Endoscopic Transcanal Corridors to the Lateral Skull … · · 2016-02-03Endoscopic Transcanal...
13
The Laryngoscope V C 2015 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS Endoscopic Transcanal Corridors to the Lateral Skull Base: Initial Experiences Daniele Marchioni, MD; Matteo Alicandri-Ciufelli, MD, FEBORL(HNS); Alessia Rubini, MD; Livio Presutti, MD Objectives/Hypothesis: Surgical approaches to the lateral skull base, internal auditory canal (IAC), and petrous bone are widely known and have been extensively recorded. Despite the benign nature and limited dimensions of lesions located in this anatomical region, extirpative surgical approaches are often required to reach and remove the disease. The aim of present report was to describe our initial experiences with minimally invasive endoscopic approaches to the lateral skull base. Study Design: Retrospective review of patients’ charts and video recordings from surgery. Methods: Twelve patients were included in the study. Three main corridors to the lateral skull base were identified: the transcanal suprageniculate corridor, the transcanal transpromontorial corridor, and the transcanal infracochlear corridor. Landmarks, tips, and pitfalls of the approaches have been reviewed and highlighted. Results: These corridors provide a direct approach to pathology involving the fundus, IAC, cochlea, petrous apex and geniculate ganglion region, without any external incision. The pathology was successfully removed in most cases with no important postoperative complications and reasonable facial nerve outcomes. Conclusions: The transcanal endoscopic approaches to the lateral skull base proved to be successful for pathology removal involving the fundus, IAC, cochlea, petrous apex, and geniculate ganglion region. Future widespread application of this kind of approach in lateral skull base surgery will depend on the development of technology, and surgical and anatomical refinements. Key Words: Inner ear, internal auditory canal, transcanal approach, endoscopic ear surgery, acoustic schwannoma, lateral skull base, temporal bone cholesteatoma, transcanal corridors. Level of Evidence: 4. Laryngoscope, 125:S1–S13, 2015 INTRODUCTION The lateral skull base constitutes an anatomic boundary between the fields of neurosurgery and otolar- yngology. Surgery in this region has always been a chal- lenge for both disciplines owing to the presence of important anatomical structures such as the internal carotid artery, the otic capsule, and the facial nerve. Sev- eral approaches have been developed to reach pathology located in the lateral skull base and in the fundus of the internal auditory canal (IAC) and petrous apex. Despite the benign nature and limited dimensions of the lesions located in this anatomical region, extensive surgical approaches are often required to reach and remove the disease. The transpetrous routes (translabyrinthine, transotic, transcochlear approaches), the retrosigmoid route and the middle cranial fossa approach are the routes most widely used to reach lateral skull base lesions. All of these approaches are open and based on the use of a microscope, and often involve significant amounts of brain retraction and neurovascular manipulation. A gradual introduction of endoscopic techniques for the treatment of middle ear pathology has taken place since the 1990s. 1 Endoscopy was used primarily for visu- alization of hidden areas such as the posterior epitympa- num during classic microscopic tympanoplasties. 2 Gradually, it was also used in surgery to replace the microscope as the main tool used during middle ear operations. 3–6 At present, the main application of endo- scopic surgery is in the surgical treatment of middle ear cholesteatoma, but with the natural evolution of the technique, there have been advances in lateral skull base surgery. From our experience over recent years, the authors have progressively noticed that the inner ear and all of the temporal bone could also be accessed in an endoscopic-assisted fashion or even with an exclusive endoscopic approach. So, based on our earlier experien- ces with transcanal endoscopic approaches to the middle ear, we started to consider the transcanal approach as a surgical corridor to reach diseases with limited extent located in the lateral skull base. 7–9 These minimally From the Otolaryngology Department (M.A.–C., A.R., L.P .), Univer- sity Hospital of Modena, Modena, Italy; the Neurosurgery Department (M.A.–C.), New Civil Hospital Sant’Agostino-Estense, Baggiovara, Italy; Otolaryngology Department (D.M.), University Hospital of Verona, Verona, Italy. Editor’s Note: This Manuscript was accepted for publication January 20, 2015. The authors have no funding, financial relationships, or conflicts of interest to disclose. Send correspondence to Alessia Rubini, MD, Otolaryngology Department, University Hospital of Modena, Via del Pozzo 71, 41100 Modena, Italy. E-mail: [email protected] DOI: 10.1002/lary.25203 Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base S1
Transcript of Endoscopic Transcanal Corridors to the Lateral Skull … · · 2016-02-03Endoscopic Transcanal...

The LaryngoscopeVC 2015 The American Laryngological,Rhinological and Otological Society, Inc.
TRIOLOGICAL SOCIETYCANDIDATE THESIS
Endoscopic Transcanal Corridors to the Lateral Skull Base:
Initial Experiences
Daniele Marchioni, MD; Matteo Alicandri-Ciufelli, MD, FEBORL(HNS);
Alessia Rubini, MD; Livio Presutti, MD
Objectives/Hypothesis: Surgical approaches to the lateral skull base, internal auditory canal (IAC), and petrous boneare widely known and have been extensively recorded. Despite the benign nature and limited dimensions of lesions locatedin this anatomical region, extirpative surgical approaches are often required to reach and remove the disease. The aim ofpresent report was to describe our initial experiences with minimally invasive endoscopic approaches to the lateral skullbase.
Study Design: Retrospective review of patients’ charts and video recordings from surgery.Methods: Twelve patients were included in the study. Three main corridors to the lateral skull base were identified: the
transcanal suprageniculate corridor, the transcanal transpromontorial corridor, and the transcanal infracochlear corridor.Landmarks, tips, and pitfalls of the approaches have been reviewed and highlighted.
Results: These corridors provide a direct approach to pathology involving the fundus, IAC, cochlea, petrous apex andgeniculate ganglion region, without any external incision. The pathology was successfully removed in most cases with noimportant postoperative complications and reasonable facial nerve outcomes.
Conclusions: The transcanal endoscopic approaches to the lateral skull base proved to be successful for pathologyremoval involving the fundus, IAC, cochlea, petrous apex, and geniculate ganglion region. Future widespread application ofthis kind of approach in lateral skull base surgery will depend on the development of technology, and surgical and anatomicalrefinements.
Key Words: Inner ear, internal auditory canal, transcanal approach, endoscopic ear surgery, acoustic schwannoma,lateral skull base, temporal bone cholesteatoma, transcanal corridors.
Level of Evidence: 4.Laryngoscope, 125:S1–S13, 2015
INTRODUCTIONThe lateral skull base constitutes an anatomic
boundary between the fields of neurosurgery and otolar-yngology. Surgery in this region has always been a chal-lenge for both disciplines owing to the presence ofimportant anatomical structures such as the internalcarotid artery, the otic capsule, and the facial nerve. Sev-eral approaches have been developed to reach pathologylocated in the lateral skull base and in the fundus of theinternal auditory canal (IAC) and petrous apex. Despitethe benign nature and limited dimensions of the lesionslocated in this anatomical region, extensive surgicalapproaches are often required to reach and remove thedisease. The transpetrous routes (translabyrinthine,
transotic, transcochlear approaches), the retrosigmoidroute and the middle cranial fossa approach are theroutes most widely used to reach lateral skull baselesions. All of these approaches are open and basedon the use of a microscope, and often involve significantamounts of brain retraction and neurovascularmanipulation.
A gradual introduction of endoscopic techniques forthe treatment of middle ear pathology has taken placesince the 1990s.1 Endoscopy was used primarily for visu-alization of hidden areas such as the posterior epitympa-num during classic microscopic tympanoplasties.2
Gradually, it was also used in surgery to replace themicroscope as the main tool used during middle earoperations.3–6 At present, the main application of endo-scopic surgery is in the surgical treatment of middle earcholesteatoma, but with the natural evolution of thetechnique, there have been advances in lateral skullbase surgery. From our experience over recent years, theauthors have progressively noticed that the inner earand all of the temporal bone could also be accessed in anendoscopic-assisted fashion or even with an exclusiveendoscopic approach. So, based on our earlier experien-ces with transcanal endoscopic approaches to the middleear, we started to consider the transcanal approach as asurgical corridor to reach diseases with limited extentlocated in the lateral skull base.7–9 These minimally
From the Otolaryngology Department (M.A.–C., A.R., L.P.), Univer-sity Hospital of Modena, Modena, Italy; the Neurosurgery Department(M.A.–C.), New Civil Hospital Sant’Agostino-Estense, Baggiovara, Italy;Otolaryngology Department (D.M.), University Hospital of Verona,Verona, Italy.
