
Endoscopic Treatment of Facial Fractures
14
Endoscopic Treatment of Facial Fractures Reid Mueller, M.D. 1 ABSTRACT The application of endoscopic surgical techniques to the treatment of craniomax- illofacial fractures not only has decreased the morbidity associated with the surgical approaches but has significantly altered the treatment philosophy for many types of fracture. Frontal sinus fractures, orbital floor fractures, zygomatic arch fractures, and subcondylar mandible fractures are the most notable examples where endoscopic techniques have found acceptance. KEYWORDS: Face, fracture, orbital floor, blowout, frontal sinus, zygomatic arch, subcondylar, mandible, endoscope, endoscopic The treatment of facial fractures has undergone several revolutions over the last century. The advent of ridged internal fixation has given us the tools to perform more accurate repairs of facial fractures while at the same time reducing much of the morbidity. Modern recon- structive surgery has focused on accurate, reliable resto- ration of the facial bony framework; however, the soft tissue sequelae of many surgical approaches persist as a lasting reminder of the original injury. The most notable examples of this are temporal wasting and scalp alopecia associated with the bicoronal approach, ectropian asso- ciated with lower lid incisions, and facial nerve injury and scar associated with approaches to subcondylar fractures. Over the last 10 years, innovative surgeons have applied alternative endoscopic approaches to facial fracture repair in an effort to achieve results equal to traditional open approaches but with reduced morbidity from the surgical approach. HISTORY OF ENDOSCOPY Endoscopy literally means to look inside (Origin: < Gk, comb. form of e´ndon within þ skopı´a, watching), typi- cally referring to looking inside the body for a medical purpose with an endoscope. Modern endoscopes consist of a ridged or flexible tube with a light delivery system usually composed of fiber optics to route light from an external source to the area of interest. There is a system of lenses in ridged endoscopes that transmit the image to an eyepiece or video camera for the surgeon. Most flexible endoscopes rely on a coherent optical fiber system to transmit the image. Many endoscopes will also have channels for irrigation, suction, or the intro- duction of surgical instruments. The first descriptions of endoscopy were by Hip- pocrates (460–375 BCE) who used rectal speculums that are little different than those used today. The Romans also had a variety of speculums used to peer into orifices and body cavities with nothing more than available light. 1 For over a century, various simple tubes were used, but the lack of good illumination hampered their use. Phillip Bozzini (1773–1809), an obstetrician, is credited with the first major endoscopic advancement to improve illumination. His invention consisted of a light guide (Lichtleiter) that would reflect candlelight via a mirror down a funnel-shaped tube. 2 The faculty in Vienna ridiculed him for his ‘‘undue curiosity’’; however, his ideas lived on. Others improved on the basic design with brighter lights and better mirrors and lens systems. 1 Division of Plastic Surgery, Oregon Health Sciences University, Portland, Oregon. Address for correspondence and reprint requests: Reid Mueller, M.D., Associate Professor, Division of Plastic Surgery, Oregon Health Sciences University, 3303 SW Bond Avenue, CH5P, Portland, OR 97239. Aesthetic Reconstruction of Head and Neck Defects; Guest Editors, Manoj T. Abraham, M.D., F.A.C.S., Keith E. Blackwell, M.D. Facial Plast Surg 2008;24:78–91. Copyright # 2008 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. DOI 10.1055/s-2008-1037452. ISSN 0736-6825. 78
Transcript of Endoscopic Treatment of Facial Fractures

Endoscopic Treatment of Facial FracturesReid Mueller, M.D.1
ABSTRACT
The application of endoscopic surgical techniques to the treatment of craniomax-illofacial fractures not only has decreased the morbidity associated with the surgicalapproaches but has significantly altered the treatment philosophy for many types of fracture.Frontal sinus fractures, orbital floor fractures, zygomatic arch fractures, and subcondylarmandible fractures are the most notable examples where endoscopic techniques have foundacceptance.
KEYWORDS: Face, fracture, orbital floor, blowout, frontal sinus, zygomatic arch,
subcondylar, mandible, endoscope, endoscopic
The treatment of facial fractures has undergoneseveral revolutions over the last century. The advent ofridged internal fixation has given us the tools to performmore accurate repairs of facial fractures while at the sametime reducing much of the morbidity. Modern recon-structive surgery has focused on accurate, reliable resto-ration of the facial bony framework; however, the softtissue sequelae of many surgical approaches persist as alasting reminder of the original injury. The most notableexamples of this are temporal wasting and scalp alopeciaassociated with the bicoronal approach, ectropian asso-ciated with lower lid incisions, and facial nerve injuryand scar associated with approaches to subcondylarfractures. Over the last 10 years, innovative surgeonshave applied alternative endoscopic approaches to facialfracture repair in an effort to achieve results equal totraditional open approaches but with reduced morbidityfrom the surgical approach.
HISTORY OF ENDOSCOPYEndoscopy literally means to look inside (Origin: <Gk,comb. form of endon withinþ skopıa, watching), typi-cally referring to looking inside the body for a medicalpurpose with an endoscope. Modern endoscopes consist
of a ridged or flexible tube with a light delivery systemusually composed of fiber optics to route light from anexternal source to the area of interest. There is a systemof lenses in ridged endoscopes that transmit the image toan eyepiece or video camera for the surgeon. Mostflexible endoscopes rely on a coherent optical fibersystem to transmit the image. Many endoscopes willalso have channels for irrigation, suction, or the intro-duction of surgical instruments.
The first descriptions of endoscopy were by Hip-pocrates (460–375 BCE) who used rectal speculums thatare little different than those used today. The Romansalso had a variety of speculums used to peer into orificesand body cavities with nothing more than availablelight.1 For over a century, various simple tubes wereused, but the lack of good illumination hampered theiruse.
Phillip Bozzini (1773–1809), an obstetrician, iscredited with the first major endoscopic advancement toimprove illumination. His invention consisted of a lightguide (Lichtleiter) that would reflect candlelight via amirror down a funnel-shaped tube.2 The faculty inVienna ridiculed him for his ‘‘undue curiosity’’; however,his ideas lived on. Others improved on the basic designwith brighter lights and better mirrors and lens systems.
1Division of Plastic Surgery, Oregon Health Sciences University,Portland, Oregon.
Address for correspondence and reprint requests: Reid Mueller,M.D., Associate Professor, Division of Plastic Surgery, Oregon HealthSciences University, 3303 SW Bond Avenue, CH5P, Portland, OR97239.
Aesthetic Reconstruction of Head and Neck Defects; Guest Editors,Manoj T. Abraham, M.D., F.A.C.S., Keith E. Blackwell, M.D.
Facial Plast Surg 2008;24:78–91. Copyright # 2008 by ThiemeMedical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001,USA. Tel: +1(212) 584-4662.DOI 10.1055/s-2008-1037452. ISSN 0736-6825.
78

Rather than shining light down a tube, MaximilianNitze (1848–1906) placed a light source on the end ofthe endoscope saying ‘‘to light up the room one mustcarry the lamp inside.’’3 He accomplished this by placinga glowing platinum wire on the end of the endoscope.A number of internal burns resulted. In further develop-ments, the glowing wire was replaced with a small lightbulb and lenses were placed into the tube to magnifyingthe image. Despite these improvements, the light andimage quality was poor.
