
En Bloc Celiac Axis Resection for Pancreatic Cancer: … · 2020. 12. 9. · BACKGROUND: En bloc...
22
WESTERN SURGICAL ASSOCIATION ARTICLES En Bloc Celiac Axis Resection for Pancreatic Cancer: Classification of Anatomical Variants Based on Tumor Extent Mark J Truty, MD, MSc, FACS, Jill J Colglazier, MD, FACS, Bernardo C Mendes, MD, David M Nagorney, MD, FACS, Thomas C Bower, MD, FACS, Rory L Smoot, MD, FACS, Randall R DeMartino, MD, FACS, Sean P Cleary, MD, FACS, Gustavo S Oderich, MD, FACS, Michael L Kendrick, MD, FACS BACKGROUND: En bloc celiac axis resection (CAR) for pancreatic cancer is considered increasingly after mod- ern neoadjuvant chemotherapy (NAC). Appleby and distal pancreatectomy with CAR are anatomically inaccurate terms, as tumors can extend beyond celiac axis proper, requiring con- current resection of the proper hepatic artery and/or superior mesenteric artery. STUDY DESIGN: A 3-level classification for CAR (class 1, 2, or 3) was developed after retrospective review of an arterial resection database describing anatomical variants that dictate pancreatectomy-type, formal arterial revascularization, and gastric preservation. Perioperative and oncologic out- comes were assessed. RESULTS: Of 90 CARs for pancreatic cancer, 89% patients received NAC, 35% requiring chemother- apeutic switch. There were 41 class 1, 33 class 2, and 16 class 3 CARs, with arterial and venous revascularization performed 62% and 66%, respectively. Ninety-day mortality decreased to 4% in the last 50 cases (p ¼ 0.035); major morbidity was unchanged (55%). Any hepatic or gastric ischemia occurred in 20% and 10% patients, respectively, and arterial revascularization was protective. R0 resection rate (88%) was associated with chemoradiation (p ¼ 0.004). Median overall survival was 36.2 months, superior with NAC (8.0 vs. 43.5 months). Predictors of survival after NAC included chemotherapy duration, carbohydrate antigen 19-9 response, pathologic response, and lymph node status. Major pathologic response (p ¼ 0.036) and extended duration NAC (p ¼ 0.007) were independent predictors on multivariate analysis. CONCLUSIONS: Current terminology for CAR inadequately describes all operative variants. Our classification, based on the largest single-center series, allows complex operative planning and standardized reporting across institutions. Extent of arterial involvement determines pancreatectomy type, need for arterial revascularization, and likelihood of gastric preservation. Operative mortality has improved, morbidity remains significant, and survival favorable after extended NAC with associated pathologic responses; given these factors, CAR should only be considered in fit patients with objective NAC responses at specialized centers. (J Am Coll Surg 2020;231: 8e29. Ó 2020 The Authors. Published by Elsevier Inc. on behalf of the American College of Surgeons. This is an open access article under the CC BY-NC-ND license [http://creativecommons.org/licenses/by-nc-nd/4.0/].) A safe and margin negative operation is the surgeon’s pri- mary oncologic contribution to patients with nonmeta- static pancreatic adenocarcinoma (PDAC). The likelihood of clear margins decreases with increased locoregional extra-anatomic extension of the primary tu- mor to involve critical vascular structures. The American Disclosure Information: Nothing to disclose. Presented at the Western Surgical Association 127th Scientific Session, Las Vegas, NV, November 2019. Received March 16, 2020; Revised May 4, 2020; Accepted May 4, 2020. From the Division of Hepatobiliary and Pancreas Surgery (Truty, Nagor- ney, Smoot, Cleary, Kendrick) and Division of Vascular Surgery (Colglazier, Mendes, Bower, DeMartino, Oderich), Mayo Clinic College of Medicine, Rochester, MN. Correspondence address: Mark J Truty, MD, MSc, FACS, Division of Hepatobiliary and Pancreas Surgery, Mayo Clinic College of Medicine, 200 First St SW, Rochester, MN 55902. email: [email protected] 8 ª 2020 The Authors. Published by Elsevier Inc. on behalf of the American College of Surgeons. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). https://doi.org/10.1016/j.jamcollsurg.2020.05.005 ISSN 1072-7515/20
Transcript of En Bloc Celiac Axis Resection for Pancreatic Cancer: … · 2020. 12. 9. · BACKGROUND: En bloc...

WESTERN SURGICAL ASSOCIATION ARTICLES
En Bloc Celiac Axis Resection forPancreatic Cancer: Classification ofAnatomical Variants Based on Tumor Extent
Mark J Truty, MD, MSc, FACS, Jill J Colglazier, MD, FACS, Bernardo C Mendes, MD,David M Nagorney, MD, FACS, Thomas C Bower, MD, FACS, Rory L Smoot, MD, FACS,Randall R DeMartino, MD, FACS, Sean P Cleary, MD, FACS, Gustavo S Oderich, MD, FACS,Michael L Kendrick, MD, FACS
BACKGROUND: En bloc celiac axis resection (CAR) for pancreatic cancer is considered increasingly after mod-ern neoadjuvant chemotherapy (NAC). Appleby and distal pancreatectomy with CAR areanatomically inaccurate terms, as tumors can extend beyond celiac axis proper, requiring con-current resection of the proper hepatic artery and/or superior mesenteric artery.
STUDY DESIGN: A 3-level classification for CAR (class 1, 2, or 3) was developed after retrospective review of anarterial resection database describing anatomical variants that dictate pancreatectomy-type,formal arterial revascularization, and gastric preservation. Perioperative and oncologic out-comes were assessed.
RESULTS: Of 90 CARs for pancreatic cancer, 89% patients received NAC, 35% requiring chemother-apeutic switch. There were 41 class 1, 33 class 2, and 16 class 3 CARs, with arterial andvenous revascularization performed 62% and 66%, respectively. Ninety-day mortalitydecreased to 4% in the last 50 cases (p ¼ 0.035); major morbidity was unchanged (55%).Any hepatic or gastric ischemia occurred in 20% and 10% patients, respectively, and arterialrevascularization was protective. R0 resection rate (88%) was associated with chemoradiation(p ¼ 0.004). Median overall survival was 36.2 months, superior with NAC (8.0 vs. 43.5months). Predictors of survival after NAC included chemotherapy duration, carbohydrateantigen 19-9 response, pathologic response, and lymph node status. Major pathologicresponse (p ¼ 0.036) and extended duration NAC (p ¼ 0.007) were independent predictorson multivariate analysis.
CONCLUSIONS: Current terminology for CAR inadequately describes all operative variants. Our classification,based on the largest single-center series, allows complex operative planning and standardizedreporting across institutions. Extent of arterial involvement determines pancreatectomy type,need for arterial revascularization, and likelihood of gastric preservation. Operative mortalityhas improved, morbidity remains significant, and survival favorable after extended NAC withassociated pathologic responses; given these factors, CAR should only be considered in fitpatients with objective NAC responses at specialized centers. (J Am Coll Surg 2020;231:8e29. ! 2020 The Authors. Published by Elsevier Inc. on behalf of the American College ofSurgeons. This is an open access article under the CC BY-NC-ND license[http://creativecommons.org/licenses/by-nc-nd/4.0/].)
A safe and margin negative operation is the surgeon’s pri-mary oncologic contribution to patients with nonmeta-static pancreatic adenocarcinoma (PDAC). The
likelihood of clear margins decreases with increasedlocoregional extra-anatomic extension of the primary tu-mor to involve critical vascular structures. The American
Disclosure Information: Nothing to disclose.
Presented at the Western Surgical Association 127th Scientific Session, LasVegas, NV, November 2019.
Received March 16, 2020; Revised May 4, 2020; Accepted May 4, 2020.
From the Division of Hepatobiliary and Pancreas Surgery (Truty, Nagor-ney, Smoot, Cleary, Kendrick) and Division of Vascular Surgery
(Colglazier, Mendes, Bower, DeMartino, Oderich), Mayo Clinic Collegeof Medicine, Rochester, MN.
Correspondence address: Mark J Truty, MD, MSc, FACS, Division ofHepatobiliary and Pancreas Surgery, Mayo Clinic College of Medicine,200 First St SW, Rochester, MN 55902. email: [email protected]
8ª 2020 The Authors. Published by Elsevier Inc. on behalf of the AmericanCollege of Surgeons. This is an open access article under the CC BY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
https://doi.org/10.1016/j.jamcollsurg.2020.05.005ISSN 1072-7515/20

