Enhancing The Intersection Between Production … The Intersection Between Production and Promoting...
61
Enhancing The Intersection Between Production and Promoting Quality Improvement: Focus on Quality Nina Brown, MPH, CHES National Health Care for the Homeless Council Regional Training Regional Meeting: Albuquerque, New Mexico November 11, 2011 Public Health Analyst, Office of Quality and Data U.S. DHHS/HRSA/BPHC 1
Transcript of Enhancing The Intersection Between Production … The Intersection Between Production and Promoting...

Enhancing The Intersection Between Production and Promoting Quality
Improvement: Focus on Quality
Nina Brown, MPH, CHES National Health Care for the Homeless Council Regional Training Regional Meeting: Albuquerque, New Mexico November 11, 2011 Public Health Analyst, Office of Quality and Data U.S. DHHS/HRSA/BPHC
1

Learning Objectives
At the end of this presentation participants will be able to:
1. Understand the role of quality within healthcare delivery system reform;
2. Understand the importance of using data in Quality Improvement efforts;
3. Locate data within EHB and the HRSA website to assist in Quality Improvement activities;
4. Be able to access and utilize BPHC’s Quality Improvement resources.
2

HCH Grantee Patients - 2010
3
Health Center Snapshot
No. of Patients
Patients 805,064 Male Patients
56%
Female Patients
44%
Age <= 19
16%
Age 20-64 81%
Age 65 and Over 3%

HCH Grantee Patients - 2010
4
Hispanic 21%
Asian 2%
American Indian/Alaskan
Native 1%
Black/African American
31%
Native Hawaiian/Other Pacific Islander
1%
White 41%
More Than One
Race 3%

HCH Grantee Patients - 2010
5
79%
5% 2%
1%
13%
100% and Below 101%-150% 151%-200% Over 200% Unknown

Health Care Delivery System Reform
• Current system lacks a single entry point • Affordable Care Act
– Allows Health Care to move towards a patient-centered, clinically integrated, accountable system.
– Modernization of Health Information Technology (HIT) – Development of new patient care models
o ACOs – Strengthen Quality Infrastructure
o National Quality Strategy – Supportive services delivered at home and in the
community
6 Source: The Heller School for Social Policy and Management. Foundations and Healthcare Reform 2010 Policy Brief. July 14, 2010

QI Critical for Delivery System Redesign
• IOM’s top challenges for delivery system redesign: – Use of performance measures/outcomes for
continuous quality improvement and accountability • What is quality health care?
– Safe, effective, patient-centered, timely, efficient, equitable
– Includes other services that are provided
7 Source: Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. March 2001, National Academies Press. 7

National Trends
• Growing awareness of the need to improve quality, costs, and outcomes – Patient and provider experience
• Push to measure quality and increase accountability • HIT enables increasing opportunities for integration, public
reporting • PCMH is becoming the de facto blueprint for delivery system
redesign – Primary care currently only accounts for 4 percent of total
health care spending
8

• Delivery reform – focus on quality – Visits are smarter and more coordinated – HIT and Patient Centric models of care
• Good for patients and good for the system
• HRSA has no minimum annual Productivity Requirements
• Team based care
9
The Take Home Message: Quality vs. Productivity

10
Inputs/ Resources
HRSA
Health Centers
HC Partners
Other HHS & Fed. Agencies
Local & National Stakeholders
Activities
Recruit and Retain Approp.
Workforce
Develop TA & QI Support
Infrastructure
Facilitate HIT Adoption & Integration
Strengthen Eval. & Innovation Infrastructure
Facilitate Communication & Collaboration
Output
Skilled Workforce Available
HIT Adopted & Used
Meaningfully
Eval. & Innovations Sustained
Collaborations & Partnerships Strengthened
Impact
Health Centers Transformed for
QI (PCMH)
Care & Services Coordinated Regionally
QI Efforts Aligned Locally
& Nationally
Outcome (HCs providing care that is...)
Safe
Effective
Efficient
Patient-Centered
Timely/ Accessible
Equitable
BPHC QI Strategy Framework
10

BPHC Quality Strategy
1. Develop and enhance access points 2. Transform HC care delivery system
– PCMH – HIT Meaningful Use
3. Recruit, develop, retain skilled workforce 4. Integrate Health Centers into local health
systems – Specialists, ER, Hospitals – ACOs – Public Health
5. Align policies and programs where possible 11

