Endovascular coiling versus neurosurgical clipping in patients
7
RESEARCH ARTICLE Open Access Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review Jin Seub Hwang 1 , Min Kyung Hyun 1* , Hyun Joo Lee 1 , Ji Eun Choi 1 , Jong Hee Kim 1 , Na Rae Lee 1 , Jin-Won Kwon 1,2 and EnJu Lee 1 Abstract Background: To compare the effects of endovascular coiling and neurosurgical clipping in patients with unruptured intracranial aneurysm. Methods: Sixteen electronic databases were searched for articles published between 1950 and July 2010 to compare clinical outcomes of clipping and coiling. Researchers reviewed all searched articles and extracted data independently. The quality of studies and evidence were evaluated using MINORS and GRADEprofiler, respectively. The odds ratio (OR) was calculated using the inverse variance meta-analysis method for each study outcome. To assess heterogeneity of ORs across cohorts, Cochran’s Q statistic and I 2 were used. Results: Of 4160 studies, 24 were identified (n = 31865). Clipping resulted in significantly higher disability using the Glasgow Outcome Scale (OR, 2.38; 95% CI, 1.33–4.26) and Modified Rankin Scale (OR, 2.83; 95% CI, 1.42–5.63) when compared with coiling. ORs for complications were also higher with clipping (ORs for neurological and cardiac complications were 1.94 with a 95% confidence interval [CI] of 1.09–3.47 and 2.51 with a 95% CI of 1.15–5.50). Clipping resulted in significantly greater disability in the short term (≤6 m)(OR on the Glasgow Outcome Scale, 2.72; 95% CI, 1.16–6.34), but not in the long term (>6 m)(OR for Glasgow Outcome Scale, 2.12; 95% CI, 0.93–4.84). Conclusions: Coiling was a better procedure for treatment of unruptured intracranial aneurysm in terms of disability, complications, especially in the short term. Because of the limitations of the reviewed studies, further studies are required to support the present results. Keywords: Unruptured intracranial aneurysm, Endovascular coiling, Neurosurgical clipping Background Recent developments in non-invasive imaging detection, such as magnetic resonance (MR) angiography and com- puted tomography (CT) angiography, have made screen- ing for unruptured intracranial aneurysm (UIA) possible in the general population [1]. Despite study results showing that it is not cost-effective to screen for asymp- tomatic UIA [2], such screening has become widespread, and UIA is being identified with increasing frequency. Patients with UIA always have risks of rupture with intracranial aneurysms. A nationwide study in Sweden showed that the 5-, 10- and 15-year risks of death after subarachnoid haemorrhage (SAH) were 12.9%, 23.6% and 35.4%, respectively [3]. Thus, patients with UIA are often treated to prevent SAH, and these prophylactic treatments include neurosurgical clipping and endovas- cular coiling. Neurosurgical clipping of the aneurysm was the standard treatment prior to the introduction of detachable coils, but endovascular coiling has recently been increasing [4]. Neurosurgical clipping is recom- mended over endovascular coiling for young patients and for small or anterior circulation aneurysms, i.e., low- risk cases [5]. Neurosurgical clipping is an order of mag- nitude more durable than endovascular coiling, but endovascular coiling is less invasive than neurosurgical * Correspondence: [email protected] 1 National Evidence-based Healthcare Collaborating Agency, Changkyung B/D 8 F, 28-7 Wonnam-dong, Seoul, Jongno-gu 110-450, Korea Full list of author information is available at the end of the article © 2012 Hwang et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Hwang et al. BMC Neurology 2012, 12:99 http://www.biomedcentral.com/1471-2377/12/99
Transcript of Endovascular coiling versus neurosurgical clipping in patients

Hwang et al BMC Neurology 2012 1299httpwwwbiomedcentralcom1471-23771299
RESEARCH ARTICLE Open Access
Endovascular coiling versus neurosurgicalclipping in patients with unruptured intracranialaneurysm a systematic reviewJin Seub Hwang1 Min Kyung Hyun1 Hyun Joo Lee1 Ji Eun Choi1 Jong Hee Kim1 Na Rae Lee1Jin-Won Kwon12 and EnJu Lee1
Abstract
Background To compare the effects of endovascular coiling and neurosurgical clipping in patients withunruptured intracranial aneurysm
Methods Sixteen electronic databases were searched for articles published between 1950 and July 2010 tocompare clinical outcomes of clipping and coiling Researchers reviewed all searched articles and extracted dataindependently The quality of studies and evidence were evaluated using MINORS and GRADEprofiler respectivelyThe odds ratio (OR) was calculated using the inverse variance meta-analysis method for each study outcome Toassess heterogeneity of ORs across cohorts Cochranrsquos Q statistic and I2 were used
Results Of 4160 studies 24 were identified (n = 31865) Clipping resulted in significantly higher disability using theGlasgow Outcome Scale (OR 238 95 CI 133ndash426) and Modified Rankin Scale (OR 283 95 CI 142ndash563) whencompared with coiling ORs for complications were also higher with clipping (ORs for neurological and cardiaccomplications were 194 with a 95 confidence interval [CI] of 109ndash347 and 251 with a 95 CI of 115ndash550)Clipping resulted in significantly greater disability in the short term (le6 m)(OR on the Glasgow Outcome Scale 27295 CI 116ndash634) but not in the long term (gt6 m)(OR for Glasgow Outcome Scale 212 95 CI 093ndash484)
Conclusions Coiling was a better procedure for treatment of unruptured intracranial aneurysm in terms ofdisability complications especially in the short term Because of the limitations of the reviewed studies furtherstudies are required to support the present results
