
뇌졸중 pdf 130227 - stroke.or.krstroke.or.kr/image/CRCS CPG 개정 (ICH)20140625.pdf ·...
334
Transcript of 뇌졸중 pdf 130227 - stroke.or.krstroke.or.kr/image/CRCS CPG 개정 (ICH)20140625.pdf ·...


뇌졸중진료지침개정판


3
CLINICAL RESEARCH CENTER FOR STROKE
뇌졸중은우리나라뿐아니라전세계적으로가장중요한사망원인이며, 성인에서장애의가장중요
한원인질환이다. 2005년통계에의하면전세계적으로뇌졸중으로인한사망자가약5백8십만명으
로추정된다.
뇌졸중은일단발생하면사망또는심각한장애를유발할수있다. 따라서적극적인일차예방이다
른어떤질환보다강조되어야하며, 뇌졸중이발생한경우적절한치료를통해뇌졸중으로인한장
애를최소화해야한다. 많은연구를통해과학적근거가분명한효과적인예방및급성기치료법들이
개발되었으며, 이러한치료법들을임상진료에적절하게적용하는것이뇌졸중으로인한질병부담
을줄일수있는가장좋은방법이다.
뇌졸중임상진료지침은과학적근거를체계적으로정리하여임상의들이현장진료에서환자의치
료를결정하는데도움을주기위한것이다. 많은나라들이각나라의실정에맞게다양한형태의뇌
졸중진료지침을개발하여보급하고있다. 미국이나유럽등의의료선진국뿐아니라가까운일본
및우리나라보다의료환경이열악한동남아국가들도뇌졸중진료지침이보급되어있다. 나라마다
의료시스템에차이가있어외국의진료지침을우리나라에그 로적용하는경우문제점이발생할
수있어, 뇌졸중임상연구센터에서2009년처음으로뇌졸중진료지침1판을발간하 다. 이후뇌졸
중임상연구센터는새로운연구결과들의과학적근거들을반 하여뇌졸중진료지침을개정하는
작업을해오고있다. 향후우리나라의인구노령화로예상되는급격한뇌졸중증가를고려하면효
율적인뇌졸중진료를위하여우리나라상황에맞는뇌졸중임상진료지침을지속적으로개발하여
보급하고진료현장에서적용되게하는과정(implementation)들이매우중요하다.
본진료지침은‘보건복지부보건의료연구개발사업’의지원을받아외국의자료들을정리한후국
내의의료환경을고려하여작성되었다. 진료지침1판이나올때에는우리나라의자료들이거의반
되지않았지만, 본개정판에서는 우리나라의연구결과들이일부추가되었으며, 최근뇌졸중분
야의임상연구들이활발하게진행되고있어향후개정본에는보다많은국내의자료들이반 될것
으로기 된다.
세계보건기구(WHO)는뇌졸중을‘뇌혈관장애(뇌혈관의폐쇄: 뇌허혈, 뇌경색; 뇌혈관의파열: 뇌출
혈)로인하여갑자기국소신경학적장애또는의식장애가발생하여 24시간이상지속하는경우 (A
focal (or at times global) neurological impairment of sudden onset, and lasting more than 24 hours (or
leading to death), and of presumed vascular origin)’라고정의하고있다. 일과성뇌허혈은24시간이내

4
CLINICAL RESEARCH CENTER FOR STROKE
에신경학적장애가회복되는경우이다.
우리나라의경우뇌졸중급성기치료및뇌졸중위험인자조절향상으로뇌졸중으로인한연간사망
이21세기첫10년동안약28.3%나감소하 다. 그러나아직도뇌졸중은주요사망원인이며, 2010년
통계청사망통계에의하면약26,500명이뇌졸중으로사망하여 (인구10만명당53.2명) 20분마다1명
이뇌졸중으로사망하고있다. 뇌졸중으로인한사망은전체사망의약10%를차지하고있고, 암에이
어사망원인2위를차지하고있지만, 단일장기질환으로는사망원인1위를차지하고있다. 우리나
라의뇌졸중사망은다른OECD 국가들과비교하여도아직높은수준이다.
다행히뇌졸중사망률은줄고있지만, 우리나라의인구고령화로인한전체뇌졸중발생은증가하고
있다. 뇌졸중발생률에관하여우리나라의경우인구집단을 상으로발병률을측정한코호트연구
는없다. 2004년심사평가원청구자료와사망통계를이용하여추정한2004년뇌졸중발생은연간약
105,000명으로 5분마다뇌졸중이발생하고있다. 뇌졸중발생률은연간인구 10만명당 216건(남자
213건, 여자220건)이며, 나이가증가할수록급격하게증가하여, 44세이하에서는연간10만명당20건
으로낮지만, 85세이상에서는연간10만명당3,297건이었다. 전체뇌졸중발병건수는여성이높았지
만이는여성이남성에비해노령의인구가많은인구구조의차이에의한것이며연령별로세분하면
10만명당발병률은모든연령 에서남성이여성보다높았다. 현재인구노령화추세를고려하면
2030년에는현재보다뇌졸중발생이약3배증가할것으로예상되어이에 한 책이시급하다.
뇌졸중의유형별로는심평원청구자료의뇌졸중입원을분석한결과2009년에는전체뇌졸중중허
혈성뇌졸중이76.1%, 출혈성뇌졸중이23.9%를차지하여, 2000년의 허혈성뇌졸중64.7%, 출혈성뇌
졸중35.3%에비하여허혈성뇌졸중의비율이점차증가하고있다. 허혈성뇌졸중의유형에 한전
체뇌졸중환자의자료는없다. 그러나우리나라주요 학병원이참여하고있는36,000 명이상의환
자들을분석한연구에의하면 혈관동맥경화에의한뇌졸중의분율이36.1%로가장높으며, 소혈관
폐색(25.4%), 그리고심장탓뇌졸중(17.1%) 순이다. 특이한것은최근에들어서심장탓뇌졸중이점차
증가하여전체허혈성뇌졸중의약 20%를차지하고있으며, 소혈관폐색에의한뇌졸중은감소하는
추세를보이고있다.
현재국내뇌졸중유병률은약 795,000명으로추정되고있는데, 2005년국민건강 양조사에의하면
19세이상의성인에서의사에의해진단된적이있는뇌졸중평생유병률은인구1,000명당15.9명(남
자16.44명, 여자15.37명)으로나타났다. 연령별로는40 6.53명, 50 24.26명, 60 57.96명이며, 70세
이상에서는67.45명으로50 이후유병률이급격하게증가하 다. 인구고령화로인한뇌졸중발생
증가와사망률감소로인하여뇌졸중후유장애를앓고있는사람들이증가하고있으며이는향후막
한사회경제적부담이될것이다. 2005년자료를바탕으로추정한뇌졸중으로인한경제적부담은
약3조7천억을상회할것으로평가되었다. 그리고세계보건기구에서전세계질병부담을장애보정인
생손실년(DALY lost, disability-adjusted life years lost)으로측정한보고서에의하면우리나라는2002년
뇌졸중으로약344,000년의건강한인생이손실되고있는것으로평가되었다.

5
CLINICAL RESEARCH CENTER FOR STROKE
본진료지침은뇌졸중의일반적인상황에 하여과학적근거가있는보편적인표준진료행위를제
시함으로써급성기와만성기의뇌졸중진료를담당하는신경과, 신경외과, 재활의학과, 내과, 가정
의학과및혈관중재시술을담당하는의사의판단에도움을주는것이목적이고, 개개환자에 한
진료행위는담당의사가환자의여러상황을고려하여최종적으로결정하여야한다. 따라서이진료
지침은현장에서진료를담당하는의료인의의료행위를제한하거나, 건강보험심사의기준으로삼
고자하는것이아니다. 더욱이특정한임상적상황에놓인환자에시행된진료행위에 한법률적
판단을하는데이용되어서는안된다.
1) 진료지침의항목결정
본뇌졸중표준진료지침은뇌졸중의일차예방과위험인자관리, 급성기뇌졸중치료, 뇌졸중의이
차예방등크게세가지주제로구성된다. 각각의주제별로기술할세부항목은2006년5월에5명으
로구성된“진료지침개발태스크포스팀(Task Force team)”에의해선정되었고, 진료지침개발운
위원회의승인을거친후집필위원회로전달되어재검토를거쳐수정, 보완되었다. 각주제별로구
성된집필위원회는태스크포스팀이도출한항목을 상으로국내현실을고려하여최종집필항목
을결정하 다.
2) 진료지침의기술방법의결정
진료지침개발태스크포스팀은총 7회의회의를거쳐진료지침개발안내서(CPG development
manual)를발간하 다. 기존에발표된각국의뇌졸중진료지침을모두검토한후, 그내용의충실성
을근거로가장수준이높은 4개의진료지침, 즉 American Stroke association(ASA), European Union
본진료지침은성인뇌졸중의일차예방, 급성기치료및재활, 이차예방에관한사항을다루었다. 소
아뇌졸중과자세한수술적기법은본진료지침에서다루지않았다. 뇌졸중중에서허혈성뇌졸중을
중심으로언급을하 으며, 출혈성뇌졸중중에서는뇌실질내출혈이포함되었으나지주막하출혈은
다루지않았다. 단비파열성뇌동맥류는일차예방분야에포함하여다루고있다.

6
Stroke Initiative (EUSI) version, Scottish Intercollegiate Guidelines Network (SIGN), Royal College of
Physician (RCP) version 을선정하 다. 본진료지침의개발은기존에발표된네개의진료지침을기반
으로하여, 각진료지침에서기술된근거와권고사항을분석, 요약하는과정을통해개발의기본구조
를완성하 다. 즉각진료지침별권고사항을정리하 고, 권고의근거로삼는문헌을별도로검색,
정리하 다. 국내진료지침의권고수준과근거수준은 US Agency for Health Care Policy and
Research(현재는Agency for Healthcare Research and Quality, AHRG)에서1993년에제안한방법으로재
정리하 다. 각진료지침집필위원회별로가장나중에발표된진료지침에서명시하고있는참고문
헌의검색기간이후에발표된문헌에 하여추가검색작업을진행하여, 근거사항에 한최신의견
을반 하고자하 다. 2009년에발표된뇌졸중진료지침초판은2007년6월30일까지발표된근거를
반 하여작성되었다. 이후주제에따라2007년6월30일이후발표된주요근거들을반 하여진료
지침의일부를개정하 다. 2012년뇌졸중진료지침개정판에서는뇌졸중일차예방분야에서‘무증
상경동맥협착’과‘아스피린의뇌졸중일차예방효과’를개정하 고, ‘뇌졸중인식도’를추가하
으며, 뇌졸중이차예방분야에서는‘‘비심장탓색전성뇌졸중또는일과성뇌허혈의항혈전치료’와
‘두개강외경동맥협착’을개정하 다. 2013년뇌졸중진료지침개정판에서는뇌졸중일차예방분야
에서‘심방세동’을개정하 고, ‘비파열뇌동맥류의선별검사’와‘비파열뇌동맥류의치료’를추가
하 으며, 급성기뇌졸중진료분야에서는‘정맥내혈전용해술’과‘동맥내혈전용해술’을개정하
다. 개정또는추가된주제들에 해서는보다구체적으로기술하여논문으로관련학회지에발표를
하 다. 국내뇌졸중진료지침에는국내의권고안뿐아니라외국의권고안도소개하여독자들이비
교할수있도록하 다.각진료지침들은권고수준과근거수준을정의하는방법에많은차이가있
다. 2009년초판에서는독자들의혼란을피하고국내권고안과통일성을유지하기위하여외국진
료지침의근거수준과권고수준을국내진료지침에서사용하고있는방식으로재정리하 다. 그러
나외국진료지침권고안의권고수준과근거수준을국내방식으로변경하는데있어모호한경우가
있을수있으며, 원문의내용을충실히반 하는것이더바람직하다는판단하에개정진료지침부
터는국내권고안방식으로변경하지않고원래의근거수준과권고수준을그 로소개하 다. 또
한진료지침의일관성을유지하기위하여뇌졸중임상연구센터운 위원회의결정에따라제1판
에소개된외국의권고안들의근거수준과권고수준을원문방식으로다시수정하 다.
3) 진료지침집필위원의선정
진료지침운 위원회는뇌졸중의일차예방과위험인자관리, 급성기뇌졸중치료, 뇌졸중의이차
예방등크게세가지주제별로각각한명의책임자를선정하 고, 각주제책임자가지역과세부전
CLINICAL RESEARCH CENTER FOR STROKE

7
CLINICAL RESEARCH CENTER FOR STROKE
진료지침의개발과정은발표된문헌들을체계적으로검토하여근거들을종합한후전문가들이근
거수준(level of evidence)과권고수준(grade of recommendation)을결정하여권고안을제시한다. 근거
공을감안하여집필위원들을추천, 진료지침운 위원회의승인을얻어집필위원회(Writing
committee)를구성하 다.
4) 집필과정
각주제별로구성된집필위원회는주제책임자의주도하에세부항목에 한기술을완료하 다.
진료지침집필위원들간에의견이일치하지않을때는토론을거쳐다수의의견으로합의안을도
출하 다. 주제책임자의일차검토를거치고내부교정을시행하여진료지침의일차완성본을운
위원회에제출하 다.
5) 운 위원회의검토
제출된진료지침의일차완성본은운 위원회에서논의와검토를거친후에, 일부수정요구사항
을반 하여수정본진료지침이제작되었다.
6) 외부전문가의검토
제출된진료지침은운 위원회에서추천된뇌졸중유관학회등연구진이외의외부전문가들에
게검토를의뢰하 고, 지적된사항에 하여내부적인의견수렴과보완을거친후최종정리가완
료되었다.
7) 진료지침개정
현재뇌졸중임상진료지침은운 위원회위원과집필진들이새로운주요연구결과들을지속적으
로모니터링하고개정이필요한주제를선정하고있다. 운 위원회는최종적으로개정의필요성
유무를결정, 집필책임자및집필진들을선정하고있으며, 진료지침의개정은지침개발태스크포
스팀에서이미마련한임상진료지침개정프로토콜을이용하여실시하고있다. 개정된주제들은
본진료지침에포함될뿐아니라개정배경이되는근거들에 한세부내용및변경된권고사항
에 해개별적인논문으로도발표하고있다.

8
CLINICAL RESEARCH CENTER FOR STROKE
Grade Recommendation
A Required - at least one randomized controlled trial as part of the body of literature of overall (Evidence Levels Ia, Ib) good quality and consistency addressing specific recommendation.
B Required - availability of well conducted clinical studies but no randomized clinical trials (Evidence Levels IIa, IIb, III) on the topic of recommendation.
C Required - evidence obtained from expert committee reports or opinions and/or clinical
(Evidence level IV) experiences of respected authorities. Indicates absence of directly applicable clinical
studies of good quality.
GPP(Good practice points)
Recommended best practice based on the clinical experience of the guideline development group.
본뇌졸중임상진료지침은 한민국보건복지부보건의료연구개발사업의지원에의하여이루어진
것이다(A102065). 이사업은각질환별임상연구를활성화하기위한목적으로보건복지부에서추진
한임상연구센터프로젝트의일부이다.
Level Type of Evidence
Ia Evidence obtained from meta-analysis of randomized controlled trials.
Ib Evidence obtained from at least one randomized controlled trial.
IIa Evidence obtained from at least one well-designed controlled study without randomization.
IIb Evidence obtained from at least one other type of well-designed quasi-experimental study.
III Evidence obtained from well-designed non-experimental descriptive studies, such as comparative studies,
correlation studies and case studies.
IV Evidence obtained from expert committee reports or opinions and/or clinical experiences of respected authorities.
수준은특정의료행위가어느정도의과학적근거를가지고있는지를나타내는것이며, 권고수준은
이러한의료행위를어느정도의강도로권고할것인가를나타내는것이다. 본위원회에서채택한근
거수준과권고수준은US Agency for Health Care Policy and Research에서제한한방식에기반을두고
아래의표와같이정의하 다.

9
CLINICAL RESEARCH CENTER FOR STROKE
뇌졸중임상연구센터는서울 학교병원윤병우교수를연구책임자로하여6개의세부과제로2006년
5월부터 9년을총연구기간으로하여시작되었다. 본사업의목표는한국의뇌졸중임상지료지침을
지속적으로보급하여임상현장에활용될수있는기반을마련하는것이다.
뇌졸중임상연구센터의 운 위원회와집필위원회는 진료지침의개발에있어본사업외에다른어
떤연구비혹은현물을제공받지않았으며정부기관, 제약회사, 병원단체및다른이익단체의 향을
받지않았음을밝혀둔다.
2013년2월
뇌졸중임상연구센터
※본진료지침은아래학회의인준을받았음. (2013년2월4일기준)
- 한뇌졸중학회 - 한신경과학회
- 한노인신경의학회 - 한뇌혈관외과학회
- 한뇌혈관내수술학회 - 한신경중재치료의학회
※본진료지침은뇌졸중임상연구센터홈페이지(http://www.stroke-crc.or.kr)를통해서도확인할수있음.

10
CLINICAL RESEARCH CENTER FOR STROKE
■총괄연구책임자 :윤병우(서울대학교의과대학신경과학교실)
■진료지침개발태스크포스팀(Task Force team)
홍근식(인제대학교의과대학신경과학교실)
권순억(울산대학교의과대학신경과학교실)
이승훈(서울대학교의과대학신경과학교실)
고상배(서울대학교의과대학신경과학교실)
최혜연(연세대학교의과대학신경과학교실)
■진료지침운영위원회
[1세부과제] 윤병우(서울대학교의과대학신경과학교실) 홍근식(인제대학교의과대학신경과학교실)
조용진(인제대학교의과대학신경과학교실) 이승훈(서울대학교의과대학신경과학교실)
[2세부과제] 허지회(연세대학교의과대학신경과학교실)
[3세부과제] 권순억(울산대학교의과대학신경과학교실)
[4세부과제] 오창완(서울대학교의과대학신경외과학교실)
[5세부과제] 배희준(서울대학교의과대학신경과학교실) 박종무(을지대학교의과대학신경과학교실)
[6세부과제] 이병철(한림대학교의과대학신경과학교실) 유경호(한림대학교의과대학신경과학교실)
■진료지침집필위원회(배열은가나다순서임)
[급성기진료]
▶책임자 나정호(인하대학교의과대학신경과학교실)
▶참여위원 강동화(울산대학교의과대학신경과학교실) 고상배(서울대학교의과대학신경과학교실)
김경문(성균관대학교의과대학신경과학교실) 김동억(동국대학교의과대학신경과학교실)
김성현(서울대학교의과대학영상의학과학교실) 김정은(서울대학교의과대학신경외과학교실)
박현선(인하대학교의과대학신경외과학교실) 손성일(계명대학교의과대학신경과학교실)
이수주(을지대학교의과대학신경과학교실) 정상욱(동국대학교의과대학신경과학교실)
정슬기(전북대학교의과대학신경과학교실) 조아현(가톨릭대학교의과대학신경과학교실)
최혜연(연세대학교의과대학신경과학교실) 허성혁(경희대학교의과대학신경과학교실)
[일차예방]
▶책임자 홍근식(인제대학교의과대학신경과학교실)
▶참여위원 강규식(을지대학교의과대학신경과학교실) 구자성(가톨릭대학교의과대학신경과학교실)
김한영(건국대학교의과대학신경과학교실) 박종무(을지대학교의과대학신경과학교실)
손영제(서울대학교의과대학신경외과학교실) 조용진(인제대학교의과대학신경과학교실)
한상원(인제대학교의과대학신경과학교실)
[이차예방]
▶책임자 유경호(한림대학교의과대학신경과학교실)
▶참여위원 고임석(국립의료원신경과) 권배주(서울대학교의과대학영상의학과학교실)
권순억(울산대학교의과대학신경과학교실) 권형민(서울대학교의과대학신경과학교실)
김요식(원광대학교의과대학신경과학교실) 박석규(원자력병원신경외과)
오미선(한림대학교의과대학신경과학교실) 이경복(순천향대학교의과대학신경과학교실)
이승훈(서울대학교의과대학신경과학교실) 이주헌(한림대학교의과대학신경과학교실)
이준(영남대학교의과대학신경과학교실) 정 산(한림대학교의과대학신경과학교실)
차재관(동아대학교의과대학신경과학교실) 한문구(서울대학교의과대학신경과학교실)
뇌졸중진료지침개발참여연구자명단 (초판: 2009년10월현재)

11
CLINICAL RESEARCH CENTER FOR STROKE
■진료지침집필위원회(배열은가나다순서임)
[급성기진료]
▶책임자 나정호(인하대학교의과대학신경과학교실)
▶참여위원 고상배(서울대학교의과대학신경과학교실) 권순억(울산대학교의과대학신경과학교실)
권오기(서울대학교의과대학신경외과학교실) 김대현(동아대학교의과대학신경과학교실)
박희권(인하대학교의과대학신경과학교실) 배희준(서울대학교의과대학신경과학교실)
오창완(서울대학교의과대학신경외과학교실) 유경호(한림대학교의과대학신경과학교실)
윤병우(서울대학교의과대학신경과학교실) 이병철(한림대학교의과대학신경과학교실)
이수주(을지대학교의과대학신경과학교실) 이 준(영남대학교의과대학신경과학교실)
조경희(고려대학교의과대학신경과학교실) 조아현(가톨릭대학교의과대학신경과학교실)
허지회(연세대학교의과대학신경과학교실) 홍근식(인제대학교의과대학신경과학교실)
[일차예방]
▶책임자 홍근식(인제대학교의과대학신경과학교실)
▶참여위원 강규식(을지대학교의과대학신경과학교실) 강현승(서울대학교의과대학신경외과학교실)
구자성(가톨릭대학교의과대학신경과학교실) 권순억(울산대학교의과대학신경과학교실)
김대원(원광대학교의과대학신경외과학교실) 김성림(가톨릭대학교의과대학신경외과학교실)
김영서(한양대학교의과대학신경과학교실) 김한영(건국대학교의과대학신경과학교실)
나정호(인하대학교의과대학신경과학교실) 박상순(서울의료원신경과)
박석규(순천향대학교의과대학신경외과학교실) 박인성(경상대학교의과대학신경외과학교실)
박종무(을지대학교의과대학신경과학교실) 배희준(서울대학교의과대학신경과학교실)
서대희(관동대학교의과대학신경외과학교실) 송 영(서울보훈병원신경외과)
신승훈(한림대학교의과대학신경외과학교실) 오창완(서울대학교의과대학신경외과학교실)
유경호(한림대학교의과대학신경과학교실) 유승훈(울산대학교의과대학신경외과학교실)
윤병우(서울대학교의과대학신경과학교실) 이병철(한림대학교의과대학신경과학교실)
이승훈(서울대학교의과대학신경과학교실) 전 평(성균관대학교의과대학영상의학과학교실)
조용진(인제대학교의과대학신경과학교실) 한상원(인제대학교의과대학신경과학교실)
허지회(연세대학교의과대학신경과학교실) 홍승철(성균관대학교의과대학신경외과학교실)
[이차예방]
▶책임자 유경호(한림대학교의과대학신경과학교실)
▶참여위원 권순억(울산대학교의과대학신경과학교실) 권오기(서울대학교의과대학신경외과학교실)
김민기(서울의료원신경과) 김성림(가톨릭대학교의과대학신경외과학교실)
나정호(인하대학교의과대학신경과학교실) 박인성(경상대학교의과대학신경외과학교실)
박태환(서울의료원신경과) 박현선(인하대학교의과대학신경외과학교실)
배희준(서울대학교의과대학신경과학교실) 오미선(한림대학교의과대학신경과학교실)
오창완(서울대학교의과대학신경외과학교실) 오형근(순천향대학교의과대학신경과학교실)
윤병우(서울대학교의과대학신경과학교실) 이병철(한림대학교의과대학신경과학교실)
정근화(서울대학교의과대학신경과학교실) 허지회(연세대학교의과대학신경과학교실)
홍근식(인제대학교의과대학신경과학교실)
뇌졸중진료지침개발개정판참여연구자명단 (개정판: 2013년2월현재)


CONTENTS
13
1.1조절할수없는위험인자 Non-modifiable risk factors 21
1.1.1 나이 (Age) 21
1.1.2 성 (Sex) 22
1.1.3 출생시저체중 (Low birth weight) 23
1.1.4 유전적요인 (Genetic factor) 24
1.2입증된조절가능한위험인자 Well-documented and modifiable risk factors 26
1.2.1 고혈압 (Hypertension) 26
1.2.2 흡연 (Smoking) 29
1.2.3 당뇨병 (Diabetes) 31
1.2.4 심방세동 (Atrial fibrillation) 2012.12 개정 34
1.2.5 기타심장질환 (Other cardiac conditions) 44
1.2.6 이상지질혈증 (Dyslipidemia) 46
1.2.7 무증상경동맥협착 (Asymptomatic carotid stenosis) 2011.10 개정 51
1.2.8 폐경후호르몬치료 (Postmenopausal hormonal therapy) 61
1.2.9 식이와 양 (Diet and nutrition) 63
1.2.10 신체활동 (Physical activity) 65
1.2.11 비만 (Obesity) 67
1.3조절가능한잠재적인위험인자Less well-documented or potentially modifiable risk factors 70
1.3.1 사증후군 (Metabolic syndrome) 70
1.3.2 음주 (Alcohol) 72
1.3.3 약물남용 (Drug abuse) 74
1.3.4 경구용피임제 (Oral contraceptive) 75
1.3.5 수면중호흡장애 (Sleep-disordered breathing) 77
1.3.6 편두통 (Migraine) 79
1.3.7 고호모시스틴혈증 (Hyperhomocysteinemia) 81
1.3.8 과다응고증 (Hypercoagulability) 84
1.3.9 염증 (Inflammation) 86
1.3.10 감염증 (Infection) 88
1.3.11 무증상열공성병변및백색질변성 (Asymptomatic lacune or white matter change) 90
1.4아스피린의뇌졸중일차예방효과 Aspirin for primary stroke prevention 2011.10 개정 92
1.5뇌졸중인식도Public awareness and education 2012.5신규 97
1.6비파열뇌동맥류Unruptured intracranial aneurysm 100
1.6.1 비파열류뇌동맥류의선별검사 (Screening of unruptured intracranial aneurysm) 2013.1 신규 100
1.6.2 비파열류뇌동맥류의치료 (Treatment of unruptured intracranial aneurysm) 2013.1 신규 103
차례
1 뇌졸중일차예방 Primary prevention of stroke 17

14
CONTENTS
2.1 진료체계Organization 117
2.1.1 내원전환자관리및처치: 응급의료서비스/119 (Prehospital management 117
and field treatment: EMS/119)
2.1.2 뇌졸중전문치료실과뇌졸중센터 (Stroke unit and stroke center) 121
2.2 급성기평가Acute evaluation 126
2.2.1 병력청취, 신체검사, 신경학적검사, 진단적검사 (History, physical exam, neurological 126
examination, laboratory test)
2.2.2 응급뇌 상검사 (Emergent neuroimaging) 133
2.3급성기치료Acute treatment 141
2.3.1 일반적보존치료 (General supportive care) 141
2.3.1.1 기도, 호흡기, 산소공급 (Airway, ventilator, oxygen supply) 141
2.3.1.2 발열 (Fever) 143
2.3.1.3 심리듬 (Cardiac rhythm) 145
2.3.1.4 혈압 (Blood pressure) 147
2.3.1.5 혈당 (Blood glucose) 150
2.3.1.6 혈역학적치료, 혈액량확장제 (Volume expansion, hemorheologic therapy) 153
2.3.2 내과적합병증의예방및치료 (Prevention and management of medical complication) 154
2.3.2.1 깊은정맥혈전증예방 (Deep vein thrombosis prophylaxis) 154
2.3.2.2 양 (Nutrition) 157
2.3.2.3 욕창 (Pressure sore) 159
2.3.2.4 흡인성폐렴 (Aspiration pneumonia) 161
2.3.2.5 비뇨기계감염 (Urinary tract infection) 162
2.3.3 혈전용해술 (Thrombolysis) 164
2.3.3.1 정맥내혈전용해술 (Intravenous thrombolysis) 2012.12 개정 164
2.3.3.2 동맥내혈전용해술 (Intra-arterial Thrombolysis) 2012.12 개정 176
2.3.4 항혈소판제 (Antiplatelet agents) 185
2.3.5 항응고제 (Anticoagulants) 187
2.3.6 신경보호제 (Neuroprotectants) 190
2.3.7 신경계합병증의치료 (Treatment of neurologic complications) 192
2.3.7.1 뇌압상승, 부종, 출혈성변환 (ICP elevation, brain edema, and hemorrhagic transformation) 192
2.3.7.2 경련 (Seizure) 196
2 급성기뇌졸중진료 Acute Stroke Management 113

15
CONFIDENTIAL 고유번호 : 10CONTENTS
2.4뇌실질내출혈의치료Treatment of intracerebral hemorrhage 198
2.4.1 뇌실질내출혈의약물치료 (Medical Treatment of Intracerebral Hemorrhage) 198
2.4.1.1 뇌압조절 (ICP control) 2014.1 개정 198
2.4.1.2 항응고제와관련된뇌실질내출혈의내과적치료 (Medical treatment of 204
intracerebral hemorrhage in patients receiving anticoagulants)
2.4.1.3 뇌실질내출혈후혈압조절 (Blood pressure management after 207
intracerebral hemorrhage) 2014.1 개정
2.4.1.4 경련의예방및치료 (Seizure prevention and treatment) 2014.1 개정 212
2.4.2 뇌실질내출혈의수술적치료 (Surgical Treatment of Intracerebral Hemorrhage) 2014.1 개정 216
2.5뇌졸중재활Rehabilitation in acute stroke 228
2.5.1 재활치료의시작 (Timing of stroke rehabilitation) 228
2.5.2 재활치료의강도 (Intensity of rehabilitation) 230
2.5.3 재활치료의접근방법 (Underlying approach to rehabilitation) 231
2.5.4 합병증관리 (Management of complication) 234
3.1위험인자조절risk factor control 243
3.1.1 고혈압 (Hypertension) 243
3.1.2 당뇨 (Diabetes) 246
3.1.3 고지질혈증 (Hyperlipidemia) 248
3.1.4 흡연 (Smoking) 251
3.1.5 음주 (Alcohol) 253
3.1.6 비만 (Obesity) 254
3.1.7 육체적활동및운동 (Physical activity and exercise) 255
3.1.8 식이 (Diet) 257
3.1.9 고호모시스테인혈증 (Hyperhomocysteinemia) 259
3.2비심장탓색전성뇌졸중또는일과성뇌허혈의항혈전제치료 261
Antithrombotic therapy for noncardioembolic stroke or transient ischemic attack
3.2.1 항혈소판제 (Antiplatelet therapy) 261
3.2.1.1 아스피린 (Aspirin) 261
3.2.1.2 Thienopyridine 계열약물 (Thienopyridine) 2010.3 개정 263
3 뇌졸중이차예방Secondary prevention of stroke 239

16
CONTENTS
3.2.1.3 기타항혈소판제 (Other antiplatelets agents: triflusal, dipyridamole, cilostazol) 2012.4 개정 254
3.2.1.4 항혈소판제병합치료 (Antiplatelet combination therapy) 258
3.2.2 항응고제 (Anticoagulation) 261
3.2.3 특정상황에서항혈소판제사용 (Specific consideration of antiplatelet agents) 263
3.2.3.1 항혈소판제복용중발생한허혈뇌졸중 (Ischemic stroke while taking antiplatelet agent) 263
3.2.3.2 뇌출혈이동반된허혈뇌졸중 (Ischemic stroke mixed with hemorrhage) 265
3.3심장탓색전성뇌졸중또는일과성허혈발작의항혈전제치료 271
Antithrombotic therapy of cardioembolic stroke or TIA
3.3.1 항응고제 (Anticoagulants) 271
3.3.2 항혈소판제또는병합치료 (Antiplatelet therapy or combination therapy) 273
3.3.3 특정질환의치료 (Specific conditions) 274
3.3.3.1 심방세동 (Atrial fibrillation) 274
3.3.3.2 울혈성심부전 (Congestive heart failure) 277
3.3.3.3 급성심근경색 (Acute myocardial infarction) 279
3.3.3.4 심장판막질환 (Valvular heart disease) 282
3.4 혈관협착-폐쇄질환에서수술또는중재적치료 286
Surgical or interventional treatment of large artery steno-occlusive disease
3.4.1 두개강외경동맥협착 (Extracranial carotid artery stenosis) 2011.11 개정 286
3.4.2 척추뇌바닥동맥협착 (Vertebrobasilar artery stenosis) 295
3.4.3 두개강내동맥협착 (Intracranial artery stenosis) 297
3.4.4 두개강외-두개강내동맥우회로술 (Extracranial-intracranial artery bypass surgery) 300
3.5기타특정질환의치료Management of other specific conditions 303
3.5.1 뇌내출혈의이차예방 (Secondary prevention of intracerebral hemorrhage) 303
3.5.2 출혈을동반한허혈뇌졸중의이차예방 (Secondary prevention in ischemic
stroke mixed with hemorrhage) 305
3.5.3 동맥박리 (Arterial dissection) 309
3.5.4 열린타원구멍과심방중격동맥류 (Patent foramen ovale and atrial septal aneurysm) 312
3.5.5 항인지질항체증후군 (Antiphospholipid antibody syndrome) 315
3.5.6 정맥성뇌경색 (Venous infarction) 317

1 뇌졸중일차예방Primary prevention of stroke
110-744 서울시종로구연건동28. 서울 학교병원임상의학연구소7208호
뇌졸중임상연구센터 표전화_02 2072 0652 FAX_02 747 0668


19
CLINICAL RESEARCH CENTER FOR STROKE
1.1 조절할수없는위험인자 Non-modifiable risk factors 21
1.1.1 나이 (Age) 21
1.1.2 성 (Sex) 22
1.1.3 출생시저체중 (Low birth weight) 23
1.1.4 유전적요인 (Genetic factor) 24
1. 뇌졸중일차예방Primary prevention of stroke
1.3 조절가능한잠재적인위험인자Less well-documented or potentially 70
modifiable risk factors
1.3.1 사증후군 (Metabolic syndrome) 70
1.3.2 음주 (Alcohol) 72
1.3.3 약물남용 (Drug abuse) 74
1.2 입증된조절가능한위험인자 Well-documented and modifiable risk factors 26
1.2.1 고혈압 (Hypertension) 26
1.2.2 흡연 (Smoking) 29
1.2.3 당뇨병 (Diabetes) 31
1.2.4 심방세동 (Atrial fibrillation) 2012.12 개정 34
1.2.5 기타심장질환 (Other cardiac conditions) 44
1.2.6 이상지질혈증 (Dyslipidemia) 46
1.2.7 무증상경동맥협착 (Asymptomatic carotid stenosis) 2011.10 개정 51
1.2.8 폐경후호르몬치료 (Postmenopausal hormonal therapy) 61
1.2.9 식이와 양 (Diet and nutrition) 63
1.2.10 신체활동 (Physical activity) 65
1.2.11 비만 (Obesity) 67

CLINICAL RESEARCH CENTER FOR STROKE
1.3.4 경구용피임제 (Oral contraceptive use) 75
1.3.5 수면중호흡장애 (Sleep-disordered breathing) 77
1.3.6 편두통 (Migraine) 79
1.3.7 고호모시스틴혈증 (Hyperhomocysteinemia) 81
1.3.8 과다응고증 (Hypercoagulability) 84
1.3.9 염증 (Inflammation) 86
1.3.10 감염증 (Infection) 88
1.3.11 무증상열공성병변및백색질변성 (Asymptomatic lacune or white matter 90
change)
1.4 아스피린의뇌졸중일차예방효과 Aspirin for primary stroke prevention 2011.10 개정 92
1.5 뇌졸중인식도Public awareness and education 2012.5신규 97
1.6 비파열뇌동맥류Unruptured intracranial aneurysm 100
1.6.1 비파열류뇌동맥류의선별검사(Screening of unruptured intracranial aneurysm) 2013.1 신규 100
1.6.2 비파열류뇌동맥류의치료(Treatment of unruptured intracranial aneurysm) 2013.1 신규 103
20

21
1-1 조절할수없는위험인자Non-modifiable risk factors
나이가들면심뇌혈관계의노화현상과뇌졸중위험인자인질병의진행으로뇌졸중의위험이높아
진다. 55세이후에는매10년마다뇌졸중의위험이2배씩증가한다.1,2
없음.
우리나라의인구1,000명당연령별뇌졸중유병률은50 24.3명, 60 58.0명, 70 이상67.5명으로연
령증가에따라상승한다.3
없음.
1. Brown RD, Whisnant JP, Sicks JD, O'Fallon WM, Wiebers DO. Stroke incidence, prevalence, and survival:
secular trends in Rochester, Minnesota, through 1989. Stroke.1996;27:373-380.
2. Wolf PA, D'Agostino RB, O'Neal MA, Sytkowski P, Kase CS, Belanger AJ, Kannel WB. Secular trends in
stroke incidence and mortality. The Framingham Study. Stroke.1992;23:1551-1555.
3. 국민건강 양조사제3기. 2005.
1.1.1. 나이Age
CLINICAL RESEARCH CENTER FOR STROKE

뇌졸중발생률은남자에서여자보다높은데, 이는생물학적요인뿐아니라뇌졸중의위험인자와관
련된생활습관의차이에의할것으로추정된다.
CLINICAL RESEARCH CENTER FOR STROKE
1.1.2. 성Sex
없음.
뇌졸중발생률은서구나우리나라모두남자에서여자보다높다.1,2단85세이상연령 에서는여자
에서남성보다뇌졸중발생률이더높은데이는고위험군남자들이85세이전에이미심뇌혈관질환
으로사망하 기때문일것으로추측된다.3미국의경우35-44세연령 에서도경구피임약이나임신
등과관련된뇌졸중으로인하여, 여자가남자보다뇌졸중발생률이더높은것으로보고되어있다. 그
러나우리나라의경우, 건강심사평가원의자료와사망통계를이용하여뇌졸중발생률을추정한결
과, 85세이상연령 를제외한모든연령 에서남자의뇌졸중발생률이여자보다높았다.1
유병률의경우, 2005년국민 양조사제3기보고에의하면의사에의해진단된인구1,000명당뇌졸
중유병률은, 남자는16.44명, 여자는15.37명으로남자의유병률이여자보다높았다.4
없음.
1. 심뇌혈관질환감시체계구축사업. 건강보험심사평가원. 2006.
2. AHA. Heart disease and Stroke Statistics-2004 update. American Heart Association. 2003.
3. Sacco RL, Boden-Albala B, Gan R, Chen X, Kargman DE, Shea S, Paik MC, Hauser WA. Stroke incidence
among white,
22

23
CLINICAL RESEARCH CENTER FOR STROKE
출생시저체중이뇌졸중발생률과사망률을증가시킨다는연구결과가있다.1 이는임신중산모의
양상태가자녀의성인시기뇌졸중발생률및사망률에 향을미칠가능성을시사하며, 한나라
에서도지역적으로뇌졸중발생률과사망률에차이를보이는현상을일부설명할수있을것이다.
없음.
잉 랜드와웨일즈지역의성인뇌졸중사망률은출생시저체중이었던군에서높았으며,1 스코틀랜
드지역의코호트연구에서는출생시체중이1kg 증가할때성인시기의연령보정뇌졸중위험도가
0.38(95% CI, 0.24-0.60)로유의하게감소하 고,2남캘리포니아의50세이하Medicaid 수혜자를 상
으로실시한연구에서도출생시체중이2,500g 미만인군이4,000g 이상인군에비하여뇌졸중발생
률이2배높았다.3
없음.
black, and Hispanic residents of an urban community: the Northern Manhattan Stroke Study. Am J
Epidemiol. 1998;147:259-268.
4. The Third Korea National Health and Nutrition Examination Survey (KNHANES III), 2005.
1.1.3. 출생시저체중Low birth weight
1. Barker DJ, Lackland DT. Prenatal influences on stroke mortality in England and Wales. Stroke. 2003;34:1598-

24
1602.
2. Lawlor DA, Ronalds G, Clark H, Smith GD, Leon DA. Birth weight is inversely associated with incident
coronary heart disease and stroke among individuals born in the 1950s: findings from the Aberdeen
Children of the 1950s prospective cohort study. Circulation. 2005;112:1414-1418.
3. Lackland DT, Egan BM, Ferguson PL. Low birth weight as a risk factor for hypertension. J Clin Hypertens
(Greenwich).2003;5:133-136.
CLINICAL RESEARCH CENTER FOR STROKE
1. Referral for genetic counseling may be considered for patients with rare genetic causes of stroke (ASA:
Class IIb, Level of Evidence C). There remain insufficient data to recommend genetic screening for the
prevention of a first stroke.
유전적요인은고혈압, 당뇨등의위험인자의발병및위험인자에 한뇌졸중민감성등에작용한
다. 또한뇌졸중과관련된드문유전병의발생에도유전적요인이관여한다. 현재까지유전적요인
은교정이불가능하지만, 유전자치료및결핍된성분을보충하는치료등이개발중이다.
1.1.4. 유전적요인Genetic factors
뇌졸중의주요위험인자인고혈압, 당뇨, 이상지질혈증등의발병과이로인한뇌졸중의발생에유
전적요인이관여한다. 뇌졸중가족력이있는경우뇌졸중발생위험이증가하는데, 유전및환경적
요인이복합적으로관련되어있다. 쌍생아연구결과는유전적요인의관련성을강하게시사하는데,
일란성쌍생아에서뇌졸중발생일치율(concordance rate)은이란성쌍생아보다약5배높다.1
뇌졸중과관련되거나혈액응고를유발하는유전병, 그리고특정질환에서가족력등이뇌졸중의발
생에유전적요인이관련된증거이다. 뇌졸중과관련된유전병으로 CADASIL (Cerebral autosomal

25
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌졸중일차예방을위하여유전검사를시행할근거는아직부족하다. (권고수준GPP)
dominant arteriopathy with subcortical infarcts and leukoencephalopathy), 마판증후군(Marfan
syndrome), 파브리병(Fabry’s disease) 등이있다. 혈액응고장애중단백질C 또는S 결핍, V 인자라이
덴(Factor V Leiden) 돌연변이등은상염색체우성유전양식을보인다. 이러한혈액응고장애유전병
들은정맥혈전증의위험을증가시키는것으로알려져있으나심근경색이나뇌졸중과같은동맥혈
전증과의관련성에 한증거는아직까지는부족하다.2가족력이관찰되는경우로는후천적혈액응
고장애인루푸스항응고인자(Lupus anticoagulant) 또는항카디오리핀항체(anticardiolipin antibody)에
서약 10%의가족력이관찰되며,3혈관이상을유발하는동맥박리, 모야모야병, 섬유근이형성증
(fibromuscular dysplasia) 등의경우에도10-20%에서유전적또는가족적요인이관찰된다.4
1. Brass LM, Isaacsohn JL, Merikangas KR, Robinette CD. A study of twins and stroke. Stroke.1992;23:221-223.
2. Hankey GJ, Eikelboom JW, van Bockxmeer FM, Lofthouse E, Staples N, Baker RI. Inherited thrombophilia in
ischemic stroke and its pathogenic subtypes. Stroke. 2001;32:1793-1799.
3. Weber M, Hayem G, DeBandt M, Palazzo E, Roux S, Kahn MF, Meyer O. The family history of patients with
primary or secondary antiphospholipid syndrome (APS). Lupus. 2000;9:258-263.
4. Begelman SM, Olin JW. Fibromuscular dysplasia. Curr Opin Rheumatol. 2000;12:41-47.

26
CLINICAL RESEARCH CENTER FOR STROKE
1.2. 입증된조절가능한위험인자Well-documented and modifiable risk factors
1.2.1. 고혈압Hypertension
고혈압은조절가능한뇌졸중위험인자중에서가장유병률이높고인구집단기여위험도(population-
attributable risk)가높은위험인자이다. 고혈압은관상동맥질환에비해뇌졸중발생과더높은관련성
이있으며, 혈압을조절하면뇌졸중발생을감소시킬수있다.
1. Blood pressure measurement is an essential component of regular health care visits. Blood pressure
should be lowered to normal levels (140/90 mm Hg, or 135/80 mm Hg in diabetics) by means of lifestyle
modification. Most hypertensive patients will also need pharmacological treatment to achieve normal
blood pressure (EUSI: Level I)
2. Regular screening for hypertension (at least every 2 years in most adults and more frequently in minority
populations and the elderly) and appropriate management (ASA: Class I, Level of Evidence A), including
dietary changes, lifestyle modification, and pharmacological therapy as summarized in JNC 7, are
recommended (Table).

27
CLINICAL RESEARCH CENTER FOR STROKE
61개전향적관찰연구의메타분석결과115/75mmHg 이상의혈압에서는수축기혈압20mmHg, 확
장기혈압 10mmHg가증가할때마다뇌졸중으로인한사망이 2배이상증가하 고, 수축기혈압
10mmHg 또는확장기혈압5mmHg를낮추면뇌졸중으로인한사망을약40% 감소시킬것으로예
측되었다.2임상시험의메타분석결과에의하면고혈압치료는뇌졸중발생을약 31%(95% CI; 26-
36%) 감소시켰다.3미국의 JNC7 지침에서제시한목표혈압은심뇌혈관질환이없는경우에는
140/90mmHg 미만이고, 당뇨혹은신장질환이있는경우에는130/80mmHg 미만이다.1,4노인성수축
Lifestyle modifications are encouraged for all and include (1) weight reduction if overweight, (2) limitation of ethyl alcohol
intake, (3) increased aerobic physical activity (30-45 minutes daily), (4) reduction of sodium intake (<2.34 g), (5) maintenance
of adequate dietary potassium (>120 mmol/d), (6) smoking cessation, and (7) DASH diet (rich in fruit, vegetables, and low-
fat dairy products and reduced in saturated and total fat).
*Compelling indications include (1) congestive heart failure, (2) MI, (3) diabetes, (4) chronic renal failure, and (5) prior
stroke.
�Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension.
Classification SBP, mm Hg DBP, mm Hg No Compelling Indication* With Compelling Indication*
Normal <120 And <80 No antihypertensive drug No antihypertensive drug
Prehypertension 120-139 Or 80-90 No antihypertensive drug Drugs for the compelling
indication
Stage 1 hypertension 140-159 Or 90-99 Thiazide-type diuretics for Drugs for the compelling
most. May consider ACEIs, indication. Other drugs
ARBs, β-blockers, calcium (diuretics, ACEIs, ARBs, β-
channel blockers, or blockers, calcium channel
combination. blockers) as needed.
Stage 2 hypertension 160 Or ≥100 Two-drug combination for Drugs for the compelling
most� (usually thiazide- indication.
type diuretic and ACEI or Other drugs (diuretics,
ARB or β-blocker or ACEIs, ARBs, β-blockers, calcium
calcium channel blocker). channel blockers) as needed.
표. 혈압의분류및고혈압의치료 (JNC 7)1

28
기고혈압(확장기혈압은90mmHg 미만이나수축기혈압이160mmHg를초과하는경우)의경우에도
고혈압을치료하면뇌졸중발생을30% 감소시킬수있다.5
뇌졸중일차예방에있어서로다른종류의항고혈압제의효과를직접비교한자료는아직불충분하
며, 특정한종류의항고혈압제가혈압조절이외의추가적인뇌졸중예방효과가있다고할근거는아
직미약하다. 그러나13개베타차단제임상시험들의메타분석결과, 1차약물로칼슘차단제또는안
지오텐신전환효소억제제(angiotensin converting enzyme inhibitors)나안지오텐신수용체차단제
(angiotensin receptor blockers) 등안지오텐신계억제제를사용할때베타차단제에비하여뇌졸중예
방효과가우수하 다.6
항고혈압제의선택은여러상황을고려하여환자에따라개별화되어야하며, 현재까지의근거에의
하면뇌졸중일차예방을위해가장중요한것은특정한종류의항고혈압제를선택하는것보다는적
절하게혈압을떨어뜨리는것이다.
CLINICAL RESEARCH CENTER FOR STROKE
1. 성인에서혈압은정기적으로측정하는것이권장되며, 노인이나심뇌혈관질환의다른위험인자를
가지고있는경우에는특히자주측정해야한다. (권고수준GPP)
2. 고혈압예방과치료를위해생활습관개선(과체중시체중감량, 저지방식이, 저염식, 운동, 절주, 금
연)이권고되며, 필요한경우약물요법을병행하여혈압을낮추어야한다. (근거수준Ia, 권고수준A)
3. 뇌졸중일차예방을위해혈압조절의목표는140/90mmHg 미만으로유지하는것이권고된다. (근거
수준Ia, 권고수준A)
4. 당뇨병과신장질환을가진환자에서혈압조절의목표는130/80mmHg 미만으로유지하는것이권
고된다. (근거수준Ia, 권고수준A)
5. 노인성수축기고혈압도일반적인고혈압과동일한원칙과방법으로치료가필요하다. (근거수준
Ia, 권고수준A)
6. 뇌졸중일차예방을위하여특정한종류의항고혈압제를선택하는것보다는적절하게혈압을떨어
뜨리는것이가장중요하다. 단, 특별한적응증이없고동일한혈압강하조건에서는베타차단제보
다는칼슘차단제나레닌안지오텐신계억제제가추천된다. (근거수준Ia, 권고수준A)

29
CLINICAL RESEARCH CENTER FOR STROKE
1. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., Jones DW, Materson BJ,
Oparil S, Wright JT, Jr., Roccella EJ. Seventh report of the Joint National Committee on Prevention,
Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.
2. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to
vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies.
Lancet. 2002;360:1903-1913.
3. Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, Weiss NS. Health
outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-
analysis. JAMA. 2003;289:2534-2544.
4. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Diabetes and Chronic
Kidney Disease. Am J Kidney Dis.2007;49:S12-154.
5. Staessen JA, Gasowski J, Wang JG, Thijs L, Den Hond E, Boissel JP, Coope J, Ekbom T, Gueyffier F, Liu
L, Kerlikowske K, Pocock S, Fagard RH. Risks of untreated and treated isolated systolic hypertension in
the elderly: meta-analysis of outcome trials. Lancet. 2000;355:865-872.
6. Wiysonge CS, Bradley H, Mayosi BM, Maroney R, Mbewu A, Opie LH, Volmink J. Beta-blockers for
hypertension. Cochrane Database Syst Rev.2007:CD002003.
1. Abstention from cigarette smoking and (for current smokers) smoking cessation are recommended (EUSI:
역학적연구결과흡연은뇌졸중의중요한위험인자임이알려졌다. 흡연은좁아진동맥에혈전을형
성시키는급성효과와죽상경화증을촉진시키는만성효과를동시에가지고있다.
1.2.2. 흡연Smoking

30
Level II) (ASA: Class I, Level of Evidence B).
2. Avoidance of environmental tobacco smoke for stroke prevention should also be considered (ASA: Class IIa,
Level of Evidence C).
3. The use of counseling, nicotine replacement, and oral smoking-cessation medications has been found to be
effective for smokers and should be considered (ASA: Class IIa, Level of Evidence B).
CLINICAL RESEARCH CENTER FOR STROKE
32개임상연구의메타분석에의하면흡연의허혈성뇌졸중비교위험도는1.9(95% CI, 1.7-2.2)이고거
미막밑출혈비교위험도는2.9(95% CI, 2.5-3.5)이다.1
몇몇임상연구의결과는간접흡연역시뇌졸중의위험인자임을시사한다.2,3흡연자가금연을하면뇌
졸중위험이1년이내50% 감소하며, 5년이지나면비흡연자와비슷한수준으로감소한다.4행동요법
과약물치료등은흡연자의금연을도와줄수있다.5-7
1. 흡연을하지말아야하며, 흡연자에게는반드시금연을권고해야한다. (근거수준III, 권고수준B)
2. 간접흡연도피해야한다. (근거수준III, 권고수준B)
3. 흡연자의금연을위해상담, 니코틴 체요법, 경구용금연보조제등이고려되어야한다. (근거수
준Ia, 권고수준A)
1. Shinton R, Beevers G. Meta-analysis of relation between cigarette smoking and stroke. BMJ.
1989;298:789-794.
2. Bonita R, Duncan J, Truelsen T, Jackson RT, Beaglehole R. Passive smoking as well as active smoking
increases the risk of acute stroke. Tob Control. 1999;8:156-160.
3. You RX, Thrift AG, McNeil JJ, Davis SM, Donnan GA. Ischemic stroke risk and passive exposure to
spouses' cigarette smoking. Melbourne Stroke Risk Factor Study (MERFS) Group. Am J Public Health.
1999;89:572-575.

31
CLINICAL RESEARCH CENTER FOR STROKE
당뇨병은주요조절가능한위험인자의하나이다. 규모환자- 조군연구또는코호트연구를통
하여당뇨병은허혈성뇌졸중의독립적위험인자인것으로보고되었다. 당뇨병환자에서적극적혈
당조절이뇌졸중발생위험을줄일수있는지에 해서는아직명확히규명되지는않았다. 그러나
엄격한혈당조절을통하여당뇨병의합병증을예방할수있음은이미잘알려져있다. 또한당뇨병
과고혈압, 고지질혈증등뇌졸중의주요위험인자들의 접한연관성을고려할때, 엄격한혈당조
절은반드시필요하다. 고혈압또는고지질혈증환자에서당뇨병이동반된경우혈압및지질에
한더욱적극적인치료가필요하다.
1. It is recommended that hypertension be tightly controlled in patients with either type 1 or type 2 diabetes
(the JNC 7 recommendation of <130/80mmHg in diabetic patients is endorsed) as part of a
comprehensive risk-reduction program (ASA: Class I, Level of Evidence A). Treatment of adults with
diabetes, especially those with additional risk factors, with a statin to lower the risk of a first stroke is
recommended (ASA: Class I, Level of Evidence A). Recommendations to consider treatment of diabetic
patients with an ACEI or ARB are endorsed.
4. Wolf PA, D'Agostino RB, Kannel WB, Bonita R, Belanger AJ. Cigarette smoking as a risk factor for
stroke. The Framingham Study. JAMA. 1988;259:1025-1029.
5. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst
Rev. 2003:CD000031.
6.Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation.
Cochrane Database Syst Rev. 2004:CD000146.
7. Fiore MC. US public health service clinical practice guideline: treating tobacco use and dependence.
Respir Care. 2000;45:1200-1262.
1.2.3. 당뇨병Diabetes

32
2. Although strict control of glucose levels in DM has not been proven to be associated with a decreased
risk of stroke, it should be encouraged because of benefits in terms of other diabetic complications (EUSI:
Level III).
CLINICAL RESEARCH CENTER FOR STROKE
많은전향적관찰연구및환자- 조군연구들에서당뇨병은허혈성뇌졸중의발생위험을1.8 -6배증
가시킨다.1또한당뇨병환자의당화혈색소(HbA1C) 수치가높을수록뇌졸중발생위험이증가하는데,
당화혈색소를1% 낮추면뇌졸중발생위험을12% 감소시킬것으로예측되었다.2
당뇨병환자들을 상으로엄격한혈당조절과고식적인혈당조절을비교한 규모무작위배정임
상연구에서뇌졸중을포함한 혈관합병증의발생은차이를보이지않았으나,3또다른메타분석에
의하면엄격한혈당조절은 혈관합병증발생을유의하게감소시켰고, 특히제 2형당뇨병환자의
경우에뇌졸중의발생위험을유의하게감소시켰다.(Incidence Rate Ratio=0.58; 95% CI, 0.46-0.74)4
당뇨병환자에서심뇌혈관질환의예방을위하여동반된위험인자에 한적극적인치료가중요하
다. 통상적인치료보다더엄격한혈압조절이뇌졸중을포함한심뇌혈관질환의발생을유의하게감
소시켰다.5특히최근의 규모무작위임상연구들에서다른위험인자들을가진당뇨병환자의아집
단분석결과안지오텐신전환효소억제약물및안지오텐신수용체차단약물들이위약및베타차단
제와비교하여심뇌혈관질환또는뇌졸중의발생위험을감소시키는것으로보고되었다.6, 7
또한최소한가지이상의위험인자를가진심뇌혈관질환의병력이없는2형당뇨병환자들을 상으
로한연구에서스타틴(statin)을이용한고지혈증치료가뇌졸중발생을48%(95% CI, 11-69%; p<0.05)
감소시켰으며,8최근보고된소규모무작위배정임상연구에서는혈당조절뿐아니라고혈압및고
지질혈증등을포함한위험인자들에 한종합적이고적극적인치료가고식적인치료에비해뇌졸
중을포함한심뇌혈관질환의발생을약47%(HR=0.47; 95% CI, 0.22-0.74; p=0.01) 감소시키는것으로보
고되었다.9
1. 당뇨병환자에서혈당조절뿐아니라고혈압, 고지질혈증, 흡연등의동반된위험인자에 한종합
적이고적극적인평가및치료가필요하다. (근거수준Ib, 권고수준A)

33
CLINICAL RESEARCH CENTER FOR STROKE
2. 당뇨병환자에서심뇌혈관질환예방을위하여보다적극적이고엄격한혈당조절이필요하다. (근
거수준 Ia, 권고수준A) 혈압조절은130/80mmHg 미만을목표로적극적으로치료하여야하며, (근
거수준 Ib, 권고수준A) 혈중지질은저 도콜레스테롤(LDL-cholesterol) 100mg/dL 미만을목표로
치료하여야한다. (근거수준 Ia, 권고수준A) 특히다른위험인자를가지고있는제2형당뇨병환자
의경우뇌졸중일차예방을위해스타틴을이용한혈중지질강하치료가추천된다. (근거수준 Ib,
권고수준A)
1. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, Culebras A, Degraba TJ, Gorelick PB,
Guyton JR, Hart RG, Howard G, Kelly-Hayes M, Nixon JV, Sacco RL. Primary prevention of ischemic stroke: A
guideline from the American Heart Association/American Stroke Association Stroke. 2006;152:27-38.
2. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR.
Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS
35): Prospective observational study. BMJ. 2000;321:405-412
3. UK prospective diabetes study (UKPDS) group. Intensive blood-glucose control with sulphonylureas or insulin
compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33).
Lancet. 1998;352:837-853
4. Stettler C, Allemann S, Juni P, Cull CA, Holman RR, Egger M, Krahenbuhl S, Diem P. Glycemic control and
macrovascular disease in types 1 and 2 diabetes mellitus: Meta-analysis of randomized trials. Am Heart J.
2006;152:27-38
5. UK prospective diabetes study group. Tight blood pressure control and risk of macrovascular and
microvascular complications in type 2 diabetes: UKPDS 38. BMJ.1998;317:703-713.
6. Heart outcomes prevention evaluation study investigators. Effects of ramipril on cardiovascular and
microvascular outcomes in people with diabetes mellitus: Results of the hope study and micro-hope
substudy. Lancet. 2000;355:253-259.
7. Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, Fyhrquist F, Julius S, Kjeldsen SE,
Kristiansson K, Lederballe-Pedersen O, Nieminen MS, Omvik P, Oparil S, Wedel H, Aurup P, Edelman J,

34
Snapinn S. Cardiovascular morbidity and mortality in patients with diabetes in the losartan intervention for
endpoint reduction in hypertension study (LIFE): A randomised trial against atenolol. Lancet. 2002;359:1004-
1010.
8. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, Thomason MJ, Mackness
MI, Charlton-Menys V, Fuller JH. Primary prevention of cardiovascular disease with atorvastatin in type 2
diabetes in the collaborative atorvastatin diabetes study (CARDS): Multicentre randomised placebo-controlled
trial. Lancet. 2004;364:685-696.
9. Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and
cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348:383-393.
CLINICAL RESEARCH CENTER FOR STROKE
1. 판막질환이동반된- 특히기계판막치환술을시행받은- 심방세동이있는환자에게는뇌졸중의
일차예방을위해항응고치료를해야한다. (권고수준A, 근거수준Ia)
2. 비판막성심방세동환자에게뇌졸중예방을위해항혈전치료(와파린또는아스피린)를해야하는데,
이는개개인의위험도, 출혈가능성, 환자의선호도및항응고효과모니터링의충실성을고려하여
1.2.4. 심방세동Atrial Fibrillation
심방세동은뇌졸중의주요위험인자로나이가들수록유병률이급격하게증가하여 80세이상인구
에서는약10%에이를것으로추정된다. 심방세동에의한뇌졸중의경우, 뇌손상범위가크고심한신
경학적장애를유발하여다른원인의뇌졸중에비해사망이나중증의장애를남길위험이높다. 그러
나심방세동에의한뇌졸중은적절한항혈전치료로효과적으로예방할수있어뇌졸중예방측면에
서매우중요하다. 최근비판막성심방세동환자에서뇌졸중및전신색전증예방을위한새로운항혈
전치료효과를평가한 규모임상시험들이발표되어, 이연구결과들을바탕으로심방세동환자에
서뇌졸중일차예방에관한2009년진료지침의권고안을개정하 다.
개정: 2012.12

35
CLINICAL RESEARCH CENTER FOR STROKE
판단한다. (권고수준A, 근거수준Ia)
3. 항응고치료에심각한부적응증이없는고위험도(1년뇌졸중위험도4% 이상) 심방세동환자에서
와파린(INR 2.0-3.0) 사용이추천된다. (권고수준A, 근거수준Ia)
4. 75세이상의고령의심방세동환자에서도뇌졸중의일차예방목적으로와파린(INR 2.0-3.0) 사용이
추천된다. (권고수준A, 근거수준Ib)
1. ESC (2010) 1
Combination therapy with aspirin 75-100 mg plus clopidogrel 75 mg daily, should be considered for
stroke prevention in patients for whom there is patient refusal to take OAC therapy or a clear
contraindication to OAC therapy (e.g. inability to cope or continue with anticoagulation monitoring),
where there is a low risk of bleeding. (Class IIa, LOE B)
2. ASA/AHA (2011) 2
For high-risk patients with atrial fibrillation deemed unsuitable for anticoagulation, dual antiplatelet
therapy with clopidogrel and aspirin offers more protection against stroke than aspirin alone but with
increased risk of major bleeding and might be reasonable (Class IIb; LOE B)
3. ASA/AHA (2012) 3
1) Warfarin (Class I; LOE A), dabigatran (Class I; LOE B), apixaban (Class I; LOE B), and rivaroxaban
(Class IIa; LOE B) are all indicated for the prevention of first and recurrent stroke in patients with
nonvalvular AF. The selection of an antithrombotic agent should be individualized on the basis of risk
factors, cost, tolerability, patient preference, potential for drug interactions, and other clinical
characteristics, including time in INR therapeutic range if the patient has been taking warfarin.
2) Dabigatran 150 mg twice daily is an efficacious alternative to warfarin for the prevention of first and
recurrent stroke in patients with nonvalvular AF and at least 1 additional risk factor who have CrCl
�30 mL/min (Class I; LOE B).
3) On the basis of pharmacokinetic data, the use of dabigatran 75 mg twice daily in patients with AF and
at least 1 additional risk factor who have a low CrCl (15-30 mL/min) may be considered, but its safety
and efficacy have not been established (Class IIb; LOE C).
36
4) Because there are no data to support the use of dabigatran in patients with more severe renal failure,
dabigatran is not recommended in patients with a CrCl �15 mL/min (Class III; LOE C).
5) Apixaban 5 mg twice daily is an efficacious alternative to aspirin in patients with nonvalvular AF
deemed unsuitable for vitamin K antagonist therapy who have at least 1 additional risk factor and no
more than 1 of the following characteristics: Age ≥80 years, weight ≤60 kg, or serum creatinine ≥
1.5 mg/dL (Class I; LOE B).
6) Although its safety and efficacy have not been established, apixaban 2.5 mg twice daily may be
considered as an alternative to aspirin in patients with nonvalvular AF deemed unsuitable for vitamin K
antagonist therapy who have at least 1 additional risk factor and �2 of the following criteria: Age ≥80
years, weight ≤60 kg, or serum creatinine ≥1.5 mg/dL (Class IIb; LOE C).
7) Apixaban 5 mg twice daily is a relatively safe and efficacious alternative to warfarin in patients with
nonvalvular AF deemed appropriate for vitamin K antagonist therapy who have at least 1 additional
risk factor and no more than 1 of the following characteristics: Age ≥80 years, weight ≤60 kg, or
serum creatinine ≥1.5 mg/dL (Class I; LOE B).
8) Although its safety and efficacy have not been established, apixaban 2.5 mg twice daily may be
considered as an alternative to warfarin in patients with nonvalvular AF deemed appropriate for
vitamin K antagonist therapy who have at least 1 additional risk factor and �2 of the following criteria:
Age ≥80 years, weight ≤60 kg, or serum creatinine ≥1.5 mg/dL (Class IIb; LOE C).
9) Apixaban should not be used if the CrCl is 〈25 mL/min (Class III; LOE C).
10) In patients with nonvalvular AF who are at moderate to high risk of stroke (prior history of TIA, stroke,
or systemic embolization or ≥2 additional risk factors), rivaroxaban 20 mg/d is reasonable as an
alternative to warfarin (Class IIa; LOE B).
11) In patients with renal impairment and nonvalvular AF who are at moderate to high risk of stroke
(prior history of TIA, stroke, or systemic embolization or≥2 additional risk factors), with a CrCl of 15 to
50 mL/min, 15 mg of rivaroxaban daily may be considered; however, its safety and efficacy have not
been established (Class IIb; LOE C).
12) Rivaroxaban should not be used if the CrCl is �15 mL/min (Class III; LOE C).
13) The safety and efficacy of combining dabigatran, rivaroxaban, or apixaban with an antiplatelet agent
have not been established (Class IIb; LOE C).
CLINICAL RESEARCH CENTER FOR STROKE

37
CLINICAL RESEARCH CENTER FOR STROKE
4. ESC (2012) 4
1) When adjusted-dose VKA (INR 2-3) cannot be used in a patient with AF where an OAC is
recommended, due to difficulties in keeping within therapeutic anticoagulation, experiencing side
effects of VKAs, or inability to attend or undertake INR monitoring, one of the NOACs, either a direct
thrombin inhibitor (dabigatran) or an oral factor Xa inhibitor (e.g. rivaroxaban, apixaban) is
recommended. (Class I; LOE B)
2) Where OAC is recommended, one of the NOACs, either a direct thrombin inhibitor (dabigatran) or an
oral factor Xa inhibitor (e.g. rivaroxaban, apixaban) should be considered rather than adjusted-dose
VKA (INR 2-3) for most patients with non-valvular AF, based on their net clinical benefit. (Class IIa; LOE A)
3) Where dabigatran is prescribed, a dose of 150 mg b.i.d. should be considered for most patients in
preference to 110 mg b.i.d., with the latter dose recommended in elderly patients, age ≥80,
concomitant use of interacting drugs (e.g. verapamil), high bleeding risk (HAS-BLED score ≥3) or
moderate renal impairment (CrCl 30-49 mL/min). (Class IIa; LOE B)
4) Where rivaroxaban is being considered, a dose of 20 mg o.d. should be considered for most patients
in preference to 15 mg o.d., with the latter dose recommended in high bleeding risk (HAS-BLED
score ≥3) or moderate renal impairment (CrCl 30-49 mL/min). (Class IIa; LOE C)
5) Baseline and subsequent regular assessment of renal function (by CrCl) is recommended in patients
following initiation of any NOAC, which should be done annually but more frequently in those with
moderate renal impairment where CrCl should be assessed 2-3 times per year. (Class IIa; LOE B)
6) NOACs (dabigatran, rivaroxaban, and apixaban) are not recommended in patients with severe renal
impairment (CrCl �30 mL/min). (Class III; LOE A)
새로발표된근거와기존의근거를종합한개정의필요성에 한근거는다음과같다.
1. 기존의근거
심방세동은단독으로뇌졸중발생위험도를3-5배증가시킨다.5뇌졸중병력이없는심방세동환자는일년
에2-4%에서허혈뇌졸중이발생한다.6, 7항혈전치료는심방세동환자의뇌졸중위험을줄일수있는데, 용
량을조절한와파린치료는62%, 아스피린은22%의위험도를줄일수있으며,8아스피린에비해와파린은

38
45%의위험도를더줄일수있다.7심방세동의뇌졸중위험도는나이와동반된위험인자에따라약20배의
차이가있다. CHADS2평가법은2001년ACC/AHA/ESC가제안한심방세동환자의뇌졸중위험도층화분류
방법으로울혈성심부전, 고혈압, 75세이상의나이와당뇨병이있는경우1점을, 과거뇌졸중이나일과성
뇌허혈증이있는경우2점을부여한다. 이방법은코호트연구를통해그타당도가입증되어가장많이사
용되고있으며, 6, 9, 10 CHADS2점수에따른뇌졸중위험도에따라뇌졸중일차예방을위한아스피린이나와
파린치료의선택이권장되고있다. 한편75세이상고령의심방세동환자에서도항응고치료가아스피린
보다우월한효과를보이는연구결과가발표된바있다.11
Congestive heart failure, hypertension, age>75 y, or diabetes = 1 point. Stroke or TIA* = 2 points.
*All nonvalvular atrial fibrillation patients with prior stroke or transient ischemic attack should be considered
high risk and treated with anticoagulants; the CHADS₂scheme should be applied for primary prevention.
�Consider patient preferences, bleeding risk, and access to good INR monitoring. For those with a CHADS₂
Score=1, the number needed to treat to prevent 1 stroke over 1 y with warfarin is �100; excellent anticoagulation
control is essential to achieve this benefit.
CLINICAL RESEARCH CENTER FOR STROKE
1) 와파린과새로운항응고제의비교
와파린은심방세동환자의뇌졸중예방효과가매우뛰어나지만음식및약물과의상호작용, 불안정한약
물효과, 정기적인 INR (international normal range) 모니터링의필요성등이문제가되었다. 이러한약점을
극복하기위해혈액모니터링이필요없고, 용량에따라일정한약물효과를기 할수있는새로운항응고
제의개발이진행되었고, 2009-2011년사이에직접트롬빈억제제 (direct thrombin inhibitor)인dabigatran,
Treatment Recommendations Based on Risk Stratification
Aspirin (75-325 mg/d)
Warfarin INR 2-3 or aspirin (75-325 mg/d)�
Warfarin INR 2-3�
Warfarin INR 2-3
Warfarin INR 2-3
Stroke Rate
1.0%/y
1.5%/y
2.5%/y
5.0%/y
>7%/y
Risk Level
Low
Low-moderate
Moderate
High
Very high
CHADS₂Score
0
1
2*
3
≥4
표. Nonvalvular Atrial Fibrillation Risk Stratification and Treatment Recommendations:
Risk Stratification by CHADS2 Scheme

39
CLINICAL RESEARCH CENTER FOR STROKE
혈액응고인자Xa 억제제 (Factor Xa inhibitor)인 rivaroxaban 및apixaban을와파린과비교한 규모임상시
험인RE-LY(Randomized Evaluation of Long-Term Anticoagulation Therapy)12, ROCKET-AF(Rivaroxaban Once
Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and
Embolism Trial in Atrial Fibrillation)13 및 ARISTOTLE(Apixaban for Reduction in Stroke and Other
Thromboembolic Events in Atrial Fibrillation)14결과가발표되어, 그근거들을바탕으로새로운항응고제들
에 한권고안을추가하 다.
RE-LY 임상시험에서dabigatran 110 mg은와파린(INR 2.0-3.0)에비하여일차결과변수(primary endpoint)인
뇌졸중및전신색전증예방효과는비슷하 지만 (1.53%/year vs. 1.69%/year; RR 0.91 [0.74-1.11]; P�0.001 for
non-inferiority), 주요출혈부작용은유의하게감소시켰다 (2.71%/year vs. 3.36%/year; RR 0.80 [0.69-0.93];
P=0.003). 반면에 dabigatran 150 mg은와파린에비해뇌졸중및전신색전증예방효과가우월하 고
(1.11%/year vs. 1.69%/year; RR 0.66 [0.53-0.82]; P� 0.001 for superiority), 주요출혈부작용은비슷하 다
(3.11%/year vs. 3.36%/year; RR 0.93 [0.81-1.07]; P=0.31). ROCKET-AF 임상시험은다른임상시험에비해상
적으로고위험군환자들이많이포함되었는데rivaroxaban은와파린에비하여뇌졸중및전신색전증예방
효과는비슷하 으며 (1.7%/year vs. 2.2%/year; RR 0.79 [0.66-0.96]; P�0.001 for non-inferiority), 주요출혈및
임상적으로유의한출혈부작용도비슷하 다(14.9%/year vs. 14.5%/year; HR 1.03 [0.96-1.11]; P=0.44).
ARISTOTLE 임상시험에서는apixaban이와파린에비하여뇌졸중및전신색전증예방효과가우월하 고
(1.27%/year vs. 1.60%/year; RR 0.79 [0.66-0.95]; P�0.001 for non-inferiority; P=0.01 for superiority), 주요출혈부
작용도낮았다(2.13%/year vs. 3.09%/year; HR 0.69 [0.60-0.80]; P�0.001).
두개내출혈은와파린군의0.74%에비해dabigatran 110 mg군에서는0.23%(RR, 0.31; 95% CI, 0.20 to 0.47; P
�0.001) dabigatran 150 mg군에서는0.30%(RR, 0.40; 95% CI, 0.27 to 0.60; P�0.001)로두용량군모두에서와
파린군보다유의하게적었다. ROCKET-AF 임상시험결과두개내출혈(0.7% vs. 0.5%; HR, 0.67; 95% CI 0.47 -
0.93; P=0.02)은rivaroxaban군에서유의하게적었다. ARISTOTLE 임상시험결과두개내출혈발생은와파린
과 apixaban군각각 0.80%와 0.33%로 apixaban군에서유의하게낮았다(HR, 0.42; 95% CI, 0.30 - 0.58; P�
0.001).
정리하면dabigatran, rivaroxaban 및apixaban 모두와파린과비교하여유효성과안전성에 해동등하거
나우월한결과를보 다. 다만각임상연구의연구 상, 연구설계및통계분석등이차이가있어어떤약
제가더우월하거나안전한것으로판단할근거는없다. 특이할만한것은가장심각한부작용인뇌출혈
의위험이와파린에비해새로운경구항응고제들모두에서33-69% 정도로유의하게감소하 다는것이

40
다. 한편RE-LY, ROCKET-AF, ARISTOTLE 임상시험모두신장기능이유의하게저하된환자들을제외하
다. 따라서비판막성심방세동환자에서새로운항응고제들이와파린을 체할수있으며신기능장애를
고려하여사용하도록권고하 다. 두가지용량에 해연구된dabigatran의경우위장출혈을포함한주요
출혈의위험이높은환자의경우150 mg 보다는110 mg 사용을우선고려하는것을권고하 다. 크레아티
닌청소률에따른제외기준은RE-LY과ROCKET-AF 연구에서는30 mL/min 미만, ARISTOTLE 연구에서는
25 mL/min 미만으로차이가있었다. 하지만신장기능장애에따른새로운항응고제사용제외기준의통일
성및안전성을고려하여제외기준을30 mL/min 미만으로통일하여기술하 다.
2) 와파린치료가부적합환자에서아스피린과새로운항혈전치료법의비교
와파린치료가부적합한심방세동환자에서아스피린단독요법과클로피도그렐과아스피린병합요법을
비교한ACTIVE A (The Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events), 아스
피린과 apixaban을비교한 AVERROES(Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial
Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment)15임상시험결과에
근거하여새로운기술을추가하 다.
ACTIVE A 임상시험에서아스피린과클로피도그렐병용요법은아스피린단독요법에비하여일차결과변
수인주요심혈관사건및허혈뇌졸중의발생을유의하게줄 다(6.8%/year vs. 7.6%/year; RR 0.89 [0.81-0.98];
P=0.01). 그러나위장출혈, 두개내출혈, 두개외출혈및이를모두포함한주요출혈과심각하지않은출혈은
클로피도그렐과아스피린병합군에서유의하게증가하 다(2.0%/year vs. 1.3%/year; RR 1.57 [1.29-1.92]; P�
0.001). 일반적으로허혈뇌졸중보다출혈뇌졸중이더치명적이고예후가불량하다는점과뇌졸중발생과
주요출혈발생을함께고려할경우순수이득이없다는점을고려할때항응고치료가부적절하다고판단
되는비판막성심방세동환자들에서병용요법이아스피린단독요법보다우월하다고단정할수는없다.
따라서와파린사용이부적합한환자에서출혈위험이높지않은경우에한하여병용요법의사용을신중
하게고려해볼수있다. AVERROES 임상시험에서apixaban은아스피린에비해뇌졸중및전신색전증을유
의하게감소시켰고(1.6%/year vs. 3.7%/year; HR 0.45 [0.32-0.62]; P� 0.001) 주요출혈의발생은비슷하여
(1.4%/year vs. 1.2%/year; HR 1.13 [0.74-1.75]; P=0.57), apixaban이아스피린에비해안전성에차이가없고효
과는우월하 다. 따라서와파린사용이부적합한비판막성심방세동환자에서아스피린보다apixaban 투
여가우선권장된다.
정리하면와파린치료가부적합한비판막성심방세동환자의경우ACTIVE A와AVERROES 연구결과에근
거하여apixaban (5 mg 1일2회) 사용이우선권장되며, 출혈위험이높지않은경우에아스피린단독요법을
CLINICAL RESEARCH CENTER FOR STROKE

41
CLINICAL RESEARCH CENTER FOR STROKE
아스피린과클로피도그렐병용요법으로 체하는것을신중히고려할수있다. AVERROES 연구에서는
크레아티닌청소률의제외기준이25 mL/min 미만이었지만, 새로운항응고제사용제외기준의통일성및
안전성을고려하고, 권고안에서제외기준을30 mL/min 미만으로기술하 다.
1. 판막질환이동반된- 특히기계판막치환술을시행받은- 심방세동이있는환자에게는뇌졸중의일차
예방을위해와파린항응고치료를해야한다. (권고수준A, 근거수준 Ia)
2. 비판막성심방세동환자에게뇌졸중예방을위해항혈전치료(와파린, dabigatran, rivaroxaban, apixaban
또는아스피린)가필요하며, 이는개개인의위험도, 출혈가능성, 환자의선호도및항응고효과모니터링
의충실성을고려하여판단한다. (권고수준A, 근거수준Ia)
3. 항응고치료에심각한부적응증이없는고위험도(1년뇌졸중위험도4% 이상) 비판막성심방세동환자
에서와파린(INR 2.0 - 3.0) 사용이권장된다. (권고수준A, 근거수준Ia) 이경우와파린의 체재로
dabigatran, rivaroxaban 및apixaban을사용할수있다. (권고수준A, 근거수준Ib)
4. Dabigatran을사용할경우150 mg 1일2회사용이권장된다. 출혈위험이높다고판단되는환자의경우
110 mg 1일2회사용이추천된다. (권고수준A, 근거수준 Ib)
5. Rivaroxaban을사용할경우20 mg 1일1회사용이권장된다. 신장기능이저하된경우(크레아티닌청소
율30 - 49 mL/min) 15 mg 1일1회사용이추천된다. (권고수준A, 근거수준 Ib)
6. Apixaban을사용할경우5 mg 1일2회사용이권장된다. 신장기능저하(혈장크레아티닌≥1.5 mg/dl),
고령(80세이상) 또는체중60 kg 이하중2가지이상의해당사항을가진경우2.5 mg 1일2회사용이추
천된다. (권고수준A, 근거수준Ib)
7. 항응고치료가필요한비판막성심방세동환자에서중등도이상의신장기능장애가동반된경우(크레
아티닌청소율30 mL/min 미만) dabigatran, rivaroxaban 및apixaban 사용은권장되지않는다. (권고수준
B, 근거수준 IIa)
8. 와파린치료가부적합한고위험도(1년뇌졸중위험도4% 이상) 비판막성심방세동환자의경우아스피
린(권고수준A, 근거수준 Ia), 아스피린과클로피도그렐병용요법(권고수준B, 근거수준IIa) 또는
apixaban (권고수준A, 근거수준 Ib) 사용이권장된다. 이중apixaban 사용이우선권장되며출혈위험이
높지않은경우아스피린단독요법보다아스피린과클로피도그렐병용요법을우선적으로고려할수
있다.

42
Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, et al. Guidelines for the management
of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society
of Cardiology (ESC). Eur Heart J. 2010;31:2369-2429
Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, et al. Guidelines for the
Primary Prevention of Stroke: A Guideline for Healthcare Professionals From the American Heart
Association/American Stroke Association. Stroke. 2011;42:517-584
Furie KL, Goldstein LB, Albers GW, Khatri P, Neyens R, Turakhia MP, et al. Oral Antithrombotic
Agents for the Prevention of Stroke in Nonvalvular Atrial Fibrillation. Stroke. 2012;43:3442-3453
Camm AJ, Lip GYH, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC
Guidelines for the management of atrial fibrillation. [First published online: August 24, 2012]. Eur Heart J.
2012:http://eurheartj.oxfordjournals.org/content/early/2012/2008/2024/eurheartj.ehs2253.short.
Accessed October 2022, 2012
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the
Framingham Study. Stroke. 1991;22:983-988
Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, et al. Anticoagulation therapy for
stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice?
JAMA. 2003;290:2685-2692
van Walraven C, Hart RG, Singer DE, Laupacis A, Connolly S, Petersen P, et al. Oral anticoagulants vs
aspirin in nonvalvular atrial fibrillation: an individual patient meta-analysis. JAMA. 2002;288:2441-
2448
Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients
with atrial fibrillation: a meta-analysis. Ann Intern Med. 1999;131:492-501
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical
classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation.
JAMA. 2001;285:2864-2870
Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BS, et al. Selecting patients with
atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
CLINICAL RESEARCH CENTER FOR STROKE

43
CLINICAL RESEARCH CENTER FOR STROKE
2004;110:2287-2292
Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, et al. Warfarin versus aspirin for
stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial
Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet.
2007;370:493-503
Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus
Warfarin in Patients with Atrial Fibrillation. N Engl J Med. 2009;361:1139-1151
Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus Warfarin in
Nonvalvular Atrial Fibrillation. N Engl J Med. 2011;365:883-891
Granger CB, Alexander JH, McMurray JJV, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus
Warfarin in Patients with Atrial Fibrillation. N Engl J Med. 2011;365:981-992
Connolly SJ, Eikelboom J, Joyner C, Diener H-C, Hart R, Golitsyn S, et al. Apixaban in Patients with
Atrial Fibrillation. N Engl J Med. 2011;364:806-817
11.
12.
13.
14.
15.

44
심방세동이외에도뇌졸중발생을증가시킬수있는심장질환에는확장성심근병증, 심장판막질환
(승모판탈출, 심내막염, 인공판막), 선천성심질환(열린타원구멍[patent foramen ovale], 심방중격결
손, 심방중격류) 등이있다.1급성심근경색증은심방세동을유발할수있을뿐아니라심장탓색전증
의원인으로작용할수있다.1개심수술의경우일반적인수술보다뇌졸중합병증의발생위험이높
다.2,3
CLINICAL RESEARCH CENTER FOR STROKE
1.2.5. 기타심장질환Other cardiac conditions
1. It is reasonable to prescribe warfarin to post-ST-segment-elevation MI patients with LV dysfunction with
extensive regional wall-motion abnormalities (ASA: Class IIa, Level of Evidence A).
2. Warfarin may be considered in patients with severe LV dysfunction, with or without congestive heart
failure (ASA: Class IIb, Level of Evidence C).
3. Various AHA (American Heart Association) / ACC (American College of Cardiology) practice guidelines
recommend strategies to reduce the risk of stroke in patients with a variety of cardiac conditions. These
include the management of patients with valvular heart disease, unstable angina, chronic stable angina,
and acute MI.
원인미상의뇌졸중(cryptogenic stroke)이발생한청장년기환자의약40%에서잠재적인심장탓색전
증의원인이발견된다.4
뇌졸중발생률은심장박출계수(ejection fraction)와반비례한다. 심근경색환자중박출계수가 29%
미만인경우가, 35% 이상인경우에비해뇌졸중의상 위험도가1.86배높다.5박출계수가5% 감소
할때마다뇌졸중발생률이18% 증가한다고알려져있다. 좌심실박출계수가감소된특발성심근병
증환자에서심장탓색전증을예방하기위한와파린(warfarin) 사용에는논란의여지가있고, 현재와
파린과항혈소판제의효능을비교하는연구가진행중이다.

45
CLINICAL RESEARCH CENTER FOR STROKE
1. ST분획상승심근경색이후심장탓색전증의발생위험이있는경우 (예, 심방세동, 심장벽혈전, 무
동부분등) 아스피린등의항혈소판제제와항응고제의병용투여가바람직하다. 항응고제의치료
기간은동반된심장질환을고려하여결정해야하는데, 심방세동이있는경우에는지속적인항응고
제치료가바람직하며, 심장벽혈전또는무동부분이있는경우에는최소3개월이상의항응고제치
료가추천된다. (근거수준Ib, 권고수준A)
2. 심부전의동반여부와상관없이좌심실기능부전이심한경우와파린사용을고려해볼수있다. (근
거수준IV, 권고수준C)
3. 뇌졸중발생률을높일수있는심장판막질환, 협심증, 급성심근경색등의치료는심장질환의일반
적인진료지침을따르는것을추천한다. (권고수준GPP)
4. 관상동맥우회로수술시고위험군(65세이상고령, 좌측주관상동맥협착, 말초혈관질환, 일과성허
혈발작또는뇌졸중의병력, 청진상경동맥잡음)에 해서는경동맥협착등의뇌졸중위험에
한평가가고려되어야한다. (권고수준GPP)
관상동맥우회로수술(coronary artery bypass graft; CABG) 후뇌졸중발생빈도는약2-9%이며,2이는
8-10%의뇌졸중발생률을보이는판막수술에비하면낮은편이다.3 CABG 수술시뇌졸중발생의주
요위험인자들로는고령, 뇌졸중의과거력, 고혈압, 당뇨병, 흡연, 신부전, 경동맥협착, 말초혈관질
환, 긴심폐우회시간(prolonged cardiopulmonary bypass time), 동맥죽상경화등이보고되어있
다.2,3,6
1. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner
FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Jr., Alpert JS, Anderson JL, Faxon DP,
Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK. ACC/AHA guidelines for
the management of patients with ST-elevation myocardial infarction: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999
Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation.2004;110:e82-292.