Primary Health Care 2011 Strategic Priorities
• Grantee Satisfaction – BPHC External Technical Assistance & Training
Strategy • Employee Satisfaction
– BPHC Internal Staff Training & Development • Timeliness/Quality
– Service Area Definition & Overlap/Collaboration • Impact
– Quality Strategy (including Meaningful Use & Patient-Centered Medical Home)
– Recovery Act Close-Out 12

13

Quality Improvement
1. QI infrastructure – Protected staff time – QI committee – Board – Policies and procedures
2. Written QI Plan 3. Evidence of Implementation
14

QI Planning Critical to Meeting Quality Goals
• Delivery system redesign • Clinical quality • Patient experience • Staff satisfaction • Financial sustainability • Leveraging resources and coordinating beyond
your four walls
15

Benefits of an Effective QI Plan
• Roadmap for HC organization – Leadership, focus, & prioritization – Efficient coordination of staff & resources – Better outcomes, patient experience, staff
satisfaction • Satisfy external requirements
– HRSA, state or multipayer pilot – Third-party quality accreditation and recognition
16

HRSA Program Requirements
• Ongoing QI/QA Plan encompassing management and clinical services, maintaining confidentiality of patient records
• Focused responsibility for QI • Periodic assessments of appropriate service use and quality
– Conducted by physicians or licensed health professionals under the supervision of physicians
– Based on systematic collection and evaluation of patient records – Identify and document the necessity for change in the provision of
services and result in the change being implemented
17

QI Program Flow
1. QI teambuilding throughout your center and QI Committee responsibilities
2. Self-assessment of areas to target 3. Goal setting
– Concrete goals – Progress measures
4. Identify strategies for improvement – Philosophy of organizational change – Specific changes to structures and process of care
18

QI Program Flow
5. Data collection and analysis – Use data to fuel QI by closing the
feedback loop 6. Periodically evaluate, celebrate, and
disseminate 7. Integrate with operations and other quality-
related activities
19

Teambuilding
• Quality as an integral part of the organizational culture
• Buy-in at all levels – Board, management, staff and patients
• Resources – Staff time, meetings, information systems
• Provide education and training
20

QI Infrastructure
• QI Committee • QI Plan & Health care plan • QI calendar • Clinical practice guidelines • Policies & procedures • Peer review • Chart audits • Patient satisfaction surveys • Tracking systems • Credentialing and privileging • Data sources
21

Self-Assessment
• Revisit mission statement and vision • Review past needs assessments and consider how the
needs of the patient population have evolved • Compare capacity and ability to supply quality services to
the need • Identify areas for improvement: high risk, high volume,
low performance
22 22

Setting Goals
• Compare yourself to your prior performance • Compare yourself to others
– EHB benchmarked performance reports
• Short and long-term time goals • Aspirational Goals
23

DATA DATA DATA
24

• Low birth weight • Entry into prenatal care • Childhood immunization • Pap tests • Adult hypertension (blood pressures) • Adult diabetes (HbA1c levels)
Uniform Data System (UDS) Clinical Measures
• Child & adolescent weight assessment & counseling • Adult weight screening & follow up • Tobacco use assessment & counseling • Asthma therapy (pharmacologic)
Current Measures New in 2011
Monitoring Quality of Care
25

Collecting Your Data
• Data collected depends on expectations of 3rd parties • Process vs. performance: Measure should reflect 3 things:
– WHAT you do – HOW you do it – HOW EFFECTIVE you are
• Include measures that you Aspire to achieve. • Challenges
– Ease and access of use – EHR Levels differ – Free Text
26

Using Data is a Team Effort!
• Staff on the floor are part of the process. They need to understand the process. – Aligned process that ties into your strategic plan
• Involve your Medical Director – Critical in gaining understanding of data and system
level performance Picture: 3 individuals holding hands united
27

Using Your Data
• Start with the end in mind – Collect it ONCE and use it MANY times – Try using data that are shared and accessed easily – Data need to be structured the same way – Weekly, quarterly pull of data if possible
• Linking data – Ex. Meaningful Use data are standardized, but the data
entry isn’t… Training of staff
28

