
Ensuring Remote Telemetry Monitoring Patient Safety · Remote Telemetry Monitoring ... – Brain...
63
Ensuring Remote Telemetry Monitoring Patient Safety IIE/Society for Health Systems February 2006 Terry Dunn Health Alliance of Greater Cincinnati
Transcript of Ensuring Remote Telemetry Monitoring Patient Safety · Remote Telemetry Monitoring ... – Brain...
Ensuring Remote Telemetry Monitoring Patient Safety
IIE/Society for Health Systems
February 2006
Terry Dunn
Health Alliance of Greater Cincinnati
Feb 2006
Session Objectives
You will learn...
1. How to create a specific and meaningful definition of safety.
2. How to build an FMEA consistent with JCAHO requirements.
3. How to measure performance against the safety definition.
4. How to select and pilot safety solutions.
5. How to include, promote, and educate stakeholders to ensure buy-in.
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Background
• Numerous studies prove: respiratory & cardiac failure is almost always presaged by observable physiologic changes 6-8 hours before the event, which can be detected for most patients by monitoring of heart rate & O2 saturation levels.
• Effective interventions for cardiac and respiratory failures must begin within 3-5 minutes to prevent long-term negative outcomes:– Death
– Brain damage
– Other systemic injury
• House-wide telemetry eases bed assignments
• Centralized (vs. unit-based) model less costly
Feb 2006
“The Right Thing to Do”
• National Patient Safety Goals (2004) – Improve effectiveness of patient care alarms
• Assure alarm systems that monitor patients are regularly tested and adjusted, if needed, to prevent any problems.
• Alarms are turned on with the correct settings and are loud enough to be heard within the patient unit.
• IHI 100,000 Lives Campaign– Rapid Response Teams – monitoring a signal when
RR appropriate!
Feb 2006
The Problem at University
• Vendor’s alpha site for centralized system—no up-front expectation of potential failures & no support to identify benchmarks
• Nurses at the hospital were often not responding to alerts AT ALL, let alone in a timely manner…– Patient deaths had occurred (though fortunately not recently!)
– Near misses were occurring regularly…
• Because of preventable system failures, some clinical events were not being detected
• Repeated examination of the problem had surfaced numerous root causes, but without significant, widespread, or lasting impact
• Project chartered under recommendations of the Board to fulfill JCAHO requirements
Feb 2006
Defining “Safety”
• Who?
• What?
• When?
• Where?
• SO WHAT?
• Why?
• What can we do about it?
Tips for Success:• Use brainstorming & fishbone
diagrams to build consensus
• Good “starters”:• What does “safe” look like?• What has to happen to
ensure safety?
• Watch out for hidden agendas!!
• Keep the focus on safety, NOT on feelings & grudges…
Tips for Success:• Use brainstorming & fishbone
diagrams to build consensus
• Good “starters”:• What does “safe” look like?• What has to happen to
ensure safety?
• Watch out for hidden agendas!!
• Keep the focus on safety, NOT on feelings & grudges…
Feb 2006
Think Systems!
Technology
Hand-offs
Communication
Processes
Shared Understanding& CommonVision
Feb 2006
Project Title:TUH CMU - Improving Safety of Centrally
Monitored Telemetry Patients
Business Case:
Objectives/Goal Statements:
Business Y: Scope: All TUH nursing units supported by CMU.
Champion: R. Fischer Assistant CNO
Process Owner: K. Ghaffari Director Pt Care Services
Finance Rep: Define 20-Feb-05 4-Feb-05 11-Feb-05 Complete
Black Belt: T. Dunn Measure 15-Mar-05 7-Feb-05 1-Apr-05 In process
Analyze 15-Apr-05 30-Apr-05
Improve 1-Jun-05 1-Jun-05
Control 15-Jul-05 15-Jul-05
Project Team: K. Bally, A. Crawford, K. Ghaffari, J. Goetz, F. McNeil
Problem: 85-90% of CMU alerts receive either no
acknowledgement from the nursing unit or response
times exceed current policy specifications.
K. Ghaffari Director Pt Care Services, A. Crawford
Clinical Mgr CMU/6S, S. Hoell Clin Mgr 6NW, W. Lowe
Clin Mgr 9CCP
Steering Team:
Timeline:
Orig Plan
End
Actual
Start
Current
End
2. Reduce acknowledgement defect rate by 70%. 1. Reduce technical alerts by 70%.
Timely & appropriate intervention to cardiac events is strongly
correlated to successful outcomes. Response to early indications can even prevent cardiac arrests. To optimize the
safety of patients monitored by CMU, we must ensure (1) the
right patients are (2) monitored using individualized
parameters (3) by a reliable system to whose alerts we respond in a (4) timely and (5) clinically appropriate manner.
Safety starts with a focused assessment, properly maintaining the equipment, and effectively communicating alerts and
responses.
Status
Volume of codes (& volume of code-related
deaths)
By June 15, 2005:
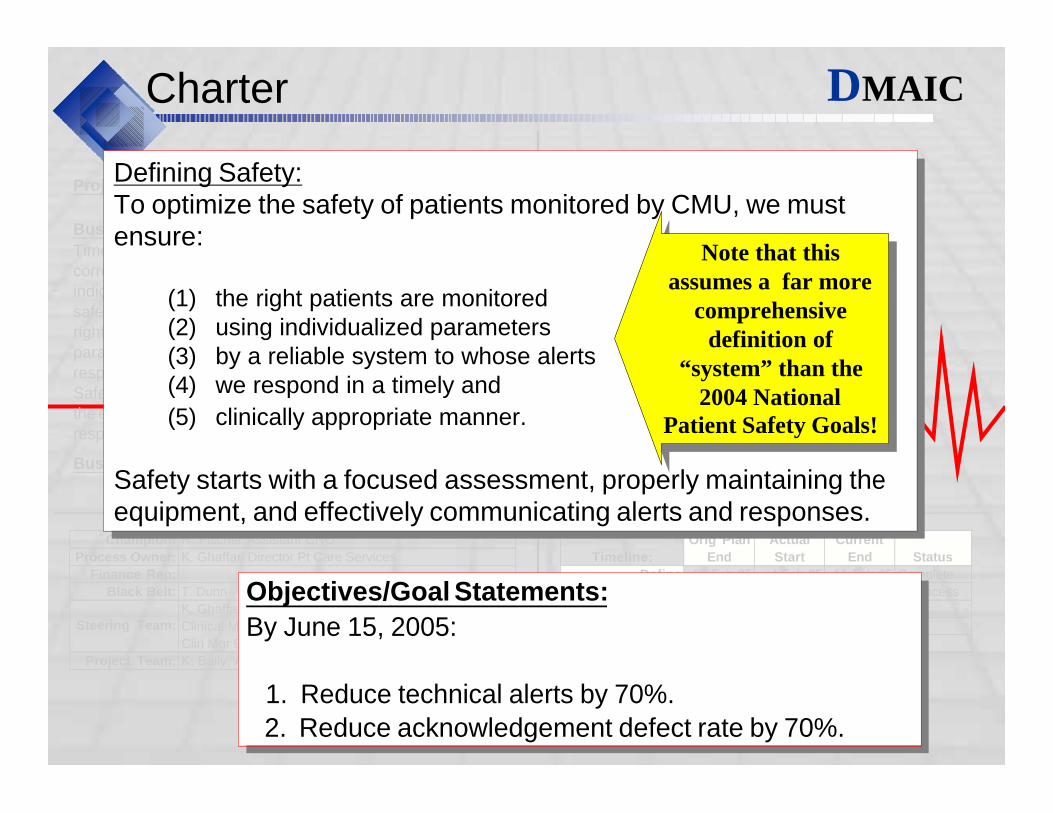
Charter DMAIC
Defining Safety:To optimize the safety of patients monitored by CMU, we must ensure:
(1) the right patients are monitored (2) using individualized parameters (3) by a reliable system to whose alerts (4) we respond in a timely and
(5) clinically appropriate manner.
Safety starts with a focused assessment, properly maintaining the equipment, and effectively communicating alerts and responses.
Defining Safety:To optimize the safety of patients monitored by CMU, we must ensure:
(1) the right patients are monitored (2) using individualized parameters (3) by a reliable system to whose alerts (4) we respond in a timely and
(5) clinically appropriate manner.
Safety starts with a focused assessment, properly maintaining the equipment, and effectively communicating alerts and responses.
Objectives/Goal Statements:
2. Reduce acknowledgement defect rate by 70%.
1. Reduce technical alerts by 70%.
By June 15, 2005:
Note that this assumes a far more
comprehensive definition of
“system” than the 2004 National
Patient Safety Goals!
Note that this assumes a far more
comprehensive definition of
“system” than the 2004 National
Patient Safety Goals!
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
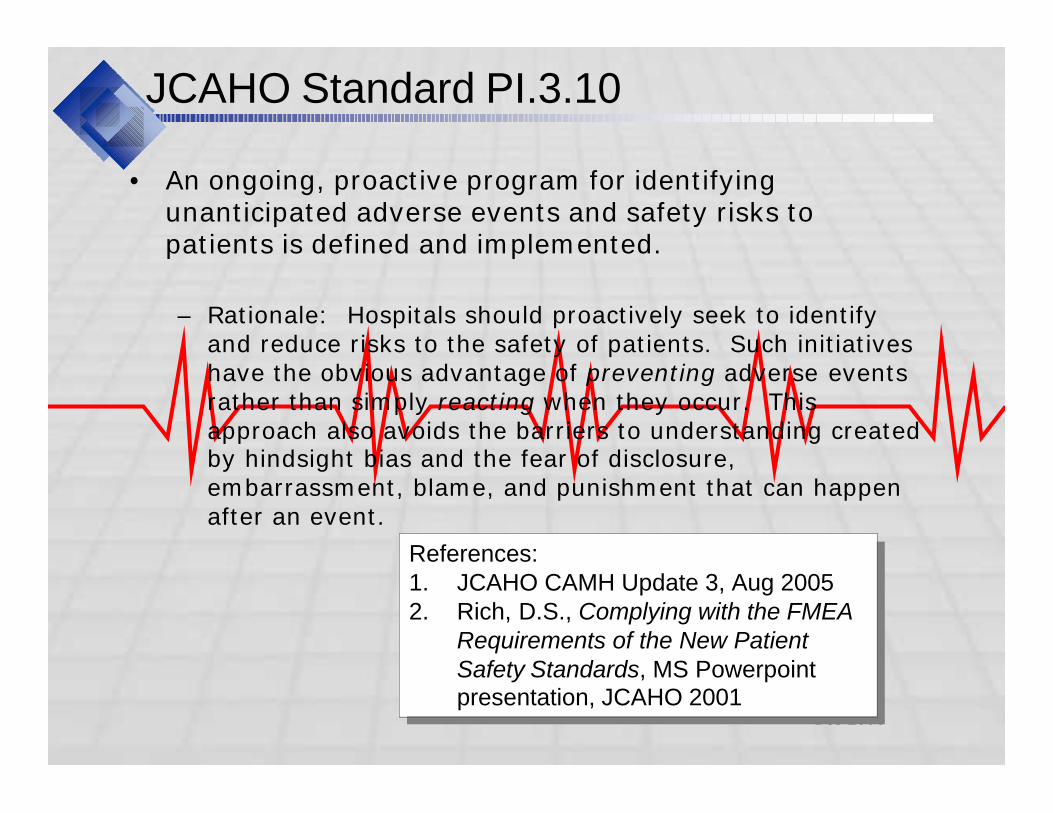
JCAHO Standard PI.3.10
• An ongoing, proactive program for identifying unanticipated adverse events and safety risks to patients is defined and implemented.
– Rationale: Hospitals should proactively seek to identify and reduce risks to the safety of patients. Such initiatives have the obvious advantage of preventing adverse events rather than simply reacting when they occur. This approach also avoids the barriers to understanding created by hindsight bias and the fear of disclosure, embarrassment, blame, and punishment that can happen after an event.
References: 1. JCAHO CAMH Update 3, Aug 20052. Rich, D.S., Complying with the FMEA
Requirements of the New Patient Safety Standards, MS Powerpoint presentation, JCAHO 2001
References: 1. JCAHO CAMH Update 3, Aug 20052. Rich, D.S., Complying with the FMEA
Requirements of the New Patient Safety Standards, MS Powerpoint presentation, JCAHO 2001
Feb 2006
JCAHO Standard PI.3.10
• Elements of Performance:
1. Select a high-risk process to be analyzed• At least one high-risk process is chosen annually—the
choice should be based in part on information published periodically by the Joint Commission about the most frequent sentinel events and risks
2. Describe the chosen process (for example through the use of a flow chart)
3. Identify the ways in which the process could break down or fail to perform its desired function (i.e., what engineers call potential “failure modes”)
4. Identify the possible effects each failure mode could have on patients and the seriousness of those effects
Feb 2006
JCAHO Standard PI.3.10
• Elements of Performance: (continued)
5. Prioritize the potential failure modes
6. Determine why the potential failure modes could occur
7. Redesign the process and/or underlying systems to minimize the risk of the effects on patients
8. Test and implement the redesigned process
9. Monitor the effectiveness of the redesigned process
Comments: 1. Note that it never says “FMEA”, but it describes the process!2. When you speak to JCAHO representatives, they can’t offer
any examples other than FMEA’s!
Comments: 1. Note that it never says “FMEA”, but it describes the process!2. When you speak to JCAHO representatives, they can’t offer
any examples other than FMEA’s!