46
2. Dafer RM. Risk estimates of stroke after coronary artery bypass graft and carotid endarterectomy. Neurol Clin.
2006;24:795-806, xi.
3. Bucerius J, Gummert JF, Borger MA, Walther T, Doll N, Onnasch JF, Metz S, Falk V, Mohr FW. Stroke after
cardiac surgery: a risk factor analysis of 16,184 consecutive adult patients. Ann Thorac Surg. 2003;75:472-478.
4. Di Pasquale G US, Pinelli G. Cardiac investigation in patients with cerebrovascular disease. In: Ginsberg M,
Bogousslavsky J, eds. Cerebrovascular Disease: Pathophysiology, Diagnosis, and Management.: Malden,
Mass: Blackwell Science; 1998.
5. Loh E, Sutton MS, Wun CC, Rouleau JL, Flaker GC, Gottlieb SS, Lamas GA, Moye LA, Goldhaber SZ, Pfeffer
MA. Ventricular dysfunction and the risk of stroke after myocardial infarction. N Engl J Med. 1997;336:251-257.
6. John R, Choudhri AF, Weinberg AD, Ting W, Rose EA, Smith CR, Oz MC. Multicenter review of preoperative risk
factors for stroke after coronary artery bypass grafting.Ann Thorac Surg.2000;69:30-35.
CLINICAL RESEARCH CENTER FOR STROKE
1. National Cholesterol Education Program III guidelines for the management of patients who have not had
a cerebrovascular event and who have elevated total cholesterol or elevated non?HDL cholesterol in the
초기역학조사에서혈중콜레스테롤수치와뇌졸중발생과는일관된관련성을보이지않았으나, 이
는허혈성뇌졸중뿐아니라출혈성뇌졸중까지연구에포함시킨결과로생각된다.1,2일반적으로남녀
모두에서혈중총콜레스테롤및저 도콜레스테롤(LDL-cholesterol) 증가와허혈성뇌졸중발생과
관련이있다. 또한혈중고 도콜레스테롤(HDL-cholesterol) 저하는남자에서만허혈성뇌졸중발생
과관련성이관찰되었다. 최근10여년간진행된연구및메타분석에따르면, 스타틴(statin)으로혈중
콜레스테롤을저하시킬경우심뇌혈관질환의일차및이차예방효과가있다는것이밝혀졌다.3또한
허혈성뇌졸중의일차및이차예방에도스타틴이효과가있다는결과들이밝혀졌다.4,5
1.2.6. 이상지질혈증Dyslipidemia

47
CLINICAL RESEARCH CENTER FOR STROKE
presence of hypertriglyceridemia are endorsed (Table).
2. It is recommended that patients with known coronary artery disease (CAD) and high-risk hypertensive
patients even with normal LDL cholesterol levels be treated with lifestyle measures and a statin (ASA:
Class I, Level of Evidence A).
3. Treatment of adults with diabetes, especially those with additional risk factors, with a statin to lower the
risk of a first stroke is recommended (ASA: Class I, Level of Evidence A).
4. Suggested treatments for patients with known CAD and low HDL cholesterol include weight loss,
increased physical activity, smoking cessation, and possibly niacin or gemfibrozil (ASA: Class IIa, Level of
Evidence B).
5. Cholesterol-lowering therapy (simvastatin) is recommended for high-risk patients (EUSI: Level I).
48
CLINICAL RESEARCH CENTER FOR STROKE
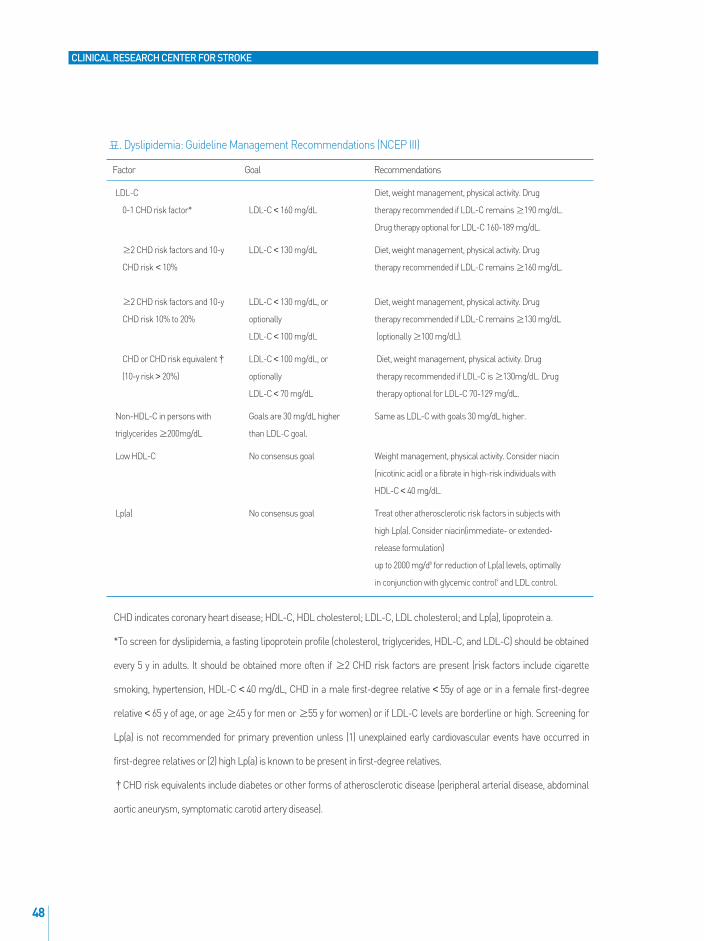
CHD indicates coronary heart disease; HDL-C, HDL cholesterol; LDL-C, LDL cholesterol; and Lp(a), lipoprotein a.
*To screen for dyslipidemia, a fasting lipoprotein profile (cholesterol, triglycerides, HDL-C, and LDL-C) should be obtained
every 5 y in adults. It should be obtained more often if ≥2 CHD risk factors are present (risk factors include cigarette
smoking, hypertension, HDL-C <40 mg/dL, CHD in a male first-degree relative <55y of age or in a female first-degree
relative <65 y of age, or age ≥45 y for men or ≥55 y for women) or if LDL-C levels are borderline or high. Screening for
Lp(a) is not recommended for primary prevention unless (1) unexplained early cardiovascular events have occurred in
first-degree relatives or (2) high Lp(a) is known to be present in first-degree relatives.
�CHD risk equivalents include diabetes or other forms of atherosclerotic disease (peripheral arterial disease, abdominal
aortic aneurysm, symptomatic carotid artery disease).
Factor Goal Recommendations
LDL-C Diet, weight management, physical activity. Drug
0-1 CHD risk factor* LDL-C <160 mg/dL therapy recommended if LDL-C remains ≥190 mg/dL.
Drug therapy optional for LDL-C 160-189 mg/dL.
≥2 CHD risk factors and 10-y LDL-C <130 mg/dL Diet, weight management, physical activity. Drug
CHD risk <10% therapy recommended if LDL-C remains ≥160 mg/dL.
≥2 CHD risk factors and 10-y LDL-C <130 mg/dL, or Diet, weight management, physical activity. Drug
CHD risk 10% to 20% optionally therapy recommended if LDL-C remains ≥130 mg/dL
LDL-C <100 mg/dL (optionally ≥100 mg/dL).
CHD or CHD risk equivalent� LDL-C <100 mg/dL, or Diet, weight management, physical activity. Drug
(10-y risk >20%) optionally therapy recommended if LDL-C is ≥130mg/dL. Drug
LDL-C <70 mg/dL therapy optional for LDL-C 70-129 mg/dL.
Non-HDL-C in persons with Goals are 30 mg/dL higher Same as LDL-C with goals 30 mg/dL higher.
triglycerides ≥200mg/dL than LDL-C goal.
Low HDL-C No consensus goal Weight management, physical activity. Consider niacin
(nicotinic acid) or a fibrate in high-risk individuals with
HDL-C <40 mg/dL.
Lp(a) No consensus goal Treat other atherosclerotic risk factors in subjects with
high Lp(a). Consider niacin(immediate- or extended-
release formulation)
up to 2000 mg/d8 for reduction of Lp(a) levels, optimally
in conjunction with glycemic control9 and LDL control.
표. Dyslipidemia: Guideline Management Recommendations (NCEP III)

49
CLINICAL RESEARCH CENTER FOR STROKE
초기역학조사이후남성을 상으로시행한 3개의전향적인연구에서총콜레스테롤수치(특히
240-270mg/dL 이상에서)가올라감에따라허혈성뇌졸중발생빈도가증가됨이알려졌으며, 이후남
녀모두에서총콜레스테롤및저 도콜레스테롤수치증가와허혈성뇌졸중발생간에는명확한관
계가있음이밝혀졌다.5그러나중성지방(triglyceride), 여성에서고 도콜레스테롤및지질단백질
(a)(lipoprotein[a])와허혈성뇌졸중과의관련성은아직불분명하며향후더많은연구가필요하다.5
최근9개의스타틴임상시험을종합하여분석한결과, 관상동맥질환이있거나고위험군환자1,000
명을5년간스타틴으로치료하면약9건의뇌졸중을예방할수있는것으로밝혀졌다.11
비스타틴지질저하약제도뇌졸중예방효과가있을가능성이있으나아직까지는근거자료가충분
하지않다. 나이아신(Niacin)을투여한경우일과성허혈발작을포함한뇌혈관질환의발생은24% 감
소시켰으나, 일과성허혈발작을제외한뇌졸중만포함하면예방효과가분명하지않았다.12관상동
맥질환이있으면서고 도콜레스테롤이낮은경우젬피브로질(gemfibrozil)을투여하면뇌졸중상
위험도가31%(95% CI, 2-52%; p=0.036)감소하 다.13나이아신섭취를비롯하여운동, 체중감소등
의복합적인요법이혈중고 도지단백질콜레스테롤을25-40% 증가시킬수있다.7
1. 저 도콜레스테롤치료목표수치는일반적인권고사항에따른다.
1) 관상동맥질환이있거나이에상당하는위험요인(경동맥질환, 말초혈관질환, 복부동맥류, 당뇨
병등)이있는경우, 저 도콜레스테롤을100mg/dL 보다낮게유지한다.
2) 위험인자2개이상인경우, 저 도콜레스테롤을130mg/dL보다낮게유지한다.
3) 위험인자1개이하인경우, 저 도콜레스테롤을160mg/dL보다낮게유지한다.
(위험인자의정의: 흡연, 고혈압, 고 도콜레스테롤<40mg/dL, 직계가족중남자는 55세미만에서,
여자는65세미만에서관상동맥질환의병력이있는경우, 위험연령 [남자는45세이상, 여자는55세
이상]) (근거수준Ia, 권고수준A)
2. 관상동맥질환이있거나관상동맥질환의위험성이높은고혈압환자의경우, 저 도콜레스테롤
수치가정상이더라도생활습관의변화와함께스타틴치료가추천된다. (근거수준Ia, 권고수준A).
3. 성인당뇨병환자의경우저 도콜레스테롤치료목표는100mg/dL 미만을권장한다. (근거수준 Ia,

50
권고수준A) 특히다른위험인자를동반한제2형당뇨병환자의경우뇌졸중1차예방을위해스타
틴을이용한혈중지질강하치료가추천된다(근거수준Ib, 권고수준A).
4. 관상동맥질환이있으면서고 도지단백질콜레스테롤수치가낮은환자는체중을줄이고, 신체활
동을늘리며, 금연등과함께, 나이아신이나젬피브로질투여가추천될수있다. (근거수준 Ib, 권고
수준A).
CLINICAL RESEARCH CENTER FOR STROKE
1. Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective
cohorts. Prospective studies collaboration. Lancet. 1995;346:1647-1653.
2. Iso H, Jacobs D, Wentworth D, Neaton J, Cohen J. Serum cholesterol levels and six-year mortality from
stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J Med.
1989;320:904-910.
3. Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R, Collins R,
Simes R. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from
90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267-1278.
4. Collins R, Armitage J, Parish S, Sleight P, Peto R. Effects of cholesterol-lowering with simvastatin on
stroke and other major vascular events in 20536 people with cerebrovascular disease or other high-risk
conditions. Lancet. 2004;363:757-767.
5. Amarenco P, Labreuche J, Lavallee P, Touboul P-J. Statins in Stroke Prevention and Carotid
Atherosclerosis: Systematic Review and Up-to-Date Meta-Analysis. Stroke. 2004;35:2902-2909.
6. Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr., Clark LT, Hunninghake DB, Pasternak RC, Smith SC,
Jr., Stone NJ. Implications of recent clinical trials for the National Cholesterol Education Program Adult
Treatment Panel III guidelines. Arterioscler Thromb Vasc Biol. 2004;24:e149-e161.
7. National Institutes of Health. Adult Treatment Panel III: Detection E, and Treatment of High Blood
Cholesterol in Adults. Bethesda, Md: National Institutes of Health; 2002.
8. Guyton JR, Goldberg AC, Kreisberg RA, Sprecher DL, Superko HR, O'Connor CM. Effectiveness of once-
nightly dosing of extended-release niacin alone and in combination for hypercholesterolemia. Am J
Cardiol. 1998;82:737-743.

51
CLINICAL RESEARCH CENTER FOR STROKE
무증상경동맥협착은연구마다차이가있지만최근에는6개월이내협착 역에허혈뇌졸중증상이
없었던경우를무증상경동맥협착으로고려하고있다.1-3진단기술의발전으로무증상경동맥협착
의발견이증가하고있는데, 65세이상에서50% 이상의협착은5-10%, 80% 이상의협착은약1% 정
도로보고되고있다.4,5 50-99%의무증상경동맥협착을가지고있는경우매년뇌졸중발생률은약
1-3.4%로알려져있다.6무증상경동맥협착의치료에있어내과적치료와경동맥내막절제술 (carotid
endarterectomy)을비교한임상시험결과가 1990년 와 2000년 초반에발표된이후, 내과적치료
와경동맥혈관성형/스텐트설치술 (carotid angioplasty and stenting)의발전이있었으며, 수술방법도
또한발전하 다. 따라서환자와임상의사는선택의폭이넓어졌지만, 한편으로는어떤치료법이최
선의선택인지를고민해야한다.
9. Arenillas JF, Molina CA, Chacon P, Rovira A, Montaner J, Coscojuela P, Sanchez E, Quintana M, Alvarez-
Sabin J. High lipoprotein (a), diabetes, and the extent of symptomatic intracranial atherosclerosis.
Neurology. 2004;63:27-32.
10. Rifai N, Ma J, Sacks FM, Ridker PM, Hernandez WJL, Stampfer MJ, Marcovina SM. Apolipoprotein(a)
Size and Lipoprotein(a) Concentration and Future Risk of Angina Pectoris with Evidence of Severe
Coronary Atherosclerosis in Men: The Physicians' Health Study. Clin Chem. 2004;50:1364-1371.
11. Amarenco P, Tonkin AM. Statins for stroke prevention: disappointment and hope. Circulation.
2004;109:III44-49.
12. Clofibrate and niacin in coronary heart disease. JAMA. 1975;231:360-381.
13. Bloomfield Rubins H, Davenport J, Babikian V, Brass LM, Collins D, Wexler L, Wagner S,
Papademetriou V, Rutan G, Robins SJ. Reduction in stroke with gemfibrozil in men with coronary heart
disease and low HDL cholesterol: The Veterans Affairs HDL Intervention Trial (VA-HIT). Circulation.
2001;103:2828-2833.
1.2.7. 무증상경동맥협착Asymptomatic carotid stenosis
개정: 2011.10
52
1. 무증상경동맥협착환자에서뇌졸중의다른치료가능한위험인자가있는지를선별하고발견된위
험인자에 하여집중적인치료를해야한다. (GPP)
2. 50% 이상의무증상경동맥협착환자에서금기사항이없는한항혈소판제제치료가권장된다. (근
거수준IIa, 권고수준B) 50%미만인경우, 환자의상황에따라항혈소판제제치료유무를결정하는
것이바람직하다. (GPP)
3. 60-99% 무증상경동맥협착에서수술관련이환율및사망률이3% 미만인경우예방적경동맥내막
절제술이추천된다. 수술 상환자의선택에있어동반된질환, 기 여명, 환자의선호도와기타
개인별요인들을신중하게고려하는것이필요하다. (근거수준Ia, 권고수준A)
4. 중증의무증상경동맥협착환자에서수술위험성을높이는동반질환이있는경우경동맥혈관성형
술및스텐트설치술이경동맥내막절제술의 안으로추천될수있다. (근거수준IIa, 권고수준B)
CLINICAL RESEARCH CENTER FOR STROKE
1. 2008 European Stroke Organization Guidelines7
1) Carotid surgery is not recommended for asymptomatic individuals with significant carotid stenosis (North
American Symptomatic Carotid Endarterectomy Trial - NASCET 60~99%), except in those at high risk of
stroke (Class I, Level C)
2) Carotid angioplasty, with or without stenting, is not recommended for patients with asymptomatic carotid
stenosis (Class IV, GCP)
3) It is recommended that patients should take aspirin before and after surgery (Class I, Level A)
2. 2010 ASA/AHA Primary Stroke Prevention Guidelines6
1) Patients with asymptomatic carotid artery stenosis should be screened for other treatable risk factors for
stroke with institution of appropriate lifestyle changes and medical therapy (Class I, Level of Evidence C).
2) Selection of asymptomatic patients for carotid revascularization should be guided by an assessment of
comorbid conditions and life expectancy, as well as other individual factors, and should include a
thorough discussion of the risks and benefits of the procedure with an understanding of patient
preferences (Class I, Level of Evidence C).
3) The use of aspirin in conjunction with CEA is recommended unless contraindicated because aspirin was used
in all of the cited trials of CEA as an antiplatelet drug (Class I, Level of Evidence C).

53
CLINICAL RESEARCH CENTER FOR STROKE
4) Prophylactic CEA performed with �3% morbidity and mortality can be useful in highly selected patients with
an asymptomatic carotid stenosis (minimum 60% by angiography, 70% by validated Doppler ultrasound)
(Class IIa, Level of Evidence A). It should be noted that the benefit of surgery may now be lower than
anticipated based on randomized trial results, and the cited 3% threshold for complication rates may be high
because of interim advances in medical therapy.
5) Prophylactic carotid artery stenting might be considered in highly selected patients with an asymptomatic
carotid stenosis (�60% on angiography, �70% on validated Doppler ultrasonography, or �80% on
computed tomographic angiography or MRA if the stenosis on ultrasonography was 50% to 69%). The
advantage of revascularization over current medical therapy alone is not well established (Class IIb, Level of
Evidence B).
6) The usefulness of CAS as an alternative to CEA in asymptomatic patients at high risk for the surgical
procedure is uncertain (Class IIb, Level of Evidence C).
7) Population screening for asymptomatic carotid artery stenosis is not recommended (Class III, Level of
Evidence B).
3. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the
management of patients with extracranial carotid and vertebral artery disease8
진단
1) In asymptomatic patients with known or suspected carotid stenosis, duplex ultrasonography, performed by a
qualified technologist in a certified laboratory, is recommended as the initial diagnostic test to detect
hemodynamically significant carotid stenosis. (Class I, Level of Evidence C)
2) It is reasonable to perform duplex ultrasonography to detect hemodynamically significant carotid stenosis in
asymptomatic patients with carotid bruit. (Class IIa, Level of Evidence C)
3) It isreasonable to repeat duplex ultrasonography annually by a qualified technologist in a certified laboratory
to assess the progression or regression of disease and response to therapeutic interventions in patients with
atherosclerosis who have had stenosis greater than 50% detected previously. Once stability has been
established over an extended period or the patient’s candidacy for further intervention has changed, longer
intervals or termination of surveillance may be appropriate. (Class IIa, Level of Evidence C)
4) Duplex ultrasonography to detect hemodynamically significant carotid stenosis may be considered in
asymptomatic patients with symptomatic PAD, coronary artery disease (CAD), or atherosclerotic aortic
aneurysm, but because such patients already have an indication for medical therapy to prevent ischemic
symptoms, it is unclear whether establishing the additional diagnosis of ECVD in those without carotid bruit
would justify actions that affect clinical outcomes. (Class IIb, Level of Evidence C)

54
CLINICAL RESEARCH CENTER FOR STROKE
5)Duplex ultrasonography might be considered to detect carotid stenosis in asymptomatic patients without
clinical evidence of atherosclerosis who have 2 or more of the following risk factors: hypertension,
hyperlipidemia, tobacco smoking, a family history in a first degree relative of atherosclerosis manifested before
age 60 years, or a family history of ischemic stroke. However, it is unclear whether establishing a diagnosis of
ECVD would justify actions that affect clinical outcomes. (Class IIb, Level of Evidence C)
6)Carotid duplex ultrasonography is not recommended for routine screening of asymptomatic patients who
have no clinical manifestations of or risk factors for atherosclerosis. (Class III, Level of Evidence C)
내과적치료
1)Antihypertensive treatment is recommended for patients with hypertension and asymptomatic
extracranial carotid or vertebral atherosclerosis to maintain blood pressure below 140/90 mm Hg. (Class I,
Level of Evidence A)
2)Patients with extracranial carotid or vertebral atherosclerosis who smoke cigarettes should be advised to quit
smoking and offered smoking cessation interventions to reduce the risks of atherosclerosis progression and
stroke. (Class I, Level of Evidence B)
3)Treatment with a statin medication is recommended for all patients with extracranial carotid or vertebral
atherosclerosis to reduce low-density lipoprotein (LDL) cholesterol below 100 mg/dL. (Class I, Level of Evidence B)
4) If treatment with a statin (including trials of higher dose statins and higher-potency statins) does not achieve
the goal selected for a patient, intensifying LDL-lowering drug therapy with an additional drug from among
those with evidence of improving outcomes (ie, bile acid sequestrants or niacin) can be effective. (Class IIa,
Level of Evidence B)
5)For patients who do not tolerate statins, LDL-lowering therapy with bile acid sequestrants and/or niacin is
reasonable. (Class IIa, Level of Evidence B)
6)Diet, exercise, and glucose-lowering drugs can be useful for patients with diabetes mellitus and extracranial
carotid or vertebral artery atherosclerosis. The stroke prevention benefit, however, of intensive glucose
lowering therapy to a glycosylated hemoglobin A1c level less than 7.0% has not been established. (Class IIa,
Level of Evidence A)
7)Administration of statin-type lipid-lowering medication at a dosage sufficient to reduce LDL cholesterol to a
level near or below 70 mg/dL is reasonable in patients with diabetes mellitus and extracranial carotid or
vertebral artery atherosclerosis for prevention of ischemic stroke and other ischemic cardiovascular events.
(Class IIa, Level of Evidence B)
8)Antiplatelet therapy with aspirin, 75 to 325 mg daily, is recommended for patients with obstructive or
nonobstructive atherosclerosis that involves the extracranial carotid and/or vertebral arteries for prevention of
MI and other ischemic cardiovascular events, although the benefit has not been established for prevention of

55
CLINICAL RESEARCH CENTER FOR STROKE
stroke in asymptomatic patients. (Class I, Level of Evidence A)
9)Antiplatelet agents are recommended rather than oral anticoagulation for patients with atherosclerosis of
the extracranial carotid or vertebral arteries with (Class I, Level of Evidence B) or without (Class I, Level of
Evidence C) ischemic symptoms.
수술또는시술적치료
1)Selection of asymptomatic patients for carotid revascularization should be guided by an assessment of
comorbid conditions, life expectancy, and other individual factors and should include a thorough discussion of
the risks and benefits of the procedure with an understanding of patient preferences. (Class I, Level of Evidence C)
2) It is reasonable to perform CEA in asymptomatic patients who have more than 70% stenosis of the internal
carotid artery if the risk of perioperative stroke, MI, and death is low. (Class IIa, Level of Evidence A)
3)Prophylactic CAS might be considered in highly selected patients with asymptomatic carotid stenosis
(minimum 60% by angiography, 70% by validated Doppler ultrasound), but its effectiveness compared with
medical therapy alone in this situation is not well established. (Class IIb, Level of Evidence B)
4) In symptomatic or asymptomatic patients at high risk of complications for carotid revascularization by either
CEA or CAS because of comorbidities, the effectiveness of revascularization versus medical therapy alone is
not well established. (Class IIb, Level of Evidence B)
무증상경동맥협착에 한기존의근거와개정의필요성에 한새로운근거는다음과같다.
1. 기존의근거
50% 이상의무증상경동맥협착증에서아스피린을사용하는내과적치료와경동맥내막절제술의효
과를비교하는MACE 연구에서는경동맥내막절제술군에서아스피린을쓰지않아심근경색이유의
하게높았으므로이후의모든연구에서는항혈소판제의사용이권장되고있다.9
무증상경동맥협착에서의내과적치료와경동맥내막절제술을비교한3개의 규모임상시험이있
었다. 50%이상의무증상경동맥협착이 상이었던Veterans Affairs Cooperative Study (VACS) 연구에서
는경동맥내막절제술이동측신경학적증상 (ipsilateral neurologic event) 발생을2년간38% 감소시켰
다.10 60%이상무증상경동맥협착을 상으로하 던 Asymptomatic Carotid Atherosclerosis Study
(ACAS)11와Asymptomatic Carotid Surgery Trial (ACST)12연구결과를종합하면수술관련합병증또는 5
년뇌졸중발생율이경동맥내막절제술을미루거나내과적치료만시행한군의11.5%에비하여경동
맥내막절제술군에서는6.0%로유의하게낮았다. 세연구를메타분석한결과약3%의수술관련합병

56
CLINICAL RESEARCH CENTER FOR STROKE
증을고려하여도, 경동맥내막절제술은내과적치료에비해서동측또는모든뇌경색 (ipsilateral
stroke and any stroke)을3년간약30% 감소시켰다.13 경동맥혈관성형/스텐트설치술은경동맥내막
절제술의위험도가높은환자에서뇌졸중예방효과가경동맥내막절제술에비해낮지않았다.14
2. 새로운근거
내과적치료의발전으로무증상경동맥협착환자에서뇌졸중발생률이감소하고있다.15,16인구집단
기반연구인Oxford Vascular study는2002년- 2009년사이에일과성허혈발작또는뇌졸중이발생한
환자1153명중에서50% 이상의무증상경동맥협착이발견된101명환자들에게집중적내과적치료
(intensive medical therapy)를시행하면서무증상경동맥협착에의한일과성허혈발작또는뇌졸중발
생을301 환자-년 (평균3년) 동안추적관찰하 다.15 그결과무증상경동맥협착이있던혈관 역에
서6건의뇌허혈증상 (1건의경미한허혈뇌졸중과5건의일과성허혈발작)이발생하여, 평균연간발
생률이동측허혈뇌졸중 0.34% (95% CI, 0.01 to 1.87), 장애를남기는동측뇌졸중 0% (95% CI, 0.00 to
0.99), 동측일과성허혈발작1.78% (95% CI, 0.58 to 4.16)로매우낮았다.
지난25년간심한무증상경동맥협착환자의내과적치료군에서뇌졸중발생위험을체계적으로검
토 (systematic review)한연구가2009년에발표되었다. 내과적치료의발전으로동측및전체일과성
허혈발작또는뇌졸중발생률이1980년 중반이후계속감소하여2000년 이후연구에서는내과
적치료만시행하 음에도불구하고수술성적이우수하 던 1990년 에발표된주요임상시험의
수술군의뇌졸중발생률과비슷하거나오히려낮아지고있다.17
내막절제술과혈관성형/시텐트설치술을비교한가장 규모임상시험인Carotid Revascularization
Endarterectomy vs. Stenting Trial (CREST) 연구결과가 2010년에발표되었다.3일차결과변수 (primary
endpoint)는수술또는혈관성형/스텐트설치술30일이내뇌졸중, 심근경색, 사망및4년이내동측뇌
졸중발생률이었고, 2502명 (1181 무증상협착; 1321 증상성협착) 환자를추적기간중앙값2.5년동안
관찰하 다. 무증상과증상성경동맥협착환자들을모두합쳐서분석하 을때일차결과변수의발
생이스텐트설치술7.2%, 수술군6.8%로두치료가차이가없는것으로결론을내렸다 (hazard ratio
with stenting, 1.11; 95% CI, 0.81 to 1.51; p=0.51). 무증상경동맥협착환자들만따로분석한결과경동맥
혈관성혈/스텐트설치술군과내막절제수술군사이에일차결과변수발생률은차이가없었다 (5.6%
vs. 4.9%; hazard ratio, 1.17; 95% CI, 0.69 to 1.98; p=0.56). 뇌졸중발생만분석하 을때에도30일이내모
든뇌졸중과30일에서4년사이의동측뇌졸중발생이혈관성형/스텐트설치술군4.5%, 수술군2.7%
로유의한차이가없었다 (hazard ratio, 1.86; 95% CI, 0.95 to 3.66; p=0.07). 30일에서4년사이의동측뇌
57
CLINICAL RESEARCH CENTER FOR STROKE
졸중발생도혈관성형/스텐트설치술군2.0%, 수술군2.4%로비슷하게낮아, 두치료모두효과가장
기적으로잘유지되었다 (durability). 그러나혈관성형/스텐트설치술과수술을내과적치료와비교하
지못한제한점이있으며, 연구진들은내과적치료를하여도무증상경동맥협착에의한뇌졸중위험
이높지않을가능성이있다고언급하 다. 증상성및무증상협착전체환자를분석한결과, 혈관성
형/스텐트설치술군에서는뇌졸중발생이유의하게많았고, 경동맥내막절제술군에서는심근경색이
더많이발생하 다. 그러나뇌졸중이심근경색에비해환자의삶의질을더악화시킨것을고려하면
두치료가동등한효과를보 다는결론에 한비판이있다.18또한심근경색에는심전도의변화만
있는경우도포함되었으나뇌졸중의경우에는일과성뇌허혈이포함되지않아형평성에문제가있다
는비판도있다. 무증상경동맥협착군만분석하 을때에도유의하지는않았지만혈관성형/스텐트
설치술군에서뇌졸중발생이높고 (혈관성형/스텐트설치술군4.5% vs. 수술군2.7%; hazard ratio, 1.86;
95% CI, 0.95 to 3.66; p=0.07), 수술군에서심근경색발생이높은경향을보 다 (혈관성형/스텐트설치
술군1.2% vs. 수술군2.2%; hazard ratio, 0.55; 95% CI, 0.22 to 1.38; p=0.20).
60%이상무증상경동맥협착을 상으로경동맥내막절제술시행군과비수술군을비교한
Asymptomatic Carotid Surgery Trial (ACST-1)12연구의10년장기예후에 한추적연구가2010년에발
표되었다.19 3120명의무증상경동맥협착환자를사망시점또는생존자에 해서는중앙값9년동안
(IQR 6-11년) 추적관찰하 으며, 수술을받은모든환자들에서수술30일이내뇌졸중또는사망발생
률은3.0% (95% CI 2.4-3.9) 다. 수술30일이후에발생한뇌졸중은첫5년간수술군4.1% vs. 수술보류
군 10.0%로 5.9% (95% CI 4.0-7.8)의절 적차이를보 고, 10년간은수술군 10.8% vs. 수술보류군
16.9%로6.1% (95% CI, 2.7?9.4)의차이를보여수술군이수술보류군에비해서뇌졸중발생이상 적으
로46% (ratio of stroke incidence rates with CEA, 0.54; 95% CI, 0.43?0.68; p<0?0001) 유의하게감소하
다. 수술로인한뇌졸중또는사망을포함하여 (30일이내뇌졸중또는사망+ 30일이후뇌졸중) 장기
적인이득을분석하여도, 첫5년동안수술군6.9% vs. 수술보류군10.9%로4.1% (95%, CI 2.0?6.2)의차
이가있었고, 10년동안은수술군13.4% vs. 수술보류군17.9%로4.6% (95% CI, 1.2?7.9)의차이를보여,
수술과연관된뇌졸중또는사망을고려하여도수술군의성적이우수하 다. 특히추적기간동안발
생한287건의뇌졸중중절반이넘는166건이사망또는심각한장애를남기는뇌졸중이었는데, 수술
한경우에서전체뇌졸중이감소한정도와비슷한정도로사망또는심각한장애를남기는뇌졸중이
감소하 다. 발생부위가확인된뇌졸중을분석한결과, 경동맥협착동측의뇌졸중발생이가장크게
감소하 다(38 vs 92; relative Risk, 0.43; 95% CI, 0.28-0.68). 그러나협착과관련이없는 역의뇌졸중도
수술군에서유의하게감소하 다(contralateral stroke 39 vs 64; vertebrobasilar stroke 11 vs 23).

58
CLINICAL RESEARCH CENTER FOR STROKE
1. 무증상경동맥협착환자에서뇌졸중의치료가능한위험인자를조사하여동반된위험인자를집
중적으로치료해야한다.
1)고혈압이동반된경우, 140/90mmHg 미만을유지하기위한혈압강하치료가필요하다.
(근거수준Ia, 권고수준A)
2)흡연자는적극적으로금연치료를시행해야한다. (GPP)
3)LDL 콜레스테롤을100mg/dL 미만으로낮추기위한스타틴치료가필요하다.
(근거수준Ia, 권고수준A)
4)당뇨가동반된경우, 식이요법, 운동요법, 약물요법등을통한엄격한혈당조절이전체심뇌혈관질
환의예방을위해필요하다. (근거수준Ia, 권고수준A)
2.50% 이상의무증상경동맥협착환자에서금기사항이없는한항혈소판제제치료가권장된다.
(근거수준 IIa, 권고수준B) 50% 미만인환자에서항혈소판제제치료는동반된위험인자와출혈
부작용위험을고려하여결정하는것이바람직하다. (GPP)
3. 60-99% 무증상경동맥협착에서수술관련합병증이3% 미만인경우예방적경동맥내막절제술
또는혈관성형/스텐트설치술을고려할수있다. (경동맥내막절제술: 근거수준 Ia, 권고수준A;
혈관성형/스텐트설치술: 근거수준IIb, 권고수준B) 수술 상환자의선택에있어동반된질환, 기
여명, 환자의선호도와기타개인별요인들을신중하게고려하고치료에따른이득과위험에 해
충분한상의가필요하다. 경동맥내막절제술의이득은내과적치료의발전으로과거에비해감소
했을가능성이있어, 수술관련합병증에 한3% 기준을낮추는것을고려할수있다. 경동맥내막
절제술과달리혈관성형/스텐트설치술의경우내과적치료와직접비교한연구결과는없다.
4.수술이필요한60-99% 무증상경동맥협착환자에서경동맥내막절제술의수술위험성을높이는
동반질환이있는경우경동맥혈관성형/스텐트설치술을고려할수있다. (근거수준 IIa, 권고수준B)
그러나수술고위험군에서혈관성형/스텐트설치술과내과적치료를직접비교한연구결과는없다.

59
CLINICAL RESEARCH CENTER FOR STROKE
1. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC
European Carotid Surgery Trial (ECST). Lancet1998;351:1379-1387.
2. Ringleb PA, Allenberg J, Bruckmann H, Eckstein HH, Fraedrich G, Hartmann M, Hennerici M, Jansen O,
Klein G, Kunze A, Marx P, Niederkorn K, Schmiedt W, Solymosi L, Stingele R, Zeumer H, Hacke W. 30 day
results fromthe SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic
patients: a randomised non-inferiority trial. Lancet 2006;368:1239-1247.
3. Brott TG, Hobson RW, 2nd, Howard G, Roubin GS, Clark WM, Brooks W, Mackey A, HillMD, Leimgruber PP,
Sheffet AJ, Howard VJ, Moore WS, Voeks JH, Hopkins LN, Cutlip DE, Cohen DJ, Popma JJ, Ferguson RD,
Cohen SN, Blackshear JL, Silver FL, Mohr JP, Lal BK, Meschia JF. Stenting versus endarterectomy for
treatment of carotid-artery stenosis. N Engl J Med 2010;363:11-23.
4. O'Leary DH, Polak JF, Kronmal RA, Kittner SJ, Bond MG, Wolfson SK, Jr., Bommer W, Price TR, Gardin JM,
Savage PJ. Distribution and correlates of sonographically detected carotid artery disease in the
Cardiovascular Health Study. The CHS Collaborative Research Group. Stroke 1992;23:1752-1760.
5. Fine-Edelstein JS, Wolf PA, O'Leary DH, Poehlman H, Belanger AJ, Kase CS, D'Agostino RB. Precursors of
extracranial carotid atherosclerosis in the Framingham Study. Neurology 1994;44:1046-1050.
6. Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, Creager MA, Culebras A, Eckel RH,
Hart RG, Hinchey JA, Howard VJ, Jauch EC, Levine SR, Meschia JF, Moore WS, Nixon JV, Pearson TA.
Guidelines for the Primary Prevention of Stroke. A Guideline for Healthcare Professionals From the American
Heart Association/American Stroke Association. Stroke 2011;42:517-584.
7. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis
2008;25:457-507.
8. Brott TG HJ, Abbara S, Bacharach JM, Barr JD, Bush RL, Cates CU, Creager MA, Fowler SB, Friday G,
Hertzberg VS, McIff EB, Moore WS, Panagos PD, Riles TS, Rosenwasser RH, Taylor AJ. Guideline on the
management of patients with extracranial carotid and vertebral artery disease. Stroke 2011;42:e420-463.
9. Results of a randomized controlled trial of carotid endarterectomy for asymptomatic carotid stenosis. Mayo
Asymptomatic Carotid Endarterectomy Study Group. Mayo Clin Proc 1992;67:513-518.
10. Hobson RW, 2nd, Weiss DG, Fields WS, Goldstone J, Moore WS, Towne JB, Wright CB. Efficacy of carotid

60
CLINICAL RESEARCH CENTER FOR STROKE
endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group.
N Engl J Med1993;328:221-227.
11.Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic
Carotid Atherosclerosis Study. JAMA 1995;273:1421-1428.
12.Halliday A, Mansfield A, Marro J, Peto C, Peto R, Potter J, Thomas D. Prevention of disabling and fatal strokes
by successful carotid endarterectomy in patients without recent neurological symptoms: randomised
controlled trial. Lancet 2004;363:1491-1502.
13.Chambers BR, Donnan GA. Carotid endarterectomy for asymptomatic carotid stenosis. Cochrane Database
Syst Rev 2005:CD001923.
14.Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, Bajwa TK, Whitlow P, Strickman NE, Jaff
MR, Popma JJ, Snead DB, Cutlip DE, Firth BG, Ouriel K. Protected carotid-artery stenting versus
endarterectomy in high-risk patients. N Engl J Med 2004;351:1493-1501.
15.Marquardt L, Geraghty OC, Mehta Z, Rothwell PM. Low risk of ipsilateral stroke in patients with asymptomatic
carotid stenosis on best medical treatment: a prospective, population-based study.Stroke2010;41:e11-17.
16.Goessens BM, Visseren FL, Kappelle LJ, Algra A, van der Graaf Y. Asymptomatic carotid artery stenosis and
the risk of new vascular events in patients with manifest arterial disease: the SMART study. Stroke
2007;38:1470-1475.
17.Abbott AL. Medical (nonsurgical) intervention alone is now best for prevention of stroke associated with
asymptomatic severe carotid stenosis: results of a systematic review and analysis. Stroke2009;40:e573-583.
18.Davis SM, Donnan GA. Carotid-Artery Stenting in Stroke Prevention. N Engl J Med 2010;363:80-82.
19.Halliday A, Harrison M, Hayter E, Kong X, Mansfield A, Marro J, Pan H, Peto R, Potter J, Rahimi K, Rau A,
Robertson S, Streifler J, Thomas D. 10-year stroke prevention after successful carotid endarterectomy for
asymptomatic stenosis (ACST-1): a multicentre randomised trial. Lancet 2010;376:1074-1084.
61
CLINICAL RESEARCH CENTER FOR STROKE
여성에서뇌졸중발생은폐경이후급격히증가한다. 폐경후호르몬치료는실험연구및관찰연구들
에서심뇌혈관질환예방및뇌졸중중증도감소등의효과가기 되었으나, 임상시험에서는오히려
뇌졸중의발생을증가시키는것으로보고되었다.
1. It is recommended that postmenopausal hormone therapy (estrogen with or without a progestin) not be
used for primary prevention of stroke (ASA: Class III, Level of Evidence A) (EUSI: Level I).
2. The use of hormone replacement therapy for other indications should be informed by the risk estimate
for vascular outcomes provided by the reviewed clinical trials.
3. There are not sufficient data to provide recommendations about the use of other forms of therapy such
as selective estrogen receptor modulators.
59,337명의폐경후여성을16년간추적관찰한Nurses’Health Study1에서에스트로젠투여와뇌졸중
발생간의뚜렷한관련성은관찰되지않았다. Heart and Estrogen/progestin Replacement Study
II(HERS II) 연구2에서건강한폐경후여성에서호르몬치료는허혈성뇌졸중의위험을증가시키는경
향이관찰되었다. Women’s Health Initiative3는폐경후여성에서호르몬치료의심뇌혈관질환의일차
예방효과를평가하기위하여시행되었다. 본연구결과, 1년에10,000명을 상으로호르몬치료를
시행하는경우오히려8건의뇌졸중이증가하 으며, 자궁적출술을시행받은환자에서도뇌졸중
발생은호르몬치료를받은피험자에서유의하게증가하 다.4 (RR 1.39; 95% CI, 1.10-1.77) 28개임상
연구의메타분석결과에서도폐경후호르몬치료에의해뇌졸중발생은유의하게증가하 고, 호르
몬치료를받고있던경우에발생한뇌졸중의예후도더나쁜것으로확인되었다.5
1.2.8. 폐경후호르몬치료Postmenopausal hormone therapy

62
1. 뇌졸중의일차예방목적으로폐경후호르몬치료를하는것은권장하지않는다. (근거수준 Ia, 권고
수준A)
2. 다른적응증으로폐경후호르몬치료가필요한경우심뇌혈관질환의위험성증가에 한설명과
상담이필요하다. (권고수준GPP)
CLINICAL RESEARCH CENTER FOR STROKE
1. Grodstein F, Manson JE, Stampfer MJ. Postmenopausal hormone use and secondary prevention of
coronary events in the nurses' health study. A prospective, observational study. Ann Intern Med.
2001;135:1-8.
2. Grady D, Herrington D, Bittner V, Blumenthal R, Davidson M, Hlatky M, Hsia J, Hulley S, Herd A, Khan S,
Newby LK, Waters D, Vittinghoff E, Wenger N. Cardiovascular disease outcomes during 6.8 years of
hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA.
2002;288:49-57.
3. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Jackson RD,
Beresford SA, Howard BV, Johnson KC, Kotchen JM, Ockene J. Risks and benefits of estrogen plus
progestin in healthy postmenopausal women: principal results From the Women's Health Initiative
randomized controlled trial. JAMA. 2002;288:321-333.
4. Anderson GL, Limacher M, Assaf AR, Bassford T, Beresford SA, Black H, Bonds D, Brunner R, Brzyski R,
Caan B, Chlebowski R, Curb D, Gass M, Hays J, Heiss G, Hendrix S, Howard BV, Hsia J, Hubbell A,
Jackson R, Johnson KC, Judd H, Kotchen JM, Kuller L, LaCroix AZ, Lane D, Langer RD, Lasser N, Lewis
CE, Manson J, Margolis K, Ockene J, O'Sullivan MJ, Phillips L, Prentice RL, Ritenbaugh C, Robbins J,
Rossouw JE, Sarto G, Stefanick ML, Van Horn L, Wactawski-Wende J, Wallace R, Wassertheil-Smoller
S. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's
Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
5. Bath PM, Gray LJ. Association between hormone replacement therapy and subsequent stroke: a meta-
analysis. BMJ.2005;330:342.

63
CLINICAL RESEARCH CENTER FOR STROKE
과일과야채를많이섭취하면뇌졸중예방에도움이된다. 나트륨섭취를줄이고칼륨섭취를늘리
는것도뇌졸중예방효과가있다. 이러한식이요법의뇌졸중예방효과는혈압강하효과에의한것
으로보인다.
1. A reduced intake of sodium and increased intake of potassium is recommended to lower blood pressure
in persons with hypertension (ASA: Class I, Level of Evidence A), which may thereby reduce the risk of
stroke. The recommended sodium intake is ≤2.3g/d (100mmol/d), and the recommended potassium
intake is ≥4.7 /d (120mmol/d).
2. The DASH diet, which emphasizes fruit, vegetables, and low-fat dairy products and is reduced in
saturated and total fat, also lowers blood pressure and is recommended (ASA: Class I, Level of Evidence A).
3. A diet that is rich in fruits and vegetables may lower the risk of stroke and may be considered. A diet
containing ≥5 servings of fruits and vegetables per day may reduce the risk of stroke (ASA: Class IIb,
Level of Evidence C).
4. A low salt, low saturated fat, high fruit and vegetable diet rich in fibre is recommended (EUSI: Level II).
5. Subjects with an elevated body mass index should take a weight reducing diet (EUSI: Level II).
관찰연구에의하면과일과야채의섭취가증가할수록뇌졸중발생은감소하는용량반응관계(dose-
response)를보인다. 과일과야채의하루섭취량이1회분량1만큼증가할때마다뇌졸중위험이6%
감소하 다.2,3
1.2.9. 식이와 양Diet and nutrition

64
CLINICAL RESEARCH CENTER FOR STROKE
생태학적(ecological) 전향적연구에의하면나트륨섭취증가는뇌졸중발생의증가, 그리고칼륨섭
취증가는뇌졸중발생감소와상관관계를보 다.4-6전향적코호트연구결과, 나트륨섭취에따른뇌
졸중발생위험은비만정도에따라차이가있었는데, 비만한사람의경우에는하루100mmol(2.3g) 이
상의나트륨섭취가뇌졸중발생위험을32% 증가시켰으나, 비만하지않은사람에게서는뇌졸중발
생위험을증가시키지않았다.4다른연구에서는하루4.3g 칼륨섭취군이하루2.4g 칼륨섭취군에비
해뇌졸중상 위험이0.62(95% CI, 0.43-0.88)로낮았다.7다른식이요소(dietary factor)도뇌졸중발생
과관련이있을가능성이있으나아직까지는충분한근거를찾을수는없다.
1. 혈압강하와뇌졸중예방을위해저나트륨식이와고칼륨식이가권장된다. (근거수준 Ia, 권고수준
A) 하루나트륨양은2.3g (100mmol) 이하, 소금으로는6g 이하가추천되며, 하루칼륨섭취량은4.7g
(120mmol) 이상이추천된다.
2. 과일, 야채, 저지방유제품(low-fat dairy product: 저지방우유, 치즈, 요거트)의섭취를늘리고포화또
는총지방량(saturated and total fat)의섭취를줄이는식이요법이권장된다. (근거수준Ib, 권고수준A)
3. 과일과야채가풍부한식이(매일5회분량이상의과일과야채)가권장된다. (근거수준III, 권고수준B)
4. 체질량지수(body mass index, BMI)가높은경우체중감량식이가권장된다. (근거수준Ib, 권고수준A)
1. 한당뇨병학회, 한 양사회, 한국 양학회. 당뇨병식사요법지침서2판. 1995.
2. Joshipura KJ, Ascherio A, Manson JE, Stampfer MJ, Rimm EB, Speizer FE, Hennekens CH, Spiegelman
D, Willett WC. Fruit and vegetable intake in relation to risk of ischemic stroke. JAMA. 1999;282:1233-1239.
3. Mozaffarian D, Kumanyika SK, Lemaitre RN, Olson JL, Burke GL, Siscovick DS. Cereal, fruit, and
vegetable fiber intake and the risk of cardiovascular disease in elderly individuals. JAMA. 2003;289:1659-
야채(시금치, 양배추, 상치, 오이, 콩나물, 호박, 당근, 무) 70g 또는익힌야채1/3컵
과일: 배1/4개, 사과1/3개, 사과주스1/2컵, 참외1/2개, 바나나1/2개, 오렌지1/2개, 오렌지쥬스1/2컵, 귤1개, 토마토1개, 딸기10개, 포도
1회분량

65
CLINICAL RESEARCH CENTER FOR STROKE
규칙적인신체활동에의해조기사망과심뇌혈관질환사망이감소하며, 이는뇌졸중예방에도도움
이된다. 이결과는신체활동이혈압을낮추고, 혈당을조절하며, 체중을감소시키는과정에의해나
타나는것으로알려져있다.
1. Increased physical activity is recommended because it is associated with a reduction in the risk of stroke
(ASA: Class I, Level of Evidence B). Exercise guidelines as recommended by the CDC and the National
Institutes of Health of regular exercise (≥30 minutes of moderate-intensity activity daily) as part of a
healthy lifestyle are reasonable (Class IIa, Level of Evidence B).
1666.
4. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA,
Windhauser MM, Lin PH, Karanja N. A clinical trial of the effects of dietary patterns on blood pressure.
DASH Collaborative Research Group. N Engl J Med. 1997;336:1117-1124.
5. He J, Ogden LG, Vupputuri S, Bazzano LA, Loria C, Whelton PK. Dietary sodium intake and subsequent
risk of cardiovascular disease in overweight adults.JAMA. 1999;282:2027-2034.
6. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, Obarzanek E, Conlin PR, Miller ER,
3rd, Simons-Morton DG, Karanja N, Lin PH. Effects on blood pressure of reduced dietary sodium and
the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research
Group. N Engl J Med. 2001;344:3-10.
7. Ascherio A, Rimm EB, Hernan MA, Giovannucci EL, Kawachi I, Stampfer MJ, Willett WC. Intake of
potassium, magnesium, calcium, and fiber and risk of stroke among US men. Circulation.
1998;98:1198-1204.
1.2.10. 신체활동Physical activity

66
2. Regular physical activity is recommended (EUSI: Level II).
CLINICAL RESEARCH CENTER FOR STROKE
신체활동의증가는허혈성뇌졸중을감소시킬수있는데, Oslo Study, Honolulu Heart Program, 그리
고 Framingham Heart Study 등은남자에서의예방효과를,1-3 그리고 Nurses’Health Study 와
Copenhagen City Heart Study 등은여자에서의예방효과를증명하 다.4,5이전의연구에서는운동량
에따른양-반응관계가명확하지않았으나,3최근의연구에서는운동량이많은경우, 운동량이적거
나중등도인경우에비하여허혈성뇌졸중발생이유의하게감소된다고보고하고있다.6하지만노인
에서격렬한운동량을보이는군의수가많지않음을고려해야한다.
신체활동에의한뇌졸중발생의감소효과는혈압을떨어뜨리고, 체중을감소시키며, 혈당을조절하
고, 심뇌혈관질환의다른위험인자들을조절하는것으로일부설명될수있다.
미국질병관리본부(CDC)와국립보건원(NIH)에서는중등도의운동을가능한매일 30분이상시행할
것을권고하고있다.7
1. 뇌졸중의일차예방을위해신체활동을늘리는것이필요하다. (근거수준III, 권고수준B).
2. 규칙적인운동(매일30분이상의중등도운동)이뇌졸중예방에도움이될수있다. (근거수준 III, 권
고수준B)
1. Haheim LL, Holme I, Hjermann I, Leren P. Risk factors of stroke incidence and mortality. A 12-year
follow-up of the Oslo study.Stroke.1993;24:1484-1489.
2. Abbott RD, Rodriguez BL, Burchfiel CM, Curb JD. Physical activity in older middle-aged men and
reduced risk of stroke: The Honolulu heart program. Am J Epidemiol. 1994;139:881-893.
3. Kiely DK, Wolf PA, Cupples LA, Beiser AS, Kannel WB. Physical activity and stroke risk: The Framingham
study. Am J Epidemiol. 1994;140:608-620.
4. Manson JE, Colditz GA, Stampfer MJ, Willett WC, Krolewski AS, Rosner B, Arky RA, Speizer FE,

67
CLINICAL RESEARCH CENTER FOR STROKE
한국인에서의비만은체질량지수[Body Mass Index(BMI): 체중(Kilogram)/{키(meter)}2]가25 이상인경
우로정의된다. 복부비만은허리둘레를기준으로, 남자는90cm, 여자는85cm 이상인경우로정의된
다. 2005년국민건강 양조사결과에의하면, 20세이상성인에서비만의유병율은 31.7%(남자:
35.1%, 여자: 28.0%)이며, 1998년의 26.3%(남자: 25.0%, 여자: 27.0%)에비하여점차증가하는추세이
다.1비만의정도가심할수록뇌졸중의발생위험이비례하여증가하는것으로알려져있다.
1. Epidemiological studies indicate that increased body weight and abdominal fat are directly associated
with stroke risk. Weight reduction is recommended because it lowers blood pressure (ASA: Class I, Level
of Evidence A) and may thereby reduce the risk of stroke.
Hennekens CH. A prospective study of maturity-onset diabetes mellitus and risk of coronary heart
disease and stroke in women. Arch Intern Med. 1991;151:1141-1147.
5. Lindenstrom E, Boysen G, Nyboe J. Lifestyle factors and risk of cerebrovascular disease in women. The
Copenhagen city heart study. Stroke. 1993;24:1468-1472.
6. Sacco RL, Gan R, Boden-Albala B, Lin IF, Kargman DE, Hauser WA, Shea S, Paik MC. Leisure-time
physical activity and ischemic stroke risk: The Northern Manhattan stroke study. Stroke. 1998;29:380-
387.
7. Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, Buchner D, Ettinger W, Heath GW,
King AC, et al. Physical activity and public health. A recommendation from the centers for disease
control and prevention and the American College of Sports Medicine. JAMA. 1995;273:402-407.
1.2.11. 비만Obesity

68
CLINICAL RESEARCH CENTER FOR STROKE
234,863명의 40-64세남성을 상으로시행한한국의료보험공단연구(Korean Medical Insurance
Corporation Study)에서BMI 1U 당전체뇌졸중의보정상 위험도는1.04(95% CI, 1.03-1.05), 허혈성뇌
졸중은1.06(95% CI, 1.04-1.07), 출혈성뇌졸중은1.02(95% CI, 1.00-1.05)이었다.2 21,414명의남성의료전
문가들을 상으로시행한연구에서과체중, 그리고비만인남성을정상체중인남성과비교할때전
체뇌졸중발생의보정상 위험도는각각1.32(95% CI, 1.14-1.54)와1.91(95% CI, 1.45-2.52)이고, 허혈성
뇌졸중은 1.35(95% CI, 1.15-1.59)와 1.87(95% CI, 1.38-2.54), 출혈성뇌졸중은 1.25(95% CI, 0.84-1.88)와
1.92(95% CI, 0.94-3.93)로보고되었다.3또한복부비만이뇌졸중의위험을더잘예측할수있다는보고
들도있다.4-6 현재까지체중을감소시켜뇌졸중발생을줄인다는임상시험은없지만, 많은연구에서
체중감소는혈압을떨어뜨리는것으로확인되었다. 25개임상시험의메타분석에의하면5.1kg의체
중감소로수축기혈압4.4mmHg, 이완기혈압3.6mmHg이감소되었다.7
1. 체중을감소시키면혈압을낮출수있고 (근거수준 Ia, 권고수준A), 혈압강하효과를통하여뇌졸중
을예방할수있다(근거수준III, 권고수준B).
1. 국민건강 양조사. 질병관리본부. 2006.
2. Song YM, Sung J, Davey Smith G, Ebrahim S. Body mass index and ischemic and hemorrhagic stroke: a
prospective study in Korean men. Stroke.2004;35:831-836.
3. Kurth T, Gaziano JM, Berger K, Kase CS, Rexrode KM, Cook NR, Buring JE, Manson JE. Body mass
index and the risk of stroke in men. Arch Intern Med. 2002;162:2557-2562.
4. Folsom AR, Prineas RJ, Kaye SA, Munger RG. Incidence of hypertension and stroke in relation to body fat
distribution and other risk factors in older women. Stroke. 1990;21:701-706.
5. Suk SH, Sacco RL, Boden-Albala B, Cheun JF, Pittman JG, Elkind MS, Paik MC. Abdominal obesity and
risk of ischemic stroke: the Northern Manhattan Stroke Study. Stroke.2003;34:1586-1592.
6. Walker SP, Rimm EB, Ascherio A, Kawachi I, Stampfer MJ, Willett WC. Body size and fat distribution as
69
CLINICAL RESEARCH CENTER FOR STROKE
predictors of stroke among US men. Am J Epidemiol.1996;144:1143-1150.
7. Neter JE, Stam BE, Kok FJ, Grobbee DE, Geleijnse JM. Influence of weight reduction on blood pressure:
a meta-analysis of randomized controlled trials. Hypertension. 2003;42:878-884.
CLINICAL RESEARCH CENTER FOR STROKE
1.3. 조절가능한잠재적위험인자Less well-documented or potentially modifiable risk factors
1.3.1. 사증후군Metabolic syndrome
사증후군은인슐린저항성과함께복부비만, 이상지질혈증, 내당기능장애, 고혈압등이동반되는
경우이다. 최근유병률이급격히증가하고있으며, 당뇨병뿐만아니라뇌졸중을비롯한심뇌혈관질
환의위험성을증가시킨다. 사증후군의다양한진단기준이제시되고있는데, 국제당뇨병연맹
(International Diabetes Federation)이제시한동양인의진단기준은표1과같다. 1
70
* 체질량지수가30 kg/m2이상인경우에는허리둘레와상관없이복부비만으로간주됨.
복부비만
허 리 둘 레*: 남자≥90cm, 여자≥80cm (아시아인기준)
복부비만과아래항목중2가지이상을가지는경우
중성지방혈증: >150mg/dL (1.7mmol/L) 또는약물치료중
고 도지단백콜레스테롤 : 남자<40mg/dL (1.03mmol/L), 여자<50mg/dL (1.29mmol/L), 또는약제치료중
혈압 : 수축기≥130mm Hg 또는이완기≥80mmHg 또는약제치료중.
공복혈당 : ≥100mg/dL (5.6mmol/L) 또는제2형당뇨병진단받은경우.
(100mg/dL 이상인경우 사증후군유무를판정하기위해서추가적인경구당부하검사를실시할필요는없으나환자의치료적측면에서권장된다.)
표. 사증후군의정의: 국제당뇨병연맹 (International Diabetes Federation) 1
1. Management of individual components of the metabolic syndrome, including lifestyle measures and
pharmacotherapy as recommended in the National Cholesterol Education Program ATP III2 and the
JNC 7,3 as reviewed in other sections of this guideline, are endorsed. Lifestyle management should
include exercise, appropriate weight loss, and proper diet. Pharmacotherapy may include medications
for blood pressure lowering, lipid lowering, glycemic control, treatment of microalbuminuria or
proteinuria, and antiplatelet therapy (eg, aspirin) according to the individual circumstance and risk. It is

71
CLINICAL RESEARCH CENTER FOR STROKE
사증후군의가장중요한요소는인슐린저항성이다. 인슐린저항성이뇌졸중의위험인자인지에
한논란이있으나, 최근의메타연구에서인슐린저항성이뇌졸중의독립적인위험인자인것으로
보고되고있다.4
2001년국민건강 양조사자료를분석한단면적연구에서국제당뇨협회기준에따른 사증후군이
있는경우뇌졸중의 응위험도는 2.3(95% CI, 1.3-4.0)으로보고되었다.5일본의전향적코호트연구
에서 사증후군의뇌졸중발생위험도(hazard ratio)는남자에서 2.0(95% CI, 1.3-3.1), 여자에서
1.5(95% CI, 1.0-2.3)로유의하게증가됨이보고되었다.6
아직까지인슐린저항성을개선하면뇌졸중발생을감소시킨다는근거는없지만, 뇌졸중예방을위
하여 사증후군의각요소들에 한생활습관개선, 약물치료등이권장되고있다.
1. 사증후군은뇌졸중의위험인자이며, 각각의요인들을조절하기위한생활방식개선, 약물치료가
권장된다. (근거수준III, 권고수준B)
not known whether agents that ameliorate aspects of the insulin resistance syndrome are useful for
reducing stroke risk. (ASA)
1. Alberti KG, Zimmet P, Shaw J. The metabolic syndrome--a new worldwide definition. Lancet. 2005;366:1059-
1062.
2. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert
Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III).
JAMA.2001;285:2486-2497.
3. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., Jones DW, Materson BJ, Oparil S,
Wright JT, Jr., Roccella EJ. Seventh report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.

72
4. Kernan WN, Inzucchi SE, Viscoli CM, Brass LM, Bravata DM, Horwitz RI. Insulin resistance and risk for stroke.
Neurology. 2002;59:809-815.
5. Choi KM, Kim SM, Kim YE, Choi DS, Baik SH, Lee J. Prevalence and cardiovascular disease risk of the
metabolic syndrome using National Cholesterol Education Program and International Diabetes Federation
definitions in the Korean population. Metabolism. 2007;56:552-558.
6. Iso H, Sato S, Kitamura A, Imano H, Kiyama M, Yamagishi K, Cui R, Tanigawa T, Shimamoto T. Metabolic
syndrome and the risk of ischemic heart disease and stroke among Japanese men and women. Stroke.
2007;38:1744-1751.
CLINICAL RESEARCH CENTER FOR STROKE
1. For those who consume alcohol, a recommendation of ≤2 drinks per day for men and ≤1 drink per
day for nonpregnant women best reflects the state of the science for alcohol and stroke risk (ASA: Class
IIb, Level of Evidence B).
2. Heavy use of alcohol should be discouraged, light or moderate alcohol consumption may be protective
against stroke (EUSI: Level I).
부분의연구에서음주량과허혈성뇌졸중의발생위험간에는“J”자모양의관련성이있다고알려
져있다.1-5즉소량혹은중등도(일반적으로하루2잔이하)의음주는술을전혀마시지않는경우에비
해뇌졸중발생이낮았고, 다량의음주는뇌졸중의위험을증가시켰다. 35개관찰연구의메타분석결
여러후향적코호트연구는소량혹은중등도의음주, 특히포도주는뇌졸중발생을감소시킨다고보
고했다. 그러나다량의음주는오히려뇌졸중발생을증가시키는것으로알려져있다.
1.3.2. 음주Alcohol

73
CLINICAL RESEARCH CENTER FOR STROKE
1. 건강의여러측면을고려하여볼때, 과도음주자(heavy drinker)는음주를줄이는것이권고된다. 음
주자의경우, 알코올과뇌졸중의위험을고려할때남성은하루2잔이하, 비임신여성은하루1잔
이하가적절하다. (근거수준III, 권고수준B)
1. Berger K, Ajani UA, Kase CS, Gaziano JM, Buring JE, Glynn RJ, Hennekens CH. Light-to-moderate
alcohol consumption and risk of stroke among U.S. male physicians. N Engl J Med.1999;341:1557-1564.
2. Djousse L, Ellison RC, Beiser A, Scaramucci A, D'Agostino RB, Wolf PA. Alcohol consumption and risk of
ischemic stroke: The Framingham Study. Stroke. 2002;33:907-912.
3. Gorelick PB, Rodin MB, Langenberg P, Hier DB, Costigan J. Weekly alcohol consumption, cigarette
smoking, and the risk of ischemic stroke: results of a case-control study at three urban medical centers
in Chicago, Illinois. Neurology. 1989;39:339-343.
4. Sacco RL, Elkind M, Boden-Albala B, Lin IF, Kargman DE, Hauser WA, Shea S, Paik MC. The protective
effect of moderate alcohol consumption on ischemic stroke. JAMA. 1999;281:53-60.
5. Stampfer MJ, Colditz GA, Willett WC, Speizer FE, Hennekens CH. A prospective study of moderate
alcohol consumption and the risk of coronary disease and stroke in women. N Engl J Med.
1988;319:267-273.
6. Reynolds K, Lewis B, Nolen JD, Kinney GL, Sathya B, He J. Alcohol consumption and risk of stroke: a
meta-analysis. JAMA. 2003;289:579-588.
과에의하면하루5잔(1잔= 알코올12g) 이상을마시는사람은전혀마시지않는사람에비하여뇌졸
중발생위험이69% 증가되었다.6

74
약물남용은수많은건강문제와함께심각한사회문제를일으키는만성적이며재발이높은질환이
다. 코카인(cocaine), 암페타민(amphetamine), 헤로인(heroin) 등의복용은뇌졸중발생과관련성이있
다.1
CLINICAL RESEARCH CENTER FOR STROKE
1.3.3. 약물남용Drug abuse
1. Successful identification and management of drug abuse can be challenging. When a patient is identified
as having a drug addiction problem, referral for appropriate counseling may be considered (ASA: Class
IIb, Level of Evidence C).
코카인, 암페타민, 헤로인등의교감신경흥분제들은뇌출혈및뇌경색발생위험을모두증가시킨
다.1,2이러한약물들은급격한혈압상승을유발하여뇌출혈위험을증가시키며, 국소적인동맥수축
과염증성혈관염을유발하여뇌경색의위험또한증가시킨다.3이외에도감염성심내막염의유발,
혈액응고성및혈소판응집력을증가시켜뇌경색을유발할수있다.3,4한연구에의하면약물남용은
모든연령에있어서뇌졸중의위험도를6.5배(95% CI, 3.1-13.6) 증가시키며, 특히35세미만에서는그
상 적위험도가11.2배(95% CI, 3.2-42.5)가되는것으로보고되어있다.5
1. 코카인, 암페타민, 헤로인등의교감신경흥분제들은뇌졸중발생위험도를증가시키므로복용하
지말아야한다. (근거수준III, 권고수준B)
2. 약물남용환자에게적절한의학적상담을권장하는것이바람직하다. (근거수준IV, 권고수준C)

75
CLINICAL RESEARCH CENTER FOR STROKE
경구용피임제가허혈성뇌졸중을유발할수있다는근거는고용량의여성호르몬이함유되어있는
1세 경구용피임제를 상으로시행된초기의연구에서나온것이다. 저용량의여성호르몬이함
유되어있는최근의경구용피임제는뇌졸중의위험을증가시키지않는것으로보인다.
1. The incremental risk of stroke associated with use of low dose oral contraceptives in women without
additional risk factors appears low, if one exists (ASA: Class III, Level of Evidence B).
2. It is suggested that oral contraceptives be discouraged in women with additional risk factors (eg,
cigarette smoking or prior thromboembolic events) (ASA: Class III, Level of Evidence C).
1.3.4. 경구용피임제Oral contraceptive use
1. O'Connor AD, Rusyniak DE, Bruno A. Cerebrovascular and cardiovascular complications of alcohol and
sympathomimetic drug abuse. Med Clin North Am. 2005;89:1343-1358.
2. Brust JCM. Neurological Aspects of Substance Abuse. 2nd ed. Philadelphia, Pa: Butterworth-Heinemann;
2004.
3. Neiman J, Haapaniemi HM, Hillbom M. Neurological complications of drug abuse: pathophysiological
mechanisms. Eur J Neurol.2000;7:595-606.
4. Siegel AJ, Sholar MB, Mendelson JH, Lukas SE, Kaufman MJ, Renshaw PF, McDonald JC, Lewandrowski
KB, Apple FS, Stec JJ, Lipinska I, Tofler GH, Ridker PM. Cocaine-Induced Erythrocytosis and Increase in von
Willebrand Factor: Evidence for Drug-Related Blood Doping and Prothrombotic Effects. Arch Intern Med.
1999;159:1925-1929.
5. Kaku DA, Lowenstein DH. Emergence of recreational drug abuse as a major risk factor for stroke in young
adults. Ann Intern Med. 1990;113:821-827.

76
3. For those who elect to assume the increased risk, aggressive therapy of stroke risk factors may be
useful (ASA: Class IIb, Level of Evidence C).
CLINICAL RESEARCH CENTER FOR STROKE
메타분석1에의하면저용량의여성호르몬이함유되어있는최근의경구용피임제는뇌졸중의위험
을증가시키지않았다. 4개의코호트연구메타분석에의하면경구용피임제의뇌졸중발생 응비
(odds ratio)는0.95(95% CI, 0.51-1.78)로유의한차이가없었다. 36세이상의연령, 흡연, 고혈압, 당뇨, 편
두통, 혈전색전증의과거력등이있는경우경구용피임제를사용하면뇌졸중의위험이증가할수있
다.2-6이러한위험인자를가지고있는여성의경우경구용피임제를피하는것이바람직하며, 부득이
하게경구용피임제를복용해야하는경우동반된뇌졸중의위험인자들에 한철저한치료를시행
하는것이바람직하다.7
1. 뇌졸중위험인자가없는여성에서저용량의경구용피임제가뇌졸중위험을증가시킬가능성은
낮다. (근거수준III, 권고수준B)
2. 흡연이나혈전색전증등의뇌졸중위험인자가있는여성에서는경구용피임제복용을피하는것이
바람직하다. (근거수준III, 권고수준B)
3. 뇌졸중위험인자가있지만경구용피임제를복용해야하는경우위험인자에 한철저한치료를
시행하는것이바람직하다. (근거수준IV, 권고수준C)
1. Chan WS, Ray J, Wai EK, Ginsburg S, Hannah ME, Corey PN, Ginsberg JS. Risk of stroke in women
exposed to low-dose oral contraceptives: A critical evaluation of the evidence. Arch Intern Med.
2004;164:741-747.
2. Ischaemic stroke and combined oral contraceptives: Results of an international, multicentre, case-
control study. WHO collaborative study of cardiovascular disease and steroid hormone contraception.
Lancet. 1996;348:498-505.

77
CLINICAL RESEARCH CENTER FOR STROKE
수면중호흡장애는고혈압, 복부비만등과같은뇌졸중위험인자들과깊은관련성을가질뿐아니
라그자체가독립적으로뇌졸중의위험인자인것으로주장되고있다.1특히충분한약물치료에도
불구하고잘조절되지않는난치성고혈압의주요요인중하나이며수면중호흡장애에 한성공
적인치료는혈압을유의하게떨어뜨리는것으로보고된바도있다.1그러나뇌졸중주요위험인자
들사이의복잡한연관관계들때문에수면중호흡장애가뇌졸중의직접적인원인인지아니면뇌
졸중위험인자의발생을증가시켜연관성을가지는것인지에 해서는아직명확하지않으며수면
중호흡장애에 한치료가뇌졸중의발생을줄일수있는가에 해구체적인임상연구또한아직
시행된바가없다.
3. Schwartz SM, Siscovick DS, Longstreth WT, Jr., Psaty BM, Beverly RK, Raghunathan TE, Lin D, Koepsell
TD. Use of low-dose oral contraceptives and stroke in young women. Ann Intern Med. 1997;127:596-
603.
4. Becker WJ. Use of oral contraceptives in patients with migraine. Neurology.1999;53:S19-25.
5. Siritho S, Thrift AG, McNeil JJ, You RX, Davis SM, Donnan GA. Risk of ischemic stroke among users of
the oral contraceptive pill: The Melbourne risk factor study (MERFS) group. Stroke. 2003;34:1575-1580.
6. Lidegaard O. Oral contraceptives, pregnancy and the risk of cerebral thromboembolism: The influence
of diabetes, hypertension, migraine and previous thrombotic disease. Br J Obstet Gynaecol.
1995;102:153-159.
7. Bousser MG, Conard J, Kittner S, de Lignieres B, MacGregor EA, Massiou H, Silberstein SD, Tzourio C.
Recommendations on the risk of ischaemic stroke associated with use of combined oral contraceptives
and hormone replacement therapy in women with migraine. The International Headache Society task
force on combined oral contraceptives & hormone replacement therapy. Cephalalgia. 2000;20:155-156.
1.3.5. 수면중호흡장애Sleep Disordered Breathing

78
1. Questioning bed partners and patients, particularly those with abdominal obesity and hypertension, about
symptoms of sleep disordered breathing (SDB) and referral to a sleep specialist for further evaluation as
appropriate may be reasonable, especially in the setting of drug-resistant hypertension (ASA: Class IIb,
Level of Evidence C).
CLINICAL RESEARCH CENTER FOR STROKE
최근에보고된 규모의전향적관찰연구에의하면수면중무호흡증은뇌졸중발생의독립적위험
인자이며, 그정도가심할수록비례하여뇌졸중의위험이증가하는것으로보고되었다.2뿐만아니라
뇌졸중의주요위험인자인고혈압및심장질환의발생위험을증가시키며,3,4특히약물치료에반응
하지않는고혈압과유의한관련성을가지는것으로보고되었다.5이와관련하여수면무호흡증에
한성공적인치료가일중평균혈압을유의하게낮추어주었다는 규모연구결과도보고된바도있
다.6그러나야간혈압은유의하게낮추는데비해낮시간의혈압조절에 한효과는아직명확하지
않으며,1또한심뇌혈관질환의발병위험을줄일수있는지에 해서도확실치는않다.2,7
1. 심뇌혈관질환의병력이있거나비만및고혈압등의위험인자를가진환자들의경우수면중습관
성코골이나낮시간졸림증과같이수면무호흡증을의심할수있는증상들의유무를알아보는것
이바람직하며, 특히약물로잘조절되지않는고혈압환자들의경우적절한평가를위해수면전문
가에게의뢰하는것을고려할수있다. (근거수준III, 권고수준B)
2. 뇌졸중예방을위하여일률적으로수면무호흡증의검사및치료를권고할근거는부족하다. (근거
수준III, 권고수준B)
1. Caples SM, Garcia-Touchard A, Somers VK. Sleep-disordered breathing and cardiovascular risk. Sleep.
2007;30:291-303.

79
CLINICAL RESEARCH CENTER FOR STROKE
편두통은 부분40 이하에서발생되며전생애에걸쳐지속되는비교적흔한질환이다. 편두통의
유병율은12%이며특히여성의유병률이남성보다3배정도높다.1편두통과뇌졸중의관련성은젊
은여성에서보고되고있다.
1. There are insufficient data to recommend a specific treatment approach that would reduce the risk
2. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a
risk factor for stroke and death. N Engl J Med.2005;353:2034-2041.
3. Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, D'Agostino RB, Newman AB, Lebowitz
MD, Pickering TG. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large
community-based study. Sleep heart health study. JAMA. 2000;283:1829-1836.
4. Yamashita T, Murakawa Y, Sezaki K, Inoue M, Hayami N, Shuzui Y, Omata M. Circadian variation of
paroxysmal atrial fibrillation. Circulation.1997;96:1537-1541.
5. Logan AG, Perlikowski SM, Mente A, Tisler A, Tkacova R, Niroumand M, Leung RS, Bradley TD. High
prevalence of unrecognized sleep apnoea in drug-resistant hypertension. J Hypertens. 2001;19:2271-
2277.
6. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, Mullins R, Jenkinson C, Stradling JR, Davies RJ.
Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway
pressure for obstructive sleep apnoea: A randomised parallel trial. Lancet. 2002;359:204-210.
7. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with
obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway
pressure: An observational study. Lancet. 2005;365:1046-1053.
1.3.6. 편두통Migraine

80
of first stroke in women with migraine, including migraine with aura (ASA).
CLINICAL RESEARCH CENTER FOR STROKE
6개환자- 조군연구의메타분석에의하면편두통과뇌졸중발생사이의 응비(odds ratio, OR)는
2.08(95% CI, 1.68-2.58)이었다.2편두통의뇌졸중발생 응비가2라는가정하에다른뇌졸중위험인자
의 향을고려하지않을경우, 20세에서44세사이여성에서의뇌졸중발생에 한편두통의인구집
단귀속위험도(population-attributable risk)는약17%로추정된다.2그러나 부분의환자- 조군연구
에서편두통의빈도및강도와뇌졸중발생과의관계를조사하지는않았으며, 현재까지편두통예방
치료가뇌졸중발생을줄인다는구체적증거는없다.1,3
전조증상을동반한편두통에서후부순환계(posterior circulation)의혈류속도및혈류량의감소, 핍혈
(oligemia)등이뇌졸중발생위험과관련되어있다고알려져있다.4또한전조증상을동반한편두통에
서비교적흔한것으로알려진열린타원구멍(patent foramen ovale, PFO)을통한역설적색전증
(paradoxical embolism)도뇌졸중발생과관련이있을것으로추정되며, 그외혈소판활성도증가가관
여한다는주장도있다.5
1. 여성편두통(전조증상을가진편두통포함) 환자에서, 뇌졸중일차예방을위하여권장할수있는편
두통치료방법에 한근거는부족하다. (근거수준IV, 권고수준C)
1. Bousser MG, Welch KM. Relation between migraine and stroke. Lancet Neurol. 2005;4:533-542.
2. Schwaag S, Nabavi DG, Frese A, Husstedt IW, Evers S. The association between migraine and juvenile
stroke: a case-control study. Headache. 2003;43:90-95.
3. Bushnell CD. Migraine and risk of ischemic stroke: an evidence-based medicine review. J Clin Outcomes
Manage. 2001;3:33-39.
4. Sanchez del Rio M, Bakker D, Wu O, Agosti R, Mitsikostas DD, Ostergaard L, Wells WA, Rosen BR,

81
CLINICAL RESEARCH CENTER FOR STROKE
호모시스테인은메치오닌 사과정중만들어지는아미노산의한종류이다. 전향적관찰연구, 환
자- 조군연구및메타분석연구들에서혈중호모시스테인이높을수록관상동맥질환과뇌졸중을
포함한심뇌혈관질환발생위험이증가하는것으로보고되었다. 또한비타민 [엽산(folic acid), 코발
라민(Cobalamine; Vitamin B12), 피리독신(pyridoxine; Vitamin B6)] 투여가혈중호모시스테인을효과적
으로낮추는것으로알려졌다. 그러나혈중호모시스테인의상승과뇌졸중을포함한심뇌혈관질환
발생과의인과관계는아직불분명하다.
1. Recommendations to meet current guidelines for daily intake of folate (400g/d), B6 (1.7g/d), and B12
(2.4g/d) by consumption of vegetables, fruits, legumes, meats, fish, and fortified grains and cereals (for
nonpregnant, nonlactating individuals) may be useful in reducing the risk of stroke (ASA: Class IIb, Level
of Evidence C). There are insufficient data to recommend a specific treatment approach that would
Sorensen G, Moskowitz MA, Cutrer FM. Perfusion weighted imaging during migraine: spontaneous
visual aura and headache. Cephalalgia. 1999;19:701-707.
5. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, Culebras A, DeGraba TJ,
Gorelick PB, Guyton JR, Hart RG, Howard G, Kelly-Hayes M, Nixon JVI, Sacco RL. Primary Prevention of
Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association
Stroke Council: Cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary
Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity,
and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working
Group: The American Academy of Neurology affirms the value of this guideline. Stroke. 2006;37:1583-
1633.
1.3.7. 고호모시스테인혈증Hyperhomocysteinemia

82
reduce the risk of first stroke in patients with elevated homocysteine levels. In the interim, use of folic acid
and B vitamins in patients with known elevated homocysteine levels may be useful given their safety and
low cost (ASA: Class IIb, Level of Evidence C).
CLINICAL RESEARCH CENTER FOR STROKE
규모의전향적관찰연구1,2및환자- 조군연구3들에서혈중호모시스테인이높으면용량의존적
으로허혈성뇌졸중및심뇌혈관질환의위험이증가하는것으로보고되었다. 또한메타분석에서도
유사한결과가보고되었는데4,5,혈중호모시스테인농도가5μmol/L 증가하면뇌졸중발생 응비(odd
ratio)가 1.59(95% CI, 1.2-1.96)로유의하게증가하는것으로보고되었다.4 한편, 환자- 조군연구들의
메타분석에서는유의한관련성을보이지만코호트연구들의메타분석에서는유의하지않았다는결
과도보고된바있다.6 허혈성뇌졸중의일차예방을1차유효성평가변수로호모시스테인강하치료
효과를평가한무작위임상연구는아직시행된바없다. 허혈성뇌졸중환자들을 상으로이차예방
을목적으로저용량과고용량의비타민투여를비교한연구에서는전체심뇌혈관질환의발생에는
유의한차이가없었으며,7급성심근경색환자들을 상으로비타민과위약투여를비교한연구에서
도전체심뇌혈관질환의발생및뇌졸중발생률에는유의한차이가없었다.8또한당뇨병혹은심뇌혈
관질환의과거력을가진환자들을 상으로한연구에서뇌졸중발생은유의하게감소하 지만
(RR=0.75; 95% CI, 0.59-0.97; p=0.03) 전체심뇌혈관질환의발생은차이가없었다.9특히이두연구모두
에서Vitamin B6를투여받은환자들에서심근경색(RR =1.17; 95% CI, 1.00-1.37; p=0.05)8및불안정성협
심증으로인한입원(RR=1.24; 95% CI, 1.04-1.49; p=0.02)9이증가하는경향을보 다. 하지만8개의무작
위배정임상연구들을메타분석한결과, 엽산투여는뇌졸중예방에유의한효과가있었는데
(RR=0.82; 95% CI, 0.68-1.00; p=0.045) 특히일차예방이있어효과가더욱뚜렷하 다. (RR=0.75; 95% CI,
0.62-0.90; p=0.002) 그외에36개월이상장기복용한경우, 엽산강화식이를시행하지않은경우, 호모
시스테인수치가치료전에비해20% 이상감소한경우등에서엽산투여는뚜렷한뇌졸중예방효과
를보 다.10

83
CLINICAL RESEARCH CENTER FOR STROKE
1. Bostom AG, Silbershatz H, Rosenberg IH, Selhub J, D'Agostino RB, Wolf PA, Jacques PF, Wilson PW.
Nonfasting plasma total homocysteine levels and all-cause and cardiovascular disease mortality in
elderly Framingham men and women. Arch Intern Med. 1999;159:1077-1080.
2. Giles WH, Croft JB, Greenlund KJ, Ford ES, Kittner SJ. Total homocyst(e)ine concentration and the
likelihood of nonfatal stroke: Results from the third National Health and Nutrition Examination Survey,
1988-1994. Stroke. 1998;29:2473-2477.
3. Tanne D, Haim M, Goldbourt U, Boyko V, Doolman R, Adler Y, Brunner D, Behar S, Sela BA. Prospective
study of serum homocysteine and risk of ischemic stroke among patients with preexisting coronary
heart disease. Stroke. 2003;34:632-636.
4. Wald DS, Law M, Morris JK. Homocysteine and cardiovascular disease: Evidence on causality from a
meta-analysis. BMJ. 2002;325:1202.
5. The Homocysteine Studies Collaboration Homocysteine and risk of ischemic heart disease and stroke: A
meta-analysis. JAMA. 2002;288:2015-2022.
6. Ford ES, Smith SJ, Stroup DF, Steinberg KK, Mueller PW, Thacker SB. Homocyst(e)ine and
cardiovascular disease: A systematic review of the evidence with special emphasis on case-control
studies and nested case-control studies. Int J Epidemiol.2002;31:59-70.
7. Toole JF, Malinow MR, Chambless LE, Spence JD, Pettigrew LC, Howard VJ, Sides EG, Wang CH,
Stampfer M. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke,
myocardial infarction, and death: The Vitamin Intervention for Stroke Prevention (VISP) randomized
controlled trial. JAMA.2004;291:565-575.
1. 일상적인식이로엽산섭취가부족한경우에는뇌졸중일차예방을위하여엽산을투여하여혈중호모
시스테인수치를저하시키는것을고려할수있다. (GPP)
2. 심뇌혈관질환의고위험군(예, 당뇨병, 관상동맥질환)에서호모시스테인강하를위한Vitamin B6 투여는
허혈성심장질환의위험을증가시킬가능성이있어주의를요한다. (근거수준IIa, 권고수준B)

84
8. Bonaa KH, Njolstad I, Ueland PM, Schirmer H, Tverdal A, Steigen T, Wang H, Nordrehaug JE, Arnesen E,
Rasmussen K. Homocysteine lowering and cardiovascular events after acute myocardial infarction. N
Engl J Med. 2006;354:1578-1588.
9. Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M, McQueen MJ, Probstfield J, Fodor G, Held C,
Genest J, Jr. Homocysteine lowering with folic acid and B vitamins in vascular disease. N Engl J Med.
2006;354:1567-1577.
10. Wang X, Qin X, Demirtas H, Li J, Mao G, Huo Y, Sun N, Liu L, Xu X. Efficacy of folic acid supplementation
in stroke prevention: A meta-analysis. Lancet. 2007;369:1876-1882.
CLINICAL RESEARCH CENTER FOR STROKE
1. There are insufficient data to support specific recommendations for primary stroke prevention in
patients with a hereditary or acquired thrombophilia (ASA).
부분의과다응고상태는정맥혈전증과관련성이있고뇌경색과의관련성은불분명하다. 그러나
항인지질항체(antiphospholipid antibody) 양성인경우뇌경색과같은동맥혈전증과관련성이있을수
뚜렷한뇌졸중위험요인이없는젊은뇌졸중환자에서는과다응고증에의한뇌졸중을고려해보아
야한다. 특히, 젊은여성의뇌경색환자에서항인지질항체(antiphospholipid antibodies)의빈도가높은
것으로보고되어있다.1그외에다른유전적인과다응고증과뇌졸중과의연관성이밝혀진것은없
다. 열린타원구멍(patent foramen ovale, PFO)이존재하는경우과다응고증과허혈성뇌졸중과의관련
성에 해서는추가적인연구가필요하다.
1.3.8. 과다응고증Hypercoagulability

85
CLINICAL RESEARCH CENTER FOR STROKE
1. 유전성또는후천성과다응고증의환자에서뇌졸중의일차예방을위해서충분한근거가있는권
고사항은없다. (근거수준III, 권고수준B)
2. 항인지질항체증후군이나암환자의경우과다응고증이동반되는경우가있으나, 뇌졸중의일차예
방을위해서항혈소판제제나항응고제의사용에 해서는충분한근거가없다. (근거수준 III, 권고
수준B)
있다. 항인지질항체의발견을위해서사용되는방법이항카디오리핀항체(anticardiolipin antibody)와
루푸스항응고인자(lupus anticoagulant) 검사방법이다. 생애첫허혈성뇌졸중환자는 조군에비해
항카디오리핀항체양성률이유의하게높아, 항인지질항체는뇌경색의유의한독립적위험인자일
가능성이있으나,2항인지질항체양성환자에서허혈성뇌졸중의재발이유의하게증가하지는않았
다.3또한항인지질항체양성을보인허혈성뇌졸중환자에서와파린(warfarin)과아스피린(aspirin)은
혈전증재발방지를위한효과에있어차이를보이지않았다.3 부분의연구에서과다응고증을일
으키는단백질C 또는S 결핍(protein C or S deficiency), 항트롬빈 III 결핍(antithrombin III deficiency), V 인
자라이덴돌연변이(factor V Leiden mutation), 프로트롬빈 20210 돌연변이(prothrombin 20210
mutations) 등과뇌졸중발생과의관련성은규명되지않았다. 프로트롬빈20210 돌연변이의빈도는
열린타원구멍이없는뇌졸중환자군에비해열린타원구멍이있는원인미상의뇌졸중(cryptogenic
stroke) 환자군에서유의하게높아, 과다응고증은열린타원구멍과동반될때혈전증의위험을증가
시킬가능성이있다.4
암환자의경우과다응고증이자주동반되며이와관련되어색전성뇌경색의위험이증가될수있다.5
암환자에서뇌졸중일차예방을위한권고안을도출할근거자료가매우부족하다. 향후암환자의생
존률증가와관련하여암과관련된뇌졸중이증가할가능성이있어이에 한연구가필요하다.
1. Brey RL, Stallworth CL, McGlasson DL, Wozniak MA, Wityk RJ, Stern BJ, Sloan MA, Sherwin R, Price TR,
Macko RF, Johnson CJ, Earley CJ, Buchholz DW, Hebel JR, Kittner SJ. Antiphospholipid antibodies and stroke
in young women. Stroke. 2002;33:2396-2400.

86
2. Anticardiolipin antibodies are an independent risk factor for first ischemic stroke. The Antiphospholipid
Antibodies in Stroke Study (APASS) Group. Neurology. 1993;43:2069-2073.
3. Levine SR, Brey RL, Tilley BC, Thompson JL, Sacco RL, Sciacca RR, Murphy A, Lu Y, Costigan TM, Rhine C,
Levin B, Triplett DA, Mohr JP. Antiphospholipid antibodies and subsequent thrombo-occlusive events in
patients with ischemic stroke. JAMA.2004;291:576-584.
4. Pezzini A, Del Zotto E, Magoni M, Costa A, Archetti S, Grassi M, Akkawi NM, Albertini A, Assanelli D, Vignolo LA,
Padovani A. Inherited thrombophilic disorders in young adults with ischemic stroke and patent foramen ovale.
Stroke. 2003;34:28-33.
5. Cestari DM, Weine DM, Panageas KS, Segal AZ, DeAngelis LM. Stroke in patients with cancer: incidence and
etiology. Neurology. 2004;62:2025-2030.
CLINICAL RESEARCH CENTER FOR STROKE
1. Currently, no evidence supports the use of high-sensitivity CRP (hs-CRP) screening of the entire adult
population as a marker of general vascular risk (ASA).
2. Aggressive risk factor modification is recommended for patients at high risk for stroke given exposure to
traditional risk factors regardless of hs-CRP level (ASA).
3. In agreement with AHA/CDC(Center for Disease Control and Prevention) guidelines, hs-CRP can be
useful in considering the intensity of risk factor modification in those at moderate general cardiovascular
risk on the basis of traditional risk factors (ASA: Class IIa, Level of Evidence B).
뇌혈관내피세포의손상을유발하는위험인자나질환들은혈관내혈전생성과뇌졸중위험도를증
가시킨다. 뇌졸중의주요원인인죽상경화(atherosclerosis)는혈관내피세포의손상에의해발생하는
만성염증성질환이다.1
1.3.9. 염증 Inflammation

87
CLINICAL RESEARCH CENTER FOR STROKE
많은코호트연구에서hs-CRP(high sensitivity C-reactive protein) 증가와심뇌혈관질환및뇌졸중발생
과의관련성이보고되었으며, 건강한성인에서hs-CRP 수치가증가함에따라뇌졸중발생위험도가
2-3배증가하는것으로보고되었다.2,3임상연구에서스타틴(statin)은관상동맥내죽상경화의진행과
심뇌혈관질환의발생을감소시켰는데, 이는hs-CRP 수치의감소와 접한관련성이있었다.4-6
hs-CRP가증가되어있지만고지혈증이없는환자군에서스타틴을투여한경우심뇌혈관질환의발
생은감소하 지만, 뇌졸중발생의감소는분명하지않았다.7죽상경화성심뇌혈관질환과염증반응
및관련된 리표지자(surrogate marker)와의관련성에 하여많은연구가진행되고있으나, 환자
치료에적용하기위해서는더많은연구가필요하다.
1. 모든성인에서심뇌혈관질환의위험도를평가하기위한선별검사로hs-CRP를측정할근거는부
족하다. (근거수준IV, 권고수준C)
2. 뇌졸중고위험군에서는hs-CRP 수치와관계없이적극적인위험인자의조절이필요하다. (근거수
준Ia, 권고수준A)
3. 심뇌혈관질환의중등도위험군에서위험인자의치료강도를결정하는데 hs-CRP 수치가고려될
수있다. (근거수준III, 권고수준B)
1. Ross R. Atherosclerosis -- An Inflammatory Disease. N Engl J Med. 1999;340:115-126.
2. Folsom AR, Aleksic N, Catellier D, Juneja HS, Wu KK. C-reactive protein and incident coronary heart disease
in the Atherosclerosis Risk in Communities (ARIC) study. Am Heart J.2002;144:233-238.
3. Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-Reactive Protein and Low-Density
Lipoprotein Cholesterol Levels in the Prediction of First Cardiovascular Events. N Engl J Med. 2002;347:1557-
1565.
4. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene
AM, the Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22

88
Investigators. Intensive versus Moderate Lipid Lowering with Statins after Acute Coronary Syndromes. N Engl
J Med.2004;350:1495-1504.
5. Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, Tsai J, Orazem J, Magorien RD, O'Shaughnessy
C, Ganz P, the Reversal of Atherosclerosis with Aggressive Lipid Lowering (REVERSAL) Investigators. Statin
Therapy, LDL Cholesterol, C-Reactive Protein, and Coronary Artery Disease. N Engl J Med. 2005;352:29-38.
6. Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, Crowe T, Howard G, Cooper CJ, Brodie
B, Grines CL, DeMaria AN. Effect of Intensive Compared With Moderate Lipid-Lowering Therapy on
Progression of Coronary Atherosclerosis: A Randomized Controlled Trial. JAMA. 2004;291:1071-1080.
7. Ridker PM, Rifai N, Clearfield M, Downs JR, Weis SE, Miles JS, Gotto AM, Jr., the Air Force/Texas Coronary
Atherosclerosis Prevention Study Investigators. Measurement of C-Reactive Protein for the Targeting of Statin
Therapy in the Primary Prevention of Acute Coronary Events. N Engl J Med. 2001;344:1959-1965.
CLINICAL RESEARCH CENTER FOR STROKE
1. Data are insufficient to recommend antibiotic therapy for stroke prevention on the basis of seropositivity
for 1 or a combination of putative pathogenic organisms. Future studies on stroke risk reduction based
on treatment of infectious diseases will require careful stratification and identification of patients at risk
for organism exposure (ASA).
1주이내의급성감염증이혈전생성을유발하여뇌졸중발생을유발할가능성이있다. 또한클라미디
아폐렴균(Chlamydia pneumoniae), 거 세포바이러스(Cytomegalovirus), 헬리코박터위염균
(Helicobacter pylori), 치주질환을일으키는그람음성균등이죽상경화증의발생과관련이있다는보
고가있다. 일생동안접촉하는다양한종류의병원균들이뇌졸중발생의각단계에복합적으로작용
할가능성이있다.
1.3.10. 감염증 Infection

89
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌졸중발생과관련된병원균의혈청반응이양성인경우라도, 뇌졸중의일차예방을위하여항생제
치료를시도할근거는부족하다. (근거수준IV, 권고수준C)
다양한병원균들이뇌졸중의발병에관여한다. United Kingdom General Practice Research Database
를분석한결과, 뇌졸중의연령보정발생률은3일이내에호흡기감염이있을경우3.19(95% CI, 2.8-
3.62), 3일이내에요로감염이있을경우에는2.72(95% CI, 2.32-3.20)로유의하게증가하 다.1
클라미디아폐렴균의혈청반응이양성일경우심뇌혈관질환이나뇌졸중의발병이증가한다고하
는증거는많이있지만2항생제치료가위험을낮춘다는증거는없다.3-6 심근경색이있었던클라미디
아폐렴균항체양성환자를 상으로실시한소규모연구에서아지스로마이신(azithromycin)이심뇌
혈질환의재발을낮춘다고하는보고가있었으나7이후의후속연구에서는아지스로마이신의효과
는입증되지않았다.3록시스로마이신(Roxithromycin),4가티플록사신(gatifloxacin),5클라리스로마이신
(clarithromycin)6등의항생제역시심뇌혈관질환이나뇌졸중을예방한다고하는증거는없다.
1. Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P. Risk of myocardial infarction and stroke
after acute infection or vaccination. N Engl J Med. 2004;351:2611-2618.
2. Cook PJ, Honeybourne D, Lip GY, Beevers DG, Wise R, Davies P. Chlamydia pneumoniae antibody titers are
significantly associated with acute stroke and transient cerebral ischemia: the West Birmingham Stroke
Project. Stroke. 1998;29:404-410.
3. Muhlestein JB, Anderson JL, Carlquist JF, Salunkhe K, Horne BD, Pearson RR, Bunch TJ, Allen A, Trehan S,
Nielson C. Randomized secondary prevention trial of azithromycin in patients with coronary artery disease:
primary clinical results of the ACADEMIC study. Circulation. 2000;102:1755-1760.
4. Gurfinkel E, Bozovich G, Beck E, Testa E, Livellara B, Mautner B. Treatment with the antibiotic roxithromycin
in patients with acute non-Q-wave coronary syndromes. The final report of the ROXIS Study. Eur Heart J.
1999;20:121-127.

