Endothelin-1 gene polymorphism in sudden sensorineural hearing loss
7
The Laryngoscope V C 2013 The American Laryngological, Rhinological and Otological Society, Inc. Endothelin-1 Gene Polymorphism in Sudden Sensorineural Hearing Loss Yasue Uchida, MD, PhD; Masaaki Teranishi, MD, PhD; Naoki Nishio, MD, PhD; Saiko Sugiura, MD, PhD; Mariko Hiramatsu, MD, PhD; Hidenori Suzuki, MD, PhD; Ken Kato, MD, PhD; Hironao Otake, MD, PhD; Tadao Yoshida, MD, PhD; Mitsuhiko Tagaya, MD, PhD; Hirokazu Suzuki, MD, PhD; Michihiko Sone, MD, PhD; Fujiko Ando, MD, PhD; Hiroshi Shimokata, MD, PhD; Tsutomu Nakashima, MD, PhD Objectives/Hypothesis: Endothelin-1 is a potent vasoconstrictor peptide that is widely distributed throughout the mammalian body including the spiral modiolar artery, vestibule, and cochlea. This study aimed to investigate the association between the Lys198Asn (G/T) polymorphism (rs5370) of the endothelin-1 gene and sudden sensorineural hearing loss (SSNHL). Study Design: Case-control study. Methods: Seventy-two SSNHL patients (mean age, 58.3 6 14.0 years) were compared with 2,159 controls included in a community-based study of aging. Multiple logistic regression was used to obtain odds ratios (ORs) for SSNHL. In subgroup analysis, patients with SSNHL who visited to the hospital within the first month of onset were selected to assess audiometric features according to genotype. Pure-tone averages at 250, 500, 1,000, 2,000, and 4,000 Hz were calculated in the affected ear. Results: Under the recessive genetic model, after adjustment for age, sex, histories of hypertension, dyslipidemia and diabetes, the crude and adjusted ORs for SSNHL risk were 2.209 (95% confidence interval [CI]: 1.140-4.281) and 2.173 (95% CI: 1.086-4.348), respectively. No significant ORs were observed under the additive and dominant models. The severity of SSNHL differed significantly between genotypes. The mean pure-tone averages at the initial visit were 78.6, 66.4, and 57.8 dB for the GG, GT, and TT genotypes, respectively (P 5.034). Conclusions: Our study indicates that the recessive genotype was significantly associated with increased SSNHL risk; however, the severity was lower in these individuals than it was in those with the wild-type genotype. Endothelin-1 may be implicated in SSNHL. Key Words: Sudden sensorineural hearing loss, endothelin-1, polymorphism, odds ratio. Level of Evidence: 3b Laryngoscope, 123:E59–E65, 2013 INTRODUCTION Endothelin-1, which is known as an extremely potent vasoconstrictor peptide, is one of the prominent endothelial mediators. 1 It is widely distributed through- out the mammalian body in cardiovascular and noncar- diovascular tissues, including the nervous system, 2,3 and is also expressed in the spiral modiolar artery, endolym- phatic sac, vestibule, stria vascularis, and spiral gan- glion cells. 4–6 The distribution provides a fair idea of how endothelin-1 functions in the inner ear. It is advo- cated that endothelin-1 plays a role in regulating the function of the inner ear as a peptide with mitogenic, antiapoptotic, and neural-transmission effects. 7 The human endothelin-1 (EDN1) gene is located on chromosome 6p and consists of five short exons and four introns. Various single nucleotide polymorphisms (SNPs) have been identified in the EDN1 gene and have been reported to be associated with the susceptibility and prognosis of various diseases, including hyperten- sion, glaucoma, heart failure, diabetic retinopathy, and atherosclerosis. 8–12 The Lys198Asn (G/T) polymorphism (rs5370) is one of the well-researched SNPs of EDN1. From the Department of Otorhinolaryngology (Y.U.), Aichi Medical University, Nagakute, Aichi; Department of Otorhinolaryngology (Y .U., S.S.), National Center for Geriatrics and Gerontology, Aichi; Department of Otorhinolaryngology (M.T., N.N., M.H., HIDENORI.S., K.K., H.O., T.Y., M.T., HIR- OKAZU.S., M.S., T.N.), Nagoya University Graduate School of Medicine, Nagoya; Department of Head and Neck Surgery (HIDENORI.S.), Aichi Can- cer Center, Nagoya; Department of Otorhinolaryngology (M.T.), Tosei General Hospital, Seto, Aichi; Department of Health and Medical Scien- ces (F .A.), Aichi Shukutoku University, Aichi; Department for Develop- ment of Preventive Medicine (F .A., H.SHIMOKATA), Center for Development of Advanced Medicine for Dementia, National Center for Geriatrics and Gerontology, Aichi, Japan. This Manuscript was received on March 20, 2013, revised on May 12, 2013, and accepted for publication on June 14, 2013. Presented orally at the First Asian Otology Meeting and the Third East Asian Symposium on Otology, Nagasaki, Japan, June 3, 2012. This study was supported in part by the Research Grant for Lon- gevity Sciences (20shi-2), by the Research Grant for Longevity Sciences (21A-17, H20-Nanchi-021) from the Ministry of Health, Labour, and Wel- fare, and by research grants (21390460, 20591979) from the Ministry of Education, Culture, Sports, Science, and Technology, Japan. The authors have no funding, financial relationships, or conflicts of interest to disclose. Address correspondence to: Yasue Uchida, MD, Department of Oto- rhinolaryngology, Aichi Medical University, Nagakute, Aichi, 480–1195 Japan. E-mail: [email protected] DOI: 10.1002/lary.24298 Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL E59
Transcript of Endothelin-1 gene polymorphism in sudden sensorineural hearing loss

The LaryngoscopeVC 2013 The American Laryngological,Rhinological and Otological Society, Inc.