To address the limitations of the Nitze opticalsystem Harold Hopkins (1918–1995) developed the rodlens system4 that replaced the air spaces between lenseswith solid glass rods cemented between the lenses. Thissignificantly increased light transmission and allowed forwider field of view, better color rendition, and smallercaliber endoscopes. This basic system is the basis forrigid endoscopes today.
Modern flexible endoscopes are not based on therod lens but on fiber optics. In 1930, Lamm, a Germanurologist, showed that a bundle of thin glass fibers wouldtransmit light despite flexure.5 The idea floundered untilthe 1950s, when Hopkins used fiber optics in a flexiblegastroscope to transmit light in and image out. Fibersthat are not aligned in an orderly manner (incoherent)can be used to transmit light into the body; fibers that arearranged identically on both ends (coherent) will trans-mit a useful image out.
Endoscopic techniques have revolutionized manyareas of surgery and have been applied to both aestheticand reconstructive procedures in head, neck, and cranio-maxillofacial surgery. The first applications in craniomax-illofacial surgery were for aesthetic procedures such asbrow-lifting,6–8 procerus resection,8 and forehead recon-touring.9,10 In short order, endoscopy was applied tomany different areas of the head and neck in craniomax-illofacial surgery, including cranial synostosis,11–19 resec-tion of forehead and scalp soft tissue and bony tumors,20–
25 treatment of frontal sinus fractures,26–35 decompres-sion for Graves opthamalopathy,36–41 treatment of orbitalwall fractures,42–71 distraction osteogenesis,72–76 andtreatment of zygoma fractures44,47,48,77–83 and subcon-dylar fractures.84–90
FRONTAL SINUSThe logical extension of an endoscopic brow-lift ap-proach was to apply the same techniques and tools to thetreatment of a variety of forehead pathologies, includinglipomas,21,22,24,25 benign bony tumors,91 frontozygo-matic dermoid cysts,23 and osteomas22 as well as endo-scopic reduction and internal fixation of anterior tablefractures.
It is important to remember that an isolated outertable frontal sinus fracture is a cosmetic defect. Often thescar, alopecia, and temporal wasting associated with a
bicoronal approach are more problematic than theunderlying contour defect from the fracture. The endo-scopic approach addresses this problem for isolated outertable fractures but has no application for those fractureswith significant posterior table displacement or naso-frontal duct disruption. There are two basic endoscopictreatment options: endoscopic reduction and miniplatefixation or camouflage of the contour defect.
The first reported use of an endoscope for treat-ment of a frontal sinus fracture was in 1996.26 Since then,a number of authors have reported on the reduction andminiplate fixation of isolated outer table fractures usingan endoscopic approach.28–30,32,33,92 The basic techniqueinvolves two or three small incisions placed behind thehairline in much the same way as one would approach anendoscopic brow-lift. A subperiosteal dissection exposesthe depressed anterior table fragments (Fig. 1).
The most challenging aspect of this technique isthe elevation of the depressed fragments. In the author’shands, the most reliable method to elevate the depressedsegments is to use a threaded fragment manipulator(Fig. 2)—basically a long self-drilling, self-tapping 2.0screw (Synthes, Paoli, PA) that is inserted through asmall stab incision and screwed into the depressed frag-ment or fragments. A rocking and pulling motion is thenused to reduce the fracture (Fig. 3). Often a surprisingamount of force is required to pull the fragment intoreduction in part because the original compressive forcesthat were generated during collapse of the anterior tableare re-created when elevating the fragment (Fig. 4).After the segments have been reduced, miniplates are
Figure 1 An endoscopic view of an isolated anterior table
frontal sinus fracture. The depressed segment is visible; a
green arrow points toward the supraorbital vessels and
nerve.
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 79
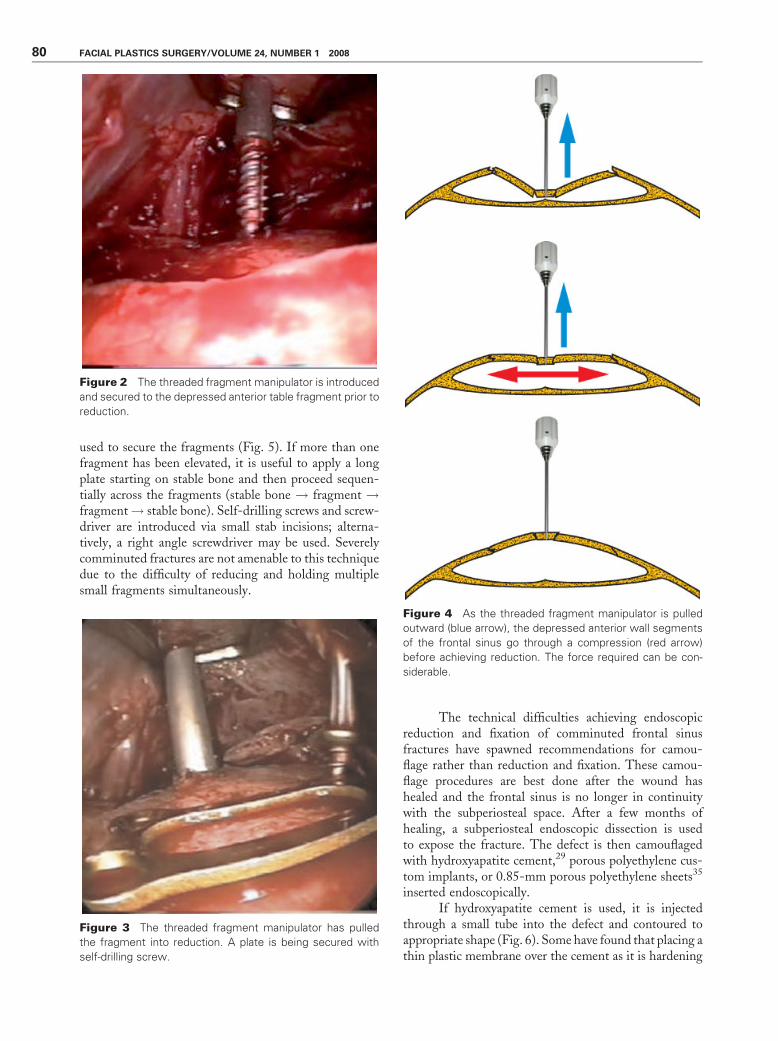
used to secure the fragments (Fig. 5). If more than onefragment has been elevated, it is useful to apply a longplate starting on stable bone and then proceed sequen-tially across the fragments (stable bone ! fragment !fragment! stable bone). Self-drilling screws and screw-driver are introduced via small stab incisions; alterna-tively, a right angle screwdriver may be used. Severelycomminuted fractures are not amenable to this techniquedue to the difficulty of reducing and holding multiplesmall fragments simultaneously.
The technical difficulties achieving endoscopicreduction and fixation of comminuted frontal sinusfractures have spawned recommendations for camou-flage rather than reduction and fixation. These camou-flage procedures are best done after the wound hashealed and the frontal sinus is no longer in continuitywith the subperiosteal space. After a few months ofhealing, a subperiosteal endoscopic dissection is usedto expose the fracture. The defect is then camouflagedwith hydroxyapatite cement,29 porous polyethylene cus-tom implants, or 0.85-mm porous polyethylene sheets35
inserted endoscopically.If hydroxyapatite cement is used, it is injected
through a small tube into the defect and contoured toappropriate shape (Fig. 6). Some have found that placing athin plastic membrane over the cement as it is hardening
Figure 2 The threaded fragment manipulator is introduced
and secured to the depressed anterior table fragment prior to
reduction.
