bone formation
Therapeutic options for osteoporosis
Stimulators of bone formationStimulators of bone formation
•• ((Fluoride) Fluoride) •• ParaThyroid Hormone ParaThyroid Hormone
rhPTH(1rhPTH(1--34)=Teriparatide(Forteo)34)=Teriparatide(Forteo)
Inhibitors of bone resorption
Bisphosphonates– Alendronate (Fosamax)– Ibandronate (Bonviva)
Zoledronate (Aclasta)
20
Recommended for all women Recommended for all women at risk for osteoporosisat risk for osteoporosis•• Calcium and vitamin DCalcium and vitamin D
– Zoledronate (Aclasta)• Calcitonin • Estrogen ± progestin• Strontium ranelate (Protos)
• Selective estrogen receptor modulators (SERMs)– Raloxifene (Evista)
FDA Approved Indication
Male OP GIOPPaget’sPostmenopausal OP
Yes Yes YesYes YesPrevention Treatment
Alendronate (Fosamax)---- ----- ----Yes Yes Yes---- ---- -------- ---- -------- ---- -------- ---- Yes
Yes Yes---- Yes---- Yes#
Yes ----Yes Yes---- Yes
# Treatment at > 5 years
if HRT is not toleratedafter menopause
Ibandronate (Bonviva)Zoledronic AcidCalcitonin (Miacalcin)HRTRaloxifene( Evista)PTH (Forteo)
CalcitoninCalcitonin
Calcitonin NS
As a result of several small studies, mostly in As a result of several small studies, mostly in Europe, the FDA approved Miacalcin Nasal Europe, the FDA approved Miacalcin Nasal Spray for the Spray for the treatment of postmenopausal treatment of postmenopausal osteoporosisosteoporosis
Restricted to patients > 5 years post menopausal Restricted to patients > 5 years post menopausal Restricted to patients who can not, prefer not, or choose Restricted to patients who can not, prefer not, or choose not to take estrogennot to take estrogen
Increases bone density in the spine Increases bone density in the spine (baseline)(baseline)
Effect on hip fracture incidence not Effect on hip fracture incidence not establishedestablished
PROOF (Prevent Recurrence Of Osteoporotic Fractures)PROOF (Prevent Recurrence Of Osteoporotic Fractures)
Chesnut III CH et al. Am J Med 2000;109:267Chesnut III CH et al. Am J Med 2000;109:267--76.76.Cummings SR and Cummings SR and Chapurlat RD.Chapurlat RD. Am J Med 2000;109:330Am J Med 2000;109:330--1.1.
N = 1255 osteoporotic postmenopausal womenN = 1255 osteoporotic postmenopausal women
Nasal CalcitoninEfficacy at the Spine and Hip (PROOF: 5-Year Analysis)
Percent Reduction in New Vertebral Fractures
Number of Hip Fracturesby Treatment Group
20
250
2010
Chesnut III CH et al. Am J Med 2000;109:267Chesnut III CH et al. Am J Med 2000;109:267--76.76.
0
5
10
15
20
Placebo 100 IU 200 IU 400 IU
1(NS)
5(NS)
7(NS)9
100 IU15%(NS) 200 IU
33%(P=0.03)
400 IU16%(NS)
1009080706050403020
NS = Not significant.NS = Not significant.
-
2009/6/28
5
RaloxifeneRaloxifene
Raloxifene: Effect on Radiographic Vertebral Fractures(MORE = Multiple Outcomes of Raloxifene Evaluation Study)
20
25
nts
with
l Fra
ctur
e Substudy1Substudy1(BMD (BMD ≤ ≤ ––2.5 and 2.5 and nono preexistingpreexisting
vertebral fractures)vertebral fractures)
Substudy 2 Substudy 2 BMD BMD ≤ ≤ ––2.5 and preexisting2.5 and preexisting
vertebral fractures)vertebral fractures)
Ettinger B et al. JAMA 1999;282:637Ettinger B et al. JAMA 1999;282:637--45.45.
0
5
10
15
Perc
ent o
f Pat
ien
Inci
dent
Ver
tebr
al
50%
30%
PlaceboN=1522
Raloxifene60 mg/dN=1490
PlaceboN=770
Raloxifene60 mg/dN=769
Hip Fractures3
s w
ith
Frac
ture
s Non-Vertebral Fractures15
Efficacy at the HIPEffect of Raloxifene on Non-Vertebral and Hip Fracture M.O.R.E. Pooled Data (60 mg and 120 mg)
Months
2
1
00 6 12 18 24 30 36
RaloxifenePooled
Placebo
Perc
ent o
f Pat
ient
sIn
cide
nt N
on-V
erte
bral
10
5
00 6 12 18 24 30 36
Months
Placebo
RaloxifenePooled
Ettinger B et al.Ettinger B et al. JAMA 1999;282:637JAMA 1999;282:637––45.45.
