
Endometriosis Update (Clinic) Dr.Engin Oral Cerrahpaşa Medical Faculty Department of Obstet &...
78
Endometriosis Update (Clinic) Dr.Engin Oral Cerrahpaşa Medical Faculty Department of Obstet & Gynecology Div of Reproductive Endocrinology
-
Upload
noreen-smith -
Category
Documents
-
view
219 -
download
1
Transcript of Endometriosis Update (Clinic) Dr.Engin Oral Cerrahpaşa Medical Faculty Department of Obstet &...
Endometriosis Update(Clinic)
Dr.Engin OralCerrahpaşa Medical Faculty
Department of Obstet & GynecologyDiv of Reproductive Endocrinology

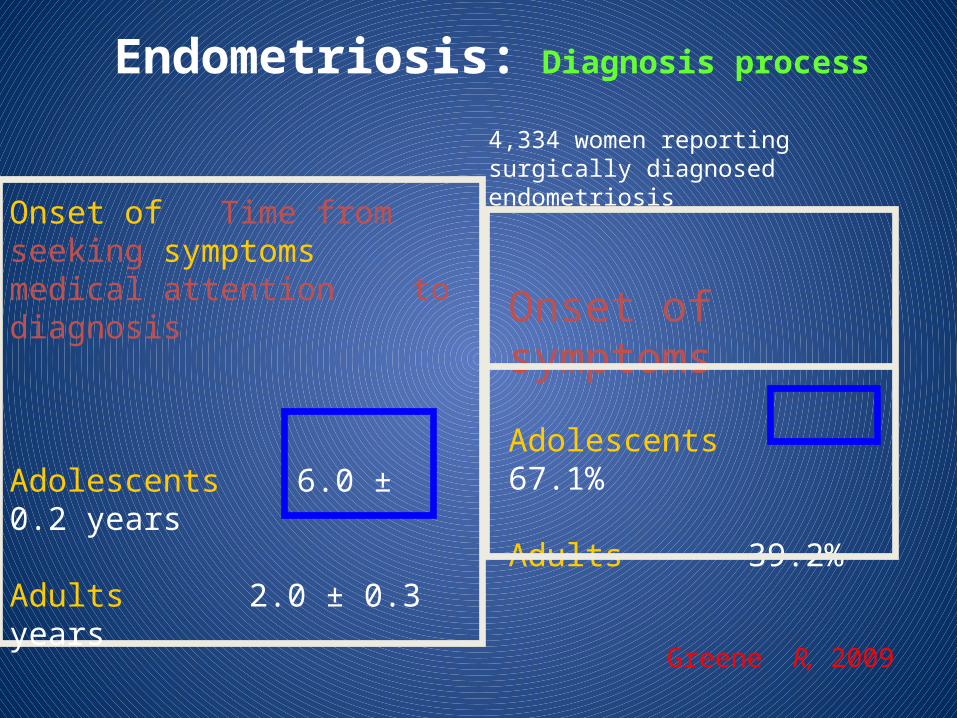
Endometriosis: Diagnosis process
Onset of symptoms
Adolescents 67.1%
Adults 39.2%
Greene R, 2009
Onset of Time from seeking symptoms medical attention to diagnosis
Adolescents 6.0 ± 0.2 years
Adults 2.0 ± 0.3 years
4,334 women reportingsurgically diagnosed endometriosis
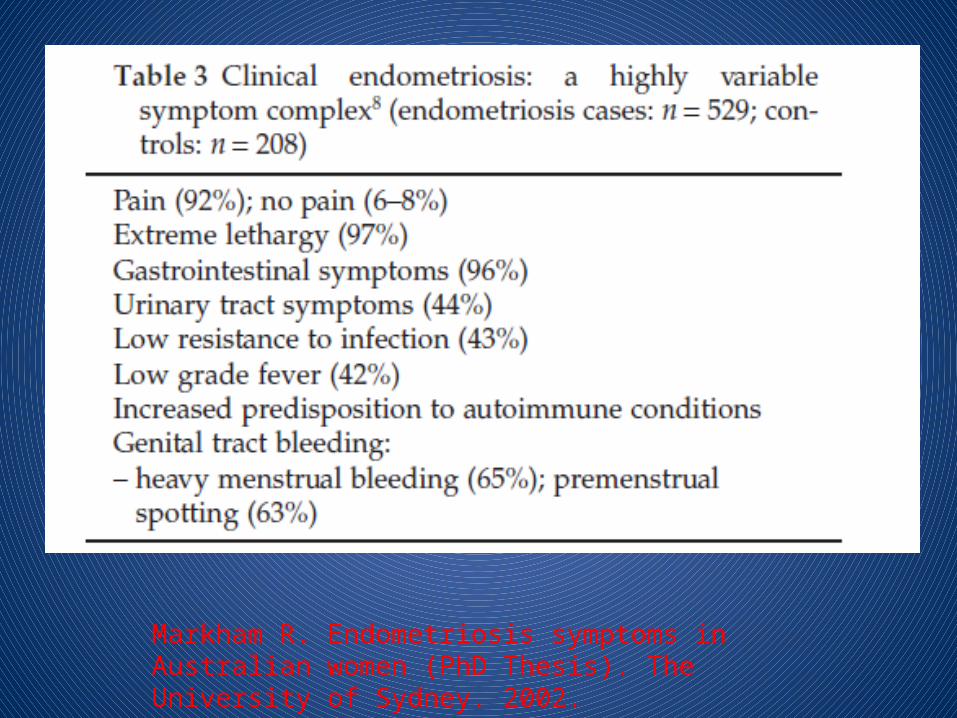
Markham R. Endometriosis symptoms in Australian women (PhD Thesis). The University of Sydney. 2002.
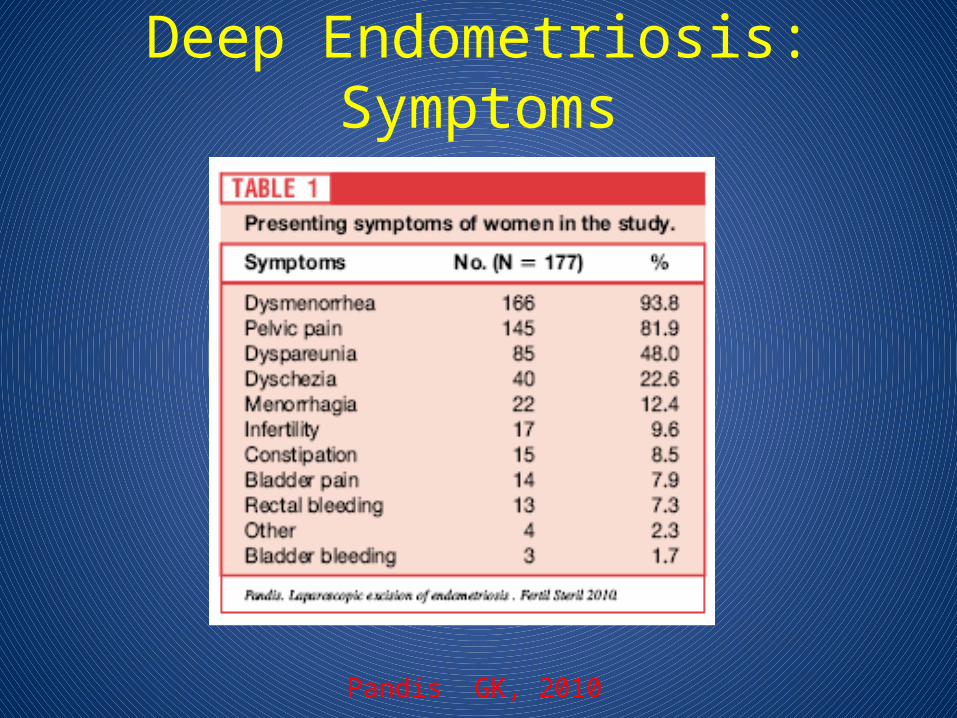
Deep Endometriosis: Symptoms
Pandis GK, 2010
Diagnosis of Endometriosis• History (The most important)• Symptoms• Physical Examination (not much help)• Serum Markers (Lacks sensitivity)• Ultrasound (of little value except endometrioma)• Magnetic Resonance Imaging (MRI) (a good guess!)• Other Imaging Modalities
– immunoscintigraphy and positron emission tomography• Transvaginal Hydrolaparoscopy• Laparoscopic Visualization of the Pelvis (The gold standard)
– Biopsy Preferable Over Visual Inspection• Novel Diagnostic Test
Rule out other Causes of Symptoms (The next most important)
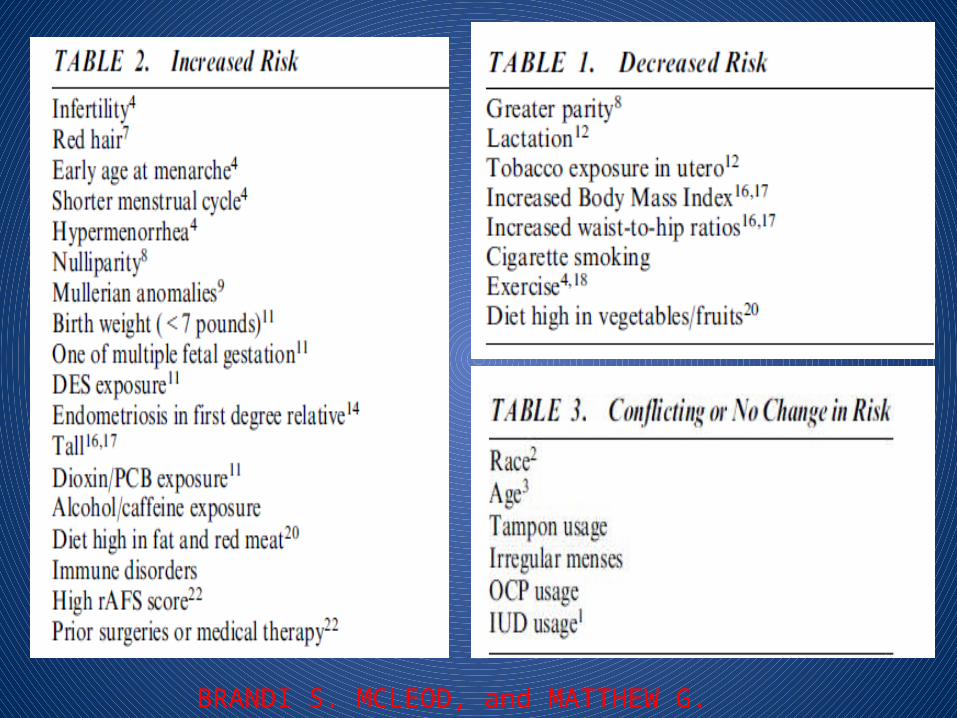
BRANDI S. MCLEOD, and MATTHEW G. RETZLOFF, 2010
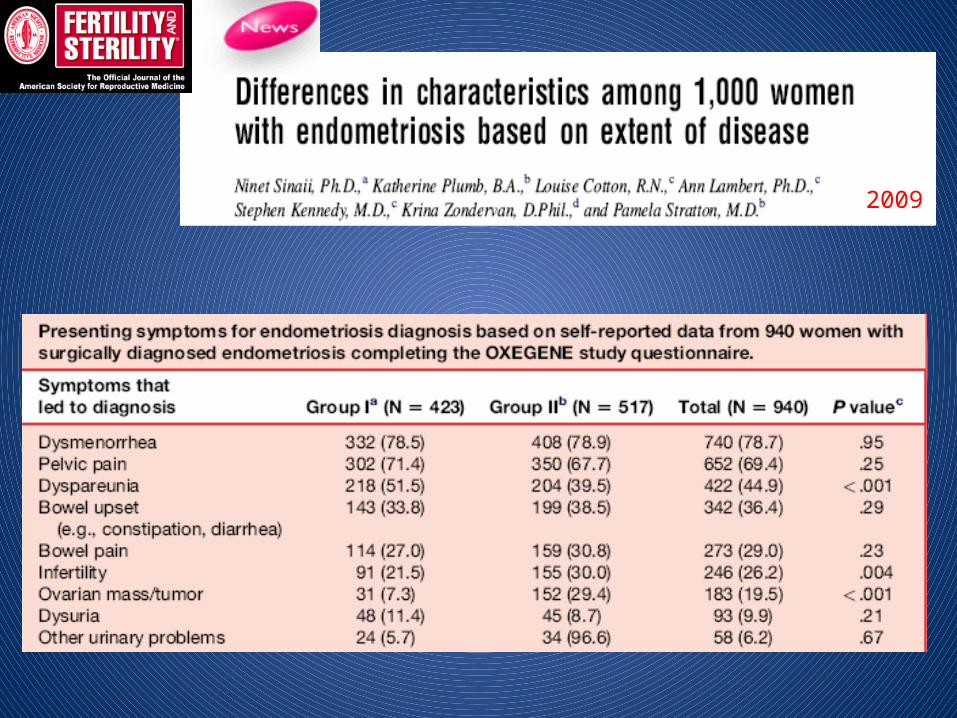
Sites of Endometriosis: Associated Signs & Symptoms
Female reproductive organs (for example: ovaries, uterus, vagina,
fallopian tubes, pelvic peritoneum)
·Dysmenorrhea (painful menstruation)
·Dyspareunia (pain during or after sexual intercourse)
·Infertility
·Pelvic pain
·Backache
·Menstruel irregularity
·Ruptured endometrioma
·Surgical scars umbilicus
·Cyclic pain and bleeding
Sites of Endometriosis: Associated Signs & Symptoms
Gastrointestinal system (for example: rectum, small intestine, colon)
·Nausea and vomiting
·Abdominal cramping
·Diarrhea
·Constipation
·Blood in stool
·Pain in the low back or tailbone
·Pain in the umbilicus
·Abdominal bloating and cramping
·Rectal bleeding
·Defecation problems
Sites of Endometriosis: Associated Signs & Symptoms
Urinary tract (for example: bladder, ureter, urethra, kidney)
·Pain or burning upon urination
·Urinary frequency, urgency, or retention
·Blood in the urine
·Flank pain
·Recurrent complaints of urinary tract infections with negative cultures
·Pulmonary (for example: lungs, pleura, diaphragm)
·Chest or shoulder pain
·Coughing up blood
·Shortness of breath
SERENA DOVEY, and JOSEPH SANFILIPPO, 2010
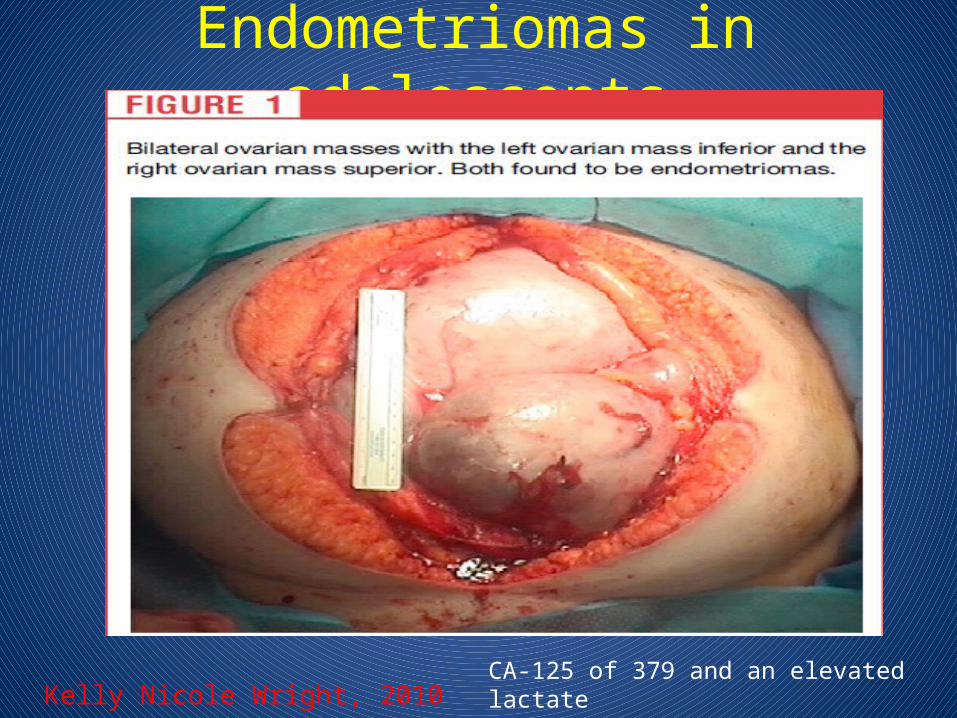
Endometriomas in adolescents
Kelly Nicole Wright, 2010CA-125 of 379 and an elevated lactatedehydrogenase (LDH) of 245.