Joint Committee on Cancer defines tumors that involvethe celiac axis and superior mesenteric artery (SMA) asT4 and surgically unresectable due to inability to rendera negative margin resection with standard pancreatectomytechniques.1 Consideration of en bloc arterial resectionduring pancreatectomy had been relatively abandonedfor decades due to the significant risk of ischemic andhemorrhagic complications, with attendant morbidityand mortality and historically poor long-term oncologicoutcomes, which were initially reported by Fortner inthe 1970s.2 However, there has been renewed interest inen bloc arterial resection for PDAC due to improvedresponse rates and associated survival benefit with moderncombination chemotherapeutic regimens with increasinguse of total neoadjuvant therapy.3-6 Concurrently, autopsyand long-term observational studies of unresectable tu-mors have demonstrated that up to 10% to 30% of pa-tients harbor a relatively nonmetastatic “locallydominant” phenotype, and some patients might deriveboth symptomatic and survival benefits from aggressivelocoregional pancreatectomy with en bloc arterial resec-tions.7-10
The first formal series (n ¼ 6) of celiac axis resections(CARs) for PDAC was reported in 1997.11 In 2005, Mak-ary and colleagues12 at Hopkins were the first US center toreport en bloc celiac resection and distal pancreatectomyfor PDAC. Since these initial descriptions, the majorityof cases have been small series or isolated case reports,and these operations have not been performed with anysignificant frequency in the US. American College of Sur-geons NSQIP data revealed only 20 (2.4%) of 822 casesat 43 institutions.13 A recent retrospective Europeancohort study on CAR from 20 hospitals in 12 countriesreported outcomes in only 68 patients.14 Although thespecific technical aspects of CAR for PDAC have beendescribed limitedly using inappropriate terms such asAppleby, modified Appleby, or more recently distal pancre-atectomy with CAR (DP-CAR), the overwhelming
majority of reported cases are distal pancreatic resectionsfor body tumors with isolated celiac axis proper onlyinvolvement, and there have been no descriptions of theother various anatomical procedural variants based on tu-mor location.15 Many patients have tumors with lateralextension beyond the distal common hepatic artery toinvolve the gastroduodenal artery (GDA) and proper he-patic artery (PHA) bifurcation and compromise thecollateral system that a traditional Appleby relies on forhepatic and gastric perfusion. In addition, there can alsobe inferior and posterior extension to involve the proximalSMA. Combined en bloc resections of the celiac axis withPHA and/or SMA have not been described. In fact, theprevious largest reported single-center series from Japanincluded a total of 80 cases, all of which were isolatedceliac-only resections without any formal arterial revascu-larization.16 This suggests that those patients with moreextensive arterial involvement and/or those that requireformal arterial revascularization are likely never consid-ered for resection by even the most experienced oncologicsurgeons, therefore, outcomes and detailed technical de-scriptions of such procedures are currently unknown.There have been no large series reporting on all of theanatomic variants of en bloc celiac resection for PDACwith formal arterial revascularization, and the currentlyused terminology and descriptions of such operationsare inaccurate in their ability to describe the extent ofresection required, predict need for formal arterial revas-cularization, determine the type of pancreatectomyneeded, or adequately understand the anatomical basisfor likelihood of gastric preservation. Therefore, we aimedto describe our institution’s extensive modern experienceand outcomes with these complex en bloc resectionaloperations that have increased dramatically since theintroduction of modern combinatorial neoadjuvantchemotherapy (NAC) and improved patient selection.
METHODSWith IRB approval, we retrospectively reviewed our Hep-atobiliary and Pancreas Surgery Divisional pancreatec-tomy data set for all major pancreatectomies forpathologically confirmed PDAC with en bloc arterialresection. We then limited our review to those undergo-ing any type of en bloc CAR from January 1995 toSeptember 2019. Patient demographics, operative details,and perioperative and oncologic outcomes were reviewed.Patients had been counseled on the historically increasedrisks of en bloc arterial resection before consenting forresection.Review of preoperative cross-sectional imaging (multi-
phase CT/MR), operative findings, resection procedures
Abbreviations and Acronyms
CA19-9 ¼ carbohydrate antigen 19-9CAR ¼ celiac axis resectionDP-CAR ¼ distal pancreatectomy with celiac axis resectionGDA ¼ gastroduodenal arteryHR ¼ hazard ratioNAC ¼ neoadjuvant chemotherapyOS ¼ overall survivalPDAC ¼ pancreatic adenocarcinomaPHA ¼ proper hepatic arteryRFS ¼ recurrence-free survivalSMA ¼ superior mesenteric artery
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 9

performed, and final pathology assisted in creation of a3-tier classification system for pancreatectomy withCAR based on tumor location that subsequently dictatesextent of arterial structures requiring en bloc resection,type of pancreatectomy required, need for arterial revascu-larization, and risk of associated need for elective gastrec-tomy due to surgical-induced ischemia (Table 1).Class 1 tumors involve the celiac axis proper and its
proximal branches without extension to the PHA/GDAbifurcation (Fig. 1A). Class 1 cases were further subclassi-fied as class 1A: typical Appleby or DP-CAR-type resec-tions requiring DP with the presence of adequatearterial collaterals after celiac resection and ligation ofthe distal common hepatic artery via SMA pancreatico-duodenal arcades to the GDA and PHA for hepatic perfu-sion and dual arterial perfusion via the right gastric andgastroepiploic arcades for gastric perfusion; class 1B,“modified Appleby”-type distal pancreatic resectionswherein intraoperative assessment reveals inadequateperfusion collaterals via the SMA, requiring formal hepat-ic arterial revascularization to mitigate postoperativeischemia; and class 1C, similar to 1B, however, requiringgastrectomy due to either inadequate dual gastric perfu-sion despite hepatic artery revascularization or local gastricinvasion precluding salvage.Class 2 tumors involve the celiac axis with extension
laterally along the common hepatic artery to involve thePHA/GDA bifurcation resulting in absence of the previ-ously described SMA collaterals after celiac/PHA resec-tion requiring formal hepatic arterial revascularization tothe distal PHA, as well as requiring total gastrectomydue to surgical induced ischemia (Fig. 1B) Class 2 caseswere further subclassified as class 2A: the tumor doesnot involve the pancreatic head/bile duct and anextended/subtotal DP is technically possible from apancreatic margin perspective with formal hepatic arterialrevascularization required for hepatic perfusion, as well astotal gastrectomy due to surgical ischemia; and class 2B:the tumor involves pancreatic head/bile duct and requires
total pancreatectomy, total gastrectomy, and formal he-patic arterial revascularization.Class 3 tumors involve the celiac axis with extension
inferiorly and posteriorly to encase the proximal SMA(Figs. 2A, 2B). Class 3 cases were further subclassifiedas class 3A: tumor involves celiac and SMA but withoutlateral extension to the PHA/GDA bifurcation and re-quires DP with en bloc celiac axis and SMA resectionwith formal dual hepatic and visceral arterial revasculari-zation for hepatic and bowel perfusion, gastrectomymight be required dependent on the distal extent ofSMA resection (involvement of inferior pancreaticoduo-denal arteries) and adequacy of the right gastric and gas-troepiploic arterial arcades; and class 3B: tumor involvesthe celiac and SMA with extension to PHA/GDA bifurca-tion and requires either subtotal or total pancreatectomy(dependent on pancreatic head/bile duct involvement),total gastrectomy, and formal dual hepatic and visceralrevascularization for hepatic and bowel perfusion.All patients had biopsy-confirmed PDAC via endo-
scopic ultrasound verified by our gastrointestinal pa-thologists. Intraoperative frozen section was used onall cases with College of American Pathology protocolsused for tumor, margin, and nodal assessment. Amargin negative resection (R0) was identified as notumor cells within < 1 mm from the inked margin.For those undergoing neoadjuvant therapy, pathologictreatment response was per College of AmericanPathology grading system: No viable cancer cells (com-plete response, grade 0), single cells, or rare smallgroups of cancer cells (near complete response, grade1), residual cancer with evident tumor regression, butmore than single cells or rare small groups of cancercells (partial response, grade 2), and extensive residualcancer with no evident tumor regression (poor or noresponse, grade 3). Adjuvant therapy receipt wasrecorded for those patients receiving postoperativechemotherapy. Serial carbohydrate antigen 19-9(CA19-9) responses were evaluated specifically after
Table 1. Celiac Axis Resection Classification SystemCeliac class Artery resection Need for revascularization Pancreatectomy type Gastric preservation
1A Celiac only No Distal Possible
1B Celiac only Yes Distal Possible
1C Celiac only Yes Distal No
2A Celiac/PHA Yes Subtotal No
2B Celiac/PHA Yes Total No
3A Celiac/SMA Yes Distal Possible
3B Celiac/PHA/SMA Yes Subtotal/total No
PHA, proper hepatic artery; SMA, superior mesenteric artery.
10 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

chemotherapy but before chemoradiation and resection.We defined “optimal CA19-9 response” as patientswith normal CA19-9 post chemotherapy, whethernormal or elevated pre chemotherapy.
Postoperative outcomes were followed up to 90 days.Complications were graded according to Clavien-Dindo, major complications were grade IIIA or higher.17
Pancreas-specific morbidity was graded according to
Figure 1. (A) Class 1 celiac axis resections with variants. (B) Class 2 celiac axis resections withvariants. (Reprinted from Mayo Foundation for Medical Education and Research, withpermission.)
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 11

International Study Group for Pancreatic Surgerycriteria.18 Any hepatic ischemic complications weredefined as 5-fold postoperative elevations of transaminaselevels with any associated radiographic ischemic infarctionwith or without associated hepatic insufficiency/failure orneed for specific interventions (operative or radiologic) toaugment hepatic arterial inflow. Any gastric ischemiccomplications were defined as postoperative gastric
dysfunction with endoscopic evidence of ischemic gastro-pathy (eg pallor or ulceration), partial or transmuralnecrosis, gastric fistula or postoperative perforation, orneed for emergency gastrectomy.Resections included either distal/subtotal pancreatec-
tomy or total pancreatectomy with associated lymphade-nectomies. Restoration of gastrointestinal continuitywas with single Roux limb for subtotal
Figure 2. (A) Class 3A celiac axis resections with variants. (B) Class 3B celiac axis resections withvariants. SMA, superior mesenteric artery. (Reprinted from Mayo Foundation for Medical Education andResearch, with permission.)
12 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