RUTH Study (Raloxifene Use for The Heart) Jul,2006 NEJM
原本希望藉由這個研究評估原本希望藉由這個研究評估EvistaEvista在心血管的好處在心血管的好處結果,在一萬多人,長達五年追蹤的研究結果發現:結果,在一萬多人,長達五年追蹤的研究結果發現:
1.1. EvistaEvista會增加致命性中風的風險達會增加致命性中風的風險達49% (49% (絕對風險增加絕對風險增加 0.7 per 1000 woman0.7 per 1000 woman--years)years)2.2. EvistaEvista會增加靜脈栓塞的風險達會增加靜脈栓塞的風險達44 % (44 % (絕對風險增加絕對風險增加 1.2 per 1000 woman1.2 per 1000 woman--years)years)3.3. EvistaEvista可以降低脊椎骨折風險達可以降低脊椎骨折風險達35 % (35 % (絕對風險減少絕對風險減少1.3 per 1000 woman1.3 per 1000 woman--years)years)4.4. EvistaEvista可以降低乳癌風險達可以降低乳癌風險達44 % 44 % ((絕對風險減少絕對風險減少1.2 per 1000 woman1.2 per 1000 woman--years)years)5.5. EvistaEvista對冠狀動脈事件的風險沒有顯著的影響對冠狀動脈事件的風險沒有顯著的影響
BarrettBarrett--Connor E, et al. N Engl J Med. 2006;355:125Connor E, et al. N Engl J Med. 2006;355:125--37. 37.
Evista 仿單Evista
-
2009/6/28
6
BisphosphonatesBisphosphonatesHydroxapatite 氫磷灰石
Mechanism of Action
FOSAMAX 藉著抑制破骨細胞的活性,降低骨質被吸收的量
FOSAMAX 會選擇性的附著在骨質吸收的部位
降低骨質被吸收的量
當新骨質形成的平均總量,大於被吸收的骨質總量時……….
…….只要持續以FOSAMAX治療,便能達到增加骨質總量至正常的效果
Cha
nge
±S
E
ALN 5 mgALN 10 mgALN 20 mg/ALN 5 mg/Placebo
-40
-30
-20
-10
0
Early and Statistically Significant Effects
Reduced markers of bone resorption at 1 month
PCP
O
O
HO OH
OHHOCH2HO CH2 CH2 NH2
Mea
n P
erce
nt C
Month
-90
-80
-70
-60
-50
40
0 12 24 36 48 60 72 84 96 108 120
N Engl J Med 350;12:1189-1199 (March 18, 2004)
Reduced markers of bone resorption at 1 month
Lumbar Spine BMD –Early Efficacy and Sustain Effect
101112131415
om B
asel
ine ALN 5 mg
ALN 10 mgALN 20 mg/ALN 5 mg/Placebo
0123456789
0 12 24 36 48 60 72 84 96 108 120
Mea
n %
Cha
nge
Fro
MonthBone H, et al. NEJM March 2004
Increased lumbar spine and hip trochanter BMD at 3 months
Reduction in Vertebral Fractures at Year 3
Patients With Preexisting Vertebral Fractures
MultipleRadiographic
12
16
Frac
ture
47%Reduction
Radiographic Clinical
0.5%
PBO = placebo; ALN = alendronate; ARR = absolute risk reduction.Black DM, et al. Lancet. 1996;348:1535–1541.FOSAMAX [package insert]. Whitehouse Station, NJ: Merck & Co., Inc.; 2004.
4
8
PBO966
% o
f Pat
ient
s W
ith F
n =
90%ReductionP
-
2009/6/28
7
Proven Vertebral Fracture Efficacy of FOSAMAX™
2
3
4
ve in
cide
nce
(%) Placebon=1817
FOSAMAX n=1841
59% reduction P
-
2009/6/28
8
Bone safety of long-term bisphosphonate
Current Medical Research and Opinion 2004;20:1291-1300
若一個地方若有沈積若一個地方若有沈積BisphophonateBisphophonate,骨代謝會較慢,就不會,骨代謝會較慢,就不會一直有機會沈積藥物,故這樣的特性使得藥物一直有機會沈積藥物,故這樣的特性使得藥物
1) 1) 選擇性且專一的抑制骨質流失較快速的骨小樑選擇性且專一的抑制骨質流失較快速的骨小樑2) 2) 負回饋機制,因此不會過度抑制負回饋機制,因此不會過度抑制
Alendronate Normalized Bone Turnover through 10 Years•• 骨質代謝指標明顯下降到婦女停經前的正常範圍骨質代謝指標明顯下降到婦女停經前的正常範圍
70
100 Bone ResorptionUrine NTx (mean value)
Bone FormationBone-specific alkaline
phosphatase (mean value)
60
80
90
25
15
20
mm
ol C
r
Alendronate 10 mg daily* Premenopausal range (±2 SD from mean)
Evaluation of BMD effects in 247 postmenopausal women treated with alendronate 10 mg for 10 years in a study of the effects of prolonged therapyBCE=bone collagen equivalentAdapted from Bone HG et al N Engl J Med 2004;350(12):1189–1199; Garnero P et al J Bone Miner Res 1996;11(3):337–349.
