Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.

of 11
-
Upload
lourdes-fernandez-cabrera -
Category
Documents
-
view
214 -
download
0
Transcript of Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
1/11
Enhancing Information Pertaining to Client Characteristics
to Facilitate Evidence-Based Practice
Jennifer L. Callahan,1 Christopher J. Heath,1 Nicki L. Aubuchon-Endsley,2
Frank L. Collins Jr.,1 and Gregory L. Herbert1
1University of North Texas2Alpert Medical School of Brown University
Objective: Evidence-based practice (EBP) includes utilization of empirically supported treatments,application of clinical expertise, and consideration of client characteristics. The following brief report
aims to elucidate barriers in the study and dissemination of research regarding these client char-
acteristics. Design: Authors examined empirical papers cited on psychologicaltreatments.org(N = 338) and categorized each according to efficacy evidence available pertaining to gender,
race/ethnicity, and socioeconomic status (SES). Results: Gender was most commonly consid-ered (7% of studies), with less than 2% of studies analyzing efficacy in relation to race/ethnicity or
SES. Conclusions: Available findings are summarized according to disorder. Researchers areencouraged to attend to client variables in efficacy studies and suggestions are offered for training
students to include client variables in EBP. C 2013 Wiley Periodicals, Inc. J. Clin. Psychol. 00:125,
2013.
Keywords: evidence-based practice; client variables; psychological treatments; dissemination
The evidence-based practice (EBP) movement dominates health care today and unites
practitioners and clinical scientists in a range of health care disciplines. Psychologists have
identified evidence-based psychological practice (EBPP) as the integration of the best available
research with clinical expertise in the context of client characteristics, culture, and preferences
(American Psychological Association [APA], 2005, p. 1). This approach sets a high bar forcompetent practice of professional psychology that serves to protect the public. The EBP
movement is relatively recent, rooted in trends toward increasing accountability for medical
outcomes in the United Kingdom (Wampold & Bhati, 2004).
In the United States, EBP in psychotherapy first became salient during the 1990s with APAs
Division 12 (Society of Clinical Psychology) Task Force on Promotion and Dissemination of
Psychological Procedures (APA, 1993). The task force outlined the importance of identifying
and utilizing Empirically Validated Psychological Treatments in addition to the effect of these
treatments on clinician training and third-party payers. Though recent, the EBP movement is
complicated and expansive. Thus, a comprehensive outline of its history is beyond the scope of the
current article. However, the current article does address existing problems with dissemination
of research on EBP (Addis, Wade & Hatgis, 2006; Gallo & Barlow, 2012; Kendall & Beidas,2007) specifically related to client variables within EBP.
The facilitation of widespread application of EBP can be achieved only by careful management
of evidence dissemination (McCabe, 2004), and many professional organizations are working
towards this goal (McHugh & Barlow, 2010). Both the Substance Abuse and Mental Health
Services Administration (SAMSHA) and Centers for Disease Control and Prevention (CDC)
provide extensive information about their funded treatment projects. However, these sites are
limited by not considering unfunded research.
Further, the CDC website (http://www.cdc.gov/DiseasesConditions/) contains little infor-
mation of use for mental health evidence dissemination, while the use of the Diagnostic and
Please address correspondence to: Jennifer L. Callahan, Department of Psychology, University of NorthTexas, 1155 Union Circle #311280, Denton TX 76203-5017. E-mail: [email protected]
*Posthumous.
JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 00(00), 125 (2013) C 2013 Wiley Periodicals, Inc.
Published online in Wiley Online Library (wileyonlinelibrary.com/journal/jclp). DOI: 10.1002/jclp.21995
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
2/11
2 Journal of Clinical Psychology, XXX 2013
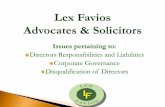
Figure 1. The intersecting roles of research evidence, patient characteristics, and practitioner expertisein forming clinical decisions that characterize evidence-based practice within a given context (adaptedfrom Spring, B., Walker, B., Brownson, R., Mullen, E., Newhousc, R., et al. [July, 2008]. Defini-tion and competencies for evidence-based behavioral practice (EBBP). Retrieved from http://ebbp.org/documents/EBBP_Competcncies.pdf)
Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) diagnostic labels is limited on
the SAMSHA website (http://www.nrepp.samhsa.gov/find.asp). The site allows for advanced
search by client characteristics, which is commendable. APAs Division 12 has also organized
evidence for dissemination on psychologicaltreatments.org. This website is organized by di-
agnosis, citing hundreds of efficacy studies. It serves to identify the best available research
evidence for common psychological disorders and explicitly reminds users that this evidence
will necessarily be combined with clinician expertise and client values and characteristics in
determining optimum approaches to treatment. However, accomplishing this integration ofeffective treatments, expertise, and client variables is challenging. Research consumers must de-
cide what to read and whether findings should change their practice (Gross & Johnston, 2009;
Stewart, Chambless, & Baron, 2012).
Following these decisions, practitioners must use their clinical expertise to determine if ev-
idence presented is relevant for particular individuals (Mazzucchelli & Sanders, 2010). As in
Figure 1, EBP requires that clinical decisions incorporate the best available research evidence
with client/population characteristics, state, needs, values, and preferences, and resources,
including practitioner expertise.
