Empowering the Frontline: What we can achieve when the ... · •Telephone clinics for routine and...
30
Empowering the Frontline: What we can achieve when the conditions are right Dr Catherine Briggs Clinical Advisor to NHS England Elective Care Transformation Programme Kate Branchett Senior Policy and Implementation Manager NHS England
Transcript of Empowering the Frontline: What we can achieve when the ... · •Telephone clinics for routine and...

Empowering the Frontline: What we can achieve when the conditions are
right
Dr Catherine Briggs Clinical Advisor to NHS England Elective Care Transformation Programme
Kate Branchett Senior Policy and Implementation Manager NHS England

Why transform elective care systems?
• National policy:• The 5YFV emphasised the need to reduce avoidable demand in
elective care services through redesign of clinical pathways.
• It highlighted unwarranted variation in referral rates between practices and between CCGs.
• The 2017-19 NHS Operational Planning and Contracting Guidance says reducing demand is a ‘must-do’.
• The NHS Standard Contract requires CCGs to ensure GP referrals are clinically appropriate and in line with agreed pathways and protocols.

Why transform elective care system?
• Clinical Perspective:
– Referral vortex– Outpatient conveyer belt
• …Improve patient experience• …?Improve clinical team experience• …Better manage demand and waiting times

National Elective Care Transformation Programme
• Specialty Based Transformation – the magic of frontline change
• High Impact Interventions - assessing evidence and working with the frontline teams and stakeholders to develop service specifications. Eg MSK clinical triage and clinical peer review specifications in 17/18; first contact practitioner and ophthalmology for 18/19
• Diversion of referrals – diverting referrals from challenged providers so more patients are seen within 18 weeks

Specialty Based TransformationSupporting local health and care systems to agree and test interventions
aimed at reducing referrals and improving outpatient arrangements in just 100 days.
Principles:• Three themes• 100 day challenge process
– Pace of change• Identifying teams• Defining the ask • Senior permission to ‘get on and do’
Re-thinkingreferrals
Shared Decision Making and Self-ManagementSupport
Transformingoutpatients

Specialty Based Transformation• Five (actually 6) waves of four sites testing
interventions in 14 high volume specialties
• Clinically led interventions
• Production of handbooks outlining the interventions tested, including challenges and successes
• Learning shared quickly to aid broader systems to deliver rapid system change.
• Many of the interventions can be applied –or adapted – to other specialties
• Stockport involvement in Waves 0,1 and 2
The ripple effect – how we influence the system

WaveSpecialities / pathways to be tested
Sites Indicative testing period
Elective Care Speciality Handbooks due date
1 • T&O• Gastro
FrimleyFylde CoastSomersetStockport
February – June 2017
March 2017 (first release to regions)November 2017 (refresh post development collaborative) HANDBOOKS PUBLISHED
2• Diabetes• Dermatology• Ophthalmology
Central NorfolkDorsetLincolnshireStockport
December – April 2018 April 2018
3• Cardiology• ENT• Urology
Doncaster & BassetlawDudleySomersetWest Suffolk
January – May 2018 June 2018
4• Respiratory• General surgery• Gynaecology
TBC May – August 2018 September 2018
5• General
medicine• Neurology• Radiology
TBC September –December 2018 January 2019
Specialty Based Transformation indicative timetable

The 100 Day Challenge Process
• Whole system teams
• Measurable goals
• Urgency
• Real time testing
• Real time data
• Coaching
• Sponsorship and support
• Permission.

Transforming MSK services
• Since 2005/6 OPD appointments increased from 60.8m to 118.6m
• MSK conditions affect 9.6 million adults in UK• Osteoarthritis causes joint pain in 8.5 million people in the UK• >20% of GP appointments for MSK problems
• NHSE Elective Care Transformation Team selected Stockport NHS/Stockport Together in collaboration with 3 other NHS trusts to rethink the orthopaedic pathway

The Stockport 100 day team
• Multidisciplinary approach to pathway redesign
– Patient representatives– Third sector– GP and practice manager– Community pharmacist– Orthopaedic consultant and Extended Scope Practitioner– Foundation Trust manager

Stockport’s 100 day approach
• Whole pathway review• Rethinking referrals – Improving the quality standardised
pathways & referral templates• Maximising shared decision making & self
management support – improved access to self-management support & education for long term conditions
• Transforming outpatients – virtual follow ups to better meet peoples needs & improve access to timely care
• https://www.england.nhs.uk/wp-content/uploads/2017/11/msk-orthopaedic-elective-care-handbook-v2.pdf