0
Month
10
20
30
40
50
0 12 24 36 48 60 72 84 96 108 1200
Month
5
10
0 12 24 36 48 60 72 84 96 108 120
nmol
BC
E/m
µg/L
No Oversuppression !!!
Safety of Osteoporosis Treatment
JADA 2008;139(1):23-30
1st case-controlled
study
General Side Effects of Intravenous (IV) Bisphosphonates
Sid ff t d t d i ti t th IVSid ff t d t d i ti t th IVSide effects documented in patients on the IV Side effects documented in patients on the IV bisphosphonates ibandronate and zoledronic acid bisphosphonates ibandronate and zoledronic acid may include:may include:•• Fever, chillsFever, chills•• Headache Headache •• AcuteAcute--phase reaction phase reaction •• Muscle, bone and joint pain Muscle, bone and joint pain •• Eye inflammation Eye inflammation •• Nephrotic syndrome Nephrotic syndrome
IV Bisphosphonates
-
2009/6/28
9
副作用
5 倍
2.3倍
4.1倍
4.1倍
Influenza-like
Nausea
MyalgiaDyspepsia
PTH (teriparatide)PTH (teriparatide)
Administration and dose determine PTH effects on bone
Mode Effect
Daily(Low Dose) Anabolic
Continuous(High Dose) Catabolic
From Dobnig & Turner, Endocrinology, 1997;138:4607-4612.
Effect of PTH on the Risk of New Vertebral Fractures
*P 1 fracture
Neer R et al. N Engl J Med. 2001;344:1434-1441.
*95% CI, 0.19-0.50 †95% CI, 0.22-0.55
-
2009/6/28
10
PTH and osteosarcoma
•• 仿單仿單 (FORTEO Teriparatide)(FORTEO Teriparatide)
•• Limit to 18 months useLimit to 18 months use•• Currently 1 case report on human use Currently 1 case report on human use
PTH withdrawal•• PTH (1PTH (1––34) increases bone formation but results in 34) increases bone formation but results in
deposition of bone that has a lower mineral contentdeposition of bone that has a lower mineral contentthan bone formed prior to PTH treatment than bone formed prior to PTH treatment
•• In the absence of antiIn the absence of anti--resorptive therapy, resorptive therapy, bone bone p py,p py,induced by PTH is likely to be rapidly resorbed, induced by PTH is likely to be rapidly resorbed, particularly if bone turnover is still increased as a particularly if bone turnover is still increased as a function of PTH therapyfunction of PTH therapy
The importance of bisphosphonate therapy in maintaining bone mass in men after therapy with teriparatide [human parathyroid hormone(1–34)] Osteoporos Int (2004) 15: 992–997
Changes in bone density 1 year after withdrawal of hPTH (1–34) treatment
Bisphosphonates versus non-pharmacologic therapy.
Bisphosphonates
Osteoporos Int (2004) 15: 992–997
No medication
8%
Changes in bone density 1 year after withdrawal of hPTH (1–34) treatment
Osteoporos Int (2004) 15: 992–997
PTH Withdrawal
2 years -1st year PTH PTH-2nd year placebo alendronate
StrontiumStrontium
-
2009/6/28
11
Protos
•• OnceOnce--daily therapydaily therapy•• Strontium is a heavy metalStrontium is a heavy metal
Dosing:Dosing:•• 22--g sachet of granules mixed with a glass ofg sachet of granules mixed with a glass of
Strontium Ranelate 鍶鹽
22 g sachet of granules mixed with a glass of g sachet of granules mixed with a glass of water at bedtime at least 2 hours after eatingwater at bedtime at least 2 hours after eating
•• Food and milk slow the absorption of the Food and milk slow the absorption of the granulesgranules
FOSAMAXFOSAMAX ACTONELACTONEL PROTOSPROTOS
Secondary Secondary PreventionPrevention
Vertebral 45% 39% 37%
Pooled Analysis of Relative Risk ReductionPooled Analysis of Relative Risk Reduction
Non-vertebral 23% 20% 14%Hip 53% 26% NP
Wrist 50% NS NDNot Head-to-Head Analysis; NS = Not Significant, ND = No Data, NP = Not sufficiently powered trial
Protos
歐盟警告鍶鹽的安全性
DRESS 啫伊紅血球增多性藥疹與全身症狀-2 名致死案例
Up to now, 16 cases of ‘drug rash with eosinophilia and systemic symptoms (DRESS)’ in patients treated with Protelos/Osseor, two of which were fatal, have been reported to the EMEA, following a total of around 570,000 patient-years of worldwide exposure. DRESS is a serious and life-threatening condition. The reported serious reactions started within 3 to 6 weeks of the initiation of the treatment, with skin rash, accompanied by a fever, swollen glands, increased numbers of white cells in the blood and effects on the liver, kidneys and lung. Having assessed the newly available data, the Agency’s Committee for Medicinal Products for Human Use (CHMP) has agreed that the product information be provisionally updated in a rapid procedure to include warnings on severe hypersensitivity syndromes, including DRESS and Stevens Johnson-Syndrome, in the prescribing and patient information, as an urgent measure.