Editor’s Note: This Manuscript was accepted for publicationJanuary 20, 2015.
The authors have no funding, financial relationships, or conflictsof interest to disclose.
Send correspondence to Alessia Rubini, MD, OtolaryngologyDepartment, University Hospital of Modena, Via del Pozzo 71, 41100Modena, Italy. E-mail: [email protected]
DOI: 10.1002/lary.25203
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S1
invasive approaches access the lateral skull base usingthe natural openings of the external auditory canal(EAC), and allow very good visualization of some ana-tomical areas lying in the petrous bone, petrous apex,and IAC. Diseases could be removed from these areaswithout brain or meningeal manipulations and withshort and safe postoperative courses.
The aim of this article was to describe our initialexperiences with transcanal endoscopic corridors to thelateral skull base, describing assumptions, indications,and procedures, and reporting our preliminary results.
MATERIALS AND METHODSBetween March 2012 and May 2014, 74 patients affected
by inner ear and lateral skull base diseases underwent surgeryat the otolaryngology department of the University Hospital ofModena. The following patients were included in the presentstudy: those affected by lateral skull base diseases with limitedextension into the suprageniculate fossa, cochlea, vestibule, fun-dus of the IAC and petrous apex, requiring surgery, and thosewho underwent transcanal endoscopic procedures.
Patients with diseases of the lateral skull base who under-went a transmastoid microscopic procedure (with or withoutendoscopic assistance) were not included in the study. The
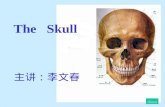
Fig. 1. The transcanal endoscopic suprageniculate approach. On the left, the schematic drawing shows the surgical route from the externalauditory canal to the suprageniculate fossa (blue arrow). On the right, the computed tomography scan in the coronal view shows the work-ing area and the bony removal (yellow area) between the middle cranial fossa and the facial nerve into the petrous apex over the cochlea,which may be performed with this approach. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.]
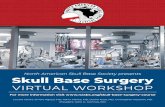
Fig. 2. Left ear. The transcanal endoscopic suprageniculate approach: on the left, schematic drawing showing a general view of the transcanalanatomy of the medial wall of the tympanic cavity related to the working area of the transcanal suprageniculate approach (orange area). Onthe right, the details of the endoscopic transcanal anatomical landmarks in this approach; the orange area indicates the bony area betweenthe middle cranial fossa superiorly, the facial nerve and geniculate ganglion inferiorly and the labyrinthine block posteriorly which may beremoved to reach the petrous apex endoscopically. aes 5 anterior epitympanic space; ca 5 carotid artery; cp 5 cochleariform process;et 5 Eustachian tube; fn 5 facial nerve; fn* 5 labyrinthine afacial nerve; gg 5 geniculate ganglion; gpt 5 greater petrosal nerve; lsc 5 lateralsemicircular canal; mcf 5 middle cranial fossa; pe 5 pyramidal eminence; pes 5 posterior epitympanic space; pr 5 promontory; rw 5 roundwindow; s 5 stapes; ttc 5 tensor tendon canal. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S2
surgery was performed by two experienced surgeons (D.M.,L.P.) with similar surgical and endoscopic experience. All oper-ations were video recorded and stored in the clinic’s digitaldatabase. Between May 2014 and June 2014, operations andpatients’ charts were reviewed, and all data were summarized
and gathered in a database for further consideration andanalyses.
All surgical procedures was performed under endoscopicview. Endoscopes were 3 or 4 mm in diameter, 18 cm in length,and 0� or 45� angled. The surgeon held the endoscope with theleft hand and the surgical instrument with the right hand; theendoscope was introduced into the EAC, reaching the tympaniccavity after tympanomeatal flap elevation. A three-chip cameraand high-definition monitor (Karl Storz, Tuttlingen, Germany)were used for all of the procedures, and videos were recordedon a computer hard disc. In all procedures, intraoperative facialnerve monitoring (Nerve Integrity Monitoring) was used.
Each approach was categorized and analyzed includingthe ear affected, the area of lateral skull base exposed, and theextent of endoscopic resection based on immediate postoperativecomputed tomography (CT) scans, compared with the preopera-tive CT scan. The following were also considered for eachpatient: intraoperative complications, postoperative complica-tions and facial nerve outcome, when preservation of hearingfunction was attempted, comparison of the postoperative audio-metric exam with the preoperative exam, and the time of recov-ery and discharge of the patients.
Based on the extent and location of the disease in thelateral skull base, three different approaches/corridors wereused and are discussed next.
Transcanal Suprageniculate CorridorThe transcanal suprageniculate corridor is illustrated in
Figure 1. When approached through the EAC, the disease wasreached located between the geniculate ganglion and the second
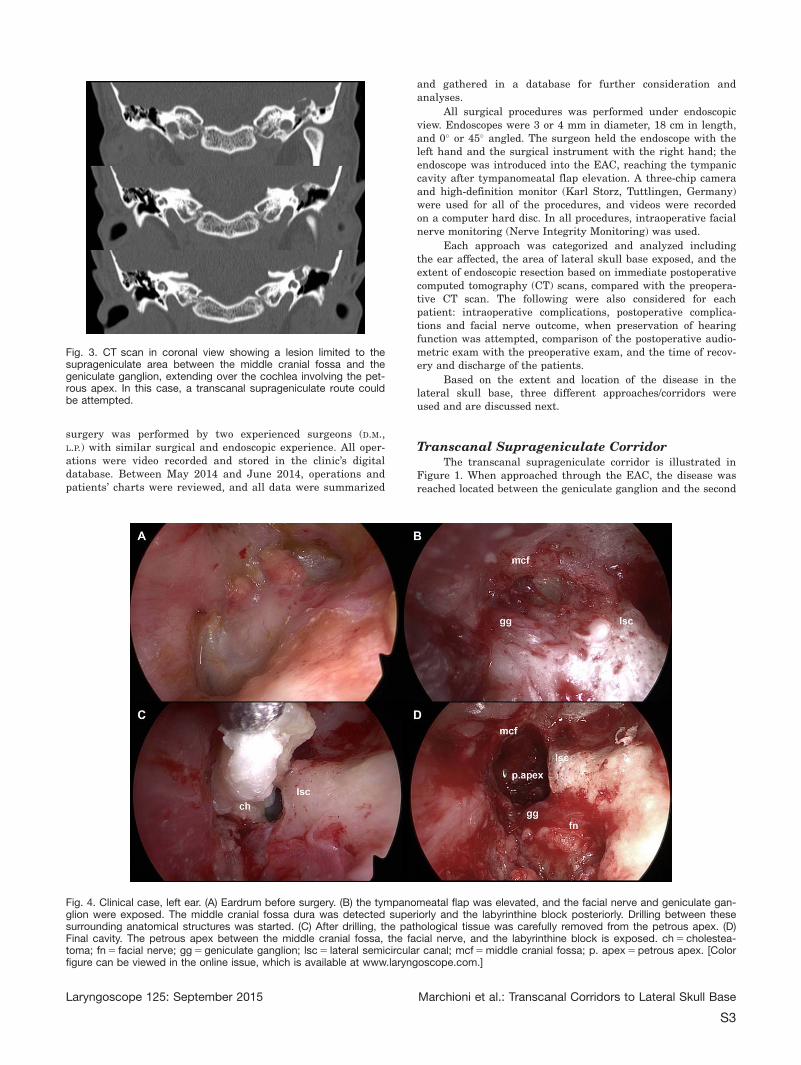
Fig. 3. CT scan in coronal view showing a lesion limited to thesuprageniculate area between the middle cranial fossa and thegeniculate ganglion, extending over the cochlea involving the pet-rous apex. In this case, a transcanal suprageniculate route couldbe attempted.