90
5. Cannon CP, Braunwald E, McCabe CH, Grayston JT, Muhlestein B, Giugliano RP, Cairns R, Skene AM.
Antibiotic treatment of Chlamydia pneumoniae after acute coronary syndrome. N Engl J Med. 2005;352:1646-
1654.
6. Jespersen CM, Als-Nielsen B, Damgaard M, Hansen JF, Hansen S, Helo OH, Hildebrandt P, Hilden J, Jensen
GB, Kastrup J, Kolmos HJ, Kjoller E, Lind I, Nielsen H, Petersen L, Gluud C. Randomised placebo controlled
multicentre trial to assess short term clarithromycin for patients with stable coronary heart disease:
CLARICOR trial. BMJ. 2006;332:22-27.
7. Gupta S, Leatham EW, Carrington D, Mendall MA, Kaski JC, Camm AJ. Elevated Chlamydia pneumoniae
antibodies, cardiovascular events, and azithromycin in male survivors of myocardial infarction. Circulation.
1997;96:404-407.
CLINICAL RESEARCH CENTER FOR STROKE
정상인의뇌자기공명 상에서무증상열공성병변이나백색질변성이흔하게발견된다. 60~90세노
인의20% 정도에서무증상열공성병변이발견되는데, 무증상병변의숫자는뇌졸중증상을유발한
병변에비해약5배정도많으며, 위험인자는증상이있는열공성뇌졸중의위험인자와차이가없다.
백색질변성은 T2-강조뇌자기공명 상이나양자 도강조 상(proton density weighted image)에서
고신호강도로관찰되는데, 백색질의소실에따른국소적수분함량의증가에의한것으로알려져있
다. 고혈압, 죽상경화증, 흡연력등이백색질변성의위험인자로보고되어있다. 노인에서흔하게관
찰되는데85세노인인경우거의100%에서관찰된다.
1.3.11. 무증상열공성병변및백색질변성Asymptomatic lacune or white matter change
없음.

91
CLINICAL RESEARCH CENTER FOR STROKE
1. Vermeer SE, Hollander M, van Dijk EJ, Hofman A, Koudstaal PJ, Breteler MM. Silent brain infarcts and
white matter lesions increase stroke risk in the general population: The Rotterdam scan study. Stroke.
2003;34:1126-1129.
2. Kobayashi S, Okada K, Koide H, Bokura H, Yamaguchi S. Subcortical silent brain infarction as a risk
factor for clinical stroke. Stroke. 1997;28:1932-1939.
3. Bernick C, Kuller L, Dulberg C, Longstreth WT, Jr., Manolio T, Beauchamp N, Price T. Silent mri infarcts
and the risk of future stroke: The cardiovascular health study. Neurology. 2001;57:1222-1229.
4. Kuller LH, Longstreth WT, Jr., Arnold AM, Bernick C, Bryan RN, Beauchamp NJ, Jr. White matter
hyperintensity on cranial magnetic resonance imaging: A predictor of stroke. Stroke. 2004;35:1821-1825.
뇌졸중병력이없는정상인의뇌자기공명 상에서무증상열공성병변이있는경우뇌졸중발생위
험이약2-10배증가한다.1-3뇌졸중의병력이없는정상인의뇌자기공명 상에서백색질변성이있
을경우역시뇌졸중발생위험이증가한다.1,4 Cardiovascular Health Study에의하면뇌졸중발병률은
심한백색질변성이있는경우에는연간 2.8%이었고, 백색질변성이없거나경미한경우에는연간
0.6%이었다.
1. 뇌졸중병력이없지만뇌자기공명 상에서무증상열공성병변이나백색질변성이발견된경우
뇌졸중일차예방을위한치료방침은동반된뇌졸중위험인자들을고려하여결정해야한다. (근거
수준IV, 권고수준C)
92
CLINICAL RESEARCH CENTER FOR STROKE
1.4. 아스피린의뇌졸중일차예방효과Aspirin for primary stroke prevention
아스피린은가장 표적인항혈소판약물로많은임상연구들을통하여심뇌혈관질환의2차예방에
한효과가입증되었다. 일차예방의경우에도아스피린은전체심뇌혈관질환의발생을유의하게
감소시켰으나각질환별로는성별에따라차이가있어남성의경우에는허혈성심장질환의예방에,
여성의경우에는일부고위험군에서허혈뇌졸중의예방에효과가있는것으로보고되었다. 그런데
최근당뇨병또는말초동맥질환환자들을 상으로한다수의무작위배정임상연구및메타분석에
서아스피린이뇌졸중을포함한심뇌혈관질환예방에유의한효과가없는것으로보고되었다. 따라
서이들연구결과를바탕으로아스피린의허혈뇌졸중일차예방효과에관한진료지침의근거수준
과권고수준을개정하 다.
1. 중년이상의남성및여성에서특히심뇌혈관질환의위험인자가한가지이상있는경우전체심뇌
혈관질환예방을위하여저용량아스피린(75-325mg, 1일1회)의사용이추천된다. (근거수준Ia, 권
고수준A)
2. 남성의경우허혈뇌졸중일차예방을위해추천되지는않으나허혈성심장질환의일차예방효과를
위해서는추천될수있다. (근거수준Ia, 권고수준A)
3. 여성의경우허혈뇌졸중의일차예방을위해추천될수있으나허혈성심장질환의일차예방을위해
서는추천되지않는다. (근거수준Ia, 권고수준A) 특히고혈압, 이상지질혈증, 또는당뇨병중한가지
이상의위험인자를가지고있는65세이상의여자환자에서허혈뇌졸중의예방효과가뚜렷하다.
4. 장기간의정기적인아스피린복용은뇌출혈을포함한출혈부작용의위험을유의하게증가시키므로,
각환자마다예방효과의이득과출혈부작용의위험성을충분히검토한후사용하는것이바람직하다.
(근거수준Ia, 권고수준A) 특히우리나라의경우서양인에비해상 적으로뇌출혈의발생률이높
은반면관상동맥질환의발생률은낮은상황을고려하는것이필요하다. (GPP)
1. ASA/AHA (2010)
1) The use of aspirin for cardiovascular (including but not specific to stroke) prophylaxis is recommended
개정: 2011.10

93
CLINICAL RESEARCH CENTER FOR STROKE
새로추가된근거와기존의근거를종합한개정의필요성에 한근거는다음과같다.
1. 기존의근거
심혈관질환의과거력이없는, 주로남자환자들을 상으로아스피린과속임약의심혈관질환 1차
예방효과를연구한5개의이중눈가림무작위배정속임약비교연구들을메타분석한결과아스피린
(75 ~ 650 mg/day)은심근경색의발생을유의하게줄여주었으나(RR=0.74; 95% CI, 0.68-0.82) 뇌졸중예
방에는유의한효과를보이지않았으며(RR=1.08; 95% CI, 0.95-1.24.) 뇌출혈의위험이유의하게증가하
다(RR=1.35, p=0.03).1 45세이상의여자만을 상으로시행된하나의이중눈가림무작위배정연구
에서 (aspirin 100 mg qod) 전체심혈관질환의발생에는유의한차이가없었으나(RR=0.91; 95% CI,
0.80-1.03) 뇌졸중발생은유의하게감소하 는데(RR=0.83; 95% CI, 0.69-0.99), 세부적으로보았을때출
혈뇌졸중은약간증가하는경향을보 지만(RR=1.24; 95% CI, 0.82-1.87) 허혈뇌졸중은유의하게감소
하 다(RR=0.76; 95% CI, 0.63-0.93).2이연구를포함하여총6개의연구를남녀성별에따라메타분석
한결과에서는전체심뇌혈관질환의발생은남녀모두에서유의하게감소하 으나(남자, OR=0.86;
95% CI, 0.78-0.94)(여자, OR=0.88; 95% CI, 0.79-0.99), 뇌졸중은여자에서만(OR=0.83, 95% CI, 0.70-0.97), 심
근경색은남자에서만(OR=0.68, 95% CI, 0.54-0.86) 유의하게감소하 고출혈의위험은남녀모두에서
유의하게증가하 다(남자, OR=1.72; 95% CI, 1.35-2.20)(여자, OR=1.68; 95% CI, 1.13-2.52).3
for persons whose risk is sufficiently high for the benefits to outweigh the risks associated with
treatment (a 10-year risk of cardiovascular events of 6% to 10%) (Class I; Level of Evidence A).
2) Aspirin(81 mg daily or 100 mg every other day) can be useful for prevention of a first stroke among
women whose risk is sufficiently high for the benefits to outweigh the risks associated with treatment
(Class IIa; Level of Evidence B).
3) Aspirin is not useful for preventing a first stroke in persons at low risk (Class III; Level of Evidence A).
4) Aspirin is not useful for preventing a first stroke in persons with diabetes or diabetes plus asymptomatic
peripheral artery disease (defined as an ankle brachial pressure index <0.99) in the absence of other
established CVD (Class III; Level of Evidence B).
5) The use of aspirin for other specific situations (eg, atrial fibrillation, carotid artery stenosis) is discussed in
the relevant sections of this statement.
2. EUSI
- 2004년권고사항이후개정안없음

94
CLINICAL RESEARCH CENTER FOR STROKE
2. 새로운근거
40세이상의제1형및2형당뇨병환자이면서발목상완지수(ankle brachial index, ABI)가0.99이하인환
자들4, 제2형당뇨병을가지고있고동맥경화성질환의병력이없는환자들5, 심뇌혈관질환이없는일
반인들중ABI가낮은사람들을6 상으로한이중눈가림무작위배정임상연구들에서아스피린은심
뇌혈관질환또는동맥경화성질환의일차예방에유의한효과가없었다. 또한심뇌혈관질환이없는
당뇨병환자들에서아스피린사용군과 조군(속임약혹은아스피린을사용하지않은경우)을비교
한무작위배정임상연구들에 한두개의메타분석연구와7-8말초동맥질환만을가진환자들에서
아스피린과속임약혹은 조군을비교한무작위배정임상연구들에 한한개의메타분석연구에
서도9아스피린은심뇌혈관질환의일차예방에유의한효과가없었다. 한편6개무작위배정임상연
구에포함된개별환자들의자료(individual patient data)를이용한메타분석에서아스피린은주요심뇌
혈관질환예방에유의한효과가있었는데(0.51% vs 0.57% per year, p=0.0001) 이는주로비치명적심근
경색의감소에의한것이었으며(0.18% vs 0.23% per year, p �0.0001) 뇌졸중예방에 한효과는유의
하지않았다.(any stroke, 0.20% vs 0.21% per year, p=0.4: hemorrhagic stroke 0.04% vs 0.03%, p=0.05; non-
hemorrhagic stroke 0.16% vs 0.18% per year, p=0.08)10성별에따른개별심뇌혈관질환예방효과에
한분석에서는심근경색의경우남성에서만유의한효과가있었고뇌졸중의경우여성에서만유의
한효과를보이는경향을보 다.10
이상의새로운연구결과들을고려할때당뇨병환자의경우심뇌혈관질환일차예방에 한아스피
린의효과는없다고판단할수있으며말초동맥질환환자의경우에도증상성말초동맥질환환자들
에서는결론내리기는힘들지만무증상말초동맥질환에서는아스피린이효과가없는것으로판단된
다. 따라서"한가지이상의위험인자를가진" 환자들에 한아스피린사용추천의권고사항은"심뇌
혈관질환발생고위험군으로주요출혈부작용발생위험에비해아스피린예방효과의이득이높은
것으로판단되는경우"로수정이필요하다고판단된다. 또한당뇨병혹은무증상말초동맥질환을가
진환자들에서전체심뇌혈관질환일차예방에아스피린이유용하지않다는권고사항의추가가필요
하다고판단하 다. 한편남성과여성을구별하여심근경색및허혈성뇌졸중일차예방을위해기술
한내용은수정할만한새로운근거는없다고판단하 다. 다만여성의경우“특히고혈압, 이상지질
혈증, 또는당뇨병중한가지이상의위험인자를가지고있는65세이상의여자환자에서허혈성뇌졸
중의예방효과가뚜렷하다.”라는권고사항은단일임상시험의아집단분석결과를반 한내용임을
고려할때삭제하는것이바람직하다고판단하 다. 신개별환자자료를이용한메타분석에서도
출혈위험이유의하게증가함이다시확인된점을고려하여예방효과의이득과출혈부작용의위험
성을신중히검토할것을강조할필요가있으며이를위해“충분히검토한후사용하는것이바람직

95
CLINICAL RESEARCH CENTER FOR STROKE
하다”라는표현을“신중히검토하여야한다”로수정하 다. 마지막으로Good Practice Points (GPP)
로기술된사항에있어관상동맥질환에 한언급은뇌졸중 역을벗어나는내용임을고려하여삭
제하는것이바람직하다고판단하 다.
1. 심뇌혈관질환발생고위험군으로주요출혈부작용발생위험에비해아스피린예방효과의이득이
높은것으로판단되는경우전체심뇌혈관질환예방을위하여저용량아스피린(75-325mg, 1일1
회)의사용이추천된다. (근거수준Ia, 권고수준A) 10년심뇌혈관질환위험도가6-10% 이상인경우
심뇌혈관질환발생고위험군으로고려할수있다.
2. 당뇨병또는말초동맥질환만있는경우, 아스피린은전체심뇌혈관질환, 허혈성심장질환및뇌졸
중의일차예방에유용하지않다. (근거수준Ia, 권고수준A)
3. 남성의경우, 아스피린은허혈뇌졸중일차예방을위해추천되지는않으나허혈성심장질환의일차
예방효과를위해서는추천될수있다. (근거수준Ia, 권고수준A)
4. 여성의경우, 아스피린은허혈뇌졸중일차예방을위해추천될수있으나허혈성심장질환의일차
예방을위해서는추천되지않는다. (근거수준Ia, 권고수준A)
5. 장기간의정기적인아스피린복용은뇌출혈을포함한출혈부작용의위험을유의하게증가시키므
로, 각환자마다예방효과의이득과출혈부작용의위험성을신중히검토하여야한다. (근거수준Ia,
권고수준A) 특히우리나라의경우서양인에비해상 적으로뇌출혈의발생률이높은점을고려
하는것이필요하다. (GPP)
1. Hart RG, Halperin JL, McBride R, Benavente O, Man-Son-Hing M, Kronmal RA. Aspirin for the primary
prevention of stroke and other major vascular events: meta-analysis and hypotheses. Arch Neurol
2000;57:326-332.
2. Ridker PM, Cook NR, Lee IM, Gordon D, Gaziano JM, Manson JE, et al. A randomized trial of low-dose
aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med2005;352:1293-1304.
3. Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary
prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized
controlled trials. JAMA2006;295:306-313.

96
CLINICAL RESEARCH CENTER FOR STROKE
4. Belch J, MacCuish A, Campbell I, Cobbe S, Taylor R, Prescott R, et al. The prevention of progression of
arterial disease and diabetes (POPADAD) trial: factorial randomised placebo controlled trial of aspirin
and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ
2008;337:a1840.
5. Ogawa H, Nakayama M, Morimoto T, Uemura S, Kanauchi M, Doi N, et al. Low-dose aspirin for primary
prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA
2008;300:2134-2141.
6. Fowkes FG, Price JF, Stewart MC, Butcher I, Leng GC, Pell AC, et al. Aspirin for prevention of
cardiovascular events in a general population screened for a low ankle brachial index: a randomized
controlled trial. JAMA2010;303:841-848.
7. De Berardis G, Sacco M, Strippoli GF, Pellegrini F, Graziano G, Tognoni G, et al. Aspirin for primary
prevention of cardiovascular events in people with diabetes: meta-analysis of randomised controlled
trials. BMJ2009;339:b4531.
8. Zhang C, Sun A, Zhang P, Wu C, Zhang S, Fu M, et al. Aspirin for primary prevention of cardiovascular
events in patients with diabetes: a meta-analysis. Diabetes Res Clin Pract 2010;87:211-218.
9. Berger JS, Krantz MJ, Kittelson JM, Hiatt WR. Aspirin for the prevention of cardiovascular events in
patients with peripheral artery disease: a meta-analysis of randomized trials. JAMA 2009;301:1909-1919.
10.Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, et al. Aspirin in the primary and
secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from
randomised trials. Lancet 2009;373:1849-1860.

CLINICAL RESEARCH CENTER FOR STROKE
1.5. 뇌졸중인식도Public awareness and education
뇌졸중은증상발생후최 한빨리치료를시작해야하는응급질환이다. 그러나, 뇌졸중증상과응급
치료의필요성에 한일반인들의인식은아직낮은편이다.
뇌졸중환자가치료를받게되기까지의과정은세단계로나눌수있다. 첫째, 환자나보호자또는주
변사람들이뇌졸중증상과응급치료의필요성을인식하는단계, 둘째, 병원에환자를후송하는응급
후송체계의단계, 그리고마지막으로병원도착후치료가시작되는단계이다. 이중뇌졸중치료를
지연시키는가장중요한단계는뇌졸중증상과응급치료의필요성을인식하는첫번째단계이다. 따
라서, 뇌졸중위험요인이있는환자와보호자를포함한일반인들에 한교육을통하여뇌졸중증상
과응급치료의필요성에 한인식도를향상시키면, 더많은환자들이치료시간을놓치지않고, 적절
한치료를받을수있으며, 뇌졸중장애로인한사회, 경제적부담을줄일수있다.
1. Educational programs to increase awareness of stroke at the population level are recommended
(ESO: Class II, Level B)
2. Educational programs to increase stroke awareness among professionals (paramedics/emergency
physicians) are recommended (ESO: Class II, Level B)
뇌졸중증상이발생하 을때, 환자나보호자또는주변사람들이신경학적이상증상을뇌졸중에의
한것이라고정확하게판단할수록병원에빨리도착하게된다.1-3또한급성기뇌졸중의치료방법인
혈전용해술에 해알고있는경우, 3시간이내에병원에도착하는환자의비율이두배높아진다
[OR=2.00; 95% CI, 1.10-3.63].3현재까지, 뇌졸중에 한일반인들의지식을향상시키기위해많은연구
가진행되었으며, 교육을하면일반인의뇌졸중지식이향상된다는점이확인되었다.4-7 일반인을
상으로8개월간 중매체와포스터를이용하여교육을실시한결과, 허혈뇌졸중환자들에서정맥혈
97
신규: 2012.5
98
CLINICAL RESEARCH CENTER FOR STROKE
전용해술치료빈도가 2.2%에서 8.7%로증가하 다.4교육의효과는 중홍보교육기간이끝난 6개
월이후에도지속되어, 허혈뇌졸중환자의정맥혈전용해술치료율이교육을받은적이없었던환자
들에서는1.4% 지만, 교육을받았던환자들에서는11.2%로높아, 교육효과가상당기간지속됨을확
인하 다.5따라서, 교육을통하여일반인들이뇌졸중증상과응급치료의필요성을올바로인식하고
있으면, 정맥혈전용해술치료율을향상시킬수있으며, 교육의효과는장기간지속된다.
우리나라에서실시하 던일반인들의뇌졸중인식도에 한설문조사연구결과, 응답자중뇌졸중
의 표적증상과뇌졸중위험인자를한가지이상알고있는비율은약60% 정도로다른나라의연구
결과와크게다르지않았으며, 학력수준이낮거나나이가많을수록뇌졸중위험인자에 한지식이
부족하 다.8, 9 혈전용해술과응급후송체계로즉시연락할필요성을인식하는비율은각각 31%와
33%로낮은편이었으며, 특히20 와30 젊은연령층들은40 이후연령층에비해혈전용해술과
응급후송체계에 한인식도가더낮았다.9 뇌졸중에 한지식은 TV 매체 (59%)나 신문/잡지매체
(33%) 를통해주로얻었으나, 건강강좌나의사등의료전문인을통한지식획득은20% 미만으로낮았
다. 20 와30 의젊은연령층에서는인터넷매체(37%)를통한뇌졸중정보습득이TV 매체다음으로
중요하 다. 의사로부터뇌졸중에 한정보를얻는경우는드물었지만, 의사로부터직접들은정보
를가장신뢰할수있다고조사되었다.9, 10따라서의료진들이여러 중매체들을이용하여일반 중
들의뇌졸중교육에더욱적극적으로나설필요가있으며, 2-30 젊은연령층교육에는인터넷매체
를적극적으로이용할필요가있다.9
일반인뿐만아니라응급후송체계에서일하는응급구조사나응급실에서근무하는응급의료진에게
도뇌졸중에 한정확한지식은꼭필요하다. 응급구조사와응급의료진을 상으로시행되었던뇌
졸중교육은뇌졸중환자의병원도착지연을감소시키고, 병원도착후치료가시작되기까지의시간
을단축시켜혈전용해술을시행받는환자의수를증가시켰다.11,12
1. 뇌졸중환자의치료시작시간을단축하고정맥혈전용해술치료율을높이기위해교육프로그램을
통하여뇌졸중인식도를향상시키는것이필요하다. (근거수준IIb, 권고수준B)
2. 중매체를통해서의료진이일반인들에 해뇌졸중교육을실시하는것이추천된다.
(근거수준III, 권고수준B)
3. 응급구조사및응급의료진을 상으로뇌졸중인식도향상을위한교육이필요하다.
(근거수준IIb, 권고수준B)

99
CLINICAL RESEARCH CENTER FOR STROKE
1. Keskin O, Kalemoglu M, Ulusoy RE. A clinic investigation into prehospital and emergency department
delays in acute stroke care. Med Princ Pract. 2005;14:408-412
2. Chang KC, Tseng MC, Tan TY. Prehospital delay after acute stroke in Kaohsiung, Taiwan. Stroke.
2004;35:700-704
3. Kim YS, Park SS, Bae HJ, Cho AH, Cho YJ, Han MK, Heo JH, Kang K, Kim DE, Kim HY, Kim GM, Kwon
SU, Kwon HM, Lee BC, Lee KB, Lee SH, Lee YS, Nam HS, Oh MS, Park JM, Rha JH, Yu KH, Yoon BW.
Stroke awareness decreases prehospital delay after acute ischemic stroke in Korea. BMC Neurol.
2011;11:2
4. Morgenstern LB, Staub L, Chan W, Wein TH, Bartholomew LK, King M, Felberg RA, Burgin WS, Groff J,
Hickenbottom SL, Saldin K, Demchuk AM, Kalra A, Dhingra A, Grotta JC. Improving delivery of acute
stroke therapy: The TLL temple foundation stroke project. Stroke. 2002;33:160-166
5. Morgenstern LB, Bartholomew LK, Grotta JC, Staub L, King M, Chan W. Sustained benefit of a
community and professional intervention to increase acute stroke therapy. Arch Intern Med.
2003;163:2198-2202
6. Hodgson C, Lindsay P, Rubini F. Can mass media influence emergency department visits for
stroke? Stroke. 2007;38:2115-2122
7. Alberts MJ, Perry A, Dawson DV, Bertels C. Effects of public and professional education on reducing
the delay in presentation and referral of stroke patients. Stroke. 1992;23:352-356
8. Bae HJ, Yoo KM, Yoon BW, Kim J, Kim JY, Kim EG, Kim BC, Roh JK. Stroke awareness in Korea: The
results of survey in the second stroke prevention campaign. J Korean Neurol Assc. 2002;20:110-117
9. Kim YS, Park SS, Bae HJ, Heo JH, Kwon SU, Lee BC, Lee SH, Oh CW, Yoon BW. Public awareness of
stroke in Korea: A population-based national survey. Stroke. 2011 [Epub ahead print]
10. Kim JS, Yoon SS. Perspectives of stroke in persons living in seoul, south Koea. A survey of 1000
subjects. Stroke. 1997;28:1165-1169
11. Kwan J, Hand P, Sandercock P. Improving the efficiency of delivery of thrombolysis for acute
stroke: A systematic review. QJM. 2004;97:273-279
12. Behrens S, Daffertshofer M, Interthal C, Ellinger K, van Ackern K, Hennerici M. Improvement in stroke
quality management by an educational programme. Cerebrovasc Dis. 2002;13:262-266

100
CLINICAL RESEARCH CENTER FOR STROKE
1.6. 비파열뇌동맥류Unruptured intracranial aneurysm
미국 3
Screening of certain high-risk populations for unruptured aneurysms is of uncertain value (Class IIb, Level
of Evidence B); advances in noninvasive imaging may be used for screening, but catheter angiography
remains the gold standard when it is clinically imperative to know if an aneurysm exists.
일본 4
비파열뇌동맥류의선별검사에는magnetic resonance angiography (MRA) (0.5T 이상)이이용되며, 수술
적응의검토를위해서는digital subtraction angiography (DSA, 카테터법에의한), 3차원혈관촬 (카테
터법에의한), 3차원-computed tomography 혈관조 술 (CTA) 등을사용하는것이바람직하다 (Grade
A: 실행이강력히권유됨).
뇌동맥류파열에의한지주막하출혈은최근치료방법의개선에도불구하고예후가극히불량하다.1
이로인한사망률과이환율을낮추기위해파열예방이중요할수있으며, 고위험군에 한선별검사
가고려되고있다.2
뇌동맥류의표준적인진단방법은DSA이나, 최근MRA나CTA의민감도와특이도가DSA와큰차이
를보이지않아선별검사에유용하다.5,6
현재까지는지주막하출혈의가족력이없는성인을 상으로비파열뇌동맥류에 한선별검사를
실시하는것은효용성이낮아고려되지않는다.3부모, 형제또는자식중에뇌동맥류환자가2명이
상인가족력이있는경우, 비파열뇌동맥류가발견될위험성이일반인에비해4.2배정도높으며유
1.6.1 비파열뇌동맥류의선별검사 Screening of unruptured intracranial aneurysm
신규: 2013.1

101
CLINICAL RESEARCH CENTER FOR STROKE
병률이8%로보고되고있다.7 또한가족력이있는경우, 다발성뇌동맥류를가질확률이높고젊은
나이에출혈이발생하는것으로보고되고있다.7따라서가족력이있는경우뇌동맥류발견을위한
선별검사가필요하다. 8-10그러나, 현재까지는개별적(individual base) 선별검사가추천되고있다.
뇌동맥류와관련이있는질환으로, 모야모야병, 뇌하수체선종, 겸상적혈구질환(sickle cell
disease), 섬유근 이형성증(fibromuscular dysplasia), 전신성 홍반성 낭창(systemic lupus
erythematosus), 동맥축착(coarctation of aorta), 뇌동정맥기형이있고, 유전성질환으로는상염색
체우성다낭신질환(autosomal dominant polycystic kidney disease), Marfan 증후군, 제1형신경섬유
종증, 제1형다발성내분비종양(multiple endocrine neoplalsia type I), 탄력섬유성가황색종
(pseudoxanthoma elasticum), 유전성출혈성모세혈관확장(hereditary hemorrhagic telangiectasia) 및
제4형Ehlers-Danlos 증후군이있다. 이질환중, 상염색체우성다낭신질환의경우, 뇌동맥류의유
병률이10%에달하므로선별검사가필요하다고판단된다.
뇌동맥류파열로치료를받은환자에서도매년 1~2% 의새로운동맥류가발생하는것으로보고된
바있으며,11특히다발성뇌동맥류의경우그빈도가더높은것으로보고되고있다.12
1. 가족내에부모, 형제자매및자녀들중2명이상의뇌동맥류환자가족력이있는경우개인별로뇌동맥
류발견을위한선별검사가고려된다. (근거수준III, 권고수준B)
2. 상염색체우성다낭신질환환자의경우선별검사를고려할수있다. (근거수준 III, 권고수준B)
3. 뇌동맥류파열로치료받은환자의경우새로운동맥류에 한정기적인검사가고려되어야한다.
(근거수준 III, 권고수준B)
1. Graves EJ. Detailed diagnoses and procedures. National hospital discharge survey, 1990. Vital Health Stat.
1992;113:1-225.
2. Broderick JP, Brott TG, Duldner JE, Tomsick T, Leach A. Initial and recurrent bleeding are the major causes
of death following subarachnoid hemorrhage. Stroke. 1994;25:1342-1347.
102
CLINICAL RESEARCH CENTER FOR STROKE
3. Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN et al. Guidelines for the
management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a
special writing group of the Stroke Council, American Heart Association. Stroke. 2009;40:994-1025.
4. The Joint committee on guidelines for the management of stroke. Japanese guideline for the management
of Stroke 2009. Tokyo, Kyowa Kikaku, Ltd., 2009. http://www.jsts.gr.jp/jss08.html[Japanese]
5. Raaymakers TW. Aneurysms in relatives of patients with subarachnoid hemorrhage: frequency and risk
factors: MARS study group: magnetic resonance angiography in relatives of patients with subarachnoid
hemorrhage. Neurology. 1999; 53:982-988.
6. Kuehn BM. FDA warning: CT scans exceeded proper doses. JAMA. 2010;303:124.
7. Raaymakers TW, Rinkel GJ, Ramos LM. Initial and follow-up screening for aneurysms in families with familial
subarachnoid hemorrhage. Neurology. 1998;51:1125-1130.
8. Bor AS, Koffijberg H, Wermer MJ, Rinkel GJ. Optimal screening strategy for familial intracranial aneurysm:
a cost-effectiveness analysis. Neurology. 2010;74:1671-1679.
9. Brown RD Jr, Huston J III, Hornung R, Foroud T, Kallmes DF, Kleindorfer D et al. Screening for brain
aneurysm in the familial intracranial aneurysm study: frequency and predictors of lesion detection.
J Neurosurg. 2008;108:1132-1138.
10. Takao H, Nojo T, Ohtomo K. Screening for familial intracranial aneurysms: decision and cost-effectiveness
analysis. Acad Radiol. 2008;15:462-471.
11. David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of
surgically treated aneurysms. J Neurosurg. 1999;91:396-401.
12. Wermer MJ, Koffijberg H, van der Schaaf IC, for the ASTRA Study Group. Effectiveness and costs of
screening for aneurysms every 5 years after subarachnoid hemorrhage. Neurology. 2008;70:2053-2062.

103
CLINICAL RESEARCH CENTER FOR STROKE
비파열뇌동맥류의치료는뇌동맥류의자연사를근거로결정되어야하나, 아직이에 한정확한자
료가부족한상황이다. 현시점에서비파열뇌동맥류의치료여부는환자의나이, 동반질환, 건강상
태등환자요인과뇌동맥류의크기, 위치, 모양등병변요인을종합적으로고려하여신중하게결정되
어야한다. 치료방법으로는결찰술이표준적방법으로이용되어왔으나, 최근사용기구의발달과더
불어혈관내치료가점진적으로많이시행되고있다. 치료방법은환자요인, 병변요인, 병원의시설및
치료성적등을고려하여결정하여야한다.
1.6.2 비파열뇌동맥류의치료 Treatment of unruptured intracranial aneurysm
미국 1
1. With rare exceptions, all symptomatic unruptured aneurysms should be treated. Extensive medical co-
morbidity, advanced age, and anatomic configuration of the aneurysm may contraindicate intervention
when treatment risks approach 25%.
2. Small, incidental aneurysms less than 5 mm in diameter should be managed conservatively in virtually
all cases. An important exception to this rule involves those young patients with severe psychological
disturbances secondary to harboring an unruptured aneurysm. In such patients, particularly those
psychologically crippled by their condition, definitive treatment can be justified and is often pursued.
3. Patients younger than 60 years of age with aneurysms larger than 5 mm should be offered treatment
unless there is a significant contraindication.
4. When managing older patients (older than 60 yr of age), the decision to treat becomes less clear. In these
situations, lesion location plays a critical role, because anterior communicating artery, posterior
communicating artery, and basilar apex aneurysms carry a higher rupture risk than aneurysms in other
locations.
5. Large, incidental aneurysms greater than 10 mm should be treated in all healthy patients younger than
70 years of age. The indications are less compelling in older individuals.
6. Microsurgical clipping rather than endovascular coiling should be the first choice in low-risk cases
(young patients with small, anterior circulation aneurysms).
신규: 2013.1

104
CLINICAL RESEARCH CENTER FOR STROKE
7. Very large and giant aneurysms and aneurysms with high neck-to-dome ratios will generally benefit
more from surgical approaches than from endovascular treatment. In the most complex aneurysms,
combined approaches such as arterial bypass techniques followed by proximal endovascular occlusion
have proved invaluable.
8. Endovascular coiling represents a reasonable alternative that should be instituted whenever open
surgical intervention carries high risk such as with elderly or medically ill patients and in anatomically
unfavorable situations (e.g., posterior projecting basilar apex aneurysm).
국(for coiling) 2
1. Current evidence on the safety and efficacy of coil embolization of unruptured intracranial aneurysms
appears adequate to support use of the procedure, provided that normal arrangements are in place for
consent, audit and clinical governance.
2. The procedure should only be performed in specialist units with expertise in the endovascular treatment
of intracranial aneurysms. Clear arrangements should be in place for the involvement of different clinical
disciplines in treatment and follow-up.
일본 3
1. 비파열뇌동맥류가발견된경우, 연령, 건강상태등의환자인자, 크기및부위, 형상등의병변인자,
비파열뇌동맥류의자연력및병원시설이나시술자의치료성적등을감안하여치료를검토하는것
이추천된다. 또한치료여부의결정이나방법의선택은충분히고지된동의(informed consent)를거쳐
결정하는것이추천된다(Grade B: 실행이권유됨).
2. 비파열뇌동맥류의자연력을고려하여, 환자의여명이10~15년이상인경우아래와같은병변에
한치료를검토하는것이추천된다(Grade C 1: 실행이고려되어도좋으나충분한과학적근거는
부족함).
①크기5 mm이상의비파열뇌동맥류
②5 mm미만이라도
A) 증상이있는뇌동맥류
B) 후방순환, 전교통동맥및내경동맥-후교통동맥부등의부위에존재하는뇌동맥류
C) 종횡비(dome-neck aspect)가크고, 부정형, 수포(bleb)를가지는등의형태적특징을가진뇌동맥류
단, 비파열뇌동맥류진단후의심각한우울증상이나불안증등이보고되고있으며, 파열률이나치료

105
CLINICAL RESEARCH CENTER FOR STROKE
합병증의위험에기반한유익/유해(benefit-risk)분석내지비용/효과분석만으로치료의적부를검토
하는것은타당하지않으며, 각증례별로검토하여충분히고지된동의하에치료방침을결정하는것
이추천된다.
3. 개두수술이나혈관내치료등의외과적치료를행하지않고경과관찰하는경우는흡연, 량음주
를피하고고혈압을치료한다(Grade A:실행이강력히권유됨). 경과관찰하는경우는반년에서약1
년마다 상에의한경과관찰을행하는것이추천된다(Grade C1).
4. 혈관내치료후에도불완전폐색이나재발등에관한경과관찰이추천된다(Grade B).
5. 개두결찰술후에도장기간추적관찰이추천된다(Grade C1).
비파열뇌동맥류의연간파열률은각연구마다큰차이가있으며,4-9그결과를절 적수치로사용
하기보다는각동맥류증례마다유연하게적용하는것이바람직하다. 동맥류파열에 향을미치
는다양한인자가보고되었다. 특히, 동맥류의크기와연간파열률의관계는여러연구에서공통적
으로양적상관관계를보 다.4-9 이러한소견은2003년발표된 ISUIA(International Study of
Unruptured Intracranial Aneurysms) 결과에서도관찰되었으며, 연간파열률은, 7mm미만의동맥류
중이전출혈이없었던경우0.15%, 이전출혈이있었던경우0.4%이고, 7~12 mm의동맥류인경우
1.2%, 13~24 mm의동맥류인경우3.1%, 25 mm이상인동맥류의경우8.6% 다.7 따라서, 동맥류의
크기는파열위험도를결정하는중요인자로, 치료여부를결정하는데우선적으로고려될수있다.
한편, 동맥류의위치에따라서도파열위험도가다른것으로알려져있으며전교통동맥, 후교통동
맥, 후방순환계동맥류의파열위험성이다른부위에비해높은것으로보고된바있다.7-9다른위험
인자로는, 다른뇌동맥류파열에의한뇌지주막하출혈의과거력,7,12 증상이있는뇌동맥류,5,10 뇌동
맥류가족력11,13다엽성혹은수포성모양,5,10등이알려져있다. 따라서, 동맥류의크기를비롯한이런
파열위험인자들이비파열동맥류의치료여부를결정하는중요인자로고려될수있다.
한편, 2010년발표된SUAVe (Small Unruptured Aneurysm Verification)8연구는5mm미만인비파열뇌
동맥류만을 상으로한전향적연구 으며, 연간파열률이0.54% (단발성: 0.34%, 다발성0.95%)로
보고되었다. 또한50세미만인경우약5배 (95% CI 1.03-26.52), 동맥류크기가4mm 이상인경우약
6배 (95%CI 1.27-26.96), 고혈압이있는경우약8배 (95% CI 1.33-47.42), 다발성동맥류를가진경우
106
CLINICAL RESEARCH CENTER FOR STROKE
약5배 (95% CI 1.62-14.65) 파열위험이증가한다고보고하 다. 이연구의결과는, 일본인의경우작
은뇌동맥류의파열률이기존의 ISUIA 보고에비하여높음을보여주고있다. 또한2012년발표된일
본의UCAS (Unruptured Cerebral Aneurysm Study of Japan)9연구에서도 ISUIA결과에비하여전순환
계작은뇌동맥류의파열률이높게보고되었고, 전체적인연간파열률은 0.95% 다. 특히본연구
에서는동맥류의위치및크기별연간파열위험성을제시하고있어, 임상적판단에큰도움이될것
으로예상된다. 아직비파열뇌동맥류자연사에관한신뢰할만한국내자료가없는상황에서, 유전
학적으로유사한일본의SUAVe 및UCAS 연구결과는국내치료지침작성시중요한근거자료로사
용될수있을것으로생각된다.
비파열뇌동맥류결찰술의합병증관련, 2003년발표된 ISUIA 결과에따르면결찰술후 1년이환및
사망률은지주막하출혈과거력이없는경우10.1%, 과거력이있는경우12.6% 다.7 국내자료로는
2010년에발표된후향적연구보고가있으며, 결찰술후30일이환율과사망률은각각8.4%와0.4%
인것으로보고되었다.14 그러나, 결찰술의합병증발생률은동맥류의크기및위치, 환자의나이, 과
거출혈여부등에따라다르며,7, 14-17전방순환계동맥류중그크기가10mm 이하로작은경우결찰
술의합병증발생률은2% 미만으로보고된바있다.14-17 체적으로, 비파열뇌동맥류의파열률과결
찰술의합병증발생률을고려하 을때, 예상여명이10년이상인환자의무증상비파열뇌동맥류는
결찰술 상으로고려될수있으며, 이러한의견은2006년Krisht 등18의연구결과에부합된다.
혈관내치료의합병증관련, ISUIA 2003년보고에따른이환및사망률은출혈병력이있는환자의경
우7.1%, 출혈이없던환자의경우9.8% 이었다.7국내의경우, 후향적으로시행된전국조사에서혈
관내치료의이환율과사망률은각각6.3%, 0.2%로보고되었다.14따라서, 결찰술과혈관내치료의합
병증발생률차이는크지않은것으로판단된다. 한편, 2007년발표된미국429개병원 상의전국
조사에서는, 결찰술이혈관내치료에비해합병증과사망률을각각 70%와 30% 증가시키는것으로
나타났지만,19좀더큰전향적연구에의한검토가필요하다. 혈관내치료의합병증역시동맥류의
크기, 위치, 모양, 환자의나이, 출혈여부등에의해 향을받으며,20-22치료방법의선택은각환자의
상태와병원의상황을고려하여선택되어야한다.
치료하지않은비파열뇌동맥류는추후크기증가가관찰될수있으며,23-25 경과관찰을하기로결
정하 을경우반드시 상추적검사가권고된다. 동맥류성장의위험인자로는동맥류의크기, 위
치, 다발성, 고혈압, 흡연및여성등이보고되었다.24,25 상추적검사는처음3년간매년MRA나CTA
를시행하고, 이후안정적인경우2~5년마다정기적인추적관찰이추천되고있으며, 이에 해서는

107
CLINICAL RESEARCH CENTER FOR STROKE
향후추가적연구가필요하다.26
결찰술과혈관내치료후동맥류재발및출혈빈도는다소차이가있으나, 두치료법에서모두발생
할수있다.27-29이와관련, 2005년 ISAT(International Subarachnoid Aneurysm Trial) 연구에서는, 치료
1년이상경과후재출혈률을수술군은 0.06%/year, 혈관내치료군은 0.2%/year로보고하 다.27이
후발표된 ISAT의장기추적결과에서는결찰술과혈관내치료후재출혈률이각각 0.032%/person
year, 0.24%/person year로혈관내치료의재출혈이8배높은것으로보고되었으며,28재발로인한재
치료또한6.9배높은것으로보고되었다.29수술후재발률에관해서는1999년Tsutsumi 등30은비파
열뇌동맥류수술후평균 8.8년간경과를관찰하여완전결찰된뇌동맥류의연간재성장률을 0.1%
로보고하 고, 새로운동맥류 (de novo aneurysm)의생성률은연간 0.2%로보고하 다. 2004년
Akyuz 등31은뇌동맥류의결찰술치료결과에 해치유율99.4%, 수술직후혈관조 술에서완전폐
색이확인된환자의99.4%에서평균47개월후에도안정적으로폐색이유지됨을보고하 다. 혈관
내치료후출혈률관련, Lanterna 등32의 1379명의메타분석결과에서는치료후연간출혈의위험
성이약 0.9%으로보고하 다. Naggara 등33의 5044명의메타분석의결과에서도연간출혈위험은
약0.2% 고, Murayama 등34은처음치료후5년이상관찰시4.1%라고보고하 다. 따라서, 혈관내
치료를이용하여치료된동맥류는반드시추적검사를시행하여야하며, 결찰술로치료된동맥류
도비교적적은빈도이지만재발할수있으므로추적검사가필요하다.
1. 치료를하지않고경과관찰을결정한경우, 고혈압치료와금연을권고하며, 증상이없더라도주기
적 상추적검사를권고한다. (근거수준: III, 권고수준: B)
2. 증상이있는비파열뇌동맥류는치료가원칙이다. 단, 동반된내과적병력이나고령, 동맥류의모양,
위치등에의해치료의위험성이매우높은경우이를고려하여치료여부를결정한다. (근거수준:
IIa, 권고수준: B)
3. 증상이없는경막외뇌동맥류는일반적으로치료가추천되지않는다. (근거수준III, 권고수준B)
4. 증상이없는비파열뇌동맥류는치료의위험도를고려해볼때환자의여명이약10년이상이면
다음과같은경우에치료의검토가추천된다.
1) 파열의위험도가상 적으로높은경우
①크기가5 mm이상(근거수준III, 권고수준B)

108
CLINICAL RESEARCH CENTER FOR STROKE
②후방순환, 전교통동맥및후교통동맥뇌동맥류(근거수준IIb, 권고수준B)
③지주막하출혈병력이있는환자(근거수준IIb, 권고수준B)
④뇌동맥류의가족력이있는환자(근거수준III, 권고수준B)
⑤경과관찰도중크기의증가나모양의변화가있는뇌동맥류(근거수준: IV, 권고수준: C)
⑥50세미만의고혈압환자에서다발성병변이있을때(근거수준III, 권고수준B)
⑦종횡비(aspect ratio, 동맥류경부의크기에 한동맥류높이의상 적인크기비율) 또는크기
비(size ratio, 모동맥크기에 한동맥류의상 적인크기비율)가크거나다엽성(multilobular)
또는수포성(bleb) 변화를보이는뇌동맥류(근거수준III, 권고수준B)
2) 환자가비파열뇌동맥류진단으로인한불안, 우울증이심할경우(근거수준IV, 권고수준C)
5. 비파열뇌동맥류가발견된경우, 환자의나이, 동반질환, 건강상태등‘환자인자’및뇌동맥류의
크기, 위치및모양등의‘병변인자’를고려하여치료여부를결정을하는것이권고된다. 또한
치료방법은병원의시설및치료성적도고려하여결정한다. 이러한결정과정에서, 환자또는환자
가족에게충분한설명을한후고지된동의를받는것이필수적이다. (근거수준IV, 권고수준C)
6. 비파열뇌동맥류의치료시혈관내치료는결찰술과비교하여결과가나쁘지않으며, 치료위험도와
재발률등을고려하여치료방법을결정한다. (근거수준Ib, 권고수준A)
7. 비파열뇌동맥류의치료후장기간경과관찰이권고된다. 특히혈관내치료후에는불완전폐색이
나재개통등을확인하기위해경과관찰을하는것이권고된다. (근거수준IIb, 권고수준B)
Komotar RJ, Mocco J, Solomon RA. Guidelines for the surgical treatment of unruptured intracranial
aneurysms: the first annual J. Lawrence pool memorial research symposium--controversies in the
management of cerebral aneurysms. Neurosurgery. 2008;62:183-94.
Coil embolisation of unruptured intracranial aneurysms. Interventional procedure guidance 105.
National Institute for Clinical Excellence, January 2005. www.nice.org.uk/IPG105distributionlist
The Joint committee on guidelines for the management of stroke. Japanese guideline for the
management of Stroke 2009. Tokyo, Kyowa Kikaku, Ltd., 2009. http://www.jsts.gr.jp/jss08.html[Japanese]
The International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial
aneurysms-risk of rupture and risks of surgical intervention. N Engl J Med.1998; 339:1725-1733.
Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a
systematic review. Stroke. 1998;29:251-256.
Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: probability of and
risk factors for aneurysm rupture. J Neurosurg.2000;93:379-387.
1.
2.
3.
4.
5.
6.

109
CLINICAL RESEARCH CENTER FOR STROKE
Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG et al, for ISUIA
Investigators. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical
and endovascular treatment. Lancet. 2003;362:103-110.
Sonobe M, Yamazaki T, Yonekura M, Kikuchi H. Small unruptured intracranial aneurysm verification
study: SUAVe study, Japan. Stroke. 2010;41:1969-1977.
The UCAS Japan Investigators. The Natural Course of Unruptured Cerebral Aneurysms in a Japanese
Cohort. N Engl J Med. 2012;366:2474-2482.
Morita A, Fujiwara S, Hashi K, Ohtsu H, Kirino T. Risk of rupture associated with intact cerebral
aneurysms in the Japanese population: a systematic review of the literature from Japan. J Neurosurg.
2005;102:601-606.
Nakagawa T, Hashi K, Kurokawa Y, Yamamura A. Family history of subarachnoid hemorrhage and the
incidence of asymptomatic, unruptured cerebral aneurysms. J Neurosurg. 1999;91:391-395.
Broderick JP, Brott TG, Duldner JE, Tomsick T, Leach A. Initial and recurrent bleeding are the major
causes of death following subarachnoid hemorrhage. Stroke. 1994;25:1342-1347.
Broderick JP, Brown RD Jr, Sauerbeck L, Hornung R, Huston J 3rd, Woo D et al, for FIA Study
Investigators. Greater rupture risk for familial as compared to sporadic unruptured intracranial
aneurysms. Stroke. 2009;40:1952-1957.
Kim JE, Lim DJ, Hong CK, Joo SP, Yoon SM, Kim BT. Treatment of unruptured intracranial aneurysms
in South Korea in 2006: a nationwide multicenter survey from the Korean Society of Cerebrovascular
Surgery. JKorean NeurosurgSoc. 2010;47:112-118.
Ogilvy CS, Carter BS. Stratification of outcome for surgically treated unruptured intracranial aneurysms.
Neurosurgery. 2003;52:82-87.
Moroi J, Hadeishi H, Suzuki A, Yasui N. Morbidity and mortality from surgical treatment of unruptured
cerebral aneurysms at Research Institute for Brain and Blood Vessels-Akita. Neurosurgery.
2005;56:224-231.
Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured
intracranial aneurysms: a meta-analysis. Stroke. 1998;29:1531-1538.
Krisht AF, Gomez J, Partington S. Outcome of surgical clipping of unruptured aneurysms as it
compares with a 10-year non-clipping survival period. Neurosurgery. 2006;58:207-216.
Higashida RT, Lahue BJ, Torbey MT, Hopkins LN, Leip E, Hanely DF. Treatment of unruptured
intracranial aneurysms: a nationwide assessment of effectiveness. AJNR Am J Neuroradiol.
2007;28:146-151
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.

110
CLINICAL RESEARCH CENTER FOR STROKE
Murayama Y, Nien YL, Duckwiler G, Gobin YP, Jahan R, Frazee J et al. Guglielmi detachable coil
embolization of cerebral aneurysms: 11 years’experience. J Neurosurg. 2003;98:959-966.
Henkes H, Fischer S, Weber W, Miloslavski E, Felber S, Brew S et al. Endovascular coil occlusion of
1811 intracranial aneurysms: early angiographic and clinical results. Neurosurgery. 2004;54:268-285.
Pierot L, Spelle L, Vitry F, for the ATENA Investigators. Immediate clinical outcome of patients
harboring unruptured intracranial aneurysms treated by endovascular approach: results of the
ATENA study. Stroke. 2008;39:2497-2504.
Burns JD, Huston J III, Layton KF, Piepgras DG, Brown RD Jr. Intracranial aneurysm enlargement on
serial magnetic resonance angiography: frequency and risk factors. Stroke. 2009;40:406-411.
Matsubara S, Hadeishi H, Suzuki A, Yasui N, Nishimura H. Incidence and risk factors for the growth of
unruptured cerebral aneurysms: observation using serial computerized tomography angiography.
J Neurosurg. 2004;101:908-914.
Juvela S, Poussa K, Porras M. Factors affecting formation and growth of intracranial aneurysms: a
long-term follow-up study. Stroke. 2001;32:485-491.
Wiebers DO. Unruptured intracranial aneurysms: natural history and clinical management. Update on the
international study of unruptured intracranial aneurysms. Neuroimaging Clin N Am. 2006;16:383-390.
Molyneux AJ, Kerr RS, Yu LM, Clarke M, Snead M, Yarnold JA, Sandercock P; International
Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International subarachnoid aneurysm trial
(ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial
aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding,
subgroups, and aneurysm occlusion. Lancet. 2005;366:809-817.
Mitchell P, Kerr R, Mendelow AD, Molyneux A. Could late rebleeding overturn the superiority of cranial
aneurysm coil embolization over clip ligation seen in the International Subarachnoid Aneurysm Trial
(ISAT)? J Neurosurg. 2008;108:437-442.
Campi A, Ramzi N, Molyneux AJ, Summers PE, Kerr RS, Sneade M, Yarnold JA, Rischmiller J, Byrne
JV. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the
International Subarachnoid Aneurysm Trial (ISAT). Stroke. 2007;38:1538-1544.
Tsutsumi K, Ueki K, Usui M, Kwak S, Kirino T. Risk of subarachnoid hemorrhage after surgical
treatment of unruptured cerebral aneurysms. Stroke. 1999;30:1181-1184.
Akyuz M, Tuncer R, Yilmaz S, Sindel T. Angiographic follow-up after surgical treatment of intracranial
aneurysms. Acta Neurochir (Wien). 2004;146:245-250.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
111
CLINICAL RESEARCH CENTER FOR STROKE
Lanterna LA, Tredici G, Dimitrov BD, Biroli F. Treatment of unruptured cerebral aneurysms by
embolization with Guglielmi detachable coils: case-fatality, morbidity, and effectiveness in preventing
bleeding-A systematic review of the literature. Neurosurgery. 2004;55:767-778.
Naggara ON, White PM, Guilbert F, Roy D, Weill A, Raymond J. Endovascular treatment of intracranial
unruptured aneurysms: systematic review and meta-analysis of the literature on safety and efficacy.
Radiology. 2010;256:887-97.
Murayama Y, Nien YL, Duckwiler G, Gobin YP, Jahan R, Frazee J, et al. Guglielmi detachable coil
embolization of cerebral aneurysms: 11 years’experience. J Neurosurg. 2003;98:959-966.

112
CLINICAL RESEARCH CENTER FOR STROKE

2 급성기뇌졸중진료Acute Stroke Management
110-744 서울시종로구연건동28. 서울 학교병원임상의학연구소7208호
뇌졸중임상연구센터 표전화_02 2072 0652 FAX_02 747 0668


115
CLINICAL RESEARCH CENTER FOR STROKE
2.1 진료체계Organization 117
2.1.1 내원전환자관리및처치: 응급의료서비스/119 (Prehospital management and 117
field treatment: EMS/119)
2.1.2 뇌졸중전문치료실과뇌졸중센터 (Stroke unit and stroke center) 121
2 급성기뇌졸중진료Acute Stroke Management
2.2 급성기평가Acute evaluation 126
2.2.1 병력청취, 신체검사, 신경학적검사, 진단적검사 (History, physical exam, 126
neurological examination, laboratory test)
2.2.2 응급뇌 상검사 (Emergent neuroimaging) 133
2.3 급성기치료Acute treatment 141
2.3.1 일반적보존치료 (General supportive care) 141
2.3.1.1 기도, 호흡기, 산소공급 (Airway, ventilator, oxygen supply) 141
2.3.1.2 발열 (Fever) 143
2.3.1.3 심리듬 (Cardiac rhythm) 145
2.3.1.4 혈압 (Blood pressure) 147
2.3.1.5 혈당 (Blood glucose) 150
2.3.1.6 혈역학적치료, 혈액량확장제 (Volume expansion, hemorheologic therapy) 153
2.3.2 내과적합병증의예방및치료 (Prevention and management of
medical complication) 154
2.3.2.1 깊은정맥혈전증예방 (Deep vein thrombosis prophylaxis) 154
2.3.2.2 양 (Nutrition) 157
2.3.2.3 욕창 (Pressure sore) 159
2.3.2.4 흡인성폐렴 (Aspiration pneumonia) 161
2.3.2.5 비뇨기계감염 (Urinary tract infection) 162

116
CLINICAL RESEARCH CENTER FOR STROKE
2.3.3 혈전용해술 (Thrombolysis) 164
2.3.3.1 정맥내혈전용해술 (Intravenous thrombolysis) 2012.12 개정 164
2.3.3.2 동맥내혈전용해술 (Intra-arterial Thrombolysis) 2012.12 개정 176
2.3.4 항혈소판제 (Antiplatelet agents) 185
2.3.5 항응고제 (Anticoagulants) 187
2.3.6 신경보호제 (Neuroprotectants) 190
2.3.7 신경계합병증의치료 (Treatment of neurologic complications) 192
2.3.7.1 뇌압상승, 부종, 출혈성변환 (ICP elevation, brain edema, 192
and hemorrhagic transformation)
2.3.7.2 경련 (Seizure) 196
2.4 뇌실질내출혈의치료Treatment of intracerebral hemorrhage 198
2.4.1 뇌실질내출혈의약물치료(Medical Treatment of Intracerebral Hemorrhage) 198
2.4.1.1 뇌압조절 (ICP control) 2014.1 개정 198
2.4.1.2 항응고제와관련된뇌실질내출혈의내과적치료 (Medical treatment of 204
intracerebral hemorrhage in patients receiving anticoagulants)
2.4.1.3 뇌실질내출혈후혈압조절 (Blood pressure management after 207
intracerebral hemorrhage) 2014.1 개정
2.4.1.4 경련의예방및치료 (Seizure prevention and treatment) 2014.1 개정 212
2.4.2 뇌실질내출혈의수술적치료 (Surgical Treatment of Intracerebral Hemorrhage) 2014.1 개정 216
2.5 뇌졸중재활Rehabilitation in acute stroke 228
2.5.1 재활치료의시작 (Timing of stroke rehabilitation) 228
2.5.2 재활치료의강도 (Intensity of rehabilitation) 230
2.5.3 재활치료의접근방법 (Underlying approach to rehabilitation) 231
2.5.4 합병증관리 (Management of complication) 234

117
2.1. 진료체계Organization
뇌졸중은내과적혹은경우에따라서는외과적응급질환이다. 여러임상연구에서뇌졸중환자의초
기 응은응급의료서비스(119)를이용한경우가증상발생후병원도착까지의시간을단축시키고
혈전용해치료율을높 다. 또한뇌졸중의적절한치료를위해서는응급의료서비스종사자들에
한교육과체계화된환자관리가필요하다.
1. Activation of the 9-1-1 system by patients or other members of the public is strongly supported because
it speeds treatment of stroke (AHA/ASA: Class I, LOE:B). Dispatchers should make stroke a priority
dispatch.
2. To increase the number of patients who can be seen and treated within the first few hours after stroke,
educational programs to increase public awareness of stroke are recommended (AHA/ASA: Class I,
LOE:B).
3. To increase the number of patients who are treated, educational programs for physicians, hospital
personnel, and EMS personnel also are recommended (AHA/ASA: Class I, LOE:B).
4. Brief assessments by EMS personnel as outlined in Tables 1 are recommended (AHA/ASA: Class I,
LOE:B).
5. The use of a stroke identification algorithm such as Los Angeles or Cincinnati screens is encouraged
(AHA/ASA: Class I, LOE:B).
6. The panel recommends that EMS personnel begin the initial management of stroke in the field, as
outlined in Table 1 (AHA/ASA: Class I, LOE:B). The development of stroke protocols to be used by EMS
2.1.1. 내원전환자관리및처치: 응급의료서비스/119
Prehospital management and field treatment: EMS/119
CLINICAL RESEARCH CENTER FOR STROKE

118
personnel is strongly encouraged.
7. Patients should be transported rapidly for evaluation and treatment to the closest institution that provides
emergency stroke care (AHA/ASA: Class I, LOE:B). In some instances, this may involve air evacuation.
EMS personnel should notify the receiving ED so that the appropriate resources may be mobilized.
CLINICAL RESEARCH CENTER FOR STROKE
뇌졸중환자의초기 응은응급의료서비스/9-1-1 (EMS/911)을이용한경우가증상발생후병원도착
까지의시간뿐만아니라초기이학적검사, CT 촬 및신경학적검진까지소요되는시간을모두단
축시켰다.1-3또한뇌졸중의판별및치료에 한교육을응급의료서비스팀, 병원및지역사회일반의
를 상으로실시한경우가그렇지않은지역보다초기혈전용해치료율이더높았으며(8.65% vs.
2.21%), 특히혈전용해술(rt-PA) 치료 상군내에서는월등히높은(52% vs. 14%) 치료결과를보 다.4
또한중학생및그가족을 상으로한임상실험에서도뇌졸중급성기 처방안에 한교육을받은
경우가받지않은 조군에비해응급의료서비스활용및뇌졸중의초기 응에서의미있는차이를
보 다.5응급의료서비스팀을통해뇌졸중환자가적절한치료를받을수있는병원으로빠르게이송
되는것이바람직하다.6,7응급의료서비스팀이뇌졸중환자를빨리파악하여필요한조치를취할수
있도록병원전단계에서사용가능한뇌졸중판별척도(Table 2) 8,9가개발되었다.
Recommended Not Recommended
Manage ABCs Dextrose-containing fluids in nonhypoglycemic patients
Cardiac monitoring Hypotension/excessive blood pressure reduction
Intravenous access Excessive intravenous fluids
Oxygen (as required O2 saturation <92%)
Assess for hypoglycemia
Nil per os (NPO)
Alert receiving ED
Rapid transport to closest appropriate facility
capable of treating acute stroke
Table 1. Guidelines for EMS management of patients with suspected stroke

119
CLINICAL RESEARCH CENTER FOR STROKE
Los Angeles Prehospital Stroke Screen
Last time patient known to be symptom free, Date Time
Screening criteria
Age >45 y Yes Unknown No
No history of seizures or epilepsy Yes Unknown No
Symptoms present <24h Yes Unknown No
Not previously bedridden or wheelchair bound
If unknown or yesYes Unknown No
Blood glucose 60 to 400 mg/dL Yes No
Examination
Facial smile grimace Normal Right drop Left drop
Grip Normal Right weak Left weak
No grip No grip
Arm length Normal Right drift Left drift
Right falls Left falls
Based on examination, patient has unilateral
weakness, if items are yes or unknown, Yes No
meets criteria for stroke
Cincinnati Prehospital Stroke Scale
Facial droop
Normal - both sides of face move equally
Abnormal - one side face does not move as well as other
Arm drift
Normal - both arms move the same or both arms do not move at all
Abnormal - one arm either does not move or drifts down compared to the other
Speech
Normal - says correct words with no slurring
Abnormal - slurs words, says the wrong words, or is unable to speak
Table 2. Prehospital stroke identification instruments
1. 뇌졸중환자후송시1-1-9/응급의료서비스를활용하는것이권장된다. (근거수준III, 권고수준B)
2. 응급의료서비스팀은뇌졸중환자를최단시간내에뇌졸중에 한적정진료가가능한병원으로
이송한다. (권고수준GPP)

120
CLINICAL RESEARCH CENTER FOR STROKE
1. Barsan WG, Brott TG, Broderick JP, et al. Time of hospital presentation in patients with acute stroke.
Arch Intern Med. 1993;153:2558-2561.
2. Morris DL, Rosamond W, Madden K, et al. Prehospital and emergency department delays after acute
stroke: The genentech stroke presentation survey.Stroke.2000;31:2585-2590.
3. Lacy CR, Suh DC, Bueno M, et al. Delay in presentation and evaluation for acute stroke: Stroke time
registry for outcomes knowledge and epidemiology (S.T.R.O.K.E.). Stroke. 2001;32:63-69.
4. Morgenstern LB, Staub L, Chan W, et al. Improving delivery of acute stroke therapy: The TLL temple
foundation stroke project.Stroke. 2002;33:160-166.
5. Morgenstern LB, Gonzales NR, Maddox KE, et al. A randomized, controlled trial to teach middle school
children to recognize stroke and call 911: The kids identifying and defeating stroke project. Stroke.
2007;38:2972-2978.
6. Morgenstern LB, Bartholomew LK, Grotta JC, et al. Sustained benefit of a community and professional
intervention to increase acute stroke therapy. Arch Intern Med. 2003;163:2198-2202.
7. Alberts MJ, Hademenos G, Latchaw RE, et al. Recommendations for the establishment of primary
stroke centers. Brain attack coalition. JAMA. 2000;283:3102-3109.
8. Kidwell CS, Starkman S, Eckstein M, Weems K, Saver JL. Identifying stroke in the field: prospective
validation of the Los Angeles Prehospital Stroke Screen (LAPSS). Stroke. 2000;31:71-76.
9. Kothari RU, Pancioli A, Liu T, Brott T, Broderick J. Cincinnati Prehospital Stroke Scale: reproducibility and
validity. Ann Emerg Med. 1999;33:373-378.

121
CLINICAL RESEARCH CENTER FOR STROKE
뇌졸중전문치료실(stroke unit)과뇌졸중센터는뇌졸중치료에특화된다학제간인력, 시설및지침
으로구성된독립된치료단위를뜻하며, 뇌졸중치료에있어그중요성이강조되고있다.
1. Stroke patients should be treated in specialized stroke units (EUSI: LOE I).
2. Stroke units should provide co-ordinated multidisciplinary care provided by medical, nursing and therapy
staff who specialize in stroke care (EUSI: LOE I).
3. The creation of Primary Stroke Center (PSC) is strongly recommended (AHA/ASA: Class I, LOE B). The
organization of such resources will depend on local variables. The design of several community-based
PSC that provide emergency care and that are closely associated with a Comprehensive Stroke Center
(CSC), which provides more extensive care, has considerable appeal.
4. The development of CSC is recommended (AHA/ASA: Class I, LOE C).
5. Certification of stroke centers by an external body, such as Joint Commission on the Accreditation of
Healthcare Organizations (JCAHO), is encouraged (AHA/ASA: Class I, LOE B). The panel encourages
additional medical centers to seek such certification.
6. For patients with suspected stroke, EMS should bypass hospitals that do not have resources to treat
stroke and go to the closest facility capable of treating acute stroke (AHA/ASA: Class I, LOE B).
1. 뇌졸중전문치료실과센터의정의
뇌졸중전문치료실(stoke unit)은일반적으로급성뇌졸중치료실[acute (neurological) stroke unit] (1
주이내), 재활치료실(rehabilitation unit), 이둘을모두포함하는포괄적뇌졸중전문치료실
(comprehensive stroke unit) 등으로분류할수있다. 유럽에서는주로뇌졸중전문치료실에서의치
료를권장하는반면미국에서는더확장된개념인뇌졸중센터의확립을강조한다. 뇌졸중센터는
2.1.2. 뇌졸중전문치료실과뇌졸중센터Stroke unit and stroke center
122
다시일차진료를담당하는일차뇌졸중센터(primary stroke center)와최상의진료기능을하는포
괄적뇌졸중센터(comprehensive stroke center)로구분된다. 뇌졸중전문치료실및센터는신경과,
신경외과, 상의학과, 재활의학과, 간호부등으로이루어진다학제간접근(multi-disciplinary
approach), 독립된치료병동및다양한진단과치료가가능한시설(structure and facility), 뇌졸중환
자를위한지침(guideline, stroke code and critical pathway) 등이중요하다.
2. 뇌졸중전문치료실의효과
2002년Cochrane Database를포함, 수차례에걸쳐시행된메타분석(meta analysis)에따르면뇌졸중
전문치료실에서치료받은환자는그렇지않은환자에비해1년후사망률이14% 감소하고(OR 0.86,
95% CI 0.71-0.94, NNT 33), 사망하거나현저한후유장애가남을확률이22% 감소한다.1(OR 0.78, 95%
CI 0.68-0.89) 이러한효과는다른뇌졸중치료방법과비교하여볼때매우큰것으로, 환자의나이,
성별, 뇌졸중의심한정도에상관없이나타났으며, 독립된병동인경우그효과가더크다. 입원기
간연장의우려가있었으나보다상세한분석결과그러한현상은관찰되지않았다. 또한뇌졸중팀
만운 하는경우뇌졸중전문치료실과같은긍정적효과는나타나지않았다.2뇌졸중전문치료실
의이러한긍정적효과는혈전용해치료율의증가및급성기합병증의감소등으로인한것으로생
각된다.3, 4
3. 뇌졸중전문치료실및센터의구성요건
1) 뇌졸중전문치료실
일반적인뇌졸중전문치료실의구성요소로는 i) 환자평가(의학적, 간호학적, 치료적), ii) 초기치
료(예. 조기재활, 저산소증의교정), iii) 재활치료등이거론되며5참고로EUSI 의뇌졸중전문치료
실의구비요건은Table 1.과같다.6
CLINICAL RESEARCH CENTER FOR STROKE

123
CLINICAL RESEARCH CENTER FOR STROKE
2) 뇌졸중센터
미국의Brain Attack Coalition에서일차뇌졸중센터(primary stroke center) (Table 2)7와포괄적뇌졸중센
터(comprehensive stroke center)8에관한권고안을각각발표하 다. 또한유럽에서도전문가들에게
의뢰한설문결과를토 로뇌졸중센터의필수요건에 해기술하 다.9그러나이를실제유럽의병
원에적용해본결과, 10% 미만의병원에서만이적절한치료가행해지고, 40% 에서는최소한의진료
수준조차도달하지못하는등의결과를보여, 제시된요건이너무이상적임을반증함과동시에, 아직
도개선할여지가많다는것을보여주었다.10
Minimum requirements for centers managing acute stroke patients
1 Availability of 24-hour CT scanning
2 Established stroke treatment guidelines and operational procedures
3 Close co-operation of neurologists, internists and rehabilitation experts
4 Specially trained nursing personnel
5 Early multidisciplinary rehabilitation including speech therapy, occupational therapy and physical therapy
6 Established network of rehabilitation facilities to provide a continuous process of care
7 Neurosonological investigations within 24 h (extracranial vessels, colour-coded duplex sonography)
8 ECG, echocardiography
9 Laboratory examinations (including coagulation parameters)
10 Monitoring of blood pressure, ECG, oxygen saturation, blood glucose, body temperature
Additional facilities recommended
1 MRI/MRA
2 Diffusion and perfusion MR
3 CTA
4 Echocardiography (transoesophageal)
5 Cerebral angiography
6 Transcranial Doppler sonography
7 Specialized neuroradiological, neurosurgical and vascular surgical consultation
Table 1. Requirement for Stroke Unit

124
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌졸중환자는뇌졸중전문치료실혹은뇌졸중센터(일차혹은포괄적)에서치료하는것이권장된
다. (근거수준Ia, 권고수준A)
1. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev. 2002:CD000197.
2. Langhorne P, Dey P, Woodman M, Kalra L, Wood-Dauphinee S, Patel N, Hamrin E. Is stroke unit care
4. 뇌졸중센터의검증(certification)
병원에설립된뇌졸중센터는제3기관을통해인증을받는것이최근선진국의경향이다. 미국의
경우Joint Commission (JC)에서일차뇌졸중센터에 한인증작업을하고있다.
Patient Care areas
Acute stroke teams
Written care protocols
Emergency medical services
Emergency department
Stroke unit*
Neurosurgical services
Support services
Commitment and support of medical organization: a stroke center director
Neuroimaging services
Laboratory services
Outcome and quality improvement activities
Continuing medical education
* A stroke unit is only required for those primary stroke centers that will
provide ongoing in-hospital care for patients with stroke.
Table 2. Major Elements of a Primary Stroke Center

125
CLINICAL RESEARCH CENTER FOR STROKE
portable? A systematic review of the clinical trials. Age Ageing. 2005;34:324-330.
3. Douglas VC, Tong DC, Gillum LA, Zhao S, Brass LM, Dostal J, Johnston SC. Do the brain attack
coalition's criteria for stroke centers improve care for ischemic stroke? Neurology. 2005;64:422-427.
4. Govan L, Langhorne P, Weir CJ. Does the prevention of complications explain the survival benefit of
organized inpatient (stroke unit) care?: Further analysis of a systematic review. Stroke. 2007;38:2536-
2540.
5. Langhorne P, Pollock A. What are the components of effective stroke unit care? Age Ageing.
2002;31:365-371.
6. Brainin M, Olsen TS, Chamorro A, Diener HC, Ferro J, Hennerici MG, Langhorne P, Sivenius J.
Organization of stroke care: Education, referral, emergency management and imaging, stroke units
and rehabilitation. European stroke initiative. Cerebrovasc Dis. 2004;17 Suppl2:1-14.
7. Alberts MJ, Hademenos G, Latchaw RE, Jagoda A, Marler JR, Mayberg MR, Starke RD, Todd HW, Viste
KM, Girgus M, Shephard T, Emr M, Shwayder P, Walker MD. Recommendations for the establishment
of primary stroke centers. Brain attack coalition. JAMA. 2000;283:3102-3109.
8. Alberts MJ, Latchaw RE, Selman WR, Shephard T, Hadley MN, Brass LM, Koroshetz W, Marler JR,
Booss J, Zorowitz RD, Croft JB, Magnis E, Mulligan D, Jagoda A, O'Connor R, Cawley CM, Connors JJ,
Rose-DeRenzy JA, Emr M, Warren M, Walker MD. Recommendations for comprehensive stroke
centers: A consensus statement from the brain attack coalition. Stroke. 2005;36:1597-1616.
9. Leys D, Ringelstein EB, Kaste M, Hacke W. The main components of stroke unit care: Results of a
European expert survey. Cerebrovasc Dis. 2007;23:344-352.
10. Leys D, Ringelstein EB, Kaste M, Hacke W. Facilities available in European hospitals treating stroke
patients. Stroke. 2007;38:2985-2991.

CLINICAL RESEARCH CENTER FOR STROKE
2.2. 급성기평가Acute evaluation
2.2.1. 병력청취, 신체검사, 신경학적검사, 진단적검사History, Physical exam, neurological examination, laboratory test
급성기허혈성뇌졸중은발생후치료가능한시간이짧으므로, 허혈성뇌경색의신속한진단과평가
가매우중요하다. 체계적인프로토콜과뇌졸중팀구성이임상적진단, 진단검사의수행, 조기치료의
결정을신속하게할수있다. 병력, 일반적인신체검사, 신경학적검사로구성된임상적진단은기본
적인핵심평가요소이고, 이에근거한임상진단이신속하게이루어져야한다. 최종목적은뇌졸중을
확진하고재조합조직플라스미노겐활성제(rtPA)와같은급성기치료의적응증과금기증을확인하
는것이다. 응급치료에서시간이중요한변수이므로진단목적의검사들은제한된수만추천된다.
1. An organized protocol for the emergency evaluation of patients with suspected stroke is recommended
(AHA/ASA: Class I, LOE B). The goal is to complete an evaluation and to decide treatment within 60
minutes of the patient's arrival in an ED. Designation of an acute stroke team that includes physicians,
nurses, and laboratory/radiology personnel is encouraged. Patients with stroke should have a careful
clinical assessment, including neurological examination.
2. 1) The use of a stroke rating scale, preferably the NIHSS, is recommended (AHA/ASA: Class I, LOE B).
2) The initial neurological assessment should document the localization of the likely cerebral area
affected (RCP: GOR C).
3) A full medical assessment should be undertaken and multidisciplinary assessment considered for all
acute stroke patients to define the nature of the event, the need for investigation, further management,
and the need for rehabilitation (SIGN: LOE IV GOR C).
3. A limited number of hematologic, coagulation, and biochemistry tests are recommended during the
126

127
CLINICAL RESEARCH CENTER FOR STROKE
initial emergency evaluation (Table 1) (AHA/ASA, Class I, LOE B).
4. Patients with clinical or other evidence of acute cardiac or pulmonary disease may warrant chest X-ray
(AHA/ASA, Class I, LOE B).
5. An ECG is recommended because of the high incidence of heart disease in patients with stroke
(AHA/ASA Class I, LOE B).
6. Most patients with stroke do not need a chest X-ray as part of their initial evaluation (AHA/ASA: Class III,
LOE B).
7.Most patients with stroke do not need an examination of the cerebrospinal fluid (AHA/ASA: Class III, LOE
B). The yield of brain imaging is very high for detection of intracranial hemorrhage. Examination of the
cerebrospinal fluid may be indicated for evaluation of a patient with a stroke that may be secondary to an
infectious illness.

128
CLINICAL RESEARCH CENTER FOR STROKE
1. 병력청취(History)
병력청취중가장중요한것은증상발생시간이다. 증상발생시간의정의는해당뇌졸중에 한
증상이처음발생한시간이다. 자다가깨어난경우와같이정확한시작시간을모르는경우에는잠
들기전정상으로확인된마지막시간을증상발생시간으로하여야한다. 일과성뇌허혈이있다가
All patients
Noncontrast brain CT or brain MRI
Blood glucose
Serum electrolytes/renal function tests
ECG
Markers of cardiac ischemia
Complete blood count, including platelet count*
Prothrombin time/international normalized ratio (INR)*
Activated partial thromboplastin time*
Oxygen saturation
Selected patients
Hepatic function tests
Toxicology screen
Blood alcohol level
Pregnancy test
Arterial blood gas tests (if hypoxia is suspected)
Chest radiography (if lung disease is suspected)
Lumbar puncture (if subarachnoid hemorrhage is suspected and CT scan is negative for blood)
Electroencephalogram (if seizures are suspected)
* Although it is desirable to know the results of these tests before giving rtPA, thrombolytic therapy should not be delayed while
awaiting the results unless
(1) there is clinical suspicion of a bleeding abnormality or thrombocytopenia,
(2) the patient has received heparin or warfarin, or
(3) use of anticoagulants is not known.
Table 1. Immediate Diagnostic Studies: Evaluation of a Patient With Suspected Acute Ischemic Stroke

129
CLINICAL RESEARCH CENTER FOR STROKE
다시뇌졸중증상이발생한경우에는처음일과성허혈성증상이시작된시점이아니라새로뇌졸
중증상이시작된시점이증상발생시간이다.1
증상이발생할당시의상황이나뇌졸중이외의다른원인일가능성을시사하는특징들에 하여
병력청취에서추가적으로확인하는것이감별진단을위해필요하다. 모든환자에서동맥경화증
과심장질환의위험요인들에 해정보를파악하고, 약물남용, 편두통, 경련발작, 감염, 외상및임
신에관한병력에 해알아보아야한다. 급성기뇌경색에서치료적중재술에 한적격성여부를
판단할병력자료를얻어야한다.2 뇌졸중과유사한증상을가지는고혈압성뇌병증, 전환장애, 저
혈당증, 편두통, 간질등의질환들과감별할수있는정보를얻는다. 응급실에서활용할수있는뇌
졸중감별진단도구들이개발되어사용되고있다.3
2. 신체검사(Physical exam)
급성뇌졸중의신체검사에는호흡수, 맥박, 혈압, 체온의평가가포함되어야한다. 두부및목부위
진찰은외상및경련발작(멍, 혀의상처), 경동맥질환(경동맥잡음), 심부전을알수있게한다. 심장
진찰은심허혈, 판막상태, 불규칙적인리듬, 드물게는 동맥박리가동반되었는지여부에초점을
맞추어야한다. 호흡및복부진찰을통해서도역시다른질환이동반되었는지찾으려고노력하여
야한다. 피부및상하지진찰을통해간기능이상, 응고병증, 혈소판기능이상(예: 황달, 색자반, 점
출혈) 등과같은중요한전신상태를가늠할수도있다.2
3. 신경학적진찰과뇌졸중척도(Neurological examination and stroke scale scores)
신경학적검사를통해측정되는뇌졸중의임상상태는예후의강력한지표가될수있다. 이때구
체적인점수체계를갖추는것이검사의질을높인다. 특히NIH stroke scale(NIHSS)은이미전세계
적으로폭넓게사용되고있는척도이다.3,4초기NIHSS 점수는환자의예후를예측할수있는중요
한도구이다.5-7재조합조직플라스미노겐활성제(rtPA) 사용시에도초기NIHSS 점수가부작용및
예후에 향을준다.8이러한척도는비신경전문의료진도폭넓게사용할수있다.7,9 표준화된신경
학적검사를사용하는것이신경학적검사의중요부분을빠뜨리지않으면서도신속하게평가할
수있게한다. 이들점수는신경손상정도를정량화하고, 보건관리전문가사이에정보교환을촉진
시키고, 조기에예후를예측할수있게하고, 합병증의가능성, 다양한중재술에 한환자의적격
성여부를판단하는데도움을준다.10-12또한뇌졸중치료를담당하는응급실의사들이표준화된

130
척도을사용함으로써뇌졸중환자를정확하게확인하고안전하게치료할수있음을보여주었다.13,14
4. 혈액학적진단검사
혈액학적진단검사를통해허혈성뇌졸중이의심되는환자에서뇌졸중과유사한증상의질환을
가진사람들을가려내고, 뇌졸중의원인규명과치료선택을위해반드시수행되어야한다. 이들검
사에는혈당, 전해질, 전체혈구계산, 프로트롬빈시간 - 국제표준화치(prothrombin time-
international normalized ratio, PT-INR), 활성부분트롬보플라스틴시간(activated partial
thromboplastin time, aPTT), 신장기능검사들이포함된다.2저혈당은뇌졸중과유사하게국소증상
을보일수있으므로뇌졸중으로오진되기도한다. 고혈당은뇌졸중의예후를나쁘게할수있다.15
항응고제를복용하거나간기능이나쁜사람에게서혈소판의수와PT-INR 검사는매우중요하고
재조합조직플라스미노겐활성제를사용하는환자에서는결과를확인하여야한다. 그러나출혈성
경향, 저혈소판증, 항응고제복용병력이의심되지않는다면, 혈액검사결과를기다림으로써재조
합조직플라스미노겐활성제치료를지연해서는안된다. 환자의개별상황에따라추가적인검사
들이시행될수있다.
5. 기타검사들
12지심전도검사상비정상소견이급성기뇌졸중에서빈번히나타나고, 3개월사망률을예측하는
데도움을줄수있다.16심장이상은뇌졸중환자들에서흔히발견되고, 그중일부환자들은심장에
해급성치료를요하는경우도있다. 즉, 급성심근경색증은뇌졸중을유발하고, 급성뇌졸중은심
근경색을유발하기도한다.17-20부가적으로심장부정맥이급성뇌경색후에발생하기도한다.18,19,21,22
심방세동은뇌경색의중요한원인이므로, 심장모니터링을통해심각한심장부정맥이존재하는지
찾아야한다.23
단순흉부촬 은급성기허혈성뇌졸중을가진모든환자에서시행되어야한다고많은치료지침에
기술되어있지만, 급성기뇌줄중에서진단적가치를제공한다는근거는없다.2,24뇌척수액검사는
거미막밑출혈이의심되는환자에서CT상출혈을확인할수없는경우에시행할수있다.2뇌파검사
는뇌졸중의초기증상으로경련이의심되는증상이발생하거나합병증으로경련이발생한환자에
서추천된다.25
CLINICAL RESEARCH CENTER FOR STROKE

131
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌졸중을진료하는병원에서는뇌졸중을신속하게진단하고평가할수있는임상지침을준비한다.
(근거수준IV, 권고수준C)
2. 급성기뇌졸중의초기검사는신경학적검사외에호흡수, 맥박, 혈압및체온의평가를포함한다.
(근거수준IV, 권고수준C)
3. 초기뇌졸중중증도의평가척도로NIHSS의사용을권장한다. (근거수준III, 권고수준B)
4. 뇌졸중환자의기본적진단검사로전혈구계산, 혈당, 전해질, 신장기능, 프로트롬빈시간국제표준
화치(PT-INR), 활성부분트롬보플라스틴시간(aPTT) 등이포함된다. (근거수준IV, 권고수준C)
5. 임상적인심장계통진찰및12지심전도검사는모든뇌졸중환자에서시행한다. (근거수준 III, 권고
수준B)
6. 단순흉부촬 은급성기허혈성뇌졸중을가진환자에서선택적으로시행할수있다. (근거수준 IV,
권고수준C)
7. 뇌척수액검사는거미막밑출혈이의심되는환자에서CT 또는MRI 에서출혈을확인할수없는경
우에시행할수있다. (근거수준IV, 권고수준C)
8. 뇌파검사는뇌졸중의초기증상으로경련이의심되는증상이발생하거나합병증으로경련이발생
한환자에서추천된다. (근거수준III, 권고수준B)
1. Kidwell CS, Alger JR, Di Salle F, Starkman S, Villablanca P, Bentson J, Saver JL. Diffusion MRI in patients
with transient ischemic attacks. Stroke. 1999;30:1174-1180.
2. Adams HP, Jr., Brott TG, Crowell RM, Furlan AJ, Gomez CR, Grotta J, Helgason CM, Marler JR, Woolson
RF, Zivin JA, et al. Guidelines for the management of patients with acute ischemic stroke. A statement for
healthcare professionals from a special writing group of the stroke council, American Heart Association.
Circulation. 1994;90:1588-1601.
3. Brott T, Adams HP, Jr., Olinger CP, Marler JR, Barsan WG, Biller J, Spilker J, Holleran R, Eberle R,
Hertzberg V, et al. Measurements of acute cerebral infarction: A clinical examination scale. Stroke.
1989;20:864-870.