DRESS:藥物疹合併嗜伊紅血症及全身症狀
藥物疹合併嗜伊紅血症及全身症狀藥物疹合併嗜伊紅血症及全身症狀(drug rash (drug rash with eosinophilia and systemic symptoms)with eosinophilia and systemic symptoms),通常,通常是在使用藥物後是在使用藥物後33至至88周開始出現症狀,包含三個主要周開始出現症狀,包含三個主要特徵,發燒,皮膚炎和內部器官的侵犯,最常見且最特徵,發燒,皮膚炎和內部器官的侵犯,最常見且最嚴重的內部器官影響是肝臟,可能會併發猛爆性肝炎嚴重的內部器官影響是肝臟,可能會併發猛爆性肝炎(fulminant hepatitis)(fulminant hepatitis),而成為病人死亡的最常見原因,,而成為病人死亡的最常見原因,其他的還有心肌炎其他的還有心肌炎(myocarditis)(myocarditis),間質性肺炎,間質性肺炎(interstitial pneumonitis)(interstitial pneumonitis),間質性腎炎,間質性腎炎(interstitial (interstitial nephritis)nephritis),甲狀腺炎,甲狀腺炎(thyroiditis)(thyroiditis),甚至腦部有嗜伊,甚至腦部有嗜伊紅性血球浸潤等。紅性血球浸潤等。
Strontium-SafetyProtos
Osteoporos Int. 2008 Jul 4
Strontium-Safety
中文仿單中文仿單
Protos
-
2009/6/28
12
Review & GuidelineReview & Guideline
脊椎骨折療效Vertebral Fracture
30
40
redu
ctio
n
50 48%**
36%**
21%**
40%**37%**
Meta-analysis of Osteoporosis Therapies
*Data not representative of head-to-head trials; **significant vs. baselineMeta-analysis to evaluate magnitude of treatment effects on fractures and BMD based on randomized controlled trials of different osteoporosis therapiesAll data statistically significant vs. baselineAdapted from Cranney A et al Endocr Rev 2002;23:570–578.
0
20
% R
isk
10
Alendronate 8 trials
(n=9360)
Risedronate 5 trials
(n=2604)
Calcitonin 1 trial
(n=1108)
Raloxifene 1 trial
(n=6828)
Etidronate 9 trials
(n=1076)
%
髖部骨折療效 Hip FractureRecent meta-analysis of osteoporosis therapies
Red
uctio
n, %
30
40
50
60 55%
36%
Data not representative of head-to-head trials
HRT = hormone replacement therapy; RR = relative risk; CI = confidence intervala5% of patients received 20 mg/day; bResults from a single fracture end-point trial are summarized (n=2946); lack of fracture data from other ibandronate studies precluded meta-analysis.Results for FOSAMAX, HRT, and risedronate were significant.Adapted from Liberman UA, et al. Int J Clin Pract. 2006;60:1394–1400.FOSAMAX™ (alendronate) is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.
Ris
k R
FOSAMAX 5 or 10 mg/daya
HRT
RR 0.45 0.64 1.50 1.1 0.47(95%CI) (0.28, 0.71) (0.49, 0.84) (0.42. 5.33) (0.6, 1.9)N 6804 27,347 2929 7705 1245 1326
0
20
10
Ibandronateb
NotSignificant
Raloxifene Calcitonin
NotSignificant
NotSignificant
Teriparatide
NotSignificant
Summary of Evidence about Drugs and Fracture Risk
Ann Intern Med. 2008;149:404-415.