Keywords Unruptured intracranial aneurysm Endovascular coiling Neurosurgical clipping
BackgroundRecent developments in non-invasive imaging detectionsuch as magnetic resonance (MR) angiography and com-puted tomography (CT) angiography have made screen-ing for unruptured intracranial aneurysm (UIA) possiblein the general population [1] Despite study resultsshowing that it is not cost-effective to screen for asymp-tomatic UIA [2] such screening has become widespreadand UIA is being identified with increasing frequencyPatients with UIA always have risks of rupture with
intracranial aneurysms A nationwide study in Sweden
Correspondence mk3threegmailcom1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 KoreaFull list of author information is available at the end of the article
copy 2012 Hwang et al licensee BioMed CentralCommons Attribution License (httpcreativecreproduction in any medium provided the or
showed that the 5- 10- and 15-year risks of death aftersubarachnoid haemorrhage (SAH) were 129 236and 354 respectively [3] Thus patients with UIA areoften treated to prevent SAH and these prophylactictreatments include neurosurgical clipping and endovas-cular coiling Neurosurgical clipping of the aneurysmwas the standard treatment prior to the introduction ofdetachable coils but endovascular coiling has recentlybeen increasing [4] Neurosurgical clipping is recom-mended over endovascular coiling for young patientsand for small or anterior circulation aneurysms ie low-risk cases [5] Neurosurgical clipping is an order of mag-nitude more durable than endovascular coiling butendovascular coiling is less invasive than neurosurgical
Ltd This is an Open Access article distributed under the terms of the Creativeommonsorglicensesby20) which permits unrestricted use distribution andiginal work is properly cited
Hwang et al BMC Neurology 2012 1299 Page 2 of 7httpwwwbiomedcentralcom1471-23771299
clipping thus it may be suitable for high-risk UIApatients (elderly or posterior aneurysms etc) [5]Using the national inpatient sample database from
2002 to 2008 Smith et al [6] showed that the major-ity of ruptured and unruptured aneurysms in the USare coiled However which treatment is better remainscontroversial and there have been no systematicreviews of patients with UIA Therefore an extensivesystematic review and meta-analysis were performedto compare the benefits and risks in UIA patientstreated with endovascular coiling vs neurosurgicalclipping
MethodsLiterature searchWe developed and adhered to a protocol for populationintervention comparison and outcome (PICO) searchmethods data extraction quality assessment meta-analysis and grading of the quality of the evidence forthis systematic reviewArticles Published before July 2010 in 16 electronic
databases were searched These databases included threeinternational databases ten Korean domestic databasesand three Japanese domestic databases (1) Ovid-Medline(2) Ovid-Embase (3) Cochrane Library (4) KISS (httpkisskstudycom) (5) KMBASE (httpkmbasemedricorkr) (6) KoreaMed (httpwwwkoreamedorg) (7) NDSL(httpwwwndslkr) (8) KiSTi (httpsocietykisti rekr) (9) J Cerebrovasc Surg (httpjkcvsksevsorg) (10)
Figure 1 Flow diagram of article selection for this study
J Korean Soc Radiol (httpwwwradiologyorkr) (11) JKorean Neurosurg Soc (httpjknsorkr) (12) Neurointervention (httpwwwksinorkr) (13) Korean JStroke (httpwwwstrokeorkr) (14) JAMAS (httpwwwjamasorjp) (15) Medical online (httpwwwmeteo-intergatecom) and (16) J-stage (httpwwwjstagejstgojp) Various combinations of Mesh head-ings and keywords were used such as ldquointracranialaneurysmrdquo ldquosubarachnoid haemorrhagerdquo ldquoembolisa-tionrdquo ldquoneurosurgical proceduresrdquo ldquoneurosurgeryrdquoldquounrupturedrdquo ldquocoilrdquo ldquoGuglielmirdquo ldquoGDCrdquo and ldquocliprdquoThe search was limited to human studies without lan-guage restrictions
Study selection data extraction and quality assessmentEligible studies were those that included adult (ge18 years)patients with UIA Patients with mycotic infectious dis-secting or fusiform aneurysms arteriovenous malforma-tion or arteriovenous fistula were excluded Case seriescase reports and publications that had not undergonepeer review were excluded In addition studies wererequired to have directly comparable outcome measuresfor endovascular coiling and neurosurgical clipping suchas overall death in-hospital mortality disability andcomplications Disability was regarded as a score of 1ndash5on the Modified Rankin Scale [mRS] and a score of 2ndash4on the Glasgow Outcome Scale [GOS] The mRS aclinician-reported measure of global disability is widelyapplied to evaluate stroke patient outcomes and scores
Hwang et al BMC Neurology 2012 1299 Page 3 of 7httpwwwbiomedcentralcom1471-23771299
run from no symptoms at all (score 0) to death (score 6)[7] The GOS assesses outcome after severe brain dam-age and runs from death (score 1) to good recovery(score 5) [8] There were various complications includ-ing bleeding or haematoma in the brain ischemia or in-farction cerebral vessel damage cerebrospinal fluidfistula infection cranial nerve disorder cognitive im-pairment encephalitis meningitis embolism cardiacdisease and pulmonary diseaseFour authors (HJL JEC JSH and MKH) independently
reviewed all searched articles and extracted data usingpre-made extraction forms that included study designfollow-up period inclusionexclusion criteria samplesize sex age aneurysm location aneurysm size racebaseline characteristics treatment protocol outcomevariables and complications Disability was calculatedbased on the percentages of categories other than deathgood recovery in mRSGOS The numbers of events foroutcomes were extracted according to the intention-to-treat principleSix authors (HJL JEC JHK JSH LRL and MKH) inde-