132
4. Goldstein LB, Bertels C, Davis JN. Interrater reliability of the NIH stroke scale. Arch Neurol. 1989;46:660-
662.
5. Adams HP, Jr., Davis PH, Leira EC, Chang KC, Bendixen BH, Clarke WR, Woolson RF, Hansen MD.
Baseline NIH stroke scale score strongly predicts outcome after stroke: A report of the trial of org 10172
in acute stroke treatment (TOAST). Neurology.1999;53:126-131.
6. Kwiatkowski TG, Libman RB, Frankel M, Tilley BC, Morgenstern LB, Lu M, Broderick JP, Lewandowski
CA, Marler JR, Levine SR, Brott T. Effects of tissue plasminogen activator for acute ischemic stroke at
one year. National institute of neurological disorders and stroke recombinant tissue plasminogen
activator stroke study group. N Engl J Med.1999;340:1781-1787.
7. Muir KW, Weir CJ, Murray GD, Povey C, Lees KR. Comparison of neurological scales and scoring
systems for acute stroke prognosis. Stroke.1996;27:1817-1820.
8. 2005 American heart association guidelines for cardiopulmonary resuscitation and emergency
cardiovascular care. Circulation. 2005;112:IV1-203.
9. Goldstein LB, Samsa GP. Reliability of the national institutes of health stroke scale. Extension to non-
neurologists in the context of a clinical trial. Stroke. 1997;28:307-310.
10. Frankel MR, Morgenstern LB, Kwiatkowski T, Lu M, Tilley BC, Broderick JP, Libman R, Levine SR,
Brott T. Predicting prognosis after stroke: A placebo group analysis from the National Institute of
Neurological Disorders and Stroke rt-PA stroke trial. Neurology. 2000;55:952-959.
11. Krieger DW. Should a hospital without a neurologist use t-PA to treat stroke? Cleve Clin J Med.
1999;66:585-586.
12. Lewandowski CA, Frankel M, Tomsick TA, Broderick J, Frey J, Clark W, Starkman S, Grotta J, Spilker J,
Khoury J, Brott T. Combined intravenous and intra-arterial r-tPA versus intra-arterial therapy of acute
ischemic stroke: Emergency management of stroke (EMS) bridging trial. Stroke.1999;30:2598-2605.
13. Kothari RU, Brott T, Broderick JP, Hamilton CA. Emergency physicians. Accuracy in the diagnosis of
stroke. Stroke. 1995;26:2238-2241.
14. Morgenstern LB, Lisabeth LD, Mecozzi AC, Smith MA, Longwell PJ, McFarling DA, Risser JM. A
population-based study of acute stroke and tia diagnosis. Neurology. 2004;62:895-900.
CLINICAL RESEARCH CENTER FOR STROKE
133
CLINICAL RESEARCH CENTER FOR STROKE
15. Gentile NT, Seftchick MW, Huynh T, Kruus LK, Gaughan J. Decreased mortality by normalizing blood
glucose after acute ischemic stroke. Acad Emerg Med.2006;13:174-180.
16. Christensen H, Fogh Christensen A, Boysen G. Abnormalities on ECG and telemetry predict stroke
outcome at 3 months. J Neurol Sci. 2005;234:99-103.
17. Dimant J, Grob D. Electrocardiographic changes and myocardial damage in patients with acute
cerebrovascular accidents. Stroke. 1977;8:448-455.
18. Oppenheimer SM. Neurogenic cardiac effects of cerebrovascular disease. Curr Opin Neurol.
1994;7:20-24
19. Oppenheimer SM, Hachinski VC. The cardiac consequences of stroke. Neurol Clin.1992;10:167-176.
20. Thompson PL, Robinson JS. Stroke after acute myocardial infarction: Relation to infarct size. Br Med J.
1978;2:457-459.
21. Norris JW, Froggatt GM, Hachinski VC. Cardiac arrhythmias in acute stroke. Stroke. 1978;9:392-396.
22. Mikolich JR, Jacobs WC, Fletcher GF. Cardiac arrhythmias in patients with acute cerebrovascular
accidents. JAMA.1981;246:1314-1317.
23. Vingerhoets F, Bogousslavsky J, Regli F, Van Melle G. Atrial fibrillation after acute stroke. Stroke.
1993;24:26-30.
24. Sagar G, Riley P, Vohrah A. Is admission chest radiography of any clinical value in acute stroke
patients? Clin Radiol. 1996;51:499-502.
25. Bladin CF, Alexandrov AV, Bellavance A, Bornstein N, Chambers B, Cote R, Lebrun L, Pirisi A, Norris
JW. Seizures after stroke: A prospective multicenter study. Arch Neurol. 2000;57:1617-1622.
급성기뇌졸중치료방법들이발달함에따라뇌 상검사는환자들의초기평가에중요한역할을한
다. 병변의크기, 위치, 뇌경색에관련된혈관분포및뇌출혈의존재에관한뇌 상소견이단기및장
2.2.2. 응급뇌 상검사 Emergent neuroimaging

134
기적치료방침의결정에 향을준다. 즉뇌 상검사를통해되살릴수있는허혈성뇌조직의범위,
뇌혈관상태, 뇌혈류학적상태에관한정보를얻을수있고, 뇌출혈의위험율, 또는혈관의폐쇄부위
를확인하여재관류치료를할수있는환자의선정에도움을준다. CT와MRI가초기 상도구로선택
될수있다.
CLINICAL RESEARCH CENTER FOR STROKE
1. Imaging of the brain is recommended before initiating any specific therapy to treat acute ischemic stroke
(AHA/ASA: Class I, LOE A).
2. In most instances, CT will provide the information to make decisions about emergency management
(AHA/ASA: Class I, LOE A).
3. The brain imaging study should be interpreted by a physician with expertise in reading CT or MRI studies
of the brain (AHA/ASA: Class I, LOE A).
4. Some findings on CT, including the presence of a dense artery sign, are associated with poor outcomes
after stroke (AHA/ASA: Class I, LOE A).
5. Multimodal CT and MRI may provide additional information that will improve diagnosis of ischemic
stroke (AHA/ASA: Class I, LOE A).
6. Emergency treatment of stroke should not be delayed in order to obtain multimodal imaging studies
(AHA/ASA: Class III, LOE C).
7. Vascular imaging is necessary as a preliminary step for intra-arterial administration of pharmacological
agents, surgical procedures, or endovascular interventions (AHA/ASA: Class III, LOE B).
1. 비조 증강CT (non-contrast-enhanced CT Scan)
응급비조 증강뇌CT를통해 부분의뇌출혈과신경학적증상을가지는비혈관성원인질환 (예,
뇌종양)을비교적정확하게진단할수있다. 그러나CT는급성기의작은피질및피질하, 특히천막
하부위의뇌경색을진단하기위한민감도는떨어진다.1최근CT의초기허혈성뇌손상소견들및
혈관폐쇄에관한징후들이치료결정과예후에 향을주는것으로알려졌다.2,3초기뇌경색 역

135
CLINICAL RESEARCH CENTER FOR STROKE
이광범위한경우재조합조직플라스미노겐활성제를사용하면출혈의위험을높일수있다.4 6시
간이내재조합조직플라스미노겐활성제를투여한European trial의분석에의하면, 중 뇌동맥
역의1/3이상침범시출혈의위험도가증가하 다.5재조합조직플라스미노겐활성제를사용할
환자가응급실을방문하면, 25분이내에CT 촬 을마칠수있어야하고, 그후20분이내에 상이
판독되는것을목표로하여야한다.6추가적인CT 촬 은환자증상이악화될때시행될수있고, 재
조합조직플라스미노겐활성제사용후출혈성변화를확인하는데도움이된다.4
2. 다중모드CT (Multimodal CT)
최근 상기술의발달로급성기뇌졸중 상의다중모드접근에관심이증가되고있다. 다중모드
CT에는비조 증강CT, 관류CT(perfusion CT), CT 혈관조 술등이포함된다. 관류CT는전뇌관류
(whole brain perfusion) CT와동적관류(dynamic perfusion) CT 두방법이있고, 전뇌관류CT는뇌혈류
량 상을얻을수있고뇌혈류량 상에서저음 은허혈성핵심(ischemic core)을나타낸다. 그러
나뇌혈류나평균통과시간(mean transit time, MTT)을측정할수는없다. 동적관류CT는뇌혈류의
절 치, MTT 및뇌혈류량을제공하여주지만2-4, 제한된뇌단면 상만얻을수있어전체뇌혈관
역을보여주지못한다는단점이있다. 그럼에도불구하고최근연구에서는관류CT가뇌경색과
허혈성반음 (ischemic penumbra)를찾는데높은민감도와특이도를보여줄수있다고하 다.7-9
나선상(Helical) CT 혈관조 술은두개강내외의혈관을신속하게검사할수있어서혈관의협착및
폐색에 한정보를준다. 특히두개강내큰혈관폐색의진단에있어서이러한방법이초음파나
디지털감산혈관조 술(digital subtraction angiography)에비해신속, 용이, 정확하 다10,11
이러한다중모드CT는빠르게 상을얻을수있고, 일반적인CT 장비로수행이가능하다는장점
이있지만, 조 제를사용해야하고부가적인방사선피폭을받아야한다는단점이있다. 그러므로
급성기뇌졸중치료의결정에서관류CT와CT 조 술의역할이아직확립되어있지않다.
3. 다중모드MRI (Multimodal MRI)
다중모드MRI는확산강조 상(diffusion-weighted imaging, DWI), 관류강조 상(perfusion-weighted
imaging, PWI), MR 혈관조 술(MR angiography, MRA) 경사에코 상(gradient echo image), 액체감쇠
역전회복(fluid-attenuated inversion recovery) 및 T2 강조 상(T2-weighted image)의순서(sequence)
로구성되어있다.
136
DWI는허혈성병변을증상발생후수분이내에보여줄수있어뇌경색의크기, 위치, 시간적경과를
조기에식별할수있게한다. 뇌경색병변을진단하는데있어DWI의민감도(88-100%)와특이도(95-
100%)는매우높다. DWI는특히작은병변, 뇌줄기와소뇌에있는병변을찾아내는데있어CT에비
해우월하다.12-14
PWI는뇌혈류역학상태의상 적측정치를제공한다. 초기DWI, PWI 병변의크기는뇌졸중의임상
적중증도및최종뇌경색병변의크기와잘부합하는것으로알려져있다.15-17
허혈성반음 은MRI상에서 략적으로추정할수있는데, PWI 병변이DWI 병변보다큰경우로
PWI-DWI 불일치(mismatch)가이에해당된다. 그러나초기DWI 병변은가역적이고, PWI 병변또한
허혈성반음 역을과장하는것으로알려져있으므로, 해석에주의를요한다.18,19
비가역적인뇌경색과가역적인뇌경색을구분하고, 혈전용해술후출혈의위험성이높은환자를
선별할수있는MRI 기준을찾아내려는연구가진행중이다. 그러나아직임상에서혈전용해술을
시행할때MRI 기준을적용하여환자를선별하기에는근거가불충분하다.
최근의전향적연구들은급성뇌출혈병변을진단하는데있어경사에코 상을포함한MRI가CT
만큼정확함을보여주었다. 이러한사실들은혈전용해술 상환자를포함한급성뇌졸중환자의
진단에MRI가CT 없이단독으로이용될수있음을시사한다.20,21그러나지주막하출혈을의심하게
하는증상으로내원한환자에서는CT를시행하여야한다.
경사에코MRI는CT에서보이지않는무증상미세출혈을보여줄수있다. 이러한미세출혈이항혈
전제또는재조합조직플라스미노겐활성제투여후발생하는출혈을예측할수있는지표가되는
지에 해서는아직의견이엇갈리고있다.22-24특히미세출혈의개수가많은경우혈전용해술치료
결정을어떻게해야하는지는불분명하다.
MRA는두개강내외혈관들을검사하는데그이용이점점증가하고있다. 디지털감산혈관조 술
과비교했을때두개강내외혈관질환을진단하는데있어민감도와특이도는70%에서100%에이
른다.25, 26
4. 기타혈관 상검사들
CT 혈관조 술과MRA 외에경두개초음파, 경동맥초음파, 고식적혈관조 술등이두개강내외혈
관질환을진단하는데이용될수있다. 경두개초음파와고식적혈관조 술은혈전용해치료의효
과를모니터링하는데도유용하다.27,28증상발생8시간이내의환자들에서중재적방사선시술 상
CLINICAL RESEARCH CENTER FOR STROKE
137
CLINICAL RESEARCH CENTER FOR STROKE
1. 급성기뇌졸중이의심되는환자는신속히뇌 상검사를시행한다. (권고수준GPP)
2. 부분의경우, 응급실에서는비조 증강CT가치료결정에중요한정보를준다. (권고수준GPP)
3. 다중모드CT 또는MRI는급성기허혈성뇌경색의진단과치료를향상시킬수있으므로사용이권
장된다. (근거수준Ib, 권고수준A)
4. 동맥혈관내약물투여및중재적수술을하는경우에는두부및경부혈관상태에관한정보를제공
하여주는혈관 상검사들(CT 혈관조 술, MRA, 고식적혈관조 술, 초음파)이필요하다. (근거수
준IIb, 권고수준B)
환자를선별하는데이러한뇌혈관검사들은유용하다.
또한뇌혈관 상검사들은뇌졸중의병태생리적원인을정확히판정하여뇌졸중재발을막는치
료방침을세우는데필수적인검사이다.29,30 어떤검사를선택할지는환자개개인과의료환경에따
라결정한다.
1. Mullins ME, Schaefer PW, Sorensen AG, Halpern EF, Ay H, He J, Koroshetz WJ, Gonzalez RG. Ct and
conventional and diffusion-weighted MR imaging in acute stroke: Study in 691 patients at presentation to the
emergency department. Radiology. 2002;224:353-360.
2. von Kummer R, Allen KL, Holle R, Bozzao L, Bastianello S, Manelfe C, Bluhmki E, Ringleb P, Meier DH,
Hacke W. Acute stroke: Usefulness of early ct findings before thrombolytic therapy. Radiology. 1997;205:327-
333.
3. von Kummer R, Nolte PN, Schnittger H, Thron A, Ringelstein EB. Detectability of cerebral hemisphere
ischaemic infarcts by CT within 6 h of stroke. Neuroradiology. 1996;38:31-33.
4. Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, Boysen G, Bluhmki E, Hoxter G, Mahagne
MH, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric
stroke. The European cooperative acute stroke study (ECASS). JAMA. 1995;274:1017-1025.
5. The National Institute of Neurological Disorders and Stroke rt-PA stroke study group. Tissue plasminogen

138
activator for acute ischemic stroke. N Engl J Med.1995;333:1581-1587.
6. Patel SC, Levine SR, Tilley BC, Grotta JC, Lu M, Frankel M, Haley EC, Jr., Brott TG, Broderick JP, Horowitz S,
Lyden PD, Lewandowski CA, Marler JR, Welch KM. Lack of clinical significance of early ischemic changes on
computed tomography in acute stroke. JAMA. 2001;286:2830-2838.
7. Ezzeddine MA, Lev MH, McDonald CT, Rordorf G, Oliveira-Filho J, Aksoy FG, Farkas J, Segal AZ, Schwamm
LH, Gonzalez RG, Koroshetz WJ. CT angiography with whole brain perfused blood volume imaging: Added
clinical value in the assessment of acute stroke. Stroke.2002;33:959-966.
8. Schramm P, Schellinger PD, Klotz E, Kallenberg K, Fiebach JB, Kulkens S, Heiland S, Knauth M, Sartor K.
Comparison of perfusion computed tomography and computed tomography angiography source images with
perfusion-weighted imaging and diffusion-weighted imaging in patients with acute stroke of less than 6 hours'
duration. Stroke. 2004;35:1652-1658.
9. Wintermark M, Reichhart M, Thiran JP, Maeder P, Chalaron M, Schnyder P, Bogousslavsky J, Meuli R.
Prognostic accuracy of cerebral blood flow measurement by perfusion computed tomography, at the time of
emergency room admission, in acute stroke patients. Ann Neurol. 2002;51:417-432.
10. Esteban JM, Cervera V. Perfusion CT and angio ct in the assessment of acute stroke. Neuroradiology.
2004;46:705-715.
11. Wildermuth S, Knauth M, Brandt T, Winter R, Sartor K, Hacke W. Role of ct angiography in patient selection
for thrombolytic therapy in acute hemispheric stroke. Stroke.1998;29:935-938.
12. Lutsep HL, Albers GW, DeCrespigny A, Kamat GN, Marks MP, Moseley ME. Clinical utility of diffusion-
weighted magnetic resonance imaging in the assessment of ischemic stroke. Ann Neurol. 1997;41:574-580.
13. Warach S, Chien D, Li W, Ronthal M, Edelman RR. Fast magnetic resonance diffusion-weighted imaging of
acute human stroke. Neurology. 1992;42:1717-1723.
14. Warach S, Gaa J, Siewert B, Wielopolski P, Edelman RR. Acute human stroke studied by whole brain echo
planar diffusion-weighted magnetic resonance imaging. Ann Neurol.1995;37:231-241.
15. Barber PA, Darby DG, Desmond PM, Yang Q, Gerraty RP, Jolley D, Donnan GA, Tress BM, Davis SM.
Prediction of stroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology.
1998;51:418-426.
CLINICAL RESEARCH CENTER FOR STROKE

139
CLINICAL RESEARCH CENTER FOR STROKE
16. Lovblad KO, Baird AE, Schlaug G, Benfield A, Siewert B, Voetsch B, Connor A, Burzynski C, Edelman RR,
Warach S. Ischemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging
correlate with clinical outcome. Ann Neurol. 1997;42:164-170.
17. Tong DC, Yenari MA, Albers GW, O'Brien M, Marks MP, Moseley ME. Correlation of perfusion- and diffusion-
weighted MRI with NIHSS score in acute (<6.5 hour) ischemic stroke. Neurology. 1998;50:864-870.
18. Kidwell CS, Alger JR, Saver JL. Beyond mismatch: Evolving paradigms in imaging the ischemic penumbra
with multimodal magnetic resonance imaging. Stroke. 2003;34:2729-2735.
19. Sobesky J, Zaro Weber O, Lehnhardt FG, Hesselmann V, Neveling M, Jacobs A, Heiss WD. Does the
mismatch match the penumbra? Magnetic resonance imaging and positron emission tomography in early
ischemic stroke. Stroke. 2005;36:980-985.
20. Fiebach JB, Schellinger PD, Gass A, Kucinski T, Siebler M, Villringer A, Olkers P, Hirsch JG, Heiland S, Wilde
P, Jansen O, Rother J, Hacke W, Sartor K. Stroke magnetic resonance imaging is accurate in hyperacute
intracerebral hemorrhage: A multicenter study on the validity of stroke imaging. Stroke. 2004;35:502-506.
21. Kidwell CS, Chalela JA, Saver JL, Starkman S, Hill MD, Demchuk AM, Butman JA, Patronas N, Alger JR,
Latour LL, Luby ML, Baird AE, Leary MC, Tremwel M, Ovbiagele B, Fredieu A, Suzuki S, Villablanca JP, Davis
S, Dunn B, Todd JW, Ezzeddine MA, Haymore J, Lynch JK, Davis L, Warach S. Comparison of MRI and CT for
detection of acute intracerebral hemorrhage.JAMA. 2004;292:1823-1830.
22. Kakuda W, Thijs VN, Lansberg MG, Bammer R, Wechsler L, Kemp S, Moseley ME, Marks MP, Albers GW.
Clinical importance of microbleeds in patients receiving IV thrombolysis. Neurology. 2005;65:1175-1178.
23. Kidwell CS, Saver JL, Villablanca JP, Duckwiler G, Fredieu A, Gough K, Leary MC, Starkman S, Gobin YP,
Jahan R, Vespa P, Liebeskind DS, Alger JR, Vinuela F. Magnetic resonance imaging detection of
microbleeds before thrombolysis: An emerging application. Stroke. 2002;33:95-98.
24. Wong KS, Chan YL, Liu JY, Gao S, Lam WW. Asymptomatic microbleeds as a risk factor for aspirin-
associated intracerebral hemorrhages. Neurology. 2003;60:511-513,
25. Qureshi AI, Isa A, Cinnamon J, Fountain J, Ottenlips JR, Braimah J, Frankel MR. Magnetic resonance
angiography in patients with brain infarction. J Neuroimaging. 1998;8:65-70.
26. Scarabino T, Carriero A, Giannatempo GM, Marano R, De Matthaeis P, Bonomo L, Salvolini U. Contrast-

140
enhanced MR angiography (CE MRA) in the study of the carotid stenosis: Comparison with digital subtraction
angiography (DSA). J Neuroradiol.1999;26:87-91.
27. Alexandrov AV, Wojner AW, Grotta JC. Clotbust: Design of a randomized trial of ultrasound-enhanced
thrombolysis for acute ischemic stroke. J Neuroimaging.2004;14:108-112.
28. Demchuk AM, Burgin WS, Christou I, Felberg RA, Barber PA, Hill MD, Alexandrov AV. Thrombolysis in brain
ischemia (TIBI) transcranial doppler flow grades predict clinical severity, early recovery, and mortality in
patients treated with intravenous tissue plasminogen activator. Stroke. 2001;32:89-93.
29. Albers GW, Hart RG, Lutsep HL, Newell DW, Sacco RL. Addendum to the supplement to the guidelines for
the management of transient ischemic attacks. Stroke. 2000;31:1001.
30. Wolf PA, Clagett GP, Easton JD, Goldstein LB, Gorelick PB, Kelly-Hayes M, Sacco RL, Whisnant JP.
Preventing ischemic stroke in patients with prior stroke and transient ischemic attack : A statement for
healthcare professionals from the stroke council of the American Heart Association. Stroke. 1999;30:1991-
1994.
CLINICAL RESEARCH CENTER FOR STROKE

141
2.3. 급성기치료Acute treatment
적절한산소공급과호흡기능의유지는허혈성반음 (ischemic penumbra)의 사기능을유지하기
위해중요할수있다. 크기가큰뇌경색이나뇌간경색에서호흡기능의장애가나타날수있으며또한
흡인성폐렴, 심부전, 폐색전증, 만성폐질환의악화등으로유발될수있다. 중증의호흡기계장애, 중
증저산소혈증/고이산화탄소혈증, 의식저하환자에서조기에기관삽관을하여인공환기를시행하는
게필요할수도있다. 그러나, 아직까지는모든뇌경색환자에게일률적으로산소를공급할근거는부
족하다.
1. Arterial oxygen concentration should be maintained within normal limit (RCP: LOE III, GOR B).
2. 1) O2 administration is recommended in case of hypoxemia (blood gas analysis or O2 sat <92% at pulse
oxymetry) (EUSI: LOE IV).
2) Intubation is recommended in case of potentially reversible respiratory insufficiency (EUSI: LOE IV).
3. 1) Airway support and ventilatory assistance are recommended for the treatment of patients with acute
stroke who have decreased consciousness or who have bulbar dysfunction causing compromise of the
airway (ASA: GOR C).
2) Hypoxic patients with stroke should receive supplemental oxygen (ASA: GOR C).
2.3.1. 일반적보존치료General supportive care
2.3.1.1. 기도, 호흡기, 산소공급 Airway, ventilator, oxygen supply
CLINICAL RESEARCH CENTER FOR STROKE

142
저산소증을막고신경학적손상의진행을방지하기위해적절한산소농도의유지는매우중요하다.
저산소증의흔한원인으로기도폐색, 저호흡(hypoventilation), 흡인성폐렴, 무기폐등이있다. 의식저
하를보이거나뇌간경색이발생한환자의경우구인두(oropharynx)의움직임이저하되고반사기능을
유지하지못해기도유지에장애가생길위험이더욱높다. 일반적으로기도삽관을요하는환자의경
우예후가나쁘며이중50%가량이뇌경색발생30일이내에사망한다는보고가있다.1,2산소공급이
혈전용해술의치료가능시간(time window)을연장할수있을것이라는연구결과도있으나,3모든뇌
경색환자에서산소공급을일괄적으로시행하는방법은뇌경색의예후에 향을미치지않는다고
보고되고있다.4,5 따라서, 환자상태와관계없는일괄적인산소공급은권장되지않는다. 그러나급성
뇌경색환자에서산소포화도모니터링은필요하며산소포화도92-95%이하로떨어지지않도록하는
것이좋다고알려져있다.6
CLINICAL RESEARCH CENTER FOR STROKE
1. 의식저하또는호흡기계통의장애를보이는환자에서는기관내삽관및필요한경우기계호흡을
시행하는것이권장되며, 연수마비로인한호흡장애가우려되는환자에서도기관내삽관이도움이
될수있다. (근거수준IV, 권고수준C)
2. 저산소증이없는뇌경색환자에의추가적산소공급은권장되지않는다. (근거수준III, 권고수준B)
1. Bushnell CD, Phillips-Bute BG, Laskowitz DT, Lynch JR, Chilukuri V, Borel CO. Survival and outcome
after endotracheal intubation for acute stroke. Neurology.1999;52:1374-1381.
2. Grotta J, Pasteur W, Khwaja G, Hamel T, Fisher M, Ramirez A. Elective intubation for neurologic
deterioration after stroke. Neurology. 1995;45:640-644.
3. Kim HY, Singhal AB, Lo EH. Normobaric hyperoxia extends the reperfusion window in focal cerebral
ischemia. Ann Neurol. 2005;57:571-575.
4. Ronning OM, Guldvog B. Should stroke victims routinely receive supplemental oxygen? A quasi-
randomized controlled trial. Stroke. 1999;30:2033-2037.

143
CLINICAL RESEARCH CENTER FOR STROKE
1. Temperature should be maintained within normal limits (RCP: LOE III, GOR B).
2. Treatment of body temperature ≥37.5℃ is recommended (EUSI: LOE IV).
3. In case of fever, the search of a possible infection (site and etiology) is recommended, in order to start
tailored antibiotic treatment (EUSI: LOE IV).
4. 1) It is generally agreed that sources of fever should be treated and antipyretic medications should be
administered to lower temperature in febrile patients with stroke (ASA: GOR B). Medications such as
acetaminophen can lower body temperature modestly, but the effectiveness of treating either febrile or
nonfebrile patients to improve neurological outcomes is not established.
2) Insufficient evidence exists to recommend hypothermia for treatment of patients with acute stroke
(ASA).
발열은급성뇌경색의예후를나쁘게하는것으로잘알려져있다.1-5따라서해열제등을이용해체온
을떨어뜨리는것이예후를호전시키는데도움이될수있다.6
5. Singhal AB. A review of oxygen therapy in ischemic stroke.NeurolRes. 2007;29:173-183.
6. Treib J, Grauer MT, Woessner R, Morgenthaler M. Treatment of stroke on an intensive stroke unit: A
novel concept. Intensive Care Med.2000;26:1598-1611.
체온상승은 사량을증가시키며, 급성뇌경색에서뇌조직의손상에악 향을미칠수있다. 급성뇌
경색환자에서발열이발생할경우, 감염에 한자세한검사가필수적이며, 이와함께적절한항생제
및해열제의사용이필요하다.
2.3.1.2. 발열 Fever

144
여러동물실험과소규모임상시험에서저체온요법이신경보호효과를가진다는것이보고되어왔
다.7-11저체온은산소, 당등의 사요구량을감소시켜그효과를나타내며, 또한, 유해한세포내단백
용해반응(proteolytic reactions), 혈액뇌장벽의파괴, 활성산소의생성및분비, 루타메이트와같은세
포독성신경전달물질의분비등을줄여신경보호효과를나타낸다고알려져있다. 동물실험에따르
면조기에저체온요법을시작할수록그효과가좋으며오래시행할수록신경보호효과가좋다고한
다. 저체온요법이후체온을회복시킬때과도한 사반응으로인한반동성뇌압상승이일어날수
있다고알려져있다. 부정맥, 감염, 전해질불균형, 혈소판감소증등의부작용이나타날수있으므로
주의가필요하다.10
CLINICAL RESEARCH CENTER FOR STROKE
1. 급성뇌경색환자의체온은가급적정상범위내로유지되도록한다. (근거수준II, 권고수준B)
2. 발열이있는경우, 적절한항생제치료를위하여감염부위및원인병원체를찾아보아야한다. (근
거수준IV, 권고수준C)
3. 열이있을경우, 체온을낮추는것이도움이될수있으며, (근거수준 IV, 권고수준C) 해열제를사용
할수있다. (근거수준IIa, 권고수준B)
1. Azzimondi G, Bassein L, Nonino F, Fiorani L, Vignatelli L, Re G, D'Alessandro R. Fever in acute stroke
worsens prognosis. A prospective study. Stroke. 1995;26:2040-2043.
2. Hajat C, Hajat S, Sharma P. Effects of poststroke pyrexia on stroke outcome: A meta-analysis of studies
in patients. Stroke. 2000;31:410-414.
3. Jorgensen HS, Reith J, Nakayama H, Kammersgaard LP, Raaschou HO, Olsen TS. What determines
good recovery in patients with the most severe strokes? The Copenhagen stroke study. Stroke.
1999;30:2008-2012.
4. Reith J, Jorgensen HS, Pedersen PM, Nakayama H, Raaschou HO, Jeppesen LL, Olsen TS. Body
temperature in acute stroke: Relation to stroke severity, infarct size, mortality, and outcome. Lancet.
1996;347:422-425.

145
CLINICAL RESEARCH CENTER FOR STROKE
5. Wang Y, Lim LL, Levi C, Heller RF, Fisher J. Influence of admission body temperature on stroke
mortality. Stroke. 2000;31:404-409.
6. Kasner SE, Wein T, Piriyawat P, Villar-Cordova CE, Chalela JA, Krieger DW, Morgenstern LB, Kimmel
SE, Grotta JC. Acetaminophen for altering body temperature in acute stroke: A randomized clinical trial.
Stroke. 2002;33:130-134.
7. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med.
2002;346:549-556.
8. Hammer MD, Krieger DW. Acute ischemic stroke: Is there a role for hypothermia? Cleve Clin J Med.
2002;69:770, 773-774, 776-777 passim.
9. Hammer MD, Krieger DW. Hypothermia for acute ischemic stroke: Not just another neuroprotectant.
Neurologist.2003;9:280-289.
10. Krieger DW, De Georgia MA, Abou-Chebl A, Andrefsky JC, Sila CA, Katzan IL, Mayberg MR, Furlan AJ.
Cooling for acute ischemic brain damage (COOL AID): An open pilot study of induced hypothermia in
acute ischemic stroke. Stroke. 2001;32:1847-1854.
11. Schwab S, Schwarz S, Spranger M, Keller E, Bertram M, Hacke W. Moderate hypothermia in the
treatment of patients with severe middle cerebral artery infarction. Stroke. 1998;29:2461-2466.
뇌경색발생이후많게는15-30%까지심장리듬의이상이발견되는것으로보고되나, 이중 부분은
뇌경색의위험요인으로우연히뇌경색발생과함께발견되는경우이다. 그러나, 특정뇌부위를침범
한경우, 2차적으로심리듬의이상을포함한심장이상이나타날수있다고보고되고있다. 심부전, 급
성심근경색, 급사등은뇌경색의임상경과중에서나타날수있다. 정상심박수를유지하기위한적
절한심박출의유지및적절한혈압유지는뇌경색치료의기본이다.
2.3.1.3. 심리듬 Cardiac rhythm

146
1. General agreement supports the use of cardiac monitoring to screen for atrial fibrillation and other
potentially serious cardiac arrhythmias that would necessitate emergency cardiac interventions. It is
generally agreed that cardiac monitoring should be performed during the first 24 hours after onset of
ischemic stroke (ASA: GOR C).
CLINICAL RESEARCH CENTER FOR STROKE
급성심근경색이나심부정맥은급성뇌경색의중요한합병증중하나이다.1,2우측반구의뇌경색, 뇌섬
엽(insular) 뇌경색의경우교감, 부교감신경계의장애가나타날수있으며이로인해심부정맥이발생
할수있다.3-6또한카테콜아민의분비와연관된심근경색의발병도뇌경색의합병증으로발생할수
있다고보고되고있다.7가장흔히발견되는부정맥은심방세동이다. 뇌경색급성기에심장리듬의이
상을발견하기위해모니터링을하는것이중요하며, 필요시내과나심장전문의의자문하에정상심
리듬으로의회복을위해약물, 심율동전환 (cardioversion), 인공심박기(pacemaker) 삽입등을시행할
수있다.
1. 뇌경색급성기동안심장리듬의모니터링이고려된다. (근거수준IV, 권고수준C)
1. Korpelainen JT, Sotaniemi KA, Makikallio A, Huikuri HV, Myllyla VV. Dynamic behavior of heart rate in
ischemic stroke. Stroke. 1999;30:1008-1013.
2. Myers MG, Norris JW, Hachinski VC, Weingert ME, Sole MJ. Cardiac sequelae of acute stroke. Stroke.
1982;13:838-842.
3. Korpelainen JT, Sotaniemi KA, Huikuri HV, Myllya VV. Abnormal heart rate variability as a manifestation of
autonomic dysfunction in hemispheric brain infarction. Stroke. 1996;27:2059-2063.
4. Lane RD, Wallace JD, Petrosky PP, Schwartz GE, Gradman AH. Supraventricular tachycardia in patients

147
CLINICAL RESEARCH CENTER FOR STROKE
1. High blood pressure should not normally be lowered in the acute phase of stroke as this may worsen
outcome (SIGN: LOE IV, GOR C).
2. Routine blood pressure lowering is not recommended, except for extremely elevated values (>200-
220mmHg systolic blood pressure or 120mmHg diastolic blood pressure for ischemic stroke,
>180/105mmHg for hemorrhagic stroke) confirmed by repeated measurements. Immediate
antihypertensive therapy for moderate hypertension is recommended in case of stroke and heart failure,
aortic dissection, acute myocardial infarction, acute renal failure, thrombolysis or intravenous heparin,
with right hemisphere strokes. Stroke. 1992;23:362-366.
5. Pasquini M, Laurent C, Kroumova M, Masse I, Deplanque D, Leclerc X, Bordet R, Leys D. Insular infarcts
and electrocardiographic changes at admission: Results of the prognostic of insular cerebral infarcts
study (PRINCESS). J Neurol. 2006;253:618-624.
6. Tatschl C, Stollberger C, Matz K, Yilmaz N, Eckhardt R, Nowotny M, Dachenhausen A, Brainin M. Insular
involvement is associated with QT prolongation: ECG abnormalities in patients with acute stroke.
Cerebrovasc Dis. 2006;21:47-53.
7. Kolin A, Norris JW. Myocardial damage from acute cerebral lesions. Stroke. 1984;15:990-993.
허혈성뇌졸중의급성기에는혈압상승이흔히관찰되므로, 혈압의모니터링과치료는중요하다. 허
혈성부위는뇌혈류자동조절능(cerebral blood flow autoregulation)에장애가발생하여, 평균동맥압이
직접적으로뇌혈류에 향을미치게된다. 그러므로, 적절한뇌관류를위해서는혈압의갑작스런하
강을피하여야한다. 급성기뇌졸중환자에서혈압하강은비교적드물지만, 만일일어날경우, 수액공
급이나심장수축촉진제(inotropic agents)에의해혈압상승을유도할수있다.
2.3.1.4. 혈압 Blood pressure
148
CLINICAL RESEARCH CENTER FOR STROKE
but should be applied cautiously. Recommended target blood pressure in patients (a) with prior
hypertension: 180/100-105mmHg, without prior hypertension: 160-180/90-100mmHg, under
thrombolysis avoid systolic blood pressure above 180mmHg. Recommended drugs for blood pressure
treatment: (a) intravenous labetalol or urapidil and intravenous sodium nitroprusside, nitroglycerine, or
oral captopril. Avoid nifedipine and any drastic blood pressure decrease. Avoid and treat hypotension
particularly in unstable patients by administering adequate amounts of fluids and, when required,
volume expanders and/or catecholamines (epinephrine 0.1-2mg/h plus dobutamine 5-50mg/h) (EUSI:
LOE IV).
3. Blood pressure should only be lowered in the acute phase where there are likely to be complications
from hypertension, e.g. hypertensive encephalopathy, aortic aneurysm with renal involvement (RCP: LOE
Ib, GOR B).
4. Treatment of arterial hypertension
1) It is generally agreed that a cautious approach to the treatment of arterial hypertension should be
recommended (ASA: GOR C). Patients who have other medical indications for aggressive treatment of
blood pressure should be treated.
2) Patients who have elevated blood pressure and are otherwise eligible for treatment of rtPA may have
their blood pressure lowered so that their systolic blood pressure is <185mmHg and their diastolic
blood pressure is <110mm Hg before lytic therapy is started (ASA: GOR C).
3) Until other data become available, consensus exists that the previously described blood pressure
recommendations should be followed in patients undergoing other acute interventions to recanalize
occluded vessels, including intra-arterial thrombolysis (ASA: GOR C).
4) It is generally agreed that patients with markedly elevated blood pressure may have their blood
pressure lowered. A reasonable goal would be to lower blood pressure by �15% during the first 24
hours after onset of stroke. The level of blood pressure that would mandate such treatment is not
known, but consensus exists that medications should be withheld unless the systolic blood pressure is
>220mmHg or the diastolic blood pressure is >120mmHg (ASA: GOR C).
5) It is generally agreed that antihypertensive medications should be restarted at 24 hours for patients

149
CLINICAL RESEARCH CENTER FOR STROKE
허혈성뇌졸중발생이후혈압이상승하는경우가많다고알려져있으나1적절한치료에 해서는
정립된바는없다. 뇌졸중으로인한스트레스, 배뇨문제, 통증, 고혈압병력, 저산소증에 한생리적
반응, 두개내압상승등의이유로혈압이상승할수있다고알려져있으며, 혈압을낮춤으로써뇌부
종의감소, 출혈성변화위험감소, 추가적인혈관손상의예방, 초기의뇌졸중재발의예방등을꾀할
수있다. 그러나, 혈압상승에 한적극적인처치는뇌경색부위의관류감소를일으켜뇌경색부위
를확장시킬수있어2 일반적으로받아들여지지않는다. 규모무작위임상시험(randomized
controlled trial)은없으나, 고혈압성뇌병증(hypertensive encephalopathy), 동맥박리, 급성신부전, 급
성폐부종, 급성심근경색등의경우를제외하고는즉각적인혈압강하를위한약물투여는권장되지
않는다. 혈압의조절이필요한기준은확립되어있지않으나2, 미국과유럽에서는전문가의견으로
수축기혈압200-220mmHg, 확장기혈압120mmHg이하의경우에서는적극적인강압제의사용을유
보하는것으로합의가되어있다. 혈전용해치료를받는환자의경우에는혈전용해치료를받는동안
을포함하여그전후의혈압이출혈성변화와 접한관계를가지므로,3,4수축기혈압185mmHg, 확
장기혈압110mmHg를기준으로하여약물을투여한다.
1. 급성기허혈성뇌졸중환자에서수축기혈압220mmHg 또는확장기혈압120mmHg이하인경우에
는적극적인강압제의사용을유보하는것이권장된다. (근거수준IV, 권고수준C)
2. 혈전용해치료를시행하 을경우에는수축기혈압185mmHg, 확장기혈압110mmHg를기준으로
하여혈압강하제사용을고려한다. (근거수준IV, 권고수준C)
3. 급성기허혈성뇌졸중환자에서일률적인혈압강하는추천되지않지만, 고혈압으로인한합병증
who have preexisting hypertension and are neurologically stable unless a specific contraindication to
restarting treatment is known (ASA: GOR C).
6) It is generally agreed that the cause of arterial hypotension in the setting of acute stroke should be
sought. Hypovolemia should be corrected with normal saline, and cardiac arrhythmias that might be
reducing cardiac output should be corrected (ASA: GOR C).

150
발생이우려되는다음상황에서는적절한혈압강하가필요하다. 고혈압성뇌병증, 신동맥이침범
된 동맥꽈리 (근거수준 Ia, 권고수준A), 심장기능부전, 동맥박리, 급성심근경색, 급성신장기능
부전, 정맥내헤파린정주(근거수준IV, 권고수준C).
4. 급성기뇌졸중환자에서저혈압이발생한경우에는원인을조사하는것이권장된다. 저혈량증
(hypovolemia)이원인인경우에는생리식염수로교정하고, 심박출량을감소시키는심장부정맥은
교정하는것이권장된다. (근거수준IV, 권고수준C)
CLINICAL RESEARCH CENTER FOR STROKE
1. Qureshi AI, Ezzeddine MA, Nasar A, Suri MF, Kirmani JF, Hussein HM, Divani AA, Reddi AS. Prevalence
of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States.
Am J Emerg Med. 2007;25:32-38.
2. Powers WJ. Acute hypertension after stroke: The scientific basis for treatment decisions. Neurology.
1993;43:461-467.
3. Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. The NINDS t-PA stroke
study group. Stroke.1997;28:2109-2118.
4. Larrue V, von Kummer R, del Zoppo G, Bluhmki E. Hemorrhagic transformation in acute ischemic
stroke. Potential contributing factors in the European cooperative acute stroke study. Stroke.
1997;28:957-960.
급성기뇌졸중환자에서당뇨병의과거력이없는경우에도스트레스나급성질환으로인해고혈당이
나타날수있으며, 또한, 새로당뇨가진단되거나, 잘조절되던당뇨병이급성질환으로인해악화되어
고혈당이발생할수도있다. 고혈당은뇌경색의예후에나쁜 향을미치며, 이는당뇨병이진단된환
2.3.1.5. 혈당 Blood glucose
151
CLINICAL RESEARCH CENTER FOR STROKE
1. Blood glucose should be maintained within normal limit (RCP: LOE III, GOR B).
2. Glucose solutions are not recommended due to the detrimental effects of hyperglycemia (EUSI: LOE IV).
3. Management of hyperglycemia
4. Evidence indicates that persistent hyperglycemia (>140mg/dL) during the first 24 hours after stroke is
associated with poor outcomes, and thus it is generally agreed that hyperglycemia should be treated in
patients with acute ischemic stroke. The minimum threshold described in previous statements likely was
too high, and lower serum glucose concentrations (possibly >140 to 185mg/dL) probably should trigger
administration of insulin, similar to the procedure in other acute situations accompanied by hyperglycemia
(ASA: GOR C). Close monitoring of glucose concentrations with adjustment of insulin doses to avoid
hypoglycemia is recommended.
5. Treatment of serum glucose levels >10mmol/l with insulin titration is recommended (EUSI: LOE IV).
6. Management of hypoglycemia
7. It is generally agreed that hypoglycemia should be treated in patients with acute ischemic stroke
(ASA: GOR C). The goal is to achieve normoglycemia. Marked elevation of blood glucose levels should be
avoided.
8. Immediate correction of hypoglycemia is recommended by intravenous dextrose bolus or infusion of 10
-20% glucose (EUSI: LOE IV).
자뿐아니라당뇨병이없는환자에도해당된다. 그러므로일시적으로인슐린치료가필요할수있
다. 또한저혈당은뇌경색과비슷한증상을일으킬수있으므로, 우선적으로감별진단및치료가필
요하다.
저혈당은뇌경색과유사한국소신경학적장애를유발할수있으며, 또한저혈당자체가뇌손상을일으킬
수있으므로반드시응급으로교정하여야한다. 당뇨병은뇌경색의주요한위험요인의하나이며, 고혈당

152
이뇌경색의예후나출혈성변화에악 향을미친다는것은여러연구에서보고된바있다.1,2또한고혈당
이중증뇌경색의결과로나타날수도있어혈당의증가를뇌혈관질환의중증도의척도로생각할수도있
다.3고혈당으로인한뇌손상의기전은정확히밝혀지지않았으나, 조직의산증(acidosis)을증가시켜무산
소당분해과정(anaerobic glycolysis) 및혈액뇌장벽(blood-brain barrier)의투과성이증가하기때문으로생각
된다. 혈당과뇌경색의연관관계는보고되고있으나, 당화혈색소(HbA1C) 수치에따른뇌경색의예후에는
차이가없었고4정상혈당수준으로유지하 을때뇌경색의예후에미치는 향에 해서는입증되지않
았다.5, 6
CLINICAL RESEARCH CENTER FOR STROKE
1. 급성기뇌경색에서고혈당은교정되어야한다. (근거수준IV, 권고수준C)
2. 저혈당이발생한경우포도당용액을투여하여교정하여야한다. (근거수준IV, 권고수준C)
3. 특별한이유가없는한, 급성기뇌졸중에서포도당용액의투여는권장되지않는다. (근거수준 IV, 권
고수준C)
1. Bruno A, Biller J, Adams HP, Jr., Clarke WR, Woolson RF, Williams LS, Hansen MD. Acute blood glucose
level and outcome from ischemic stroke. Trial of org 10172 in acute stroke treatment (TOAST)
investigators. Neurology. 1999;52:280-284.
2. Candelise L, Landi G, Orazio EN, Boccardi E. Prognostic significance of hyperglycemia in acute stroke.
Arch Neurol. 1985;42:661-663.
3. Weir CJ, Murray GD, Dyker AG, Lees KR. Is hyperglycaemia an independent predictor of poor outcome
after acute stroke? Results of a long-term follow up study.BMJ. 1997;314:1303-1306.
4. Murros K, Fogelholm R, Kettunen S, Vuorela AL, Valve J. Blood glucose, glycosylated haemoglobin, and
outcome of ischemic brain infarction.J Neurol Sci.1992;111:59-64.
5. Gray CS, Hildreth AJ, Sandercock PA, O'Connell JE, Johnston DE, Cartlidge NE, Bamford JM, James OF,
Alberti KG. Glucose-potassium-insulin infusions in the management of post-stroke hyperglycaemia: The
153
CLINICAL RESEARCH CENTER FOR STROKE
1. Hydration should be maintained within normal limits (RCP: LOE III, GOR B).
2. Routine use of drugs to limit neural damage, including plasma volume expanders, is of no proven benefit
and should be discouraged (SIGN: LOE Ia & Ib, GOR A).
3. Hemodilution with or without venesection and volume expansion is not recommended for treatment of
patients with acute ischemic stroke (ASA: GOR A).
적절한심박출량을유지하는것은급성기뇌손상을줄이기위해중요하다. 저혈량증 (hypovolemia)
의교정, 심박출량에 향을줄수있는심장이상의교정이이를위해도움이될수있다. 그러나이러
한이상소견이동반되지않는경우, 급성기뇌경색의예후에혈액희석이별 향을주지않는다는
보고가있었으며, 측부순환을증가시키는점에서도혈액희석의효과에 한근거는없다.1-4
UK glucose insulin in stroke trial (GIST-UK). Lancet Neurol.2007;6:397-406.
6. Scott JF, Robinson GM, French JM, O'Connell JE, Alberti KG, Gray CS. Glucose potassium insulin
infusions in the treatment of acute stroke patients with mild to moderate hyperglycemia: The glucose
insulin in stroke trial (GIST). Stroke. 1999;30:793-799.
뇌경색진행의예방과허혈성반음 역(ischemic penumbra)의뇌경색방지를위해뇌관류(cerebral
perfusion)의유지가중요하며, 혈액희석(hemodilution)은손상된뇌조직으로의혈류를개선시켜뇌경
색의크기를줄일수있다는주장이있다.
2.3.1.6. 혈역학적치료, 혈액량확장제 Volume expansion, hemorheologic therapy
1. 급성기뇌경색의호전또는예후향상을위해모든환자에게혈액희석및혈액량확장제를사용하
는것은근거가부족하다. 그러나환자에따라서는사용을고려할수있다. (근거수준IV, 권고수준C)

154
CLINICAL RESEARCH CENTER FOR STROKE
1. Haemodilution in acute stroke: Results of the Italian haemodilution trial. Italian acute stroke study group.
Lancet. 1988;1:318-321.
2. Multicenter trial of hemodilution in acute ischemic stroke. Results of subgroup analyses. Scandinavian
stroke study group. Stroke. 1988;19:464-471.
3. Aichner FT, Fazekas F, Brainin M, Polz W, Mamoli B, Zeiler K. Hypervolemic hemodilution in acute
ischemic stroke: The multicenter Austrian hemodilution stroke trial (MAHST). Stroke. 1998;29:743-749.
4. Asplund K. Haemodilution for acute ischaemic stroke. Cochrane Database Syst Rev. 2002:CD000103.
깊은정맥혈전증(deep vein thrombosis)은신경학적장애가심할수록호발하나, 실제임상적으로폐동
맥색전증등의증세로발현되는경우는1% 내외로알려져있다.1깊은정맥혈전증은심한호흡기증
상을유발할수있으며뇌졸중의재활및회복의장애요인이되므로예방이중요하다.
1. ASA
1) Early mobilization of less severely affected patients and measures to prevent subacute complications of
stroke are recommended (Class I, Level of Evidence C).
2) Subcutaneous administration of anticoagulants is recommended for treatment of immobilized patients
to prevent deep vein thrombosis (Class I, Level of Evidence A). The ideal timing for starting these
medications is not known.
3) Aspirin is a potential intervention to prevent deep vein thrombosis but is less effective than
anticoagulants (Class IIa, Level of Evidence A).
4) The use of of intermittent external compression devices is recommended for treatment of patients who
cannot receive anticoagulants (Class IIa, Level of Evidence B).
2.3.2. 내과적합병증의예방및치료Prevention and management of medical complication
2.3.2.1. 깊은정맥혈전증예방 Deep vein thrombosis prophylaxis

155
CLINICAL RESEARCH CENTER FOR STROKE
2. RCP
1) Aspirin (50-300 mg daily) should be given according to the guidance in the recommendations in 3.5.3
on antithrombotic treatment (LOE Ib)
2) Compression stockings should be applied in stroke patients with weak or paralysed legs (once the
patient’s peripheral circulation, sensation and the state of the skin have been assessed) (LOE Ib)
3) Mobilisation and optimal hydration should be maintained as far as possible from the outset (LOE IV)
4) Prophylactic anticoagulation should not be used routinely (LOE Ia)
3. SIGN
1) Aspirin (initial starting dose 150-300 mg/day and 75mg/day or more therafter) should be given to all
patients with acute ischemic stroke in the first two weeks following stroke onset to help prevent deep
vein thrombosis and pulmonary embolism (provided there are no known contraindications to aspirin
therapy). Aspirin can be given by nasogastric tube or rectally (using 300 mg/day suppositories) for those
who are unable to swallow. (LOE 1++, GOR A)
2) Two weeks following acute ischemic stroke, clinicians should reassess the patient’s risk for DVT and
consider starting additional prophylactic medical treatment (e.g. heparin). (LOE 4, GOR D).
3) Physical methods (e.g. graduated elastic compression stockings) are preferred for patients recovering
from haemorrhagic stroke (LOE 4, GOR D).
4) Selected use of graduated elastic compression stockings may be justified for some high risk stroke
patients (LOE 1+, GOR C).
4. EUSI
1) Administration of heparin or low molecular weight heparin in bedridden patients after stroke is
recommended to reduce the number of deep venous thrombosis and pulmonary embolisms, however,
there is a risk of additional intracranial bleeding (Level I)
2) Early mobilization is helpful to prevent numerous complications after stroke, including aspiration
pneumonia, deep venous thrombosis and decubital ulcers (no evidence level)
깊은정맥혈전증은고령이고마비가심하며, 움직이지못하는환자에서더많이발생하므로, 되도록
빨리침 에서움직이는것이필요하다.2 마비가심한환자들에서깊은정맥혈전증과폐동맥색전증
을예방하는데에항응고제가도움이된다는결론은 부분뇌졸중이아닌환자를 상으로진행된
연구를통해얻어졌으나, 뇌졸중환자를 상으로시행된연구의메타분석에서도헤파린(heparin)
사용군이깊은정맥혈전증의발생을감소시키는데에효과가있는것으로알려져있다.3저분자량

156
CLINICAL RESEARCH CENTER FOR STROKE
1. 급성기뇌졸중환자에서깊은정맥혈전증을예방하기위해조기재활이도움이될수있다. (근거수
준III, 권고수준C)
2. 깊은정맥혈전증의발생위험이높은환자군은예방을위해헤파린피하주사를사용할수있으나출
혈의위험이증가하는것을고려해야한다. (근거수준 Ia, 권고수준A) 헤파린피하주사 신에저분
자량헤파린을사용할수도있다. (근거수준Ib, 권고수준A)
3. 항혈소판제제의투여로도어느정도는깊은정맥혈전증을예방하는데에효과가있으므로, 급성기
뇌경색환자에서항혈소판제제는투여되어야한다. (근거수준Ia, 권고수준A).
4. 깊은정맥혈전증의예방을위한탄력스타킹(compressive stocking)이나공기압박(pneumatic
compression machine) 단독요법의효과는뚜렷하지않으나, 과응고상태가의심되는경우또는마비
된상, 하지등에서다른치료방법의보조요법으로사용을고려할수있다. (근거수준IIb, 권고수준B)
헤파린(LMWH, low molecular weight heparin)과통상적헤파린(UFH, unfractionated heparin) 사이에효
과나부작용등의차이는없으며,4 장기간의약물투여가필요하면경구항응고제[와파린(warfarin)]의
사용이추천된다. 항응고제의사용이제한되는조건에서는아스피린(aspirin) 사용만으로도위약사용
군에비해깊은정맥혈전증의절 위험도(absolute risk reduction)를9% 감소시키는효과가있다.5일
부연구에서공기압박(pneumatic compression)이효과가있다는보고를하고있으나적은수의환자
를 상으로한연구로아직일반화하기는어렵다. 다만뇌출혈환자등항응고제혹은항혈전제를사
용하기어려울때는적극고려해볼수있다또한폐동맥혈전증환자에서항혈전제사용이금기인경
우하 정맥필터를사용해볼수있다.6,7
1. Wijdicks EF, Scott JP. Pulmonary embolism associated with acute stroke. Mayo Clin Proc. 1997;72:297-
300.
2. Desmukh M, Bisignani M, Landau P, Orchard TJ. Deep vein thrombosis in rehabilitating stroke patients.
Incidence, risk factors and prophylaxis. Am J Phys Med Rehabil.1991;70:313-316.
3. Sandercock PA, van den Belt AG, Lindley RI, Slattery J. Antithrombotic therapy in acute ischaemic stroke:
an overview of the completed randomised trials. Br Med J.1993;56:17.
4. Harvey RL, Lovell LL, Belanger N, Roth EJ. The effectiveness of anticoagulant and antiplatelet agents in
preventing venous thromboembolism during stroke rehabilitation: a historical cohort study. Arch Phys
Med Rehabil. 2004;85:1070-1075.

157
CLINICAL RESEARCH CENTER FOR STROKE
1. ASA
1) Patients who cannot take food and fluids orally should receive nasogastric, nasoduodenal, or PEG
feedings to maintain hydration and nutrition while undergoing efforts to restore swallowing (Class IIa,
Level of Evidence B). The timing of the placement of a PEG is uncertain.
2) Nutritional supplements are not needed (Class III, Level of Evidence B).
2. RCP
1) Every patient should have his/her nutritional status screened by appropriately trained personnel, using
a valid nutritional screening method, within 48 hours of admission (LOE IIa, GOR B)
2) Nutritional and hydration support should be considered in any patient with malnutrition or difficulties
feeding (LOE Ia, GOR B)
3) Enteral feeding tubes should be considered where patients are unable to maintain adequate nutrition
orally (LOE Ia, GOR A)
4) Every patient with nutritional problems, including dysphagia, who requires food of modified consistency
should be referred to a dietitian (LOE IV, GOR C)
5. Antiplatelet Trialists C. Collaborative overview of randomised trials of antiplatelet therapy-III: Reduction
in venous thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and medical
patients. Br Med J.1994;308:235-246.
6. Black PM, Crowell RM, Abbott WM. External pneumatic calf compression reduces deep venous
thrombosis in patients with ruptured intracranial aneurysms. Neurosurgery. 1986;18:25-28.
7. Kamran SI, Downey D, Ruff RL. Pneumatic sequential compression reduces the risk of deep vein
thrombosis in stroke patients. Neurology. 1998;50:1683.
급성기뇌졸중환자는삼킴장애로인해충분한경구 양공급이이루어지지못하는경우가많으며,
뇌졸중증상이심해의식이저하된경우에는흡인성폐렴의위험성때문에더욱식이섭취가제한적일
수밖에없다. 이러한 양불균형혹은 양실조는뇌졸중환자의회복에도좋지않은 향을미친다.1
2.3.2.2. 양 Nutrition

158
CLINICAL RESEARCH CENTER FOR STROKE
경구섭취장애로인해발생한탈수증및 양불균형은뇌졸중환자의회복을더디게한다.2따라서연
하곤란으로인해경구섭취가충분하지않을때는 양공급과경구약물투여의목적으로비위관
(Nasogastric tube)를삽입하기도한다.3비위관을유지하기곤란한환자나장기간의비위관삽입이필
요할것으로예상되는일부의환자에서는경피적위루술(percutaneous endoscopic gastrostomy)을시
행하기도한다.4뇌졸중환자의 양에관해현재까지이루어진 규모임상연구의결과에의하면, 연
하곤란으로인하여충분한경구섭취가어려울때, 비위관을통한 양공급이뇌졸중발생7일이내에
이루어지면, 그렇지않은환자군에비하여사망률을줄이는것으로알려져있다. 7일이내에시술되
는비위관과경피적위루술의임상효과를비교한부분에서는비위관이경피적위루술보다환자의
사망률과회복에유리한경향을보 으나통계적으로유의성은없었다.5한편뇌졸중환자의 양공
급을위한경구 양제임상시험에서경구 양제치료군이 조군에비하여사망률이나예후불량
군에서유의한차이를보이지않았다.6
3. SIGN
1) Routine use of nutritional supplements is not recommended. Early placement of a nasogastric feeding
tube should be considered in patients identified as unable to take adequate oral intake. (LOE 1++. GOR A).
1. 급성뇌졸중환자들에서연하곤란여부에 한평가와기본 양상태에 한평가가입원후가능
한한빠른시기에이루어져야한다. (근거수준IIb, 권고수준B)
2. 경구섭취가불충분한환자는비위관삽입을통해 양공급과약물투여를시행하도록하며, 연하
곤란에 한치료를지속하면서일정한간격으로연하곤란에 한재평가를통해비위관유지의
필요성을검토하도록노력한다. (근거수준IIb, 권고수준B)
3. 양실조가있는환자에서는 양균형을찾기위해노력하여야하나, 모든뇌졸중환자에서일률
적으로 양제를추가할필요는없다. (근거수준Ib, 권고수준A)
4. 장기간비위관유지가필요하거나, 기타이유로비위관을유지하기가곤란할때는경피적위루술을
고려해볼수있다. (근거수준IV, 권고수준C)
1. FOOD Trialis Collaboration, Poor nutritional status on admission predicts poor outcomes after stroke:

159
CLINICAL RESEARCH CENTER FOR STROKE
1. ASA
1) Ealy mobilization of less severely affected patients and measures to prevent subacute complications of
stroke are recommended (Class I, Level of Evidence C).
2. RCP
1) Staff should position patients to minimize the risk of complications such as pressure sores (LOE Ia,
GOR B).
3. SIGN
1) Hospital managers should ensure that nursing expertise, staffing and equipment levels are sufficient to
prevent pressure ulcers. Hospitals should have up to date policies on risk assessment, pressure ulcer
prevention and treatment. (LOE 4, GOR D).
observational data from the FOOD trial. Stroke. 2003;34:1450-1456.
2. Choi-Kwon S, Yang YH, Kim EK, Jeon MY, Kim JS. Nutritional status in acute stroke: undernutrition
versus overnutrition in different stroke subtypes. Acta Neurol Scand. 1998;98:187-192.
3. O'Mahony D, McIntyre AS. Artificial Feeding for Elderly Patients after Stroke. Age Ageing. 2006;24:533-
535.
4. James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy
feeding in patients with dysphagic stroke. Age Ageing. 1998;27:671-676.
5. Dennis MS, Lewis SC, Warlow C. Effect of timing and method of enteral tube feeding for dysphagic
stroke patients (FOOD): a multicentre randomised controlled trial. Lancet.2005;365:764-772.
6. Dennis MS, Lewis SC, Warlow C. Routine oral nutritional supplementation for stroke patients in hospital
(FOOD): a multicentre randomised controlled trial.Lancet. 2005;365:755-763.
욕창은장기간입원한환자에서경험하게되는합병증이다. 일단한번발생하면치료하기가어렵고
이로인한재원기간도길어지므로, 욕창의예방은매우중요하다.
2.3.2.3. 욕창 Pressure sore
160
CLINICAL RESEARCH CENTER FOR STROKE
일반적으로욕창은장기간침상안정을한환자에서주로발생하므로, 가능한한조기거동을하는것
이욕창의예방에도움이된다는보고가있다.1뇌졸중환자를 상으로시행된연구는아니지만, 일
반적으로전신 양상태가좋지않을때에도욕창의위험도가증가하므로, 적절한 양공급이도움
이될수있다.2,3 고위험군의환자는자주체위를변경해주면욕창의예방에도움이되며, 공기매트리
스(air mattress) 혹은공기유동형침 (air-fluidized bed)의사용도도움이된다는보고가있다.2이러한
고위험군환자에서는욕창의동반여부에 해항상주의를기울여야한다.4
4. EUSI
1) Early mobilization is helpful to prevent numerous complications after stroke, including aspiration
pneumonia, deep venous thrombosis and decubital ulcers (no evidence level)
1. 뇌졸중환자에서욕창이동반되었는지의여부는자주확인하는것이좋다. (권고사항GPP)
2. 욕창의예방에조기거동이도움이될수있다. (권고사항C, 근거사항IV)
3. 조기거동이불가능할경우, 침상에서자주체위를변경해주거나공기매트리스(air mattress) 의사
용을고려해볼수있다. (권고사항B, 근거사항IIb)
1. Langhorne P. Measures to improve recovery in the acute phase of stroke. Cerebrovasc Dis. 1999;9:2-5.
2. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: A systematic review. JAMA.2006;296:974.
3. Bourdel-Marchasson I, Barateau M, Rondeau V, Dequae-Merchadou L, Salles-Montaudon N, Emeriau
JP, Manciet G, Dartigues JF. A multi-center trial of the effects of oral nutritional supplementation in
critically ill older inpatients. Nutrition. 2000;16:1-5.
4. Berlowitz DR, Brandeis GH, Anderson JJ, Ash AS, Kader B, Morris JN, Moskowitz MA. Evaluation of a
risk-adjustment model for pressure ulcer development using the minimum data set. J Am Geriatr Soc.
2001;49:872-876.

161
CLINICAL RESEARCH CENTER FOR STROKE
1. ASA
1) Patients with suspected pneumonia or urinary tract infections should be treated with antibiotics (Class I,
Level of Evidence B).
2) Prophylactic administration of antibiotics is not recommended (Class III, Level of Evidence B).
2. RCP
1) Patients presenting with features indicating dysphagia and/or risk of pulmonary aspiration should
receive a full clinical assessment of swallowing by an appropriately trained specialist who should also
advise on safe swallow and consistency of diet and fluids (GOR A)
3. SIGN
1) A swallowing assessment should be undertaken at home or hospital as part of the clinical assessment
of stroke (Grade B, Level III).
4. EUSI
1) Aspiration pneumonia may not be prevented by nasogastric feeding (LOE IV)
흡인성폐렴은뇌졸중환자에서가장중요한염증성합병증이며, 뇌졸중환자의주요사망원인이다.1
따라서뇌졸중환자가발열이있을때흡인성폐렴의여부를가장먼저확인하여야하며, 적절한항생
제치료가필요하다. 일반적으로의식이저하되거나뇌졸중의중증도가높아신경학적손상이많은
경우, 또는기침반사가저하된환자에서흡인성폐렴이자주발생하는것으로알려져있으므로, 뇌졸
중환자에서흡인성폐렴의가능성에 한선별검사가필요하다.2,3연하곤란이있는환자는비위관을
통해음식물을섭취하게하면, 직접적인흡인의위험성은줄여줄수있으나, 비위관으로는유동식이
투여되므로, 유동식의역류에의해흡인의위험이증가할가능성이있고, 구강내타액으로인한흡인
성폐렴은방지할수없으므로비위관을사용하더라도흡인의위험성이완전히사라지지않는다.4
급성기뇌졸중으로인해발생하는연하곤란은흔히흡인성폐렴으로발전할수있다. 흡인성폐렴은
뇌졸중환자의급성기사망에있어중요한원인이다.1
2.3.2.4. 흡인성폐렴Aspiration pneumonia

162
1. 뇌졸중환자가발열이있으면흡인성폐렴의여부를먼저확인하고치료여부를결정하는것이필
요하다. (권고사항GPP)
2. 경구식이를시작하기전에연하곤란검사등의적절한선별검사를통해흡인성폐렴의위험도가
높은환자를파악하는것이필요하다. (권고사항B, 근거사항III)
3.흡인성폐렴의위험도가높다고판단되면, 경구식이보다는비위관을통한음식물을공급하는것이
권고된다. (권고사항C, 근거사항IV)
CLINICAL RESEARCH CENTER FOR STROKE
1. Nakagawa T, Sekizawa K, Arai H, Kikuchi R, Manabe K, Sasaki H. High incidence of pneumonia in elderly
patients with basal ganglia infarction. Arch Intern Med. 1997;157(3):321-324.
2. Smithard DG, O'Neill PA, Park C, et al. Can bedside assessment reliably exclude aspiration following
acute stroke? Age Ageing. 1998;27:99-106.
3. Nakajoh K, Nakagawa T, Sekizawa K, Matsui T, Arai H, Sasaki H. Relation between incidence of
pneumonia and protective reflexes in post-stroke patients with oral or tube feeding. J Intern Med
2000;247:39-42.
4. Finucane TE, Bynum JP. Use of tube feeding to prevent aspiration pneumonia. Lancet. 1996;348:1421-
1424.
비뇨기계감염은급성기뇌졸중환자에서발생하는중요한감염성합병증으로, 조기에발견하여치
료하지못하면환자의신경학적예후에좋지않은 향을미칠수있다.1
2.3.2.5. 비뇨기계감염 Urinary tract infection

163
CLINICAL RESEARCH CENTER FOR STROKE
1. ASA
1) Patients with suspected pneumonia or urinary tract infections should be treated with antibiotics (Class I,
Level of Evidence B).
2. . EUSI
1) Infections after stroke should be treated with appropriate antibiotics (no evidence level)
뇌졸중으로인한신경학적장애로인해, 배뇨장애를겪는뇌졸중환자는매우흔하다. 문헌에따르
면급성기뇌졸중환자의약절반에이르는환자가배뇨장애를겪게된다고하며,2 환자의나이가많
을수록더욱빈발하는경향이있다.3배뇨장애를조절하기위해시행되는방광내배뇨관거치술이병
원내비뇨기계감염과관련이깊은것으로알려져있다.4뇌졸중환자를 상으로시행된연구는아
니지만, 방광내배뇨관을거치해두면세균뇨와방광감염이증가한다고알려져있다.5,6 도관을계속
삽입해두지않고, 필요할때마다간헐적인도관삽입을하면비뇨기계감염을줄일가능성이있으나
확실한근거는없다. 일단비뇨기계감염이확인되면, 원인균을규명하고적절한항생제치료가이루
어져야하나, 예방적항생제요법이비뇨기계감염을방지할수있다는근거는없다.
1. 비뇨기계감염이확인되면적절한항생제치료가필요하다. (권고사항GPP)
2. 비뇨기계감염을방지하기위한목적의예방적항생제요법은추천되지않는다. (권고사항GPP)
3. 방광내배뇨관거치술은꼭필요한경우에가능한짧은기간동안만시행하는것을추천한다. (권고
사항C, 근거사항IV)
1. Meijer R, Ihnenfeldt DS, de Groot I, van Limbeek J, Vermeulen M, de Haan R. Prognostic factors for
ambulation and activities of daily living in the subacute phase after stroke. A systematic review of the literature.
Clin Rehabil. 2003;17:119-129.
2. Thomas LH, Barrett J, Cross S, French B, Leathley M, Legg L, Sutton C, Watkins C. Prevention and treatment
of urinary incontinence after stroke in adults. Cochrane Database Syst Rev.2005:CD004462

164
3. J�rgensen L, Engstad T, Jacobsen BK. Self-reported urinary incontinence in noninstitutionalized long-term
stroke survivors: A population-based study. Arch Phys Med Rehab. 2005;86:416-420.
4. Gerberding JL. Hospital-onset infections: A patient safety issue. Ann Intern Med. 2002;137:665.
5.Sabanathan K, Castleden CM, Mitchell CJ. The problem of bacteriuria with indwelling urethral catheterization.
Age Ageing. 1985;14:85-90.
6. Warren JW, Tenney JH, Hoopes JM, Muncie HL, Anthony WC. A prospective microbiologic study of bacteriuria
in patients with chronic indwelling urethral catheters. J Infect Dis. 1982;146:719-723.
CLINICAL RESEARCH CENTER FOR STROKE
뇌경색은혈전이나색전등으로뇌혈관이막혀시간이경과하면서뇌세포가허혈손상을받아발생
하므로, 이러한기전이진행하기전에신속히혈전을용해시켜혈류를재개통시키는치료가혈전용
해술이다. Tissue plasminogen activator(tPA)를사용한정맥내(intravenous, 이하 IV) 혈전용해술은1995
년National Institute of Neurological Disorders and Stroke(NINDS) 연구에의해뇌졸중증상발생3시간
이내에투여하면허혈성뇌졸중환자의예후를개선시킬수있다는것이입증된이후뇌졸중급성기
에공인된유일한치료제로서사용되어왔다.1그러나3시간이라는제한시간이너무짧아이러한상
황을개선시키기위해투여제한시간을연장하려는지속적인노력들이있어왔으며,2,3발생3시간이
후에도 tPA를투여하 던기존연구들의자료들을 상으로메타분석한결과 IV tPA의효과는투여
시간이빠를수록좋고시간이경과함에따라감소하나, 3시간이후약4.5 시간까지도효과가있을것
으로예상되었다.4결국이를입증하기위해ECASS-3 연구가진행되어예견된 로 4.5시간까지는
tPA를투여하여도효과가있다는것을입증하 다.5따라서혈전용해술진료지침에서초급성허혈성
뇌졸중의 IV tPA 투여적응증을3시간에서4.5시간까지로연장하는개정이필요하 다. 그러나tPA 투
여가빠를수록그효과는더크기때문에치료시간이연장되었다하더라도가능한신속히치료를시
작하도록노력하여야하고, 또한3시간이후의투여기준은기존3시간이내의투여기준과몇가지차
이점이있어이를숙지할필요가있다.
2.3.3. 혈전용해술Thrombolysis
2.3.3.1. 정맥내혈전용해술 Intravenous Thrombolysis
개정: 2012.12

165
CLINICAL RESEARCH CENTER FOR STROKE
2009 AHA/ASA Science Advisory 6
1. rtPA should be administered to eligible patients who can be treated in the time period of 3 to 4.5 hours
after stroke (Class I Recommendation, Level of Evidence B). The eligibility criteria for treatment in this
time period are similar to those for persons treated at earlier time periods, with any one of the following
additional exclusion criteria: Patients older than 80 years, those taking oral anticoagulants with an
international normalized ratio ≤1.7, those with a baseline National Institutes of Health Stroke Scale
score �25, or those with both a history of stroke and diabetes. Therefore, for the 3-to-4.5-hour window,
all patients receiving an oral anticoagulant are excluded regardless of their international normalized
ratio. The relative utility of rtPA in this time window compared with other methods of thrombus
dissolution or removal has not been established.
2. The efficacy of intravenous treatment with rtPA within 3 to 4.5 hours after stroke in patients with these
exclusion criteria is not well established (Class IIb Recommendation, Level of Evidence C) and requires
further study.
1. 증상발생3시간이내에내원한허혈성뇌졸중환자의경우, 재조합조직플라스미노겐활성제
(tPA) 치료를고려하여야한다. (근거수준Ia, 권고수준A)
2. 단, 상검사에서뇌출혈이배제되어야하며, 다음적응증을기준으로한다(표1).
3. 재조합조직플라스미노겐활성제치료는치료하지않은군에비하여유의한뇌출혈의증가를
일으키므로그위험성에 하여숙지하고있어야한다. (근거수준Ia, 권고수준A)
4. 정맥내스트렙토키나아제(streptokinase)는출혈의위험이유의하게높으므로사용하지말아야
한다. (근거수준Ia, 권고수준A)
5. 재조합조직플라스미노겐활성제이외의정맥내혈전용해제(유로키나아제[urokinase], 테넥테플
레이즈[tenecteplase], 데스모테플레이즈[desmoteplase])의효과는아직입증되지않았다.
(근거수준IV, 권고수준C)
6. 정맥내재조합조직플라스미노겐활성제치료는적응증과금기증을확인한후가능한빨리시작
되어야한다. (근거수준Ia, 권고수준A)

166
2009 European Stroke Organization Guidelines7
1. Intravenous rtPA (0.9 mg/kg body weight, maximum 90 mg), with 10% of the dose given as a bolus
followed by a 60-minute infusion, is recommended within 4.5 hours of onset of ischaemic stroke (Class I,
Level A), although treatment between 3 and 4.5 h is currently not included in the European labelling
(modified January 2009).
2012 9th American College of Chest Physicians Guidelines8
2.1 IV Recombinant Tissue Plasminogen Activator (r-tPA) for Patients With Acute Ischemic Stroke
2.1.1. In patients with acute ischemic stroke in whom treatment can be initiated within 3 h of symptom
onset, we recommend IV r-tPA over no IV r-tPA (Grade 1A).
2.1.2. In patients with acute ischemic stroke in whom treatment can be initiated within 4.5 but not within 3
h of symptom onset, we suggest IV r-tPA over no IV r-tPA (Grade 2C).
2.1.3. In patients with acute ischemic stroke in whom treatment cannot be initiated within 4.5 h of
symptom onset, we recommend against IV r-tPA (Grade 1B).
CLINICAL RESEARCH CENTER FOR STROKE
1. 기존의근거
1995년발표된NINDS tPA 연구는624 명의급성뇌경색환자들을 상으로 tPA 또는위약치료를3시
간이내에시행하여그효과및안전성에관한결과를발표하 다. Part 1과Part 2로구성되었는데,
Part 2에서 tPA군이 조군에비하여양호한임상경과(mRS≤1)를보일확률이최소30% 이상높았
다.1 주된합병증인뇌출혈의위험은 tPA군이 조군에비하여약10배정도높은것으로나타났으며
(6.4% vs. 0.6%, p�0.01), 치료전CT 에서심한뇌부종이나종괴효과(mass effect)가있는경우증후성
출혈성변화가발생할가능성이높았다.9뇌출혈이외의드문부작용들로써, 전신출혈, 심근파열, 혈
관성부종등이보고되었다.10,11
정맥내혈전용해술의또다른 규모임상연구로는ECASS,12 ECASS II13가있으며, 이두연구는tPA 효
과를증명하지못했는데이는용량 (1.1mg/kg) 과주입시간(발생후6시간이내)이NINDS tPA 연구와
달랐기때문으로생각된다. 그러나사후분석(post hoc analysis)에서 3시간이내치료한환자들에서
tPA의효과는입증되었다.14 이후지역기반4상연구인CASES15, STARS16, SITS-MOST17등에서도역시3
시간이내 tPA 투여의효과와안전성이입증되었으며, 오히려출혈의위험이기존3상연구결과에비

167
CLINICAL RESEARCH CENTER FOR STROKE
하여낮은것으로보고되었다.
치료시간을연장하여3시간에서5시간까지 tPA 치료를시도한연구에서는90일째임상호전이양그
룹에서차이를보이지않았으며 tPA 치료군에서증후성뇌출혈이유의하게많았다(7% vs 1%).18따라
서3시간이후의치료효과에관한연구에서는 tPA 효과가입증되지못했다. 그러나여섯개의무작위
임상연구를분석한병합분석(pooled analysis)에서는181분에서270분이내치료한군에서양호한임
상경과에 한 응비(odds ratio)가1.4(95% CI, 1.1~1.9)로3시간이후로치료가능시간이연장될수있
는가능성을보여주었다.4또한빠른치료시간의중요성이하위집단분석(subgroup analysis) 에서보고
되었는데, 90분이내치료한군은3개월째양호한임상경과를보일 응비가2.11(95% CI, 1.33 - 3.55)
이었고, 90분에서180분사이에치료한군은1.69(95% CI, 1.09-2.62)로, 치료를빨리시작할수록예후가
더좋았다.4,19
유럽에서는여전히 tPA의위험-효용비(risk benefit ratio)를의심하고있으며임상시험의환자수가효
과를입증하기에는부족하다고염려하고있다. 그러나, 최근유럽여러국가들에서시행된4상임상
연구들을통하여 tPA 정맥내투여가기본적인치료로안전하고효과적임이밝혀지면서,17 최근혈전
용해술을권장하고있다.
스트렙토키나아제(Streptokinase)는출혈이유의하게증가하여연구가중단되었다.20-23유로키나아
제(Urokinase) 정맥주사치료는체계적연구가된바가없다. 테넥테플레이즈(Tenecteplase)는뇌경
색을 상으로예비연구가진행중이다.24데스모테플레이즈(Desmoteplase)는MRI를기준으로환
자선택기준을사용한예비연구가성공하여, 3상연구가진행되었으나그효과를증명하는데실
패하 다.25,26
이처럼현재까지근거가확립된정맥내혈전용해술을바탕으로하여, 혈전이존재하는병변부위
의 혈관으로 직접 혈전용해제를 추가로 투여하는 방법들이 연구되고 있다. 최근에 시행된
Emergency Management of Stroke (EMS) trial(무작위배정 1상임상연구)27에서증상발생 3시간이
내에정맥내/동맥내복합혈전용해술과동맥내혈전용해술만시행한군을비교한결과, 3개월째
임상적예후는동일하 으나정맥내/동맥내복합혈전용해술에서보다나은혈관재개통율
(recanalization rate)을보 다. 그효과와관련하여비맹검단일집단예비연구(open-labeled single-
arm pilot study)인 Interventional management of stroke (IMS) trial이수행되었고, 정맥내/동맥내복
합혈전용해술이 NINDS tPA 연구의 조군에비하여나은임상경과(3개월째사망률: IMS 16%,
NINDS 연구 tPA군21%, NINDS 연구 조군24%)를보여주는등활발히연구가진행되고있다.28

168
CLINICAL RESEARCH CENTER FOR STROKE
European Cooperative Acute Stroke Study-3 (ECASS-3)
위에서배경설명한바와같이증상발생3시간에서4.5 시간까지 IV tPA 투여효과를입증하기위해
시행된연구가ECASS-3 이다.5이연구는다기관, 전향적, 무작위배정, 위약 조군연구로, 증상발
생 3시간에서 4.5시간내의환자들을 상으로 tPA 치료군(418명)과 조군(403명)을비교하 다.
환자선정에있어기존3시간이내 tPA 치료제외기준이외에80세초과환자, NIHSS 점수25점초과,
항응고제복용중, 뇌졸중병력과당뇨병의동반을제외기준에추가하 다. 그결과일차유효성결
과변수(primary efficacy outcome)인 3개월modified Rankin Score (mRS) 점수 0-1점의분율이 tPA 치
료군(52.4%)에서 조군(45.2%)에비해유의하게증가하 다 (OR 1.34, 95% CI 1.02~1.76, P=0.04).
ECASS-3 정의에따른증후성뇌출혈발생은 tPA 투여군10명 (2.4%), 조군1명으로 (0.2%) tPA 치료
군에서유의하게증가하 지만 (OR 9.85, 95% CI 1.26~77.32, P=0.008) 이로인해사망률이더증가하
지는않았다 (치료군 7.7% vs 조군 8.4%; P=0.68). ECASS-3 임상시험은메타분석에서관찰되었던
3~4.5 시간 의 tPA 효과를실제임상시험을통하여입증한중요한연구이다. 다만위의제외기준에
해당되는환자군의3~4.5 시간 IV tPA 효과에 해서는근거를확보할수없어향후추가연구의필
요성이제시되었다.
Safe Implementation of Thrombolysis in Stroke-International Stroke Treatment Registry (SITS-ISTR) 3-to-
4.5 hour study
같은해발표된SITS-ISTR 3-to-4.5 hour 연구는유럽에서진행하고있는뇌졸중등록연구에서2002년
12월부터2007년11월까지의자료를분석한것으로, 증상발생3시간이내에tPA를투여받은11865명
의환자군과3시간에서4.5시간사이에투여받은664명의환자군을비교한관찰연구이다.29사망, 증
후성뇌출혈, 그리고3개월mRS 0-2점비율에있어3시간이내치료를받은군과3-4.5시간 에치료
를받은군사이에유의한차이가없어3~4.5시간 IV tPA 치료효과의또하나의근거로제시된다. 이
연구에서는3시간이후치료받은환자들의72%에서3시간에서3.5시간사이에 tPA가투여되었다는
점을유의할필요가있다.
International Stroke Trial-3 (IST-3)
가장최근에발표된 IST-3는81세이상의환자들까지포함하고 tPA 투여시간기준을6시간까지늘려
서진행한무작위배정 조군연구로, 3035명의환자들이 (tPA 군1515명, 조군1520명) 참여하 으
며, 이중 1617명이 (53%) 81세이상이었다.30이연구에서는일차결과변수를mRS 척도의변형인
169
CLINICAL RESEARCH CENTER FOR STROKE
Oxford Handicap Score (OHS)으로 6개월째에평가하 다. 일차분석은독립적일상생활이가능한정
도로회복된경우(OHS 0~2)의분율을비교하 는데 tPA군554명(37%), 조군534명(35%, adjusted OR
1.13 95% CI 0.95~1.35, p=0.181)으로차이가없었다. 그러나미리예정하 던이차분석방법인순위척
도분석(ordinal analysis)에서는 조군에비해 tPA 치료군에서OHS 장애가한단계개선될확률(shift)
이유의하게증가하 다 (OR 1.27, 95% CI 1.10~1.47, p=0.001). 안전성측면에서1주이내의증상성두개
내출혈은 tPA군104명(7%), 조군16명(1%), 1주이내의사망은 tPA군163명(11%), 조군107명(7%)
으로 tPA 군이 조군보다위험하 다. 그러나 1주이후부터는 조군에서 tPA군에비해사망이더
증가하여6개월사망률은두군간에차이가없었다. IST-3 결과를포함한메타분석결과에서는81세
이상의환자들에서도80세이하환자들과마찬가지로 tPA의효과가입증되어결론적으로 IST-3 연구
는 tPA의적용 상환자의연령을 81세이상으로연장할근거를제시하 다고할수있다.31그러나
시간기준을6시간까지로연장할가능성에 해서는, 일차분석방법으로정했던OHS 0-2 분율을유
의하게증가시키지못하 기때문에새로운근거로인정받기에는미흡하다고평가된다.
기타정맥내혈전용해술연구들및전망
앞으로도더많은허혈성뇌졸중환자에게현재로서유일하게공인된치료제인 IV tPA의효과를볼수
있도록하기위해효과적인뇌졸중진료체계구축(organization of stroke care)과함께 IV tPA 적응증을
확 하려는노력또한병행될것이다. 최근에는 IV tPA 의금기증각각이그과학적근거가불충분함
에도불구하고너무종류가많아실제tPA가투여되는환자가너무적어지는결과를초래한다는인식
이확산되고있어이를현실적으로재조정하자는SMART thrombolysis 연구가제시되었다.32제외기
준을 폭완화하는이모형에따르면현재5% 전후에불과한전체급성뇌졸중환자의 IV tPA의투여
율을약20% 가까이높일수있을것으로예측되었다. 또한 IV tPA 투여의제외기준중하나인“minor
stroke”에 한정의에 해서도논란들이있다. 이는임상에서 tPA 치료를배제하는가장흔한이유
인데, minor stroke 으로판단하고 tPA를투여받지않은환자의약25%에서나쁜예후를보이는것으
로보고되어, 소극적인 IV tPA 사용의 표적사례로지적되고있다.33,34미국뇌졸중관련학술-산업원
탁회의인Stroke Treatment Academic Industry Roundtable (STAIR) 에서도정맥내혈전용해술의활성화
를위해서는금기증중일부를절 적이아닌상 적기준으로인식하여야한다는입장을포함한
STAIR VII 권고안을발표하 다.35
정맥내혈전용해술의적응증을시간으로만규정하기보다조직의상태를감안한“mismatch based”
정맥내혈전용해술을적용하려는연구도계속진행되어왔다. 2010년기존의정맥내혈전용해술연

170
CLINICAL RESEARCH CENTER FOR STROKE
구들을메타분석한결과가발표되었는데, 아직임상적으로적용하기에는근거가부족하다는결론
이었다.36최근에는 diffusion-perfusion mismatch 외에도 clinical-diffusion mismatch, diffusion-MRA
mismatch 등다양한mismatch의정의가사용되고있으며, Fluid Attenuated Inversion Recovery(FLAIR)-
diffusion mismatch 는발생시간이불분명한경우에적용가능성이연구되고있다.37,38
한편으로는 tPA 외의약제를사용한정맥내혈전용해술연구도지속적으로진행되고있는데,
desmoteplase를사용한Desmoteplase in Acute Ischemic Stroke(DIAS)-3,4 연구가계속진행중이며조
만간환자모집이끝날전망이다. 최근에는 tPA 일부를유전자변형시켜약리학적특성을향상시킨
tenecteplase가발생6시간이내의허혈성뇌졸중에서정맥투여시 tPA 보다재관류및임상효과에서
우월하다는연구가발표되어주목을받고있다.39그러나CT 관류 상병변이CT 뇌경색보다20%이
상크고, CT angiography 에서동맥폐색이확인된75명의환자들만을 상으로한IIb 연구이므로새로
운근거로인정하기에는미흡하며관련후속연구를지켜볼필요가있다.
정맥내혈전용해술에서인종에따른 tPA 최적용량에 해서는아직논란이있다.40일본에서는자국
의관찰연구를근거로0.6mg/kg 를사용하고있으나0.9mg/kg 용량과비교한3상연구는아직없어
동양인에서 tPA 사용후출혈이더많다는뚜렷한근거는없다. 또한최근에한국, 중국, 인도, 싱가폴
에서함께진행한SITS-NEW registry 연구결과는유럽의SITS-MOST registry 결과와비교하여출혈등
안전성에서유의한차이가없었으며오히려3개월째독립생활을보이는확률이더높아서이러한우
려와상반되는결과를나타내었다.41현재호주와아시아국가들에서 IV tPA 용량 0.6 mg/kg 과 0.9
mg/kg 을직접비교하는 ENhanced Control of Hypertension ANd Thrombolysis strokE study
(ENCHANTED) 연구가계획되고있어그결과가주목된다.
1. 허혈성뇌졸중환자에서증상발생(최종적으로정상이었던시간기준) 3시간이내에투여가가능
한경우, IV tPA 치료를한다. (근거수준Ia, 권고수준A) 단, 상검사에서뇌출혈이배제되어야하며,
그외적응증은표2. 에따른다. - 문구개정
2. 위의치료는81세이상의환자에서도적용가능하다. (근거수준Ib, 권고수준A) - 추가
3. 허혈성뇌졸중환자에서증상발생(최종적으로정상이었던시간기준) 3~4.5 시간사이에투여가
가능한경우IV tPA 투여를할수있다. (근거수준Ia, 권고수준A) - 추가

171
CLINICAL RESEARCH CENTER FOR STROKE
* 단, 80세이상, 심한신경학적장애(NIHSS점수25점초과), 과거뇌졸중과당뇨병의병력이함께있는
환자, 경구항응고제를복용하고있는환자에서는3~4.5 시간투여할근거가부족하다.
4. IV tPA 치료는치료하지않은군에비하여유의하게높은뇌출혈의위험이있으므로그위험성에
하여숙지하고있어야한다. (근거수준Ia, 권고수준A)
5. 정맥내스트렙토키나아제(streptokinase)는출혈의위험이유의하게높으므로사용하지말아야
한다. (근거수준Ia, 권고수준A)
6. 허혈성뇌졸중에서tPA 이외의정맥내혈전용해제(urokinase, tenecteplase, desmoteplase)의효과는
아직입증되지않았다. (근거수준IV, 권고수준C)
7. IV tPA 치료는조기에투여될수록환자의예후가좋아지므로, 적응증과금기증을확인한후가능한
신속히시작하도록한다. (근거수준Ia, 권고수준A)
8. IV tPA 투여방법은표2. 에따른다. (근거수준Ia, 권고수준A) - 추가
1. 신경학적장애가동반되고경미하지않은허혈성뇌졸중
2. 신경학적장애가자발적으로신속히호전되지않아야함
3. 신경학적장애가심한환자는치료시주의해야함
4. 거미막하출혈(subarachnoid hemorrhage)으로인한증상이아니어야함
5. 최근3개월이내에두부외상 (head trauma) 및뇌졸중이없어야함
6. 최근3개월이내에심근경색이없어야함
7. 최근21일이내에소화기및비뇨기계출혈이없어야함
8. 최근14일이내에주요수술(major surgery)을시행하지않았어야함
9. 최근7일이내압박불가능한동맥천자(arterial puncture)를시행하지않았어야함
10. 두개내출혈(intracranial hemorrhage)의과거력이없어야함
11. 혈압은수축기혈압185mmHg 및확장기혈압110mmHg 이내로조절되어야함
12. 신체검진당시, 출혈및외상(골절포함)이발견되지않아야함
13. 경구항응고제를복용하고있다면 INR 1.7 이하여야함
14. 과거48시간이내헤파린을투여받았다면, aPTT가정상범위이내로조절되어야함
15. 혈소판수치는100,000mm3이상이어야함
16. 혈당수치는50mg/dL (2.7 mmol/L) 이상이어야함
17. 경련(seizure) 후발생한신경학적장애가아니어야함
18. CT에서저음 병변이뇌반구의1/3 이상인다엽경색(multilobar infarction)이아니어야함
19. 환자또는보호자가치료에따르는위험과이득에 해이해하고있어야함
표 1. 정맥내혈전용해술적응증
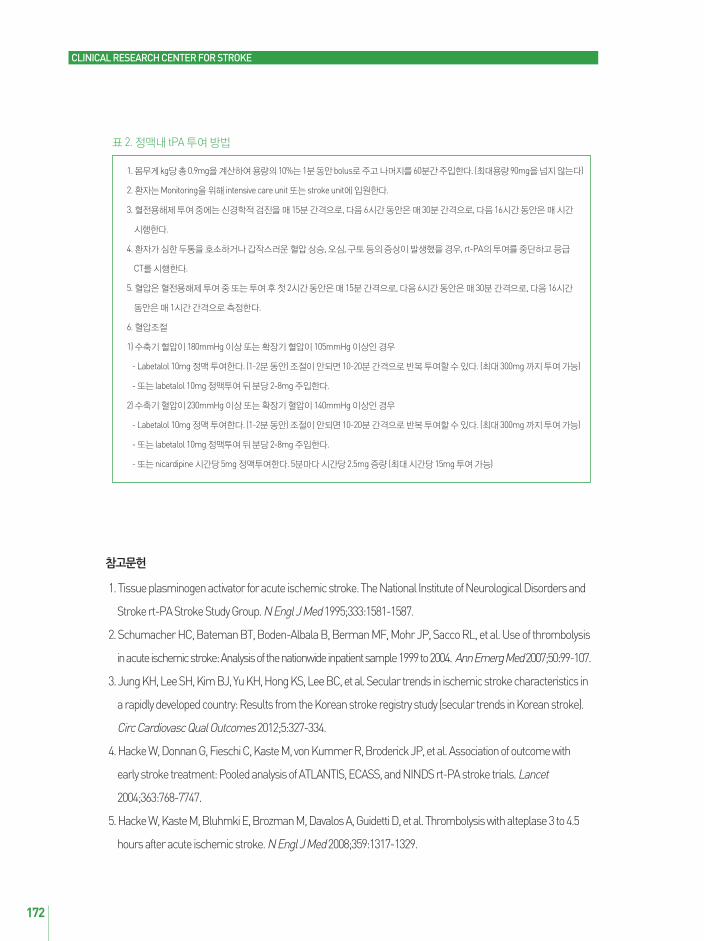
172
CLINICAL RESEARCH CENTER FOR STROKE
1. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and
Stroke rt-PA Stroke Study Group. N Engl J Med1995;333:1581-1587.
2. Schumacher HC, Bateman BT, Boden-Albala B, Berman MF, Mohr JP, Sacco RL, et al. Use of thrombolysis
in acute ischemic stroke: Analysis of the nationwide inpatient sample 1999 to 2004. Ann Emerg Med 2007;50:99-107.
3. Jung KH, Lee SH, Kim BJ, Yu KH, Hong KS, Lee BC, et al. Secular trends in ischemic stroke characteristics in
a rapidly developed country: Results from the Korean stroke registry study (secular trends in Korean stroke).
Circ Cardiovasc Qual Outcomes2012;5:327-334.
4. Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP, et al. Association of outcome with
early stroke treatment: Pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet
2004;363:768-7747.
5. Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5
hours after acute ischemic stroke. N Engl J Med 2008;359:1317-1329.
1. 몸무게kg당총0.9mg을계산하여용량의10%는1분동안bolus로주고나머지를60분간주입한다. (최 용량90mg을넘지않는다)
2. 환자는Monitoring을위해 intensive care unit 또는stroke unit에입원한다.
3. 혈전용해제투여중에는신경학적검진을매15분간격으로, 다음6시간동안은매30분간격으로, 다음16시간동안은매시간
시행한다.
4. 환자가심한두통을호소하거나갑작스러운혈압상승, 오심, 구토등의증상이발생했을경우, rt-PA의투여를중단하고응급
CT를시행한다.
5. 혈압은혈전용해제투여중또는투여후첫2시간동안은매15분간격으로, 다음6시간동안은매30분간격으로, 다음16시간
동안은매1시간간격으로측정한다.
6. 혈압조절
1) 수축기혈압이180mmHg 이상또는확장기혈압이105mmHg 이상인경우
- Labetalol 10mg 정맥투여한다. (1-2분동안) 조절이안되면10-20분간격으로반복투여할수있다. (최 300mg 까지투여가능)
- 또는 labetalol 10mg 정맥투여뒤분당2-8mg 주입한다.
2) 수축기혈압이230mmHg 이상또는확장기혈압이140mmHg 이상인경우
- Labetalol 10mg 정맥투여한다. (1-2분동안) 조절이안되면10-20분간격으로반복투여할수있다. (최 300mg 까지투여가능)
- 또는 labetalol 10mg 정맥투여뒤분당2-8mg 주입한다.
- 또는nicardipine 시간당5mg 정맥투여한다. 5분마다시간당2.5mg 증량 (최 시간당15mg 투여가능)
표 2. 정맥내 tPA 투여방법

173
CLINICAL RESEARCH CENTER FOR STROKE
6. Del Zoppo GJ, Saver JL, Jauch EC, Adams HP, Jr. Expansion of the time window for treatment of acute
ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart
Association/American Stroke Association.Stroke 2009;40:2945-2948.
7. Guidelines for management of ischaemic stroke and transient ischaemic attack. [database on the Internet]
http://www.eso-stroke.org/pdf/ESO%20Guidelines_update_Jan_2009.pdf.
8. Lansberg MG, O'Donnell MJ, Khatri P, Lang ES, Nguyen-Huynh MN, Schwartz NE, et al. Antithrombotic and
thrombolytic therapy for ischemic stroke: Antithrombotic therapy and prevention of thrombosis, 9th ed:
American college of chest physicians evidence-based clinical practice guidelines. Chest2012;141:e601S-636S.
9. The NINDS t-PA Stroke Study Group. Intracerebral hemorrhage after intravenous t-PA therapy for ischemic
stroke. Stroke. 1997;28:2109-2118.
10. Lyden P. Thrombolytic Therapy for Acute Stroke. 2nd ed, Totowa, NJ: Humana Press, 2005.
11. Engelter ST, Fluri F, Buitrago-Tellez C, Marsch S, Steck AJ, Ruegg S, Lyrer PA. Life-threatening orolingual
angioedema during thrombolysis in acute ischemic stroke. J Neurol. 2005;252:1167-1170.
12. Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, Boysen G, Bluhmki E, Hoxter G, Mahagne
MH, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric
stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA. 1995;274:1017-1025.
13. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, Larrue V, Bluhmki E, Davis S, Donnan G,
Schneider D, Diez-Tejedor E, Trouillas P. Randomised double-blind placebo-controlled trial of thrombolytic
therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian
Acute Stroke Study Investigators. Lancet. 1998;352:1245-1251.
14. Steiner T, Bluhmki E, Kaste M, Toni D, Trouillas P, von Kummer R, Hacke W. The ECASS 3-hour cohort.
Secondary analysis of ECASS data by time stratification. ECASS Study Group. European Cooperative Acute
Stroke Study. Cerebrovasc Dis. 1998;8:198-203.
15. Hill MD, Buchan AM. Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke
Effectiveness Study. CMAJ. 2005;172:1307-1312.
16. Albers GW, Bates VE, Clark WM, Bell R, Verro P, Hamilton SA. Intravenous tissue-type plasminogen
activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS)
study. JAMA. 2000;283:1145-1150.
17. Wahlgren N, Ahmed N, Davalos A, Ford GA, Grond M, Hacke W, Hennerici MG, Kaste M, Kuelkens S, Larrue
V, Lees KR, Roine RO, Soinne L, Toni D, Vanhooren G. Thrombolysis with alteplase for acute ischaemic stroke
in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study.