Fig. 4. Clinical case, left ear. (A) Eardrum before surgery. (B) the tympanomeatal flap was elevated, and the facial nerve and geniculate gan-glion were exposed. The middle cranial fossa dura was detected superiorly and the labyrinthine block posteriorly. Drilling between thesesurrounding anatomical structures was started. (C) After drilling, the pathological tissue was carefully removed from the petrous apex. (D)Final cavity. The petrous apex between the middle cranial fossa, the facial nerve, and the labyrinthine block is exposed. ch 5 cholestea-toma; fn 5 facial nerve; gg 5 geniculate ganglion; lsc 5 lateral semicircular canal; mcf 5 middle cranial fossa; p. apex 5 petrous apex. [Colorfigure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S3
portion of the facial nerve inferiorly, the middle cranial fossa(MCF) lying superiorly, and the labyrinthine bloc posteriorly.Working above the cochlea and labyrinth, sensorineural hearingfunction was preserved (Fig. 2), although an ossiculoplasty wasrequired after disease removal.
The correct indication for this approach required diseasewith limited extension into an anatomical triangle composed ofthe MCF, facial nerve, and labyrinthine bloc as shown in Fig-ures 2 and 3. This area can be reached endoscopically by atranscanal route avoiding an MCF approach. The surgical stepsrequired the creation of a wide tympanomeatal flap to exposethe tympanic cavity; the flap was then transposed inferiorlyand detached from the handle of the malleus to obtain goodexposure of the medial wall of the tympanic cavity. When the
ossicular chain was present and intact, removal of the incusand head of the malleus was required to expose the entire sec-ond portion of the facial nerve, from the second genu to thegeniculate ganglion and the greater petrosal nerve area. Thecog and the cochleariform process were identified endoscopicallyand used as an anatomical landmark for the geniculate gan-glion area owing to the close anatomical relationship betweenthe geniculate ganglion and these structures.4 The dura of theMCF was exposed by removing bone from the tegmen of theanterior epitympanum, and represented the upper surgicallimit. The lateral semicircular canal was also detected endo-scopically, posteriorly and superiorly, with respect to the secondgenu of the facial nerve, representing the posterior limit of thesurgical dissection (see Fig. 4 B). The cog was gently removed
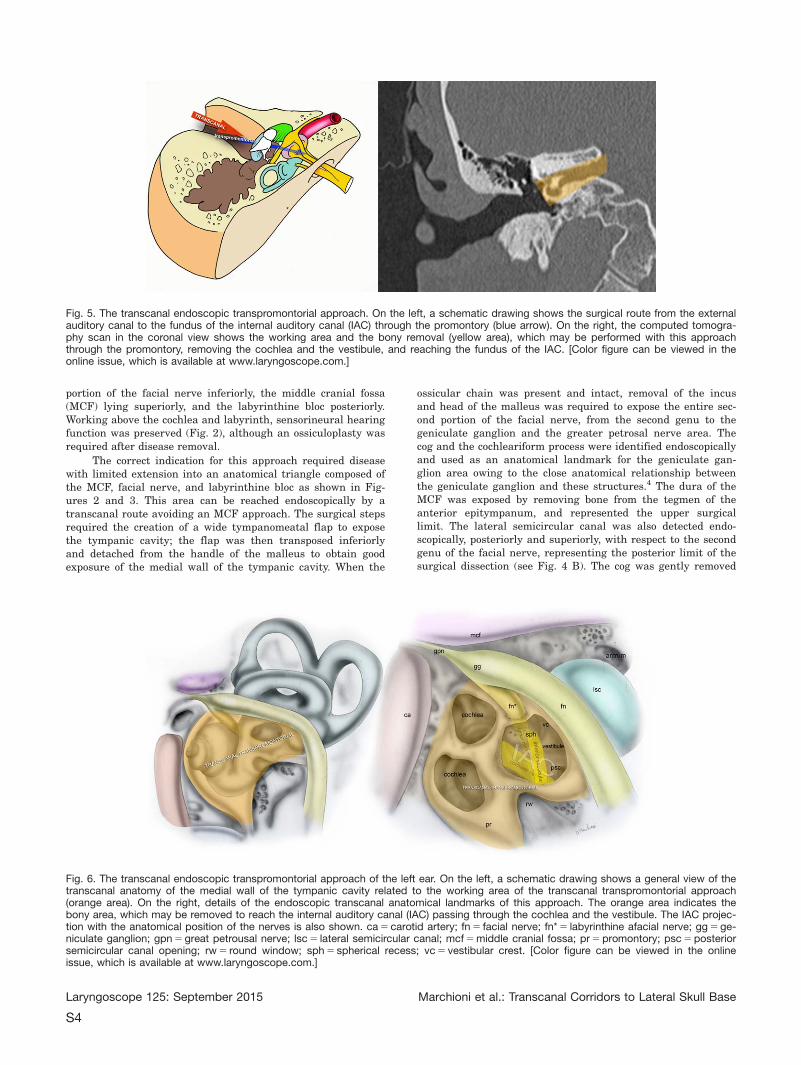
Fig. 5. The transcanal endoscopic transpromontorial approach. On the left, a schematic drawing shows the surgical route from the externalauditory canal to the fundus of the internal auditory canal (IAC) through the promontory (blue arrow). On the right, the computed tomogra-phy scan in the coronal view shows the working area and the bony removal (yellow area), which may be performed with this approachthrough the promontory, removing the cochlea and the vestibule, and reaching the fundus of the IAC. [Color figure can be viewed in theonline issue, which is available at www.laryngoscope.com.]
Fig. 6. The transcanal endoscopic transpromontorial approach of the left ear. On the left, a schematic drawing shows a general view of thetranscanal anatomy of the medial wall of the tympanic cavity related to the working area of the transcanal transpromontorial approach(orange area). On the right, details of the endoscopic transcanal anatomical landmarks of this approach. The orange area indicates thebony area, which may be removed to reach the internal auditory canal (IAC) passing through the cochlea and the vestibule. The IAC projec-tion with the anatomical position of the nerves is also shown. ca 5 carotid artery; fn 5 facial nerve; fn* 5 labyrinthine afacial nerve; gg 5 ge-niculate ganglion; gpn 5 great petrousal nerve; lsc 5 lateral semicircular canal; mcf 5 middle cranial fossa; pr 5 promontory; psc 5 posteriorsemicircular canal opening; rw 5 round window; sph 5 spherical recess; vc 5 vestibular crest. [Color figure can be viewed in the onlineissue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S4

using a microcurette, increasing the exposure of the geniculateganglion area, and when required, the greater petrosal nervewas also exposed just anteriorly to the geniculate ganglion.Based on the extent of the disease, a diamond burr or a Piezo-surgery device (Mectron, Carasco/Genova, Italy) was used toremove the bone between the MCF superiorly, the labyrinthinebloc posteriorly, and the facial nerve inferiorly, reaching thepathological tissue in this area (Fig. 4C,D). After diseaseremoval, a fragment of temporal muscle was used to obliteratethe cavity created, an ossicular chain reconstruction was per-formed at the same time as the surgery, and the tympanomeatalflap was replaced.