Endothelin-1 Gene Polymorphism in Sudden Sensorineural Hearing
Loss
Yasue Uchida, MD, PhD; Masaaki Teranishi, MD, PhD; Naoki Nishio, MD, PhD;
Saiko Sugiura, MD, PhD; Mariko Hiramatsu, MD, PhD; Hidenori Suzuki, MD, PhD;
Ken Kato, MD, PhD; Hironao Otake, MD, PhD; Tadao Yoshida, MD, PhD; Mitsuhiko Tagaya, MD, PhD;
Hirokazu Suzuki, MD, PhD; Michihiko Sone, MD, PhD; Fujiko Ando, MD, PhD;
Hiroshi Shimokata, MD, PhD; Tsutomu Nakashima, MD, PhD
Objectives/Hypothesis: Endothelin-1 is a potent vasoconstrictor peptide that is widely distributed throughout themammalian body including the spiral modiolar artery, vestibule, and cochlea. This study aimed to investigate the associationbetween the Lys198Asn (G/T) polymorphism (rs5370) of the endothelin-1 gene and sudden sensorineural hearing loss(SSNHL).
Study Design: Case-control study.Methods: Seventy-two SSNHL patients (mean age, 58.36 14.0 years) were compared with 2,159 controls included in a
community-based study of aging. Multiple logistic regression was used to obtain odds ratios (ORs) for SSNHL. In subgroupanalysis, patients with SSNHL who visited to the hospital within the first month of onset were selected to assess audiometricfeatures according to genotype. Pure-tone averages at 250, 500, 1,000, 2,000, and 4,000 Hz were calculated in the affectedear.
Results: Under the recessive genetic model, after adjustment for age, sex, histories of hypertension, dyslipidemia anddiabetes, the crude and adjusted ORs for SSNHL risk were 2.209 (95% confidence interval [CI]: 1.140-4.281) and 2.173 (95%CI: 1.086-4.348), respectively. No significant ORs were observed under the additive and dominant models. The severity ofSSNHL differed significantly between genotypes. The mean pure-tone averages at the initial visit were 78.6, 66.4, and 57.8 dBfor the GG, GT, and TT genotypes, respectively (P5.034).
Conclusions: Our study indicates that the recessive genotype was significantly associated with increased SSNHL risk;however, the severity was lower in these individuals than it was in those with the wild-type genotype. Endothelin-1 may beimplicated in SSNHL.
Key Words: Sudden sensorineural hearing loss, endothelin-1, polymorphism, odds ratio.Level of Evidence: 3b
Laryngoscope, 123:E59–E65, 2013
INTRODUCTIONEndothelin-1, which is known as an extremely
potent vasoconstrictor peptide, is one of the prominentendothelial mediators.1 It is widely distributed through-out the mammalian body in cardiovascular and noncar-diovascular tissues, including the nervous system,2,3 andis also expressed in the spiral modiolar artery, endolym-phatic sac, vestibule, stria vascularis, and spiral gan-glion cells.4–6 The distribution provides a fair idea ofhow endothelin-1 functions in the inner ear. It is advo-cated that endothelin-1 plays a role in regulating thefunction of the inner ear as a peptide with mitogenic,antiapoptotic, and neural-transmission effects.7
The human endothelin-1 (EDN1) gene is located onchromosome 6p and consists of five short exons and fourintrons. Various single nucleotide polymorphisms (SNPs)have been identified in the EDN1 gene and have beenreported to be associated with the susceptibilityand prognosis of various diseases, including hyperten-sion, glaucoma, heart failure, diabetic retinopathy, andatherosclerosis.8–12 The Lys198Asn (G/T) polymorphism(rs5370) is one of the well-researched SNPs of EDN1.