174
CLINICAL RESEARCH CENTER FOR STROKE
Lancet. 2007;369:275-282.
18. Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type
plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study:
a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic
Stroke. JAMA. 1999;282:2019-2026.
19. Marler JR, Tilley BC, Lu M, Brott TG, Lyden PC, Grotta JC, Broderick JP, Levine SR, Frankel MP, Horowitz SH,
Haley EC, Jr., Lewandowski CA, Kwiatkowski TP. Early stroke treatment associated with better outcome: the
NINDS rt-PA stroke study. Neurology. 2000;55:1649-1655.
20. Donnan GA, Hommel M, Davis SM, McNeil JJ. Streptokinase in acute ischaemic stroke. Steering
Committees of the ASK and MAST-E trials. Australian Streptokinase Trial. Lancet. 1995;346:56.
21. Hommel M, Boissel JP, Cornu C, Boutitie F, Lees KR, Besson G, Leys D, Amarenco P, Bogaert M.
Termination of trial of streptokinase in severe acute ischaemic stroke. MAST Study Group. Lancet.
1995;345:57.
22. Thrombolytic therapy with streptokinase in acute ischemic stroke. The Multicenter Acute Stroke Trial -
Europe Study Group. N Engl J Med. 1996;335:145-150.
23. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute
ischaemic stroke. Multicentre Acute Stroke Trial--Italy (MAST-I) Group. Lancet. 1995;346:1509-1514.
24. Haley EC, Jr., Lyden PD, Johnston KC, Hemmen TM. A pilot dose-escalation safety study of tenecteplase in
acute ischemic stroke. Stroke. 2005;36:607-612.
25. Furlan AJ, Eyding D, Albers GW, Al-Rawi Y, Lees KR, Rowley HA, Sachara C, Soehngen M, Warach S, Hacke
W. Dose Escalation of Desmoteplase for Acute Ischemic Stroke (DEDAS): evidence of safety and efficacy 3 to 9
hours after stroke onset. Stroke. 2006;37:1227-1231.
26. Hacke W. FA, for the DIAS-2 Investigators. Results from the phase III study of desmoteplase in acute
ischemic stroke trial, 2 (DIAS 2). Cerebrovasc Dis. 2007;23 (Suppl 2):54.
27. Lewandowski CA, Frankel M, Tomsick TA, Broderick J, Frey J, Clark W, Starkman S, Grotta J, Spilker J,
Khoury J. Combined intravenous and intra-arterial r-tPA versus intra-arterial therapy of acute ischemic
stroke: Emergency Management of Stroke (EMS) Bridging Trial. Stroke. 1999;30:2598-2605.
28. Combined intravenous and intra-arterial recanalization for acute ischemic stroke: The interventional
management of stroke study. Stroke. 2004;35:904-911.
29. Wahlgren N, Ahmed N, Davalos A, Hacke W, Millan M, Muir K, et al. Thrombolysis with alteplase 3-4.5 h after
acute ischaemic stroke (SITS-ISTR): an observational study. Lancet 2008;372:1303-1309.

175
CLINICAL RESEARCH CENTER FOR STROKE
30. Sandercock P, Wardlaw JM, Lindley RI, Dennis M, Cohen G, Murray G, et al. The benefits and harms of
intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke
(the third international stroke trial [IST-3]): A randomised controlled trial. Lancet2012;379:2352-2363.
31. Wardlaw JM, Murray V, Berge E, del Zoppo G, Sandercock P, Lindley RL, et al. Recombinant tissue
plasminogen activator for acute ischaemic stroke: An updated systematic review and meta-analysis. Lancet
2012;379:2364-2372.
32. Tong D. Are all iv thrombolysis exclusion criteria necessary? Being smart about evidence-based medicine.
Neurology 2011;76:1780-1781.
33. Balucani C, Levine SR. Mild stroke and rapidly improving symptoms: It's not always a happy ending. Stroke
2011;42:3005-3007.
34. Smith EE, Fonarow GC, Reeves MJ, Cox M, Olson DM, Hernandez AF, et al. Outcomes in mild or rapidly
improving stroke not treated with intravenous recombinant tissue-type plasminogen activator: Findings from
get with the guidelines-stroke. Stroke2011;42:3110-3115.
35. Albers GW, Goldstein LB, Hess DC, Wechsler LR, Furie KL, Gorelick PB, et al. Stroke treatment academic
industry roundtable (STAIR) recommendations for maximizing the use of intravenous thrombolytics and
expanding treatment options with intra-arterial and neuroprotective therapies. Stroke2011;42:2645-2650.
36. Mishra NK, Albers GW, Davis SM, Donnan GA, Furlan AJ, Hacke W, et al. Mismatch-based delayed
thrombolysis: A meta-analysis. Stroke2010;41:e25-33.
37. Thomalla G, Cheng B, Ebinger M, Hao Q, Tourdias T, Wu O, et al. DWI-FLAIR mismatch for the identification
of patients with acute ischaemic stroke within 4.5 h of symptom onset (pre-FLAIR): A multicentre
observational study. Lancet Neurol2011;10:978-986.
38. Huisa BN, Liebeskind DS, Raman R, Hao Q, Meyer BC, Meyer DM, et al. Diffusion-weighted imaging-fluid
attenuated inversion recovery mismatch in nocturnal stroke patients with unknown time of onset. J Stroke
CerebrovascDis 2012;1-6.
39. Parsons M, Spratt N, Bivard A, Campbell B, Chung K, Miteff F, et al. A randomized trial of tenecteplase versus
alteplase for acute ischemic stroke. N Engl J Med2012;366:1099-1107.
40. Sharma VK, Ng KW, Venketasubramanian N, Saqqur M, Teoh HL, Kaul S, et al. Current status of intravenous
thrombolysis for acute ischemic stroke in Asia. Int J Stroke2011;6:523-530.
41. Rha JH, Shrivastava VP, Wang Y, Lee KE, Ahmed N, Bluhmki E, et al. Thrombolysis for acute ischaemic
stroke with alteplase in an Asian population: Results of the multicenter, multinational safe implementation of
thrombolysis in stroke-non-European union world (SITS-NEW). Int J Stroke2012.

176
CLINICAL RESEARCH CENTER FOR STROKE
1. 동맥내혈전용해술은6시간이내에발생한중 뇌동맥이나내경동맥폐색환자중정맥내혈전용
해술치료의적응증이되지않는환자(권고수준A, 근거수준Ib), 혹은최근의수술등으로정맥내혈
전용해술이금기인환자(권고수준B, 근거수준III)를 상으로고려할수있다.
2. 동맥내혈전용해술을시행하는기관은뇌혈관조 장비가즉각적으로사용가능해야하며훈련
받은중재시술전문가가있어야한다. 각기관은기관내에동맥내혈전용해술을시행하는의사의
판단기준을마련하도록노력해야한다. (권고수준B, 근거수준III)
3. 뇌바닥동맥(basilar artery) 폐색과같은후방순환계뇌졸중환자에서동맥내혈전용해술을기관내
기준에따라치료방법으로사용할수있다. (권고수준C, 근거수준IV)
동맥내(Intra-Arterial, 이하 IA) 혈전용해술은동맥이막힌부위에직접카테터를통하여혈전용해제를
투여하거나물리적으로혈전을제거하여혈류를재개통시키는방법으로, 준비된시설이필요하고
더오랜시간이걸린다는단점이있으나, 높은재개통성공률을보이고, 기계적 (mechanical) 혈전용해
술의경우혈전용해제를투여하지않을수있어출혈위험을낮출수있는등의장점들이있어정맥내
혈전용해술이실패하거나또는적응증이되지않는경우적용할수있는치료법이다. 동맥내혈전용
해술은그특성상 규모임상연구가어려워다른치료법에비해상 적으로근거가충분하지못하
으나, 그동안축적된많은연구를바탕으로최근에메타연구가발표되었고1현재는상당한근거가
있는치료법으로인정되고있어진료지침에이를새로이반 할필요성이있다. 또한기계적혈전용
해술방법으로MERCI device, Penumbra system, EKOS microcatheter 등다양한기구들이그간사용되
어왔으나최근에는Solitaire, TREVO 같이스텐트를응용하여혈전을꺼내는방법들이MERCI 같은기
존방법보다더좋은결과를보여주고있어, 향후이러한stent retriever 계열이동맥내혈전용해술의
주요방법으로부상할전망이다.
2.3.3.2. 동맥내혈전용해술 Intra-arterial thrombolysis
개정: 2012.12
177
CLINICAL RESEARCH CENTER FOR STROKE
2009 AHA Scientific Statement 2
Intra-Arterial Thrombolysis
1. Intra-arterial thrombolysis is indicated for treatment of selected patients with major stroke of �6 hours’
duration due to an occlusion of the middle cerebral artery (Class I, Level of Evidence B). (This
recommendation has not changed since the publication of previous guidelines.)
2. Intra-arterial thrombolysis is reasonable for patients who have contraindications to the use of
intravenous thrombolysis, such as recent surgery (Class IIa, Level of Evidence C). (This recommendation
was not included in the previous guidelines.)
3. The availability of intra-arterial thrombolysis should generally not preclude the intravenous
administration of rt-PA in otherwise eligible patients (Class I, Level of Evidence A).
4. Treatment requires the patient to be at an experienced stroke center with immediate access to cerebral
angiography and qualified interventionalists. Facilities should define criteria to credential individuals who
can perform intra-arterial thrombolysis (Class I, Level of Evidence C).
Mechanical Clot Extraction
1. Although the Concentric Merci device can be useful for extraction of intra-arterial thrombi in
appropriately selected patients, the utility of the device in improving outcomes after stroke remains
unclear (Class IIb, Level of Evidence B).
2. The usefulness of other endovascular devices is not yet established, but they may be beneficial.
(Class IIb, Level of Evidence C).
2012 9th American College of Chest Physicians Guidelines 3
2.2 Intraarterial Thrombolysis in Patients With Acute Ischemic Stroke
2.2.1. In patients with acute ischemic stroke due to proximal cerebral artery occlusions who do not meet
eligibility criteria for treatment with IV r-tPA, we suggest intraarterial (IA) r-tPA initiated within 6 h of
symptom onset over no IA r-tPA (Grade 2C).
2.2.2. In patients with acute ischemic stroke we suggest IV r-tPA over the combination IV/IA r-tPA (Grade 2C).
Remarks: Carefully selected patients who value the uncertain benefits of combination IV/IA thrombolysis
higher than the associated risks may choose this intervention. Patients who prefer to avoid risk in the
setting of uncertain benefits are more likely to choose IV r-tPA alone.
2.3 Mechanical Thrombectomy in Patients With Acute Ischemic Stroke

178
CLINICAL RESEARCH CENTER FOR STROKE
2.3. In patients with acute ischemic stroke, we suggest against the use of mechanical thrombectomy
(Grade 2C).
Remarks: Carefully selected patients who value the uncertain benefit of mechanical thrombectomy higher
than the associated risks may choose this intervention.
2012 Standards of Practice Committee of the Society of NeuroInterventional Surgery 4
1. The availability of intra-arterial therapy should generally not preclude the intravenous administration of
recombinant tissue plasminogen activator (rt-PA) in otherwise eligible patients (American Heart
Association (AHA) Class I, Level of Evidence A, Centre for Evidence Based Medicine (CEBM) level 1b, grade A-B).*
2. Treatment requires the patient to be at an experienced stroke center with rapid access to cerebral
angiography and qualified interventionalists (AHA Class I, Level of Evidence C, CEBM level 2C, grade C).*
3. Intra-arterial chemical thrombolysis is an option for the treatment of selected patients with major stroke
of �6 h duration due to an occlusion of the middle cerebral artery and who are not otherwise candidates
for intravenous rt-PA (AHA Class I, Level of Evidence B, CEBM level 2b, grade B).*
4. Intra-arterial chemical thrombolysis is reasonable for patients who have contraindications to the use of
intravenous thrombolysis, such as recent surgery (AHA Class IIa, Level of Evidence C, CEBM level 4,
grade C).*
5. Combination intravenous/intra-arterial therapy is reasonable in selected patients who present with
major stroke of �4.5 h duration (AHA Class IIa, Level of Evidence B, CEBM level 2a, grade B).
6. Intra-arterial thrombus removal with the Penumbra aspiration system or Concentric MERCI clot
retrieval device is reasonable in selected patients with major stroke where care has been initiated at �8 h
duration although data regarding improvement of clinical outcomes is unclear (AHA Class IIa, Level of
Evidence B, CEBM level 2a, grade B).
7. The usefulness of other endovascular devices is not yet established, but they may be beneficial and may
be considered (AHA Class IIb, Level of Evidence C, CEBM level 4, grade C.)*
8. The usefulness of endovascular treatment in the posterior circulation is not yet established, but it may be
beneficial and may be considered, even beyond the 6-8 h time window typical for anterior circulation
stroke (AHA Class IIB, Level of Evidence C).
*As already defined by the AHA guidelines for the early management of adults with ischemic stroke
(Circulation 2007) and AHA statement regarding indications for the performance of intracranial
endovascular neurointerventional procedures (Circulation 2009).

179
CLINICAL RESEARCH CENTER FOR STROKE
1. 기존의근거
PROACT II 임상연구에따르면전-우로키나아제를사용한환자군은 조군에비하여높은혈관재개
통률(recanalization rate)를보 으며(66% vs 18%, p� 0.01), 뇌출혈의빈도는전-우로키나아제그룹이
높은경향을보 으나통계적인유의성은없었다.(10% vs 2%, p =0.06) 5
최근에수술받은환자에발생한뇌경색에서정맥내혈전용해술은금기증이므로사용하지못하나, 동
맥내혈전용해술의경우역시출혈의위험은높이지만정맥내혈전용해술보다는그위험정도가낮
을것으로추정되어사용이가능하다고한다.6,7 후방순환계뇌졸중(posterior circulation stroke)에서동맥
내혈전용해술의효과를밝히고자한임상연구에따르면, 증상발현후24시간이내의환자중뇌혈관
조 술에서혈관폐색의증거가있는경우에동맥내우로키나아제투여는8명중4명에서좋은예후를
보 으나, 조군에서는8명중1명에서만좋은예후를보여통계적으로유의한차이를보 다.8
2. 새로운근거
Intra-Arterial Thrombolysis Meta-Analysis
허혈성뇌졸중에서동맥내혈전용해술의효과를입증한단일연구는 pro-urokinase 를이용한
PROACT II 연구가유일하다.5그러나단일 II상연구이고, 그효과도크다고할수는없어, 당시에미국
FDA 승인을받지는못하 다. 이후에도동맥내혈전용해술에 한연구는지속적으로진행되었으나
그특성상다른치료법들에비해상 적으로연구참여자수가적어통계검정력이부족하기때문에
뚜렷하게효과를입증한단일무작위배정 조군임상연구는발표되지않았다. 그러나이미임상적
으로는그효용성이인정되어실제로널리쓰이고있는상황이며, 최근에동맥내혈전용해술무작위
배정임상연구5개에 한메타분석연구결과가발표되어그근거가보강되었다.1동맥내혈전용해
술을받은허혈성뇌졸중환자224명과 조군171명의90일째혹은연구종료시점의예후를비교했
을때, 치료를받은군에서mRS 0-2점일확률(odds ratio[OR]=2.05; 95% CI, 1.33 to 3.14; P=0.001)과0-1점
일확률(OR=2.14; 95% CI, 1.31 to 3.51; P=0.003) 모두뚜렷이유의하게증가했고, 혈관재개통확률과도
유의한연관성을보 다 (완전재개통, OR=4.62; 95% CI, 2.02 to 10.56; P=0.0003). 신경 상적및증후
성뇌내출혈은동맥내혈전용해술을받은치료군에서증가하 지만, 양군간에사망률의차이는없
었다. 이연구는동맥내혈전용해술치료의근거를제시하는연구로서의의가있다.

180
CLINICAL RESEARCH CENTER FOR STROKE
Basilar Artery International Cooperative Study (BASICS)
전체뇌경색의 3-5%를차지하는뇌바닥동맥폐색은환자의예후가나쁘고, 앞순환부경색과달리
NIHSS점수로증상의심각도가정확히반 되지않아그간제 로구성된전향적연구결과가부족한
실정이었는데2009년에 규모전향적연구가발표되었다.9 2002년부터2007년까지미국과유럽에서
확인된총619명의급성뇌바닥동맥폐색환자중치료를받지않은27명을제외한592명의환자들을
전향적으로관찰한결과, 402명(68%)의환자가1개월째불량한예후 (mRS≥4)를보 고그중214명
(36%)의환자가사망하 으며동맥내혈전용해술과정맥내혈전용해술의단순비교에서동맥내치
료의우월성이입증되지는못하 다. 그러나뇌바닥동맥폐색의매우불량한예후는정맥내혈전용
해술이실패하거나적응증이아닌경우동맥내혈전용해술고려의필요성을시사한다.
Multi-MERCI (Mechanical Embolus Removal in Cerebral Ischemia)
Multi-MERCI 는concentric clot retriever 기구를사용하여혈전을제거하는다기관연구로 IV tPA 치료
에도불구하고주요혈관이재개통되지않은164명의환자들을 상으로발생8시간이내치료결과
를보고하 는데, 기구만사용해서는57.3%, 혈전용해제까지투여한경우69.5% 의재개통률을보
다.10 참여환자의NIHSS 중앙값이19 점으로증상이심한환자를 상으로진행하 다는점을감안하
여도사망률은34%로높은편이어서이후동맥내혈전용해술에 한부정적인식의원인중하나가
되었으며나중에개발된기계적혈정용해술(mechanical thrombolysis) 기구의주요비교 상이되었
다. 이후기존의MERCI 연구결과를포함한pooled analysis를실시하여예후관련인자분석을실시했
는데, 그결과재개통여부가예후에가장중요한요인이었다.11
Penumbra Pivotal Trial and Post-Marketing Study
Penumbra device 는혈전을잘게부수어흡입하는방식의mechanical thrombolysis 기구로첫보고에
서발생8시간이내의125명환자를 상으로81.5% 라는높은재개통률을 (Thrombolysis in Myocardial
Ischemia, 이하 TIMI, Grade 2~3) 보 고12이후발표된시판후연구(post-marketing study)에서도역시
87%라는높은재개통률을보여많은주목을받았다.13그러나기구특성상혈관박리같은혈관손상
위험성이있어서비교적많은경험을필요로하고, 다른mechanical thrombolysis 기구와의직접적인
비교연구가없다는등의단점들이지적되고있어향후추가적인후속연구를필요로하고있다.14
Solitaire With the Intention For Thrombectomy (SWIFT)
Solitaire는뇌혈관동맥류코일시술시에혈관을지지하는용도로개발되었던스텐트로이기구를사
용하여뇌혈관내혈전을비교적용이하게제거할수있다는사실이알려지면서이러한목적으로새

181
CLINICAL RESEARCH CENTER FOR STROKE
로이개발된 stent retriever이다. 처음 22명을 상으로한후향적관찰연구에서 Thrombolysis in
Cerebral Infarction (이하TICI) grade 2a,b/3 재개통률90.9% 라는놀라운결과를보고하 다.15이후113
명의환자를 상으로기존의MERCI device 와직접적인무작위비교를한SWIFT 연구에서TIMI 2,3 재
개통률이각각Solitaire 61%, MERCI 24% 라는큰차이를보여 (OR 4.87 [2.4~11.10], 비열등성p�0.0001,
우월성p=0.0001) 비열등성디자인연구임에도불구하고Solitaire의우월성이입증되었다.16임상적으
로도3개월째좋은신경학적예후(mRS 0-2 등) 분율Solitaire 58%, MERCI 33% (OR 2.78 [1.25~6.22], 비열
등성 p=0.0001, 우월성 p=0.02), 3개월사망률 Solitaire 17%, MERCI 38% (OR 0.34 [0.14~0.81], 비열등성
p=0.0001, 우월성p=0.02) 으로유의한차이를보 다.
Trevo 2
Trevo device도Solitaire 같은stent retriever 로서SWIFT 처럼MERCI와비교한전향적무작위배정연구
를진행하 다.17발생8시간이내의뇌졸중환자를 상으로Trevo 군88명과MERCI 군90명을비교한
결과일차결과변수인TICI grade 2,3 의재개통률이Trevo 86%, MERCI 60%로역시큰차이로Trevo 의
우월성이입증되었다 (OR 4.22 [2.01~8.86], 비열등성및우월성p�0.0001). 안정성측면에서3개월사망
률은Trevo 15%, MERCI 23%로유의한차이는없었으나(p=0.1826) 임상효과에서는3개월째mRS 0-2
분율Trevo 40%, MERCI 22% (OR 2.39 [1.16~4.95], 비열등성p=0.013) 으로유의한차이를보 다. 이렇듯
최근에진행된동맥내혈전용해술연구결과들은일관되게stent retriever 형태의우월성을보이고있
어앞으로stent retriever 가동맥내혈전용해술을주도할전망이다.
기타동맥내혈전용해술연구들및전망
비교적최근까지만해도동맥내혈전용해술, 특히물리적혈전용해술에 해서는높은재개통률에
상응할만큼환자의예후가호전이되지않는결과를보여그임상적근거가부족하다는회의적시각
들이있었고18,19 최근발표된ACCP 진료지침에서도이러한분위기를반 하여물리적혈전용해술에
해부정적으로기술되었다.3그러나최근SWIFT 와TREVO 결과가나란히발표되면서이러한분위
기가반전되는계기가되고있다.20
처음에정맥내혈전용해술을시행한후반응이없는경우동맥내혈전용해술을이어서시도하는
combined (briding) IV/IA thrombolysis는이미국내를포함한다수의병원들에서선별적으로시행하고
있으나아직근거가충분하지않은상황인데, 이를비교하는다기관전향적연구인 IMS-III 연구는현
재중단된것으로알려져서향후추이를지켜볼필요가있다.21

182
CLINICAL RESEARCH CENTER FOR STROKE
1. 동맥내혈전용해술은6시간이내에발생한중 뇌동맥이나내경동맥폐색환자중정맥내혈전용
해술치료의적응증이되지않거나최근수술등으로금기인환자를 상으로고려할수있다. (근거
수준Ia, 권고수준A) - 근거수준및권고수준개정
2. 동맥내혈전용해술을시행하는기관은뇌혈관조 장비가즉각적으로사용가능해야하며훈련받
은중재시술전문가가있어야한다. 각기관은동맥내혈전용해술을시행하는의사의기준을마련
하도록노력해야한다. (GPP) - 근거수준및권고수준개정
3. 뇌바닥동맥(basilar artery) 폐색과같은뒷순환계뇌졸중환자에서동맥내혈전용해술을기관내기
준에따라치료방법으로사용할수있다. (근거수준III, 권고수준B) - 근거수준및권고수준개정
4. 정맥내혈전용해술이가능하면우선시행하고, 반응이없는경우추가적으로동맥내혈전용해술을
시도할수있다. (근거수준III, 권고수준B) - 추가
5. 물리적혈전용해술은8시간이내에발생한주요동맥폐색허혈성뇌졸중환자에게시행할수있
다. 기구선택은stent retriever 계열을우선고려할수있으며, 환자의상태에따라시행자가결정할
수있다. (근거수준Ib, 권고수준A) - 추가
1. Lee M, Hong KS, Saver JL. Efficacy of intra-arterial fibrinolysis for acute ischemic stroke: meta-analysis
of randomized controlled trials. Stroke2010;41:932-937.
2. Meyers PM, Schumacher HC, Higashida RT, Barnwell SL, Creager MA, Gupta R, et al. Indications for the
performance of intracranial endovascular neurointerventional procedures: a scientific statement from
the American Heart Association Council on Cardiovascular Radiology and Intervention, Stroke Council,
Council on Cardiovascular Surgery and Anesthesia, Interdisciplinary Council on Peripheral Vascular
Disease, and Interdisciplinary Council on Quality of Care and Outcomes Research. Circulation
2009;119:2235-2249.
3. Lansberg MG, O'Donnell MJ, Khatri P, Lang ES, Nguyen-Huynh MN, Schwartz NE, et al. Antithrombotic
and thrombolytic therapy for ischemic stroke: Antithrombotic therapy and prevention of thrombosis, 9th
ed: American college of chest physicians evidence-based clinical practice guidelines. Chest
2012;141:e601S-636S.
4. Blackham KA, Meyers PM, Abruzzo TA, Albuquerque FC, Fiorella D, Fraser J, et al. Endovascular

183
CLINICAL RESEARCH CENTER FOR STROKE
therapy of acute ischemic stroke: Report of the standards of practice committee of the society of
neurointerventional surgery. JNeurointerv Surg2012;4:87-93.
5. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, Pessin M, Ahuja A, Callahan F, Clark WM,
Silver F, Rivera F. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a
randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 1999;282:2003-11.
6. Chalela JA, Katzan I, Liebeskind DS, Rasmussen P, Zaidat O, Suarez JI, Chiu D, Klucznick RP, Jauch E,
Cucchiara BL, Saver J, Kasner SE. Safety of intra-arterial thrombolysis in the postoperative period.
Stroke 2001;32:1365-9.
7. Choi JH, Bateman BT, Mangla S, Marshall RS, Prabhakaran S, Chong J, Mohr JP, Mast H, Pile-
Spellman J. Endovascular recanalization therapy in acute ischemic stroke. Stroke 2006;37:419-24.
8. Macleod MR, Davis SM, Mitchell PJ, Gerraty RP, Fitt G, Hankey GJ, Stewart-Wynne EG, Rosen D, McNeil
JJ, Bladin CF, Chambers BR, Herkes GK, Young D, Donnan GA. Results of a multicentre, randomised
controlled trial of intra-arterial urokinase in the treatment of acute posterior circulation ischaemic stroke.
Cerebrovasc Dis 2005;20:12-7.
9. Schonewille WJ, Wijman CA, Michel P, Rueckert CM, Weimar C, Mattle HP, et al. Treatment and
outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS):
a prospective registry study.Lancet Neurol 2009;8:724-730.
10. Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al. Mechanical thrombectomy for
acute ischemic stroke: final results of the Multi MERCI trial. Stroke2008;39:1205-1212.
11. Nogueira RG, Liebeskind DS, Sung G, Duckwiler G, Smith WS. Predictors of good clinical outcomes,
mortality, and successful revascularization in patients with acute ischemic stroke undergoing
thrombectomy: pooled analysis of the Mechanical Embolus Removal in Cerebral Ischemia (MERCI) and
Multi MERCI Trials. Stroke 2009;40:3777-3783.
12. The penumbra pivotal stroke trial investigators. Safety and effectiveness of a new generation of
mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke2009;40:2761-
2768.
13. Tarr R, Hsu D, Kulcsar Z, Bonvin C, Rufenacht D, Alfke K, et al. The POST trial: Initial post-market
experience of the penumbra system: Revascularization of large vessel occlusion in acute ischemic
stroke in the United States and Europe. J Neurointerv Surg2010;2:341-344.

184
CLINICAL RESEARCH CENTER FOR STROKE
14. Hussain SI, Zaidat OO, Fitzsimmons BF. The penumbra system for mechanical thrombectomy in
endovascular acute ischemic stroke therapy. Neurology 2012;79:S135-141.
15. Roth C, Papanagiotou P, Behnke S, Walter S, Haass A, Becker C, et al. Stent-assisted mechanical
recanalization for treatment of acute intracerebral artery occlusions. Stroke 2010;41:2559-2567.
16. Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al. Solitaire flow restoration device
versus the MERCI retriever in patients with acute ischaemic stroke (SWIFT): A randomised, parallel-
group, non-inferiority trial.Lancet2012;380:1241-1249.
17. Nogueira RG, Lutsep HL, Gupta R, Jovin TG, Albers GW, Walker GA, et al. Trevo versus MERCI
retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke
(trevo 2): A randomised trial. Lancet 2012;380:1231-1240.
18. Baker WL, Colby JA, Tongbram V, Talati R, Silverman IE, White CM, et al. Neurothrombectomy devices
for the treatment of acute ischemic stroke: State of the evidence. Ann Intern Med 2011;154:243-252.
19. Brinjikji W, Rabinstein AA, Kallmes DF, Cloft HJ. Patient outcomes with endovascular embolectomy
therapy for acute ischemic stroke: A study of the national inpatient sample: 2006 to 2008. Stroke
2011;42:1648-1652.
20. Gorelick PB. Assessment of stent retrievers in acute ischaemic stroke. Lancet2012;380:1208-1210.
21. NINDS statement. Interventional management of stroke III trial.
http://www.ninds.nih.gov/disorders/clinicaltrialsINCT00359424.htm

185
CLINICAL RESEARCH CENTER FOR STROKE
아스피린을48시간이내에투여하 을때, 2개의 규모임상시험1,2과이들의메타분석3에서허혈성
뇌졸중발생 48시간이내에아스피린(하루용량 160-300mg)을투여하면출혈성뇌졸중의위험을
1000명당2명정도다소증가시키지만(p=0.07), 허혈성뇌졸중재발을1000명당7명정도유의하게
감소시키며(p<0.01), 사망을포함한심각한심뇌혈관질환발생을1000명당9명정도로유의하게감
소시킬수있다고한다.(p<0.01, NNT=111). 이러한이득이아스피린의조기투여가경색자체에 향
을주기때문인지, 뇌경색의재발을예방하기때문인지에 해서는아직확실하지않다. 급성기(특
히6시간이내) 뇌경색에서혈전용해술을받은환자가(NNT=16) 아스피린을사용한경우(NNT=83)에
1. The oral administration of aspirin (initial dose is 325mg) within 24 to 48 hours after stroke onset is
recommended for treatment of most patients (ASA: Class I, LOE A).
2. Aspirin should not be considered a substitute for other acute interventions for treatment of stroke,
including the intravenous administration of rtPA (ASA: Class III, LOE B).
3. The administration of aspirin as an adjunctive therapy within 24 hours of thrombolytic therapy is not
recommended (ASA: Class III, LOE A).
4. The administration of clopidogrel alone or in combination with aspirin is not recommended for the
treatment of acute ischemic stroke. The panel supports research testing the usefulness of emergency
administration of clopidogrel in the treatment of patients with acute stroke (ASA: Class III, LOE C).
5. Outside the setting of clinical trials, the intravenous administration of antiplatelet agents that inhibit the
glycoprotein IIb/IIIa receptor is not recommended (ASA: Class III, LOE B).
허혈성뇌졸중은 부분색전및혈전에의한뇌혈관폐색에의해발생한다. 아스피린(aspirin)을급성
기에투여하면허혈성뇌졸중으로인한사망, 장애, 재발및기타심혈관계질환의발생을감소시킬
수있을것으로기 된다.
2.3.4. 항혈소판제Antiplatelet agents

186
CLINICAL RESEARCH CENTER FOR STROKE
1. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic
stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet. 1997;349:1641-1649.
2. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of
aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke.
Lancet. 1997;349:1569-1581.
3. Chen ZM, Sandercock P, Pan HC, Counsell C, Collins R, Liu LS, Xie JX, Warlow C, Peto R. Indications for
early aspirin use in acute ischemic stroke : A combined analysis of 40 000 randomized patients from the
비해예후가좋다는것을보고한계통적분석이있다.4
비교적유용한14개의임상시험에관한메타분석에서혈전용해술24시간이내의항혈전제사용은24
시간이내에사용하지않은경우(OR; 1.93 vs 1.14)에비해출혈의위험이의미있게높았다.5
MATCH 연구에의하면클로피도그렐(clopidogrel)에아스피린을추가투여하 을때, 급성뇌경색또
는일과성허혈발작환자에서1% 정도재발의위험을감소시켰으나, 1.3% 정도출혈의위험을증가
시켰으며둘다통계적인의미는없었다.6
압식시맙(Abciximab)에관한 2개의임상시험에서통계적으로의미있는출혈의증가는없고예후에
어느정도좋은 향을주는것으로나타났으나, 제3상임상시험에서출혈이의미있게증가하여연구
가중단되었다.7,8
1. 뇌출혈의가능성이배제된급성기허혈성뇌졸중환자에서는아스피린을뇌경색발생 24-48시간
이내에경구투여(초기용량160-300mg)해야한다. (근거수준Ia, 권고수준A)
2. 아스피린이정맥내혈전용해술을포함한급성중재치료를 체하지는못한다. (근거수준 Ia, 권고
수준A)
3. 혈전용해술을시행한경우24시간이내에아스피린을투여하면안된다. (근거수준Ia, 권고수준A)
4. 당단백 IIb/IIIa 수용체(glycoprotein IIb/IIIa receptor)에길항하는항혈소판제제[압식시맙(abciximab) 등]
의정맥주사는급성기허혈성뇌졸중환자에서추천되지않는다. (근거수준Ib, 권고수준A)

187
CLINICAL RESEARCH CENTER FOR STROKE
항응고제는허혈성뇌졸중의예방치료를위해널리쓰이는약이지만급성기환자의치료에 한유
용성에서는논란이많다. 항응고제의종류, 투입시기및방법, 적정용량, 치료의지속기간등에 해
아직의견이정립되지않은상태이나현재까지의 규모 조군연구의결과에서항응고제는급성
기허혈성뇌졸중의치료제로서근거가부족한상태이다.
chinese acute stroke trial and the international stroke trial. On behalf of the CAST and IST collaborative
groups. Stroke. 2000;31:1240-1249.
4. Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs, and effects on
individuals and populations. Lancet. 1999;354:1457-1463.
5. Wardlaw JM. Overview of Cochrane thrombolysis meta-analysis. Neurology. 2001;57:S69-76.
6. Diener HC, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M, Leys D, Matias-Guiu J,
Rupprecht HJ. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke
or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-
controlled trial. Lancet. 2004;364:331-337.
7. The Abciximab in Ischemic Stroke Investigators. Abciximab in acute ischemic stroke: a randomized,
double-blind, placebo-controlled, dose-escalation study. Stroke.2000;31:601-609.
8. Abciximab Emergent Stroke Treatment Trial (AbESTT) Investigators. Emergency administration of
abciximab for treatment of patients with acute ischemic stroke: results of a randomized phase 2 trial.
Stroke. 2005;36:880-890
1. Urgent anticoagulation with the goal of preventing early recurrent stroke, halting neurological worsening,
or improving outcomes after acute ischemic stroke is not recommended for treatment of patients with
acute ischemic stroke (ASA, RCP: LOE Ia, GOR A). This recommendation may change if additional data
2.3.5. 항응고제Anticoagulants

188
demonstrate the usefulness of very early intravenous administration of anticoagulants for treatment of
patients with infarctions secondary to large-artery thrombosis or cardioembolism. Urgent
anticoagulation should not be used in lieu of intravenous thrombolysis for treatment of otherwise eligible
patients (ASA: LOE Ia, GOR A).
2. Urgent anticoagulation is not recommended for patients with moderate to severe strokes because of an
increased risk of serious intracranial hemorrhagic complications (ASA: LOE Ia, GOR A).
3. Initiation of anticoagulant therapy within 24 hours of treatment with intravenously administered rtPA is
not recommended (ASA: LOE IIa, GOR B).
4. Full-dose heparin may be used when there are selected indications such as cardiac sources with high
risk of re-embolism, arterial dissection, or high-grade stenosis prior to surgery (EUSI: LOE IV, GOR C).
CLINICAL RESEARCH CENTER FOR STROKE
헤파린을급성기에적용한 규모임상시험인 International Stroke Trial(IST)에서중등량정도의헤파
린(heparin) 투여군(12,500단위피하주입, 1일2회, 2주간투여), 소량헤파린투여군(5,000단위), 헤파린
비투여군으로나누어2주후와6개월후에사망, 뇌졸중재발, 기능예후, 출혈합병증을조사한결과,
헤파린의유효성은입증되지못하 다. 또한급성허혈성뇌졸중환자에서헤파린혹은저분자량헤
파린/헤파리노이드(heparinoid)의사용은출혈의합병증을증가시켰다.1이런약제들은뇌경색부위
의출혈성변이를조장하며특히뇌경색이심한환자에서두드러진경향을보 다. 혈전용해제보다
는출혈의합병증은적다고보고되나치료의득실을고려했을때급성기에항응고제사용은신중하
게고려하여야한다.
IST 연구에서심장탓색전증원인의 부분을차지하는비판막성심방세동사례(비헤파린투여군)의
급성기14일이내의재발율이4.9%로낮았다. 따라서비판막성심방세동에의한뇌경색에서항응고
제를급성기부터바로시작해야하는지에 한부정적인의견이있다.
3시간이내재조합조직플라스미노겐활성제를사용한NINDS 임상시험에서재조합조직플라스미
노겐활성제주입후24시간이내항응고제의사용은금지하고있으나2이부분에 한임상시험이나
메타분석은이루어지지않았다.
저분자헤파린에 해서는나드로파린(nadroparin)이발병후48시간이내의뇌경색환자에게유효하
다는보고가있었는데3 규모시험에서는그유효성을확인할수없었다. 미국에서행해진발병24시
189
CLINICAL RESEARCH CENTER FOR STROKE
1. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of
aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet.
1997;349:1569 -1581.
2. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen
activator for acute ischemic stroke. N Engl J Med.1995;333:1581-1587.
3. Kay R, Wong KS, Yu YL, et al. Low-molecular-weight heparin for the treatment of acute ischemic stroke. N
Engl J Med. 1995;333:1588 -1593.
4. Adams HP Jr, Bendixen BH, Leira E, et al. Antithrombotic treatment of ischemic stroke among patients with
1. 허혈성뇌경색발병48시간내의환자에게헤파린투여의유용성에관한과학적근거는없으며아
스피린(aspirin) 투여와비교하여출혈의합병증을증가시킬수있다. (근거수준Ia, 권고수준A)
2. 뇌경색의조기치료로저분자헤파린, 헤파리노이드의사용은추천되지않는다. (근거수준 Ia, 권고
수준A)
3. 재조합조직플라스미노겐활성제(rtPA) 투여후24시간이내항응고제의투여는추천되지않는다.
(근거수준IIa, 권고수준B)
간이내의뇌경색을 상으로한헤파리노이드ORG 10172(다나파로이드[danaparoid]) 7일간정주임
상시험(TOAST)에서는전체적으로는부정적인결과를보 다. 그러나층화분석결과죽상혈전성뇌
경색(atherothrombotic infarction)에서 3개월후의기능회복이양호한사례가뚜렷하게증가하여, 이
아군(subgroup)에유효할가능성이제기되었다.4그러나저분자헤파린, 헤파리노이드의메타분석에
서는이러한유효성은확인되지않았다.5또한Cochrane Review에서급성기뇌경색증사례에 한항
응고치료법의유용성을22개시험, 23,547 사례를 상으로메타분석을시행하 으나항응고치료
법의유용성은입증하지못하 다.6선택적항트롬빈제인아가트로반(agatroban)은증상발생 12시
간이내의뇌혈전증(특히피질경색)에사용시출혈성합병증은증가하지않았다는보고가있으나7
치료의유효성에 한보고는아직없다.
190
CLINICAL RESEARCH CENTER FOR STROKE
1. At present, no intervention with putative neuroprotective actions has been established as effective in
improving outcomes after stroke, and therefore none currently can be recommended (ASA: LOE Ia, GOR
A).
occlusion or severe stenosis of the internal carotid artery: a report of the Trial of Org 10172 in Acute Stroke
Treatment (TOAST). Neurology. 1999;53:122-125.
5. Bath PM, Iddenden R, Bath FJ. Low-molecular-weight heparins and heparinoids in acute ischemic stroke: a
meta-analysis of randomized controlled trials. Stroke. 2000;31:1770-1778.
6. Gubitz G, Counsell C, Sandercock P, et al. Anticoagulants for acute ischaemic stroke. Cochrane Database Syst
Rev. 2004;CD000024.
7. LaMonte MP, Nash ML, Wang DZ, et al.; ARGIS-1 Investigators. Argatroban anticoagulation in patients with
acute ischemic stroke (ARGIS-1): a randomized, placebo-controlled safety study. Stroke. 2004;35:1677-1682.
뇌혈류의차단에의한산소와포도당의중단은ATP고갈을초래하며, 이후신경세포가손상된다. 그
기전으로 루타메이트와그수용체의지속적흥분에의한과도한칼슘이온의유입설, 유리산소기,
단백분해효소, 염증에의한손상, 세포사멸(apoptosis) 등의가설이주장되고있다. 신경세포보호제로
현재까지동물실험에서효과가입증된많은종류의신경보호제들이임상시험에서는유효성입증에
실패하 다. NMDA-수용체길항제, 칼슘통로억제제, 마그네슘, 자유유리기제거제, 세포막안정제,
저체온요법등이 규모무작위배정 조군임상시험에서유효성을입증하지못하 다. 향후좀더
근본적인원인분석이필요하며, 치료시간의단축과병합치료를통한효과증 에관한임상시험들
이진행중이다.
2.3.6. 신경보호제Neuroprotectants
191
CLINICAL RESEARCH CENTER FOR STROKE
1. 허혈성뇌경색발병후급성기신경보호제치료는일반적으로추천되지않는다. (근거수준 Ia, 권고
수준A)
1. Kaste M, Castillo J. Neuroprotection in brain ischemia: an update. Cerebrovas dis. 2006;21(Suppl 2):1-132.
2. Stroke-Acute Ischemic NXY Treatment (SAINT I) Trial Investigators. NXY-059 for acute ischemic stroke. N
Engl J Med. 2006;354:588-600.
3. SAINT II Trial Investigators. NXY-059 for the treatment of acute ischemic stroke. N Engl J Med. 2007;357:562-
571.
4. Clark WM, Warach SJ, Pettigrew LC, et al.Citicoline Stroke Study Group. A randomized dose-response trial of
citicoline in acute ischemic stroke patients. Neurology. 1997;49:671-678.
5. Clark WM, Williams BJ, Selzer KA, et al. A randomized efficacy trial of citicoline in patients with acute ischemic
칼슘통로길항제인니모디핀(nimodipine), 플루나리진(flunarizine), GABA 작동제인클로메티아졸
(clomethiazole), opioid 길항제인 날리네펜 (nalinefene), 모노시알로갱 리오사이드
(monosialoganglioside), 루타메이트길항제인MK-801, 덱스트로판(dextrophan), 자유유리기제거제
인티릴라자드[tirilazad(21-amino steroid)] 등이동물실험에서뇌보호효과가입증되었으나실제임상
시험에서는효과를인정받지못하 다.1 2005년 규모위약 조임상시험에서자유유리기제거제
인NXY-059의뇌보호효과가발표되었으나,2 2007년2차임상시험결과에서는효과를입증하는데실
패하 다.3
시티콜린(citicoline)은세포막안정제로각각의임상시험에서일관적인유효성을입증되지않았으
나,4-6 2002년의메타분석에의하면중등도이상의장애를가진급성뇌경색환자에있어서24시간이
내투여했을경우유효성이있는것으로분석되었다.7
신경세포사멸자체가여러기전이복합적으로작용하고어느한기전을봉쇄하여도다음기전에의
한손상이발생한다는점을고려하면신경세포보호제의복합적사용의필요성이제기된다. 더나아
가급성기에혈전용해제와신경세포보호제를함께사용하면좋은결과를얻을가능성이있다.

192
CLINICAL RESEARCH CENTER FOR STROKE
1. Patients with major infarctions affecting the cerebral hemisphere or cerebellum are at high risk for
complicating brain edema and increased intracranial pressure. Measures to lessen the risk of edema
and close monitoring of the patient for signs of neurological worsening during the first days after stroke
are recommended (ASA: Class I, LOE B). Because many hospitals may not have neurosurgical expertise,
transfer of patients at risk for malignant brain edema to an institution that has such expertise should be
considered.
2. Patients with acute hydrocephalus secondary to an ischemic stroke most commonly affecting the
cerebellum can be treated with placement of a ventricular drain (ASA: Class I, LOE B).
3. Decompressive surgical evacuation of a space occupying cerebellar infarction is a potentially lifesaving
measure and clinical recovery may be very good (ASA: Class I, LOE B). Although data from clinical trials
are not available, it is recommended for patients with major cerebellar infarction.
뇌경색이후뇌부종은24-48시간후에나타난다. 뇌반구나소뇌를침범하는큰뇌경색으로인한뇌
부종은뇌압상승과뇌탈출(herniation)을일으키며, 의식저하와더불어생명을위협할수있다.1, 2
2.3.7. 신경계합병증의치료Treatment of neurologic complications
2.3.7.1. 뇌압상승, 부종, 출혈성변환ICP elevation, brain edema and hemorrhagic transformation
stroke. Stroke. 1999;30:2592-2597.
6. Clark WM, Wechsler LR, Sabounjian LA, et al. Citicoline Stroke Study Group. A phase III randomized efficacy trial of
2000 mg citicoline in acute ischemic stroke patients. Neurology. 2001;57:1595-1602.
7. Davalos A, Castillo J, Alvarez-Sabin J, et al. Oral citicoline in acute ischemic stroke: an individual patient data pooling
analysis of clinical trials. Stroke. 2002;33:2850 -2857.

193
CLINICAL RESEARCH CENTER FOR STROKE
뇌부종은중 뇌동맥기시부가막혔을때2~4일사이에일어난다.3증상발생12시간이내에뇌CT에
서중 뇌동맥 역의50% 이상을차지하는저음 과고 도중 뇌동맥증후(hyperdense MCA sign)
가발견되면신경학적악화를예측할수있다.4이러한환자들에게는부종을악화시킬수있는유리
수분(free water)이나저삼투액을제한할필요가있음이알려져있다. 또한저산소증, 고이산화탄소
증, 발열등도교정할필요가있다. 머리를20-30�도정도올려서정맥혈이잘배출될수있도록하며,
혈관확장을일으키는항고혈압제의사용은피하는것이좋다. 두개내압상승에 한현재의치료법
은과호흡, 삼투압치료, 뇌척수액배액등이있으나임상시험에바탕을둔근거는불충분하다. 고용
량의스테로이드사용은효과가불확실하고감염의위험을높이는것으로보고되어있다.5
4. Although aggressive medical measures, including osmotherapy, have been recommended for
treatment of deteriorating patients with malignant brain edema after large cerebral infarction, these
measures are unproven (ASA: Class IIa, LOE C). Hyperventilation is a short-lived intervention. Medical
measures may delay decompressive surgery.
5. Decompressive surgery for malignant edema of the cerebral hemisphere may be life-saving, but the
impact of morbidity is unknown. Both the age of the patient and the side of the infarction (dominant
versus nondominant hemisphere) may affect decisions about surgery. Although the surgery may be
recommended for treatment of seriously affected patients, the physician should advise the patient’s
family about the potential outcomes, including survival with severe disability (ASA: Class IIa, LOE B).
6. No specific recommendation is made for treatment of patients with asymptomatic hemorrhagic
transformation after ischemic stroke (ASA: Class IIb, LOE C). Treatment of symptomatic hemorrhagic
transformation is addressed in the intracerebral hemorrhage management guideline being issued
contemporaneously with this statement. Measures to lessen the likelihood of hemorrhagic
complications of thrombolytic agents or other interventions to restore or improve perfusion such as
careful control of arterial blood pressure are recommended.
7. Because of lack of evidence of efficacy and the potential to increase the risk of infectious complications,
corticosteroids (in conventional or large doses) are not recommended for treatment of cerebral edema
and increased intracranial pressure complicating ischemic stroke (ASA: Class III, LOE A).

194
CLINICAL RESEARCH CENTER FOR STROKE
최근세개의임상시험에의하면악성중 뇌동맥경색환자의경우48시간이내에개두술을시행하
면사망률을줄이고신경학적호전을기 할수있다.6-8
CT를이용한연구에따르면뇌경색이후임상적악화를동반한출혈성변성은 략5%정도발생한
다.9혈전용해술이나항응고제의사용이출혈변성과더욱관련이깊으며혈종을형성해신경학적인
악화를초래할수도있다.10
1. 뇌반구나소뇌를침범하는큰뇌경색의경우뇌부종이생기고뇌압이상승할가능성이높다. 부
종을줄이고환자가신경학적으로악화되는것을확인하기위해집중적인관찰을하는것이바람
직하다. (근거수준III, 권고수준B)
2. 소뇌경색등에의해수두증이생긴경우뇌실외배액(extraventricular drainage)을시행하여뇌압을
낮추는것이필요하다. (근거수준III, 권고수준B)
3. 크기가큰소뇌경색으로뇌간압박증후가나타나는경우수술적감압술을시행하는것이필요하
다. (근거수준III, 권고수준B)
4. 뇌경색이후악성뇌부종에삼투압치료(osmotherapy)를포함한여러약물적인뇌압강하요법을사
용할수있다. 과호흡은뇌압감소효과가지속되는시간이짧으며뇌경색환자의예후에미치는
향이불확실하다. 이러한내과적치료가감압수술시점을연장시킬가능성이있다. (근거수준 III, 권
고수준B)
5. 뇌반구경색에의한악성부종에 해감압수술을시행할경우환자의생명을구할수있고신경
학적인호전도기 할수있다. 연령과경색위치(비우성혹은우성반구) 등이수술결정요소가될
수있다. 심각한환자에게수술을추천하지만의사는심한장애를안고살아가야하는예후에 해
서충분히상의하는것이필요하다. (근거수준IIa, 권고수준B)
6. 뇌경색이후무증상출혈성변환(hemorrhagic transformation)에 한특별한치료는없다. 증상이
있는출혈성변환은뇌출혈의치료가이드라인을따른다. 혈전용해술이나경동맥스텐트(stent) 삽
입술이후에생길수있는출혈성변환의가능성을줄이기위한혈압조절을고려할수있다. (근거
수준IV, 권고수준C)
7. 뇌경색환자에서뇌압조절을목적으로효과가불확실하고감염의위험성을증가시키는상용량혹
은 용량피질스테로이드(corticosteroids)의사용은추천되지않는다. (근거수준Ib, 권고수준A)

195
CLINICAL RESEARCH CENTER FOR STROKE
1. Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. 'malignant' middle cerebral
artery territory infarction: Clinical course and prognostic signs. Arch Neurol.1996;53:309-315.
2. Rieke K, Schwab S, Krieger D, von Kummer R, Aschoff A, Schuchardt V, Hacke W. Decompressive
surgery in space-occupying hemispheric infarction: Results of an open, prospective trial. Crit Care Med.
1995;23:1576-1587.
3. Qureshi AI, Suarez JI, Yahia AM, Mohammad Y, Uzun G, Suri MF, Zaidat OO, Ayata C, Ali Z, Wityk RJ.
Timing of neurologic deterioration in massive middle cerebral artery infarction: A multicenter review. Crit
Care Med. 2003;31:272-277.
4. Manno EM, Nichols DA, Fulgham JR, Wijdicks EF. Computed tomographic determinants of neurologic
deterioration in patients with large middle cerebral artery infarctions. Mayo Clin Proc.2003;78:156-160.
5. Norris JW, Hachinski VC. High dose steroid treatment in cerebral infarction. Br Med J (Clin Res Ed).
1986;292:21-23.
6. Juttler E, Schwab S, Schmiedek P, Unterberg A, Hennerici M, Woitzik J, Witte S, Jenetzky E, Hacke W.
Decompressive surgery for the treatment of malignant infarction of the middle cerebral artery
(DESTINY): A randomized, controlled trial. Stroke. 2007;38:2518-2525.
7. Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, Amelink GJ, Schmiedeck P, Schwab S,
Rothwell PM, Bousser MG, van der Worp HB, Hacke W. Early decompressive surgery in malignant
infarction of the middle cerebral artery: A pooled analysis of three randomised controlled trials. Lancet
Neurol.2007;6:215-222.
8. Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, Boutron C, Couvreur G, Rouanet F, Touze E,
Guillon B, Carpentier A, Yelnik A, George B, Payen D, Bousser MG. Sequential-design, multicenter,
randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery
infarction (DECIMAL trial). Stroke. 2007;38:2506-2517.
9. Hornig CR, Dorndorf W, Agnoli AL. Hemorrhagic cerebral infarction--a prospective study. Stroke.
1986;17:179-185.
10. Warach S, Latour LL. Evidence of reperfusion injury, exacerbated by thrombolytic therapy, in human
focal brain ischemia using a novel imaging marker of early blood-brain barrier disruption. Stroke.
2004;35:2659-2661.

196
CLINICAL RESEARCH CENTER FOR STROKE
1. Recurrent seizures should be treated as with any other acute neurological condition (ASA: LOE IV, GOR
C). Prophylactic administration of anticonvulsants to patients who have had stroke but not seizures is not
recommended (ASA: GOR C).
2. In patients with intracerebral hemorrhage, prophylactic antiepileptic therapy (preferably phenytoin with
doses titrated according to drug levels [14 to 23 μg/mL]) may be considered for 1 month and then tapered
and discontinued if no seizure activity occurs during treatment, although data supporting this therapy are
lacking (ASA: LOE IV, GOR C).
뇌졸중급성기에발생되는경련의빈도는4-43%에이른다. 주로뇌졸중발병24시간이내에국소성
경련으로발생하고 2차적인전신경련도드물지않고, 이후경련이재발하는경우는 략 20-80%에
달한다. 간헐적경련이뇌졸중의예후에 향을주지는않는것으로생각되나, 드물게발생하는지속
성간질중첩증은생명을위협할수있다.1,2
급성뇌졸중후예방적항경련제의유용성에 한근거는없다.1,2또한, 뇌졸중급성기에발생한최초
경련(early seizures)에 한항경련제치료여부및적절한항경련제선택에 한본격적인연구는수
행된적이없다.1,2그러나환자에따라, 특히급성기경련이뇌졸중을악화시킬가능성이있거나또는
지속성간질중첩증으로진행될가능성이있는경우항경련제치료가권장된다.1,2
항경련제선택에관해 International League Against Epilepsy에서는저용량라모트리진(lamotrigine) 또
는가바펜틴(gabapentin)을추천하고있다.2이약제들은항응고제및항혈전제와상호작용이없고뇌
졸중후기능적회복을저해하지않으며골 사에 향을주지않는다고알려져있다.2골다공증위험
뇌졸중급성기에발생되는경련은주로뇌졸중발병24시간이내에국소성경련으로발생하고2차적
인전신경련이드물지않다. 간헐적경련이뇌졸중의예후에 향을주지는않는것으로생각되나, 드
물게발생하는지속성간질중첩증은생명을위협할수있다.
2.3.7.2. 경련Seizure

197
CLINICAL RESEARCH CENTER FOR STROKE
1. Adams HP, Jr., Adams RJ, Brott T, del Zoppo GJ, Furlan A, Goldstein LB, Grubb RL, Higashida R, Kidwell C,
Kwiatkowski TG, Marler JR, Hademenos GJ. Guidelines for the early management of patients with ischemic
stroke: A scientific statement from the stroke council of the American Stroke Association. Stroke.
2003;34:1056-1083.
2. Ryvlin P, Montavont A, Nighoghossian N. Optimizing therapy of seizures in stroke patients. Neurology.
2006;67:S3-9.
3. Broderick JP, Connolly S, Feldmann E, Hanley D, Krieger D, Mayberg M, Morgenstern L, Ogilvy CS, Vespa P,
Zuccarello M. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007
update: A guideline from the American Heart Association/American Stroke Association Stroke Council. High
Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary
Working Group: the American Academy of Neurology affirms the value of this guideline as an educational tool
for neurologists.Stroke. 2007;38:2001-2023.
1. 급성뇌졸중후경련이없었던환자에게일률적인항경련예방치료는고려되지않는다. (근거수준
IV, 권고수준C)
2. 뇌졸중급성기경련치료도기타신경계질환의급성기에발생한경련에 한치료법에준하여치
료하는것을고려할수있다. (근거수준IV, 권고수준C)
3. 뇌졸중급성기경련이뇌졸중을악화시킬가능성이있거나또는지속성간질중첩증으로진행될가
능성이있는경우항경련제치료를고려할후있다. (근거수준IV, 권고수준C)
4. 엽상뇌출혈의경우1개월정도예방적으로항경련제를사용하다가경련이없을경우서서히끊어
보는방법을고려할수있다. (근거수준IV, 권고수준C)
성이나항응고제의필요성이없는경우, 경제적이면서합리적인 체약물로는저용량의지속형카
바마제핀(carbamazepine)을추천하고있다.2엽상뇌출혈의경우1개월정도예방적으로항경련제를
사용하다가경련이없을경우서서히끊어보는방법을고려할수있다.3

198
CLINICAL RESEARCH CENTER FOR STROKE
2.4 뇌실질내출혈의치료Treatment of intracerebral hemorrhage
뇌출혈의발생은국내에서계속감소하고있지만, 아직전체뇌졸중의약 25%를차지하며, 외국의
10-15%의비율에비해서는여전히높은수준이다..1뇌출혈로인해뇌실질내용적이증가하면, 뇌압
이상승하게된다.2출혈의양이더욱증가하거나, 부종이나수두증이동반되면뇌압은더욱상승하게
된다. 뇌압이상승하면환자의신경학적증상이악화되고뇌탈출(herniation)이초래되어사망에이르
거나신경학적예후가불량하게된다. 따라서, 뇌출혈의양이많거나뇌탈출증상이의심되는경우에
는뇌압을감시하여적절한수준으로조절할필요가있다.
1. 급성기뇌출혈환자는뇌압상승, 혈압조절, 기도삽관및기계호흡등의필요때문에집중치료실에서
치료및관찰하는것을권장한다. (근거수준III, 권고수준B)
2. 상승된뇌압의조절은간단한처치부터단계적으로적극적방법을고려한다. 우선환자의머리를
30�정도위로올리고, 통증및불안정한상태를보이는환자에서제한적으로진통제및진정제
사용을고려한다. (근거수준IV, 권고수준C)
3. 좀더적극적인뇌압조절이필요한경우는삼투이뇨법(mannitol and hypertonic saline solution), 뇌실
내카테터삽입을통한배액(drainage of CSF via ventricular catheter), 신경근육차단(neuromuscular
blockade) 및과호흡요법(hyperventilation) 을이용할수있다. 일반적으로뇌압및혈압을모니터링
하면서뇌관류압(CPP)이70mmHg 이상을유지하도록권장한다. (근거수준IV, 권고수준C)
2.4.1. 뇌실질내출혈의약물치료Medical treatment of intracerebral hemorrhage
2.4.1.1. 뇌압조절 ICP control
개정: 2014.1

199
CLINICAL RESEARCH CENTER FOR STROKE
1. People with intracerebral haemorrhage should be monitored by specialists in neurosurgical or
stroke care for deterioration in function and referred immediately for brain imaging when necessary.
(RCP 2008, LOE: consensus)
2. Patients with a GCS score of ≤8, those with clinical evidence of transtentorial herniation, or those
with significant intraventricular hemorrhage (IVH) or hydrocephalus might be considered for
intracranial pressure (ICP) monitoring and treatment. A cerebral perfusion pressure of 50 to 70 mm
Hg may be reasonable to maintain depending on the status of cerebral autoregulation.
(ASA 2010: Class IIb; Level of Evidence: C)
3. Ventricular drainage as treatment for hydrocephalus is reasonable in patients with decreased level
of consciousness. (ASA 2010: Class IIa; Level of Evidence B)
4. Corticosteroid should not be used for treatment of primary intracerebral haemorrhage.
(SIGN 2008: LOE 1++, GOR B)
5. Intravenous mannitol should not be used routinely for treatment of raised intracranial pressure in
patients with primary intracerebral haemorrhage.(SIGN 2008: LOE 1+, GOR B).
기존의근거와새로추가된연구를근거를종합할때개정의필요성에 한근거는다음과같다. 뇌
출혈환자에서뇌압의측정, 조절방법및그결과에관해새로시행된무작위배정임상연구는없지
만, 뇌외상환자에서뇌압조절에관한내용이반 되면서2010년미국뇌졸중학회의뇌출혈진료지
침이개정되었다. 또한, 기존에시행된무작위배정임상시험의재분석결과가추가되면서, 이를근거
로하여부분개정의필요성이발생하 다. 지난진료지침에서는 2007년 7월 31까지발표된연구를
기반으로하 으므로, 그이후에새롭게발표된연구결과는문헌검색을통하여추가하 다
(Supplement 1).
뇌압상승환자를치료하는데있어첫단계는정확한뇌압을측정하는것이다. 뇌조직에삽입하여
직접뇌압을측정하는Camino�모니터등은출혈주변의뇌압을정확하게반 하므로, 이차뇌손
상이흔히발생하는혈종주변부위의혈역학적정보를적절하게모니터할수있는장점이있다. 반

200
면, 뇌실외배액카테터(Extraventricular drainage catheter)를이용하여측정하는뇌압은전반적인뇌압
이며, 뇌압측정의표준으로간주된다. 또한, 카테터를통해뇌척수액이나뇌실내출혈을배출할수있
으므로, 뇌실외배액카테터를통한뇌압측정은주로뇌실내출혈이동반된환자에서시도된다. 시술
과관련된합병증의발생률은카테터삽입시발생하는염증과출혈을포함하여 체로3% ~ 4% 수준
으로알려져있다.3
뇌출혈환자에서심한뇌압상승이얼마나흔하게발생하는지는잘알려져있지않다. 뇌실내출혈이
있어뇌압상승이의심되는환자들에서뇌실외배액카테터를삽입하면서뇌압을측정한연구를보
면, 삽입시측정된첫뇌압은뇌실내출혈의양이나뇌출혈의양과는직접관련이없었고일일평균뇌
압의정도도뇌출혈의총량과는관련이없었다.4이처럼, 뇌실내출혈의유무가그자체로뇌압상승을
의미하지는않지만, 뇌실내출혈은신경학적예후가불량한것과관련이있는데, 아마도이는수두증
이발생하기때문으로추정된다. STICH 연구에서는902명의환자중377의환자 (42%)에서뇌실내출
혈이동반되었으며, 총208명 (총환자중23%; 뇌실내출혈환자중55% )에서수두증이발생하 다. 뇌
실내출혈이동반되었던환자중6개월째신경학적예후가양호한환자는15% 에불과하 으나, 뇌실
내출혈이없는환자는31%에서예후가양호하여(P �0.00001) 뇌실내출혈의유무와신경학적예후와
의관련성이있었다.5더구나, 뇌실내출혈이있는환자에서수두증이동반되면, 예후가양호한환자의
비율이20% 에서12% 로감소하 다(P �0.031). 따라서, 수두증의동반여부는중요한예후인자라고
간주되었다.6이처럼뇌실내출혈은뇌출혈환자에서중요한예후인자로받아들여져서, 뇌출혈환자
의1개월사망률및12개월예후를예측하는데에이용하는뇌출혈점수표(ICH score)에반 되었다.7-9
결론적으로, 뇌실내출혈이나수두증이동반된뇌출혈환자에서는뇌압의측정이필요하고, 수두증
으로인해의식상태가악화될때는뇌실내배액카테터를삽입하는것을고려해야한다.
뇌출혈환자에서뇌압모니터링의적응증에 해서는잘알려져있지않으나, 뇌외상환자에서는 증
상의중증도가심한 ( 래스고우혼수척도3~8) 경우뇌압모니터링을권고하고있다.10,11또한천막상
부병변이큰경우에는뇌탈출로인한이차적뇌간압박의위험성이있기때문에뇌압모니터링의적
응증이되며12,13, 임상적으로뇌탈출의징후가있는경우에도뇌압을감시하여야한다.
뇌압을측정한다면평균동맥압과의차이로부터뇌관류압을계산할수있다. 뇌출혈환자에서뇌관류
압의범위를어느정도로유지하여야하는지에 해서는아직이론의여지가있다. 하지만2007년발
표한미국뇌졸중학회의진료지침에서는70mm Hg 이상을, 2010년에개정된지침에서는조금낮추
CLINICAL RESEARCH CENTER FOR STROKE

201
CLINICAL RESEARCH CENTER FOR STROKE
어50mmHg - 70mm Hg을권고하고있다.14 뇌출혈환자에서새롭게진행된연구는없지만, 기존의
연구를정리하여2007년뇌외상환자의진료지침에서뇌관류압에 한권고사항을개정하게되었
고, 그결과를차용하여뇌출혈환자에서도뇌관류압의범위가변경되게되었다.11뇌관류압권고수
치의하단이50mm Hg 이상으로제시된것은외상환자를 상으로이루어진작은연구에근거한다.
심한뇌손상이있었던환자에서뇌관류압이평균32 mmHg 정도로저하되었을때, 적절한강압제를
사용하여평균 68mmHg 정도로상승시키면뇌조직의산소분압이상승하 다. 뇌조직의산소분압
은임상적예후와관련되므로낮은뇌관류압을피하여야한다는근거를시사한다.15아울러뇌조직
사를모니터링하는미세투석법(microdialysis)을이용한연구결과에서는뇌관류압이 50mmHg 이
하로저하되면혐기성포도당 사로의이행을나타내는지표인젖산/피루브산비율이상승한다.16
위결과를통해보면뇌관류압은최소50 mmHg 이상은유지하여야함을시사한다.11뇌관류압의상
부기준이70mm Hg으로설정된것도뇌외상환자를 상으로시행된연구에근거한다.17중증도외
상환자를 상으로뇌관류압목표치 70mm Hg 이상과 50~70mm Hg 군으로나누어효과를비교한
무작위배정연구에서, 70mm Hg 이상군에서경정맥산소포화도의저하(JvSO2 �50%)가10분이상
지속되는빈도가더적었지만3개월및6개월예후는차이가없었다. 또한, 높은뇌관류압을유지한
환자군은수액치료를더많이받고승압제를더오래사용하기때문에급성호흡증후군이발생하는
비율이 5배증가하 다.17따라서, 외상환자에서는뇌관류압을 70 mmHg 이상으로유지하는것이
권고되지않는다.11 2010년미국진료지침에서는외상환자의뇌관류압권고안을차용하여뇌출혈환
자에서도동일한범위의뇌관류압을제시하게되지만, 앞에서살펴본것처럼뇌출혈환자를 상으
로시행된연구가아니므로구체적인뇌관류압의권고치를제시하기에는미흡하다. 중환자실에입
원할정도로혼수상태의뇌출혈환자에서뇌관류압을 80mmHg으로유지하는것이뇌산소분압이
더잘유지된다는연구는있으나전체뇌출혈환자로일반화하기에는더많은연구가필요하다.18
결론적으로뇌출혈환자에서특별히권고할수있는뇌관류압의범위는명확하지않다.
뇌압이상승한경우에는뇌압을낮추기위해다양한치료가시도되는데, 표적인것으로삼투압제
재(만니톨및고장성식염수), 과호흡법및저체온요법등이있다. 삼투압제재는투여되는약물에따
라삼투압의정도가다양하기때문에, 동일한삼투압정도를사용하여비교한연구를분석해보면,
만니톨은고장성식염수와 체로비슷한효과를보인다고알려져있다. 하지만최근시행된메타분
석에따르면, 뇌압을조절하는정도는고장성식염수가더우수하다.19뇌압상승이삼투압제재사용

202
CLINICAL RESEARCH CENTER FOR STROKE
으로도반응하지않는경우에는, 체온을33~35�C 로낮추는치료가시도될수있다. 뇌압조절에미치
는저체온치료의효과는 체로삼투압제제의효과와비슷하다고알려져있다.20일부연구에서는치
료적저체온요법이혈종주변의부종을감소시킨다는보고는있으나, 폐렴을포함한전신감염의비
율이상승하므로, 저체온요법의사용은환자개개인의상황에맞추어결정되어야한다21 .
1. 급성기뇌출혈환자는뇌압상승, 혈압조절, 기도삽관및기계호흡등의필요때문에집중치료실에
서치료및관찰하는것을권장하며한다. (근거수준III, 권고수준B)
2. 입원시 래스고우코마점수(GCS score) 가3-8점, 혹은임상적으로뇌탈출이의심되거나상당한
양의뇌실내출혈이나수두증이동반된경우에는선택적으로뇌압측정이필요할수있다.
(근거수준III, 권고수준B, 새로추가됨)
3. 수두증으로인해의식이저하된경우는뇌실배액술을시행할수있다
(근거수준III, 권고수준B, 새로추가됨)
4. 상승된뇌압의조절은간단한처치부터단계적으로적극적방법을고려한다. 우선환자의머리를
30�정도위로올리고, 통증및불안정한상태를보이는환자에서제한적으로진통제및진정제
사용을고려한다. (근거수준IV, 권고수준C)
5. 좀더적극적인뇌압조절이필요한경우는삼투요법(mannitol or hypertonic saline solution), 신경근
육차단 (neuromuscular blockade), 저체온요법 (hypothermia) 및과호흡요법 (hyperventilation) 등을
사용할수있다. (근거수준IV, 권고수준C)
1. Hong K-S, Bang OY, Kang D-W, Yu K-H, Bae H-J, Lee JS, et al. Stroke statistics in korea: Part i. Epidemiology
and risk factors: A report from the korean stroke society and clinical research center for stroke. J Stroke.
2013;15:2-20
2.Mokri B. The monro-kellie hypothesis: Applications in csf volume depletion. Neurology.2001;56:1746-1748
3.Guyot LL, Dowling C, Diaz FG, Michael DB. Cerebral monitoring devices: Analysis of complications. Acta

203
CLINICAL RESEARCH CENTER FOR STROKE
Neurochir Suppl.1998;71:47-49
4.Ziai WC, Torbey MT, Naff NJ, Williams MA, Bullock R, Marmarou A, et al. Frequency of sustained intracranial
pressure elevation during treatment of severe intraventricular hemorrhage. Cerebrovasc Dis. 2009;27:403-410
5.Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, et al. Early surgery versus
initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the
international surgical trial in intracerebral haemorrhage (stich): A randomised trial. Lancet. 2005;365:387-397
6.Bhattathiri PS, Gregson B, Prasad KS, Mendelow AD. Intraventricular hemorrhage and hydrocephalus after
spontaneous intracerebral hemorrhage: Results from the stich trial. Acta Neurochir Suppl. 2006;96:65-68
7.Clarke JL, Johnston SC, Farrant M, Bernstein R, Tong D, Hemphill JC, 3rd. External validation of the ich score.
Neurocrit Care. 2004;1:53-60
8.Hemphill JC, 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ich score: A simple, reliable
grading scale for intracerebral hemorrhage. Stroke. 2001;32:891-897
9.Hemphill JC, 3rd, Farrant M, Neill TA, Jr. Prospective validation of the ich score for 12-month functional
outcome. Neurology. 2009;73:1088-1094
10.Narayan RK, Kishore PR, Becker DP, Ward JD, Enas GG, Greenberg RP, et al. Intracranial pressure: To
monitor or not to monitor? A review of our experience with severe head injury. J Neurosurg. 1982;56:650-659
11.Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, et al. Guidelines for the
management of severe traumatic brain injury. Viii. Intracranial pressure thresholds. J Neurotrauma. 2007;24
Suppl 1:S55-58
12. Andrews BT, Chiles BW, 3rd, Olsen WL, Pitts LH. The effect of intracerebral hematoma location on the risk of
brain-stem compression and on clinical outcome. J Neurosurg. 1988;69:518-522
13. Qureshi AI, Geocadin RG, Suarez JI, Ulatowski JA. Long-term outcome after medical reversal of
transtentorial herniation in patients with supratentorial mass lesions. Crit Care Med. 2000;28:1556-1564
14. Anderson CS, Huang Y, Arima H, Heeley E, Skulina C, Parsons MW, et al. Effects of early intensive blood
pressure-lowering treatment on the growth of hematoma and perihematomal edema in acute intracerebral
hemorrhage: The intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT). Stroke.
2010;41:307-312
15. Kiening KL, Hartl R, Unterberg AW, Schneider GH, Bardt T, Lanksch WR. Brain tissue po2-monitoring in
comatose patients: Implications for therapy. Neurol Res. 1997;19:233-240

204
CLINICAL RESEARCH CENTER FOR STROKE
와파린(warfarin) 또는헤파린(heparin) 등의항응고제를사용하는환자에서뇌실질내출혈이발생하
을경우프로트롬빈시간 - 국제표준화치(prothrombin time-international normalized ratio, PT-INR) 또
는활성부분트롬보플라스틴시간(activated partial thromboplastin time, aPTT)의상승정도가혈종의
증가및예후와상관이있어빠른교정이중요하다.
16. Nordstrom CH, Reinstrup P, Xu W, Gardenfors A, Ungerstedt U. Assessment of the lower limit for cerebral
perfusion pressure in severe head injuries by bedside monitoring of regional energy metabolism.
Anesthesiology. 2003;98:809-814
17. Robertson CS, Valadka AB, Hannay HJ, Contant CF, Gopinath SP, Cormio M, et al. Prevention of secondary
ischemic insults after severe head injury. Crit Care Med. 1999;27:2086-2095
18. Ko SB, Choi HA, Parikh G, Helbok R, Schmidt JM, Lee K, et al. Multimodality monitoring for cerebral
perfusion pressure optimization in comatose patients with intracerebral hemorrhage. Stroke.
2011;42:3087-3092
19. Kamel H, Navi BB, Nakagawa K, Hemphill JC, 3rd, Ko NU. Hypertonic saline versus mannitol for the
treatment of elevated intracranial pressure: A meta-analysis of randomized clinical trials. Crit Care Med.
2011;39:554-559
20. Schreckinger M, Marion DW. Contemporary management of traumatic intracranial hypertension: Is there a
role for therapeutic hypothermia? Neurocrit Care. 2009;11:427-436
21. Kollmar R, Staykov D, Dorfler A, Schellinger PD, Schwab S, Bardutzky J. Hypothermia reduces
perihemorrhagic edema after intracerebral hemorrhage. Stroke. 2010;41:1684-1689
22. Schreckinger M, Marion DW. Contemporary management of traumatic intracranial hypertension: Is there a
role for therapeutic hypothermia? Neurocrit Care. 2009;11:427-436
23. Kollmar R, Staykov D, Dorfler A, Schellinger PD, Schwab S, Bardutzky J. Hypothermia reduces
perihemorrhagic edema after intracerebral hemorrhage. Stroke. 2010;41:1684-1689
2.4.1.2. 항응고제와관련된뇌실질내출혈의내과적치료Medical treatment of intracerebral hemorrhage in patients receiving anticoagulants

205
CLINICAL RESEARCH CENTER FOR STROKE
1. Protamine sulfate should be used to reverse heparin-associated ICH, with the dose depending on the
time from cessation of heparin (ASA: Class I, LOE B).
2. Patients with warfarin-associated ICH should be treated with intravenous vitamin K to reverse the effects
of warfarin and with treatment to replace clotting factors (ASA: Class I, LOE B).
3. Prothrombin complex concentrate, factor IX complex concentrate, and rFVIIa normalize the laboratory
elevation of the INR very rapidly and with lower volumes of fluid than FFP but with greater potential of
thromboembolism. FFP is another potential choice but is associated with greater volumes and much
longer infusion times (ASA: Class IIb, LOE B).
항응고제치료중생긴뇌실질내혈종의치료에 한무작위전향적연구는없다. 각각의사정에따라
적절한길항제를사용하게되는데, 헤파린(heparin) 사용후에발생한출혈의경우헤파린의길항제인
프로타민(protamine sulfate)를투여하며, 헤파린 100U 당 1mg의용량이추천되고있다. 빠른주입은
전신저혈압을유발할수있어주의하여야하며, 5mg/min의속도를넘지않고총용량이50mg을넘지
않도록주의하여야한다. 와파린사용후에발생한경우에는길항제인비타민K(vitamin K)를약10mg
용량을정맥주사한다.1정맥주사시에빈도는낮으나아나필락시스(anaphylaxis)의위험이있어피하
로주사하여위험을줄일수있다는보고가있다.2일반적으로 INR을정상화하는데6시간이상걸리
므로, 단독으로사용하지는않는다.3모든항응고제사용과관련된출혈에는혈액응고인자의보충을
시도하게되는데, 가장많이사용되는것이신선동결혈장(fresh frozen plasma)이다. 신선동결혈장은
비타민K보다작용시간이빠르지만추천용량인15-20mL/kg을사용하려면용적이매우커서모두수
혈하는데시간이지체되고심장과부하에의한심부전의위험이있는단점이있기도하다.4또한신선
동결혈장을주사하더라도여전히혈중응고인자 IX의농도가낮을수있음을주의하여야한다.5프로
트롬빈복합제농축액(prothrombin complex concentrate)은비타민K 의존성응고인자(Factor II, VII, X)
를, 응고인자 IX 복합체농축액(factor IX complex concentrate)은응고인자 II, VII, IX, X을포함하고있는수
혈제제로신선동결혈장에비해응고이상의교정이빠르지만혈전색전증의위험이있음을주의하여
야한다.6, 7현재국내에서는잘사용하지않으나재조합활성응고인자VII는와파린복용환자에서INR

206
의정상화를빠르게하여8뇌실질내출혈치료에서효과가있다는보고들이있다.9-11
CLINICAL RESEARCH CENTER FOR STROKE
1. 헤파린으로인한뇌실질내출혈환자에서헤파린을즉시중단하고, 프로타민(protamine sulfate)를
사용하여헤파린의효과를중화시켜주는것을고려할수있다. (근거수준IV, 권고수준C)
2. 와파린(warfarin)으로인한뇌실질내출혈환자에서와파린을즉시중단하고비타민K를정주하여
와파린의효과를중화시키고, 응고인자들을보충할수있는치료를함께사용하는것을고려할수
있다. (근거수준IV, 권고수준C)
3. 프로트롬빈복합제농축액, 응고인자 IX 복합체농축액, 재조합활성응고인자VII는신선동결혈장
에비하여적은양의용적으로도 INR를빨리교정할수있어, 뇌실질내출혈환자에서응고이상을
교정하기위해사용할수있으나혈전색전증의발생위험이있다. 다른치료방법으로신선동결혈장
투여가추천될수있으나, 교정을위해정주되는용적이크고, 주입속도가느린단점이있다. (근거
수준IV, 권고수준C)
1. Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oral anticoagulant therapy:
Current practices and unresolved questions. Stroke. 2006;37:256-262.
2. Raj G, Kumar R, McKinney WP. Time course of reversal of anticoagulant effect of warfarin by intravenous
and subcutaneous phytonadione. Arch Intern Med. 1999;159:2721-2724.
3. Guidelines on oral anticoagulation: Third edition. Br J Haematol.1998;101:374-387.
4. Schulman S. Clinical practice. Care of patients receiving long-term anticoagulant therapy. NEngl J Med.
2003;349:675-683.
5. Makris M, Greaves M, Phillips WS, Kitchen S, Rosendaal FR, Preston EF. Emergency oral anticoagulant
reversal: The relative efficacy of infusions of fresh frozen plasma and clotting factor concentrate on
correction of the coagulopathy. Thromb Haemost. 1997;77:477-480.
6. Lankiewicz MW, Hays J, Friedman KD, Tinkoff G, Blatt PM. Urgent reversal of warfarin with prothrombin
complex concentrate. J Thromb Haemost. 2006;4:967-970.