Figure 3 The threaded fragment manipulator has pulled
the fragment into reduction. A plate is being secured with
self-drilling screw.
Figure 4 As the threaded fragment manipulator is pulled
outward (blue arrow), the depressed anterior wall segments
of the frontal sinus go through a compression (red arrow)
before achieving reduction. The force required can be con-
siderable.
80 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

makes it easier to contour the cement without fragmen-tation.
Porous polyethylene implants may be insertedendoscopically to camouflage the defect. Experimentalwork in cadavers has shown that if the defect is not toolarge, using a porous (0.85 mm) polyethylene sheetsecured with several screws is just as effective as a customimplant in resorting forehead contour.35 In addition, thesheet is readily available, inexpensive, and easy to insertthrough a small incision.
ORBITEndoscopy has been used for orbital decompression inGraves disease,36–41 transantral diagnosis of orbital frac-
tures,68,71 and assistance in locating the posterior edge inopen orbital floor repair.66 Endoscopic approaches forrepair of orbital fractures include transnasal approachwith balloon catheter stabilization,46 transconjunctivalmedial approach for medial blowout fractures,42,43,55,59
transnasal approach for medial blowout fractures,54,60,65
and transantral repair of orbital floor fractures withbone,63,70 titanium mesh,64 and porous polyethylenesheets49,50,56,64,69; endoscopic approaches can also beused for balloon stabilization52,58 and placement ofresorbable plates.61
The most accepted endoscopic approach is thetransantral approach via an upper sulcus incision andmaxillary antrostomy. Most authors agree that the bestcandidates for this procedure are those with trapdoorfractures or blowout fractures located between theinfraorbital nerve and the medial wall of the orbit.Large orbit fractures require careful restoration of orbitshape and volume that is simply not possible with thistechnique.
The approach involves an upper buccal sulcusincision and subperiosteal dissection to expose the maxillaand inferior orbital nerve. A maxillary antrostomy meas-uring about 2� 1 cm is made just below the nerve andabove the canine tooth root. A small cutout on theinferior aspect of the antrostomy forms a stable restingspot for the endoscope (Fig. 7). The endoscope is insertedinto the sinus and directed up toward the orbital floor(Fig. 8). Oxymetolazine-soaked pledgets will decreasebleeding and improve visualization. A Freerer-typeelevator is used to strip the mucosa from the margins ofthe defect and free the orbital contents from the fracturemargins. Loose, unstable bone should be removed. Oncethe entire defect is visualized and stable bone is identified,the implant can be cut to size. In the author’s opinion, thebest material for repair of the defect is 0.85-mm-thickporous polyethylene. It is possible to use titanium mesh,
Figure 5 The frontal sinus fracture is reduced then fixed
with a miniplate.
Figure 6 Hydroxyapatite cement is placed into an anterior
table fracture and contoured. The cement was introduced
through a separate stab incision; however, it may also be
applied via the other access incisions.
Figure 7 A 2� 1-cm antrostomy is made below the inferior
alveolar nerve, avoiding the canine tooth root and pyriform
aperture. A notch is cut in the inferior aspect to accommo-
date the endoscope.
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 81

bone, or bioresporbable sheets; however, the flexibility ofthe polyethylene sheets makes the placement of theimplant much easier.
The implant is cut just slightly large than thedefect. This is often a trial and error process to get the
size just right. The implant is placed into the defect inmuch the same way an acoustic ceiling tile is placed bysliding one edge into the defect, sliding the implant toone side to allow the opposite side to lift over the edge,and then sliding the implant back to the middle (Fig. 9).
Figure 8 The endoscope is inserted into the maxillary sinus to view the roof of the sinus and the floor of the orbit. A porous
polyethylene sheet is inserted from the sinus to repair the orbital floor.
Figure 9 An orbital blowout fracture is repaired via a transantral approach. (A) The blowout fracture with orbital fat bulging into
the maxillary sinus. (B) The sinus after limited mucosal stripping from the periphery of the fracture, removal of loose bone, and
insertion of a piece of porous polyethylene. (C) The prosthetic material partially inserted into the defect. (D) The implant is fully in
place and the defect repaired. Note the limited mucosal stripping. The asterisk shows the location of the maxillary sinus ostia.
82 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

One must pay particular attention to the infraorbitalnerve and make sure the implant is not impinging uponit. A forced duction test is done to make sure there is noentrapment of orbital contents.
ZYGOMAEndoscopic approaches for zygomatic arch fractureshave received the least acceptance from the craniomax-illofacial community and will only be mentioned briefly.Kobayashi et al first described the endoscopic approachfor a fractured zygoma and reported success but difficultywith the fixation.77 Lee and colleagues advocated re-moving the comminuted segment of zygoma and attach-ing a miniplate ex vivo with subsequent reinsertion andfixation proximally and distally.47,48,78 Subsequently,other authors found that 25% of patients who had exvivo plating had resorption of the arch on long-termfollow-up.81 The author has had some success withprecontouring a plate and lagging the fractured archsegments up to the plate, thereby reducing the risk ofabsorption of the comminuted segment. The techniqueinvolves an incision superior to the ear and endoscopicdissection on top of the deep temporal fascia down to thearch. At this point, a precontoured plate may be intro-duced and the fractured arch segments lagged up to theplate. This can be accomplished with a right anglescrewdriver or a small stab incision for screw application.There are several reports of transient frontal nervepalsy with endoscopic zygomatic arch approaches.80
SUBCONDYLAR MANDIBLE FRACTURESFew aspects of mandible fracture management generatemore controversy than the management of condylarprocess fractures. Traditionally, the majority of thesefractures have been managed with closed techniques.Proponents of closed treatment point to a large body ofliterature that suggests that most patients do well after aperiod of maxillomandibular fixation (MMF) followedby physiotherapy and training elastics. Although accept-able outcomes have usually been achieved with closedtreatment, clinicians advocating open reduction arguethat the failure of MMF to restore anatomy leads tocondylar deformity, mandibular dysfunction, and facialasymmetry. Open approaches have been reserved forcertain specific circumstances,93,94 which many regardas too restrictive given modern techniques. Eager forbetter and more predictable outcomes, some have turnedto open reduction with ridged fixation, and recent workreveals comparable if not superior results with the openapproach.95–107
Proponents of endoscopic-assisted approaches tocondylar process fractures have strived to accomplishequivalent anatomic reduction and ridged fixation seenwith traditional open approaches while eliminating
much of the morbidity that concerns critics of opentreatment. When applied to favorable fractures, endo-scopic-assisted treatment combines the best of open andclosed treatments. In the final analysis, it seems clear thatwe should not ask ourselves ‘‘Should condylar processfractures be treated open or closed?’’ but rather ‘‘What isthe best treatment for this particular fracture?’’ basingour decision on the patient’s age, fracture geometry, andour patient’s informed preference.