Using Your Data
• Align – How to prevent failure – Identify the failure – Bring into balance
• Balanced Measures – Strategic plan… Align measures – Plan Do Study Act (PDSA) – Scorecards: Determining who’s responsible for what
measure
29

Using Your Data
• Measure the process to drill down to the outcome • Achieve your goals
– Through processes and structure using root cause analysis (contributing and restricting factors)
• Case studies help! – Select 20 patients & the data points that stand out – Stories personalize the data
• Utilize your consumer board members to help you know if the process is working.
30

Data Sources for Quality Improvement
• Public site for UDS data: http://bphc.hrsa.gov/healthcenterdatastatistics/index.html
• HRSA Data Warehouse: http://datawarehouse.hrsa.gov/
• Reports Available in EHB – Health Center Trend Report (National/State/Grantee) – Health Center Summary Report (National/State/Grantee) – Performance Profile (National/State) -- Number &
Percent of Health Centers
31

EHB Reports
• This graphic highlights the EHB home page and directs participants to the area they can access reports within EHB. It is denoted by a red circle
32
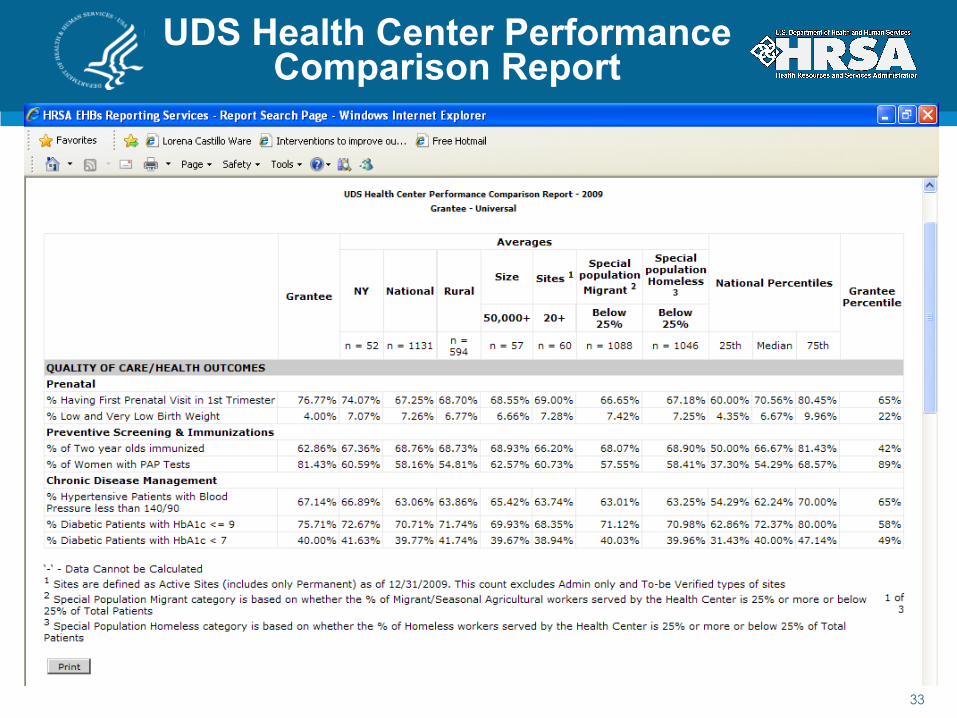
UDS Health Center Performance Comparison Report
33
• This graphic shows the report that grantees can access within EHB. The report shows the specific grantee and how their clinical performance compares to their state and national. It also shows comparison amongst grantees of different sizes and special populations.

UDS Health Center Performance Comparison Report
34
• This is a continuation of the previous report. It highlights how the grantee compares on costs to their state and national. It also shows comparison amongst grantees of different sizes and special populations.

UDS Health Center Performance Comparison Report
35
• This is a continuation of the previous report. It highlights how the grantee compares on costs to their state and national. It also shows comparison amongst grantees of different sizes and special populations.

UDS Health Center Trend Report
36
• This is an EHB report that shows the three year trend for the specific grantee on key performance measures.