Therefore, to move toward EBP, we must also consider the relationship of client characteristics
to treatment efficacy. In particular, prevalence rates for various mental health issues (e.g., Axis
II disorders; Golomb, Fava, Abraham, & Rosenbaum, 1995) may be a function of gender.Psychopathology may also vary as a function of socioeconomic status (SES), ethnicity, and
a range of other individual variables (Dohrenwend et al., 1992; Nguyen, Huang, Arganza, &
Liao, 2007). A risk to successful delivery of EBP is to become focused on empirically supported
treatments (ESTs) to an extent that important components of EBP are neglected. Although
ESTs are important, they contribute only one component of EBP.
The current article attempts to gather findings regarding individual differences and their
effects on psychotherapy outcomes. Although knowing the answers to these questions would
not address all components of EBP, it would move the discussion beyond a focus on treatment
evidence towards comprehensive foreground questions that inform clinical practice with indi-
viduals. This review examined accessible empirical studies cited on psychologicaltreatments.org
to assist practitioners in responding to such foreground questions. Each study was consideredwith respect to gender, race/ethnicity, and SES, and those providing supporting evidence for
treatment efficacy were summarized.
Each study was examined to determine if there was: insufficient (not reported) informa-
tion regarding client diversity; insufficient diversity (10% of reported N) but no corresponding efficacy
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
3/11
Facilitating EBP Via Information Disemmination 3
analyses; inclusion of diversity in efficacy analyses with a finding of significant differences by
group; or evidence that the treatment was equally effective (no significant group differences)
for diverse clients. See Appendices for summary.
Overall Patterns Observed in the Cited Studies
Fully 93% (N= 315) of studies did not examine gender differences. Disorders that contained no
cited gender difference studies included borderline personality disorder (BPD), generalized anx-
iety disorder (GAD), obsessive-compulsive disorder (OCD), and specific phobia. Cited studies
for BPD included only women. Citations for the remaining disorders described adequate gender
representation to examine differences. The few studies examining differential treatment efficacy
by gender report no significant differences (see Table A1). However, multicomponent cognitive-
behavioral therapy for rheumatologic pain (Keefe et al., 1990a, 1990b) and reminiscence/life
review therapy for depression (Fry, 1983) were more effective for women.
Five studies addressed treatment efficacy as a function of race/ethnicity (1.5%; see Table A2).
The Robinson-Wheelan et al. (2007) study results revealed that self-management/self-control
therapy for depression was effective across groups. Similarly, efficacy of behavior ther-apy/behavior activation treatment of depression was found to be independent of race/ethnicity
(Arean et al., 2005). With respect to schizophrenia, race/ethnicity did not significantly co-vary
with treatment efficacy of cognitive adaptation training (Velligan et al., 2000; Velligan et al.,
2002). Finally, Davidson and colleagues (2004) reported no differences in efficacy between Cau-
casian and racial/ethnic minority clients for cognitive and behavioral therapy for social phobia.
Few studies (N= 4; 1.2%), evaluated SES differences in treatment efficacy (see Table A3).
No differences were found in family-focused therapy for bipolar disorder (Miklowitz, George,
Richards, Simoneau, & Suddath, 2003), self-management / self-control therapy for depression
(Robinson-Whelen, Hughes, Taylor, Hall, & Rehm, 2007), behavioral weight loss treatment
for obesity and pediatric overweight (Israel, Silverman, & Solotar, 1986), or eye movement
desensitization and reprocessing for posttraumatic stress disorder (PTSD; Wilson, Becker, &Tinker, 1995). Most studies were noted as containing insufficient information. Although many
recent studies included information about education or employment status, this was not sufficient
for characterizing SES.
Disorder Specific Findings
Tables A4 thru A16 provide details on all empirical studies cited on the Division 12 website,
clustered into tables by disorder. Several listed disorders did not inform foreground questions.
However, eight disorders included one or more treatment(s) that evaluated client characteristics,
which are summarized below.
Regarding bipolar disorder, differential prevalence rates have not been established based onrace, ethnicity, or gender although gender may play a role in the number, type, and onset of manic
and major depressive episodes (American Psychiatric Association, 2000). Prevalence, however,
does vary by age (6% of U.S. adults aged 1829 years, 5% aged 3044 years, 5% aged 4559 years,
and 1% aged 60+ years; Kessler et al., 2005). Three studies from the website showed support
of treatment efficacy independent of gender, including family-focused therapy (Miklowitz et al.,
2003; Rea et al., 2003) and interpersonal and social rhythm therapy (Frank et al., 2005). Most
studies (18 of 21 studies; 86%) failed to examine gender differences, examined one gender, or
provided insufficient information in the methods to provide support. One study showed support
independent of SES (family-focused therapy; Miklowitz et al., 2003) and no studies addressed
race/ethnicity.
Depression prevalence varies by gender (70% more likely in women), race (40% more likelyin White, non-Hispanic individuals than Black, non-Hispanic individuals), and age (9% of U.S.
adults aged 1825 years, 7% aged 2649 years, and 5% aged 50+ years; Kessler et al., 2005).
Several studies found support for treatment of Depression independent of gender, including
behavior therapy/behavioral activation (Arean et al., 2005; Hopko, Lejuez, Lepage, Hokpo,
& McNeil, 2003), cognitive behavioral analysis system of psychotherapy (Klein et al., 2004;
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
4/11
4 Journal of Clinical Psychology, XXX 2013
Manber et al., 2003), interpersonal therapy (Reynolds et al., 1999), problem-solving therapy
(Reynolds et al., 1999), self-management/self-control therapy (Rokke, Tomhave, & Jocic, 2000),
and behavioral couple therapy (Christensen, Atkins, Yi, Baucom, & George, 2006).
