Engaging and Retaining Abused Women in Perinatal Home ...aSchool of Nursing, and dBiostatistics,...
8
Engaging and Retaining Abused Women in Perinatal Home Visitation Programs abstract OBJECTIVES: Intimate partner violence (IPV) during pregnancy affects 0.9% to 17% of women and affects maternal health significantly. The impact of IPV extends to the health of children, including an increased risk of complications during pregnancy and the neonatal period, men- tal health problems, and cognitive delays. Despite substantial sequelae, there is limited research substantiating best practices for engaging and retaining high-risk families in perinatal home visiting (HV) programs, which have been shown to improve infant development and reduce maltreatment. METHODS: The Domestic Violence Enhanced Home Visitation Program (DOVE) is a multistate longitudinal study testing the effectiveness of a structured IPV intervention integrated into health department peri- natal HV programs. The DOVE intervention, based on an empowerment model, combined 2 evidence-based interventions: a 10-minute brochure- based IPV intervention and nurse home visitation. RESULTS: Across all sites, 689 referrals were received from participat- ing health departments. A total of 339 abused pregnant women were eligible for randomization; 42 women refused, and 239 women were randomly assigned (124 DOVE; 115 usual care), resulting in a 71% re- cruitment rate. Retention rates from baseline included 93% at delivery, 80% at 3 months, 76% at 6 months, and 72% at 12 months. CONCLUSIONS: Challenges for HV programs include identifying and retaining abused pregnant women in their programs. DOVE strategies for engaging and retaining abused pregnant women should be inte- grated into HV programs’ federal government mandates for the ap- propriate identification and intervention of women and children exposed to IPV. Pediatrics 2013;132:S134–S139 AUTHORS: Phyllis Sharps, PhD, RN, FAAN, a Jeanne L. Alhusen, PhD, CRNP, a Linda Bullock, PhD, RN, FAAN, b Shreya Bhandari, PhD, MSW, MS, c Sharon Ghazarian, PhD, d Ifeyinwa E. Udo, DrPH, MS, CPH, e and Jacquelyn Campbell, PhD, RN, FAAN a a School of Nursing, and d Biostatistics, Epidemiology and Data Management (BEAD) Core, Johns Hopkins University, Baltimore, Maryland; b University of Virginia School of Nursing, Charlottesville, Virginia; c Department of Social Work, Wright State University, Dayton, Ohio; and e Montgomery County Department of Health and Human Services, Rockville, Maryland KEY WORDS intimate partner violence, home visitation, Domestic Violence Enhanced Home Visitation Program, violence during pregnancy ABBREVIATIONS DOVE—Domestic Violence Enhanced Home Visitation Program HD—health department HV—home visitation IPV—intimate partner violence MIECHV—Maternal, Infant, and Early Childhood Home Visiting Program UC—usual care Drs Sharps and Bullock conceptualized and designed the study and drafted the Methods and Discussion sections of the manuscript; Dr Alhusen assisted with the interpretation of data, drafted the outline and introduction and the Discussion section of the manuscript, and critically reviewed and revised the manuscript; Dr Bhandari assisted in drafting the Discussion section; Dr Ghazarian carried out the initial analyses and reviewed and revised the manuscript; Ms Udo assisted with the initial analyses and reviewed and revised the manuscript; Dr Campbell assisted in the conceptualization and design of the study and drafted the Discussion section; and all authors approved the final manuscript as submitted. This trial has been registered with the NINR (identifier NCT00465556). www.pediatrics.org/cgi/doi/10.1542/peds.2013-1021L doi:10.1542/peds.2013-1021L Address correspondence to Phyllis Sharps, PhD, RN, FAAN, School of Nursing, Johns Hopkins University, 525 N. Wolfe Street, Baltimore, MD 21205. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: All phases of this study were supported by NIH/NINR grant R01009093. Funded by the National Institutes of Health (NIH). POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. S134 SHARPS et al by guest on January 29, 2020 www.aappublications.org/news Downloaded from
Transcript of Engaging and Retaining Abused Women in Perinatal Home ...aSchool of Nursing, and dBiostatistics,...