pendently evaluated the quality of the studies using theMethodological Index for Nonrandomised Studies(MINORS) [9] In the case of disagreement consensuswas reached through discussion and negotiations withpartners If a consensus could not be achieved within
Table 1 Meta-analysis of neurosurgical clipping vs endovascu
Outcome Studiesn
Patientsn
RaO
Overall death
Overall 5 1967 14
le6 months measurement time 4 1950 12
In-hospital mortality
Overall 5 15
Adjusted OR 3 33
Disability (GOS)
Overall 9 754 23
le6 months measurement time 4 314 27
gt6 months measurement time 4 331 21
Asian races 4 413 24
Western races 5 341 23
Disability (mRS) 2 262 28
Complication
Cerebral haemorrhage 8 7419 19
Cerebral infarction 12 7635 10
Neurological complication 11 7661 19
Cardiac complication 6 7067 25
Abbreviations OR odds ratio CI confidence interval mRS modified Rankin Scalereported
the group a third party was involved and then an agree-ment was reached by majority rule
Meta-analysis and grading the quality of the evidenceA meta-analysis was performed to synthesise the out-comes except for missing data among 24 articles Binaryoutcomes were expressed as odds ratios (ORs) Thereporting methods for in-hospital mortality were diverseincluding the number of patients unadjusted ORs andadjusted ORs Therefore lnOR and standard error werecalculated using statistical equationsFixed and random effects inverse-variance meta-analysis
was used to combine the studies and obtain the averageeffects and 95 confidence intervals (CI) The subgroupanalyses were performed by outcome measurement times(short time le6 months long time gt6 months) accordingto medical expertsrsquo opinionsTo assess heterogeneity across studies funnel plots were
visually examined and Cochranrsquos Q statistic and the I2
statistic were used Publication bias was also assessedusing funnel plots Begg and Mazumdarrsquos rank correlation(Beggrsquos test) and Eggerrsquos linear regression asymmetry testof the intercept (Eggerrsquos test) Finally the quality of thebody of evidence was graded as ldquohighrdquo ldquomoderaterdquo ldquolowrdquoor ldquovery lowrdquo [10]
lar coiling for each outcome
ndom effectsR (95 CI)
Fixed effectsOR (95 CI)
I2 HeterogeneityP
2 (050 404) 142 (050 404) 0 069
5 (042 374) 125 (042 374) 0 065
5 (091 261) 135 (107 170) 52 008
5 (091 1230) 346 (220 544) 83 0003
8 (133 426) 238 (133 426) 0 099
2 (116 634) 272 (116 634) 0 081
2 (093 484) 212 (093 484) 0 090
1 (119 490) 241 (119 490) 0 084
2 (084 639) 232 (084 639) 0 092
3 (142 563) 283 (142 563) 0 081
0 072
6 (083 464) 144 (103 202) 63 001
7 (069 166) 096 (074 123) 39 008
4 (109-347) 138 (112 171) 58 0009
1 (115 550) 251 (115 550) 0 098
GOS Glasgow Outcome Scale Values for a random-effects model are
Hwang et al BMC Neurology 2012 1299 Page 4 of 7httpwwwbiomedcentralcom1471-23771299
Meta-analyses were conducted using ComprehensiveMeta-analysis 20 (Biostat Englewood NJ USA) and thequality of evidence and strength of recommendation weregraded using GRADEprofiler 322 (GRADE WorkingGroup)
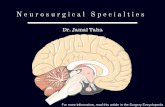
ResultsThe authors independently reviewed titles and abstractsof 3135 identified unique studies 2462 studies wereexcluded The full-text publications of the remaining673 potentially eligible studies were reviewed in detailOf these 645 were excluded based on the inclusion andexclusion criteria (Figure 1) Of 1581 international stud-ies 1480 Korean domestic studies and 1099 Japanese do-mestic studies 24 observational studies reporting datafrom 31 865 patients were selected for the comprehen-sive meta-analysis Characteristics of these studies are
(A) Overall death
(B) In-hospital mortality
(C) Disability measured by the Glasgow Outcome S
Figure 2 Outcomes from neurosurgical clipping vs endovascular coil
presented in Additional file 1 and the quality of studiesare listed in Additional file 1
Meta-analysisFour outcome types (disability measured by mRS andGOS neurological and cardiac complications) showedstatistically significant differences between coiling andclipping (Table 1 Figure 2 Figure 3) Clipping had sig-nificantly higher disability as measured by GOS (OR238 95 CI 133ndash426) and mRS (OR 283 95 CI142ndash563) when compared with coiling ORs for neuro-logical (OR 194 95 CI 109ndash347) and cardiac (OR251 95 CI 115ndash550) complications were also higherwith clippingOn the other hand overall mortality in-hospital mor-
tality and complications of cerebral haemorrhage andcerebral infarction showed no statistically significant dif-ferences between the two groups There was evidence of
cale
ing
Hwang et al BMC Neurology 2012 1299 Page 5 of 7httpwwwbiomedcentralcom1471-23771299
statistical heterogeneity and the I2 range was 39 to83 which represents moderate or substantial hetero-geneity Therefore overall mortality in-hospital mortal-ity and complications of cerebral haemorrhage andcerebral infarction were incorporated into a random-effects model
(A) Cerebral haemorrhage (complications)
(B) Cerebral infarction (complications)
(C) Neurological complications
(D) Cardiac complications
Figure 3 Outcomes from neurosurgical clipping vs endovascular coil
In subgroup analysis by outcome-measurement timeclipping showed significantly higher disability measuredby GOS (OR 272 95 CI 116ndash634) in the short term(le6 m) However disability (GOS) was not significantlydifferent in the long term (gt6 m) (OR 212 95 CI093ndash484) (Table 1)
ing (complications)
Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 2 of 7httpwwwbiomedcentralcom1471-23771299
clipping thus it may be suitable for high-risk UIApatients (elderly or posterior aneurysms etc) [5]Using the national inpatient sample database from
