

Emory Osteoarthritis Clinical Pathwayortho.emory.edu/documents/Symposium 2016 Talks/Mines-OA...
40
Emory Osteoarthritis Clinical Pathway Brandon Mines, MD Emory Sports Medicine Center
Transcript of Emory Osteoarthritis Clinical Pathwayortho.emory.edu/documents/Symposium 2016 Talks/Mines-OA...
Emory Osteoarthritis
Clinical PathwayBrandon Mines, MD
Emory Sports Medicine Center
Nothing to disclose
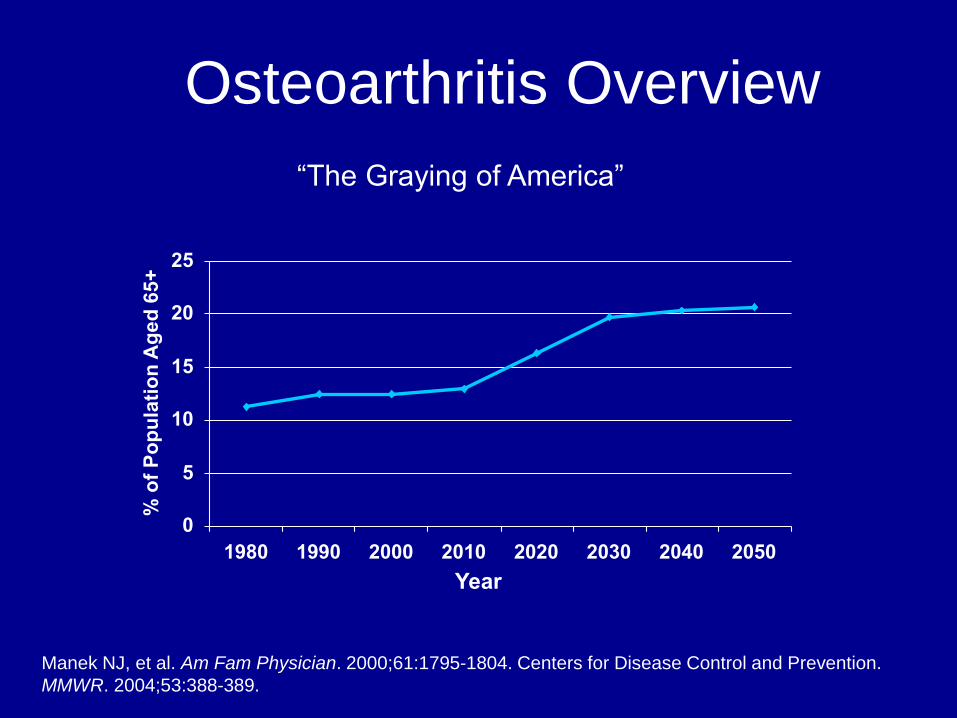
Osteoarthritis Overview
“The Graying of America”
Manek NJ, et al. Am Fam Physician. 2000;61:1795-1804. Centers for Disease Control and Prevention.
MMWR. 2004;53:388-389.
Year
0
5
10
15
20
25
1980 1990 2000 2010 2020 2030 2040 2050
% o
f P
op
ula
tio
n A
ge
d 6
5+

OA Prevalence Most common form of joint disease worldwide
Radiographic evidence
>50% at 65 years of age
≈80% at 75 years of age and older
Symptomatic OA of knee
11% of people >64 years of age
Manek NJ, et al. Am Fam Physician. 2000;61:1795-1804.

OA Pathophysiology Erosion of cartilage
Decrease in concentration and viscosity of synovial fluid
Decreased lubricating and cushioning properties of the joint
Secondary inflammation
Subchondral damage
Microfractures
Cyst formation

Clinical Pathway
A work in progress
Broad spectrum of physicians, interests, experiences
and opinions
We see different types of patients
Different patients have different expectations

Clinical Pathway That being said…
First, do no harm
Least Most invasive
Educate
Don’t give false hope, but be optimistic
Be brutally honest...in a nice way
Social network is important
Friends
Family
Support groups/system
If one feels defeated, then one is defeated