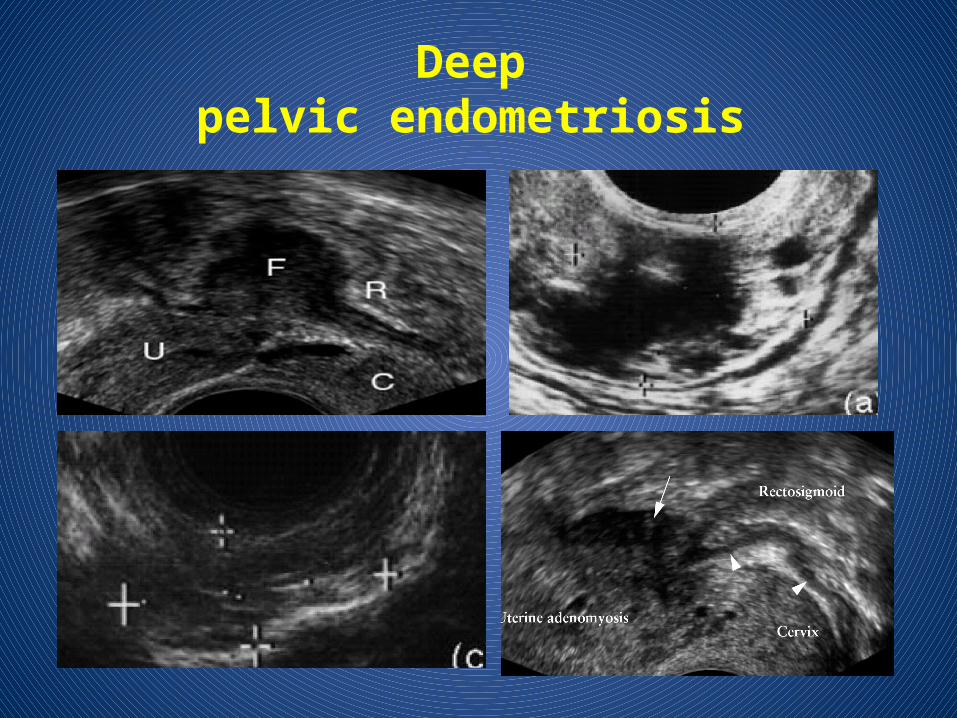
Deeppelvic endometriosis
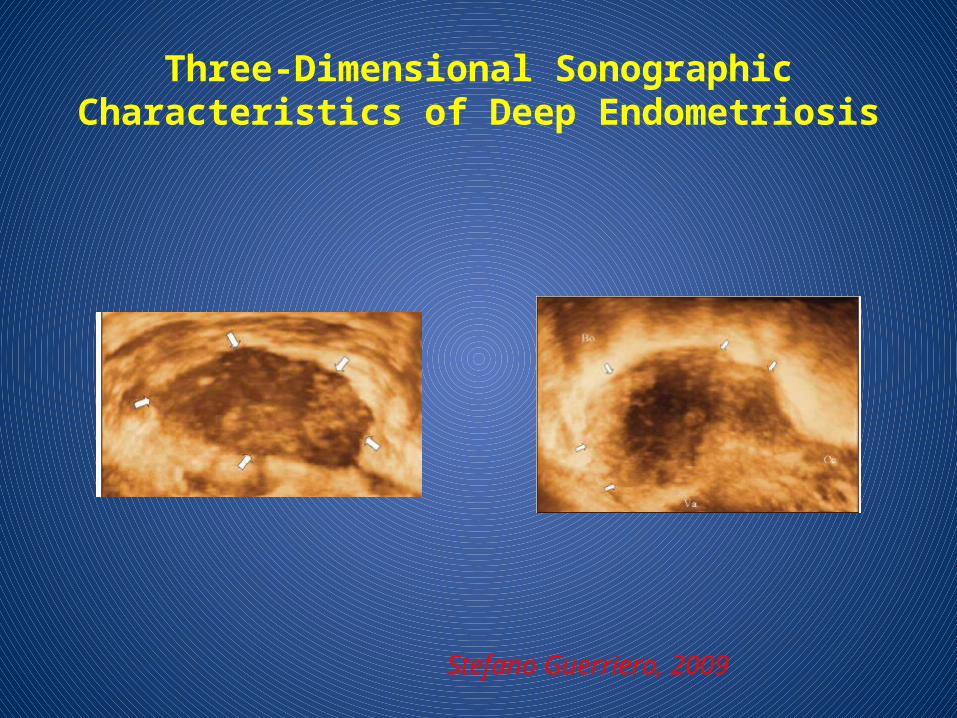
Three-Dimensional SonographicCharacteristics of Deep Endometriosis
Stefano Guerriero, 2009
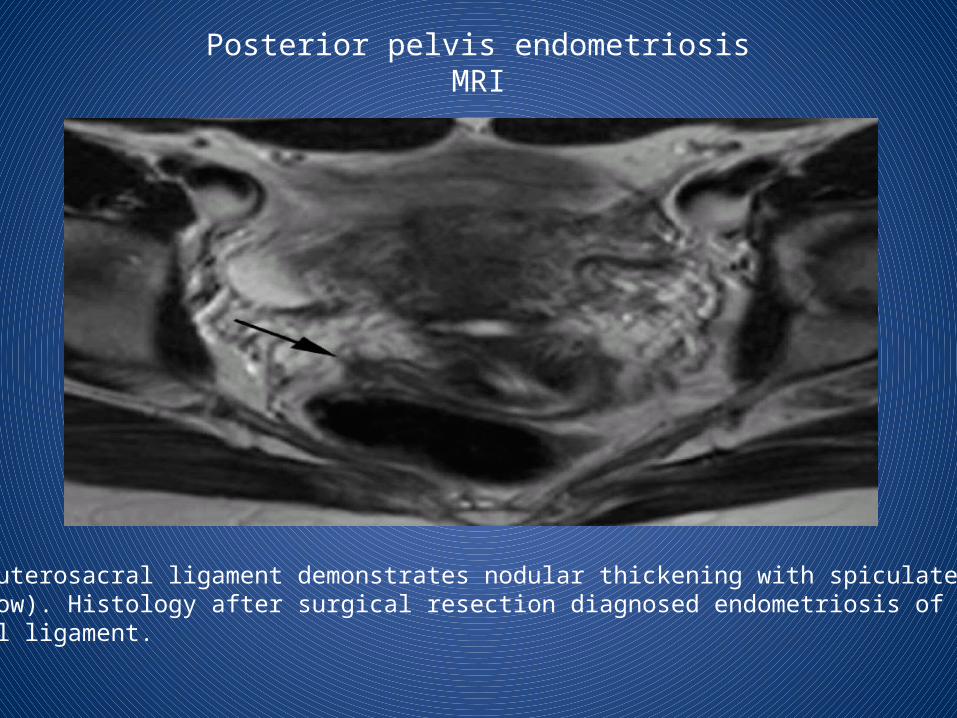
Posterior pelvis endometriosisMRI
The right uterosacral ligament demonstrates nodular thickening with spiculated borders (black arrow). Histology after surgical resection diagnosed endometriosis of the right uterosacral ligament.
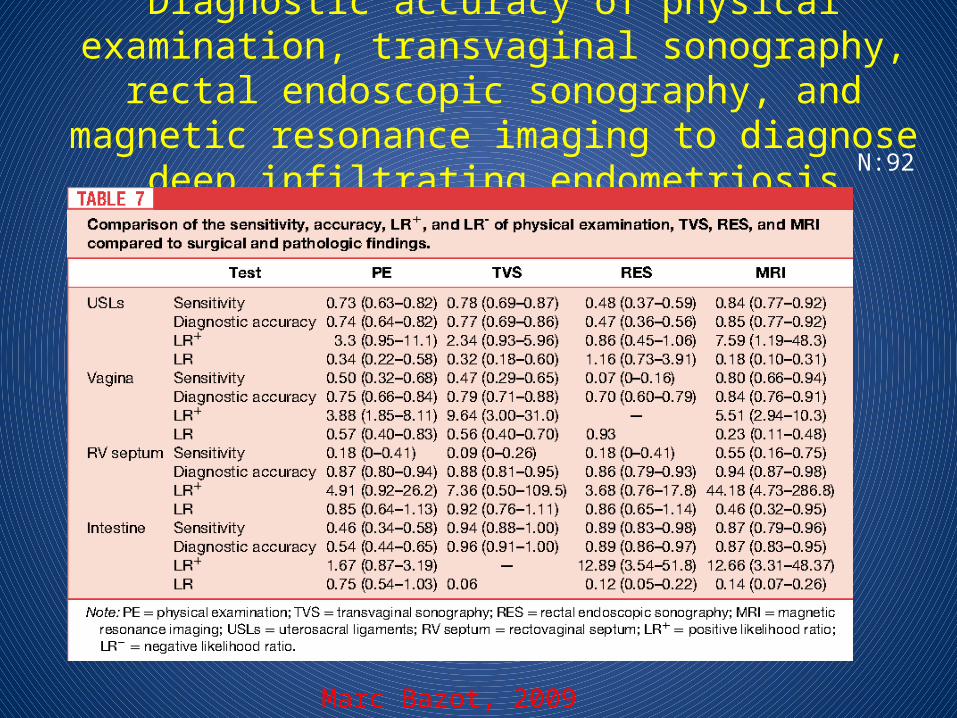
Diagnostic accuracy of physical examination, transvaginal sonography, rectal endoscopic sonography, and magnetic
resonance imaging to diagnose deep infiltrating endometriosis
Marc Bazot, 2009
N:92
Urinary tract endometriosis (UTE)• Urinary tract endometriosis (UTE) includes the presence of endometrial
tissue in or around the bladder, ureters, urethra, or kidney. This disease, once considered to be a rare clinical entity, is now increasingly recognized .
• Recently, its incidence was estimated to range from 0.3% to 6% among women with endometriosis . The percentage of bladder involvement in these cases is 84%–90% .
• Within the urinary system, the bladder is the most commonly affected (80%-84%), followed by the ureter (15%), kidney (4%), and urethra (2%).
• In the bladder, the retrotrigone and dome are the most frequently affected sites. Two possible ureteral lesions must be considered:intrinsic and extrinsic.