2002 to 2008 Smith et al [6] showed that the major-ity of ruptured and unruptured aneurysms in the USare coiled However which treatment is better remainscontroversial and there have been no systematicreviews of patients with UIA Therefore an extensivesystematic review and meta-analysis were performedto compare the benefits and risks in UIA patientstreated with endovascular coiling vs neurosurgicalclipping
MethodsLiterature searchWe developed and adhered to a protocol for populationintervention comparison and outcome (PICO) searchmethods data extraction quality assessment meta-analysis and grading of the quality of the evidence forthis systematic reviewArticles Published before July 2010 in 16 electronic
databases were searched These databases included threeinternational databases ten Korean domestic databasesand three Japanese domestic databases (1) Ovid-Medline(2) Ovid-Embase (3) Cochrane Library (4) KISS (httpkisskstudycom) (5) KMBASE (httpkmbasemedricorkr) (6) KoreaMed (httpwwwkoreamedorg) (7) NDSL(httpwwwndslkr) (8) KiSTi (httpsocietykisti rekr) (9) J Cerebrovasc Surg (httpjkcvsksevsorg) (10)
Figure 1 Flow diagram of article selection for this study
J Korean Soc Radiol (httpwwwradiologyorkr) (11) JKorean Neurosurg Soc (httpjknsorkr) (12) Neurointervention (httpwwwksinorkr) (13) Korean JStroke (httpwwwstrokeorkr) (14) JAMAS (httpwwwjamasorjp) (15) Medical online (httpwwwmeteo-intergatecom) and (16) J-stage (httpwwwjstagejstgojp) Various combinations of Mesh head-ings and keywords were used such as ldquointracranialaneurysmrdquo ldquosubarachnoid haemorrhagerdquo ldquoembolisa-tionrdquo ldquoneurosurgical proceduresrdquo ldquoneurosurgeryrdquoldquounrupturedrdquo ldquocoilrdquo ldquoGuglielmirdquo ldquoGDCrdquo and ldquocliprdquoThe search was limited to human studies without lan-guage restrictions
Study selection data extraction and quality assessmentEligible studies were those that included adult (ge18 years)patients with UIA Patients with mycotic infectious dis-secting or fusiform aneurysms arteriovenous malforma-tion or arteriovenous fistula were excluded Case seriescase reports and publications that had not undergonepeer review were excluded In addition studies wererequired to have directly comparable outcome measuresfor endovascular coiling and neurosurgical clipping suchas overall death in-hospital mortality disability andcomplications Disability was regarded as a score of 1ndash5on the Modified Rankin Scale [mRS] and a score of 2ndash4on the Glasgow Outcome Scale [GOS] The mRS aclinician-reported measure of global disability is widelyapplied to evaluate stroke patient outcomes and scores
Hwang et al BMC Neurology 2012 1299 Page 3 of 7httpwwwbiomedcentralcom1471-23771299
run from no symptoms at all (score 0) to death (score 6)[7] The GOS assesses outcome after severe brain dam-age and runs from death (score 1) to good recovery(score 5) [8] There were various complications includ-ing bleeding or haematoma in the brain ischemia or in-farction cerebral vessel damage cerebrospinal fluidfistula infection cranial nerve disorder cognitive im-pairment encephalitis meningitis embolism cardiacdisease and pulmonary diseaseFour authors (HJL JEC JSH and MKH) independently
reviewed all searched articles and extracted data usingpre-made extraction forms that included study designfollow-up period inclusionexclusion criteria samplesize sex age aneurysm location aneurysm size racebaseline characteristics treatment protocol outcomevariables and complications Disability was calculatedbased on the percentages of categories other than deathgood recovery in mRSGOS The numbers of events foroutcomes were extracted according to the intention-to-treat principleSix authors (HJL JEC JHK JSH LRL and MKH) inde-
pendently evaluated the quality of the studies using theMethodological Index for Nonrandomised Studies(MINORS) [9] In the case of disagreement consensuswas reached through discussion and negotiations withpartners If a consensus could not be achieved within
Table 1 Meta-analysis of neurosurgical clipping vs endovascu
Outcome Studiesn
Patientsn
RaO
Overall death
Overall 5 1967 14
le6 months measurement time 4 1950 12
In-hospital mortality
Overall 5 15
Adjusted OR 3 33
Disability (GOS)
Overall 9 754 23
le6 months measurement time 4 314 27
gt6 months measurement time 4 331 21
Asian races 4 413 24
Western races 5 341 23
Disability (mRS) 2 262 28
Complication
Cerebral haemorrhage 8 7419 19
Cerebral infarction 12 7635 10
Neurological complication 11 7661 19
Cardiac complication 6 7067 25
Abbreviations OR odds ratio CI confidence interval mRS modified Rankin Scalereported
the group a third party was involved and then an agree-ment was reached by majority rule
Meta-analysis and grading the quality of the evidenceA meta-analysis was performed to synthesise the out-comes except for missing data among 24 articles Binaryoutcomes were expressed as odds ratios (ORs) Thereporting methods for in-hospital mortality were diverseincluding the number of patients unadjusted ORs andadjusted ORs Therefore lnOR and standard error werecalculated using statistical equationsFixed and random effects inverse-variance meta-analysis
was used to combine the studies and obtain the averageeffects and 95 confidence intervals (CI) The subgroupanalyses were performed by outcome measurement times(short time le6 months long time gt6 months) accordingto medical expertsrsquo opinionsTo assess heterogeneity across studies funnel plots were
visually examined and Cochranrsquos Q statistic and the I2