pancreatectomy/gastrectomy or dual Roux limb for thosepatients undergoing total pancreatectomy/gastrectomy. Avariety of graft conduits were used, ranging from autolo-gous veins (left renal vein, reversed saphenous), autolo-gous splenic artery or superficial femoral artery,synthetic PTFE, rifampin-soaked Dacron grafts, and,most recently, cadaveric cryopreserved arterial grafts (aor-toiliac or superficial femoral). The choice of arterial con-duits has evolved during the time of the study, movingaway from synthetic and vein grafts to more autologousor cadaveric arterial grafts to prevent graft infection andbreakdown with resulting hemorrhage or ischemia.Feeding tubes were placed at the discretion of the oper-ating surgeon and most often used for higher complexityresections (class 3). Pedicled soft tissue coverage flaps,such as omental or round ligament, were used if availableto cover all arterial revascularization conduits with judi-cious drain placement. All patients underwent routinepostoperative imaging with percutaneous drainage ofpotential leaks or suspicious fluid near grafts. In recentyears, empiric extended duration antibiotics (7 days),based on our infection mitigation protocols with intrao-perative bile duct cultures, IV octreotide therapy, as well
as parenteral nutrition (7 to 10 days), have been used inmost cases in an attempt to improve healing and mini-mize complications.19 All patients are managed alongwith our endocrine and nutrition teams both pre- andpostoperatively. Postoperatively, radiologic and biochem-ical (CA19-9) follow-up was performed every 3 to 4months for the first 3 years, every 6 months for years 4to 5, and annually beyond 5 years, according to institu-tional protocols, with phone calls to living patients every3 months for those patients undergoing long-term surveil-lance by local providers.Descriptive statistics were reported as number and/or
percentage for discrete and median and/or mean forcontinuous variables. Variable associations used Fisherexact or Pearson chi-square for discrete categorical vari-ables with continuous variables compared using t-test,Mann-Whitney U test, or Kruskal-Wallis test, as appro-priate. Recurrence-free survival (RFS) was measuredfrom date of resection until detection of local, peritoneal,or distant metastases or death or last censored visit. Over-all survival (OS) was measured from date of tissue diag-nosis until death or last censored visit. Rates of medianRFS and OS were estimated by Kaplan-Meier methodand log-rank test with 95% CIs and a p value < 0.05was considered significant. Univariate associations forRFS and OS were assessed using Cox model and multi-variable Cox model for RFS and OS was used for relevantvariables identified on univariate analysis. All statisticalanalyses were performed using IBM SPSS software,version 26 (IBM Corp).
RESULTSWe identified 178 patients that underwent pancreatec-tomy with any en bloc arterial resection from January1995 to September 2019 (Fig. 3A) Of those, there were90 patients with PDAC who underwent pancreatic resec-tion with en bloc CAR (Fig. 3B). Patient demographiccharacteristics are shown in Table 2. There were 41 class1 (45.5%), 33 class 2 (36.7%), and 16 class 3 (17.8%) enbloc celiac resections (Figs. 4 to 7). There was a significantincrease (p < 0.001) in cases over time, with 82 (91%)cases in the modern era (2011 to present).Neoadjuvant systemic induction chemotherapy was
used in 80 cases (89%), with a marked increase in themodern era (12.5% vs 96.3%; p < 0.001). Chemothera-peutic regimen was FOLFIRINOX (ie leuocovorin,5-FU, irinotecan, oxaliplatin) in 74 patients (93%) andgemcitabine/nab-paclitaxel in 34 patients (43%), with28 patients (35%) receiving both regimens with chemo-therapeutic due to toxicities, lack of objective response,or nonmetastatic progression based on restaging
Figure 3. (A) Overall arterial resection types performed at ourinstitution over time. (B) Celiac axis resections performed at ourinstitution over time. SMA, superior mesenteric artery.
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 13

Table 2. Patient Demographic and VariablesVariable Patient data (n ¼ 90)
Era of operation, n (%)
Pre to 2011 8 (9)
2011 to present 82 (91)
Celiac classification, n (%)
Class 1: celiac only 41 (45.5)
Class 2: celiac þ PHA 33 (36.7)
Class 3: celiac þ superiormesenteric artery # PHA
16 (17.8)
Sex, n (%)
Male 50 (56)
Female 40 (44)
BMI, kg/m2
Mean (SD) 26.1 (4.9)
Median 25.9
Range 17.3e41.0
Overweight, n (%) 46 (51.1)
Obese, n (%) 15 (16.7)
Age at operation, y
Mean (SD) 62.4 (10.4)
Median 62.8
Range 19.0e82.9
$ 65 y, n (%) 33 (37)
CA19-9 at diagnosis, U/mL
Mean (SD) 827 (413)
Median 218
Range 5e8,900
Nonsecretors, n (%) 10 (11.1)
Normal, n (%) 22 (28)
Elevated, n (%) 57 (72)
$ 500 U/mL, n (%) 27 (32)
Chemotherapy type (of neoadjuvantpatients), n (%)
Any FOLFIRINOX 74 (92.5)
Any GA 34 (42.5)
Chemotherapy switch 28 (35.0)
No. chemotherapy cycles
Mean (SD) 8.4 (3.1)
Median 8.0
Range 2.0e18.0
$ 8, n (%) 51 (63.8)
Preoperative chemoradiation, n (%)
No 15 (17)
Yes 75 (83)
Length of therapy, mo
Mean (SD) 9.9 (4.3)
Median 9.7
Range 2.0e24.7
(Continued)
Table 2. ContinuedVariable Patient data (n ¼ 90)
Optimal CA19-9 response,* n (%)
No 37 (41)
Yes 53 (59)
Previous resection attempt, n (%)
No 84 (93.3)
Yes 6 (6.7)
Preoperative arterial embolization, n(%)
No 86 (95.6)
Yes 4 (4.4)
Pancreatectomy type, n (%)
Total 29 (32)
Distal/subtotal 61 (68)
Surgical approach, n (%)
Open 75 (83.3)
Laparoscopic 15 (13.3)
Conversion 3 (20.0)
Operative time
Mean (SD), min 512 (146)
Median, min 500
Range, min 211e891
$ 10 h, n (%) 30 (33)
Estimated blood loss, mL
Mean (SD) 1,496 (1,348)
Median 1,200
Range 100e9,000
$ 1,000, n (%) 59 (66)
Operative packed RBC transfusion, n(%)
No 28 (31)
Yes 62 (69)
No. of packed RBC units transfused,n (%)
1e2 37 (60.0)
$ 3 25 (40.0)
Arterial revascularization, n (%)
No 34 (38)
Yes 56 (62)
Venous reconstruction, n (%)
No 31 (34)
Yes 59 (66)
Multivisceral organ resection, n (%)
No 18 (20)
Yes 72 (80)
Gastrectomy 41 (45.5)
Nephrectomy/adrenalectomy 55 (61.1)
Partial colectomy 5 (5.6)
(Continued)
14 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

Table 2. ContinuedVariable Patient data (n ¼ 90)
No. of lymph nodes removed
Mean (SD) 21.1 (10.2)
Median 19.5
Range 1.0e55.0
Positive lymph node, n (%)
No 70 (78)
Yes 20 (22)
No. of positive lymph nodes, n (%)
1 10 (11.1)
2e3 6 (6.9)
$ 4 4 (4.7)
Resection margin status
Negative, n (%) 79 (88)
Positive, n (%) 11 (12)
Positive margin withchemoradiation, %
7
Positive margin withoutchemoradiation, %
33
Pathologic treatment response, n (%)
Score 0: complete 9 (11)
Score 1: near complete 20 (25)
Score 2: partial 43 (54)
Score 3: poor/none 8 (10)
Any complication, n (%)
No 24 (27)
Yes 66 (73)
Major (grade III or higher) 48 (53.3)
Any hepatic ischemia, n (%)
No 72 (80)
Yes 18 (20)
Any gastric ischemia,y n (%)
No 40 (81.6)
Yes 9 (18.4)
Emergent gastrectomy 5 (10.2)
Any reoperation, n (%)
No 74 (82.2)
Yes 16 (17.8)
Grade B/C delayed gastric emptying,y
n (%)
No 33 (67.3)
Yes 16 (32.6)
Grade B/C postoperative pancreaticfistula,z n (%)
No 42 (68.8)
Yes 19 (31.1)
Post-pancreatectomy hemorrhage (B/C), n (%)
No 72 (80)
Yes 18 (20)
(Continued)
Table 2. ContinuedVariable Patient data (n ¼ 90)
Other morbidity, n (%)
Any surgical site infection 25 (27.8)
Any venous thromboembolism/pulmonary embolismx
16 (17.8)
Any gastric ischemia 14 (15.6)
Any pulmonary 13 (14.4)
Any genitourinary 11 (12.2)
Any cardiac 8 (8.9)
Any wound 6 (6.7)
Postoperative diarrhea,jj n (%)
No 56 (62.2)
Yes 34 (37.8)
Length of stay, d
Mean (SD) 17.2 (14.8)
Median 12.5
Range (4.0e123.0)
$ 15 d, n (%) 38 (42)
Readmission, n (%)
No 55 (61.1)
Yes 35 (38.9)
ICU admission for $ 24 h, n (%)
No 30 (33.3)
Yes 60 (67.7)
90-d operative mortality, n (%)
No 81 (90)
Yes 9 (10)
Modern era 6 (7.3)
Last consecutive 50 cases 2 (4.0)
Adjuvant chemotherapy, n (%)
No 71 (79)
Yes 19 (21)
Recurrent disease, n (%)
No 52 (58)
Yes 38 (42)
Recurrence type, n (% total, % allrecurrence)
Local 10 (10, 26)
Peritoneal 18 (20, 47)
Distant 25 (28, 69)
Multisite 14 (16, 37)
Vital status at last follow-up, n (%)
Alive, no evidence of disease 38 (42)
Alive, with disease 13 (14)
Not alive 39 (43)
*Normal or normalized after chemotherapy.yIn those undergoing gastric preservation.zExcluding total pancreatectomy patients.xIncludes all postoperative portomesenteric and extremity venous thrombosis.kRequiring medical management.CA19-9, carbohydrate antigen 19-9; FOLFIRINOX, leuocovorin, 5-FU, irino-tecan, oxaliplatin; GA, gemcitabine plus nab-paclitaxel; PHA, proper hepaticartery.
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 15