As noted above, reminiscence/life review therapy found greater efficacy for women. Only two
treatments, behavior therapy/behavior activation (Arean et al., 2005) and self-management/self-
control therapy (Robinson-Whelen et al., 2007) examined race/ethnicity influences on treatmentefficacy. Both studies found treatment to be equally effective for Caucasian and ethnic minority
clients. Self-management/self-control therapy (Robinson-Whelen et al., 2007) was also found to
be equally effective regardless of SES.
Eating disorder prevalence varies by demographic characteristics depending on the specific
disorder. Prevalence of anorexia nervosa, bulimia nervosa, and binge eating disorder is two to
three times greater in women and more likely in industrialized societies (Hudson, Hiripi, Pope, &
Kessler, 2007). Although the incidence of anorexia nervosa does not appear to vary by age, those
younger than 60 years of age are significantly more to develop bulimia nervosa and binge eating
disorder compared with other age groups (Hudson et al., 2007). Studies supported behavioral
weight loss for obesity and pediatric overweight as equally effective across gender (Tuomilehto
et al., 2001; Wing, Blair, Marcus, Epstein, Harvey, 1994) and not differentially influenced byparental SES (Israel et al., 1986).
EMG biofeedback was found to be equally effective for insomnia in women and men
(Barrowsky, Moskowitz, & Zweig, 1990), despite a greater prevalence of the disorder in women.
Psychoanalytic treatment for panic disorder was also equally effective for both women and men,
though there is a greater incidence of diagnosis in women (Milrod et al., 2007). Eye movement
desensitization and reprocessing therapy for PTSD was equally effective across gender and SES
categories (Wilson et al., 1995). Cognitive adaptation training for schizophrenia was equally
effective for men and women, independent of race/ethnicity (Velligan et al., 2000; Velligan
et al., 2002), although it is manifested differently by gender. Treatment effects were independent
of gender and race/ethnicity for cognitive and behavioral therapy for social phobia (Davidson
et al., 2004) and independent of gender for cognitive therapy (Clark et al., 2003), even thoughSocial Phobia is more common in women.
Discussion
The goal of the current study was to assist practitioners as they aim to provide high quality
EBP. However, as we carried out the study, we came to more fully appreciate the frequent lack
of consideration of client characteristics by researchers studying treatment efficacy. Overall,
evidence for treatment efficacy rarely addresses foreground questions of gender, race/ethnicity,
or SES. This is unfortunate as client variables reflect a range of factors contributing to individ-
ual uniqueness. Such variables may include the clients presenting problems (e.g., variations in
etiology, symptoms, behavior, etc.), views of treatment (e.g., readiness to change, preferences,expectations, etc.), sociocultural and familial factors (e.g., religion, values, beliefs, etc.), environ-
mental factors (e.g., employment, major life events, etc.), or other factors like age or development
level (APA, 2006).
While research indicates that client characteristics play an important role in treatment out-
comes (see Clarkin & Levy, 2004; Zane, Sue, Young, Nunez, & Hall, 2004) and should be
incorporated in EBP to treat individuals (Beutler, Forrester, Gallagher-Thompson, Thompson,
& Tomlins, 2012), the tables provided in Appendices support that client variables are frequently
overlooked in research. It is not possible to determine from these data whether practitioners also
overlook these variables. In the absence of such information, it may be helpful for practitioners
to keep in mind a few easily recalled findings from broad psychotherapy literature that are not
evident from studies considered in this review.
Client Variables in the Broad Literature
Age and gender. Consideration of client characteristics reveals that, among adults, ageis not strongly related to treatment retention or outcome in the broad psychotherapy literature
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
5/11
Facilitating EBP Via Information Disemmination 5
(Dubrin & Zastowny, 1988; Sledge, Moras, Hartley, & Levine, 1990). Although, more recently it
has been reported that younger individuals are more likely to have used mental health services and
report greater likelihood of using such services in the future (Smith, Peck, & McGovern 2004).
Similarly, research generally reveals no gender differences in therapy outcome in adults
(Garfield, 1994; Petry, Tennen, & Affleck, 2000), with some exceptions pertaining to treat-
ment for depression (Thase, Frank, Kornstein, & Yonkers, 2000) or substance abuse disorders(Blood & Cornwall, 1994; Rivers, Greenbaum, & Goldberg, 2001). Recent reports do indicate
that gender may influence clients willingness to initiate treatment and evaluation of treatment
options (Green, Polen, Dickinson, Lynch, & Bennett, 2002; Smith, Peck, & McGovern, 2004).
Race and ethnicity. For racial and ethnic minority clients, research suggests that theworking alliance (connection between client and practitioner with respect to goals, tasks, and
bond; Gelso & Hayes, 1998) may be especially important in fostering positive outcomes, and
some approaches may foster more positive alliances (e.g., Duan & Wang, 2000; Ortega & Alegra,
2002; Wong, Kim, & Zane, 2003). Other research suggests that the impact of therapist attitude
on treatment outcomes might be related to SES, rather than ethnicity (Lerner, 1972).
Demeanor. Beyond demographics, it is also important in EBP to consider client variableslike demeanor and preferences. Thornton et al. (2003) reported that behaviorally oriented,
structured treatments worked better with clients who had a helpless demeanor, while a less
structured, facilitative treatment milieu was found to be more efficacious for others.
Preferences. Swift and Callahan (2009) conducted a meta-analytic review summarizingdata from 26 studies including 2,300 clients and found that those who received preferred treat-
ment were half as likely to drop out and had a 58% chance of showing greater improvement.