statistic were used Publication bias was also assessedusing funnel plots Begg and Mazumdarrsquos rank correlation(Beggrsquos test) and Eggerrsquos linear regression asymmetry testof the intercept (Eggerrsquos test) Finally the quality of thebody of evidence was graded as ldquohighrdquo ldquomoderaterdquo ldquolowrdquoor ldquovery lowrdquo [10]
lar coiling for each outcome
ndom effectsR (95 CI)
Fixed effectsOR (95 CI)
I2 HeterogeneityP
2 (050 404) 142 (050 404) 0 069
5 (042 374) 125 (042 374) 0 065
5 (091 261) 135 (107 170) 52 008
5 (091 1230) 346 (220 544) 83 0003
8 (133 426) 238 (133 426) 0 099
2 (116 634) 272 (116 634) 0 081
2 (093 484) 212 (093 484) 0 090
1 (119 490) 241 (119 490) 0 084
2 (084 639) 232 (084 639) 0 092
3 (142 563) 283 (142 563) 0 081
0 072
6 (083 464) 144 (103 202) 63 001
7 (069 166) 096 (074 123) 39 008
4 (109-347) 138 (112 171) 58 0009
1 (115 550) 251 (115 550) 0 098
GOS Glasgow Outcome Scale Values for a random-effects model are
Hwang et al BMC Neurology 2012 1299 Page 4 of 7httpwwwbiomedcentralcom1471-23771299
Meta-analyses were conducted using ComprehensiveMeta-analysis 20 (Biostat Englewood NJ USA) and thequality of evidence and strength of recommendation weregraded using GRADEprofiler 322 (GRADE WorkingGroup)
ResultsThe authors independently reviewed titles and abstractsof 3135 identified unique studies 2462 studies wereexcluded The full-text publications of the remaining673 potentially eligible studies were reviewed in detailOf these 645 were excluded based on the inclusion andexclusion criteria (Figure 1) Of 1581 international stud-ies 1480 Korean domestic studies and 1099 Japanese do-mestic studies 24 observational studies reporting datafrom 31 865 patients were selected for the comprehen-sive meta-analysis Characteristics of these studies are
(A) Overall death
(B) In-hospital mortality
(C) Disability measured by the Glasgow Outcome S
Figure 2 Outcomes from neurosurgical clipping vs endovascular coil
presented in Additional file 1 and the quality of studiesare listed in Additional file 1
Meta-analysisFour outcome types (disability measured by mRS andGOS neurological and cardiac complications) showedstatistically significant differences between coiling andclipping (Table 1 Figure 2 Figure 3) Clipping had sig-nificantly higher disability as measured by GOS (OR238 95 CI 133ndash426) and mRS (OR 283 95 CI142ndash563) when compared with coiling ORs for neuro-logical (OR 194 95 CI 109ndash347) and cardiac (OR251 95 CI 115ndash550) complications were also higherwith clippingOn the other hand overall mortality in-hospital mor-
tality and complications of cerebral haemorrhage andcerebral infarction showed no statistically significant dif-ferences between the two groups There was evidence of
cale
ing
Hwang et al BMC Neurology 2012 1299 Page 5 of 7httpwwwbiomedcentralcom1471-23771299
statistical heterogeneity and the I2 range was 39 to83 which represents moderate or substantial hetero-geneity Therefore overall mortality in-hospital mortal-ity and complications of cerebral haemorrhage andcerebral infarction were incorporated into a random-effects model
(A) Cerebral haemorrhage (complications)
(B) Cerebral infarction (complications)
(C) Neurological complications
(D) Cardiac complications
Figure 3 Outcomes from neurosurgical clipping vs endovascular coil
In subgroup analysis by outcome-measurement timeclipping showed significantly higher disability measuredby GOS (OR 272 95 CI 116ndash634) in the short term(le6 m) However disability (GOS) was not significantlydifferent in the long term (gt6 m) (OR 212 95 CI093ndash484) (Table 1)
ing (complications)
Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 3 of 7httpwwwbiomedcentralcom1471-23771299
run from no symptoms at all (score 0) to death (score 6)[7] The GOS assesses outcome after severe brain dam-age and runs from death (score 1) to good recovery(score 5) [8] There were various complications includ-ing bleeding or haematoma in the brain ischemia or in-farction cerebral vessel damage cerebrospinal fluidfistula infection cranial nerve disorder cognitive im-pairment encephalitis meningitis embolism cardiacdisease and pulmonary diseaseFour authors (HJL JEC JSH and MKH) independently
reviewed all searched articles and extracted data usingpre-made extraction forms that included study designfollow-up period inclusionexclusion criteria samplesize sex age aneurysm location aneurysm size racebaseline characteristics treatment protocol outcomevariables and complications Disability was calculatedbased on the percentages of categories other than deathgood recovery in mRSGOS The numbers of events foroutcomes were extracted according to the intention-to-treat principleSix authors (HJL JEC JHK JSH LRL and MKH) inde-
pendently evaluated the quality of the studies using theMethodological Index for Nonrandomised Studies(MINORS) [9] In the case of disagreement consensuswas reached through discussion and negotiations withpartners If a consensus could not be achieved within
Table 1 Meta-analysis of neurosurgical clipping vs endovascu
Outcome Studiesn
Patientsn
RaO
Overall death
Overall 5 1967 14
le6 months measurement time 4 1950 12
In-hospital mortality
Overall 5 15
Adjusted OR 3 33
Disability (GOS)
Overall 9 754 23
le6 months measurement time 4 314 27
gt6 months measurement time 4 331 21
Asian races 4 413 24
Western races 5 341 23
Disability (mRS) 2 262 28
Complication
Cerebral haemorrhage 8 7419 19
Cerebral infarction 12 7635 10
Neurological complication 11 7661 19
Cardiac complication 6 7067 25
Abbreviations OR odds ratio CI confidence interval mRS modified Rankin Scalereported
the group a third party was involved and then an agree-ment was reached by majority rule