207
CLINICAL RESEARCH CENTER FOR STROKE
7. Baker RI, Coughlin PB, Gallus AS, Harper PL, Salem HH, Wood EM. Warfarin reversal: Consensus
guidelines, on behalf of the australasian society of thrombosis and haemostasis. Med J Aust.
2004;181:492-497.
8. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant
human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
9. Mayer SA, Brun NC, Begtrup K, Broderick J, Davis S, Diringer MN, Skolnick BE, Steiner T. Recombinant
activated factor vii for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
10. Freeman WD, Brott TG, Barrett KM, Castillo PR, Deen HG, Jr., Czervionke LF, Meschia JF.
Recombinant factor viia for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage.
Mayo Clin Proc. 2004;79:1495-1500.
11. Brody DL, Aiyagari V, Shackleford AM, Diringer MN. Use of recombinant factor VIIa in patients with
warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
고혈압은뇌출혈의중요한위험인자이고, 뇌출혈발생급성기에는 개일시적으로혈압이증가한
다. 뇌출혈발생직후의고혈압은혈종의크기를증가시킬가능성이있어조절이필요하며, 구체적인
혈압조절의범위에 해시행된최근연구들이있다.
2.4.1.3. 뇌실질내출혈후혈압조절Blood pressure management after intracerebral hemorrhage
개정: 2014.1
1. 뇌실질내출혈환자의급성기치료에서의혈압조절에 해다음과같은지침이추천된다. (근거수준
III, 권고수준B)
1. 수축기혈압이�200mmHg 이거나평균동맥압이�150mmHg이면, 매5분간격으로혈압을측정하면
서정맥주입혈압강하제를통하여혈압을적극적으로떨어뜨린다.
208
기존의근거와새로추가된연구를근거를종합할때개정의필요성에 한근거는다음과같다. 뇌출
혈환자에서혈압의조절범위에관해새로시행된무작위배정임상연구가추가되었고, 일부연구결과
를반 하여2010년미국뇌졸중학회의뇌출혈진료지침이개정되었다. 지난진료지침에서는2007년7
월31까지발표된연구를기반으로하 으므로, 그이후에새롭게발표된연구결과는문헌검색을통하
여추가하 다(Supplement 1).
급성기뇌출혈환자의혈압조절에관한기존의권고사항은 부분소규모관찰연구로부터얻어진결
과에근거한다. 초기연구에서는혈종의증가와혈압과의관련성에 해주목하 는데, 입원당시측정
된수축기혈압이200 mm Hg 이상이면, 5일후시행한CT검사에서혈종의크기가증가되는환자가더
많았다는연구결과가있어수축기혈압을200 mm Hg 이하로유지할것을권고하 다.1.뇌출혈환자들
2. 수축기혈압이�180mmHg 이거나, 평균동맥압이�130mmHg이면서뇌압증가의증거가있거나의
심되면, 뇌압감시장치를통하여뇌관류압을�60-80mmHg로유지하면서간헐적또는지속적인정맥
주입혈압강하제를통하여혈압을떨어뜨린다.
3. 수축기혈압이�180mmHg 이거나, 평균동맥압이�130mmHg이면서뇌압증가의증거가없으면, 15
분간격으로환자를임상적으로평가하면서간헐적또는지속적인정맥주입혈압강하제를통하여평
균동맥압을110mmHg, 혈압을160/90mmHg에맞추어적절하게조절한다.
CLINICAL RESEARCH CENTER FOR STROKE
1. ASA (2010)
1. Until ongoing clinical trials of BP intervention for ICH are completed, physicians must manage BP on
the basis of the present incomplete efficacy evidence. Current suggested recommendations for
target BP in various situations are listed in Table 6 and may be considered (Class IIb; Level of
Evidence: C). (Unchanged from the previous guideline)
2. In patients presenting with a systolic BP of 150 to 220 mm Hg, acute lowering of systolic BP to 140
mm Hg is probably safe (Class IIa; Level of Evidence: B). (New recommendation)

209
CLINICAL RESEARCH CENTER FOR STROKE
의상당수는고혈압을가지고있고, 고혈압환자에서뇌혈류의자동조절능이유지되는혈압의범위는
일반인에비해더높은범위로편위되어있는점을고려하면, 급성기에혈압을낮추는것이뇌출혈환
자에서항상안전한가에관해서는의문이있어왔다. 따라서초기권고사항에서는혈압강하치료의안
전성을고려하여, 고혈압병력이있는환자에서는수축기혈압 180-185mmHg 이하, 이완기혈압 105-
110mmHg 이하를권고하 고, 고혈압병력이없는환자는수축기혈압160-170mmHg 이하, 이완기혈
압95-100mgHg 이하로유지할것을추천하 다.2 1997년과2007년에발표된미국뇌졸중학회의진료지
침에서는위권고사항을평균동맥압으로표기를변형하여, 평균혈압을130mm Hg 이하로유지하도록
권고하고있다.3, 4
2007년미국뇌졸중학회의진료지침이발표된이후, 급성기뇌출혈환자에서혈압조절과예후와의관
련성에관한새로운연구가발표되었다. 2008년에발표된INTERACT (INTensive blood pressure reduction
in Acute cerebral hemorrhage Trial)연구는증상발생6시간이내의급성기뇌출혈환자중수축기혈압이
150mm Hg - 220 mm Hg 범위로증가된사람들을 상으로하여, 수축기혈압140mm Hg 미만을목표로
조절하는경우(중등도조절군, 203명)와180mm Hg 미만을목표로조절하는경우(경도조절군, 201명)의
혈종증가와부작용을비교한예비연구다.5무작위배정24시간후에뇌CT를촬 하여혈종의크기증
가정도를비교하 을때, 경도조절군에서는평균혈종의크기가36.3% 증가하 으나, 중등도조절군
에서는13.7% 증가하여혈압을적극적으로조절하는것이혈종증가를억제함을보 다(P =0.04). 한편,
두군간에신경학적악화의빈도는차이가없었고, 3개월째사망률및수정바텔지수(mRS) 3-5의심한
기능장애가동반된환자의비율은두군간에차이가없었다. 이처럼급성기에수축기혈압을 140mm
Hg 이하로조절하는것이비교적안전하다는것은확인할수있었으나, 두군간의혈종크기의차이는
1.7cc 에불과하여, 적극적혈압조절의실용성에 해서는의문이남게되었다. 또한 부분의환자(중
등도조절군[85%] 및경도조절군[95%])에서혈압조절을위해사용된약제가일반적으로혈압조절의
목적으로는잘사용하지않는이뇨제와혈관확장제여서, 실제임상상황과는많은차이가난다. 이러한
제한점에도불구하고, 위연구는급성기뇌출혈환자에서혈압조절의안정성을보여준의의가있다. 이
보다실제진료상황을더잘반 한연구는2009년에발표된ATACH (Antihypertensive Treatment of Acute
Cerebral Hemorrhage) 연구이다.6이연구도역시발생6시간이내, 수축기혈압이170 mm Hg 이상인급
성기뇌출혈환자들에서, Nicardipine 정맥주사를통해수축기혈압을각각 170-200 mm Hg (18명), 140-
170mm Hg (20명), 110-140mm Hg (22명)의세가지기준에맞춰24시간유지하고, 그유용성과부작용의
정도를72시간동안비교하 다. 일차변수는치료의용이도와72시간까지의안전성여부 는데, 부작
210
CLINICAL RESEARCH CENTER FOR STROKE
용의발생빈도는수축기혈압을140 ~ 170 mmHg으로조절한환자군에서두명, 수축기혈압을110-140
mmHg 으로조절한환자군에서세명이었으나, 어느혈압군에서도투약중단이필요할만큼심한부작
용은발생하지않았다. 따라서, 급성기뇌출혈환자에서nicardipine 을이용한혈압조절은안전하다고
할수있다.6. 하지만, 위연구는각혈압조절군에배정된환자가18-22명에불과하여통계적유의성을
검정하기에는적절하지않으므로, 임상적의의를확인하기위해제 3상임상시험이진행중이다
(ATACH-II).7
최근급성기뇌출혈환자에서혈압강하의효과를연구한 규모제3상임상시험인 INTERACT II 연구
결과가발표되었다.8발생6시간이내의급성기뇌출혈환자2839 명을 상으로연구가이루어졌는데,
초기수축기혈압이150 mm Hg 과220 mm Hg 사이일경우, 적극적으로혈압을조절하는치료군(1시간
이내에수축기혈압�140 mm Hg 도달을목표로조절)과기존진료지침치료군(수축기혈압�180 mm
Hg 도달을목표로조절)으로임의배정되었다. 항고혈압제제의선택은치료하는의료진의판단에맡
겨졌다. 일차결과변수는3개월째사망또는주요장애 (수정바텔지수3-6점) 의정도 다. 적극적치료
군에서는사망또는주요장애의정도가52%로, 표준치료군의55.6%에비해더적게발생하는경향성
은보 으나통계적차이를입증하지는못했다. (우도비0.87; 95% 신뢰구간, 0.75-1.01; P=0.06). 하지만,
수정바텔지수의서열분석(ordinal analysis)을이차변수로하여분석하면, 적극적치료군에서수정바텔
지수가불량할확률이더낮았고 (우도비, 0.87; 95% 신뢰구간, 0.77-1.00; P=0.04), 안전성정도는두군에
서차이가없었다. 혈종크기의증가정도는두군에서거의차이가없었고, 평균혈종의부피차이는
1.4cc 정도로미미하여, 적극적치료군에서어떠한기전으로예후가좋게되었는지는명확하지않다.
한편, 급성기에혈압을강하시키는데있어가장우려되는점은혈종주변에존재할지도모르는반음
로인해혈압을감소시킬때허혈손상이발생하는것이다. 이점을명확하게하기위해혈압감소에
따른뇌혈류를측정하는무작위배정임상연구가시행되었다.9연구에포함된환자들은18세이상, 발
생 24시간이내의급성기출혈환자로, 수축기혈압이 150 mm Hg 이상이었다. 환자들은수축기혈압
150 mm Hg 목표군(39명)과180 mm Hg 이하목표군(36명)으로나뉘어서혈압조절이이루어졌고, 두군
간에혈종주위뇌혈류량의차이를비교하기위해관류CT 상촬 이행해졌다. 연구결과두환자군에
서혈압감소의정도와혈종주위뇌혈류와는관련이없어, 급성기뇌출혈환자에서적극적인혈압강하
치료를하더라도안전함을보여주었다.
이러한결과를바탕으로급성기뇌출혈환자에서수축기혈압을140 mm Hg 이하로낮추는것은안전
하며, 기능적예후에관해서도도움이될가능성이있다.
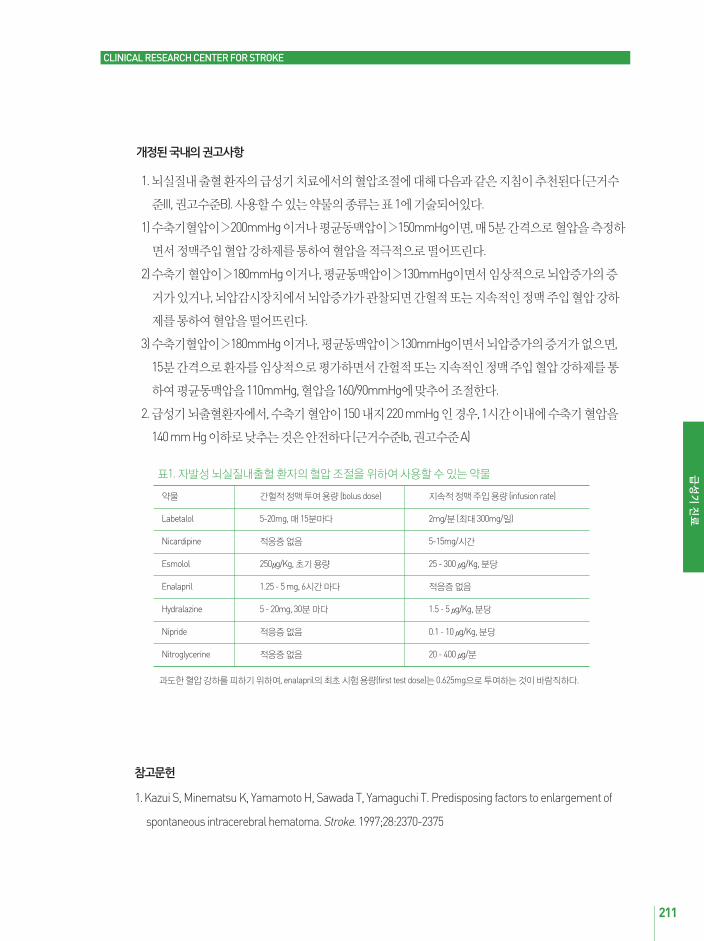
211
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌실질내출혈환자의급성기치료에서의혈압조절에 해다음과같은지침이추천된다(근거수
준III, 권고수준B). 사용할수있는약물의종류는표1에기술되어있다.
1) 수축기혈압이�200mmHg 이거나평균동맥압이�150mmHg이면, 매5분간격으로혈압을측정하
면서정맥주입혈압강하제를통하여혈압을적극적으로떨어뜨린다.
2) 수축기혈압이�180mmHg 이거나, 평균동맥압이�130mmHg이면서임상적으로뇌압증가의증
거가있거나, 뇌압감시장치에서뇌압증가가관찰되면간헐적또는지속적인정맥주입혈압강하
제를통하여혈압을떨어뜨린다.
3) 수축기혈압이�180mmHg 이거나, 평균동맥압이�130mmHg이면서뇌압증가의증거가없으면,
15분간격으로환자를임상적으로평가하면서간헐적또는지속적인정맥주입혈압강하제를통
하여평균동맥압을110mmHg, 혈압을160/90mmHg에맞추어조절한다.
2. 급성기뇌출혈환자에서, 수축기혈압이150 내지220 mmHg 인경우, 1시간이내에수축기혈압을
140 mm Hg 이하로낮추는것은안전하다(근거수준Ib, 권고수준A)
1. Kazui S, Minematsu K, Yamamoto H, Sawada T, Yamaguchi T. Predisposing factors to enlargement of
spontaneous intracerebral hematoma. Stroke. 1997;28:2370-2375
약물 간헐적정맥투여용량 (bolus dose) 지속적정맥주입용량 (infusion rate)
Labetalol 5-20mg, 매15분마다 2mg/분 (최 300mg/일)
Nicardipine 적응증없음 5-15mg/시간
Esmolol 250μg/Kg, 초기용량 25 - 300 μg/Kg, 분당
Enalapril 1.25 - 5 mg, 6시간마다 적응증없음
Hydralazine 5 - 20mg, 30분마다 1.5 - 5 μg/Kg, 분당
Nipride 적응증없음 0.1 - 10 μg/Kg, 분당
Nitroglycerine 적응증없음 20 - 400 μg/분
과도한혈압강하를피하기위하여, enalapril의최초시험용량(first test dose)는0.625mg으로투여하는것이바람직하다.
표1. 자발성뇌실질내출혈환자의혈압조절을위하여사용할수있는약물

212
2. Brott T, Reed RL. Intensive care for acute stroke in the community hospital setting. The first 24 hours. Stroke.
1989;20:694-697
3. Broderick JP, Adams HP, Jr., Barsan W, Feinberg W, Feldmann E, Grotta J, et al. Guidelines for the
management of spontaneous intracerebral hemorrhage: A statement for healthcare professionals from a
special writing group of the stroke council, american heart association. Stroke. 1999;30:905-915
4. Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, et al. Guidelines for the management of
spontaneous intracerebral hemorrhage in adults: 2007 update: A guideline from the american heart
association/american stroke association stroke council, high blood pressure research council, and the quality
of care and outcomes in research interdisciplinary working group. Stroke. 2007;38:2001-2023
5. Anderson CS, Huang Y, Wang JG, Arima H, Neal B, Peng B, et al. Intensive blood pressure reduction in acute
cerebral haemorrhage trial (INTERACT): A randomised pilot trial. Lancet Neurol. 2008;7:391-399
6. Antihypertensive treatment of acute cerebral hemorrhage. Crit Care Med. 2010;38:637-648
7. Qureshi AI, Palesch YY. Antihypertensive treatment of acute cerebral hemorrhage (ATACH) II: Design,
methods, and rationale. Neurocrit Care. 2011;15:559-576
8. Anderson CS, Heeley E, Huang Y, Wang J, Stapf C, Delcourt C, et al. Rapid blood-pressure lowering in patients
with acute intracerebral hemorrhage. N Engl J Med. 2013;368:2355-2365
9. Butcher KS, Jeerakathil T, Hill M, Demchuk AM, Dowlatshahi D, Coutts SB, et al. The intracerebral
hemorrhage acutely decreasing arterial pressure trial. Stroke. 2013;44:620-626
CLINICAL RESEARCH CENTER FOR STROKE
경련발작은뇌출혈이후에중요한합병증중의하나이다. 허혈뇌졸중보다는뇌출혈환자에서경련
발작이더흔하고, 주로증상발생48시간이내에발생한다고알려져있다. 경련발작은임상양상의악
화와뇌중심선(midline)의편위를가져오는것으로알려져있으나, 원인-결과관계는불명확하다.
2.4.1.4. 경련의예방및치료Seizure prevention and treatment
개정: 2014.1

213
CLINICAL RESEARCH CENTER FOR STROKE
기존의근거와새로추가된연구를근거를종합할때개정의필요성에 한근거는다음과같다. 뇌
출혈환자에서예방적항경련제의효과에관해기존에임상연구를새롭게분석한이차분석연구결
과가발표되었고, 그결과를반 하여2010년미국뇌졸중학회의뇌출혈진료지침이개정되었다. 또
한, 뇌출혈환자에서발생하는경련의빈도에관한관찰연구가발표되고, 최근예방적항경련제의
효과에 한무작위배정임상시험이발표되어이를근거로하여부분개정의필요성이발생하 다.
지난진료지침에서는2007년7월31까지발표된연구를기반으로하 으므로, 그이후에새롭게발
표된연구결과는문헌검색을통하여추가하 다(Supplement 1).
1. 뇌출혈후경련이발생하면적절한항경련제를사용해야한다. (근거수준Ib, 권고수준A)
2. 엽상출혈직후단기간의항경련제의사용은조기경련의발생을줄일수있어사용이추천된다.
(근거수준IIa, 권고수준B)
3. 뇌출혈시에항경련제를사용하는경우, 재발이없으면줄여서끊도록한다. 재발이있는경우만성
치료요법을고려할수있다(근거수준IV, 권고수준C).
1. ASA (2010)
1. Clinical seizures should be treated with antiepileptic drugs (Class I; Level of Evidence: A). (Revised
from the previous guideline)
2. Continuous electroencephalogram (EEG) monitoring is probably indicated in ICH patients with
depressed mental status out of proportion to the degree of brain injury (Class IIa; Level of Evidence: B).
3. Patients with a change in mental status who are found to have electrographic seizures on EEG
should be treated with antiepileptic drugs (Class I; Level of Evidence: C).
4. Prophylactic anticonvulsant medication should not be used (Class III; Level of Evidence:B). (New
recommendation)

214
CLINICAL RESEARCH CENTER FOR STROKE
뇌출혈이후의경련발작의발생빈도는경련의정의와연구 상환자에따라매우다양하다. 하지만,
출혈발생1주이내의환자에서경련발작의발생률은 체로5% ~ 19% 로보고되어있다.1-4임상적으
로확인되는경련보다뇌파로만확인할수있는전기적경련은약4배가량더흔한것으로알려져있
다3, 5 또한, 전기적경련이있는환자의약 39% 는비경련성간질중첩증(non-convulsive status
epilepticus)인것으로알려져있다.
뇌출혈이후의경련발작의위험인자는엽상출혈1,2피질을침범한경우1, 혈종의팽창3등이다. 비록경
련발작이종괴효과나신경학적증상의악화와관련된다는보고가있지만, 원인-결과관계는아직명
확하지않다.5 경련이발생하더라도신경학적예후가악화된다는직접적인결과도확실하지않다.1,3
따라서, 예방적항경련제의사용이반드시필요할지는의문이다.
최근, CHANT 연구의위약투약군을 상으로이차분석한연구결과가발표되었는데, 항경련제를예
방적으로투여받은환자들에서90일째신경학적예후가불량(수정바텔지수5 or 6)할위험도가6.8이
어서, (95% 신뢰구간2.2-21.3), 항경련제를예방적으로사용하는것에 한안전성에 한문제가
두되었다.6하지만, 78% 에해당하는 부분의환자가페니토인을투여받았으므로, 그보다안전성이
입증된새로개발된항경련제제로도비슷한정도로불량한결과가나올지는확실하지않다. 최근발
프로산( valproic acid)을이용하여뇌출혈후경련을예방하고자한연구에서, 치료군(36명)은위약투여
군(36명)에비교하여경련발생률의차이가없었다.7하지만, 발프로산을투약받은환자군에서는이전
연구와는다르게신경학적예후가나쁘지않았다. 따라서, 페니토인을제외한다른항경련제를사용
하는것이신경학적예후를나쁘게하는지에 해서는아직근거가명확하지는않다.
결론적으로, 뇌출혈이후임상적인경련발작은아마도신경학적악화와직접관련되지는않을것으
로보인다. 또한, 뇌출혈이후항경련제의예방적치료가신경학적예후가불량한것과관련될수있지
만, 페니토인을제외한새로운항경련제에서도비슷한정도로 향이있을지는불분명하다. 따라서,
항경련제를예방적으로투여하는것은일반적으로권고되지않고, 각환자별로위험도와치료에따
른효과를고려하여결정하여야하며, 임상적경련이발생하면적절한항경련제를사용하여조절하
는것이필요하다.

215
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌출혈이후에발생한경련발작은적절한항경련제를사용하여치료하도록한다.
(근거수준Ib, 권고수준A)
2. 뇌출혈환자에서의식저하를설명할만한원인이뚜렷하지않으면, 전기적경련의가능성을배제
하기위해(연속) 뇌파촬 이필요하며, 전기적경련이확인되면항경련제를이용하여치료하는것
이바람직하다. (근거수준III, 권고수준B)
3. 예방적인항경련제의사용은각환자의경련발작의위험도와항경련제의부작용을고려하여개별
적으로결정하여야한다. 경련발작의위험도를고려하지않고, 일괄적으로모든환자에게항경련
제를사용하는것은추천되지않는다. (근거수준IIa, 권고수준B)
1. De Herdt V, Dumont F, Henon H, Derambure P, Vonck K, Leys D, et al. Early seizures in intracerebral
hemorrhage: Incidence, associated factors, and outcome. Neurology.2011
2. Alberti A, Paciaroni M, Caso V, Venti M, Palmerini F, Agnelli G. Early seizures in patients with acute stroke:
Frequency, predictive factors, and effect on clinical outcome. Vasc Health Risk Manag. 2008;4:715-720
3. Claassen J, Jette N, Chum F, Green R, Schmidt M, Choi H, et al. Electrographic seizures and periodic
discharges after intracerebral hemorrhage. Neurology. 2007;69:1356-1365
4. Passero S, Rocchi R, Rossi S, Ulivelli M, Vatti G. Seizures after spontaneous supratentorial intracerebral
hemorrhage. Epilepsia. 2002;43:1175-1180
5. Vespa PM, O'Phelan K, Shah M, MirabelliJ, Starkman S, Kidwell C, et al. Acute seizures after intracerebral
hemorrhage: A factor in progressive midline shift and outcome. Neurology. 2003;60:1441-1446
6. Messe SR, Sansing LH, Cucchiara BL, Herman ST, Lyden PD, Kasner SE. Prophylactic antiepileptic drug use
is associated with poor outcome following ich. Neurocrit Care. 2009;11:38-44
7. Gilad R, Boaz M, Dabby R, Sadeh M, Lampl Y. Are post intracerebral hemorrhage seizures prevented by anti-
epileptic treatment? Epilepsy Res. 2011;95:227-231
216
CLINICAL RESEARCH CENTER FOR STROKE
뇌출혈의이상적인치료의목적은혈종의팽창을막고, 초기신경학적결손의적절한치료를통해진
행하는신경학적손상을최소화하는데있다. 수술의적응증에해당한다면, 수술자체에의한직접적
인뇌손상을최소화하면서혈종의제거를고려해볼수있다. 어떤경우에는출혈의위치와크기에따
라내과적치료를포함한보존적인치료가수술보다우선할수있다. 수술에관해서도다양한수술법
들이개발되고시도되고있다. 따라서이런관점에서명확한임상진료지침이필요하다.
2.4.2. 뇌실질내출혈의수술적치료Surgical treatment of intracerebral hemorrhage
1. AHA/ASA27)
1) Recommendation for the management of IVH
i. Although intraventricular administration of recombinant tissue-type plasminogen activator (tPA)
in IVH appears to have a fairly low complication rate, efficacy and safety of this treatment is
uncertain and is considered investigational (Class IIb; LOE B).
개정: 2014.1
1. 뇌탈출(cerebral herniation)이의심되거나급격한의식의악화가있는경우조기에개두술을통한혈
종제거를고려할수있다. (근거수준IV, 권고수준C)
2. 의식수준이 래스고우혼수척도(GCS) 9-12 사이에있고, 표면에서1 cm 이내에위치한엽상출혈
(lobar hemorrhage)의경우개두술을고려한다. (근거수준IIb, 권고수준B)
3. 직경3 cm 이상이거나뇌간압박또는수두증의증상이있는소뇌출혈의경우개두술이권장된다.
(근거수준IIb, 권고수준B)
4. 심부에위치한출혈의경우비개두술적수술을고려할수있다. (근거수준IV, 권고수준C)
5. 뇌실내출혈의경우뇌실천자(ventricular puncture)를통한혈전용해술(thrombolysis)을고려할수
있다. (근거수준IV, 권고수준C)
217
CLINICAL RESEARCH CENTER FOR STROKE
2) Recommendations for clot removal
2. The Japan Stroke Society (Japan) (http://www.jsts.gr.jp/jss08.html [Japanese, translated])
i. For most patients with ICH, the usefulness of surgery is uncertain (Class IIb; LOE C). Specific
exceptions to this recommendation follow
ii. Patients with cerebellar hemorrhage who are deteriorating neurologically or who have
brainstem compression and/or hydrocephalus from ventricular obstruction should undergo
surgical removal of the hemorrhage as soon as possible (Class I; LOE B). Initial treatment of
these patients with ventricular drainage alone rather than surgical evacuation is not
recommended (Class III; LOE C).
iii. For patients presenting with lobar clots �30 mL and within 1 cm of the surface, evacuation of
supratentorial ICH by standard craniotomy might be considered (Class IIb; LOE B).
iv. The effectiveness of minimally invasive clot evacuation utilizing either stereotactic or
endoscopic aspiration with or without thrombolytic usage is uncertain and is considered
investigational (Class IIb; LOE B).
v. Although theoretically attractive, no clear evidence at present indicates that ultra-early removal
of supratentorial ICH improves functional outcome or mortality rate. Very early craniotomy may
be harmful due to increased risk of recurrent bleeding (Class III; LOE B).
Surgery is not indicated for patients with small amount of hematoma less than 10 ml or with
mild neurologic deficits (Grade D). There is no evidence for clot removal for patients with level of
consciousness with Japan Coma Scale III-300 (Grade C2).
Putaminal hemorrhage: Surgery is considered for putaminal hemorrhage with moderate
neurologic deficits or high grade of compression due to hematoma over 30 ml (Grade C1).
Especially, stereotactic clot removal is recommended in the case accompanied by level of
consciousness with Japan Coma Scale II-20~30 (Grade B).
Thalamic hemorrhage: There is no evidence for clot removal as an acute management (Grade
C2). For severe ventricular enlargement as a result of ventricular rupture, ventricular drainage
may be considered (Grade C1).
Subcortical hemorrhage: Surgery may be considered for hematoma located in 1 cm or less in
depth from cortical surface (Grade C1). Craniotomy is recommend as a surgical method (Grade C1)
Cerebellar hemorrhage: Surgery is indicated when there is neurologic deterioration or
1)
2)
3)
4)
5)
218
CLINICAL RESEARCH CENTER FOR STROKE
1. 개두술 혈종제거
다기관임상연구인STICH (the International Surgical Trial in Intracerebral Hemorrhage)21)는 1995년시
작되어8년간107개기관에서1033명의환자를무작위배당하여연구가진행되었으며, 2005년그결
과가발표되었다. 연구에포함된기준은1) 출혈발생후72시간이내에무작위배정되었고, 96시간이
내에수술을받은경우2) 장경이2 cm 이상의혈종3) 글래스고우혼수척도가5점이상의경우였다.
무작위는조기수술군과신경외과의사가수술의이득을확신할수없어초기내과치료군의두군으
로배정되었다.
이연구의일차목표점(primary end point)은 6개월시점의확장글래스고우결과척도(extended
3. European Stroke Initiative (EUSI, Europe)36)
hydrocephalus due to compression of brain stem in the case of cerebellar hemorrhage with 3
cm or longer in maximal diameter (Grade C1).
Brain stem hemorrhage: There is no evidence for clot removal in the acute stage of brain stem
hemorrhage (Grade C2). Ventricular drainage may be considered when the ventricular hemorrhage
which results from brain stem hemorrhage is main with enlarged ventricles (Grade C1).
IVH in adults: Evaluation of the cause of IVH is desirable when vascular abnormality is suspected
(Grade C1). Ventricular drainage is considered when acute hydrocephalus is suspected (Grade C1).
6)
7)
Consider craniotomy if there is deterioration in consciousness (from GCS level of between 12 and
9 to 8 or lower), if the ICH is superficial (the clot is subcortical≤1cm from the surface and does
not reach deep basal ganglia) or if it is located in the cerebellum (Level C recommendation).
Deep-seated haematomas do not benefit from craniotomy. Stereotaxic aspiration may be
considered, especially if mass effect is present (Class IV evidence).
External ventricular drainage (EVD) for hydrocephalus can be ventricular or via the lumbar route
if it is a communicating type of hydrocephalus. Lumbar drainage is definitely contra-indicated
with all types of obstructive hydrocephalus or if the aetiology is in doubt (Class IV evidence).
Intraventricular thrombolysis trials may be considered if an EVD becomes necessary but not in
infants (Class IV evidence).
1)
2)
3)
4)

219
CLINICAL RESEARCH CENTER FOR STROKE
Glasgow Outcome Scale)이었고, 이차목표점(secondary end point)은 6개월째사망률, 수정랜킨지수,
바텔지수(Barthel Index) 다. 506명의환자가조기수술군에, 530명의환자가알려진모든변수가일
치하는초기내과치료군으로배정되었다. 치료의향분석법(intention-to-treat analysis)에서 96기간이
내의조기수술군은6개월째예후를이분화한확장 래스고우결과척도에서2.3%의이득을보 으
나, 통계적으로유의하지않았다. 6개월째사망률[조기수술군의절 이득(absolute benefit) 1.2%
(-4.9% to 7.2%)], 수정랜킨지수[조기수술군의절 이득 4.7% (-1.2% to 10.5%)], 바텔지수[조기수술군
의절 이득4.1% (-1.4% to 9.5%)] 역시통계적으로유의하지않았다. 그러나, 초기내과치료군의26%
가재출혈, 신경학적인악화의이유로결국수술군으로이동하 고, 이환자중85%에서개두술이시
행되었다. 반면에조기수술군의 75%에서개두술이, 나머지는여러최소침습수술이시행되었다.
96%의환자에서6개월째분석이가능하 다. 추가로연령, 래스고우혼수척도, 혈종의위치및양,
피질면에서의거리, 수술방법, 반신마비또는실어증의중등도, 추가적인섬유소용해제의사용여
부, 참가국가의하위집단분석(subgroup analysis)이추가로시행되었는데, 이역시두군간에통계적
으로차이를보이지않았다. 그러나, 래스고우혼수척도가9점에서12점사이이고, 혈종이피질면
에서1 cm 이내에위치한엽상출혈의경우통계적인유의성을보이지는않았으나, 개두술에의한효
과가있는것으로나타났다. 이하위집단분석의결과에따라표층에위치하는엽상출혈의경우조
기수술이초기내과치료군에비해효과가있을것이라는가정하에 STICH II 연구가시작되었다.
STICH II 연구22)에는1) 전산화단층촬 에서피질면에서1 cm 이내에위치하며, 10-100 ml의자발성
엽상출혈 2) 발병시점에서부터 48시간이내 3) 래스고우혼수척도에서최상의운동점수(motor
score)가5점또는6점이고, 최상의개안점수(eye score)가2점이상인경우의환자601명을 상으로
하여, 조기수술군과초기내과치료군의두군으로무작위배정하 다. 이환자들중에서291명의환
자가무작위배정12시간이내에조기혈종제거술을받았고, 286명의환자는초기내과치료군에배
정되어치료를받았다. 이연구의초기목표점은6개월째확장 래스고우결과척도를이분화한좋
은결과와나쁜결과의예후기반결과 다. 전체적으로조기수술군의 59%가, 초기내과치료군의
62%가6개월째나쁜결과를보 으나, 통계적으로두군간의차이는없었다. 연구의이차목표점이
사망률에서는조기수술군이사망률의감소를보 으나, 이역시통계학적유의성은없었다. 그러나,
하위집단분석에서 래스고우혼수척도9점에서12점사이의하위집단의환자에서조기수술의경
우사망률에서51%의통계적으로유의한효과를나타냈다. 이에따라STICH II 연구는조기수술군에
서6개월째합병율과유병율에서효과를보이지는못하 지만뇌실내출혈을동반하지않는표재성
일차성뇌출혈환자에서작지만임상적으로적절한장점이있을수도있을것이라는결론을내렸다.
그러나, 이연구에서도초기내과치료군에서조기수술군으로많은환자가이동하여, 62명(21%)의환
자가초기내과치료중악화되어수술을받았다. 두군간의이동한환자들은좋지않은결과를보이기

220
CLINICAL RESEARCH CENTER FOR STROKE
는하 지만, 이러한치료의향분석법에서는두군간의이동이조기수술군의효과를상쇄할수있는
결과를나타낼수도있다는비판이제기되었다..
일차성뇌출혈에서수술의효과에 한부정적인결과를나타내는다른작은무작위 조군연구들
이발표되었다12,26,45). 이결과들에서는천막상부의뇌출혈에서일차성뇌출혈에 한수술적치료
가예후를향상시키는데실패하 다. Teernstra 등39)은STICH 연구를포함한9개의천막상부의일차
성뇌출혈에 한무작위 조군연구들의메타분석에서수술적치료가장점을가지고있다는합리
적인증거를찾아내지못하 다. 반면에, 천막상부피질하또는피각부의30 ml이상의뇌출혈에 해
출혈발생8시간이내에수술또는내과적치료로108명의환자를무작위배분한연구에서는수술한
군에서 1년째 래스고우혼수지수에서좋은회복(good recovery) 또는중등도의장애(moderate
disability)의좋은성적을보 다35). 그러나, 이연구에서도전체생존률에서는두군간에차이를보이
지않았고, 환자수가작은것이단점으로지적된다. 최근에자발성천막상부뇌출혈의하위집단메타
분석(meta-analysis)의결과가발표되었다8). 이메타연구는8개의연구로부터2186명의환자를 상
으로하 는데, 수술이출혈발생으로부터8시간이내에시행된경우, 또는혈종의부피가20-50 ml의
경우, 또는 래스고우혼수척도가9점에서12점사이인경우, 수술에서좋은결과를보 다. 더욱이,
근거의강도가약하기는하지만, 혈종이뇌실내혈종을포함하지않으면서, 보다표재성일경우수술
이효과가있었다8).
소뇌출혈의경우는비무작위배정임상연구들에서일관되게뇌간압박, 수두증을동반하거나, 혈종
의직경이 3cm이넘는경우수술로서치료한경우가성적이좋았다5,17,19,28,37,41). 더욱이, 혈종을
제거하지않고, 뇌실외배액술만을시행하는것은특히수조가압박을받는환자에서는일반적으로
권고되지않는다41). 시상출혈과뇌교출혈의수술적혈종제거는한계가있는것으로알려져있다
14,16,28).
수술의적절한시기에 해서는아직논란이많다. 많은임상연구들의결과에서수술의적절한시기
는증상이생긴후수술까지4시간에서96시간까지다양하다21,26,35,45). 후향적연구에서, Kaneko 등
15)은증상이발생하고 7시간이내에수술한 100명의피각부출혈(putaminal hemorrhage) 환자의수
술성적을발표하 는데, 이중60명은발생3시간이내에수술받았다. 7명(7%)이사망한반면에, 15명
(15%)은완전회복을보 고, 35명(35%)은수술후6개월째집에서독립적인생활이가능하 다. 그러
나, 이후발표된무작위연구들에서는증상발생12시간이내에수술한경우다양한결과들이발표되
었다26,35,45). 발병4시간이내에무작위배정을하 던연구에서조기수술의단점으로는재출혈의위
험성이높아진다는것이었다25). 발병24시간38), 48시간1,12), 72시간40,43), 및96시간내21)에수술에
한무작위배정을했던연구들에서는수술이내과적치료에비해명확한잇점을보여주지못했다.

221
CLINICAL RESEARCH CENTER FOR STROKE
2. 최소침습적수술적혈종제거술(minimally invasive hematoma removal)
일차성뇌출혈에 한최소침습적수술의이론적배경은 (1) 임상상황에서조기혈종배출의가능성
(2) 수술시간의단축 (3) 특히심부에위치한혈종의경우주변뇌조직에 한추가손상감소 (4) 국소
마취하에서시행등이다. 반면에단점은 (1) 섬유소용해제(fibrinolytics) 사용에따른재출혈의가능성
(2) 지속적인카테터유지에따른감염의위험성증가등이다. 최소침습적수술의방법으로는혈전
용해제또는섬유소용해제를사용한혈종용해술을병행또는병행하지않는정위적흡인술
(stereotactic aspiration) 또는내시경적흡인술(endoscopic aspiration)이있다.
Hattori 등10)은중등도의신경학적인결손을갖는피각부뇌출혈환자490명의무작위배정연구에
서, 혈종의정위적흡인술이신경학적3등급(자발적으로눈을뜨지는않지만, 강한자극에눈을뜨는
경우) 환자에서사망률을줄이고, 보다많은환자에서기능적으로독립적인회복이가능하게하 다
고보고하 다.
최근에Wang 등43)은중국의42개의병원에서465명의기저핵뇌출혈환자를 상으로하여다기관
무작위 조군임상연구결과를발표하 다. 이연구에서는 377명의기저핵뇌출혈(basal ganglia
hemorrhage) 환자중 195명은최소침습적두개천공술(craniopuncture)로, 182명은보존적 조군에
무작위배정되었다. 이연구에서는치료14일째신경학적결손, 수술후3개월째일상생활척도및사
망률을비교하 다. 14일째최소침습적두개천공술을받은군에서신경학적호전이통계적으로유
의하 고, 3개월째일상생활척도(activities of daily living score) 역시최소침습적두개천공술군에서
더나았다. 수술후3개월째수정랜킨지수가3점이상인경우, 즉독립적인생활이가능하지않은생
존률부분에서두개천공술군은40.9%로 조군의63.0% 보다낮았고, 이는통계적으로유의하 다.
그러나, 수술후3개월째, 누적치사율(cumulative fatality rate)은두개천공술군에서6.7%, 조군에서
8.8%로두개천공술군에서낮았으나, 통계적유의성은없었다.
이와같은무작위배정연구와더불어, 정위적혈종흡인술을이용한, 다수의무작위배정연구에서
초기혈종흡인률(aspiration rate)은 30% 에서90% 고1,3,13,18), 재출혈률(rebleeding rate)은기존의
개두술의0%에서10%와비교하여비슷하 다1,3,13,18,33,34).
71명의환자를 상으로한, 다기관무작위배정 조군연구인 Stereotactic Treatment of ICH by
means of a Plasminogen Activator (SICHPA)는증상발현이후48-72시간내에6시간간격으로유로키
나제(urokinase) 5000 IU을정위적으로주사한결과를보여준다40). 연구에포함된적응증은45세이
상, 혈종의양이 10 ml 이상인경우, 래스고우혼수척도에서안지수및운동지수가 2점에서 10점
사이, 최소한한쪽동공반사가남아있는경우, 정상적인혈액응고상태 다. 연구의일차목표점은6
개월째수정랜킨지수로표현되는기능적장애및사망률이었다. 6개월째전체사망률은 57% 고,
이중수술군이56%, 비수술군이59% 다. 뇌혈종의부피감소는수술군에서10-20% 고, 우도비가

222
CLINICAL RESEARCH CENTER FOR STROKE
0.23으로효과가있을가능성이있었지만, 통계적으로유의하지는않았다. 6개월째수정랜킨지수5점
을포함사망률의우도비역시0.52 으나, 통계적으로유의하지는않았다. 1999년에제조과정에서의
바이러스오염의가능성이제기되어, 미국에서유로키나제사용이금지된이후, 뇌출혈의치료에서
조직플라스미노겐활성인자(tissue plasminogen activator)가사용되고있다2,39).
Vespa 등42)은5 ml 이상의기저핵또는내포(internal capsule) 출혈이있었던28명의환자에서틀이없
는(frameless) 정위적흡인술과혈종용해술을시행한2상연구를발표하 다. 컴퓨터단층촬 에서카
테터의정확한위치를확인한이후, 조직플라스미노겐활성인자 1 mg을카테터를통해주입하 고,
30분간카테터를잠가혈종내에스며들게하 으며, 이후폐쇄회로모음장치를통해배액하 다. 조
직플라스미노겐활성인자는48시간동안8시간간격으로주입되었다. 이연구에서심부에위치한자
발성뇌혈종에 한조직플라스미노겐활성인자를통한혈전용해술을포함한틀없는정위적흡인술
은안전하고, 혈종부피감소에효과적이며, 국립보건원뇌졸중척도(NIH Stroke Scale)의조기향상으
로임상적인효과가있을가능성이높다고보고되었다. 이연구결과를바탕으로하여, 다기관무작위
배정 조군연구인Minimally Invasive Stereotactic Surgery with rtPA for ICH Evacuation (MISTIE)가시작
되어, 혈종이있는공간에조직플라스미노겐활성인자를주입하는군과보존적인내과치료군의두군
을 상으로연구가진행되고있다. 이연구의초기연구결과에의하면, 수술군이급성기평균혈종
감소율은46%로내과치료군의4%에배해효과적이었으며, 30일째사망률이8%, 증상이있는재출혈
이8%, 세균성뇌실염이0%로안전하 다24). MISTIE 2상연구가2005년에서2013년까지조직플라스
미노겐활성인자를이용한최소침습적수술의안전성과효과를입증하기위해진행되었는데, 2013년
세계뇌졸중학회(International Stroke Conference)에서발표된예비결과에서는수술군에서수정랜킨
지수 0-2점으로 14%에서임상적호전을보 고, 병원재원기간을줄 고, 환자당 44,000 미국달러의
비용이절감되었으며, 장기요양기관(long term care facility)으로의전원률이 14% 감소하 다(미출판
내용). 또한, MISTIE II 연구자들은혈종의제거가뇌출혈이후이차신경학적악화의원인중의하나인
혈종주변의뇌부종을의미있게감소시켰고, 혈종주변의뇌부종은조직플라스미노겐활성인자에의
해악화되지않았다고보고하 다29).
자발성천막상부뇌출혈[피질하, 피각부및시상(thalamus)] 환자100명을 상으로하여내시경을이
용한혈종제거와내과적치료를비교한무작위배정 조군연구결과가발표되었는데1), 내시경혈
종제거술의적응증은(1) 환자의나이가30세에서80세사이(2) 혈종의양이10 ml 이상인경우(3) 신경
학적결손혹은의식의소실이있는경우 (4) 내과적, 마취과적관점에서수술이적절한경우 (5) 혈종
발생후48시간이내에제거술이일어난경우 다. 내시경적혈종제거술군에서혈종의양이50 ml 이
상인경우사망률을낮추었으며, 50 ml 보다작은경우의환자에서기능적으로높은회복률을보여주
었다. 이러한효과는수술전의식이명료하거나(alert) 졸린상태(somnolent state) 정도의의식하의60

223
CLINICAL RESEARCH CENTER FOR STROKE
세이하의엽상출혈환자에국한되었다. 향후많은수의환자군을통한연구가천막상부의뇌출혈환
자에서내시경적흡인술의효과를보다명확하게해줄가능성이있다. 자발성기저핵출혈에서내시
경수술, 정위적수술및개두술의안전성, 신경학적효과및비용 비효과를비교한, 또다른전향적
무작위배정연구가수행되어90명의혼수상태가아닌(non-comatose) 환자들이세군으로무작위배
정되었다4). 이연구에서는내시경수술과정위적수술이3개월째합병증및사망률을낮추었고, 6개
월째신경학적으로더나은결과를보 다. 하지만, 이연구에서정위적수술의 기시간이내시경수
술보다더길었고, 내시경수술이바텔지수및기능적독립성(functional independence)을기준으로볼
때, 개두술에비해비용 비효과가더나은것으로판명되었다.
최소침습적수술(정위적수술및내시경수술)에 한높은수준의무작위배정 조군연구들을이용
한메타분석이최근에발표되었다44). 이연구는12개의높은수준의무작위배정 조군연구들에서
1955명의환자들을포함하고있는데, 천막상부뇌출혈에서최소침습적수술이다른치료법에비해효
과적이라는결론을내리고있다. 이중에서도가장효과적인하위집단은남성과여성포함양성, 래
스고우혼수척도가9점이상, 혈종의부피가25-40 ml인경우, 증상발현후72시간이내인경우 다44).
3. 뇌실내출혈
뇌실내출혈은일차성뇌출혈환자의 40%에서동반된다9). 뇌실내출혈은뇌실내에국한된일차성
뇌실내출혈과기저핵또는시상부위의고혈압성뇌출혈, 혈관기형에의한뇌출혈이뇌실내로터져나
온이차성뇌실내출혈로구분된다6,9). 전통적인뇌실내출혈의치료는뇌실안의혈종의제거를위한
뇌실외배액술과폐쇄성수두증(obstructive hydrocephalus)의치료로이루어진다. 이론적으로뇌실내
카테터거치를통한뇌실외배액술은뇌실내의혈종을배액하고, 혈종이차있는뇌실로부터뇌척수액
을배액하는데도움을줄수있으나, 흔히혈종에의해카테터폐색이발생하고, 뇌실내혈종을배액하
는데오랜시간이걸리는점, 뇌실내혈종이녹으면서나오는물질에의해발생되는염증반응에의한
교통성수두증(communicating hydrocephalus)을예방할수없는점등으로불충분한치료가되는경우
가많다11). 따라서, 최근에뇌실내카테터를통한섬유소용해제투여가치료로서관심을끌게되었다.
동물실험및임상연구를통한몇몇보고에의하면유로키나제, 스트렙토키나제(streptokinase), 조직플
라스미노겐활성인자등의섬유소용해제의뇌실내주입이뇌실내혈종의제거에효과적이면서합병
률, 사망률을감소시킬수있음이확인되었다7,20,30-32,35). 무작위임상연구인 the Clot Lysis: Evaluating
Accelerated Resolution of IVH (CLEAR-IVH)는뇌실내혈종을녹여배출시키기위해뇌실내카테터를통
하여8시간간격으로최 9회1.0 mg의조직플라스미노겐활성인자를주입하는치료의안전성및효
과를밝히고자진행중이다23). 2008년에발표된예비결과에의하면, 급성기치료후평균혈종감소는
46% 고, 30일사망률은8%인반면에, 증상이있는재출혈은4%, 세균성뇌실염은0% 다23).

224
CLINICAL RESEARCH CENTER FOR STROKE
1. 혈종의종괴효과에의한의식의악화가있을때, 조기개두술을고려해볼수있다.
(근거수준IV, 권고수준C)
2, 래스고우혼수척도가9-12이고, 혈종이피질면(cortical surface)에서1 cm 이내에위치한엽상
출혈의경우개두술을고려해볼수있다. (근거수준IIb, 권고수준B)
3, 래스고우혼수척도가9점이상, 혈종의부피가25-40 ml인경우, 증상발현후72시간이내인천막
상부뇌출혈의경우, 최소침습적수술에의한혈종의제거가추천된다. (근거수준IIb, 권고수준B)
4, 소뇌출혈의경우, 최 직경이3 cm이상인경우, 또는뇌간압박, 수두증의증상이있는경우개두술
이추천된다. (근거수준IIb, 권고수준B)
5, 뇌실내출혈의경우, 뇌실천자에의한혈종용해술을고려해볼수있다. (근거수준IV, 권고수준C)
1. Auer LM, Deinsberger W, Niederkorn K, Gell G, Kleinert R, Schneider G, et al.: Endoscopic surgery versus medical
treatment for spontaneous intracerebral hematoma: a randomized study. J Neurosurg70: 530-535, 1989.
2. Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, et al.: Guidelines for the management of
spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart
Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the
Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke38: 2001-2023, 2007.
3. Broderick JP, Brott T, Zuccarello M: Management of intracerebral hemorrhage, in Batjer HH (ed):
Cerebrovascular Disease. Philadelphia, PA: Lippincott-Raven, 1997, pp611-627.
4. Cho DY, Chen CC, Chang CS, Lee WY, Tso M: Endoscopic surgery for spontaneous basal ganglia
hemorrhage: comparing endoscopic surgery, stereotactic aspiration, and craniotomy in noncomatose
patients. Surg Neurol 65: 547-555; discussion 555-546, 2006.
5. Da Pian R, Bazzan A, Pasqualin A: Surgical versus medical treatment of spontaneous posterior fossa
haematomas: a cooperative study on 205 cases.Neurol Res 6: 145-151, 1984.
6. Engelhard HH, Andrews CO, Slavin KV, Charbel FT: Current management of intraventricular hemorrhage.
Surg Neurol 60: 15-21; discussion 21-12, 2003.
7. Fountas KN, Kapsalaki EZ, Parish DC, Smith B, Smisson HF, Johnston KW, et al.: Intraventricular
administration of rt-PA in patients with intraventricular hemorrhage. South Med J 98: 767-773, 2005.
8. Gregson BA, Broderick JP, Auer LM, Batjer H, Chen XC, Juvela S, et al.: Individual patient data subgroup

225
CLINICAL RESEARCH CENTER FOR STROKE
meta-analysis of surgery for spontaneous supratentorial intracerebral hemorrhage. Stroke43: 1496-1504, 2012.
9. Hallevi H, Albright KC, Aronowski J, Barreto AD, Martin-Schild S, Khaja AM, et al.: Intraventricular
hemorrhage: Anatomic relationships and clinical implications. Neurology 70: 848-852, 2008.
10. Hattori N, Katayama Y, Maya Y, Gatherer A: Impact of stereotactic hematoma evacuation on activities of daily
living during the chronic period following spontaneous putaminal hemorrhage: a randomized study. J
Neurosurg 101: 417-420, 2004.
11. Huttner HB, Kohrmann M, Berger C, Georgiadis D, Schwab S: Influence of intraventricular hemorrhage and
occlusive hydrocephalus on the long-term outcome of treated patients with basal ganglia hemorrhage: a
case-control study. J Neurosurg 105: 412-417, 2006.
12. Juvela S, Heiskanen O, Poranen A, Valtonen S, Kuurne T, Kaste M, et al.: The treatment of spontaneous
intracerebral hemorrhage. A prospective randomized trial of surgical and conservative treatment. J
Neurosurg 70: 755-758, 1989.
13. Kanaya H, Kuroda K: Development in neurosurgical approaches to hypertensive intracerebral hemorrhage
in Japan, in Kaufman HH (ed): Intracerebral hematomas. New York, NY: Raven Press, 1992, pp197-210.
14. Kanaya H, Saiki I, Ohuchi T: Update on surgical treatment, in Mizukami M, Kanaya K, Yamori Y (eds):
Hypertensive Intracerebral Hemorrhage. New York, NY: Raven Press, 1983, pp147-163.
15. Kaneko M, Tanaka K, Shimada T, Sato K, Uemura K: Long-term evaluation of ultra-early operation for
hypertensive intracerebral hemorrhage in 100 cases. J Neurosurg 58: 838-842, 1983.
16. Kanno T, Sano H, Shinomiya Y, Katada K, Nagata J, Hoshino M, et al.: Role of surgery in hypertensive
intracerebral hematoma. A comparative study of 305 nonsurgical and 154 surgical cases.J Neurosurg 61:
1091-1099, 1984.
17. Kase C: Cerebellar hemorrhage, in Kase C, Caplan L (eds): Intracerebral Hemorrhage. Boston:
Butterworth- Heinemann, 1994, pp425-443.
18. Kaufman HH: Stereotactic aspiration with fibrinolytic and mechanical assistance, in Kaufman HH (ed):
Intracerebral Hematoma. New York, NY: Raven Press, 1992, pp182-185.
19. Kirollos RW, Tyagi AK, Ross SA, van Hille PT, Marks PV: Management of spontaneous cerebellar
hematomas: a prospective treatment protocol. Neurosurgery49: 1378-1386; discussion 1386-1377, 2001.
20. Lapointe M, Haines S: Fibrinolytic therapy for intraventricular hemorrhage in adults. Cochrane Database
Syst Rev: CD003692, 2002.
21. Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, et al.: Early surgery versus
initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the
International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial.Lancet365: 387-397, 2005.
226
CLINICAL RESEARCH CENTER FOR STROKE
22. Mendelow AD, Gregson BA, Rowan EN, Murray GD, Gholkar A, Mitchell PM, et al.: Early surgery versus initial
conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas
(STICH II): a randomised trial. Lancet 382: 397-408, 2013.
23. Morgan T, Awad I, Keyl P, Lane K, Hanley D: Preliminary report of the clot lysis evaluating accelerated
resolution of intraventricular hemorrhage (CLEAR-IVH) clinical trial. Acta Neurochir Suppl 105: 217-220, 2008.
24. Morgan T, Zuccarello M, Narayan R, Keyl P, Lane K, Hanley D: Preliminary findings of the minimally-invasive
surgery plus rtPA for intracerebral hemorrhage evacuation (MISTIE) clinical trial. Acta Neurochir Suppl 105:
147-151, 2008.
25. Morgenstern LB, Demchuk AM, Kim DH, Frankowski RF, Grotta JC: Rebleeding leads to poor outcome in
ultra-early craniotomy for intracerebral hemorrhage. Neurology 56: 1294-1299, 2001.
26. Morgenstern LB, Frankowski RF, Shedden P, Pasteur W, Grotta JC: Surgical treatment for intracerebral
hemorrhage (STICH): a single-center, randomized clinical trial.Neurology51: 1359-1363, 1998.
27. Morgenstern LB, Hemphill JC, 3rd, Anderson C, Becker K, Broderick JP, Connolly ES, Jr., et al.: Guidelines
for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals
from the American Heart Association/American Stroke Association. Stroke 41: 2108-2129, 2010.
28. Morioka J, Fujii M, Kato S, Fujisawa H, Akimura T, Suzuki M, et al.: Surgery for spontaneous intracerebral
hemorrhage has greater remedial value than conservative therapy. Surg Neurol65: 67-72; discussion 72-63, 2006.
29. Mould WA, Carhuapoma JR, Muschelli J, Lane K, Morgan TC, McBee NA, et al.: Minimally Invasive Surgery
Plus Recombinant Tissue-type Plasminogen Activator for Intracerebral Hemorrhage Evacuation Decreases
Perihematomal Edema. Stroke44: 627-634, 2013.
30. Murry KR, Rhoney DH, Coplin WM: Urokinase in the treatment of intraventricular hemorrhage. Ann
Pharmacother 32: 256-258, 1998.
31. Naff NJ, Hanley DF, Keyl PM, Tuhrim S, Kraut M, Bederson J, et al.: Intraventricular thrombolysis speeds
blood clot resolution: results of a pilot, prospective, randomized, double-blind, controlled trial. Neurosurgery
54: 577-583; discussion 583-574, 2004.
32. Nieuwkamp DJ, de Gans K, Rinkel GJ, Algra A: Treatment and outcome of severe intraventricular extension
in patients with subarachnoid or intracerebral hemorrhage: a systematic review of the literature. J Neurol 247:
117-121, 2000.
33. Niizuma H, Shimizu Y, Yonemitsu T, Nakasato N, Suzuki J: Results of stereotactic aspiration in 175 cases of
putaminal hemorrhage. Neurosurgery24: 814-819, 1989.
34. Niizuma H, Yonemitsu T, Jokura H, Nakasato N, Suzuki J, Yoshimoto T: Stereotactic aspiration of thalamic
hematoma. Overall results of 75 aspirated and 70 nonaspirated cases. Stereotact Funct Neurosurg54-55:

227
CLINICAL RESEARCH CENTER FOR STROKE
438-444, 1990.
35. Pantazis G, Tsitsopoulos P, Mihas C, Katsiva V, Stavrianos V, Zymaris S: Early surgical treatment vs
conservative management for spontaneous supratentorial intracerebral hematomas: A prospective
randomized study. Surg Neurol66: 492-501; discussion 501-492, 2006.
36.Steiner T, Kaste M, Forsting M, Mendelow D, Kwiecinski H, Szikora I, et al.: Recommendations for the
management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European
Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee.
Cerebrovasc Dis 22: 294-316, 2006.
37. Sypert G, Arpin-Sypert E: Spontaneous posterior fossa hematomas, in Kaufman H (ed): Intracerebral
Hematomas. New York, NY: Raven Press, 1992, pp187-196.
38. Tan SH, Ng PY, Yeo TT, Wong SH, Ong PL, Venketasubramanian N: Hypertensive basal ganglia
hemorrhage: a prospective study comparing surgical and nonsurgical management. Surg Neurol 56: 287-
292; discussion 292-283, 2001.
39. Teernstra OP, Evers SM, Kessels AH: Meta analyses in treatment of spontaneous supratentorial
intracerebral haematoma. Acta Neurochir (Wien) 148: 521-528; discussion 528, 2006.
40. Teernstra OP, Evers SM, Lodder J, Leffers P, Franke CL, Blaauw G: Stereotactic treatment of intracerebral
hematoma by means of a plasminogen activator: a multicenter randomized controlled trial (SICHPA). Stroke
34: 968-974, 2003.
41. van Loon J, Van Calenbergh F, Goffin J, Plets C: Controversies in the management of spontaneous
cerebellar haemorrhage. A consecutive series of 49 cases and review of the literature.Acta Neurochir (Wien)
122: 187-193, 1993.
42. Vespa P, McArthur D, Miller C, O'Phelan K, Frazee J, Kidwell C, et al.: Frameless stereotactic aspiration and
thrombolysis of deep intracerebral hemorrhage is associated with reduction of hemorrhage volume and
neurological improvement. Neurocrit Care2: 274-281, 2005.
43. Wang WZ, Jiang B, Liu HM, Li D, Lu CZ, Zhao YD, et al.: Minimally invasive craniopuncture therapy vs.
conservative treatment for spontaneous intracerebral hemorrhage: results from a randomized clinical trial
in China.Int J Stroke 4: 11-16, 2009.
44. Zhou X, Chen J, Li Q, Ren G, Yao G, Liu M, et al.: Minimally invasive surgery for spontaneous supratentorial
intracerebral hemorrhage: a meta-analysis of randomized controlled trials. Stroke43: 2923-2930, 2012.
45. Zuccarello M, Brott T, Derex L, Kothari R, Sauerbeck L, Tew J, et al.: Early surgical treatment for
supratentorial intracerebral hemorrhage: a randomized feasibility study. Stroke 30: 1833-1839, 1999.

CLINICAL RESEARCH CENTER FOR STROKE
2.5 뇌졸중의재활Rehabilitation of stroke
2.5.1. 재활치료의시작Timing of stroke rehabilitation
뇌졸중환자에서조기재활치료는깊은정맥혈전증, 관절구축, 욕창등의합병증을예방하고이동동
작, 일상생활동작등의기능적회복을증진시키는것으로알려져있다. 따라서뇌졸중후환자가내
과적, 신경학적으로안정이되면재활치료를시작하여야한다. 재활치료의시작시기는뇌졸중의중
증도, 환자의신경학적상태에따라 향을받을수있으며시기에따라치료의강도(intensity)를조절
하여야한다.
1. It is strongly recommended that rehabilitation therapy start as early as possible, once medical stability is
reached (AHA/ASA, RCP, SIGN, EUSI: LOE Ib, GOR A)
228
조기재활치료(early rehabilitation)의효과에 해서는많은무작위 조군연구가보고되었으며메타
연구및계통적고찰을통해서도효과가밝혀져있다. 36개의무작위 조군연구및 79개의 조군
연구를메타분석한결과의하면, 조직된재활치료를받은환자들의기능회복정도가 조군보다좋
다고알려져있으며, 이러한기능호전은재활치료의기간보다재활치료의조기시행과관련이있다
고알려져있다.1,2또한뇌졸중이후의기능회복에있어서도, 조직적인재활치료를받은환자들이더
낮은사망률(OR, 0.86; 95% CI, 0.71-0.94)을보이며장기요양시설로퇴원하는경우가감소(OR, 0.80;
95% CI, 0.71-0.91)하 으며뇌졸중으로인한장애도비교적양호(OR, 0.78; 95% CI, 0.68-0.89)한것으로
분석되었다. 즉, 조직적인재활치료를통하여더욱양호한예후를기 할수있는것으로알려져있
다.3이러한조기재활치료를통하여깊은정맥혈전증, 관절구축과같은합병증을예방할수있으며,
이동동작, 일상생활동작등의회복이촉진될수있어, 내과적으로안정이되면가능한한빨리재활

229
CLINICAL RESEARCH CENTER FOR STROKE
1. 급성기뇌졸중환자의재활치료는내과적으로안정이되면가능한한빠른시간내에시작해야한
다. (근거수준Ia, 권고수준A)
치료를시작하는것이필요하다. 4-6
구체적인재활치료의시작시기는뇌졸중의중증도및환자의신경학적상태를고려하여결정하는
것이원칙이다. 여러연구를통하여조기에재활치료를시작하는경우보다양호한예후를기 할
수있다는것이알려져있다.7,8 뇌졸중후72시간이내에재활치료를시작하는경우, 보행상태가호
전되고입원기간이단축될수있다는연구결과9를고려하여, 뇌졸중환자는뇌졸중후48시간에서
72시간이내에급성기치료와병행하여재활치료를시작하는것이바람직하다. 단, 뇌졸중발생1주
이내에는재활치료의강도를조절하여최소한의움직임으로시작하고, 발병1주이후에치료시간과
강도를늘리는것을고려할수있다.
1. Ottenbacher KJ, Jannell S. The results of clinical trials in stroke rehabilitation research. Arch Neurol. 1993; 50:
37
2. Cifu DX, Stewart DG. Factors affecting functional outcome after stroke: a critical review of rehabilitation
interventions. Arch Phys Med Rehabil. 1999; 80: S35
3. Stroke Unit Trialists’Collaboration: Organised inpatient (stroke unit) care for stroke (Cochrane Review). In:
The Cochrane Library, Issue 3, 2007. Chichester, UK: John Wiley and Sons
4. Langhome P, Pollock A for the Stroke Unit Trialists’Collaboration. What are the components of effective
stroke unit care? Age Ageing. 2002; 31: 1
5. Arias M, Smith L. Early mobilization of acute stroke patients. J Clin Nurs. 2007; 16:282
6. Fang Y, Chen X, Li H, Lin J, Huang R, Zeng J. A study on additional early physiotherapy after stroke and factors
affecting functional recovery. Clin Rehabil. 2003;17:608
7. Paolucci S, Antonucci G, Grasso MG, Morelli D, Troisi E, Coiro P, Bragoni M. Early versus delayed inpatient
stroke rehabilitation: a matched comparison conducted in Italy. Arch Phys Med Rehabil. 2000; 81: 695
230
뇌졸중후재활치료의강도는환자의순응도, 뇌손상의정도, 의학적안정정도, 인지기능및운동기
능의손상정도등다양한요소들에의해달라질수있다. 재활치료의강도를설정하는것은중요하지
만, 치료강도를표준화하기어렵고, 재활치료를구성하는여러가지요소를정량적으로측정하기어
렵다는문제점을가지고있다.
CLINICAL RESEARCH CENTER FOR STROKE
2.5.2. 재활치료의강도 Intensity of rehabilitation
8. Musicco M, Emberti L, Nappi G, Caltagirone C. Early and long-term outcome of rehabilitation in stroke
patients: The role of patient characteristics, time of initiation, and duration of interventions. Arch Phys Med
Rehabil. 2003; 84: 551
9. Hayes S, Carroll S. Early intervention care in the acute stroke patient. Arch Phys Med Rehabil. 1986; 67: 319
1. Recommend that the patient receive as much therapy as "needed" to adapt, recover, and/or reestablish
the premorbid or optimal level of functional independence (AHA/ASA, RCP: LOE Ib, GOR A).
2. The team should promote the practice of skills gained in therapy into the patient’s daily routine in a
consistent manner (RCP: LOE Ia, GOR A).
많은연구들이재활치료가기능적인향상을가져오는것을보고하고있으며, 특히장애가적은환자
에서더효과적이었음을보고하고있다. 또한뇌졸중발생후재활치료의강도가높을수록예후가호
전됨이알려져있다.1-3세부적으로보아, 상지기능훈련의강도를높일경우상지기능의회복이증가
되는것으로알려져있다.3특히상지및하지의기능에중점을둔재활치료를시행한결과, 상지의기
민성(dexterity)과하지의보행능력이호전됨이보고되었다.4가장최근에발표된 규모메타분석결

231
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌졸중환자는적응할수있는범위내에서기능회복에필요한충분한재활치료를받는것이권장
된다. (근거수준Ia, 권고수준A)
2. 재활치료로얻어진기술은환자의일상생활에서지속적이고반복적으로사용하도록권장된다.
(근거수준Ia, 권고수준A)
과,5치료강도를높일경우일상생활활동도(Activity of Daily Living, ADL)가향상될수있으며, 이효과는
뇌졸중후급성기에충분한재활치료가시행될경우더욱뚜렷함이보고되었다.
1. Langhorne P, Wagenaar R, Partridge C. Physiotherapy after stroke: more is better. Physiother Res Int.
1996;1:75.
2. Kwakkel G, Wagenaar R, Koelman T. Effects of intensity of rehabilitation after stroke: a research synthesis.
Stroke. 1997;28:1550.
3. van der Lee JH, Snels IA, Beckerman H, Lankhorst GJ, Wagenaar RC, Bouter LM. Exercise therapy for arm
function in stroke patients: a systematic review of randomized controlled trials. Clin Rehabil. 2001;15:20.
4. Kwakkel G, Wagenaar R, Twisk J, Lankhorst G, Koetsier J. Intensity of leg and arm training after primary
middle-cerebral-artery stroke: a randomised trial. Lancet. 1999;354:191.
5. Kwakkel G, van Peppen R, Wagennar RC, Dauphinee SW, Richards C, Ashburn A, Miller K, Lincoln N,
Partridge C, Wellwood I, Langhorne P. Effects of augmented exercise therapy time after stroke: A meta-
analysis. Stroke. 2004;35;2529.
일상생활에서장애를줄이고기능을호전시키기위한방법으로다양한재활치료가시도되고있다.
2.5.3. 재활치료의접근방법Underlying approach to rehabilitation

232
재활치료는자극의종류또는작업훈련의특이성또는적용되는학습원리의차이등에의해구분된
다. 재활치료를제공하는모든팀원들이재활치료에서일관된접근에 한중요성을인식하고기능
적회복을최 화시킬수있는방향으로치료를시행하여야하는것이매우중요하다. 운동재학습을
포함한다양한치료방법들이시행되고있으나, 치료의내용및효과에 한결과가다양하여비교분
석이어렵다.
CLINICAL RESEARCH CENTER FOR STROKE
1. One of the current therapeutic approaches to movement re-education should be used to improve
function (RCP: LOE Ia, GOR A).
2. Patients should be given the opportunity to repeatedly practice functional skills and activities (RCP: LOE
Ia, GOR A).
3. All staff should be trained in the recognition and basic management of emotional, communication and
cognitive problems (RCP: LOE IV, GOR C).
4. All team members handling patients should be taught safe and appropriate ways of moving and
handling (RCP: LOE IV, GOR C).
5. Goals should be meaningful and challenging but achievable (RCP: LOE III, GOR B).
6. There should be both short- and long-term goals (RCP: LOE IV, GOR C).
7. Goal-setting should involve the patient (RCP: LOE III, GOR B), and the family if appropriate (RCP: LOE IV,
GOR C).
8. Goal-setting should be set at the team level as well as at the level of an individual clinician (RCP: LOE IV,
GOR C).
9. Judging progress against goals set (‘goal attainment scaling’) may be helpful (RCP: LOE IIb, GOR B).
뇌졸중후한가지방법의운동치료만을적용한경우에는의미있는효과가없었으나, 운동재학습을
포함하여여러치료방법을같이적용한경우치료를하지않은군에비해예후가호전됨이밝혀졌
다.1,2하지만또다른메타분석의결과, 근력강화에미치는 향을보았을때, 운동재학습이뇌졸중

233
CLINICAL RESEARCH CENTER FOR STROKE
1. 운동기능향상을위해운동재학습, 신경생리적접근, 생역학적접근등여러치료방법들을환자의
상태에따라조합하여개별적으로적용할것을권장한다. (근거수준Ia, 권고수준A)
2. 재활목표설정시환자와보호자도같이참여할것이추천된다. (근거수준IIb, 권고수준B)
3. 재활목표는단기및장기목표로설정하며목표의달성정도를평가하고재설정하는것이고려된
다. (근거수준IV, 권고수준C)
의예후에의미있는효과를보이지않음이보고되었다.3또한뇌졸중후기능적훈련을반복하면재
활치료의효과가향상된다는연구가보고되었다.4,5그리고뇌졸중발생60일이내의환자에서반복
적인보행훈련을물리치료와함께시행할때, 물리치료만을단독으로시행한군에비해보행기능
이증가함도알려져있다.6
뇌졸중환자에서목표설정이뇌졸중후의기능회복에도움을준다는사실이보고되었다.7특히의
사, 물리치료사및환자가함께참여하는목표설정및평가회의를통하여, 환자의요구사항을더고
려할수있으며, 환자및보호자그리고재활치료팀의협조가원활해지며, 구체적이고성취가능한
목표를설정할수있음이알려졌다.8,9
1. Pollock A, Baer G, Pomeroy V, Langhorne P. Physiotherapy treatment approaches for the recovery of postural
control and lower limb function following stroke. Cochrane Database Syst Rev. 2003;CD001920.
2. Pollock A, Baer G, Pomeroy V, Langhorne P. Physiotherapy treatment approaches for the recovery of postural
control and lower limb function following stroke. Cochrane Database Syst Rev. 2007;CD001920.
3. Ada L, Dorsch S, Canning CG. Strengthening intervention increase strength and improve activity after stroke:
a systematic review. Aust J Physiother. 2006;52:241.
4. Langhorne P, Wagenaar R, Partridge C. Physiotherapy after stroke: more is better. Physiother Res Int.
1996;1:75.
5. Kwakkel G, Wagenaar R, Twisk J, Lankhorst G, Koetsier J. Intensity of leg and arm training after primary
middle-cerebral-artery stroke: a randomised trial. Lancet. 1999;354:191.

234
6. Pohl M, Werner C, Holzgraefe M, Kroczec G, Mehrholz J, Wingendorf I, Hoelig G, Koch R, Hesse S. Repetitive
locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: a single-
blind, randomized multicentre trial. Clin Rehabil. 2007;21:17.
7. van Vliet P, Sheridan M, Kerwin D, Fentem P. The influence of functional goals on the kinematics of reaching
following stroke. Neurology report. 1995;19:11.
8. Monaghan J, Channell K, McDowell D, Sharma AK. Improving patient and carer communication,
multidisciplinary team working and goal-setting in stroke rehabilitation. Clin Rehabil. 2005;19:194.
9. Hollidaty RC, Ballinger C, Playford ED. Goal setting in neurological rehabilitation: Patients’perspectives.
Disabil Rehabil. 2007;29:389.
CLINICAL RESEARCH CENTER FOR STROKE
1. Recommend that a thorough assessment of skin integrity be completed on admission and monitored at
least daily thereafter (AHA/ASA: LOE IV, GOR C).
2. Recommend the use of proper positioning, turning, and transferring techniques and judicious use of
barrier sprays, lubricants, special mattresses, and protective dressings and padding to avoid skin injury
due to friction or excessive pressure (AHA/ASA, RCP: LOE IV, GOR C).
3. Recommend that all patients be mobilized as soon as possible (the act of getting a patient to move in the
bed, sit up, stand, and eventually walk) (AHA/ASA: LOE IV, GOR C) (RCP: LOE IIa, GOR B) (SIGN: LOE Ib,
뇌졸중후발생하는흔한합병증으로욕창, 흡인성폐렴, 관절구축, 낙상및골절, 통증등이있고, 이
와같은합병증이발생할경우적극적인재활치료가어려워져예후에부정적인 향을미친다. 그러
므로, 발생가능한합병증을효과적으로관리하는것이재활치료의결과를향상시키는데큰도움이
될것이다.
2.5.4. 합병증관리Management of complications

235
CLINICAL RESEARCH CENTER FOR STROKE
뇌졸중발생후1년간추적관찰한결과, 욕창발병은기능저하와연관되어있다.1또한급성뇌졸중
환자의16-19%에서흡인성폐렴이발생한다고알려져있으며, 특히뇌간에발생한뇌졸중에서높은
빈도를보 다. 폐렴의위험도는삼킴장애를가진환자에서더높다.2뇌졸중발생후조기에적절한
자세교정치료를시행할경우, 뇌졸중후의관절구축을방지하는효과가있다.3-4특히어깨관절의
구축예방을위하여어깨를최 한외회전하는자세가유용하다는보고가있다.3많은관찰적연구
들의메타분석결과, 조기거동을통하여뇌졸중후기능적회복이향상될수있음이보고되었다.5그
외, 뇌졸중환자에서흔히발생할수있는 퇴골골절의예방을위하여엽산(folate)과비타민
B12(vitamin B12)의병용요법6과리세드로네이트(risedronate)7,8가효과적이라는보고가있다. 그외,
일부연구는비타민D(vitamin D)를투여할때근육위축예방효과를통해낙상빈도가감소했다고발
표하 고, 다른연구는뇌졸중환자에게좌우 칭체중분배훈련을하여낙상이감소함이보고하
GOR A).
4. Recommend a pain management plan that includes assessment of the following: likely etiology (i.e.,
musculoskeletal and neuropathic); pain location; pain quality, quantity, duration, and intensity; and what
aggravates or relieve the pain (AHA/ASA: LOE IV, GOR C).
5. All pain suffered by a person with stroke should be subject to a full clinical diagnosis, including a referral
to an appropriate specialist service if needed (RCP: GOR GPP).
6. Neuropathic pain may respond to tricyclic antidepressants (eg amitriptyline) or anticonvulsants (eg
gabapentin) (RCP: GPP) (SIGN: LOE Ib, GOR A) (AHA/ASA: LOE IV, GOR C).
7. Recommend the use of lower doses of centrally acting analgesics, which may cause confusion and
deterioration of cognitive performance and interfere with the rehabilitation process (AHA/ASA: LOE IV,
GOR C). Hip protectors are recommended in men and women at high risk of hip fracture (particularly
older people in care homes) although problems with compliance should be recognized (SIGN: LOE Ia,
GOR A).
8. Infection after stroke should be treated with appropriate antibiotics (EUSI: LOE III, GOR B).
9. Aspiration pneumonia may be prevented by nasogastric feeding (EUSI: LOE III, GOR B).

236
1. 뇌졸중후욕창의발생은기능회복을저해하므로예방조치를취하는것이바람직하다. (근거수준
III, 권고수준B)
2. 욕창의예방을위하여주기적인피부평가, 올바른자세, 주기적인자세변화가고려된다. (근거수
준IV, 권고수준C)
3. 뇌졸중후관절구축예방을위해올바른자세유지가권장된다. (근거수준Ib, 권고수준A)
4. 뇌졸중후관절구축, 흡인성폐렴, 중추성통증, 심부정맥혈전증등의합병증예방을위해조기움
직임이추천된다. (근거수준III, 권고수준B)
5. 뇌졸중환자에서낙상및골절의위험도를평가하는것이권장된다. (권고수준GPP)
6. 뇌졸중환자에서발생한통증에 한평가가필요하다. (권고수준GPP)
다.9뇌졸중후중추성통증에아미트립틸린(amitriptyline)과라모트리진(lamotrigine)이유용하다는보
고가있으며, 가바펜틴(gabapentin)이일부환자에서효과적이었다고한다.10
CLINICAL RESEARCH CENTER FOR STROKE
1. Landi F, Onder G, Cesari M, Zamboni V, Russo A, Barillaro C, Bernabei R, on behalf of the Silvernet-HC
study group. Functional decline in frail community-dwelling stroke patients. Eur J Neurol. 2006;13:17.
2. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: Incidence,
diagnosis, and pulmonary complications. Stroke. 2005;36:2756.
3. Ada L, Goddard E, McCully J, Stavrinos T, Bampton J. Thirty minutes of positioning reduces the
development of shoulder external rotation contracture after stroke: a randomized controlled trial. Arch
Phys Med Rehabil. 2005;86:230.
4. de Jong LD, Nieuwboer A, Aufdemkampe G. Contracture preventive positioning of the hemiplegic arm in
subacute stroke patients: a pilot randomized controlled trial. Clin Rehabil. 2006;20:656.
5. Disrens K, Michel P, Bogousslavsky J. Early mobilization after stroke: Reviews of the Literature.
Cerebrovasc Dis. 2006;22:183.
6. Sato Y, Honda Y, Iwamoto J, Kanoko T, Satoh K. Effect of folate and mecobalamin on hip fractures in

237
CLINICAL RESEARCH CENTER FOR STROKE
patients with stroke: a randomized controlled trial. JAMA. 2005;293:1082-1088
7. Sato Y, Iwamoto J, Kanoko T, Satoh K. Risedronate therapy for prevention of hip fracture after stroke in
elderly women. Neurology. 2005;64:811-816
8. Sato Y, Iwamoto J, Kanoko T, Satoh K. Risedronate sodium therapy for prevention of hip fracture in men
65 years or older after stroke. Arch Intern Med. 2005;165:1743-1748
9. Sato Y, Iwamoto J, Kanoko T, Satoh K. Low-dose vitamin D prevents muscular atrophy and reduces falls
and hip fractures in women after stroke: a randomized controlled trial. Cerebrovasc Dis. 2005;20:187-
192
10. Frese A, Husstedt IW, Ringelstein EB, Evers S. Pharmacologic treatment of central post-stroke pain.
Clin J Pain. 2006;22:252-260


3 뇌졸중이차예방Secondary prevention of stroke
110-744 서울시종로구연건동28. 서울 학교병원임상의학연구소7208호
뇌졸중임상연구센터 표전화_02 2072 0652 FAX_02 747 0668


241
3.1 위험인자조절 (risk factor control) 243
3.1.1 고혈압 (Hypertension) 243
3.1.2 당뇨 (Diabetes) 246
3.1.3 고지질혈증 (Hyperlipidemia) 248
3.1.4 흡연 (Smoking) 251
3.1.5 음주 (Alcohol) 253
3.1.6 비만 (Obesity) 254
3.1.7 육체적활동및운동 (Physical activity and exercise) 255
3.1.8 식이 (Diet) 257
3.1.9 고호모시스테인혈증 (Hyperhomocysteinemia) 259
3 뇌졸중이차예방Secondary prevention of stroke
3.2 비심장탓색전성뇌졸중또는일과성뇌허혈의항혈전제치료 261
Antithrombotic therapy for noncardioembolic stroke or transient ischemic attack
3.2.1 항혈소판제 (Antiplatelet therapy) 261
3.2.1.1 아스피린 (Aspirin) 261
3.2.1.2 Thienopyridine 계열약물 (Thienopyridine) 2010.3 개정 263
3.2.1.3 기타항혈소판제(Other antiplatelets agents: triflusal, dipyridamole, cilostazol) 2012.4 개정 266
3.2.1.4 항혈소판제병합치료 (Antiplatelet combination therapy) 270
3.2.2 항응고제 (Anticoagulation) 273
3.2.3 특정상황에서항혈소판제사용 (Specific consideration of antiplatelet agents) 275
3.2.3.1 항혈소판제복용중발생한허혈뇌졸중 (Ischemic stroke 275
while taking antiplatelet agent)
3.2.3.2 뇌출혈이동반된허혈뇌졸중 (Ischemic stroke mixed with hemorrhage) 277
CLINICAL RESEARCH CENTER FOR STROKE

242
CLINICAL RESEARCH CENTER FOR STROKE
3.3.1 항응고제 (Anticoagulants) 283
3.3.2 항혈소판제또는병합치료 (Antiplatelet therapy or combination therapy) 285
3.3.3 특정질환의치료 (Specific conditions) 286
3.3.3.1 심방세동 (Atrial fibrillation) 286
3.3.3.2 울혈성심부전 (Congestive heart failure) 289
3.3.3.3 급성심근경색 (Acute myocardial infarction) 291
3.3.3.4 심장판막질환 (Valvular heart disease) 294
3.4.1 두개강외경동맥협착 (Extracranial carotid artery stenosis) 2011.11 개정 298
3.4.2 척추뇌바닥동맥협착 (Vertebrobasilar artery stenosis) 307
3.4.3 두개강내동맥협착 (Intracranial artery stenosis) 309
3.4.4 두개강외-두개강내동맥우회로술(Extracranial-intracranial artery bypass surgery) 312
3.3 심장탓색전성뇌졸중또는일과성허혈발작의항혈전제치료 283
Antithrombotic therapy of cardioembolic stroke or TIA
3.4 혈관협착-폐쇄질환에서수술또는중재적치료 298
Surgical or interventional treatment of large artery steno-occlusive disease
3.5.1 뇌내출혈의이차예방 (Secondary prevention of intracerebral hemorrhage) 315
3.5.2 출혈을동반한허혈뇌졸중의이차예방 (Secondary prevention in ischemic 317
stroke mixed with hemorrhage)
3.5.3 동맥박리 (Arterial dissection) 321
3.5.4 열린타원구멍과심방중격동맥류(Patent foramen ovale and atrial septal aneurysm) 324
3.5.5 항인지질항체증후군 (Antiphospholipid antibody syndrome) 327
3.5.6 정맥성뇌경색 (Venous infarction) 329
3.5 기타특정질환의치료Management of other specific conditions 315

243
3.1. 위험인자조절Risk factor contol
고혈압의치료에따른뇌졸중의일차예방효과는무작위 조군연구(Randomized controlled trial;
RCT)의메타분석결과30-40%에이르는것으로확인되었지만,1뇌졸중이후이차예방을위한고혈압
치료의근거는비교적미흡한실정이다.1,2그러나최근까지발표된무작위 조군연구를취합한
규모메타분석2연구결과, 뇌졸중환자들의혈압치료를통해사망률과뇌졸중및혈관질환의재발이
유의하게감소하는것이확인되었다.
1. Antihypertensive treatment is recommended for both prevention of recurrent stroke and prevention of
other vascular events in persons who have had an ischemic stroke or TIA and are beyond the hyperacute
period (ASA Class 1 Level of Evidence A). Because this benefit extends to persons with and without a
history of hypertension, this recommendation should be considered for all ischemic stroke and TIA
patients (ASA: Class IIa, Level of Evidence B).
2. After stroke or TIA, blood pressure should be lowered, irrespective of its level, with a diuretic and/or an
ACE inhibitor, subject to toleration of the treatment. (EUSI: LEVEL I) The effectiveness of other classes of
BP lowering drugs has not yet been established by controlled trials.
3. An absolute target BP level and reduction are uncertain and should be individualized, but benefit has
been associated with an average reduction of 10/5 mm Hg, and normal BP levels have been defined as
<120/80mmHg by JNC-7 (ASA: Class IIa, Level of Evidence B). The optimal drug regimen remains
uncertain; however, the available data support the use of diuretics and the combination of diuretics and
an ACEI (ASA: Class I, Level of Evidence A).
4. Several lifestyle modifications have been associated with blood pressure reductions and should be
3.1.1. 고혈압Hypertension
CLINICAL RESEARCH CENTER FOR STROKE

included as part of a comprehensive antihypertensive therapy (ASA: Class IIb, Level of Evidence C).
5. The choice of specific drugs and targets should be individualized on the basis of reviewed data and
consideration of specific patient characteristics (eg, extracranial cerebrovascular occlusive disease, renal
impairment, cardiac disease, and diabetes) (ASA: Class IIb, Level of Evidence C).
CLINICAL RESEARCH CENTER FOR STROKE
발병3주-14개월이후의일과성허혈발작과허혈및출혈뇌졸중환자를 상으로진행되었던7개의
고혈압약물무작위 조군연구를취합하여메타분석한결과, 적절한혈압치료는 상환자들의뇌
졸중, 혈관질환및사망률감소에유의한효과를보 다.2
혈압저하정도와뇌졸중이차예방효과의관련성은아직논란이있는분야이다. 특히 Heart
Outcomes Prevention Evaluation(HOPE) 연구3 결과, 안지오텐신전환효소억제제 (angiotension
converting enzyme inhibitor; ACEI)인라미프릴(ramipril) 투약군과 조군간에혈압차이는뚜렷하지않
았음에도불구하고,(평균차이3/2mmHg) 뇌졸중, 심근경색및사망률이24% 감소하 다.(95% CI, 5-
40%) 그러나이러한결과는혈압측정방법의차이로인한것일수도있다는보고가있으므로결과의
해석에주의를요한다.4
약6,000여명의뇌졸중및일과성허혈발작환자를 상으로ACEI인페린도프릴(perindopril)과이뇨제
인인다파마이드(indapamide)를병용투여하여무작위 조군연구를진행한 Perindopril Protection
Against Recurrent Stroke Study(PROGRESS) 연구5결과, ACEI와이뇨제를복합투여한경우뇌졸중재
발은43%(95% CI, 30-54%), 주요혈관질환재발은40%(95% CI, 29-49%) 감소하 다. 흥미롭게도이연
구에서ACEI의단독투여는유의한효과를보이지않았다는점, 그리고혈압이높지않았던뇌졸중환
자들도ACEI와이뇨제병용투여로혈관질환의재발을효과적으로감소시킬수있었다는점이보고
되었다. 이러한결과로 Joint National Committee-7(JNC 7) 보고서는허혈뇌졸중환자들에게ACEI와
이뇨제병용투여를권장하고있다.6
특정항고혈압제가뇌졸중환자들의이차예방에효과적이라는확실한근거는아직부족하다. 그렇
지만PROGRESS 연구를포함한메타분석을통해이뇨제와ACEI의병용투여가뇌졸중이차예방에효
과적이라는사실이알려졌다.2그러나메타분석결과에서도ACEI의단독투여또는ACEI와베타차단
제의병용투여는유의한이차예방효과를보이지않았다.2따라서아직까지뇌졸중의이차예방에유
244

CLINICAL RESEARCH CENTER FOR STROKE
1. 급성기이후허혈뇌졸중또는일과성허혈발작환자의혈압치료는뇌졸중및주요혈관질환의재
발감소에중요하다. (근거수준 Ia, 권고수준A) 이러한치료효과는뇌졸중발병전의고혈압병력과
는무관하므로, 모든허혈뇌졸중환자들은적절하게혈압을조절하는것이권장된다. (근거수준
Ib, 권고수준A)
2. 고혈압약제의선택과혈압저하의목표치는협착혹은폐쇄성두개외혈관질환유무, 당뇨병이나
신장질환동반유무등환자의상태에따라선택적으로고려되어야한다. (근거수준IV, 권고수준C)
3. 허혈뇌졸중환자를위한적절한고혈압약제선택은관련근거가부족하여아직논란이있으나,
ACEI와이뇨제의병용투여가권장될수있다. (근거수준Ib, 권고수준A)
4. 혈압조절을위해약물요법과함께다양한생활방식개선이동반되어야한다. (근거수준 IV, 권고수
준C)
효한항고혈압제계열및같은계열의항고혈압제중더욱효과적인약물에 해서는결론을내리기
어렵다.
허혈뇌졸중발생1주일이내의급성기환자를 상으로진행된무작위 조군연구에서안지오텐신
수용체차단제(angiotencin-receptor blocker; ARB)를 1주일간투여한후, 12개월이후사망률에유의
한차이가관찰되었다.7 (OR, 0.475; 95% CI, 0.252-0.895) 이결과를통해비교적급성기에투여한ARB
의치료효과에 한기 가모아지고있으나향후좀더 규모연구가진행되어야할것이다.
245
1. Lawes CM, Bennett DA, Feigin VL, Rodgers A. Blood pressure and stroke: An overview of published reviews.
Stroke.2004;35:776-785.
2. Rashid P, Leonardi-Bee J, Bath P. Blood pressure reduction and secondary prevention of stroke and other
vascular events: A systematic review. Stroke. 2003;34:2741-2748.
3. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme
inhibitor, ramipril, on cardiovascular events in high-risk patients. The heart outcomes prevention evaluation
study investigators. N Engl J Med. 2000;342:145-153.

4. Svensson P, de Faire U, Sleight P, Yusuf S, Ostergren J. Comparative effects of ramipril on ambulatory and
office blood pressures: A HOPE substudy. Hypertension. 2001;38:E28-32.
5. PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen
among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet.2001;358:1033-1041.
6. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., Jones DW, Materson BJ, Oparil S,
Wright JT, Jr., Roccella EJ. The seventh report of the Joint National Committee on prevention, detection,
evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA. 2003;289:2560-2572.
7. Schrader J, Luders S, Kulschewski A, Berger J, Zidek W, Treib J, Einhaupl K, Diener HC, Dominiak P. The
ACCESS study: Evaluation of acute candesartan cilexetil therapy in stroke survivors. Stroke. 2003;34:1699-
1703.
CLINICAL RESEARCH CENTER FOR STROKE
246
당뇨병은허혈뇌졸중환자의15-33%에서동반된다.1,2이는뇌졸중재발의중요한예측인자이며,3다
발성열공경색과높은연관성을보인다고알려져있다.4
여러임상연구에서혈당조절은소혈관합병증의발생빈도를낮추는효과가보고되어,5,6여러뇌졸중
및심혈관질환의이차예방을위한진료지침에서혈당조절을권고하고있다. 그러나혈당조절이
혈관합병증의발생에미치는효과에 한근거는제한적이다.
3.1.2 당뇨Diabetes
1. Glucose control is recommended to near normoglycemic levels among diabetics with ischemic stroke
or TIA to reduce microvascular complications (ASA: Class I, Level of Evidence A) and possibly
macrovascular complications (ASA: Class IIb, Level of Evidence B).
2. The goal for hemoglobin A1c should be <7% (ASA: Class IIa, Level of Evidence B).

CLINICAL RESEARCH CENTER FOR STROKE
당뇨병을갖고있는뇌졸중환자는당뇨병이없는경우에비하여뇌졸중재발률이1.85배증가되며,
재발된뇌졸중의9.1%는당뇨병에기인하는것으로알려져있다.7
제1형과2형당뇨환자에서철저한혈당조절은심혈관질환의위험을감소시키는경향을보 으나
통계적인유의성은없었다.8한편무작위배정임상연구들의분석결과에서정상수치로지속적인혈
당조절을하 을때혈관질환의발생빈도가감소함을보여주었다.9
1. 당뇨병을동반한뇌졸중환자에서소혈관합병증(근거수준 Ia, 권고수준A) 및 혈관합병증(근거
수준IIa, 권고수준B)의예방을위해혈당을가능한한정상수준으로조절하도록추천된다.
2. HbA1c의목표수치가7%미만이되도록혈당을조절하는것이바람직하다. (근거수준 IIb, 권고수준
B)
247
1. Karapanayiotides T, Piechowski-Jozwiak B, van Melle G, Bogousslavsky J, Devuyst G. Stroke patterns,
etiology, and prognosis in patients with diabetes mellitus. Neurology. 2004;62:1558-1562.
2. Megherbi SE, Milan C, Minier D, Couvreur G, Osseby GV, Tilling K, Di Carlo A, Inzitari D, Wolfe CD, Moreau T,
Giroud M. Association between diabetes and stroke subtype on survival and functional outcome 3 months
after stroke: Data from the European Biomed stroke project. Stroke. 2003;34:688-694.
3. Petty GW, Brown RD, Jr., Whisnant JP, Sicks JD, O'Fallon WM, Wiebers DO. Survival and recurrence after first
cerebral infarction: A population-based study in Rochester, Minnesota, 1975 through 1989. Neurology.
1998;50:208-216.
4. Mast H, Thompson JL, Lee SH, Mohr JP, Sacco RL. Hypertension and diabetes mellitus as determinants of
multiple lacunar infarcts. Stroke. 1995;26:30-33.
5. Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, Kojima Y, Furuyoshi N, Shichiri M. Intensive
insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with
non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. Diabetes Res Clin Pract.