Feb 2006
High Risk Processes
• Processes that involve risks or may result in sentinel events– Medication use
– Operative and other procedures
– Use of blood and blood components
– Restraint use
– Seclusion, when a part of care
– Care/services provided to high-risk populations
– Resuscitation
Feb 2006
Constructing an FMEA Table
1. Flow-chart the process
2. Identify actual AND potential failure points in the process
3. Document each failure point
• What failure can/does occur (“mode”)
• Each separate effect resulting from the failure (“effects”)
4. Evaluate each mode/effect pair
• S = Severity of effect
• F = Approximate frequency
• D = Ability of system to prevent, control, or detect the failure
5. Calculate Risk Priority Number: RPN = S x F x D
Feb 2006
Process Flows
10/10/2005 1
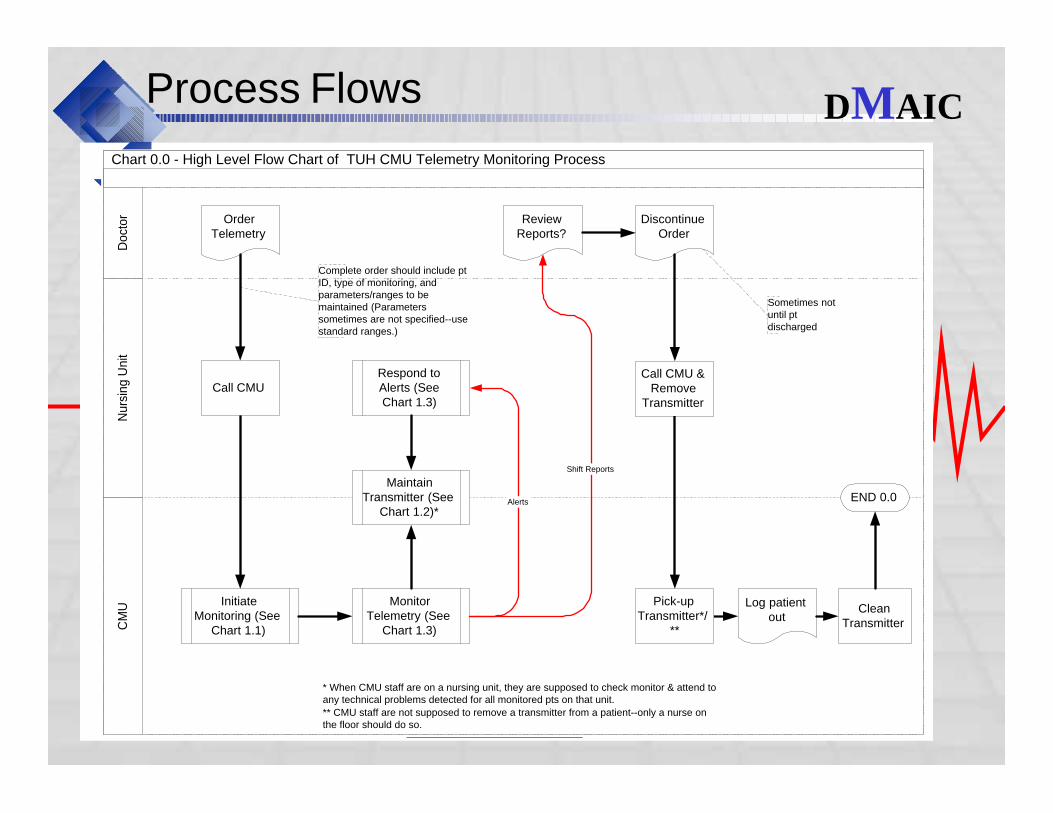
Chart 0.0 - High Level Flow Chart of TUH CMU Telemetry Monitoring Process
Nu
rsin
g U
nit
CM
UD
oct
or
MonitorTelemetry (See
Chart 1.3)
MaintainTransmitter (See
Chart 1.2)*
Respond toAlerts (SeeChart 1.3)
InitiateMonitoring (See
Chart 1.1)
OrderTelemetry
DiscontinueOrder
ReviewReports?
END 0.0
Shift Reports
Alerts
Call CMUCall CMU &
RemoveTransmitter
Pick-upTransmitter*/
**
CleanTransmitter
Complete order should include ptID, type of monitoring, andparameters/ranges to bemaintained (Parameterssometimes are not specified--usestandard ranges.)
* When CMU staff are on a nursing unit, they are supposed to check monitor & attend toany technical problems detected for all monitored pts on that unit.
Sometimes notuntil ptdischarged
** CMU staff are not supposed to remove a transmitter from a patient--only a nurse onthe floor should do so.
Log patientout
DMAIC
Feb 2006
Process Flows
9/21/2005 2
Chart 1.1 - CMU Initiates Telemetry Monitoring
CM
UN
urs
ing
Un
itD
oct
or
Receive Callfrom Nursing
Unit
Runneravailable?
Log pt oncharge list &admit board
Runner selects& programs/
tests transmitter
Enter pt info & parametersinto monitor "sector"
assigned to transmitter #
Runner takes transmitterto patient & places leads
Inform nursing unit ofexpected delay &/or
request they come to pickup transmitter
Runneravailable?
Pull & program/test transmitter
Set transmitteraside for pick-up
END 1.1
No
Yes
No
YesParallel whenrunneravailable
Run admission strip(once placed) &
interpret
9/21/2005 1
Chart 0.0 - High Level Flow Chart of TUH CMU Telemetry Monitoring Process
Nurs
ing U
nit
CM
UD
oct
or
MonitorTelemetry (See
Chart 1.3)
MaintainTransmitter (See
Chart 1.2)*
Respond toAlerts (SeeChart 1.3)
InitiateMonitoring (See
Chart 1.1)
OrderTelemetry
DiscontinueOrder
ReviewReports?
END 0.0
Shift Reports
Alerts
Call CMUCall CMU &
RemoveTransmitter
Pick-upTransmitter*/
**
CleanTransmitter
Complete order should include ptID, type of monitoring, andparameters/ranges to bemaintained (Parameterssometimes are not specified--usestandard ranges.)
* When CMU staff are on a nursing unit, they are supposed to check monitor & attend toany technical problems detected for all monitored pts on that unit.
Sometimes notuntil ptdischarged
** CMU staff are not supposed to remove a transmitter from a patient--only a nurse onthe floor should do so.
Log patientout
9/21/2005 3
Chart 1.2 - CMU Telemetry Transmitter Maintenance
CM
UN
urs
ing U
nit
Doct
or
Pt onMonitoring
Recordcharges
Set up dailylog Enter
charges
Remove & repositiontransmitter when ptoff unit (see chart
1.2.1)
Replace batteriesq24 (q8 if SpO2
monitoring)
Check &replace leads
q24
Troubleshootplacement, batteries,
leads, etc. PRN
Pt onMonitoring
3 days?Stamp MD notes to
ask re: discontinuatin
N
Y
Run strips q8Round q8 tomount strips
in charts
9/21/2005 4
Chart 1.2.1 - CMU Telemetry Transmitter Maintenance - Patient Leaves/Returns to Unit
CM
UN
urs
ing
Un
itD
oct
or
Pt to leave unit fortest/procedure
Dialysis?Transporter
arrives
Transporterasks nurseto removetransmitter
Nurse callsCMU &
removestransmitter
Pt offunit
Pt off unit
Transporterarrives
Transporternotifiesnurse toreplace
transmitter
Nurserepositionstransmitter
Routine monitoringresumes upon
reception of signal
Place "pt off unit"indicator on
monitor sector
Nurse should checkleads & batteries forreplacement
Y
N
9/21/2005 5
Chart 1.3 - Monitor Telemetry / Respond to Alerts
CM
UN
urs
ing
Un
itD
oct
or
Pt onMonitoring
Systemdetects
abnormalcondition
CMU techinterprets
alarm
Speed-dialredphone
on nsg unit
Lethalrhythm?
Enter textmsg & pageRN of record
Logincident
Timelyresponse?
Receivealarm
Assess ptneed
Acknowledgealarm
Log acknow-ledgement
Resolvealarm/need
Repeat/Escalate alert
Continue
Y
N
N
Y
DMAIC
Feb 2006
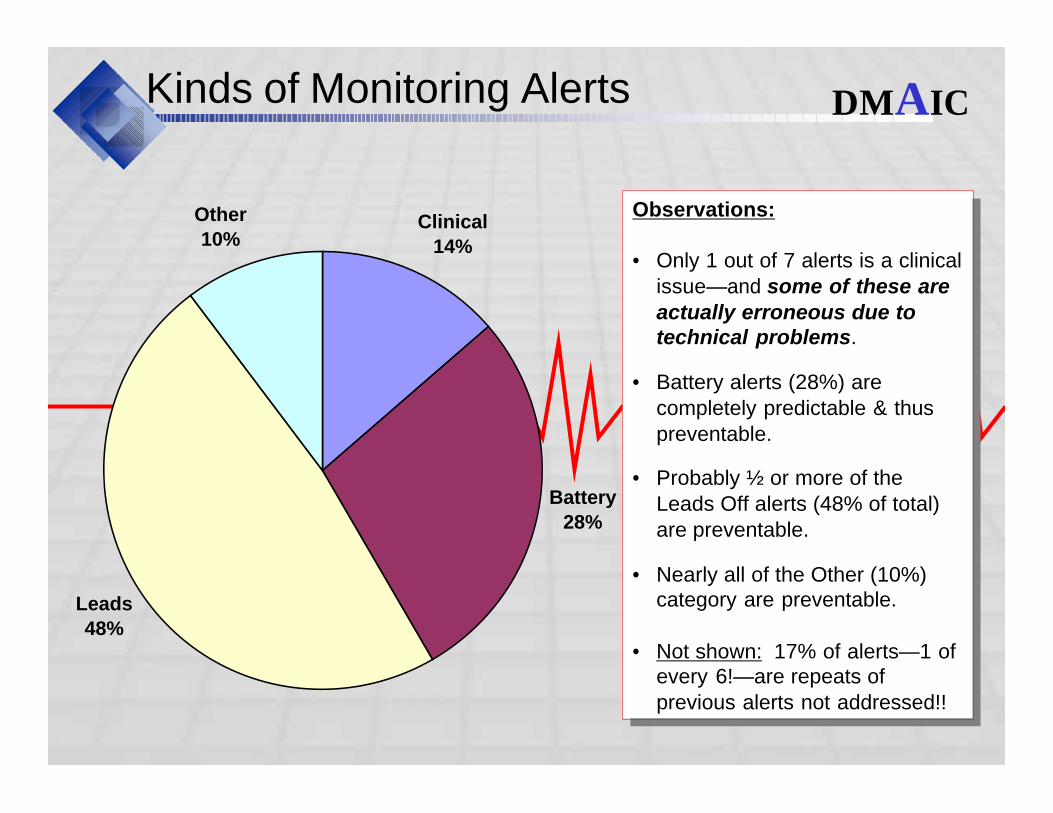
Kinds of Monitoring AlertsDistribution of Alerts - Before
Clinical
14%
Battery
28%
Leads
48%
Other
10%
DMAIC
Observations:
• Only 1 out of 7 alerts is a clinical issue—and some of these are actually erroneous due to technical problems.
• Battery alerts (28%) are completely predictable & thus preventable.
• Probably ½ or more of the Leads Off alerts (48% of total) are preventable.
• Nearly all of the Other (10%) category are preventable.
• Not shown: 17% of alerts—1 of every 6!—are repeats of previous alerts not addressed!!
Observations:
• Only 1 out of 7 alerts is a clinical issue—and some of these are actually erroneous due to technical problems.
• Battery alerts (28%) are completely predictable & thus preventable.
• Probably ½ or more of the Leads Off alerts (48% of total) are preventable.
• Nearly all of the Other (10%) category are preventable.
• Not shown: 17% of alerts—1 of every 6!—are repeats of previous alerts not addressed!!
Feb 2006
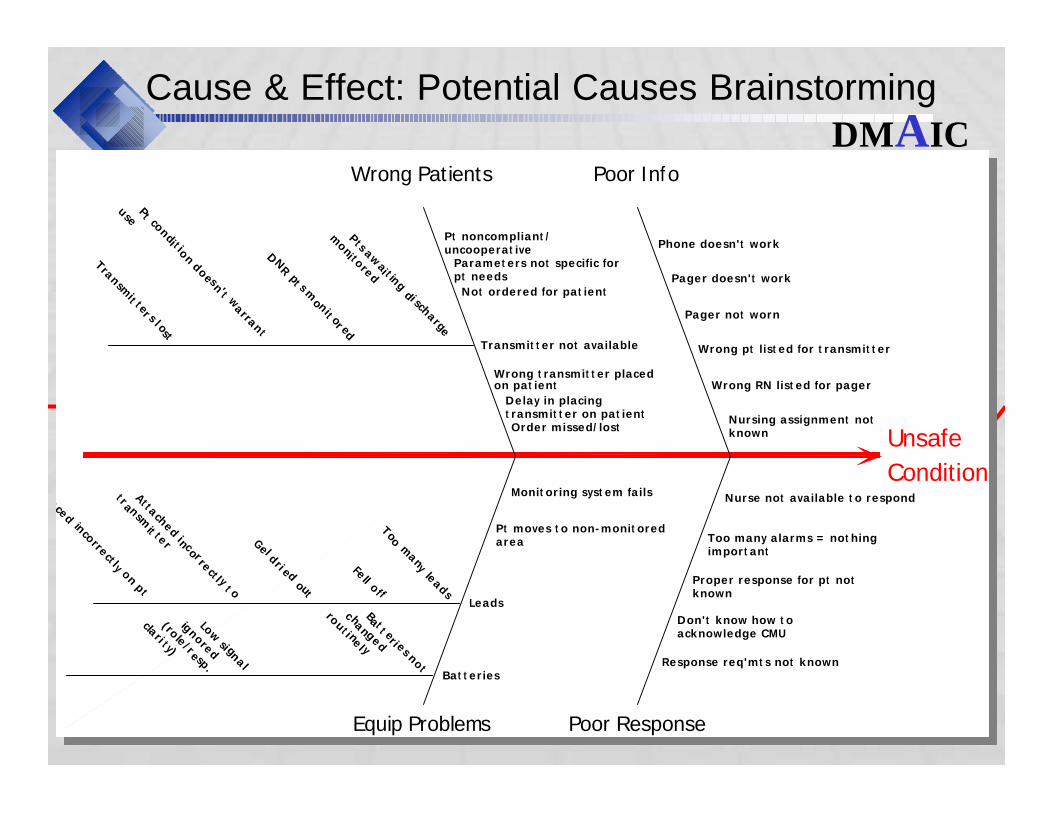
Cause & Effect: Potential Causes Brainstorming
Unsafe
Condition
Equip Problems
Wrong Patients
Poor Response
Poor Info
Nursing assignment notknown
Wrong RN list ed for pager
Wrong pt list ed for t ransmit t er
Pager not worn
Pager doesn't work
Phone doesn't work
Nurse not available t o respond
Too many alarms = not hingimport ant
Proper response for pt notknown
Don't know how t oacknowledge CMU
Response req'mt s not known
Order missed/lost
Delay in placingt ransmit t er on pat ient
Wrong t ransmit t er placedon pat ient
Transmit t er not available
Not ordered for pat ient
Paramet ers not specific forpt needs
Pt noncompliant /uncooperat ive
Monit oring syst em fails
Pt moves t o non-monit oredarea
Leads
Bat t eries
Pts a
wai t in
g di sch
arg
e
moni to
red
DNR p
t s mon
it or e
d
Pt co
ndi t io
n d
oes
n't warra
nt
use
Tra
nsm
it ter s l o
st
Bat
t eri e
s no
t
c hang
ed
rou
t i nel y
Low
si gnal
ignore
d
(role
/resp
.
clari t y)
Too m
any le
ads
Fell o
f f
Gel d
ri ed ou
t
At ta
ched inc
orre
ct l y t o
t ran
smit te
r
Pla
ced in
corre
ct ly on p
t
What could reduce monitored patient safety?