Meta-analysis and grading the quality of the evidenceA meta-analysis was performed to synthesise the out-comes except for missing data among 24 articles Binaryoutcomes were expressed as odds ratios (ORs) Thereporting methods for in-hospital mortality were diverseincluding the number of patients unadjusted ORs andadjusted ORs Therefore lnOR and standard error werecalculated using statistical equationsFixed and random effects inverse-variance meta-analysis
was used to combine the studies and obtain the averageeffects and 95 confidence intervals (CI) The subgroupanalyses were performed by outcome measurement times(short time le6 months long time gt6 months) accordingto medical expertsrsquo opinionsTo assess heterogeneity across studies funnel plots were
visually examined and Cochranrsquos Q statistic and the I2
statistic were used Publication bias was also assessedusing funnel plots Begg and Mazumdarrsquos rank correlation(Beggrsquos test) and Eggerrsquos linear regression asymmetry testof the intercept (Eggerrsquos test) Finally the quality of thebody of evidence was graded as ldquohighrdquo ldquomoderaterdquo ldquolowrdquoor ldquovery lowrdquo [10]
lar coiling for each outcome
ndom effectsR (95 CI)
Fixed effectsOR (95 CI)
I2 HeterogeneityP
2 (050 404) 142 (050 404) 0 069
5 (042 374) 125 (042 374) 0 065
5 (091 261) 135 (107 170) 52 008
5 (091 1230) 346 (220 544) 83 0003
8 (133 426) 238 (133 426) 0 099
2 (116 634) 272 (116 634) 0 081
2 (093 484) 212 (093 484) 0 090
1 (119 490) 241 (119 490) 0 084
2 (084 639) 232 (084 639) 0 092
3 (142 563) 283 (142 563) 0 081
0 072
6 (083 464) 144 (103 202) 63 001
7 (069 166) 096 (074 123) 39 008
4 (109-347) 138 (112 171) 58 0009
1 (115 550) 251 (115 550) 0 098
GOS Glasgow Outcome Scale Values for a random-effects model are
Hwang et al BMC Neurology 2012 1299 Page 4 of 7httpwwwbiomedcentralcom1471-23771299
Meta-analyses were conducted using ComprehensiveMeta-analysis 20 (Biostat Englewood NJ USA) and thequality of evidence and strength of recommendation weregraded using GRADEprofiler 322 (GRADE WorkingGroup)
ResultsThe authors independently reviewed titles and abstractsof 3135 identified unique studies 2462 studies wereexcluded The full-text publications of the remaining673 potentially eligible studies were reviewed in detailOf these 645 were excluded based on the inclusion andexclusion criteria (Figure 1) Of 1581 international stud-ies 1480 Korean domestic studies and 1099 Japanese do-mestic studies 24 observational studies reporting datafrom 31 865 patients were selected for the comprehen-sive meta-analysis Characteristics of these studies are
(A) Overall death
(B) In-hospital mortality
(C) Disability measured by the Glasgow Outcome S
Figure 2 Outcomes from neurosurgical clipping vs endovascular coil
presented in Additional file 1 and the quality of studiesare listed in Additional file 1
Meta-analysisFour outcome types (disability measured by mRS andGOS neurological and cardiac complications) showedstatistically significant differences between coiling andclipping (Table 1 Figure 2 Figure 3) Clipping had sig-nificantly higher disability as measured by GOS (OR238 95 CI 133ndash426) and mRS (OR 283 95 CI142ndash563) when compared with coiling ORs for neuro-logical (OR 194 95 CI 109ndash347) and cardiac (OR251 95 CI 115ndash550) complications were also higherwith clippingOn the other hand overall mortality in-hospital mor-
tality and complications of cerebral haemorrhage andcerebral infarction showed no statistically significant dif-ferences between the two groups There was evidence of
cale
ing
Hwang et al BMC Neurology 2012 1299 Page 5 of 7httpwwwbiomedcentralcom1471-23771299
statistical heterogeneity and the I2 range was 39 to83 which represents moderate or substantial hetero-geneity Therefore overall mortality in-hospital mortal-ity and complications of cerebral haemorrhage andcerebral infarction were incorporated into a random-effects model
(A) Cerebral haemorrhage (complications)
(B) Cerebral infarction (complications)
(C) Neurological complications
(D) Cardiac complications
Figure 3 Outcomes from neurosurgical clipping vs endovascular coil
In subgroup analysis by outcome-measurement timeclipping showed significantly higher disability measuredby GOS (OR 272 95 CI 116ndash634) in the short term(le6 m) However disability (GOS) was not significantlydifferent in the long term (gt6 m) (OR 212 95 CI093ndash484) (Table 1)
ing (complications)
Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 4 of 7httpwwwbiomedcentralcom1471-23771299
Meta-analyses were conducted using ComprehensiveMeta-analysis 20 (Biostat Englewood NJ USA) and thequality of evidence and strength of recommendation weregraded using GRADEprofiler 322 (GRADE WorkingGroup)
ResultsThe authors independently reviewed titles and abstractsof 3135 identified unique studies 2462 studies wereexcluded The full-text publications of the remaining673 potentially eligible studies were reviewed in detailOf these 645 were excluded based on the inclusion andexclusion criteria (Figure 1) Of 1581 international stud-ies 1480 Korean domestic studies and 1099 Japanese do-mestic studies 24 observational studies reporting datafrom 31 865 patients were selected for the comprehen-sive meta-analysis Characteristics of these studies are
(A) Overall death
(B) In-hospital mortality
(C) Disability measured by the Glasgow Outcome S
Figure 2 Outcomes from neurosurgical clipping vs endovascular coil
presented in Additional file 1 and the quality of studiesare listed in Additional file 1
Meta-analysisFour outcome types (disability measured by mRS andGOS neurological and cardiac complications) showedstatistically significant differences between coiling andclipping (Table 1 Figure 2 Figure 3) Clipping had sig-nificantly higher disability as measured by GOS (OR238 95 CI 133ndash426) and mRS (OR 283 95 CI142ndash563) when compared with coiling ORs for neuro-logical (OR 194 95 CI 109ndash347) and cardiac (OR251 95 CI 115ndash550) complications were also higherwith clippingOn the other hand overall mortality in-hospital mor-