examinations (CT, CA19-9, and PET) to first-lineregimen. Median number of chemotherapy cycles was 8(range 2 to 18). Sequential locoregional chemoradiationwas used preoperatively in 75 patients (83%) and in allpatients receiving initial induction chemotherapy withvarious radiosensitizers. The overall median duration ofneoadjuvant therapy was 9.7 months (range 3 to 24.7months) and this varied by era of operation, with greaterduration of NAC in modern era. At time of operation, 53patients (59%) had either baseline normal or normalizedCA19-9 levels after induction chemotherapy. There were4 patients (8%) who underwent preoperative hepatic ar-tery embolization in an effort to augment arterial perfu-sion collaterals.Operative approach was open in 75 patients (83%) and
laparoscopic in 15 patients (17%), with 3 patients (20%)requiring conversion to open resection after initial laparo-scopic attempts. Formal arterial revascularization (hepaticand/or visceral) was performed in 56 patients (62%).Concomitant venous resection and reconstruction of theportal/superior mesenteric vein were performed in 59 pa-tients (66%), and this increased in the modern era (25%vs 70%; p ¼ 0.019). Multivisceral resection was requiredin 72 patients (80%). The median operative time was 500minutes (range 211 to 891 minutes), with 30 procedures(33%) lasting more than 10 hours. Median operativeblood loss was 1,200 mL (range 100 to 9,000 mL), andmore than 1,000 mL in 59 patients (66%); perioperativeblood transfusion was required in 62 patients (69%), witha median of 2 packed RBC units transfused (range 1 to 24units).Any grade (minor and major) postoperative complica-
tions occurred in 66 patients (73%); 48 patients (53%)had grade IIIA or higher complications. Overallmorbidity rates did not change over time (p ¼ 0.588).Any hepatic ischemic complications occurred in 18 pa-tients (20%). For those patients with an intact stomach,postoperative gastric ischemic complications occurred in9 patients (18%). Reoperation for any cause was requiredfor 16 patients (18%), and this improved in the modernera (50% vs 14%; p ¼ 0.028). Nine patients (10%)required reoperation due to ischemic indications andthis also improved over time (p ¼ 0.013), with 4 patientsrequiring emergent gastrectomy for ischemia, of whichnone underwent formal arterial revascularization at indexoperation. Bowel ischemia did not develop in any patientswith class 3 tumors after mesenteric (SMA) revasculariza-tion. Factors predictive of any hepatic or gastric ischemiccomplications in this series included morbid obesity(p ¼ 0.044), perioperative packed RBC transfusion(p ¼ 0.040), and preoperative hepatic arterial emboliza-tion (p ¼ 0.020); formal arterial revascularization
(p ¼ 0.002) was protective for ischemic complications.The overall 90-day operative mortality rate for the entirecohort was 10% (9 patients), with a significant improve-ment in the modern era (37.5% vs 7.3%; p ¼ 0.035).Operative mortality has improved recently, with a 4%mortality rate in the last 50 consecutive cases. All mortal-ities were secondary to hemorrhagic, ischemic, or infec-tious complications: 3 deaths from hepatic vascular(arterial and venous) thrombosis and fulminant liver fail-ure, 3 deaths from complications after postoperativegastric necrosis, 2 deaths from uncontrolled hemorrhagesecondary to postoperative pancreatic fistula, and 1 deathfrom sepsis and multi-organ failure due to postoperativepancreatic fistula. Factors associated with 90-day majormorbidity and mortality are shown in Table 3. Specif-ically, the extent of resection (ie celiac classification, con-current venous resection, or multivisceral resection) didnot negatively impact major morbidity or mortality inthis series. Operative approach also did not predict out-comes, however, the majority of laparoscopic resectionswere class 1 only cases.On pathologic examination, 76 cases (88%) were
margin negative (R0) resections. The median number oflymph nodes resected was 19 (range 1 to 55) with 19(22%) having positive regional lymph node metastases,with a median of 2 (range 1 to 7) positive nodes. Preop-erative locoregional chemoradiation was associated withlower positive lymph nodes (p ¼ 0.012) and negativemargins (p¼ 0.004). In those patients undergoing neoad-juvant therapy, major pathologic treatment response(complete/major) was seen in 38% of patients, partial re-sponses in 51%, and no treatment response in 11%.Adjuvant chemotherapy was completed in 19 patients(22%), 6 (60%) of which underwent upfront operations,and in 11 patients (15%) who received neoadjuvant sys-temic chemotherapy.Median follow-up was 24.6 months. At the time of this
analysis, recurrent disease developed in 38 patients (44%),with distant failure in 25 (29%), peritoneal failure in 18(21%), local failure in 10 (12%), and multisite recurrencein 14 (16%). Median RFS was 17.3 months; 5.0 monthsfor patients who underwent upfront operations and 19.9months for patients receiving NAC (log-rank p < 0.001).Median OS was 36.2 months (43.5 months excludingoperative deaths); 8.0 months (13.5 months excludingoperative deaths) for patients who underwent upfront op-erations and 43.5 months (48.7 months excluding opera-tive deaths) for patients receiving NAC (log-rankp < 0.001). Univariate predictors of RFS and OS areshown in Table 4 and included NAC, extended durationchemotherapy (more than 6 cycles), optimal CA19-9response (normal or normalized), major pathologic
16 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

response, and lymph node status. Specifically, extent ofresection (celiac class) did not negatively influence RFSor OS. When limiting the analysis to only those patientsin the modern era undergoing NAC, on multivariate anal-ysis only major pathologic response (p ¼ 0.046;p ¼ 0.036; hazard ratio [HR], 0.41; HR, 0.29) andextended duration (more than 6 cycles) NAC(p ¼ 0.019; p ¼ 0.007, HR, 0.32; HR, 0.22) were inde-pendently prognostic for improved survival for both RFSand OS, respectively.
DISCUSSIONThis is the largest single-institution series of en bloc CARsfor PDAC, the largest overall series with formal arterialrevascularization, and the only report describing all poten-tial anatomical resectional variants. Our data suggest thatsuch complex resections are technically feasible, however,they carry significantly higher risk than standard anatom-ical plane-based pancreatic operations and, given theserisks, upfront resection has no role whatsoever. In this se-ries, neither the extent of resection nor need for formalarterial revascularization had any detrimental influenceon short-term morbidity, mortality, or long-term onco-logic survival, suggesting that such aggressive resections,if coupled with an effective upfront neoadjuvant strategyand management of associated complications, can havesubstantial benefit for a highly select subset of patientsand might be oncologically sound.En bloc resection of the celiac axis for malignancy has a
markedly limited but well-described history. Specific de-scriptions and terms used for these operations, such asAppleby, modified Appleby, or DP-CAR, have been errone-ously propagated due to a misunderstanding of the earlyliterature and unawareness of all the potential anatomicalresectional variations. In 1952, Appleby20 originallydescribed a series of 13 en bloc CARs for locally advancedgastric cancer, remarkably without operative mortality. Inhis original report, the celiac trunk was resected en blocwith the stomach, distal pancreas, and spleen, with liga-tion of the common hepatic artery proximal to thePHA/GDA bifurcation. Arterial perfusion to the liverwas preserved due to the rich network of collaterals withinthe pancreatic head and duodenum from the SMA to theGDA and PHA via the pancreaticoduodenal arcadesarising from the SMA. The modified Appleby procedurewas described in 1992 and, like its predecessor, is also spe-cifically a gastric cancer operation, with the modificationrequiring formal hepatic arterial revascularization in thosepatients whose pancreaticoduodenal arterial collateralswere inadequate for hepatic perfusion after celiac resec-tion.21 In these initial gastric cancer descriptions, the
stomach was not preserved, so these terms should belimited to locally advanced gastric cancer operations, asthey have different indications and anatomical conse-quences when applied to PDAC, specifically with regardto gastric perfusion and preservation, one of the leadingcauses of mortality when performed for PDAC. Morethan 20 years after Appleby’s original gastric cancer oper-ation, Nimura and colleagues22 reported the first case ofDP with en bloc CAR for PDAC. In 2007, the alternativeterm DP-CAR was suggested for a series of 23 patients us-ing the similarly described arterial collateral-sparing tech-niques for hepatic perfusion; however, this term onlydescribes operations for tumors involving the celiac axisproper undergoing DP only, and does not infer anyneed for revascularization. As many patients have tumorsthat extend beyond the celiac axis proper, arising fromeither the pancreatic body or head/uncinate, such termsare both inappropriate and inadequate.23 None of thesedescriptions consider the extent of arterial involvement,type of pancreatectomy required, and specific need forrevascularization, or likelihood of gastric preservation insuch cases, therefore, in our opinion, these misappropri-ated terms should be abandoned. Our proposed classifica-tion system allows for a logical and clinically relevantanatomic understanding of the extent of any planned enbloc CAR and allows unified reporting so that specific op-erations and outcomes can be compared directly acrossspecialized centers, as these types of procedures are beingconsidered in several high-volume centers due toimproved systemic chemotherapeutic options.Outside of isolated case reports, CARs for PDAC have
not been performed with any significant frequency andprimarily only describe class 1-type resections with lowrates of arterial revascularization. A recent single-institutional report described 11 celiac resection caseswith only 3 requiring arterial revascularization.24 Thisreport also reviewed the literature and found only 28 casesof revascularization from a total of 12 previous studies,with the overwhelming majority class 1 resectionsalone.25-35 The previous 2 largest US series reportedincluded 17 and 30 cases, respectively, only 2 of whichrequired arterial revascularization, and primarilydescribed class 1 cases with DP alone.36,37 A single system-atic review and meta-analysis on celiac resection forPDAC identified a total 283 cases, of which 18 studieswere included. All resections were class 1 with only a12% revascularization rate.38 The most recent studyincluded 23 centers from Europe, Japan, and the US,with a total of 174 PDAC patients included, all DPwith celiac axis only resections (class 1). In this contempo-rary analysis, they identified “high-volume centers” asthose performing at least 1 case per year, of which there
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 17

were only 3 centers that met that criteria, again demon-strating the global rarity of such procedures.39 The com-mon theme in all of these studies included higher ratesof complications and increased operative mortality (upto 20%) compared with standard pancreatectomy
operations, leading to appropriate hesitancy to considersuch operations in general. As our data reveal, morbidityis significant and has not changed over time, primarilydriven by hemorrhagic, ischemia, or infectious complica-tions. Mortality, however, has decreased significantly with
Figure 4. (A) Example of a class 1A celiac axis resection (open). (B) Example of a class 1A celiac axisresection (laparoscopic). (C, D) Two examples of class 1B celiac axis resections with hepatic arterialrevascularization (autologous superficial femoral artery) and gastric preservation. (E, F) Two examples ofclass 1C celiac axis resections with hepatic arterial revascularization (autologous superficial femoralartery) and total gastrectomy.
18 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

