
Enthesial lesions and spondylarthropathies: clinical and ... · Enthesial lesions and...
35
Enthesial lesions and spondylarthropathies: clinical and paleopathological insights Carina Marques Centro de Investigação em Antropologia e Saúde Department of Anthropology, University of Coimbra Portugal [email protected] Workshop in Musculoskeletal Stress Markers (MSM): limitations and achievements in the reconstruction of past activity patterns
Transcript of Enthesial lesions and spondylarthropathies: clinical and ... · Enthesial lesions and...

Enthesial lesions and spondylarthropathies:
clinical and paleopathological insights
Carina MarquesCentro de Investigação em Antropologia e SaúdeCe t o de est gação e t opo og a e SaúdeDepartment of Anthropology, University of [email protected]
Workshop in Musculoskeletal Stress Markers (MSM): limitations and
achievements in the reconstructionof past activity patterns
ConceptSpondylarthropathies
Broad group of inflammatory chronic arthropathies or erosive arthropathies
Spondylarthropathy (SpA)
Concept: that comprises different clinical entities
Share common etiological pathophysiological and clinical featuresShare common etiological, pathophysiological and clinical features

ConceptSpondylarthropathies
According to the European Spondylarthropathy Study Group (1991)
•Axial inflammation [sacroiliitis, spondylitis] Ankylosing spondylitis (AS) Reactive arthritis (ReA)Axial inflammation [sacroiliitis, spondylitis]
• Peripheral arthritis
[Inflammatory chronic disease of the spine ]( )
[Arthritis consequence of extra-articular infection -generally genitourinary and/or gastrointestinal]
• Enthesitis
• Eye and mucocutaneous lesions
Psoriatic arthritis (PsA)
[Arthritis associated with psoriasis] Undifferentiated )
y
• Genetic features
spondyloarthritis (uSpA)[Clinical spectrum does not correspond to any other entity]
• Association with HLA-B27 antigen
Enteropathic arthritis (EA)
[Arthritis connected with inflammatory bowel disease ]
Juvenile SpA
[Arthritis connected with inflammatory bowel disease ]
SAPHO- ?

ConceptSpondylarthropathies
Between entities: overlap of symptoms and signs
Each entity: heterogeneity of disease phenotypey g y p yp

EpidemiologySpondylarthropathies
General prevalence: 0,5% - 2%p
Prevalence Sex Age
Ankylosing spondylitis (AS) 0 2-1 2% M>F 20-30Ankylosing spondylitis (AS) 0,2 1,2% M>F 20 30
Reactive arthritis (ReA) 0,1% M>F 20-35
Psoriatic arthritis (PsA) 0,1-1% M=F 40-50
Enteropathic arthritis (EA) 0,2% M=F 20-30
Undifferentiated spondyloarthritis (uSpA) 0,7-2% F>M 20-30
Haida Indians, Canada: 4.2% ASquen
cy
Haida Indians, Canada: 4.2% AS
Navajo (USA), Pawaia Papua New Guinea,
Alaska Natives Chukotka RussiaHLA-
B27
freq
Alaska Natives, Chukotka Russia
High
H

EtiologySpondylarthropathies
Interaction
■ Immune systemHLA-B27 allele
E i t l ti li
HLA B27 allele
Mechanical stress
■ Environmental stimuli Bacterial pathogens
Mechanical stress

PathologySpondylarthropathies
The abnormal inflammatory response characterizes these conditions:The abnormal inflammatory response characterizes these conditions:
Enthesitis and synovitis are the fundamental pathological characteristics in SpA
The inflammation occurs primarily at the enthesis or at the synovium?

Target of inflammation: hypothesisSpondylarthropathies
I- Primarily enthesial disease
• Postulated during the 70’s Ball and co-workers: First description of inflammation at the enthesis on SpA
• Reviewed by Fourier et al. (2004): “entheseal territory” - Broaden the concept of “entheses” to include the
amphiarthroses and diartho-amphiarthroses
main and initial target of the disease process in SpAmain and initial target of the disease process in SpA
• McGonagle & Benjamin research group: “enthesis organ”
Primary event: Enthesitis (fibrocartilaginous enthesis)
Secondary spread of inflammation to the synovium

Spondylarthropathies Target of inflammation: hypothesis
II The synoviumII- The synovium
O h li f h i fl f h j i b l i d b h i i l • Other lines of research : inflammatory process of the joints cannot be explained by enthesitis alone.
[François et al., 2000; François et al., 2001; Lories et al., 2004; Helliwell & Porter, 2007]
III - The bone
• Other lines of research : crucial role of bone marrow inflammation, as initial process in SpA. Autoimmunity is at the core of this proposal
[Jacques et al., 2008]