Postmenopausal Osteoporosis: Treatment Summary (ISCD 2007)
Documented Fracture ReductionDocumented Fracture Reduction CommentsComments
Spine Spine NonNon--
vertebral vertebral
Hip Hip
AntiAnti--ResorptivesResorptives
藥價 (daily)
AlendronateAlendronate 11 OO OO OOIbandronate Ibandronate 22 OO -- --Raloxifene Raloxifene 33 OO -- --Calcitonin Calcitonin 44 OO -- --Anabolic AgentsAnabolic AgentsTeriparatide Teriparatide 55 OO OO --
4 Chesnut CH, et al. Am J Med. 2000;109:2674 Chesnut CH, et al. Am J Med. 2000;109:267––276.276.5 Neer RM, et al. N Engl J Med. 2001;344:14345 Neer RM, et al. N Engl J Med. 2001;344:1434––14411441
1 Black DM, et al. Lancet. 1996;348:1535–1541.2 Chesnut CH, et al. J Bone Min Res. 2004;19:1241–1249.3 Ettinger B, et al. JAMA. 1999;282:637–645.
1048 (37)3343 (37) 1209 (43)3892 (139)
15766 (563)
-
2009/6/28
13
FOSAMAX PLUS 健保給付規定:
•• alendronatealendronate(如(如FosamaxFosamax):):(87/11/1(87/11/1、、91/7/191/7/1、、91/10/191/10/1、、93/8/1)93/8/1)
1.1. 需同時符合下列各項規定者:需同時符合下列各項規定者:a)a) 停經後婦女或停經後婦女或男性男性因骨質疏鬆症引起之脊椎壓因骨質疏鬆症引起之脊椎壓
迫性骨折或迫性骨折或髖骨骨折病患髖骨骨折病患(需於病歷詳細記(需於病歷詳細記迫性骨折或迫性骨折或髖骨骨折病患髖骨骨折病患(需於病歷詳細記(需於病歷詳細記載)。載)。(93/8/1)(93/8/1)
b)b) 血清肌酸酐血清肌酸酐(serum creatinine)(serum creatinine)小於或等於小於或等於1.6 1.6 mg/dlmg/dl的患者。的患者。
2.2. 本藥品不得併用本藥品不得併用calcitonincalcitonin、、raloxifeneraloxifene及活性維及活性維生素生素D3D3等藥物。等藥物。
FOSAMAX + Vitamin D=Bisphosphonates + Vitamin D
確保病患每週補充維生素 D‧增加鈣質吸收‧改善下肢功能‧預防跌倒
‧快速提升骨密度‧強效預防髖部及脊椎骨折
保密 防跌+
Osteoporosis Myths
•• Osteoporosis evaluation takes too much timeOsteoporosis evaluation takes too much time•• Prevention is ineffectivePrevention is ineffective•• Treatment is ineffectiveTreatment is ineffective
T t t i diffi ltT t t i diffi lt•• Treatment is difficultTreatment is difficult•• Other doctors will take the responsibilityOther doctors will take the responsibility•• Treatment impairs fracture healingTreatment impairs fracture healing•• Once a fracture has Occurred, it is too lateOnce a fracture has Occurred, it is too late------------------------------------------------------------------------------------------------------------------------------------J. KaufmanJ. Kaufman
•• Osteoporosis is commonOsteoporosis is common•• Osteoporosis is seriousOsteoporosis is serious
Fractures cause increased morbidity and mortalityFractures cause increased morbidity and mortality
•• Osteoporosis is easy to diagnose Osteoporosis is easy to diagnose •• Good treatments are availableGood treatments are available
Fracture risk can be reduced by about 50%Fracture risk can be reduced by about 50%
www.iscd.org
Thank You Thank You
-
2009/6/28
14
Primary and secondary prevention of osteoporotic fragility fractures infragility fractures in postmenopausal women
2008
Implementing NICE guidance
NICE technology appraisal guidance 160 and 161
UK NICE GuidelinePrimary Prevention初級預防
FOSAMAX (Alendronate)FOSAMAX (Alendronate)為首選藥物為首選藥物第二線第二線 Risedronate Risedronate 或或etidronateetidronateEvista (raloxifene)Evista (raloxifene)則不推薦則不推薦
Information about NICE technology appraisal guidance 161 Issue date: October 2008
UK NICE Guideline2nd Prevention次級預防