Rethinking Referrals
• Standardised referral template – improve consistency of information– fit for surgery information included– Less work rather than more
• Shared with practices– continued increase in use with continued effort to
engage and support • Challenge in encouraging practices to trial

Referral Template
Practice Details Patient Details
GP Practice address: Organisation Full Address (stacked) GP Practice Telephone: Organisation Telephone Number GP Practice Fax No: Organisation Fax Number Referring GP: GMC number: Usual GP: Usual GP Full Name GMC number: Usual GP GMC Number Date of referral: Short date letter merged
Patient name: Full Name Title Calling Name Surname Address: Home Full Address (stacked) NHS No: NHS Number Hospital No: DoB: Date of Birth Gender: Gender Home telephone: Patient Home Telephone Mobile telephone: Patient Mobile Telephone Alternate number: Email address: Patient E-mail Address Interpreter required? : Yes No If yes, language: Main Language
Speciality requested: (including specific clinic if relevant) Free Text Prompt Advice or Appointment?: Free Text Prompt Urgent or Routine?: Free Text Prompt Reason for Referral (what is the question that needs answering?) Free Text Prompt Last relevant consultation(s): Consultations Additional history / examination findings, if not covered in consultations above: (include previous investigations and treatments tried) Any information regarding patient’s understanding or expectation of referral? Medication Please enter reason if any medication stopped: Allergies / adverse reactions: Allergies Significant Co-Morbidities: (including details of other consultants involved in care) Enter free text here: Problems
Other relevant issues – (including mental capacity, carer role, social situation) Is patient being referred for consideration of surgery? Please answer Yes or No Free Text Prompt Is the procedure covered by EUR policy? Please answer Yes or No or N/A Free Text Prompt If the procedure is covered by EUR policies please indicate the justification for referral: Is the patient fit for surgery? (including advice regarding smoking cessation and weight loss where appropriate) Please answer Yes or No or N/A Free Text Prompt BP: Single Code Entry: O/E - blood pressure reading Weight: Single Code Entry: O/E - weight BMI: Single Code Entry: Body mass index Tobacco: Single Code Entry: Tobacco consumption HbA1C: Single Code Entry: Hb. A1C - diabetic control Hb: Single Code Entry: Haemoglobin estimation TSH: Single Code Entry: Serum TSH level eGFR: Single Code Entry: GFR calculated abbreviated MDRD Admissions avoidance care plan? : Agreed: Single Code Entry: Admission avoidance care plan agreed Review: Single Code Entry: Review of admission avoidance care plan Ended: Single Code Entry: Admission avoidance care ended Fitness rating (ECOG): 0 - Fully active 1 - Unable to do strenuous activity 2 - Able to walk and self-care 3 - Only able to carry out limited self-care. Mainly confined to bed/chair 4 - Bed/chair bound. Unable to self-care Does patient have mental capacity to consent to investigation? : Yes No Number of attachments (Please see below)
V17 Referral form

Shared Decision Making and Self-Management Support
• In 100 day time frame, set up and delivered workshop
• GP or Self referral – advertised in pharmacies, golf clubs, GP surgeries
• Distribution of ‘Patient Passport’ to aid self management


OA Knee Workshop• 90 minute self referral workshop• Multidisciplinary team, social care
organisations and expert patients delivering talks on all aspects of OA knee, eg what is OA? Surgical risks, what your pharmacy can do for you, OA mythbusters
• Stands by different organisations –eg podiatry, TPA, abl, PARIS
• Since April 2017, 8 workshops with 223 attendees
• Excellent feedback• Next workshop 11th June 2018


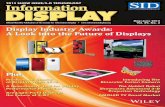
OA Knee Self Referred Workshop
6 8
7
50
9
2
48
0
10
20
30
40
50
60
70
Before event After event
Num
ber o
f res
ponc
es
Patient confidence in managing their condition before and after event
(28/06/17)
Very confident in managing knee condition
Patially confident in managing knee condition
Not confident in managing knee condition
No answer

Qualitative Analysis of Knee Workshop – June 2017
34
18
3 1
9
0
5
10
15
20
25
30
35
40
Mostdefinitely
Probably Not really No, not atall.
NotAnswered
# of
pat
ient
s
Patient view on whether workshop would have been beneficial when knee pain first
started(28/06/17)
32
19
1 3
9
0
5
10
15
20
25
30
35
Extremelylikely
Likely Don't know Extremelyunlikely
NotAnswered
# of
pat
ient
s
Patient view on whether they would recommend the workshop
(28/06/17)