In 1997, Honda et al reported on the use ofan endoscope to improve visualization for resection ofthe mandibular angle in cases of masseteric hypertro-phy.108 The following year, Lee and colleagues pio-neered the use of endoscopy to assist in the reductionand fixation of subcondylar fractures.84,109 Over thelast decade, a number of authors have used puretransoral, transoral with cheek trochar, or submandib-ular incisions for endoscopic reduction and internalfixation.85,86,88–90,110–117 In addition to fracture treat-ment, orthognathic applications for condylectomy,costochondral graft reconstruction, and mandibularvertical ramus osteotomy have been successfully per-formed.74,87,118 In addition, foreign bodies have alsobeen successfully removed from the condylar process119
and temporomandibular joint.120
Open approaches to condylar neck fractures havenot found broader application outside the traditionalindications set forth by Zide and Kent94 in 1983 becauseof technical demands of the open approach, external scar,fear of facial nerve injury, and the belief that a closedapproach was adequate. Most surgeons accept, on anintellectual level, that fracture reduction and rigid fix-ation with restoration of anatomy is a laudable goal if itcan be achieved without undue morbidity. For mostsurgeons, the risk and demands of an external approachhave not warranted its use for routine condylar neckfractures. The endoscopic approach described here hasthe potential to reduce morbidity by limiting scar,reducing the risk to the facial nerve, and eliminatingthe need for MMF, all the while embracing the acceptedadvantages of anatomic reduction and rigid fixation. Thereduced morbidity associated with endoscopic reductionmay well expand the indications for reduction and rigidfixation in the future.
Patients with condylar process fractures are se-lected for endoscopic-assisted reduction and fixationbased on age, location of fracture, degree of comminution,direction of proximal fragment displacement, dislocationof condylar head, concomitant medical or surgical illness,and—importantly—patient choice. Contraindications arelisted in Table 1. The guidelines put forth by Zide andKent in 198394 for open treatment of condylar fracturesform a starting point for surgical decision making; how-ever, their relative indications should be broadened in thecontext of current surgical technique and decreased mor-bidity when using an endoscopic approach.
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 83

AGEThere is a consensus of opinion that most fractures inchildren are best treated with MMF. This belief is notentirely founded on solid science, and some endoscopicenthusiasts have successfully used endoscopy to assist infracture reduction for severely displaced fractures with orwithout ridged fixation. Endoscopy can be used inselected cases if conditions would otherwise favor tradi-tional open approach.
LOCATION OF FRACTUREFractures within the joint capsule and those of thecondylar neck are not amenable to endoscopic repairbecause the proximal fragment will not afford sufficient
room to accommodate at least two screws of a 2.0 plate.Most subcondylar fractures will have enough length onthe proximal fragment distal to the joint capsule toaccommodate two or three screws (Fig. 10).
DEGREE OF COMMINUTIONHigh-energy comminuted fractures are a relative contra-indication for endoscopic repair and should not beattempted by the inexperienced endoscopic surgeon.During reduction, the anterior and posterior border ofthe fracture line is used as an anatomic landmark toassess accurate reduction. Comminuted fractures willoften have fracture fragments that involve the borderand thereby obscure the landmarks. Microcomminutionwill obscure the interdigitation of small irregularitiesalong the fracture line, which ordinarily assist in precisereduction. Unfortunately, the visual limitations of en-doscopy make reliable assessment of reduction decep-tively challenging in the face of comminution.
DIRECTION OF PROXIMAL FRAGMENTDISPLACEMENTFractures with lateral displacement of the proximalfragment are the most favorable for endoscopic repair.The proximal fragment is much easier to control whenabutting the lateral surface of the distal fragment, andreduction is achieved with medially directed pressure viaa cheek trochar. When the proximal fragment is located
Table 1 Contraindications for Endoscopic Reductionand Ridged Fixation of Mandibular Condyle Fractures
Absolute Relative
Intercondylar fractures Child <12 y old
Condylar neck fractures
without sufficient room
for two fixation screws
Comminuted fracture
Any patient with medical
illness or other serious
injury who may be harmed
by a longer surgical procedure
or extended general anesthesia
Medial override of the
proximal fragment
When a simpler
method is equally
effective
Figure 10 Three broad groups of condylar fractures are: intracapsular, involving the condylar head proximal to the insertion of
the joint capsule; neck just distal to the joint capsule at the thin and slightly constricted portion of the bone; and subcondylar,
which typically extends from the lowest point of the sigmoid notch obliquely toward the posterior border of the ascending
ramus. Those fracture within the shaded area may be approached with endoscopic assistance.
84 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

medially, it is difficult to control and is partially hiddenbehind the distal fragment (Fig. 11). The mechanicsrequired for control and reduction of these fracturesrequire some experience with the technique and shouldbe reserved for those with some endoscopic experience.
DISLOCATED CONDYLAR HEADFractures associated with nondislocated condylar headsare the most favorable for endoscopic repair. A dis-placed condylar head without true dislocation canusually be relocated easily into anatomic position;however, those fractures with dislocation of the con-dylar head are more challenging.
CONCOMITANT MEDICAL OR SURGICALILLNESSAny patient with medical illness or other serious injurythat may be harmed by a longer surgical procedure orextended general anesthetic should not undergo endo-scopic repair. Patients with even mild coagulopathiespresent difficulties from persistent bleeding that mayobscure the limited visual field.
PATIENT PREFERENCEWhen no absolute of relative contraindication exists forendoscopic repair, every patient has the right to choosetheir treatment after a discussion as to the risks, benefits,and alternatives. They need to understand that the dataregarding open versus closed treatment of condylarfractures are imperfect, but that in general functionaloutcomes are at least as good if not better with openapproaches. They should clearly understand the risks oftraditional open approaches including significant scar
(especially in dark-skinned individuals) and facial nerveinjury. They should also understand that endoscopy canoffer reduced morbidity and good outcomes but that nolong-term data are yet available.
SURGICAL TECHNIQUEThe operation begins with the application of arch barsand treatment of other associated mandible fractures.Precise reduction and fixation of the other fractures willrestore the dental arch and make reduction of thecondylar segment more straightforward. After the otherfractures have been addressed, MMF is released andreplaced with elastic MMF. Elastic MMF should betight enough to maintaining proper occlusal relation-ships but not so tight as to prevent distraction of thefracture when downward traction is applied to the angleof the mandible.
The intraoral incision site and the lateral aspect ofthe mandible and condylar region are injected with a1:200,000 epinephrine solution 10 minutes prior tomaking the incision. The surgeon stands on the ipsi-lateral side, and the assistant stands on the contralateralside (Fig. 12). The endoscope video monitor is located atthe head of the bed slightly toward the contralateralshoulder. A 2-cm intraoral incision along the anteriorborder of the ascending ramus is carried down toperiosteum with electrocautery (Fig. 13). The approachis much like that used for transoral vertical ramusosteotomy. A subperiosteal dissection is used to elevatethe masseteric attachments and liberate the pterygomas-seteric sling from the posterior and inferior ramus. Widesubperiosteal dissection allows for increased mobility ofthe soft tissue envelope and improved visualization byvirtue of a larger optical cavity. It is very important thatthe dissection be strictly subperiosteal to avoid bleeding
Figure 11 A three-dimensional and coronal computed tomography scans of a patient with bilateral subcondylar fractures. The
green arrow points to the right fracture, which has a medial override of the condylar fragment. The arrow also depicts the
direction of visualization and surgical approach highlighting the inherent difficulties in controlling the condylar fragment with
medial override. To simplify the approach to these fractures, the medial override fragment should be converted to a lateral
override by distracting the fracture and displacing the fragment laterally.