They also found that study design served as a moderator, causing partially randomized pref-
erence trials to likely underestimate the effect of client treatment preferences. A subsequent
meta-analysis (Swift, Callahan, & Vollmer, 2011) replicated this finding. Meta-regression of thisdata found that client preferences are important to all clients, regardless of age, gender, ethnicity,
educational level, or marital status (Swift, Callahan, Ivanovic, & Kominiak, 2013).
The current article illustrates the dearth of research related to the influence of client
variables on treatment outcomes. The information presented is often characterized by false
dichotomies (e.g., ethnicity treated as Caucasian/not Caucasian). Additionally, gender is
presented as dichotomous despite evidence that this construct may not accurately reflect gender
identity (Lorber, 1995). These dichotomies prevent a nuanced understanding of the literature
and reflect difficulties in collecting representative samples. Increased understanding of these
non-dichotomous constructs will allow for more clinically applicable findings in research. The
efficacy of a psychological treatment with any given individual is even far more complicated.
The requirement of clinical expertise in true EBP underscores the challenge in competentlybridging the nomothetic-idiographic divide when engaged in professional practice. Although
consideration of clinical expertise variables in EBP is beyond the scope of this review (though
we encourage this to complement the existing Division 12 website and the current study tables in
appendices), we wish to conclude by offering a few suggestions on training of students in EBP.
Promoting Client Variables During Training in EBP
Training students to integrate client variables into EBP can be challenging because they often are
highly desirous of learning ESTs and are prone to mistakenly conclude that using an EST is EBP.
The lack of attention to client variables in the cited studies on the psychologicaltreatments.org
website may inadvertently reinforce the mistaken perception by students that use of an EST is
EBP. This lack of distinction between EST and EBP may not be unique to students.A number of studies and literature reviews substitute the term evidence-based practice with
other terms (e.g., Chambless & Ollendick, 2001), thereby possibly adding to definitional confu-
sion. Westen and colleagues (Westen, Novotnoy & Thompson-Brenner, 2004; Westen & Bradley,
2005) highlight that although ESTs are often seen as the fundamental basis of EBP, they com-
prise only one component of EBP. This ignores other aspects of psychotherapy practice and
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
6/11
6 Journal of Clinical Psychology, XXX 2013
research that contribute to EBP such as common factors (Wampold & Bhati, 2004) and client
treatment preferences (Swift & Callahan, 2009). True adherence to EBP guidelines must account
for these and other research/factors in treatment provision, which should also be incorporated
into training (Spring, 2007).
Aside from encouraging a range of practicum experiences that bring students into contact
with a variety of clients from diverse backgrounds, characteristics, values, and preferences, wesuggest formal instruction in shared decision-making in clinical practice (Adams & Drake,
2006). A collaborative interaction between therapist and client should be emphasized with both
influencing treatment decisions (Beutler et al., 2012; Ford, Schofield, & Hope, 2003).
Four components are inherent to successful application of the shared decision-making model:
(a) two parties are involved, (b) both share information, (c) both discuss preferences for treat-
ment, and (d) an agreement is reached as to implement treatment (Charles, Whelan, Gafni,
Willan, & Farrell, 2003). The use of a shared decision-making model coupled with diverse
practicum experiences may further trainee development in EBP. Practicum supervisors are
strongly encouraged to routinely discuss client and trainee values, preferences, goals, plans,
progress, etc., during supervision, especially when treatment decisions are considered. In con-
trast, supervisors are discouraged from simply monitoring treatment adherence (an importantpart of effective EST supervision) as the sole indicator of EBP.
Promoting Client Variables With Lifelong Learning in EBP
EBP also requires lifelong learning via consumption of research (Spring, 2007). To facilitate this,
we suggest that practitioners specifically attend to client characteristics information as research
consumers. Lifelong learning could be promoted by encouraging future research regarding EPBs
at the division, professional societies, and other levels. Additionally, dissemination of updates
to research in EBPs should be encouraged at conferences in addition to associated clinical
trainings. It is also vital to recognize that publication bias limits dissemination of psychotherapy
research (Song et al., 2010), suggesting that greater emphasis on null or unpublished findingsmay be particularly helpful. In particular, research consumers and reviewers should encourage
investigators to publish their broad range of findings.
Finally, with respect to dissemination efforts, organizations should include pertinent client
information (e.g., Division 12 could add a section to each disorders page) or create dynamic
websites that allow for searching according to client characteristics or embed within sites the
necessary programming code to open and simultaneously search other databases.
In sum, the lack of research addressing the effect of client variables currently prevents reliably
generalizable conclusions being drawn from papers reviewed. The dearth of investigation into
these variables is therefore identified as a vital area for growth within the larger sphere of
psychotherapy research.
References
Adams, J. R., & Drake, R. E. (2006). Shared decision-making and evidence-based practice: A commentary.
Community Mental Health, 42, 87105. doi:10.1007/s10597-005-9011-x.
Addis, M. E., Wade, W. A., & Hatgis, C. (2006). Barriers to dissemination of evidence-based practices:
Addressing practitioners concerns about manual-based psychotherapies. Clinical Psychology: Science
and Practice, 6(4), 430441. doi:10.1093/clipsy.6.4.430
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.,
text rev.). Washington, DC: Author.
American Psychological Association. (2005). Policy statement on evidence-based practice in psychology.