Engaging and Retaining Abused Women in PerinatalHome Visitation Programs
abstractOBJECTIVES: Intimate partner violence (IPV) during pregnancy affects0.9% to 17% of women and affects maternal health significantly. Theimpact of IPV extends to the health of children, including an increasedrisk of complications during pregnancy and the neonatal period, men-tal health problems, and cognitive delays. Despite substantial sequelae,there is limited research substantiating best practices for engagingand retaining high-risk families in perinatal home visiting (HV)programs, which have been shown to improve infant developmentand reduce maltreatment.
METHODS: The Domestic Violence Enhanced Home Visitation Program(DOVE) is a multistate longitudinal study testing the effectiveness ofa structured IPV intervention integrated into health department peri-natal HV programs. The DOVE intervention, based on an empowermentmodel, combined 2 evidence-based interventions: a 10-minute brochure-based IPV intervention and nurse home visitation.
RESULTS: Across all sites, 689 referrals were received from participat-ing health departments. A total of 339 abused pregnant women wereeligible for randomization; 42 women refused, and 239 women wererandomly assigned (124 DOVE; 115 usual care), resulting in a 71% re-cruitment rate. Retention rates from baseline included 93% at delivery,80% at 3 months, 76% at 6 months, and 72% at 12 months.
CONCLUSIONS: Challenges for HV programs include identifying andretaining abused pregnant women in their programs. DOVE strategiesfor engaging and retaining abused pregnant women should be inte-grated into HV programs’ federal government mandates for the ap-propriate identification and intervention of women and childrenexposed to IPV. Pediatrics 2013;132:S134–S139
AUTHORS: Phyllis Sharps, PhD, RN, FAAN,a Jeanne L.Alhusen, PhD, CRNP,a Linda Bullock, PhD, RN, FAAN,b ShreyaBhandari, PhD, MSW, MS,c Sharon Ghazarian, PhD,d
Ifeyinwa E. Udo, DrPH, MS, CPH,e and Jacquelyn Campbell,PhD, RN, FAANa
aSchool of Nursing, and dBiostatistics, Epidemiology and DataManagement (BEAD) Core, Johns Hopkins University, Baltimore,Maryland; bUniversity of Virginia School of Nursing,Charlottesville, Virginia; cDepartment of Social Work, WrightState University, Dayton, Ohio; and eMontgomery CountyDepartment of Health and Human Services, Rockville, Maryland
KEY WORDSintimate partner violence, home visitation, Domestic ViolenceEnhanced Home Visitation Program, violence during pregnancy
ABBREVIATIONSDOVE—Domestic Violence Enhanced Home Visitation ProgramHD—health departmentHV—home visitationIPV—intimate partner violenceMIECHV—Maternal, Infant, and Early Childhood Home VisitingProgramUC—usual care
Drs Sharps and Bullock conceptualized and designed the studyand drafted the Methods and Discussion sections of themanuscript; Dr Alhusen assisted with the interpretation of data,drafted the outline and introduction and the Discussion sectionof the manuscript, and critically reviewed and revised themanuscript; Dr Bhandari assisted in drafting the Discussionsection; Dr Ghazarian carried out the initial analyses andreviewed and revised the manuscript; Ms Udo assisted with theinitial analyses and reviewed and revised the manuscript; DrCampbell assisted in the conceptualization and design of thestudy and drafted the Discussion section; and all authorsapproved the final manuscript as submitted.
This trial has been registered with the NINR (identifierNCT00465556).
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1021L
doi:10.1542/peds.2013-1021L
Address correspondence to Phyllis Sharps, PhD, RN, FAAN, Schoolof Nursing, Johns Hopkins University, 525 N. Wolfe Street,Baltimore, MD 21205. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: All phases of this study were supported by NIH/NINRgrant R01009093. Funded by the National Institutes of Health(NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
S134 SHARPS et al by guest on January 29, 2020www.aappublications.org/newsDownloaded from

Intimate partner violence (IPV) is aglobal public health issue affectingwomen of all demographic, ethnic, cul-tural, and socioeconomic backgrounds.Women of childbearing age are at thehighest risk for IPV, and the majority ofstudies have found the prevalence of IPVduring pregnancy ranging from 3.9% to8.3%.1,2 IPV confers considerable risk tothe health of the woman, and childrenexposed to IPVare at an elevated risk foremotional, behavioral, and cognitiveproblems.3,4
Given the well-documented adverseeffects of IPV on both mother and child,home visiting (HV) programs have beenregarded as a particularly salientstrategy for high-risk families who mayhave difficulty engaging in other serv-ices.5–7 Indeed, the creation of the Ma-ternal, Infant, and Early ChildhoodHome Visiting Program (MIECHV)marked an unprecedented fiscal com-mitment to HV programs designed toserve at-risk children and families. Afundamental MIECHV benchmark isappropriate screening, referrals, andsafety planning for families identifiedfor the presence of IPV.