1995;28:103-117.
6. Reichard P, Nilsson BY, Rosenqvist U. The effect of long-term intensified insulin treatment on the development
of microvascular complications of diabetes mellitus. N Engl J Med. 1993;329:304-309.
7. Hillen T, Coshall C, Tilling K, Rudd AG, McGovern R, Wolfe CD. Cause of stroke recurrence is multifactorial:
Patterns, risk factors, and outcomes of stroke recurrence in the south London stroke register. Stroke.
2003;34:1457-1463.
8. UK prospective diabetes study (UKPDS) group. Intensive blood-glucose control with sulphonylureas or insulin
compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33).
Lancet.1998;352:837-853.
9. American Diabetic Association. Standards of medical care for patients with diabetes mellitus. Diabetes Care.
2003;26 Suppl 1:S33-50.
CLINICAL RESEARCH CENTER FOR STROKE
1. Ischemic stroke or TIA patients with elevated cholesterol, comorbid CAD, or evidence of an
248
고지질혈증은관상동맥질환의중요한위험요인이지만, 일반적으로뇌졸중과의연관성은뚜렷하지
않다.1뇌졸중이관상동맥질환과병리기전의상당부분을공유하면서도고지질혈증과의연관성이
뚜렷하지않은이유는, 뇌졸중의다양한아형때문인것으로생각되고있다. 출혈뇌졸중의경우, 많
은코호트연구에서낮은콜레스테롤농도와출혈뇌졸중의발생률및사망률이연관된다는결과가
있다.2,3따라서서양에비해출혈뇌졸중환자가많은국내사황을고려할때, 이에 한조심스런접근
이필요하다. 한편허혈뇌졸중, 특히죽상경화성뇌졸중은고지질혈증이중요한위험요인으로작용
할것으로생각되며, 이는여러스타틴(statin) 관련임상연구를통해밝혀졌다.4,5특히스타틴은콜레스
테롤저하작용뿐아니라다양한세포보호기전을가지고있으므로이에 한고려가필요하다.
3.1.3 고지질혈증Hyperlipidemia

CLINICAL RESEARCH CENTER FOR STROKE
고지혈증의조절에관한사항은 National Cholesterol Education Program(NCEP) Expert Panel on
Detection, Evaluation, and Treatment of High Cholesterol in Adults(Adult Treatment Panel III)에서자세히
고찰한바있다.6,7그러나이지침이발간될당시 부분의연구는고지혈증혹은관상동맥질환을가
지고있는환자에서시행된것으로뇌졸중이차예방을위한연구는없었다. 최근결과가발표된
SPARCL(Stroke Prevention by Aggressive Reduction in Cholesterol Levels Study) 연구는4저 도콜레스
테롤(LDL cholesterol)이 100-190mg/dL인뇌졸중혹은일과성허혈발작(transient ischemic attack) 환
자 4,731 명을 상으로아토바스타틴(atorvastatin)을하루 80mg 투여한무작위 조군연구로서,
조군에비해치료군에서 5년뇌졸중의발생률을 16%(hazard ratio, 0.84) 감소시키는효과를보 다.
하지만이연구에서는출혈뇌졸중환자가불과93명(2.0%) 밖에포함되지않았고, 출혈뇌졸중의발
생률은 조군에비해66% 증가한결과(hazard ratio, 1.66)을보 으므로해석에유의를요한다. 출혈
뇌졸중만을 상으로진행된직접적인연구는아직없으나, 많은양질의코호트연구와계통적분석
에서낮은콜레스테롤농도가출혈뇌졸중의발생률및사망률을증가시킨다는보고를한바있다.2,3
atherosclerotic origin should be managed according to NCEP III guidelines, which include lifestyle
modification, dietary guidelines, and medication recommendations (ASA: Class I, Level of Evidence A,
EUSI: level I).
2. Statin agents are recommended, and the target goal for cholesterol lowering for those with CHD or
symptomatic atherosclerotic disease is an LDL-C of <100mg/dL and LDL-C <70mg/dL for very-high-
risk persons with multiple risk factors (ASA: Class I, Level of Evidence A).
3. Patients with ischemic stroke or TIA presumed to be due to an atherosclerotic origin but with no
preexisting indications for statins (normal cholesterol levels, no comorbid CAD, or no evidence of
atherosclerosis) are reasonable to consider for treatment with a statin agent to reduce the risk of
vascular events (ASA: Class IIa, Level of Evidence B).
249

1. 허혈뇌졸중의경우, 고지질혈증은반드시교정되어야하며, 죽상경화성동맥질환에의한허혈뇌
졸중이나관상동맥질환을동반한허혈뇌졸중환자의고지질혈증치료기준은NCEP-ATP III의기
준을따른다. 생활방식의변경, 식이요법, 약물등이고려될수있으며, 약물의경우에는스타틴약
제의사용이추천된다. (근거수준Ia, 권고수준A)
2. 관상동맥질환을동반하거나증후성죽상경화성허혈뇌졸중환자의콜레스테롤교정목표는저
도콜레스테롤을기준으로하여100mg/dL 이하이다. (근거수준Ia, 권고수준A)
3. 다발성의위험질환을동반한고위험군환자들의경우, 더욱적극적인치료를고려해볼수있다.
(근거수준Ia, 권고수준A)
CLINICAL RESEARCH CENTER FOR STROKE
1. Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective
cohorts. Prospective studies collaboration. Lancet. 1995;346:1647-1653.
2. Blood pressure, cholesterol, and stroke in Eastern Asia. Eastern stroke and coronary heart disease
collaborative research group. Lancet. 1998;352:1801-1807.
3. Iso H, Jacobs DR, Jr., Wentworth D, Neaton JD, Cohen JD. Serum cholesterol levels and six-year
mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J
Med. 1989;320:904-910.
4. Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, Sillesen H,
Simunovic L, Szarek M, Welch KM, Zivin JA. High-dose atorvastatin after stroke or transient ischemic
attack. N Engl J Med. 2006;355:549-559.
5. Amarenco P, Tonkin AM. Statins for stroke prevention: Disappointment and hope. Circulation.
2004;109:III44-49.
6. Executive summary of the third report of the national cholesterol education program (NCEP) expert
panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel
III). JAMA. 2001;285:2486-2497.
7. Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr., Clark LT, Hunninghake DB, Pasternak RC, Smith SC,
250

CLINICAL RESEARCH CENTER FOR STROKE
흡연은모든연령, 성별, 인종에서1,2허혈뇌졸중의중요한독립적위험인자로서,1,3비흡연자에비해
흡연자에서뇌졸중의위험도는2배정도증가한다.1흡연이뇌졸중의위험을증가시키는기전은혈
류역학적인변화와4혈관협착으로생각된다.5,6
1. All healthcare providers should strongly advise every patient with stroke or TIA who has smoked in the
last year to quit (ASA: Class I, Level of Evidence C).
2. Avoidance of environmental tobacco smoke is recommended (ASA: Class IIa, Level of Evidence C).
3. Counseling, nicotine products, and oral smoking cessation medications have been found to be effective in
helping smokers to quit (ASA: Class IIa, Level of Evidence B).
윤리적인문제로뇌졸중후흡연에 한무작위임상연구를수행할수없으므로, 뇌졸중후금연에
한임상연구근거는없다. 그러나관찰연구결과금연후뇌졸중의위험이감소하기시작하며, 흡
연으로인해증가되었던위험도는금연5년이지나면소실됨을알수있다.2,7더욱이금연은뇌졸중
과연관된입원비율을감소시켜8간접적인이차예방효과가있음을뒷받침하고있다.
간접흡연도뇌졸중을포함한심혈관계질환의위험을높인다는연구가있고,9,10흡연의빈도가높은
것을감안한다면간접흡연도중요한위험요인으로고려해야할것이다.
흡연에 한만성의존의치료에있어효과적인행동및약물치료요법이도움이된다. 니코틴 체
요법11과사회적지지요법, 그리고행동훈련이금연의효과적인치료방법이다.
Jr., Stone NJ. Implications of recent clinical trials for the national cholesterol education program adult
treatment panel III guidelines. Circulation. 2004;110:227-239.
3.1.4 흡연Smoking
251
1. 흡연하는뇌졸중환자에게금연을강력히권고하여야한다. (근거수준IV, 권고수준C)
2. 뇌졸중환자는간접흡연도피하도록권고하여야한다. (근거수준IIb, 권고수준B)
CLINICAL RESEARCH CENTER FOR STROKE
1. Shinton R, Beevers G. Meta-analysis of relation between cigarette smoking and stroke. Bmj.
1989;298:789-794.
2. Wannamethee SG, Shaper AG, Whincup PH, Walker M. Smoking cessation and the risk of stroke in
middle-aged men. JAMA. 1995;274:155-160.
3. Robbins AS, Manson JE, Lee IM, Satterfield S, Hennekens CH. Cigarette smoking and stroke in a cohort
of U.S. Male physicians. Ann Intern Med. 1994;120:458-462.
4. O'Donnell CJ, Larson MG, Feng D, Sutherland PA, Lindpaintner K, Myers RH, D'Agostino RA, Levy D,
Tofler GH. Genetic and environmental contributions to platelet aggregation: The Framingham heart
study. Circulation. 2001;103:3051-3056.
5. Kool MJ, Hoeks AP, Struijker Boudier HA, Reneman RS, Van Bortel LM. Short- and long-term effects of
smoking on arterial wall properties in habitual smokers. J Am Coll Cardiol. 1993;22:1881-1886.
6. Mast H, Thompson JL, Lin IF, Hofmeister C, Hartmann A, Marx P, Mohr JP, Sacco RL. Cigarette
smoking as a determinant of high-grade carotid artery stenosis in Hispanic, black, and white patients
with stroke or transient ischemic attack. Stroke. 1998;29:908-912.
7. Kawachi I, Colditz GA, Stampfer MJ, Willett WC, Manson JE, Rosner B, Speizer FE, Hennekens CH.
Smoking cessation and decreased risk of stroke in women. JAMA.1993;269:232-236.
8. Naidoo B, Stevens W, McPherson K. Modelling the short term consequences of smoking cessation in
England on the hospitalisation rates for acute myocardial infarction and stroke. Tob Control. 2000;9:397-
400.
9. You RX, Thrift AG, McNeil JJ, Davis SM, Donnan GA. Ischemic stroke risk and passive exposure to
spouses' cigarette smoking. Melbourne stroke risk factor study (MERFS) group. Am J Public Health.
1999;89:572-575.
252

CLINICAL RESEARCH CENTER FOR STROKE
음주는고혈압, 과응고경향, 뇌혈류감소, 심방세동등과연관되어뇌졸중의독립적인위험인자중
하나로알려져있다.
1. Patients with ischemic stroke or TIA who are heavy drinkers should eliminate or reduce their
consumption of alcohol (ASA; Class I, Level of Evidence A).
2. Light to moderate levels of no more than 2 drinks per day for men and 1 drink per day for nonpregnant
women may be considered (ASA, Class IIb, Level of Evidence C).
ASA에서는뇌졸중환자의과도한음주를제한해야한다고명시하면서높은수준의근거가있다고
하 지만, 실제로뇌졸중발생이후이차예방에있어서음주에관한연구가제 로수행된바는없
다. 그러나, 과도한음주는일차예방에서의결과와크게다르지않을것이고, 사회적으로도중요한
이슈이기때문에일반적으로과도한음주를자제하도록권고하고있다. 2003년도출판된Reynolds
등의메타분석결과1는일차예방에관한것으로여기에서는다루지않는다.
10. He J, Vupputuri S, Allen K, Prerost MR, Hughes J, Whelton PK. Passive smoking and the risk of
coronary heart disease--a meta-analysis of epidemiologic studies. N Engl J Med.1999;340:920-926.
11. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation.
Cochrane Database Syst Rev. 2004:CD000146.
3.1.5 음주Alcohol
253

1. 뇌졸중환자중과도음주자(heavy alcoholics)는최 한음주량을줄여야한다. (근거수준 IV, 권고수
준C)
CLINICAL RESEARCH CENTER FOR STROKE
1. Reynolds K, Lewis B, Nolen JD, Kinney GL, Sathya B, He J. Alcohol consumption and risk of stroke: A
meta-analysis. JAMA. 2003;289:579-588.
1. Weight reduction may be considered for all overweight ischemic stroke and TIA patients to maintain the
goal of a BMI of between 18.5 and 24.9 kg/m2 and a waist circumference of <35 in for women and <40 in
for men (ASA: Class IIb, Level of Evidence C).
2. Clinicians should encourage weight management through an appropriate balance of calorie intake,
physical activity, and behavioral counseling.
한국의보험공단자료를분석한연구결과에따르면비만과과체중을가진 상군이정상군에서비해
허혈및출혈뇌졸중의상 위험도가높았고,1체중이증가할수록뇌졸중의위험도가증가한다.1-3비
록체중을줄여뇌졸중의발생률을감소시켰다는임상연구는시행된바없으나, 체중감량은혈압강
하를통해뇌졸중의발병률감소에기여한다고알려져있다.4
254
비만과과체중은뇌졸중의발병과관련이있다고생각되고있으며, 그정도는체중의증가와비례한
다고알려져있다.
3.1.6 비만Obesity
CLINICAL RESEARCH CENTER FOR STROKE
1. 체중의증가는뇌졸중발생률의증가와관련되어있으며, 이는용량의존적인관계를보여준다. 따
라서과체중혹은비만일경우적극적으로체중을감량하는것이권장된다. (근거수준 IV, 권고수준
C)
255
1. Song Y, Sung J, Davey Smith G, Ebrahim S. Body mass index and ischemic and hemorrhagic stroke: A
prospective study in Korean men. Stroke. 2004;35:831- 836.
2. Kurth T, Gaziano J, Berger K, Kase C, Manson J. Body mass index and the risk of stroke in men. Arch Intern
Med.2002;162:2557-2562.
3. Rich-Edwards J, Speizer F, Manson J. A prospective study of body mass index, weight change, and risk of
stroke in women. JAMA.1997;277:1539 -1545.
4. Neter J, Stam B, Kok F, Grobbee D, Gelejinse J. Influence of weight reduction on blood pressure: A meta-
analysis of randomized controlled trials. Hypertension. 2003;42:878-884.
1. For patients with ischemic stroke or TIA who are capable of engaging in physical activity, at least 30 minutes
of moderate-intensity physical exercise most days may be considered to reduce the risk factors and
comorbid conditions that increase the likelihood of recurrence of stroke (ASA: Class IIb, Level of Evidence C).
3.1.7 육체적활동및운동Physical activity and exercise
신체활동은뇌졸중발병위험과반비례관계가있는것으로여겨진다. 하지만이러한관계가심층적
으로연구된바없다. 신체활동과운동은뇌졸중의위험인자를감소시켜발병위험을억제하는것으
로알려져있다.

2. For those individuals with disability after ischemic stroke, a supervised therapeutic exercise regimen is
recommended.
CLINICAL RESEARCH CENTER FOR STROKE
The Framingham Heart Study, Honolulu Heart Program 및Oslo Study 등은신체활동이남자에게있어
서뇌졸중에 해보호효과를가지는것을보고하 고,1-3 Nurses’Health Study와 Copenhagen City
Heart Study 등은여성에있어신체활동이뇌졸중의발병률과반비례관계를가짐을보여주었다.4,5신
체적활동이가지는보호효과는체중의감소및고혈압, 당뇨등뇌졸중위험인자의조절등을통해
나타나는것으로알려져있으며,5-7이러한효과외에도혈장내피브리노겐및혈소판의기능을감소
시키고조직플라스미노겐활성제의기능과고 도콜레스테롤(HDL cholesterol)의농도를상승시키
는것으로알려져있다.8-10
1. 신체활동과운동은혈압강하, 체중의감소, 혈중콜레스테롤의변화등을통해뇌졸중의위험을낮
추는것으로알려져있으므로규칙적인운동이추천된다. (근거수준IV, 권고수준C).
1. Abbott R, Rodriguez B, Burchfiel C, Curb J. Physical activity in older middle-aged men and reduced risk
of stroke: The Honolulu heart program. Am J Epidemiol1994;139:881- 893.
2. Haheim L, Holme I, Hjermann I, Leren P. Risk factors of stroke incidence and mortality. A 12-year follow-
up of the Oslo study. Stroke. 1993;24:1484 -1489.
3. Kiely DK, Wolf PA, Cupples LA, Beiser AS, Kannel WB. Physical activity and stroke risk: The Framingham
study. Am J Epidemiol. 1994;140:608-620.
4. Lindenstrom E, Boysen G, Nyboe J. Lifestyle factors and risk of cerebrovascular disease in women. The
Copenhagen city heart study. Stroke. 1993;24:1468 -1472.
5. Manson J, Colditz G, Stampfer M. A prospective study of maturity-onset diabetes mellitus and risk of
256
CLINICAL RESEARCH CENTER FOR STROKE
식이습관이뇌졸중의위험도와관련이있다는것은여러연구에서밝혀졌다. 과일과채소를많이
섭취하면뇌졸중의위험도를낮출수있다고알려져있고, 나트륨과칼륨같은무기질도뇌졸중의
발병과관련되어있다.
1. A reduced intake of sodium and increased intake of potassium is recommended to lower blood pressure in
persons with hypertension, which may thereby reduce the risk of stroke (ASA: Class I, Level of Evidence A).
2. The recommended sodium intake is ≤2.3g/d (100mmol/d), and the recommended potassium intake is
≥4.7g/d (120mmol/d).
3. The DASH diet, which emphasizes fruit, vegetables, and low-fat dairy products and is reduced in
coronary heart disease and stroke in women. Arch Intern Med1991;151:1141-1147.
6. Kokkinos P, Holland J, Pittaras A, Naraya P, Dotson C, Papademetriou V. Cardiorespiratory fitness and
coronary heart disease risk factor association in women. J Am Coll Cardiol.1995;26:358 -364.
7. Paffenbarger R, Jr, Gibbons L. Influences of cardiorespiratory fitness and other precursors on
cardiovascular disease and all-cause mortality in men and women. JAMA.1996;276:205-210.
8. Lakka T, Salonen J. Moderate to high intensity conditioning leisure time physical activity and high
cardiorespiratory fitness are associated with reduced plasma fibrinogen in eastern Finnish men. J Clin
Epidemiol.1993;46:1119 -1127.
9. Wang H, Bashore T, Friedman E. Exercise reduces age-dependent decrease in platelet protein kinase c
activity and translocation. J Gerontol A Biol Sci Med Sci.1995;50A:M12-M16.
10. Williams P. High-density lipoprotein cholesterol and other risk factors for coronary heart disease in
female runners. N Engl J Med. 1996;334:1298-1303.
3.1.8 식이Diet
257

saturated and total fat, also lowers blood pressure and is recommended (ASA: Class Ia, Level of Evidence A).
4. A diet that is rich in fruits and vegetables may lower the risk of stroke and may be considered (ASA: Class
III, Level of Evidence C).
CLINICAL RESEARCH CENTER FOR STROKE
여러전향적인연구를통하여, 과일과채소의섭취가증가하면뇌졸중의위험도가섭취량에비례하
여감소한다고보고되었다.1-4나트륨의섭취가증가하면뇌졸중의위험도가상승하며, 반 로칼륨
섭취량이증가하면뇌졸중의위험도가감소한다.5-8 이같은효과는이들무기질이주로혈압에 향
을주기때문이지만, 혈압과무관한기전으로도뇌졸중의발생에 향을미치는것으로알려져있다.9
1. 나트륨의일일섭취량을줄이고칼륨의섭취량을늘리는것이뇌졸중의예방을위해권장된다. (권
고수준GPP)
2. 과일과채소를많이섭취하는것이뇌졸중예방에도움이될수있다. (권고수준GPP)
1. Steffen L, Jacobs D, Jr., Stevens J, Shahar E, Carithers T, Folsom A. Associations of whole-grain, refined-
grain, and fruit and vegetable consumption with risks of all-cause mortality and incident coronary artery
disease and ischemic stroke: The atherosclerosis risk in communities (ARIC) study. Am J Clin Nutr.
2003;78:383-390.
2. Sauvaget C, Nagano J, Allen N, Kodama K. Vegetable and fruit intake and stroke mortality in the
Hiroshima/Nagasaki life span study. Stroke. 2003;34:2355-2360.
3. Johnsen S, Overvad K, Stripp C, Tjonneland A, Husted S, Sorensen H. Intake of fruit and vegetables and
the risk of ischemic stroke in a cohort of Danish men and women. Am J Clin Nutr.2003;78:57-64.
4. Joshipura K, Ascherio A, Manson J, Stampter M, Rimm E, Speizer F, Hennekens C, Spiegelman D,
Wallett W. Fruit and vegetable intake in relation to risk of ischemic stroke. JAMA. 1999;282:1233-1239
5. He J, Ogden L, Vupputuri S, Bazzano L, Loria C, Whelton P. Dietary sodium intake and subsequent risk of
258

CLINICAL RESEARCH CENTER FOR STROKE
고호모시스테인혈증은뇌졸중과관상동맥질환을포함하는죽상경화증의발병에기여한다고알려
져있다. 그러나엽산등의비타민을투여하여혈중호모시스테인농도를낮추었을때뇌졸중의위
험도가감소하는지는아직뚜렷하지않다.
1. For patients with ischemic stroke or TIA and hyperhomocysteinemia (levels > 10μmol/L), daily standard
multivitamin preparations with adequate B6 (1.7mg/d), B12 (2.4μg/d), and folate (400μg/d) are reasonable to
reduce the level of homocysteine, given their safety and low cost (ASA: Class IIa, Level of Evidence B).
However, there is no evidence that reducing homocysteine levels will lead to a reduction in stroke recurrence.
cardiovascular disease in overweight adults. JAMA. 1999;282:2027-2034.
6. Nagata C, Takatsuka N, Shimizu N, Shimizu H. Sodium intake and risk of death from stroke in
Japanese men and women. Stroke. 2004;35:1543-1547.
7. Khaw K, Barrett-Connor E. Dietary potassium and stroke-associated mortality. A 12-year prospective
population study. N Engl J Med. 1987;316:235-240.
8. Ascherio A, Rimm E, Hernan M, Giovannucci E, Kawachi I, Stampfer M, Wellet W. Intake of potassium,
magnesium, calcium, and fiber and risk of stroke among US men. Circulation. 1998;98:1198-1204.
9. Tobian L, Lange J, Ulm K, Wold L, Iwai J. Potassium prevents death from strokes in hypertensive rats
without lowering blood pressure. J Hypertens. 1984;2:S363-S366.
3.1.9 고호모시스테인혈증Hyperhomocysteinemia
259
혈중아미노산의 사산물인호모시스테인의상승이죽상경화를유발하고관상동맥질환이나뇌경색등
의허혈질환과관련되어있다는것은잘알려져있다.1이에따라엽산이나비타민B6, 비타민B12등의보

조인자의투여를통해혈중호모시스테인의농도를감소시킴으로써허혈뇌졸중의위험도를낮출수있
다는가설이제기되었다. 그러나고농도의비타민을투여했을때혈중호모시스테인의농도가낮아진다
는보고는많이발표되었으나, 실제뇌경색의발병자체를낮춘다는근거는아직없다.2
구미의연구에서는혈중호모시스테인농도가뇌경색과깊은관계가있다고하는보고가있으며, 일본의
연구에서는혈중호모시스테인농도가 조군(7.3nmol/mL)에비해뇌경색군에서(13.1nmol/mL) 높았다고
한다.3혈중호모시스테인농도는엽산의섭취로낮출수있는데, 뇌경색재발예방에도효과가있는지에
해서는향후의검토과제로언급하고있다. 국내의연구에서도 조군에비해뇌경색군에서혈중호모시
스테인의농도가높았다.4 (13.4±6.6 μmol/L vs. 10.3±2.6 μmol/L)
CLINICAL RESEARCH CENTER FOR STROKE
1. 고호모시스테인혈증은기존의고혈압, 당뇨, 고지혈증같은장기적인약물치료를요하는혈관질환
의위험인자와달리, 적은비용으로비교적쉽게치료될수있으므로치료가고려될수있다. (근거
수준IV, 권고수준C)
1. Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart disease and stroke: A
meta-analysis. JAMA.2002;288:2015-2022.
2. Toole J, Malinow M, Chambless L, Spence J, Pettigrew L, Howard V, Sides E, Wang C, Stampfer M.
Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial
infarction, and death: The vitamin intervention for stroke prevention (VISP) randomized controlled trial.
JAMA. 2004;291:565-575.
3. Araki A, Sako Y, Fukushima Y, Matsumoto M, Asada T, Kita T. Plasma sulphydryl-containing amino acids
in patients with cerebral infarction and in hypertensive subjects. Atherosclerosis. 1989;79:139-146.
4. 이명희. 뇌경색위험인자로서의혈청호모시스테인. 한진단검사의학회지. 2005;25:234-240.
260

261
3.2 비심장탓색전성뇌졸중또는일과성뇌허혈의항혈전제치료Antithrombotic therapy for noncardioembolic stroke or transient ischemic attack
1. For patients with non-cardioembolic ischemic stroke or TIA, antiplatelet agents rather than oral
anticoagulation are recommended to reduce the risk of recurrent stroke and other cardiovascular
events (ASA: Class I, Level of Evidence A, EUSI: Level I). Aspirin monotherapy, the combination of aspirin
and extended-release dipyridamole, and clopidogrel monotherapy are all acceptable options for initial
therapy (ASA: Class IIa, Level of Evidence A, EUSI: Level I, RCP: Grade of Recommendation A).
2. Low or medium-dose aspirin (50-325mg) should be given as first choice agent to reduce stroke
recurrence (ASA: Class IIa, Level of Evidence A, EUSI: Level I).
Antithrombotic Trialists Collaboration은뇌경색과일과성허혈발작후하루50-1300mg의경구용아스
피린복용으로, 위약군에비해뇌경색재발, 심근경색, 혈관질환으로인한사망률이22%정도감소하
다고발표하 다.1또한허혈뇌졸중환자에서아스피린을복용하는것은위약복용에비해약1000
명당27명정도의뇌졸중발생이감소한다고보고하여, 아스피린의이차적예방효과를실증하 다.1
CLINICAL RESEARCH CENTER FOR STROKE
저용량아스피린(aspirin)의복용은혈전성그리고색전성뇌경색예방에효과적인것으로알려져있
다. 아스피린의 acetyl기는혈소판막과결합하여 cyclooxygenase를비가역적으로억제하므로
Thromboxane A2 형성을억제한다. 이러한기전을통해아스피린은심근경색, 뇌경색, 그리고말초혈
관질환등의동맥폐쇄성질환의재발방지에효과가있다.
3.2.1. 항혈소판제Antiplatelet therapy
3.2.1.1 아스피린 Aspirin

허혈뇌졸중환자에서아스피린과함께이차예방에사용할수있는약제로는 CAPRIE (Clopidogrel
versus aspirin in patients at risk of ischemic events)2 연구에서보여준클로피도그렐과 ESPS-2
(European stroke prevention study 2)3연구와ESPIRIT (Aspirin plus dipyridamole versus aspirin alone after
cerebral ischaemia of arterial origin)4연구에서보여준아스피린과디피리다몰이있다. 두가지무작위
배정 조군연구결과, 아스피린의용량차이에따른효과의차이는나타나지않았다.5,6그러나하루
300mg 이상의비교적고농도아스피린사용은, 하루300mg 이하의용량과비교해그효과의우수성
이확실히밝혀지지않았다. 또한하루300mg 이상의아스피린을복용할때오히려위장관출혈발생
의가능성이높아사용을피하는것이좋다.7
CLINICAL RESEARCH CENTER FOR STROKE
1. 심장탓뇌색전증을제외한뇌경색과일과성허혈발작환자들은허혈증상재발방지를위해하루
50-300mg 사이의아스피린을사용할수있다.(근거수준Ia, 권고수준A)
1. Antiplatelet trialists' collaboration. Collaborative overview of randomised trials of antiplatelet therapy--I:
Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various
categories of patients.BMJ. 1994;308:81-106.
2. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk
of ischaemic events (CAPRIE). Lancet. 1996;348:1329-1339.
3. Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A. European Stroke Prevention Study 2.
Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke.J Neurol Sci1996;143:1-13.
4. ESPRIT Study Group, Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A. Aspirin plus
dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised
controlled trial. Lancet. 2006;367(9523):1665-1673.
5. The Dutch TIA trial: Protective effects of low-dose aspirin and atenolol in patients with transient ischemic
attacks or nondisabling stroke. The Dutch TIA study group.Stroke. 1988;19:512-517.
262

CLINICAL RESEARCH CENTER FOR STROKE
1. All patients with ischemic stroke or TIA who are not on anticoagulation should be taking an antiplatelet
agent, ie aspirin (50-300mg), daily or clopidogrel, or a combination of low-dose aspirin and dipyridamole
modified release (MR) (RCP: Grade of Recommendation A).
2. Clopidogrel is slightly more effective than aspirin in the prevention of further vascular events (EUSI: Level
of Evidence I, AHA/ASA: Class IIb, Level of Evidence B).
3. Where patients are aspirin intolerant, an alternative antiplatelet agent (eg clopidogrel 75mg daily or
dipyridamole MR 200mg twice daily) should be used (RCP: Grade of Recommendation A, AHA/ASA:
Class IIa, Level of Evidence B).
6. Farrell B, Godwin J, Richards S, Warlow C. The United Kingdom transient ischaemic attack (UK-TIA)
aspirin trial: Final results. J Neurol Neurosurg Psychiatry. 1991;54:1044-1054.
7. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius S, Menard J, Rahn KH, Wedel H,
Westerling S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with
hypertension: Principal results of the hypertension optimal treatment (HOT) randomised trial. Hot study
group. Lancet. 1998;351:1755-1762.
263
비심장탓허혈뇌졸중을가진환자에서뇌졸중의이차적예방을위해서투여되는항혈소판제인
thienopyridine 제재에는티클로피딘(ticlopidine)과클로피도그렐(clopidogrel)이있으며, 이들약제는아
스피린과함께일차약제로선택될수있다. 티클로피딘은호중구감소증이발생할수있으므로안전
성측면에서상 적으로우수한클로피도그렐에비해서유용성이떨어진다.
3.2.1.2 Thienopyridine 계열약물Thienopyridine
개정: 2010.3

CLINICAL RESEARCH CENTER FOR STROKE
264
허혈뇌졸중환자를 상으로실시한연구에서티클로피딘은위약군과비교하여혈관질환의발생
을감소시켰다.1 허혈뇌졸중환자를 상으로티클로피딘을투여할경우아스피린을투여한환자보
다뇌졸중발생이감소한다는보고가있지만, 뇌졸중, 심근경색, 혈관성질환으로인한사망을복합
적인결과로비교하 을때는양군에서의미있는차이가보이지않았다.2,3일과성허혈발작환자와
경도의뇌경색환자를 상으로하루1300mg의아스피린을복용한군과하루250mg의티클로피딘
을2회복용한환자군을비교한TASS (Ticlopidine Aspirin Stroke Study) 연구가진행되었다.2티클로피
딘투여군에서아스피린투여군보다사망이나뇌졸중의발생이13% 감소하 으며, 뇌졸중발생만
을고려하면3년간21%의감소를보여주었다. 이연구에서는뇌졸중과사망률의상 적위험감소
율이초기1년간42%를보 으며, 이런감소율은2년간유지되었다. 하지만, 티클로피딘의상 적인
우위는흑인을 상으로시행된연구(AAASPS, Aftrican American Antiplatelet Stroke Prevention Study)
에서뇌졸중의재발, 심근경색, 또는혈관질환으로인한사망을모두고려할때유의한차이를입증
하지못했다.3
뇌졸중, 심근경색, 말초혈관질환을가진환자를 상으로하루 75mg의클로피도그렐과 325mg의
아스피린을투여한후 3년간뇌경색, 심근경색, 혈관질환으로인한사망률을비교한 CAPRIE
(Clopidogrel versus aspirin in patients at risk of ischemic events) 연구에서, 클로피도그렐이아스피린보
다혈관질환의발생을감소시켰다. (상 위험률감소, 8.7%) 하지만, 뇌졸중환자만을 상으로분석
하 을때는의미있는결과를보여주지못했다.4이연구의사후검정에서뇌경색의과거력또는뇌
허혈의증상이있었던관상동맥질환, 당뇨병환자에서는클로피도그렐이아스피린에비해이차예
방효과가우수하 다.5.6
티클로피딘을투여받은환자중 0.5-2% 정도의환자에서호중구감소증이나타났으나클로피도그
렐은아스피린과 등한결과를보 으므로, 안전성을고려할때클로피도그렐이장점을보 다고
할수있다.1,2,7 클로피도그렐을투여받은군에서는호중구감소증이심각한문제가되지는않았지만
드물게혈전성혈소판감소자색반(thrombotic thrombocytopenic purpura)이보고되었으므로유념해
야한다.8클로피도그렐은325mg의아스피린과비교할때위장출혈이적고, (odds ratio [OR] 0.71; 95%
CI 0.6-0.9) 상부위장장애도적었다. 4,9 (OR 0.84; 95% CI 0.8-0.9) 그러나아스피린과비교할때피부발
진이흔하고 (OR 1.34; 95% CI 1.2-1.5) 설사의발생이많았다. (OR 1.34; 95% CI 1.2 - 1.6) 심장탓뇌경색

CLINICAL RESEARCH CENTER FOR STROKE
265
1. Gent M, Blakely JA, Easton JD, Ellis DJ, Hachinski VC, Harbison JW, Panak E, Roberts RS, Sicurella J, Turpie
AG. The Canadian American Ticlopidine Study (CATS) in thromboembolic stroke. Lancet. 1989;1:1215-1220.
2. Hass WK, Easton JD, Adams HP, Jr., Pryse-Phillips W, Molony BA, Anderson S, Kamm B. A randomized trial
comparing ticlopidine hydrochloride with aspirin for the prevention of stroke in high-risk patients. Ticlopidine
Aspirin Stroke Study Group. N Engl J Med. 1989;321:501-507.
3. Gorelick PB, Richardson D, Kelly M, Ruland S, Hung E, Harris Y, Kittner S, Leurgans S. Aspirin and ticlopidine
for prevention of recurrent stroke in black patients: a randomized trial. JAMA.2003;289:2947-2957.
4. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of
ischaemic events (CAPRIE). Lancet. 1996;348:1329-1339.
5. Bhatt DL, Marso SP, Hirsch AT, Ringleb PA, Hacke W, Topol EJ. Amplified benefit of clopidogrel versus aspirin
in patients with diabetes mellitus. Am J Cardiol. 2002;90:625-628.
환자를제외한1172명의뇌경색환자를 상으로하루75mg의클로피도그렐을복용한군과200mg
의티클로피딘을하루1회복용한환자군을52주동안관찰한연구에서클로피도그렐군이우수한안
전성을보 으나, (7.0% vs 15.1%; p = 0.001) 효과에서는양군간에유의한차이를보여주지못했다.9
1. 클로피도그렐단독투여는아스피린단독투여, 또는아스피린과서방형디피리다몰(dipyridamole)
의복합투여와함께비심장탓허혈뇌졸중환자의일차선택약제로사용할수있다. (근거수준 Ib, 권
고수준A)
2. 아스피린에과민증이있는환자에게는클로피도그렐등다른항혈소판제가권장된다. (근거수준
Ib, 권고수준A)
3. 티클로피딘은아스피린과비교하 을때뇌졸중의이차적예방에도움을줄수있다. (근거수준1b,
권고수준A). 하지만호중구감소증등의위험성이있으므로투약시주의가필요하다.(근거수준 Ib,
권고수준A)

6. Ringleb PA, Bhatt DL, Hirsch AT, Topol EJ, Hacke W. Benefit of clopidogrel over aspirin is amplified in patients
with a history of ischemic events. Stroke.2004;35:528-532.
7. Love BB, Biller J, Gent M. Adverse haematological effects of ticlopidine. Prevention, recognition and
management. Drug Saf.1998;19:89-98.
8. Bennett CL, Connors JM, Carwile JM, Moake JL, Bell WR, Tarantolo SR, McCarthy LJ, Sarode R, Hatfield AJ,
Feldman MD, Davidson CJ, Tsai HM. Thrombotic thrombocytopenic purpura associated with clopidogrel. N
Engl J Med. 2000;342:1773-1777.
9. Fukuuchi Y, Tohgi H, Okudera T, Ikeda Y, Miyanaga Y, Uchiyama S, Hirano M, Shinohara Y, Matsumoto M,
Yamaguchi T. A randomized, double-blind study comparing the safety and efficacy of clopidogrel versus
ticlopidine in Japanese patients with noncardioembolic cerebral infarction. Cerebrovasc Dis 2008;25:40-49.
CLINICAL RESEARCH CENTER FOR STROKE
266
항혈소판제는심장탓뇌색전증을제외한허혈뇌졸중(non-cardioembolic ischemic stroke)의이차예방
을위해서사용된다. 표적인항혈소판제인아스피린(aspirin)과클로피도그렐(clopidogrel) 이외에도
트리플루잘(triflusal)과실로스타졸(cilostazol)이우리나라에서널리사용되고있다. 트리플루잘과실
로스타졸은아스피린이나클로피도그렐과는혈소판응집억제기전이나작용부위가다른항혈소판
제로서출혈의부작용이아스피린보다낮은것으로보고되었다. 디피리다몰(dipyridamole)은아스피
린과병용하여사용할경우에뇌졸중의이차예방에우수한효과를보이고있다.
한편, 제1판한국뇌졸중임상진료지침발간이후인2010년과2011년에실로스타졸의뇌졸중이차예
방효과를아스피린과비교한무작위배정임상연구와1 메타분석결과가2 각각발표되었다. 비록두
연구결과들이최근에보고되어외국의임상진료지침에아직그결과가반 되지않았으나, 연구의
상집단이인종적으로우리와같고실로스타졸이국내에서널리사용되는항혈소판제인점을고려
하여집필위원회에서는이들연구결과를바탕으로실로스타졸에 한진료지침의근거수준과권고
수준을개정하 다.
3.2.1.3 기타항혈소판제Other antiplatelet agents: Triflusal, Dipyridamole, Cilostazol
개정: 2012.4

CLINICAL RESEARCH CENTER FOR STROKE
실로스타졸은phosphodiesterase를억제함으로서혈소판활성화를막고혈관내피세포의기능을안
정화시킨다. 먼저중국에서실시된 Cilostazol versus Aspirin for Secondary Ischaemic Stroke
Prevention (CASISP) 연구는720명의뇌경색환자를 상으로실로스타졸하루200 mg과아스피린하
루100 mg을무작위배정하여평균1년반동안일차종결점으로허혈뇌졸중과출혈뇌졸중또는지
주막하출혈의발생을비교하 다.3비록실로스타졸군의일차종결점발생률이3.6%로아스피린군
의6.4%보다낮았지만통계적으로유의한결과는아니었다. 2010년에발표된CSPS2 연구는무작위
배정된2,757명의뇌경색환자를 상으로실로스타졸100 mg 1일2회투여와아스피린81 mg 1일1
회투여를비교하 다.1평균29개월의추적관찰기간동안뇌경색, 뇌출혈또는지주막하출혈을포
함하는모든유형의뇌졸중이실로스타졸사용군에서2.76%, 아스피린사용군에서는3.71%로실로
스타졸군이아스피린군에비해26%의뇌졸중재발감소효과가있었다. 특히뇌출혈, 지주막하출혈
또는입원을요하는출혈을포함하는주요출혈사건의발생률이실로스타졸사용군에서0.77%로아
267
1. 저용량의아스피린과서방형디피리다몰을함께사용하는것은뇌졸중의이차예방을위한초기치
료로사용할수있다. (근거수준Ib, 권고수준A)
2. 트리플루잘과실로스타졸은아스피린이나클로피도그렐을사용하기어려운경우에뇌졸중의이
차예방목적으로고려될수있다. (근거수준II, 권고수준B)
3. 뇌출혈을포함한심각한출혈의위험이있는환자에게항혈소판제치료가필요할때, 트리플루잘
은뇌졸중의이차예방을위해서추천될수있다. (근거수준Ib, 권고수준A)
1. Compared with aspirin alone, the combination of aspirin and extended-release dipyridamole is safe and
an acceptable option for initial therapy for secondary stroke prevention (AHA/ASA: Class IIa, Level of
Evidence A, EUSI: Level of Evidence I).
2. Patients who do not tolerate either aspirin or clopidogrel may be treated with dipyridamole 200 mg twice
daily (EUSI: Level of Evidence II).

CLINICAL RESEARCH CENTER FOR STROKE
268
스피린투여군의1.78%와비교하여54% 더낮았다. 한편CASISP와CSPS2를합친메타분석에서2 뇌
졸중과심근경색또는혈관성사망을합친병합결과의발생률이실로스타졸사용군에서아스피린
사용군에비해 28% 더났았으며, 출혈뇌졸중의발생은실로스타졸군이약 74% 더낮았다. 하지만
CSPS2 연구 상환자의65%가열공성뇌경색이고, 발생한달후의환자를 상으로하 던점은낮
은재발빈도와함께논란의여지가있는부분이다.
디피리다몰은혈소판활성화경로에있는 phosphodiserase 효소를억제한다.4 European stroke
prevention study-2(ESPS-2) 연구는뇌졸중이나일과성허혈발작의병력이있는 6,602명의환자들을
상으로 (1)아스피린하루50mg과서방형디피리다몰400mg 복합복용군 (2)아스피린만복용한군
(3)서방형디피리다몰을복용한군 (4)위약을복용한군으로나누어비교하 다. 이연구에서뇌졸중
의발생위험은위약군에비해서아스피린사용군에서 18%, 디피리다몰단독사용군에서 16%, 그리
고아스피린과디피리다몰을함께사용한군에서37% 감소하 다.4사망만을비교한경우에는치료
군간의유의한차이가없었다. 그러나이연구는아스피린의용량이너무작았다는점과이전시행한
소규모연구들에서는두가지약제의복합의효과가입증되지않았다는점등의이유로연구결과에
한이론이제기되고있다. 그러나, 2006년에보고된 European/Australasian Stroke Prevention in
Reversible Ischaemia Trial (ESPRIT) 연구는ESPS-2 연구와일치된결과를보고하 다.5 ESPRIT 연구는
무작위배정비맹검방법으로뇌졸중의이차예방에 한아스피린과디피리다몰병용의효과를아
스피린단독투여와비교하여평가하 다. 뇌경색환자에서아스피린과디피리다몰을함께사용하
는것이아스피린을단독으로사용하는것보다뇌졸중, 심근경색및혈관성사망을20% 정도감소시
키는것으로보고되었다. 결론적으로, 통계학적으로충분한검증력을가진연구들을통해서복합제
재의우수성이입증되었다.
Triflusal versus aspirin in cerebral infarction prevention (TACIP) 연구는최근뇌졸중이나일과성뇌허혈
이있었던, 113명의환자를트리플루잘하루600mg 투여군과아스피린하루325mg 투여군으로나눠
서평균30개월을비교하 다.6이연구에서트리플루잘과아스피린은허혈뇌졸중, 심근경색이나혈
관질환에의한사망률에서유의한차이가없었다. (트리플루잘군13.1%, 아스피린군12.4%) 그러나전
체출혈발생률이나심각한출혈발생률이트리플루잘군에서유의하게낮았다. Triflusal versus
aspirin for the prevention of infarction: a randomized stroke study (TAPIRSS) 연구는431명의환자를트리
플루잘600mg 군과아스피린325mg 군으로무작위배정하여평균586일을투여하 다. TAPIRSS연
구에서도역시트리플루잘과아스피린은뇌졸중의이차예방면에서동등한효과를보 으나, 주요
혹은경미한출혈의발생률이트리플루잘군에서유의하게낮았다.7

CLINICAL RESEARCH CENTER FOR STROKE
269
1. 실로스타졸단독치료는비심인성뇌졸중환자, 특히열공성뇌경색환자에서뇌졸중의이차예방에
사용할수있다. (근거수준Ia, 권고수준A)-신설
2. 저용량의아스피린과서방형디피리다몰을함께사용하는것은뇌졸중의이차예방을위한초기치
료로사용할수있다. (근거수준Ib, 권고수준A)
3. 트리플루잘은아스피린이나클로피도그렐을사용하기어려운경우에뇌졸중의이차예방목적으
로고려될수있다. (근거수준Ib, 권고수준A)-수정
4. 뇌출혈을포함한심각한출혈의위험이있는환자에게항혈소판제치료가필요할때, 실로스타졸
또는트리플루잘은뇌졸중의이차예방을위해서추천될수있다. (근거수준Ib, 권고수준A)-수정
1. Shinohara Y, Katayama Y, Uchiyama S, Yamaguchi T, Handa S, Matsuoka K, Ohashi Y, Tanahashi N,
Yamamoto H, Genka C, Kitagawa Y, Kusuoka H, Nishimaru K, Tsushima M, Koretsune Y, Sawada T, Hamada
C. Cilostazol for prevention of secondary stroke (CSPS 2): An aspirin-controlled, double-blind, randomised
non-inferiority trial. Lancet Neurol. 2010;9:959-968.
2. Kamal AK, Naqvi I, Husain MR, Khealani BA. Cilostazol versus aspirin for secondary prevention of
vascular events after stroke of arterial origin. Cochrane Database Syst Rev. 2011:CD008076.
3. Huang Y, Cheng Y, Wu J, Li Y, Xu E, Hong Z, Li Z, Zhang W, Ding M, Gao X, Fan D, Zeng J, Wong
K, Lu C, Xiao J, Yao C. Cilostazol as an alternative to aspirin after ischaemic stroke: A randomised, double-
blind, pilot study. Lancet Neurol. 2008;7:494-499.
4. Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A. European stroke prevention
study 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci.
1996;143:1-13.
CLINICAL RESEARCH CENTER FOR STROKE
270
심장탓뇌색전증을제외한허혈뇌졸중이나일과성허혈발작의재발을막기위한효과적인방법으
로, 기전이서로다른항혈소판제의복합투여가시도되어왔다. 이중아스피린(aspirin)과디피리다몰
(dipyridamole)의복합사용은허혈뇌졸중과일과성허혈발작의재발위험을유의하게감소시켰으나,
클로피도그렐(clopidogrel)과아스피린의복합사용은심장질환과동반된일부뇌졸중외에는실망스
러운결과를보여줬다. 그러나, 보다효과적인재발방지및항혈소판제의단독사용중발생하는뇌
졸중을막기위한항혈소판제의복합사용에관한연구는계속되고있다.
1. Aspirin (50 to 325mg/d), the combination of aspirin and extended release dipyridamole, and clopidogrel
are all acceptable options for initial therapy (AHA/ASA: Class IIa, Level of Evidence A, EUSI: Level of
Evidence I,RCP: Grade of Recommendation A).
5. Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A. Aspirin plus dipyridamole versus aspirin
alone after cerebral ischaemia of arterial origin (ESPRIT): Randomised controlled trial. Lancet.
2006;367:1665-1673.
6. Matias-Guiu J, Ferro JM, Alvarez-Sabin J, Torres F, Jimenez MD, Lago A, Melo T. Comparison of
triflusal and aspirin for prevention of vascular events in patients after cerebral infarction: The TACIP
study: A randomized, double-blind, multicenter trial. Stroke. 2003;34:840-848.
7. Culebras A, Rotta-Escalante R, Vila J, Dominguez R, Abiusi G, Famulari A, Rey R, Bauso-Tosselli L,
Gori H, Ferrari J, Reich E. Triflusal vs aspirin for prevention of cerebral infarction: A randomized stroke
study. Neurology. 2004;62:1073-1080.
3.2.1.4 항혈소판제병합치료Antiplatelet combination therapy

CLINICAL RESEARCH CENTER FOR STROKE
6,602명의허혈뇌졸중이나일과성허혈발작환자를 상으로하여시행된 ESPS-2(The European
Stroke Prevention Study-2)1연구에서아스피린(하루50mg)과서방형디피리다몰(하루400mg)을복합
투여시아스피린이나디피리다몰을단독사용한경우에비하여뇌졸중재발이각각23%, 25% 감소
하는것이보고되었다. 또한, 2006년 ESPRIT (European/Australasian Stroke Prevention in Reversible
Ischaemia Trial) study 결과,2다양한용량의아스피린(하루30-325mg)과디피리다몰(200mg 하루2회)
을복합사용시아스피린을단독으로사용한것에비해우수한효과를보이는것이알려졌다.
한편클로피도그렐과아스피린복합사용에 한임상시험3,4의경우기 에미치지못하는결과가
보고되었으며, 일부심장질환이동반된경우에만유의한효과가있는것으로나타났다.5 7,599명의
환자들을 상으로시행된MATCH(The Management of Atherothrombosis With Clopidogrel in High-
Risk Patients With TIA or Stroke) 연구에서클로피도그렐(하루75mg) - 아스피린(하루75mg)을복합사
용한경우, 클로피도그렐(하루 75mg) 단독사용에비하여재발방지에있어유의한효과없이출혈
부작용이의미있게증가하는결과가보고되었다. 또한아스피린단독사용과클로피도그렐-아스피
린복합사용을비교한CHARISMA (Clpirogrel for High Atherothrombotic Risk and Ischemic Stabliliztion,
Mangement and Avoidance) 연구에서도복합사용의우월한효과는없는것으로보고되었다.
최근시행된여러임상연구들에서는실로스타졸과아스피린의복합처방이안전하며관상동맥스
텐트삽입술후의혈관재협착이나6,7유증상두개내동맥협착의진행을예방하는효과8가있는것으
로보고되었다.
271
2. The combination of aspirin and extended-release dipyridamole is suggested instead of aspirin alone
(AHA/ASA: Class IIa Level of Evidence A, RCP: Grade of Recommendation A, EUSI: Level of Evidence I).
3. The addition of aspirin to clopidogrel increases the risk of hemorrhage and is not routinely
recommended for ischemic stroke or TIA patients (AHA/ASA: Class III, Level of Evidence A ).
4. Patients with TIA or ischemic stroke and unstable angina or non-Q-wave MI should be treated with a
combination of clopidogrel 75mg and aspirin 75mg (EUSI: Level of Evidence III).

1. 심장탓뇌색전증을제외한허혈뇌졸중이나일과성허혈발작의재발을막기위해아스피린과서방
형디피리다몰의복합투여는아스피린단독투여에비해효과적일수있다. (근거수준Ia, 권고수준A)
2. 뇌졸중의이차예방을위해서클로피도그렐과아스피린의복합투여는관상동맥질환(unstable
angina, non Q-wave MI)을동반한일부환자에게는효과적일수있으나, 두개내출혈의위험성이있
으므로이를고려하여사용하여야한다. (근거수준Ia, 권고수준A)
3. 실로스타졸은유증상두개강내동맥협착환자에게고려될수있다. (근거수준III, 권고수준B)
CLINICAL RESEARCH CENTER FOR STROKE
1. Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A. European stroke prevention study. 2.
Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
2. Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A. Aspirin plus dipyridamole versus aspirin alone
after cerebral ischaemia of arterial origin (ESPRIT): Randomised controlled trial. Lancet. 2006;367:1665-
1673.
3. Diener HC, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M, Leys D, Matias-Guiu J,
Rupprecht HJ. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or
transient ischaemic attack in high-risk patients (MATCH): Randomised, double-blind, placebo-controlled
trial. Lancet.2004;364:331-337.
4. Bhatt DL, Fox KA, Hacke W, Berger PB, Black HR, Boden WE, Cacoub P, Cohen EA, Creager MA, Easton
JD, Flather MD, Haffner SM, Hamm CW, Hankey GJ, Johnston SC, Mak KH, Mas JL, Montalescot G,
Pearson TA, Steg PG, Steinhubl SR, Weber MA, Brennan DM, Fabry-Ribaudo L, Booth J, Topol EJ.
Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med.
2006;354:1706-1717.
5. Bhatt DL, Kapadia SR, Yadav JS, Topol EJ. Update on clinical trials of antiplatelet therapy for
cerebrovascular diseases.Cerebrovasc Dis. 2000;10 Suppl 5:34-40.
272

CLINICAL RESEARCH CENTER FOR STROKE
심장탓뇌색전증을제외한허혈뇌졸중이나일과성허혈발작환자에서항응고제가항혈소판제이
상의이차예방효과가있는지를알기위한연구가꾸준히시도되었다. 그러나, 현재까지경구용항
응고제는항혈소판제에비해더나은재발방지효과를보이지는못한반면, 출혈을포함한심각한
부작용은더많이발생하는결과를보여주었다.
1. For patients with noncardioembolic ischemic stroke or TIA, antiplatelet agents rather than oral
anticoagulation are recommended to reduce the risk of recurrent stroke and other cardiovascular
events (AHA/ASA: Class I, Level of Evidence A ). Anticoaulants should not be used for patients in
sinus rhythm (RCP: Grade of Recommendation A), unless there is a major source of cardiac embolism
6. Park SW, Lee CW, Kim HS, Lee NH, Nah DY, Hong MK, Kim JJ, Park SJ. Effects of cilostazol on
angiographic restenosis after coronary stent placement. Am J Cardiol. 2000;86:499-503.
7. Douglas JS, Jr., Holmes DR, Jr., Kereiakes DJ, Grines CL, Block E, Ghazzal ZM, Morris DC, Liberman H,
Parker K, Jurkovitz C, Murrah N, Foster J, Hyde P, Mancini GB, Weintraub WS. Coronary stent
restenosis in patients treated with cilostazol. Circulation.2005;112:2826-2832.
8. Kwon SU, Cho YJ, Koo JS, Bae HJ, Lee YS, Hong KS, Lee JH, Kim JS. Cilostazol prevents the
progression of the symptomatic intracranial arterial stenosis: The multicenter double-blind placebo-
controlled trial of cilostazol in symptomatic intracranial arterial stenosis. Stroke. 2005;36:782-786.
3.2.2. 항응고제Anticoagulation
273

CLINICAL RESEARCH CENTER FOR STROKE
허혈뇌졸중이나일과성허혈발작환자의이차예방에서경구용항응고제의효과를알기위한 규
모무작위연구들이시행되었다. 고용량의경구용항응고제(INR, 3.0-4.5)와아스피린(aspirin, 하루
30mg)을비교한SPIRIT(The Stroke Prevention in Reversible Ischemia Trial) 연구는항응고제사용환자
군에서심각한출혈부작용이발생함에따라윤리적이유로조기종료되었다.1,2또한2,206명의심장
탓뇌색전증이외의뇌졸중환자를 상으로와파린(warfarin)(INR, 1.4-2.8)과아스피린(325mg)을비교
한WARSS (The Wafarin Aspirin Recurrent Stroke Study)3연구에서는재발방지효과는유사했으며,(와
파린17.8%; 아스피린16.0%) 출혈부작용도큰차이는나타나지않았다.(와파린2.2%; 아스피린1.5%)
WASID(Warfarin-Aspirin Symptomatic Intracranial Disease)4연구역시와파린의심각한부작용에의해
조기종료된연구로, 두개내혈관협착이50% 이상인환자만을 상으로와파린(INR 2-3)과아스피린
을비교한결과, 재발방지효과는유사한반면각종부작용은와파린사용환자군에서유의하게많이
발생하 다. 즉, 평균1.8년간의추적연구기간동안사망(아스피린4.3%; 와파린9.7%), 치명적인출혈
(아스피린3.2%; 와파린8.3%) 및심근경색혹은급사(아스피린2.9%; 와파린7.3%)가와파린사용환자
군에서더많이발생하 다. 최근 ESPRIT (European/Australasian Stroke Prevention in Reversible
Ischaemia Trial) study group5에서도경구용항응고제(INR 2,0-3.0)와아스피린(하루 30-325mg)을비교
한결과, 심장탓뇌색전증을제외한허혈뇌졸중의이차예방에있어항응고제가우월한효과를보이
지는않다는결과를보고하 다.
(RCP: Grade of Recommendation D).
2. Anticoagulation should not be used after non-cardioembolic ischemic stroke, except in some specific
situations, such as aortic atheroma, fusiform aneurysms of the basilar artery or cervical artery dissection
(EUSI: Level of Evidence IV).
1. 심장탓뇌색전증을제외한허혈뇌졸중이나일과성허혈발작의재발을막기위해서는경구용항응
고제보다는항혈소판제사용이권고된다. (근거수준Ia, 권고수준A)
274

CLINICAL RESEARCH CENTER FOR STROKE
275
1. The stroke prevention in reversible ischemia trial (SPIRIT) study group. A randomized trial of
anticoagulants versus aspirin after cerebral ischemia of presumed arterial origin. Ann Neurol.
1997;42:857-865.
2. Gorter JW. Major bleeding during anticoagulation after cerebral ischemia: Patterns and risk factors.
Stroke prevention in reversible ischemia trial (SPIRIT). European atrial fibrillation trial (EAFT) study
groups. Neurology. 1999;53:1319-1327.
3. Mohr JP, Thompson JL, Lazar RM, Levin B, Sacco RL, Furie KL, Kistler JP, Albers GW, Pettigrew LC,
Adams HP, Jr., Jackson CM, Pullicino P. A comparison of warfarin and aspirin for the prevention of
recurrent ischemic stroke. N Engl J Med.2001;345:1444-1451.
4. Chimowitz MI, Kokkinos J, Strong J, Brown MB, Levine SR, Silliman S, Pessin MS, Weichel E, Sila CA,
Furlan AJ, et al. The warfarin-aspirin symptomatic intracranial disease study. Neurology. 1995;45:1488-
1493.
5. Algra A. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin
(ESPRIT): A randomised controlled trial. Lancet Neurol.2007;6:115-124.
항혈소판제를복용하고있던환자에서허혈뇌졸중이재발하는경우, 복용하고있던항혈소판제를
다른기전의항혈소판제로변경하거나, 기존약과함께다른항혈소판제를추가투여하는것을고려
할수있다. 그러나, 항혈소판제의투약을결정할때해당약제의효과뿐만아니라동반될수있는부
작용이함께고려되어야한다. 최근두가지이상의항혈소판제를복합투여한연구의결과들이보고
되었으므로, 이런연구결과들을고려하여투약을결정하여야한다. 항혈소판제의선택은환자의개
별적인위험인자나임상적인특이성, 약물내성에따라서차별화되어야한다.
3.2.3. 특정상황에서항혈소판제사용Specific consideration of antiplatelet agents
3.2.3.1. 항혈소판제복용중발생한허혈뇌졸중Ischemic stroke while taking antiplatelet agent

CLINICAL RESEARCH CENTER FOR STROKE
아스피린(aspirin)을이미복용하고있는환자에서허혈뇌졸중이재발했을때단독제재나복합제재
를직접적으로비교한유용한연구는아직까지발표되지않았다. 따라서기존의연구를참조하고, 환
자개개인의특성과약제의특성, 위험성을고려하여처방이이루어져야할것이다.
허혈뇌졸중이나일과성허혈발작을보인환자들을 상으로실시한2개의 규모임상시험에서, 아
스피린의용량에따른혈관질환발생률의차이는없었다.1,2하지만아스피린의용량증가는위장출혈
의위험성을증가시킬수있다.1
ESPS-2 (European Stroke Prevention Study 2) 연구는허혈뇌졸중을가진3,299명의환자를 상으로,
아스피린(50mg) - 서방형 (extended release) 디피리다몰(dipyridamole, 하루400mg)의복합제를복용한
집단및아스피린(50mg)을단독으로복용한집단을비교하여심각한혈관성질환의발생을연구하
다.2 이연구에서는복합제를복용한환자들이아스피린을단독으로복용한환자들보다혈관성질환
발생의상 적위험이22% 감소한반면,(95% CI, 9-33%) 주요출혈의발생은의미있게증가하지않았
다.(RR 1.35; 95% CI, 0.8-2.4; p=NS) 이후진행된 ESPRIT(Europen/Australasian Stroke Prevention in
Reversible Ischemia Trial) 연구에서복합제재의효과가다시한번확인되었다.3뇌졸중, 심근경색및혈
관질환으로인한사망, 또는주요출혈의발생이아스피린(30-325mg)과서방형디피리다몰(400mg)을
함께복용한집단에서아스피린(30-325mg)을단독복용한집단보다효과적으로감소하 다.(RRR
20%; 95% CI, 2-34%) 또한주요출혈의발생도복합제재와단독투여사이에서의미있는차이가나타
나지않았다.(hazard ratio 0.67; 95% CI, 0.44-1.03)
1. 아스피린을복용하고있는허혈뇌졸중환자에서허혈뇌졸중이재발했을때아스피린의용량을
276
1. For patients who have an ischemic stroke while taking aspirin, there is no evidence that increasing the
dose of aspirin provides additional benefit. Although alternative antiplatelet agents are often considered
for noncardioembolic patients, no single agent or combination has been studied in patients who have
hand an event while receiving aspirin (AHA/ASA).

CLINICAL RESEARCH CENTER FOR STROKE
증가시키는것이뇌졸중의추가재발방지에도움이된다는근거는없다. 또한기존에아스피린을
복용하고있는비심장탓허혈뇌졸중환자에서허혈뇌졸중이재발하 을때단일항혈소판제나
복합제재를투여하는것이도움이된다는유용한연구결과도없다. 따라서아스피린을복용하고
있는환자에서허혈뇌졸중이재발했을때이후약제의선택은환자개개인의특성과약제의위험
을고려하여처방이이루어져야한다. (근거수준IV, 권고수준C)
2. 기존에아스피린을복용하고있는비심장탓허혈뇌졸중환자에서허혈뇌졸중이재발하 을때
담당의사의판단과환자의개별적인특성을고려해서서방형디피리다몰과아스피린의복합제를
투여할수있다. 만일서방형디피리다몰투여가적절하지않는경우에는클로피도그렐
(clopidogrel)을단일제제로변경투여할수있다. 그외의약제의선택에 해서는아직까지유용한
연구결과가미흡한실정이다. (근거수준IV, 권고수준C)
3. 아스피린이외의항혈소판제를복용하고있던비심장탓허혈뇌졸중환자에서허혈뇌졸중이재
발했을때이후에처방되어야하는적절한약제에 한유용한연구결과는아직까지없다. (근거
수준IV, 권고수준C)
277
1. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial
infarction, and stroke in high risk patients. BMJ. 2002;324:71-86.
2. Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A. European Stroke Prevention Study 2.
Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
3. Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A. Aspirin plus dipyridamole versus aspirin alone after
cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
뇌출혈을동반한환자에게항혈전제(antithrombotic agent)를투여할때안전성과효과에 해서는아
3.2.3.2. 뇌출혈이동반된허혈뇌졸중Ischemic stroke mixed with hemorrhage

직까지명확한기준이정립되지않았다. 그러나과거뇌출혈병력을가진환자에서뇌경색이발생할
수있으며, 혈전용해술이후에도이와관련된뇌출혈이발생할수있으므로이에 한실질적인연구
가필요하다. 엽상출혈(lobar hemorrhage)이나심부출혈(deep hemorrhage)을동반한심방세동을가
진환자에서항응고제를투여하는경우출혈의재발과허혈질환의발생에따른환자의삶의질이라
는측면에서고려되어야할것이다. 또한, 뇌출혈의발생후항혈소판제의투약은재출혈의가능성이
낮은환자에게고려되어야한다.
뇌 상검사기법이발전하여뇌미세출혈(cerebral microbleeding)이경사에코(Gradient-echo) MRI에서
저신호강도소견으로흔히관찰되는데, 이는임상적으로 부분무증상의소혈관출혈을의미한다.1
뇌미세출혈은아시아인과비아시아인사이에서다양한유병률차이를보이며고령에서나고혈압을
가진경우뇌미세출혈의출현이증가된다고보고되었다.2,3 그러나, 뇌미세출혈과항혈전제치료의관
련성에관해서는여전히논란이있으므로이에 한전향적인연구가필요하다.
CLINICAL RESEARCH CENTER FOR STROKE
1. The decision to restart antithrombotic therapy after ICH related to antithrombotic therapy depends on the
risk of subsequent arterial or venous thromboembolism, the risk of recurrent ICH, and the overall state
of the patient. For patients with a comparatively lower risk of cerebral infarction (eg, AF without prior
ischemic stroke) and a higher risk of amyloid angiopathy (eg, elderly patients with lobar ICH) or with very
poor overall neurological function, an antiplatelet agent may be an overall better choice for prevention of
ischemic stroke than warfarin. In patients with a very high risk of thromboembolism in whom restarting
warfarin is considered, warfarin therapy may be restarted at 7 to 10 days after onset of the original ICH
(AHA/ASA: Class IIb, Level of Evidence B).
2. After having re-checked the indication for anticoagulation (following the EUSI recommendation on
ischaemeic stroke) oral anticoagulation treatment may be continued after 10-14 days, depending on the
perceived risk of thromboembolic occlusion and ICH recurrence (EUSI; Level of Evidence IV).
와파린(warfarin) 복용중에뇌출혈이생긴환자에서와파린을재투여하는것은개개인환자의뇌경
278

CLINICAL RESEARCH CENTER FOR STROKE
색발생위험도를고려해서결정하게된다. 뇌색전의발생은뇌경색의병력이없는비판막성심방세
동환자에서연5%,4이전에허혈뇌졸중을가진환자에서는연12%,5인공판막을갖고있는환자에
서는최소연4%의발생률을보인다.6와파린복용중에출혈이발생한환자에서와파린을재투여하
는것은허혈뇌졸중의예방이라는면과뇌출혈의재발위험성이라는양면의균형을고려해서결정
해야한다.7하지만와파린투여동안뇌출혈의재발에관련된유용한보고가아직까지없다. 뇌출혈
을가진114명의환자집단에서와파린을중단하고신선냉동혈장(fresh frozen plasma)으로혈액응
고기능을회복시켰을때, 평균 7-10일동안 6명의환자(5%)에서색전증이발생했으며, 1명의환자
(0.8%)에서항응고제의투약과관련된재출혈이발생했다는보고가있다.8-10항응고제의역전을위한
프로트롬빈복합체농축물(prothrombin complex concentrate) 투여시, 4례(5%)의혈전색전증이발생
했으며혈종의확장이5명의환자(6%)에서지속되었다.11-16위와같은제한된자료들을통해서인공
판막이나만성비판막성심방세동을가진환자에서뇌출혈후에7~10일간에걸쳐서신선냉동혈장
이나프로트롬빈복합체농축물로항응고제를역전시키는경우에도낮은색전의발생률을보 고,
이후와파린을재투여하는것이안전한것으로관찰되었다.17
일반적으로아 로이드혈관병증(amyloid angiopathy)과관련된엽출혈을가진고령의환자는와파
린을지속적으로투여할때나쁜예후를보일가능성이높고, 작은심부출혈을가진환자에서는와
파린을투여하는것과중단하는것이비슷한위험성을보 다. 뇌출혈을가진환자에서항응고제투
여여부및투여시기에 한논란은전향적연구가시행되어야해결될수있을것이다. 하지만뇌경
색의위험성이낮은환자와아 로이드혈관병증의위험성이높은환자에서는, 뇌경색의발생을막
기위해서항혈소판제의투여가와파린을투여하는것보다는좋은선택이될것으로보인다.
항혈소판제를투여받은환자들에서뇌출혈이발생했을때항혈소판제의복용여부가예후에 향
을미치는지에 한연구가이루어졌지만, 연구에따라서서로다른결과가보고되었다. 뇌출혈발
생시에아스피린을규칙적으로복용하 던것이뇌출혈과관련된사망에 한독립된위험인자로
작용한다는후향적인연구결과가있었다.(RR, 2.5:95% CI, 1.3-4.6) 한편457명의뇌실질출혈을동반
한환자중94명(20.5%)이항혈소판제를복용하고있었지만, 항혈소판제복용여부가기능적인회복
에 향을미치지않는다는보고도있다.18,19뇌출혈이발생한207명의환자중, 뇌출혈발생이후항
혈소판제가투여된46명(22%)에 한후향적인연구에서항혈소판제의투여는뇌출혈의재발에
향을미치지않는것으로나타났다.20하지만이연구에서는항혈소판제투여가허혈심혈관질환의
279
발생에중요한기여를했다는것이불명확하므로, 결과해석에유의하여야한다. 결국뇌출혈후항혈
소판제의투여를결정할때적응증과재출혈의상 적위험성을고려해서제한된환자에게투여되
어야한다.
급성뇌경색환자에서뇌출혈발생의위험인자로뇌미세출혈이작용할수있는지를전향적으로관
찰한연구에서121명의급성뇌경색환자중43명(35.5%)에서뇌미세출혈이관찰되었다. 추적기간중
11명에서뇌졸중이발생하 으나이는뇌미세출혈유무와는무관하 다.(p=0.841) 이연구에서는추
적기간동안뇌출혈이발생한 5명의환자중 4명에서뇌미세출혈이기초검사에서관찰되었
고,(p=0.053) 5명의환자중에서3명은aspirin을복용하고있었고2명은와파린을복용하고있었다. 이
는뇌미세출혈을가진환자가항혈전제를복용하고있을때뇌출혈의위험성이증가될수있다는점
을시사한다.21항혈소판제를복용한환자630명과항응고제를복용한환자210명을 상으로항혈전
제의복용과뇌미세출혈사이에통계적으로유의성은없었다.22급성뇌경색환자에서실시한MRI에
서뇌미세출혈이관찰될때정맥을통한 tPA 혈전용해술을시행하는것이뇌출혈의발생을증가시킬
수있는지를관찰한연구에서, 뇌미세출혈이관찰된경우가그렇지않은경우보다자발성뇌출혈의
발생이 3.1% 더높았지만통계적으로유의한연관성을보여주지않았다.23(95% CI,-2.0-8.3) 아직까지
뇌미세출혈의유무가치료의결정에 향을미친다는의미있는근거는없다.
CLINICAL RESEARCH CENTER FOR STROKE
1. 뇌출혈이발생한환자에서항혈전제투약을다시시작해야할지를결정할때혈전의발생위험성,
뇌출혈의재발위험성및환자의전반적인위험인자등상태를고려해서결정되어야한다. (근거수
준IV, 권고수준C)
2. 항응고제복용이후뇌출혈이발생한환자에서뇌색전증의재발가능성이낮은경우나출혈의위
험성이높은경우에는항응고제 신항혈소판제가투여될수도있지만, 뇌색전증의발생위험이
매우높은환자에서는항응고제가다시투여되어야한다. 재투여를시작하는시기는이전뇌출혈
발생후7-10일이후가될수있다. (근거수준III, 권고수준B)
3. 뇌미세출혈과항혈전제의연관성에 한유용한전향적인연구가발표되지않았으므로, 뇌미세출
혈을가진환자에서항혈전제의투약을제한할필요는없을것으로고려된다. (근거수준 IV, 권고수
준C)
280

CLINICAL RESEARCH CENTER FOR STROKE
281
1. Roob G, Schmidt R, Kapeller P, Lechner A, Hartung HP, Fazekas F. MRI evidence of past cerebral
microbleeds in a healthy elderly population. Neurology.1999;52:991-994.
2. Koennecke HC. Cerebral microbleeds on MRI: prevalence, associations, and potential clinical
implications. Neurology. 2006;66:165-171.
3. Lee SH, Park JM, Kwon SJ, Kim H, Kim YH, Roh JK, Yoon BW. Left ventricular hypertrophy is associated
with cerebral microbleeds in hypertensive patients. Neurology. 2004;63:16-21.
4. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data
from five randomized controlled trials. Arch Intern Med. 1994;154:1449-1457.
5. EAFT (European Atrial Fibrillation Trial) Study Group. Secondary prevention in non-rheumatic atrial
fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
6. Cannegieter SC, Rosendaal FR, Wintzen AR, van der Meer FJ, Vandenbroucke JP, Briet E. Optimal oral
anticoagulant therapy in patients with mechanical heart valves. N Engl J Med. 1995;333:11-17.
7. Hacke W. The dilemma of reinstituting anticoagulation for patients with cardioembolic sources and
intracranial hemorrhage: how wide is the strait between Skylla and Karybdis? Arch Neurol.
2000;57:1682-1684.
8. Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valve patients after intracranial
haemorrhage: a 2-year follow-up. Br J Haematol.1998;103:1064-1066.
9. Wijdicks EF, Schievink WI, Brown RD, Mullany CJ. The dilemma of discontinuation of anticoagulation
therapy for patients with intracranial hemorrhage and mechanical heart valves. Neurosurgery.
1998;42:769-773.
10. Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagulation in patients with intracranial
hemorrhage at high thromboembolic risk. Arch Neurol.2000;57:1710-1713.
11. Makris M, Greaves M, Phillips WS, Kitchen S, Rosendaal FR, Preston EF. Emergency oral anticoagulant
reversal: the relative efficacy of infusions of fresh frozen plasma and clotting factor concentrate on
correction of the coagulopathy. Thromb Haemost. 1997;77:477-480.
12. Boulis NM, Bobek MP, Schmaier A, Hoff JT. Use of factor IX complex in warfarin-related intracranial
hemorrhage. Neurosurgery. 1999;45:1113-1118; discussion 1118-1119.

13. Cartmill M, Dolan G, Byrne JL, Byrne PO. Prothrombin complex concentrate for oral anticoagulant
reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
14. Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeutic dilemma: patients with
spontaneous intracerebral hemorrhage and urgent need for anticoagulation. J Neurol. 2000;247:209-
214.
15. Sjoblom L, Hardemark HG, Lindgren A, Norrving B, Fahlen M, Samuelsson M, Stigendal L, Stockelberg
D, Taghavi A, Wallrup L, Wallvik J. Management and prognostic features of intracerebral hemorrhage
during anticoagulant therapy: a Swedish multicenter study. Stroke. 2001;32:2567-2574.
16. Yasaka M, Sakata T, Minematsu K, Naritomi H. Correction of INR by prothrombin complex concentrate
and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res.2002;108:25-30.
17. Estol CJ, Kase CS. Need for Continued Use of Anticoagulants After Intracerebral Hemorrhage. Curr
Treat Options Cardiovasc Med. 2003;5:201-209.
18. Saloheimo P, Ahonen M, Juvela S, Pyhtinen J, Savolainen ER, Hillbom M. Regular aspirin-use
preceding the onset of primary intracerebral hemorrhage is an independent predictor for death. Stroke.
2006;37:129-133.
19. Caso V, Paciaroni M, Venti M, Alberti A, Palmerini F, Milia P, Billeci AM, Silvestrelli G, Biagini S, Agnelli G.
Effect of on-admission antiplatelet treatment on patients with cerebral hemorrhage. Cerebrovasc Dis.
2007;24:215-218.
20. Viswanathan A, Rakich SM, Engel C, Snider R, Rosand J, Greenberg SM, Smith EE. Antiplatelet use
after intracerebral hemorrhage. Neurology.2006;66:206-209.
21. Fan YH, Zhang L, Lam WW, Mok VC, Wong KS. Cerebral microbleeds as a risk factor for subsequent
intracerebral hemorrhages among patients with acute ischemic stroke. Stroke. 2003;34:2459-2462.
22. Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds: systematic review,
subgroup analyses and standards for study design and reporting. Brain. 2007;130:1988-2003.
23. Fiehler J, Albers GW, Boulanger JM, Derex L, Gass A, Hjort N, Kim JS, Liebeskind DS, Neumann-
Haefelin T, Pedraza S, Rother J, Rothwell P, Rovira A, Schellinger PD, Trenkler J. Bleeding risk analysis
in stroke imaging before thromboLysis (BRASIL): pooled analysis of T2*-weighted magnetic resonance
imaging data from 570 patients. Stroke. 2007;38:2738-2744.
CLINICAL RESEARCH CENTER FOR STROKE
282

283
3.3. 심장탓색전성뇌졸중또는일과성허혈발작의항혈전제치료Antithrombotic therapy of cardioembolic stroke or TIA
외국의역학자료에의하면심장탓색전성뇌졸중은전체허혈뇌졸중의약20%에달하는것으로알
려져있으나,1우리나라의병원기반등록자료에의하면이보다는적은것으로보고되었다.2각각의뇌
졸중환자에서그기전을명확히규명하기는매우어렵지만, 일반적으로색전증의위험성이높은심
장질환이있으면서허혈뇌졸중이발생한경우심장탓색전증의가능성이높다. 최근의연구자료에
의하면색전증의고위험군에해당하는심장질환은아래표와같으며, 이들심장질환이있는경우연
간허혈뇌졸중의발생률은2% 이상으로예상할수있다3.
3.3.1. 항응고제Anticoagulants
CLINICAL RESEARCH CENTER FOR STROKE
표허혈성뇌졸중의위험을증가시키는요인3
�좌심방혈전(Left atrial thrombus)
�좌심실혈전(Left ventricular thrombus)
�심방세동(Atrial fibrillation)
�발작심방된떨림(발작심방조동, Paroxysmal atrial fibrillation)
�동결절기능부전증후군(Sick sinus syndrome)
�지속심방된떨림(지속심방조동, Sustained atrial flutter)
�1개월이내발생한심근경색(Recent myocardial infarction, within 1 month)
�류마티스승모판혹은 동맥판질환(Rheumatoid mitral or aortic valve disease)
�생체혹은기계적심장판막(Bioprosthetic and mechanical heart valves)
�28% 미만의낮은심장박출량이동반된만성심근경색(Chronic myocardial infarction together with low ejection fraction less than 28%)
�30% 미만의낮은심장박출량이동반된증후성울혈심장부전(Symptomatic congestive heart failure with ejection fraction less than 30%)
�확장심근병증(Dilated cardiomyopathy)
�비-세균성혈전성심내막염(Nonbacterial thrombotic endocarditis)

1. Patients with proven cardio-embolic stroke should be anticoagulated, if the risk of recurrence is high,
with a target INR between 2.0 and 3.0 (EUSI: level of Evidence lll).
CLINICAL RESEARCH CENTER FOR STROKE
심장탓색전성뇌졸중의이차예방에 한연구는 부분질환별로연구되었다. 따라서, 심장탓색전
성뇌졸중전체를 상으로한항응고제치료의이차예방효과에 한구체적인연구결과는없으며,
각질환별연구의결과를통해유추할수밖에없다. 각각의심장질환에서항응고제치료의효과에
해서는“3.5. 특정질환의치료”에서자세히기술한다. 심장탓색전증으로인한뇌졸중이나일과성
허혈발작이명확한경우, 이차예방을위한항응고제투여는특별한금기증이없는한필수적으로고
려되어야한다.
1. 색전증의위험이높은심장질환을동반한뇌졸중또는일과성허혈발작환자는심장탓색전성뇌
졸중또는일과성허혈발작의재발가능성이높으므로특별한금기가없는한 INR 2.0-3.0 목표의와
파린치료가권장된다. (근거수준III, 권고수준C, GPP)
1. Cardiogenic brain embolism. The second report of the cerebral embolism task force. Arch Neurol.
1989;46:727-743.
2. KH Yu, HJ Bae, SU Kwon, DW Kang, KS Hong, YS Lee, JH Rha, JS Koo,JS Kim, JH Kim, JH Lee, SJ Cho,
SH Hwang, S Jung, MK Han, KH Cho, BC Kim, DJ Shin, Dl Chang, JH Park, EG Kim, DS Jung, MY Ahn,
DH Lee, KW Park, YJ Kim, KY Lee, JH Heo, SH Kim, KH Lee, CS Chung, JK Cha, JH Lee, KY Uhm, BC
Lee, JK Roh,. Analysis of 10,811 cases with acute ischemic stroke from Korean stroke registry: Hospital-
based multicenter prospective registration study. J Korean Neurol Assoc. 2006;24:535-543.
3. Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ. An evidence-based causative
284

CLINICAL RESEARCH CENTER FOR STROKE
심장탓색전, 특히심방세동에의한허혈뇌졸중의일차치료제는와파린(warfarin)으로알려져있다. 그
러나항응고제의금기또는적절한항응고제투여에도불구하고허혈뇌졸중이재발한환자의경우, 항
응고제의강도를높이거나항혈소판제 체치료또는항혈소판제와병용투여를고려할수있다.
1. Oral anticoagulation (INR 2.0-3.0) is indicated after ischemic stroke associated with atrial fibrillation
(EUSI: level I). Oral anticoagulation is not advisable in patients with comorbid conditions such as falls,
epilepsy, severe dementia, or gastro-intestinal bleedings.
고령, 위장출혈, 간질(epilepsy) 환자와알코올의존이나치매등약물순응도가낮아항응고제투여가
어려운심장탓색전허혈뇌졸중환자에서항혈소판제는이차예방치료로고려될수있다. 3개 규
모임상시험분석결과,1-3심방세동에의한허혈뇌졸중이아스피린(aspirin) 투여군에서 조군에비
해21%의비교위험도감소율을보 다.(95% CI, 0-38) 그러나다른종류의항혈소판제가심방세동에
의한허혈뇌졸중에미치는예방효과에 한연구결과는아직불충분하다.4적절한항응고제치료
중색전증이재발한경우에는, 항응고제와아스피린의병용투여를고려할수있으나이에 해서는
관련근거가부족하다.
classification system for acute ischemic stroke. Ann Neurol. 2005;58:688-697.
1. 항응고제치료를할수없는심장탓색전으로인한허혈뇌졸중또는일과성허혈발작환자의이차
예방을위해서아스피린투여를고려할수있다. (권고수준GPP)
3.3.2. 항혈소판제또는병합치료Antiplatelet therapy or combination therapy
285

1. Stroke Prevention in Atrial Fibrillation Investigators. Adjusted-dose warfarin versus low-intensity, fixed-
dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke prevention in atrial
fibrillation iii randomised clinical trial. Lancet. 1996;348:633-638.
2. EAFT (European atrial fibrillation trial) study group. Secondary prevention in non-rheumatic atrial
fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
3. Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of prophylactic
anticoagulation for patients with nonrheumatic atrial fibrillation. N Engl J Med. 1996;335:540-546.
4. Dale J, Myhre E, Storstein O, Stormorken H, Efskind L. Prevention of arterial thromboembolism with
acetylsalicylic acid. A controlled clinical study in patients with aortic ball valves. Am Heart J. 1977;94:101-
111.
CLINICAL RESEARCH CENTER FOR STROKE
286
외국의역학자료에의하면, 허혈뇌경색의약 16%(11-29%)가비판막성심방세동(nonvalvular atrial
fibrillation)으로인하여발생하는것으로보고되고있다.1-4우리나라에서1993년발표된병원기반역학
자료에의하면, 뇌경색환자의8.4%에서비판막성심방세동이있는것으로보고되고있어서구보다
상 적으로적은비중을차지하고있다.5그러나심방세동환자에서매년약4.5% 확률로뇌졸중이발
생하며,6특히심방세동으로이미뇌졸중이발생한환자에서는뇌졸중재발확률이매년12%로보고
되고있어,7심방세동은허혈뇌경색의고위험인자로알려져있다. 또한고령, 울혈심부전증, 고혈압,
당뇨병및과거의혈전색전증은뇌졸중의위험성을더욱높인다. 심방세동은나이가증가함에따라
유병률이높아지기때문에,8빠르게고령화되고있는우리나라에서는점점그중요성이커지고있다.
3.3.3. 특정질환의치료Specific conditions
3.3.3.1. 심방세동 Atrial fibrillation
CLINICAL RESEARCH CENTER FOR STROKE
1. For patients with ischemic stroke or transient ischemic accident with persistent or paroxysmal atrial
fibrillation, anticoagulation with adjusted-dose warfarin (INR 2.0-3.0) is recommended unless
contraindicated (ASA: Class I, Level of Evidence A, EUSI: level I).
2. For patients unable to take oral anticoagulants, aspirin 325mg/day is recommended (ASA: Class I, Level
of Evidence A).
5개의일차예방임상연구를메타분석(individual patient data meta-analyses; pooled analyses)한결과
와파린(warfarin) 투여시 조군에비하여뇌졸중발생의비교위험도(relative risk reduction)가68% 감
소하 다고하며, 연간뇌졸중발생률도와파린투여군에서1.4%로 조군의4.5%에비하여유의한
감소를보 다.9이러한, 와파린의효과는일과성허혈발작또는경미한뇌졸중이있었던환자를
상으로한이차예방임상시험European Atrial Fibrillation Trial(EAFT)에서도증명되었다.7이연구에의
하면, 아스피린(aspirin)과비교하여와파린은연간뇌졸중의발생률을12%에서4%로감소시켰다.
심방세동을가진환자의와파린치료에서적절한 INR 범위는2-3이다. INR<2에서는항응고제의예
방효과가현저히감소하는것으로알려져있다.7,10,11또한, 무작위 조연구인 Stroke Prevention in
Atrial Fibrillation II(SPAFII)에의하면뇌출혈부작용의 부분은 INR>3에서발생하 다.12따라서, 특
별한금기가없는한심방세동환자에서뇌졸중의이차예방을위해 INR 2-3 목표의와파린치료가
추천된다. 그러나적절한항응고제투여에도불구하고허혈뇌졸중또는일과성허혈발작이재발된
심방세동환자의경우, INR 목표치를높이거나항혈소판제를병용투여하는치료가허혈뇌졸중을
더효과적으로예방할수있는지에 해서는관련근거가부족하다.
아스피린의예방효과는와파린에비해훨씬약하다. 메타분석결과에의하면, 아스피린을투여할경
우뇌졸중의비교위험도감소율은22% 으며, 이차예방으로국한할경우연간뇌졸중의절 위험
도는2.5% 감소하 다.13심방세동환자에서아스피린의뇌졸중예방효과는하루75mg을투여한연
구보다하루 325mg을투여한연구에서상 적으로더높았다.9따라서항응고제를투여할수없는
환자에서외국에서는아스피린하루 325mg 투여가권장되고있으나, 325mg에근접하여국내에서
실제처방가능한용량인하루300mg 투여를고려할수있다.
287

CLINICAL RESEARCH CENTER FOR STROKE
1. 지속또는발작심방세동을가진허혈뇌졸중또는일과성허혈발작환자에서, 특별한금기가없는
한INR 2.0-3.0 목표의와파린치료가권장된다. (근거수준Ia, 권고수준A)
2. 항응고제를투여할수없다면, 아스피린을투여할수있다. (근거수준 Ia, 권고수준A) 적절한아스피
린용량으로는하루 325mg가권장되나, 우리나라에서는실제처방가능한용량인하루 300mg을
고려할수있다. (근거수준IV, 권고수준GPP)
3. 적절한항응고제치료를받던심방세동환자에서허헐뇌졸중또는일과성허혈발작이재발한경
우, INR 2.5-3.5로치료목표를높이거나항혈소판제병용투여를고려할수있다. (근거수준 IV, 권고
수준C)
1. Mohr JP, Caplan LR, Melski JW, Goldstein RJ, Duncan GW, Kistler JP, Pessin MS, Bleich HL. The
Harvard cooperative stroke registry: A prospective registry. Neurology. 1978;28:754-762.
2. Bogousslavsky J, Cachin C, Regli F, Despland PA, Van Melle G, Kappenberger L. Cardiac sources of
embolism and cerebral infarction--clinical consequences and vascular concomitants: The Lausanne
stroke registry. Neurology. 1991;41:855-859.
3. Sandercock P, Bamford J, Dennis M, Burn J, Slattery J, Jones L, Boonyakarnkul S, Warlow C. Atrial
fibrillation and stroke: Prevalence in different types of stroke and influence on early and long term
prognosis (Oxfordshire community stroke project). BMJ.1992;305:1460-1465.
4. Hornig CR, Brainin M, Mast H. Cardioembolic stroke: Results from three current stroke data banks.
Neuroepidemiology.1994;13:318-323.
5. The Korean Neurological Association. Epidemiology of cerebrovascular disease in Korea - a collaborative
study, 1989-1990. J Korean Med Sci.1993;8:281-289.
6. Stern S, Altkorn D, Levinson W. Anticoagulation for chronic atrial fibrillation. JAMA.2000;283:2901-2903.
7. EAFT(European Atrial Fibrillation Trial) Study Group. Secondary prevention in non-rheumatic atrial
fibrillation after transient ischaemic attack or minor stroke. EAFT (European atrial fibrillation trial) study
group. Lancet. 1993;342:1255-1262.
288

CLINICAL RESEARCH CENTER FOR STROKE
8. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: A major contributor to stroke in the elderly. The
Framingham study. Arch Intern Med. 1987;147:1561-1564.
9. Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial
fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med.
1994;154:1449-1457.
10. Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of
prophylactic anticoagulation for patients with nonrheumatic atrial fibrillation. N Engl J Med.
1996;335:540-546.
11. Stroke Prevention in Atrial Fibrillation Investigators. Adjusted-dose warfarin versus low-intensity, fixed-
dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke prevention in atrial
fibrillation III randomised clinical trial. Lancet.1996;348:633-638.
12. Stroke Prevention in Atrial Fibrillation Investigators. Warfarin versus aspirin for prevention of
thromboembolism in atrial fibrillation: Stroke prevention in atrial fibrillation II study. Lancet.
1994;343:687-691.
13. Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with
atrial fibrillation: A meta-analysis. Ann Intern Med. 1999;131:492-501.
289
낮은좌심실박출계수(left ventricular ejection fraction, LVEF)를보이는심장근육병증(cardiomyopathy)
은심장탓허혈뇌졸중의원인질환으로알려져있다. 심장근육병증에는관상동맥질환으로인한허
혈심장근육병증과비허혈확장성심장근육병증(dilated cardiomyoapthy)이있다. 좌심실박출계수가
낮을수록뇌졸중발생빈도가증가하므로, 심부전(congestive heart failure)으로좌심실박출계수가낮
은환자들은적극적인뇌졸중이차예방이요구된다.
3.3.3.2. 울혈성심부전Congestive heart failure
CLINICAL RESEARCH CENTER FOR STROKE
1. For patients with ischemic stroke or TIA who have dilated cardiomyopathy, either warfarin (INR, 2.0 to 3.0)
or antiplatelet therapy may be considered for prevention of recurrent events (ASA; Class IIb, Level of
Evidence C).
두개의 규모연구를통하여좌심실박출계수와뇌졸중발생빈도는역의상관관계가있으며, 박출
계수가5% 감소할때마다뇌졸중발병위험이18% 증가한다는것이알려졌다.1,2
심장근육병증환자에서장기적항응고제치료가색전증을감소시킨다는보고도있으나, 이에 한
무작위 조연구는아직없으며일부연구들에서는항응고제의효과에 한반 의견들도있어와
파린(warfarin) 사용에는논란의여지가있다.3,4심부전환자를 상으로시행된 PROBE(Prospectve
Randomized Open-label Blinded End point) 디자인연구인WASH(Warfarin/Aspirin Study in Heart Failure)
연구는 조군에비하여와파린(INR 2.5) 혹은아스피린(aspirin, 하루300mg)을투여받은군에서뇌졸
중, 심근경색및사망의발생이유의하게감소하지않았다는결과를보고하 다.5 35% 이하의좌심실
박출계수를가진심부전환자를 상으로한 PROBE 디자인의WATCH(the Warfarin and Antiplatelet
Therapy in Chronic Heart Failure Trial) 연구는와파린(target INR, 2.5-3.0)과아스피린162mg 또는클로
피도그렐(clopidogrel) 75mg을비교하 으나환자등록부진으로연구가조기종료되었다.6그러나관
찰연구에의하면심근경색후좌심실부전환자에서와파린과아스피린을투여하면뇌졸중발생위
험도를줄일수있으며,1아스피린은뇌졸중의발생을20%까지감소시키는것으로보고되었다.7현재
감소된박출계수를가진환자에서일차또는이차뇌졸중예방에 한와파린과항혈소판제의효능
을비교하는무작위배정이중맹검연구가진행중에있다.8
1. 낮은좌심실박출계수를보이는심장근육병증의뇌졸중이차예방을위해서와파린또는항혈소판
제사용을고려해볼수있다. (권고수준GPP)
290

CLINICAL RESEARCH CENTER FOR STROKE
291
1. Loh E, Sutton MSJ, Wun C-CC, Rouleau JL, Flaker GC, Gottlieb SS, Lamas GA, Moye LA, Goldhaber SZ,
Pfeffer MA. Ventricular dysfunction and the risk of stroke after myocardial infarction. N Engl J MEd.
1997;336:251-257.
2. Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ, Cuddy TE, Davis BR, Geltman EM, Goldman S, Flaker
GC, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after
myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE investigators. N Engl
J MEd. 1992;327:669-677.
3. Ezekowitz M. Antithrombotics for left-ventricular impairment? The Lancet. 1998;351:1904.
4. Falk RH. A plea for a clinical trial of anticoagulation in dilated cardiomyopathy. Am J Cardiol. 1990;65:914-915.
5. Cleland JGF, Findlay I, Jafri S, Sutton G, Falk R, Bulpitt C, Prentice C, Ford I, Trainer A, Poole-Wilson PA. The
warfarin/aspirin study in heart failure (WASH): A randomized trial comparing antithrombotic strategies for
patients with heart failure. Am Heart J. 2004;148:157-164.
6. Massie BM, Krol WF, Ammon SE, Armstrong PW, Cleland JG, Collins JF, Ezekowitz M, Jafri SM, O'Connor
CM, Packer M, Schulman KA, Teo K, Warren S. The warfarin and antiplatelet therapy in heart failure trial
(WATCH): Rationale, design, and baseline patient characteristics. J Card Fail. 2004;10:101-112.
7. Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction.
N Engl J Med. 2002;347:969-974.
8. Pullicino P, Thompson JLP, Barton B, Levin B, Graham S, Freudenberger RS. Warfarin versus aspirin in
patients with reduced cardiac ejection fraction (WARCEF): Rationale, objectives, and design. J Card Fail.
2006;12:39-46.
좌심실혈전이동반된급성심근경색은허혈뇌졸중의심장탓색전증의고위험요인중하나이며, 특
히전방심근경색환자의급성기에허혈뇌졸중의발생빈도가높다고알려져있다.
3.3.3.3. 급성심근경색Acute myocardial infarction

1. For patients with an ischemic stroke or TIA caused by an acute MI in whom LV mural thrombus is
identified by echocardiography or another form of cardiac imaging, oral anticoagulation is reasonable,
aiming for an INR of 2.0 to 3.0 for at least 3 months and up to 1 year (ASA: Class IIa, Level of Evidence B).
2. Aspirin should be used concurrently for ischemic coronary artery disease during oral anticoagulant
therapy in doses up to 162 mg/d (ASA: Class IIa, Level of Evidence A).
CLINICAL RESEARCH CENTER FOR STROKE
좌심실혈전이동반된급성심근경색환자의12%에서허혈뇌졸중이발생하며, 특히전방심근경색
환자의경우20%까지그위험도가증가한다.1색전증의위험은심근경색발생첫1~3개월이내에가
장높으나, 심근경색이지속되거나심실세동혹은심부전증이동반되는환자에서는급성기이후에
도색전증이발생할수있다. 급성심근경색환자를 상으로한두개의무작위배정 조연구
(ASPECT-2, n=993; WARIS-2, n=3640)에서아스피린(aspirin) 단독치료보다아스피린과와파린
(warfarin)의병용치료가심근경색의재발과허혈뇌졸중예방에효과적이라고보고하 다.2,3또한10
개의무작위 조연구를메타분석한결과아스피린과와파린의병용치료는허혈뇌졸중발생률을
54% (CI, 23-73%) 감소시켰으며, 아스피린단독치료에비하여허혈뇌졸중을더효과적으로예방하
다.4따라서급성심근경색후색전증의위험요소인심방세동, 좌심실혈전, 낮은좌심실박출율(left
ventricular ejection fraction, LVEF) 등이있는환자에서아스피린과와파린의병용치료가추천되고있
다.5,6
1. 좌심실혈전을동반한급성심근경색에의한허혈뇌졸중또는일과성허혈발작환자에서, 항응고
치료의특별한금기가없는한 INR 2.0-3.0으로최소3개월에서1년동안와파린치료를하는것이
바람직하다. (근거수준IIa, 권고수준B)
2. 항응고제투여기간동안에도아스피린을병용투여해야한다. (근거수준Ia, 권고수준A)
292

CLINICAL RESEARCH CENTER FOR STROKE
293
1. Visser CA, Kan G, Meltzer RS, Lie KI, Durrer D. Long-term follow-up of left ventricular thrombus after acute
myocardial infarction. A two-dimensional echocardiographic study in 96 patients.Chest.1984;86:532-536.
2. Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin or both after myocardial infarction.
N Engl J Med.2002;347:969-974.
3. Van Es RF, Jonker JJC, Verheugt FWA, Deckers JW, Grobbee DE. Aspirin and coumadin after acute coronary
syndromes (the ASPECT-2 study): A randomised controlled trial.The Lancet. 2002;360:109-113.
4. Rothberg MB, Celestin C, Fiore LD, Lawler E, Cook JR. Warfarin plus aspirin after myocardial infarction or the
acute coronary syndrome: Meta-analysis with estimates of risk and benefit. Ann Intern Med. 2005;143:241-
250.
5. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner
FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith Jr SC, Antman EM, Smith Jr SC, Alpert
JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs
AK, Ornato JP. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction--
executive summary: A report of the American College of Cardiology/American Heart Association task force
on practice guidelines (writing committee to revise the 1999 guidelines for the management of patients with
acute myocardial infarction). J Am Coll Cardiol. 2004;44:671-719.
6. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS, Jones RH, Kereiakes D,
Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE, Steward DE, Theroux P, Gibbons RJ, Antman
EM, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Hiratzka LF, Jacobs AK, Smith SC. ACC/AHA 2002 guideline
update for the management of patients with unstable angina and non-ST-segment elevation myocardial
infarction--summary article: A report of the American College of Cardiology/American Heart Association task
force on practice guidelines (committee on the management of patients with unstable angina). J Am Coll
Cardiol.2002;40:1366-1374.