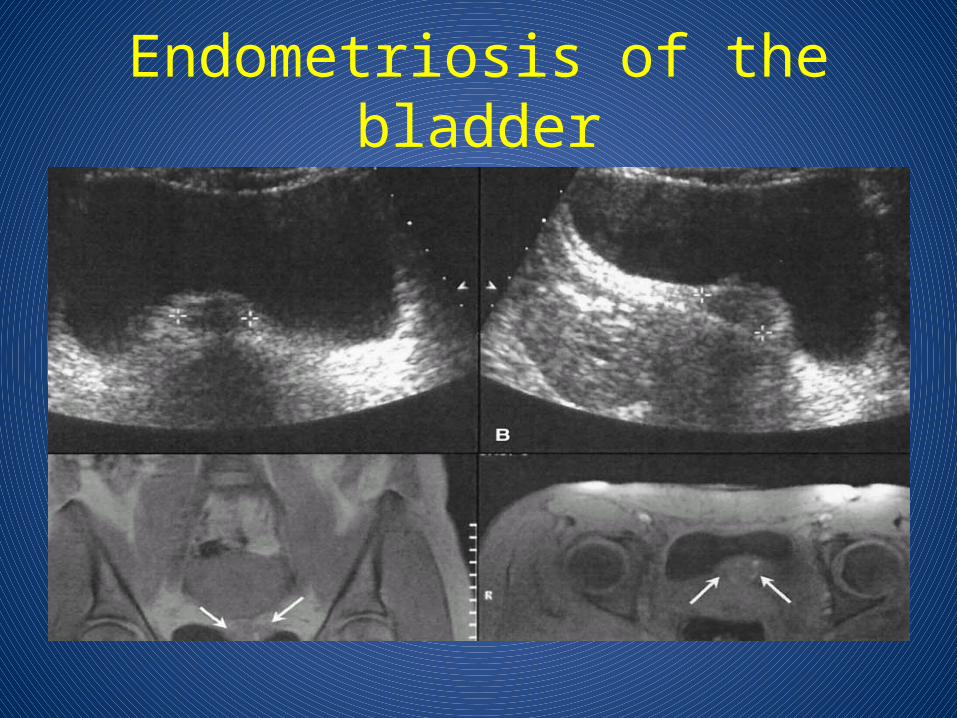
Endometriosis of the bladder
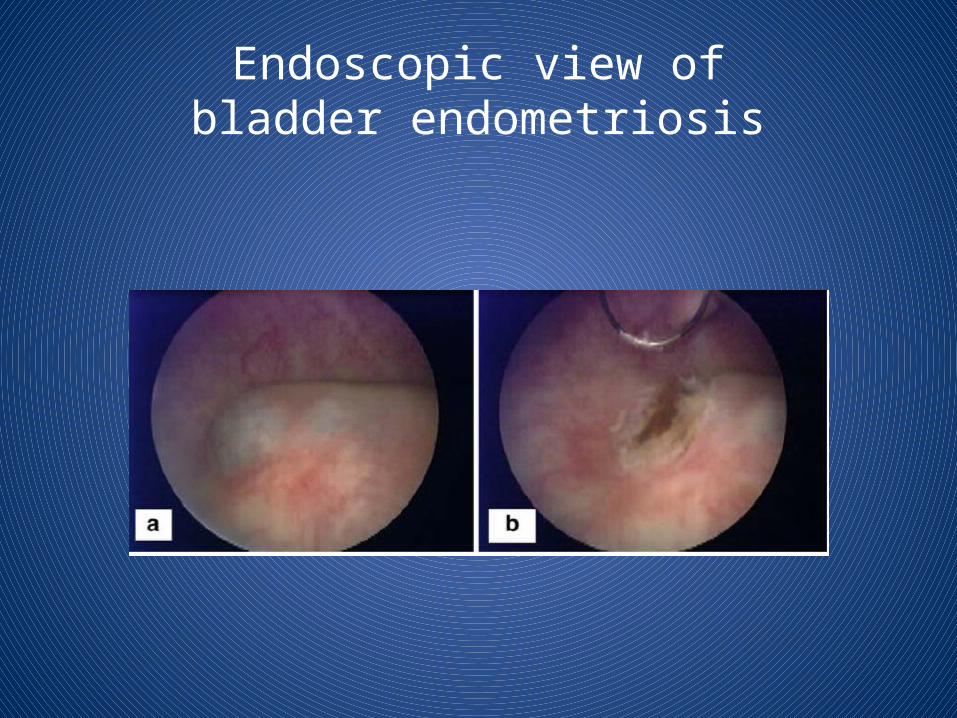
Endoscopic view ofbladder endometriosis
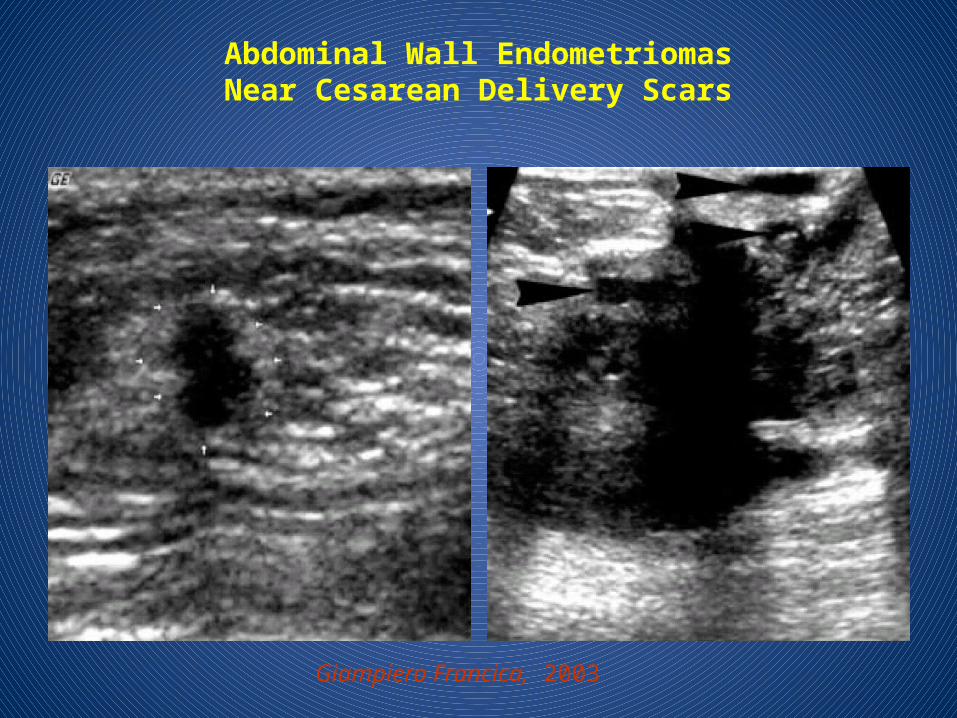
Abdominal Wall EndometriomasNear Cesarean Delivery Scars
Giampiero Francica, 2003
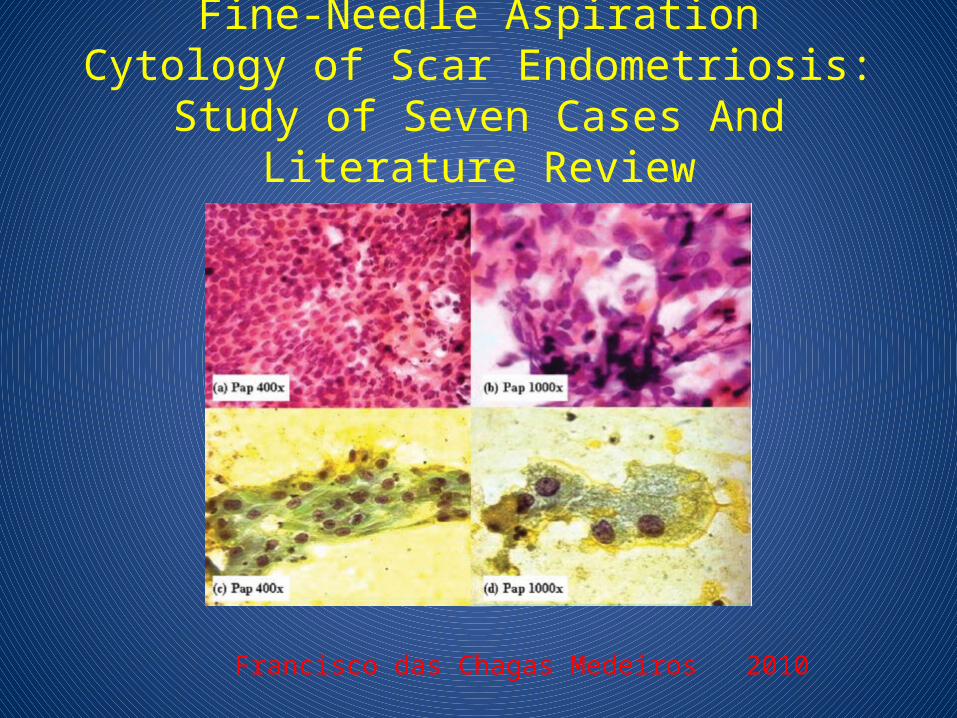
Fine-Needle AspirationCytology of Scar Endometriosis:
Study of Seven Cases And Literature Review
Francisco das Chagas Medeiros 2010
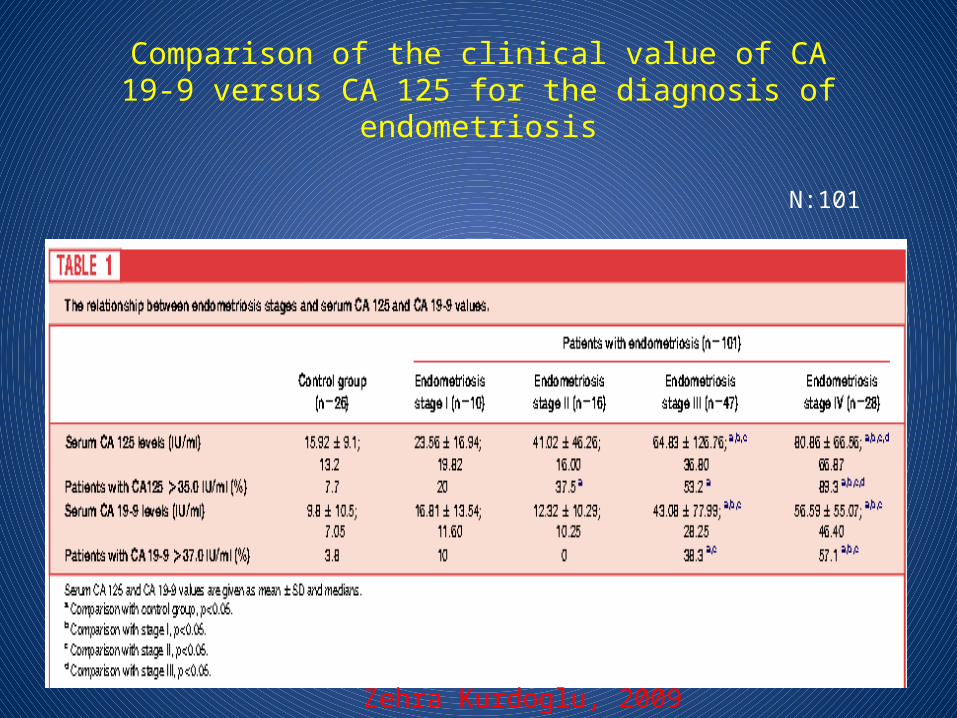
Comparison of the clinical value of CA19-9 versus CA 125 for the diagnosis of
endometriosis
Zehra Kurdoglu, 2009
N:101
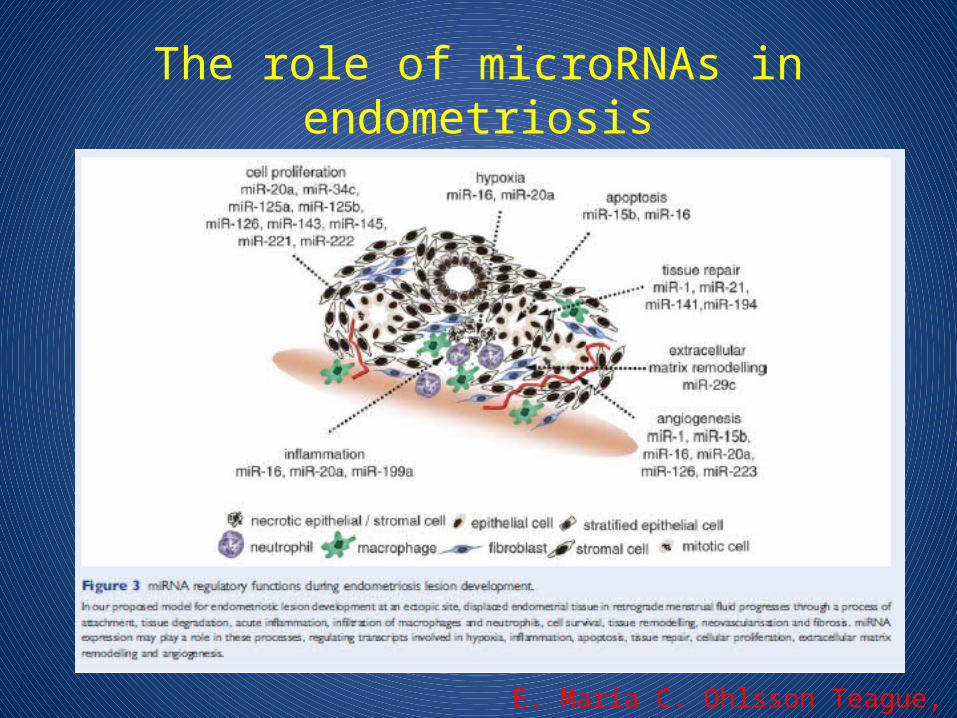
The role of microRNAs inendometriosis
E. Maria C. Ohlsson Teague, 2010
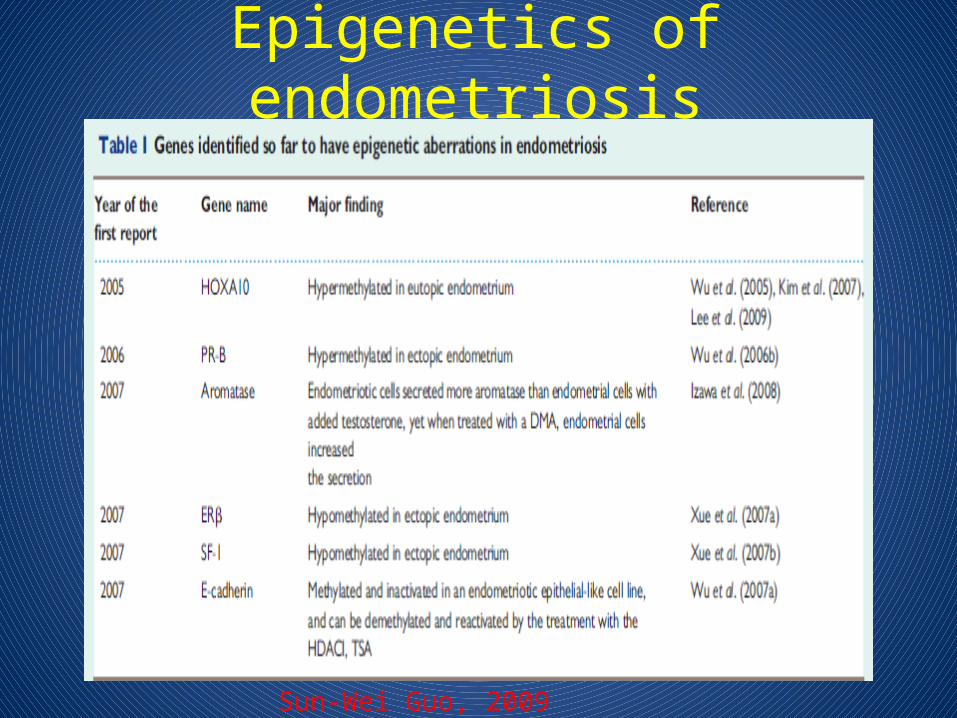
Epigenetics of endometriosis
Sun-Wei Guo, 2009
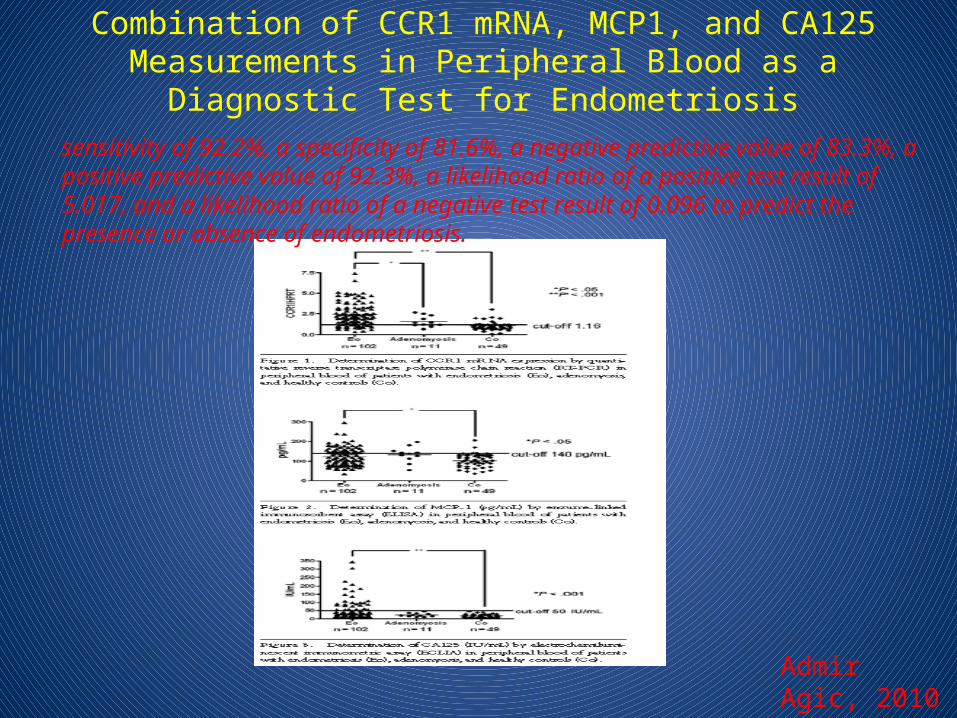
Combination of CCR1 mRNA, MCP1, and CA125 Measurements in Peripheral Blood as a Diagnostic Test for Endometriosis
Admir Agic, 2010
sensitivity of 92.2%, a specificity of 81.6%, a negative predictive value of 83.3%, a positive predictive value of 92.3%, a likelihood ratio of a positive test result of 5.017, and a likelihood ratio of a negative test result of 0.096 to predict the presence or absence of endometriosis.
