
Endemic and Epidemic Acinetobacter Species in a University Hospital
7
JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2009, p. 3593–3599 Vol. 47, No. 11 0095-1137/09/$12.00 doi:10.1128/JCM.00967-09 Copyright © 2009, American Society for Microbiology. All Rights Reserved. Endemic and Epidemic Acinetobacter Species in a University Hospital: an 8-Year Survey P. J. van den Broek, 1 * T. J. K. van der Reijden, 1 E. van Strijen, 1 A. V. Helmig-Schurter, 1 A. T. Bernards, 2 and L. Dijkshoorn 1 Department of Infectious Diseases, Leiden University Medical Centre, Leiden, The Netherlands, 1 and Department of Medical Microbiology, Leiden University Medical Centre, Leiden, The Netherlands 2 Received 15 May 2009/Returned for modification 13 July 2009/Accepted 18 September 2009 The prevalence of the currently known Acinetobacter species and related trends of antimicrobial resistance in a Dutch university hospital were studied. Between 1999 and 2006, Acinetobacter isolates from clinical samples were collected prospectively. Isolates were analyzed by amplified fragment length polymorphism fingerprinting. For species identification, a profile similarity cutoff level of 50% was used, and for strain identification, a cutoff level of 90% was used. Susceptibility for antimicrobial agents was tested by disk diffusion by following the CLSI guideline. The incidences of Acinetobacter isolates ranged from 1.7 to 3.7 per 10,000 patients per year, without a trend of increase, during the study years. Twenty different species were distinguished. Acinetobacter baumannii (27%) and Acinetobacter genomic species (gen. sp.) 3 (26%) were the most prevalent. Other species seen relatively frequently were Acinetobacter lwoffii (11%), Acinetobacter ursingii (4%), Acinetobacter johnsonii (4%), and Acin- etobacter junii (3%). One large cluster of A. baumannii, involving 31 patients, and 16 smaller clusters of various species, involving in total 39 patients, with at most 5 patients in 1 cluster, occurred. Overall, 37% of the A. baumannii isolates were fully susceptible to the tested antibiotics. There was a borderline significant (P 0.059) trend of decreasing susceptibility. A. baumannii was the Acinetobacter species causing the largest burden of multiple-antibiotic resistance and transmissions in the hospital. More than 30 named and unnamed species of Acinetobacter have been described (14), some of which are of clinical impor- tance, including A. baumannii, Acinetobacter gen. sp. 3, and Acinetobacter gen. sp. 13TU, while other species, like A. junii, A. johnsonii, A. ursingii, and Acinetobacter schindleri, can also incidentally be associated with infections (8). Much attention has been paid to outbreaks caused by acinetobacters (28), which in most cases are caused by A. baumannii (15, 23). Notably, in diagnostic microbiology, isolates identified as A. baumannii may also include the closely related species Acin- etobacter gen. sp. 3 or Acinetobacter gen. sp. 13TU. Bacteria belonging to other Acinetobacter species are frequently not further identified as or designated Acinetobacter species, as this would require genotypic methods that are usually not available in clinical diagnostic microbiology. These difficulties in identi- fication explain why, overall, not much is known about the occurrences of the different Acinetobacter species in the hos- pital. The aim of the present study was to determine the preva- lences of the currently known Acinetobacter species and related trends of antimicrobial resistance in our hospital through the years. To this aim, we identified all available Acinetobacter isolates obtained from our hospital in the period between 1999 and 2006 to the species level by amplified fragment length polymorphism (AFLP) analysis, a well-validated method for Acinetobacter species identification (7, 8). Furthermore, we tested the susceptibilities of the isolates to antibiotics and used AFLP analysis to assess strain relatedness as an indication of transmission of strains in the hospital. MATERIALS AND METHODS Setting. The study was performed in the Leiden University Medical Centre, The Netherlands, between 1999 and 2006. In 2006, the hospital had 18,908 admissions, with a mean duration of stay of 7.5 days and a total of 141,128 patient-days. In addition, for the purpose of day care, 11,957 patients were admitted. Isolates. Acinetobacter strains were isolated from clinical specimens in the diagnostic microbiology laboratory of the hospital. Identification of the organ- isms as belonging to the genus Acinetobacter or, presumptively, as Acinetobacter species was done with the Vitek 2 system (bioMerieux, Boxtel, The Netherlands). For each patient, each colony morphotype possibly representing a unique strain was analyzed by AFLP typing (see below), and depending on the outcome, each unique strain per patient was included. Isolates were collected prospectively and stored at minus 80°C in glycerol broth. Isolates were classified as hospital related when the specimen from which the organism was cultured was taken during the stay in the hospital or within 14 days after discharge of the patient from the hospital. AFLP analysis for species and strain identification. Selective amplification of genomic restriction fragments by AFLP was performed as described previously (12). Briefly, purified DNA was digested using EcoRI and MseI, and amplifica- tion was done with a Cy5-labeled EcoRIA primer and an MseIC primer (A and C are selective bases). The ALF express II DNA analysis system (Amersham Biosciences, Roosendaal, The Netherlands) was used for fragment separation. The fingerprints of fragments of 50 to 500 bp were investigated by cluster analysis using the Bionumerics 4.5 software package (Applied Maths, Sint-Martens- Latem, Belgium), with the Pearson product moment coefficient (r) as a similarity measure and the unweighted-pair group method using arithmetic averages for grouping. For species identification, isolates were compared to a library of strains of all described (genomic) species, using a similarity cutoff level of 50%, above which strains were considered to belong to the same species (7, 12). Isolates were considered to belong to the same clone or strain if they grouped together at a level greater than or equal to 80% or 90%, respectively (7). * Corresponding author. Mailing address: Department of Infectious Diseases, C5-P, P.O. Box 9600, 2300 RC Leiden, The Netherlands. Phone: 0031715262290. Fax: 0031715266758. E-mail: p.j.van_den_broek @lumc.nl. Published ahead of print on 30 September 2009. 3593 Downloaded from https://journals.asm.org/journal/jcm on 21 November 2021 by 46.16.122.189.