tality and complications of cerebral haemorrhage andcerebral infarction showed no statistically significant dif-ferences between the two groups There was evidence of
cale
ing
Hwang et al BMC Neurology 2012 1299 Page 5 of 7httpwwwbiomedcentralcom1471-23771299
statistical heterogeneity and the I2 range was 39 to83 which represents moderate or substantial hetero-geneity Therefore overall mortality in-hospital mortal-ity and complications of cerebral haemorrhage andcerebral infarction were incorporated into a random-effects model
(A) Cerebral haemorrhage (complications)
(B) Cerebral infarction (complications)
(C) Neurological complications
(D) Cardiac complications
Figure 3 Outcomes from neurosurgical clipping vs endovascular coil
In subgroup analysis by outcome-measurement timeclipping showed significantly higher disability measuredby GOS (OR 272 95 CI 116ndash634) in the short term(le6 m) However disability (GOS) was not significantlydifferent in the long term (gt6 m) (OR 212 95 CI093ndash484) (Table 1)
ing (complications)
Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 5 of 7httpwwwbiomedcentralcom1471-23771299
statistical heterogeneity and the I2 range was 39 to83 which represents moderate or substantial hetero-geneity Therefore overall mortality in-hospital mortal-ity and complications of cerebral haemorrhage andcerebral infarction were incorporated into a random-effects model
(A) Cerebral haemorrhage (complications)
(B) Cerebral infarction (complications)
(C) Neurological complications
(D) Cardiac complications
Figure 3 Outcomes from neurosurgical clipping vs endovascular coil
In subgroup analysis by outcome-measurement timeclipping showed significantly higher disability measuredby GOS (OR 272 95 CI 116ndash634) in the short term(le6 m) However disability (GOS) was not significantlydifferent in the long term (gt6 m) (OR 212 95 CI093ndash484) (Table 1)
ing (complications)
Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 6 of 7httpwwwbiomedcentralcom1471-23771299
We found no apparent systematic bias in the overalland subgroup meta-analyses as assessed by a funnel plotand test (Table 2)
Additional analysisThe re-intervention rate for endovascular coiling was 2to 154 in five studies Coil compaction within thefollow-up period is a common cause in most cases Incontrast only two clipping studies reported re-intervention the rate of neurosurgical clipping was 0in one study and 23 in the other
DiscussionThis study showed that coiling is associated with lessharm than clipping in terms of disability measured bymRS and GOS neurological and cardiac complicationsbut all of the studies included were observational It isdifficult to randomise controlled trials of surgical inter-vention in terms of such factors consequently observa-tional studies may be the best available evidence This isthe first comprehensive systematic review and meta-analysis comparing clipping and coiling in patients withUIA King et al [11] and Raaymakers et al [12] foundmortality rates of 10 and 26 and morbidity rates of41 and 109 respectively in meta-analyses of the out-come of clipping for UIA Ontario [13] performed a sys-tematic review on the outcome of clipping forintracranial aneurysms including UIA These previousstudies were systematic reviews of only a single interven-tion and did not compare interventions with one an-other Therefore the present study is meaningful despitesome limitationsSixteen accessible electronic databases were searched
including major international databases and Korean andJapanese domestic databases without language restric-tion The aneurismal subarachnoid haemorrhage inci-dence rate in Japan is more than double those in otherregions [14] so Japanese domestic databases wereincluded in the searchAfter an extensive search and review 24 studies were
identified (n = 31 865) among 4160 studies Clipping
Table 2 Publication-bias test
Outcome Egger Test P-value Begg Test P-value
Overall death 05762 1000
In-hospital mortality 03218 04624
Disability (GOS) 07071 09170
Complication
Cerebral haemorrhage 04102 09015
Cerebral infarction 05302 06312
Neurological complication 02501 08763
Cardiac complication 08927 07071
resulted in significantly higher disability as measured byGOS (overall and short-term [le6 m]) but this significantdifference between the two groups disappeared over thelong term (gt6 m) Clipping is considered a type of crani-otomy and a more invasive treatment than coilingTherefore patients may suffer short-term andor long-term disability as a result of surgery However some ofthese disabilities may disappear over time with healingand therapyClipping had 2ndash25 times as many neurological compli-
cations and cardiac complications than coiling The majorcomplication differed based on the treatment method forexample ischemic injury caused by vasoocclusion andvasoconstriction during surgery was common in clippingwhereas thromboembolism caused by the endovascularprocedure and procedure-related rupture during endovas-cular therapy were common in coilingHowever although the cause of ischemic or haemor-
rhagic brain injury differed the types of injury weresimilar (ischemic or haemorrhagic) Therefore thesecomplications were directly compared between the clip-ping and coiling groups No significant differences werefound between clipping and coiling in the present studyHowever another study using the national impatientsample database showed that in-hospital deaths andperioperative complications (ie intracerebral haemor-rhage and acute ischemic stroke) were higher with clip-ping than with coiling [15]This study had several limitations First the selected