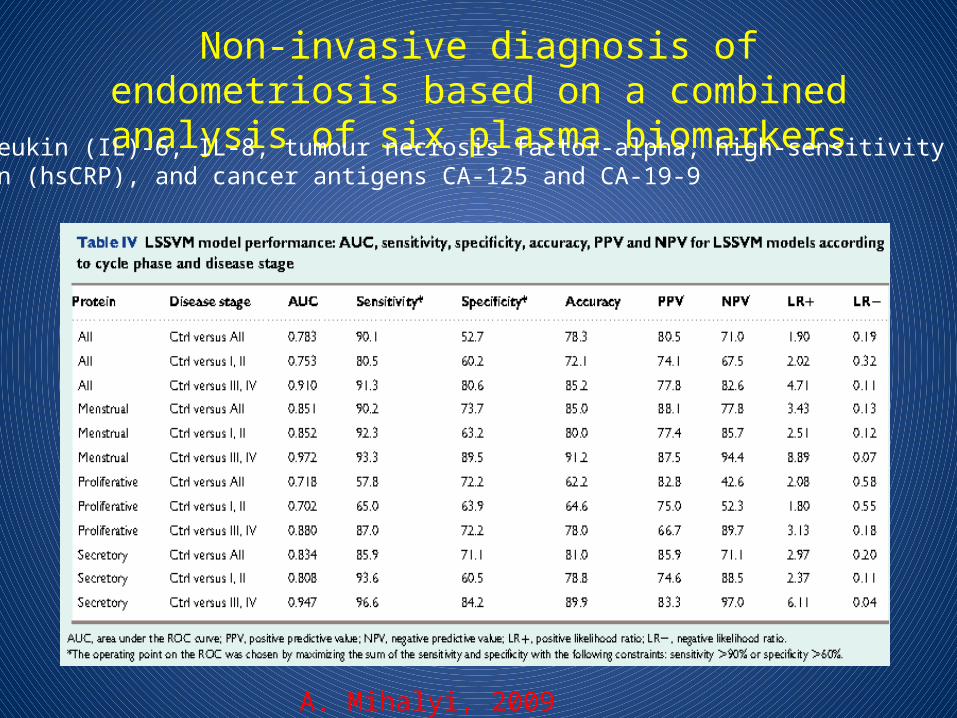
Non-invasive diagnosis of endometriosis based on a combined analysis of six plasma biomarkers
A. Mihalyi, 2009
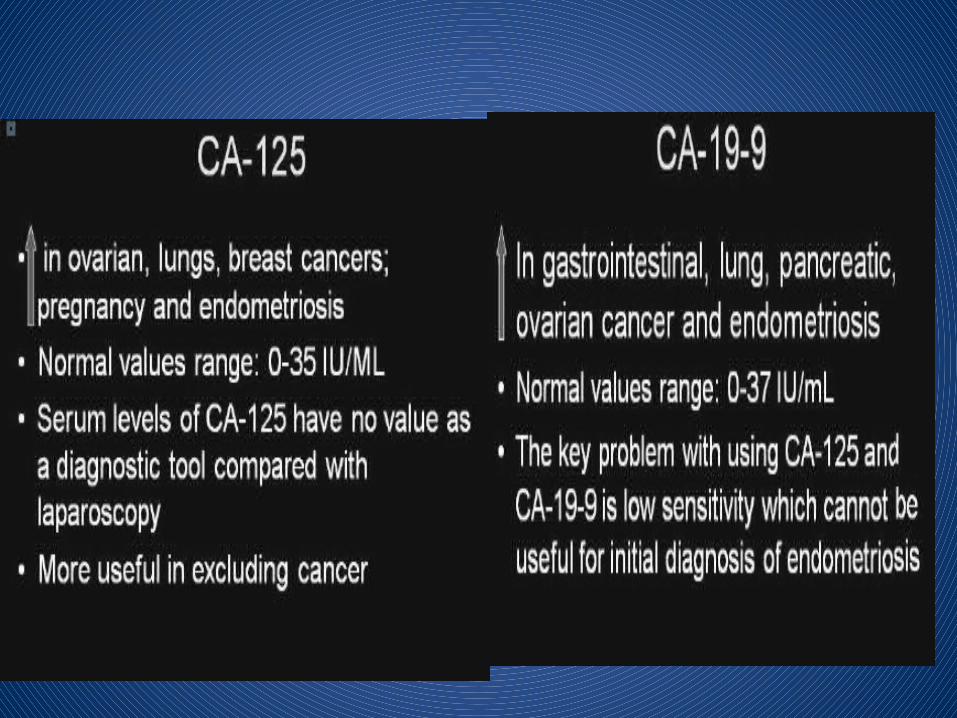
interleukin (IL)-6, IL-8, tumour necrosis factor-alpha, high-sensitivity C-reactiveprotein (hsCRP), and cancer antigens CA-125 and CA-19-9
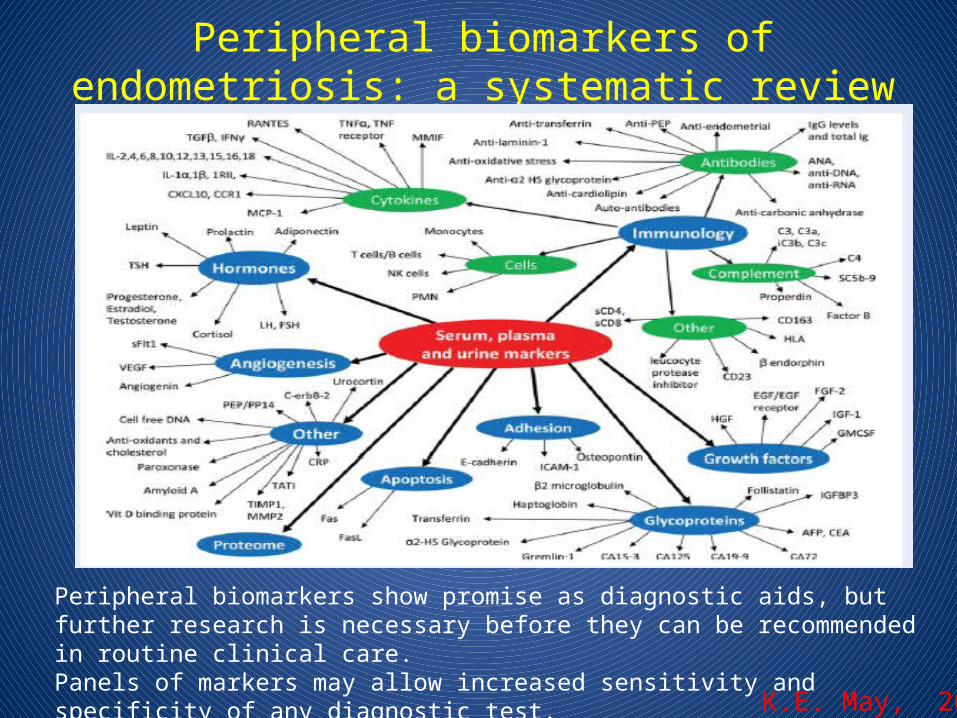
Peripheral biomarkers ofendometriosis: a systematic review
K.E. May, 2010
Peripheral biomarkers show promise as diagnostic aids, but further research is necessary before they can be recommended in routine clinical care. Panels of markers may allow increased sensitivity and specificity of any diagnostic test.
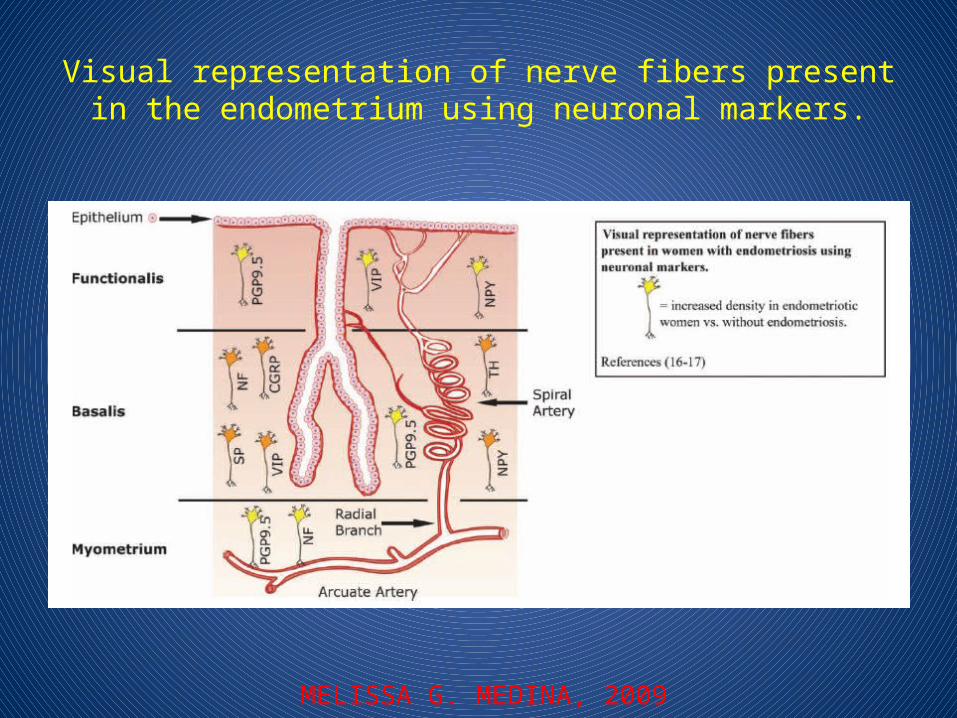
Visual representation of nerve fibers present in the endometrium using neuronal markers.
MELISSA G. MEDINA, 2009
A pilot study to evaluate the relative efficacy of endometrialbiopsy and full curettage in making a diagnosis of
endometriosis by the detection of endometrialnerve fibers
• Endometrial biopsies with precise, consistent technique and curettings were taken from 37 women (20 with endometriosis and 17 without endometriosis).
• Small nerve fibers were detected in all endometrial biopsies and curettings from all 20 women with endometriosis, but were not detected in endometrium taken from 17 women without endometriosis
Moamar Al-Jefout, 2007
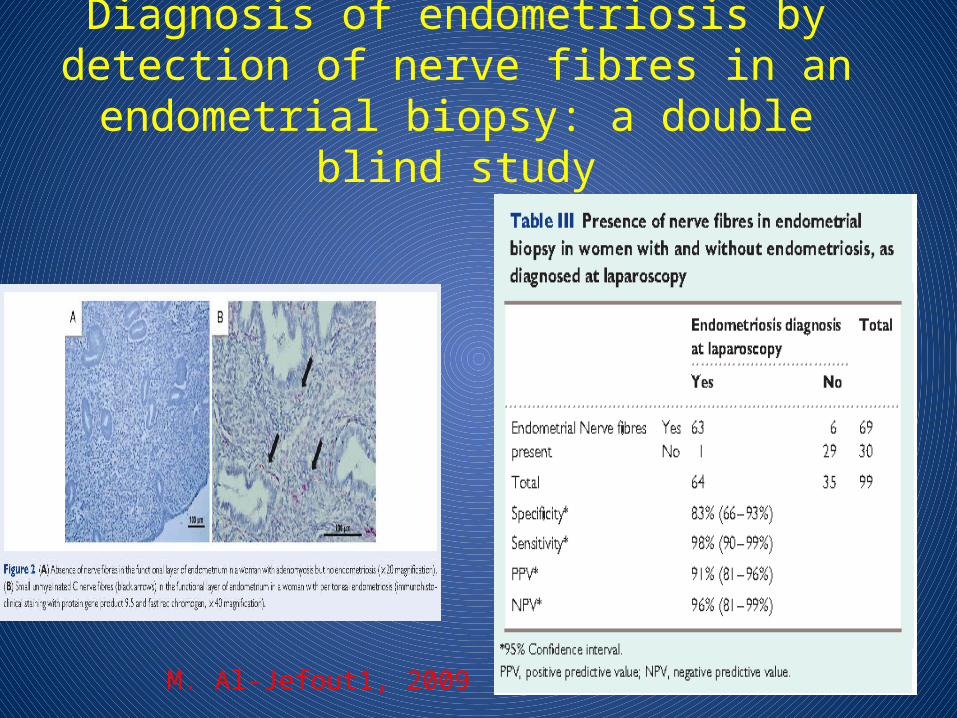
Diagnosis of endometriosis by detection of nerve fibres in an endometrial biopsy: a double
blind study
M. Al-Jefout1, 2009
Density of small diameter sensory nerve fibres in endometrium: a semi-invasive diagnostic test for
minimal to mild endometriosis
• Secretory phase endometrium samples (n 40), obtained from women with laparoscopically/histologically confirmed minimal–mild endometriosis (n 20) and from women with a normal pelvis (n 20) were selected
• The density of small nerve fibres was 14 times higher in endometrium from patients with minimal–mild endometriosis (1.96+2.73) when compared with women with a normal pelvis (0.14+0.46, P , 0.0001).
• The combined analysis of neural markers PGP9.5, VIP and SP could predict the presence of minimal–mild endometriosis with 95% sensitivity, 100% specificity and 97.5% accuracy.
A. Bokor, 2009
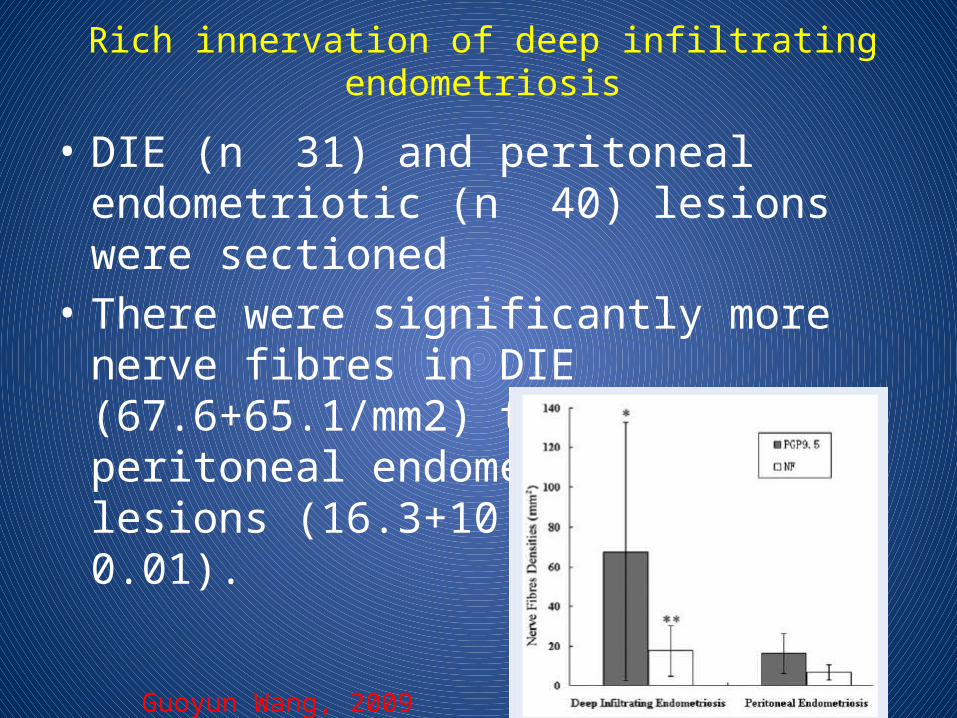
Rich innervation of deep infiltratingendometriosis
• DIE (n 31) and peritoneal endometriotic (n 40) lesions were sectioned
• There were significantly more nerve fibres in DIE (67.6+65.1/mm2) than in peritoneal endometriotic lesions (16.3+10.0/mm2) (P , 0.01).