Case
45 yo male, recreational athlete
Enjoys running, tennis,
mountain biking and cross fit
Intermittent knee pain
No reported injuries
Overall, feels limited on how
much he can do and how long
he can do it
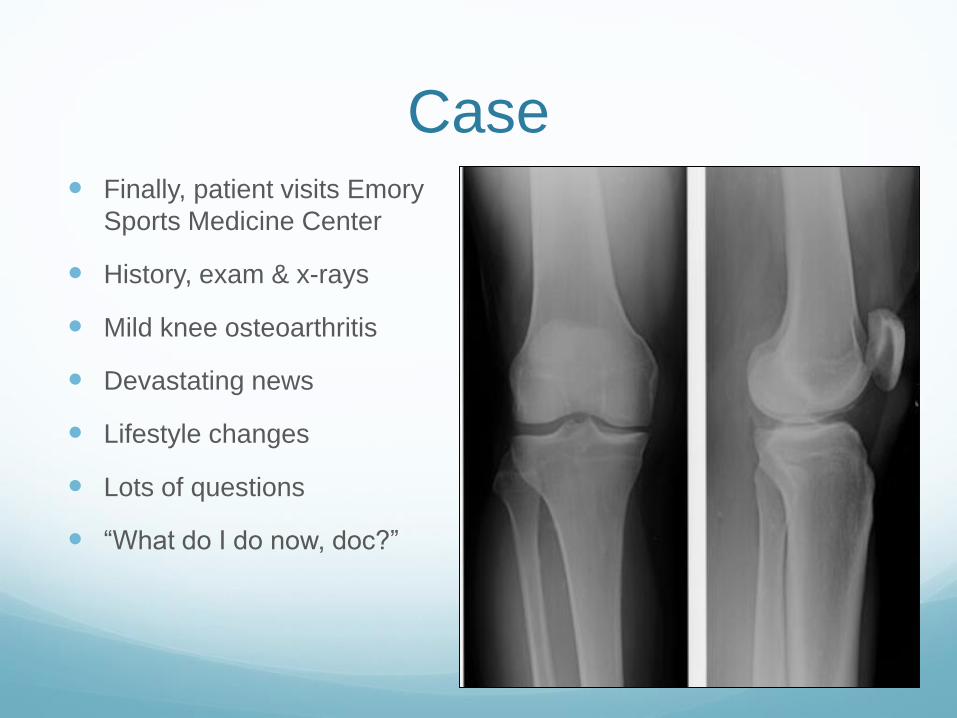
Case Finally, patient visits Emory
Sports Medicine Center
History, exam & x-rays
Mild knee osteoarthritis
Devastating news
Lifestyle changes
Lots of questions
“What do I do now, doc?”

Osteoarthritis
www.physio-pedia.com

Osteoarthritis Pathway
Currently a work in progress for us
Reviewing data & best clinical practices
Evidence based medicine vs. consensus statement
What I have always done versus what the evidence
says I should do
What does our patient need to hear 1st?...
Education:
Takes time, but needs to understand what he is up against
Needs to be in terms he can digest & accept
Don’t forget learner types See it, read it, hear it
Needs to absorb/accept diagnosis

Education This gets glossed over very
often
At Emory:
Anatomical models
Tablet videos
Pictures
Website recommendations
www.arthritis.org
www.emoryhealthcare.org
Takes time, but time well spent!

Rehabilitation “I already have a trainer at the gym”
“I’ll just get some exercises off the internet”
At Emory:
Vitally important to discuss the role of rehabilitation
Explain differences
personal trainer
google-derived exercises
physical therapy
Several studies have shown beneficial outcomes in regards to
rehabilitation and self-management programs

Rehabilitation
Coleman et al, 2012
Patients in a 6 week self-management program
Statistically significant
Improved WOMAC score
Less stiffness
Improved function
Rehabilitation
Deyle et al, 2000
Physical therapy and Osteoarthritis
Statistically significant:
Improvement in WOMAC scores with PT and knee
exercises

What fits your schedule better? Exercising 1 hour per day or
being dead 24 hours a day?

Case “Ok, Ok, I hear ya doc, but
what exercise CAN I do?”
Exercise:
At Emory: Keep moving!
Watch out for impact
activities
Prefer bike, elliptical,
walking, etc.
Water sports/aerobics
Everything in moderation

We assume patient KNOWS they need to lose
weight....
Makes an out of you & me
Patient says, “you think that would make a real
difference?”

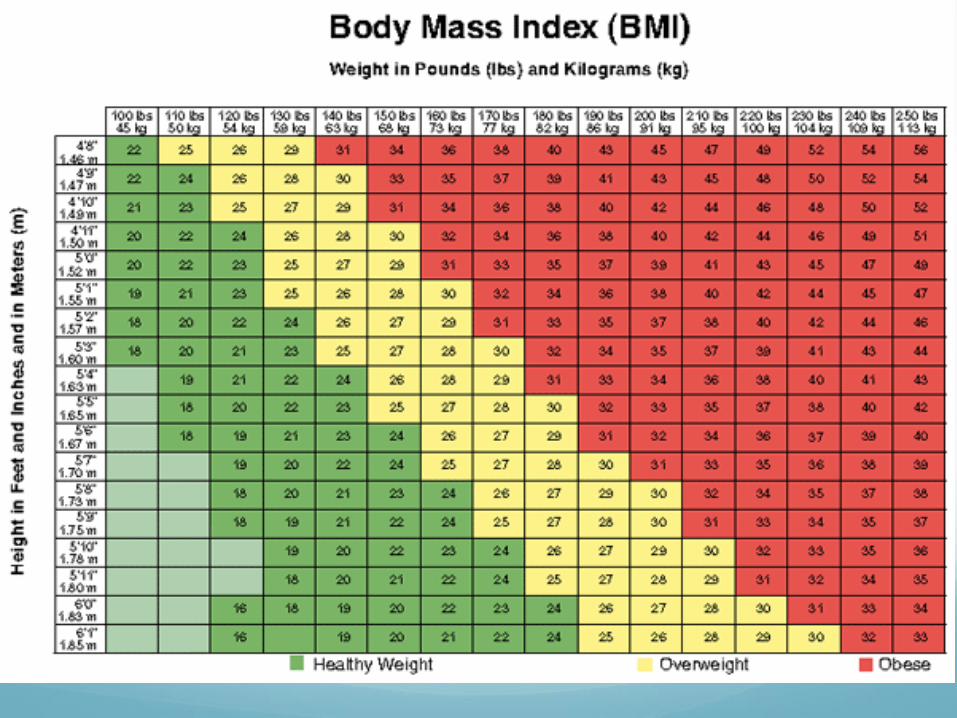
Case: Weight Loss
How much is suggested?
At Emory:
Goal is getting to ideal body weight
Surgical standpoint:
Under 30-35 BMI at least