Unsafe
Condition
Equip Problems
Wrong Patients
Poor Response
Poor Info
Nursing assignment notknown
Wrong RN list ed for pager
Wrong pt list ed for t ransmit t er
Pager not worn
Pager doesn't work
Phone doesn't work
Nurse not available t o respond
Too many alarms = not hingimport ant
Proper response for pt notknown
Don't know how t oacknowledge CMU
Response req'mt s not known
Order missed/lost
Delay in placingt ransmit t er on pat ient
Wrong t ransmit t er placedon pat ient
Transmit t er not available
Not ordered for pat ient
Paramet ers not specific forpt needs
Pt noncompliant /uncooperat ive
Monit oring syst em fails
Pt moves t o non-monit oredarea
Leads
Bat t eries
Pts a
wai t in
g di sch
arg
e
moni to
red
DNR p
t s mon
it or e
d
Pt co
ndi t io
n d
oes
n't warra
nt
use
Tra
nsm
it ter s l o
st
Bat
t eri e
s no
t
c hang
ed
rou
t i nel y
Low
si gnal
ignore
d
(role
/resp
.
clari t y)
Too m
any le
ads
Fell o
f f
Gel d
ri ed ou
t
At ta
ched inc
orre
ct l y t o
t ran
smit te
r
Pla
ced in
corre
ct ly on p
t
What could reduce monitored patient safety?DMAIC
Feb 2006
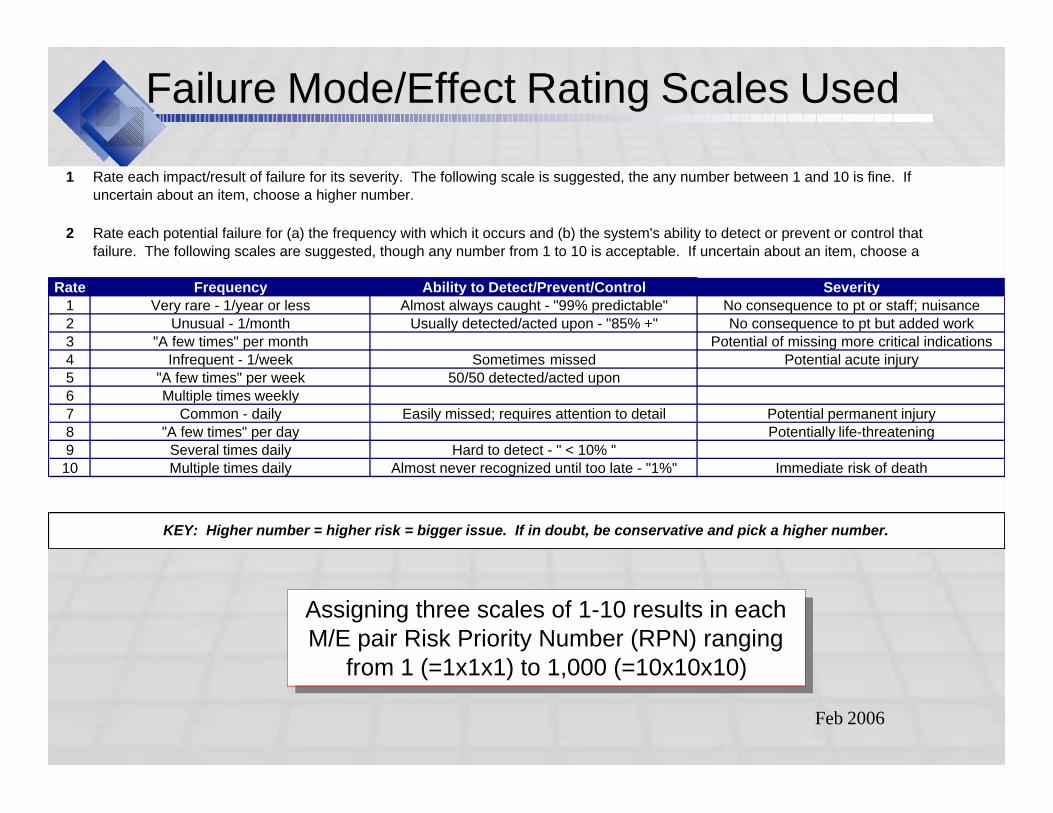
Failure Mode/Effect Rating Scales Used
1
2
Rate Frequency Ability to Detect/Prevent/Control1 Very rare - 1/year or less Almost always caught - "99% predictable"2 Unusual - 1/month Usually detected/acted upon - "85% +"3 "A few times" per month4 Infrequent - 1/week Sometimes missed5 "A few times" per week 50/50 detected/acted upon6 Multiple times weekly7 Common - daily Easily missed; requires attention to detail8 "A few times" per day9 Several times daily Hard to detect - " < 10% "10 Multiple times daily Almost never recognized until too late - "1%"
Rate each impact/result of failure for its severity. The following scale is suggested, the any number between 1 and 10 is fine. If uncertain about an item, choose a higher number.
Rate each potential failure for (a) the frequency with which it occurs and (b) the system's ability to detect or prevent or control that failure. The following scales are suggested, though any number from 1 to 10 is acceptable. If uncertain about an item, choose a
Potential permanent injury
KEY: Higher number = higher risk = bigger issue. If in doubt, be conservative and pick a higher number.
Potentially life-threatening
Immediate risk of death
SeverityNo consequence to pt or staff; nuisanceNo consequence to pt but added work
Potential of missing more critical indicationsPotential acute injury
Assigning three scales of 1-10 results in each M/E pair Risk Priority Number (RPN) ranging
from 1 (=1x1x1) to 1,000 (=10x10x10)
Assigning three scales of 1-10 results in each M/E pair Risk Priority Number (RPN) ranging
from 1 (=1x1x1) to 1,000 (=10x10x10)
Feb 2006
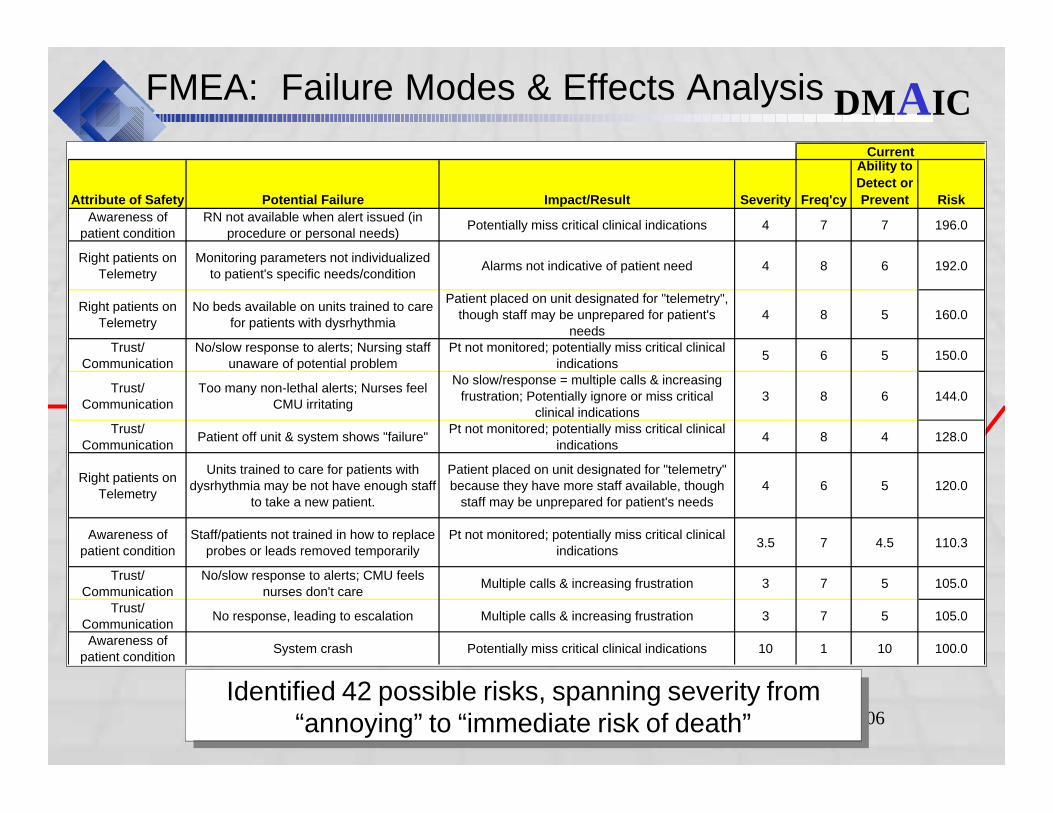
FMEA: Failure Modes & Effects Analysis
Attribute of Safety Potential Failure Impact/Result Severity Freq'cy
Ability to
Detect or
Prevent Risk
Awareness of patient condition
RN not available when alert issued (in procedure or personal needs)
Potentially miss critical clinical indications 4 7 7 196.0
Right patients on Telemetry
Monitoring parameters not individualized to patient's specific needs/condition
Alarms not indicative of patient need 4 8 6 192.0
Right patients on Telemetry
No beds available on units trained to care for patients with dysrhythmia
Patient placed on unit designated for "telemetry", though staff may be unprepared for patient's
needs4 8 5 160.0
Trust/ Communication
No/slow response to alerts; Nursing staff unaware of potential problem
Pt not monitored; potentially miss critical clinical indications
5 6 5 150.0
Trust/ Communication
Too many non-lethal alerts; Nurses feel CMU irritating
No slow/response = multiple calls & increasing frustration; Potentially ignore or miss critical
clinical indications3 8 6 144.0
Trust/ Communication
Patient off unit & system shows "failure"Pt not monitored; potentially miss critical clinical
indications4 8 4 128.0
Right patients on Telemetry
Units trained to care for patients with dysrhythmia may be not have enough staff
to take a new patient.
Patient placed on unit designated for "telemetry" because they have more staff available, though
staff may be unprepared for patient's needs4 6 5 120.0
Awareness of patient condition
Staff/patients not trained in how to replace probes or leads removed temporarily
Pt not monitored; potentially miss critical clinical indications
3.5 7 4.5 110.3
Trust/ Communication
No/slow response to alerts; CMU feels nurses don't care
Multiple calls & increasing frustration 3 7 5 105.0
Trust/ Communication
No response, leading to escalation Multiple calls & increasing frustration 3 7 5 105.0
Awareness of patient condition
System crash Potentially miss critical clinical indications 10 1 10 100.0
Current
Identified 42 possible risks, spanning severity from “annoying” to “immediate risk of death”
Identified 42 possible risks, spanning severity from “annoying” to “immediate risk of death”
DMAIC
Feb 2006
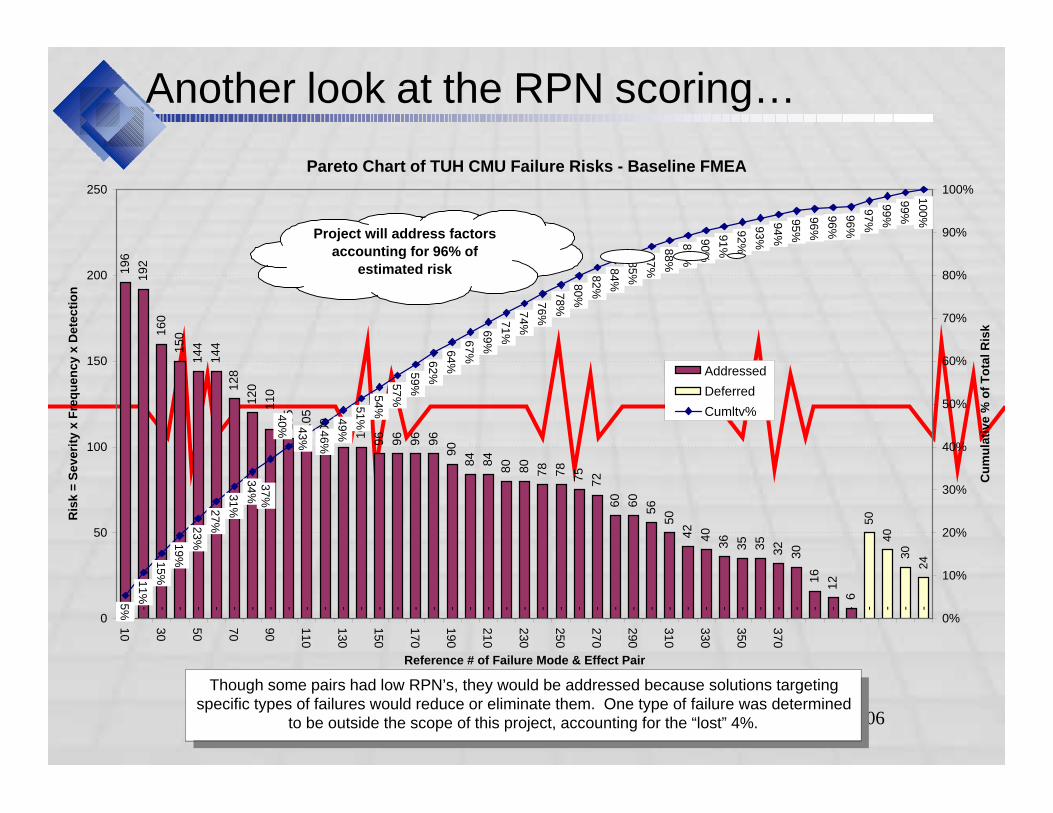
Another look at the RPN scoring…
Pareto Chart of TUH CMU Failure Risks - Baseline FMEA
196
192
160
150
144
144
128
120
105
105
100
100
100
96
96
96
96
90
84
84
80
80
78
78
75
72
60
60
56
50
42
40
36
35
35
32
30
16
12
6
- - - -- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
50
40
30
24
110
5%
11
%
15
%
19
%
23
%
27
%
31
%
34
%
46
%
49
%
51
%
54
%
57
%
59
%
62
%
64
%
67
%
69
%
71
%
74
%
76
%
78
%
80
%
82
%
84
%
85
%
87
%
88
%
89
%
90
%
91
%
92
%
93
%
94
%
95
%
96
%
96
%
96
%
97
%
99
%
99
%
10
0%
43
%
40
%
37
%
0
50
100
150
200
250
10
30
50
70
90
110
130
150
170
190
210
230
250
270
290
310
330
350
370
Reference # of Failure Mode & Effect Pair
Ris
k =
Severi
ty x
Fre
qu
en
cy x
Dete
cti
on
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cu
mu
lati
ve %
of
To
tal R
isk
Addressed
Deferred
Cumltv%
Project will address factors
accounting for 96% of
estimated risk
Though some pairs had low RPN’s, they would be addressed because solutions targeting specific types of failures would reduce or eliminate them. One type of failure was determined
to be outside the scope of this project, accounting for the “lost” 4%.
