Endocrine Agents
53
-
Upload
mean-elepano -
Category
Documents
-
view
131 -
download
0
Transcript of Endocrine Agents



Growth Hormone (GH)2 Hormones Regulate GH 1. Growth hormone-releasing hormone (GN-RH) 2. Growth hormone-inhibiting hormone (GN-IH)
* NOT given orally given thru SQ or IM
* Can cause DM

Deficiency of GH
somatrem (Protropin)somatropin (Humatrope) – C/I for pedia patients
with growth deficiency due to Prader Willi syndrome, severely obese, severe respiratory impairment
Promotes bone growth at epiphyseal plates of long bones

Excess of GH
Gigantism – during childhoodAcromegaly – after puberty
* Due to GH hypersecretion or pituitary tumor
bromocriptine mesylate (Parlodel) – inhibits the release of GH from pituitary
octreotide (Sandostatin) – also used for severe diarrhea due to carcinoid tumor

Thyroid-Stimulating Hormone (TSH)Releases thyroxine (T4) and triiodothyronine (T3)
Excess TSH – HyperthyroidismDeficit TSH – Hypothyroidism. Maybe caused by
thyroid gland disorder (primary) or decrease in TSH secretion (secondary)
thyrotropin (Thyropar) – purified extract of TSH used to diagnose primary and secondary hypothyroidism

Adrenocorticotropic hormone (ACTH) Stimulates the release of the ff:
1. glucocorticoids (cortisol)2. mineralocorticoids (aldosterone)3. androgen* follows diurnal rythmn
corticotropin (Acthar) given IV or IM Agent in the diagnosis of adrenal gland disorder Used in the treatment of adrenal gland
insufficiency Suppresses inflammatory and immune response

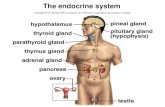
secretes Antidiuretic Hormone/Vasopressin AND Oxytocin
ADH promotes water reabsorptionADH deficit leads to Diabetes Insipidus
desmopressin (DDAVP – desmopressin acetate)vasopressin (Pitressin)Given intranasally or injection

Nursing ProcessAssessment:1. Determine urinary output and weight2. Assess for infectious process3. Compare child’s growth with standards
Diagnosis:Ineffective health maintenanceDelayed growth and development
Interventions:ADH Monitor V/S, increase HR, decrease systolic
pressure (hypovolemia)

ACTH Observe client’s weight for possible edema.
Side effect is sodium and water retention Taper dose Electrolyte monitoring
GH Monitor blood sugar and electrolyte levels
(possible hyperglycemia)

THYROID GLANDSThyroid hormones stimulate metabolism and cardiac
function, and are essential for normal growth and development of the nervous and musculoskeletal systems.
Hypothyroidism is the abnormally decreased secretion of thyroid hormone.

Caused by: Primary cause (thyroid gland disorder) Secondary cause (lack of TSH secretion)
Cretinism is hypothyroidism in infants.
Unless treated early, the infant will be short in stature and delayed in mental and physical development.

Myxedema is hypothyroidism in adults.
Manifestations: bradycardia, cold and dry skin, brittle hair, low
body temperature, fatigue, cold intolerance, flat affect, slowed cognition, and weight gain

Drug Therapy:
Levothyroxine (Synthroid, Levothroid), the most commonly used replacement
- used to treat simple goiter and chronic lymphocytic (Hashimoto) thyroiditis
Liothyronine (Cytomel), synthetic T3, useful in treating Myxedema Coma, better absorbed from GI, NOT for maintenance therapy

Liotrix (Euthroid, Thyrolar)Mixture of levothyroxine sodium and liothyronine
sodium in 4:1 ratio

Antithyroid Agents Hyperthyroidism is the abnormal increase secretion of thyroid hormone. Grave’s disease/thyrotoxicosis
- common Manifestations:
tachycardia, dysrhythmias, palpitations, excessive perspiration, heat intolerance, nervousness, irritability, exopthalmos, weight loss
*** can be treated by surgery