Transcript of Endemic and Epidemic Acinetobacter Species in a University Hospital

JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2009, p. 3593–3599 Vol. 47, No. 110095-1137/09/$12.00 doi:10.1128/JCM.00967-09Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Endemic and Epidemic Acinetobacter Species in aUniversity Hospital: an 8-Year Survey�
P. J. van den Broek,1* T. J. K. van der Reijden,1 E. van Strijen,1 A. V. Helmig-Schurter,1A. T. Bernards,2 and L. Dijkshoorn1
Department of Infectious Diseases, Leiden University Medical Centre, Leiden, The Netherlands,1 and Department ofMedical Microbiology, Leiden University Medical Centre, Leiden, The Netherlands2
Received 15 May 2009/Returned for modification 13 July 2009/Accepted 18 September 2009
The prevalence of the currently known Acinetobacter species and related trends of antimicrobial resistancein a Dutch university hospital were studied. Between 1999 and 2006, Acinetobacter isolates from clinical sampleswere collected prospectively. Isolates were analyzed by amplified fragment length polymorphism fingerprinting.For species identification, a profile similarity cutoff level of 50% was used, and for strain identification, a cutofflevel of 90% was used. Susceptibility for antimicrobial agents was tested by disk diffusion by following the CLSIguideline.
The incidences of Acinetobacter isolates ranged from 1.7 to 3.7 per 10,000 patients per year, without a trendof increase, during the study years. Twenty different species were distinguished. Acinetobacter baumannii (27%)and Acinetobacter genomic species (gen. sp.) 3 (26%) were the most prevalent. Other species seen relativelyfrequently were Acinetobacter lwoffii (11%), Acinetobacter ursingii (4%), Acinetobacter johnsonii (4%), and Acin-etobacter junii (3%). One large cluster of A. baumannii, involving 31 patients, and 16 smaller clusters of variousspecies, involving in total 39 patients, with at most 5 patients in 1 cluster, occurred. Overall, 37% of the A.baumannii isolates were fully susceptible to the tested antibiotics. There was a borderline significant (P �0.059) trend of decreasing susceptibility. A. baumannii was the Acinetobacter species causing the largest burdenof multiple-antibiotic resistance and transmissions in the hospital.
More than 30 named and unnamed species of Acinetobacterhave been described (14), some of which are of clinical impor-tance, including A. baumannii, Acinetobacter gen. sp. 3, andAcinetobacter gen. sp. 13TU, while other species, like A. junii,A. johnsonii, A. ursingii, and Acinetobacter schindleri, can alsoincidentally be associated with infections (8). Much attentionhas been paid to outbreaks caused by acinetobacters (28),which in most cases are caused by A. baumannii (15, 23).Notably, in diagnostic microbiology, isolates identified as A.baumannii may also include the closely related species Acin-etobacter gen. sp. 3 or Acinetobacter gen. sp. 13TU. Bacteriabelonging to other Acinetobacter species are frequently notfurther identified as or designated Acinetobacter species, as thiswould require genotypic methods that are usually not availablein clinical diagnostic microbiology. These difficulties in identi-fication explain why, overall, not much is known about theoccurrences of the different Acinetobacter species in the hos-pital.
The aim of the present study was to determine the preva-lences of the currently known Acinetobacter species and relatedtrends of antimicrobial resistance in our hospital through theyears. To this aim, we identified all available Acinetobacterisolates obtained from our hospital in the period between 1999and 2006 to the species level by amplified fragment lengthpolymorphism (AFLP) analysis, a well-validated method forAcinetobacter species identification (7, 8). Furthermore, we
tested the susceptibilities of the isolates to antibiotics and usedAFLP analysis to assess strain relatedness as an indication oftransmission of strains in the hospital.
MATERIALS AND METHODS
Setting. The study was performed in the Leiden University Medical Centre,The Netherlands, between 1999 and 2006. In 2006, the hospital had 18,908admissions, with a mean duration of stay of 7.5 days and a total of 141,128patient-days. In addition, for the purpose of day care, 11,957 patients wereadmitted.
Isolates. Acinetobacter strains were isolated from clinical specimens in thediagnostic microbiology laboratory of the hospital. Identification of the organ-isms as belonging to the genus Acinetobacter or, presumptively, as Acinetobacterspecies was done with the Vitek 2 system (bioMerieux, Boxtel, The Netherlands).For each patient, each colony morphotype possibly representing a unique strainwas analyzed by AFLP typing (see below), and depending on the outcome, eachunique strain per patient was included. Isolates were collected prospectively andstored at minus 80°C in glycerol broth.
Isolates were classified as hospital related when the specimen from which theorganism was cultured was taken during the stay in the hospital or within 14 daysafter discharge of the patient from the hospital.
