ENDLINE SURVEY FINAL REPORT SAVE THE CHILDREN, MALAWI ... · RAcE Endline Survey Final Report vi...
78
ENDLINE SURVEY FINAL REPORT SAVE THE CHILDREN, MALAWI Prepared by ICF and Save the Children for WHO Rapid Access Expansion (RAcE) Program MARCH 31, 2017 AUTHORS: Kirsten Zalisk, Tanya Gunther, Emmanuel Chimbalanga, Humphreys Nsona
Transcript of ENDLINE SURVEY FINAL REPORT SAVE THE CHILDREN, MALAWI ... · RAcE Endline Survey Final Report vi...

ENDLINE SURVEY
FINAL REPORT
SAVE THE
CHILDREN,
MALAWI
ENDLINE SURVEY
FINAL REPORT
SAVE THE
CHILDREN,
MALAWI
Prepared by ICF and Save the
Children for WHO Rapid Access
Expansion (RAcE) Program
MARCH 31, 2017
AUTHORS: Kirsten Zalisk, Tanya
Gunther, Emmanuel Chimbalanga,
Humphreys Nsona
pared by ICF and Save the Children
for WHO Rapid Access Expansion
(RAcE) Program
MARCH 31, 2017
AUTHORS: Kirsten Zalisk, Tanya
Gunther, Emmanuel Chimbalanga,
Humphreys Nsona

RAcE Endline Survey Final Report ii
ACKNOWLEDGEMENTS
ICF and Save the Children would like to thank the National Statistics Office and the Malawi Ministry of
Health for their contributions to this work. We would also like to thank the health surveillance
assistants (Malawi’s community health workers), who work hard to provide services to caregivers and
children in communities, and to the caregivers who give so much to ensure and improve the health of
their children. This work was made possible by the World Health Organization through funding by the
Canadian Government.

RAcE Endline Survey Final Report iii
TABLE OF CONTENTS
ABBREVIATIONS ............................................................................................................................................................. iv
EXECUTIVE SUMMARY .................................................................................................................................................. v
1 BACKGROUND .................................................................................................................................................... 11
1.1 RAcE Program Goals and Objectives ....................................................................................................... 11
1.2 Save the Children, Malawi Project Background ..................................................................................... 11
1.3 Endline Survey Objectives ........................................................................................................................... 14
2 SURVEY METHODS .............................................................................................................................................. 15
2.1 Survey Implementation and Partnership .................................................................................................. 15
2.2 Survey Design ................................................................................................................................................. 15
2.3 Survey Questionnaire ................................................................................................................................... 16
2.4 Selection and Training of Survey Staff ...................................................................................................... 17
2.5 Data Collection .............................................................................................................................................. 18
2.6 Data Entry and Management ...................................................................................................................... 18
2.7 Data Analysis .................................................................................................................................................. 19
2.8 Survey Indicators ........................................................................................................................................... 19
2.9 Survey Limitations ......................................................................................................................................... 19
3 FINDINGS ................................................................................................................................................................ 21
3.1 Characteristics of Sick Children and Caregivers ................................................................................... 21
3.2 Caregiver Knowledge and Their Perceptions of CCM-Trained HSAs ............................................. 23
3.3 Decision-Making ............................................................................................................................................ 25
3.4 Care-Seeking................................................................................................................................................... 26
3.5 Assessment ..................................................................................................................................................... 28
3.6 Treatment Coverage .................................................................................................................................... 30
3.7 First Dose of Treatment and Counseling from HSA ............................................................................ 32
3.8 Referral Adherence ....................................................................................................................................... 33
3.9 Sick Child Follow-Up .................................................................................................................................... 33
3.10 Illness Management and Diagnostics by Sex ........................................................................................... 34
4 DISCUSSION .......................................................................................................................................................... 35
Annex A. List of Key Persons Involved in the Survey............................................................................................. 39
Annex B. Endline Sample ............................................................................................................................................... 40
Annex C1. Endline Survey Household Questionnaire ............................................................................................ 45
Annex C2. Endline Survey HSA Questionnaire........................................................................................................ 46
Annex D. Training Schedule .......................................................................................................................................... 47
Annex E. Key Indicator Summary Tables for Sub-Areas ........................................................................................ 52
Annex F. Illness Management and Diagnostics by Sex Results Tables ................................................................ 62
Annex G. Supplementary 60 Cluster Results Tables .............................................................................................. 65
Annex H. Results of Endline HSA Survey .................................................................................................................. 74

RAcE Endline Survey Final Report iv
ABBREVIATIONS
ACT artemisinin-based combination therapy
CCM community case management
EA enumeration area
HSA health surveillance assistant
HTRA hard-to-reach area
iCCM integrated community case management
IMCI Integrated Management of Child Illnesses
MOH Ministry of Health
mRDT malaria rapid diagnostic test
NSO National Statistics Office
ORS oral rehydration solution
RAcE Rapid Access Expansion
WHO World Health Organization

RAcE Endline Survey Final Report v
EXECUTIVE SUMMARY
Since April 2013, Save the Children has been leading the implementation of the Rapid Access Expansion
(RAcE) program in Malawi, managing a consortium of organizations that includes D-tree International
and Medical Care Development International and working in close collaboration with the Ministry of
Health (MOH) Integrated Management of Childhood Illness (IMCI) unit, which is providing oversight.
The RAcE project began in four districts: Dedza, Mzimba North, Ntcheu, and Ntchisi. In 2014, the
project expanded geographically to include the districts of Likoma, Lilongwe Rural, Nkhatabay, and
Rumphi. The project helped to address challenges that the Malawi’s national integrated community case
management (iCCM) program faced, including supporting HSAs with supplies and supervision, expand
iCCM services to more communities, and update the iCCM protocol to align with World Health
Organization recommendations for management of fever and suspected pneumonia.
In August 2016, the National Statistics Office conducted the RAcE endline survey in the four original
project districts, with technical assistance from ICF and technical, logistical, administrative, and financial
support from Save the Children. We compared baseline and endline data to assess changes in sick child
care-seeking, assessment, and treatment coverage as well as caregivers’ knowledge of childhood illnesses
and perceptions of health surveillance assistant (HSA) services, and used the information to make
inferences about project accomplishments.
The survey results show that caregivers were less likely to be aware of a community case management
(CCM)-trained HSA in their community at endline compared to baseline (p<0.05), and perceptions of
the HSAs as trusted, convenient providers of high iCCM services also decreased from baseline to
endline (see Table 1, indicators 4, 5 and 7). Although these results could indicate that iCCM service
availability and quality deteriorated during the implementation of the RAcE project, the survey results
also show increases in indicators measuring HSAs as the first source of care for cases of cough with
difficult or fast breathing, malaria testing, and respiratory rate assessment over the course of the project.
More increases may not have been seen because the baseline survey was not a “true” pre-iCCM
baseline; more than 400 CCM-trained HSAs were already working in the project districts at the time of
the baseline survey. We, therefore, cannot expect to see increases over the course of the project that
might accompany the introduction of iCCM services. Furthermore, the survey results were likely diluted
because iCCM services were not available in all 60 clusters surveyed at endline. Many areas targeted for
iCCM at baseline, as RAcE was beginning, ultimately did not gain access to iCCM by the time of the
endline survey; only 33 (55 percent) of surveyed clusters had an active CCM-trained HSA present at
endline. Several HSA posts were vacant, and some district managers did not allow HSAs who were not
residents of their catchment areas to attend iCCM trainings and provide iCCM services. In addition, the
HSA survey revealed that only one-quarter of HSAs providing iCCM services met the strict definition of
functionality: being a resident in their catchment area and providing iCCM services at least five days per
week.
The survey data were explored further through sub-analyses of the 33 clusters confirmed to have an
active CCM-trained HSA and the 27 clusters confirmed not to have an active CCM-trained HSA at

RAcE Endline Survey Final Report vi
endline.1These sub-analyses show that at endline in the 33 clusters with an active iCCM HSA there were
higher levels of care-seeking from HSAs and more positive perceptions of services provided by HSAs
compared to the 27 clusters without an active iCCM HSA.
Despite iCCM being a mature program in Malawi, large service gaps remain due to the absence of fully
functional CCM-trained HSAs in eligible communities. Addressing HSA deployment issues, however, will
require dealing with issues beyond the control of the MOH IMCI unit, which does not manage the
broader HSA program. Implementation of the RAcE project in Malawi will soon be winding down, and
the MOH will continue to implement iCCM services on its own. The findings of the household and HSA
surveys highlight the importance of ensuring that HSAs are deployed in hard-to-reach areas and also that
they are available at their village clinics so that caregivers can access their services. Going forward, the
MOH IMCI unit and partners need to find ways to ensure the availability of HSAs at their village clinics
and maintain the quality of their services. They need to better understand why caregivers prefer seeking
care from providers other than HSAs when their children are sick. The findings also show that there are
some illness management patterns that need to be explored and better understood, including why HSAs
do not prescribe zinc more often and why HSAs and health facility staff are not using malaria diagnostic
tests more often to assess cases of fever.
Table 1. Summary of key indicators
Indicators highlighted in green had a statistically significant increase from baseline to endline, determined by a p-value of less than 0.05. Indicators highlighted in red had a statistically significant decrease from baseline to endline, determined by a p-value of less than 0.05.
Indicator Baseline Endline
% point change
p-value % (CI %) % (CI %)
Caregiver knowledge
1
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who are aware of the presence of the CCM-trained HSA in their community
90.0 (83.3 - 94.2)
83.4 (74.7 - 89.6)
-6.6 0.0355
2
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know the role of the CCM-trained HSA in their community
35.0 (29.6 - 40.9)
34.0 (28.7 - 39.7)
-1.0 0.7930
3
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know two or more signs of childhood illness that require immediate assessment by an appropriately trained provider
97.5 (96.1 - 98.4)
95.7 (93.5 - 97.1)
-1.8 0.0824
Caregiver perceptions of iCCM services
1 Confirmation was obtained through a mapping exercise that Save the Children conducted in January 2017.

RAcE Endline Survey Final Report vii
4
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who view CCM-trained HSAs as trusted health care providers
82.3 (77.5 - 86.2)
70.3 (62.8 - 76.8)
-12.0 0.0004
5
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who believe CCM-trained HSAs provide quality services
68.4 (63.7 - 72.7)
57.6 (52.3 - 62.7)
-10.8 0.0007
6
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who found the CCM-trained HSA at first visit
86.5 (79.3 - 91.5)
84.0 (78.2 - 88.4)
-2.5 0.5414
7
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who cite the CCM-trained HSA as a convenient source of treatment
59.6 (52.5 - 66.3)
47.3 (39.9 - 54.8)
-12.3 0.0045
Sick child care-seeking
8
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey for whom advice or treatment was sought from an appropriate provider
Overall 65.6
(60.7 - 70.1) 70.0
(65.4 - 74.2) 4.5 0.0740
Fever 70.3
(64.4 - 75.6) 73.9
(68.9 - 78.4) 3.6 0.2575
Diarrhea 64.0
(57.9 - 69.7) 69.8
(63.9 - 75.0) 5.8 0.1202
Cough with difficult or fast breathing 61.9
(55.5 - 67.9) 65.6
(59.8 - 71.1) 3.7 0.2465
9
Percentage of children age 2-59 months who were sick in two weeks preceding the survey taken to a CCM-trained HSA as first source of care
Overall 25.7
(20.2 - 32.1) 33.4
(27.1 - 40.3) 7.7 0.0278
Fever 26.4
(20.2 - 33.6) 34.0
(27.2 - 41.5) 7.6 0.0547
Diarrhea 30.8
(24.0 - 38.5) 37.5
(30.5 - 45.1) 6.7 0.0925
Cough with difficult or fast breathing 20.9
(15.5 - 27.5) 29.5
(23.2 - 36.6) 8.6 0.0246
Sick child assessment
10 Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had finger or heel stick
35.6 (30.0 - 41.7)
59.0 (53.7 - 64.2)
23.4 0.0000

RAcE Endline Survey Final Report viii
11
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had a finger or heel stick in the two weeks preceding the survey
96.9 (92.6 - 98.7)
97.3 (95.0 - 98.6)
0.4 0.7610
12
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing
25.6 (20.6 - 31.4)
38.5 (33.5 - 43.7)
12.8 0.0007
Sick child assessment by HSA
13
Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had a finger or heel stick by an HSA (among those who sought care from an HSA)
0 61.7
(52.7 - 70.0) 61.7 0.0000
14
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had a finger or heel stick by an HSA in the two weeks preceding the survey (among those who sought care from an HSA)
0* 98.4
(93.3 - 99.6) 98.4 na
15
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing by an HSA (among those who sought care from an HSA)
29.6 (21.0 - 40.0)
55.8 (46.0 - 65.1)
26.2 0.0003
Sick child treatment
16
Percentage of children age 2-59 months who have been sick in two weeks preceding the survey who received appropriate treatment
Overall 42.7
(38.2 - 47.2) 47.1
(43.3 - 51.0) 4.5 0.0720
Fever (ACT within 24 hours)* 61.9
(54.8 - 68.4) 59.2
(52.5 - 65.7) -2.6 0.5721
Diarrhea (ORS and zinc) 18.4
(13.8 - 24.1) 21.2
(16.9 - 26.3) 2.8 0.3976
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
53.3 (47.3 - 59.2)
61.8 (56.4 - 66.9)
8.5 0.0165
17
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received appropriate treatment from a CCM-trained HSA
Overall 13.9
(10.3 - 18.6) 16.6
(12.6 - 21.5) 2.7 0.3085

RAcE Endline Survey Final Report ix
Fever (ACT within 24 hours)* 29.3
(21.9 - 37.9) 24.8
(17.4 - 34.1) -4.5 0.3708
Diarrhea (ORS and zinc) 7.1
(4.3 - 11.6) 10.6
(7.2 - 15.4) 3.5 0.1828
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
12.0 (8.2 - 17.3)
17.4 (13.4 - 22.3)
5.4 0.0922
18
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received the first dose of treatment in the presence of an HSA
Overall 37.3
(27.4 - 48.4) 49.4
(41.9 - 56.8) 12.1 0.0531
Fever (ACT) 39.2
(29.6 - 49.7) 56.2
(45.1 - 66.7) 17.0 0.0209
Diarrhea (ORS and zinc) 23.1
(11.8 - 40.3) 22.0
(11.7 - 37.3) -1.1 0.9056
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
41.5 (25.0 - 60.2)
54.1 (43.9 - 64.0)
12.6 0.2539
19
Percentage of sick children age 2-59 months for whom their caregivers received counseling on how to provide the treatment(s) among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 100 97.8
(94.0 - 99.2) -2.2 0.1369
Fever (ACT) 100 99.1
(93.0 - 99.9) -1.0 0.4176
Diarrhea (ORS and zinc) 100 95.1
(81.7 - 98.8) -4.9 0.2467
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin) 100
97.7 (90.7 - 99.4)
-2.4 0.2751
Sick child referral and follow-up
20
Percentage of sick children age 2-59 who were referred in the two weeks preceding the survey whose caregiver adhered to referral advice
88.6 (77.6 - 94.6)
87.1 (80.0 - 92.0)
-1.5 0.7981
21
Percentage of sick children age 2-59 months receiving treatment from an HSA in the two weeks preceding the survey whose caregiver followed up with the HSA after the initial consultation
19.4 (13.8 - 26.6)
21.7 (17.1 - 27.1)
2.3 0.5028
na = not applicable; ORS=oral rehydration solution *Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs; confirmed malaria treatment at endline by HSAs; confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.

RAcE Endline Survey Final Report x

RAcE Endline Survey Final Report 11
1 BACKGROUND
1.1 RAcE Program Goals and Objectives
In 2013, the World Health Organization (WHO) launched the Rapid Access Expansion (RAcE) program
in five sub-Saharan African countries—Democratic Republic of Congo, Malawi, Mozambique, Niger, and
Nigeria. The goal of the program was to increase coverage of diagnostic, treatment, and referral services
for malaria, pneumonia, and diarrhea to decrease overall mortality and the number of severe cases
among children aged 2-59 months. The program would accomplish this goal through the following
objectives:
Catalyze the scale-up of integrated community case management (iCCM) as an integral part of
government-provided health services in sub-Saharan Africa.
Stimulate policy review and regulatory update in each country on disease case management.
Accelerate adaptation of supply management and surveillance systems to include services at the
community level.
This effort came at a time when there was great momentum for iCCM at the country level and a high
degree of interest among the global health community to understand how to best measure success and
how to build country ownership and capacity to sustain iCCM interventions.
1.2 Save the Children, Malawi Project Background
The under-five child mortality rate in Malawi has been decreasing steadily since 1992, from 234 deaths
per 1,000 live births in 1992 to 64 deaths per 1,000 live births in 2015.2 Despite this progress, large
numbers of children continue to die from conditions that are easily preventable and treatable. Malaria,
diarrhea, and pneumonia account for approximately half of the deaths among children aged
1-59 months.3 Pneumonia alone accounts for more than 13 percent of the deaths in hospitalized children
under 5 years of age.4
To address the issue of preventable deaths of children under five, the Government of Malawi started an
iCCM program through the Ministry of Health (MOH) Integrated Management of Childhood Illness
(IMCI) unit in 2008. Health surveillance assistants (HSAs) offer iCCM services at village clinics in hard-
to-reach areas (HTRAs). In a country where human resources for health care are in short supply, HSAs
often serve as the first line of defense against childhood illnesses.
HSAs are a community-based cadre who were meant to serve approximately 1,000 residents, but in
practice they often have much larger catchment areas of 2,000 residents or more. They are centrally
recruited and on the payroll of the MOH, but they are deployed to and stationed in the communities
2 UNICEF and World Health Organization. 2015. Countdown to 2015 maternal, newborn & child survival: A
decade of tracking progress for maternal, newborn and child survival—The 2015 report. Available at
http://www.countdown2015mnch.org/documents/2015Report/Countdown_to_2015_final_report.pdf. 3 WHO, Malawi neonatal and child health country profile. Available at
http://www.who.int/maternal_child_adolescent/epidemiology/profiles/neonatal_child/mwi.pdf. 4 Bjornstad, et al. Determining the quality of IMCI pneumonia care in Malawian children. 2014. Paedeatrics and
International Child Health, 34(1).

RAcE Endline Survey Final Report 12
that they serve. For supervision and support purposes, HSAs are attached to the nearest health facility.
HSAs are also expected to perform specific tasks at health facilities, such as HIV counseling,
administration of immunizations, and growth monitoring, among others.
HSAs initially provided iCCM services to communities in HTRAs located more than eight km from a
health facility. In 2013, the Government of Malawi changed the definition of HTRAs, decreasing the
distance to the nearest health facility from eight km to five km. The change in definition means that
communities located more than five km from a health facility are now eligible to receive iCCM services.
Since April 2013, RAcE has supported iCCM in four districts in Malawi: Dedza, Mzimba North, Ntcheu,
and Ntchisi. Save the Children is the lead implementing partner. It manages a consortium of
organizations that includes D-tree International and Medical Care Development International and works
in close collaboration with the MOH IMCI unit, which is providing oversight.
When RAcE started in 2013, HSAs trained in iCCM were already working in the four project districts.
Through RAcE, Save the Children is expanding iCCM coverage and strengthening iCCM implementation
in HTRAs of the project districts.
Within the project districts, Save the Children supports iCCM by training HSAs, HSA supervisors, and
HSA mentors; organizing community mobilization activities; and procuring and distributing key iCCM
commodities to village clinics. Save the Children also has staff members who serve as district
coordinators and work in close collaboration with the district health management team in each project
district. At the national level, the project has shared experiences and collaborated with other
organizations implementing iCCM activities, contributed to strategies such as the Child Health Strategy,
and helped improve iCCM data availability in DHIS2. Save the Children has also rolled out iCCM
interventions to align with changes in national policy. For example, it replaced cotrimoxazole with
amoxicillin after the MOH IMCI unit approved amoxicillin as the first-line treatment for cough with fast
breathing at the community level. It also moved from presumptive malaria treatment at village clinics to
having HSAs use malaria rapid diagnostic tests (mRDTs) to confirm that a child with fever needs
artemisinin-based combination therapy (ACT) treatment.
The project expanded geographically in 2014 to include the districts of Likoma, Lilongwe Rural,
Nkhatabay, and Rumphi. In 2014, Save the Children also introduced a community-based maternal and
newborn care component to the project in Ntcheu district.
As of September 2016, the project is supporting 810 HSAs, covering a total population of 2,298,981
across the 8 project districts, including 390,827 children under 5 years of age. Table 2 contains key
project implementation indicators as of September 2016.