Guoyun Wang, 2009
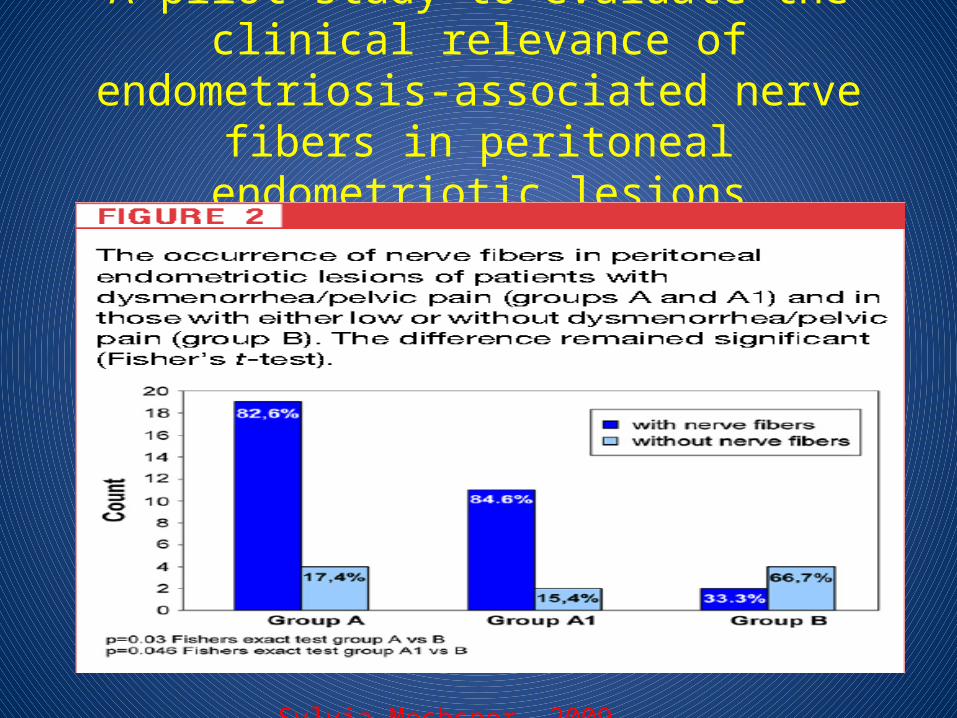
A pilot study to evaluate the clinical relevance ofendometriosis-associated nerve fibers in
peritoneal endometriotic lesions
Sylvia Mechsner, 2009
Nerve fibres in ovarian endometrioticlesions in women with ovarian endometriosis
Xinmei Zhang, 2010
• Histological sections of ovarian endometriotic lesions from 61 women with ovarian endometriosis (Stages II–IV) who underwent laparoscopic endometrioma
• Nerve fibres stained with PGP9.5 were detected in ovarian endometriotic lesions in 31.1% of women, and most appeared in fibrotic interstitium of ovarian endometriotic lesions. The density of PGP9.5-immunoactive fibres in ovarian endometriotic lesions in women with pain symptoms (n 35) was higher than in women with no pain symptoms (n 26, P 0.039), although the percentage (positive cases/total) of PGP9.5-positive fibres did not differ cystectomy
Effect of progestogens and combined oralcontraceptives on nerve fibers in peritoneal
endometriosis• Biopsy samples from peritoneal endometriotic lesions in
hormonally treated and untreated women with endometriosis. (N: 22 vs. N:40)
• The nerve fiber density (mean standard deviation/mm2) in peritoneal endometriotic lesions from hormone-treated women with endometriosis (10.6 2.2/mm2) was statistically significantly lower than in peritoneal endometriotic lesions from untreated women with endometriosis (16.3 10.0/mm2).
• Progestogens and combined oral contraceptives reduced nerve fiber density and nerve growth factor and nerve growth factor receptor p75 expression in peritoneal endometriotic lesions.
Natsuko Tokushige, 2009
Endometrial nerve fibers in women with endometriosis, adenomyosis, and uterine fibroids
• To determine whether nerve fibers in the functional layer endometrium are caused by an endometriosis itself or a common symptom of pain, endometrial tissues from 30 women with endometriosis, 40 women with adenomyosis, 41 women with uterine fibroids, and 47 endometriosis women with adenomyosis were stained immunohistochemically using the highly specific polyclonal rabbit antiprotein gene product 9.5 (PGP9.5) and monoclonal mouse antineurofilament protein.
• We demonstrated PGP9.5-immunoactive nerve fibers in the functional layer of endometrium in women with pain symptoms, but not in women without pain symptoms, whether the women had endometriosis, adenomyosis, uterine fibroids, or endometriosis with adenomyosis, suggesting a role of PGP9.5-immunoactive nerve fibers in the functional layer of the endometrium playing in pain generation in these disorders
Xinmei Zhang, 2009
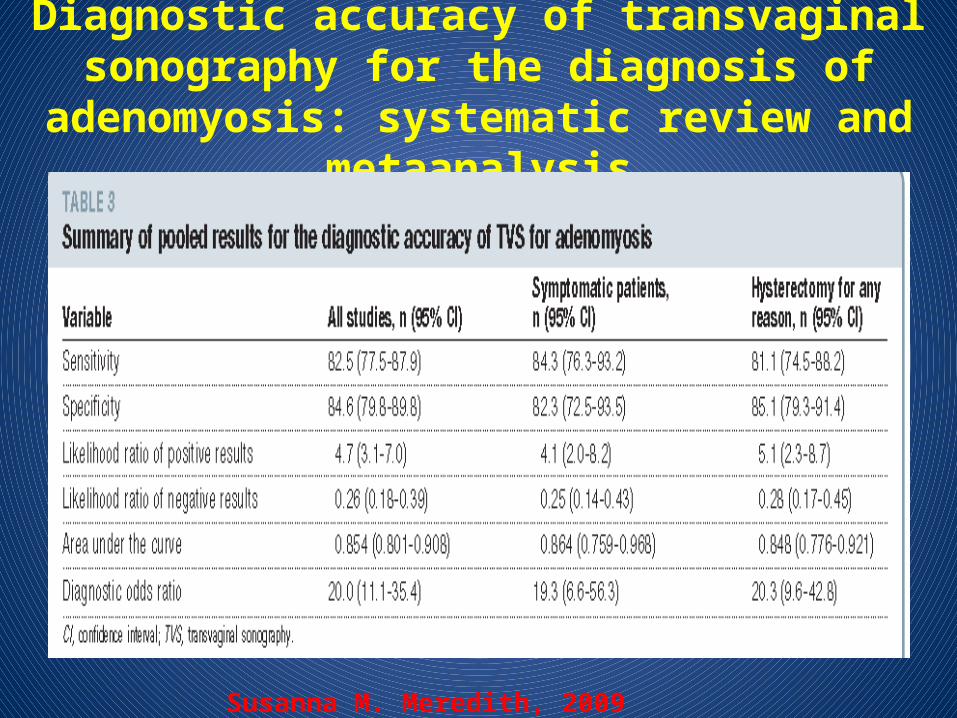
Diagnostic accuracy of transvaginal sonography for the diagnosis of adenomyosis: systematic review and
metaanalysis
Susanna M. Meredith, 2009
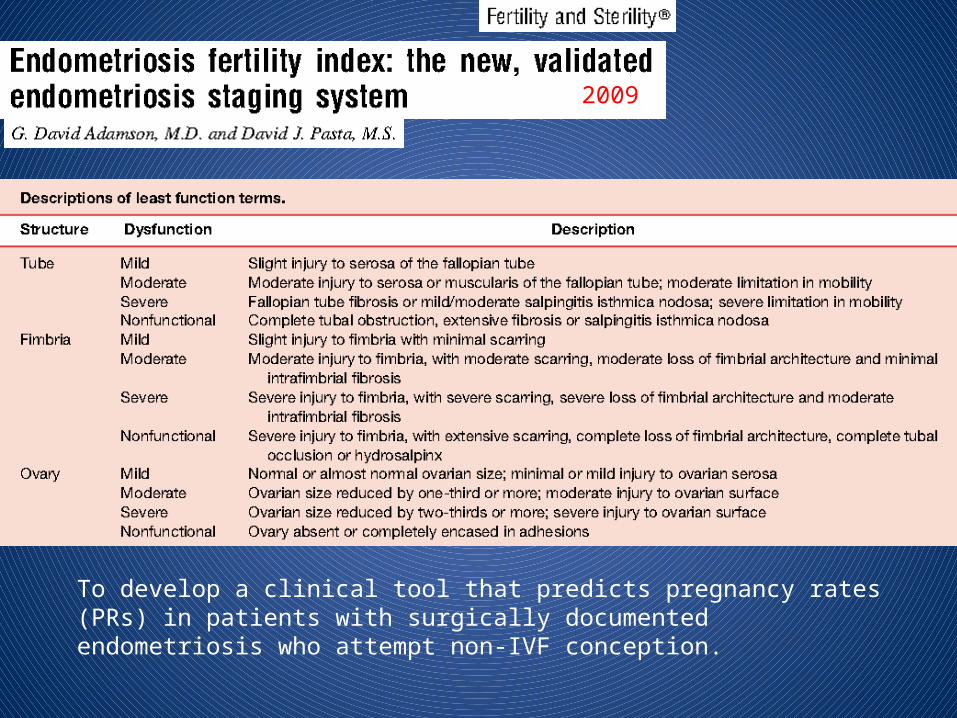
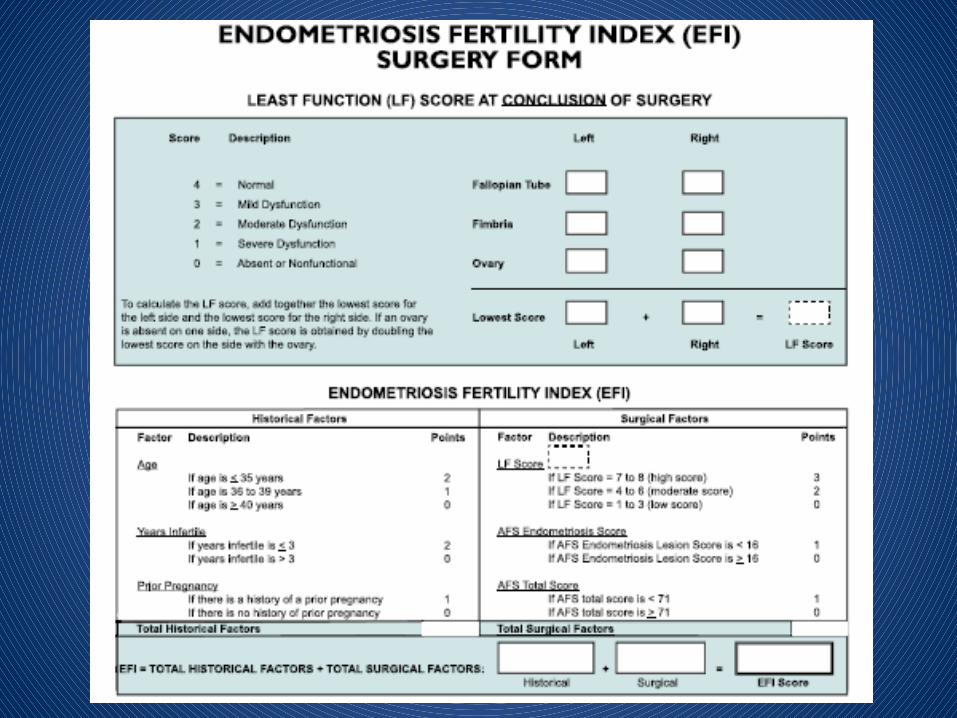
To develop a clinical tool that predicts pregnancy rates (PRs) in patients with surgically documented endometriosis who attempt non-IVF conception.
2009
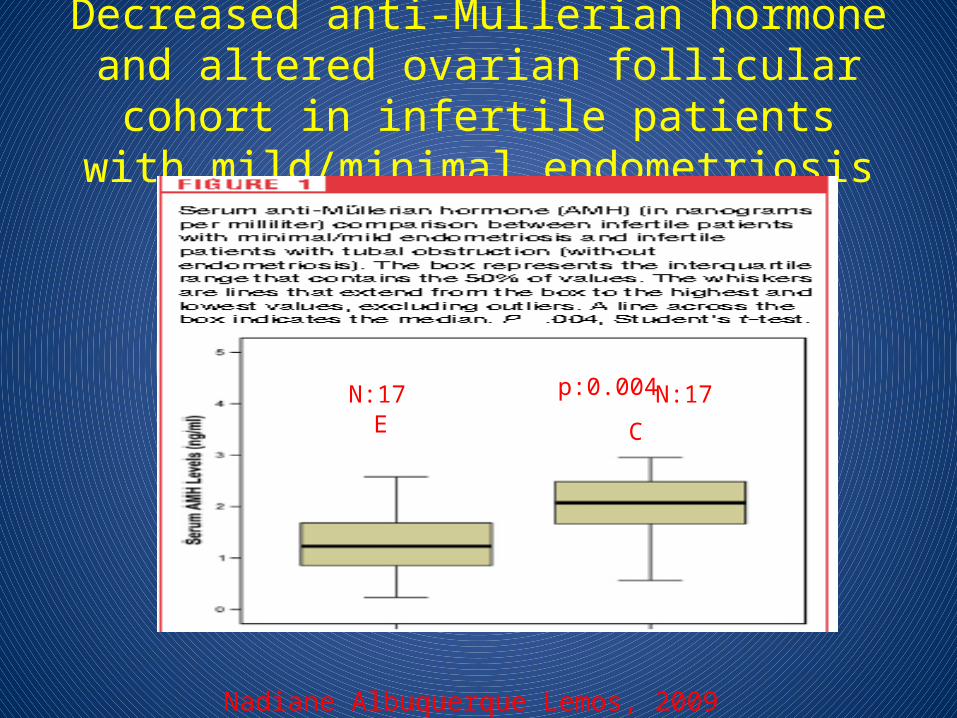
Decreased anti-Mullerian hormone and altered ovarian follicular cohort in infertile patients with
mild/minimal endometriosis
Nadiane Albuquerque Lemos, 2009
EE CC
p:0.004N:17 N:17
Anti mullerian hormone serum levels in women with endometriosis:
A case–control study
• 909 patients undergoing in vitro fertilisation/intracytoplasmic sperm injection (IVF/ICSI) treatment or consulting our specific endometriosis unit.
• Mean AMH serum level was significantly lower in the study than in the control group (2.75+2.0 ng/ml vs. 3.46+2.30 ng/ml, p 0.001).
• In women with mild endometriosis (rAFS I-II), the mean AMH level was almost equal to the control group (3.28+1.93 ng/ml vs. 3.44+2.06 ng/ml; p 0.61).
• A significant difference in mean AMH serum level was found between women with severe endometriosis (rAFS III-IV) and the control group (2.38+1.83 ng/ml vs. 3.58+2.46 ng/ml; p 0.0001).