From the Department of Otorhinolaryngology (Y.U.), Aichi MedicalUniversity, Nagakute, Aichi; Department of Otorhinolaryngology (Y.U.,S.S.), National Center for Geriatrics and Gerontology, Aichi; Departmentof Otorhinolaryngology (M.T., N.N., M.H., HIDENORI.S., K.K., H.O., T.Y., M.T., HIR-
OKAZU.S., M.S., T.N.), Nagoya University Graduate School of Medicine,Nagoya; Department of Head and Neck Surgery (HIDENORI.S.), Aichi Can-cer Center, Nagoya; Department of Otorhinolaryngology (M.T.), ToseiGeneral Hospital, Seto, Aichi; Department of Health and Medical Scien-ces (F.A.), Aichi Shukutoku University, Aichi; Department for Develop-ment of Preventive Medicine (F.A., H.SHIMOKATA), Center for Developmentof Advanced Medicine for Dementia, National Center for Geriatrics andGerontology, Aichi, Japan.
This Manuscript was received on March 20, 2013, revised on May12, 2013, and accepted for publication on June 14, 2013.
Presented orally at the First Asian Otology Meeting and the ThirdEast Asian Symposium on Otology, Nagasaki, Japan, June 3, 2012.
This study was supported in part by the Research Grant for Lon-gevity Sciences (20shi-2), by the Research Grant for Longevity Sciences(21A-17, H20-Nanchi-021) from the Ministry of Health, Labour, and Wel-fare, and by research grants (21390460, 20591979) from the Ministry ofEducation, Culture, Sports, Science, and Technology, Japan.
The authors have no funding, financial relationships, or conflictsof interest to disclose.
Address correspondence to: Yasue Uchida, MD, Department of Oto-rhinolaryngology, Aichi Medical University, Nagakute, Aichi, 480–1195Japan. E-mail: [email protected]
DOI: 10.1002/lary.24298
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E59

Recent association studies suggest that this polymor-phism is associated with blood pressure levels andhypertension in some populations, such as in overweightindividuals.13,14 The objectives of the present study,which was designed as a case-control study, were toinvestigate the association between the rs5370 polymor-phism in the EDN1 gene and sudden sensorineuralhearing loss (SSNHL) and to investigate whether thereare any specific audiometric features in these patientsaccording to the genotypes of the rs5370 polymorphism.
MATERIALS AND METHODS
CasesSeventy-two patients (36 male and 36 female; mean age,
58.3 6 14.0 years; range, 22–82 years) affected by SSNHL whovisited the Department of Otorhinolaryngology of the NagoyaUniversity Hospital between November 2007 and January 2010were consecutively recruited and enrolled in this study. Idio-pathic SSNHL was defined according to the criteria establishedby the Sudden Deafness Research Committee of the Ministry ofHealth and Welfare, Japan. The detailed diagnostic criteriawere as described previously.15 Demographic data wererecorded via medical interviews or self-reporting. All patientshad a similar therapeutic strategy. A steroid, which was intra-venous hydrocortisone 200 mg per day and taper, vitamin Bcomplex, and adenosine triphosphate were administered inprinciple.
ControlsThe controls used in this study were derived from the
National Institute for Longevity Sciences–Longitudinal Study ofAging (NILS–LSA), which is an ongoing population-based bien-nial survey. The participants in the NILS–LSA are citizens whowere selected randomly from a database stratified according toboth age and sex, in cooperation with the local government. TheNILS–LSA study area is located within 30 km of the NagoyaUniversity Hospital. The details of the NILS–LSA have beendescribed elsewhere.16 Participants filled out a series of ques-tionnaires in advance of the examination visit. Demographicdata were recorded via self-reported questionnaires and medicalinterviews. Of these controls, 33 participants who reported ahistory of SSNHL defined as self-reported otolaryngologist diag-nosis were excluded. Overall, 2,159 participants (1,086 maleand 1,073 female; mean age, 59.2 6 10.9 years; range, 40–79years) were selected. They completed the first wave of NILS–LSA examinations between November 1997 and April 2000 andprovided blood samples for the SNP genotype analyses. Histor-ies of hypertension, diabetes, and dyslipidemia were categorizedas the presence or absence.
EthicsThe study protocol was reviewed and approved by the
ethics committees of Nagoya University (370-4) and the NationalCenter for Geriatrics and Gerontology (#14, #52, #74). Writteninformed consent was obtained from all participants.
Genotype AnalysisDNA samples were isolated from peripheral blood cells.
