Endoscopic Ultrasound in Chronic Pancreatitis Jon Schneider March, 2011.
26
Endoscopic Ultrasound in Chronic Pancreatitis Jon Schneider March, 2011
-
Upload
jasmine-parsons -
Category
Documents
-
view
224 -
download
2
Transcript of Endoscopic Ultrasound in Chronic Pancreatitis Jon Schneider March, 2011.

Endoscopic Ultrasoundin Chronic
Pancreatitis
Jon Schneider
March, 2011

Origin of EUS
• EUS was developed initially for improving imaging of the pancreas– Sivak MV, Kaufman A. Endoscopic ultrasonography in
the differential diagnosis of pancreatic disease. A preliminary report. Scand J Gastro, 1986
• The close proximity of the pancreas to the gastric and duodenal lumen permits EUS to obtain high resolution imaging without interference by overlying bowel gas

Sonographic features ofa normal pancreas
• The following findings were noted in a study involving 130,951 patients who underwent a screening examination with transabdominal ultrasonography– PD diameter was dilated (>3 mm) in only 0.49 % of individuals
(more common in men & in older individuals).
– Cystic lesions were detected in 0.21% and calcifications in
0.05% of individuals

EUS features ofa normal pancreas
• 3 studies have evaluated the pancreas with EUS in populations of patients without clinical features or obvious risk factors for chronic pancreatitis– homogeneous fine granular appearance with smooth
margins
– main PD diameter was 2.4 mm in the head, 1.8 mm in the body, and 1.2 mm in the tail
– without evidence of side-branch ectasia
– more echogenic than liver
– A ventral anlage was detected in 45 & 66%

Reference Standards
• No agreement on an appropriate reference standard for CP– findings on EUS have been correlated with
histology, pancreatic function testing, pancreatography
– particularly problematic with early or minimal change CP

Comparison of EUS findings with
histopathology in chronic pancreatitis • 34 patients who underwent EUS followed by
pancreatectomy or open surgical biopsy– 21 for CP, 12 for pancreatic cancer
• Overall, 68% were considered to have CP based upon the histologic findings
• Total # of EUS criteria present were predictive of histologic CP
• Sensitivity & specificity using a threshold diagnosis for:– ≥3 criteria were 87% and 64%– ≥4 criteria were 78% and 73%– ≥5 criteria were 60% and 83%– ≥6 criteria were 43% and 91%
Zimmerman, MJ, Mishra, G. GIE 1997


• Aim of study was to compare ERP and EUS for the prediction of exocrine insufficiency as detected by a secretin endoscopic PFT
• Secretin PFT, EUS, ERP performed
• EUS + if >2 criteria seen
• ERCP + if Cambridge Class II or worse– >3 abnl side-branches, normal or minimally dilated PD

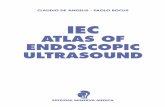
ERP findings of CP
•A: CC 0 (normal):normal main duct, noabnormal side-branches•B: CC II (mild): minimally dilated MPD with numerous abnormalside-branches•C CC III (moderate):dilated MPD &numerous abnormal side-branches,•D CC IV (severe):Dilated MPD with stones or strictures

•EUS & ERP demonstrate good agreement and are equally diagnostic in the presence of both mild and severe structural changes
•Given less risk with EUS, safer test for diagnosis of CP

• Purpose was to establish a consensus-based criteria for EUS features of CP
• 32 internationally recognized endosonographers anonymously voted on terminology of EUS features, rank order, and category (major vs minor criteria)
• Consensus was defined as greater than two thirds agreement among participants
Bradley Shepherd, MD




Normal CP-Lobularity, hyperechoic stranding, irregular PD

NormalMild: lobularity, hyperechoic foci and strands, duct irregularity
Severe: hyperechoic foci & strands, parenchymal calcifications, cystic change, lobularity
Severe: ductal dilation and intraductal calcification

•Calcification within the wall of the dilated MPD
•Parenchymal echogenic foci are present

Lobularity

Dilated pancreatic duct (7 mm) with MPD calculi with shadowing

Dilated PD with marked contour irregularity

Dilated PD with side-branch ectasia

PD with hyperechoic borders

• Interobserver Reliability Wiersema, Endoscopy, 1993
– varies depending upon the specific finding– agreement was:
• 88 % for hyperechoic foci• 94 % for focal reduced echogenicity• 94 % for lobularity• 83 % for hyperechoic duct margins• 94 % for duct irregularity
• Linear versus Radial EUS Stevens, Endoscopy, 2009
– noninferiority study of 100 patients– no significant difference between linear EUS and
radial EUS with regard to sensitivity, specificity, accuracy

Distinguishing chronic pancreatitis from pancreatic cancer
• EUS-FNA of the pancreas is challenging in patients with CP– EUS alone cannot reliably differentiate
malignant from inflammatory lesions– Cytologic evaluation of pancreatic tissue in
the setting of chronic inflammation is very difficult

•282 consecutive patients who underwent a total of 300 EUS-FNA
•The diagnostic yield and accuracy of EUS-FNA was compared between patients with and without CP
•CP defined as >4 criteria

Conclusion
• The EUS diagnosis of CP relies on quantitative and qualitative parenchymal and ductal criteria
• Generally accepted that in the absence of any criteria, CP is unlikely
• If ≥5 criteria are present, CP is likely– Despite ERCP findings
• The clinical significance of fewer (1 to 4) features found on EUS is unclear