EMR Can anyone do this? - American College of...
23
Norio Fukami, MD EMR Can anyone do this? Norio Fukami, MD University of Colorado Piecemeal resection? Piecemeal resection? ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology 1
-
Upload
truongtruc -
Category
Documents
-
view
219 -
download
2
Transcript of EMR Can anyone do this? - American College of...

Norio Fukami, MD
EMRCan anyone do this?
Norio Fukami, MD
University of Colorado
Piecemeal resection?Piecemeal resection?
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
1

Norio Fukami, MD
Endoscopic mucosal resection (EMR) and
Endoscopic submucosal dissection (ESD)
Endoscopic mucosal resection (EMR) and
Endoscopic submucosal dissection (ESD)
Endoscopic removal of premalignant or malignant
gastrointestinal epithelium
= Minimally invasive endosurgical treatment of GI
tumors = Diagnostic and Therapeutic procedure
• Can remove certain submucosal tumors
e.g. Granular cell tumor, Carcinoid; GIST (?)
History of EMR & ESDHistory of EMR & ESDSimple snare removal (1968)
Saline injection and snare resection (1983)(1983)
Double channel - pinch and cut (1984)
Band and resect (1993)
Movement to explore Endoscopic removal as an alternative to Surgery
EMR cap method (1993)
Endoscopic submucosal dissection (mid-late 1990s) Soetikno et al. GIE. 2003(4)
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
2

Norio Fukami, MD
EMR toolsEMR tools
• Snare
• injection
• Cap-EMR
• Band-EMR
ESD knivesESD knives
KD 10Q-1
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
3

Norio Fukami, MD
EMR/ESD for the cure of cancer
EMR/ESD for the cure of cancer
Resection of premalignant or malignant lesion as an alternative to surgeryas an alternative to surgery
Aimed for R0 resection
Negative lateral and deep margin = local recurrence
Cure = No or very low risk for lymph node metastasis or distant metastasis
Preprocedural assessment is mandatoryPreprocedural assessment is mandatory
Know when to do it! - Exclude possible non-candidate
Weigh risk and benefit
Re-assessment after resection: Pathological evaluation
Cancer T stageCancer T stage
• Depth of cancer invasion
T3T1 T2
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
4

Norio Fukami, MD
Sub-classification of T1 tumorSub-classification of T1 tumor
• m1: limited within mucosa (HGD)
• m2: invades into lamina propria
• m3: invades into muscularis mucosae
T1
T2• sm1 - 3:
• divide submucosal layer in three even thickness
Soetikno et al. GIE. 2003(4)
T2
Esophageal cancerEsophageal cancer
AJCC/UICC TNM, 7th edition
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
5

Norio Fukami, MD
Colon cancerColon cancer
AJCC/UICC TNM, 7th edition
Lymph node metastasis risk for T1 tumor varies
Lymph node metastasis risk for T1 tumor varies
EMR b l t i di ti• EMR absolute indication
Esophagus SCC
Esophagus Adeno Ca
Stomach Colon
m1 0%0%
0-0.4% 0%m2 3%
m3 9% 2 3%
Important Factors: lymphovascular invasion, tumor differentiation, tumor budding
m3 9% 2-3%
sm1 15-20%
13~48%
~2.5%
10~%sm235~50% ~20%
sm3
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
6

Norio Fukami, MD
How far can we go?
Expanded indications
How far can we go?
Expanded indicationspp
Esophageal cancer (mostly SCC)
Esophageal cancer (mostly SCC)
T1-m1-m2: LN mets 0-3%
T1 m3-sm1: LN mets 10-20%
• But, LN mets 4% if “differentiated type”&
• “no LV invasion”
• “expansion growth”*1
*1 Oyama et al. 2002
&
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
7

Norio Fukami, MD
Esophageal cancer (Barrett cancer)
Esophageal cancer (Barrett cancer)
sm1 invasion: 9.5% LN mets if LV(-) vs. 20% if LV (+) *1
sm1 invasion with LV(-), differentiated type, expansive growth:
•- No clinical evidence of metastasis, cancer death during the mean f/u 62 months *2
*1 Badreddine et al. CGH 2010*2 Manner et al. AJG 2008
Gastric cancerGastric cancer
Expanded indication
less than 500 μm
Soetikno et al. J Clin Oncol. 2005LN mets; 0-2.5% Gotoda et al. Gastric Cancer 2000
0-0.96% Hirasawa et al. Gastric Cancer 2009
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
8