AFLP analysis for species and strain identification. Selective amplification ofgenomic restriction fragments by AFLP was performed as described previously(12). Briefly, purified DNA was digested using EcoRI and MseI, and amplifica-tion was done with a Cy5-labeled EcoRI�A primer and an MseI�C primer (Aand C are selective bases). The ALF express II DNA analysis system (AmershamBiosciences, Roosendaal, The Netherlands) was used for fragment separation.The fingerprints of fragments of 50 to 500 bp were investigated by cluster analysisusing the Bionumerics 4.5 software package (Applied Maths, Sint-Martens-Latem, Belgium), with the Pearson product moment coefficient (r) as a similaritymeasure and the unweighted-pair group method using arithmetic averages forgrouping. For species identification, isolates were compared to a library of strainsof all described (genomic) species, using a similarity cutoff level of 50%, abovewhich strains were considered to belong to the same species (7, 12). Isolates wereconsidered to belong to the same clone or strain if they grouped together at alevel greater than or equal to 80% or 90%, respectively (7).
* Corresponding author. Mailing address: Department of InfectiousDiseases, C5-P, P.O. Box 9600, 2300 RC Leiden, The Netherlands.Phone: 0031715262290. Fax: 0031715266758. E-mail: [email protected].
� Published ahead of print on 30 September 2009.
3593
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.

Susceptibility testing. Resistance to 12 antimicrobial agents or combinationsof agents which are effective against susceptible A. baumannii strains wasdetermined by disk diffusion by following the CLSI guidelines. The semiau-tomated Biomic image analysis system, release 2005 (Giles Scientific, Inc.,New York, NY), was used to read and interpret zone sizes. The controlstrains were Escherichia coli ATCC 35218, E. coli 25922, Enterococcus faecalisATCC 29212, and Acinetobacter strains LUH 4624 and LUH 4576, receivedfrom A. Nemec (National Institute Public Health, Prague, Czech Republic).Bacterial isolates were suspended in 2 ml saline to a turbidity correspondingto a 0.5 McFarland standard. The agents (Oxoid) (values in parenthesesrepresent content levels [�g/disc], susceptibility breakpoints [mm], and resis-tance breakpoints [mm], in that order) were gentamicin (10, �15, and �12),netilmicin (30, �15, and �12), tobramycin (10, �15, and �12), amikacin(30, �17, and �14), ampicillin and sulbactam (10 and 10, respectively; �15;and �11), piperacillin (100, �21, and �17), ceftazidime (30, �18, and �14),meropenem (10, �16, and �13), imipenem (10, �16, and �13), ofloxacin(5, �16, and �12), sulfamethoxazole and trimethoprim (23.75 and 1.25,respectively; �16; and �10), and tetracycline (30, �19, and �14). The plateswere incubated 24 h at 37°C and then read by using the Biomic system. Thecategory of susceptibility was determined from the zones of inhibition assusceptible, intermediate, or resistant. Trends in susceptibility over the yearswere analyzed by the chi-square test, with linear-by-linear association, usingthe statistical package SPSS.
RESULTS
Patients. During the years 1999 to 2006, the numbers ofpatients with hospital-related Acinetobacter spp. varied be-tween 28 and 58 (Table 1). The incidences ranged from 1.7 to3.7 per 10,000 patient-days and were highest in 2001, 2003, and2005. In 2001, an Acinetobacter baumannii cluster that startedin November 2000 and lasted until October 2001 dominated.The cluster involved 31 patients (23). When the patients be-longing to the cluster were omitted, the incidence was found to
be 2.3 per 10,000 patient-days for both years. Apart from thisbig cluster, the years 2003 and 2005 were distinguished byrelatively high numbers of secondary cases, defined as clustersof two or more patients with the same genotype at the sameperiod at the same ward. Four small clusters of transmission,involving totals of nine and eight patients in 2003 and 2005,respectively, were observed. After correction for the secondarycases of these clusters, the incidences in 2003 and 2005 were3.0 and 3.3 per 10,000 patient-days, respectively.
The ratio of men to women was 1.6, varying from 1.1 to 2.7.The mean ratio of men to women admitted to the hospitalduring the study years was 0.96 (range, 0.91 to 1), indicatingthat Acinetobacter is seen more often in men than in women.The median ages of the patients per year ranged from 47 to 52years. The youngest patients were newborns a few days old inthe neonatology intensive care unit. The oldest patient was 91years old. Forty-six percent of the patients were admitted toone of the intensive care units of the hospital. Next in fre-quency were patients from the departments of urology andhematology.
Acinetobacter isolates. Of the 365 patients with documentedAcinetobacter cultures, isolates from 331 patients were avail-able for further investigation. If multiple isolates per patientwere available, the first isolate of a series of samples from eachpositive body site was taken for study. If patients had recurrentepisodes of positive cultures, the first sample of each periodwas studied. For each patient, isolates were compared byAFLP analysis for strain relatedness (similarity, �90%) and,next, replicate isolates were excluded. All together, a total of
TABLE 1. Overview of hospital-related Acinetobacter isolates in 331 patients
ParameterValue for indicated yr
1999 2000 2001 2002 2003 2004 2005 2006
No. of patients 28 49 58 36 54 46 57 37No. of patients/10,000 patient-daysa 1.7 2.9 3.7 2.3 3.5 2.9 3.7 2.4No. of secondary casesb 2 11 21 1 8 2 7 1No. of patients with isolate(s) typeda 22 47 51 24 52 43 56 36No. of single strains 25 48 56 25 59 45 61 40
A. baumannii 5 23 29 5 20 11 23 13A. junii 3 4 2 2 1A. ursingii 1 4 1 1 2 2 2 2A. lwoffii 1 1 8 2 10 3 9 4Acinetobacter gen. sp. 13TU 1 1 2 3 1 1Acinetobacter gen. sp. “close to 13TU” 1Acinetobacter gen. sp. 15TU 1 2Acinetobacter gen. sp. 3 4 12 8 10 15 16 14 14A. radioresistens 1 2 1A. calcoaceticus 1 1 2 1 1Acinetobacter gen. sp. 10 2 1 1Acinetobacter gen. sp. 11 1 1 1 1A. johnsonii 2 1 3 1 3 3A. haemolyticus 1 2A. gyllenbergii 1 1Acinetobacter gen. sp. 14BJ 1 1 1Acinetobacter gen. sp. “between 1 and 3” 1A. beijerinckii 2 3A. parvus 1Acinetobacter gen. sp. 16 1Unidentified 2 4 2 2 2
a Secondary cases were included.b Secondary cases are defined as patients with the same genotype at the same period at the same ward.