Transcanal Transpromontorial CorridorThe transcanal transpromontorial corridor is illustrated in
Figure 5. When approached through the EAC, the fundus of theIAC was reached by passing through the promontory, and dis-ease located in the vestibule, cochlea, and/or IAC was removed.With this surgical approach, hearing loss was expected owing tothe extirpation of the promontory area to form a passage
through the cochlea to reach the IAC (Fig. 6). The surgical stepswere as follows: a circumferential incision was made on theEAC, 2 cm from the tympanic membrane, and a wide tympano-meatal flap was created by skin degloving, and all of the ear-drum with the meatal skin flap of the EAC was removed. Adiamond burr was used to perform a wide meatoplasty, and thebony annulus was drilled circumferentially until the hypotym-panum, retrotympanum, and protympanum were exposed endo-scopically so as to obtain optimal surgical space and control ofthe whole medial wall of the tympanic cavity. The scutum wasremoved to uncover the incudomalleolar joint. The incus wasremoved, and the tensor tendon was cut removing the malleus(Fig. 7A). Using a hook, the stapes was removed to expose thevestibule. The spherical recess, representing the cribrose areawhere the inferior vestibular nerve was attached and a land-mark for the internal auditory canal,8 was detected endoscopi-cally in the saccular fossa (Figs. 6 and 7B). When the diseaseinvolved the vestibule without IAC extension, the oval windowopening was enlarged inferiorly on the promontory using amicrocurette, allowing direct access to the medial wall of thevestibule, and the disease from the depth of the vestibule was
Fig. 7. Transcanal endoscopic transpromontorial approach of the left ear. (A) The medial wall of the tympanic cavity after ossicular chainand eardrum removal. (B) The stapes was removed exposing the medial wall of the vestibule. (C) The promontory was drilled, detecting thebasal, medial, and apical turns of the cochlea. (D) The cochlea was opened just below the vestibule exposing the tumor in the internal audi-tory canal (IAC). (E) A careful dissection of the tumor from the facial nerve in the IAC was performed.(F) Final cavity after tumor removal.coh 5 cochlea; cp 5 cochleariform process; et 5 eustachian tube; fn 5 facial nerve; fn** 5 facial nerve in the IAC; lsc 5 lateral semicircularcanal; ve 5 vestibule; pr 5 promontory; rw 5 round window; s 5 stapes; tum 5 tumor. [Color figure can be viewed in the online issue, whichis available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S5
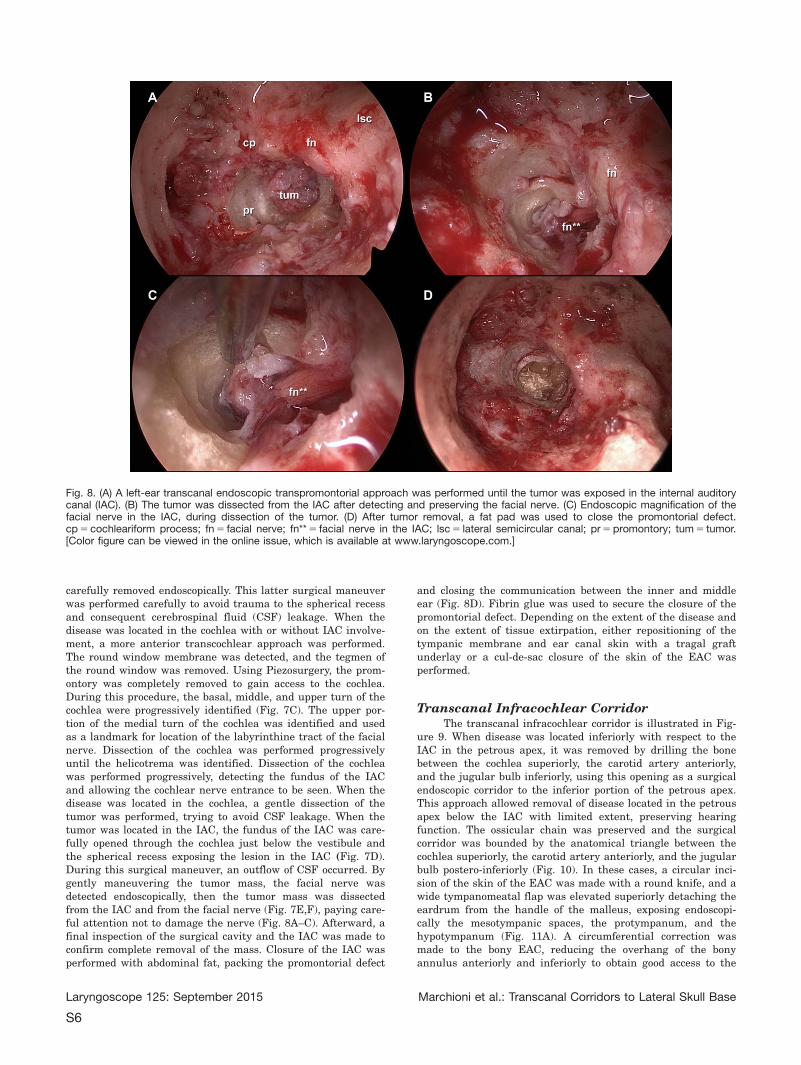
carefully removed endoscopically. This latter surgical maneuverwas performed carefully to avoid trauma to the spherical recessand consequent cerebrospinal fluid (CSF) leakage. When thedisease was located in the cochlea with or without IAC involve-ment, a more anterior transcochlear approach was performed.The round window membrane was detected, and the tegmen ofthe round window was removed. Using Piezosurgery, the prom-ontory was completely removed to gain access to the cochlea.During this procedure, the basal, middle, and upper turn of thecochlea were progressively identified (Fig. 7C). The upper por-tion of the medial turn of the cochlea was identified and usedas a landmark for location of the labyrinthine tract of the facialnerve. Dissection of the cochlea was performed progressivelyuntil the helicotrema was identified. Dissection of the cochleawas performed progressively, detecting the fundus of the IACand allowing the cochlear nerve entrance to be seen. When thedisease was located in the cochlea, a gentle dissection of thetumor was performed, trying to avoid CSF leakage. When thetumor was located in the IAC, the fundus of the IAC was care-fully opened through the cochlea just below the vestibule andthe spherical recess exposing the lesion in the IAC (Fig. 7D).During this surgical maneuver, an outflow of CSF occurred. Bygently maneuvering the tumor mass, the facial nerve wasdetected endoscopically, then the tumor mass was dissectedfrom the IAC and from the facial nerve (Fig. 7E,F), paying care-ful attention not to damage the nerve (Fig. 8A–C). Afterward, afinal inspection of the surgical cavity and the IAC was made toconfirm complete removal of the mass. Closure of the IAC wasperformed with abdominal fat, packing the promontorial defect
and closing the communication between the inner and middleear (Fig. 8D). Fibrin glue was used to secure the closure of thepromontorial defect. Depending on the extent of the disease andon the extent of tissue extirpation, either repositioning of thetympanic membrane and ear canal skin with a tragal graftunderlay or a cul-de-sac closure of the skin of the EAC wasperformed.