increased volumes, technical experience, and concurrentcomplication mitigation and management. Survival out-comes have varied significantly in previous studies, largelydue to variability in the use of neoadjuvant therapy overtime and the specifics of such therapeutic modalities.With the advent of modern combinatorial chemo-
therapy and improvements in response and associated sur-vival, a dramatic shift in our overall perception of“anatomic resectability” has taken place. The casesdescribed herein are considered “unresectable” by all cur-rent anatomical guidelines, yet survival outcomes can besignificantly favorable, suggesting the current criteria arepoor indicators of potential surgical survival benefit.Anatomic designations, such as “borderline resectable”or “locally advanced” were specifically created only todetermine whether preoperative treatment was warranted,based on the degree of vascular involvement and the pre-dicted margin risk in patients undergoing upfront opera-tion using standard pancreatectomy techniques. However,in the context of neoadjuvant therapy and nonstandard enbloc resection techniques, these terms do not in any way
imply inoperability or poor oncologic outcomes. For tu-mors beyond standard anatomic criteria undergoing neo-adjuvant therapy, new modern concepts of resectabilityare required, and in our center include the following pri-mary fundamental principles: responsivity, reconstruct-ability, and recoverability. Only in the context of these3 guiding criteria can we then determine whether suchadvanced procedures make oncologic sense in any givenpatient.As occult metastatic disease is the greatest threat to
long-term survival in PDAC patients, objective demon-stration of the effectiveness of preoperative systemicchemotherapy is necessary. Responsivity is measured us-ing a variety of surrogates of response, including clinical,biochemical, radiologic, and/or metabolic responses.Although clinical improvement (pain, diabetes, nutrition)during therapy can predict therapeutic response, they arenot always present and are poorly quantifiable. As CA19-9 elevation has been predictive of worse long-term sur-vival, associated decreases with chemotherapy arerequired; however, in up to 40% of patients, such
Figure 5. (A, B) Two examples of class 2A celiac axis resections with hepatic arterial revascularization(autologous superficial femoral artery), total gastrectomy, and distal pancreatectomy. (C, D). Two ex-amples of class 2B celiac axis resections with hepatic arterial revascularization (autologous superficialfemoral artery), total gastrectomy, and total pancreatectomy.
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 19

biochemical responses cannot be assessed (10% are nonse-cretors, 30% are normal at diagnosis).40-43 In addition, ithas been well established that no significant radiologicresponse on cross-sectional imaging (CT) is anticipatedwith tumors encasing arterial structures.44 To compensatefor these deficiencies, we have heavily incorporated meta-bolic (PET) response in our practice, as it is both quantifi-able and, in our experience, highly correlative withsubsequent pathologic response, a major predictor of sur-vival after resection.5 Simply the absence of metastaticprogression alone after NAC is not enough to warrantexploration; the more complex (increased risks) the antic-ipated operation will be, the more we need to confirmobjective responses to justify those risks.44-46 For suchcases, thorough pretreatment staging with triple-phasecross-sectional imaging (CT/MRI), metabolic imaging(PET), laboratory testing (eg CA19-9, CEA, and cell-free DNA), and peritoneal evaluation (laparoscopy andcytology) is required at our center, given the higher likeli-hood of harboring occult systemic and peritoneal
metastases. We use extended duration combinatorialchemotherapy that is specifically surgeon-directed, oftenwith consideration of chemotherapeutic switch (one-thirdof cases in this series) to assure that chemotherapy isdemonstrably effective. Similar to our previous report,extended duration chemotherapy, optimal CA19-9 re-sponses, and major pathologic response were factors thatpredicted survival in this cohort.5 Pathologic treatmentresponse is typically known only postoperatively. Weassess residual metabolic (PET) activity after chemo-therapy as a surrogate of pathologic response and ourgoal during induction chemotherapy was to accomplishcomplete or near-complete metabolic responses beforeconsideration of moving on to locoregional chemoradia-tion and eventual resection, as the response to systemictherapy is likely predictive of systemic response, incontrast to responses to locoregional chemoradiation,which likely have no direct impact on occult metastaticdisease. In our experience, the majority of treatment-naı̈vePDACs have PET-avid tumors, however, we do use PET/
Figure 6. (AeD) Four examples of class 3A celiac axis resections with hepatic and visceral arterialrevascularization (rifampin-soaked Dacron), with or without total gastrectomy, and distalpancreatectomy.
20 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

MRI over PET/CT if at all possible due to its highermetabolic sensitivity and greater anatomical resolution.47
We do favor consolidative chemoradiation in all patientsrequiring significant vascular resection in an effort to in-crease our ability to perform margin negative resection,which was predictive in this series, as well as to minimizelocal recurrence rates. Our preference is for long-coursechemoradiation over stereotactic body radiotherapy dueto markedly varying radiation dosing and treatmentextent with concerns for out-of-field relapses with thelimited treatment volumes used for stereotactic bodyradiotherapy.48 As the majority of medical oncologistscannot comprehend that gravity of such operations interms of patient recovery, any form of adjuvant therapyis highly unlikely to oncologically salvage patients aftersuch extended resections if appropriate and effective ther-apy was not administered before operation. Our survivaloutcomes are favorable and likely a result of optimalpatient selection and extremely strict guidelines for oper-ative candidacy.Reconstructability is an evolving concept and has been
defined fluidly, varying by institution and by surgeon expe-rience, skillset, and comfort. For patients with more
anatomically advanced tumors encasing vascular struc-tures, this requires an en bloc nonanatomical plane-basedresection to remove all gross tumor, as well as “at risk” tis-sue, with a wide circumferential radial margin combinedwith the need to re-establish durable end-organ arterialperfusion, venous outflow, biliary drainage, and restorationof gastrointestinal continuity. Such an approach mirrorsthe anatomical and functional criteria for resectability inliver resection. As en bloc arterial resections require dissec-tion in nonanatomic planes, within the retroperitoneumand root of the mesentery, a mastery of vascular anatomicaldetail is required, as such cases are customized and truly“bespoke” for any given patient. In our opinion, no patientshould undergo “exploration” without a specific and defin-itive operative resection and revascularization plan withhigh likelihood of technical success. If this cannot beassured, then patients should be referred to centers thatcan perform all aspects of these operations, to avoid ahigh proportion of nontherapeutic laparotomies. Some au-thors have described intraoperative incisional biopsies todetermine tumor viability and obviate the need for arterialresection and dissecting the fibrotic tumors from the ar-teries. We do not support this recommendation, given its
Figure 7. (AeD) Five examples of class 3B celiac axis resections with hepatic and visceral arterial revascularization (autologous superficialfemoral artery/cryopreserved cadaveric aorto-iliac and femoral artery), total gastrectomy, and total pancreatectomy.
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 21

Table 3. Factors Associated with Major Morbidity and Operative Mortality
Variable
Major morbidity (90-d grade IIIA or higher)(n ¼ 48 of 90 [53.3%])
Operative mortality (90-d)(n ¼ 9 of 90 [10.0%])
No (n ¼ 42) Yes (n ¼ 48) p Value No (n ¼ 81) Yes (n ¼ 9) p Value
Era of operation, n (%) 0.719* 0.031*
Pre to 2011 3 (37.5) 5 (62.5) 5 (62.5) 3 (37.5)
2011 to present 39 (47.6) 43 (52.4) 76 (92.7) 6 (7.3)
Celiac resection classification, n (%) 0.661y 0.248*
Class 1 17 (41.5) 24 (58.5) 35 (85.4) 6 (14.6)
Class 2 17 (51.5) 16 (48.5) 30 (90.9) 3 (9.1)
Class 3 8 (50.0) 8 (50.0) 16 (100) 0 (0)
Sex n (%) 0.571y 0.504*
Male 22 (44.0) 28 (56.0) 46 (92.0) 4 (8.0)
Female 20 (50.0) 20 (50.0) 35 (87.5) 5 (12.5)
BMI, kg/m2 0.541z 0.536z
Mean (SD) 25.8 (4.5) 26.2 (5.2) 26.0 (4.7) 26.0 (6.8)
Median 26.4 25.2 26.0 23.3
Range 17.3e34.1 18.0e41.0 17.3e41.0 18.3e38.1
BMI class, n (%) 0.325y 0.173*
< 20 kg/m2 11 (37.9) 18 (62.1) 24 (82.8) 5 (17.2)
21e29 kg/m2 25 (54.3) 21 (45.7) 44 (95.7) 2 (4.3)
$ 30 kg/m2 6 (40.0) 9 (60.0) 13 (86.7) 2 (13.3)
Age at operation, y 0.365z 0.026z
Mean (SD) 63.4 (10.7) 61.6 (10.0) 61.7 (10.6) 68.6 (5.2)
Median 64.0 62.4 62.4 68.0
Range 38.2e82.9 19.0e79.8 19e82.9 61.8e77.4
Previous resection attempt, n (%) 0.094* 0.479*
No 37 (44.0) 47 (56.0) 76 (90.1) 8 (9.9)
Yes 5 (83.3) 1 (16.7) 5 (83.3) 1 (16.7)
Preoperative arterial embolization, n (%) 0.056* 0.003*
No 42 (48.8) 44 (51.2) 80 (93.0) 6 (7.0)
Yes 0 (0) 4 (100) 1 (25.0) 3 (75.0)
Pancreatectomy type, n (%) 0.117y 0.269*
Subtotal/distal 26 (41.3) 37 (58.7) 55 (87.3) 8 (12.7)
Total 16 (59.3) 11 (40.7) 26 (96.3) 1 (3.7)
Surgical approach, n (%) 0.384y 0.097*
Laparoscopic 7 (58.3) 5 (41.7) 9 (75.0) 3 (25.0)
Open 35 (45.5) 43 (54.5) 72 (92.3) 6 (7.7)
Operative time, min 0.541z 0.536z
Mean (SD) 518 (140) 504 (152) 514 (147) 477 (135)
Median 518 488 516 482
Range 211e891 272e864 211e891 309e751
Operating room time $ 10 h, n (%) 1.000y 0.262*
No 28 (46.7) 32 (53.3) 52 (86.7) 8 (13.3)
Yes 14 (46.7) 16 (53.3) 29 (96.7) 1 (3.3)
EBL, mL 0.968z 0.514z
Mean (SD) 1,429 (1,090) 1,555 (1,549) 1452 (1,122) 1,894 (2,731)
Median 1,225 1152 1,200 900
Range 100e5,700 100e9,000 100e6,500 250e9,000
(Continued)
22 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