3594 VAN DEN BROEK ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.

359 single strains were found in the 331 patients (including thesecondary cases, i.e., patients with the same AFLP type in thesame period and ward).
At the species cutoff level of 50% (Fig. 1), as determined byAFLP analysis, 20 different species were distinguished (Table1), whereas 12 isolates could not be identified. The most prev-alent species were A. baumannii (27%, with the large clusternot included) and Acinetobacter gen. sp. 3 (26%) (Table 1).Other species seen relatively frequently were A. lwoffii (11%),A. ursingii (4%), A. johnsonii (4%), and A. junii (3%).
Thirty-two percent of the 359 single strains were isolatedfrom airway secretions, 16% from wounds and wound drains,15% from blood or intravascular lines, and 9% from urine. A.baumannii and Acinetobacter gen. sp. 3 were most frequentlyisolated from sputum samples (48 and 32%, respectively) andwound samples (19 and 18%, respectively). A. lwoffii wasmainly isolated from blood samples or intravascular lines(42%).
Inspection of AFLP profiles for possible strain relatedness(�90%) showed a number of clusters possibly indicative of
FIG. 1. Dendrogram of cluster analysis of AFLP profiles of sets of strains possibly involved in transmission. The horizontal axis represents thesimilarity level at which strains are grouped. This level is determined by Pearson’s product moment correlation coefficient. Grouping was obtainedby the unweighted-pair group method using average linkages. Similarity levels of 50% and 90% (dotted lines) are considered to represent thespecies and strain cutoff levels, respectively. “Ungrouped 1” and “ungrouped 2” represent strains that could not be identified as the described(genomic) species. Strains marked in gray represent a prolonged cluster in the hospital. Opt, optimization (shift allowed between any two patternsfor the best possible matching).
VOL. 47, 2009 ENDEMIC AND EPIDEMIC ACINETOBACTER SPP. IN A HOSPITAL 3595
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.
transmission, a subset of which is shown in Fig. 1. Apart fromthe large cluster of A. baumannii in 31 patients observed in2000 and 2001, 16 small clusters of isolates involving 39 pa-tients were observed. Nine of the clusters involved A. bauman-nii; two clusters A. ursingii and Acinetobacter gen. sp. 3; and onecluster Acinetobacter gen. sp. 13TU, Acinetobacter gen. sp. 10,and Acinetobacter beyerinckii. Twelve clusters involved two pa-tients, two clusters three patients, one cluster four patients,and one cluster five patients. Two clusters (the big clusterobserved in 2000 and 2001 and a smaller cluster observed in2003) were recognized while occurring. The other clusters wereidentified through the investigations of the present study.
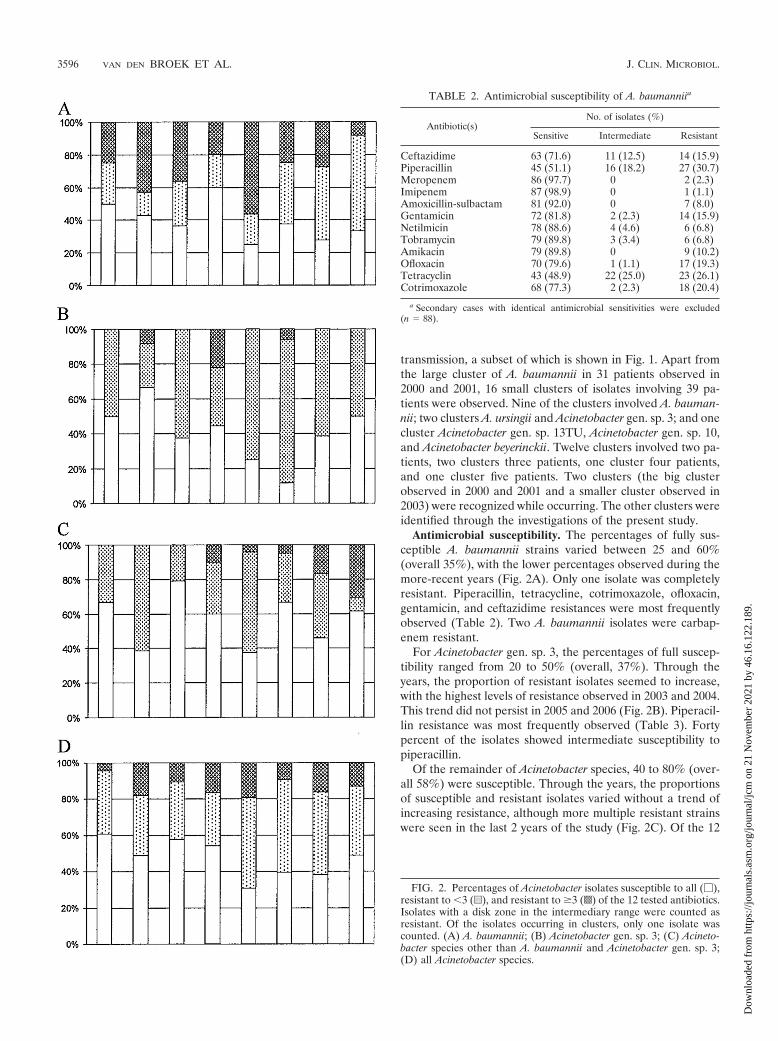
Antimicrobial susceptibility. The percentages of fully sus-ceptible A. baumannii strains varied between 25 and 60%(overall 35%), with the lower percentages observed during themore-recent years (Fig. 2A). Only one isolate was completelyresistant. Piperacillin, tetracycline, cotrimoxazole, ofloxacin,gentamicin, and ceftazidime resistances were most frequentlyobserved (Table 2). Two A. baumannii isolates were carbap-enem resistant.