Transcanal Infracochlear CorridorThe transcanal infracochlear corridor is illustrated in Fig-
ure 9. When disease was located inferiorly with respect to theIAC in the petrous apex, it was removed by drilling the bonebetween the cochlea superiorly, the carotid artery anteriorly,and the jugular bulb inferiorly, using this opening as a surgicalendoscopic corridor to the inferior portion of the petrous apex.This approach allowed removal of disease located in the petrousapex below the IAC with limited extent, preserving hearingfunction. The ossicular chain was preserved and the surgicalcorridor was bounded by the anatomical triangle between thecochlea superiorly, the carotid artery anteriorly, and the jugularbulb postero-inferiorly (Fig. 10). In these cases, a circular inci-sion of the skin of the EAC was made with a round knife, and awide tympanomeatal flap was elevated superiorly detaching theeardrum from the handle of the malleus, exposing endoscopi-cally the mesotympanic spaces, the protympanum, and thehypotympanum (Fig. 11A). A circumferential correction wasmade to the bony EAC, reducing the overhang of the bonyannulus anteriorly and inferiorly to obtain good access to the
Fig. 8. (A) A left-ear transcanal endoscopic transpromontorial approach was performed until the tumor was exposed in the internal auditorycanal (IAC). (B) The tumor was dissected from the IAC after detecting and preserving the facial nerve. (C) Endoscopic magnification of thefacial nerve in the IAC, during dissection of the tumor. (D) After tumor removal, a fat pad was used to close the promontorial defect.cp 5 cochleariform process; fn 5 facial nerve; fn** 5 facial nerve in the IAC; lsc 5 lateral semicircular canal; pr 5 promontory; tum 5 tumor.[Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S6
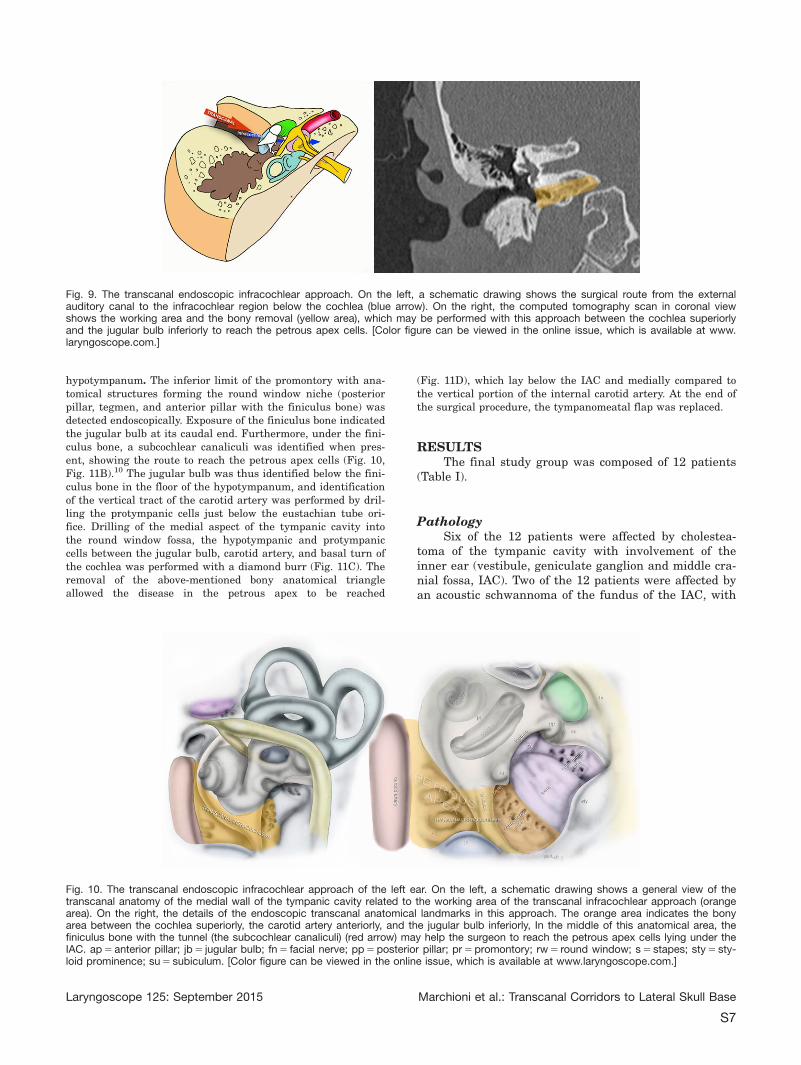
hypotympanum. The inferior limit of the promontory with ana-tomical structures forming the round window niche (posteriorpillar, tegmen, and anterior pillar with the finiculus bone) wasdetected endoscopically. Exposure of the finiculus bone indicatedthe jugular bulb at its caudal end. Furthermore, under the fini-culus bone, a subcochlear canaliculi was identified when pres-ent, showing the route to reach the petrous apex cells (Fig. 10,Fig. 11B).10 The jugular bulb was thus identified below the fini-culus bone in the floor of the hypotympanum, and identificationof the vertical tract of the carotid artery was performed by dril-ling the protympanic cells just below the eustachian tube ori-fice. Drilling of the medial aspect of the tympanic cavity intothe round window fossa, the hypotympanic and protympaniccells between the jugular bulb, carotid artery, and basal turn ofthe cochlea was performed with a diamond burr (Fig. 11C). Theremoval of the above-mentioned bony anatomical triangleallowed the disease in the petrous apex to be reached
(Fig. 11D), which lay below the IAC and medially compared tothe vertical portion of the internal carotid artery. At the end ofthe surgical procedure, the tympanomeatal flap was replaced.
RESULTSThe final study group was composed of 12 patients
(Table I).
PathologySix of the 12 patients were affected by cholestea-
toma of the tympanic cavity with involvement of theinner ear (vestibule, geniculate ganglion and middle cra-nial fossa, IAC). Two of the 12 patients were affected byan acoustic schwannoma of the fundus of the IAC, with
Fig. 9. The transcanal endoscopic infracochlear approach. On the left, a schematic drawing shows the surgical route from the externalauditory canal to the infracochlear region below the cochlea (blue arrow). On the right, the computed tomography scan in coronal viewshows the working area and the bony removal (yellow area), which may be performed with this approach between the cochlea superiorlyand the jugular bulb inferiorly to reach the petrous apex cells. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Fig. 10. The transcanal endoscopic infracochlear approach of the left ear. On the left, a schematic drawing shows a general view of thetranscanal anatomy of the medial wall of the tympanic cavity related to the working area of the transcanal infracochlear approach (orangearea). On the right, the details of the endoscopic transcanal anatomical landmarks in this approach. The orange area indicates the bonyarea between the cochlea superiorly, the carotid artery anteriorly, and the jugular bulb inferiorly, In the middle of this anatomical area, thefiniculus bone with the tunnel (the subcochlear canaliculi) (red arrow) may help the surgeon to reach the petrous apex cells lying under theIAC. ap 5 anterior pillar; jb 5 jugular bulb; fn 5 facial nerve; pp 5 posterior pillar; pr 5 promontory; rw 5 round window; s 5 stapes; sty 5 sty-loid prominence; su 5 subiculum. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S7
hearing loss on the same side, and with growth of theschwannoma detected by magnetic resonance imaging(MRI) during follow-up. One patient was affected by acochlear schwannoma involving the fundus of the IAC,with hearing loss on the same side and with growth ofthe schwannoma detected by MRI during follow-up. Onepatient was affected by a meningioma of the IAC erodingthe cochlea with only residual hearing on the same side.One patient was affected by an indefinite lesion in thepetrous apex (chondroma) with internal carotid arteryinvolvement requiring biopsy. One patient was affectedby a hemangioma of the facial nerve (geniculate gan-glion) involving the middle cranial fossa superiorly withintradural extension.
Surgical Procedures and IntraoperativeFindings
Out of 12 endoscopic transcanal lateral skull baseapproaches, three patients underwent an endoscopictranscanal suprageniculate approach, five patientsunderwent an endoscopic transcanal transpromontorialapproach, and four patients underwent an endoscopictranscanal infracochlear approach.
In 10/12 patients, the disease was completelyremoved from the lateral skull base. In one patient, aminimally invasive biopsy was performed via the trans-canal infracochlear route to reach disease located in theinferior aspect of the petrous apex, preserving the ossic-ular chain and hearing function. As a result of adhesionof the lesion to the inferior aspect of the IAC, CSF leak-age occurred that required repair with Lyodura. In one
patient, a meningioma of the IAC was found, partiallyextending into the cerebellopontine angle. The pathologywas not radically removed because of adhesions to thefacial nerve, and a subtotal removal was performed, pre-serving the facial nerve function.
In 2/6 patients affected by cholesteatoma, a poste-rior extension of the disease into the mastoid cells wasfound; therefore, a microscopic mastoidectomy wasadded after the endoscopic transcanal lateral skull basemanagement to remove disease from the mastoid cavity.
In 5/12 patients (four transpromontorial approachesand one infracochlear approach), CSF leakage occurredduring surgery because of opening of the fundus of theIAC. In all transpromontorial procedures, a fat padpushed into the promontorial defect was used to stop theleakage, closing the promontorial defect. In the infraco-chlear approach, it was repaired by pulling a muscle graftinto the defect. These grafts were secured with fibrin glue.
In all 12 surgical procedures, the facial nerve wasdetected endoscopically and preserved in 11/12 patients.In one patient, facial nerve sacrifice was necessary toremove the neoplasm (hemangioma of the facial nerve),and reconstruction of the facial nerve was attemptedduring the same surgical procedure using an auricularnerve cable graft.