OMAR SHEBL, 2009
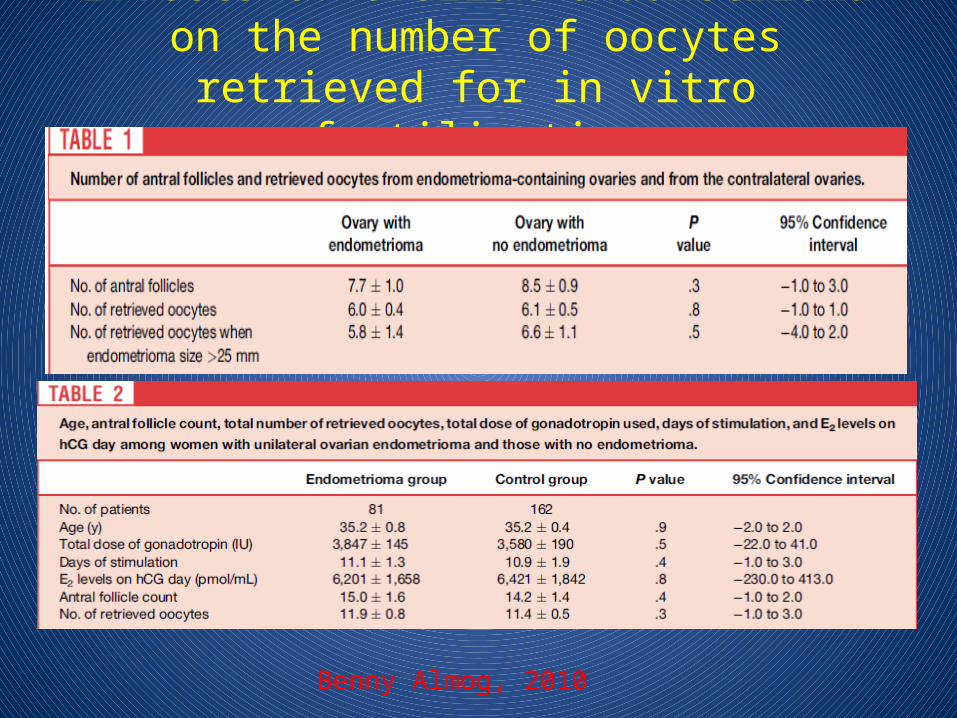
Effects of ovarian endometrioma on the number of oocytes retrieved for in vitro fertilization
Benny Almog, 2010
The impact of electrocoagulation on ovarian reserve after laparoscopic excision of ovarian
cysts: a prospective clinical study of 191 patients• 191 patients with benign ovarian cysts undergoing ovarian cystectomy.• When comparing the bipolar group and ultrasonic scalpel group with the
suture group, a statistically significant increase of the mean FSH value was found in bilateral-cyst patients at 1-, 3-, 6-, and 12-month follow-up evaluations and in unilateral-cyst patients at the 1-month follow-up evaluation.
• Statistically significant decreases of basal antral follicle number and mean ovarian diameter were found during the 3-, 6-, 12-month follow-up evaluations as well as statistically significant decreases of peak systolic velocity at all of the follow-up evaluations.
• Conclusion(s): Electrocoagulation after laparoscopic excision of ovarian cysts is associated with a statistically significant reduction in ovarian reserve, which is partly a consequence of the damage to the ovarian vascular system.
Chang-Zhong Li, 2009
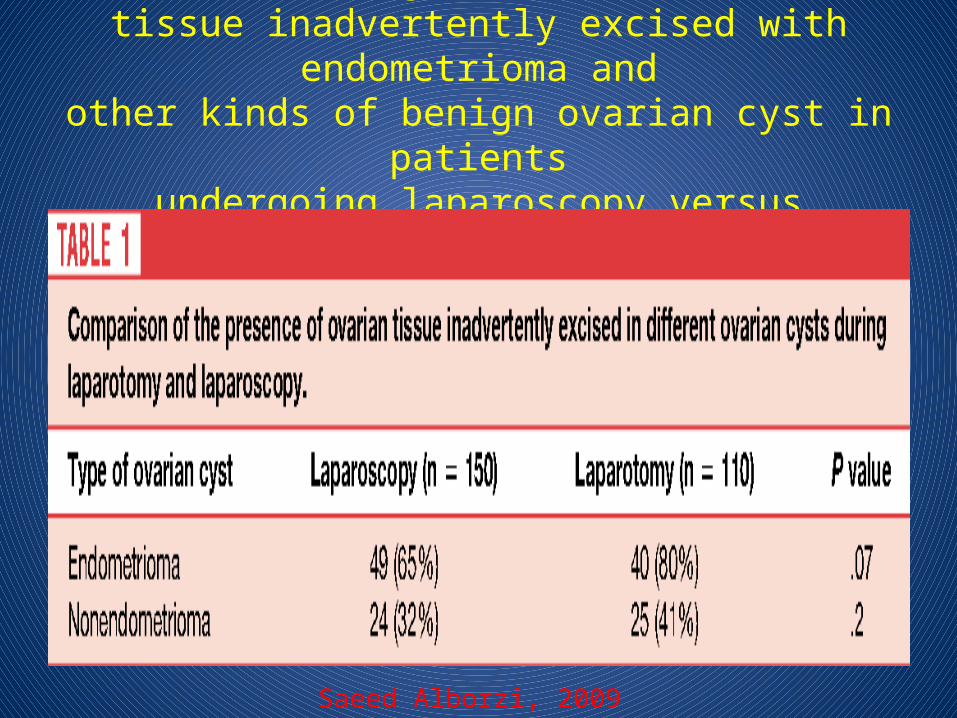
A comparison of histopathologic findings of ovariantissue inadvertently excised with endometrioma and
other kinds of benign ovarian cyst in patientsundergoing laparoscopy versus laparotomy
Saeed Alborzi, 2009
Analysis of risk factors for the removalof normal ovarian tissue during laparoscopic cystectomy for
ovarian endometriosis
• A total of 121 patients who had histologically confirmed ovarian endometriosis and 56 control patients who had other histologically confirmed benign cysts were included
• Normal ovarian tissue adjacent to the cyst wall was detected in 71 patients (58.7%) with endometriosis, whereas normal ovarian tissue was removed from only three patients (5.4%) with other benign cysts.
• A significant factor that was independently associated with the removal of normal ovarian tissue with ovarian endometriosis was pre-operative medical treatment
Sachiko Matsuzaki1,2009
Endometriosis/Endometrioma-ART
• Does Endometriosis/endometrioma affect the ovarian reserve ? – Yes, but pregnancy rates do not change
• Does Endometriosis/endometrioma surgery affect the ovarian reserve ?• Yes• Spontan pregnancy rates may increase, but Ivf
results do not change (except bilateral cases)
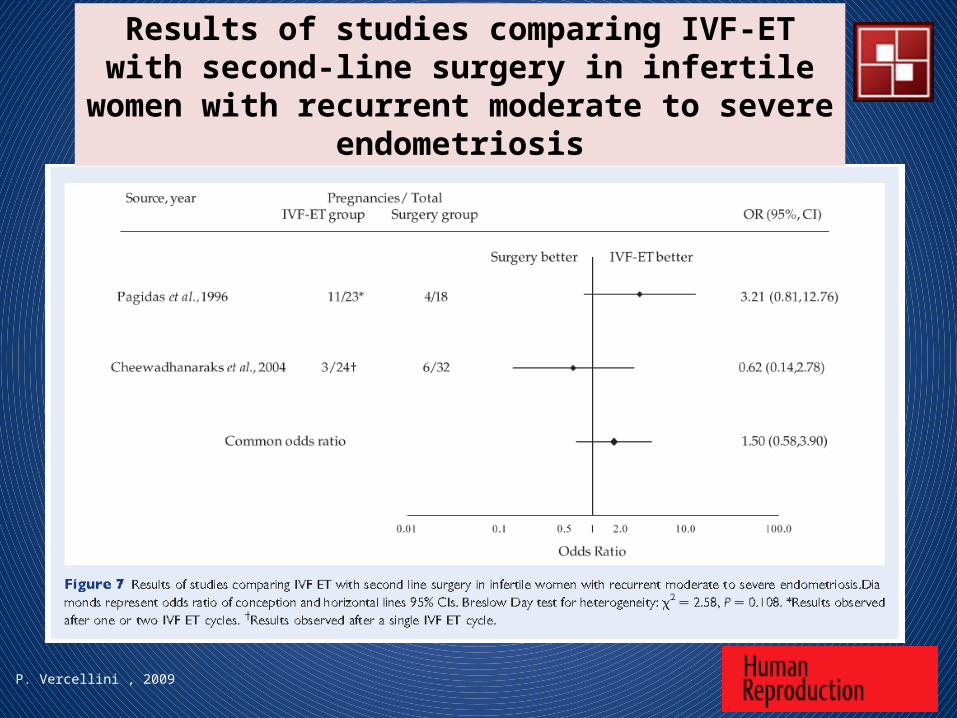
P. Vercellini , 2009
Results of studies comparing IVF-ET with second-line surgery in infertile women with recurrent moderate to
severe endometriosis
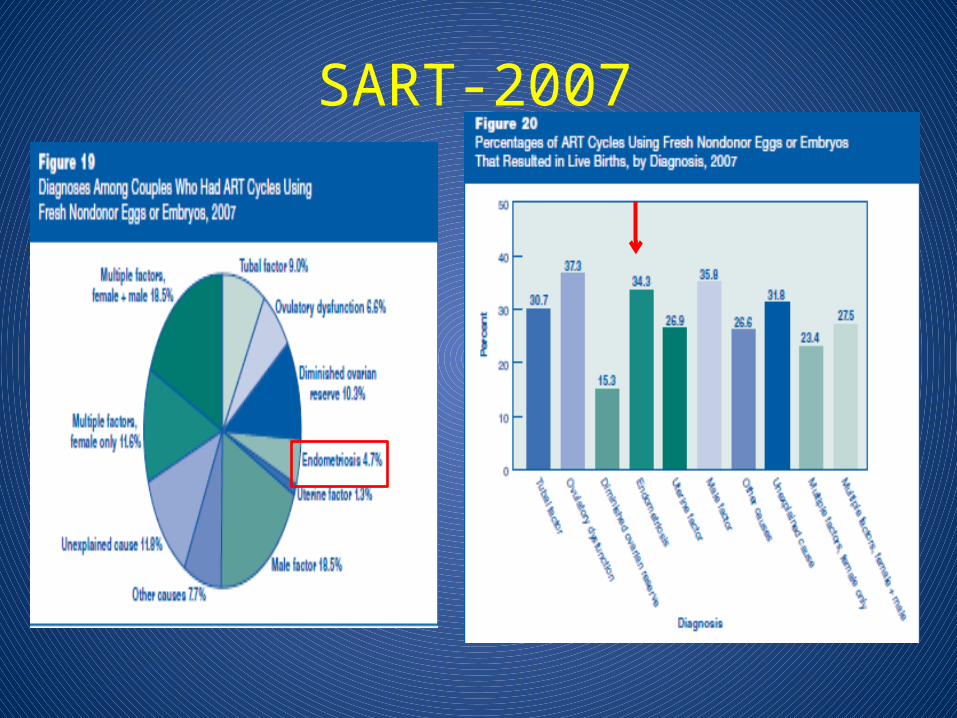
SART-2007
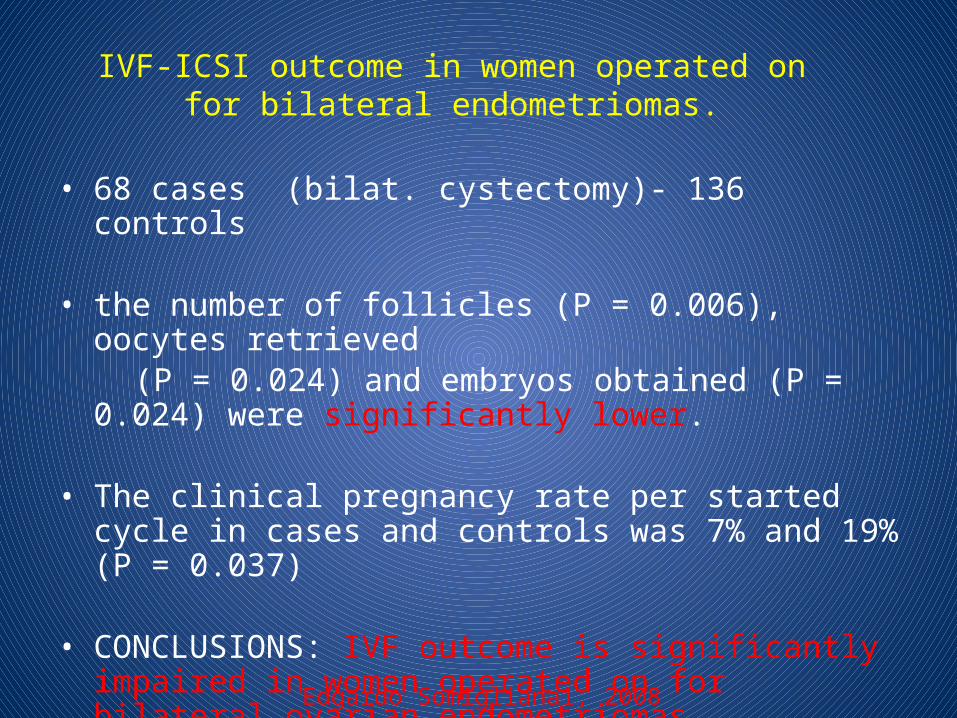
IVF-ICSI outcome in women operated on for bilateral endometriomas.
• 68 cases (bilat. cystectomy)- 136 controls
• the number of follicles (P = 0.006), oocytes retrieved (P = 0.024) and embryos obtained (P = 0.024) were
significantly lower.
• The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P = 0.037)
• CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas.
Edgardo Somigliana1, 2008
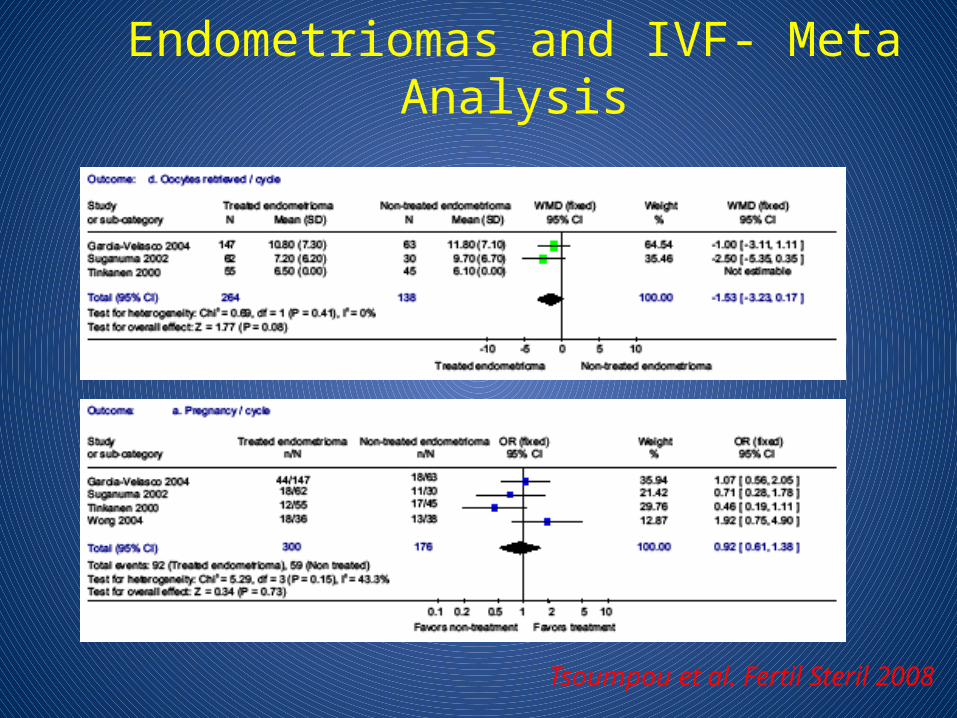
Endometriomas and IVF- Meta Analysis
Tsoumpou et al. Fertil Steril 2008
30 June 2007
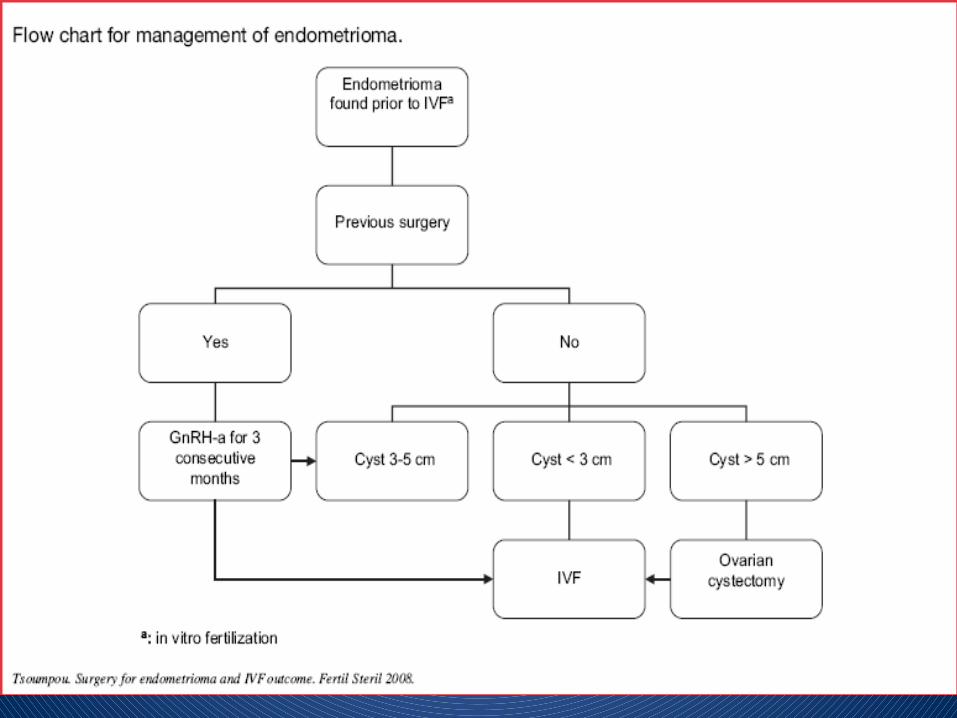
Laparoscopic ovarian cystectomy is recommended if anovarian endometrioma ≥4 cm in diameter is present to confirm the diagnosis histologically; reduce the risk of infection; improve access to follicles and possibly improve ovarian response. The woman should be counselled regarding the risks of reduced ovarian function after surgery and the loss of the ovary. The decision should be reconsidered if she has had previous ovarian surgery.