For Acinetobacter gen. sp. 3, the percentages of full suscep-tibility ranged from 20 to 50% (overall, 37%). Through theyears, the proportion of resistant isolates seemed to increase,with the highest levels of resistance observed in 2003 and 2004.This trend did not persist in 2005 and 2006 (Fig. 2B). Piperacil-lin resistance was most frequently observed (Table 3). Fortypercent of the isolates showed intermediate susceptibility topiperacillin.
Of the remainder of Acinetobacter species, 40 to 80% (over-all 58%) were susceptible. Through the years, the proportionsof susceptible and resistant isolates varied without a trend ofincreasing resistance, although more multiple resistant strainswere seen in the last 2 years of the study (Fig. 2C). Of the 12
FIG. 2. Percentages of Acinetobacter isolates susceptible to all (�),resistant to �3 (u), and resistant to �3 (s) of the 12 tested antibiotics.Isolates with a disk zone in the intermediary range were counted asresistant. Of the isolates occurring in clusters, only one isolate wascounted. (A) A. baumannii; (B) Acinetobacter gen. sp. 3; (C) Acineto-bacter species other than A. baumannii and Acinetobacter gen. sp. 3;(D) all Acinetobacter species.
TABLE 2. Antimicrobial susceptibility of A. baumanniia
Antibiotic(s)No. of isolates (%)
Sensitive Intermediate Resistant
Ceftazidime 63 (71.6) 11 (12.5) 14 (15.9)Piperacillin 45 (51.1) 16 (18.2) 27 (30.7)Meropenem 86 (97.7) 0 2 (2.3)Imipenem 87 (98.9) 0 1 (1.1)Amoxicillin-sulbactam 81 (92.0) 0 7 (8.0)Gentamicin 72 (81.8) 2 (2.3) 14 (15.9)Netilmicin 78 (88.6) 4 (4.6) 6 (6.8)Tobramycin 79 (89.8) 3 (3.4) 6 (6.8)Amikacin 79 (89.8) 0 9 (10.2)Ofloxacin 70 (79.6) 1 (1.1) 17 (19.3)Tetracyclin 43 (48.9) 22 (25.0) 23 (26.1)Cotrimoxazole 68 (77.3) 2 (2.3) 18 (20.4)
a Secondary cases with identical antimicrobial sensitivities were excluded(n � 88).
3596 VAN DEN BROEK ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.

multiple-resistant strains, 6 were identified as A. ursingii. Fortypercent of the A. ursingii isolates were multiple resistant, com-pared to 15% of the A. Johnsonii isolates and none of the A.junii isolates.
Overall, 82 isolates (23%) were multiresistant, defined asresistant to three or more antibiotics. Sixty-five of these 82multiresistant isolates were A. baumannii. For all Acinetobacterisolates together, there was a borderline significant trend (P �0.059) of decreasing susceptibility between 1999 and 2006. ForA. baumannii (P � 0.302), Acinetobacter gen. sp. 3 (P � 0.225),and the other Acinetobacter species (P � 0.46), analyzed sep-arately, no trend was demonstrated.
Comparison of isolates with European clones I to III. Pre-vious studies have shown that three major groups of highlysimilar strains which are considered to represent three lineagesof descent (European clones I to III) occur among epidemicstrains of A. baumannii in Europe (6, 13, 24). These studieshave shown that strains of these clones can be separated byAFLP profiling, with �80% being considered the cutoff level,above which strains are considered to belong to the sameclone. In the current study, we compared the AFLP profiles ofthe A. baumannii strains to those of sets of strains of the threeclones available in the Leiden University Medical Center cul-ture collection. Thus, five isolates from 2003 were identified asbelonging to European clone I (data not shown). These iso-lates showed a high level of similarity to each other (�95%)and were from the same time-space frame, indicating epidemicspread. Five other isolates were identified as belonging toEuropean clone II; two of these, obtained in 1999, were con-sidered to represent a common strain that had spread betweentwo patients (data not shown). Altogether, strains of the Eu-ropean clones were relatively rare among the A. baumanniistrains of our study.
DISCUSSION
The present study shows that through the years, the inci-dences of patients with an Acinetobacter isolate from a clinicalspecimen varied in our hospital under conditions of endemicitybetween 1.7 and 3.7 per 10.000 patient-days with secondarycases included and between 1.7 and 3.3 with secondary cases
excluded. Between 1999 and 2006, the incidences showed notrend of increase.