FOSAMAX (Alendronate)FOSAMAX (Alendronate)為首選藥物為首選藥物第二線第二線 Risedronate Risedronate 或或etidronateetidronate
Information about NICE technology appraisal guidance 161 Issue date: October 2008
IV BP後線使用
IV BP後線使用
New Standard of Osteoporosis Treatment :
-
2009/6/28
15
不可不知的維生素D
‧‧維生素,是身體無法自行充份合成的重要成份(維維生素,是身體無法自行充份合成的重要成份(維生素D就是要靠日曬或從外部攝取)生素D就是要靠日曬或從外部攝取)
‧‧以往以為台灣日照充足,維生素以往以為台灣日照充足,維生素DD不會到缺乏,也不會到缺乏,也不需要補充 但其實不用到維生素D缺乏 到不足不需要補充 但其實不用到維生素D缺乏 到不足不需要補充,但其實不用到維生素D缺乏,到不足不需要補充,但其實不用到維生素D缺乏,到不足的時候就會對骨骼健康有影響的時候就會對骨骼健康有影響
‧‧維生素D不足會加重骨質疏鬆維生素D不足會加重骨質疏鬆
‧‧偶爾的日曬,及適當的飲食,如果有需要,應該補偶爾的日曬,及適當的飲食,如果有需要,應該補充維生素D補充劑,才不會維生素D不足充維生素D補充劑,才不會維生素D不足
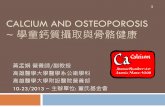
Vit D Inadequacy : Taiwan dataWe measured serum 25- hydroxyvitamin D (25-OHD), of 262 healthy Chinese women aged from 40 to 72 years
高達50%
•• Patients >60 years old Patients >60 years old hospitalized for hospitalized for nontraumatic fractures nontraumatic fractures S 25(OH)D 30S 25(OH)D 30
在另一個近期的研究指出,
ce (%
)
60708090
100N=548 98.9%98.0%95.6%92.7%
81.0%
68.4%
骨質疏鬆引起之骨折的住院病患,幾乎均有維生素 D 不足!!!!
*Vitamin D inadequacy was defined as serum 25(OH)D 60 years who were hospitalized with hip fractures to assess the prevalence of vitamin D inadequacy (measured by serum 25[OH]D).Adapted from Gallacher SJ et al Curr Med Res Opin 2005;21:1355–1361; Heaney RP Osteoporos Int 2000;11:553–555.
•• Serum 25(OH)D ≈30 Serum 25(OH)D ≈30 ng/ml ng/ml in 97.8% in 97.8%
•• Patients had no vitamin Patients had no vitamin D supplementationD supplementation
Cutoff points for 25(OH)D concentration (ng/ml)
Prev
alen
c
0
5040302010
60
-
2009/6/28
16
維生素維生素DD可幫助鈣質吸收可幫助鈣質吸收維生素D足夠下:
一星期喝9公升的牛奶,可以攝取到一星期所需的鈣
維生素D不夠下:
一星期要喝到15公升的牛奶,才可以攝取到一星期所需的鈣
Vitamin D
↑M l t th
Anti-Fracture Efficacy of Vitamin D
↑Muscle strength↑balance
↑lower extremity function
↓Fall risk> 20%
↑ BMD
↓ Fxs25%
Bischoff-Ferrari HA, Dawson-Hughes B, et al. JAMA 2004 and 2005
Relationship of 25(OH)D and Lower-Extremity Function
•• US survey US survey conducted in 4100 conducted in 4100 ambulatory adults ambulatory adults included in NHANES included in NHANES IIIIII
cond
s)
4.5Reference
range
Lower-extremity function improvement
•• 60 to 60 to ≥≥ 90 years90 years•• EightEight--foot walking foot walking
speed testspeed test•• LOWESS regression LOWESS regression
plotplot
NHANES=National Health and Nutrition Examination Survey; LOWESS=locally weighted regression plotAdapted from Bischoff-Ferrari HA et al Am J Clin Nutr 2004;80:752–758.
Serum 25(OH)D (ng/ml)0 8 16 32 48 64
Wal
k tim
e (s
ec
24 40 563.5
4.0
Effect of Vitamin D and Calcium Supplementation on Risk of Falling
•• 122 women122 women•• Age: 63Age: 63––99 years99 years•• Randomized, doubleRandomized, double--blind, blind,
controlled trialcontrolled trial•• Calcium 1200 mg/dayCalcium 1200 mg/day 0.8
1.0
1.2
Reduction in falls
p=0.01
•• Calcium 1200 mg/day Calcium 1200 mg/day + vitamin D 800 IU/day+ vitamin D 800 IU/day
•• 1212--week durationweek duration•• Mean serum 25(OH)D Mean serum 25(OH)D
12 ng/ml at baseline12 ng/ml at baseline•• Women living in longWomen living in long--term term
care unitscare units
Adapted from Bischoff HA et al J Bone Miner Res 2003;18:343–351.