GPP
http://guidelines.endometriosis.org
Endometrioma and IVF
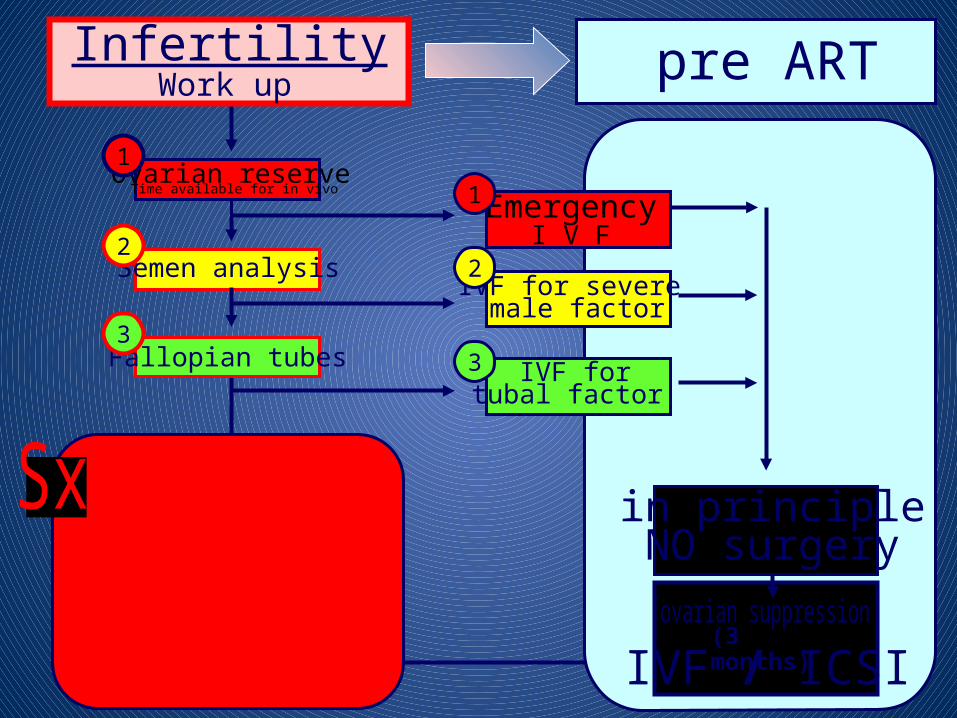
Semen analysis
Fallopian tubes
2
3
Ovarian reserveTime available for in vivo
1
if not pregnant
SurgeryProvide 6-18 mofor spontaneous preg.
pre ART
IVF for severe male factor
IVF fortubal factor
Emergency I V F
IVF / ICSI
2
3
1
(3 months)
in principleNO surgery
InfertilityWork up
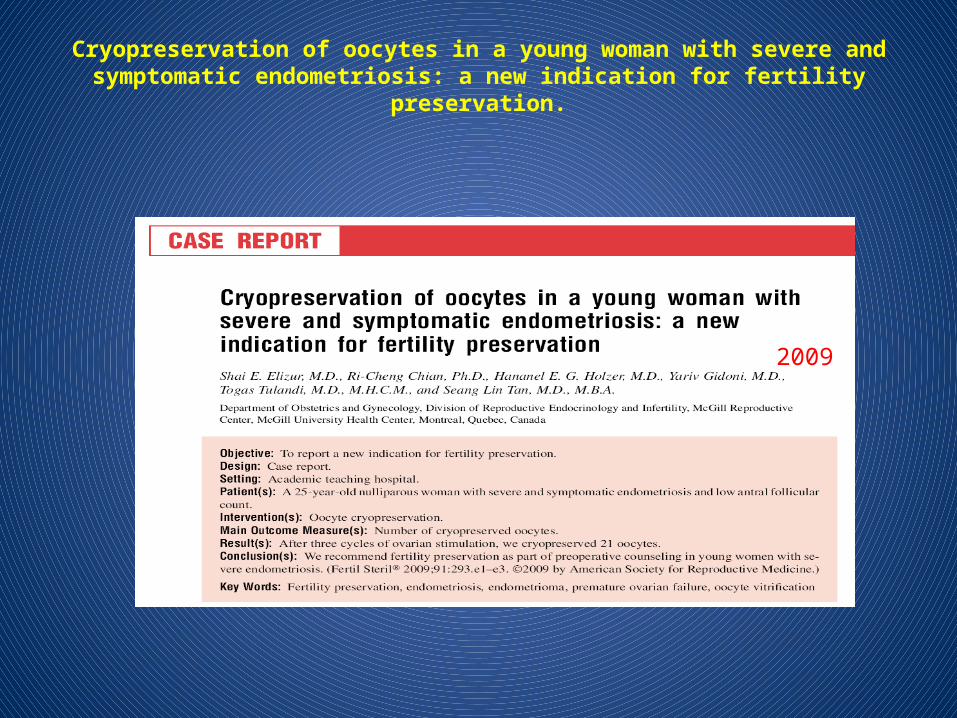
Cryopreservation of oocytes in a young woman with severe and symptomatic endometriosis: a new indication for fertility preservation.
2009
2008
Endometriosis-GnRHa
• Pain• After operation for the prevention • Before IVF • Empirical
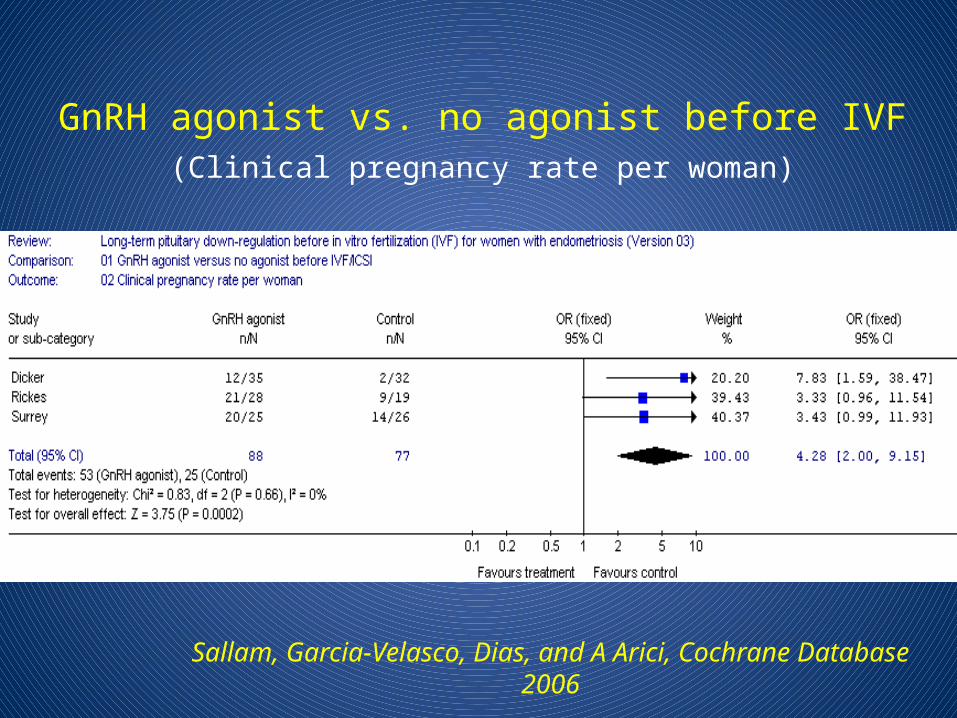
GnRH agonist vs. no agonist before IVF(Clinical pregnancy rate per woman)
Sallam, Garcia-Velasco, Dias, and A Arici, Cochrane Database 2006
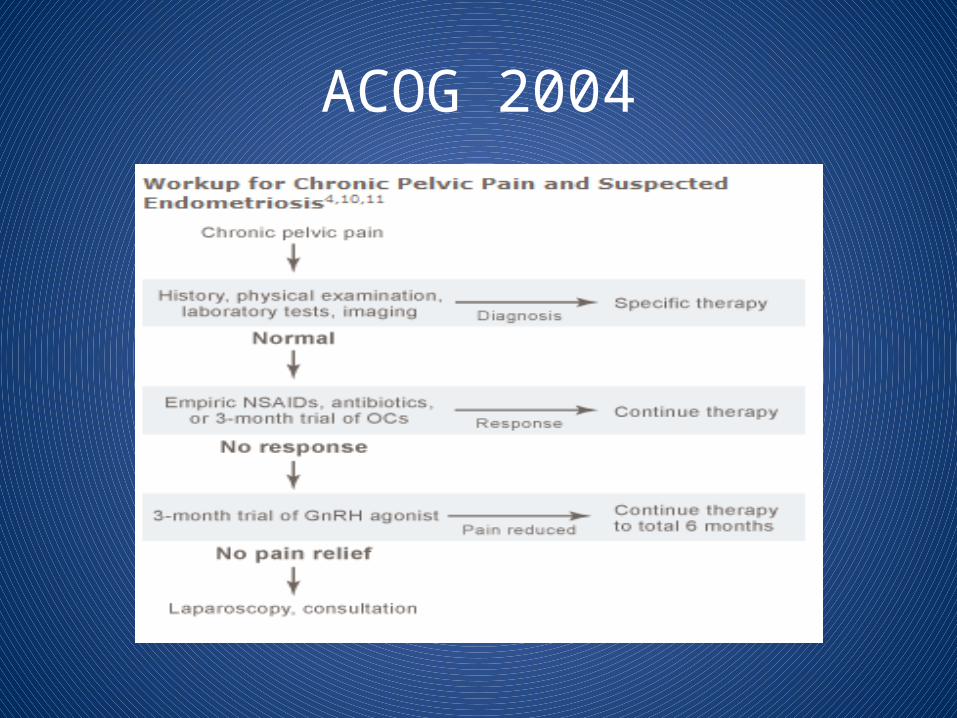
ACOG 2004
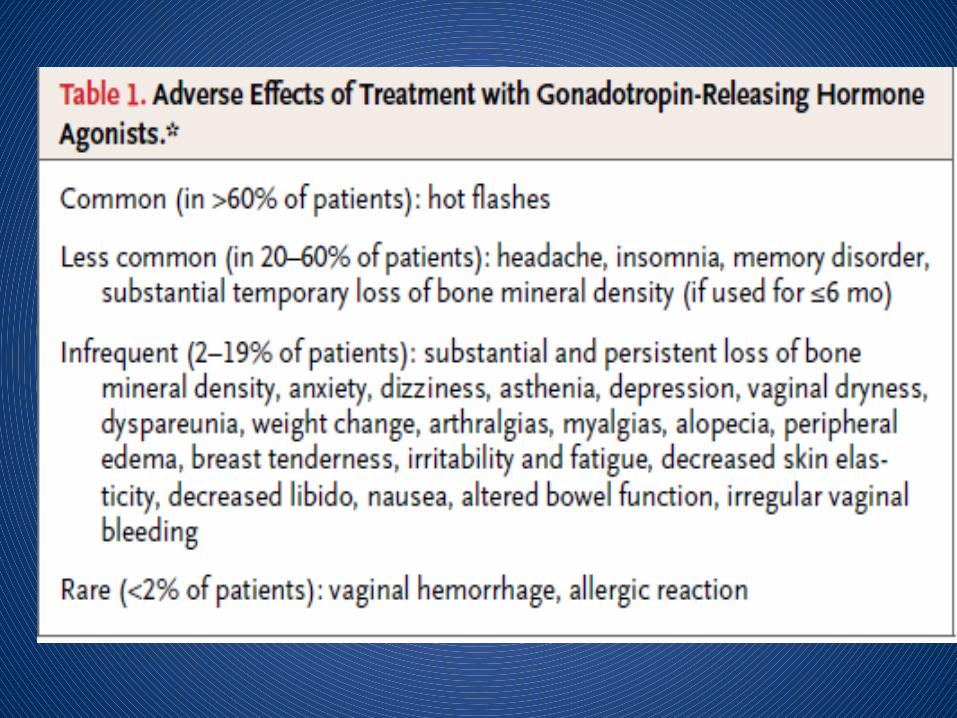
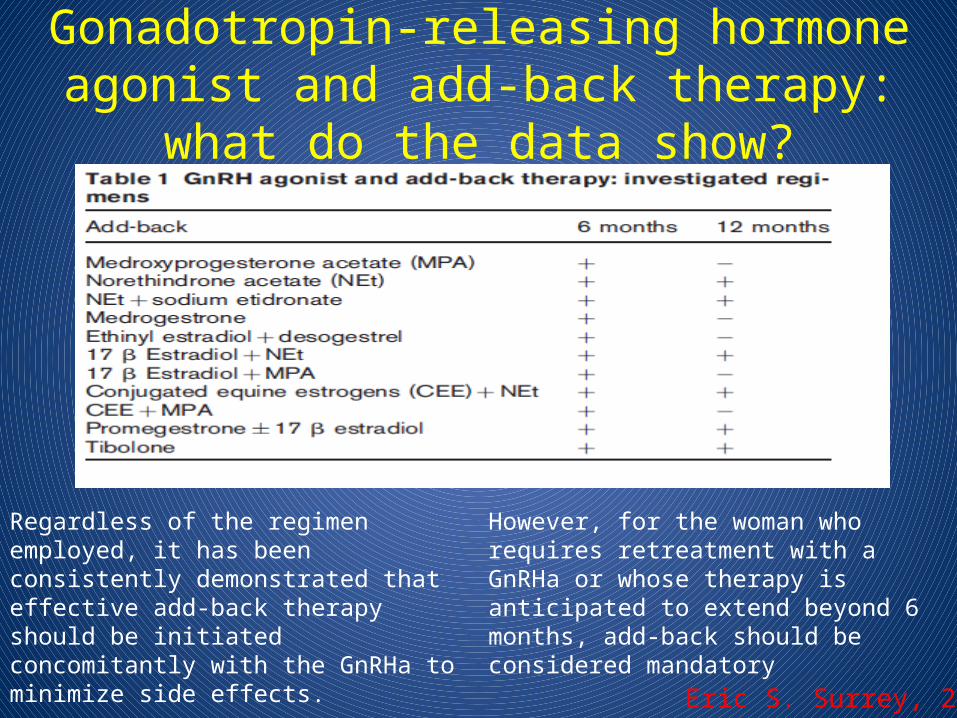
Gonadotropin-releasing hormone agonist and add-back therapy: what do the data show?