Table 3. Continued
Variable
Major morbidity (90-d grade IIIA or higher)(n ¼ 48 of 90 [53.3%])
Operative mortality (90-d)(n ¼ 9 of 90 [10.0%])
No (n ¼ 42) Yes (n ¼ 48) p Value No (n ¼ 81) Yes (n ¼ 9) p Value
EBL $ 1,000 mL, n (%) 0.813y 0.266*
No 15 (48.4) 16 (51.6) 26 (83.9) 5 (16.1)
Yes 27 (45.8) 32 (54.2) 55 (93.2) 4 (6.9)
Operative packed RBC transfusion, n (%) 0.378y 0.452*
No 15 (53.6) 13 (46.4) 24 (85.7) 4 (14.3)
Yes 27 (43.5) 35 (56.5) 57 (91.9) 5 (8.1)
Any venous reconstruction, n (%) 0.495y 0.713*
No 16 (51.6) 15 (48.4) 29 (93.5) 2 (6.5)
Yes 26 (44.1) 33 (55.9) 52 (88.1) 7 (11.9)
Arterial revascularization, n (%) 0.954y 0.077*
No 16 (47.1) 18 (52.9) 28 (82.4) 6 (17.6)
Yes 26 (46.4) 30 (53.6) 53 (94.6) 3 (5.4)
Multivisceral organ resection, n (%) 0.460y 1.000*
No 7 (38.9) 11 (61.1) 16 (88.9) 2 (11.1)
Yes 35 (48.6) 37 (51.4) 65 (90.3) 7 (9.7)
Any morbidity, n (%) d 0.106*
No d d 24 (100.0) 0 (0.0)
Yes d d 57 (86.4) 9 (13.6)
Major morbidity, n (%) d 0.003*
No d d 42 (100.0) 0 (0.0)
Yes d d 39 (81.3) 9 (18.7)
Any gastric ischemia, n (%) d 0.005*
No d d 76 (93.8) 5 (6.2)
Yes d d 5 (55.5) 4 (44.4)
Any hepatic ischemia, n (%) d 0.014*
No d d 68 (94.4) 4 (5.6)
Yes d d 13 (72.2) 5 (27.8)
Reoperation (any indication), n (%) d 0.001*
No d d 71 (95.9) 3 (4.1)
Yes d d 10 (62.5) 6 (37.5)
Emergent gastrectomy, n (%) d 0.006*
No d d 79 (92.9) 6 (7.1)
Yes d d 2 (40.0) 3 (60.0)
DGE (B/C), n (%) d 0.044*
No d d 63 (94.0) 4 (6.0)
Yes d d 18 (78.3) 5 (21.7)
POPF (B/C), n (%) d 1.000*
No d d 61 (89.7) 7 (10.3)
Yes d d 20 (90.9) 2 (9.1)
PPH (B/C), n (%) d 0.075*
No d d 67 (93.1) 5 (6.9)
Yes d d 14 (77.8) 4 (22.2)
Any cardiac morbidity, n (%) d 0.003*
No d d 77 (93.9) 5 (6.1)
Yes d d 4 (50.0) 4 (50.0)
(Continued)
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 23

complete lack of oncologic principles, with risk of seedingthe abdominal cavity with viable tumor cells, and we havenot found this to be technically possible without riskingsubstantial vascular injury and risk of vascular complica-tions postoperatively (pseudoaneuryms).49 As systemiccontrol has improved, prevention of locoregional recur-rence will likely become a surgical quality indicator and aless than complete resection has the same oncologic valueas debulking or an R2 resection, that is, no benefit.Although the technical aspects of CAR and the variantsdescribed here are beyond the scope of this article, severalkey points need to be stressed in detail with regard to gastricpreservation to mitigate poor outcomes. Gastric preserva-tion is possible in select class 1 and 3 tumors. In contrastto Appleby’s original description in which the stomachwas removed, when en bloc CAR is performed for pancre-atic cancer with the goal of stomach preservation, lessercurvature perfusion via the left gastric artery from the celiacaxis and fundic perfusion by the short gastric arteries via thesplenic artery are taken with the dissection, resulting inrelative ischemia of the proximal and medial stomach.However, fulminant necrosis and emergency gastrectomycan be prevented with both the preservation and anatom-ical adequacy of the SMA/PDA collaterals via retrograde
perfusion of both the right gastroepiploic artery arcadevia the GDA and the right gastric artery arcade, which typi-cally arises from the PHA, allowing sufficient arterial perfu-sion along the greater and lesser curvatures of the stomach,respectively. Adequacy of both perfusion routes (rightgastric artery and right gastroepiploic artery) is requiredfor prevention of gastric ischemia, contrary to popularthought that only a single vascular arcade is sufficient;this critical anatomical distinction is likely the cause offailed attempts at gastric preservation in previous studiesresulting in high morbidity and mortality. If this dualperfusion cannot be assured, then consideration of totalgastrectomy should be strongly considered, given thehighmortality rate associated with postoperative gastric ne-crosis. We have not had any emergency gastrectomies;however, in patients undergoing formal arterial revascular-ization with gastric preservation, suggesting that theaugmented or “supercharged” dual (lesser and greater cur-vature) circulation is critical in preventing ischemic issuespostoperatively. In those patients with gastric ischemia inthis series, despite patent GDA and right gastroepiploic ar-tery vessels, there was inadequate right gastric artery perfu-sion. We heavily use intraoperative Doppler ultrasoundand indocyanine green angiography to assess and confirm
Table 3. Continued
Variable
Major morbidity (90-d grade IIIA or higher)(n ¼ 48 of 90 [53.3%])
Operative mortality (90-d)(n ¼ 9 of 90 [10.0%])
No (n ¼ 42) Yes (n ¼ 48) p Value No (n ¼ 81) Yes (n ¼ 9) p Value
Any pulmonary morbidity, n (%) d 0.023*
No d d 72 (93.5) 5 (6.5)
Yes d d 9 (69.2) 4 (30.8)
Any VT/PE morbidity, n (%) d 0.008*
No d d 70 (94.6) 4 (5.4)
Yes d d 11 (68.8) 5 (31.2)
Any GI morbidity, n (%) d 0.295*
No d d 36 (85.7) 6 (14.3)
Yes d d 45 (93.8) 3 (6.2)
Any GU morbidity, n (%) d 0.097*
No d d 72 (92.3) 6 (7.7)
Yes d d 9 (75.0) 3 (25.0)
Any wound morbidity, n (%) d 0.020*
No d d 77 (92.8) 6 (7.2)
Yes d d 4 (57.1) 3 (42.9)
Any SSI morbidity, n (%) d 0.257*
No d d 60 (92.3) 5 (7.7)
Yes d d 21 (84.0) 4 (16.0)
*Fisher exact test.yPearson chi-square.zKruskal-Wallis.CA19-9, carbohydrate antigen 19-9; DGE, delayed gastric emptying; FOLFIRINOX, leuocovorin, 5-FU, irinotecan, oxaliplatin; GA, gemcitabine plus nab-paclitaxel; GI, gastric ischemia; GU, genitourinary; POPF, postoperative pancreatic fistula; PPH, post-pancreatectomy hemorrhage; SSI, surgical siteinfection; VT/PE, venous thromboembolism/pulmonary embolism.
24 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

Table 4. Factors Associated with Recurrence-Free and Overall Survival
Variable
Recurrence-free survival Overall survival
HR (95% CI) p Value HR (95% CI) p Value
Era of operation 0.032 <0.001
Pre to 2011 1.0 (ref) 1.0 (ref)
2011 present 0.21 (0.05e0.88) 0.03 (0.004e0.17)
Celiac classification 0.970 0.696
1 1.0 (ref) 1.0 (ref)
2 1.09 (0.53e2.20) 0.75 (0.34e1.69)
3 0.99 (0.41e2.41) 1.14 (0.43e2.99)
Sex 0.382 0.650
Female 1.0 (ref) 1.0 (ref)
Male 0.75 (0.39e1.44) 1.19 (0.57e2.47)
BMI class 0.651 0.543
< 20 kg/m2 1.0 (ref) 1.0 (ref)
20e29 kg/m2 0.82 (0.39e1.69) 0.65 (0.29e1.48)
$ 30 kg/m2 0.61 (0.22e1.69) 0.74 (0.23e2.40)
Age at operation 0.126 0.199
< 65 y 1.0 (ref) 1.0 (ref)
$ 65 y 1.68 (0.86e3.22) 1.62 (0.77e3.40)
CA19-9 at diagnosis, category 0.228 0.410
Normal 1.0 (ref) 1.0 (ref)
Elevated 1.93 (0.97e3.85) 1.82 (0.82e4.04)
Nonesecretor 1.26 (0.20e7.84) 1.53 (0.19e11.97)
CA19-9 at diagnosis, $ 500 U/mL 0.657 0.503
No 1.0 (ref) 1.0 (ref)
Yes 1.34 (0.67e2.69) 1.54 (0.71e3.38)
Neoadjuvant chemotherapy <0.001 <0.001
No 1.0 (ref) 1.0 (ref)
Yes 0.08 (0.02e0.32) 0.002 (0.00e0.01)
Chemotherapy type 0.208 0.437
FOLFIRINOX 1.0 (ref) 1.0 (ref)
GA 1.65 (0.76e3.60) 1.44 (0.57e3.61)
Chemotherapy switch 0.682 0.642
No 1.0 (ref) 1.0 (ref)
Yes 1.19 (0.52e2.72) 1.26 (0.48e3.30)
$6 Chemotherapy cycles 0.002 <0.001
No 1.0 (ref) 1.0 (ref)
Yes 0.09 (0.21e0.42) 0.04 (0.01e0.22)
Optimal CA19-9 response* 0.010 0.011
No 1.0 (ref) 1.0 (ref)
Yes 0.40 (0.20e0.81) 0.36 (0.17e0.80)
Previous resection attempt 0.331
No 1.0 (ref) 1.0 (ref)
Yes 2.66 (0.37e19.18) 1.51 (0.28e8.12)
Pancreatectomy type 0.738 0.077
Subtotal/distal 1.0 (ref) 1.0 (ref)
Total 0.88 (0.42e1.83) 0.48 (0.22e1.08)
Surgical approach 0.060 0.642
Open 1.0 (ref) 1.0 (ref)
(Continued)
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 25