No significant intraoperative complications wererecorded in the present case series.
Postoperative CourseA CT scan was performed in all cases several hours
after the surgery (Fig. 12). In the case of IAC
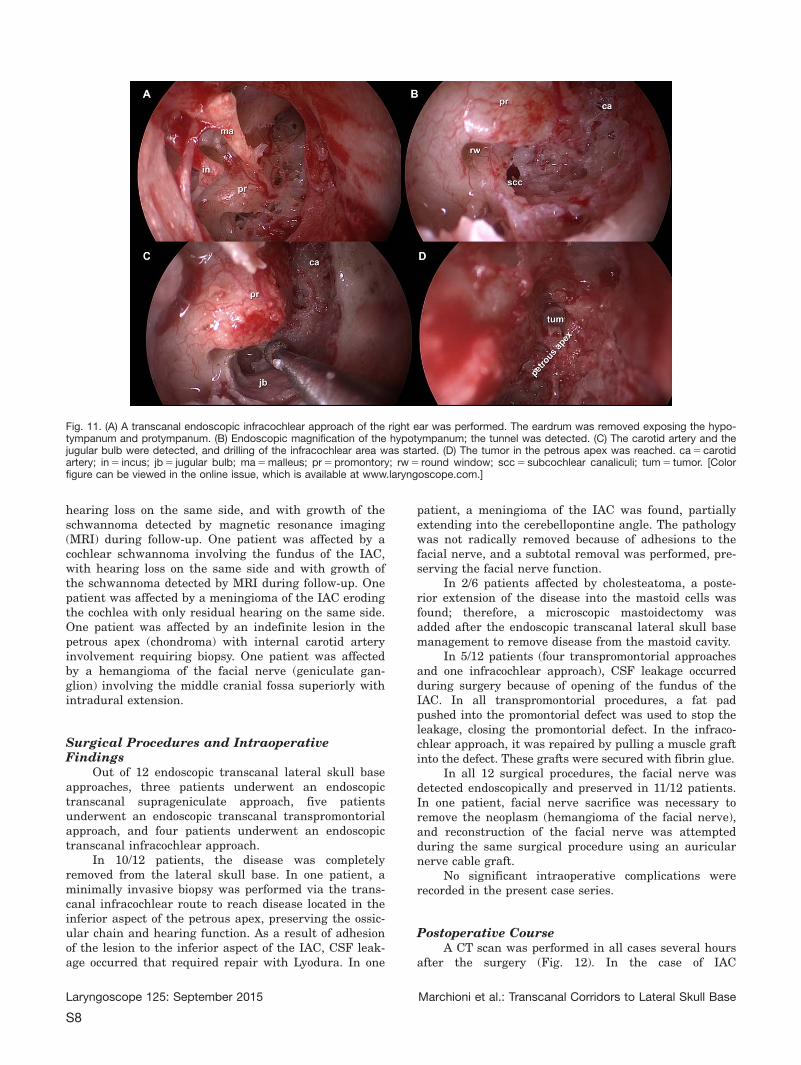
Fig. 11. (A) A transcanal endoscopic infracochlear approach of the right ear was performed. The eardrum was removed exposing the hypo-tympanum and protympanum. (B) Endoscopic magnification of the hypotympanum; the tunnel was detected. (C) The carotid artery and thejugular bulb were detected, and drilling of the infracochlear area was started. (D) The tumor in the petrous apex was reached. ca 5 carotidartery; in 5 incus; jb 5 jugular bulb; ma 5 malleus; pr 5 promontory; rw 5 round window; scc 5 subcochlear canaliculi; tum 5 tumor. [Colorfigure can be viewed in the online issue, which is available at www.laryngoscope.com.]
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S8

TAB
LE
I.C
hara
cte
ristics
of
the
Fin
alS
tud
yG
roup
.
Patient
Ag
e,
yr
Sex
Dis
ease
Surg
ical
Ro
ute
Pre
op
era
tive
Facia
lF
unctio
n(R
GS
)
Po
sto
pera
tive
Facia
lF
unctio
n(R
GS
)
Pre
op
era
tive
Hearing
Functio
n(P
TA)
Po
sto
pera
tive
Hearing
Functio
n(P
TA)
Co
mp
licatio
ns
Ho
sp
italiz
atio
n,
d
A.A
.77
MF
acia
lnerv
ehem
ang
iom
aS
up
rag
enic
ula
te2
6S
NB
C5
22.5
,A
C5
60
SN
BC
526.2
5,
AC
556.2
5N
one
7
B.G
.44
MA
co
ustic
neuro
ma
Transp
rom
onto
rial
11
Anacusi
sA
nacusi
sE
ard
rum
perf
ora
tio
n6
C.M
.58
MC
ho
nd
rom
aIn
fraco
chle
ar
(bio
psy)
11
NA
DX
BC
519.5
,A
C5
42.5
Eard
rum
perf
ora
tio
n6
M.E
.17
FC
ho
leste
ato
ma
Sup
rag
enic
ula
te(c
om
bin
ed
ap
pro
ach)
11
SN
BC
515,
AC
531.2
5S
NB
C5
10,
AC
546.2
5N
one
3
O.D
.25
FC
ho
leste
ato
ma
(recurr
ence)
Sup
rag
enic
ula
te3
1S
NB
C5
12.5
,A
C5
51.7
5S
NB
C5
12.5
,A
C5
46.2
5N
one
3
K.A
.40
MC
ochle
ar
schw
anno
ma
Transp
rom
onto
rial
11
Anacusi
sA
nacusi
sD
ela
yed
facia
lp
als
y,g
ranula
tio
ntissue
inth
eexte
rnal
aud
ito
rycanal
10
T.I.
62
FA
co
ustic
neuro
ma
Transp
rom
onto
rial
11
SN
BC
547.5
,A
C5
43
Anacusi
sTr
ansito
ryfa
cia
lp
als
y5
B.V
.27
FC
ho
leste
ato
ma
(recurr
ence)
Transp
rom
onto
rial
11
Anacusi
sA
nacusi
sN
one
1
S.O
.29
MC
ho
leste
ato
ma
Infr
aco
chle
ar
11
DX
BC
57,
AC
525
NA
No
ne
1
A.D
.M.
13
FC
ho
leste
ato
ma
Infr
aco
chle
ar
11
DX
BC
510,
AC
550
DX
BC
55,
AC
552.5
No
ne
3
D.G
.G.
45
MIA
Cm
enin
gio
ma
Transp
rom
onto
rial
11
Anacusi
sA
nacusi
sN
one
7
N.M
.D.
63
FC
ho
leste
ato
ma
Infr
aco
cle
ar
(co
mb
ined
ap
pro
ach)
11
SN
BC
526.2
5,
AC
556.7
5S
NB
C5
26.2
5,
AC
5N
AN
one
5
PTA
was
calc
ula
ted
as
ap
ure
-to
ne
air-c
ond
uctio
n(A
C)
and
bo
ne-c
ond
uctio
n(B
C)
thre
sho
ldavera
ge
at
500,
1,0
00,
2,0
00,
and
4,0
00
Hz.
F5
fem
ale
;G
G5
genic
ula
teg
ang
lion;
IAC
5in
tern
al
aud
ito
rycanal;
M5
male
;M
CF
5m
idd
lecra
nia
lfo
ssa;
NA
5no
tavaila
ble
;P
TA5
pure
-to
ne
avera
ge;
RG
S5
Ro
ug
hF
acia
lN
erv
eG
rad
ing
Syste
m;
SN
5le
ft;
DX
5rig
ht.
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S9

involvement, an MRI scan was also planned after 1 to 2months. In all cases, the postoperative pain was wellcontrolled using intravenous paracetamol. Antibiotictherapy (1 g of intravenous cefazoline twice a day) wasadministered for 48 hours after surgery.