Targeted outcomes of HV programs arelargely reliant on parental involvement,and research demonstrates that fami-lies with greater participation showlarger benefits.8,9 A challenge confront-ing many HV programs is low programretention rates; thus, increasing re-tention rates is critical to increase theeffectiveness of HV programs. Severalreviews have noted low rates of pro-gram retention, with up to 51% of fam-ilies leaving HV programs within 12months10 and up to 67% of familiesleaving before program completion.11
Multiple determinants have been shownto influence retention rates in HV pro-grams (eg, attributes of families, pro-grams, and communities),5,12,13 and thepresence of IPV in the home has beenlinked to poorer program retentionrates and less response to HV support.14
This is of particular concern given theestablished negative sequelae of IPV forboth maternal and child physical andmental health.
This article provides an overview of theDomestic Violence Enhanced HomeVisitationProgram(DOVE), a structuredIPV intervention integrated into existingHV programs in urban and rural set-tings, which shows great promise inidentifying and retaining abused preg-nant women in perinatal HV programs.
METHODS
Procedures
Humansubjectsapprovalswereobtainedfrom all participating academic institu-tions (2 universities) and the rural andurban health departments (HDs). Addi-tionally, a Certificate of Confidentialitywas obtained from theNational Institutesof Health.
Study Design, Setting, and Sample
The DOVE is a multistate longitudinalrandomized clinical trial testing the ef-fectiveness of a structured IPV inter-vention integrated into HD perinatal HVprograms. The DOVE intervention, basedon an empowerment model, combined 2evidence-based interventions: a 10-min-ute brochure-based IPV intervention andperinatal nurse home visitation.
Participants were recruited from anurban East Coast HD, 12 rural mid-western HDs, and 1 midwestern ruralNurse Family Partnership (NFP) pro-gram. Eligible participantswere English-speakingwomen,#31weeks’ gestation,reporting abuse within the last 12months, and currently enrolled in aperinatal HV program of a participatingHD. Referrals for the study were re-ceived from the participating HDs, andthe DOVE research team contacted allreferred women. Women were scree-ned for IPV using the Abuse AssessmentScreen15 and the Women’s Experi-ence with Battering Scale.16 Informed
consent was obtained from all eligiblewomen who expressed an interest instudy participation. In the urban site,women were randomly assigned to ei-ther the usual care (UC) group or theDOVE intervention group. The UC groupreceived the standard HV and IPV pro-tocols instituted by the HDs, and theDOVE intervention group received thestandard HV and IPV protocols in addi-tion to the DOVE IPV intervention. Womenin the DOVE intervention group received3 prenatal and 3 postnatal DOVE sessionsin addition to their HV protocols. In therural sites, among the 12 county HDsparticipating in the study, 6 county HDswere randomly assigned to use DOVE IPVprotocols and 6 counties were assignedto use the usual IPV protocol. Womenparticipating in the NFP program andenrolled in the current study receivedthe DOVE intervention, which was in-tegrated into the NFP protocols asagreed to by David Olds, PhD.