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 85

that will quickly obscure the endoscopic view. Hypo-tensive anesthesia will help to minimize bleeding; how-ever, if bleeding should occur from the retromandibularvein, it is best to pack a gauze into the wound, applyexternal pressure, and wait 5 to 10 minutes—the bleed-ing will usually stop.
A 4-mm 30-degree endoscope fitted with anendoscopic brow sheath (Stortz, Carver City, CA) isinserted into the optical cavity. With the endoscope inone hand and a periosteal elevator in the other, thesubperiosteal dissection is carried proximally. Theassistant may hold the endoscope while the surgeonuses the periosteal elevator and suction to continue thedissection proximally to reveal the condylar fragment.A common mistake is to inadvertently dissect under(or medial) to the proximal fragment. This occursbecause of a failure to appreciate the degree of lateraloverride and coronal plane angulation of the proximalfragment. Once the proximal fragment is identified,the subperiosteal dissection continues on the lateralsurface up to the joint capsule, or a sufficient distanceto place the fixation hardware. Once the fracture isexposed, a cheek trochar is passed through the cheekdirectly opposite the fracture at the posterior border ofthe mandible.
Appreciation of the position of the condylarfragment will shed light on maneuvers needed to reducethe fracture. Typically, the proximal fragment issituated with a lateral override and in a flexed posture.
At this point in the operation, pharmacological musclerelaxation will assist in the reduction by paralyzingthe lateral pterygoid and masseter muscles. The initialmaneuver to reduce the fracture should be distractionof the mandibular angle downward and medialpressure on the condyle with the cheek (Fig. 14). Thedownward traction on the angle can then be released.Frequently, interfragmentary friction will hold thefracture in reduction without pressure from the cheektrochar.
Fractures are stabilized with standard five- or six-hole 2.0 craniofacial zygoma dynamic compression plates(Synthes, Paoli, PA). This particular plate is thin andmalleable enough that in situ self-contouring is possible,yet it is strong enough that plate failures are rare. Theplate is affixed with at least two 6-mm screws on eitherside of the fracture. The plate is temporarily mounted ona plate delivery device with a hinge mechanism thatallows for precise positioning of the plate (Fig. 15).Others have simply delivered the plate into the woundon a long clamp or dangling from a suture. The plateshould be positioned with at least two holes on eitherside of the fracture along the posterior border of themandible.
Figure 12 Arrangement of the surgeon, assistant, and
endoscopic video monitor in relation to a fracture.
Figure 13 Endoscopic view of the initial incision and the
subsequent dissection of the optical cavity in a subperiosteal
plane to reveal the proximal condylar fragment. Note the
angulation of the proximal fragment.
86 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

Before completing fixation, a check of the reduc-tion should be done. The anterior and posterior borderof the fracture should be inspected for anatomic align-ment. In noncomminuted fractures, this is usuallystraightforward; however, a fracture with even slightcomminution will be difficult to assess. If reduction isnot acceptable, then one screw may be removed and thefragments repositioned. Once reduction has been con-firmed, the remaining screws are placed via the cheektrochar. If possible, a second plate should be placed.
Careful inspection of the anterior and posteriorborder of the fracture will confirm proper reduction(Fig. 16). Any comminution will make assessment ofthe reduction more difficult. If the condyle was dislo-cated preoperatively and there is any uncertainty aboutthe reduction, a cross-table intraoperative lateral ceph-alogram should be obtained. The elastic MMF isreleased and the fixation is inspected while openingand closing the mouth to confirm stable fixation.MMF is not needed postoperatively. The intraoral in-cision is closed with absorbable suture.
Lee et al84 published their initial series of 22fractures in 20 patients and reported 43-mm interincisaljaw opening after 8 weeks, with restoration of premorbidocclusion and radiographic evidence of anatomic reduc-tion in 21 of 22 fractures. Patients were pleased with theaesthetic restoration of their chin projection, jaw line,and the symmetric midline movement of the chin pointon jaw opening. Late radiographs showed stable fixation,good bone healing, and no condylar resorption. Otherreports have shown encouraging results with minimalmorbidity85,87,110,112,121,122; however, good prospectivedata are not yet available.
The author has collected data on 80 fractures in72 patients: 78 of 80 fractures had anatomic reduction,and two high-energy severely comminuted fractureswhere inadequately reduced and required a second endo-scopic procedure for reduction. Interincisal opening hasaveraged 42 mm after 8 weeks. The operative time has
Figure 14 The maneuvers needed for reduction are shown. (A) Initial configuration; (B) distraction of the fracture by a
downward pull on the mandibular angle and rotation of the proximal fragment out of a flexed posture; (C) final reduction after
release of downward pull on the angle. Often the fracture will be stable in this configuration by virtue of interfragmentary friction.
Figure 15 Plate delivery device. A five- or six-hole 2.0 plate
is attached with a locking screw to this delivery device, which
is hinged to allow for positioning of the plate. After the plate is
affixed to the mandible, the plate is released from the device
with a quarter turn of the locking screw.
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 87

been decreasing as experience is gained. The averageoperative time for simple noncomminuted fractures withlateral override is about 70 minutes. There was one lateplate fracture without functional detriment to the pa-tient. One transient frontal branch palsy was observed.All patients have been pleased with the cosmetic out-come.
CONCLUSIONThe application of endoscopic techniques in cranio-maxillofacial surgery has been substantially slowercompared with other specialties. It is hoped thatcontinued technical refinements in techniques, equip-ment, and case selection will allow the endoscopicapproach to give our patients the best possible treat-ment for their fractures. Many ingenious surgicalapproaches and procedures have been identified whereendoscopic assistance significantly facilitates a givenprocedure or decreases morbidity. In many cases, theendoscope is not only an aid; it significantly alters thetreatment philosophy. The future of endoscopic cra-niomaxillofacial surgery is bright. We await goodrandomized trials to confirm our gut feeling that wecan provide equivalent care with reduced morbidityand improved patient satisfaction with the aid of anendoscope.