Genotypes were determined using an allele-specific primer/poly-merase chain reaction (PCR) assay system (Toyobo Gene Analy-sis, Tsuruga, Japan). Genotypes were also determined in control
blood samples known to be from subjects who are homozygousfor the wild-type genotype and heterozygous and homozygousfor each variant genotype. The SNP in EDN1 investigated inthe present study was a G-to-T transversion in exon 5 thatcauses a Lys-to-Asn substitution at codon 198. To determine theEDN1 genotype, the polymorphic region of the gene was ampli-fied by PCR using allele-specific sense primers labeled at the 50
end either with fluorescein isothiocyanate (50-CCAAGCT-GAAAGGCAXGC-30) or with Texas Red (50-CCCAAGCTGAAAGGCAXTC-30), and with an antisense primer labeled at the 50
end with biotin (50-TCACATAACGCTCTCTGGAGG-30). Detailsof EDN1 genotyping in a series of the current study have beengiven elsewhere.17
Audiometric Evaluation in SSNHL CasesAudiometric measurements in the SSNHL cases were per-
formed using an audiometer (model AA-79S; Rion, Tokyo,Japan) in a soundproof chamber. The initial audiograms wereobtained at the first visit, and the final audiograms were taken2 months after the onset of illness or when the impaired hear-ing was recovered completely. This timing to assess outcomemeasurement was determined to conform to our earlier study.18
Only SSNHL cases whose initial visit to our hospital was withinthe first month after the onset were selected for the analysis ofaudiometric configuration according to EDN1 genotype. Audio-gram shapes obtained from 52 SSNHL cases were assessed.Pure-tone averages (PTAs) at the initial visit were calculated asthe arithmetic mean of the hearing thresholds at 250, 500,1,000, 2,000, and 4,000 Hz in the affected ear. The severity ofhearing loss was classified, based on the PTA described above,as follows: grade 1 (<40 dB), grade 2 (40–59 dB), grade 3 (60–89 dB), and grade 4 (�90 dB), using the criteria of the gradingsystem determined by the Research Committee on Acute Pro-found Deafness of the Ministry of Health and Welfare in Japan.
The outcome of SSNHL was evaluated using the criteriaof the Ministry of Health and Welfare, Japan.19 Recovery wasranked as follows: no change (improvement in hearing of <10dB on average); slight improvement (improvement in hearing of�10 dB, but <30 dB on average); remarkable improvement(improvement in hearing of �30 dB on average); and completerecovery (all five frequencies on the final audiogram were �20dB or there was improvement to the same degree of hearing asin the contralateral ear). Complete recovery and remarkableimprovement were defined as good recovery. Slight improve-ment and no recovery were defined as poor recovery.
Statistical AnalysesStatistical analyses were performed using the Statistical
Analysis System (SAS) version 9.1.3 (SAS Institute, Cary, NC).For univariate analysis, a t test was used to assess differencesin continuous variables between two groups, and comparisonsof categorical variables were performed using the v2 test. Thedistribution of severity classification according to genotype wascompared using the Cochran-Mantel-Haenszel statistics. Fisherexact test was used when the number of cell samples was <5.Unless otherwise noted, values are expressed as the mean-6 standard deviation. For multivariate analysis, a multiplelogistic regression was performed, to obtain odds ratios (ORs)for SSNHL in individuals with the polymorphism. Genotypeswere coded as follows: wild-type homozygous, GG; heterozygous,GT; and mutant homozygous, TT. We considered three differentmodes of inheritance. The additive genetic model assumes thatthere is a linear gradient in risk of SSNHL with an increasingnumber of the mutated T allele. In the dominant model, a com-parison was performed between the GG genotype and the
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E60

combined GT and TT genotypes. Finally, in the recessive model,a comparison was performed between the combined GG and GTgenotypes and the TT genotype. Subsequently, each geneticmodel was analyzed with and without adjustment for confound-ing variables as follows: in model 1, unadjusted; in model 2,adjustment for age and sex; in model 3, adjustment for historiesof hypertension, dyslipidemia, and diabetes, in addition to thoseof model 2. In model 3, 15 samples with uncertain medical his-tories were eliminated.
RESULTSTable I shows the profiles of the SSNHL case and
control groups. No significant differences in sex or agewere found between SSNHL cases and controls. Theobserved differences between cases and controls regard-ing rs5370 genotype frequencies were marginally signifi-cant (P 5.054). The TT genotype frequencies in SSNHLcases and controls were 15.3 % and 7.6 %, respectively.The minor allele frequencies were 32.6% and 27.2%,respectively (P 5.153). The characteristics of the subjectsdid not differ significantly between cases and controlsexcept for the prevalence of diabetes. The prevalence ofdiabetes was significantly higher in the cases than incontrols (P 5.011).
ORs for SSNHL under additive, dominant, andrecessive genetic models obtained by multiple logisticregression are presented in Table II. The crude OR forSSNHL risk was 2.209 (95% confidence interval [CI]:1.140-4.281) and adjusted OR in model 2 and 3 were2.000 (95% CI: 1.005-3.978) and 2.173 (95% CI: 1.086-4.348), respectively, under the recessive model. A signifi-cant effect of the recessive homozygous (TT) genotype onthe increase in SSNHL risk was shown. The ORs forSSNHL risk in models 1, 2, and 3 were 1.290 (95% CI:0.907-1.835), 1.236 (95% CI: 0.864-1.766), and 1.261(95% CI: 0.878-1.811), respectively, under the additivemodel, and 1.131 (95% CI: 0.707-1.809), 1.101 (95% CI:0.686-1.767), and 1.105 (95% CI: 0.688-1.776), respec-tively, under the dominant model. No statistically signif-icant ORs were observed under the additive anddominant genetic models.