Before implementation of the study’sresearch protocols, the principal in-vestigators (PIs) conducted training forhome visitors in all participating HDs.The 4-hour training included infor-mation about IPV, with attention to IPVduring pregnancy and the importanceof screening and intervening for IPVduring pregnancy. The home visitorsdelivering the DOVE intervention atten-ded an additional 4-hour training thatincluded topics specific to the researchprotocol, use of the screening and as-sessment instruments, delivering thebrochure-based DOVE intervention, de-veloping an individualized safety planfor each DOVE participant, strategies forrevisiting and reinforcing the safetyplan at each subsequent home visit, andappropriate documentation of the DOVEintervention and other pertinent in-formation about the visit. The format ofthe trainings included providing in-formation and providing numerous op-portunities for role playing in screeningfor IPV and implementing the DOVE
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S135 by guest on January 29, 2020www.aappublications.org/newsDownloaded from
intervention. Additionally, all DOVE homevisitors were trained on safety proto-cols including necessary actions to im-plement if the abuser came homeduring the visit, how to safely engagethe abuser during the home visit, andhow to conclude the home visit if nec-essary, keeping both the mother andthe home visitor safe. Over the courseof the 5-year study there were annualbooster training sessions for the in-tervention home visitors. Newly hiredhome visitors were trained individually.The research team also received exten-sive training in IPV, working with abusedwomen, implementing the researchprotocol, and data collection consid-erations.
RESULTS
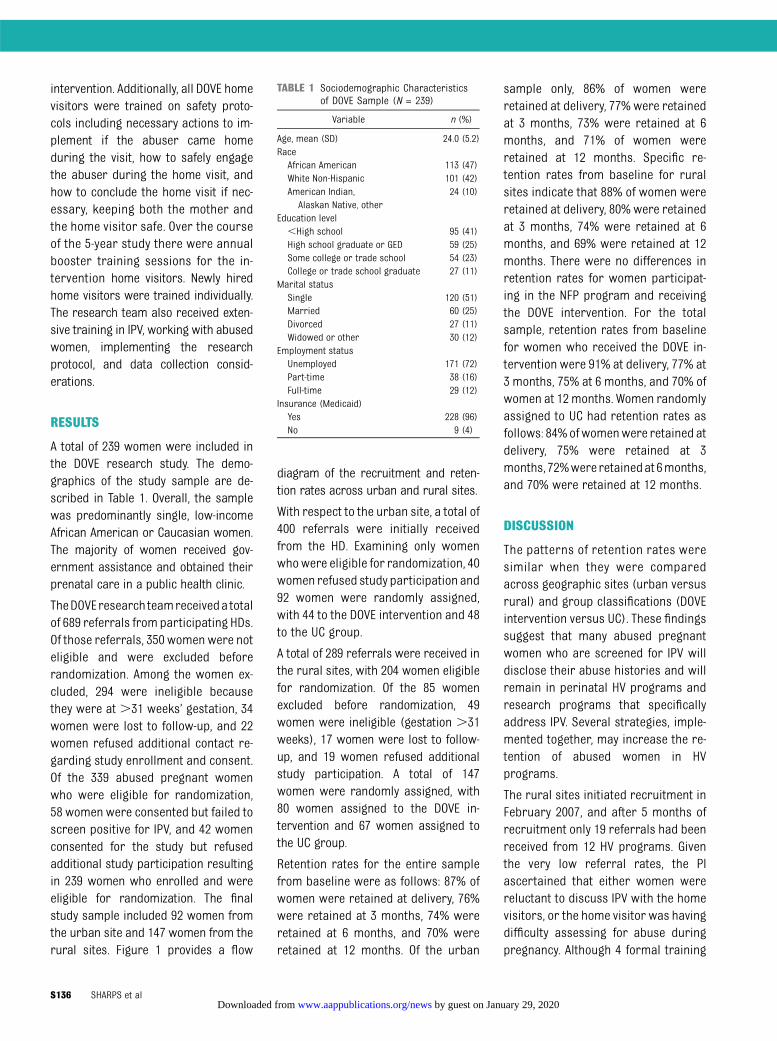
A total of 239 women were included inthe DOVE research study. The demo-graphics of the study sample are de-scribed in Table 1. Overall, the samplewas predominantly single, low-incomeAfrican American or Caucasian women.The majority of women received gov-ernment assistance and obtained theirprenatal care in a public health clinic.