Transcanal Suprageniculate ApproachIn the three patients who underwent an transcanal
suprageniculate approach, no postoperative complica-tions were observed. The postoperative CT scan showeda regular outcome for the transcanal suprageniculateapproach. All these patients were discharged withoutcomplications between the third and seventh postopera-tive day.
Transcanal Transpromontorial ApproachFour out of five patients who underwent a transca-
nal transpromontorial approach were kept in bed for 3days after surgery owing to CSF leakage during surgeryafter opening the IAC. Three of five patients in the samegroup reported postoperative horizontal nystagmus inassociation with vertiginous and neurovegetative symp-toms. The dizziness gradually improved during the hos-pital stay. All of these patients were discharged withoutcomplications: 2/5 patients were discharged on the ninthpostoperative day, and 2/5 patients were discharged onthe sixth postoperative day. One patient was dischargedon the first postoperative day, because the extent of dis-ease was limited to the vestibule without IACinvolvement.
Transcanal Infracochlear ApproachNo postoperative complications were observed in
any of the four patients who underwent the transcanalinfracochlear approach. One patient was discharged onthe sixth day after surgery, because CSF leakageoccurred during surgery, and the patient was kept inbed for 3 days after surgery. Three of four patients weredischarged on the third day after surgery.
Hearing ResultsOut of the five patients who underwent a transca-
nal transpromontorial corridor approach for removal oftheir pathology, five patients had postoperative anacusis.Preoperatively, 4/5 patients had profound hearing loss oranacusis.
Out of the four patients who underwent a transca-nal infracochlear corridor approach, two had normalhearing preoperatively, whereas two had middle ear con-ductive hearing loss. Of the two patients with preopera-tive normal hearing, one maintained a normal hearingfunction, whereas the other patient reported middle earconductive hearing loss postoperatively. Of the twopatients with preoperative hearing loss, one maintainedthe same bone- and air-conduction pure-tone audiometry(PTA) values postoperatively, whereas in the otherpatient, PTA air conduction was not available, and bonePTA was preserved.
Out of the three patients who underwent a transca-nal suprageniculate corridor approach, all of them hadconductive hearing loss preoperatively, and postopera-tively they maintained approximately the same hearingfunction from both bone and air PTA values.
Facial Function OutcomePreoperatively, 10/12 patients presented with grade
I of the Rough Facial Nerve Grading System (RGS).11
One patient affected by hemangioma of the geniculateganglion presented with RGS grade II, and one patientaffected by cholesteatoma involving the geniculate gan-glion with extension into the petrous apex presentedwith RGS grade III.
Analyzing facial nerve function after surgery, 11/12patients maintained their RGS grade I score during thepostoperative follow-up. Of these patients, one patientpresented a delayed facial palsy (RGS grade III) 2 daysafter surgery. After 6 days, recovery of facial functionwas observed (RGS grade I). One patient presentedwith RGS grade III facial palsy in the immediate post-operative period because of difficult dissection of thetumor from the nerve. In this case, a recovery of facialnerve function (RGS grade I) was also observed 1month after surgery. For the patient who presented pre-operatively with RGS grade III (cholesteatoma involv-ing the petrous apex), facial nerve paresis improved tograde II at discharge. During the follow-up period, thefacial nerve recovered completely to RGS grade I aftersome months.
One patient (hemangioma of the facial nerve) pre-sented a RGS grade VI after surgery. Dissection of thetumor had required sacrifice of the second portion of thefacial nerve, and a great auricular nerve graft was usedto reconstruct the continuity of the facial nerve.
Follow-upThe mean postoperative follow-up period was 12
months (range, 1–51 months). One patient required asurgical ambulatory procedure under local anesthesiafor the presence of granulation tissue in the externalauditory canal. Two patients presented a slight perfora-tion of the eardrum. During the follow-up period, norecurrence of disease was found.
DISCUSSIONIn recent years, there has been an increasing num-
ber of studies in the literature3,6 on the exclusive endo-scopic approach to the tympanic cavity. This approachrepresents a minimally invasive technique through theEAC, and is used when disease is located in the tym-panic cavity without mastoid involvement. The develop-ment of this approach, together with the development ofdedicated instruments,12 and technological advance-ments allow endoscopic tympanoplasty to be performed,removing the diseases and reconstructing the middle earwithout any external incision or mastoidectomy.3,13–15
Nevertheless, transcanal endoscopic approaches to mid-dle ear diseases, such as tympanic cavity cholesteatoma,
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S10

are not yet widely accepted as preferable to conventionalmicroscope-based canal wall down or canal wall upapproaches. Certainly, with the recent application of theendoscopic technique for cholesteatoma removal, out-come studies that directly compare the results withrespect to extent of disease, patients’ quality of life,recurrence, residual disease, morbidity, length of stay,and cost are lacking. And despite the surgical evolutionof the endoscopic technique in anterior skull base sur-gery and in the management of malignant tumors of theparanasal/anterior skull base, few ear surgeons are rou-tinely adopting the endoscope during surgery for ear dis-ease, because there is a lack of adequate training toreach the optimal skill levels with this tool. Advances inthe field of skull base surgery aim to maximize anatomi-cal exposure while minimizing patient morbidity.
Owing to complex anatomy, the petrous bone in thelateral skull base is wedged between the sphenoid andoccipital bones, containing or in close relationship to thefacial nerve, the IAC with the cochlea and vestibularlabyrinth, and the main vascular structures such as thejugular and internal carotid artery. To reach lesionslying at this anatomical boundary represents a challengefor surgical access, despite the limited dimensions andthe benign nature of the disease. To reach lesions lyingin the lateral skull, brain retraction, structural manipu-lation, and facial nerve palsy are often associated withopen procedures. This is also the case for removal ofbenign lesions with limited dimensions.
It is obvious that a detailed knowledge of the anat-omy of this area and the characteristics of the lesion areessential in choosing and executing the best surgicalroute. The anatomy of this area has been well describedin the literature from a transtemporal, transmastoidmicroscopic point of view, but studies on the endoscopicanatomy through the EAC are scarce. From our experi-ence with endoscopic approaches to the middle ear, wehave gradually come to the opinion that the medial wall
of the tympanic cavity could represent a surgicalcorridor to reach the lateral skull base and inner ear8,9
(vestibule, fundus of the IAC, suprageniculate area, pet-rous apex), in the same fashion as the nasal/sphenoidsurgical corridor is used for access to sellar disease andthe anterior skull base.
Several dissections were performed by our group togain the necessary anatomical knowledge and surgicalskills, studying the anatomy from the EAC to the IACfrom an endoscopic point of view, and using the EAC asa natural opening to access the lateral skull base.8
From these dissections and from our initial clinicalexperiences reported above, three main endoscopic cor-ridors have been identified in the lateral skull base: thetranscanal suprageniculate route, the transcanal trans-promontorial route, and the transcanal infracochlearroute. Some considerations on these surgical routes areoutlined next.
Regarding the infracochlear route, when performedwith a microscope, this is a route that has been wellknown for decades to gain access to pathologies locatedin the infracochlear region. It was mainly used in thepast for cholesterol granuloma drainage. As mentionedabove, by using an endoscope for visualization, it is pos-sible to extend the indications for petrous apex lesions,and for pathology extending inferiorly to the IAC. Cho-lesteatoma can also be treated with this approach. Threemain structures represent the limits and, at the sametime, the landmarks for this approach: the carotid arteryanteriorly, the internal jugular vein posteriorly, and thecochlea inferiorly. The subcochlear canaliculus, a smalltunnel that connects the round window chamber regionto the petrous apex, can be followed from a lateral to amedial direction, indicating the correct route.10
The suprageniculate route is considered when a dis-ease with limited dimensions is lying in the suprageni-culate fossa. Anatomically, we can consider thesuprageniculate fossa to be a triangular anatomical area
Fig. 12. Postoperative computedtomography scan in the coronalview (A, B) and axial view (C, D) ofa transcanal endoscopic transpro-montorial approach. Note the surgi-cal corridor extending from theexternal auditory canal to the inter-nal auditory canal.