과거에색전증이있었던류마티스승모판막질환환자의30-65%에서색전증이재발하며,1-4승모판막
성형술만으로는색전증의위험을충분히감소시킬수없는것으로보인다.5,6따라서적극적인혈전
예방약물치료가요구된다.
인공판막의경우, 판막의종류와위치, 항응고제또는항혈소판제치료여부및강도, 과거색전증의
병력등에따라색전증의위험이달라질수있다. 예를들어, 기계적인공판막의하나인‘St. Jude
Medical bileaflet valves’로승모판막치환술을받은경우, 색전증예방을위한약물치료를하지않으면
연간22%의혈전색전증이발생한다고알려져있다.7따라서, 적절한혈전예방약물치료가요구된다.
CLINICAL RESEARCH CENTER FOR STROKE
1. For patients with ischemic stroke or TIA who have rheumatic mitral valve disease, whether or not AF is
present, long-term warfarin therapy is reasonable, with a target INR between 2.0 and 3.0 (ASA: Class IIa,
Level of Evidence C).
2. For patients with rheumatic mitral valve disease, whether or not AF is present, who have a recurrent
embolism while receiving warfarin, adding low dose aspirin is suggested (ASA: Class IIa, Level of
Evidence C).
3. For patients with ischemic stroke or TIA who have mechanical prosthetic heart valves, oral
anticoagulants are recommended, with a target INR between 2.5 and 3.5 (ASA: Class I, Level of Evidence
B, EUSI: level II).
4. For patients with mechanical prosthetic heart valves, whether or not AF is present, who have a recurrent
embolism while receiving warfarin, adding low-dose aspirin is reasonable (ASA: Class IIa, Level of
Evidence B).
5. For patients with ischemic stroke or TIA who have bioprosthetic heart valves with no other source of
thromboembolism, anticoagulation with warfarin (INR 2.0 to 3.0) may be considered (ASA: Class IIb,
Level of Evidence C).
294
3.3.3.4. 심장판막질환 Valvular heart disease

CLINICAL RESEARCH CENTER FOR STROKE
1. 류마티스승모판막질환이동반된허혈뇌졸중또는일과성허혈발작환자에서심방세동유무와관
계없이특별한금기가없는한INR 2.0-3.0 목표의와파린치료가추천된다. (근거수준III, 권고수준B)
여러관찰연구에의하면, 류마티스승모판막질환환자에서장기적항응고제치료는색전증을효과
적으로감소시킬수있는것으로보인다.1-4또한, 좌심방에혈전이동반된승모판막협착증환자에서
장기적항응고제투여시혈전이사라지는것이보고된바도있다.5따라서류마티스승모판막질환환
자에서적절한항응고제치료를받지않던중허혈뇌졸중또는일과성허혈발작이발생한경우라면,
심방세동과동일한강도의 INR 2-3을목표로와파린(warfarin) 투여가권장된다. 적절한항응고제투
여에도불구하고색전증이재발한경우라면항응고제치료와함께아스피린(aspirin)의병용투여를
고려할수있지만, 이에 해서는관련근거가부족하다.
판막치환술을받은환자에서장기적항응고제치료의효과에 하여지금까지가장신뢰성높은임
상연구결과는와파린과항혈소판제를비교한임상연구결과이다.6이연구에의하면, 와파린은항혈
소판제보다혈전색전증의위험을현저히감소시켰다. 판막의종류와위치에따라다르지만, 일반적
으로기계적인공판막치환술을받은경우는혈전색전증의위험이특히높아서, 통상적인INR 범위보
다더높은강도(2.5-3.5 또는그이상)를목표로장기적와파린투여가권고되고있다.7따라서, 기계적
인공판막치환술후적절한항응고제치료를받지않던중허혈뇌졸중또는일과성허혈발작이발생
한경우라면, 일차예방권고안에따라 INR 2.5-3.5 범위를목표로와파린투여가권장된다. 기계적인
공판막치환술후적절한항응고제투여에도불구하고색전증이재발한경우에는, 항응고제치료와
함께아스피린의병용투여를고려할수있다. 소규모무작위임상연구에의하면, 색전증의위험성이
높은생체인공판막치환술환자나기계적인공판막치환술환자에서아스피린하루100mg의병용
투여결과약간의출혈부작용증가에도불구하고사망률과색전증의발생이감소하 다.8
생체인공판막치환술을받은경우는기계적인공판막보다혈전색전증의위험이상 적으로적어,
승모판막치환술인경우초기3개월만 INR 2-3 목표의와파린투여가권장되고있다.9그러나생체인
공판막치환술후뇌졸중이발생한경우라면장기적항응고제치료를고려할수있지만, 이에 해서
는관련근거가부족하다.
295
2. 류마티스승모판막질환이동반된허혈뇌졸중또는일과성허혈발작환자에서적절한항응고제투
여에도불구하고색전증이재발한경우, 저용량(하루100mg)의아스피린병용투여를고려할수있
다. (근거수준IV, 권고수준C)
3. 기계적인공판막치환술후발생한허혈뇌졸중또는일과성허혈발작환자에서특별한금기가없
는한, INR 2.5-3.5 목표의와파린치료가추천된다. (근거수준IIb, 권고수준B)
4. 기계적인공판막치환술후적절한항응고제투여에도불구하고색전증이재발한경우, 저용량(하
루100mg)의아스피린병용투여가추천된다. (근거수준IIa, 권고수준B)
5. 생체인공판막치환술후발생한허혈뇌졸중또는일과성허혈발작환자에서다른혈전색전증의
원인이없다면, INR 2.0-3.0 목표의와파린치료를고려할수있다. (근거수준IV, 권고수준C)
CLINICAL RESEARCH CENTER FOR STROKE
1. Adams GF, Merrett JD, Hutchinson WM, Pollock AM. Cerebral embolism and mitral stenosis: Survival
with and without anticoagulants. J Neurol Neurosurg Psychiatry.1974;37:378-383.
2. Fleming HA. Anticoagulants in rheumatic heart-disease.Lancet.1971;2:486.
3. Roy D, Marchand E, Gagne P, Chabot M, Cartier R. Usefulness of anticoagulant therapy in the prevention
of embolic complications of atrial fibrillation. Am Heart J. 1986;112:1039-1043.
4. Szekely P. Systemic embolism and anticoagulant prophylaxis in rheumatic heart disease. Br Med J.
1964;1:1209-1212.
5. Silaruks S, Thinkhamrop B, Tantikosum W, Wongvipaporn C, Tatsanavivat P, Klungboonkrong V. A
prognostic model for predicting the disappearance of left atrial thrombi among candidates for
percutaneous transvenous mitral commissurotomy. J Am Coll Cardiol. 2002;39:886-891.
6. Mok CK, Boey J, Wang R, Chan TK, Cheung KL, Lee PK, Chow J, Ng RP, Tse TF. Warfarin versus
dipyridamole-aspirin and pentoxifylline-aspirin for the prevention of prosthetic heart valve
thromboembolism: A prospective randomized clinical trial. Circulation. 1985;72:1059-1063.
7. Cannegieter SC, Rosendaal FR, Wintzen AR, van der Meer FJ, Vandenbroucke JP, Briet E. Optimal oral
anticoagulant therapy in patients with mechanical heart valves. N Engl J Med. 1995;333:11-17.
8. Turpie AG, Gent M, Laupacis A, Latour Y, Gunstensen J, Basile F, Klimek M, Hirsh J. A comparison of
296

CLINICAL RESEARCH CENTER FOR STROKE
aspirin with placebo in patients treated with warfarin after heart-valve replacement. N Engl J Med.
1993;329:524-529.
9. Salem DN, Stein PD, Al-Ahmad A, Bussey HI, Horstkotte D, Miller N, Pauker SG. Antithrombotic
therapy in valvular heart disease--native and prosthetic: The seventh ACCP conference on
antithrombotic and thrombolytic therapy. Chest.2004;126:457S-482S.
297

CLINICAL RESEARCH CENTER FOR STROKE
298
3.4. 혈관협착-폐쇄질환에서수술또는중재적치료Surgical or interventional treatment of large artery steno-occlusive disease
〈경동맥내막절제술〉
1. 최근6개월이내에일과성허혈발작이나뇌경색이있었던심한내경동맥협착환자(협착정도70-
99%)는경동맥내막절제술을하는것이권장된다. 경동맥내막절제술수술은수술전후의이환율과
사망률이낮은경험많은외과의사가시행하는것이권장된다. (근거수준Ib, 권고수준A)
2. 최근에일과성허혈발작이나뇌경색이있었던중등도내경동맥협착(50-69%) 환자의경우환자의
연령, 성별, 동반된질환, 처음증상의정도를고려하여경동맥내막절제술을시행할수있다.
(근거수준Ib, 권고수준A)
3. 경도의내경동맥협착(50% 미만) 환자에게는내과적인치료가우선권장된다. (근거수준Ib, 권고수준A)
4. 증상이없는중등도내경동맥협착(60-99%)을가진40세-75세환자의경우, 기 수명이5년이상이면
경동맥내막절제술을고려하는것이바람직하다. (근거수준Ib, 권고수준A) 이경우수술전후의이
환율과사망률이낮은경험많은외과의사가시행하는것이추천된다.
유증상두개강외경동맥협착치료에 해서최근임상진료에 향을미칠수있는 규모무작위배정
연구결과들이다수발표되었다. 유증상의심한경동맥협착환자에서경동맥내막절제술의효과는
확실히입증되어있었으나, 최근경동맥내막절제술과경동맥스텐트설치술의단기간및중장기효
과및안전성비교연구들과이를기반으로한메타분석및소집단분석연구들이발표되었다. 이에따
라외국의임상진료지침이개정되었고국내에서도많은논란이되고있어서, 집필위원회에서는이들
연구결과를바탕으로유증상두개강외경동맥협착치료에관한진료지침의근거수준과권고수준을
개정하 다특히, 이번개정에서는경동맥협착환자의치료법을결정할때경동맥내막절제술, 경동
맥스텐트설치술, 및약물치료를동시에고려할수있도록통합적인지침을제안하고자하 다.
개정: 2011.11
3.4.1. 두개강외경동맥협착Extracranial carotid artery stenosis

CLINICAL RESEARCH CENTER FOR STROKE
5. 경동맥내막절제술은허혈증상이발생한뒤2주이내에시술하는경우더좋은예후를기 할수
있다. (근거수준Ib, 권고수준A)
〈경동맥성형술/스텐트〉
1. 의학적사유로경동맥내막절제술시행이어려운경우, 스텐트설치술이추천될수있다.
(근거수준IIb, 권고수준B)
2. 시술전후의이환율과사망률이낮은숙련된중재시술자에게스텐트설치술을받는것이바람직
하다. (근거수준IIb, 권고수준B)
3. 유증상의심한내경동맥협착환자(70% 이상)와무증상협착환자(80% 이상)에서스텐트설치술을
고려할수있다. (근거수준IV, 권고수준C)
4. 스텐트설치술직전과시술후최소1개월동안클로피도그렐과아스피린복합요법을유지하는것
이고려된다. (근거수준IV, 권고수준C)
1. ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS (2011)
∙Patients at average or low surgical risk who experience nondisabling ischemic stroke or transient
cerebral ischemic symptoms, including hemispheric events or amaurosis fugax, within 6 months
(symptomatic patients) should undergo CEA if the diameter of the lumen of the ipsilateral internal
carotid artery is reduced more than 70% as documented by noninvasive imaging (Class I; Level of
Evidence: A) or more than 50% as documented by catheter angiography (Class I; Level of Evidence: B)
and the anticipated rate of perioperative stroke or mortality is less than 6%.
∙CAS is indicated as an alternative to CEA for symptomatic patients at average or low risk of
complications associated with endovascular intervention when the diameter of the lumen of the internal
carotid artery is reduced by more than 70% as documented by noninvasive imaging or more than 50%
as documented by catheter angiography and the anticipated rate of periprocedural stroke or mortality is
less than 6%. (Class I; Level of Evidence: B)
∙Selection of asymptomatic patients for carotid revascularization should be guided by an assessment of
comorbid conditions, life expectancy, and other individual factors and should include a thorough
discussion of the risks and benefits of the procedure with an understanding of patient preferences.
(Class I; Level of Evidence: C)
299

∙It is reasonable to perform CEA in asymptomatic patients who have more than 70% stenosis of the
internal carotid artery if the risk of perioperative stroke, MI, and death is low. (Class IIa; Level of Evidence: A)
∙It is reasonable to choose CEA over CAS when revascularization is indicated in older patients, particularly
when arterial pathoanatomy is unfavorable for endovascular intervention. (Class IIa; Level of Evidence: B)
∙It is reasonable to choose CAS over CEA when revascularization is indicated in patients with neck
anatomy unfavorable for arterial surgery. (Class IIa; Level of Evidence: B)
∙When revascularization is indicated for patients with TIA or stroke and there are no contraindications to
early revascularization, intervention within 2 weeks of the index event is reasonable rather than delaying
surgery. (Class IIa; Level of Evidence: B)
∙Prophylactic CAS might be considered in highly selected patients with asymptomatic carotid stenosis
(minimum 60% by angiography, 70% by validated Doppler ultrasound), but its effectiveness compared
with medical therapy alone in this situation is not well established. (Class IIb; Level of Evidence: B)
∙In symptomatic or asymptomatic patients at high risk of complications for carotid revascularization by
either CEA or CAS because of comorbidities, the effectiveness of revascularization versus medical
therapy alone is not well established. (Class IIb; Level of Evidence: B)
∙Aspirin (81 to 325 mg daily) is recommended before CEA and may be continued indefinitely
postoperatively. (Class I; Level of Evidence: A)
∙Beyond the first month after CEA, aspirin (75 to 325 mg daily), clopidogrel (75 mg daily), or the
combination of low-dose aspirin plus extended-release dipyridamole (25 and 200 mg twice daily,
respectively) should be administered for long-term prophylaxis against ischemic cardiovascular events.
(Class I; Level of Evidence: B)
∙Administration of antihypertensive medication is recommended as needed to control blood pressure
before and after CEA. (Class I; Level of Evidence: C)
∙The findings on clinical neurological examination should be documented within 24 hours before and
after CEA. (Class I; Level of Evidence: C)
∙Patch angioplasty can be beneficial for closure of the arteriotomy after CEA. (Class IIa; Level of Evidence: B)
∙Administration of statin lipid-lowering medication for prevention of ischemic events is reasonable for
patients who have undergone CEA irrespective of serum lipid levels, although the optimum agent and
dose and the efficacy for prevention of restenosis have not been established. (Class IIa; Level of Evidence: B)
∙Noninvasive imaging of the extracranial carotid arteries is reasonable 1 month, 6 months, and annually
CLINICAL RESEARCH CENTER FOR STROKE
300

CLINICAL RESEARCH CENTER FOR STROKE
301
after CEA to assess patency and exclude the development of new or contralateral lesions. Once stability
has been established over an extended period, surveillance at longer intervals may be appropriate.
Termination of surveillance is reasonable when the patient is no longer a candidate for
intervention. (Class IIa; Level of Evidence: C)
∙Before and for a minimum of 30 days after CAS, dual-antiplatelet therapy with aspirin (81 to 325 mg
daily) plus clopidogrel (75 mg daily) is recommended. For patients intolerant of clopidogrel, ticlopidine
(250 mg twice daily) may be substituted. (Class I; Level of Evidence: C)
∙Administration of antihypertensive medication is recommended to control blood pressure before and
after CAS. (Class I; Level of Evidence: C)
∙The findings on clinical neurological examination should be documented within 24 hours before and
after CAS. (Class I; Level of Evidence: C)
∙Embolic protection device (EPD) deployment during CAS can be beneficial to reduce the risk of stroke
when the risk of vascular injury is low. (Class IIa; Level of Evidence: C)
∙Noninvasive imaging of the extracranial carotid arteries is reasonable 1 month, 6 months, and annually
after revascularization to assess patency and exclude the development of new or contralateral lesions.
Once stability has been established over an extended period, surveillance at extended intervals may be
appropriate. Termination of surveillance is reasonable when the patient is no longer a candidate for
intervention. (Class IIa; Level of Evidence: C)
2. European Stroke Organization (ESO) guideline (2008)
∙CEA is recommended for patients with 70-99% stenosis (Class I, Level A). CEA should only be
performed in centres with a perioperative complication rate (all strokes and death) of less than 6%
(Class I, Level A)
∙It is recommended that CEA be performed as soon as possible after the last ischaemic event, ideally
within 2 weeks (Class II, Level B)
∙It is recommended that CEA may be indicated for certain patients with stenosis of 50-69%; males with
very recent hemispheric symptoms are most likely to benefit (Class III, Level C). CEA for stenosis of 50-
69% should only be performed in centres with a perioperative complication rate (all stroke and death) of
less than 3% (Class I, Level A)
∙CEA is not recommended for patients with stenosis of less than 50% (Class I, Level A)

CLINICAL RESEARCH CENTER FOR STROKE
302
새로추가된근거와기존의근거를종합한개정의필요성에 한근거는다음과같다.
일과성허혈발작이나뇌경색이최근 6개월이내에발생하 던심한내경동맥협착 (70-99%) 환자
에서경동맥내막절제술은 30일째및 5년후뇌졸중발생및사망률을각각 6.2%, 15% 감소시키
는효과가입증되어있다.1중등도협착 (50-69%)에서는 5년후 6.5% 절 위험도감소효과를보
으나, 50% 미만의협착에서는약물치료군과비교할때유의한차이는없었다.1최근에발표된
SPACE2,3, EVA-3S4,5, ICSS6등 부분의연구는경동맥협착증치료법으로스텐트의설치술보다
이러한경동맥내막절제술을지지하 다. 스텐트의설치술후뇌졸중발생및사망률의증가는
Percutaneous Angioplasty of the Carotid Artery versus Endarterectomy (SPACE), Endarterectomy
Versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial (EVA-3S),
International Carotid Stenting Study (ICSS)를 상으로한메타분석에서도공통적으로증명되었
고 (8.9% 5.8%, p=0.0006),7자기공명 상을이용한 ICSS의소그룹분석에서8내막절제술에비
하여스텐트설치술후 1일째확산강조자기공명 상에서새로운병변들이유의하게증가하
다(50% 17%; p�0.0001). 그러나, Carotid And Vertebral Artery Transluminal Angioplasty Study
(CAVATAS)9,10, Stenting and Angioplasty with Protection in Patients at High Risk of Endarterectomy
(SAPPHIRE)11,12등장기간추적관찰연구에서는선별된환자의경우혈관성형술및스텐트설치
술이내막절제술의 체치료법으로사용될수있는근거를보여주었다. 무작위배정연구는아
니었지만 Carotid revascularization using endarterectomy or stenting systems (CaRESS) 연구에서
도13유증상및무증상경동맥협착환자들을 4년간추적관찰하 을때재협착률은스텐트군에
서높았지만뇌졸중, 사망, 심근경색발생은두군에서차이가없었다 (내막절제술: 27.0%, 스텐
∙It is recommended that patients remain on antiplatelet therapy both before and after surgery
(Class I, Level A)
∙Carotid percutaneous transluminal angioplasty and/or stenting (CAS) is only recommended in selected
patients (Class I, Level A). It should be restricted to the following subgroups of patients with severe
symptomatic carotid artery stenosis: those with contra-indications to CEA, stenosis at a surgically
inaccessible site, re-stenosis after earlier CEA, and post-radiation stenosis (Class IV, GCP). Patients
should receive a combination of clopidogrel and aspirin immediately before and for at least 1 month
after stenting (Class IV, GCP)

CLINICAL RESEARCH CENTER FOR STROKE
303
트: 21.7%, p=0.361). 특히, 80세미만의나이에서는스텐트설치술에의한뇌졸중위험도의감소
가의미있게관찰되었다 (p=0.030). Carotid Revascularisation Endarterectomy Versus Stenting
Trial (CREST) 연구에서도14스텐트설치술이경동맥내막절제술과비교해서심근경색발생관련
안전성과 70세미만환자에서치료효과가우월함이제시되었다. 시술또는수술이후 30일째까
지의예후에서는스텐트설치술군이상 적으로뇌졸중의발생이많은반면(4.1% 2.3%,
p=0.01), 내막절제술군에서는심근경색증발생이유의하게높았으며(2.3% 1.1%; p=0.03) 뇌신
경장애의발생이많았다(4.8% 0.3%; p�0.0001). 2009년제1판뇌졸중임상진료지침에서는경
동맥내막절제술과경동맥성형술및스텐트설치술에 한근거자료와권고사항을나누어기
술하 다. 그러나, 스텐트설치술과내막절제술이서로다른적응증을가지기보다는상호보완
적으로사용될수있기때문에이번개정판에서는기존의분리된진료지침을하나로통합하여
기술하 다.
이번개정에서가장특징적인것중하나는유증상의내경동맥협착(50% 이상)을가진환자에서
스텐트설치술이내막절제술의 체치료로사용될수있다는문구를근거수준 Ib, 권고수준A로
제시하 다는것이다. 그러나, 스텐트설치술의효과는환자의나이, 약물, 기구, 시술자의경험
에따라차이가날수있다. 따라서, 이번개정판에는최근CREST 결과가반 된미국뇌졸중학회
진료지침을참고하여‘유증상의내경동맥협착(50% 이상)을가진환자에서스텐트설치술이내
막절제술의 체치료로사용될수있다.’라는문구에“단, 내막절제술또는스텐트설치술을선
택할때, 환자의나이, 센터의특성, 수술전후의뇌졸중발생률및사망률을고려할필요가있다”
는문구를삽입하 다. (Good practice point, GPP)
내막절제술후이환율과사망률은 규모연구에서 3-6% 으나스텐트설치술후뇌졸중발생
및사망률은 6-10%로이를상회하 다. 최근미국, 유럽의개정진료지침에서는15-17수술관련
최 허용위험도를6%로제안하고있기때문에이번개정내용에는수술의사의자격을구체화
하는것이필요할것으로판단되었다. 따라서, ‘경동맥내막절제술수술은수술전후의이환율
과사망률이낮은경험많은외과의사가시행하는것이권장된다’는문구는‘뇌졸중발생률또
는사망률이6% 미만인의사가시행하는것이권장된다’는문구로수정하 다.
현재한국뇌졸중임상진료지침에서는 ECST 연구와NASCET 연구의통합연구18결과를기반으
로, 경동맥내막절제술을허혈증상이발생후 2주이내에시술하는것을권고하고있다. 최근
2008년까지발표된경동맥내막절제술연구자료를기반으로뇌졸중양상에따른수술시기별
뇌졸중발생및사망위험도를분석한연구결과가발표되었다.19진행성뇌졸중의경우응급으

CLINICAL RESEARCH CENTER FOR STROKE
304
로시행한내막절제술후뇌졸중발생및사망의절 위험도는 20.2% (95% 신뢰구간: 12.0-28.4)
고, 반복적, 진행성의일과성허혈발작의경우절 위험도는 11.4% (95% 신뢰구간:6.1-16.7)
다. 그러나, 안정적인뇌졸중이나일과성허혈발작의경우에는응급및지연수술에따른수술위
험도차이는없었다 (p=0.13). 수술시기는, 미국뇌졸중학회의개정지침에도기술된바와같이불
안정한뇌졸중의경우조기수술에따른합병증발생의위험성이증가할수있으므로‘조기수술
의금기사항이없다면’이라는문구를추가하 고, 근거수준과권고수준을하향수정하 다.
스텐트설치술의효과는약물, 기구, 시술자의경험에따라차이가날수있다. 뇌졸중발생률또
는사망률이 6% 미만으로감소될수있다면혈관성형술및스텐트설치술의중장기적인안전성,
유효성도증가할수있다. 따라서, 이번개정판에는최근 CREST 결과가반 된미국뇌졸중학회
진료지침을참고하여‘유증상의내경동맥협착(50% 이상)을가진환자에서 6% 미만의뇌졸중발
생률또는사망률이예측되는경우스텐트설치술이내막절제술의 체치료로사용될수있다.’
라는문구를근거수준 Ib, 권고수준A로제시하 다. 경동맥협착환자의치료효과를높이기위해
서는적절한약물치료병행을통해서수술및시술직후뇌졸중및심근경색발생을줄이는것이
중요하다. 유증상경동맥협착증의치료과정에서항혈소판제및스타틴계지질저하제사용, 위
험인자의적극적인조절이병행되어야한다는문구를근거수준 IIb, 권고수준B로포함하 다. 기
존에언급된스텐트설치술직전과시술후최소 1개월동안클로피도그렐과아스피린병용투여
를유지하는것이고려된다는문구는근거수준 IIb, 권고수준B로상향조정하 다.
1. 유증상의(최근6개월이내에협착 역에일과성허혈발작이나뇌경색이있었던경동맥협착) 심한
내경동맥협착환자(협착정도70-99%)는경동맥내막절제술을시행하는것이권장되며, 경동맥내
막절제술은수술전후의뇌졸중발생률또는사망률이6% 미만인의사가시행하는것이권장된다.
(근거수준Ib, 권고수준A)
2. 유증상의중등도내경동맥협착(협착정도50-69%) 환자의경우환자의연령, 성별, 동반된질환, 처
음증상의정도를고려하여경동맥내막절제술을시행할수있다. (근거수준Ib, 권고수준A)
3. 유증상의경도의내경동맥협착(50% 미만) 환자에게는내과적인치료가우선권장된다.
(근거수준Ib, 권고수준A)
4. 경동맥내막절제술은조기수술의금기사항이없다면허혈증상이발생한뒤2주이내에시술하는

CLINICAL RESEARCH CENTER FOR STROKE
1. RothwellPM, Eliasziw M, Gutnikov SA, Fox AJ, Taylor DW, Mayberg MR, et al. Analysis of pooled data
from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet
2003;361:107-115.
2. The SPACE Collaborative Group. 30 day results from the SPACE trial of stent-protected angioplasty
versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet
2006;368:1239-1247.
3. Eckstein HH, Ringleb P, Allenberg JR, Berger J, Fraedrich G, Hacke W, et al. Results of the Stent-
Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at
2 years: a multinational, prospective, randomized trial. LancetNeurol2008; 7: 893-902.
4. Mas JL, Chatellier G, Beyssen B, EVA-3S Investigators. Carotid angioplasty and stenting with and
without cerebral protection: clinical alert from the Endarterectomy Versus Angioplasty in Patients With
Symptomatic Severe Carotid Stenosis (EVA-3S) trial. Stroke2004;35:e18-20.
5. Mas JL, Trinquart L, Leys D, Albucher JF, Rousseau H, Viguier A, et al. Endarterectomy Versus
Angioplasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) trial: results up to 4 years
from a randomised, multicentre trial. Lancet Neurol2008; 7: 885-892.
6. Ederle J, Dobson J, Featherstone RL, Bonati LH, van der Worp HB, de Borst GJ, et al. Carotid artery
경우더좋은예후를기 할수있다. (근거수준IIb, 권고수준B) 스텐트설치술의수술시기에 한
근거자료는아직없다.
5. 유증상의내경동맥협착(50% 이상)을가진환자에서6% 미만의뇌졸중발생률또는사망률이
예측되는경우스텐트설치술이내막절제술의 체치료로사용될수있다.
(근거수준Ib, 권고수준A) 단, 내막절제술또는스텐트설치술을선택할때, 환자의나이, 성별, 병원
의특성을고려할필요가있다. (GPP)
6. 스텐트설치술직전과시술후최소1개월동안클로피도그렐과아스피린병용투여를유지하는것
이추천된다. (근거수준IIb, 권고수준B)
7. 유증상경동맥협착치료과정에서항혈소판제및스타틴계지질저하제사용, 위험인자의적극적
인조절이병행되어야한다. (근거수준IIb, 권고수준B)
305

stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International
Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010;375:985-997.
7. Carotid Stenting Trialists’Collaboration. Short-term outcome after stenting versus endarterectomy for
symptomatic carotid stenosis: a preplanned meta-analysis of individual patient data. Lancet
2010;376:1062-1073.
8. Bonati LH, Jongen LM, Haller S, Flach HZ, Dobson J, Nederkoorn PJ, et al, for the ICSS-MRI study
group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid
stenosis: a substudy of the International Carotid Stenting Study (ICSS). Lancet Neurol2010;9:353-362.
9. CAVATAS Investigators. Endovascular versus surgical treatment in patients with carotid stenosis in the
Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS). Lancet 2001;357:1729-1237.
10. Ederle J, Bonati LH, Dobson J, Featherstone RL, Gaines PA, Beard JD, et al, on behalf of the CAVATAS
investigators. Endovascular treatment with angioplasty or stenting versus endarterectomy in patients
with carotid artery stenosis in the Carotid And Vertebral Artery Transluminal Angioplasty Study
(CAVATAS): long-term follow-up of a randomised trial.Lancet Neurol2009;8:898-907.
11. Yadav JS,Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Protected carotid-artery stenting
versus endarterectomy in high-risk patients. N Engl J Med2004;351:1493-1501.
12. Gurm HS, Yadav JS, Fayad P, Katzen BT, Mishkel GJ, Bajwa TK, et al. Long-term results of carotid
stenting versus endarterectomy in high-risk patients.N Engl J Med2008;358:1572-1579.
13. Zarins CK, White RA, Diethrich EB, Shackelton RJ, Siami FS; CaRESS Steering Committee and
CaRESS Investigators. Carotid revascularization using endarterectomy or stenting systems (CaRESS): 4-
year outcomes. J Endovasc Ther2009;16:397-409.
14. Brott TG, Hobson RW 2nd, Howard G, et al, for the CREST investigators. Stenting versus
endarterectomy for treatment of carotid-artery stenosis.N Engl J Med2010;363:11-23.
15. Furie KL, Kasner SE, Adams RJ, Albers GW, Bush RL, Fagan SC, et al. Guidelines for the Prevention of
Stroke in Patients with Stroke or Transient Ischemic Attack. A Guideline for Healthcare Professionals
From the American Heart Association/American Stroke Association. Stroke2011;42:227-276.
16. Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, et al. 2011
ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the
CLINICAL RESEARCH CENTER FOR STROKE
306

CLINICAL RESEARCH CENTER FOR STROKE
307
척추뇌바닥동맥의폐쇄성혈관질환의치료효과에관한연구들은증례연구수준이고 규모의무
작위배정 조군연구는매우적다. 죽상경화성협착은척추동맥의기시부와두개골을통과하는부
위에서많이발생하고, 동맥박리도이부위에서많이발생된다. 이러한질환을치료하는데내과적
치료와외과적치료중무엇이더우월한지에 해서는더많은무작위배정연구가필요하다.
3.4.2. 척추뇌바닥동맥협착Vertebrobasilar artery stenosis
Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the
American College of Cardiology Foundation/American Heart Association Task Force on Practice
Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses,
American Association of Neurological Surgeons, American College of Radiology, American Society of
Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and
Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional
Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for
Vascular Surgery. Stroke 2011;42:e464-540.
17. European Stroke Organisation (ESO) executive committee; ESO writing committee. Guidelines for
management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis2008;25:457-507.
18. Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJM. Endarterectomy for symptomatic
carotid stenosis in relation to clinical subgroups and timing of surgery. Lancet 2004;363:915-924.
19. Rerkasem K, Rothwell PM. Systematic review of the operative risks of carotid endarterectomy for
recently symptomatic stenosis in relation to the timing of surgery.Stroke2009;40:e564-72.

CLINICAL RESEARCH CENTER FOR STROKE
1. Endovascular treatment of patients with symptomatic extracranial vertebral stenosis may be considered
when patients are having symptoms despite medical therapies (antithrombotic, statins, and other
treatment for risk factors) (ASA: Class IIb, Level of Evidence C).
2. For vertebral artery dissection, patients who have definite recurrent ischemic events despite
antithrombotic therapy, endovascular therapy (stenting) may be considered (ASA: Class IIb, Level of
Evidence C). Patients who fail or are not candidates for endovascular therapy may be considered for
surgical treatment (ASA: Class IIb, Level of Evidence C).
척추동맥의죽상경화성협착때문에발생하는허혈증상이적절한내과적치료에도불구하고반복되
는경우는혈관재건술로써혈류를개선하고증상을완화할수있다.1-5이러한연구들은 부분증례
연구들이고 규모무작위배정연구는아직없다. CAVATAS(Carotid And Vertebral Artery Transluminal
Angioplasty Study) 연구에서6스텐트설치술시행군과내과적치료군을평균4.5년이상추적하여예후
를비교한결과, 혈관내중재적시술(endovascular treatment)군이내과적치료보다우월하다는사실을
증명하지못했다. 그러나 상환자수가16명으로작다는한계가있어해석에주의를요한다.
1. 척추뇌바닥동맥협착이있는환자에서적절한내과적치료에도불구하고허혈증상이반복되는경
우에는혈관내중재적시술로스텐트설치술을고려할수있다. (근거수준IV, 권고수준C)
1. Chastain HD, 2nd, Campbell MS, Iyer S, Roubin GS, Vitek J, Mathur A, Al-Mubarak NA, Terry JB, Yates V,
Kretzer K, Alred D, Gomez CR. Extracranial vertebral artery stent placement: In-hospital and follow-up
308

CLINICAL RESEARCH CENTER FOR STROKE
죽상경화성두개내동맥협착은허혈뇌졸중의중요한원인중하나이다. 약물치료에도뇌졸중이재
발할가능성이비교적높으나, 아직까지는수술을포함하여효과적인예방법이알려져있지않다.
최근에중재기구및기법이발달하면서혈관성형술이뇌졸중예방을위한방법으로부각되었다. 혈
관성형술은협착부위를확장시켜즉시혈류를개선한다는장점은있으나, 이제시작단계이므로
앞으로좀더신뢰할수있는연구결과가나와야안전성과유용성을결정할수있을것이다.
results. J Neurosurg.1999;91:547-552.
2. Jenkins JS, White CJ, Ramee SR, Collins TJ, Chilakamarri VK, McKinley KL, Jain SP. Vertebral artery
stenting. Catheter Cardiovasc Interv. 2001;54:1-5.
3. Malek AM, Higashida RT, Phatouros CC, Lempert TE, Meyers PM, Gress DR, Dowd CF, Halbach VV.
Treatment of posterior circulation ischemia with extracranial percutaneous balloon angioplasty and
stent placement. Stroke. 1999;30:2073-2085.
4. Piotin M, Spelle L, Martin JB, Weill A, Rancurel G, Ross IB, Rufenacht DA, Chiras J. Percutaneous
transluminal angioplasty and stenting of the proximal vertebral artery for symptomatic stenosis.Am J
Neuroradiol. 2000;21:727-731.
5. Storey GS, Marks MP, Dake M, Norbash AM, Steinberg GK. Vertebral artery stenting following
percutaneous transluminal angioplasty. Technical note. J Neurosurg. 1996;84:883-887.
6. Coward LJ, McCabe DJ, Ederle J, Featherstone RL, Clifton A, Brown MM. Long-term outcome after
angioplasty and stenting for symptomatic vertebral artery stenosis compared with medical treatment in
the carotid and vertebral artery transluminal angioplasty study (CAVATAS): A randomized trial. Stroke.
2007;38:1526-1530.
3.4.3. 두개강내동맥협착 Intracranial artery stenosis
309

CLINICAL RESEARCH CENTER FOR STROKE
1. For patients with hemodynamically significant intracranial stenosis who have symptoms despite medical
therapies (antithrombotics, statins, and other treatments for risk factors), the usefulness of endovascular
therapy (angioplasty and/or stent placement) is uncertain and is considered investigational (ASA: Class
IIb, LOE C).
현재까지죽상경화성두개내동맥협착에 한혈관성형술및스텐트설치술의유용성을알기위한
무작위배정 조군연구혹은비교연구(Comparative study)는발표된바없다.1 다수연구는하나혹
은소수의센터가참여한후향적증례연구(case studies)로시행되었으며2-7 다양한합병증을보 다.
전체적으로 30일째뇌졸중혹은사망의빈도는 5.8-8.3%로보고되었으며, 1년이내뇌졸중발생은
8.8%로알려졌다. 이결과는WASID(warfarin and aspirin for symptomatic intracranial arterial disease) 연
구8결과의1년뇌졸중빈도인12% 보다일견우수하나, 단일기관연구의통계적비뚤림(bias)을고려
하면혈관내중재적시술이더우수하다는확고한근거는없다고할수있다. 다기관단완성전향적가
능성연구(Multicenter, single-arm, prospective feasibility study)로서뇌혈관협착용풍선-확장형스텐트
인Neurolink�를이용한연구는, 30일째뇌졸중혹은사망의빈도가6.6%로기존에발표되었던연구
들의성적과다르지않으나6개월이내재협착발생이32%에달했고1년이내뇌졸중발생역시14%
로서기존의후향적연구보다좋지않은결과를보여주었다.9최근뇌혈관협착용자가팽창형스텐트
인Wingspan�을이용한다기관단완성전향적연구의결과가발표되었다. 이는협착부위의정상내
경보다작은풍선카테터로혈관성형술을한후자가팽창형스텐트를설치하고나오는비교적단순
한시술로, 30일째뇌졸중혹은사망발생은4.5%, 6개월째재협착률은7.5%, 그리고1년이내동일한
역의뇌졸중은9.3%로상당히유망한성적을보여주었다.10그러므로, 두개내동맥협착에 한혈
관성형술및스텐트설치술은비교적안전하게시행할수있으나, 신뢰할수있는장기간의성적은
많지않아아직은약물치료에비해예후가좋을수있다는가정만할수있을뿐이다. 특히, 약물복용
후에도협착동맥 역에뇌졸중이재발할위험이매우높은것으로알려진, 첫증상발생후2주이내
이며70% 이상의협착이있는환자에게더욱이득이있을것으로추정할수있다.11
결론적으로, 죽상경화성두개내동맥협착으로인한뇌졸중의이차예방을위해혈관성형술및스텐
310

CLINICAL RESEARCH CENTER FOR STROKE
1. 50% 이상의죽상경화성두개내동맥협착에 해약물치료가실패한경우뇌졸중예방을위해혈관
성형술혹은자가팽창형스텐트설치술이고려될수있다. (근거수준IV, 권고수준C)
2. 동맥경화성두개내동맥협착의뇌졸중예방을위한방법으로서, 스텐트설치술이혈관성형술에비
해더좋은근거는미흡하다. (근거수준IV, 권고수준C)
트설치술을일상적인방법으로이용하기에는아직근거가부족하나, 상기한바와같이약물치료가
실패하고뇌졸중재발의위험이매우높은환자에서는선택적으로시행할수있을것으로보인다.
311
1. Cruz-Flores S, Diamond AL. Angioplasty for intracranial artery stenosis. Cochrane Database Syst Rev.
2006;3:CD004133.
2. de Rochemont Rdu M, Turowski B, Buchkremer M, Sitzer M, Zanella FE, Berkefeld J. Recurrent
symptomatic high-grade intracranial stenoses: Safety and efficacy of undersized stents--initial experience.
Radiology. 2004;231:45-49.
3. Jiang WJ, Du B, Leung TW, Xu XT, Jin M, Dong KH. Symptomatic intracranial stenosis: Cerebrovascular
complications from elective stent placement. Radiology. 2007;243:188-197.
4. Jiang WJ, Wang YJ, Du B, Wang SX, Wang GH, Jin M, Dai JP. Stenting of symptomatic M1 stenosis of middle
cerebral artery: An initial experience of 40 patients. Stroke. 2004;35:1375-1380.
5. Marks MP, Marcellus ML, Do HM, Schraedley-Desmond PK, Steinberg GK, Tong DC, Albers GW. Intracranial
angioplasty without stenting for symptomatic atherosclerotic stenosis: Long-term follow-up. Am J
Neuroradiol. 2005;26:525-530.
6. Marks MP, Wojak JC, Al-Ali F, Jayaraman M, Marcellus ML, Connors JJ, Do HM. Angioplasty for
symptomatic intracranial stenosis: Clinical outcome. Stroke. 2006;37:1016-1020.
7. Yoon W, Seo JJ, Cho KH, Kim MK, Kim BC, Park MS, Kim TS, Kim JK, Kang HK. Symptomatic middle
cerebral artery stenosis treated with intracranial angioplasty: Experience in 32 patients. Radiology.
2005;237:620-626.
8. Chimowitz MI, Lynn MJ, Howlett-Smith H, Stern BJ, Hertzberg VS, Frankel MR, Levine SR, Chaturvedi S,
Kasner SE, Benesch CG, Sila CA, Jovin TG, Romano JG. Comparison of warfarin and aspirin for symptomatic
intracranial arterial stenosis. N Engl J Med. 2005;352:1305-1316.
9. The SSYLVIA Study Investigators. Stenting of symptomatic atherosclerotic lesions in the vertebral or
intracranial arteries (SSYLVIA): Study results. Stroke. 2004;35:1388-1392.
10. Bose A, Hartmann M, Henkes H, Liu HM, Teng MM, Szikora I, Berlis A, Reul J, Yu SC, Forsting M, Lui M, Lim
W, Sit SP. A novel, self-expanding, nitinol stent in medically refractory intracranial atherosclerotic stenoses:
The Wingspan study. Stroke. 2007;38:1531-1537.
11. Kasner SE, Chimowitz MI, Lynn MJ, Howlett-Smith H, Stern BJ, Hertzberg VS, Frankel MR, Levine SR,
Chaturvedi S, Benesch CG, Sila CA, Jovin TG, Romano JG, Cloft HJ. Predictors of ischemic stroke in the
territory of a symptomatic intracranial arterial stenosis. Circulation. 2006;113:555-563.
CLINICAL RESEARCH CENTER FOR STROKE
1. Among patients with symptomatic carotid occlusion, EC/IC bypass surgery is not routinely
recommended (ASA: Class III, LOE A).
312
뇌혈관이막혀있는경우측부순환을통해부족한뇌혈류를공급받지만그것이원활하지않아일과
성허혈발작이나뇌경색이발생한다. 이때혈류를개선시키고뇌경색의재발을막기위해두개외-두
개내우회로조성술(EC/IC bypass surgery) 등의수술을고려할수있다. 하지만아직까지약물치료에
비해두개외-두개내우회로조성술이더효과적이라는명확한결론은없는실정이다.
3.4.4. 두개강외-두개강내동맥우회로조성술Extracranial-intracranial artery bypass surgery

CLINICAL RESEARCH CENTER FOR STROKE
1970년 에두개외-두개내우회로조성술이죽상경화성동맥폐쇄질환의경우비교적널리사용되
었다. 그러나1977-1985년사이에1,377명을 상으로약56개월동안경과를추적한 규모무작위
임상연구의결과는내과적치료에비해두개외-두개내우회로조성술이이득이없음을보여주었
다.1 하지만이연구의가장큰단점은환자의뇌혈류상태가반 되지않았다는점이다. 그래서현재
까지도뇌졸중의발생율이높은일부경동맥폐쇄환자의경우우회로조성술이뇌혈류를개선시키
고뇌졸중의재발을막을수있을것으로기 하여시행되고있다. 최근뇌혈류를측정하는기법과
발달된양전자방출단층촬 의기술을이용해수술치료의효과가클것으로예상되는환자를선별
할수있게되었으며, 이에관한 규모의임상연구가진행중이다.2
과거의몇몇증례연구결과급성기에수술을하는것은뇌졸중의예후에좋은 향이없었으며오
히려수술후합병증인뇌출혈이높은것으로나타났다.3
1. 증후성경동맥폐쇄환자의경우, 두개외-두개내우회로조성술을일률적으로시행하는것은권장
되지않는다. (근거수준Ib, 권고수준A)
2. 뇌경색이나일과성허혈발작을경험한경동맥폐쇄환자중뇌혈류상태를평가하여시술로인한
치료효과가기 되는일부환자에서는두개외-두개내우회로조성술을시행할수있다. (근거수준
IV, 권고수준C)
3. 급성기에두개외-두개내우회로조성술을시행하는것은권고되지않는다. (근거수준III, 권고수준B)
313
1. The EC/IC bypass study group. Failure of extracranial-intracranial arterial bypass to reduce the risk of
ischemic stroke. Results of an international randomized trial. N Engl J Med.1985;313:1191-1200.

CLINICAL RESEARCH CENTER FOR STROKE
314
2. Grubb RL, Jr., Powers WJ, Derdeyn CP, Adams HP, Jr., Clarke WR. The carotid occlusion surgery study.
Neurosurg Focus. 2003;14:e9.
3. Crowell R. STA-MCA bypass for acute focal cerebral ischemia. Microsurgery for stroke. 1977:244-250.

3.5. 기타특정질환의치료Management of other specific conditions
CLINICAL RESEARCH CENTER FOR STROKE
뇌출혈은높은이환율과사망률을나타내기때문에이의재발을막기위해서는위험인자의파악과
조절이중요하다. 뇌출혈의위험인자로고혈압이가장중요하며, 고혈압을적절하게조절하면뇌출
혈의재발을절반으로감소시킬수있다. 뇌출혈과혈압조절의중요성은고혈압의병력을가지고있
지않은환자에게도해당된다.
1. Treating hypertension in the non-acute setting is the most important step to reduce the risk of ICH and
probably recurrent ICH as well (ASA: Class I, LOE A).
2. Smoking, heavy alcohol use, and cocaine use are risk factors for ICH, and discontinuation should be
recommended for prevention of ICH recurrence (ASA: Class I, LOE B).
뇌출혈의재발에있어나이가중요한역할을하며65세가넘을경우재발률이2.8배나되는것으로알
려져있다. 비록나이는조절이불가능한위험인자이긴하지만, 이러한연구결과는환자에게유용한
예후에관한정보를제공하며적극적인위험인자감소의필요성을주지시킬수있다.1
고혈압이뇌출혈의가장중요한위험인자이며이의조절이뇌출혈의일차예방뿐아니라재발을막
는데도가장중요하다는것은잘알려져있다. 고혈압을치료받지않은환자의뇌출혈위험도가3.5
배에달하는것에비해고혈압치료를받은환자의경우는1.4배로감소하는연구결과는, 고혈압치
료를통해뇌출혈을예방할수있다는것을시사한다.2그외여러연구에서고혈압의치료를통해뇌
출혈의발생을절반정도로감소시킬수있다고보고하 다.3,4
3.5.1. 뇌내출혈의이차예방Secondary prevention of intracerebral hemorrhage
315

316
그밖에흡연이나과음, 마약등의복용은뇌출혈의위험도를높이는것으로알려져있으며, 이들은
뇌출혈발병이후재발방지를위해중단해야한다.5-9
1. 뇌출혈의재발방지를위해고혈압의철저한치료가필요하다. (근거수준Ia, 권고수준A)
2. 흡연이나과음은뇌출혈의이차예방을위해중단하는것이바람직하다. (근거수준III, 권고수준B)
1. Vermeer S, Algra A, Franke C, Koudstaal P, Rinkel G. Long-term prognosis after recovery from primary
intracerebral hemorrhage. Neurology. 2002;59:205-209.
2. Woo D, Haverbusch M, Sekar P, Kissela B, Khoury J, Schneider A, Kleindorfer D, Szaflarski J, Pancioli A,
E J, Moomaw C, Sauerbeck L, Gebel J, Broderick J. Effect of untreated hypertension on hemorrhagic
stroke. Stroke. 2004;35:1703-1708.
3. Perry H, Jr, Davis B, Price T, Applegate W, Fields W, Guralnik J, Kuller L, Pressel S, Stamler J, Probstfield
J. Effect of treating isolated systolic hypertension on the risk of developing various types and subtypes of
stroke: The systolic hypertension in the elderly program (SHEP). JAMA. 2000;284:465-471.
4. Chapman N, Huxley R, Anderson C, Bousser M, Chalmers J, Colman S, Davis S, Donnan G, MacMahon
S, Neal B, Warlow C, Woodward M. Effects of a perindopril-based blood pressure-lowering regimen on
the risk of recurrent stroke according to stroke subtype and medical history: The PROGRESS trial.
Stroke. 2004;35:116-121.
5. Thrift A, Donnan G, McNeil J. Heavy drinking, but not moderate or intermediate drinking, increases the
risk of intracerebral hemorrhage. Epidemiology. 1999;10:307-312.
6. Kurth T, Kase C, Berger K, Schaeffner E, Buring J, Gaziano J. Smoking and the risk of hemorrhagic
stroke in men. Stroke. 2003;34:1151-1155.
7. Kurth T, Kase C, Berger K, Gaziano J, Cook N, Buring J. Smoking and risk of hemorrhagic stroke in
women. Stroke. 2003;34:2792-2795.
8. Iso H, Baba S, Mannami T, Sasaki S, Okada K, Konishi M, Tsugane S. Alcohol consumption and risk of
CLINICAL RESEARCH CENTER FOR STROKE
317
CLINICAL RESEARCH CENTER FOR STROKE
뇌출혈을동반한허혈뇌졸중환자에게항혈전제(antithrombotic agent)를투여할때의안전성과효과
에관하여아직까지명확한기준이정립되지않았다. 그러나, 과거뇌출혈병력을가진환자에서뇌
경색이발생할수있으며, 혈전용해술이후에도이와관련된뇌출혈이발생할수있으므로이에
한실질적인연구가필요하다. 엽상출혈(lobar hemorrhage)이나심부출혈(deep hemorrhage)을동반
한심방세동을가진환자에서항응고제를투여하는경우출혈의재발과허혈질환의발생에따른환
자의삶의질을고려하여야한다. 또한, 뇌출혈발생후항혈소판제의투약은재출혈의가능성이낮
은환자에게고려되어야한다.
1. The decision to restart antithrombotic therapy after ICH related to antithrombotic therapy depends on the
risk of subsequent arterial or venous thromboembolism, the risk of recurrent ICH, and the overall state
of the patient. For patients with a comparatively lower risk of cerebral infarction (eg, AF without prior
ischemic stroke) and a higher risk of amyloid angiopathy (eg, elderly patients with lobar ICH) or with very
poor overall neurological function, an antiplatelet agent may be an overall better choice for prevention of
ischemic stroke than warfarin. In patients with a very high risk of thromboembolism in whom restarting
warfarin is considered, warfarin therapy may be restarted at 7 to 10 days after onset of the original ICH
(ASA: Class IIb, LOE B).
2. After having re-checked the indication for anticoagulation (following the EUSI recommendation on
stroke among middle-aged men: The JPHC study cohort I. Stroke. 2004;35:1124-1129.
9. Feldmann E, Broderick J, Kernan W, Viscoli C, Brass L, Brott T, Morgenstern L, Wilterdink J, Horwitz R.
Major risk factors for intracerebral hemorrhage in the young are modifiable. Stroke.2005;36:1881-1885.
3.5.2. 출혈을동반한허혈뇌졸중의이차예방Secondary prevention in ischemic stroke mixed with hemorrhage

CLINICAL RESEARCH CENTER FOR STROKE
318
ischaemeic stroke) oral anticoagulation treatment may be continued after 10-14 days, depending on the
perceived risk of thromboembolic occlusion and ICH recurrence (EUSI: Class IV evidnece).
와파린(warfarin) 복용중에뇌출혈이생긴환자에서와파린을재투여하는것은개별환자의뇌경색
발생위험도를고려해서결정하게된다. 뇌색전증의발생은뇌경색의병력이없는비판막성심방세
동환자에서연5%,1이전에허혈뇌졸중을가진환자에서는연12%,2인공판막을갖고있는환자에서
는최소연4%의발생률을보인다.3와파린복용중에출혈이발생한환자에서와파린을재투여하는
것은허혈뇌졸중의예방이라는면과뇌출혈의재발위험성이라는양면의균형을고려해서결정해
야한다.4하지만와파린을투여하는동안발생한뇌출혈재발에관련된유용한보고가아직까지없
다. 3개의임상연구에서뇌출혈을가진 114명의환자집단에서와파린을중단하고신선냉동혈장
(fresh frozen plasma)으로혈액응고기능을회복시켰을때평균7~10일동안6명(5%)의환자에서색전
증이발생했으며, 1명(0.8%)의환자에서항응고제의투약과관련된재출혈이발생했다.5-7 78명을 상
으로한7개의연구에서항응고제의역전을위해서프로트롬빈복합체농축물(prothrombin complex
concentrate)의투여시4례(5%)의혈전색전증이발생했으며, 혈종의확장이5명(6%)의환자에서지속
되었다.8-13위와같은제한된자료들을통해서인공판막이나만성비판막성심방세동을가진환자에
서뇌출혈후에7-10일간에걸쳐서신선냉동혈장이나프로트롬빈복합체농축물로항응고제를역전
시키는경우에도낮은색전의발생률을보 고, 이후와파린을재투여하는것이안전한것으로관찰
되었다.14
일반적으로아 로이드혈관병증(amyloid angiopathy)과관련된엽상출혈을가진고령의환자는와파
린을지속적으로투여할때나쁜예후를보일가능성이높고, 작은심부출혈을가진환자에서는와파
린을투여하는것과중단하는것이비슷한위험성을보 다. 이러한논란은뇌출혈을가진환자에서
항응고제를투여할것인지, 언제부터투여해야하는지는전향적연구가이루어질때까지해결되지
않을문제이다. 하지만뇌경색의위험성이낮은환자와아 로이드혈관병증의위험성이높은환자
에서는뇌경색의발생을막기위해서항혈소판제의투여가와파린을투여하는것보다는좋은선택
이될것으로보인다. 항혈소판제를투여받은환자들에서뇌출혈이발생했을때항혈소판제의복용
여부가예후에 향을미치는지에 한연구가이루어졌지만, 연구에따라서상이한결과를보여주

CLINICAL RESEARCH CENTER FOR STROKE
319
1. 뇌출혈이발생한환자에서항혈전제투약을다시시작해야할지를결정할때, 혈전의발생위험성,
뇌출혈의재발위험성, 환자의전반적인위험인자등을고려하여결정해야한다. (근거수준 IV, 권고
수준C)
2. 항응고제복용이후뇌출혈이발생한환자에서뇌색전증의재발가능성이낮은경우나출혈의위
험성이높은경우는항응고제 신항혈소판제가투여될수도있지만, 뇌색전증의발생위험이매
우높은환자에서는항응고제가다시투여되는것이바람직하다. 재투여를시작하는시기는이전
뇌출혈발생후7-10일이후가될수있다. (근거수준III, 권고수준B)
었다.
뇌출혈발생시에아스피린(aspirin)을규칙적으로복용하는것이뇌출혈과관련된사망에 한독립
적위험인자로작용한다는후향적인연구결과가있었다.(RR, 2.5; 95% CI, 1.3-4.6) 한편457명의뇌실
질출혈을동반한환자중94명(20.5%)이항혈소판제를복용하고있었지만, 항혈소판제복용여부가
기능적인회복에 향을미치지않는다는보고도있다.15,16뇌출혈이발생한207명의환자중뇌출혈
발생이후항혈소판제가투여된46명(22%)에 한후향적인연구에서, 항혈소판제의투여는뇌출혈
의재발에 향을미치지않는것으로나타났다.17하지만이연구에서는항혈소판제투여가허혈심
혈관질환의발생에중요한기여를했다는것이불명확하므로결과해석에유의하여야한다. 결국뇌
출혈후항혈소판제의투여를결정할때적응증과재출혈의상 적위험성을고려해서제한된환자
에게투여되어야한다.
1. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from
five randomized controlled trials. Arch Intern Med. 1994;154:1449-1457.
2. EAFT (European Atrial Fibrillation Trial) Study Group. Secondary prevention in non-rheumatic atrial fibrillation
after transient ischaemic attack or minor stroke.Lancet. 1993;342:1255-1262.
3. Cannegieter SC, Rosendaal FR, Wintzen AR, van der Meer FJ, Vandenbroucke JP, Briet E. Optimal oral
anticoagulant therapy in patients with mechanical heart valves. N Engl J Med.1995;333:11-17.

CLINICAL RESEARCH CENTER FOR STROKE
320
4. Hacke W. The dilemma of reinstituting anticoagulation for patients with cardioembolic sources and
intracranial hemorrhage: How wide is the strait between Skylla and Karybdis? Arch Neurol. 2000;57:1682-
1684.
5. Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valve patients after intracranial
haemorrhage: A 2-year follow-up. Br J Haematol. 1998;103:1064-1066.
6. Wijdicks EF, Schievink WI, Brown RD, Mullany CJ. The dilemma of discontinuation of anticoagulation therapy
for patients with intracranial hemorrhage and mechanical heart valves. Neurosurgery. 1998;42:769-773.
7. Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagulation in patients with intracranial
hemorrhage at high thromboembolic risk. Arch Neurol. 2000;57:1710-1713.
8. Makris M, Greaves M, Phillips WS, Kitchen S, Rosendaal FR, Preston EF. Emergency oral anticoagulant
reversal: the relative efficacy of infusions of fresh frozen plasma and clotting factor concentrate on correction of
the coagulopathy. Thromb Haemost.1997;77:477-480.
9. Boulis NM, Bobek MP, Schmaier A, Hoff JT. Use of factor IX complex in warfarin-related intracranial
hemorrhage. Neurosurgery. 1999;45:1113-1118.
10. Cartmill M, Dolan G, Byrne JL, Byrne PO. Prothrombin complex concentrate for oral anticoagulant reversal
in neurosurgical emergencies. Br J Neurosurg.2000;14:458-461.
11. Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeutic dilemma: patients with
spontaneous intracerebral hemorrhage and urgent need for anticoagulation. J Neurol. 2000;247:209-214.
12. Sjoblom L, Hardemark HG, Lindgren A, Norrving B, Fahlen M, Samuelsson M, Stigendal L, Stockelberg D,
Taghavi A, Wallrup L, Wallvik J. Management and prognostic features of intracerebral hemorrhage during
anticoagulant therapy: a Swedish multicenter study. Stroke. 2001;32:2567-2574.
13. Yasaka M, Sakata T, Minematsu K, Naritomi H. Correction of INR by prothrombin complex concentrate and
vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
14. Estol CJ, Kase CS. Need for Continued Use of Anticoagulants After Intracerebral Hemorrhage. Curr Treat
Options Cardiovasc Med. 2003;5:201-209.
15. Saloheimo P, Ahonen M, Juvela S, Pyhtinen J, Savolainen ER, Hillbom M. Regular aspirin-use preceding the
onset of primary intracerebral hemorrhage is an independent predictor for death. Stroke. 2006;37:129-133.

CLINICAL RESEARCH CENTER FOR STROKE
321
두개강외경동맥박리와척추동맥박리는젊은성인뇌졸중의주요원인중하나로동맥-동맥색전
증이나근위부동맥의협착및폐색을유발하여허혈뇌졸중을일으킬수있으며, 일부에서는거짓
동맥류를생성함으로써혈전을발생시키기도한다. 또한, 두개내동맥박리가척추뇌바닥동맥에서
발생하면혈관파열과거미막밑출혈이발생할수있다. 동맥박리에의한허혈뇌졸중의치료는허
혈뇌졸중의재발을막고박리혈관을치료하기위해시행되며, 주로항응고제의사용[정주용헤파
린(heparin) 또는경구용항응고제]이나항혈소판제의투여, 스텐트설치술을사용한혈관내막의치
료, 수술적치료등이가능하다.
1. For patients with ischemic stroke or TIA and extracranial arterial dissection, use of warfarin for 3 to 6
months or use of antiplatelet agents is reasonable (ASA: Class IIa, LOE B). Beyond 3 to 6 months, long-
term antiplatelet therapy is reasonable for most stroke or TIA patients. Anticoaulant therapy beyond 3 to
6 months may be considered among patients with recurrent ischemic events (ASA: Class IIb, LOE C).
2. For patients who have definite recurrent ischemic events despite adequate antithrombotic therapy,
endovascular therapy (stenting) may be considered (ASA: Class IIb, LOE C). Patients who fail or are not
candidates for endovascular therapy may be considered for surgical treatment (ASA: Class IIb, LOE C).
3. Cross-sectional MRI should be considered with MRA where arterial dissection needs to be excluded
16. Caso V, Paciaroni M, Venti M, Alberti A, Palmerini F, Milia P, Billeci AM, Silvestrelli G, Biagini S, Agnelli G.
Effect of on-admission antiplatelet treatment on patients with cerebral hemorrhage. Cerebrovasc Dis.
2007;24:215-218.
17. Viswanathan A, Rakich SM, Engel C, Snider R, Rosand J, Greenberg SM, Smith EE. Antiplatelet use after
intracerebral hemorrhage. Neurology.2006;66:206-209.
3.5.3. 동맥박리Arterial dissection

CLINICAL RESEARCH CENTER FOR STROKE
322
(RCP: D,LOE IV).
동맥박리에의한뇌졸중의재발빈도는비교적낮아, 첫발생후2-5년사이에1-4%가재발한다.1,2 400
명이상의경동맥박리환자를 상으로한 규모연구에서뇌졸중의재발률과박리의재발율은각
각1% 으며,2박리환자116명을 상으로한전향적연구에따르면뇌졸중의재발율은4%이었다.3
재개통을비롯한해부학적치료가전체환자의72-100%에서일어나며,4-6박리의완전한치료와뇌졸
중재발의연관관계는없는것으로보여진다.2,7뇌졸중의동반유무와상관없이혈관박리환자는정
맥내헤파린주입후와파린(warfarin)을3-6개월간사용하는것이일반적이나, 이에 한전향적인무
작위연구는시행된적이없다. 단지일부연구에서경동맥박리시정맥내헤파린투여가색전을예
방하는효과가있음이확인되었다.4-6,8 헤파린사용이출혈을일으키는위험성은5% 미만으로높지않
았으나5거미막밑출혈이있는경우는사용금기이다. 항응고제와항혈소판제의효과를비교한작은
규모의연구에서는두군간에차이는없는것으로나타났다.4,9스텐트는내과적치료가실패하는경
우고려 상이되며, 혈관협착의정도를줄이고박리의확장과거짓동맥류의발생을막는것으로
보여지나무작위연구는시행된적이없다.10-13수술적치료도시도되지만합병증이발생할가능성이
비교적높다.13-15
1. 두개강외동맥박리에의해허혈뇌졸중이나일과성허혈발작이발생한경우3-6개월간의항응고
제나항혈소판제의복용이권유되며, (근거수준 IIa, 권고수준B) 이후에도장기간의항혈소판제의
복용을고려할수있다. (근거수준IV, 권고수준C)
2. 적절한약물적치료에도불구하고재발이있는경우는스텐트시술이권유되며, (근거수준 III, 권고
수준B) 스텐트시술이어려운경우는수술적치료가고려될수있다. (근거수준IV, 권고수준C)
1. Bassetti C, Carruzzo A, Sturzenegger M, Tuncdogan E. Recurrence of cervical artery dissection. A prospective

CLINICAL RESEARCH CENTER FOR STROKE
323
study of 81 patients. Stroke. 1996;27:1804-1807.
2. Touze E, Gauvrit JY, Moulin T, Meder JF, Bracard S, Mas JL. Risk of stroke and recurrent dissection after a
cervical artery dissection: A multicenter study. Neurology. 2003;61:1347-1351.
3. Beletsky V, Nadareishvili Z, Lynch J, Shuaib A, Woolfenden A, Norris JW. Cervical arterial dissection: Time for
a therapeutic trial? Stroke. 2003;34:2856-2860.
4. Engelter ST, Lyrer PA, Kirsch EC, Steck AJ. Long-term follow-up after extracranial internal carotid artery
dissection. Eur Neurol. 2000;44:199-204.
5. Jacobs A, Lanfermann H, Neveling M, Szelies B, Schroder R, Heiss WD. MRI- and MRA-guided therapy of
carotid and vertebral artery dissections. J Neurol Sci. 1997;147:27-34.
6. Schievink WI. The treatment of spontaneous carotid and vertebral artery dissections. Curr Opin Cardiol.
2000;15:316-321.
7. Guillon B, Brunereau L, Biousse V, Djouhri H, Levy C, Bousser MG. Long-term follow-up of aneurysms
developed during extracranial internal carotid artery dissection. Neurology. 1999;53:117-122.
8. Bassi P, Lattuada P, Gomitoni A. Cervical cerebral artery dissection: A multicenter prospective study
(preliminary report). Neurol Sci. 2003;24 Suppl 1:S4-7.
9. Lyrer P, Engelter S. Antithrombotic drugs for carotid artery dissection. Cochrane Database Syst Rev.
2003:CD000255.
10. Cohen JE, Leker RR, Gotkine M, Gomori M, Ben-Hur T. Emergent stenting to treat patients with carotid
artery dissection: Clinically and radiologically directed therapeutic decision making. Stroke. 2003;34:e254-
257.
11. Lylyk P, Cohen JE, Ceratto R, Ferrario A, Miranda C. Angioplasty and stent placement in intracranial
atherosclerotic stenoses and dissections. Am J Neuroradiol. 2002;23:430-436.
12. Malek AM, Higashida RT, Phatouros CC, Lempert TE, Meyers PM, Smith WS, Dowd CF, Halbach VV.
Endovascular management of extracranial carotid artery dissection achieved using stent angioplasty. Am J
Neuroradiol. 2000;21:1280-1292.
13. Muller BT, Luther B, Hort W, Neumann-Haefelin T, Aulich A, Sandmann W. Surgical treatment of 50 carotid
dissections: Indications and results. J Vasc Surg. 2000;31:980-988.

CLINICAL RESEARCH CENTER FOR STROKE
324
열린타원구멍(patent foramen ovale)은비교적흔한선천성심장질환으로젊은나이에서발생하는원
인불명(cryptogenic)의허혈뇌졸중또는일과성허혈발작의주요원인질환이다. 특히심방격벽동맥
류(atrial septal aneurysm)가동반되는경우는뇌졸중발생의위험이높아진다고알려져있다.
3.5.4. 열린타원구멍과심방중격동맥류Patent foramen ovale and atrial septal aneurysm
1. For patients with an ischemic stroke or TIA and PFO, antiplatelet therapy is reasonable to prevent a
recurrent event (ASA: Class IIa, LOE B). Warfarin is reasonable for high-risk patients who have other
indications for oral anticoagulation such as those with an underlying hypercoagulable state or evidence of
venous thrombosis (ASA: Class IIa, LOE C).
2. Insufficient data exist to make a recommendation about PFO closure in patients with a first stroke and a
PFO. PFO closure may be considered for patients with recurrent cryptogenic stroke despite optimal
medical therapy (ASA: Class IIb, LOE C).
55세이하의젊은원인불명허혈뇌졸중환자(n=581)를분석한연구에서, 열린타원구멍의유병률은
46%로보고되었다.1환자- 조군연구의메타분석에서55세이하의허혈뇌졸중환자들중열린타원
구멍(OR=3.1; 95% CI, 2.3-4.2), 심방격벽동맥류(OR=6.1; 95% CI, 2.5-15.2%), 열린타원구멍과심방격벽
14. Balas P, Ioannou N, Milas P, Klonaris C. Surgical treatment of spontaneous internal carotid dissection. Int
Angiol. 1998;17:125-128.
15. Nussbaum ES, Erickson DL. Extracranial-intracranial bypass for ischemic cerebrovascular disease
refractory to maximal medical therapy. Neurosurgery.2000;46:37-42.

CLINICAL RESEARCH CENTER FOR STROKE
325
동맥류동반질환(OR=15.59; 95% CI, 2.83-85.87)을갖고있는환자의위험도가높았다.2
Patent Foramen Ovale in Cryptogenic Stroke Study(PICSS)는열린타원구멍환자에서아스피린(aspirin)
과와파린(warfarin)의효과를비교한유일한무작위 조연구로, 전체630명의허혈뇌졸중환자중
203명(33.8%) 그리고 265명의원인불명허혈뇌졸중환자중 98명(39.2%)에서열린타원구멍이발견
되었다.3이연구는열린타원구멍이발견된원인불명허혈뇌졸중환자들을하루325mg의아스피린
(17.9%, n=56) 투여군과와파린(9.5%, n=42) 투여군으로무작위배정하고평균 24개월간비교하 으
며, 양치료군에서허혈뇌졸중재발률및사망률에서유의한차이가없었다.(p=0.49; HR 0.52; 95% CI,
0.16-1.67; 2년발생률 16.5% vs. 13.2%) 그러나 PICSS 연구는Warfarin/Aspirin Recurrent Stroke
Study(WARSS)의 sub-study로실질적인무작위 조연구보다는전향적코호트연구의성격을띠고
있으므로해석에유의해야한다. 다른전향적코호트연구인Lausanne study에서도아스피린, 와파
린, 수술적닫힘치료를받은환자들의허혈뇌졸중발생에의미있는차이가없었다.4열린타원구멍
을가진허혈뇌졸중환자에서아스피린과와파린의이차예방효과의우열을결정하기에는관련근
거가부족하다. 하지만PICSS에서양군의주요출혈발생률은비슷했으나경미한출혈의발생은와
파린군에서많았다.3 (RR=2.64, p<0.001)
열린타원구멍의닫힘치료와약물치료의이차예방효과를비교한전향적무작위배정연구는아직
보고된바가없다. 열린타원구멍의수술적닫힘치료에 한환자증례연구들에서수술적닫힘치료
의안정성과효과는상반된결과를보 다.5,6 1,355명의카테터닫힘치료와895명의약물치료를받
은열린타원구멍을가진허혈뇌졸중환자들을비교분석한계통적분석연구(systematic review)에서
1년간허혈뇌졸중재발률이카테터닫힘치료군에서 0-4.9%이었으며, 895명의약물치료군에서
3.8-12.0%이었다.7그러나이논문에서언급된연구들은모두비무작위배정연구이며열린타원구멍
의카테터닫힘치료의효과에 한무작위배정연구는현재진행중에있다.
1. 젊은나이의원인불명허혈뇌졸중환자에서는열린타원구멍또는심방격벽동맥류에 한검사를
실시하는것이바람직하다. (근거수준III, 권고수준B)
2. 열린타원구멍을가진원인불명허혈뇌졸중환자에서항혈소판제투여를하는것이바람직하다.
(근거수준IIb, 권고수준B)

CLINICAL RESEARCH CENTER FOR STROKE
326
3. 열린타원구멍을가진원인불명허혈뇌졸중환자에서과응고질환(hypercoagulable disease) 또는
깊은정맥혈전증(deep vein thrombosis)이동반된경우에는와파린치료를하는것을고려해볼수
있다. (근거수준IV, 권고수준C)
4. 열린타원구멍환자에서허혈뇌졸중이처음으로발생한경우, 열린타원구멍닫힘(PFO closure) 치료
의유용성에 한근거는불충분하다. 그러나적절한약물치료에도불구하고원인불명의허혈뇌
졸중이재발하는환자에서는열린타원구멍닫힘치료가고려될수있다. (근거수준III, 권고수준B)
1. Lamy C, Giannesini C, Zuber M, Arquizan C, Meder JF, Trystram D, Coste J, Mas JL. Clinical and imaging
findings in cryptogenic stroke patients with and without patent foramen ovale: The PFO-ASA study.
Stroke. 2002;33:706-711.
2. Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: A meta-analysis of case-control
studies. Neurology. 2000;55:1172-1179.
3. Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP, for the PFOiCSSI. Effect of medical treatment in
stroke patients with patent foramen ovale: Patent foramen ovale in cryptogenic stroke study. Circulation.
2002;105:2625-2631.
4. Bogousslavsky J GS, Jeanrenaud X, et al. Stroke recurrence in patients with patent foramen ovale: The
Lausanne study. Lausanne stroke with paradoxical embolism study group. Neurology. 1993;46:1301-
1305.
5. Homma S, Di Tullio MR, Sacco RL, Sciacca RR, Smith C, Mohr JP. Surgical closure of patent foramen
ovale in cryptogenic stroke patients. Stroke.1997;28:2376-2381.
6. Ruchat P, Bogousslavsky J, Hurni M, Fischer AP, Jeanrenaud X, von Segesser LK. Systematic surgical
closure of patent foramen ovale in selected patients with cerebrovascular events due to paradoxical
embolism. Early results of a preliminary study. Eur J Cardiothorac Surg.1997;11:824-827.
7. Khairy P, O'Donnell CP, Landzberg MJ. Transcatheter closure versus medical therapy of patent foramen
ovale and presumed paradoxical thromboemboli: A systematic review. Ann Intern Med. 2003;139:753-
760.

CLINICAL RESEARCH CENTER FOR STROKE
327
항인지질항체(antiphospholipid antibody)는일반인의 1-6.5%에서관찰되며노인에서나루푸스환자
에서더높게관찰된다.1항인지질항체는뇌졸중환자의 8.2-9.7%에서관찰되며,2특히 50세이하의
젊은뇌졸중환자에서는항인지질항체의존재와뇌졸중의관련성이높다.3항인지질항체증후군은
여러장기의정맥과동맥이폐색되거나, 유산혹은그물울혈반(livedo reticularis)을유발하는드문임
상증후군이다.4임상양상의다양성과진단의어려움으로인해서항인지질항체증후군환자들을치
료하기위한잘계획된임상연구는드물다. 그러므로항인지질항체증후군에 한현재까지의진료
지침은매우제한적인내용만을담고있다.
1. For cases of cryptogenic ischemic stroke or TIA and positive APL(anti-phospho lipid) antibodies,
antiplatelet therapy is reasonable (ASA: Class IIa, LOE B).
2. For patients with ischemic stroke or TIA who meet the criteria for the APL antibody syndrome with
venous and arterial occlusive disease in multiple organs, miscarriages, and livedo reticularis, oral
anticoagulation with target INR of 2 to 3 is reasonable (ASA: Class IIa, LOE B).
항인지질항체를가지고있는젊은환자들에서뇌졸중의재발률이높다는여러연구가보고되고있
다.5,6. 작은이중맹검무작위배정임상시험을통해서항인지질항체와혈전증의병력이있는환자에
서 INR 3.1-4.0의고강도와파린(warfarin) 치료와 INR 2.0-3.0의중등도와파린치료의혈전예방효과
를비교하 다. 이연구에서는 INR 2.0-3.0의와파린치료가혈전재발률이더낮고더안전하 다.7
따라서항인지질항체증후군환자에서는 INR 2.0-3.0의와파린치료가권장된다. 그러나노인을 상
으로하는연구들에서항인지질의존재와뇌졸중재발과의연관성에 해서논란이있다.
WARSS/APASS collaboration은와파린(INR 1.4-2.8)과아스피린(325mg)를무작위배정하여뇌졸중이
차예방효과를비교하 다. APASS는WARSS 피험자들중에서 720명의항인지질항체양성환자를
3.5.5. 항인지질항체증후Antiphospholipid antibody syndrome

CLINICAL RESEARCH CENTER FOR STROKE
328
상으로하 다. 전체허혈성사건발생률은항인지질항체양성인환자군에서22.2%로항인지질항
체음성인환자21.8%에비해서높지않았다. 또한와파린을사용한군이나아스피린을사용한군에
서어떤종류에의한사망, 허혈뇌졸중, 일과성허혈발작, 심근경색, 깊은정맥혈전증, 폐색전증등을
포함하는주관찰변수에서차이가없었다.8
1. 기전이불명확한허혈뇌졸중이나일과성허혈발작환자에서항인지질항체양성인경우항혈소판
제의사용이권장된다. (근거수준III, 권고수준B)
2. 여러장기의정맥이나동맥혈전증, 유산, 그물울혈반의증상등항인지질항체증후군의진단기준
을만족하는허혈뇌졸중이나일과성허혈발작환자에서는경구항응고제 (INR 2-3)의사용이권장
된다. (근거수준III, 권고수준B)
1. Vila P, Hernandez MC, Lopez-Fernandez MF, Batlle J. Prevalence, follow-up and clinical significance of
the anticardiolipin antibodies in normal subjects. Thromb Haemost. 1994;72:209-213.
2. The antiphospholipid antibodies in stroke study (APASS) group. Anticardiolipin antibodies are an
independent risk factor for first ischemic stroke. Neurology.1993;43:2069-2073.
3. Nencini P, Baruffi MC, Abbate R, Massai G, Amaducci L, Inzitari D. Lupus anticoagulant and
anticardiolipin antibodies in young adults with cerebral ischemia. Stroke. 1992;23:189-193.
4. Cervera R, Font J, Gomez-Puerta JA, Espinosa G, Cucho M, Bucciarelli S, Ramos-Casals M, Ingelmo M,
Piette JC, Shoenfeld Y, Asherson RA. Validation of the preliminary criteria for the classification of
catastrophic antiphospholipid syndrome. Ann Rheum Dis. 2005;64:1205-1209.
5. Kittner SJ, Gorelick PB. Antiphospholipid antibodies and stroke: An epidemiological perspective. Stroke.
1992;23:I19-22.
6. Levine SR, Brey RL, Sawaya KL, Salowich-Palm L, Kokkinos J, Kostrzema B, Perry M, Havstad S, Carey
J. Recurrent stroke and thrombo-occlusive events in the antiphospholipid syndrome. Ann Neurol.
1995;38:119-124.

CLINICAL RESEARCH CENTER FOR STROKE
329
정맥성뇌경색으로인하여두통, 국소적신경계결손, 발작, 의식장애, 유두부종등과같은매우다양
한증상이나타날수있으며, CT 및MRI에서미세한변화만나타나진단이쉽지않은편이다. 과거침
습적혈관조 술이확진에사용되었으나, 현재MR 정맥혈관촬 이가장널리사용된다. 정맥경색
에서는출혈과혈관탓부종(vasogenic edema)이동반되는경우가많으며, 규모의무작위임상연
구는시행되지않았으나최근내과적치료로헤파린(UFH, unfrationated heparin)과저분자량헤파린
(LMWH, low-molecular-weight heparin)이사용된다.
1. For patients with cerebral venous thrombosis, UFH (unfrationated heparin) or LMWH (low-molecular-
weight heparin) is reasonable even in the presence of hemorrhagic infarction (ASA: Class IIa, LOE B).
Continuation of anticoagulation with an oral anticoagulant agent is reasonable for 3 to 6 months, followed
by antiplatelet therapy (ASA: Class IIa, LOE C).
2. Cross-sectional MRI should be performed with MR venogram where venous thrombosis needs to be
excluded and has not been demonstrated on CT (RCP: D LOEIV).
3. Cases with suspected or confirmed cerebral venous thrombosis should be commenced on heparin
7. Crowther MA, Ginsberg JS, Julian J, Denburg J, Hirsh J, Douketis J, Laskin C, Fortin P, Anderson D,
Kearon C, Clarke A, Geerts W, Forgie M, Green D, Costantini L, Yacura W, Wilson S, Gent M, Kovacs MJ.
A comparison of two intensities of warfarin for the prevention of recurrent thrombosis in patients with
the antiphospholipid antibody syndrome. N Engl J Med. 2003;349:1133-1138.
8. Levine SR, Brey RL, Tilley BC, Thompson JL, Sacco RL, Sciacca RR, Murphy A, Lu Y, Costigan TM, Rhine
C, Levin B, Triplett DA, Mohr JP. Antiphospholipid antibodies and subsequent thrombo-occlusive events
in patients with ischemic stroke. Jama. 2004;291:576-584.
3.5.6. 정맥성뇌경색Venous Infarction

CLINICAL RESEARCH CENTER FOR STROKE
330
정맥성뇌경색환자를 상으로헤파린(PTT를2배로유지함)과위약을비교한연구는헤파린사용군
의의미있는효과때문에20명만의데이터를수집한후조기종료되었다.1(p<0.01) 이연구에서무작
위로배정되어헤파린을사용한10명의환자중8명은완전히회복하 고2명은경한신경계결손만
이남았으나, 위약군에서는1명만완전히회복되었고3명은사망하 다. 또한, 43명의 뇌출혈을동
반한정맥경색환자에서도 27명의환자들은저분자량헤파린을사용한결과미사용군에비해유의
하게사망률이적은것으로나타났다.1 이보다더많은환자들을(n=59) 상으로나드로파린
(nadroparin)과위약을비교한연구가이루어졌다. 정맥성뇌경색발생이후3개월간추적한결과, 나
드로파린사용군에서 13%, 위약군에서 21%의사망및mRS 3 이상의불량한결과가관찰되었으
나,(p=NS) 나드로파린군에서2명이사망한반면위약군에서는4명이사망하 다.2기타다른관찰연
구에서도헤파린(UFH)과저분자량헤파린(LMWH)이모두안전하며효과적이었고, 출혈이동반된정
맥성뇌경색에서도항응고제의사용은바람직한것으로나타났다. 항응고제의사용기간에 한연
구는없었으나일반적으로 3-6개월간의경구용항응고제사용이추천된다. 항응고제를사용함에도
증상이악화되는경우는혈전용해제를국소적으로혈전내로주입하는것이좋다는보고도있으나3
이에 해서는향후계속적인연구가필요하다.
(RCP: B LOEIV).
1. 정맥경색은출혈이동반된경우라도헤파린(UFH)이나저분자량헤파린(LMWH)을사용할수있다.
(근거수준IIa, 권고수준B)
2. 초기3-6 개월간경구용항응고제를사용할수있으며, 이후일정기간이상의항혈소판제의사용
이고려된다. (근거수준IV, 권고수준C).
1. Einhaupl KM, Villringer A, Meister W, Mehraein S, Garner C, Pellkofer M, Haberl RL, Pfister HW, Schmiedek P.
Heparin treatment in sinus venous thrombosis. Lancet.1991;338:597-600.

CLINICAL RESEARCH CENTER FOR STROKE
331
2. de Bruijn SF, Stam J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-
weight heparin for cerebral sinus thrombosis. Stroke. 1999;30:484-488.
3. Frey JL, Muro GJ, McDougall CG, Dean BL, Jahnke HK. Cerebral venous thrombosis: Combined
intrathrombus rtpa and intravenous heparin. Stroke. 1999;30:489-494.

제목 | 뇌졸중진료지침(개정판)
발행 | 초판1쇄발행 / 2009년10월30일
2판1쇄발행 / 2013년2월22일
저자 | 뇌졸중임상연구센터
발행인 | 보건복지부지정뇌졸중임상연구센터
주소 | 110-744 서울시종로구대학로101 서울대학교병원임상의학연구소7208호
연락처 | (02)2072-1835
가격 | 비매품
ISBN 978-89-94181-20-2
※이책의전부또는일부내용을재사용하려면사전에저작권자와서면에의한동의를받아야합니다.
※본진료지침은뇌졸중임상연구센터홈페이지(http://www.stroke-crc.or.kr)를통해서도확인할수있습니다.














![Pertemuan 2 130227 Statistika Ekonomi Dan Bisnis2 [Compatibility Mode]](https://static.fdocuments.net/doc/165x107/55cf98ba550346d0339953f0/pertemuan-2-130227-statistika-ekonomi-dan-bisnis2-compatibility-mode.jpg)