Weight Loss Toivanen et al
22 year follow up
Risk of knee OA was 7 times greater for BMI > 30
compared to BMI < 25
Case “Doc, how am I suppose to lose weight and stay active
if my knee hurts so bad right now?”
NSAIDs:
At Emory:
Start with OTCs
Less $
Easier access
Educate on how to take them

NSAIDS
Many studies have looked at this
Selective NSAIDs (i.e. Celebrex)
Non-selective NSAIDs (i.e. Ibuprofen)
Statistically significant improvements in pain
Compared to placebo

Case: NSAIDs
May need to try prescription NSAIDs
Topicals may be better tolerated
Diclofenac – less cardiac, GI, renal side effects
Tylenol has been shown to not be better than placebo
We recommend avoiding Tylenol at this time
Not helping pain
People tend to take too much

Case “I’m going to need something that starts making me feel
better faster than that!”
Corticosteroid injections:
Widely done and widely accepted as OK to do
Chao et al, 2010
Compared to saline
WOMAC scores statistically better at 4 weeks

Case: Corticosteroid Technique may make a difference
Ultrasound guidance, when needed/able
Patient comfort for knee aspiration
Quick point-of-care hip joint injection
No need to re-schedule for fluoro-guided injection
If time allows, can do right there in office
Mild OA responds better than severe OA

Case “that’s great doc, but do you have something that may
give relief longer than cortisone?”
Viscosupplementation:
Hyaluronic acid
Rooster comb; recombinant DNA/bacteria
Lubricate joint
Controversial product
Does it really work?

Case American Academy of Orthopaedic Surgeons (AAOS) does not
recommend but American Medical Society for Sports Medicine (AMSSM) does recommend
Based on method of reviewing the data
Complicated but related to how you interpret patient pain scores
In either case, it is still covered by insurance plans
In my hands…
70% - 75% of mild/moderate knee OA patients are happy they did it
Severe OA success drops to 20% - 30% of patients get relief
Generally getting 6-9 months of some type of relief (mild/moderate OA)
Typically, start with CSI, then add on visco when needed

Viscosupplementation Several preparations
One injection
3 injections
5 injections
No clinical difference seen in any of them
Some are more biologically “clean”
Less inflammatory reactions

Case “But what can I do myself. I’m not that excited about
injections!”
Unloader knee braces:
Medial > lateral
Custom fit
Bulky to low-profile
Literature is +/- with utility of these braces
Will offer, for the willing patient, who may be adverse to
injections



Knee braces Brouwer et al, 2006
Multi-center RCT; medial knee OA
Showed small effects in improving pain scores
Kirkley et al 1999
RCT; medial knee OA
Significant benefit from using medial unloader

Knee braces
Anecdotally, seems to work minority of the time
Doesn’t fit well with the more obese leg
Insurance covered expense, but tends to still be
expensive for patient
As a general rule, we aren’t that excited about it, but we
don’t steer people away from it

“I heard supplements are good to take?!”
Glucosamine/chondroitin:
Studies are 50/50 on if it helps or not
Hard to know what to take from that
Glucosamine tends to be the more important ingredient
We consider risk/benefit with this
$$, allergies, mild increase in diabetic blood sugar
Not invasive, patient is “doing” something, placebo affect?
Definitely not something we tend to outright recommend, but if all else fails, tend to be OK with people trying it

Case “I still don’t want joint replacement. What about those
platelet injections, or stem cells?”
PRP or Stem cell injections:
Controversial
Studies are hit and miss regarding efficacy
Seems to be better for knee than hip
Orthobiologics May be helpful in mild/moderate knee osteoarthritis
Insurance not covering these injections
Offer it as an option but with caveats
Still under heavy research/scrutiny
Won’t hurt you, but not sure if it will help as much as you want
You are not “re-growing” cartilage
You still have osteoarthritis & we don’t know how to stop it from progressing

Surgery “I’m ready to get this problem fixed”
Total joint replacement
When patient is fed up with pain
Pros outweigh cons


