Plan Your Quality Intervention
• Establish project-specific QI team that represents all staff integral to the service or issue
• Utilize QI tools and techniques to understand the problem that you are facing – Flow charts, root cause analysis, cause and effect
diagrams, facilitated brainstorming
• Identify potential solutions to make improvement to the systems of care, both short and long term
• Develop timeline for reporting findings and improvement strategies
37

Evaluation of the Intervention
• Document and track progress in activity logs, workplans, meeting minutes
• If historical data are available, trend analysis • Display and distribute data to communicate
findings and results. – Plan to inform CQI committee and staff of results – Graphic presentation of data readings over time
• Report progress to the rest of the organization on a regular basis
• Celebrate and share beyond your four walls
38

HIT and Quality
39

Role of HIT in QI
• Neither necessary nor sufficient, but can really make QI a lot easier
• Can’t just use EHRs like paper charts – Interoperability and standard terminology
and codes • Consensus-based quality measures: e-
specification • HIT adoption: what is needed for MU? • UDS and Patient Experience
40

Key Features of EHR for QI
• Population management/registries • Clinical quality dashboards • Decision support • Integration with other clinical record systems (lab, oral, BH) • Health Information Exchange, e-prescribing • Patient self-management support • Enhanced access and communication with patients • Reporting quality measures
41

Benefits of HIT
• Provider-to-provider communication • Safety enhancements: drug interactions, handwriting
foibles • Better prepared providers, with the right information
and evidence-based practice guidelines or clinical protocols
• Family and personal health history collected and used
• Information on the whole person: what about oral and behavioral health?
• Patient encounters with providers can be more productive
42

How HRSA Supports You!
43

BPHC Quality Initiatives in Health Centers
• National Quality Recognition – PCMH & PCMH Supplemental – Accreditation – CMS Advanced Primary Care Demonstration Project – Resources 4 Readiness
• FTCA • Health Information Technology (HIT)
– HCCNs and Beacon Communities – Meaningful Use
• Quality Guidance
44

National Quality Recognition
• Goal: 100% of Health Centers strive to receive national quality recognition, starting with 25 percent of grantees by 2013
• Where are we? – Accreditation (~25%) – Patient Centered Medical Home Recognition (16
grantees representing 46 sites) o Enhance access & continuity o Track and coordinate care o Identify and manage patient populations o Provide self care support & community resources o Track and coordinate care
45

National Quality Recognition
• Additional NQR Initiatives – FY2011 PCMH Supplemental Funding
o 904 Grantees Awarded – CMS Advanced Primary Care Demonstration
o 500 sites to be selected – PCMH Supplemental, NOI Requirement
46

FTCA
• Federal Tort Claims Act Deeming – Health centers and free clinics – New 2012 deeming requirements
o FTCA Policy Manual (PIN 2011-01) http://bphc.hrsa.gov/policiesregulations/policies/
pdfs/pin201101manual.pdf – ECRI Institute resources: Free and available to all!
o https://www.ecri.org/Pages/default.aspx
47

New Application Requirements
• Minutes from last six QI/QA committee meetings – Remove patient names and other identifiers
• Minutes from the last six Board meetings that reflect Board approval of QI/QA activities – Remove all information not related to QI/QA activity
• Board-approved Credentialing and Privileging policies – Must be signed and dated by the Board
48

New Application Requirements (continued)
§ Clinical policies and procedures for the following activities:
q Referral Tracking q Hospitalization Tracking q X-Ray Tracking q Lab Result Tracking
49

Additional Application Requirements
• A complete initial or redeeming application must include:
1. An Application Form completed in EHB 2. An approved Quality Improvement/Quality
Assurance Plan, including governing board signature and approval date
3. Summary of professional liability history for cases filed or closed within the last 5 years, if applicable
v Name of provider(s) involved v Area of practice/Specialty v Date of Occurrence v Summary of allegations v Status and outcome of claim
50

Additional Application Requirements (continued)
4. Explanation of any “NO” responses 5. Deeming applications for any sub-recipients (as
documented on the organization’s most recent approved scope from FORM 5B - see “sub-recipient submission instructions.”)
51

Additional Application Requirements (continued)
6. Credentialing list (in an excel spreadsheet) of all licensed and/or certified health care personnel employed and/or contracted by the health center, with the following information: o Name & Professional Designation (e.g., MD/DO, RN, CNM,
DDS) o Title/Position o Specialty o Employment Status (full-time employee, part-time
employee, contractor, volunteer) o Date of Hire o Initial Credentialing Date (the first time the individual was
credentialed by your organization) o Most Recent Credentialing Date o Next Expected Credentialing Date
52