RAcE Endline Survey Final Report 13
Table 2. Key project implementation indicators, September 2016
Indicator Value*
Target population**
Total population in HTRAs of the eight project districts 2,298,981
Under five population in HTRAs of the eight project districts 390,827
Training
Number of HSAs trained in iCCM 1,121
Number of HSA supervisors trained to support iCCM 364
Community treatment
Percentage of trained HSAs providing services 90%
(810/896)
Number of malaria cases treated by HSAs 136,295
Number of fast breathing cases treated by HSAs 54,736
Number of diarrhea cases treated by HSAs 33,532
HSA reporting and activity levels
Percentage of HSA monthly iCCM reports received 86%
(697/810)
Supervision
Percentage of HSA supervision visits completed 81%
(656/810)
Note: These indicators were extracted from Save the Children’s Year 4 Semiannual Narrative Report submitted to WHO on November 15, 2016.
* All reported percentages are averages of monthly data for the first two quarters of Save the Children’s fourth year of implementation. The numbers of cases treated are cumulative values for the first two quarters of Save the Children’s fourth year of implementation.
** According to Save the Children’s Year 1 Annual Report Annex 1, Project Context, in the four original project districts, the target area population is 1,189,741, including 190,359 children under 5 years of age.
The RAcE project had planned to train 1,356 HSAs across the targeted districts but did not reach these
targets primarily because of deployment issues related to the broader HSA program in Malawi, which is
managed by a unit other than the IMCI unit that implements the iCCM program. The Government of
Malawi last recruited HSAs in 2008. When the iCCM program was introduced, HSAs who already
existed in HTRAs were trained to implement iCCM services. Over time, the number of HSAs has
decreased due to several factors, including drop out, change of career, transfer, and death. Some HSAs
who were assigned HTRAs have since been promoted to senior HSAs and are based at facilities. In
other cases, targeted HSAs did not reside in their catchment areas, and the districts did not agree to
train them in iCCM unless they resided full-time in their catchment area. Because of this, there are
HTRAs eligible for iCCM that do not have access to iCCM services.
Save the Children, in collaboration with the National Statistics Office (NSO) and with technical support
from ICF, conducted the RAcE baseline household survey in September 2013 in the four original project
districts.

RAcE Endline Survey Final Report 14
1.3 Endline Survey Objectives
The objective of the RAcE endline household survey is to assess care-seeking behavior for sick children,
iCCM coverage, and caregiver knowledge, attitudes, and practices related to pneumonia, diarrhea, and
malaria in the RAcE Malawi intervention areas. We compared baseline and endline data to assess
changes in sick child care-seeking, assessment, and treatment coverage as well as caregivers’ knowledge
of childhood illnesses and perceptions of HSA services, and used the information to make inferences
about project accomplishments.

RAcE Endline Survey Final Report 15
2 SURVEY METHODS
2.1 Survey Implementation and Partnership
Save the Children conducted the RAcE endline survey in collaboration with NSO and with technical
assistance from ICF. NSO is experienced in implementing all aspects of large household surveys,
including enumerator recruitment, training, data collection, data entry, and analysis, and NSO also led
the baseline survey implementation for RAcE Malawi. NSO worked with Save the Children and ICF to
finalize the endline questionnaire; led the training of enumerators, data entry operators, and supervisors;
conducted data collection and data entry; and provided oversight to the entire implementation process.
The survey protocol received ethical approval from ICF’s Institutional Review Board and from Malawi’s
National Health Sciences Research Committee.
Annex A contains a complete list of the key people involved in the survey and their roles.
2.2 Survey Design
Household survey: This was a cross-sectional cluster-based household survey, targeting primary
caregivers of children aged 2–59 months who had recently been sick with diarrhea, fever, or cough with
difficult or fast breathing. All primary caregivers of children aged 2–59 months reported to have
experienced diarrhea, fever, or cough with fast breathing in the two weeks before the interview were
considered eligible for inclusion in the survey. ICF developed standardized sampling guidance for all
RAcE projects, which was adapted for Save the Children Malawi.
To be able to detect a 20 percent difference at 90 percent power with a two-tailed test and 95 percent
confidence using cluster sampling, 263 cases were needed for each disease. ICF rounded up to 300 cases
to ensure a consistent number of interviews per cluster and a slight increase in the precision of the
coverage estimates.
Save the Children Malawi used a 60 x15 multi-stage cluster sampling methodology. The entire RAcE
project area, iCCM-eligible areas—more than five km from a health facility—in the four original project
districts comprised the target population. The primary sampling units selected at the first stage were the
census enumerations areas (EAs) defined for the 2008 Malawi Population and Housing Census that were
eligible for iCCM (located at least five km from a health facility). EAs, which have an average of about
235 households, are the smallest operational areas established for the census with well-defined
boundaries. The listing of all EAs for each of the four study districts was obtained from NSO, and all EAs
located within five km of a health facility were excluded from the sampling frame. A total of 60 EAs were
randomly selected proportional to population size across the project districts. The same EAs, or
clusters, visited for the baseline survey were visited for the endline survey.
Within each cluster, interviewers visited all households to explain the nature and purpose of the endline
survey. Each visited household was assigned an identification number. The interviewers administered a
screening questionnaire to the household head or its nominated representative to establish the numbers
and ages of all usual members of the household and any lodgers or people who sleep there regularly to
identify the number of caregivers of children aged 2–59 months and number of children aged 2–59
months. If the interviewer was unable to make contact with a responsible adult in a household, or if the
household representative requested time to discuss participation in the interview, then the household

RAcE Endline Survey Final Report 16
was visited one more time before the household information was considered to be unobtainable. After
listing all the households, the team crossed out all ineligible households (those households with no
children under five who have been sick with diarrhea, fever, or cough with difficult or fast breathing in
the past two weeks before the survey).
The survey team then randomly selected 15 households to visit from that listing. They also selected a
backup group of 15 households to visit in case the survey team did not find the required number of
illness cases in the first group of 15. The survey team visited each selected household in the first group
of 15, even if all required cases of illness were attained before the fifteenth household.5 If after the first
15 households were visited, the survey team did not have 5 cases of diarrhea, fever, and cough with fast
breathing, the team went down the list of backup households that were also randomly selected from the
cluster household listing until 5 cases of that illness were found.
In each cluster, at least 5 interviews were conducted for each of the 3 illness modules—diarrhea, fever,
and fast breathing—for a total of at least 15 interviews per cluster, or 300 interviews per each illness
across the project area.
At each household, the interviewer first determined if an eligible child lived there. An eligible child was
aged 2–59 months and had been sick with diarrhea, fever, cough with fast breathing, or any combination
of the three illnesses in the two weeks preceding the survey.
If there was an eligible child in the household, the interviewer administered the questionnaire, including
all applicable illness modules, to the caregiver of the eligible child. If more than one child was eligible, and
they were sick with different illnesses, their caregiver was asked about each instance of illness. If there
was more than one eligible child in the household for an illness, the interviewer randomly selected one
of the eligible children and interviewed his or her caregiver. If there were multiple children selected for
inclusion in the survey, and the children had different primary caregivers, each primary caregiver of the
selected children was interviewed, but one of the caregivers was randomly selected to answer the
household asset questions.
The clusters included in the baseline and endline surveys are listed in Annex B.
HSA survey: As part of the endline survey, Save the Children conducted a survey of HSAs alongside the
household survey to assess the implementation strength and quality of iCCM services delivered by
HSAs. The objective of the HSA survey was to gain a better understanding of the HSAs’ background
characteristics, activity levels, and support and supervision received to help interpret the results of the
household survey. The HSAs serving the 60 clusters selected for the endline household survey formed
the sample population for the HSA survey. The EAs did not align perfectly with HSA catchment areas,
and in some cases more than one HSA was associated with a given cluster or the EA did not have any
community case management (CCM)-trained or active HSAs providing services. If a selected EA had
more than one HSA who was trained in CCM, only one HSA was randomly selected for the interview.
2.3 Survey Questionnaire
ICF developed a standard household questionnaire for all RAcE grantees to use for their baseline
surveys. Each grantee adjusted the questionnaire to fit the local iCCM program and country context. In
5 Otherwise, the sample will be biased toward households with more types of diseases.

RAcE Endline Survey Final Report 17
Malawi, Save the Children replaced the template terminology with the appropriate local terminology for
community health workers, care-seeking locations, and treatment options. The same questionnaire used
for the baseline survey was used at endline, with the addition of two questions to each illness module to
gather information about reasons caregivers did not seek care at all or did not seek care from an HSA.
The survey questionnaire contains seven modules: caregiver and household background information;
caregivers’ knowledge of iCCM activities in their community; caregivers’ knowledge of childhood illness
danger signs; household decision-making; and a module for each major childhood illness: fever, diarrhea,
and fast breathing. In addition to collecting information about caregiver knowledge, care-seeking, and
treatment coverage, the questionnaire collects standard Demographic and Health Survey data on
household ownership of selected assets, materials used for housing construction, and types of water
access and sanitation facilities, which ICF will analyze and use for the final evaluation.
The survey questionnaire was translated into the local language, Chichewa, by NSO and Save the
Children. The survey took approximately one hour to administer in each household, depending on the
number of modules to which each caregiver responded.
The household survey was pretested in communities that were not in the survey sample, in the local
language, during enumerator and supervisor training. A few minor adjustments were identified as
necessary to the questionnaire during field testing.
The HSA survey questionnaire was developed based on tools used in the previous iCCM program
funded by CIDA from 2009 to 2012. The questionnaire was translated to Chichewa by NSO and Save the
Children and pretested during the enumerator and supervisor training (same as the household survey
questionnaire). Trained enumerators administered the questionnaire to selected HSAs alongside the
household survey (when the team was in the selected EA).
Annex C1 contains the endline household survey questionnaire, and Annex C2 contains the HSA
questionnaire.
2.4 Selection and Training of Survey Staff
NSO recruited data collectors, supervisors, and data keyers. All survey staff were required to have a
Malawi Schools Certificate with at least a credit pass in English and mathematics. Most of the recruited
supervisors, enumerators, and data entry clerks were full-time NSO staff, and a number of them had
participated in the baseline survey.
Data collectors and supervisors received a 12-day training, which covered the following:
Overview of the RAcE project goals and activities
Review of how the data to be collected related to the project’s objectives
Review of the translated questionnaire and the questions and the topics covered by the
questionnaire, including consistency of the questions asked
Practice on the techniques of interviewing and the informed consent form
Practice on the techniques of collecting data from respondents
Overview of the roles of interviewers and supervisors
An ICF staff member provided in-person technical support during the second week of training. Two days
of the interviewer training session, day 4 and day 12, were devoted to field testing the translated

RAcE Endline Survey Final Report 18
questionnaire and informed consent form and practicing interviewing techniques. The areas selected for
field testing were not areas included in the survey. All interviewers were also trained on precautions and
avoidance of harm while in the field.
Annex D contains the survey training schedule.
2.5 Data Collection
Twenty-seven trained interviewers were divided into nine survey teams, each led by a supervisor. NSO
and Save the Children staff managed the day-to-day implementation of the survey. An ICF staff member
provided in-person technical support during the first week of data collection. Data were collected over
25 days, from August 5 to 29, 2016. There was not an official fieldwork schedule to include in this
report; teams were assigned a set of clusters and moved from cluster to cluster as they completed their
interviews. Each survey team was assigned approximately eight clusters, and each cluster took about
three days to complete.
Written informed consent was obtained for household interviews with primary caregivers of children
aged 2–59 months who had been sick with diarrhea or fever or cough with difficult or fast breathing in
the past two weeks in all study districts and for HSAs associated with the selected EA. Participation in
the study was voluntary, and there was no penalty for non-participation. Study respondents were not
compensated for their time away from income-earning activities or daily duties for participating in the
endline data collection.
Supervisors were responsible for ensuring that the survey team followed protocols throughout data
collection in the field. At the end of each day, supervisors in the field reviewed each completed
questionnaire and addressed any concerns or issues regarding the data quality. A quality assurance team
traveled among the clusters to ensure that data collection conformed to agreed-upon protocol and to
address any sampling issues. The quality assurance team also collected completed questionnaires from
the field and delivered them to the data entry supervisor.
2.6 Data Entry and Management
Data entry training took place over a five-day period after data collection was completed. Many of the
enumerators also served as keyers. Data entry took place over a month, from September 5 to
October 3. Data entry operators double-entered the survey data into a database using a CSPro tool
developed by ICF for the baseline and endline surveys. After two data entry operators entered the data
separately for a cluster, the data entry supervisor ran a quality check built into the CSPro tool to
compare the first and second entries for the cluster. If the check found any discrepancies, the data entry
operators used the paper questionnaires to verify the correct values and then resolved the
discrepancies using the CSPro tool. The supervisor again ran the quality check, and if it resulted in no
discrepancies, the data for the cluster were considered clean.
Names of participants were only collected for purposes of listing but were not used during any stage of
data analysis. Data entered could not be traced back to the individuals. Access to data was restricted to
authorized personnel only. After data for all clusters were entered and validated, NSO stripped the final
dataset of any identifying information and shared it with ICF for analysis.

RAcE Endline Survey Final Report 19
2.7 Data Analysis
ICF analyzed the survey data using Stata v14 and Microsoft Excel. The ICF analyst imported the endline
household CSPro data files into Stata and merged them into one file. The baseline data file was
appended to the endline data file, and the merged file was checked, cleaned, and coded for the analysis.
The ICF analyst calculated point estimates and 95 percent confidence intervals accounting for cluster
effects. To test for statistically significant changes between indicators at baseline and endline, a Pearson’s
chi-squared test was used for binary and categorical variables and regression for continuous variables.
Indicators with p-values less than 0.05 show a statistically significant change between baseline and
endline.
ICF conducted the initial analysis of the HSA survey and provided tables with point estimates and
95 percent confidence intervals for a set of indicators developed by Save the Children. Save the Children
reviewed the tables and conducted additional analyses as needed. The detailed results of the HSA survey
are included in Annex H.
2.8 Survey Indicators
The household survey collected 21 key indicators related to caregiver knowledge of HSAs and child
illnesses; caregiver perceptions of HSAs; and sick child care-seeking, assessment, treatment, referral
adherence, and follow-up. The survey also collected information on household and caregiver
characteristics and household decision-making.
The HSA survey collected 22 indicators related to HSA residency, functionality, medicine and
diagnostics availability, supervision, service availability and activity levels, recording completeness,
knowledge, and data display and use. The survey also collected information on HSA background
characteristics.
2.9 Survey Limitations
The survey provides estimates for the four original RAcE project districts as a whole; it is not powered
to provide district-specific estimates and does not include the four project expansion districts.
Furthermore, the endline survey included areas not receiving RAcE interventions, thus diluting the
changes measured over the project implementation period. The sampling frame was based on census
EAs, which do not align perfectly with iCCM-eligible areas, so some of the EAs included in the sampling
frame may have included areas not eligible for iCCM. Save the Children also noted that it was not able
to implement RAcE activities in all iCCM-eligible areas of the four original districts because several HSA
posts were vacant, and in some districts, the district managers did not allow HSAs who did not reside in
their catchment areas to be trained in iCCM and implement iCCM services. As a result, several of the
60 EAs included in the survey either did not have an active CCM-trained HSA providing services or had
an active CCM-trained HSA serving only a subset of the EA at the time of the endline survey.
Through a mapping exercise conducted after the survey, Save the Children confirmed that 33 of the 60
clusters had an active CCM-trained HSA at the time of the endline survey, but 27 clusters did not. Key
indicators for sub-analyses of the 33 clusters with an active CCM-trained HSA and the 27 clusters
without an active CCM-trained HSA are included in Annex E. Relevant results are also highlighted in the
discussion section of the narrative.

RAcE Endline Survey Final Report 20
During supervision of the endline data collection, the quality assurance team reported that the survey
attracted more interest than anticipated from communities. When community members noticed the
teams were only interviewing caregivers whose children were sick, some may have stated that their
child had recently been sick to participate even though the child had not been sick in the two weeks
prior to the survey. The quality assurance team was unsure how widespread the issue was, but they
dealt with the issue as soon as it was recognized. Via the WhatsApp group created for communication
with and among the data collection teams, they advised survey teams to intensify caregiver screening to
ensure only children who had been sick in the two weeks prior to the survey were included.
Lastly, there are known potential biases and limitations with the indicators that assess caregiver recall of
malaria diagnostic testing and coverage of appropriate treatment for children with fever and cough with
difficult or fast breathing. The potential biases and limitations of these indicators are further detailed in
the findings section.

RAcE Endline Survey Final Report 21
3 FINDINGS
3.1 Characteristics of Sick Children and Caregivers
As shown in Table 3, 807 children were included in the baseline survey, and 873 children were included
in the endline survey. Of the sick children included, approximately 46 percent had diarrhea and
60 percent had cough with difficult or fast breathing in the two weeks preceding the survey. At baseline,
approximately 60 percent had fever in the two weeks preceding the survey, but at endline slightly more
than 70 percent had fever in the same time period.
Approximately half of the children were male in both surveys, and their age breakdown by year was
consistent across the surveys as well, with the smallest percentage of children in the oldest age category
(48–59 months).
Among the children surveyed, the baseline survey had 455 cases of fever, 364 cases of diarrhea, and 441
cases of cough with difficult or fast breathing; the endline survey had 571 cases of fever, 387 cases of
diarrhea, and 489 cases of cough with difficult or fast breathing.
Table 3. Characteristics of sick children included in survey
Characteristic Baseline % (CI %)
Endline % (CI %)
Sex of sick children included in survey
Male, % 51.4
(47.7 - 55.2) 49.8
(46.7 - 52.9)
Female, % 48.6
(44.8 - 52.3) 50.2
(47.1 - 53.3)
Age (months) of sick children included in survey
2–11 months, % 22.1
(19.1 - 25.7) 22.1
(19.5 - 25.0)
12–23 months, % 24.7
(21.7 - 27.8) 24.6
(22.1 - 27.3)
24–35 months, % 22.7
(19.9 - 25.7) 20.3
(17.5 - 23.4)
36–47 months, % 17.2
(14.9 - 19.9) 20.3
(17.5 - 23.4)
48–59 months, % 13.3
(10.7 - 16.3) 14.8
(12.6 - 17.3)
Two-week history of illness of children included in survey
Had fever, % 59.9
(56.4 - 63.2) 70.7
(66.9 - 74.2)
Had diarrhea, % 46.5
(43.7 - 49.2) 46.1
(43.3 - 48.9)
Had cough with difficult or fast breathing, % 58.5
(55.4 - 61.6) 60.0
(56.6 - 63.3)
Average number of illnesses, N 1.6 1.8
Total number of sick children included in survey 807 873
Cases of illness included in survey Fever, N 455 571 Diarrhea, N 364 387 Cough with difficult or fast breathing, N 441 489
Total number of sick child cases included in survey 1,260 1,447

RAcE Endline Survey Final Report 22
At baseline, 720 primary caregivers of sick children were interviewed, and at endline, 783 primary
caregivers of sick children interviewed. As shown in Table 4, the mean age and highest education level of
the caregivers were similar in the surveys. A larger percentage of caregivers were married at the time of
the baseline survey (85 percent) than at the time of the endline survey (75 percent); however, the
percentage of caregivers either married or living with a partner as if married was similar in both surveys.
Table 4. Caregiver characteristics
Characteristic Baseline % (CI%)
Endline % (CI%)
Age (years)
15–24 35.8
(32.7 - 39.1) 40.2
(36.4 - 44.2)
25–34 44.3
(40.6 - 48.1) 40.0
(36.7 - 43.4)
35–44 15.6
(13.3 - 18.1) 15.7
(13.2 - 18.6)
45–76 4.3
(2.9 - 6.4) 4.1
(2.7 - 6.2) Mean age (years) 28.6 years 28.3 years
Highest level of education
None 14.4
(11.1 - 18.6) 12.1
(9.5 - 15.4)
Primary, ≤ year 4 32.2
(28.4 - 36.3) 36.0
(31.8 - 40.5)
Primary, ≥ year 5 43.5
(38.6 - 48.5) 39.1
(34.3 - 44.1)
Secondary or higher 9.9
(7.6 - 12.7) 12.8
(10.2 - 15.8)
Marital status
Currently married 84.9
(81.1 - 88.0) 75.4
(71.4 - 78.9)
Not married but living with partner 3.8
(2.2 - 6.4) 9.2
(6.4 - 13.1)
Not in union 11.4
(8.9 - 14.5) 15.5
(13.1 - 18.1)
Partner living with caregiver (among those in union)*
Yes 88.6
(85.2 - 91.2) 89.0
(86.1 - 91.3)
Total number of caregivers 720 783
*638 caregivers in a union at baseline, and 662 caregivers in a union at endline
On average, caregivers reported that they lived 10.5 km from the nearest health facility at baseline and
9.4 km from the nearest health facility at endline (see Table 5). Interestingly, at both baseline and
endline, approximately 10 percent of caregivers reported that they lived fewer than 5 km from the
nearest health facility, which means that they lived in areas that were not classified as hard-to-reach and
therefore technically did not live in areas that qualified for iCCM services, although they may have still
accessed iCCM services.
The majority of caregivers reported walking to the health facility in both surveys, with most stating that
it took more than an hour to reach the nearest health facility. On average, it took caregivers
approximately two hours to reach the nearest health facility in at both baseline and endline.