Retrieved from http://search.apa.org/search?query=Policy%20statement%20of%20evidence-based%20practice%20in%20psychology
American Psychological Association, Division 12. (1993). Task force on promotion and dissemination of
psychological procedures. Retrieved from http://www.apa.org/divisions/div12/est/chamble2.pdf
American Psychological Association Presidential Task Force on Evidence-Based Practice. (2006). Evidence-
based practice in psychology. American Psychologist, 61, 271285. doi:10.1037/0003-066X.61.4.271
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
7/11
Facilitating EBP Via Information Disemmination 7
Arean, P. A., Gum, A., McCulloch, C. E., Bostrom, A., Gallagher-Thompson, D., & Thompson, L.
(2005). Treatment of depression in low-income older adults. Psychology and Aging, 20, 601609.
doi:10.1037/0882-7974.20.4.601
Barrowsky, E. I., Moskowitz, J., Zweig, J. B. (1990). Biofeedback for disorders of initiating and main-
taining sleep. Annals of the New York Academy of Sciences, 602, 97103. doi:10.1111/j.1749-
6632.1990.tb22731.xBeutler, L. E., Forrester, B., Gallagher-Thompson, D., Thompson, L., & Tomlins, J. B. (2012). Common,
specific, and treatment fit variables in psychotherapy outcome. Journal of Psychotherapy Integration,
22(3), 255281. doi:10.1037/a0029695
Blood, L., & Cornwall, A. (1994). Pretreatment variables that predict completion of an adolescent substance
abuse treatment program. Journal of Nervous and Mental Disease, 182, 1419. doi:10.1097/00005053-
199401000-00004
Chambless, D. L. & Ollendick, T. H. (2001). Empirically supported psychological interventions: Controver-
sies and evidence. Annual Review of Psychology, 52, 685716. doi:0066-4308/01/0201-0685
Charles, C. A., Whelan, T., Gafni, A., Willan, A., & Farrell, S. (2003). Shared treatment de-
cision making: What does it mean to physicians? Journal of Clinical Oncology, 21, 932936.
doi:10.1200/JCO.2003.05.057
Christensen, A., Atkins, D. C., Yi, J., Baucom, D. H., & George, W. H. (2006). Couple and individ-
ual adjustment for two years following a randomized clinical trial comparing traditional versus in-
tegrative behavioral couple therapy. Journal of Consulting and Clinical Psychology, 74, 11801191.
doi:10.1037/0022-006X.74.6.1180
Clark, D. M., Ehlers, A., McManus, F., Hackmann, A., Fennell, M., Campbell, H., . . . Louis, B. (2003).
Cognitive therapy versus fluoxetine in generalized social phobia: A randomized placebo-controlled trial.
Journal of Consulting and Clinical Psychology, 71, 10581067. doi:10.1037/0022-006X.71.6.1058
Clarkin, J. F., & Levy, K. N. (2004). The influence of client variables on psychotherapy. In M. J. Lambert
(Ed.), Bergin and Garfields handbook of psychotherapy and behavior change (5 th ed., pp. 194226).
New York, NY: Wiley.
Davidson, J. R. T., Edna, B., Hupperty, J. D., Keefe, F. J., Franklin, M. E., Compton, J. S., . . . Gadde,
K. S. (2004). Fluoxetine, comprehensive cognitive behavioral therapy, and placebo in generalized socialphobia. Archives of General Psychiatry, 61, 10051013. Retrieved from www.archgenpsychiatry.com
Dohrenwend, B. P., Levav, I., Shrout, P. E., Schwartz, S., Naveh, G., Link, B. G., Skodol, A. E., & Steuve,
A. (1992). Socioeconomic status and psychiatric disorders: The causation-selection issue. Science, 255,
946952. doi:10.1126/science.154629
Duan, C., & Wang, L. (2000). Counseling in the Chinese cultural context: Accommodating both
individualistic and collectivistic values. Asian Journal of Counseling, 7, 121. Retrieved from
http://www.fed.cuhk.edu.hk/en/ajc/0701/
Dubrin, J. R., & Zastowny, T. R. (1988). Predicting early attrition from psychotherapy: An analysis of a
large private practice cohort. Psychotherapy, 25, 393408. doi:10.1037/h0085361
Ford, S., Schofield, T., & Hope, T. (2003). What are the ingredients for a successful evidence-based client
choice consultation?: A qualitative study. Social Science & Medicine, 56, 589602. doi:10.1016/S0277-9536(02)00056-4
Frank, E., Kupfer, D. J., Thase, M. E., Mallinger, A. G., Swartz, H. A., Fagiolini, A. M., . . . Monk, T.
(2005). Two-year outcomes for interpersonal and social rhythm therapy in individuals with bipolar I
disorder. Archives of General Psychiatry, 62, 9961004. doi:10.1001/archpsyc.62.9.996
Fry, P. S. (1983). Structured and unstructured reminiscence training and depression among the elderly.
Clinical Gerontologist, 1, 1537. doi:10.1300/J018v01n03_06
Gallo, K. P., & Barlow, D. H. (2012). Factors involved in clinician adoption and nonadoption of
evidence-based interventions in mental health. Clinical Psychology: Science & Practice, 19(1), 93106.
doi:10.1111/j.1468-2850.2012.01276.x
Garfield, S. L. (1994). Research on client variables in psychotherapy. In S. L. Garfield & A. E. Bergin (Eds.),
Handbook of psychotherapy and behavior change (4th ed., pp. 72113). New York, NY: John Wiley.