studies were all observational because we did not findany well-designed prospective randomised compara-tive clinical trials Therefore the levels of evidence forall outcomes were ldquovery lowrdquo in keeping with the qual-ity of evidence assessment dictated by GRADEprofilerSecond the analysis did not examine outcomes accord-ing to the size and location of aneurysms The infor-mation about sizelocation of aneurysms in theselected studies was either not found or was uselessbecause treatment outcomes were not reported foreach size and location
ConclusionsIn conclusion endovascular coiling has benefits in UIAtreatment in terms of low disability after treatment inthe short term and fewer complications compared withneurosurgical clipping However because most of thereviewed studies were retrospective cohort studies fur-ther well-designed prospective randomised comparativeclinical trials are required to verify these results
Additional file
Additional file 1 Characteristics of identified publications
Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-

Hwang et al BMC Neurology 2012 1299 Page 7 of 7httpwwwbiomedcentralcom1471-23771299
Competing interestsThe author(s) declare that we have no competing interests
Authors contributionsMKH Draft the protocol M K H JEC Develop a search strategy MKH JECSearch for articles NRL EJL Obtain copies of articles HJL JEC JSHMKHSelect which articles to include HJL JEC JSHMKH Extract data from articlesHJL JEC JHK JSH NRL MKH Evaluate the quality of articles MKH JSH Carryout the analysis MKH JSH Interpret the analysis MKH JSH JWK Draft thefinal review MKH Update the review All authors read and approved thefinal manuscript
AcknowledgementsThis study was funded by the National Evidence-based HealthcareCollaborating Agency (NECA) project no NA2010-012
Author details1National Evidence-based Healthcare Collaborating Agency Changkyung BD8 F 28-7 Wonnam-dong Seoul Jongno-gu 110-450 Korea 2KyungpookNational University 80 Daehakro Daegu Bukgou 702-701 Korea
Received 29 November 2011 Accepted 18 September 2012Published 22 September 2012
References1 Byun HS Recent trends in the treatment of cerebral aneurysms
comparison between endovascular coil embolization and surgicalclipping Neurointervention 2009 41ndash5
2 Yoshimoto Y Wakai S Cost-effectiveness analysis of screening forasymptomatic unruptured intracranial aneurysms A mathematical modelStroke 1999 30(8)1621ndash1627
3 Nieuwkamp DJ Algra A Blomqvist P Adami J Buskens E Koffijberg HRinkel GJ Excess mortality and cardiovascular events in patientssurviving subarachnoid hemorrhage a nationwide study in SwedenStroke 2011 42(4)902ndash907
4 Van Der Schaaf I Algra A Wermer M Molyneux A Clarke M Van Gijn JRinkel G Endovascular coiling versus neurosurgical clipping for patientswith aneurysmal subarachnoid haemorrhage Cochrane Database Syst Rev2005 19(4)CD003085
5 Komotar RJ Mocco J Solomon RA Guidelines for the surgical treatmentof unruptured intracranial aneurysms the first annual J Lawrence poolmemorial research symposium--controversies in the management ofcerebral aneurysms Neurosurgery 2008 62(1)183ndash193 discussion 193ndash184
6 Smith GA Dagostino P Maltenfort MG Dumont AS Ratliff JK Geographicvariation and regional trends in adoption of endovascular techniques forcerebral aneurysms J Neurosurg 2011 114(6)1768ndash1777
7 Banks JL Marotta CA Outcomes validity and reliability of the modifiedRankin scale implications for stroke clinical trials a literature review andsynthesis Stroke 2007 38(3)1091ndash1096
8 Jennett B Snoek J Bond MR Brooks N Disability after severe head injuryobservations on the use of the Glasgow Outcome Scale J NeurolNeurosurg Psychiatry 1981 44(4)285ndash293
9 Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi JMethodological index for non-randomized studies (minors)development and validation of a new instrument ANZ J Surg 200373(9)712ndash716
10 In Cochrane handbook for systematic reviews of interventions version 510 TheCochrane Collaboration 2011 Edited by Higgins JPT Green S Available fromwwwcochrane-handbookorg
11 King JT Jr Berlin JA Flamm ES Morbidity and mortality from electivesurgery for asymptomatic unruptured intracranial aneurysms ameta-analysis J Neurosurg 1994 81(6)837ndash842
12 Raaymakers TW Rinkel GJ Limburg M Algra A Mortality and morbidity ofsurgery for unruptured intracranial aneurysms a meta-analysis Stroke1998 29(8)1531ndash1538
13 Secretariat MA Coil embolization for intracranial aneurysms anevidence-based analysis Ontario Health Technology Assessment Series 20066(1)1ndash114
14 de Rooij NK Linn FH van der Plas JA Algra A Rinkel GJ Incidence ofsubarachnoid haemorrhage a systematic review with emphasis onregion age gender and time trends J Neurol Neurosurg Psychiatry 200778(12)1365ndash1372
15 Alshekhlee A Mehta S Edgell RC Vora N Feen E Mohammadi A Kale SPCruz-Flores S Hospital mortality and complications of electively clippedor coiled unruptured intracranial aneurysm Stroke 2010 41(7)1471ndash1476
doi1011861471-2377-12-99Cite this article as Hwang et al Endovascular coiling versusneurosurgical clipping in patients with unruptured intracranialaneurysm a systematic review BMC Neurology 2012 1299
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
- Abstract
-
- Background
- Methods
- Results
- Conclusions
-
- Background
- Methods
-
- Literature search
- Study selection data extraction and quality assessment
- Meta-analysis and grading the quality of the evidence
-
- Results
-
- Meta-analysis
- Additional analysis
-
- Discussion
- Conclusions
- Additional file
- Competing interests
- Authors contributions
- Acknowledgements
- Author details
- References
-