RAcE Endline Survey Final Report 23
Table 5. Reported distance and mode of transport to nearest health facility
Travel to nearest facility Baseline Endline
% (CI%) % (CI%)
Distance to nearest facility
< 5 km
9.0 (4.8 - 16.4)
13.0 (7.9 - 20.5)
5-9 km
20.6 (15.1 - 27.4)
50.1 (41.2 - 58.9)
10-14 km
46.5 (38.9 - 54.2)
22.0 (15.7 - 29.8)
15-19 km
17.8 (12.6 - 24.5)
6.9 (4.5 - 10.6)
>= 20 km
6.2 (3.6 – 10.1)
8.1 (4.5 – 14.2)
Mean distance to nearest facility 10.5 km 9.4 km Number of caregivers 719 779
Mode of transport
Walk 78.8
(72.8 - 83.7) 70.5
(63.7 - 76.4)
Motorbike/taxi/bus 17.0
(12.7 - 22.4) 23.0
(17.8 - 29.2)
Other 4.2
(1.7 - 9.9) 6.5
(3.4 - 12.2) Number of caregivers 716 782
Time to nearest facility (among those who go to the facility)
< 30 minutes
5.5 (3.0 - 9.7)
3.3 (1.7 - 6.3)
30 – 59 minutes
5.6 (3.4 - 9.0)
12.4 (8.9 - 17.1)
1 – < 2 hours
24.1 (19.1 - 30.0)
34.3 (28.2 - 41.1)
2 – < 3 hours
43.6 (37.3 - 50.1)
23.9 (20.5 - 27.8)
3 hours or more
21.3 (15.5 - 28.6)
26.0 (19.7 - 33.5)
Mean time to nearest facility
1 hour 58 minutes
1 hour 59 minutes
Total number of caregivers 714 781
3.2 Caregiver Knowledge and Their Perceptions of CCM-Trained
HSAs
Caregiver knowledge of childhood illnesses was high at baseline and remained high at endline, as shown
by the indicators in Table 6. Among the illness signs that caregivers stated as reasons to seek treatment
for their child, fever was the most commonly mentioned (approximately 95 percent at baseline and
88 percent at endline). Diarrhea with dehydration (approximately 45 percent in both surveys) and child
vomits everything (approximately 42 percent in both surveys) were the two next most common
responses. A complete list of child illness signs included in the survey questionnaires and responses that
caregivers gave is included in Annex G, Table G1.

RAcE Endline Survey Final Report 24
Table 6. Caregiver knowledge of childhood illnesses
Caregiver knowledge Baseline Endline
p-value % (CI %) % (CI %)
Knows 2+ child illness signs 97.5
(96.1 - 98.4) 95.7
(93.5 - 97.1) 0.0824
Knows 3+ child illness signs 73.8
(69.3 - 77.7) 75.6
(70.9 - 79.8) 0.5506
Knows cause of malaria 90.7
(86.9 - 93.5) 86.0
(82.6 - 88.7) 0.0461
Knows fever is a sign of malaria 85.7
(82.9 - 88.1) 88.4
(85.3 - 90.9) 0.1845
Knows malaria treatment 90.1
(87.0 - 92.6) 95.3
(93.5 - 96.6) 0.0002
Total number of caregivers 720 783
As shown in Table 7, the percentage of caregivers who knew that a CCM-trained HSA worked in their
community decreased from 90 percent at baseline to 83 percent at endline (p<0.05). At both baseline
and endline, approximately one-third of caregivers could name at least two curative services that HSAs
offered, with the most common service being to provide treatment for malaria (39 percent at baseline
and 32 percent at endline). A complete listing of HSA activities included in the survey questionnaires and
responses that caregivers gave is included in Annex G, Table G2.
Table 7. Caregiver knowledge of HSA
Caregiver knowledge Baseline Endline
p-value % (CI %) % (CI %)
Knows CCM-trained HSA works in community 90.0
(83.3 - 94.2) 83.4
(74.7 - 89.6) 0.0355
Total number of caregivers 720 783
Knows location of HSA* 93.4
(87.8 - 96.5) 93.6
(86.2 - 97.1) 0.9523
Knows 2+ HSA curative services* 35.0
(29.6 - 40.9) 34.0
(28.7 - 39.7) 0.7930
Total number of caregivers 648 653
*Only asked of caregivers who stated that there was a CCM-trained HSA in their community
Among caregivers who knew that a CCM-trained HSA worked in their community, perceptions of HSAs
as trusted, convenient health care providers of quality services decreased between the baseline and
endline surveys (see Table 8). The reasons for these decreases are unclear. At baseline, HSAs treated
malaria presumptively, meaning that any child presenting with fever received ACT, whereas at endline
HSAs tested children with fever using mRDTs before administering ACT. If HSAs did not have mRDTs
in stock, the child was supposed to be referred to a health center (even if the HSA had ACTs in stock).
It is possible that these shifts in the treatment protocol may have contributed to the perception of
lower-quality services by caregivers who had become used to presumptive treatment.

RAcE Endline Survey Final Report 25
Table 8. Caregiver perceptions of CCM-trained HSAs
Caregiver perceptions Baseline Endline
p-value % (CI %) % (CI %)
View CCM-trained HSAs as trusted health care providers 82.3
(77.5 - 86.2) 70.3
(62.8 - 76.8) 0.0004
Believe CCM-trained HSAs provide quality services 68.4
(63.7 - 72.7) 57.6
(52.3 - 62.7) 0.0007
Cite the CCM-trained HSA as a convenient source of treatment 59.6
(52.5 - 66.3) 47.3
(39.9 - 54.8) 0.0045
Found the CCM-trained HSA at first visit (for all instances of care-seeking included in survey)*
86.5 (79.3 - 91.5)
84.0 (78.2 - 88.4)
0.5414
Total number of caregivers 648 653 * Denominator is 230 caregivers at baseline and 312 caregivers at endline—only those who sought care from an HSA for at least one sick child are included.
3.3 Decision-Making
Among caregivers who were married or living with a partner as if married, there were increases in joint
decision-making indicators over the course of the project (see Table 9). At baseline, 10 percent of
caregivers reported that they decided how to use household income jointly with their partner, and at
endline 39 percent of caregivers reported doing so (p<0.001). Also at baseline, 21 percent of caregivers
reported that they decided when to seek healthcare outside of the home jointly with their partner, and
at endline, 44 percent of caregivers reported doing so (p<0.001). Although joint household-level
decision-making increased over the project implementation period, the percentage of sick child cases for
which the decision to seek care was made jointly by the children’s caregiver and their partner did not
change. Table 10 shows that for nearly half (47 percent) of all sick child cases, caregivers reported that
they made the decision to seek care for their sick child jointly with their partner at baseline. This was
consistent among all three iCCM illnesses, and the percentages at endline were similar.
Table 9. Usual decision-maker in household around income and care-seeking
Decision-maker
Income decisions
p-value
Care-seeking decisions
p-value Baseline Endline Baseline Endline % (CI%) % (CI%) % (CI%) % (CI%)
Caregiver 16.6
(13.5 - 20.3) 11.9
(9.2 - 15.4) 43.8
(38.9 - 48.8) 32.9
(28.0 - 38.1) Caregiver’s husband or partner
72.1 (67.9 - 76.0)
47.1 (41.6 - 52.8)
35.6 (31.1 - 40.3)
23.3 (19.2 - 27.9)
Caregiver and partner jointly
10.0 (7.6 - 13.1)
39.4 (34.0 - 45.1)
0.0000 20.6
(17.2 - 24.5) 43.8
(38.4 - 49.4) 0.0000
Other 1.3
(0.6 - 2.7) 1.5
(0.7 - 3.2) 0.0 0.0
Total number of caregivers
638 662
635 657

RAcE Endline Survey Final Report 26
Table 10. Joint decision-making to seek care for sick child
Illness Baseline Endline
p-value Baseline
N Endline
N % (CI %) % (CI %)
Overall 47.3
(42.5 - 52.1) 46.4
(41.0 - 52.0) 0.8063 1,115 1,223
Fever 48.6
(42.8 - 54.5) 47.9
(41.4 - 54.5) 0.8569 401 486
Diarrhea 46.0
(39.5 - 52.6) 44.1
(37.7 - 50.8) 0.6601 322 324
Cough with difficult or fast breathing 46.9
(41.6 - 52.3) 46.5
(40.4 - 52.7) 0.9102 392 413
3.4 Care-Seeking
Care-seeking from an appropriate provider (hospital, health center, health post, nongovernmental
organization center, or HSA) increased slightly between baseline and endline, but the change was not
statistically significant (see Table 11). However, the percentage of sick child cases in which caregivers
sought care first from an HSA increased significantly between baseline (26 percent) and endline (33
percent) (p<0.05). The increases across the three illnesses were consistent—approximately 7 to 9
percentage points—although only the increase for care-seeking for cases of cough with difficult or fast
breathing was statistically significant (p<0.05).
Table 11. Care-seeking behavior among all sick child cases
Illness
Sought care from appropriate provider*
p-value
HSA was first source of care
p-value Baseline
N Endline
N Baseline Endline Baseline Endline
% (CI %) % (CI %) % (CI %) % (CI %)
Overall 65.6
(60.7 - 70.1) 70.0
(65.4 - 74.2) 0.0740
25.7 (20.2 - 32.1)
33.4 (27.1 - 40.3)
0.0278 1,260 1,447
Fever 70.3
(64.4 - 75.6) 73.9
(68.9 - 78.4) 0.2575
26.4 (20.2 - 33.6)
34.0 (27.2 - 41.5)
0.0547 455 571
Diarrhea 64.0
(57.9 - 69.7) 69.8
(63.9 - 75.0) 0.1202
30.8 (24.0 - 38.5)
37.5 (30.5 - 45.1)
0.0925 364 387
Cough with difficult or fast breathing
61.9 (55.5 - 67.9)
65.6 (59.8 - 71.1)
0.2465 20.9
(15.5 - 27.5) 29.5
(23.2 - 36.6) 0.0246 441 489
* Appropriate providers included hospital, health center, health post, nongovernmental organization center, and HSA
Among cases of illness for which caregivers sought any care, those who went to an HSA first increased
significantly between baseline and endline for all three illnesses (see Table 12), with increases ranging
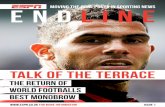
from 10 to almost 12 percentage points. Figure 1 shows where care was sought for sick child cases in
which any care was sought. Traditional practitioners and “other” sources were omitted from the figure
because when combined they accounted for less than 5 percent of responses for both source of care
and first source of care. The figure highlights the increase in care-seeking from HSAs at endline and
corresponding decreases in care-seeking from public facilities and stores/pharmacies.

RAcE Endline Survey Final Report 27
Table 12. Care-seeking behavior among those who sought any care
Illness
HSA was first source of care among those who sought any care
p-value Baseline
N Endline
N Baseline Endline
% (CI %) % (CI %)
Overall 30.1
(23.7 - 37.4) 40.5
(33.2 - 48.2) 0.0123 1,076 1,194
Fever 29.3
(22.5 - 37.2) 39.2
(31.6 - 47.4) 0.0290 409 495
Diarrhea 38.6
(30.3 - 47.7) 48.5
(40.0 - 57.1) 0.0362 290 299
Cough with difficult or fast breathing
24.4 (18.2 - 31.9)
36.0 (28.6 - 44.2)
0.0114 377 400
Figure 1. Care-seeking sources among those who sought care
As shown in Table 13, the percentage of illness cases in which caregivers did not seek care for their sick
child did not significantly change from baseline (14.6 percent) to endline (17.5 percent). At endline, the
most commonly cited reason for not seeking any care6 was that the caregiver did not believe that the
illness was serious (30 percent). The two other most common responses were that caregivers did not
have money (21 percent) or could treat the condition at home or with medicines already on hand (22
percent). Other responses included 15 percent who said that the place of care was too far, 13 percent
who said that the condition passed, and 7 percent who said that they did not have the time. Annex G,
Table G3, contains a complete list of reasons caregivers did not seek care from any source.
The percentage of illness cases in which caregivers sought care but sought care from a source other
than an HSA decreased between baseline (68 percent overall) and endline (59 percent overall) (p<0.05).
This almost 10 percentage point decrease may be primarily explained to the significant increase in care-
seeking from an HSA for cases of cough with difficult or fast breathing (see Table 13). Among those who
6 This question was only included in the endline survey; caregivers were allowed to give multiple responses.
45
8
3225
43
12
41
17
39
5
3023
35
9
41
15
Public facility Private clinic HSA Store, pharmacy ormarket
Per
cen
tage
of
sick
ch
ild c
ases
Source of care - baseline Source of care - endline
First source - baseline First source - endline

RAcE Endline Survey Final Report 28
sought care but did not go to an HSA at endline,7 the majority (80 percent) stated that they preferred to
go to another provider. The next most common reasons cited were that the HSA was not available (18
percent) and that the HSA was too far away (5 percent). Few caregivers indicated that they thought the
condition was too serious (3 percent), that the HSA did not have medicines or supplies (1 percent), or
that they did not trust the HSA to provide care (1 percent). Annex G, Table G4, contains a complete
list of reasons caregivers did not seek care from any source.
Table 13. Did not seek care or sought care from sources other than HSA
Illness
Did not seek care Sought care but not
from HSA
Baseline % (CI %)
Endline % (CI %)
p-value Baseline % (CI %)
Endline % (CI %)
p-value
Overall 14.6
(11.9 - 17.8) 17.5
(14.9 - 20.4) 0.0874
68.3 (60.8 - 75.0)
59.1 (51.3 - 66.4)
0.0277
Fever 10.1
(7.3 - 13.9) 13.3
(10.4 - 17.0) 0.1668
69.2 (61.0 - 76.3)
60.4 (52.1 - 68.2)
0.0524
Diarrhea 20.3
(15.7 - 25.9) 22.7
(18.5 - 27.6) 0.4947
59.7 (50.7 - 68.1)
51.2 (42.6 - 59.7)
0.0752
Cough with difficult or fast breathing
14.5 (10.8 - 19.3)
18.2 (15.0 - 21.9)
0.0844 74.0
(65.8 - 80.8) 63.3
(54.9 - 70.8) 0.0266
Total number of sick child cases
1,260 1,447 1,076 1,194
3.5 Assessment
The percentage of fever cases in which blood was taken for testing increased significantly between
baseline and endline, both among all fever cases and among fever cases managed by an HSA at a village
clinic (see Table 14). mRDTs were not available for HSAs to use at village clinics at the time of the
baseline survey; at baseline, cases of fever received presumptive malaria treatment. mRDTs were
gradually rolled out as part of the iCCM program in the RAcE project districts in 2014 and 2015. Thus
among cases managed by an HSAs at a village clinics at baseline, none of the 126 fever cases for which
care was sought from an HSA had blood drawn. At endline, approximately 60 percent of fever cases
were tested, both by any provider and by HSAs at village clinics. It is important to note, though, that
studies have shown caregiver recall of malaria diagnostic testing to be poor, so the assessment
indicators should be interpreted with caution.8
Although the percentage of fever cases tested for malaria improved between baseline and endline, about
40 percent of cases managed by HSAs at endline did not receive an mRDT. The HSA survey results
show that most HSAs had mRDTs in stock at the time of the survey (89 percent) and that stockouts of
mRDTs in the previous month was also not a large issue (13 percent HSAs had stockout of mRDTs)
(see Annex H), suggesting that mRDT stockouts is only part of the explanation for the relatively low
percentage of cases of fever tested.
When a malaria diagnostic test was given at endline, in most cases (approximately 97 percent),
caregivers received the result of the blood test from the provider, and approximately three-quarters of
the test results were reported to be positive for malaria. Among fever cases that had a positive test
7 This question was only included in the endline survey; caregivers were allowed to give multiple responses. 8 The Maternal and Child Health Integrated Program. 2013. Indicator Guide: Monitoring and Evaluating Integrated
Community Case Management.

RAcE Endline Survey Final Report 29
result at endline, the majority received ACT (92 percent overall and 90 percent of cases managed by
HSAs).
Although HSAs are not supposed to provide ACTs to children aged 2–4 months with fever, they are
supposed to administer an mRDT and refer to a health facility. Among the 14 fever cases in which care
was sought from an HSA for children aged 2–4 months at endline, 6 caregivers reported that their child
had blood drawn. Of these, 5 caregivers received the result of the test, and all 4 fever cases that tested
positive for malaria received ACT from the HSA. In addition, one fever case for a child under five
months who did not have blood taken received ACT from an HSA. Neither of the two fever cases
among children aged 2–4 months for which care was sought from an HSA at baseline were referred to a
health facility by the HSA, and only 1 of 12 fever cases among children aged 2–4 months was referred at
endline.
Table 14. Malaria assessment among children with fever
Fever assessment
Cases managed by HSA at village clinic
p-value All cases
p-value Baseline Endline Baseline Endline
% (CI %) % (CI %) % (CI %) % (CI %)
Child had blood drawn* 0 61.7
(52.7 - 70.0) 0.0000
35.6 (30.0 - 41.7)
59.0 (53.7 - 64.2)
0.0000
Caregiver received result of blood test
na 98.4
(93.3 - 99.6) na
96.9 (92.6 - 98.7)
97.3 (95.0 - 98.6)
0.7610
Blood test positive for malaria na 79.8
(70.6 - 86.7) na
77.7 (69.9 - 84.0)
74.4 (69.1 - 79.1)
0.4020
Received ACT among those who had a positive blood test result
na 89.5
(79.8 - 94.8) na
84.4 (77.0 - 89.8)
92.2 (87.7 - 95.2)
0.0365
Total number of fever cases 126 196 455 571 na = not applicable *For cases in which child had blood drawn among cases managed by HSA, only cases in which the caregiver reported the test being done by an HSA at the village clinic were included in the numerator. Three caregivers reported that their children had blood taken by an HSA at a village clinic in the baseline survey, but Save the Children Malawi confirmed that this was not possible because malaria blood tests were not available at that time.
Among cases of cough with difficult or fast breathing, there was a statistically significant increase in the
percentage that had their respiratory rate assessed comparing baseline to endline, both among all cases
and among cases managed by an HSA at a village clinic (p<0.001) (see Table 15). The overall increase in
assessment of respiratory rate by any provider was driven by the large increase respiratory rate
assessment by HSAs. At baseline, 27 percent of cases of cough with difficult or fast breathing that had
their respiratory rate assessed had it done at by an HSA at a village clinic, and over the course of the
project this increased to 45 percent. Conversely, the percentage of cases that had their respiratory rate
assessed at a government hospital decreased, from 62 percent at baseline to 46 percent at endline.
Annex G contains tables with the location (Table G5) and provider (Table G6) of sick child assessments.