Thyroid crisis (or “storm”) characterized by hyperthermia, tachycardia, and profound weakness, behavioral changes
Drug Therapy: Thiourea derivatives (Thioamides) – drug of choice.
Blocks thyroid hormone2 thioamides:
propylthiouracil (PTU) - Inhibit peripheral conversion of T4 to T3methimazole (Tapazole) – 10 times more potent, with longer half-life

Iodide preparations have been used to suppress thyroid function for those who have undergone subtotal thyroidectomy.
strong iodine solution (Lugol’s solution, Potassium iodide solution)
SE: teeth discoloration

Nursing ProcessAssessment1. Assess serum T3, T4, and TSH levels
2. Drug history because of drug-drug interactions like oral anticoagulants, digoxin, insulin, oral hypoglycemics,
3. Assess for signs of thyroid crisis

Client health teaching:
For hypothyroidism-Take drug same time each day, pre-breakfast-To report signs of hyperthyroidism-Avoid foods that can inhibit thyroid
secretions(strawberry, peach, pear, cabbage, cauliflower, radish, peas)

For hyperthyroidism-Taken with meals-Avoid iodine and iodine-containing food, OTC
cough meds-Do not discontinue abruptly-Avoid the drugs if pregnant or breastfeeding

Parathyroid Glands
Parathyroid hormone (PTH) regulates calcium levels in the blood.
Decrease in serum calcium stimulates the release of PTHCalcitonin decreases serum calcium
PTH agents treat hypoparathyroidism Synthetic calcitonin is used for decreasing serum
calcium levels (hyperparathyroidism)

Hypoparathyroidism and Hypocalcemia Agentscalcitriol (Rocaltrol) – Increases serum calcium with
long onset of action.calcifediol (Calderol) – bone disease and
hypocalcemia associated with chronic renal disease and dialysis
Hyperparathyroidism and Hypercalcemia Agentscalcitonin (human) (Cibacalcin) – Paget’s diseasecalcitonin (salmon) (Calcimar)


Nursing Process
Assessment Assess for symptoms of tetany in hypocalcemia:
twitching of the mouth, tingling and numbness of the fingers, carpopedal and laryngeal and carpopedal spasm

Interventions1. Monitor serum Ca levels (reference is 8.5-
10.5 mg/dl)
2. Client teaching: Report signs of tetany and hypercalcemia
(bone pain, anorexia, N/V, thirst, constipation, lethargy, bradycardia, polyuria)
Check OTC drugs

Adrenal GlandsAdrenal cortex produces two hormones or
corticosteroids: glucocorticoids (cortisol) and mineralocorticoids (aldosterone)
It affects carbohydrate, protein and fat metabolism; Na retention and water reabsorption and K excretion; have antinflammatory, antiallergic, and anti-stress effects
Addison’s disease- decrease in corticosteroidCushing’s syndrome - increase in corticosteroid

Addison’s disease: weight loss, fatigue, hyperpigmentation, muscle weakness, low blood pressure


1. Glucocorticoids Short-acting cortisone acetate (Cortone Acetate) hydrocortisone (Cortef, Hydrocortone)
Intermediate-actingmethylprednisolone (Medrol, Solu-Medrol)prednisolone (Hydeltrasol) prednisone (Deltasone)

Long-actingbetamethasone (Celestone)dexamethasone (Decadron)
2. Glucocorticoid InhibitorsUsed in treating clients with Cushing’s syndrome
ketoconazole (Nizoral)aminogluthethimide (Cytadren)Mitotane (Lysodren) – ANTINEOPLASTIC hormone
antagonist

3. Mineralocorticoids (aldosterone)Secrete aldosterone that maintain fluid balance
fludrocortisone (Florinef) – oral mineralocorticoid

Nursing ProcessAssessment1. Monitor electrolyte (hypokalemia) ana blood sugar2. Obtain weight and urine outputInterventions1. Watch out for increase in BP2. Report weight gain of 5 lbs in several days3. Encourage foods high in potassium4. Taper the dose:5. Taken with meals