Calcium only
(n=44)
Calcium + vitamin D
(n=45)
Fall
risk
0.0
0.2
0.4
0.6–49%
Vitamin D and Falls; Meta-Analysis
Pfeifer, et al, 2000Pfeifer, et al, 2000 (n=137)(n=137) 0.47 (0.200.47 (0.20––1.10)1.10)Bischoff, et al, 2003Bischoff, et al, 2003 (n=122)(n=122) 0.68 (0.300.68 (0.30––1.54)1.54)Gallagher, et al, 2001Gallagher, et al, 2001 (n=246)(n=246) 0.53 (0.320.53 (0.32––0.88)0.88)Dukas, et al, 2004Dukas, et al, 2004 (n=378)(n=378) 0.69 (0.410.69 (0.41––1.16)1.16)
Primary analysisOdds ratio(95% CI)
Favorsvitamin D
Favorscontrol
Gallagher, et al. J Clin Endocrinol Metab, 86:3618–3628, 2001 Dukas L, et al. J Am Geriatr Soc. 2004;52:230–236, 2004Graafmans, et al. Am J Epidemiol, 143:1129–1136, 1996
( )( ) (( ))Graafmans, et al, 1996Graafmans, et al, 1996 (n=354)(n=354) 0.91 (0.590.91 (0.59––1.40)1.40)Pooled (uncorrected)Pooled (uncorrected) (n=1237)(n=1237) 0.69 (0.530.69 (0.53––0.88)0.88)Pooled (corrected)Pooled (corrected) (n=1237)(n=1237) 0.78 (0.640.78 (0.64––0.92)0.92)
0.1 0.5 1.0 5.0 10.0
Odds Ratio
22%
Adapted from Bischoff-Ferrari. JAMA, 291:1999–2006, 2004Pfeifer, et al. J Bone Miner Res. 2000;15:1113–1118, 2005Bischoff, et al. J Bone Miner Res,18:343–351, 2003
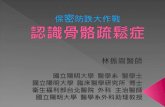
Vitamin D Supplementation Decreases Fracture Risk
•• FiveFive--year randomized, year randomized, doubledouble--blind, controlled blind, controlled trialtrial
•• N=2686N=2686
tive
risk
arm
, spi
ne)
–33%
p=0.02
0.8
1.0
1.2
•• Age 65Age 65––85 years85 years•• Vitamin D = Vitamin D = 100,000 IU once 100,000 IU once
every four months every four months (equivalent to 800 IU/day)(equivalent to 800 IU/day)
•• Men and women living Men and women living in the communityin the community
•• Composite fracture Composite fracture endpointendpoint
Adapted from Trivedi D et al BMJ 2003;326:469.
Frac
ture
rela
t(h
ip, w
rist,
fore
a
Untreated(n=1341)
Treated(n=1345)
0.0
0.2
0.4
0.6
-
2009/6/28
17
Vitamin D and Calcium Supplementation Reduce Fracture Risk
•• PopulationPopulation--based, based, threethree--year, Danish year, Danish intervention studyintervention studyEld l itEld l it l
ativ
e R
isk* –22%
p=0.025
0 6
0.8
1.0
1.2
•• Elderly, communityElderly, community--dwelling population dwelling population
•• Age: Age: εε66 years66 years•• Vitamin D=400 IU/dayVitamin D=400 IU/day•• Calcium=1000 mg/dayCalcium=1000 mg/day
*Humerus, distal forearm, vertebral column, pelvis, cervical femur, intertrochanteric femurAdapted from Larsen ER et al. J Bone Mineral Res 2004;19:370–378.
Frac
ture
Re
Controls(n=1273)
Vitamin D + calcium(n=2983)
0.0
0.2
0.4
0.6
Vitamin D 700 to 800 IU Daily Reduced Fracture Risk
Hip Fracture Nonvertebral Fracture
Chapuy, et al, 2002a
Favors Vitamin D Favors Control
Pfeifer, et al, 2000d
Ch t l 1994b
Favors Vitamin D Favors Control
Chapuy, et al, 2002a
In a subgroup of a meta-analysis,
0.2 5.0
Relative Risk (95% CI)0.5 1.0
Chapuy, et al, 1994b
Trivedi, et al, 2003c
Pooled
0.2 5.0
Relative Risk (95% CI)0.5 1.0
Chapuy, et al, 1994b
Trivedi, et al, 2003c
Pooled
Dawson-Hughes, et al, 1997b
CI = confidence intervala24 mo; b36 mo; c60 mo; d12 moAdapted from Bischoff-Ferrari HA, et al. JAMA. 2005; 293:2257–2264.