TheDOVEresearch teamreceiveda totalof 689 referrals from participating HDs.Of those referrals, 350 women were noteligible and were excluded beforerandomization. Among the women ex-cluded, 294 were ineligible becausethey were at .31 weeks’ gestation, 34women were lost to follow-up, and 22women refused additional contact re-garding study enrollment and consent.Of the 339 abused pregnant womenwho were eligible for randomization,58 women were consented but failed toscreen positive for IPV, and 42 womenconsented for the study but refusedadditional study participation resultingin 239 women who enrolled and wereeligible for randomization. The finalstudy sample included 92 women fromthe urban site and 147 women from therural sites. Figure 1 provides a flow
diagram of the recruitment and reten-tion rates across urban and rural sites.
With respect to the urban site, a total of400 referrals were initially receivedfrom the HD. Examining only womenwhowere eligible for randomization, 40women refused study participation and92 women were randomly assigned,with 44 to the DOVE intervention and 48to the UC group.
A total of 289 referrals were received inthe rural sites, with 204 women eligiblefor randomization. Of the 85 womenexcluded before randomization, 49women were ineligible (gestation .31weeks), 17 women were lost to follow-up, and 19 women refused additionalstudy participation. A total of 147women were randomly assigned, with80 women assigned to the DOVE in-tervention and 67 women assigned tothe UC group.
Retention rates for the entire samplefrom baseline were as follows: 87% ofwomen were retained at delivery, 76%were retained at 3 months, 74% wereretained at 6 months, and 70% wereretained at 12 months. Of the urban
sample only, 86% of women wereretained at delivery, 77% were retainedat 3 months, 73% were retained at 6months, and 71% of women wereretained at 12 months. Specific re-tention rates from baseline for ruralsites indicate that 88% of women wereretained at delivery, 80% were retainedat 3 months, 74% were retained at 6months, and 69% were retained at 12months. There were no differences inretention rates for women participat-ing in the NFP program and receivingthe DOVE intervention. For the totalsample, retention rates from baselinefor women who received the DOVE in-tervention were 91% at delivery, 77% at3 months, 75% at 6 months, and 70% ofwomen at 12months. Women randomlyassigned to UC had retention rates asfollows: 84%ofwomenwere retained atdelivery, 75% were retained at 3months, 72%wereretainedat 6months,and 70% were retained at 12 months.
DISCUSSION
The patterns of retention rates weresimilar when they were comparedacross geographic sites (urban versusrural) and group classifications (DOVEintervention versus UC). These findingssuggest that many abused pregnantwomen who are screened for IPV willdisclose their abuse histories and willremain in perinatal HV programs andresearch programs that specificallyaddress IPV. Several strategies, imple-mented together, may increase the re-tention of abused women in HVprograms.
The rural sites initiated recruitment inFebruary 2007, and after 5 months ofrecruitment only 19 referrals had beenreceived from 12 HV programs. Giventhe very low referral rates, the PIascertained that either women werereluctant to discuss IPV with the homevisitors, or the home visitor was havingdifficulty assessing for abuse duringpregnancy. Although 4 formal training
TABLE 1 Sociodemographic Characteristicsof DOVE Sample (N = 239)
Variable n (%)
Age, mean (SD) 24.0 (5.2)RaceAfrican American 113 (47)White Non-Hispanic 101 (42)American Indian,
Alaskan Native, other24 (10)
Education level,High school 95 (41)High school graduate or GED 59 (25)Some college or trade school 54 (23)College or trade school graduate 27 (11)
Marital statusSingle 120 (51)Married 60 (25)Divorced 27 (11)Widowed or other 30 (12)
Employment statusUnemployed 171 (72)Part-time 38 (16)Full-time 29 (12)
Insurance (Medicaid)Yes 228 (96)No 9 (4)
S136 SHARPS et al by guest on January 29, 2020www.aappublications.org/newsDownloaded from

programs, consisting of at least a half-day session, had been provided to allhome visitors in all 12 programs, a fifthtraining session was planned andimplemented.17 Barriers and facili-tators to screening were discussed, andthe most common barriers discussedby home visitors included fear of eitherbeing a victim of violence from theabusive partner or having the clientwithdraw from HV because discussingIPV would be too sensitive and intru-sive for participants. Thus, the study
protocol was modified so that homevisitors obtained only the woman’sconsent to provide her name and con-tact information, to be given to the re-search team. With this modification,the research team could assess for IPVafter the women consented to be in thestudy. This change led to a substantialincrease in the number of referralsreceived from participating HDs. Asdemonstrated in Fig 1, only 58 of the270 women screened negative forabuse. This indicates that 80% of the
women referred to the study were ex-periencing abuse. Our findings dem-onstrate that.70% of women enrolledin the DOVE study were retained. Thissuggests that women were not afraidor unwilling to discuss their abusehistories, and were engaged in re-search aimed at mitigating the effectsof abuse on women and children.