Blood glucose is regulated by insulin. Responsible for:
◦Facilitating the passage of glucose into cells for energy
◦Suppressing excess production of sugar in the liver and muscles
◦Suppressing the breakdown of fat for energy

ANTIDIABETIC AGENTS
Two Major Classes of Drugs: Insulins Oral Hypoglycemic Agents
These agents can be used as monotherapy in the treatment of type 2 diabetes
May be used in combination therapy with insulin in the treatment of type 1 diabetes

INSULINS INSULINS
Two Main Sources:Two Main Sources:Domesticated animals Domesticated animals Recombinant DNA technologyRecombinant DNA technology


Activity Classification Brand RAPID-ACTING Humalog
lisproSHORT-ACTING Humulin R,
regular
INTERMEDIATE-ACTINGNPH insulinHumulin NLente insulinHumulin L insulin

LONG-ACTING-Ultralente insulin-Lantus
CombinationsHumulin 70/30 – isophane NPH 70%, regular 30%Humulin 50/50 – isophane NPH 50%, regular 50%

InsulinTypes: Onset Peak DurationRapid-acting 5 min 0.5-1 hr 2-4 hrs
Short-acting 0.5-1 hr 2-4 hrs 6-8 hrs
Intermediate-acting 1-2 hrs 6-12 hrs 18-24 hrs
Long-acting 5-8 hrs 14-20 hrs 30-36 hrs
Premixed Insulin- 0.5 hour 4-8 hrs 22-24 hrs

Complications of Insulin Administration: Allergic reactions Insulin lipodystrophy(lipoatrophy, lipohypertrophy) Insulin resistance Somogyi and Dawn phenomenon
Easier Administration:Insulin pen injectorsInsulin pumpsInsulin jet injectors



Interventions:Avoid extremes in temperature when storing insulinBefore injection, insulin should be at room
temperatureInjection sites are abdomen, arms, thighs, and hipsDon’t use same site more than once in a 2- 3 week
period

Use a syringe with a matched calibration of units to the insulin concentration
1-2 week supply of insulin may be preparedRegular insulin firstREGULAR INSULIN THE ONLY ONE THAT CAN BE
GIVEN IV

Oral Antidiabetic Drugs
First and Second-Generation Sulfonylureas- Stimulate pancreatic beta cells to secrete more
insulin
First Generation1. Short-acting
tolbutamide (Orinase)2. Intermediate-acting
acetohexamide (Dymelor)tolazamide (Tolinase)

3. Long-actingchlorpropamide (Diabinese)
Second Generation- Increase tissue response to insulin, decrease
glucose production of the liverGlimepiride (Amaryl), glipizide (Glucotrol)

Non-Sulfonylureas
1. BIGUANIDES Reduces hepatic production of glucose by inhibiting
glycogenolysis; decreasing intestinal absorption of glucose; and improving lipid profile.
metformin (Glucophage)

2. ALPHA-GLUCOSIDASE INHIBITORS Inhibits alpha-glucosidase enzymes in the small
intestine and alpha-amylase in the pancreas. The result is reduced rate of glucose absorption postprandially.
acarbose (Precose)miglitol (Glyset)

3. THIAZOLIDINEDIONES Functions primarily by enhancing insulin action at
the receptor sites and decreases insulin resistance
rosiglitazone (Avandia)
4. MEGLITINIDE Also increases insulin secretion.
repaglinide (Prandin)nateglinide (Starlix)

5. Incretin Modifier Increase level of incretin hormones, increase
insulin secretion, decrease glucagon secretion to reduce glucose production
sitaglipitin phosphate (Januvia)

Nursing ProcessAssessment1. Note blood sugar levels2. Determine knowledge of DM and oral
antidiabeticsIntervention1. Teach symptoms of hypoglycemia2. Insulin might be needed during stress,
surgery, or serious infection3. No alcohol, no skipping/delaying meals

Hyperglycemic Agents
Glucagon – stimulates glycogen breakdown- Available parenteral use (SC, IM, IV)
diazoxide (Proglycem, Hyperstat)- inhibits insulin release- parenteral form