Eric S. Surrey, 2010
Regardless of the regimen employed, it has been consistently demonstrated that effective add-back therapy should be initiated concomitantly with the GnRHa tominimize side effects.
However, for the woman whorequires retreatment with a GnRHa or whose therapy is anticipated to extend beyond 6 months, add-back should be considered mandatory
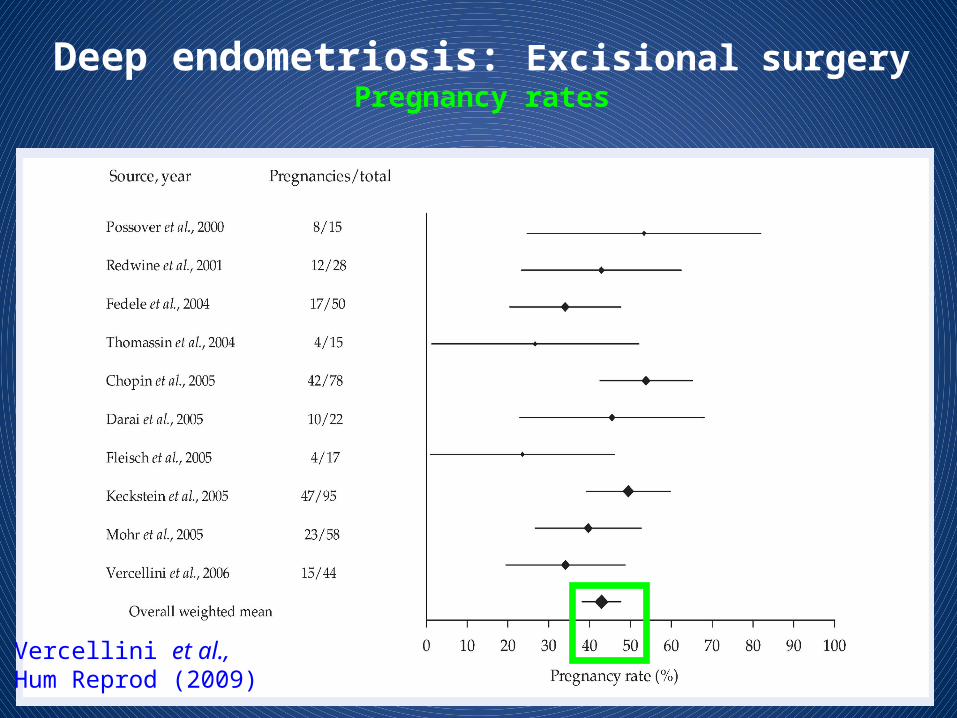
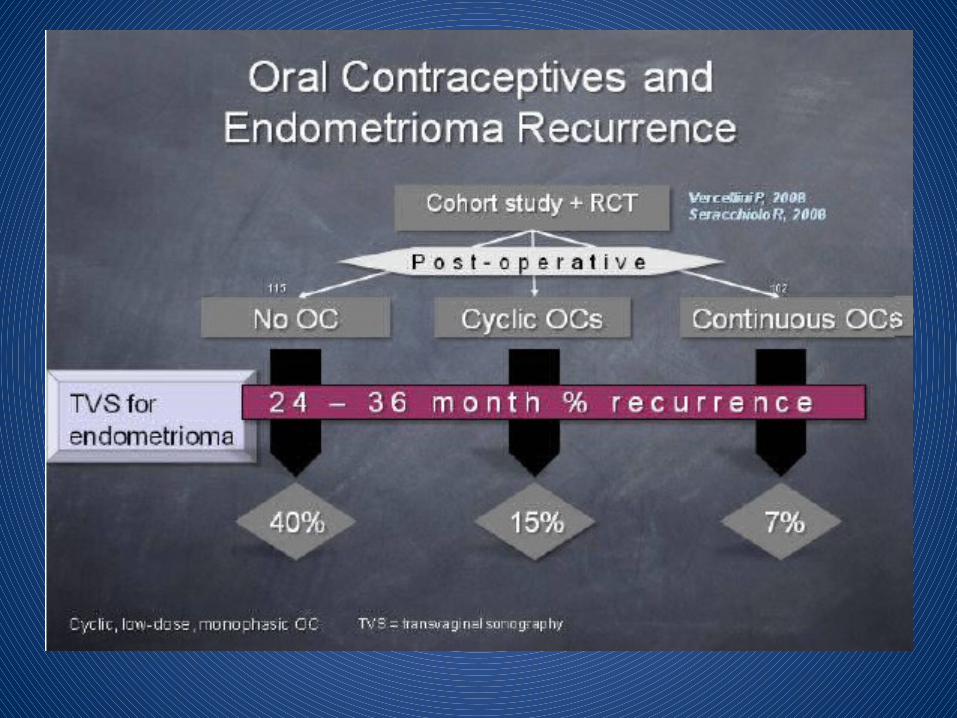
Deep endometriosis: Excisional surgeryPregnancy rates
Vercellini et al., Hum Reprod (2009)
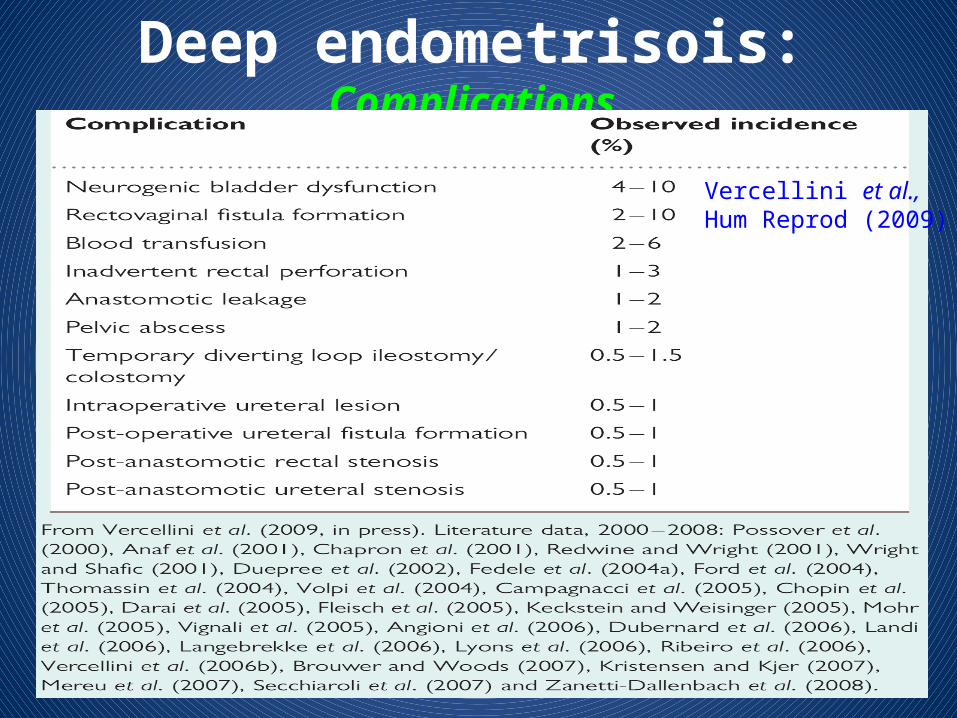
Deep endometrisois: Complications
Vercellini et al., Hum Reprod (2009)
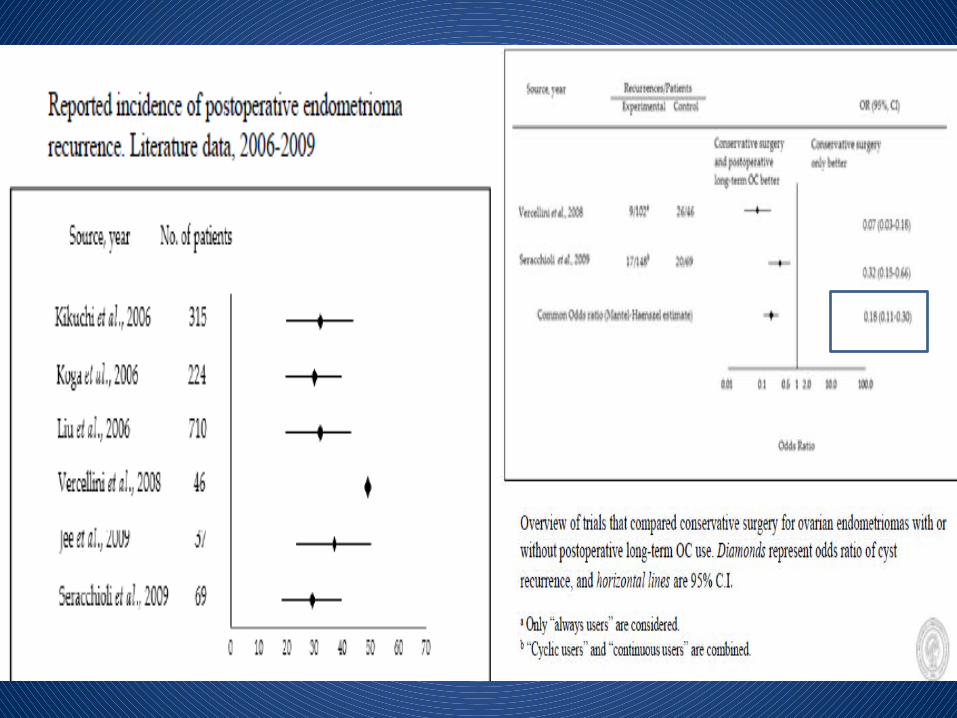
The reported recurrence rate was high, estimated as 21.5% at 2 years and 40-50% at 5 years.
Endometriosis – Higher Prevalence forOvarian Cancer
Review of an ovarian endometrioma cohort (6398) follow up of 17 years: 46 ovarian cancers
Standardized Incidence Ratio (SIR) 8.95
Independent predictors: age > 40 yearsendometrioma size > 9 cmslightly elevated CA-125
Kobayashi 2009, Int J Clin Oncol; 14: 378-382Ovarian cancer in endometriosis: epidemiology, natural history, and clinical diagnosis
Endometriosis – Higher Prevalence forOvarian Cancer
Review of an ovarian endometrioma cohort (6398) follow up of 17 years: 46 ovarian cancers
Standardized Incidence Ratio (SIR) 8.95
Independent predictors: age > 40 yearsendometrioma size > 9 cmslightly elevated CA-125
Kobayashi 2009, Int J Clin Oncol; 14: 378-382Ovarian cancer in endometriosis: epidemiology, natural history, and clinical diagnosis
Endometrioid and Clear Cell Ovarian Cancers – Risk Factors
Decreased risk: - Increasing parity- OC for => 5 years- breast feeding- tubal ligation
Increased risk: - endometriosis OR 2.2 endometrioid OR 3.0 clear cell
Nagle et al., 2008. Eur J Cancer; 44: 2477-2484Endometrioid and clear cell ovarian cancers: a comparative analysis of risk factors
Endometrioid and Clear Cell Ovarian Cancers – Risk Factors
Decreased risk: - Increasing parity- OC for => 5 years- breast feeding- tubal ligation
Increased risk: - endometriosis OR 2.2 endometrioid OR 3.0 clear cell
Nagle et al., 2008. Eur J Cancer; 44: 2477-2484Endometrioid and clear cell ovarian cancers: a comparative analysis of risk factors
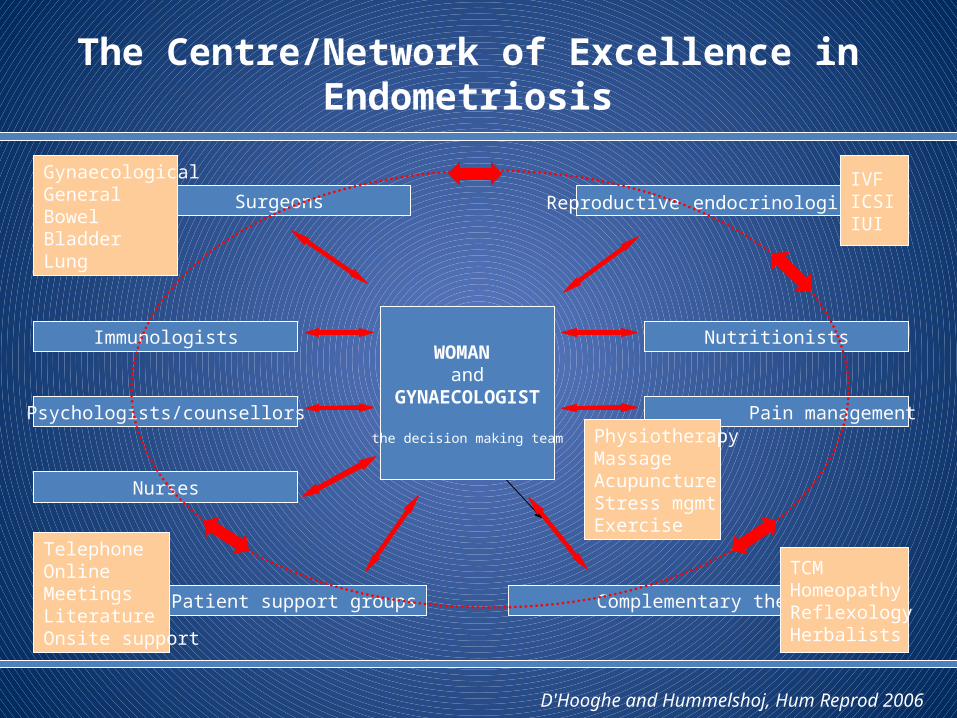
The Centre/Network of Excellence in Endometriosis
Surgeons Reproductive endocrinologists
Immunologists Nutritionists
Psychologists/counsellors Pain management
Patient support groups
Nurses
Complementary therapies
WOMAN and
GYNAECOLOGIST
the decision making team
TCMHomeopathyReflexologyHerbalists
TelephoneOnlineMeetingsLiteratureOnsite support
GynaecologicalGeneralBowelBladderLung
IVFICSIIUI
PhysiotherapyMassageAcupunctureStress mgmtExercise
D'Hooghe and Hummelshoj, Hum Reprod 2006


