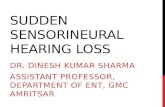
Audiometric shapes according to genotype weredemonstrated in the analysis of the subgroup patientswho visited our hospital within 1 month after SSNHL
onset. Twenty-eight individuals had GG genotype, 15had the GT genotype, and nine had the TT genotype.Overlapping audiograms according to the group ofEDN1 genotype at the first and final measurement arepresented in Figure 1. The distribution of severity classi-fication and recovery outcome according to group ofEDN1 genotype is shown in Table III. Severity differedsignificantly among genotypes (Cochran-Mantel-Haens-zel test, P 5.019). The mean PTAs at the initial visitwere 78.6, 66.4, and 57.8 dB for the GG, GT, and TTgenotypes, respectively. There was a statistically signifi-cant difference in the mean PTAs according to genotype(analysis of variance, P 5.034). In the final measure-ment, the good recovery rates were 32.1, 53.3, and33.3% for the GG, GT, and TT genotypes, respectively.There was no significant difference among genotypesregarding the recovery outcome (v2 test, P 5.373). Otherbaseline clinical characteristics, such as age, period fromonset to first visit to our hospital, vertigo, and tinnitus,which can affect the prognosis of hearing recovery, werenot significantly different among the three groups.
DISCUSSIONIn the present study, a significant association was
observed between the rs5370 EDN1 polymorphism andSSNHL risk, although the impact of the polymorphismon the increase in SSNHL risk was limited to recessivehomozygotes. Interestingly, the severity of SSNHL inthe cases of recessive homozygotes seemed to be lesssevere than that observed for the other genotypes, espe-cially in wild-type homozygotes. In other words, therecessive homozygous genotype of the rs5370 polymor-phism can be susceptible to SSNHL, but the severity ofthe disease can be relatively mild. History of diabeteswas significantly prevalent in SSNHL cases, but the sig-nificance observed in OR for SSNHL risk was firmunder the recessive model with or without moderatingvariables including diabetes. Diabetes prevalence did notsignificantly differ between the GG/GT genotypes andthe TT genotype in both SSNHL cases and controls(Fisher exact test; cases, P 5.192; controls, P 5.136).
Endothelin-1 has various biological functions.7 Theendothelin-1 system is involved in the regulation of apo-ptosis, in the autocrine actions (such as proinflammatory,
TABLE I.Basic Information and Genotype Frequencies of Cases and Controls Analyzed (N 5 2,231).
SSNHL Group, n 5 72 Control Group, n 5 2,159 P
GG, n (%) 1182 (53.0) 36 (50.0) 1146 (53.1) .054
GT, n (%) 875 (39.2) 25 (34.7) 850 (39.4)
TT, n (%) 174 (7.8) 11 (15.3) 163 (7.6)
Age, yr 58.3 6 14.0 59.2 6 10.9 .480
Sex, % male 50.0 50.3 .960
Hypertension, % 33.3 25.5* .136
Diabetes, % 16.7 8.2 .011
Dyslipidemia, % 13.9 16.9† .501
*Seven persons were eliminated from the number of controls because of uncertain history of hypertension.†Twelve persons were eliminated from the number of controls because of uncertain history of dyslipidemia.
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E61

vasoconstrictor, and mitogenic actions), and may contrib-ute to tumor growth and modulate tumor-hostinteractions.20,21
The phenotypic functional role of this polymorphismis not straightforward. Rankinen et al. observed a signif-icant effect of the interaction between the genotype andcardiorespiratory fitness level on the risk of hyperten-sion.8 In that study, among low-fitness subjects, thers5370 minor allele (T; 198Asn) was associated with ahigher risk of hypertension (OR: 1.95; 95% CI: 1.36-2.81;P 5.0003), whereas this risk did not differ among geno-types in high-fitness individuals. Those authors notedthat the G-to-T transversion induced a nonsynonymousamino acid change in codon 198 of the preproendothelin-1 molecule; in contrast, codon 198 was cleaved out fromthe biologically active endothelin-1 peptides. Therefore,the functional significance of rs5370 remains to be eluci-dated. Alternative causal mechanisms, such as an effecton mRNA stability or tagging of another functional SNPor a group of functional sequence variants by rs5370must be considered.