Acinetobacter was found half as frequently in men as inwomen. A small study of Acinetobacter anitratus blood cultureisolates reported a male/female ratio of 2.7:1 (16). Our studysubstantiates the overrepresentation of men, which is not ex-plained by a higher admission rate. The opposite is true;slightly more women than men are admitted to our hospital.
A variety of species was found. Only a quarter of the isolateswere A. baumannii. Acinetobacter gen. sp. 3 was seen as oftenas A. baumannii.
Three-quarters of the isolates belonged to species known tobe associated with infections in humans. Next to A. baumanniiand Acinetobacter gen. sp. 3, these are A. junii (2), A. ursingii (5,12), Acinetobacter gen. sp. 13TU (11, 25), and A. johnsonii (18).A. lwoffii, a well-known colonizer of the human skin, made up11% of the isolates. It was frequently found on tips of intra-vascular catheters and in blood cultures. The question iswhether this must be considered contamination of the culturesor represents infection.
Only a few studies have investigated the distribution of acin-etobacters in clinical specimens at the species level, and con-siderable differences in outcome have been reported. For ex-ample, our data differ from the observations made by Struelenset al. (20) in a Belgian hospital. Under circumstances of ende-micity, about half of their Acinetobacter isolates were identifiedas A. baumannii, twice as many as we found. Acinetobacter gen.sp. 3 was found in 5% of their isolates, compared to 24% in oursurvey. This inconsistency may be explained either by the useof biweekly surveillance cultures in the Belgian study or by theuse of different methods for species identification. We usedAFLP analysis, a well-validated method for species identifica-tion (8), while Struelens et al. used the phenotypic systemdeveloped by Bouvet and Grimont (4). It is of note that theidentification of Acinetobacter gen. sp. 3 with this system is notperfect (65%) (9). Seifert et al. (17), also using the system ofBouvet and Grimont, identified 73% of the Acinetobacter iso-lates from clinical samples as A. baumannii. Acinetobacter gen.sp. 3 was found in 9%, A. johnsonii in 5%, and A. lwoffii in 4%of the isolates.
Traub and Bauer (22) identified 45% of 2,359 clinical iso-lates of Acinetobacter as gen. sp. 3, 15% as gen. sp. 13, and 14%as A. baumannii by phenotypic identification. The origin oftheir isolates is not described, and therefore, it is not clearwhether their collection is representative of the situation ofendemicity or concerns a selection of strains.
Tjernberg and Ursing (21), who used DNA-DNA hybridiza-tion, a robust method for species identification, also found apredominance of Acinetobacter gen. sp. 3 among consecutiveclinical Acinetobacter isolates in a Swedish hospital. In a recentstudy from Ireland, Acinetobacter gen. sp. 3 was the most fre-quent species found, representing 39% of 114 isolates over a30-month period (3). A. baumannii was second, with 22%. ForA. baumannii, our findings are in line with this Irish study;however, for Acinetobacter gen. sp. 3, the difference is consid-erable. Whether these differences are due to geographic, meth-odological, or epidemiological differences between the studiesis hard to say.
Antimicrobial resistance is one of the major problems asso-ciated with Acinetobacter. In our survey, resistance was evi-
TABLE 3. Antimicrobial susceptibilities of Acinetobacter gen. sp. 3a
Antibiotic(s)No. of isolates (%)
Sensitive Intermediate Resistant
Ceftazidime 83 (93.3) 5 (5.6) 1 (1.1)Piperacillin 41 (46.1) 36 (40.4) 12 (13.5)Meropenem 89 (100) 0 0Imipenem 89 (100) 0 0Amoxicillin-sulbactam 89 (100) 0 0Gentamicin 85 (95.5) 0 4 (4.5)Netilmicin 85 (95.5) 2 (2.2) 2 (2.2)Tobramycin 88 (98.9) 0 1 (1.1)Amikacin 87 (97.8) 2 (2.2) 0Ofloxacin 88 (98.9) 0 1 (1.1)Tetracyclin 76 (85.4) 9 (10.1) 4 (4.5)Cotrimoxazole 89 (100) 0 0
a Secondary cases with identical antimicrobial sensitivities were excluded(n � 89).
VOL. 47, 2009 ENDEMIC AND EPIDEMIC ACINETOBACTER SPP. IN A HOSPITAL 3597
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.

dently present, although not at the scale often reported (27).Multiple resistance, defined as resistance to three or moreantibiotics, occurred predominantly in A. baumannii. Carbap-enem resistance was seen in only two of the A. baumanniiisolates. A likely explanation for the relatively low level ofresistant Acinetobacter isolates in the hospital is the restricteduse of antibiotics, which is in line with the Dutch practiceregarding antimicrobial therapy, the strict isolation of patientswith multiresistant isolates, and the immediate beginning ofinfection control measures when several patients are infectedwith the same strain.