Pathological featuresSpondylarthropathies
Key features:
Enthesis [Fibrocartilaginous] -- Synovial joints -- Cartilaginous joints[ ] y j g j
• Articular
• Extra-articular
Distinctive characteristic Erosions New bone
formationAnkylosis
SKELETON: Axial and appendicular

Pattern of distributionSpondylarthropathies
AXIAL ARTICULAR LESIONS
• Sacroiliac (SI)• Vertebral body • Zygapophyseal Zygapophyseal • Costovertebral
• Pubic symphysis
M b i t l• Manubriosternal
• Acromioclavicular
• Sternocostoclavicular
APPENDICULAR
• Hands and feet• Shoulder• Hip• Knee

Paleopathological featuresSpondylarthropathies
• Sacroiliac Joint (SI)
ISCMB, SI Joint
Skn.
º118
3.
ISCMB. SI Joint

Spondylarthropathies
C l t b l b d
Paleopathological features
• Column: vertebral body
Syndesmophytes: thin, marginal, vertical growths - Inflammation ony p y g g
the insertion of the outer fibers of the anulus fibrosus and short
fibers of the anterior longitudinal ligament. [Entesophytes]
ebra
e
From: Freemont (2002) pg. 5 - Syndesmophyte formation.
hora
cic ve
rte
ISCM
B. T
h
Spondylarthropathies
C l t b l b d
Paleopathological features
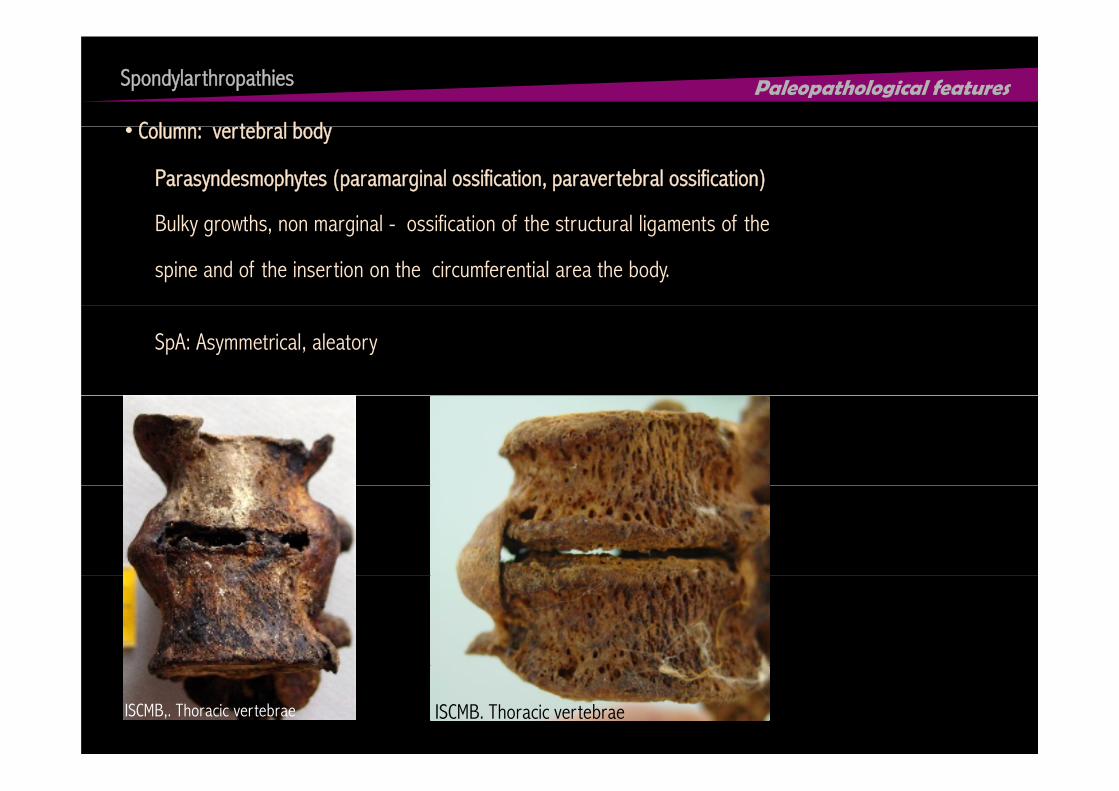
Parasyndesmophytes (paramarginal ossification, paravertebral ossification)
B lk h i l ifi i f h l li f h
• Column: vertebral body
Bulky growths, non marginal - ossification of the structural ligaments of the
spine and of the insertion on the circumferential area the body.
SpA: Asymmetrical, aleatory
ISCMB. Thoracic vertebraeISCMB,. Thoracic vertebrae