Kaparianos et al. examined the involvement of thers5370 polymorphism and of an adenine insertion poly-morphism located 138 bp downstream of the transcrip-tion start site in the 50 untranslated region in exon 1(1138 3A/4A) in emphysematous and bronchitic chronicobstructive pulmonary disease phenotypes.20 The TTgenotype of rs5370 was protective against the develop-ment of emphysema.
Regarding plasma endothelin-1 levels, pregnantwomen with the Asn/Asn (TT) genotype have signifi-cantly elevated plasma endothelin-1 levels, and the Asnallele (T allele) has been associated with raised systolicblood pressure during pregnancy.22 The combination ofLys198Lys with another EDN-1 gene polymorphismwas associated with lower endothelin-1 levels in
high-altitude natives and was considered as an adapta-tion to hypobaric hypoxic conditions.23 Expression stud-ies have shown an absence of differences in endothelin-1levels between Asn (T allele) carriers and Lys (G allele)carriers. It has been suggested that this polymorphismis in linkage disequilibrium with other EDN1 variants/genes/environmental factors that may influenceendothelin-1 expression.1
Several theories have been proposed to explain theetiopathogenesis of SSNHL, including viral infection,vascular occlusion, breaks of labyrinthine membranes,immune-mediated mechanisms, and abnormal cellularstress responses within the cochlea.24 Among thehypothesized pathologies of SSNHL, impaired inner earperfusion and ischemic vascular damage of the cochleaare widely recognized as possible pathogenic mecha-nisms. Although the recessive TT homozygous genotypemay contribute to susceptibility to SSNHL, this diseasewas less severe in these individuals than in cases withthe wild-type homozygous genotype. This finding sug-gests that endothelin-1 plays a complex role in thepathogenesis of SSNHL. Furthermore, the expressionand localization of endothelin-1 and its receptors in thecochlea may be responsible for the severity of SSNHL.Previous reports demonstrated the extensive distributionof endothelin-1 in the cochlear lateral wall5 and in thespiral ganglions in guinea pigs.6 In addition, Liu et al.reported that EDN1 and the genes encoding the endo-thelin type-A receptor (EDNRA) and endothelin type-Breceptor (EDNRB) were expressed in mouse spiral gan-glion tissues.7 It was speculated that the distribution ofendothelin-1 in the spiral ganglion neurons suggests itspotential function as a neurotransmitter to transmitsound signals, or as a neuromodulator to modulate therelease of other neural factors. Interestingly, however,the localization of endothelin-1, EDNRA and EDNRB in
TABLE II.Odds Ratios for SSNHL Risk by Polymorphisms in EDN1.
Mode of Inheritance
GG (T 5 0) GT (T51) TT (T52) P
Additive genetic model* Model 1 1 1.290 (0.907-1.835)/T-allele .156
Model 2 1 1.236 (0.864-1.766)/T-allele .246
Model 3† 1 1.261 (0.878-1.811)/T-allele .209
GG GT/TT P
Dominant genetic model Model 1 1 1.131 (0.707-1.809) .607
Model 2 1 1.101 (0.686-1.767) .691
Model 3† 1 1.105 (0.688-1.776) .679
GG/GT TT P
Recessive genetic model Model 1 1 2.209 (1.140-4.281) .019
Model 2 1 2.000 (1.005-3.978) .048
Model 3† 1 2.173 (1.086-4.348) .028
Moderating variables: model 1: no variables, model 2: age and sex, model 3: histories of hypertension, dyslipidemia, and diabetes, in addition to thoseof model 2. Parenthetical reference shows 95% confidence interval.
*The additive genetic model assumes that there is a linear gradient in risk between the GG, GT, and TT genotypes (GG genotype base). This is equiva-lent to a comparison of the T allele versus the G allele.
†Analyzed samples declined by 15 because of missing variables (uncertain medical histories).
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E62

Fig. 1. Overlapping audiograms by groups of EDN1 genotype at the first and final measurement. The initial audiograms were obtained atthe first visit and the final audiograms were taken 2 months after the onset of illness or when the impaired hearing was recoveredcompletely.
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E63

the spiral ganglion neurons of mouse cochlea, detectedby immunohistochemistry, differed respectively. Theydemonstrated that endothelin-1 and EDNRA were pre-dominantly immunoreactive in the cytoplasm, whereasEDNRB was mainly immunostained in the nucleus ofthe neuron bodies. The authors inferred that the distri-bution difference between EDNRA and EDNRB in thespiral ganglion neurons implies different signal path-ways they activate and different roles they play. Thesereceptor gene polymorphisms also could have profoundimplications for the functional activity of endothelin-1 inthe cochlea; however, they were not examined in thepresent study. In addition, there could be another biolog-ical explanation concerning the location where the neu-rovascular action of endothelin-1 functions. Franz et al.studied the distribution of endothelin-1 and endothelin-3via indirect immunostaining of decalcified guinea pig andrat cochleae,25 and no endothelin-1 expression wasobserved in hair cells. Those authors reported that thecytoplasm of hair cells remained unstained forendothelin-1, whereas a reaction product was observed inthe synaptic areas of sensory cells. The rs5370 polymor-phism may therefore not directly affect hair cells. Thislopsided distribution of endothelin-1 may help explain thepresent results, discrepancy between susceptibility andseverity; however, the role of endothelin-1 in the develop-ment of SSNHL requires further study.