Gelso, C. J., & Hayes, J. A. (1998). The psychotherapy relationship: Theory, research and practice (pp.
2246). New York, NY: John Wiley.
Golomb, M., Fava, M., Abraham, M., & Rosenbaum, J. F. (1995). Gender differences in personal-
ity disorders. The American Journal of Psychiatry, 152(4), 579582. Retrieved from Retrieved from
http://ajp.psychiatryonline.org
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
8/11
8 Journal of Clinical Psychology, XXX 2013
Green, C. A., Polen, M. R., Dickinson, D. M., Lynch, F. L., & Bennett, M. D. (2002). Gender differences in
predictors of initiation, retention, and completionin an HMO-basedsubstance abuse treatment program.
Journal of Substance Abuse Treatment, 23, 285295. doi:10.1016/S0740-5472(02)00278-7
Gross, R. A., & Johnston, K. C. (2009). Levels of evidence: Taking Neurology R to the next level. Neurology,
72, 810. doi:10.1212/01.wnl.0000342200.58823.6a
Hopko, D. R., Lejuez, C. W., Lepage, J. P., Hopko, S. D., & McNeil, D. W. (2003). A brief behavioralactivation treatment for depression: A randomized pilot trial within an inpatient psychiatric hospital.
Behavioral Modification, 27, 458469. doi:10.1177/0145445503255489
Hudson, J. I., Hiripi, E., Pope, H. G., & Kessler, R. C. (2007). The prevalence and correlates
of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry, 61,
34858.
Israel, A. C., Silverman, W. K., & Solotar, L. C. (1986). An investigation of family influences on initial
weight status, attrition, and treatment outcome in a childhood obesity program. Behavior Therapy, 17,
131143. doi:10.1016/S0005-7894(86)80081-8
Keefe, F. J., Caldwell, D. S., Williams, D. A., Gil, K. M., Mitchell, D., Robertson, C., . . . Helms, M. (1990a).
Pain coping skills training in the management of osteopathic knee pain: A comparative study. Behavior
Therapy, 21, 4962. doi:10.1016/S0005-7894(05)80188-1
Keefe, F. J., Caldwell, D. S., Williams, D. A., Gil, K. M., Mitchell, D., Robertson, C., . . . Helms, M. (1990b).
Pain coping skills training in the management of osteopathic knee pain-II: Follow-up results. Behavior
Therapy, 21, 435447. doi:10.1016/S0005-7894(05)80357-0
Kendall, P. C., & Beidas, R.S. (2007). Smoothing trail for dissemination of evidence-based practices
for youth: Flexibility within fidelity. Professional Psychology: Research and Practice, 38(1), 1320.
doi:10.1037/0735-7028.38.1.13
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime
prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey
Replication (NCS-R). Archives of General Psychiatry, 62(6), 593602.
Klein, D. N., Santiago, N. J., Vivian, D., Arnow, B. A., Blalock, J. A., Dunner, D. L., . . . Keller, M. B. (2004).
Cognitive behavioral analysis system of psychotherapy as a maintenance treatment for chronic depres-
sion. Journal of Consulting and Clinical Psychology, 72, 681688. doi:10.1037/0022-006X.72.4.681Lerner, B. (1972). Therapy in the ghetto. Baltimore, MD: Johns Hopkins University Press.
Lorber, J. (1995). Paradoxes of gender. New Haven, CT: Yale University Press.
Manber, R., Arnow, B. A., Blasey, C., Vivian, D., McCullough, J. P., Blalock, J. A., . . . Keller, M. B.
(2003). Clients therapeutic skill acquisition and response to psychotherapy, alone and in combination
with medication. Journal of Psychological Medicine, 33, 693702. doi:10.1017/S0033291703007608
Mazzucchelli, T. G., & Sanders, M. R. (2010). Facilitating practitioner flexibility within an empirically
supported intervention: Lessons from a system of parenting support. Clinical Psychology: Science &
Practice, 17(3), 238252. doi:10.1111/j.14682850.2010.01215.x
McCabe, O. L. (2004). Crossing the quality chasm in behavioral health care: The role of evidence-based
practice. Professional Psychology: Research & Practice, 35, 571. doi:10.1037/0735-7028.35.6.571
McHugh, R., & Barlow, D. H. (2010). The dissemination and implementation of evidence-based psycholog-ical treatments: A review of current efforts. American Psychologist, 65(2), 7384.
Miklowitz, D. J., George, E. L., Richards, J. A., Simoneau, T. L., & Suddath, R. L. (2003). A randomized
study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar
disorder. Archives of General Psychiatry, 60, 904912. doi:10.1001/archpsyc.60.9.904
Milrod, B., Leon, A. C., Busch, F., Rudden, M., Schwalberg, M., Clarkin, J., . . . Shear, M. K. (2007).
A randomized controlled clinical trial of psychoanalytic psychotherapy for panic disorder. American
Journal of Psychiatry, 164, 265272. doi:10.1176/appi.ajp.164.2.265
Nguyen, L., Huang, L. N., Arganza, G. F., & Liao, Q. (2007). The influence of race and ethnicity on psy-
chiatric diagnoses and clinical characteristics of children and adolescents in childrens services. Cultural
Diversity & Ethnic Minority Psychology, 13(1), 1825. doi:10.1037/1099-9809.13.1.18
Ortega, A. N., & Alegra, M. (2002). Self-reliance, mental health need, and the use of men-tal healthcare among Island Puerto Ricans. Mental Health Services Research, 4, 131140.
doi:10.1023/A:1019707012403
Petry, N. M., Tennen, H., & Affleck, G. (2000). Stalking the elusive client variable in psychotherapy research.