Though some pairs had low RPN’s, they would be addressed because solutions targeting specific types of failures would reduce or eliminate them. One type of failure was determined
to be outside the scope of this project, accounting for the “lost” 4%.
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Metrics
• Critical to Quality (CTQ) Project Requirements
– 100% detection of unsafe events
– High confidence in validity of alerts
– Timely response to alerts
– No rework
• Operational Metrics Defined:
– Business Metrics• Volume of codes
• Volume of deaths related to codes
– Process Metrics• Technical alerts per monitored patient day
• Acknowledgement defects (i.e., no or slow responses) as % of alerts
– Financial Metrics• No significant cost or revenue changes anticipated
– Consequential Metrics• None identified
DMAIC
Feb 2006
Original Baseline
• Nearly 90% of telemetry alerts are not acknowledged in a timely manner, as outlined by hospital policy– Over 1/2 of alerts receive no acknowledgement *
– Over 30% receive acknowledgements outside of specified times
– Acknowledgement of lethal rhythms only slightly lower defect rate than other: 84% defective vs. 91%
• 10 telemetry transmitters lost (@ $2,500each)
Can we be sure a patient is safe if we’re not sure anyone checks & resolves a detected problem?
Can we be sure a patient is safe if we’re not sure anyone checks & resolves a detected problem?
* This is not saying “patient need not addressed”. Rather, CMU had no feedback from the nurse.
DMAIC
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Conclusions: Key Drivers of Defects
• “Noise” overload: Too many non-critical pages & possible misuse of red phones
• Knowledge deficits: – Transmitters are tied to specific units, programmed for
specific patients
– Acknowledging alerts much easier than most realize!
• Missing/broken processes:– Transmitter maintenance
– Return of transmitters to CMU at discontinuation
– Transport of monitored patients
– Back-up coverage when nurse temporarily not available
– Back-up coverage for system failure
– Incomplete data
– Communication system failure
• Incomplete/unclear orders for telemetry
DMAIC
Feb 2006
Solutions
Solutions target 3 separate groups:
• CMU
• Physicians
• Nursing Unit Staff
DMAIC
Feb 2006
Reducing measurement error
• Analysis of log data revealed incomplete recording of alerts & times
• Appeared defects might have been overstated…
• …but retesting suggested the severity of the problem was actually underestimated!!
• New checklist-based logs implemented to simplify recording & summarization/analysis
DMAIC
Feb 2006
Other CMU Department Changes
• Established on each unit a single location to collect transmitters removed from patients when telemetry discontinued
• Began writing patient name on transmitter pouches, and instituted “double check” procedures to verify new patient set-up
• Developed new orientation & annual competency educational materials for nurses
• Developed departmental procedure for routinely testing red phones
• Discontinuing daily pager tests– Inconsistent use & response
– Duplicates diagnostic analysis available from paging system
DMAIC
Feb 2006
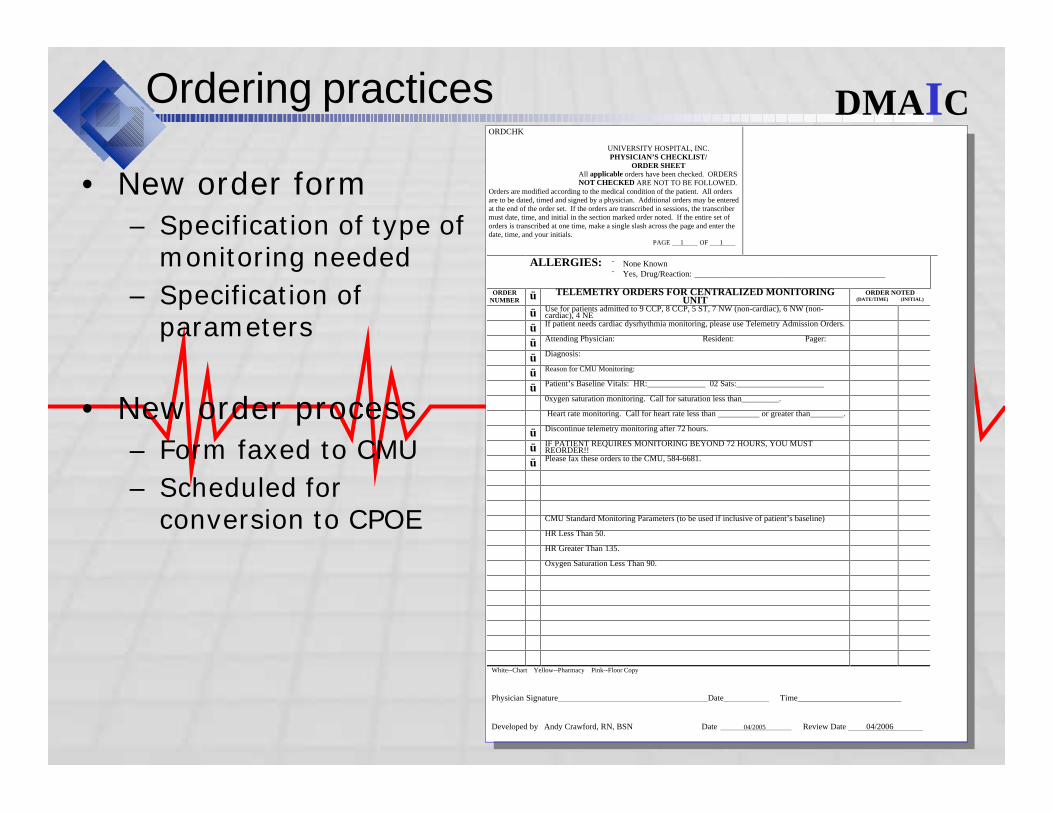
Ordering practices
• New order form– Specification of type of
monitoring needed
– Specification of parameters
• New order process– Form faxed to CMU
– Scheduled for conversion to CPOE
Insert picture of order form here…
ORDCHK
UNIVERSITY HOSPITAL, INC. PHYSICIAN’S CHECKLIST/
ORDER SHEET All applicable orders have been checked. ORDERS NOT CHECKED ARE NOT TO BE FOLLOWED.
Orders are modified according to the medical condition of the patient. All orders are to be dated, timed and signed by a physician. Additional orders may be entered at the end of the order set. If the orders are transcribed in sessions, the transcriber must date, time, and initial in the section marked order noted. If the entire set of orders is transcribed at one time, make a single slash across the page and enter the date, time, and your initials. PAGE 1 OF 1
ALLERGIES: ¨ None Known ¨ Yes, Drug/Reaction: ______________________________________________
ORDER NUMBER ü TELEMETRY ORDERS FOR CENTRALIZED MONITORING
UNIT ORDER NOTED
(DATE/TIME) (INITIAL)
ü Use for patients admitted to 9 CCP, 8 CCP, 5 ST, 7 NW (non-cardiac), 6 NW (non-cardiac), 4 NE
ü If patient needs cardiac dysrhythmia monitoring, please use Telemetry Admission Orders.
ü Attending Physician: Resident: Pager:
ü Diagnosis:
ü Reason for CMU Monitoring:
ü Patient’s Baseline Vitals: HR:______________ 02 Sats:_____________________
0xygen saturation monitoring. Call for saturation less than_________.
Heart rate monitoring. Call for heart rate less than __________ or greater than________.
ü Discontinue telemetry monitoring after 72 hours.
ü IF PATIENT REQUIRES MONITORING BEYOND 72 HOURS, YOU MUST REORDER!!
ü Please fax these orders to the CMU, 584-6681.
CMU Standard Monitoring Parameters (to be used if inclusive of patient’s baseline)
HR Less Than 50.
HR Greater Than 135.
Oxygen Saturation Less Than 90.
White--Chart Yellow--Pharmacy Pink--Floor Copy Physician Signature Date Time_________________________ Developed by Andy Crawford, RN, BSN Date 04/2005 Review Date 04/2006
DMAIC
Feb 2006
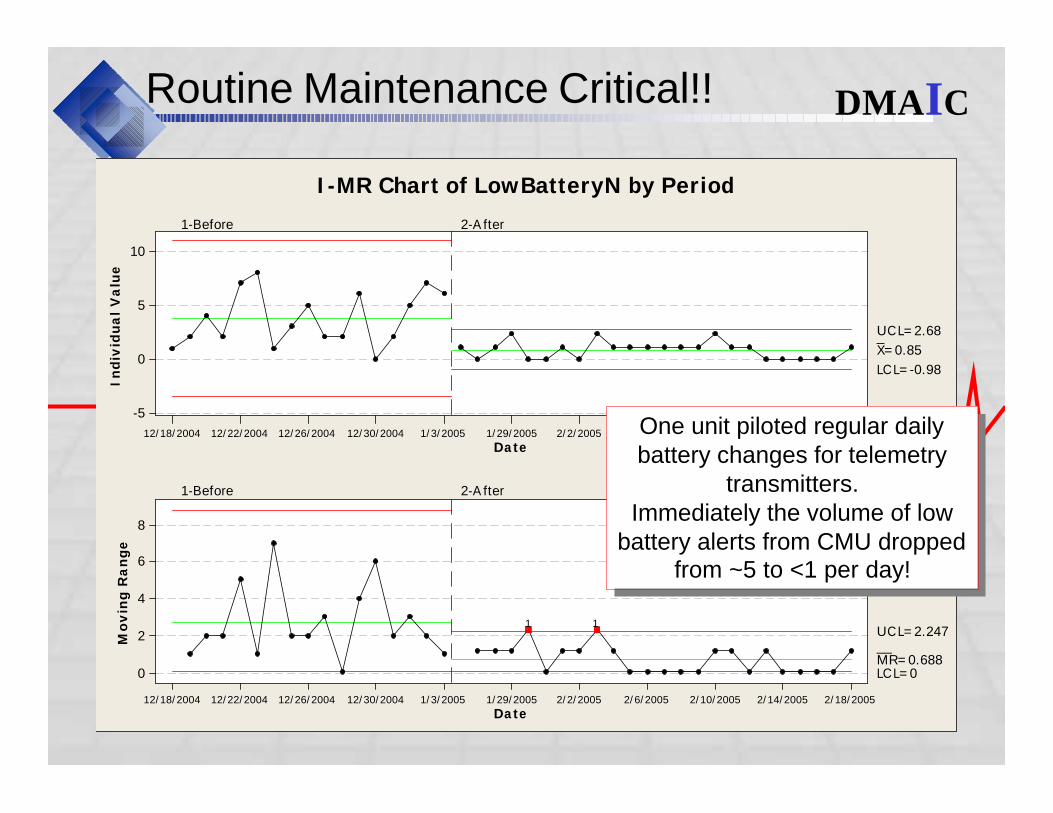
Routine Maintenance Critical!!
Date
In
div
idu
al
Va
lue
2/18/20052/14/20052/10/20052/6/20052/2/20051/29/20051/3/200512/30/200412/26/200412/22/200412/18/2004
10
5
0
-5
_X=0.85
UC L=2.68
LC L=-0.98
1-Before 2-A fter
Date
Mo
vin
g R
an
ge
2/18/20052/14/20052/10/20052/6/20052/2/20051/29/20051/3/200512/30/200412/26/200412/22/200412/18/2004
8
6
4
2
0
__MR=0.688
UC L=2.247
LC L=0
1-Before 2-A fter
11
I-MR Chart of LowBatteryN by Period
DMAIC
One unit piloted regular daily battery changes for telemetry
transmitters.Immediately the volume of low
battery alerts from CMU dropped from ~5 to <1 per day!
One unit piloted regular daily battery changes for telemetry
transmitters.Immediately the volume of low
battery alerts from CMU dropped from ~5 to <1 per day!
Feb 2006
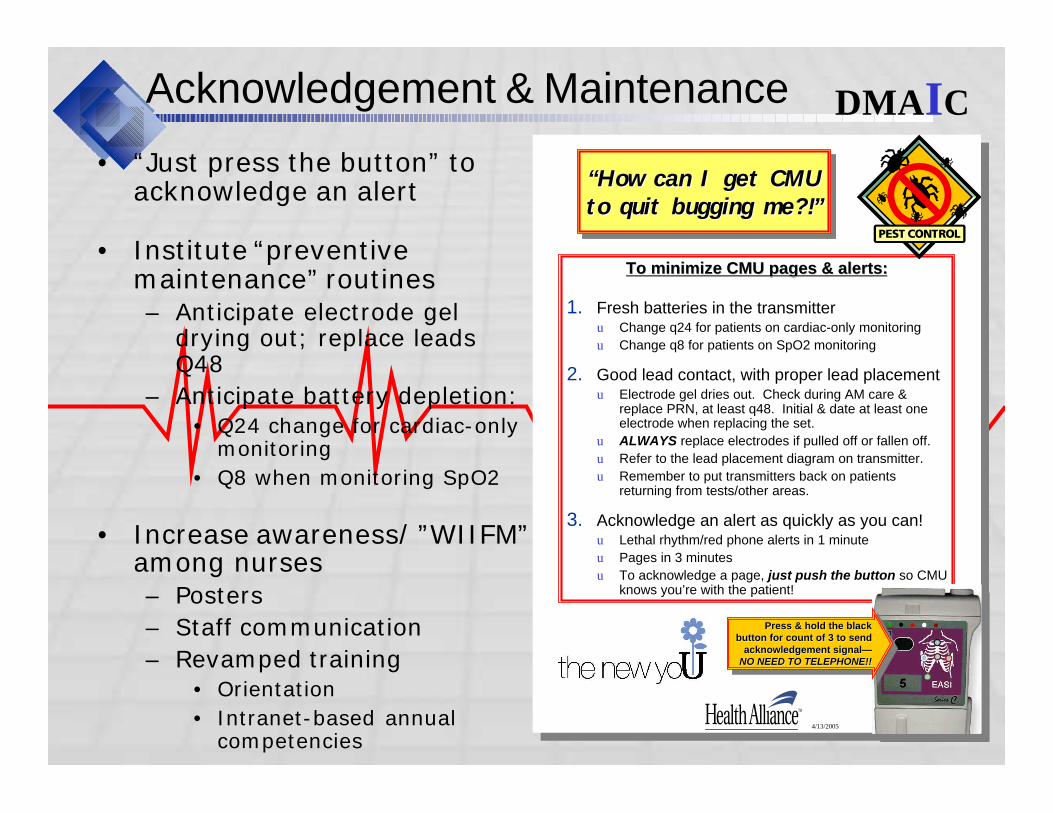
Acknowledgement & Maintenance
4/13/2005 1
“How can I get CMU to quit bugging me?!”