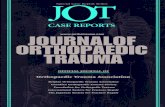
About meName:
DOB: NHS Number:GP:
Which joints cause me pain?
My X-Ray/Scan results (last 5 years)
Investigation
Joint (left/right)
Date (DD/MM/YY)
ResultVerif
ied by
Previous surgery/physiotherapy/injection for myknee pain
Surgery (type): Date:
Outcome:
Physiotherapy: Date:
Outcome:
Injection: Date:
Outcome:
Long Term Health Conditions e.g.Diabetes/angina etc.
Current Medication (attach prescription if easier)
My Height: Weight:BMI:
Non smoker Ex smoker Smoker (no per
day) Alcohol (units per week)My Knee OsteoarthritisPassport
About me
My Knee Osteoarthritis Passport

Transforming Out-patients• Telephone clinics for routine and post-diagnostic
orthopaedic follow ups • Run by ESP’s and advanced nurse practitioners• Initially piloted in knee, shoulder and hand clinics for 100
day project • Now also Spine and virtual fracture clinics • Telephone follow ups now account for 9.8% of all
orthopaedic follow ups (exclude # and paeds) compared with 2% last year
• Virtual Fracture Clinic – 27% reduction in new F2F fracture clinic appointments (consistent with no. discharged from virtual with advice)

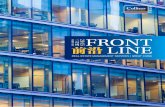
As of 31st August 2017, 13.5% of telephone FU contacted required converting to a F2F, 50% were discharged from telephone FU, 37 % were further managed from telephone appointment eg listed for surgery, referred further investigations. (N=147 outcomed as
contacted)
List for guided injection, 5
List for surgery, 22
Further investigation , 9
Further phone follow-up, 12
Redirect to physio, 6
Face to face required, 20
Discharged(inc lg term arthroplasty fu n=11), 63
Redirect to more appropriate service, 6
Discharged to physio, 4
Comparison of Telephone Outcomes - discharged v F2F rebooked v further management by telephone
List for guided injection
List for surgery
Further investigation
Further phone follow-up
Redirect to physio
Face to face required
Discharged(inc lg termarthroplasty fu n=11)
Redirect to moreappropriate service
Discharged to physio
RED - F2F requiredBLUE - avoided unnecessary F2F and further clinical decision made egsurgery/investigationsGREEN - discharged from Relevant Orthopaedic Speciality

22
3
Preference of telephone v F2F appoiontment
prefers telephone apt prefers f2fno preference
As of 31st August, 88% (21 )patients who responded to a survey regarding the telephone follow up appointments would prefer telephone follow up to F2F appointment.
Qualitative Analysis of Telephone Follow Up
2080%
14%
Patients satisfaction with the outcome of the telephone
consultation?
Very happy quite happy fairly happy
80% (20 )patients who responded to a survey regarding the telephone follow up appointments were completely satisfied with the approach, advice and outcome,

Other Rapid Testing Projects undertaken locally
• Cardio-Respiratory Breathe Clinic• Gastroenterology – IBD and fatty liver pathways• Diabetes – Upskilling primary care and patient
education workshops• Dermatology –One Stop Clinics, Virtual Transfer
of Images (Advice and Guidance), ‘Direct’ Listing from Dermatology to ENT
• Ophthalmology -Virtual Glaucoma clinics within primary care optometry practices

Outcomes so far..
• 100 day projects started in 2016• All new services from Wave 0 continue
• Breathe clinic• Telephone/opt in follow up for IBD with rapid access for urgent
flare ups
• Wave 1• Work shared through NHS England Handbooks in gastro and
MSK
• Wave 2 • Ongoing work – day 80

Outcomes so far..
• Better cross-team working and learning from each other (cardio/resp)
• Shorter waits for urgent appointments (IBD) • Potential for positive impact on urgent care
• Cross GM working (Dermatology)• Community optometrist-led glaucoma clinics
• Ongoing data collection to quantify benefits

Capturing the Magic..
• Multidisciplinary approach (cross-system)• Clarity of high level aims given to team• Permission to design ‘without interference’• Freedom to learn from mistakes and change plans ‘as you go’• Maintenance of pace
• Day 25/50/75/100 touch base meetings• New energy level from teams when given freedom to develop
own ideas• 100 day ideas and approach adapted into other specialties

Hold these ideas….
Please…:• Capture your thoughts• Consider opportunities within localities?• Take ideas into the workshops and afternoon sessions• We want to hear from you
?Join:– NHS England Community of Practice– NHS England Clinical Advocate Network

References and contacts
• [email protected]• [email protected]
• http://www.england.nhs.uk/elective-care-transformation/handbooks-and-case-studies/