REFERENCES
1. Milne JS. Surgical Instruments in Greek and Roman Times.Oxford: Clarendon Press; 1907:187
2. Bozzini P. Lichtleiter, eine Erfindung zur Anschauunginnerer Teile und Krankheiten. Journal der PraktischenHeilkunde 1806;24:107–124
3. Hausmann H. [Our urologic heritage: Maximilian Nitze(1848–1906). His importance in the development ofurology]. Z Urol Nephrol 1987;80:539–543
4. Hopkins H, Kapany N. A flexible fiberscope. Nature1954;173:39–41
5. Lamm H. Biegsame Optische Gerate. Zeitschrift Instru-mentenkunde 1930;50:579–581
6. Vasconez LO, Core GB, Gamboa-Bobadilla M, et al.Endoscopic techniques in coronal brow lifting. PlastReconstr Surg 1994;94:788–793
7. McCain LA, Jones G. Application of endoscopic techniquesin aesthetic plastic surgery. Plast Surg Nurs 1995;15:149–157
8. Ramirez OM. Endoscopic subperiosteal browlift and face-lift. Clin Plast Surg 1995;22:639–660
9. Song IC, Pozner JN, Sadeh AE, Shin MS. Endoscopic-assisted recontouring of the facial skeleton: the forehead.Ann Plast Surg 1995;34:323–325; discussion 325
10. Onishi K, Maruyama Y, Sawaizumi M. Use of endoscopicsurgery for forehead recontouring. Plast Reconstr Surg1997;100:1327–1332
11. Jimenez DF, Barone CM. Endoscopic craniectomy for earlysurgical correction of sagittal craniosynostosis. J Neurosurg1998;88:77–81
12. Barone CM, Jimenez DF. Endoscopic craniectomy for earlycorrection of craniosynostosis. Plast Reconstr Surg 1999;104:1965–1973; discussion 1974–1975
13. Jimenez DF, Barone CM. Endoscopy-assisted wide-vertexcraniectomy, "barrel-stave" osteotomies, and postoperativehelmet molding therapy in the early management of sagittalsuture craniosynostosis. Neurosurg Focus 2000;9:e2
14. Jimenez DF, Barone CM, Cartwright CC, Baker L. Earlymanagement of craniosynostosis using endoscopic-assistedstrip craniectomies and cranial orthotic molding therapy.Pediatrics 2002;110(1 Pt 1):97–104
15. Stelnicki EJ. Endoscopic treatment of craniosynostosis.Atlas Oral Maxillofac Surg Clin North Am 2002;10:57–72
16. Cartwright CC, Jimenez DF, Barone CM, Baker L.Endoscopic strip craniectomy: a minimally invasive treat-ment for early correction of craniosynostosis. J NeurosciNurs 2003;35:130–138
17. Jimenez DF, Barone CM, McGee ME, Cartwright CC,Baker CL. Endoscopy-assisted wide-vertex craniectomy,barrel stave osteotomies, and postoperative helmet moldingtherapy in the management of sagittal suture craniosynos-tosis. J Neurosurg; 2004:100(5 Suppl Pediatrics)407–417
18. Cohen SR, Holmes RE, Ozgur BM, Meltzer HS, LevyML. Fronto-orbital and cranial osteotomies with resorbablefixation using an endoscopic approach. Clin Plast Surg2004;31:429–442vi
19. Murad GJ, Clayman M, Seagle MB, et al. Endoscopic-assisted repair of craniosynostosis. Neurosurg Focus 2005;19:E6
20. Weiss DD, Robson CD, Mulliken JB. Transnasal endo-scopic excision of midline nasal dermoid from the anteriorcranial base. Plast Reconstr Surg 1998;102:2119–2123
21. Kokoska MS, Branham GH, Hamilton MM, Thomas JR.Endoscopic excision of a forehead mass. Arch OtolaryngolHead Neck Surg 1997;123:815–817
22. Cronin ED, Ruiz-Razura A, Livingston CK, Katzen JT.Endoscopic approach for the resection of forehead masses.Plast Reconstr Surg 2000;105:2459–2463
Figure 16 Before and after coronal computed tomography
scans of a patient with bilateral subcondylar fractures. The
right panels show the left fracture after reduction and after
fixation.
88 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

23. Guerrissi JO. Endoscopic excision of frontozygomaticdermoid cysts. J Craniofac Surg 2004;15:618–622
24. Meningaud JP, Pitak-Arnnop P, Rigolet A, Bertrand JC.Endoscopic excision of forehead lipomas. Int J OralMaxillofac Surg 2006;35:951–953
25. Lin SD, Lee SS, Chang KP, et al. Endoscopic excision ofbenign tumors in the forehead and brow. Ann Plast Surg2001;46:1–4
26. Graham HD III, Spring P. Endoscopic repair of frontalsinus fracture: case report. J Craniomaxillofac Trauma 1996;2:52–55
27. Barone CM, Boschert MT, Jimenez DF. Usefulness ofendoscopy in craniofacial trauma. J CraniomaxillofacTrauma 1998;4:36–41
28. Lappert PW, Lee JW. Treatment of an isolated outer tablefrontal sinus fracture using endoscopic reduction andfixation. Plast Reconstr Surg 1998;102:1642–1645
29. Strong EB, Buchalter GM, Moulthrop TH. Endoscopicrepair of isolated anterior table frontal sinus fractures. ArchFacial Plast Surg 2003;5:514–521
30. Chen DJ, Chen CT, Chen YR, Feng GM. Endoscopicallyassisted repair of frontal sinus fracture. J Trauma 2003;55:378–382
31. Verret DJ, Ducic Y, Oxford L, Smith J. Hydroxyapatitecement in craniofacial reconstruction. Otolaryngol HeadNeck Surg 2005;133:897–899
32. Shumrick KA. Endoscopic management of frontal sinusfractures. Facial Plast Surg Clin North Am 2006;14:31–35
33. Steiger JD, Chiu AG, Francis DO, Palmer JN. Endoscopic-assisted reduction of anterior table frontal sinus fractures.Laryngoscope 2006;116:1936–1939
34. Strong EB, Kellman RM. Endoscopic repair of anteriortable—frontal sinus fractures. Facial Plast Surg Clin NorthAm 2006;14:25–29
35. Kim KK, Mueller RV, Huang F, Strong EB. Endoscopicrepair of anterior table: frontal sinus fractures with a medporimplant. Otolaryngol Head Neck Surg 2007;136:568–572
36. Metson R, Dallow RL, Shore JW. Endoscopic orbitaldecompression. Laryngoscope 1994;104(8 Pt 1):950–957
37. Metson R, Shore JW, Gliklich RE, Dallow RL. Endoscopicorbital decompression under local anesthesia. OtolaryngolHead Neck Surg 1995;113:661–667
38. Khan JA, Wagner DV, Tiojanco JK, Hoover LA.Combined transconjunctival and external approach forendoscopic orbital apex decompression in Graves’ disease.Laryngoscope 1995;105:203–206
39. White WA, White WL, Shapiro PE. Combined endoscopicmedial and inferior orbital decompression with transcuta-neous lateral orbital decompression in Graves’ orbitopathy.Ophthalmology 2003;110:1827–1832
40. Levy J, Puterman M, Lifshitz T, et al. Endoscopic orbitaldecompression for Graves’ ophthalmopathy. Isr Med AssocJ 2004;6:673–676
41. Kasperbauer JL, Hinkley L. Endoscopic orbital decom-pression for Graves’ ophthalmopathy. Am J Rhinol 2005;19:603–606
42. Chen CT, Chen YR, Tung TC, Lai JP, Rohrich RJ.Endoscopically assisted reconstruction of orbital medial wallfractures. Plast Reconstr Surg 1999;103:714–720; quiz 721
43. Barone CM, Gigantelli JW. Endoscopic repair of post-traumatic enophthalmos using medial transconjunctival