“How can I get CMU “How can I get CMU to quit bugging me?!”to quit bugging me?!”
To minimize CMU pages & alerts:To minimize CMU pages & alerts:
1. Fresh batteries in the transmitteru Change q24 for patients on cardiac-only monitoring
u Change q8 for patients on SpO2 monitoring
2. Good lead contact, with proper lead placementu Electrode gel dries out. Check during AM care &
replace PRN, at least q48. Initial & date at least one electrode when replacing the set.
u ALWAYS replace electrodes if pulled off or fallen off.
u Refer to the lead placement diagram on transmitter.
u Remember to put transmitters back on patients returning from tests/other areas.
3. Acknowledge an alert as quickly as you can!u Lethal rhythm/red phone alerts in 1 minute
u Pages in 3 minutes
u To acknowledge a page, just push the button so CMU knows you’re with the patient!
Press & hold the black button for count of 3 to send
acknowledgement signal—NO NEED TO TELEPHONE!!
Press & hold the black Press & hold the black button for count of 3 to send button for count of 3 to send
acknowledgement signalacknowledgement signal——NO NEED TO TELEPHONE!!NO NEED TO TELEPHONE!!
4/13/2005 1
“How can I get CMU to quit bugging me?!”
“How can I get CMU “How can I get CMU to quit bugging me?!”to quit bugging me?!”
To minimize CMU pages & alerts:To minimize CMU pages & alerts:
1. Fresh batteries in the transmitteru Change q24 for patients on cardiac-only monitoring
u Change q8 for patients on SpO2 monitoring
2. Good lead contact, with proper lead placementu Electrode gel dries out. Check during AM care &
replace PRN, at least q48. Initial & date at least one electrode when replacing the set.
u ALWAYS replace electrodes if pulled off or fallen off.
u Refer to the lead placement diagram on transmitter.
u Remember to put transmitters back on patients returning from tests/other areas.
3. Acknowledge an alert as quickly as you can!u Lethal rhythm/red phone alerts in 1 minute
u Pages in 3 minutes
u To acknowledge a page, just push the button so CMU knows you’re with the patient!
Press & hold the black button for count of 3 to send
acknowledgement signal—NO NEED TO TELEPHONE!!
Press & hold the black Press & hold the black button for count of 3 to send button for count of 3 to send
acknowledgement signalacknowledgement signal——NO NEED TO TELEPHONE!!NO NEED TO TELEPHONE!!
DMAIC
• “Just press the button” to acknowledge an alert
• Institute “preventive maintenance” routines– Anticipate electrode gel
drying out; replace leads Q48
– Anticipate battery depletion:• Q24 change for cardiac-only
monitoring
• Q8 when monitoring SpO2
• Increase awareness/ ”WIIFM” among nurses– Posters
– Staff communication
– Revamped training• Orientation
• Intranet-based annual competencies
Feb 2006
Transport & Back-up
• Drafted new policy outlining procedure for transporting monitored patients– Transporters reminded that they must check-in with
patients’ nurses before taking a patient
– Reflects community standards Codifies intended (but currently not standard) practice at University
– Will be incorporated into education for nurses, HUC’s, and transporters
• Drafted policy outlining back-up procedures for system failure– Will be incorporated into education for nurses, HUC’s,
and other Patient Care Services personnel
DMAIC
Feb 2006
CALL TO ACTION – July 2005
What unit managers/leaders need to do NOW
• Incorporate battery & lead changes into routine shift vitals
• Remind staff:– All alerts & responses are logged, including who was alerted
– Get a “buddy” to hold your pager when you won’t be available (off unit, break, in procedure, etc.)
– “Just push the button” to acknowledge an alert
– Put discontinued transmitters & logs in the return boxes
• Look for news of next steps:– Policy & procedure updates
– New ordering process
– New educational materials
– Results of remeasurement
What we asked of
managers in July…
What we asked of
managers in July…
DMAIC
Feb 2006
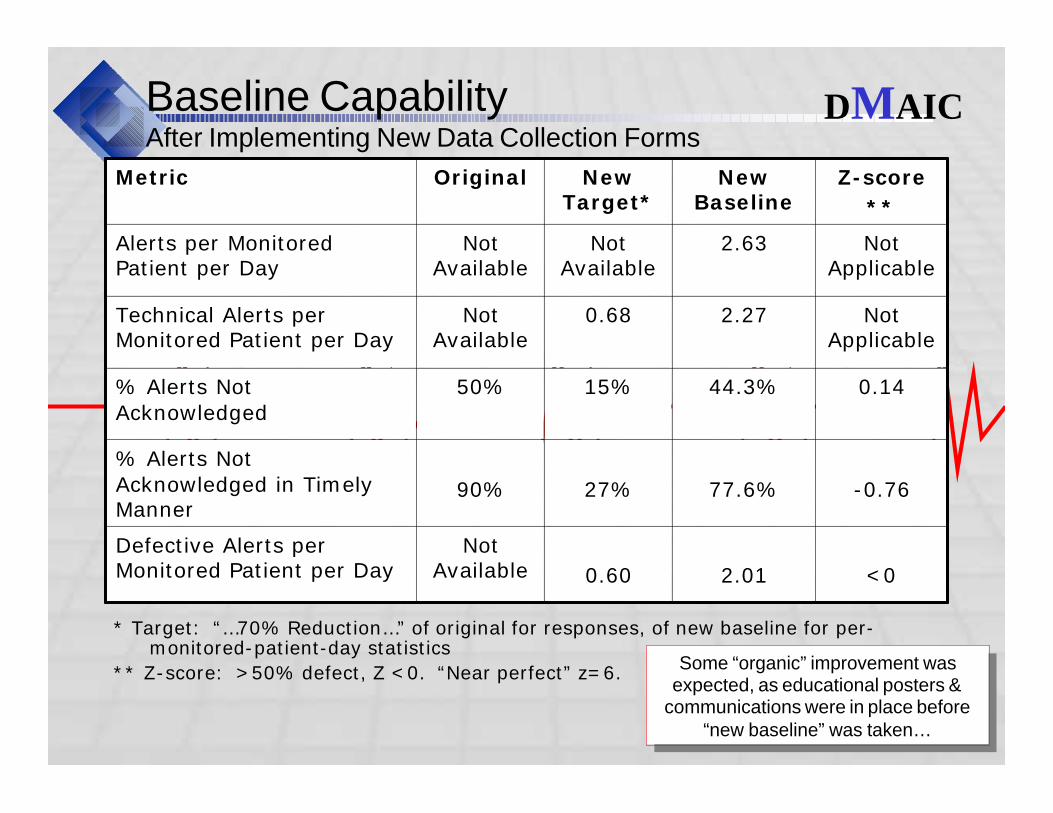
Baseline CapabilityAfter Implementing New Data Collection Forms
* Target: “…70% Reduction…” of original for responses, of new baseline for per-monitored-patient-day statistics
** Z-score: >50% defect, Z <0. “Near perfect” z=6.
Not Applicable
2.270.68Not Available
Technical Alerts per Monitored Patient per Day
Not Applicable
2.63Not Available
Not Available
Alerts per Monitored Patient per Day
-0.7677.6%27%90%
% Alerts Not Acknowledged in Timely Manner
2.01
44.3%
New Baseline
<00.60
Not Available
Defective Alerts per Monitored Patient per Day
0.1415%50%% Alerts Not Acknowledged
Z-score
**
New Target*
OriginalMetric
Some “organic” improvement was expected, as educational posters &
communications were in place before “new baseline” was taken…
Some “organic” improvement was expected, as educational posters &