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S11

between the tympanic portion of the facial nerve, thegeniculate ganglion and the greater petrosal nerve infe-riorly, the middle cranial fossa superiorly, and the laby-rinthine bloc posteriorly. In this preliminary experiencewith endoscopic visualization, the suprageniculate routeallowed us to reach this anatomical triangle directly, andthe bony tissue between these anatomical structureswas removed to reach the petrous apex cells lying supe-riorly to the geniculate ganglion, the labyrinthine facialnerve, and the IAC. The possibility to control the patho-logic tissues lying in the suprageniculate fossa throughthe EAC may help the surgeon to perform minimallyinvasive surgery, avoiding middle cranial fossa craniot-omy and brain tissue manipulation.
The transpromontorial route is considered when adisease with limited dimensions involves the cochlea,the vestibule, and the fundus of the IAC. Classically,benign pathologies such as cholesteatoma, acousticschwannomas, or cochlear schwannomas involving thefundus of the IAC or the cochlea have been treated withopen approaches with translabyrinthine or transotic sur-gery to reach the fundus of the IAC and cochlea. Thesetechniques provide wide exposure and manipulation ofthe dura of the middle cranial fossa, and can alsorequire facial nerve skeletonization. Anatomically, theremoval of the promontory area gives good access to thecochlea and vestibule. These anatomical structures arein close relationship with the fundus of the IAC. Asshown in earlier articles,8 the medial wall of the vesti-bule and the spherical recess represent crucial anatomi-cal landmarks used to detect the fundus of the IAC,because the end of the inferior vestibular nerve isattached in the spherical recess. On the other hand, thecranial portion of the apical and medial turn of the coch-lea are crucial landmarks for detection of the labyrin-thine facial nerve, which runs just above thesestructures. Anatomical knowledge of these structuresfrom an endoscopic point of view allowed us to reach thefundus of the IAC, removing diseases lying in this areaand avoiding the transpetrous open approaches. In par-ticular, in the future development of this approach, man-agement of acoustic schwannomas of the fundus couldbe modified, with the alternative to wait and carry outscans in patients with hearing loss and growing tumors.
Although these initial experiences are promising inthe authors’ opinion, some surgical risks should be con-sidered. During the transcanal transpromontorialapproach, possible risk of injury to the internal auditoryartery or of some anterior inferior cerebellar artery,loops must be considered, and a preoperative MRI evalu-ation of the vessels in the IAC is mandatory. Moreover,management of the facial nerve in the IAC could be diffi-cult, and careful surgical maneuvers are required toavoid damage to the nerve. A possible transitory facialnerve palsy should be considered with this approach,although total recovery was present in our case series.In fact, one patient presented transitory facial nervepalsy on the second postoperative day, and anotherpatient presented facial palsy grade III because of dis-section of the tumor, which was tightly adherent to thefacial nerve.
The present article is based on a limited number ofcases and represents the initial experiences using atranscanal endoscopic approach to lateral skull baselesions, describing the transcanal surgical corridors.Despite this, the techniques seem promising, and mayrepresent an advance in the lateral skull base surgeryfield. These approaches require long-term validation andfollow-up that may possibly indicate drawbacks or con-firm our results. Certainly, these endoscopic transcanalapproaches are only indicated at present in limitedcases, especially when a benign lesion is present withlimited extension into the inner ear and lateral skullbase lying beyond the tympanic cavity. When a lesion islying in the suprageniculate fossa, the petrous apex, thecochlea, vestibule, and IAC, a CT scan and MRI study ofthis lesion are mandatory to understand its anatomicalrelationship with the tympanic cavity, and to decidewhether a transcanal endoscopic route should beattempted through the EAC, avoiding open approaches.
Last but not least, these approaches require thedevelopment of adequate endoscopic skills, because sev-eral endoscopic ear dissections may be necessary tounderstand the transcanal anatomy from the EAC to theIAC. Neuro-otological skills are necessary because theendoscopic approach may be changed or combined withtraditional microscopic approaches, if required, duringthe surgical procedures.
CONCLUSIONThe transcanal endoscopic approach to the lateral
skull base has proven to be successful for removal ofpathology involving the fundus, IAC, cochlea, petrousapex, and geniculate ganglion region, with lower compli-cation rates and less invasive procedures compared totraditional microscopic approaches. Three main corridorsto the lateral skull base have been identified: the trans-canal suprageniculate corridor, the transcanal transpro-montorial corridor, and the transcanal infracochlearcorridor. Future applications of this kind of approach inlateral skull base surgery will depend on the develop-ment of technology, and surgical and anatomicalrefinements.
BIBLIOGRAPHY
1. Thomassin JM, Korchia D, Doris JM. Endoscopic guided otosurgery in theprevention of residual cholesteatomas. Laryngoscope 1993;103:939–943.
2. Presutti L, Marchioni D, Mattioli F, Villari D, Alicandri-Ciufelli M. Endo-scopic management of acquired cholesteatoma: our experience.J Otolaryngol Head Neck Surg 2008;37:481–487.
3. Marchioni D, Alicandri-Ciufelli M, Molteni G, Genovese E, Presutti L.Endoscopic tympanoplasty in patients with attic retraction pockets.Laryngoscope 2010;120:1847–1855.
4. Marchioni D, Alicandri-Ciufelli M, Piccinini A, et al. Surgical anatomy oftranscanal endoscopic approach to the tympanic facial nerve. Laryngo-scope 2011;121:1565–1573.
5. Marchioni D, Villari D, Alicandri-Ciufelli M, Piccinini A, Presutti L. Endo-scopic open technique in patients with middle ear cholesteatoma. EurArch Otorhinolaryngol 2011;268:1557–1563.
6. Tarabichi M. Endoscopic management of limited attic cholesteatoma.Laryngoscope 2004;114:1157–1162.
7. Presutti L, Nogueira JF, Alicandri-Ciufelli M, Marchioni D. Beyond themiddle ear: endoscopic surgical anatomy and approaches to inner earand lateral skull base. Otolaryngol Clin North Am 2013;46:189–200.
8. Marchioni D, Alicandri-Ciufelli M, Mattioli F, et al. From external to inter-nal auditory canal: surgical anatomy by an exclusive endoscopicapproach. Eur Arch Otorhinolaryngol 2013;270:1267–1275.
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S12

9. Presutti L, Alicandri-Ciufelli M, Rubini A, Gioacchini FM, Marchioni D.Combined lateral microscopic/endoscopic approaches to petrous apexlesions: pilot clinical experiences. Ann Otol Rhinol Laryngol 2014;123:550–559.
10. Marchioni D, Alicandri-Ciufelli M, Pothier DD, Rubini A, Presutti L. Theround window region and contiguous areas: endoscopic anatomy andsurgical implications [published online ahead of print February 9, 2014].Eur Arch Otorhinolaryngol. doi: 10.1007/s00405-014-2923-8.
11. Alicandri-Ciufelli M, Piccinini A, Grammatica A, et al. A step backward:the ‘Rough’ facial nerve grading system. J Craniomaxillofac Surg 2013;41:e175–e179.
12. Kakehata S, Watanabe T, Ito T, Kubota T, Furukawa T. Extension of indi-cations for transcanal endoscopic ear surgery using an ultrasonic bonecurette for cholesteatomas. Otol Neurotol 2014;35:101–107.
13. Tarabichi M, Nogueira JF, Marchioni D, Presutti L, Pothier DD, Ayache S.Transcanal endoscopic management of cholesteatoma. Otolaryngol ClinNorth Am 2013;46:107–130.
14. Migirov L, Shapira Y, Horowitz Z, Wolf M. Exclusive endoscopic ear sur-gery for acquired cholesteatoma: preliminary results. Otol Neurotol2011;32:433–436.
15. Ayache S, Tramier B, Strunski V. Otoendoscopy in cholesteatoma surgery of themiddle ear: what benefits can be expected? Otol Neurotol 2008;29:1085–1090.
Laryngoscope 125: September 2015 Marchioni et al.: Transcanal Corridors to Lateral Skull Base
S13