Similar challenges were evident in theurbansetting. That is, recruitment rateswere thought to be low because therewere several layers of screening for IPVbefore referral by the HD to the re-search team. When the PI requestedthat the research nurse accompany thehome visitors on each new visit to ex-plain the study and perform the as-sessment for IPV, dramatic increaseswere noted in recruitment rates andpositive IPV screens. Across both studysites, a collaborative partnership thatreinforced the IPV training and role-modeled screening helped the homevisitors gain confidence in screeningfor IPV. Our results indicate that homevisitors’ confidence in screening for IPVincreased with additional training andopportunities to observe health careprofessionals screen women for IPVand educate women on IPV. Ultimately,the goal is that home visitors will becomfortable to integrate IPV screeninginto a routine piece of the HV protocols.
Retaining low-income, abused womenin rural and urban settings over a pe-riod of 2 years in a research study is notfree of challenges. However, a commit-ted research team that successfullycollaborated with home visitors wasintegral to the program’s success. Aroutine protocol in workingwith abusedwomen is to ask about their level ofsafety and obtain contact informationfor other safe contacts of the woman.Research suggests that obtaining safecontacts in addition to participant con-tact information improves the ability toappropriately follow up with abusedwomen.18 Therefore, the DOVE research
FIGURE 1Study recruitment and retention flow diagram.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S137 by guest on January 29, 2020www.aappublications.org/newsDownloaded from

nurses documented a safe address andphone number for every participantduring the initial interview, and in mostcases women provided contact in-formation of a close relative or friend.Research nurses also sought permis-sion to contact the HD home visitors inthe event theywere not able to reach thewoman or her related contacts. Formany women in the study, telephoneservice was inconsistent because offinancial strain. Thus, research nursescontinually searched for updated in-formation and routinely tried to re-establish contact through previousdisconnected phone numbers. If thestudy team was unable to reach theparticipant through phone calls ormailings, the research nurse contactedthe home visitors to discuss additionaloptions for additional contact. Formany women, the consistent contactwith home visitors afforded the studyteam the greatest opportunity forcontact. However, there were timeswhen women continued in the re-search study but withdrew from thestate’s HV program. This may in part bedue to women’s comfort in engagingwith the research nurses and feelingthat they were able to speak about vi-olence in their lives that had been re-luctantly addressed or not addressedat all by the home visitors.
The research nurseswere persistent intheir attempts to retain study partic-ipants. If the research nurse was notable to contact the woman via phone,mailings, the home visitor, or additionalcontacts, she went to the woman’s res-idence without an appointment. Thisstrategy often led to scheduling an ap-pointment at a later date, verifying orrevising contact information, or col-lecting data if the visit was within theappropriate time frame. However, if theparticipant was not home, the researchnurse left a note with neutral termssuch as “Women’s Health Study” toprotect the participant’s privacy and
safety. Other strategies to increase re-tention rates included sending birthdayand holiday cards to every participant,which also assisted with notification ofaddress changes. Additionally, duringeach visit, the research nurses gave theparticipants children’s books and dia-pers (both received as a donation) asa token of appreciation. Finally, eachstudy participant was provided with thestudy’s toll-free number, which wasprinted on business cards and magne-tized promotional materials, facilitatingcommunication with research staff.Again, these materials did not includeterms such as “intimate partner vio-lence”; rather, they referred to women’shealth during the perinatal period.