communications were in place before “new baseline” was taken…
DMAIC
Feb 2006
Results of Communication Audit
• Overall, 90% of questions asked were answered correctly!!
• Of missed answers, 80% from 3 questions:– #18 – Transmitters can be matched to the patient by
comparing the name on the pouch to the patient’s ID
– #19/20 – Dealt with transportation. If going to Dialysis, nurse should call CMU to get a transmitter that will work in Dialysis. Otherwise, the nurse should notify CMU the patient will be off-unit, and leave the transmitter in the patient’s room.
Conclusion: Communication was received—staff know what to do!
Conclusion: Communication was received—staff know what to do!
DMAIC
Feb 2006
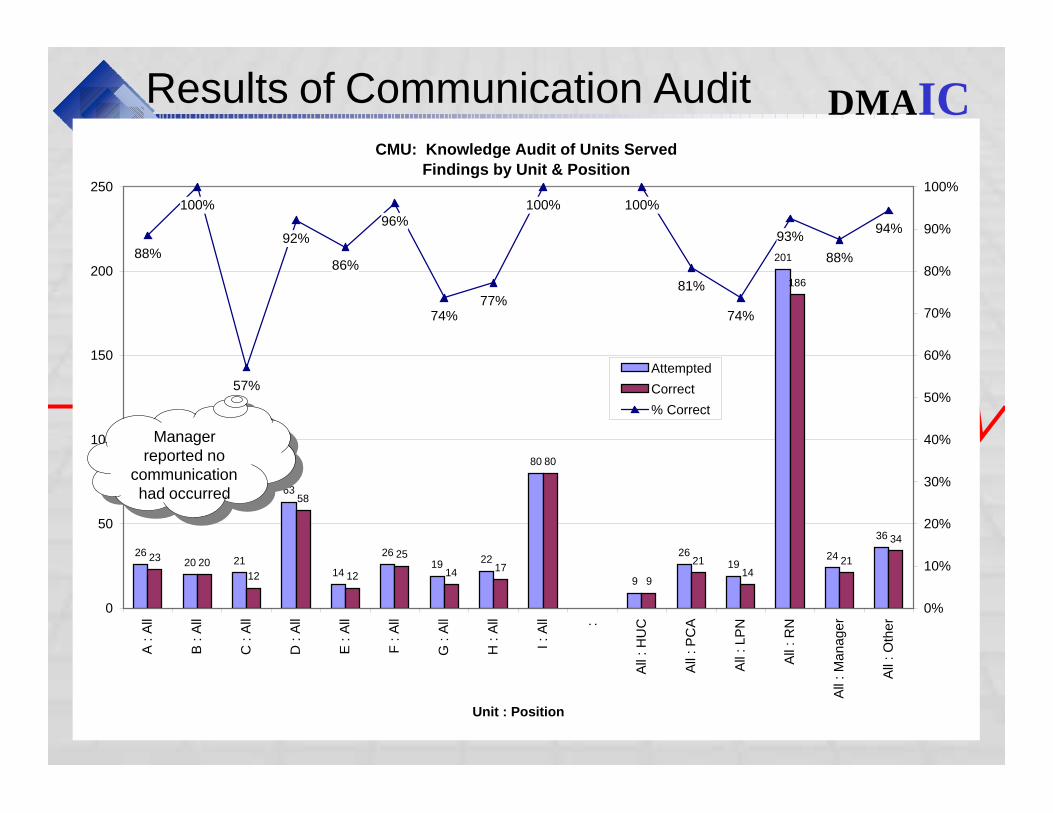
CMU: Knowledge Audit of Units Served
Findings by Unit & Position
2620 21
63
14
2619 22
80
9
2619
201
24
36
23 20
12
58
12
25
14 17
80
9
2114
186
21
34
88%
100%
57%
92%
86%
96%
74%77%
100% 100%
81%
74%
93%
88%
94%
0
50
100
150
200
250
A : A
ll
B : A
ll
C : A
ll
D : A
ll
E : A
ll
F : A
ll
G : A
ll
H : A
ll
I : A
ll :
All
: H
UC
All
: P
CA
All
: LP
N
All
: R
N
All
: M
anager
All
: O
ther
Unit : Position
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Attempted
Correct
% Correct
Results of Communication Audit
Manager reported no
communication had occurred
Manager reported no
communication had occurred
DMAIC
Feb 2006
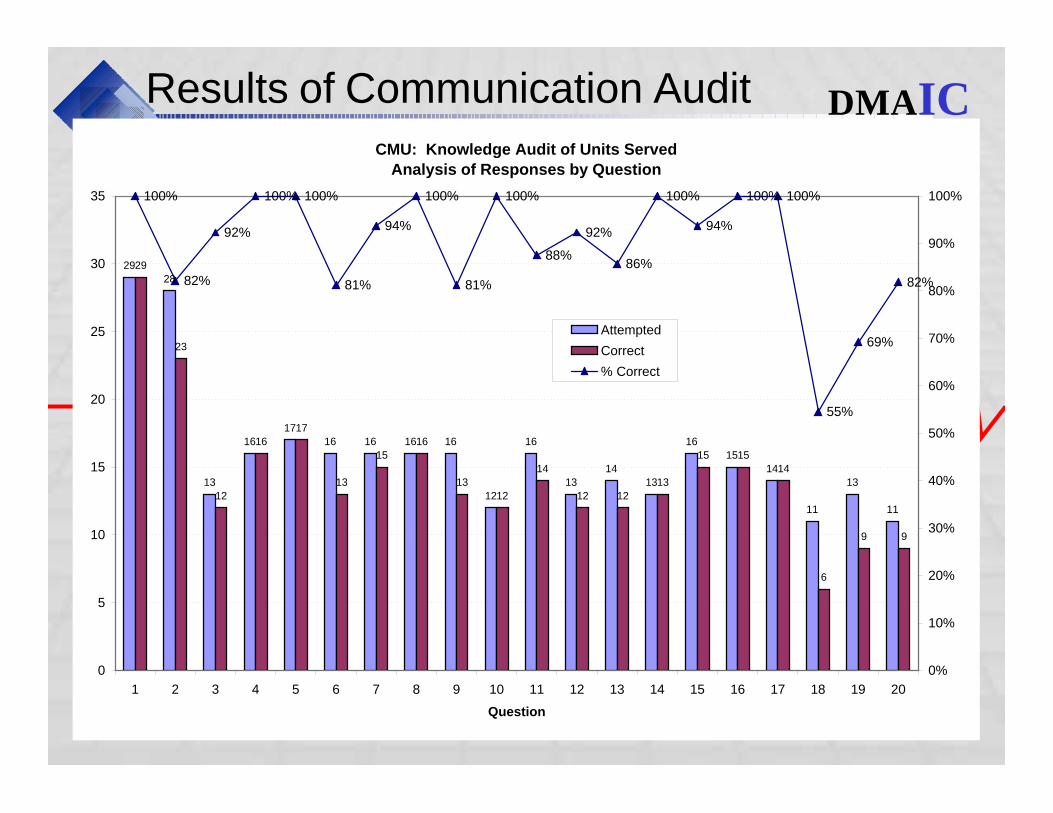
CMU: Knowledge Audit of Units Served
Analysis of Responses by Question
29
28
13
16
17
16 16 16 16
12
16
13
14
13
16
15
14
11
13
11
29
23
12
16
17
13
15
16
13
12
14
12 12
13
15 15
14
6
9 9
100%
82%
92%
100% 100%
81%
94%
100%
81%
100%
88%
92%
86%
100%
94%
100% 100%
55%
69%
82%
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Question
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Attempted
Correct
% Correct
Results of Communication Audit DMAIC
Feb 2006
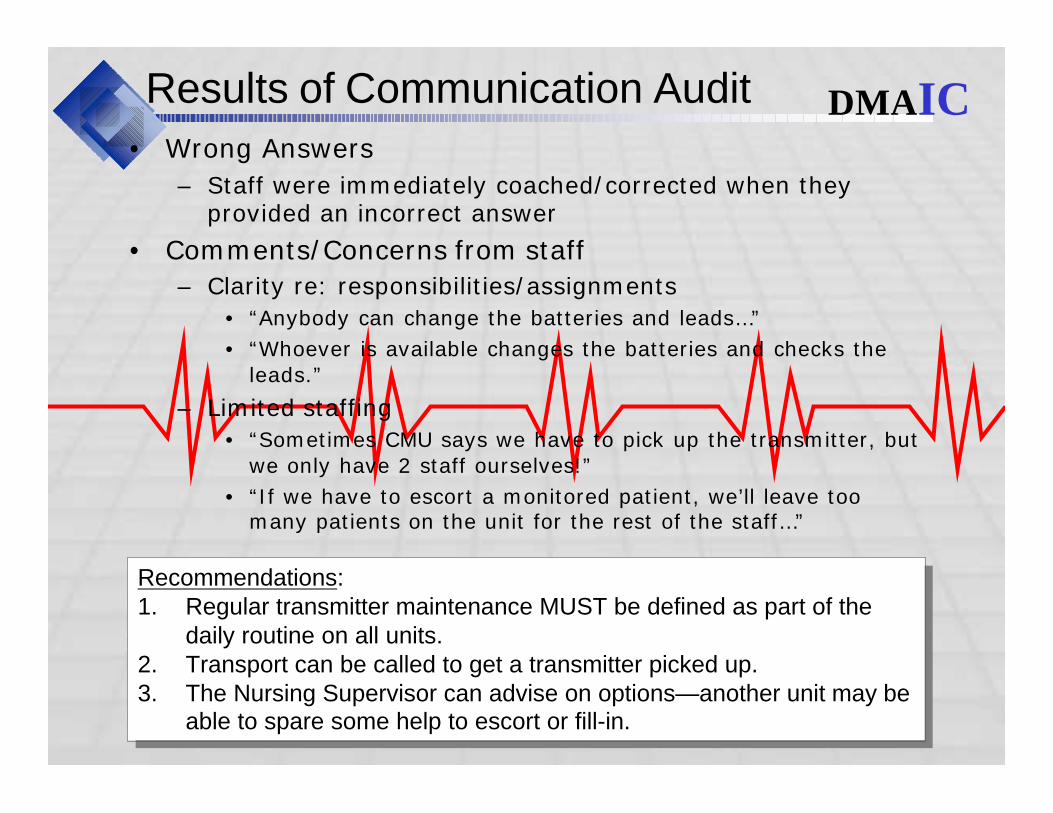
Results of Communication Audit
• Wrong Answers
– Staff were immediately coached/corrected when they provided an incorrect answer
• Comments/Concerns from staff
– Clarity re: responsibilities/assignments
• “Anybody can change the batteries and leads…”
• “Whoever is available changes the batteries and checks the leads.”
– Limited staffing
• “Sometimes CMU says we have to pick up the transmitter, but we only have 2 staff ourselves!”
• “If we have to escort a monitored patient, we’ll leave too many patients on the unit for the rest of the staff…”
Recommendations: 1. Regular transmitter maintenance MUST be defined as part of the
daily routine on all units.2. Transport can be called to get a transmitter picked up.3. The Nursing Supervisor can advise on options—another unit may be
able to spare some help to escort or fill-in.
Recommendations: 1. Regular transmitter maintenance MUST be defined as part of the
daily routine on all units.2. Transport can be called to get a transmitter picked up.3. The Nursing Supervisor can advise on options—another unit may be
able to spare some help to escort or fill-in.
DMAIC
Feb 2006
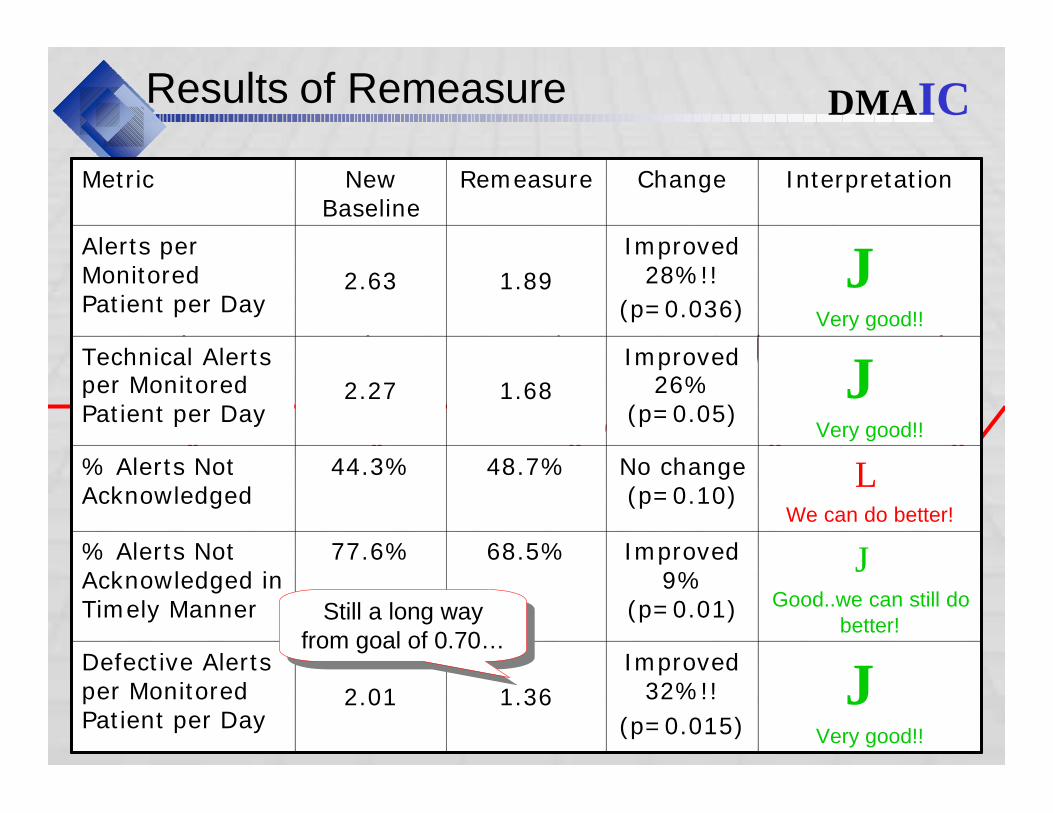
Results of Remeasure
JVery good!!
Improved 26%
(p=0.05) 1.682.27
Technical Alerts per Monitored Patient per Day
JVery good!!
Improved 28%!!
(p=0.036)1.892.63
Alerts per Monitored Patient per Day
Improved 32%!!
(p=0.015)
Improved 9%
(p=0.01)
No change (p=0.10)
Change
JGood..we can still do
better!
68.5%77.6%% Alerts Not Acknowledged in Timely Manner
JVery good!!
1.362.01
Defective Alerts per Monitored Patient per Day
LWe can do better!
Interpretation
48.7%44.3%% Alerts Not Acknowledged
RemeasureNew Baseline
Metric
Still a long way from goal of 0.70…
Still a long way from goal of 0.70…
DMAIC
Feb 2006
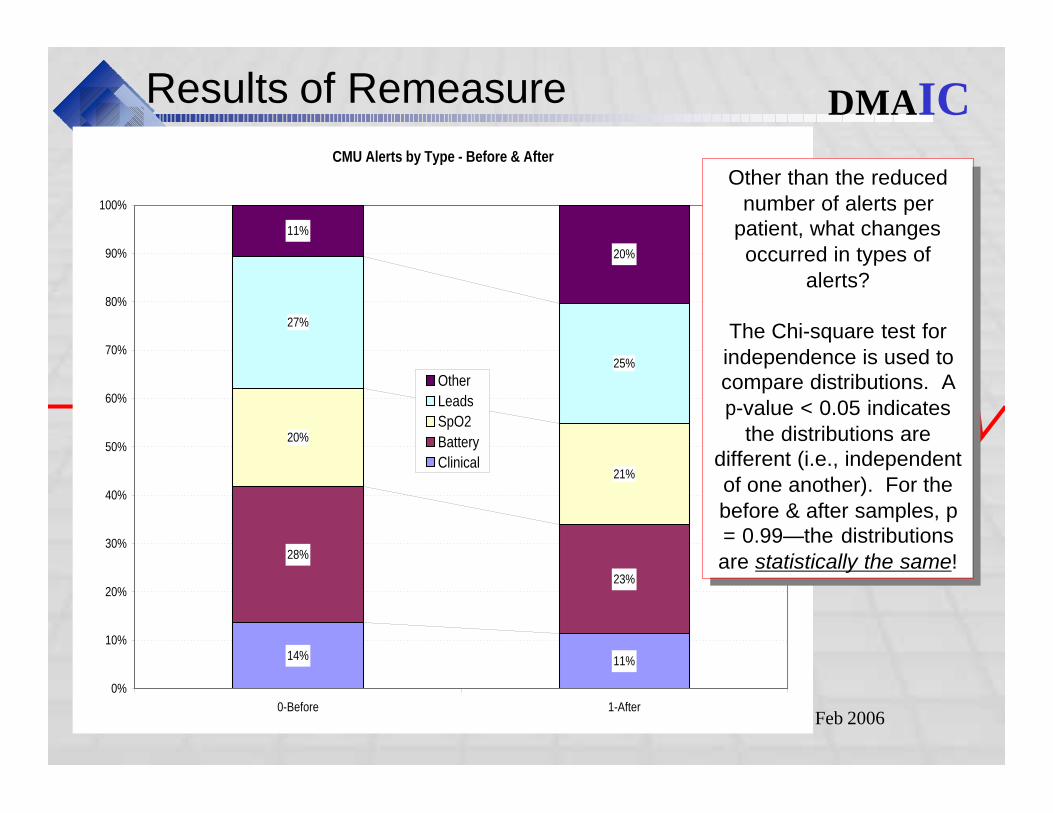
Results of Remeasure
CMU Alerts by Type - Before & After
14% 11%
28%
23%
20%
21%
27%
25%
11%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-Before 1-After
Other
Leads
SpO2
Battery
Clinical
Other than the reduced number of alerts per
patient, what changes occurred in types of
alerts?
The Chi-square test for independence is used to compare distributions. A p-value < 0.05 indicates
the distributions are different (i.e., independent of one another). For the before & after samples, p = 0.99—the distributions are statistically the same!
Other than the reduced number of alerts per
patient, what changes occurred in types of
alerts?
The Chi-square test for independence is used to compare distributions. A p-value < 0.05 indicates
the distributions are different (i.e., independent of one another). For the before & after samples, p = 0.99—the distributions are statistically the same!
DMAIC
Feb 2006
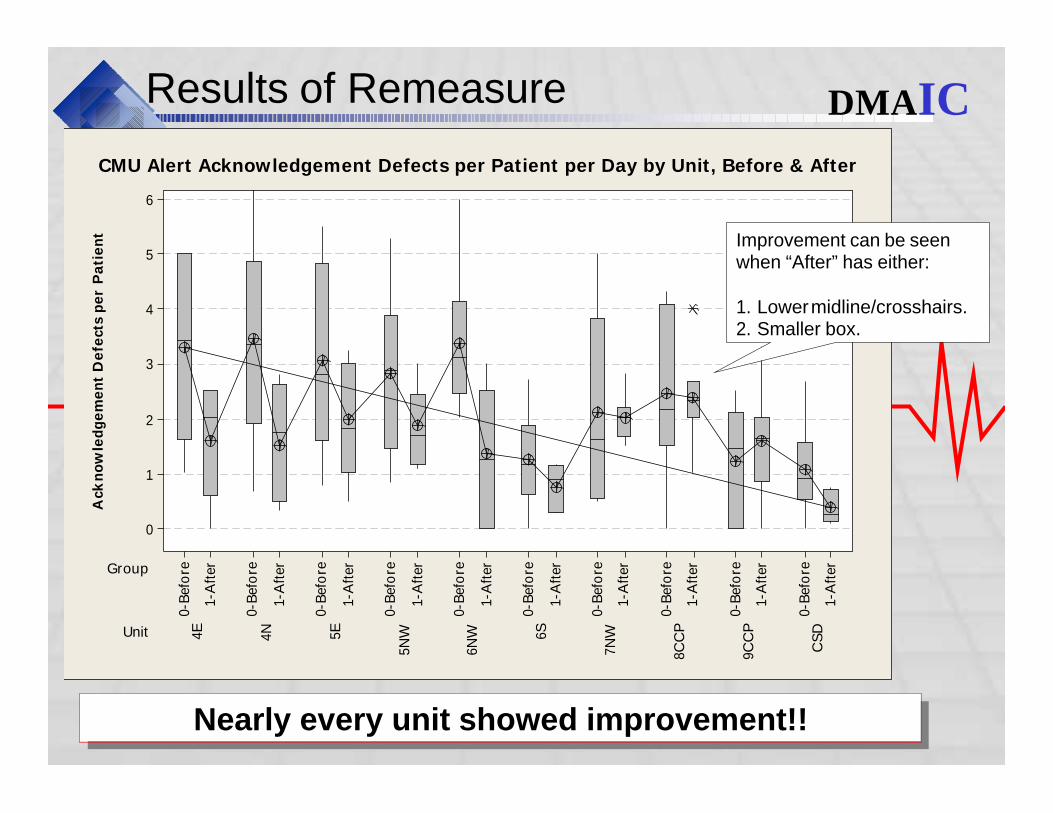
Results of Remeasure
Nearly every unit showed improvement!!Nearly every unit showed improvement!!