RAcE Endline Survey Final Report 30
Table 15. Fast breathing assessment
Respiratory rate assessment
Cases managed by HSA at village clinic
p-value All cases
p-value Baseline Endline Baseline Endline % (CI %) % (CI %) % (CI %) % (CI %)
Respiratory rate assessed 31.0
(22.4 - 41.2) 56.1
(46.4 - 65.4) 0.0004
25.6 (20.6 - 31.4)
38.5 (33.5 - 43.7)
0.0007
Total number of cough with difficult or fast breathing cases
100 148 441 489
3.6 Treatment Coverage
Appropriate treatment for fever is defined as receiving ACT the same day or day after the fever started
among children aged 5–59 months who had a positive malaria diagnostic test result for treatment
provided by all providers at endline and by all providers except HSAs at baseline. At baseline,
presumptive malaria treatment by an HSA was considered appropriate because that was the policy at
the time. According to national iCCM policy, HSAs can give children aged 2–4 months with fever an
mRDT, but they are supposed to refer them to a health facility for treatment. Appropriate treatment
for diarrhea was considered receiving both ORS and zinc, and appropriate treatment for cough with
difficult or fast breathing was considered receiving cotrimoxazole at baseline and amoxicillin at endline.
As with the fever assessment indicators, the appropriate treatment coverage indicators should be
interpreted with caution. The overall and fever indicators include confirmed malaria cases, and as stated
in the assessment section, caregiver recall of malaria diagnostic testing has been shown to be poor. In
addition, the HSA protocol for malaria treatment at endline was different from that at baseline.
Furthermore, pneumonia treatment, for which the cough with difficult or fast breathing appropriate
treatment indicator is a proxy, is globally recognized to have validity issues because diagnosis of
presumptive pneumonia is often inaccurate in comparison with a clinical diagnosis of pneumonia at
health facilities.9 Therefore, the number of cases of cough with difficult or fast breathing is likely an
overestimate of actual clinical pneumonia cases, and the percentage of these treated with amoxicillin
can, and should, reasonably not be 100 percent.
As shown in Table 16, among all sick child cases, appropriate treatment coverage did not change
significantly from baseline (43 percent) to endline (47 percent). Likewise, appropriate treatment
coverage of diarrhea cases and fever cases did not change over the course of the project, but
appropriate treatment of cases of cough with difficult or fast breathing increased significantly, from 53
percent at baseline to 62 percent at endline (p<0.05). The small non-significant decreases in the
appropriate fever treatment indicators may be related to the introduction of mRDTs, which impacted
the measurement of all appropriate fever treatment indicators as well as the overall appropriate
treatment indicators. Among cases of illness for which care was sought from an HSA, there were not
9 Campbell H, el Arifeen S, Hazir T, O'Kelly J, Bryce J, Rudan I, et al. 2013. Measuring coverage in MNCH:
Challenges in monitoring the proportion of young children with pneumonia who receive antibiotic treatment. PLoS
Med, 10(5): e1001421. doi:10.1371/journal.pmed.1001421

RAcE Endline Survey Final Report 31
any statistically significant increases in appropriate treatment coverage by an HSA when comparing
baseline to endline (see Table 17).
Table 16. Appropriate treatment coverage among all sick child cases
Illness (treatment)
Received appropriate treatment from HSA p-
value
Received appropriate treatment p-
value Baseline
N Endline
N Baseline Endline Baseline Endline % (CI %) % (CI %) % (CI %) % (CI %)
Overall 13.9
(10.3 - 18.6) 16.6
(12.6 - 21.5) 0.3085
42.7 (38.2 - 47.2)
47.1 (43.3 - 51.0)
0.0720 1,020 1,114
Fever (ACT same or next day)*
29.3 (21.9 - 37.9)
24.8 (17.4 - 34.1)
0.3708 61.9
(54.8 - 68.4) 59.2
(52.5 - 65.7) 0.5721 215 238
Diarrhea (ORS and zinc)
7.1 (4.3 - 11.6)
10.6 (7.2 - 15.4)
0.1828 18.4
(13.8 - 24.1) 21.2
(16.9 - 26.3) 0.3976 364 387
Cough with difficult or fast breathing (cotrimoxazole/ amoxicillin)
12.0 (8.2 - 17.3)
17.4 (13.4 - 22.3)
0.0922 53.3
(47.3 - 59.2) 61.8
(56.4 - 66.9) 0.0165 441 489
*Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs, confirmed malaria treatment at endline by HSAs, confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.
Table 17. Appropriate treatment coverage among those who sought care from an HSA
Illness (treatment) Baseline Endline
p-value Baseline N Endline N % (CI %) % (CI %)
Overall 46.1
(39.2 - 53.2) 45.9
(39.8 - 52.1) 0.9635 308 401
Fever (ACT same or next day) * 67.7
(58.1 - 76.1) 54.6
(43.7 - 65.1) 0.0679 93 108
Diarrhea (ORS and zinc) 22.2
(14.1 - 33.3) 27.4
(20.0 - 36.3) 0.4207 117 146
Cough with difficult or fast breathing (cotrimoxazole/amoxicillin)
54.1 (41.2 - 66.5)
57.8 (50.8 - 64.5)
0.6284 98 147
*Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs, confirmed malaria treatment at endline by HSAs, confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.
In addition to treatment with ORS and zinc, diarrhea cases should receive continued fluids and feeding
during the illness, and HSAs and other health providers are trained to counsel providers accordingly.
Among cases of diarrhea, approximately 50 percent were offered the same amount or more to drink,
and approximately 35 percent were offered the same amount or more to eat at both baseline and
endline (see Annex G, Table G7).
Because the iCCM fever assessment and malaria treatment protocol changed with the introduction of
mRDTs, additional analyses were conducted to look at treatment with ACT when malaria diagnostic
test results were reported to be positive and reported to be negative, and also when no diagnostic test
was given. These are not standard indicators, and have validity issues including poor caregiver recall as
described above. These results are provided in Annex G, Table G8.

RAcE Endline Survey Final Report 32
Annex G also includes tables that detail treatments taken for diarrhea (Table G9), fever (Table G10),
and cough with difficult or fast breathing (Table G11) and source of ACT (Table G12), ORS (Table
G13), zinc (Table G14), and cotrimoxazole/amoxicillin (Table G15).
3.7 First Dose of Treatment and Counseling from HSA
As shown in Table 18, there was not a significant increase in the percentage of cases of illness provided
the first dose of treatment in presence of an HSA, but the increase in cases of fever provided the first
dose of treatment in presence of an HSA was statistically significant (p<0.05).
Table 18. First dose of treatment in presence of HSA
Illness (treatment)
First dose received in presence of HSA
p-value Baseline
N Endline
N Baseline Endline % (CI %) % (CI %)
Overall* 37.3
(27.4 - 48.4) 49.4
(41.9 - 56.8) 0.0531 153 231
Fever (ACT)** 39.2
(29.6 - 49.7) 56.2
(45.1 - 66.7) 0.0209 74 105
Diarrhea (ORS) 31.7
(24.9 - 39.4) 32.5
(23.6 - 42.8) 0.8937 101 117
Diarrhea (zinc) 36.7
(21.3 - 55.3) 27.9
(16.6 - 43.0) 0.3805 30 43
Diarrhea (ORS and zinc)*** 23.1
(11.8 - 40.3) 22.0
(11.7 - 37.3) 0.9056 26 41
Cough with difficult or fast breathing (cotrimoxazole/amoxicillin)
41.5 (25.0 - 60.2)
54.1 (43.9 - 64.0)
0.2539 53 85
* Overall calculation includes confirmed malaria (ACT), diarrhea (ORS and zinc), and cough with difficult or fast breathing (cotrimoxazole/amoxicillin) ** Baseline includes presumptive treatment, which was the policy at the time *** Includes only cases in which child received both ORS and zinc
As shown in Table 19, among sick child cases that received treatment from an HSA, all caregivers
received counseling on how to administer the medicine to their children from the HSA at baseline, and
almost all (97 percent) of caregivers received this counseling at endline.
Table 19. Counseling on treatment administration by HSA
Illness (treatment)
Counseled on treatment administration
p-value Baseline
N Endline
N Baseline Endline % (CI %) % (CI %)
Overall* 100 97.8
(94.0 - 99.2) 0.1369 153 231
Fever (ACT)** 100 99.1
(93.0 - 99.9) 0.4176 74 105
Diarrhea (ORS) 98.0
(86.8 - 99.7) 99.2
(94.0 - 99.9) 0.5384 101 117
Diarrhea (zinc) 100 95.4
(82.5 - 98.9) 0.2234 30 43
Diarrhea (ORS and zinc)*** 100 95.1
(81.7 - 98.8) 0.2467 26 41
Cough with difficult or fast breathing (cotrimoxazole/amoxicillin)
100 97.7
(90.7 - 99.4) 0.2751 53 85
* Overall calculation includes confirmed malaria (ACT), diarrhea (ORS and zinc), and cough with difficult or fast breathing (cotrimoxazole/amoxicillin) ** Baseline includes presumptive treatment, which was the policy at the time *** Includes only cases in which child received both ORS and zinc

RAcE Endline Survey Final Report 33
3.8 Referral Adherence
Among sick child cases for which care was sought from an HSA, 79 of 340 cases of illness were referred
to a health facility by an HSA at baseline (23 percent), and 101 of 489 cases of illness were referred to a
health facility by an HSA at endline (21 percent). Of those referred, there was no change in referral
adherence over the project implementation period; approximately 88 percent adhered to the referral
advice at both baseline and endline (see Table 20).
Table 20. Caregiver adherence to HSA referral
Illness Baseline Endline
p-value Baseline
N Endline
N % (CI %) % (CI %)
Overall 88.6
(77.6 - 94.6) 87.1
(80.0 - 92.0) 0.7981 79 101
Fever 93.1
(74.5 - 98.4) 80.0
(67.8 - 88.4) 0.1431 29 40
Diarrhea 87.1
(64.0 - 96.2) 92.6
(73.9 - 98.2) 0.5320 31 27
Cough with difficult or fast breathing
84.2 (58.2 - 95.3)
91.2 (75.6 - 97.2)
0.4568 19 34
At baseline, the most common reason that caregivers cited for not adhering to the HSA’s referral was
that the child improved (78 percent of sick child cases). At endline, the most common reasons that
caregivers cited for not adhering to the HSA’s referral were that the child improved (46 percent of sick
child cases) and that they did not have money (31 percent of sick child cases). Annex G, Table G16,
contains a complete list of reasons caregivers did not adhere to the HSA’s referral.
3.9 Sick Child Follow-Up
According to the national iCCM protocol, HSAs are to encourage caregivers to return for follow-up
within three days after the initial consultation. Among sick child cases for which care was sought from an
HSA, approximately 22 percent returned to the HSA for a follow-up visit after the initial sick child
consultation at baseline and endline (see Table 21). Thus there was no change over the project
implementation period. It is important to note that the children included in the survey were sick
sometime during the two weeks preceding the caregiver’s interview, so they may not have yet returned
for follow-up by the time of the survey.
Of those sick child cases taken for follow-up with an HSA at baseline, most followed up three days after
the initial consultation (35 percent); otherwise the timing of the visits varied from one day to more than
five days after the initial consultation. At endline, children were most commonly taken for follow-up two
days (31 percent) or three days (25 percent) after the initial consultation. Annex G, Table G17, contains
a complete list of when follow-up visits occurred.
Table 21. Sick child follow-up
Illness Baseline Endline
p-value Baseline N Endline N % (CI %) % (CI %)
Overall 21.6
(15.2 - 29.8) 22.7
(16.8 - 29.9) 0.7784 236 309
Fever 20.6
(14.3 - 28.8) 19.9
(15.3 - 25.4) 0.8419 126 196
Diarrhea 20.7
(13.7 - 30.0) 23.3
(17.0 - 31.0) 0.6044 116 146

RAcE Endline Survey Final Report 34
Cough with fast breathing 16.3
(10.1 - 25.4) 22.5
(16.0 - 30.5) 0.1977 98 147
3.10 Illness Management and Diagnostics by Sex
Endline data for care-seeking and treatment of fever, diarrhea, and cough with difficult or fast breathing
were disaggregated by sex. The following four results showed statistically significant differences between
males (boys) and females (girls):
Caregivers were more likely to seek any care for girls with diarrhea (81 percent) than for boys with
diarrhea (74 percent) (p<0.05).
Caregivers were more likely to seek care from an appropriate provider for girls with fever
(77 percent) than for boys with fever (71 percent) (p<0.05).
Girls with fever were more likely to have their blood taken to test for malaria (62 percent) than
boys with fever (56 percent) (p<0.05).
Boys with a positive malaria diagnostic test result were more likely to receive ACT the same day or
day after the onset of fever (65 percent), compared to girls with a positive malaria diagnostic test
result (54 percent) (p<0.05).
The complete sex-disaggregated result tables can be found in Annex F.

RAcE Endline Survey Final Report 35
4 DISCUSSION
When RAcE started in 2013, iCCM was already well-established across Malawi. As of September 2011,
3,296 HSAs had completed iCCM training from an estimated 3,452 HTRAs targeted for iCCM by the
MOH.10 However, the MOH-led program faced challenges supporting HSAs with supplies and
supervision, and there was a need to expand iCCM services to more communities and to update the
iCCM protocol to align with WHO recommendations for management of fever and suspected
pneumonia. The RAcE project supported this expansion by training additional HSAs in iCCM who were
located in areas between five and eight km from a health facility. RAcE also supported the MOH to
introduce mRDTs at village clinics and to replace cotrimoxazole with amoxicillin as first-line treatment
for pneumonia.
The 2016 RAcE endline survey results show significant increases in indicators measuring HSAs as the
first source of care for cases of cough with difficult or fast breathing, malaria testing, and respiratory
rate assessment over the course of the project. The baseline survey, however, was not a “true”
pre-iCCM baseline; more than 400 CCM-trained HSAs were already working in the project districts at
the time of the baseline survey, so we cannot expect to see increases that might accompany the
introduction of iCCM services over the course of the project. Furthermore, the survey results were
likely diluted because iCCM services were not available in all 60 clusters surveyed at endline. Save the
Children was unable to implement RAcE activities in all HTRAs of their project districts as initially
planned because several HSA posts were vacant, and some district managers did not allow HSAs who
were not residents of their catchment areas to attend iCCM trainings or to provide iCCM services.
Therefore, the endline survey data were explored further through sub-analyses of the 33 clusters
confirmed to have an active CCM-trained HSA (referred to as active clusters) and the 27 clusters
confirmed not to have an active CCM-trained HSA at endline (referred to as inactive clusters).11
The survey results show that caregiver perceptions of HSAs as trusted sources of care and providers of
high-quality care decreased over the course of the project. However, in the 33 active clusters, the
endline results were similar to the baseline results, indicating that there was no change in the
perceptions of HSAs as trusted sources of care and providers of high-quality services over the project
implementation period. It follows that the presence of a CCM-trained HSA in a community is related to
perceptions of trust in HSAs, but it is a topic worth investigating further to understand what factors are
contributing to the lowered confidence in the quality of care provided by HSAs. The HSA survey results,
for example, indicate that iCCM services are not regularly available in many areas where HSAs trained in
iCCM work. Although most HSAs interviewed (94 percent) met the MOH definition for functionality
(providing iCCM services in last month and providing iCCM at least two days per week), only
26 percent were providing regular iCCM services (residing in their catchment areas, providing iCCM
services in the last month, and providing iCCM services at least 5 days per week). Across the full survey
sample (including areas known not to have an active CCM-trained HSA), only 20 percent of clusters had
10 Nsona et al. 2012. Scaling up integrated community case management of childhood illness: Update from Malawi.
Am. J. Trop. Med. Hyg., 87(Suppl 5), 54–60. 11 Confirmation was obtained through a mapping exercise that Save the Children conducted in January 2017.

RAcE Endline Survey Final Report 36
access to a resident HSA providing iCCM at least 5 days per week, and 70 percent had access to an
HSA providing iCCM at least 2 days per week (see Annex H for details).
Care-seeking from an appropriate provider did not change over the course of the project among all
cases of illness (approximately 70 percent at both baseline and endline), with 41 percent of cases seeking
care from an HSA at endline (55 percent in active clusters, 23 percent in inactive clusters). Among cases
of illness for which care was sought, but not from an HSA, 80 percent of caregivers reported a
preference for another provider. This finding is consistent across the full survey sample and sub-analyses
of active and inactive clusters. The reasons why caregivers prefer providers other than HSAs require
further exploration.
The percentage of cases for which caregivers sought care from an HSA first among those who sought
any care increased significantly for all three iCCM illnesses (p<0.05). At endline, HSAs were the first
source of care for 41 percent of cases of illness for which care was sought (54 percent in active clusters,
23 percent in inactive clusters), indicating that if caregivers sought care from an HSA, the HSA was
almost always the first source of care.
In terms of illness assessment, survey results show improvements in the assessment of fever cases for
malaria and of cough with difficult or fast breathing cases for high respiratory rate for age. The
percentage of fever cases that were tested for malaria nearly doubled over the course of the project,
from 36 percent at baseline to 59 percent at endline for all fever cases, with HSAs performing more
than a third of all tests (37 percent). The majority of caregivers received the results of the test, and
nearly all fever cases that tested positive for malaria received ACTs at endline (89 percent).
The protocol for fever management changed during the project implementation period with the
introduction of mRDTs, and thus appropriate fever treatment was different at endline than it was at
baseline, which makes interpretation of this indicator difficult. On the whole, however, results suggest
improved management of fever cases, with statistically significant increases from baseline to endline in
the percentage of fever cases tested for malaria and the percentage of mRDT-positive fever cases that
received ACTs, as well as significant reductions in the percentage of mRDT-negative fever cases that
received ACTs (see Annex G, Table G8).
Although the use of mRDTs increased between baseline and endline, presumptive treatment of malaria
by all providers was still reported at endline. At endline, about 30 percent of all fever cases for which
care was sought and 38 percent of fever cases managed by HSAs did not have a malaria diagnostic test
performed. Among fever cases managed by HSAs but not tested using an mRDT, 26 percent still
received ACTs. Results of the HSA survey showed that 89 percent of HSAs had mRDTs in stock at the
time of interview, and 87 percent had not experienced a stockout of mRDTs in the month before the
survey, suggesting that stockouts of mRDTs were likely not the reason for presumptive treatment. It is
possible that HSAs may have felt pressure to provide ACT treatment for fever from caregivers as was
done under the old iCCM protocol. Limitations of caregiver recall may also contribute to this finding.
The percentage of cases of cough with difficult or fast breathing that had their respiratory rate assessed
increased significantly, from 26 percent at baseline to 39 percent at endline for all cases (p<0.001), and
from 30 percent at baseline to 56 percent at endline for cases managed by HSAs (p<0.001).
Furthermore, of cases of cough with difficult or fast breathing that received cotrimoxazole or amoxicillin
from an HSA, 45 percent had their respiratory rate assessed by an HSA at baseline, and 60 percent had
their respiratory rate assessed by an HSA at endline. The endline percentage is positive sign, because