During the 8 years of our survey, one large cluster of A.baumannii involving 31 patients occurred. Fifteen smaller clus-ters were seen, most of them caused by A. baumannii. A varietyof other species were involved: Acinetobacter gen. sp. 3, Acin-etobacter gen. sp. 10, Acinetobacter gen. sp. 13TU, and thenovel species A. beyerinckii (14). Although A. baumannii andAcinetobacter gen. sp. 3 clinical isolates were found in almostequal numbers, the former species was involved in nine clus-ters, among which the largest clusters occurred, and Acineto-bacter gen. sp. 3 was observed in only two small clusters, in-volving a total of five patients. Outbreaks caused by A.baumannii are well known and get a lot of attention in theliterature (15, 23). Outbreaks caused by other species havebeen reported much less often (1, 10, 25, 26), which may, inpart, be due to underreporting. Indeed, identification of Acin-etobacter isolates to the species level, as we did in the presentstudy, is not usual in routine microbiological diagnostics. TheVitek 2 system is unreliable for species identification of Acin-etobacter (3). The question is whether speciation should bedone routinely. Easy methods for species identification do notexist, so the costs of species identification should be out-weighed by the benefit of it for the management of patientsand the timely institution of control measures. For daily prac-tice, the relevance of knowing the species is limited. Treatmentis primarily determined by the susceptibility pattern of theisolate and not by the species to which it belongs. This may bedifferent for infection control measures. In The Netherlands, itis common practice to put patients infected by multiresistantbacteria in strict isolation, for which an isolation room isneeded in the case of A. baumannii. Patients infected by spe-cies with a lower risk of transmission can be treated with lessradical precautions, like contact isolation (see WIP [www.wip.nl/], a guideline for highly resistant microorganisms). This is inthe interest of the patients because nursing in isolation roomsis accompanied by inferior care (19). The results of the presentstudy show that the majority of the multidrug-resistant Acin-etobacter isolates are A. baumannii. Therefore, identification atthe species level will have a minor impact on isolation ofpatients infected with multiresistant Acinetobacter. Speciesidentification is indispensable for analysis of outbreaks. Thetypes of measures differ, dependent on whether multiple spe-cies are found or different strains of one species or a singlestrain of one species is involved (23).
Not many A. baumannii isolates that belonged to one of thethree major European clones were found (6, 24), but most ofthose found were associated with cross-infection, which em-phasizes the epidemiological potential of these clones. Four ofthe eight secondary cases observed in 2003 were due to clone
I. Clone II was observed five times, one of which involved asecondary case.
In conclusion, we found that under endemic conditions, awide range of Acinetobacter species was isolated from clinicalsamples in our hospital. The incidence of Acinetobacter re-mained stable over the study years, while there was a border-line significant trend toward decreased susceptibility to anti-microbial drugs. Small clusters of transmission occurredregularly. A. baumannii was seen as often as Acinetobacter gen.sp. 3. Half of the isolates belonged to these two species. A.baumannii causes the largest burden of multiple antimicrobialresistance and transmissions in the hospital.
REFERENCES
1. Bernards, A. T., A. J. de Beaufort, L. Dijkshoorn, and C. P. van Boven. 1997.Outbreak of septicaemia in neonates caused by Acinetobacter junii investi-gated by amplified ribosomal DNA restriction analysis (ARDRA) and fourtyping methods. J. Hosp. Infect. 35:129–140.
2. Bernards, A. T., H. I. Harinck, L. Dijkshoorn, T. van der Reijden, and P. J.van den Broek. 2004. Persistent Acinetobacter baumannii? Look inside yourmedical equipment. Infect. Control Hosp. Epidemiol. 25:1002–1004.
3. Boo, T. W., F. Walsh, and B. Crowley. 2009. Molecular characterization ofcarbapenem-resistant Acinetobacter species in an Irish university hospital:predominance of Acinetobacter genomic species 3. J. Med. Microbiol. 58:209–216.
4. Bouvet, P. J. M., and P. A. D. Grimont. 1986. Taxonomy of the genusAcinetobacter with the recognition of Acinetobacter baumannii sp. nov., Acin-etobacter haemolyticus sp. nov., Acinetobacter johnsonii sp. nov., and Acineto-bacter junii sp. nov. and emended descriptions of Acinetobacter calcoaceticusand Acinetobacter lwoffii. Int. J. Syst. Bacteriol. 36:228–240.
5. de la Tabla Ducasse, V. O., C. M. Gonzalez, J. A. Saez-Nieto, and F. Guti-errez. 2008. First case of post-endoscopic retrograde cholangiopancreatog-raphy bacteraemia caused by Acinetobacter ursingii in a patient with choled-ocholithiasis and cholangitis. J. Med. Microbiol. 57:1170–1171.
6. Dijkshoorn, L., H. Aucken, P. Gerner-Smidt, P. Janssen, M. E. Kaufmann,J. Garaizar, J. Ursing, and T. L. Pitt. 1996. Comparison of outbreak andnonoutbreak Acinetobacter baumannii strains by genotypic and phenotypicmethods. J. Clin. Microbiol. 34:1519–1525.
7. Dijkshoorn, L., and A. Nemec. 2008. The diversity of the genus Acinetobacter,p. 1–34. In U. Gerischer (ed.), Acinetobacter molecular microbiology. CaisterAcademic Press, Norfolk, United Kingdom.
8. Dijkshoorn, L., A. Nemec, and H. Seifert. 2007. An increasing threat inhospitals: multidrug-resistant Acinetobacter baumannii. Nat. Rev. Microbiol.5:939–951.
9. Gerner-Smidt, P., I. Tjernberg, and J. Ursing. 1991. Reliability of pheno-typic tests for identification of Acinetobacter species. J. Clin. Microbiol.29:277–282.
10. Horrevorts, A., K. Bergman, L. Kollee, I. Breuker, I. Tjernberg, and L.Dijkshoorn. 1995. Clinical and epidemiological investigations of Acineto-bacter genomospecies 3 in a neonatal intensive care unit. J. Clin. Microbiol.33:1567–1572.
11. McDonald, A., S. G. Amyes, and R. Paton. 1999. The persistence and clonalspread of a single strain of Acinetobacter 13TU in a large Scottish teachinghospital. J. Chemother. 11:338–344.