Table 4. Continued
Variable
Recurrence-free survival Overall survival
HR (95% CI) p Value HR (95% CI) p Value
Laparoscopic 2.62 (0.96e7.18) 1.32 (0.41e4.20)
Operating room time $ 10 h 0.951 0.988
No 1.0 (ref) 1.0 (ref)
Yes 1.02 (0.53e1.98) 1.01 (0.48e2.13)
Estimated blood loss $ 1,000 mL 0.884 0.793
No 1.0 (ref) 1.0 (ref)
Yes 1.05 (0.53e2.08) 1.11 (0.51e2.41)
Packed RBC transfusion 0.794 0.174
No 1.0 (ref) 1.0 (ref)
Yes 1.09 (0.55e2.19) 1.72 (0.79e3.73)
Venous reconstruction 0.885 0.732
No 1.0 (ref) 1.0 (ref)
Yes 1.05 (0.54e2.05) 1.14 (0.54e2.44)
Arterial revascularization 0.464 0.621
No 1.0 (ref) 1.0 (ref)
Yes 0.78 (0.40e1.51) 1.21 (0.58e2.54)
Multivisceral organ resection 0.599 0.616
No 1.0 (ref) 1.0 (ref)
Yes 0.82 (0.39e1.72) 0.80 (0.34e1.89)
Positive lymph node 0.043 0.022
No 1.0 (ref) 1.0 (ref)
Yes 2.55 (1.03e6.31) 3.24 (1.19e8.86)
Resection margin 0.592 0.287
Negative 1.0 (ref) 1.0 (ref)
Positive 1.30 (0.50e3.38) 1.77 (0.62e5.08)
Pathologic treatment response <0.001 <0.001
Score 0/1: major 1.0 (ref) 1.0 (ref)
Score 2: partial 2.30 (1.11e4.77) 3.21 (1.40e7.51)
Score 3: poor/none 8.20 (1.85e36.22) 10.87 (2.22e55.23)
Any morbidity 0.514 0.199
No 1.0 (ref) 1.0 (ref)
Yes 0.79 (0.39e1.60) 1.67 (0.76e3.64)
Major morbidity 0.610 0.246
No 1.0 (ref) 1.0 (ref)
Yes 1.18 (0.63e2.24) 1.53 (0.75e3.14)
Any gastric or hepatic ischemia 0.607 0.106
No 1.0 (ref) 1.0 (ref)
Yes 1.26 (0.52e3.07) 2.25 (0.84e6.02)
Reoperation 0.972 0.176
No 1.0 (ref) 1.0 (ref)
Yes 1.02 (0.39e2.63) 2.15 (0.71e6.48)
Delayed gastric emptying (B/C) 0.612 0.276
No 1.0 (ref) 1.0 (ref)
Yes 0.81 (0.36e1.83) 0.60 (0.24e1.50)
Postoperative pancreatic fistula (B/C) 0.373 0.610
No 1.0 (ref) 1.0 (ref)
Yes 0.73 (0.36e1.46) 0.81 (0.36e1.84)
(Continued)
26 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

adequate organ perfusion. Some centers routinely use pre-operative hepatic or left gastric arterial embolization to in-crease collateral flow before celiac resection.26 We have notused this technique to any significant degree, however, thisparadoxically increased the risk of postoperative ischemiccomplications in this series and we have abandoned suchtechniques and focused more on optimized revasculariza-tion techniques. In some cases, where the left gastric arteryarises either as a separate branch directly from the aorta orarises very proximal on the celiac trunk itself near its aorticorigin without tumor involvement, this can be safely pre-served dependent on location of the tumor to allow forgastric arterial perfusion after CAR more distally. Suchanatomical variation, although uncommon, can have sig-nificant positive influence on either total or partial gastricperseveration and should always be assessed on cross-sectional imaging and intraoperatively. Given the fre-quency of replaced or accessory arterial variants that cansimplify or complicate such operations, surgeons need toaccurately understand any given patient’s vascular anatomyand consequences of resection and need for alternativeperfusion procedures.Finally, to consider such procedures as oncologically
relevant, we consider “recoverability” in relation to thecomplexity of resection, risks of perioperative morbidityand mortality, patient fitness and associated comorbid-ities, effects on postoperative quality of life, and the over-all benefit to survival with such resections compared withcurrent nonoperative modalities. We have shown thatoverall morbidity has not changed over time; however,the associated mortality has improved significantly, sug-gesting better complication recognition and patientsalvage. As a result of our early experience, we have insti-tuted a host of perioperative measures to hasten patientrecovery with significant involvement of our medicalcolleagues in endocrinology, infectious disease, medical
nutrition, and physical rehabilitation during all phasesof care. With attentive management and close follow-upof all our patients, the majority are quite satisfied withtheir postoperative quality of life to date, however, wecounsel patients that full recovery typically takes 3 to 6months or longer, dependent on the extent of operationand severity of any associated complications. Long-termprospective evaluations are needed to fully understandthe physiologic consequences of such complex resectionalprocedures, particularly with patients living longer thanever before. Finally, as survival outcomes for nonoperativetreatment (systemic chemotherapy followed by locore-gional chemoradiation alone) continue to improve, weneed to determine what the added long-term benefit ofan aggressive resection provides, with appropriatecomparative outcomes analyses, given the known short-terms risks of surgical resection.
CONCLUSIONSOur proposed classification system does have limitationsand cannot completely predict all variants of tumor andpatient anatomy; the operative surgeon has a host ofanatomic considerations to keep in mind, much greaterin consequence than any standard pancreatectomy formore anatomically localized PDAC. This current pro-posed descriptive system allows for simple yet highly pre-dictive terminology in most patients, and such a newsystem is likely critically needed, as we anticipate therewill be an increased demand and frequency of suchlocoregional en bloc resections over time at specializedcenters. With availability of effective systemic therapiesand better patient selection, we will need to compareinstitutional outcomes with better clarity and granularityto assure we are making the appropriate comparisons anddecisions when it comes to patient safety and long-term
Table 4. Continued
Variable
Recurrence-free survival Overall survival
HR (95% CI) p Value HR (95% CI) p Value
Post-pancreatectomy hemorrhage (B/C) 0.876 0.185
No 1.0 (ref) 1.0 (ref)
Yes 1.08 (0.43e2.72) 1.99 (0.72e5.50)
Readmission 0.712 0.725
No 1.0 (ref) 1.0 (ref)
Yes 1.13 (0.59e2.18) 1.14 (0.55e2.37)
Adjuvant therapy 0.014 0.049
No 1.0 (ref) 1.0 (ref)
Yes 2.45 (1.19e5.03) 2.24 (1.00e5.02)
CA19-9, carbohydrate antigen 19-9; FOLFIRINOX, leuocovorin, 5-FU, irinotecan, oxaliplatin; GA, gemcitabine plus nab-paclitaxel; HR, hazard ratio; ref,reference.*Normal or normalized after chemotherapy.
Vol. 231, No. 1, July 2020 Truty et al Celiac Axis Resection in Pancreatic Cancer 27

oncologic benefits when considering more advancedresection techniques. The purpose of this work was notto propose that such operations should be considered inall patients or at all centers, but rather stress anatomicalfeasibility of such extended operations that can offerpotentially significant survival benefit in highly selectedpatients after appropriate neoadjuvant sequencing whendone at centers with expertise with acceptable risks anddedication to the long-term management of any associ-ated consequences of such aggressive operations.
Author ContributionsStudy conception and design: Truty, Colglazier, Mendes,Nagorney, Bower, DeMartino, Oderich, Kendrick
Acquisition of data: Truty, Colglazier, Mendes, Nagor-ney, Bower, Smoot, DeMartino, Cleary, Oderich,Kendrick
Analysis and interpretation of data: Truty, Nagorney,Smoot, Cleary, Kendrick
Drafting of manuscript: Truty, Colglazier, Mendes,Nagorney, Bower, Smoot, DeMartino, Cleary, Oder-ich, Kendrick
Critical revision: Truty, Nagorney, Smoot, Cleary,Kendrick
REFERENCES
1. Berriochoa CA, Abdel-Wahab M, Leyrer CM, Khorana A,et al. Neoadjuvant chemoradiation for non-metastatic pancre-atic cancer increases margin-negative and node-negative ratesat resection. J Dig Dis 2017;18:642e649.
2. Fortner JG. Regional resection of cancer of the pancreas: a newsurgical approach. Surgery 1973;73:307e320.
3. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versusgemcitabine for metastatic pancreatic cancer. N Engl J Med2011;364:1817e1825.
4. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival inpancreatic cancer with nab-paclitaxel plus gemcitabine. N EnglJ Med 2013;369:1691e1703.
5. Truty MJ, Kendrick ML, Nagorney DM, et al. Factors predict-ing response, perioperative outcomes, and survival following to-tal neoadjuvant therapy for borderline/locally advancedpancreatic cancer. Ann Surg 2019 Apr 5 [Epub ahead of print].
6. Tee MC, Krajewski AC, Groeschl RT, et al. Indications andperioperative outcomes for pancreatectomy with arterial resec-tion. J Am Coll Surg 2018;227:255e269.
7. Iacobuzio-Donahue CA, Fu B, Yachida S, et al. DPC4 genestatus of the primary carcinoma correlates with patterns of fail-ure in patients with pancreatic cancer. J Clin Oncol 2009;27:1806e1813.
8. Kamisawa T, Isawa T, Koike M, et al. Hematogenous metas-tases of pancreatic ductal carcinoma. Pancreas 1995;11:345e349.
9. Mao C, Domenico DR, Kim K, et al. Observations on thedevelopmental patterns and the consequences of pancreaticexocrine adenocarcinoma. Findings of 154 autopsies. ArchSurg 1995;130:125e134.
10. Peixoto RD, Speers C, McGahan CE, et al. Prognostic factorsand sites of metastasis in unresectable locally advanced pancre-atic cancer. Cancer Med 2015;4:1171e1177.
11. Mayumi T, Nimura Y, Kamiya J, et al. Distal pancreatectomywith en bloc resection of the celiac artery for carcinoma of thebody and tail of the pancreas. Int J Pancreatol 1997;22:15e21.
12. Makary MA, Fishman EK, Cameron JL. Resection of the ce-liac axis for invasive pancreatic cancer. J Gastrointest Surg2005;9:503e507.
13. Beane JD, House MG, Pitt SC, et al. Distal pancreatectomywith celiac axis resection: what are the added risks? HPB (Ox-ford) 2015;17:777e784.
14. Klompmaker S, van Hilst J, Gerritsen SL, et al. Outcomes af-ter distal pancreatectomy with celiac axis resection for pancre-atic cancer: a Pan-European Retrospective Cohort Study. AnnSurg Oncol 2018;25:1440e1447.
15. Smoot RL, Donohue JH. Modified Appleby procedure forresection of tumors of the pancreatic body and tail with celiacaxis involvement. J Gastrointest Surg 2012;16:2167e2169.
16. Nakamura T, Hirano S, Noji T, et al. Distal pancreatectomywith en bloc celiac axis resection (modified Appleby proced-ure) for locally advanced pancreatic body cancer: a single-center review of 80 consecutive patients. Ann Surg Oncol2016;23[Suppl 5]:969e975.
17. Dindo D, Demartines N, Clavien PA. Classification of surgicalcomplications: a new proposal with evaluation in a cohort of6336 patients and results of a survey. Ann Surg 2004;240:205e213.
18. Bassi C, Dervenis C, Butturini G, et al. Postoperative pancre-atic fistula: an international study group (ISGPF) definition.Surgery 2005;138:8e13.
19. Shubert CR, Kendrick ML, Habermann EB, et al. Implemen-tation of prospective, surgeon-driven, risk-based pathway forpancreatoduodenectomy results in improved clinical outcomesand first year cost savings of $1 million. Surgery 2018;163:495e502.
20. Appleby LH. The coeliac axis in the expansion of the operationfor gastric carcinoma. Cancer 1953;6:704e707.
21. Takenaka H, Iwase K, Ohshima S, Hiranaka T. A new tech-nique for the resection of gastric cancer: modified Applebyprocedure with reconstruction of hepatic artery. World JSurg 1992;16:947e951.
22. Nimura Y, Hattori T, Miura K, et al. Resection of advancedpancreatic body-tail carcinoma by Appleby’s operation. Shu-jutu 1976;30:885e889.
23. Hirano S, Kondo S, Hara T, et al. Distal pancreatectomywith en bloc celiac axis resection for locally advanced pancre-atic body cancer: long-term results. Ann Surg 2007;246:46e51.
24. Latona JA, Lamb KM, Pucci MJ, et al. Modified Applebyprocedure with arterial reconstruction for locally advancedpancreatic adenocarcinoma: a literature review and reportof three unusual cases. J Gastrointest Surg 2016;20:300e306.
25. Konishi M, Kinoshita T, Nakagori T, et al. Distal pancreatec-tomy with resection of the celiac axis and reconstruction of thehepatic artery for carcinoma of the body and tail of thepancreas. J Hepatobiliary Pancreat Surg 2000;7:183e187.
26. Miyakawa S, Horiguchi A, Hanai T, et al. Monitoring hepaticvenous hemoglobin oxygen saturation during Appleby opera-tion for pancreatic cancer. Hepatogastroenterology 2002;49:817e821.
28 Truty et al Celiac Axis Resection in Pancreatic Cancer J Am Coll Surg