RAcE Endline Survey Final Report 37
respiratory rate assessment by HSAs was a focus of the project, but this should be interpreted with
caution because of the small sample size (53 cases at baseline and 85 cases at endline).
Appropriate treatment coverage of sick child cases increased but not significantly from baseline to
endline for all cases and for cases managed by HSAs. Overall, appropriate treatment of sick child cases
by HSAs is low; 17 percent of all sick child cases received appropriate treatment from an HSA at
endline. Sub-analyses show appropriate treatment from an HSA was, as expected, higher in active iCCM
clusters (23 percent) and lower (only 9 percent) in clusters where HSAs were not providing iCCM
services. These findings indicate that, where active, HSAs provide a larger percentage of total
appropriate treatment. Among those that sought care from an HSA, approximately 45 percent reported
receiving appropriate treatment from the HSA. These findings were consistent across both the active
and inactive clusters.
Appropriate treatment coverage for diarrhea (5 percent at baseline and 7 percent at endline) continues
to lag far behind the treatment for other illnesses targeted by iCCM. Provision of zinc was the limiting
factor in providing appropriate treatment, and many more cases of diarrhea received ORS regardless of
source of care. Although caregivers reported that their child received ORS in approximately 70 percent
of diarrhea cases, the percentage of caregivers who reported that their child received zinc was much
lower (only 21 percent of diarrhea cases at baseline and 24 percent of diarrhea cases at endline). The
HSA survey shows that most HSAs had zinc in stock at the time of the survey (83 percent) and few
reported stockouts in the month before the survey (19 percent). The reasons for low provision of zinc
by HSAs are unclear, but Save the Children Malawi staff noted that HSAs and health facility staff may not
consider zinc an essential drug for treatment of diarrhea; providers seem to give zinc as a supplement
and not necessarily as treatment. HSAs, therefore, likely do not prioritize giving zinc when treating
children with diarrhea. Further follow-up with HSAs, health facility staff, and community members would
be helpful to better understand the barriers to appropriate treatment for diarrhea.
Among fever cases managed by HSAs, the survey results show an improvement in the provision of the
first dose of ACT in the presence of an HSA (p<0.05), and counseling on treatment administration
remained high (at or close to 100 percent) for all three illnesses. Caregiver adherence to HSA referrals
and follow-up after an initial HSA consultation did not change over the course of the project. Adherence
to referrals made by HSAs was high at both baseline and endline, with caregivers reporting completing
referrals as recommended in more than 85 percent of cases. In contrast, at both baseline and endline,
less than 25 percent of caregivers returned to HSAs for follow-up as recommended in the national
iCCM protocol.
Many areas targeted for iCCM at baseline, as RAcE was beginning, ultimately did not gain access to
iCCM by the time of the endline survey; only 33 (55 percent) of surveyed clusters had an active
CCM-trained HSA present. Furthermore, the HSA survey revealed that only a quarter of HSAs
providing iCCM services met the strict definition of functionality: being a resident in their catchment
areas and providing iCCM at least five days per week. Sub-analysis of the 33 clusters with active
CCM-trained HSAs showed higher levels of care-seeking from HSAs and more positive perceptions of
services provided by HSAs, compared to the 27 clusters without active CCM-trained HSAs at the time
of the endline survey. Addressing these HSA deployment issues, however, will require dealing with
issues beyond the control of the MOH IMCI unit, which does not manage the broader HSA program.

RAcE Endline Survey Final Report 38
Despite iCCM being a mature program in Malawi, large service gaps remain due to the absence of fully
functional CCM-trained HSAs in eligible communities. Implementation of the RAcE project in Malawi will
soon be winding down, and the MOH will continue to implement iCCM services on its own. The
findings of the household and HSA surveys highlight the importance of ensuring that HSAs are deployed
in HTRAs, that they are trained in iCCM, and also that they are available at their village clinics so that
caregivers can access their services. Going forward, the MOH and partners need to find ways to ensure
the availability of HSAs at their village clinics and maintain the quality of their services. They need to
better understand why caregivers prefer seeking care from providers other than HSAs when their
children are sick. The findings also show that there are some illness management patterns that need to
be explored and better understood, including why HSAs do not prescribe zinc more often and why
HSAs and health facility staff are not using malaria diagnostic tests more often to assess cases of fever.

RAcE Endline Survey Final Report 39
ANNEX A. LIST OF KEY PERSONS INVOLVED IN THE SURVEY
Name Organization Role
1. Emmanuel Chimbalanga Save the Children Malawi Survey coordinator
2. George Kasawala Save the Children Malawi RAcE project manager
3. Gomezgani Jenda Save the Children Malawi RAcE senior child health advisor
4. Enoce Nyanda Save the Children Malawi Data collector trainer and field work supervisor
5. Humphreys Nsona MOH, IMCI Provider of overall leadership
6. Fannie Kachale MOH, RHD Provider of technical input on community-based maternal and newborn care survey component
7. Tiope Mleme NSO Data collection coordinator
8. Lewis Gombwa NSO Data quality assurance coordinator and data entry lead
9. Kirsten Zalisk ICF Provider of remote technical support
10. Lwendo Moonzwe ICF Provider of in-country technical support
11. Debra Prosnitz ICF RAcE project manager

RAcE Endline Survey Final Report 40
ANNEX B. ENDLINE SAMPLE
The table in this annex contains the endline survey clusters, along with the district, traditional authority,
enumeration area and villages associated with each – as well as the number of households listed in each
cluster. The iCCM implementation status of the cluster is listed in the last column. The status
sometimes varies by village within a cluster; if the status is the same for the entire cluster, it list listed
once, but if the status varies, it is listed for each village. Implementation status is defined as follows:
Yes: there is an active CCM-trained HSA
No – Vacant: there is not an active CCM-trained HSA, and the HSA post is vacant
No – HSA: there is not an active CCM-trained HSA, but there is an HSA
Yes but transferred: there was an active CCM-trained HSA, likely within the past year but had been
transferred by the time of the endline survey
The same clusters were used in the baseline survey but the number of households listed in each cluster
and the implementation status of the cluster may have been different at the time of the baseline survey.
Table B1. Endline survey cluster information
District Traditional Authority
EA Cluster Villages Households Listed
Implementation status
Mzimba TA Mtwalo 3 1 Mwelekete Wankhama Kumwenda
145 Yes
Mzimba TA Mtwalo 31 2 Jacob Chakuluntha Kalama Estate N’dili Nthembe ya Mwana
266 Yes but transferred
Mzimba TA Mtwalo 48 3 Saulosi Mofat Shadreck Makwakwa
176 Yes but transferred
Mzimba TA Mtwalo 51 4 Longwe Residence Makhetani Singini Mkopeka Khowoya Msekeni Nkabelani Yesaya Chinombo Jere
278 No – Vacant
Mzimba TA Mtwalo 67 5 Bich Moyo Jalani Khongolo Paulosi Khongolo
230 No – Vacant
Mzimba TA Mtwalo 95 6 Kabindula Nkhonjera Mabwanya Liche Muntwani Hara Nyandolo Ziba Safari Ziga Tembo
149 Yes
Mzimba TA Mtwalo 100 7 David Sibande Mateyu Ng’oma Muhlolo Ndolo
131 Yes
Mzimba TA Mpherembe 21 8 Chiminyira Bota Kalema Estate Mtambalika Nkhawanawo Estate Wombe Bota
204 Yes

RAcE Endline Survey Final Report 41
District Traditional Authority
EA Cluster Villages Households Listed
Implementation status
Mzimba TA Mpherembe 38 9 Chauluma Nyirenda Chibula Mandhlopa Chilinkhu Farm Hannock Botha Langa Mgemezulu Nemoni Mlotha Sandres Mlotha
275 Yes
Ntchisi TA Chikho 2 10 Chibwenje Chipokosa Katola Masache Mtongo Ndudu Nyanga
400 Yes No – Vacant Yes Yes No – Vacant Yes Yes
Ntchisi TA Chikho 8 11 Masache 216 Yes
Ntchisi TA Kalumo 3 12 Bingamvula Chimbalu Chiopsa Kalasamkuwa
279 Yes No – HSA No – HSA Yes
Ntchisi TA Kalumo 30 13 Chithonje Kachelenga Kachilanduzi Kapichila Kasakula Lambulira Machira Maguya Makwesa Maluwa Mbuluma Mwamulo
605 No – HSA No – HSA Yes No – HSA No – HSA No – HSA No – HSA No – HSA No – HSA No – HSA No – HSA No – HSA
Ntchisi TA Kalumo 59 14 Chapuchapu Chawanda Mkambisi Mphanda
249 No – Vacant
Ntchisi STA Chilooko 8 15 Kavulala Liwenga Mkwindo
144 No – HSA No – HSA No – Vacant
Ntchisi STA Chilooko 14 16 Chisamba Mankhaka Mndesi Mndesi Farm
229 Yes
Ntchisi STA Chilooko 32 17 Kafulu Mateche Mayembe
189 No – HSA
Ntchisi STA Chilooko 40 18 Chankhozi Estate Chimbili Kandale
210 Yes
Ntchisi STA Chilooko 47 19 Lumbe Malambo M’njale Mwinama Nduwa Nsulu
325 No – HSA No – HSA No – HSA Yes No – HSA No – HSA

RAcE Endline Survey Final Report 42
District Traditional Authority
EA Cluster Villages Households Listed
Implementation status
Dedza TA Pemba (now TA Kachere)
39 20 Chingalunyamuka Bamusi Mkwaila Ndinga Willie Themuka
391 Yes
Dedza STA Chilikumwendo 29 21 Chidewere Trading Centre Chimkokota Kaluzi Kumalawi Kumtengo Mkwezalamba Mwambula Mzumazi Wandawanda
148 Yes
Dedza STA Chilikumwendo 49 22 Chimodzi Chipeni Magomero Trading Centre Moses Rufesi
511 Yes but transferred
Dedza TA Kaphuka 14 23 Falikile Kamkodo Mkanda Mngongonda Zakalamba
264 Yes
Dedza TA Kaphuka 31 24 Chipampha Mlamba Mlinga Nkhanganya
367 Yes
Dedza TA Kaphuka 38 25 Chagalawanda Chakhala Chiphoola Kambuzi Kamitengo Nyombe
495 No – HSA
Dedza TA Kaphuka 58 26 Chimpeni Kabango Mtsimba Phalula
412 No – HSA
Dedza TA Kaphuka 63 27 Katsache Kudemela Mwasadzu Paiwe
527 Yes
Dedza TA Kaphuka 80 28 Dzololo Hinda
448 Yes
Dedza TA Kaphuka 85 29 Kachala Malindima Mananga Ngunda
201 Yes
Dedza TA Kaphuka 93 30 Chilopa Kanyemba Kanyosole Kumano Mang'umbi Nyangu
377 Yes
Dedza TA Kaphuka 97 31 Kambewa Mwachalo Njolo
426 No – HSA

RAcE Endline Survey Final Report 43
District Traditional Authority
EA Cluster Villages Households Listed
Implementation status
Dedza TA Tambala 6 32 Chete, Chioza Kazembe Liu Mchalo Mpombe Tsuchi
365 Yes
Dedza TA Tambala 801 33 Chiphwanya Gosheni Kwizyo Mdendere, Mkajenda
533 No – Vacant
Dedza TA Kasumbu 8 34 Adini Chapola Chembe Kambwiri Mbimbi Mdala Mzoola
508 No – Vacant
Dedza TA Kasumbu 31 35 Boko Chigome Damison Gwazaudwale Maluwa Pinji
452 Yes but transferred
Dedza TA Kasumbu 49 36 Chakana Kayendele Mkhalapadzuwa Mpalale Ngwere
321 No – HSA
Dedza TA Kachindamoto 35 37 Dziko Galuanenenji
422 Yes
Dedza TA Kachindamoto 46 38 Diena Estate Kapiri 2 Msuka Sitolo 2
263 Yes
Dedza TA Kachindamoto 54 39 Abraham Asani
290 Yes
Dedza TA Kamenyagwaza 21 40 Khanganya 249 No – HSA
Ntcheu TA Phambala 5 41 Kanzati Kapulula Magombo Malota
262 Yes but moved out early 2016
Ntcheu TA Phambala 53 42 Kambalame 152 Yes
Ntcheu TA Phambala 58 43 Bayani Katsalam'bande
345 Yes
Ntcheu TA Makwangwala 1 44 Kalimbirana Loti Chinsinula
509 No – HSA
Ntcheu TA Makwangwala
9 45 Akubilila I Menyani Penga Penga
410 Yes
Ntcheu TA Makwangwala 24 46 Kukhola Mlambwadza
239 Yes
Ntcheu TA Makwangwala 53 47 Kalimanjira III Mwenda Wilson II
210 Yes

RAcE Endline Survey Final Report 44
District Traditional Authority
EA Cluster Villages Households Listed
Implementation status
Ntcheu TA Makwangwala 58 48 Chasasa Helani Kayinga Ntentha
394 No – Vacant Yes Yes Yes
Ntcheu TA Njolomole 21 49 Ben Zikagoya Kazembe Magola Zande
502 Yes
Ntcheu TA Njolomole 28 50 Bonga Chinkwandala Kanzende Mulodzanyama Zimenyana
354 Yes
Ntcheu TA Goodson Ganya 25 51 Manjanja Thunga
396 No – Vacant
Ntcheu TA Goodson Ganya 39 52 Kadam'manja Matapila
151 Yes
Ntcheu TA Goodson Ganya 57 53 Machaka 164 Yes
Ntcheu TA Goodson Ganya 63 54 Zande 262 Yes
Ntcheu TA Goodson Ganya 85 55 Chawanje 298 No – Vacant
Ntcheu TA Goodson Ganya 90 56 Sanjani 259 No – Vacant
Ntcheu TA Goodson Ganya 96 57 Kaimaima 414 Yes
Dedza12 TA Masasa 13 58 Kalumo Nsamala Pitala
342 No – Vacant
Ntcheu TA Masasa 17 59 Chikhumba Chiwembu, Foso
467 Yes
Ntcheu TA Masasa 24 60 Masese II 183 Yes
12 Was mistakenly noted as in Ntcheu district rather than in Dedza district

RAcE Endline Survey Final Report 45
ANNEX C1. ENDLINE SURVEY HOUSEHOLD QUESTIONNAIRE
See attached.

RAcE Endline Survey Final Report 46
ANNEX C2. ENDLINE SURVEY HSA QUESTIONNAIRE
See attached.

RAcE Endline Survey Final Report 47
ANNEX D. TRAINING SCHEDULE
Monday 25 July
Time Topic Facilitator
Day 1
(Materials needed: copies of training schedule; Training manuals, Questionnaires)
09:00 Session1: Orientation (Duration: 1hr)
- Opening statements
- Personal introductions
- Review of the training schedule
T Mleme
10:00 Session 2: RAcE Project (Duration: 30 min)
- RAcE Survey Objectives
-
E Chimbalanga
10:30 Session 3: Roles and responsibilities of the interviewer
(Duration: 45 min)
- Overview of Survey Modules, Teams and Roles
- Introduction to interviewers roles and responsibilities
- Regulations for Survey team
S Wachepa
11:15 BREAK (Duration: 15 min)
11:30 Session 4: Field work procedures (Duration: 1hr)
- Selection of households and respondents in the household, Daily Assignment sheets, making call backs
- Ensuring confidentiality
- Data quality checks (questionnaire review)
L Gombwa
12:30 LUNCH (Duration: 1hr)
13:30 Session 5: Interview procedures and tips (Duration: 2hr)
- Approach to the household
- Identify the respondent and administer informed consents
- Conducting the interview
F Matumula
15:30 BREAK (Duration: 15 min)
15:45 Session 6: Household questionnaire (Duration: 30min)
- Child Identifier
T Mleme
16:15 Session 7: Questions/ Concerns (Duration 15min)
16:30 ADJOURN

RAcE Endline Survey Final Report 48
Tuesday 26 July
Time Topic Facilitator
Day 2: Paper Questionnaires
(materials needed: printed questionnaire and manual for each participant)
08:30 Review Day 1/ Answer any questions (Duration 30 min) OK Banda
09:00 Session 8: Household questionnaire (Duration: 1 hr)
- Care giver's background
- Care giver's Decision making
- Care giver's knowledge of CCM trained HSAs & illness
S Wachepa
10:00 Session 9: Household questionnaire (Duration: 30 min)
- Diarrhoea & Fever
E Nyanda
10:30 BREAK (Duration: 15 min)
10:45 Session 10: Household questionnaire (Duration: 1 hr)
- Rapid Breath & Observations
E Nyanda
11:45 Session 11: Questions/ Concerns (Duration 30min) S Wachepa
12:15 LUNCH (Duration: 1hr)
13:15 Session 12: Practice (Duration : 2hr)
- Enter paper questionnaires
- Mock interviews
ALL
15:15 BREAK (Duration: 15 min)
15:30 Session 13: QUIZ (1 hr) ALL
16:30 ADJOURN
Wednesday 27 July
Time Topic Facilitator
Day 3: Questionnaires Practice
(Materials needed: questionnaires and manuals)
08:30 Review Day 2/ Answer any questions (Duration 30 min) E Dandaula
09:00 Session 14: Practice (Duration: 2hr)
- Enter paper questionnaires
- Mock Interviews
ALL
11:15 BREAK (Duration: 15 min)

RAcE Endline Survey Final Report 49
11:30 Session 15: Practice (Duration: 1hr)
- Enter paper questionnaires
- Mock Interviews
ALL
12:30 LUNCH (Duration: 1hr)
13:30 Session 16: Practice (Duration: 2hr)
- Enter paper questionnaires
- Mock Interviews
ALL
15:30 BREAK (Duration: 15 min)
15:45 Session 16: Practice (Duration: 1hr)
- Enter paper questionnaires
- Mock Interviews
ALL
16:45 ADJOURN
Thursday 28 July
Time Topic Facilitator
Day 4: (Materials needed: paper questionnaires, pens
07:30 Preparation for Field Practice (Duration 30 min) F Matumula
08:00 Session 17: Field Practice (Duration: Full day) ALL
15:00 Session 18: Review of field practice (Duration: 1hr) S Wachepa
16:00 ADJOURN
Friday 29 July
Time Topic Facilitator
Day 5: (Materials needed: questionnaires and manuals)
8:30 Review Day 4/ Answer any questions (Duration 30 min) T Maonga
09:00 Session 19: Test Review (Duration: 1hr) ALL
10:00 BREAK (Duration: 15 min)
10:15 Session 20: Practice (Duration: 2hr)
- Enter paper questionnaires
- Mock Interviews
ALL
12:15 LUNCH (Duration: 1hr)

RAcE Endline Survey Final Report 50
13:15 Session 21: Practice (Duration: 2hr)
- Enter paper questionnaires
- Mock Interviews
ALL
15:15 BREAK (Duration: 15 min)
15:30 Session 22: TEST (Duration:1hr)
ALL
16:30 ADJOURN
Saturday 30 July
Time Topic Facilitator
Day 6: (Materials needed: paper questionnaires, pens
07:30 Preparation for Field Practice (Duration 30 min) F Matumula
08:00 Session 23: Field Practice (Duration: Full day) ALL
15:00 Session 24: Review of field practice (Duration: 1hr) ALL
16:00 ADJOURN
Monday 01 August
Time Topic Facilitator
Day 7: HSA Questionnaire and Supervisors Training (Supervisors Only in room A)
(materials needed: Supervisor manual, HSA questionnaire)
09:00 Session 1: Supervisor Role and Duties (2hr)
- Team Leadership
- Selection of Households
T Mleme
11:00 BREAK (Duration: 15 min)
11:15 Session 2: HSA questionnaire (Duration: 1h)
- HSA Identifier
- HSA background
- HSA Supervision
L Gombwa
12:15 LUNCH (Duration: 1hr)