In C.R. Synder & R.E. Ingram (Eds.), Handbook of psychological change: psychotherapy processes and
practices for the 21st century (pp. 88108). New York, NY: John Wiley & Sons.
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
9/11
Facilitating EBP Via Information Disemmination 9
Rea, M. M., Tompson, M., Miklowitz, D. J., Goldstein, M. J., Hwang, S., & Mintz, J. (2003). Family focused
treatment vs. individual treatment for bipolar disorder: Results of a randomized clinical trial. Journal of
Consulting and Clinical Psychology, 71, 482492. doi:10.1037/0022-006X.71.3.482
Reynolds, C. F., Miller, M. D., Pasternak, R. D., Frank, E., Perel, J. M., & Cornes, C., . . . Kupfer, D. J.
(1999). Treatment of bereavement-related major depressive episodes in later life: A controlled study of
acute and continuation treatment with nortriptyline and interpersonal psychotherapy. American Journalof Psychiatry, 156, 202208. Retrieved from http://ajp.psychiatryonline.org
Rivers, S. M., Greenbaum, R. L., & Goldberg, E. (2001). Hospital-based adolescent substance abuse
treatment: Comorbidity, outcomes, and gender. Journal of Nervous and Mental Disease, 189, 229237.
doi:10.1097/00005053-200104000-00004
Robinson-Whelen, S., Hughes, R. B., Taylor, H. B., Hall, J. W., & Rehm, L. P. (2007). Depression self-
management program for ruralwomen with physical disabilities. Rehabilitation Psychology, 52, 254262.
doi:10.1037/0090-5550.52.3.254
Rokke, P. D., Tomhave, J. A., & Jocic, Z. (2000). Self-management therapy and educational group therapy
for depressed elders. Cognitive Therapy and Research, 24, 99119. doi:0.1023/A:1005407125992
Sledge, W. H., Moras, K., Hartley, D., & Levine, M. (1990). Effect of time-limited psychother-
apy on client dropout rates. American Journal of Psychiatry, 147, 13411347. Retrieved from
http://ajp.psychiatryonline.org/content/vol147/issue10/index.dtl
Smith, L. D., Peck, P. L., & McGovern, R. J. (2004). Factors contributing to the utilization of mental health
services in a rural setting. Psychological Reports, 95, 435442. doi:10.2466/PR0.95.6.435-442
Song, F., Parekh, S., Hooper, L., Loke, Y., Ryder, J., Sutton, A., . . . Harvey, I. (2010). Dissemination and
publication of research findings: an updated review of related biases. Health Technology Assessment,
14(8), 1220. doi:10.3310/hta14080
Spring, B. (2007). Evidence-based practice in clinical psychology: What it is, why it matters, what you need
to know. Journal of Clinical Psychology, 63(7), 611631. doi:10.1002/jclp.20373
Spring, B., Walker, B., Brownson, R., Mullen, E., Newhouse, R., Satterfield, J., . . . Hitchcock, K.
(2008). Definition and competencies for evidence-based behavioral practice (EBBP). Retrieved from
http://ebbp.org/documents/EBBP_Competencies.pdf
Stewart, R. E., Chambless, D. L., & Baron, J. (2012). Theoretical and practical barriers to practitionerswillingness to seek training in empirically supported treatments. Journal of Clinical Psychology, 68(1),
823. doi:10.1002/jclp.20832
Swift,J. K.,& Callahan, J. L. (2009). Theimpact of clienttreatment preferences on outcome: A meta-analysis.
Journal of Clinical Psychology, 65, 368381. doi:10.1002/jclp.20553
Swift, J. K., Callahan, J. L., Ivanovic, M., & Kominiak, N. (2013). Further examination of the psychotherapy
preference effect: a meta-regression analysis. journal of psychotherapy integration. Advance online
publication. doi: 10.1037/a0031423
Swift, J. K., Callahan, J. L., & Vollmer (2011). Preferences. Journal of Clinical Psychology: In Session, 67,
155165.
Thase, M. E., Frank, E., Kornstein, S., & Yonkers, K. A. (2000). Genderdifferences in response to treatments
of depression. In E. Frank (Ed.), Gender and Its effects on psychopathology (pp. 103129). Washington,DC: American Psychiatric Press.
Thornton, C. C., Patkar, A. A., Murray, H. W., Mannelli, P., Gottheil, E., Vergare, M. J., & Weinstein,
S. P. (2003). High- and low-structure treatments for substance dependence: Role of learned helplessness.
The American Journal of Drug and Alcohol Abuse, 29, 567584. doi:10.1081/ADA-120023459
Tuomilehto, J., Lindstrom, J., Eriksson, J. G., Valle, T. T., Hamalainen, H., Ilanne-Parikka, P.,
. . . Uusitupa, M. (2001). Prevention of type 2 diabetes mellitus by changes in lifestyle among
subjects with impaired glucose tolerance. New England Journal of Medicine, 344, 13431350.
doi:10.1056/NEJM200105033441801
Velligan, D. I., Bow-Thomas, C. C., Huntzinger, C., Ledbetter, N., Prihoda, T. J., & Miller, A. L.