27. Kondo S, Ambo Y, Katoh H, et al. Middle colic artery-gastroepiploic artery bypass for compromised collateral flowin distal pancreatectomy with celiac artery resection. Hepato-gastroenterology 2003;50:305e307.
28. Gagandeep S, Artinyan A, Jabbour N, et al. Extended pancre-atectomy with resection of the celiac axis: the modifiedAppleby operation. Am J Surg 2006;192:330e335.
29. Machado MA, Surjan RC, Nishinari K, et al. Iliac-hepaticarterial bypass for compromised collateral flow during modi-fied Appleby operation for advanced pancreatic cancer. Eur JSurg Oncol 2009;35:1124e1127.
30. Wu X, Tao R, Lei R, et al. Distal pancreatectomy combinedwith celiac axis resection in treatment of carcinoma of thebody/tail of the pancreas: a single-center experience. AnnSurg Oncol 2010;17:1359e1366.
31. Bockhorn M, Burdelski C, Bogoevski D, et al. Arterial en blocresection for pancreatic carcinoma. Br J Surg 2011;98:86e92.
32. Baumgartner JM, Krasinskas A, Daouadi M, et al. Distalpancreatectomy with en bloc celiac axis resection for locallyadvanced pancreatic adenocarcinoma following neoadjuvanttherapy. J Gastrointest Surg 2012;16:1152e1159.
33. Ielpo B, Ferri V, Caruso R, et al. Alternative arterial recon-struction after extended pancreatectomy. Case report andsome considerations of locally advanced pancreatic cancer.JOP 2013;14:432e437.
34. Christians KK, Pilgrim CH, Tsai S, et al. Arterial resection atthe time of pancreatectomy for cancer. Surgery 2014;155:919e926.
35. Mittal A, de Reuver PR, Shanbhag S, et al. Distal pancreatec-tomy, splenectomy, and celiac axis resection (DPS-CAR): com-mon hepatic arterial stump pressure should determine the needfor arterial reconstruction. Surgery 2015;157:811e817.
36. Peters NA, Javed AA, Cameron JL, et al. Modified Applebyprocedure for pancreatic adenocarcinoma: does improved neo-adjuvant therapy warrant such an aggressive approach? AnnSurg Oncol 2016;23:3757e3764.
37. Ocuin LM, Miller-Ocuin JL, Novak SM, et al. Robotic andopen distal pancreatectomy with celiac axis resection for locallyadvanced pancreatic body tumors: a single institutional assess-ment of perioperative outcomes and survival. HPB (Oxford)2016;18:835e842.
38. Gong H, Ma R, Gong J, et al. Distal pancreatectomy with enbloc celiac axis resection for locally advanced pancreatic cancer:a systematic review and meta-analysis. Medicine 2016;95:e3061.
39. Klompmaker S, Peters NA, van Hilst J, et al. Outcomes andrisk score for distal pancreatectomy with celiac axis resection(DP-CAR): an international multicenter analysis. Ann SurgOncol 2019;26:772e781.
40. Reni M, Zanon S, Balzano G, et al. Selecting patients forresection after primary chemotherapy for non-metastaticpancreatic adenocarcinoma. Ann Oncol 2017;28:2786e2792.
41. van Veldhuisen E, Vogel JA, Klompmaker S, et al. Addedvalue of CA19-9 response in predicting resectability of locallyadvanced pancreatic cancer following induction chemotherapy.HPB (Oxford) 2018;20:605e611.
42. Bergquist JR, Puig CA, Shubert CR, et al. Carbohydrate anti-gen 19-9 elevation in anatomically resectable, early stagepancreatic cancer is independently associated with decreasedoverall survival and an indication for neoadjuvant therapy: aNational Cancer Database study. J Am Coll Surg 2016;223:52e65.
43. Hartwig W, Strobel O, Hinz U, et al. CA19-9 in potentiallyresectable pancreatic cancer: perspective to adjust surgical andperioperative therapy. Ann Surg Oncol 2013;20:2188e2196.
44. Cassinotto C, Mouries A, Lafourcade JP, et al. Locallyadvanced pancreatic adenocarcinoma: reassessment of responsewith CT after neoadjuvant chemotherapy and radiation ther-apy. Radiology 2014;273:108e116.
45. Ferrone CR, Marchegiani G, Hong TS, et al. Radiological andsurgical implications of neoadjuvant treatment with FOLFIR-INOX for locally advanced and borderline resectable pancre-atic cancer. Ann Surg 2015;261:12e17.
46. Katz MH, Fleming JB, Bhosale P, et al. Response of borderlineresectable pancreatic cancer to neoadjuvant therapy is not re-flected by radiographic indicators. Cancer 2012;118:5749e5756.
47. Panda A, Garg I, Johnson GB, et al. Molecular radionuclideimaging of pancreatic neoplasms. Lancet Gastroenterol Hepa-tol 2019;4:559e570.
48. Kharofa J, Mierzwa M, Olowokure O, et al. Pattern of mar-ginal local failure in a phase ii trial of neoadjuvant chemo-therapy and stereotactic body radiation therapy for resectableand borderline resectable pancreas cancer. Am J Clin Oncol2019;42:247e252.
49. Hackert T, Strobel O, Michalski CW, et al. The TRIANGLEoperationdradical surgery after neoadjuvant treatment foradvanced pancreatic cancer: a single arm observational study.HPB (Oxford) 2017;19:1001e1007.
Discussion
DR AMANDA ARRINGTON (Tucson, AZ): The authors report a24-year history of celiac access resection for pancreatic cancer. Indoing so, they described the classification system of celiac involve-ment based on the extent of arterial involvement. Most of the casesin this series were within the Class I and Class II subcategories,which involved the celiac access, and to a much lesser extent, thesuperior mesenteric artery (SMA). Class III arterial involvementinvolved the SMA in its entirety.
Even in my own institution, I suggest that this level of involve-ment of cancer, particularly in the Class III cases, is unresectable,and we give all these patients chemotherapy. One of the biggest pre-dictors is response to chemotherapy, as well as the extent of chemo-therapy up front.
The authors acknowledge high complication and recurrencerates, with nearly all patients having a recurrence within 2 years.With today’s chemotherapy, a lot of these patients are survivingto 2 years without this type of operation. Your study reports verysignificant complication, with an overall morbidity rate of 74%,with all grades. That is obviously well beyond the standard ofcomplication profile of a basic pancreatic cancer without arterialinvolvement. Is there a “never” event that you would considertoo great of a complication to suggest this operation? Other thanmentioning there were no patients with Class III tumors who devel-oped bowel ischemia after SMA revascularization, was the compli-cation profile in the Class III cases higher than in the other 2 cases?
Vol. 231, No. 1, July 2020 Truty et al Discussion 29


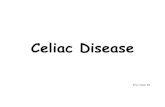








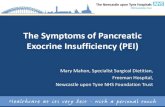






![Pancreatic Cancer: Are We Moving Forward Yet?advanced pancreatic cancer. Early studies, such GITSG [6] have shown a benefit of adjuvant chemo-radiotherapy after surgical resection](https://static.fdocuments.net/doc/165x107/5e98446cfcb7211c445def30/pancreatic-cancer-are-we-moving-forward-yet-advanced-pancreatic-cancer-early.jpg)