RAcE Endline Survey Final Report 51
13:15 Session 3: HSA questionnaire (Duration: 2hr)
- iCCM Medicines and Supplies
- iCCM Activities and Register Review
- Data display templates and data use
Romas
E Chimbalanga
15:15 BREAK (Duration: 15 min)
15:30 Session 4: HSA questionnaire (Duration: 1hr)
- Training and Knowledge of Newborn Health
- Newborn Health, Equipment, Supplies and Register Review
- Newborn Health Supervision
Romas
16:30 ADJOURN
Tuesday 02 August
Time Topic Presenter
Day 8: Interviewers and Supervisors supplements (materials needed: questionnaire and manuals)
08:30 Review Day 6/ Answer any questions (Duration 30 min)
09:00 Session 25: Listing and Mapping (Duration: 2h) Frank matumula
11:00 BREAK (Duration: 15 min)
11:15 Session 26: Field Stationary and Forms Completion (Duration: 1hr)
OK Banda
12:15 LUNCH (Duration: 1hr)
13:15 Session 27: Preparations for Fieldwork and Departure S Wachepa
16:00 END OF TRAINING

RAcE Endline Survey Final Report 52
ANNEX E. KEY INDICATOR SUMMARY TABLES FOR SUB-AREAS
E.1 Key Indicator Summary Table Comparing 33 Active Clusters and 27 Inactive
Clusters
Indicator Active Inactive % point
change % (CI %) % (CI %)
Caregiver knowledge
1
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who are aware of the presence of the CCM-trained HSA in their community
93.1 (87.4 - 96.3)
72.1 (55.7 - 84.2)
21.0
2
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know the role of the CCM-trained HSA in their community
35.0 (27.8 - 42.8)
32.6 (24.7 - 41.6)
2.4
3
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know two or more signs of childhood illness that require immediate assessment by an appropriately trained provider
96.2 (93.3 - 97.9)
95.0 (90.9 - 97.4)
1.2
Caregiver perceptions of iCCM services
4
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who view CCM-trained HSAs as trusted health care providers
77.8 (68.3 - 85.1)
59.0 (47.2 - 69.9)
18.8
5
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who believe CCM-trained HSAs provide quality services
62.0 (55.3 - 68.2)
51.0 (42.7 - 59.1)
11.0
6
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who found the CCM-trained HSA at first visit
84.1 (76.5 - 89.6)
83.5 (73.8 - 90.1)
0.6
7
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who cite the CCM-trained HSA as a convenient source of treatment
60.1 (52.0 - 67.7)
32.3 (22.2 - 44.5)
27.8
Sick child care-seeking
8
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey for whom advice or treatment was sought from an appropriate provider
Overall 73.9
(67.6 - 79.4) 65.3
(58.3 - 71.7) 8.6
Fever 76.5
(69.9 - 82.0) 70.6
(62.4 - 77.8) 5.9
Diarrhea 72.6
(64.3 - 79.7) 66.3
(57.5 - 74.1) 6.3
Cough with difficult or fast breathing 71.8
(63.4 - 79.0) 58.7
(50.4 - 66.5) 13.1
9
Percentage of children age 2-59 months who were sick in two weeks preceding the survey taken to a CCM-trained HSA as first source of care
Overall 45.8
(37.4 - 54.5) 18.4
(12.0 - 27.2) 27.4

RAcE Endline Survey Final Report 53
Indicator Active Inactive % point
change % (CI %) % (CI %)
Fever 47.0
(37.6 - 56.6) 17.5
(11.1 - 26.4) 29.5
Diarrhea 48.1
(38.7 - 57.7) 24.6
(15.8 - 36.1) 23.5
Cough with difficult or fast breathing 42.5
(33.8 - 51.6) 14.8
(9.0 - 23.3) 27.7
Sick child assessment
10 Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had finger or heel stick
60.8 (53.5 - 67.7)
56.8 (48.3 - 64.8)
4.0
11
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had had finger or heel stick in the two weeks preceding the survey
96.9 (93.4 - 98.6)
97.9 (93.2 - 99.4)
-1.0
12
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing
44.4 (37.7 - 51.4)
31.7 (24.9 - 39.5)
12.7
Sick child assessment by HSA
13
Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had a finger or heel stick by an HSA at a village clinic (among those who sought care from an HSA)
61.2 (50.6 - 70.8)
63.6 (44.4 - 79.4)
-2.4
14
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had a finger or heel stick by an HSA at a village clinic in the two weeks preceding the survey (among those who sought care from an HSA)
97.9 (91.2 - 99.5)
100 -2.1
15
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing by an HSA at a village clinic (among those who sought care from an HSA)
57.5 (45.3 - 68.9)
51.4 (36.7 - 65.9)
6.1
Sick child treatment
16
Percentage of children age 2-59 months who have been sick in two weeks preceding the survey who received appropriate treatment
Overall 50.8
(45.5 - 56.1) 42.7
(37.3 - 48.2) 8.1
Fever (ACT with 24 hours) * 61.3
(51.6 - 70.2) 56.4
(46.5 - 65.9) 4.9
Diarrhea (ORS and zinc) 24.5
(18.3 - 32.1) 17.1
(11.6 - 24.6) 7.4
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-amoxicillin)
66.8 (59.0 - 73.8)
56.1 (48.6 - 63.3)
10.7
17
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received appropriate treatment from a CCM-trained HSA
Overall 22.7
(17.1 - 29.4) 9.3
(5.0 - 16.7) 13.4
Fever (ACT with 24 hours) * 33.6
(23.8 - 45.1) 12.9
(4.9 - 29.9) 20.7

RAcE Endline Survey Final Report 54
Indicator Active Inactive % point
change % (CI %) % (CI %)
Diarrhea (ORS and zinc) 13.7
(8.7 - 20.9) 6.9
(3.0 - 14.8) 6.8
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-amoxicillin)
24.3 (18.6 - 31.2)
9.6 (5.6 - 15.9)
14.7
18
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received the first dose of treatment in the presence of an HSA among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 50.6
(41.2 - 59.9) 45.5
(34.7 - 56.6) 5.1
Fever (ACT) 54.8
(42.2 - 66.8) 61.9
(35.3 - 82.9) -7.1
Diarrhea (ORS and zinc) 24.1
(11.6 - 43.5) 16.7
(3.6 - 51.9) 7.4
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-amoxicillin)
57.1 (44.3 - 69.1)
45.5 (28.8 - 63.3)
11.6
19
Percentage of sick children age 2-59 months for whom their caregivers received counseling on how to provide the treatment(s) among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 97.2
(92.0 - 99.0) 100 -2.8
Fever (ACT) 98.8
(91.0 - 99.9) 100 -1.2
Diarrhea (ORS and zinc) 93.1
(74.6 - 98.4) 100 -6.9
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-amoxicillin)
96.8 (87.2 - 99.3)
100 -3.2
Sick child referral and follow-up
20 Percentage of sick children age 2-59 who were referred in the two weeks preceding the survey whose caregiver adhered to referral advice
89.5 (80.5 - 94.6)
80.0 (64.8 - 89.7)
9.5
21
Percentage of sick children age 2-59 months receiving treatment from an HSA in the two weeks preceding the survey whose caregiver followed up with the HSA after the initial consultation
23.1 (17.3 - 30.1)
17.4 (11.9 - 24.7)
5.7
*Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs, confirmed malaria treatment at endline by HSAs, confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.

RAcE Endline Survey Final Report 55
E.2 Key Indicator Summary Table Comparing Baseline and Endline Results for
33 Active Clusters
Indicators highlighted in green had a statistically significant increase from baseline to endline, determined by a p-value of less than 0.05. Indicators highlighted in red had a statistically significant decrease from baseline to endline, determined by a p-value of less than 0.05.
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Caregiver knowledge
1
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who are aware of the presence of the CCM-trained HSA in their community
92.4 (85.4 - 96.2)
93.1 (87.4 - 96.3)
0.7 0.7392
2
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know the role of the CCM-trained HSA in their community
38.4 (30.8 - 46.6)
35.0 (27.8 - 42.8)
-3.5 0.4923
3
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know two or more signs of childhood illness that require immediate assessment by an appropriately trained provider
98.0 (95.9 - 99.1)
96.2 (93.3 - 97.9)
-1.8 0.1724
Caregiver perceptions of iCCM services
4
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who view CCM-trained HSAs as trusted health care providers
84.5 (77.9 - 89.5)
77.8 (68.3 - 85.1)
-6.7 0.0638
5
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who believe CCM-trained HSAs provide quality services
67.7 (61.8 - 73.2)
62.0 (55.3 - 68.2)
-5.7 0.1378
6
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who found the CCM-trained HSA at first visit
87.0 (76.1 - 93.4)
84.1 (76.5 - 89.6)
-2.9 0.6081
7
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who cite the CCM-trained HSA as a convenient source of treatment
64.0 (54.7 - 72.4)
60.1 (52.0 - 67.7)
-3.9 0.4257
Sick child care-seeking
8
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey for whom advice or treatment was sought from an appropriate provider
Overall 68.5
(63.1 - 73.4) 73.9
(67.6 - 79.4) 5.4 0.1102
Fever 72.8
(65.5 - 79.1) 76.5
(69.9 - 82.0) 3.7 0.3820
Diarrhea 69.3
(62.7 - 75.2) 72.6
(64.3 - 79.7) 3.3 0.4725

RAcE Endline Survey Final Report 56
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Cough with difficult or fast breathing 63.3
(56.0 - 70.1) 71.8
(63.4 - 79.0) 8.5 0.0528
9
Percentage of children age 2-59 months who were sick in two weeks preceding the survey taken to a CCM-trained HSA as first source of care
Overall 30.4
(22.9 - 39.0) 45.8
(37.4 - 54.5) 15.4 0.0007
Fever 30.7
(23.1 - 39.4) 47.0
(37.6 - 56.6) 16.4 0.0005
Diarrhea 37.1
(27.3 - 48.1) 48.1
(38.7 - 57.7) 11.0 0.0479
Cough with difficult or fast breathing 24.6
(17.2 - 33.9) 42.5
(33.8 - 51.6) 17.9 0.0007
Sick child assessment
10 Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had finger or heel stick
32.2 (24.4 - 41.2)
60.8 (53.5 - 67.7)
28.6 0.0000
11
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had had finger or heel stick in the two weeks preceding the survey
96.4 (89.0 - 98.9)
96.9 (93.4 - 98.6)
0.5 0.8233
12
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing
29.4 (22.8 - 37.1)
44.4 (37.7 - 51.4)
15.0 0.0026
Sick child assessment by HSA
13
Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had a finger or heel stick by an HSA at a village clinic (among those who sought care from an HSA)
0 61.2
(50.6 - 70.8) 61.2 0.0000
14
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had a finger or heel stick by an HSA at a village clinic in the two weeks preceding the survey (among those who sought care from an HSA)
0* 97.9
(91.2 - 99.5) 97.9 na
15
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing by an HSA at a village clinic (among those who sought care from an HSA)
29.9 (20.3 - 41.6)
57.5 (45.3 - 68.9)
27.7 0.0005
Sick child treatment
16
Percentage of children age 2-59 months who have been sick in two weeks preceding the survey who received appropriate treatment
Overall 45.3
(39.4 - 51.4) 50.8
(45.5 - 56.1) 5.5 0.1133

RAcE Endline Survey Final Report 57
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Fever (ACT with 24 hours) * 63.9
(54.9 - 72.0) 61.3
(51.6 - 70.2) -2.5 0.6931
Diarrhea (ORS and zinc) 19.8
(13.5 - 28.2) 24.5
(18.3 - 32.1) 4.7 0.3283
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
56.5 (48.2 - 64.3)
66.8 (59.0 - 73.8)
10.3 0.0278
17
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received appropriate treatment from a CCM-trained HSA
Overall 16.6
(11.8 - 22.8) 22.7
(17.1 - 29.4) 6.1 0.0753
Fever (ACT with 24 hours) * 34.6
(25.4 - 45.2) 33.6
(23.8 - 45.1) -1.0 0.8647
Diarrhea (ORS and zinc) 8.9
(4.9 - 15.7) 13.7
(8.7 - 20.9) 4.8 0.2168
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
13.3 (8.1 - 21.1)
24.3 (18.6 - 31.2)
11.0 0.0228
18
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received the first dose of treatment in the presence of an HSA among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 38.2
(25.9 - 52.4) 50.6
(41.2 - 59.9) 12.3 0.1000
Fever (ACT) 45.1
(34.3 - 56.4) 54.8
(42.2 - 66.8) 9.7 0.1809
Diarrhea (ORS and zinc) 16.7
(5.6 - 40.4) 24.1
(11.6 - 43.5) 7.5 0.5357
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
39.4 (17.2 - 67.1)
57.1 (44.3 - 69.1)
17.7 0.2615
19
Percentage of sick children age 2-59 months for whom their caregivers received counseling on how to provide the treatment(s) among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 100 97.2
(92.0 - 99.0) -2.8 0.1710
Fever (ACT) 100 98.8
(91.0 - 99.9) -1.2 0.4574
Diarrhea (ORS and zinc) 100 93.1
(74.6 - 98.4) -6.9 0.2401
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin) 100
96.8 (87.2 - 99.3)
-3.2 0.3274
Sick child referral and follow-up
20
Percentage of sick children age 2-59 who were referred in the two weeks preceding the survey whose caregiver adhered to referral advice
87.0 (68.5 - 95.3)
89.5 (80.5 - 94.6)
2.5 0.7510

RAcE Endline Survey Final Report 58
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
21
Percentage of sick children age 2-59 months receiving treatment from an HSA in the two weeks preceding the survey whose caregiver followed up with the HSA after the initial consultation
16.7 (10.1 - 26.4)
23.1 (17.3 - 30.1)
6.4 0.1435
na = not applicable *Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs, confirmed malaria treatment at endline by HSAs, confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.
E.3 Key Indicator Summary Table Comparing Baseline and Endline Results for
27 Inactive Clusters
Indicators highlighted in green had a statistically significant increase from baseline to endline, determined by a p-value of less than 0.05. Indicators highlighted in red had a statistically significant decrease from baseline to endline, determined by a p-value of less than 0.05.
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Caregiver knowledge
1
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who are aware of the presence of the CCM-trained has in their community
86.9 (72.3 - 94.4)
72.1 (55.7 - 84.2)
-14.8 0.0239
2
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know the role of the CCM-trained HSA in their community
30.4 (23.1 - 38.9)
32.6 (24.7 - 41.6)
2.2 0.7403
3
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who know two or more signs of childhood illness that require immediate assessment by an appropriately trained provider
96.8 (94.2 - 98.3)
95.0 (90.9 - 97.4)
-1.8 0.3035
Caregiver perceptions of iCCM services
4
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who view CCM-trained HSAs as trusted health care providers
79.1 (71.6 - 85.1)
59.0 (47.2 - 69.9)
-20.1 0.0025
5
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who believe CCM-trained HSAs provide quality services
69.2 (61.2 - 76.3)
51.0 (42.7 - 59.1)
-18.3 0.0009
6
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who found the CCM-trained HSA at first visit
85.5 (75.8 - 91.8)
83.5 (73.8 - 90.1)
-2.0 0.7302
7
Percentage of caregivers of children age 2-59 months who have been sick in the two weeks preceding the survey who cite the CCM-trained HSA as a convenient source of treatment
53.8 (42.6 - 64.6)
32.3 (22.2 - 44.5)
-21.5 0.0043

RAcE Endline Survey Final Report 59
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Sick child care-seeking
8
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey for whom advice or treatment was sought from an appropriate provider
Overall 61.8
(52.7 - 70.1) 65.3
(58.3 - 71.7) 3.5 0.3604
Fever 67.0
(56.4 - 76.2) 70.6
(62.4 - 77.8) 3.6 0.4592
Diarrhea 57.4
(46.7 - 67.5) 66.3
(57.5 - 74.1) 8.9 0.1489
Cough with difficult or fast breathing 60.1
(48.3 - 70.9) 58.7
(50.4 - 66.5) -1.4 0.7822
9
Percentage of children age 2-59 months who were sick in two weeks preceding the survey taken to a CCM-trained HSA as first source of care
Overall 19.7
(12.4 - 29.7) 18.4
(12.0 - 27.2) -1.3 0.8124
Fever 20.6
(11.5 - 34.3) 17.5
(11.1 - 26.4) -3.2 0.6192
Diarrhea 22.8
(14.9 - 33.4) 24.6
(15.8 - 36.1) 1.7 0.7698
Cough with difficult or fast breathing 16.1
(9.2 - 26.5) 14.8
(9.0 - 23.3) -1.3 0.8093
Sick child assessment
10 Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had finger or heel stick
40.2 (32.9 - 48.0)
56.8 (48.3 - 64.8)
16.5 0.0029
11
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had had finger or heel stick in the two weeks preceding the survey
97.4 (89.3 - 99.4)
97.9 (93.2 - 99.4)
0.5 0.7777
12
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who had their respiratory rate counted to assess fast breathing
20.7 (13.5 - 30.5)
31.7 (24.9 - 39.5)
11.0 0.0685
Sick child assessment by HSA
13
Percentage of children age 2-59 months with fever in the two weeks preceding the survey who had a finger or heel stick by an HSA at a village clinic (among those who sought care from an HSA)
0 63.6
(44.4 - 79.4) 63.6 0.0000
14
Percentage of children age 2-59 months for whom their caregiver received the results of the malaria diagnostic test of the children who had a finger or heel stick by an HSA at a village clinic in the two weeks preceding the survey (among those who sought care from an HSA)
0* 100 0.0 na
15
Percentage of children age 2-59 months with cough and difficult or rapid breathing (suspected pneumonia) in the two weeks preceding the survey who
33.3 (17.1 - 54.8)
51.4 (36.7 - 65.9)
18.1 0.2194

RAcE Endline Survey Final Report 60
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
had their respiratory rate counted to assess fast breathing by an HSA at a village clinic (among those who sought care from an HSA)
Sick child treatment
16
Percentage of children age 2-59 months who have been sick in two weeks preceding the survey who received appropriate treatment
Overall 39.1
(32.2 - 46.5) 42.7
(37.3 - 48.2) 3.6 0.3365
Fever (ACT with 24 hours) * 58.8
(46.4 - 70.2) 56.4
(46.5 - 65.9) -2.4 0.7280
Diarrhea (ORS and zinc) 16.7
(10.4 - 25.7) 17.1
(11.6 - 24.6) 0.5 0.9166
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
49.2 (40.2 - 58.3)
56.1 (48.6 - 63.3)
6.9 0.2102
17
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received appropriate treatment from a CCM-trained HSA
Overall 10.5
(5.6 - 18.8) 9.3
(5.0 - 16.7) -1.2 0.7774
Fever (ACT with 24 hours) * 21.2
(10.5 - 38.1) 12.9
(4.9 - 29.9) -8.3 0.3504
Diarrhea (ORS and zinc) 4.9
(1.8 - 12.7) 6.9
(3.0 - 14.8) 1.9 0.5854
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
10.4 (5.4 - 19.1)
9.6 (5.6 - 15.9)
-0.8 0.8379
18
Percentage of children age 2-59 months who have been sick in the two weeks preceding the survey who received the first dose of treatment in the presence of an HSA among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 35.3
(19.2 - 55.7) 45.5
(34.7 - 56.6) 10.2 0.3942
Fever (ACT) 26.1
(9.7 - 53.6) 61.9
(35.3 - 82.9) 35.8 0.0634
Diarrhea (ORS and zinc) 37.5
(16.9 - 63.8) 16.7
(3.6 - 51.9) -20.8 0.2063
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin)
45.0 (24.9 - 66.8)
45.5 (28.8 - 63.3)
0.5 0.9755
19
Percentage of sick children age 2-59 months for whom their caregivers received counseling on how to provide the treatment(s) among those who received prescription medicines for a CCM condition in the two weeks preceding the survey
Overall 100 100 0 na
Fever (ACT) 100 100 0 na
Diarrhea (ORS and zinc) 100 100 0 na

RAcE Endline Survey Final Report 61
Indicator Baseline Endline % point
change p-value
% (CI %) % (CI %)
Cough with difficult or fast breathing (Baseline-cotrimoxazole; endline-
amoxicillin) 100 100 0 na
Sick Child Referral and Follow-up
20
Percentage of sick children age 2-59 who were referred in the two weeks preceding the survey whose caregiver adhered to referral advice
90.9 (74.6 - 97.2)
80.0 (64.8 - 89.7)
-10.9 0.2031
21
Percentage of sick children age 2-59 months receiving treatment from an HSA in the two weeks preceding the survey whose caregiver followed up with the HSA after the initial consultation
24.8 (15.8 - 36.6)
17.4 (11.9 - 24.7)
-7.4 0.1685
na = not applicable *Appropriate fever treatment includes presumptive malaria treatment at baseline by HSAs, confirmed malaria treatment at endline by HSAs, confirmed malaria treatment by all other providers at baseline and endline. Presumptive treatment includes cases in which ACT was given but no there was no finger prick or heel stick. Confirmed malaria treatment includes cases in which ACT was given, there was a finger or heel stick, and the result of the test was positive. Appropriate treatment for fever cases was restricted to include only children aged 5–59 months.