(2000). Randomized controlled trial of the use of compensatory strategies to enhance adaptive
functioning in outpatients with schizophrenia. American Journal of Psychiatry, 157, 13171323.
doi:10.1176/appi.ajp.157.8.1317
Velligan, D. I., Prihoda, T. J., Ritch, J. L., Maples, N., Bow-Thomas, C. C., & Dassori, A. (2002). A
randomized single-blind pilot study of compensatory strategies in schizophrenia oupatients. Schizophre-
nia Bulletin, 28, 283292. Retrieved from http://schizophreniabulletin.oxfordjournals.org/content/
28/2.toc
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
10/11
10 Journal of Clinical Psychology, XXX 2013
Walker, B. B., & Thorn, B. E. (2008). Tips for trainers: Using evidence-based practice in the clinical
practicum. Paper presented at the midwinter meeting of the Council of University Directors of Clinical
Psychology, San Antonio, TX.
Wampold, B. E. & Bhati, K.S. (2004). Attending to theomissions: A historical examination of evidence-based
practice movements. Professional Psychology: Research and Practice. 35(6), 563570. doi:10.1037/0735-
7028.35.6.563Wampold, B. E., Imel, Z. E., & Miller, S. D. (2009). Barriers to the dissemination of empirically supported
treatments: Matching messages to the evidence. The Behavior Therapist, 32, 144155. Retrieved from:
http://www.abct.org/Members/?m=mMembers&fa=JournalsPeriodicals#sec3
Westen, D., & Bradley, R. (2005). Empirically supported complexity: Rethinking evidence-based practice
in psychotherapy. Current Directions in Psychological Science, 14(5), 266271. doi:10.1111/j.0963-
7214.2005.00378.x
Wilson, S. A., Becker, L. A., & Tinker, R. H. (1995). Eye movement desensitization and reprocessing
(EMDR) treatment for psychologically traumatized individuals. Journal of Consulting and Clinical
Psychology, 63, 928937. doi:10.1037/0022-006X.63.6.928
Wing, R. R., Blair, E., Marcus, M., Epstein, L. H., Harvey, J. (1994). Year-long weight loss treatment for
obese clients with type II diabetes: does including an intermittent very-low-calorie diet improve outcome?
American Journal of Medicine, 97, 354362. doi:10.1016/0002-9343(94)90302-6
Wong, E. C., Kim, B. S. K., Zane, N. W. S. (2003). Examining culturally based variables associated with
ethnicity: Influences on credibility perceptions of empirically supported interventions. Cultural Diversity
& Ethnic Minority Psychology, 9, 8896. doi:10.1037/1099-9809.9.1.88
Zane, S. H., Sue, S., Young, K., Nunez, J., & Hall, G. N. (2004). Research on psychotherapy with culturally
diverse populations. In M. J. Lambert (Ed.), Bergin and Garfields handbook of psychotherapy and
behavior change (5th ed., pp. 767804). New York, NY: Wiley.
Appendix
Table A1Gender
Bipolar disorder 3 0 16 1 1
BDP 0 0 0 8 0
Chronic pain 0 2 11 2 0
Depression 8 1 35 10 1Eating disorders 2 0 30 58 7
GAD 0 0 9 0 1
Insomnia 1 0 16 1 0
OCD 0 0 6 0 1
Panic 1 0 5 0 0
PTSD 1 0 2 12 0
Schizophrenia 2 0 26 5 2
Social phobia 2 0 18 1 2
Specific phobia 0 0 19 6 3
Notes. N= 338; Evidence for each group; Analyzed subgroups; Sufficient N, no analysis;
Insufficient N, < 10%; Insufficient information reported.BPD= borderline personality disorder; GAD= generalized anxiety disorder; OCD= obsessive-compulsive
disorder; PTSD = posttraumatic stress disorder.
-
7/30/2019 Enhancing Information Pertaining to Client Characteristics to Facilitate Evidence-Based Practice.
11/11
Facilitating EBP Via Information Disemmination 11
Table A2Race/Ethnicity
Bipolar disorder 0 0 6 4 11
BDP 0 0 3 1 4
Chronic pain 0 0 1 1 13
Depression 2 0 19 13 21
Eating disorders 0 0 30 16 51
GAD 0 0 1 2 7
Insomnia 0 0 3 2 13
OCD 0 0 0 1 6
Panic 0 0 2 1 3
PTSD 0 0 9 2 4
Schizophrenia 2 0 16 2 15
Social phobia 1 0 3 2 17
Specific phobia 0 0 2 1 25
Notes. N= 338; Evidence for each group; Analyzed subgroups; Sufficient N, no analysis;
Insufficient N, < 10%; Insufficient information reported.
BPD= borderline personality disorder; GAD= generalized anxiety disorder; OCD= obsessive-compulsive
disorder; PTSD = posttraumatic stress disorder.
Table A3SES
Bipolar disorder 1 0 5 0 15
BDP 0 0 2 0 6
Chronic pain 0 0 1 0 14
Depression 1 0 3 2 49
Eating disorders 1 0 9 0 87
GAD 0 0 0 0 10
Insomnia 0 0 0 0 18
OCD 0 0 0 0 7
Panic 0 0 0 0 6
PTSD 1 0 6 0 8
Schizophrenia 0 0 3 4 28
Social phobia 0 0 2 0 21
Specific phobia 0 0 2 0 26
Notes. N = 338; Evidence for each group; Analyzed subgroups; Sufficient N, no analysis;
Insufficient N, < 10%; Insufficient information reported.
BPD= borderline personality disorder; GAD= generalized anxiety disorder; OCD= obsessive-compulsive
disorder; PTSD = posttraumatic stress disorder.