approach: a case report. J Craniomaxillofac Trauma 1998;4:22–26
44. Forrest CR. Application of endoscope-assisted minimal-access techniques in orbitozygomatic complex, orbital floor,and frontal sinus fractures. J Craniomaxillofac Trauma1999;5:7–12; discussion 13–14
45. Jin HR, Yeon JY, Shin SO, Choi YS, Lee DW. Endoscopicversus external repair of orbital blowout fractures. Otolar-yngol Head Neck Surg 2007;136:38–44
46. Ikeda K, Suzuki H, Oshima T, Takasaka T. Endoscopicendonasal repair of orbital floor fracture. Arch OtolaryngolHead Neck Surg 1999;125:59–63
47. Lee CH, Lee C, Trabulsy PP, Alexander JT, Lee K. Acadaveric and clinical evaluation of endoscopically assistedzygomatic fracture repair. Plast Reconstr Surg 1998;101:333–345; discussion 346–337
48. Lee C, Jacobovicz J, Mueller RV. Endoscopic repair of acomplex midfacial fracture. J Craniofac Surg 1997;8:170–175
49. Strong EB, Kim KK, Diaz RC. Endoscopic approach toorbital blowout fracture repair. Otolaryngol Head NeckSurg 2004;131:683–695
50. Strong EB. Endoscopic repair of orbital blow-out fractures.Facial Plast Surg 2004;20:223–230
51. Wallace TD, Moore CC, Bromwich MA, Matic DB.Endoscopic repair of orbital floor fractures: computedtomographic analysis using a cadaveric model. J Otolaryngol2006;35:1–7
52. Miki T, Wada J, Haraoka J, Inaba I. Endoscopic trans-maxillary reduction and balloon technique for blowoutfractures of the orbital floor. Minim Invasive Neurosurg2004;47:359–364
53. Hinohira Y, Yumoto E, Shimamura I. Endoscopic endo-nasal reduction of blowout fractures of the orbital floor.Otolaryngol Head Neck Surg 2005;133:741–747
54. Rhee JS, Lynch J, Loehrl TA. Intranasal endoscopy-assistedrepair of medial orbital wall fractures. Arch Facial Plast Surg2000;2:269–273
55. Rhee JS, Chen CT. Endoscopic approach to medial orbitalwall fractures. Facial Plast Surg Clin North Am 2006;14:17–23
56. Farwell DG, Strong EB. Endoscopic repair of orbitalfloor fractures. Facial Plast Surg Clin North Am 2006;14:11–16
57. Mohadjer Y, Hartstein ME. Endoscopic orbital fracturerepair. Otolaryngol Clin North Am 2006;39:1049–1057
58. Otori N, Haruna S, Moriyama H. Endoscopic endonasal ortransmaxillary repair of orbital floor fracture: a study of 88patients treated in our department. Acta Otolaryngol 2003;123:718–723
59. Mun GH, Song YH, Bang SI. Endoscopically assistedtransconjunctival approach in orbital medial wall fractures.Ann Plast Surg 2002;49:337–343; discussion 344
60. Naraghi M, Kashfi A. Endonasal endoscopic treatment ofmedial orbital wall fracture via rotational repositioning. AmJ Otolaryngol 2002;23:312–315
61. Persons BL, Wong GB. Transantral endoscopic orbital floorrepair using resorbable plate. J Craniofac Surg 2002;13:483–488; discussion 488–489
62. Miloro M. Endoscopically assisted repair of orbital floorfractures. Arch Facial Plast Surg 2002;4:124–125
63. Mohammad JA, Warnke PH, Shenaq SM. Endoscopicexploration of the orbital floor: a technique for transantral
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 89

grafting of floor blowout fractures. J CraniomaxillofacTrauma 1998;4:16–19; discussion 15
64. Chen CT, Chen YR. Endoscopically assisted repair oforbital floor fractures. Plast Reconstr Surg 2001;108:2011–2018; discussion 2019
65. Jin HR, Shin SO, Choo MJ, Choi YS. Endonasal endo-scopic reduction of blowout fractures of the medial orbitalwall. J Oral Maxillofac Surg 2000;58:847–851
66. Saunders CJ, Whetzel TP, Stokes RB, Wong GB, Steven-son TR. Transantral endoscopic orbital floor exploration: acadaver and clinical study. Plast Reconstr Surg 1997;100:575–581
67. Geyer G, Rochels R. [Endoscopic and echographicdiagnosis of orbital fractures]. Fortschr Ophthalmol 1984;81:119–121
68. Sandler NA, Carrau RL, Ochs MW, Beatty RL. The useof maxillary sinus endoscopy in the diagnosis of orbitalfloor fractures. J Oral Maxillofac Surg 1999;57:399–403
69. Chen CT, Chen YR. Endoscopic orbital surgery. Atlas OralMaxillofac Surg Clin North Am 2003;11:179–208
70. Nishiike S, Nagai M, Nakagawa A, et al. Endoscopictransantral orbital floor repair with antral bone grafts. ArchOtolaryngol Head Neck Surg 2005;131:911–915
71. Westphal D, Kreidler JF. Sinuscopy for the diagnosis ofblow-out fractures. J Maxillofac Surg 1977;5:180–183
72. Wiltfang J, Kessler P, Neukam FW. [Endoscopically-assisted LeFort I osteotomy in distraction procedures ofthe maxilla]. Mund Kiefer Gesichtschir 2002;6:231–235
73. Wiltfang J, Kessler P. Endoscopically assisted Le Fort Iosteotomy to correct transverse and sagittal discrepancies ofthe maxilla. J Oral Maxillofac Surg 2002;60:1142–1145;discussion 1146
74. Troulis MJ, Perrott DH, Kaban LB. Endoscopic mandib-ular osteotomy, and placement and activation of a semi-buried distractor. J Oral Maxillofac Surg 1999;57:1110–1113
75. Hierl T, Hemprich A. Endoscopically assisted intraoralmandibular distraction osteogenesis. Int J Oral MaxillofacSurg 2001;30:339–341
76. Rubin JP, Posnick JC, Yaremchuk MJ. Role of endoscopicand distraction techniques in facial and reconstructivesurgery: new technology or improved results. J CraniofacSurg 1998;9:285–299
77. Kobayashi S, Sakai Y, Yamada A, Ohmori K. Approachingthe zygoma with an endoscope. J Craniofac Surg 1995;6:519–524
78. Lee CH, Lee C, Trabulsy PP. Endoscopic-assisted repair ofa malar fracture. Ann Plast Surg 1996;37:178–183
79. Cheski PJ, Matthews TW. Endoscopic reduction andinternal cyanoacrylate fixation of the zygoma. J Otolaryngol1997;26:75–79
80. Chen CT, Lai JP, Chen YR, et al. Application of endoscopein zygomatic fracture repair. Br J Plast Surg 2000;53:100–105
81. Krimmel M, Cornelius CP, Reinert S. Endoscopicallyassisted zygomatic fracture reduction and osteosynthesisrevisited. Int J Oral Maxillofac Surg 2002;31:485–488
82. Czerwinski M, Lee C. Traumatic arch injury: indicationsand an endoscopic method of repair. Facial Plast Surg 2004;20:231–238
83. Czerwinski M, Lee C. The rationale and technique ofendoscopic approach to the zygomatic arch in facial trauma.Facial Plast Surg Clin North Am 2006;14:37–43
84. Lee C, Mueller RV, Lee K, Mathes SJ. Endoscopicsubcondylar fracture repair: functional, aesthetic, and radio-graphic outcomes. Plast Reconstr Surg 1998;102:1434–1443;discussion 1444–1435
85. Schmelzeisen R, Lauer G, Wichmann U. [Endoscope-assisted fixation of condylar fractures of the mandible].Mund Kiefer Gesichtschir 1998;2(Suppl 1):S168–S170