Norio Fukami, MD
Colon cancerColon cancer
SM invasion is not considered to be absolute surgical contraindication for endoscopic therapy
- no LN mets in the absence of LV invasion less than 3000 μm invasion depth for polypoid less than 1000 μm invasion depth for non-polypoid lesions*1
*1 Kitajima et al. J Gastroenterol 2004p yp
SM indication for EMR/ESD: less than 1000 μm depth of invasion, differentiated type, no LVI, and no tumor budding.
j
Master’s guide for endoscopic diagnosis. Tajiri and Saito. 2011
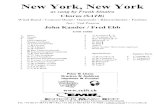
Lymph node metastasis risk for T1 tumor
Lymph node metastasis risk for T1 tumor
EMR b l t i di ti d d i di ti• EMR absolute indication expanded indication
Esophagus SCC
Esophagus Adeno Ca
Stomach Colon
m1 0%0%
0-0.4% 0%m2 3%
m3 9% 2 3%
Important Factors: lymphovascular invasion, tumor differentiation, tumor budding
m3 9% 2-3%
sm1 15-20%
13~48%
~2.5%
10~%sm235~50% ~20%
sm3
1000 μm500 μm superficial sm invasion
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
9

Norio Fukami, MD
Diagnostic or Therapeutic?p
Basic techniquefor
pathology specimen processing
Specimen processingSpecimen processingEvaluation of the margins (lateral/deep) requires perpendicular slices
Pinnig specimens onto the boardonto the board before formalin fixation
Good!
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
10

Norio Fukami, MD
Stage/depth assessmentStage/depth assessment
Meticulous evaluation:
Endoscopic assessment of cancer to predict T stage
Endoscopic assessment of cancer to predict T stage
Meticulous evaluation: 85-95% accurate (Tm1-2, 3 vs. sm superficial vs. deep invasion)
- superficial type of esophageal SCC p yp p g(0-IIa-c) and <2cm = m1-2
EUS with HF probe: 80-90% accuracy
Paris workshop group. GIE 2003
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
11

Norio Fukami, MD
What to look for?What to look for?
Configuration
Fold convergence (thickening, irregularity etc.)
Depression
Loss of surface patterns or abnormal vessels
Stiffness of the wall
What to look for as a sign of deep invasion?
Master’s guide for endoscopic diagnosis. Tajiri and Saito. 2011
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
12

Norio Fukami, MD
Case studyesophagusCase studyesophagus
SCC moderately differentiated, 2.4cm, sm1 no LV invasion
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
13

Norio Fukami, MD
well differentiated adenocarcinoma, T1a (m2)
poorly differentiated adenocarcinoma, T3N1
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
14

Norio Fukami, MD
Barrett’s esophagus with LGD
adecarcinoma in Barrett’s, T1sm-T2
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
15

Norio Fukami, MD
Barrett’s esophagus with poorly differentiated adenocarcinomaT1sm, N1 at upper paratracheal LN
stomachstomach
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
16

Norio Fukami, MD
well differentiated adenocarcinoma, T1a (m2)
6cm poorly differentiated adenocarcinoma, T1bpositive deep margin total gastrectomy no tumor and negative LN
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
17

Norio Fukami, MD
differentiated adenocarcinoma, T1a (m3), UL +
Master’s guide for endoscopic diagnosis. Tajiri and Saito. 2011
Master’s guide for endoscopic diagnosis. Tajiri and Saito. 2011
poorly differentiated adenocarcinoma, T1a (m3)
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
18

Norio Fukami, MD
coloncolon
Tubular adenoma
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
19

Norio Fukami, MD
invasive adenocarcinoma, T2
High Grade Dysplasia
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
20

Norio Fukami, MD
Master’s guide for endoscopic diagnosis. Tajiri and Saito. 2011
8mm moderately differentiated adenocarcinoma, T1sm, 3700 μm
adenocarcinoma, T2
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
21

Norio Fukami, MD
adenocarcinoma, Tis (invasive to lp)
LST, granular type 5.5cm, Tis
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
22

Norio Fukami, MD
ConclusionsConclusions
• You can do it! - Learn the proper steps
Understand the proper indication and the assessment for curative resection
Pre-EMR/ESD evaluation is important to select the treatment modality - cut BIG as necessary!
Process the specimen properly = prediction of the outcome and risk for recurrence
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
23