Spondylarthropathies
C l t i i
Paleopathological features
• Column: posterior region
tebr
aeTh
orac
ic ve
rtIS
CMB.
T
Lesions• Zygapophyseal joint• Costovertebral joint• Spinous process

Spondylarthropathies Paleopathological features
ISCMB.Bamboo spine

Spondylarthropathies Paleopathological features
A di l k l t i h l j i t • Appendicular skeleton: peripheral joints
sal
imal
met
atar
s
nxl
ISCM
B. P
roxi
SCM
B. P
halan
eal jo
int
IS
nter
phala
nge
ISCM
B. I

Spondylarthropathies Paleopathological features
A di l k l t• Appendicular skeleton
Scap
ula
ISCMB. Humerus
ISCM
B. S
ISCMB. Knee Joint
ISCMB.Radius

Pattern of distributionSpondylarthropathies
AXIAL ARTICULAR LESIONS CLASSIC ENTHESES
• Iliac crests• Ischial tuberosities • Vertebral spinous processesVertebral spinous processes• Calcaneus [Achilles tendon and plantar fascia]
APPENDICULAR
• Ligaments of hand and feet • Patella • Tibial tubercle Tibial tubercle • Greater lesser throchanters• Shoulder
H meral epicond les• Humeral epicondyles
•Ulna (olecranon)

Entheses Spondylarthropathies
In SpA , the lesions at entheses are important features
The scrutiny of these conditions should be performed when analyzing entesophytes
on the research of human activity patterns. y p
How attainable is to identify SpA in paleopathology ?

Work hypothesisSpondylarthropathies
Identified Skeletal Collection Museu Bocage
Museu Nacional de História Natural, Lisboa
Hypothesis: Methodological impact on the assessment of spondylarthropathies in past populationsHypothesis: Methodological impact on the assessment of spondylarthropathies in past populations
Based on previous paleopathology data
• Considered rare
• Variation of the diagnostic criteria used
• Scarce population approach to SpA
• Existent studies present accentuated range of disease prevalence

Sample Spondylarthropathies
Identified Skeletal Collection Museu Bocage
Museu Nacional de História Natural LisboaMuseu Nacional de História Natural, Lisboa
N= 573 adults [ Age range: 20 98 years old]N= 573 adults [ Age range: 20-98 years old]
N= 314 ♀ [55%]
N= 259 ♂ [45%]
Biographical data
N= 259 ♂ [45%]
Escola Politécnica, início séc. XX. ©Câmara Municipal de Lisboa
Biographical data
• Sex
• Chronology: 19th- 20th centuries• Age at death
• Year and cause of death
• Place of birth
• Occupation

MethodologySpondylarthropathies
Lesions analysis
• Macroscopic observation
Methodological Test
• Diagnostic criteria described on the works of: • Diagnostic criteria described on the works of:
•Rothschild (2002), Rothschild et al. (1999), Rothschild e Martin (1993), Rothschild e Woods (1991) EqualRothschild e Woods (1991)
• Martin-Dupont (2005)
R W ld (1995) R t l (1987)
Equal• Sample • Observer• Observation parameters• Rogers e Waldron (1995), Rogers et al. (1987) Observation parameters

Results & DiscussionSpondylarthropathies
9,9%10,7%
1,8%
n= 51 n= 55 5,1%
n= 263,7%
19 %
Syndesmophytes[N 514]
Paravertebral[N 514]
Lesion peripheral joints
Fusionperipheral joints
Zygapophysis[N 514]
Sacroiliac[N 496]
1,8%n= 9
n= 19 1,2%n= 6
[N=514] [N=514] peripheral joints[N=510]
peripheral joints[N=510]
[N=514][N=496]

Results & DiscussionSpondylarthropathies
21 [41,2%]
18 [32,7%]
45
50
55
Sem associaçãoNo association [isolated lesion]Nº In
divid
uals
p< 0,0535
40
Sem associação
Com associação
No association [isolated lesion]
With association [association with at least one other
SpA feature]
N
p> 0,05
37 [67 3%]
6 [23,1%]
20
25
30p> 0,05
30 [58,8%]
37 [67,3%]
20 [76,9%]16 [84,2%]2 [22,2%]
3 [15,8%]
10
15
7 [77,8%]2 [33,3%]
4 [66,7%]
0
5
Sacro-ilíaca Apófises vertebrais Sindesmófitos Paravertebral Lesões articulações periféricas
Fusões articulações periféricas
Sacroiliac Zygapophysis Syndesmophytes Paravertebral Lesion peripheral joints
Fusionperipheral joints

Results & DiscussionSpondylarthropathies
This results confirmed that:
• The most “typical” and complete pattern
was infrequent
ISCMB.