12. Nemec, A., T. De Baere, I. Tjernberg, M. Vaneechoutte, T. van der Reijden,and L. Dijkshoorn. 2001. Acinetobacter ursingii sp. nov. and Acinetobacterschindleri sp. nov., isolated from human clinical specimens. Int. J. Syst. Evol.Microbiol. 51:1891–1899.
13. Nemec, A., L. Dijkshoorn, and T. van der Reijden. 2004. Long-term pre-dominance of two pan-European clones among multi-resistant Acinetobacterbaumannii strains in the Czech Republic. J. Med. Microbiol. 53:147–153.
14. Nemec, A., M. Mulisek, M. Maixnerova, T. De Baere, T. van der Reijden, M.Vaneechoutte, and L. Dijkshoorn. 2009. Acinetobacter beijerinckii sp. nov.and Acinetobacter gyllenbergii sp. nov., haemoytic organisms isolated fromhumans. Int. J. Syst. Evol. Microbiol. 59:1376–1381.
15. Peleg, A. Y., H. Seifert, and D. L. Paterson. 2008. Acinetobacter baumannii:emergence of a successful pathogen. Clin. Microbiol. Rev. 21:538–582.
16. Ramphal, R., and R. M. Kluge. 1979. Acinetobacter calcoaceticus varietyanitratus: an increasing nosocomial problem. Am. J. Med. Sci. 277:57–66.
17. Seifert, H., R. Baginski, A. Schulze, and G. Pulverer. 1993. The distributionof Acinetobacter species in clinical culture materials. Zentralbl. Bakteriol.279:544–552.
18. Seifert, H., A. Strate, A. Schulze, and G. Pulverer. 1993. Vascular catheter-related bloodstream infection due to Acinetobacter johnsonii (formerly Acin-etobacter calcoaceticus var. lwoffi): report of 13 cases. Clin. Infect. Dis.17:632–636.
3598 VAN DEN BROEK ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.

19. Stelfox, H. T., D. W. Bates, and D. A. Redelmeier. 2003. Safety of patientsisolated for infection control. JAMA 290:1899–1905.
20. Struelens, M. J., E. Carlier, N. Maes, E. Serruys, W. G. Quint, and A. vanBelkum. 1993. Nosocomial colonization and infection with multiresistantAcinetobacter baumannii: outbreak delineation using DNA macrorestrictionanalysis and PCR-fingerprinting. J. Hosp. Infect. 25:15–32.
21. Tjernberg, I., and J. Ursing. 1989. Clinical strains of Acinetobacter classifiedby DNA-DNA hybridization. APMIS 97:595–605.
22. Traub, W. H., and D. Bauer. 2000. Surveillance of nosocomial cross-infec-tions due to three Acinetobacter genospecies (Acinetobacter baumannii,genospecies 3 and genospecies 13) during a 10-year observation period:serotyping, macrorestriction analysis of genomic DNA and antibiotic suscep-tibilities. Chemotherapy 46:282–292.
23. van den Broek, P. J., J. Arends, A. T. Bernards, E. De Brauwer, E. M.Mascini, T. van der Reijden, L. Spanjaard, E. A. Thewessen, A. van der Zee,J. H. van Zeijl, and L. Dijkshoorn. 2006. Epidemiology of multiple Acineto-bacter outbreaks in The Netherlands during the period 1999–2001. Clin.Microbiol. Infect. 12:837–843.
24. van Dessel, H., L. Dijkshoorn, T. van der Reijden, N. Bakker, A. Paauw, P.van den Broek, J. Verhoef, and S. Brisse. 2004. Identification of a newgeographically widespread multiresistant Acinetobacter baumannii clonefrom European hospitals. Res. Microbiol. 155:105–112.
25. van Dessel, H., T. E. Kamp-Hopmans, A. C. Fluit, S. Brisse, A. M. de Smet,L. Dijkshoorn, A. Troelstra, J. Verhoef, and E. M. Mascini. 2002. Outbreakof a susceptible strain of Acinetobacter species 13 (sensu Tjernberg andUrsing) in an adult neurosurgical intensive care unit. J. Hosp. Infect.51:89–95.
26. Vaneechoutte, M., A. Elaichouni, K. Maquelin, G. Claeys, A. VanLiedekerke, H. Louagie, G. Verschraegen, and L. Dijkshoorn. 1995. Com-parison of arbitrarily primed polymerase chain reaction and cell envelopeprotein electrophoresis for analysis of Acinetobacter baumannii and A. juniioutbreaks. Res. Microbiol. 146:457–465.
27. Van Looveren, M., and H. Goossens. 2004. Antimicrobial resistance of Acin-etobacter spp. in Europe. Clin. Microbiol. Infect. 10:684–704.
28. Villegas, M. V., and A. I. Hartstein. 2003. Acinetobacter outbreaks, 1977–2000. Infect. Control Hosp. Epidemiol. 24:284–295.
VOL. 47, 2009 ENDEMIC AND EPIDEMIC ACINETOBACTER SPP. IN A HOSPITAL 3599
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 21
Nov
embe
r 20
21 b
y 46
.16.
122.
189.









![Spatio-Temporal Analysis of Epidemic Phenomena Using the R ... · 4 surveillance: Spatio-Temporal Analysis of Epidemic Phenomena concept. Both the endemic o set ˆ [s][t] and the](https://static.fdocuments.net/doc/165x107/5ec51643ebbd507e821b3308/spatio-temporal-analysis-of-epidemic-phenomena-using-the-r-4-surveillance-spatio-temporal.jpg)