RAcE Endline Survey Final Report 62
ANNEX F. ILLNESS MANAGEMENT AND DIAGNOSTICS BY SEX RESULTS TABLES
Table F1. Fever management
Sought any advice or treatment
Sought treatment from an
appropriate provider*
Sought treatment from
an HSA
Sought treatment from an HSA as first
choice
Had blood taken from
finger or heel
Malaria treatment Number of
children with fever
Any anti-malarial
ACT ACT within 24 hours
Overall 86.7
(83.1 - 89.6) 73.9
(68.9 - 78.4) 34.3
(27.4 - 42.0) 34.0
(27.2 - 41.5) 59.0
(53.7 - 64.2) 52.0
(47.5 - 56.5) 50.3
(45.6 - 54.9) 30.7
(26.6 - 35.0) 571
Male 84.6
(79.5 - 88.6) 70.5
(64.0 - 76.3) 36.5
(28.7 - 45.1) 36.1
(28.5 - 44.6) 55.8
(49.2 - 62.2) 50.2
(44.4 - 56.0) 49.1
(43.5 - 54.8) 31.2
(26.1 - 36.8) 285
Female 88.8
(85.0 - 91.8) 77.3
(71.7 - 82.1) 32.2
(24.8 - 40.5) 31.8
(24.5 - 40.1) 62.2
(55.7 - 68.4) 53.9
(48.0 - 59.6) 51.4
(45.4 - 57.4) 30.1
(24.9 - 35.8) 286
* Refers to those who sought care from a hospital, health center, health post, village clinic (HSA), mobile/outreach clinic, or private hospital, clinic, or physician.
Table F2. Confirmed malaria treatment
Confirmed malaria treatment Number of children with a positive blood
test
Any Anti-malarial
ACT ACT within 24 hours
% (CI %) % (CI %) % (CI %)
Overall 95.1
(91.5 - 97.2) 92.2
(87.7 - 95.2) 59.0
(52.1 - 65.6) 244
Male 96.5
(90.6 - 98.7) 94.7
(88.4 - 97.7) 64.9
(55.6 - 73.2) 114
Female 93.9
(88.5 - 96.8) 90.0
(83.7 - 94.1) 53.9
(45.1 - 62.3) 130

RAcE Endline Survey Final Report 63
Table F3. Fever diagnostics
Had blood taken from
finger or heel
Among those who had blood taken
Number of children
with fever Were given
results Test result
positive
Overall 59.0
(53.7 - 64.2) 97.3
(95.0 - 98.6) 74.4
(69.1 - 79.1) 571
Male 55.8
(49.2 - 62.2) 96.9
(92.8 - 98.7) 74.0
(66.9 - 80.1) 285
Female 62.2
(55.7 - 68.4) 97.8
(94.0 - 99.2) 74.7
(67.0 - 81.1) 286
Table F4. Diarrhea management
Sought any advice or treatment
Sought treatment from an
appropriate provider*
Sought treatment
from an HSA
Sought treatment from an
HSA as first choice
Given same or
more than usual to
drink
Given same or
more than usual to
eat
Treatment Treated
with ORS AND Zinc
Number of
children with
diarrhea
ORS Home- made fluid
Zinc
Overall 77.3
(72.4 - 81.5) 69.8
(63.9 - 75.0) 37.7
(30.7 - 45.3) 37.5
(30.5 - 45.1) 50.4
(44.9 - 55.9) 32.6
(27.5 - 38.1) 68.5
(63.2 - 73.3) N/A
24.0 (19.1 - 29.8)
21.2 (16.9 - 26.3)
387
Male 73.7
(66.8 - 79.6) 68.8
(61.8 - 75.0) 39.5
(30.7 - 49.1) 39.5
(30.7 - 49.1) 51.7
(45.1 - 58.3) 29.8
(23.5 - 36.9) 67.8
(61.2 - 73.8) N/A
22.0 (16.8 - 28.2)
19.5 (14.5 - 25.8)
205
Female 81.3
(74.2 - 86.8) 70.9
(62.6 - 78.0) 35.7
(27.1 - 45.3) 35.2
(26.7 - 44.7) 48.9
(40.8 - 57.1) 35.7
(28.6 - 43.6) 69.2
(60.5 - 76.8) N/A
26.4 (19.6 - 34.5)
23.1 (17.1 - 30.4)
182
N/A=not available * Refers to those who sought care from a hospital, health center, health post, village clinic (HSA), mobile/outreach clinic, or private hospital, clinic, or physician.

RAcE Endline Survey Final Report 64
Table F5. Cough with difficult or fast breathing management
Sought any advice or treatment
Sought treatment from an appropriate
provider*
Sought treatment from
an HSA
Sought treatment from an HSA as first
choice
Assessed for rapid breathing
Treatment Number of children with cough and difficult or
fast breathing
Any antibiotic Amoxicillin
Overall 81.8
(78.1 - 85.0) 65.6
(59.8 - 71.1) 30.1
(23.7 - 37.3) 29.5
(23.2 - 36.6) 38.5
(33.5 - 43.7) 65.0
(59.6 - 70.1) 61.8
(56.4 - 66.9) 489
Male 79.8
(73.8 - 84.7) 64.6
(56.3 - 72.0) 29.1
(22.0 - 37.4) 27.9
(20.9 - 36.0) 35.4
(28.4 - 43.2) 61.6
(53.7 - 69.0) 59.1
(51.3 - 66.4) 237
Female 83.7
(78.6 - 87.8) 66.7
(60.4 - 72.4) 31.0
(24.0 - 38.9) 31.0
(24.0 - 38.9) 41.3
(34.9 - 48.0) 68.3
(61.8 - 74.1) 64.3
(57.4 - 70.6) 252
* Refers to those who sought care from a hospital, health center, health post, village clinic (HSA), mobile/outreach clinic, or private hospital, clinic, or physician.

RAcE Endline Survey Final Report 65
ANNEX G. SUPPLEMENTARY 60 CLUSTER RESULTS TABLES
Table G1. Caregiver knowledge of child illness or danger signs
Child Illness or danger sign Baseline % (CI %)
Endline % (CI %)
Child under two months old 0.3
(0.1 - 1.1) 0.0
(0.0 - 0.0)
Fever 94.0
(91.7 - 95.7) 65.5
(59.9 - 70.8)
Fever for seven days or more 1.5
(0.7 - 3.2) 22.9
(18.9 - 27.4)
Diarrhea with blood in stool 6.0
(4.3 - 8.3) 17.0
(13.7 - 20.9)
Diarrhea with dehydration 45.6
(40.8 - 50.4) 47.0
(42.1 - 52.0)
Diarrhea for 14 days or more 9.9
(7.6 - 12.8) 8.2
(5.9 - 11.3)
Fast or difficult breathing/chest in-drawing 28.9
(24.6 - 33.6) 36.0
(31.6 - 40.7)
Cough for 21 days or more 24.4
(21.0 - 28.2) 17.2
(14.0 - 21.1)
Refusal to breastfeed 11.4
(8.7 - 14.7) 9.1
(7.0 - 11.6)
Not able to drink or feed 16.4
(12.7 - 20.9) 13.4
(10.5 - 17.0)
Vomits everything 42.4
(37.9 - 46.9) 42.4
(38.3 - 46.7) Yellow or red MUAC result/skinny upper arm and swelling of both feet
2.2 (1.3 - 3.7)
5.5 (3.8 - 7.8)
Convulsions 12.6
(9.6 - 16.5) 17.9
(15.0 - 21.2)
Loss of consciousness 11.5
(8.7 - 15.1) 19.3
(15.6 - 23.6)
Lethargic/tired/slow to respond/does not want to play 17.6
(13.0 - 23.5) 16.7
(13.5 - 20.6)
Stiff next 1.8
(1.0 - 3.2) 0.6
(0.2 - 2.1)
Don't know 0.1
(0.0 - 1.0) 0.0
(0.0 - 0.0) Number of caregivers 720 783
MUAC=mid-upper arm circumference

RAcE Endline Survey Final Report 66
Table G2. Caregiver knowledge of HSA activities
HSA activity Baseline % (CI %)
Endline % (CI %)
Community mobilization 26.2
(20.8 - 32.5) 23.6
(18.2 - 30.0)
Organization of health campaigns 18.2
(13.9 - 23.5) 26.8
(20.8 - 33.8)
Dissemination of health messages 19.4
(14.9 - 24.9) 36.0
(30.3 - 42.1)
Provide health information in households 64.8
(57.7 - 71.3) 44.9
(39.2 - 50.7)
Provide health information at community events 17.0
(14.2 - 20.2) 13.2
(10.2 - 16.9)
Collect information on health 6.5
(4.5 - 9.2) 6.6
(4.4 - 9.8)
Other preventative activity 8.3
(5.7 - 12.1) 11.6
(7.9 - 16.8)
Refer to health facility 18.5
(14.6 - 23.2) 13.5
(10.4 - 17.3)
Test for malaria 2.8
(1.7 - 4.6) 13.0
(9.7 - 17.2)
Assess for suspected pneumonia 4.5
(2.7 - 7.4) 6.6
(4.6 - 9.3)
Provide treatment for malaria 38.7
(33.4 - 44.3) 32.0
(25.6 - 39.2)
Provide treatment for pneumonia 5.9
(4.1 - 8.3) 10.6
(7.5 - 14.7)
Provide ORS for diarrhea 32.1
(26.8 - 37.9) 17.6
(13.9 - 22.1)
Provide zinc for diarrhea 3.7
(2.4 - 5.8) 4.9
(3.5 - 6.7)
Assess for malnutrition 5.6
(3.3 - 9.1) 13.6
(10.4 - 17.7)
Follow up sick children at home 7.9
(4.9 - 12.4) 9.8
(7.4 - 12.9)
Other curative activity 5.4
(3.4 - 8.6) 11.2
(7.8 - 15.9)
Don't know 0.5
(0.1 - 2.0) 0.8
(0.3 - 2.1) Number of caregivers 648 653

RAcE Endline Survey Final Report 67
Table G3. Reasons caregivers did not seek care from any source (endline only)
Reason Overall
% (CI %) Fever
% (CI %) Diarrhea % (CI %)
Cough* % (CI %)
Did not think the condition was serious 30.4
(24.6 - 37.0) 26.3
(18.9 - 35.4) 39.8
(28.5 - 52.3) 24.7
(17.5 - 33.7)
Condition passed 12.7
(8.9 - 17.7) 15.8
(8.6 - 27.2) 14.8
(8.8 - 23.7) 7.9
(3.6 - 16.2)
Place of care was too far 14.6
(9.5 - 21.9) 11.8
(5.9 - 22.4) 12.5
(7.2 - 20.9) 19.1
(11.0 - 31.2)
Did not have time 7.1
(4.0 - 12.5) 4.0
(1.2 - 11.9) 6.8
(2.7 - 16.4) 10.1
(5.1 - 19.1)
Did not have permission 0.4
(0.1 - 2.9) 0.0 0.0
1.1 (0.2 - 7.9)
Did not have money 21.0
(13.9 - 30.4) 25.0
(14.4 - 39.8) 18.2
(9.4 - 32.3) 20.2
(12.2 - 31.6) Could treat the condition at home or with medicines already on hand
22.1 (16.4 - 29.2)
23.7 (14.8 - 35.6)
11.4 (5.5 - 22.1)
31.5 (21.9 - 43.0)
Other 7.1
(4.1 - 12.0) 5.3
(2.0 - 13.3) 9.1
(4.1 - 19.0) 6.7
(3.1 - 14.0) Number of caregivers who didn't seek care
253 76 88 89
*Cough with difficult or fast breathing
Table G4. Reasons caregivers did not seek care from an HSA, among those who sought care
(endline only)
Reason Overall
% (CI %) Fever
% (CI %) Diarrhea % (CI %)
Cough* % (CI %)
HSA was not available 18.2
(11.6 - 27.2) 17.7
(11.3 - 26.7) 17.7
(10.3 - 28.7) 19.0
(11.4 - 30.0)
HSA did not have medicines or supplies 1.1
(0.4 - 3.5) 2.0
(0.7 - 5.4) 0.7
(0.1 - 4.8) 0.4
(0.1 - 2.9)
Did not trust HSA to provide care 1.0
(0.4 - 2.2) 2.0
(0.9 - 4.3) 0.0
0.4 (0.1 - 2.9)
Thought condition was too serious 2.6
(1.3 - 4.9) 3.3
(1.6 - 6.7) 2.0
(0.5 - 8.0) 2.0
(0.7 - 5.6)
Preferred to go to another provider 80.4
(73.1 - 86.2) 78.3
(70.6 - 84.4) 84.3
(72.3 - 91.7) 80.6
(72.3 - 86.9)
HSA was too far away 5.3
(3.3 - 8.2) 5.7
(3.4 - 9.4) 2.0
(0.5 - 8.1) 6.7
(3.8 - 11.7)
Other 1.6
(0.9 - 2.7) 1.3
(0.5 - 3.4) 1.3
(0.3 - 5.0) 2.0
(0.9 - 4.5) Number of caregivers who sought care—but not from HSA 705 299 153 253
*Cough with difficult or fast breathing

RAcE Endline Survey Final Report 68
Table G5. Location of sick child assessment
Location* Malaria Fast breathing
Baseline Endline Baseline Endline % (CI %) % (CI %) % (CI %) % (CI %)
Village clinic** 2.5
(0.7 - 8.2) 36.5
(27.8 - 46.2) 27.4
(18.3 - 39.0) 45.2
(34.8 - 56.1)
Government hospital 81.5
(70.6 - 89.0) 51.3
(42.6 - 60.0) 62.0
(50.7 - 72.1) 45.2
(36.1 - 54.6)
Mission hospital (CHAM) 10.5
(4.5 - 22.5) 5.9
(3.3 - 10.4) 6.2
(2.7 - 13.6) 5.3
(3.0 - 9.2)
Private health facility 5.6
(2.9 - 10.3) 8.0
(4.8 - 13.2) 6.2
(2.9 - 12.6) 9.6
(5.3 - 16.7)
Other 0.0 0.3
(0.0 - 2.2) 0.0 0.0
Total number of illness cases assessed
162 337 113 188
* The dataset only contained one response per caregiver in the baseline survey but allowed for multiple responses in the endline survey. ** Three caregivers reported that their children had blood taken by an HSA at a village clinic in the baseline survey, but Save the Children Malawi confirmed that this was not possible because malaria blood tests were not available at that time; one caregiver reported that his or her child had blood drawn by a nurse at a village clinic.
Table G6. Provider of sick child assessment
Provider Malaria Fast breathing
Baseline Endline Baseline Endline % (CI %) % (CI %) % (CI %) % (CI %)
HSA* 9.3
(5.3 - 15.7) 43.0
(34.5 - 52.0) 30.1
(21.2 - 40.8) 47.9
(37.7 - 58.2)
Medical assistant 54.3
(44.0 - 64.3) 28.5
(22.5 - 35.4) 35.4
(26.2 - 45.8) 28.7
(21.3 - 37.5)
Clinical officer 13.0
(6.8 - 23.3) 2.1
(0.9 - 4.8) 15.9
(9.3 - 26.0) 2.7
(0.9 - 7.3)
Nurse 17.9
(10.9 - 27.9) 18.4
(13.4 - 24.8) 15.9
(9.8 - 24.9) 20.2
(13.7 - 28.9)
Doctor 4.3
(1.9 - 9.7) 3.6
(1.8 - 7.0) 5.3
(2.5 - 11.0) 3.7
(1.8 - 7.6)
Other 0.6
(0.1 - 4.4) 6.5
(3.8 - 11.1) 0.0
1.6 (0.4 - 6.9)
Don't know 0.6
(0.1 - 4.5) 0.6
(0.2 - 2.3) 0.0
0.5 (0.1 - 3.9)
Total number of illness cases assessed
162 337 113 188
* HSAs may have taken blood from a child at a health center; mRDTs were not available at village clinics at the time of the baseline survey.
Table G7. Sick child care for children with diarrhea
Treatment Baseline Endline
p-value % (CI %) % (CI %)
Continued fluids 52.5
(47.2 - 57.7) 50.4
(44.9 - 55.9) 0.6193
Continued feeding 35.2
(30.5 - 40.2) 32.6
(27.5 - 38.1) 0.4735
Total number of children with diarrhea
364 387

RAcE Endline Survey Final Report 69
Table G8. Fever treatment coverage*
Received Treatment From HSA Among Those Who Sought
Care From HSA
Received Treatment Among all Fever Cases
Baseline Endline p-
value Baseline
N Endline
N
Baseline Endline p-value
Baseline N
Endline N % (CI %) % (CI %) % (CI %) % (CI %)
Received ACT 59.7
(51.2 - 67.7) 54.4
(45.2 - 63.2) 0.4456 124 184 52.1
(46.5 - 57.6) 51.5
(46.6 - 56.3) 0.8723 438 542
Received ACT within 24 hours
52.4 (43.9 - 60.8)
38.6 (30.6 - 47.3)
0.0263 124 184 40.2 (34.1 - 46.6)
31.7 (27.6 - 36.2)
0.0140 438 542
Received ACT within 24 hours, positive blood test*
na 64.8
(53.8 - 74.5) na 0 91 57.4
(47.5 - 66.7) 59.2
(52.5 - 65.7) 0.7467 122 238
Received ACT
Blood test positive na 89.0
(79.1 - 94.6) na 0 91 84.4
(77.0 - 89.8) 92.4
(87.9 - 95.4) 0.0318 122 238
Blood test negative na 4.4
(0.5 - 30.1) na 0 23 20.6
(9.5 - 39.0) 7.7
(3.5 - 16.1) 0.0592 34 78
No blood test** 59.7
(51.1 - 67.7) 26.1
(16.7 - 38.3) 0.0002 124 69 48.9
(41.5 - 56.4) 35.2
(27.5 - 43.6) 0.0096 235 145
Did not receive ACT
Blood test positive na 11.0
(5.4 - 20.9) na 0 91 15.6
(10.2 - 23.0) 7.6
(4.6 - 12.1) 0.0318 122 238
Blood test negative na 95.7
(70.0 - 99.5) na 0 23 79.4
(61.0 - 90.5) 92.3
(83.9 - 96.5) 0.0592 34 78
No blood test** 40.3
(32.3 - 48.9) 73.9
(61.7 - 83.3) 0.0002 124 69
51.1 (43.6 - 58.5)
64.8 (56.4 - 72.5)
0.0096 235 145
na = not applicable
* 3 caregivers reported that their child got a finger prick or heel stick by an HSA at a village clinic at baseline even though mRDTs were not available at village clinics at the time of the baseline survey. All indicators in this table were restricted to include only children 5 - 59 months.
** Included only cases in which any care was sought among all fever cases