Ack
no
wle
dg
em
en
t D
efe
cts
pe
r P
ati
en
t
Unit
Group
CSD
9CC
P
8CC
P
7NW6S
6NW
5NW5E4N4E
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
1-A
fter
0-B
efore
6
5
4
3
2
1
0
CMU Alert Acknowledgement Defects per Patient per Day by Unit, Before & After
Improvement can be seen when “After” has either:
1. Lower midline/crosshairs.2. Smaller box.
DMAIC
Feb 2006
Results of Remeasure
• Observations from data:
– 17% of alerts were repeats/escalations• Repeats were NOT occurring in 5-minute intervals—15-60
minutes passed between attempts
– Documented incidents:• Nurses took their pagers with them off-unit & did not respond
for hours
• Missed red phone alert (phone tested by communications and no operational problems found)
• Abusive & avoidance behaviors toward CMU when non-acknowledgement followed-up by telephone calls to unit
– Results varied by individuals on same units: some always responded on time, others in same area never responded.
This variability points to individual non-compliance and management practice rather than system flaws. Incidents of neglect, abuse, and habitual
noncompliance are reported to unit managers and ACNO’s via e-mail, to facilitate individual coaching…
This variability points to individual non-compliance and management practice rather than system flaws. Incidents of neglect, abuse, and habitual
noncompliance are reported to unit managers and ACNO’s via e-mail, to facilitate individual coaching…
DMAIC
Feb 2006
What might be happening?
• If folks know what they’re supposed to do & how, but aren’t doing it, why?
– Simply forget/make mistake (why CMU tries multiple times)
– Can’t
• More pressing priorities (happens/understandable)
• Patient or nurse off-unit (preventable, with communication)
– Won’t (resistance due to misunderstanding or attitude)
• Don’t accept responsibility for taking appropriate action—”…not my problem…”
• Don’t appreciate potential risks
• Don’t understand accountability
• Don’t recognize that CMU isn’t aware of what’s happening on unit—only what the monitor says…
DMAIC
This variability points to individual non-compliance and management practice rather than system flaws. Incidents of neglect, abuse, and habitual
noncompliance are reported to unit managers and ACNO’s via e-mail, to facilitate individual coaching…
This variability points to individual non-compliance and management practice rather than system flaws. Incidents of neglect, abuse, and habitual
noncompliance are reported to unit managers and ACNO’s via e-mail, to facilitate individual coaching…
Feb 2006
Overall Conclusions
• Staff generally know what to do.
• Specifics of how maintenance is completed not clearly defined on every unit (when audited)
• Marked improvement in performance!
• Still some way to go toward goal…
• Still a gap between knowledge and behavior…
DMAIC
Feb 2006
2nd Remeasure (Alerts per Patient)
Remeasure Results - CMU Alerts per Monitored Patient
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
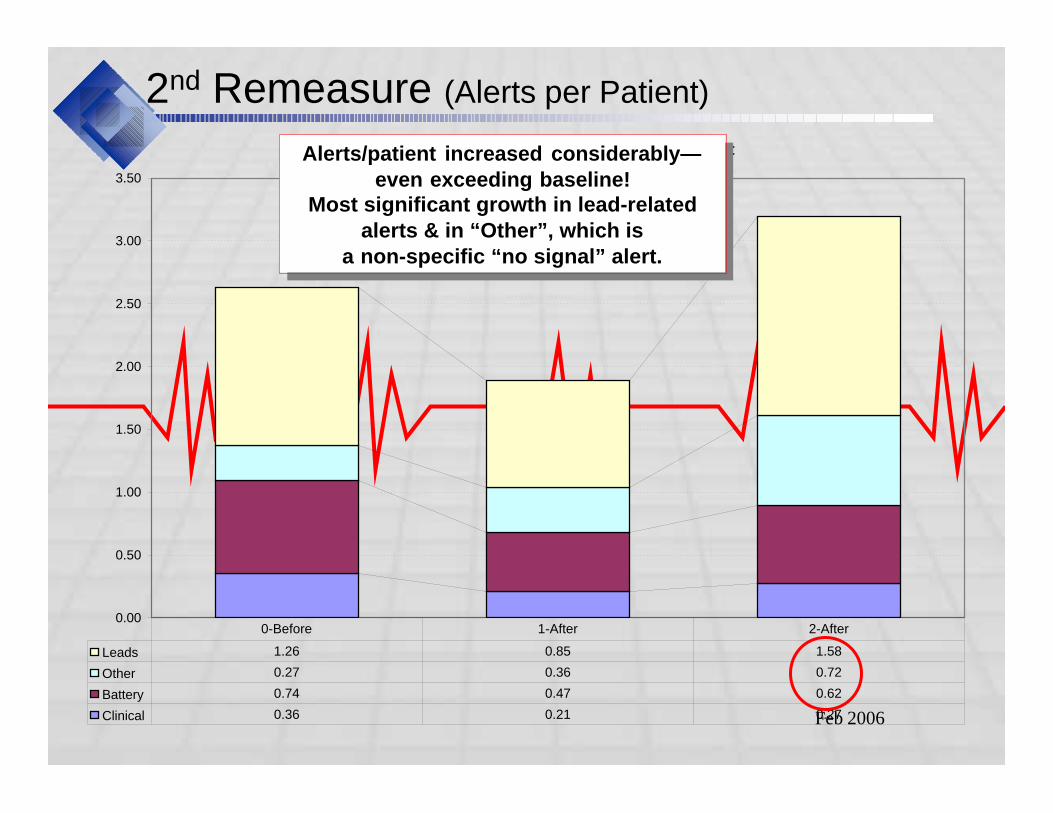
Leads 1.26 0.85 1.58
Other 0.27 0.36 0.72
Battery 0.74 0.47 0.62
Clinical 0.36 0.21 0.27
0-Before 1-After 2-After
Alerts/patient increased considerably—even exceeding baseline!
Most significant growth in lead-related alerts & in “Other”, which is
a non-specific “no signal” alert.
Alerts/patient increased considerably—even exceeding baseline!
Most significant growth in lead-related alerts & in “Other”, which is
a non-specific “no signal” alert.
Feb 2006
Drill-Down: Variability in Alerts per Patient
• Closer review of the data revealed special cause variation:
– 8CCP experienced an exceptionally high volume of SpO2-related calls on Thursday, Friday, and Saturday of the data period. This suggests at least one patient during this time was very non-compliant in wearing the SpO2 lead correctly, or at all! This is further evidenced by the high number of repeat alerts
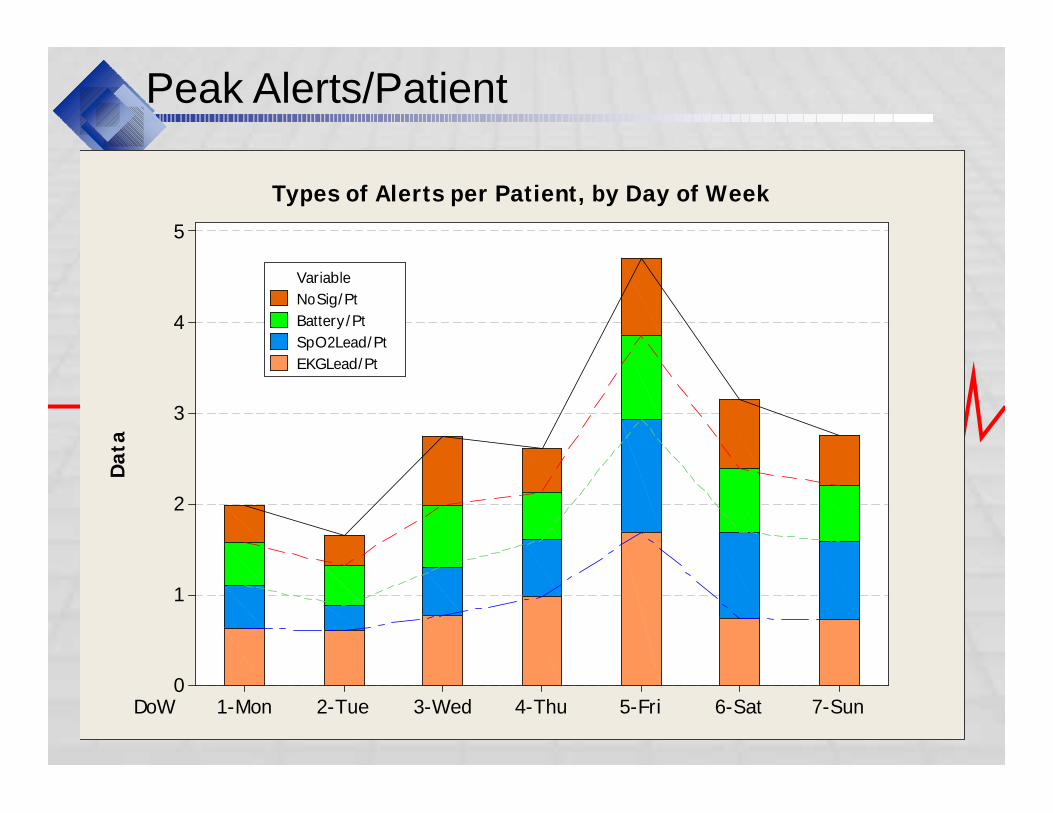
– SpO2 usage was much higher toward the end of the week, driving up:
• Battery alerts (SpO2 drains batteries 3 times faster!)
• Lead alerts (which includes patients taking off the finger probe)
– Total patients on CMU telemetry does not vary significantly from day to day, but admissions & discharges both peak on Friday, increasingopportunities for errors. E.g., removing a transmitter to discharge a patient without first notifying CMU would drive up:
• Lead-related alerts
• “No signal”/other alerts
Feb 2006
Peak Alerts/PatientD
ata
DoW 7-Sun6-Sat5-Fri4-Thu3-Wed2-Tue1-Mon
5
4
3
2
1
0
Variable
NoSig/Pt
Battery/Pt
SpO2Lead/Pt
EKGLead/Pt
Types of Alerts per Patient, by Day of Week
Feb 2006
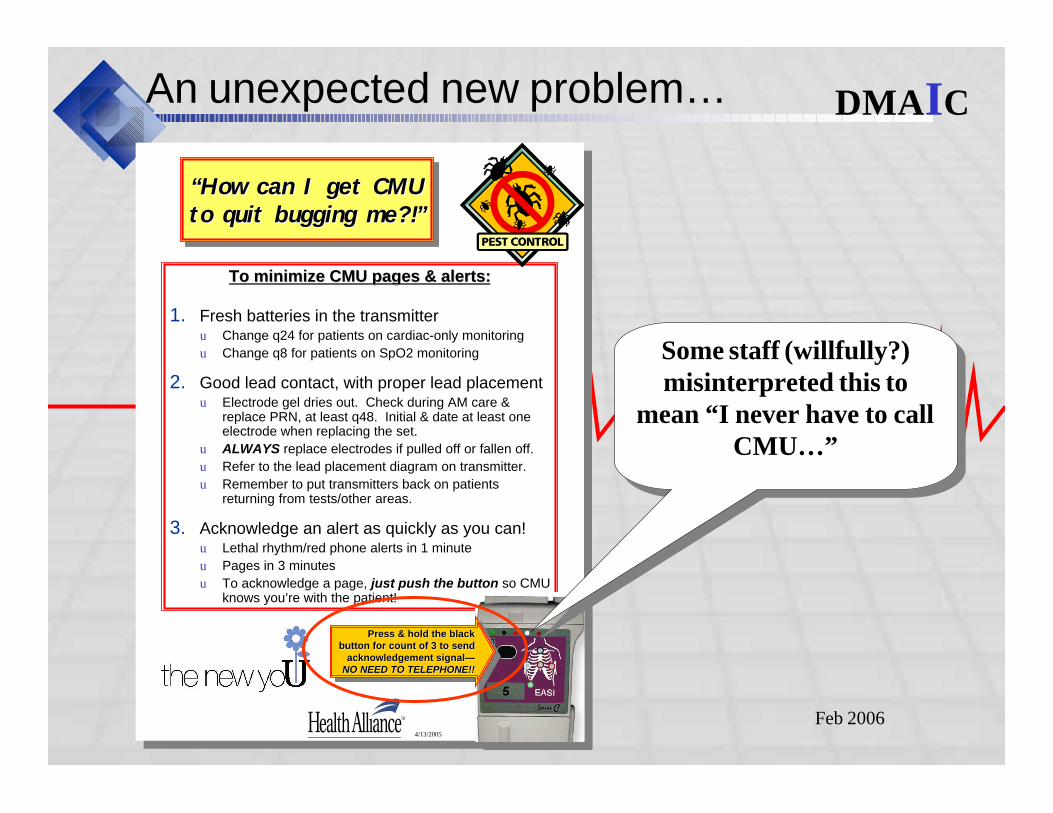
An unexpected new problem…
4/13/2005 1
“How can I get CMU to quit bugging me?!”
“How can I get CMU “How can I get CMU to quit bugging me?!”to quit bugging me?!”