Results & DiscussionSpondylarthropathies
11,7%
6,8%
4,9%
10 7%
15,6%
10,7%
3,9%
Rogers e Col Martin-Dupont Rothschild e Col
n= 80n= 55n= 20
A B CRogers e Col. Martin Dupont(2005)
Rothschild e Col.A B C

Results & DiscussionSpondylarthropathies
Clinical Report Lesion Clinical diagnosis
Erb et al. ( 2005)Braun & Sieper (1996)
• Sacroiliitis Lupus, sarcoidosis, infectious diseaseBraun & Sieper (1996)
Hoshino et al. (2006) • Sacroiliitis Acute myeloid leukemia
Rombauts et al (2000) • Zygapophyseal ankylosis Septic ArthritisRombauts et al. (2000) • Zygapophyseal ankylosis Septic Arthritis
Van Offel et al. (1995) • Sacroiliac ankylosis, zygapophysealankylosis (intra-articular) erosive arthritis
Ochronosisankylosis (intra articular), erosive arthritiswith bone formation on hand and feet
Canhão et al. (1996) • Bambu spine, sacroliac andzygapophyseal ankylosis, hand and feet
Ochronosisyg p p y y ,
arthritis
Fiske et al. (1995) • Bambu spine, sacroliac ankylosis Paralisys secundary to amyotrophic( ) p y y y y plateral sclerosis
Additionally Calcium pyrophosphate deposition disease (CPDD) is clinically evoked as a differential diagnosis

Results & DiscussionSpondylarthropathies
Sample by the method of Rogers & colN= 20Mean age at death= 75 years old
Entesopathy % (N=20)
Mean age at death= 75 years old
Entesopathy % (N=20)
Iliac crests 58%
Ischial tuberosities 44%
Calcaneus [Achilles tendon and plantar fascia] 44%
Patella 42 %
Tibia [anterior tuberosity] 21%
Femur [greater and lesser throchanters] 42%
Humeral head 47%Humeral head 47%
Humeral lateral and medial epicondyles 15%
Ulna [olecranon] 35%

Results & DiscussionSpondylarthropathies
ISCMB. Calcaneus
ISCMB. Iliac crest
ISCMB. Calcaneus

Results & DiscussionSpondylarthropathies
ISCMB. UlnaISCMB.Humeral head

Cl l D
Results & DiscussionSpondylarthropathies
Clinical Data
• Reduced assessment of occurrence of peripheral entheses - under diagnosed
• Generally co-exists with other clinical manifestations of SpA, but isolated occurrence was reported by D’Agostino & Olivieri (2006): 14% of individuals with juvenile onset disease and 9% reported by D Agostino & Olivieri (2006): 14% of individuals with juvenile-onset disease and 9% with late-onset
Peripheral Enthesitis
• Peripheral enthesitis: observed in all forms of SpA and all phases (D’Agostino & Olivieri, 2006)
D’Agostino & Olivieri (2006)
Turan et al. (2009)
Ankylosing spondylitis (AS) 25-58% 78.3%• Entesopathy of the calcaneus:
Reactive arthritis (ReA) 33–58% 93%
Psoriatic arthritis (PsA) 20% -
one of the most frequent and early sign
Enteropathic arthritis (EA) 10% -
PsA+ EA+ USpA 82.4%

ConclusionSpondylarthropathies
Even if SpA diagnosis is problematic - methodological controversy
E h f h i d l i Each of the mentioned lesions
• Sacroiliac or zygapophyseal joints: erosion/ new bone formation or intra-
articular ankylosisRelevant Signs
articular ankylosis
• Syndesmophytes To be considered on the
evaluation of entesophytes• Presence of paramarginal (paravertebral) ossifications
• Erosive lesions with bone proliferation or intra-articular ankylosis on the
evaluation of entesophytes
as activity marker
peripheral joints

ConclusionSpondylarthropathies
• Methodological impact on the assessment of SpA : limits population comparison
without taking into consideration the diagnostic criteria applied
• Further research on the variability of the morphology of lesion is required
• Improvement of differential diagnosis
• Enthesitis is key feature of SpA: although the more distinctive are the ones of the
axial skeletonaxial skeleton
• The recognition of the SpA is important on the analysis of markers of activityThe recognition of the SpA is important on the analysis of markers of activity
ConclusionSpondylarthropathies
Acknowledgments
Fundação para a Ciência e a Tecnologia
Museu Bocageuseu ocage
CIAS
Eugénia Cunhag
Don Ortner
Vítor Matos
Ana Luísa Santos
Cláudia Umbelino


