RAcE Endline Survey Final Report 70
Table G9. Diarrhea treatment taken
Treatment Baseline % (CI %)
Endline % (CI %)
ORS 70.1
(64.4 - 75.1) 68.5
(63.2 - 73.3)
Zinc 21.4
(16.8 - 26.9) 24.0
(19.1 - 29.8) Homemade fluid N/A N/A Number of children with diarrhea 364 387
Other treatment Baseline % (CI %)
Endline % (CI %)
Antibiotic pill/syrup 32.6
(22.6 - 44.4) 18.3
(11.9 - 27.0)
Anti-motility pill/syrup 2.3
(0.5 - 8.8) 11.8
(5.3 - 24.2)
Other pill/syrup 2.3
(0.5 - 8.9) 2.2
(0.5 - 8.5)
Unknown pill/syrup 13.5
(8.0 - 22.0) 15.1
(9.0 - 24.1)
Antibiotic injection 3.4
(1.1 - 9.9) 5.4
(2.2 - 12.4)
Non-antibiotic injection 1.1
(0.2 - 7.9) 1.1
(0.1 - 7.8)
Unknown injection 1.1
(0.2 - 7.3) 1.1
(0.2 - 7.5)
Intravenous treatment 1.1
(0.2 - 7.9) 0.0
(0.0 - 0.0)
Home remedy/herbal medicine 11.2
(6.1 - 19.8) 12.9
(6.6 - 23.6)
Other 39.3
(29.9 - 49.7) 41.9
(31.9 - 52.7) Number of children with diarrhea who took other medication
89 93
N/A=not available
Table G10. Fever treatment taken
Treatment Baseline % (CI %)
Endline % (CI %)
ACT (LA) 59.4
(54.1 - 64.5) 61.9
(57.1 - 66.4)
Quinine 2.9
(1.5 - 5.5) 3.9
(2.4 - 6.2)
SP/Fansidar 1.3
(0.6 - 3.1) 1.3
(0.4 - 4.0) Antibiotic pill/syrup (not corimoxazole or amoxicillin)
5.2 (3.2 - 8.3)
1.7 (0.8 - 3.7)
Antibiotic injection 1.3
(0.5 - 3.1) 2.6
(1.4 - 4.8)
Cotrimoxazole/amoxicillin 19.8
(15.3 - 25.2) 19.4
(16.3 - 22.9)
Aspirin 12.5
(9.3 - 16.5) 5.4
(3.4 - 8.6)
Paracetamol 63.3
(58.0 - 68.2) 84.5
(81.3 - 87.2)
Other 6.3
(3.9 - 10.0) 4.5
(2.9 - 7.1)
Don't know 0.3
(0.0 - 1.9) 0.2
(0.0 - 1.6) Number of children with fever who took any medication
384 464

RAcE Endline Survey Final Report 71
Table G11. Cough with difficult or fast breathing treatment taken
Treatment Baseline % (CI %)
Endline % (CI %)
ACT (LA) 4.7
(2.9 - 7.5) 4.7
(2.8 - 8.0)
Quinine 0.6
(0.1 - 2.2) 1.1
(0.3 - 3.5)
SP/Fansidar 0.0
(0.0 - 0.0) 0.8
(0.3 - 2.4)
Antibiotic cough syrup 22.5
(17.3 - 28.6) 9.7
(6.6 - 14.2)
Antibiotic injection 2.2
(1.1 - 4.2) 1.3
(0.5 - 3.7)
Cotrimoxazole/amoxicillin 64.4
(59.0 - 69.4) 79.5
(73.7 - 84.3)
Aspirin 5.8
(3.5 - 9.2) 2.9
(1.7 - 5.0)
Paracetamol 35.3
(29.7 - 41.4) 41.8
(36.7 - 47.1)
Other 12.6
(8.9 - 17.6) 8.2
(5.4 - 12.1)
Don't know 0.3
(0.0 - 2.0) 1.6
(0.7 - 3.4) Number of children with difficult or fast breathing who took any medication
365 380
Table G12. Source of ACT
Location Source of treatment
Baseline Endline % (CI %) % (CI %)
Public facility 53.1
(44.1 - 61.8) 44.6
(36.1 - 53.4)
Private facility 9.7
(5.5 - 16.5) 12.5
(7.9 - 19.3)
HSA 32.5
(24.0 - 42.2) 36.6
(27.8 - 46.3)
Shop or pharmacy 4.4
(2.0 - 9.6) 5.9
(3.5 - 9.8) Traditional practitioner 0.0 0.0
Other 0.4
(0.1 - 3.1) 0.4
(0.1 - 2.5) Total number of fever cases receiving ACT 228 287

RAcE Endline Survey Final Report 72
Table G13. Source of ORS
Location Source of treatment
Baseline Endline % (CI %) % (CI %)
Public facility 37.7
(29.7 - 46.4) 33.2
(25.5 - 42.0)
Private facility 4.3
(2.1 - 8.7) 8.3
(4.8 - 14.0)
HSA 39.6
(30.8 - 49.2) 44.2
(35.3 - 53.4)
Shop or pharmacy 16.1
(11.5 - 22.0) 11.3
(7.5 - 16.7) Traditional practitioner 0.0 0.0
Other 2.4
(1.1 - 5.1) 3.0
(1.4 - 6.3) Total number of diarrhea cases receiving ORS
255 265
Table G14. Source of zinc
Location Source of treatment
Baseline Endline % (CI %) % (CI %)
Public facility 44.9
(31.9 - 58.6) 43.0
(30.4 - 56.6)
Private facility 9.0
(3.3 - 22.3) 7.5
(3.2 - 16.9)
HSA 38.5
(25.5 - 53.3) 46.2
(33.7 - 59.2)
Shop or pharmacy 5.1
(1.8 - 13.5) 3.2
(1.0 - 9.7) Traditional practitioner 0.0 0.0
Other 2.6
(0.6 - 10.1) 0.0
Total number of diarrhea cases receiving zinc 78 93
Table G15. Source of cotrimoxazole/amoxicillin
Location Source of treatment*
Baseline Endline % (CI %) % (CI %)
Public facility 47.8
(39.9 - 55.9) 44.0
(37.0 - 51.3)
Private facility 4.7
(2.3 - 9.4) 9.9
(6.2 - 15.6)
HSA 22.8
(16.0 - 31.5) 28.2
(22.2 - 35.0)
Shop or pharmacy 23.7
(18.0 - 30.6) 15.9
(12.0 - 20.7) Traditional practitioner 0.0 0.0
Other 0.9
(0.2 - 3.5) 2.0
(0.9 - 4.4) Total number of cough with fast breathing cases receiving cotrimoxazole/amoxicillin
232 302
* Source of treatment was missing for three respondents who indicated that they received cotrimoxazole or amoxicillin.

RAcE Endline Survey Final Report 73
G16. Reason did not comply with HSA referral
Reason Baseline Endline
% (CI %) % (CI %)
Too far 11.1
(1.2 - 55.7) 0.0
Did not have money 11.1
(1.2 - 55.7) 30.8
(11.9 - 59.3)
No transport 0.0 15.4
(3.3 - 49.2)
Did not think illness was serious 0.0 7.7
(0.9 - 44.1)
Child improved 77.8
(37.2 - 95.4) 46.2
(22.2 - 72.0)
No time 0.0 7.7
(0.9 - 44.1)
Went somewhere else 0.0 0.0
Did not have husband's permission 0.0 0.0
Other 0.0 7.7
(0.9 - 44.1)
Total number of caregivers who did not comply with referral
9 13
G17. Time of follow-up visit to HSA (days after initial consultation)
When did follow-up take place? Baseline Endline
% (CI %) % (CI %)
One day
21.4 (8.7 - 43.9)
9.5 (2.7 - 28.9)
Two days
14.3 (5.0 - 34.4)
28.6 (12.5 - 52.8)
Three days
32.1 (12.1 - 62.1)
42.9 (23.1 - 65.1)
Four days
3.6 (0.5 - 22.5)
9.5 (2.0 - 34.9)
Five days
3.6 (0.4 - 27.2)
0.0 (0.0 - 0.0)
More than five days
25.0 (6.6 - 61.3)
9.5 (1.9 - 36.8)
Total number of sick children who were followed up by an HSA
28 21

RAcE Endline Survey Final Report 74
ANNEX H. RESULTS OF ENDLINE HSA SURVEY
INTRODUCTION
As part of the endline evaluation, the National Statistics Office, ICF, and Save the Children conducted a
survey of health surveillance assistants (HSAs) to assess the implementation strength and quality of
integrated community case management (iCCM) services delivered by them. The HSA survey was
conducted alongside the endline household survey in four districts (Dedza, Mzimba North, Ntcheu, and
Ntchisi) to assess care-seeking practices and treatment coverage for iCCM conditions. The objective of
the HSA survey was to gain a better understanding of the HSAs’ background characteristics, activity
levels, and support and supervision received to help interpret the results of the coverage survey.
The HSAs serving the 60 clusters selected for the endline household survey formed the sample
population for the HSA survey. The clusters do not align perfectly with HSA catchment areas, and in
some cases there could be more than one HSA associated with a given cluster, or the cluster might not
have any community case management (CCM)-trained or active HSAs providing services. If a selected
cluster had more than one HSA who was trained in CCM, one was randomly selected for interview.
Data collection was carried out during August 2016.
RESULTS
A summary indicator table is provided in Table 1 and the main findings are summarized below. An HSA
could not be located in 13 (22 percent) of the 60 clusters (5 in Dedza, 6 in Ntcheu, and 2 in Ntchisi).
Thus, interviews were completed with a total of 47 HSAs:
District Number of clusters Number of HSAs
interviewed
Percentage of clusters with HSA
interviewed
Dedza 21 16 76%
Mzimba North 9 9 100%
Ntcheu 20 14 70%
Ntchisi 10 8 80%
Total 60 47 78%
HSA profile: Seventy percent of sampled HSAs were male (33/47) and most had completed Form 4
(62 percent) or Form 2 (32 percent) education. Two-thirds (68 percent) were between 29 and 40 years
of age.
HSA catchment areas: Most HSAs (83 percent) resided in their catchment areas. The main modes of
transportation were push bike (74 percent) or walking (19 percent). About one-third of HSAs
(36 percent) reported that it took less than 1 hour to reach the nearest health facility, 43 percent
reported that it took between 1–2 hours, and 21 percent reported that it took 2 hours or more. For
those not living in their catchment areas, most (5/8) reported that they could reach their village clinic
within 30 minutes.
Supervision: Two-thirds of HSAs (31/47) reported receiving at least 1 supervisory visit in the last
3 months, and 30 percent had received 2 or more visits. Senior HSAs (72 percent) and district staff
(22 percent) were the most frequently mentioned providers of supervision during the most recent visit.
Among those who reported supervision, all reported that the supervisors used a supervision checklist,
and most indicated that records and supply availability were reviewed and that they received feedback
on their iCCM activities. A smaller percentage of HSAs mentioned that the supervisor had administered
a case scenario (84 percent), observed sick child care (72 percent), observed a malaria rapid diagnostic

RAcE Endline Survey Final Report 75
test (mRDT) (72 percent), or talked with village leaders (56 percent). About half of HSAs (55 percent)
reported one or more mentorship sessions in which sick child care was observed in the last three
months.
Availability of iCCM medicines and diagnostics: The majority of HSAs (87 percent, 41/47) had at
least one age formulation of first-line antimalarial medicine (Coartem; LA 1x6 or 2x6) in stock on the
day of observation, and 79 percent (37/47) had both. Most HSAs were observed to have paracetamol
(89 percent), zinc (83 percent), amoxicillin (79 percent), and oral rehydration solution (ORS)
(79 percent). Regarding diagnostics, 89 percent of HSAs had rapid diagnostic tests (RDTs), and 87
percent had a functional timer. Overall, about 40 percent of HSAs had all iCCM medicines and supplies
available on the day of the survey, and 60 percent had all essential iCCM medicines and supplies.13
Stockouts of iCCM items were relatively common, with only 64 percent of HSAs reporting no
stockouts of any essential iCCM medicine or RDTs in the last one month.14 The most frequently
reported stockouts were amoxicillin and LA 2x6. About 13 percent of HSAs reporting referring one or
more sick children due to stockouts of medicine in the last month.
HSA functionality: About 89 percent of HSAs had provided iCCM services in the past month and
reported provided iCCM services at least 2 days per week. However, only 26 percent met a stricter
definition of functionality, in which they resided in their catchment areas, provided iCCM services in the
last month, and reported providing iCCM at least 5 days per week.
Activity levels and record-keeping: Most HSAs (94 percent) reported providing iCCM services at least
2 days per week, but only one-quarter (26 percent) reported providing iCCM 5 or more days per week.
HSAs reported operating their village clinics for an average of 3.3 days per week and 12.8 days per
month (median 10). Register reviews indicated that HSAs treated an average of 43.5 sick child cases
(median 37; range 0–220) in the last month. About 6 percent of HSAs had not treated any sick child
cases in the past one month. Interestingly, HSAs meeting the stricter definition of functionality treated
slightly fewer sick child cases per month on average (41.8 percent) than those who did not meet that
definition (44.1 percent). More than one-third (36 percent) of HSAs had referred one or more sick
children for danger signs in the last month (mean of 0.5; range 0–3). Completeness of recording of cases
in the registers was high for RDT results (91 percent) for the 5 most recent fever cases, but slightly
lower for results of respiratory rate counts (85 percent) for the 5 most recent cough cases.
HSA data use: About 72 percent of HSAs (34/47) reported being trained in the data use package. Of
those trained, 71 percent (24/34) had received the data use templates, 33 percent had wall charts
displayed (13/34), and 29 percent (10/34) had completed charts with data filled out for the past three
months.
IMPLICATIONS
These findings have several implications for iCCM in Malawi:
Only 78 percent of the 60 endline survey clusters had a CCM-trained HSA available for interview.
Although most of the available HSAs met the Ministry of Health (MOH) definition for functionality
(providing iCCM services in last month and providing iCCM at least two days per week), only one in
four were providing regular iCCM services (living in their catchment areas, and providing iCCM at
13 LA (at least 1x6 or 2x6), amoxicillin, ORS, zinc, RDTs, and functional timer 14 LA (stock-outs of both 1x6 and 2x6), amoxicillin, ORS, zinc, and RDTs

RAcE Endline Survey Final Report 76
least five days per week). Thus, when considering the full sample of 60 clusters, only 20 percent of
sampled areas had access to an HSA providing iCCM at least 5 days per week, and 70 percent had
access to an HSA providing iCCM at least 2 days per week. However, all HSAs, even those who did
not meet the stricter definition of functionality, still treated relatively high numbers of sick child
cases on a monthly basis, reflecting the high demand for iCCM services in the community.
Despite program support through RAcE and supply chain support tools such as c-stock, HSAs are
still experiencing shortages of iCCM medicines and supplies that limit their ability to provide quality
care. Only about 60 percent of HSAs had all essential medicines and diagnostics to deliver quality
iCCM, and reports of stockouts in the previous month were common. Amoxicillin was introduced
as first-line treatment for suspected pneumonia in RAcE districts, and monitoring data suggest that
overtreatment with antibiotics is still common and could be contributing to shortages, because
procurement is based on expected cases. Concurrent efforts are needed to identify and address the
underlying causes of overtreatment and to strengthen the supply chain management system for case
management at facility and HSA levels.
Supervision and mentoring levels reported by HSAs were substantially lower than targeted in the
RAcE program. After senior HSAs, RAcE district supervisors were among the primary providers of
onsite supervision. This raises concerns regarding the level of supervision and clinical mentoring that
will be maintained when support from the RAcE program ends and MOH takes on full responsibility.
Distance to HSAs, transportation gaps, competing time demands, and other factors are known
barriers to supervision. Numerous attempts have been made to address these issues with limited
sustained success. New approaches to providing clinical support and mentoring of HSAs that are
less demanding of over-stretched facility staff will likely need to be identified as part of the transition
plan.
Data use by HSAs is an area for further strengthening—many HSAs were trained in the package but
not all had received the templates and few were filling them on a regular basis.
Table H1. Summary of indicators for iCCM service delivery by HSAs
Domain Indicator Result
Residency Percentage of CCM-trained HSAs residing in their catchment area 83% (39/47) (95% CI: 69%-91%)
Functionality Percentage of CCM-trained HSAs who are functional (MOH definition): i) have provided iCCM services in past month ii) report operating village clinic for at least two days per week
89% (42/47) (95% CI: 76%-96%)
Percentage of CCM-trained HSAs who are functional (stricter version): i) reside in their catchment area ii) have provided iCCM services in past month iii) report operating village clinic for at least five days per week
26% (12/47) (95% CI: 15%-40%)
Medicine and diagnostics availability
Percentage of HSAs with all key iCCM medicines and diagnostics in stock on day of assessment (LA, amoxicillin, ORS, zinc, RDTs, timer)
60% (28/47) (95% CI: 45%-73%)
LA (1x6) 87%
LA (2x6) 79%
RDTs 89%
Amoxicillin 79%
ORS 79%
Zinc 83%
Timer 87%
Paracetemol 89%
Eye antibiotic ointment 68%

RAcE Endline Survey Final Report 77
Domain Indicator Result
Percentage of HSAs with all medicines and diagnostics in stock on the day of assessment (all above medicines and supplies)
40% (19/47) (95% CI: 27%-55%)
Percentage of HSAs reporting no stockouts of essential iCCM supplies lasting seven days or more in the month before the survey (LA 1x6 and 2x6, RDTs, amoxicillin, ORS, zinc)
64% (30/47) (95% CI: 49%-77%)
LA (1x6) 83%
LA (2x6) 79%
RDTs 87%
Amoxicillin 75%
ORS 79%
Zinc 81%
Percentage of HSAs reporting no stockouts of all iCCM medicines and supplies lasting seven days or more in the month before the survey
47% (22/47) (95% CI: 33%-61%)
Percentage of HSAs who referred sick child cases due to medicine stockouts in the last one month (based on register review)
13% (95% CI: 6%-26%) Mean: 1.5 cases Range: 0-30 cases
Supervision Percentage of HSAs who received at least one supervision session during the prior three months during which registers were reviewed
66% (31/47) (95% CI: 51%-78%)
A. Review your treatment register? 97%
B. Check your supplies and equipment levels? 97%
C. Use a supervision checklist? 100%
D. Administer a case scenario? 84%
E. Observe you manage a sick child? 72%
F. Observe an mRDT being performed? 72%
G. Meet with village leaders? 56%
H. Give you feedback on your CCM activities? 97%
Percentage of HSAs who received at least one mentorship session during the prior three months with observation of case management (clinical supervision)
55% (26/47) (95% CI: 41%-69%)
Service availability and activity levels
Percentage of HSAs who report typically operating their village clinic:
i) Less than two days per week 6%
ii) Two or more days per week 94%
iii) Five or more days per week 26%
Number of days HSAs report operating village clinic per week Mean: 3.3 Median: 2.0
Percentage of HSAs who report typically operating their village clinic:
i) Less than eight days in the past month 34%
ii) Eight or more days in the past month 66%
iii) 16 or more days in the past month 32%
Number of days HSAs report operating village clinic per month Mean: 12.8 Median: 10.0
Number of days HSAs report working from health facility in last month Mean: 5.5 Median: 4.0
Number of sick child cases treated in the last one month Mean: 43.5 Median: 37.0 Range: 0-220
Percentage of HSAs who referred one or more sick child cases for danger signs in the last one month
36% (17/47) (95% CI: 23%-51%) Mean: 0.5 cases Range: 0-3 cases
Recording completeness
Percentage of HSAs with complete recording for use of mRDTs for five most recent cases presenting with fever
91% (43/47) (95% CI: 79%-97%)
Percentage of HSAs with complete recording of respiratory rate for five most recent cases presenting with cough/difficult breathing
85% (40/47) (95% CI: 71%-93%)
Data display and use
Percentage of HSAs who were trained on the data use display package and received data use templates 51% (24/47)

RAcE Endline Survey Final Report 78
Domain Indicator Result
Percentage of HSAs trained in the package who report using the templates and can show completed templates for the last three completed months 33% (13/34)
Percentage of HSAs trained in the package who have the data use templates displayed where can be easily seen (e.g., on wall or other visible location) 29% (10/34)
Percentage of HSAs trained in the package who give one or more examples of how they use the data N/A
N/A = not available