To minimize CMU pages & alerts:To minimize CMU pages & alerts:
1. Fresh batteries in the transmitteru Change q24 for patients on cardiac-only monitoring
u Change q8 for patients on SpO2 monitoring
2. Good lead contact, with proper lead placementu Electrode gel dries out. Check during AM care &
replace PRN, at least q48. Initial & date at least one electrode when replacing the set.
u ALWAYS replace electrodes if pulled off or fallen off.
u Refer to the lead placement diagram on transmitter.
u Remember to put transmitters back on patients returning from tests/other areas.
3. Acknowledge an alert as quickly as you can!u Lethal rhythm/red phone alerts in 1 minute
u Pages in 3 minutes
u To acknowledge a page, just push the button so CMU knows you’re with the patient!
Press & hold the black button for count of 3 to send
acknowledgement signal—NO NEED TO TELEPHONE!!
Press & hold the black Press & hold the black button for count of 3 to send button for count of 3 to send
acknowledgement signalacknowledgement signal——NO NEED TO TELEPHONE!!NO NEED TO TELEPHONE!!
4/13/2005 1
“How can I get CMU to quit bugging me?!”
“How can I get CMU “How can I get CMU to quit bugging me?!”to quit bugging me?!”
To minimize CMU pages & alerts:To minimize CMU pages & alerts:
1. Fresh batteries in the transmitteru Change q24 for patients on cardiac-only monitoring
u Change q8 for patients on SpO2 monitoring
2. Good lead contact, with proper lead placementu Electrode gel dries out. Check during AM care &
replace PRN, at least q48. Initial & date at least one electrode when replacing the set.
u ALWAYS replace electrodes if pulled off or fallen off.
u Refer to the lead placement diagram on transmitter.
u Remember to put transmitters back on patients returning from tests/other areas.
3. Acknowledge an alert as quickly as you can!u Lethal rhythm/red phone alerts in 1 minute
u Pages in 3 minutes
u To acknowledge a page, just push the button so CMU knows you’re with the patient!
Press & hold the black button for count of 3 to send
acknowledgement signal—NO NEED TO TELEPHONE!!
Press & hold the black Press & hold the black button for count of 3 to send button for count of 3 to send
acknowledgement signalacknowledgement signal——NO NEED TO TELEPHONE!!NO NEED TO TELEPHONE!!
DMAIC
Some staff (willfully?) misinterpreted this to
mean “I never have to call CMU…”
Some staff (willfully?) misinterpreted this to
mean “I never have to call CMU…”
Feb 2006
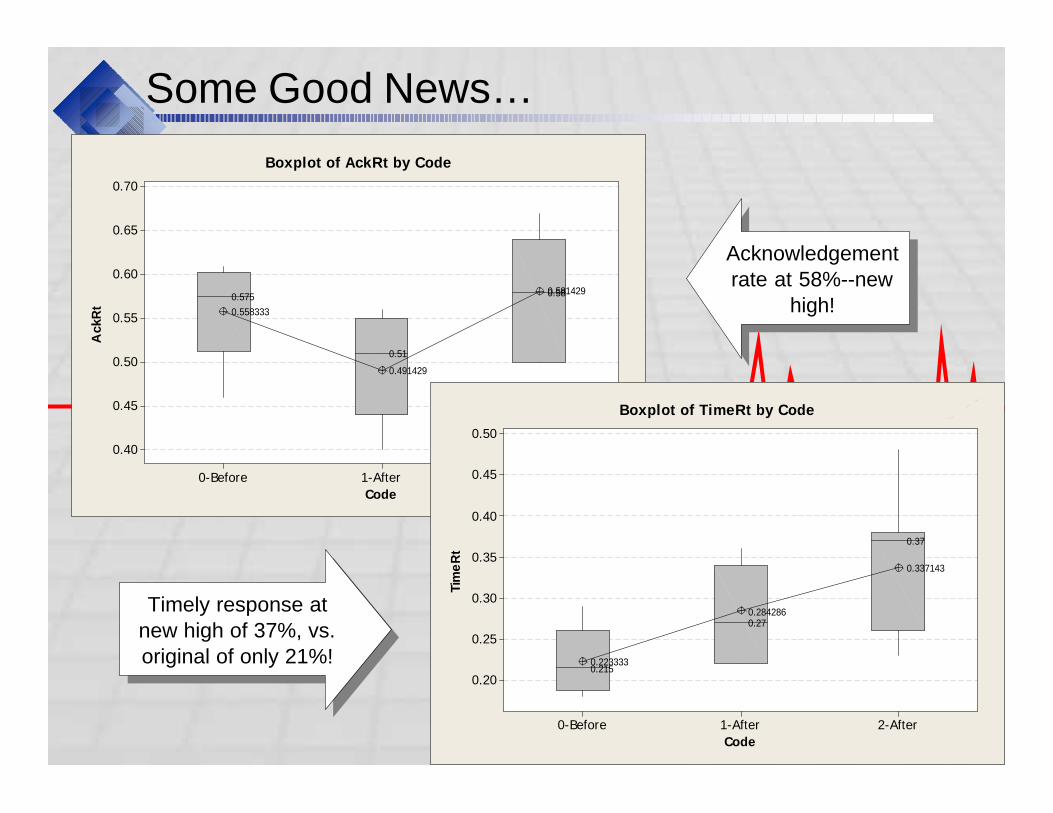
Some Good News…
Code
AckR
t
2-After1-After0-Before
0.70
0.65
0.60
0.55
0.50
0.45
0.40
0.58
0.51
0.5750.581429
0.491429
0.558333
Boxplot of AckRt by Code
Code
Tim
eR
t
2-After1-After0-Before
0.50
0.45
0.40
0.35
0.30
0.25
0.20
0.37
0.27
0.215
0.337143
0.284286
0.223333
Boxplot of TimeRt by Code
Acknowledgement rate at 58%--new
high!
Acknowledgement rate at 58%--new
high!
Timely response at new high of 37%, vs. original of only 21%!
Timely response at new high of 37%, vs. original of only 21%!
Feb 2006
2nd Remeasure Summary
• Standardize battery policy, on every unit CMU supports:– Stock 9V batteries on the vitals checking devices.
– All CMU transmitter batteries to be changed when AM vitals check.
– For any patient with SpO2 monitoring, batteries must be changed when vitals checked on every shift.
• At discharge or when removing transmitter: CALL CMU first!
• Explore IS&T support in “automatically signaling” needs:– Battery & lead change requirements print on MAR or other nursing
patient care “checklists” (e.g., “pending orders”)?
– Discharges print to CMU?
• Emphasize to patients and families that wearing the SpO2 finger probe continuously & correctly is a responsibility in participating in their care/recovery.– Get orders to remove non-compliant patients from telemetry.
• Consider 48-hour automatic discontinuation to reduce opportunity for errors.
Feb 2006
Radically Rethinking “Central” Monitoring
• Human Nature– What gets measured…
– Out of sight = out of mind
– Everyone’s responsibility = nobody’s job
– Non-clinical (85%+ of alarms) = non-priority
• New experiment: What if responsibility were consolidated to one person per unit?– Advantages
• Local, & closer personal relationship to nurses
• Defined priority; doesn’t have to be a nurse!
• Less “noise” bothering nurses
– Disadvantages• Other tasks competing for attention
“If you always do what you’ve always done,
you’ll always get what you always got.”-
unknown
“Systems deliver exactly the results they
are designed to produce” – D. Berwick
“The significant problems we have
cannot be solved at the same level of thinking with which we created
them.” - Einstein
“If you always do what you’ve always done,
you’ll always get what you always got.”-
unknown
“Systems deliver exactly the results they
are designed to produce” – D. Berwick
“The significant problems we have
cannot be solved at the same level of thinking with which we created
them.” - Einstein
Feb 2006
The “Radical” Experiment
Concerns
• Competing priorities
• Disruptive to nursing unit
• Resistance from CMU
• Decentralizing Centralization?!!
Strategies
• Dedicated/only assignment
• “Watch” as well as “do”
• Volunteer unit
• Short pilot
• Emphasize benefits to RN’s
• Paint picture of success
• “Let’s try it and see…”
• Recognize “safety net”
• If it’s the wrong thing, we need to fix it!
Feb 2006
Results
• PCA identified & resolved 92% of “alert conditions” without having to be notified by CMU.
– Of those missed, the PCA was with another patient or at lunch.
– PCA addressed missed alerts upon notification
– Because PCA did not perform “preventive maintenance” in changing batteries & leads, volume of alerts was higher than necessary.
• Of all the alert conditions, 35 were clinical: 28* low SpO2 and 7 rhythm.
– Of these, the PCA checked the patient and resolved the issue before CMU called 31 of the 35 times (89%)
– Of CMU’s calls, 3 were low SpO2 & 1 was for heart rate
Results of "Radical" Experiment
* This number is somewhat higher than usual, as CMU often waits until a definite pattern of low SpO2 emerges, as patient behaviors can lead to false alarms or temporary drops that resolve themselves.

Feb 2006
Interpreting the Results
• More responsive: Consolidating responsibility to a single individual increased acknowledgement/resolution rate to 100%
• Faster response: Consolidating responsibility & watching the monitor increased timeliness of response to 100%
• Less “noise”: Watching the monitor reduced CMU call volumes 87% (using normalized SpO2 alert volumes—not the total the PCA acted on).
Results of "Radical" Experiment
Feb 2006
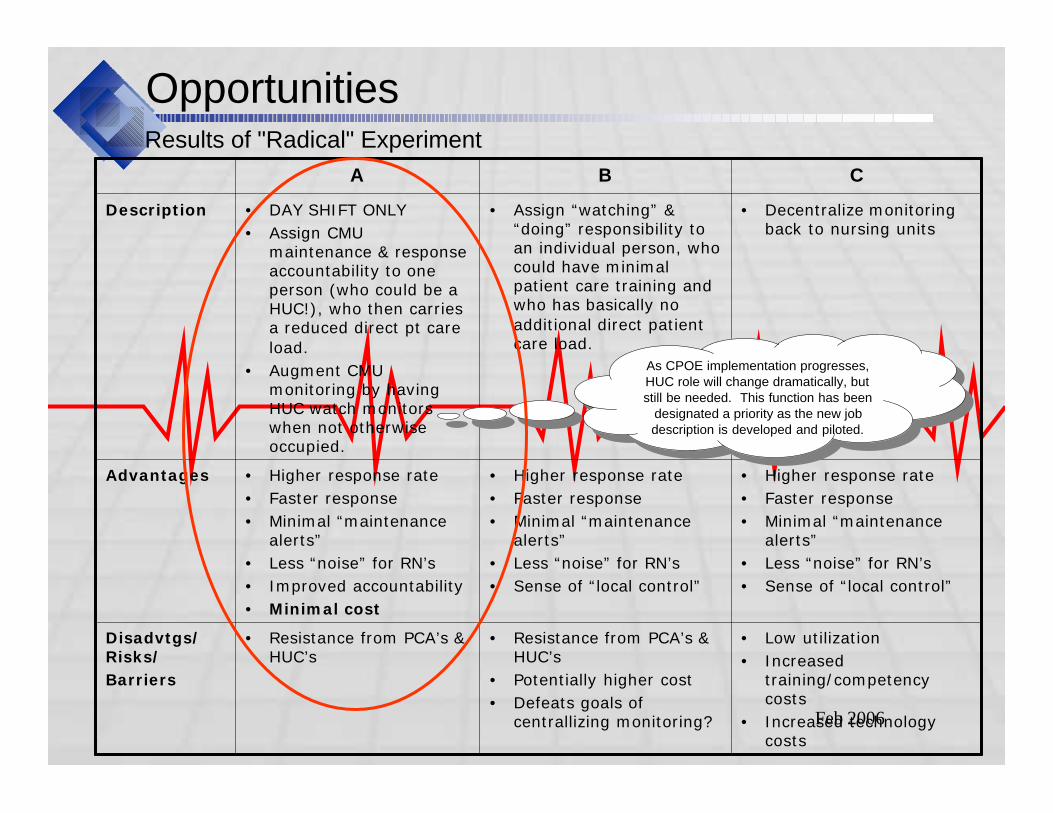
OpportunitiesResults of "Radical" Experiment
• Resistance from PCA’s & HUC’s
• Potentially higher cost
• Defeats goals of centrallizing monitoring?
• Higher response rate
• Faster response
• Minimal “maintenance alerts”
• Less “noise” for RN’s
• Sense of “local control”
• Assign “watching” & “doing” responsibility to an individual person, who could have minimal patient care training and who has basically no additional direct patient care load.
B
• Low utilization
• Increased training/competency costs
• Increased technology costs
• Higher response rate
• Faster response
• Minimal “maintenance alerts”
• Less “noise” for RN’s
• Sense of “local control”
• Decentralize monitoring back to nursing units
C
• Resistance from PCA’s & HUC’s
Disadvtgs/ Risks/
Barriers
• Higher response rate
• Faster response
• Minimal “maintenance alerts”
• Less “noise” for RN’s
• Improved accountability
• Minimal cost
Advantages
• DAY SHIFT ONLY
• Assign CMU maintenance & response accountability to one person (who could be a HUC!), who then carries a reduced direct pt care load.
• Augment CMU monitoring by having HUC watch monitors when not otherwise occupied.
Description
A
As CPOE implementation progresses, HUC role will change dramatically, but still be needed. This function has been
designated a priority as the new job description is developed and piloted.
As CPOE implementation progresses, HUC role will change dramatically, but still be needed. This function has been
designated a priority as the new job description is developed and piloted.
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Getting & Maintaining Support
• Mandated from the top
• Team-based: CMU + Nursing Units
• Regular progress reporting to unit managers
• Frequent outreach to nurses– Promotional
– Educational
– One-on-one
• Pilots with results reporting
• Process for ongoing monitoring & feedback
Feb 2006
Overview
• Defining Safety
• FMEA’s & JCAHO
• Measuring Safety Performance
• Selecting & Piloting Solutions
• Strategies to Effect Change
• Summary
Feb 2006
Summary: The Actual Process
1. Define “safety”: what are the observable signs?
2. Determine metrics
3. Establish baseline performance
4. Document & analyze process– Flow charts
– Cause & Effect brainstorming (Fishbone)
– FMEA to prioritize
5. Identify solutions– Focused brainstorming on FMEA priorities
– Data-driven imperatives—”reap what you sow”
– Ensure behavior changes hold
6. Pilot & re-measure
7. Feedback mechanisms
Feb 2006
Questions?
Terry Dunn Six Sigma Black BeltHealth Alliance of Greater Cincinnati513/[email protected]


