86. Sandler NA, Andreasen KH, Johns FR. The use ofendoscopy in the management of subcondylar fractures ofthe mandible: a cadaver study. Oral Surg Oral Med OralPathol Oral Radiol Endod 1999;88:529–531
87. Troulis MJ, Kaban LB. Endoscopic approach to the ramus/condyle unit: clinical applications. J Oral Maxillofac Surg2001;59:503–509
88. Schon R, Gutwald R, Schramm A, Gellrich NC, Schmel-zeisen R. Endoscopy-assisted open treatment of condylarfractures of the mandible: extraoral vs intraoral approach. IntJ Oral Maxillofac Surg 2002;31:237–243
89. Kellman RM. Endoscopically assisted repair of subcondylarfractures of the mandible: an evolving technique. ArchFacial Plast Surg 2003;5:244–250
90. Kellman RM. Endoscopic approach to subcondylar man-dible fractures. Facial Plast Surg 2004;20:239–247
91. Onishi K, Osaki M, Maruyama Y. Endoscopic osteosyn-thesis for frontal bone fracture. Ann Plast Surg 1998;40:650–654
92. Shumrick KA, Ryzenman JM. Endoscopic management offacial fractures. Facial Plast Surg Clin North Am 2001;9:469–474
93. Zide MF. Open reduction of mandibular condyle fractures.Indications and technique. Clin Plast Surg 1989;16:69–76
94. Zide MF, Kent JN. Indications for open reduction ofmandibular condyle fractures. J Oral Maxillofac Surg 1983;41:89–98
95. de Amaratunga NA. Mouth opening after release ofmaxillomandibular fixation in fracture patients. J OralMaxillofac Surg 1987;45:383–385
96. Ellis E III, Throckmorton GS. Bite forces after open orclosed treatment of mandibular condylar process fractures.J Oral Maxillofac Surg 2001;59:389–395
97. Ellis E III, Simon P, Throckmorton GS. Occlusal resultsafter open or closed treatment of fractures of the mandibularcondylar process. J Oral Maxillofac Surg 2000;58:260–268
98. Ellis E III, Throckmorton G. Facial symmetry after closedand open treatment of fractures of the mandibular condylarprocess. J Oral Maxillofac Surg 2000;58:719–728; discussion729–730
99. Jeter TS, Van Sickels JE, Nishioka GJ. Intraoral openreduction with rigid internal fixation of mandibularsubcondylar fractures. J Oral Maxillofac Surg 1988;46:1113–1116
100. Klotch DW, Lundy LB. Condylar neck fractures of themandible. Otolaryngol Clin North Am 1991;24:181–194
101. Konstantinovic VS, Dimitrijevic B. Surgical versus con-servative treatment of unilateral condylar process fractures:clinical and radiographic evaluation of 80 patients. J OralMaxillofac Surg 1992;50:349–352; discussion 352–343
102. Lachner J, Clanton JT, Waite PD. Open reduction andinternal rigid fixation of subcondylar fractures via anintraoral approach. Oral Surg Oral Med Oral Pathol 1991;71:257–261
90 FACIAL PLASTICS SURGERY/VOLUME 24, NUMBER 1 2008

103. Palmieri C, Ellis E III, Throckmorton G. Mandibularmotion after closed and open treatment of unilateralmandibular condylar process fractures. J Oral MaxillofacSurg 1999;57:764–775; discussion 775–766
104. Raveh J, Vuillemin T, Ladrach K. Open reduction of thedislocated, fractured condylar process: indications and surgicalprocedures. J Oral Maxillofac Surg 1989;47:120–127
105. Throckmorton GS, Ellis E III. Recovery of mandibularmotion after closed and open treatment of unilateralmandibular condylar process fractures. Int J Oral MaxillofacSurg 2000;29:421–427
106. Worsaae N, Thorn JJ. Surgical versus nonsurgical treatmentof unilateral dislocated low subcondylar fractures: a clinicalstudy of 52 cases. J Oral Maxillofac Surg 1994;52:353–360;discussion 360–351
107. Worsaae N, Thorn JJ. [Surgical versus non-surgicaltreatment of unilateral dislocated fractures of the lowermandibular condyle]. Ugeskr Laeger 1995;157:3472–3476
108. Honda T, Sasaki K, Takeuchi M, Nozaki M. Endoscope-assisted intraoral approach for masseteric hypertrophy. AnnPlast Surg 1997;38:9–14
109. Jacobovicz J, Lee C, Trabulsy PP. Endoscopic repair ofmandibular subcondylar fractures. Plast Reconstr Surg1998;101:437–441
110. Chen CT, Lai JP, Tung TC, Chen YR. Endoscopicallyassisted mandibular subcondylar fracture repair. PlastReconstr Surg 1999;103:60–65
111. Honda T, Nozaki M, Isono N, Sasaki K. Endoscope-assisted facial fracture repair. World J Surg 2001;25:1075–1083
112. Sandler NA. Endoscopic-assisted reduction and fixation of amandibular subcondylar fracture: report of a case. J OralMaxillofac Surg 2001;59:1479–1482
113. Miloro M. Endoscopic-assisted repair of subcondylarfractures. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:387–391
114. Schon R, Schramm A, Gellrich NC, Schmelzeisen R.Follow-up of condylar fractures of the mandible in 8patients at 18 months after transoral endoscopic-assistedopen treatment. J Oral Maxillofac Surg 2003;61:49–54
115. Troulis MJ. Endoscopic open reduction and internal rigidfixation of subcondylar fractures. J Oral Maxillofac Surg2004;62:1269–1271
116. Vural E. Treatment of adult subcondylar mandibularfractures: closed vs open vs endoscopic approach. ArchOtolaryngol Head Neck Surg 2004;130:1228–1230
117. Mueller RV, Czerwinski M, Lee C, Kellman RM. Condylarfracture repair: use of the endoscope to advance traditionaltreatment philosophy. Facial Plast Surg Clin North Am2006;14:1–9
118. Troulis MJ, Nahlieli O, Castano F, Kaban LB. Minimallyinvasive orthognathic surgery: endoscopic verticalramus osteotomy. Int J Oral Maxillofac Surg 2000;29:239–242
119. Suarez-Cunqueiro MM, Schon R, Gellrich NC, Schmel-zeisen R. Endoscopic assistance in the removal of a foreignbody in the condylar process. J Craniofac Surg 2004;15:98–101
120. Mueller RV. Endoscopic removal of a bullet from thetemporomandibular joint. Portland; 1998
121. Lauer G, Schmelzeisen R. Endoscope-assisted fixation ofmandibular condylar process fractures. J Oral MaxillofacSurg 1999;57:36–39; discussion 39–40
122. Lee C, Stiebel M, Young DM. Cranial nerve VII region ofthe traumatized facial skeleton: optimizing fracture repairwith the endoscope. J Trauma 2000;48:423–431; discussion431–422
ENDOSCOPIC TREATMENT OF FACIAL FRACTURES/MUELLER 91












![Cronicon · fractures [2]. Being the most prominent mobile bone of the facial skeleton, Mandibular fractures are among the most common injuries to the facial skeleton, with a 6:2](https://static.fdocuments.net/doc/165x107/5f2b985f1c26767db7383601/cronicon-fractures-2-being-the-most-prominent-mobile-bone-of-the-facial-skeleton.jpg)