26% 23%
所有的骨鬆研究都是在確保病患有補充維生素 D下進行
Pharmacologic Pharmacologic TherapyTherapy
Fracture TrialsFracture Trials Vitamin DVitamin D
AlendronateAlendronate Lancet 1996; 348: 1535Lancet 1996; 348: 1535––4141 Vit D 250IUVit D 250IU
RaloxifeneRaloxifene JAMA. 1999;282:637JAMA. 1999;282:637––645.645. Vit D 400Vit D 400--600IU600IU
TeriparatideTeriparatide N Engl J Med. 2001;344:1434N Engl J Med. 2001;344:1434––14411441 Vit D 1200IUVit D 1200IU
IbandronateIbandronate J Bone Min Res. 2004;19:1241J Bone Min Res. 2004;19:1241––1249.1249.
Vit D 400IUVit D 400IU
ZoledronateZoledronate N Engl J Med 2007;356:1809N Engl J Med 2007;356:1809--22.22. Vit D 400Vit D 400--1200IU1200IU
StrontiumStrontium N Engl J Med 2004;350:459N Engl J Med 2004;350:459--68.68. Vit D 400Vit D 400--800IU800IU
Vitamin D and Fractures
Vitamin D deficiencyVitamin D deficiencyMuscle weakness and increased fall riskMuscle weakness and increased fall riskBone loss and fracture riskBone loss and fracture riskD l f t h liD l f t h liDelays fracture healingDelays fracture healingBlunts BMD and fracture response to Blunts BMD and fracture response to bisphosphonate therapybisphosphonate therapy
To reduce falls and fractures, daily intake of at least To reduce falls and fractures, daily intake of at least 800 IU vitamin D800 IU vitamin D33 is requiredis required
Adami S et al. Osteoporos Int. 2008 Jun 13. [Epub ahead of print].
若Vitamin D缺乏即使使用治療藥物也沒有療效
Vitamin D with alendronate in one weekly pill optimises current care最新的治療趨勢是-直接在每週一次的治療藥物當中添加維生素D
•• Because of the high prevalence of vitamin D Because of the high prevalence of vitamin D inadequacyinadequacy
•• Because vitamin D inadequacy causes secondary Because vitamin D inadequacy causes secondary hyperparathyroidism, bone loss, falls and fractures hyperparathyroidism, bone loss, falls and fractures
•• Because adherence to daily/multiple pills is poorBecause adherence to daily/multiple pills is poor•• Because RCT on antiBecause RCT on anti--resorptive agents included resorptive agents included
Vitamin D (and calcium) supplementsVitamin D (and calcium) supplements•• Because alendronate + Vitamin D prevents worsening Because alendronate + Vitamin D prevents worsening
of vitamin D inadequacy and Alendronate has proven of vitamin D inadequacy and Alendronate has proven antianti--fracture efficacyfracture efficacy
-
2009/6/28
18
Every day there is more interesting literature about the potential extra-skeletal benefits of Vitamin D
2525--Hydroxyvitamin D and Risk of Hydroxyvitamin D and Risk of Myocardial Myocardial InfarctionInfarction in Men: A Prospective Studyin Men: A Prospective StudyArch Intern Med 2008;168 1174Arch Intern Med 2008;168 1174--11801180
Vitamin D and Vitamin D and prostate cancerprostate cancer riskrisk----a less sunny a less sunny outlook? outlook? J Natl Cancer Inst 2008 Jun 4;100(11):759J Natl Cancer Inst 2008 Jun 4;100(11):759--6161
Review: vitamin D, immunity and Review: vitamin D, immunity and lupuslupus..Lupus. 2008;17(1):6Lupus. 2008;17(1):6--10. Review. 10. Review.
Vitamin D as a potential modifier of Vitamin D as a potential modifier of diabetes riskdiabetes risk..Nat Clin Pract Endocrinol Metab. 2008 Nat Clin Pract Endocrinol Metab. 2008
Apr;4(4):182Apr;4(4):182--3.3.
Vitamin D as an analgesic for patients with type Vitamin D as an analgesic for patients with type 2 diabetes and 2 diabetes and neuropathic painneuropathic pain..Arch Intern Med. 2008 Apr Arch Intern Med. 2008 Apr
Back-up slides
5-2
Bisphosphonates are the Major Class of Osteoporosis Treatment:
BisphosphonatesPTH
Nature Review-Drug Discovery September 2008 Vol 7 No 9
SERMOthers
(StrontiumCalcitonin)
5.5.3.6.2 ibandronic acid 3mg/3ml (如Bonviva 3mg/3ml solution for injection)(97/8/1)
限同時符合下列各項規定:
(1)停經後婦女因骨質疏鬆症(BMD T-score < -2.5 SD) 引起 之脊椎壓迫性骨折(需於病歷詳細記載)。
(2)血清肌酸酐(serum creatinine)小於或等於2.3mg/dl的患者。
(3)本藥品不得併用calcitonin、raloxifene及活性維生素D3等藥物。