The research team, together with homevisitors, met often to discuss any par-ticular challenges in locating individualparticipants. Many of the home visitorswere from the same communities asparticipants and were keenly aware ofthe difficulties these women faced onmany levels. Thus, they could offer ad-ditional insight into developing creativestrategies for engaging participants.These sessions also sustained teammembers’motivation for locating hard-to-find participants and demonstratedto home visitors how important theywere in promoting the health and well-being of the women and their children.
The similar retention rates across theUC and intervention group suggests thatroutine screening for violence may fa-cilitate conversation about healthy andunhealthy relationships. Additionally,screening may help women understandoptions in a violent relationship andraise their awareness of the links be-tween violence and other negative out-comes. Many of the women in this studydid not realize violence was such a con-cerning issue until they were asked, atevery study visit, about their relation-ships. One woman stated, “It [screeningfor violence] just made me realize howdangerous a situation I was in and how
muchworse it really was than I ever evenrealized. I knew it was a bad situation, butnever realized it was that bad or howmany different types of abuse I had ex-perienced.” Screening for IPV can suc-cessfully identify survivors and mayreduce violence and improve outcomes.19
Less studied is how to successfully im-plement screening, particularly in thehome setting while ensuring both thehome visitor’s and the participant’scomfort with screening. The strategiesimplemented in this study offer insightsinto how to leverage the ongoing rela-tionships created in the HV context tosafely and effectively screen for IPV.
The current study has several limitations.The samplewas largely low-income ruraland urban women participating in peri-natal HV programs, so results may notbe generalizable to women participat-ing in other HV programs. The DOVEresearch team was able to contactonly women who were referred byparticipating HDs and enrolled in theHD’s HV programs. It is possible thatwomen enrolled in the study maynot be representative of all abusedwomen. Nonetheless, the study hasseveral strengths. This was a longitu-dinal study of women abused duringthe perinatal period and included thewomen’s infants and toddlers. The col-laborative efforts of the HV staff andresearch nurses resulted in strategiesand study methods that safely main-tained abused women and their chil-dren over the course of the 2-yearstudy period. Our results indicate thatabused women can be retained in HVprograms, and related research stud-ies, when screened for IPV. Screeningfor IPV may indicate to women thathealth care providers have a vestedinterest in their health and well-beingand are able to connect them to much-needed resources.
Therecently initiatedfederalgovernmentmandates included in the enhancementsof Title 5,MIECHV, requireHVprograms to
S138 SHARPS et al by guest on January 29, 2020www.aappublications.org/newsDownloaded from

implement evidence-based protocols forscreening and intervening for domesticviolence. Specifically, the bill targetscommunitieswithhighconcentrationsofpreterm births, low birth weight infants,infant mortality, or related risk factorsincluding domestic violence. HV pro-grams must screen for IPV and pro-vide necessary referrals. Our findings
demonstrate that with adequate trainingand collaboration with local HD person-nel, home visitors can feel confident inscreening for IPVwith theknowledgethatit will not affect participant retention inHV programs. HV programs aiming forthe best outcomes must implementuniversal screening for IPV and imple-ment evidence-based interventions to
address violence in the perinatal period.Abusedwomenareoftenmoredifficult tosuccessfully recruit, engage, and retainin HV programs.14 Our findings offerseveral strategies for assessing and in-tervening with abused women in col-laboration with HV programs in ruraland urban areas to optimize maternaland infant health outcomes.