The strength of this study is found in a featureof the control group. The controls included here con-sisted of the NILS–LSA cohort of inhabitants whowere selected randomly from a register and stratified
according to both age and sex. The risk of genotypic biasin controls was therefore likely to be minimal. Theminor allele frequencies of the rs5370 single nucleotidevariation were reported in the HapMap database as0.221 in CEU (Utah residents with Northern and West-ern European ancestry from the Centre d’Etude du Poly-morphisme Humain collection), 0.314 in HapMap-HCB(Han Chinese in Beijing, China), and 0.273 in HapMap-JPT (Japanese in Tokyo). The genotype frequencies inHapMap-JPT were 0.512 for GG, 0.430 for GT, and 0.058for TT. There were no significant differences in minorallele frequency and in genotype frequencies betweenthe HapMap-JPT values and those obtained for the cur-rent controls.
Several potential limitations of the present studyshould be cited. We have to be cautious about this nota-ble result because of the small size of the case sampleused and the unconfirmed functional significance ofrs5370. Lack of replication has been cited frequently asa major problem in genetic studies of multifactorialtraits. Inadequate statistical power, and thereforeinflated type 2 error rates, are often credited for the lowreplication rates. On the basis of the current results, werealized the necessity to develop further investigation,for example, multicenter survey, to increase the numberof SSNHL cases, and to examine the functional relation-ship of rs5370 polymorphism and other EDN-1 genepolymorphisms. In parallel, studies from other popula-tions and evidence supported by basic science aredesired to clarify the etiologic contribution of endothelin-1 to SSNHL.
TABLE III.Related Information, Distribution of Severity Classification, and Recovery Outcome by Groups of EDN1 Genotype (Subgroup Patients,
n 5 52).
Related Information
Genotypes
PGG GT TT
N 28 15 9
Age of onset, yr, mean 6 SD 60.0 6 13.8 55.5 6 13.9 56.0 6 17.0 .566
Period from onset, d, mean6 SD 7.3 6 8.7 4.6 6 4.8 5.9 6 5.6 .504
Patients with vertigo (% in row) 12 (42.9) 5 (33.3) 2 (22.2) .511
Patients with tinnitus (% in row) 23 (82.1) 13 (86.7) 7 (77.8) .851
Initial measurement
Severity grade of hearing loss n (% in row) P
Grade 1, <40 dB 0 (0.0) 3 (20.0) 2 (22.2) .019
Grade 2, 40–59 dB 8 (28.6) 2 (13.3) 2 (22.2)
Grade 3, 60–89 dB 10 (35.7) 8 (53.4) 5 (55.6)
Grade 4, �90 db 10 (35.7) 2 (13.3) 0 (0.0)
Mean PTA 6 SD, dB 78.6 6 21.1 66.4 6 23.8 57.8 6 21.2 .034
Final measurement n (% in row) P
Recovery outcome
Good recovery 9 (32.1) 8 (53.3) 3 (33.3) .373
Poor recovery 19 (67.9) 7 (46.7) 6 (66.7)
PTA 5 pure-tone average; SD 5 standard deviation.
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E64

CONCLUSIONThe present case-control study demonstrated that
the recessive homozygous genotype of the EDN1 rs5370polymorphism was significantly associated with anincreased risk for SSNHL, and that the severity of SSNHLwas lower in these individuals than it was in cases withthe wild-type homozygous genotype. Endothelin-1 has vari-ous biological functions. Although the phenotypic func-tional role of the rs5370 polymorphism remains to beelucidated, endothelin-1 may be implicated in SSNHL.
ACKNOWLEDGMENTSThe authors thank all of the health professionals andresearchers from the department of Preventive Medicine,National Center for Geriatrics and Gerontology who wereinvolved in the data collection and analyses.
BIBLIOGRAPHY
1. Vadapalli S, Rani HS, Sastry B, Nallari P. Endothelin-1 and endothelialnitric oxide polymorphisms in idiopathic pulmonary arterial hyperten-sion. Int J Mol Epidemiol Genet 2010;1:208–213.
2. Naidoo V, Naidoo S, Mahabeer R, Raidoo DM. Cellular distribution of theendothelin system in the human brain. J Chem Neuroanat 2004;27:87–98.