Health Information Technology
• Health Information Technology – Coordinating adoption, meaningful use, health info
exchange – Health Center Controlled Networks
o 3 or more health centers o Increased buying power o Collaboration to improve access to care, enhance quality
of care, and achieve cost efficiencies. – Supplemental funding for health centers in Beacon
communities o Part of the HITECH Act o Comprised of different health care systems, clinicians,
payers, employers, patient advocates, and IT leaders
53

Adoption and Meaningful Use of HIT
• Goal: 100% of Health Centers meaningfully use a certified EHR system – 50.7% report having EHR in use at all sites for all providers, and
14.1% report having EHR in use at some sites or for some providers.
• Where are we? – Baseline data collection – EHR questions in UDS, HCs participating
in HCCNs – Other data sources – REC program, GW/NACHC Survey, NAMCS
survey
• Strategy – Support for and TA from HCCNs/PCAs/NACHC.
• Partnerships/Collaborations – CMS EHR Incentive Program – ONC REC Program, State HIE Program, Beacon Communities,
Community College Program 54

Other Focus Areas
• Patient experience measurement • The role of mental health and substance abuse
services in the medical home – SAMHSA/HRSA Center for Integrated Health Solutions
• Integration with local health care, public health, and social services landscape
• Telehealth • National priorities: tobacco, healthy weight, HIV,
oral health • Supporting Affordable Care Act implementation
and delivery system reform 55

Conclusion
• Focus on quality • Support for planning and implementation of
Quality Improvement strategies – QI Plan Learning Series – Further guidance – Resources and technical assistance – Third-party quality recognition
• Invest in your QI infrastructure – Clinical quality and beyond
• Effectively use your data to achieve your goals • Focus on implementation
– This work never ends 56

Resources
• Technical assistance through HRSA, NCAs • Third-party quality recognition
– Accreditation: http://bphc.hrsa.gov/policiesregulations/accreditation.html
o AAAHC, TJC – NCQA recognition: http://bphc.hrsa.gov/policiesregulations/
policies/pal201101.html
– Comparison chart: http://bphc.hrsa.gov/policiesregulations/policies/qualrecogn.pdf
57

QI Resources
• HRSA – FTCA website http://bphc.hrsa.gov/ftca/
index.html
– BPHC QI Plan Learning Series and Modules http://bphc.hrsa.gov/policiesregulations/quality/index.html
– BPHC Office of Training and Technical Assistance http://bphc.hrsa.gov/technicalassistance/tatopics/qualitymanagementimprovement/index.html
– HRSA Office of HIT and Quality http://www.hrsa.gov/quality/toolsresources.html
– HIV/AIDS bureau http://nationalqualitycenter.org/
• Safety Net Medical Home Initiative http://www.qhmedicalhome.org/safety-net/qistrategy.cfm
58

PCMH Resources
– Agency for Healthcare Research and Quality (AHRQ) PCMH Resource Center: http://www.pcmh.ahrq.gov/portal/server.pt/community/pcmh__home/1483
o Clinical Practice Guidelines: http://www.ahrq.gov/clinic/cpgsix.htm
o US Preventative Services Task Force: http://www.uspreventiveservicestaskforce.org/tools.htm
o Consumer Assessment of Healthcare Providers and Systems (CAHPS patient experience survey): https://www.cahps.ahrq.gov/default.asp
o Innovations Exchange: http://www.innovations.ahrq.gov/
o Patient Health literacy toolkit: http://www.ahrq.gov/qual/literacy/
– Patient-Centered Primary Care Collaborative (PCPCC): http://www.pcpcc.net/content/pcmh-outcome-evidence-quality
59

Contributors
• Emily Jones, MPP – Public Health Analyst – Quality Branch, BPHC/OQD
• Harriet McCombs, Ph.D – Senior Public Health Analyst – Quality Branch, BPHC/OQD
• Christopher Gibbs, JD, MPH – Public Health Analyst – FTCA Branch, BPHC/OQD
• Michael Witte, MPH – Public Health Analyst – HIT Branch, BPHC/OQD
60

Contact Information
Nina Brown, MPH, CHES Public Health Analyst
Office of Quality and Data Quality Branch
Bureau of Primary Health Care Health Resources and Services Administration
301-443-1921 [email protected]
61