REFERENCES
1. Martin SL, Mackie L, Kupper LL, BuescherPA, Moracco KE. Physical abuse of womenbefore, during, and after pregnancy. JAMA.2001;285(12):1581–1584
2. Saltzman LE, Johnson CH, Gilbert BC,Goodwin MM. Physical abuse around thetime of pregnancy: an examination ofprevalence and risk factors in 16 states.Matern Child Health J. 2003;7(1):31–43
3. Kitzmann KM, Gaylord NK, Holt AR, KennyED. Child witnesses to domestic violence:a meta-analytic review. J Consult Clin Psy-chol. 2003;71(2):339–352
4. Wolfe DA, Crooks CV, Lee V, McIntyre-SmithA, Jaffe PG. The effects of children’s expo-sure to domestic violence: a meta-analysisand critique. Clin Child Fam Psychol Rev.2003;6(3):171–187
5. Duggan A, Windham A, McFarlane E, et al.Hawaii’s Healthy Start Program of homevisiting for at-risk families: evaluation offamily identification, family engagement,and service delivery. Pediatrics. 2000;105(1pt 3):250–259
6. Leventhal JM. The prevention of child abuseand neglect: successfully out of the blocks.Child Abuse Negl. 2001;25(4):431–439
7. Olds DL, Henderson CR Jr, Phelps C, KitzmanH, Hanks C. Effect of prenatal and infancy
nurse home visitation on governmentspending. Med Care. 1993;31(2):155–174
8. Olds DL, Henderson CR Jr, Kitzman HJ,Eckenrode JJ, Cole RE, Tatelbaum RC. Pre-natal and infancy home visitation bynurses: recent findings. Future Child. 1999;9(1):44–65, 190–191
9. Wagner MM, Clayton SL. The Parents asTeachers program: results from two dem-onstrations. Future Child. 1999;9(1):91–115,179–189
10. Guterman N. Stopping Child MaltreatmentBefore It Starts: Emerging Horizons in EarlyHome Visitation Services. Thousand Oaks,CA: Sage; 2001
11. Gomby DS, Culross PL, Behrman RE. Homevisiting: recent program evaluations—analysis and recommendations. FutureChild. 1999;9(1):4–26, 195–223
12. McCurdy K, Daro D. Parent involvement infamily support programs: an integratedtheory. Fam Relat. 2001;50(2):113–121
13. McCurdy K, Hurvis S, Clark J. Engaging andretaining families in child abuse preventionprograms. The APSAC Advisor. 1996;9(3):3–9
14. Eckenrode J, Ganzel B, Henderson CR Jr,et al. Preventing child abuse and neglectwith a program of nurse home visitation:
the limiting effects of domestic violence.JAMA. 2000;284(11):1385–1391
15. Soeken K, Parker B, McFarlane J, Lominak MC.The abuse assessment screen: A clinical in-strument to measure frequency, severity andperpetrator of abuse against women. In:Campbell J, ed. Empowering Survivors ofAbuse: Health Care for Battered Women andTheir Children. Thousand Oaks, CA: Sage; 1998
16. Smith PH, Earp JA, DeVellis R. Measuringbattering: Development of the women’s Ex-perience With Battering (WEB) scale.Womens Health. 1995;1(4):273–288
17. Eddy T, Kilburn E, Chang C, Bullock L,Sharps P. Facilitators and barriers forimplementing home visit interventions toaddress intimate partner violence: townand gown partnerships. Nurs Clin NorthAm. 2008;43(3):419–435, ix
18. Sullivan CM, Rumptz MH, Campbell R, Eby KK,Davidson WS. Retaining participants in longi-tudinal community research: a comprehensiveprotocol. J Appl Behav Sci. 1996;32(3):262–276
19. Nelson HD, Bougatsos C, Blazina I. Screen-ing women for intimate partner violence:a systematic review to update the U.S.Preventive Services Task Force recommen-dation. Ann Intern Med. 2012;156(11):796–808, W-279, W-280, W-281, W-282
SUPPLEMENT ARTICLE
PEDIATRICS Volume 132, Supplement 2, November 2013 S139 by guest on January 29, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1021L2013;132;S134Pediatrics
Ghazarian, Ifeyinwa E. Udo and Jacquelyn CampbellPhyllis Sharps, Jeanne L. Alhusen, Linda Bullock, Shreya Bhandari, Sharon
Engaging and Retaining Abused Women in Perinatal Home Visitation Programs
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/132/Supplement_2/S134including high resolution figures, can be found at:
References
#BIBLhttp://pediatrics.aappublications.org/content/132/Supplement_2/S134This article cites 17 articles, 1 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on January 29, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1021L2013;132;S134Pediatrics
Ghazarian, Ifeyinwa E. Udo and Jacquelyn CampbellPhyllis Sharps, Jeanne L. Alhusen, Linda Bullock, Shreya Bhandari, Sharon
Engaging and Retaining Abused Women in Perinatal Home Visitation Programs
http://pediatrics.aappublications.org/content/132/Supplement_2/S134located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on January 29, 2020www.aappublications.org/newsDownloaded from