3. Naidoo V, Naidoo S, Raidoo DM. Immunolocalisation of endothelin-1 inhuman brain. J Chem Neuroanat 2004;27:193–200.
4. Jinnouchi K, Tomiyama S, Pawankar R, Ikezono T, Yagi T. Distribution ofendothelin-1-like activity in the cochlea of normal guinea pigs. Acta Oto-laryngol 1997;117:41–45.
5. Xu DY, Tang YD, Liu SX, Liu J. Distribution and significance of endothelin1 in guinea pig cochlear lateral wall. J Laryngol Otol 2007;121:721–724.
6. Xu D, Tang Y, Liu S, Liu J. Expression and significance of endothelin 1 inspiral ganglion cells of guinea pig. Int J Pediatr Otorhinolaryngol 2008;72:189–192.
7. Liu T, Long L, Tang T, et al. Expression and localization of endothelin-1and its receptors in the spiral ganglion neurons of mouse. Cell Mol Neu-robiol 2009;29:739–745.
8. Rankinen T, Church T, Rice T, et al. Effect of endothelin 1 genotype onblood pressure is dependent on physical activity or fitness levels. Hyper-tension 2007;50:1120–1125.
9. Kim SH, Kim JY, Kim DM, et al. Investigations on the associationbetween normal tension glaucoma and single nucleotide polymorphismsof the endothelin-1 and endothelin receptor genes. Mol Vis 2006;12:1016–1021.
10. Colombo MG, Ciofini E, Paradossi U, Bevilacqua S, Biagini A. ET-1Lys198Asn and ET(A) receptor H323H polymorphisms in heart failure.A case-control study. Cardiology 2006;105:246–252.
11. Li H, Louey JW, Choy KW, et al. EDN1 Lys198Asn is associated with dia-betic retinopathy in type 2 diabetes. Mol Vis 2008;14:1698–1704.
12. Yasuda H, Kamide K, Takiuchi S, et al. Association of single nucleotidepolymorphisms in endothelin family genes with the progression of ather-osclerosis in patients with essential hypertension. J Hum Hypertens2007;21:883–892.
13. Asai T, Ohkubo T, Katsuya T, et al. Endothelin-1 gene variant associateswith blood pressure in obese Japanese subjects: the Ohasama Study.Hypertension 2001;38:1321–1324.
14. Jin JJ, Nakura J, Wu Z, et al. Association of endothelin-1 gene variantwith hypertension. Hypertension 2003;41:163–167.
15. Teranishi M, Katayama N, Uchida Y, Tominaga M, Nakashima T. Thirty-year trends in sudden deafness from four nationwide epidemiologicalsurveys in Japan. Acta Otolaryngol 2007;127:1259–1265.
16. Uchida Y, Nakashima T, Ando F, Niino N, Shimokata H. Is there a rele-vant effect of noise and smoking on hearing? A population-based agingstudy. Int J Audiol 2005;44:86–91.
17. Uchida Y, Sugiura S, Nakashima T, Ando F, Shimokata H. Endothelin-1gene polymorphism and hearing impairment in elderly Japanese. Laryn-goscope 2009;119:938–943.
18. Nakashima T, Yanagita N. Outcome of sudden deafness with and withoutvertigo. Laryngoscope 1993;103:1145–1149.
19. Nakashima T, Kuno K, Yanagita N. Evaluation of prostaglandin E1 ther-apy for sudden deafness. Laryngoscope 1989;99:542–546.
20. Kaparianos A, Sampsonas F, Lykouras D, et al. Association of ET-1 genepolymorphisms with COPD phenotypes in a Caucasian population. Mon-aldi Arch Chest Dis 2011;75:126–131.
21. Wen YF, Qi B, Liu H, et al. Polymorphisms in the endothelin-1 and endo-thelin a receptor genes and survival in patients with locoregionallyadvanced nasopharyngeal carcinoma. Clin Cancer Res 2011;17:2451–2458.
22. Barden AE, Herbison CE, Beilin LJ, Michael CA, Walters BN, VanBockxmeer FM. Association between the endothelin-1 gene Lys198Asnpolymorphism blood pressure and plasma endothelin-1 levels in normaland pre-eclamptic pregnancy. J Hypertens 2001;19:1775–1782.
23. Rajput C, Najib S, Norboo T, Afrin F, Qadar Pasha MA. Endothelin-1 genevariants and levels associate with adaptation to hypobaric hypoxia inhigh-altitude natives. Biochem Biophys Res Commun 2006;341:1218–1224.
24. Merchant SN, Durand ML, Adams JC. Sudden deafness: Is it viral? ORLJ Otorhinolaryngol Relat Spec 2008;70:52–60.
25. Franz P, Hauser-Kronberger C, Egerbacher M, et al. Localization ofendothelin-1 and endothelin-3 in the cochlea. Acta Otolaryngol 1997;117:358–362.
Laryngoscope 123: November 2013 Uchida et al.: Endothelin-1 Gene Polymorphism in SSNHL
E65