
EMERGENCY EEG AND DIAGNOSTIC YIELD
3
Acta Clin Croat 2009; 48:283-285 Original Scientific Paper EMERGENCY EEG AND DIAGNOSTIC YIELD Hrvoje Hecimovic, Jelena Bosnjak, Snjeiana Miskov, Ruiica Covic-Negovetic and Vida Demarin Zagreb Epilepsy Center, University Department of Neurology, Reference Center for Neurovascular Disorders and Reference Center for Headache of the Ministry of Health and Social Welfare of Republic of Croatia, Sestre milosrdnice University Hospital, Zagreb, Croatia SUMMARY - The aim of the study was to determine whether an acute loss of consciousness, mental status change or related symptoms correlated with the presence of epileptiform abnormalities on urgent EEG. We analyzed 228 consecutive patients admitted to Emergency Room during the past 12 months and referred for urgent EEG evaluation. All patients had either a briefloss of consci- ousness or acute brain disorder, with a clinical diagnosis of epilepsy, syncope, head trauma, heada- che, transient ischemic attack (TIA) or vertigo. Statistical analysis was performed using Spearman's rho test for group comparison and multivariate regression analysis. The mean age of patients was 48±20 years. The frequency of referring clinical diagnoses was as follows: epilepsy 44.7% (1021228), TIA 15.8% (36/228), syncope 15.4% (35/228), headache 11% (25/228), vertigo 7.9% (18/228) and acute head trauma 5.3% (12/228). EEG indicated epileptiform abnormalities in 14.9%(34/228) and focal slowing in 9.2% (21/228) of patients. The majority ofthem (26%; 21/81) had a clinical diagno - sis of epilepsy. There was a significant correlation between clinical diagnosis of epilepsy and epilep- tiform EEG (Spearman's rho=O.13; P<O.04). Multivariate regression analysis showed that there was no predictive value in the clinical diagnosis of epilepsy and epileptiform EEG P=0.16). In conclusion, epilepsy was the most common clinical diagnosis in patients referred for urgent EEG. There was a significant correlation between the diagnosis and specific EEG abnormalities, however, the diagnosis of epilepsy failed to predict epileptiform activity on EEG. Study results suggested urgent EEG to have a high yield in patients with epilepsy. Key words: Seirures-: diagnosis; Seizures- etiology; Electroencephalography; Status epilepticus - diagnosis Introduction Diagnostic evaluation of patients with transient loss of consciousness, change in mental status or ab- normal motor activity often presents a challenge for the physician!". Differential diagnosis is complex and needs to be performed without delay. Electroen- cephalography (EEG) has a great value in diagnosing cerebral dysfunction, from seizure activity to EEG changes in infectious, encephalopathic and neuro- Correspondence to: Hrooje Heomooic, MD, PhD, Zagreb Epilep- sy Center, University Department of Neurology, Sestre milosrd- nice University Hospital, Vinogradska c. 29, HR-l0000 Zagreb, Croatia E-mail: Hecimovicei'inet.hr degenerative disorders'r':". EEG can be performed in emergency situations, as it is noninvasive and techni- cally simple for use. The aim of the present study was to test the hy- pothesis that the emergency room (ER) clinician can with high specificity diagnose seizure as being epilep- tic on the basis of the patient's clinical history. This means that EEG findings will be concordant with clinical diagnosis established at ER and predict 'posi- tive' EEG findings, i.e. EEG epileptic abnormality in this group. We evaluated patients admitted to ER with transient loss of consciousness, change in mental status or acute cerebral symptoms, such as epilepsy, syncope, head trauma, headache, transient ischemic attack (TIA) and vertigo. 283
Transcript of EMERGENCY EEG AND DIAGNOSTIC YIELD

Acta Clin Croat 2009; 48:283-285 Original Scientific Paper
EMERGENCY EEG AND DIAGNOSTIC YIELD
Hrvoje Hecimovic, Jelena Bosnjak, Snjeiana Miskov, Ruiica Covic-Negovetic and Vida Demarin
Zagreb Epilepsy Center, University Department of Neurology, Reference Center for Neurovascular Disorders and
Reference Center for Headache of the Ministry of Health and Social Welfare of Republic of Croatia,
Sestre milosrdnice University Hospital, Zagreb, Croatia
SUMMARY - The aim of the study was to determine whether an acute loss of consciousness,
mental status change or related symptoms correlated with the presence ofepileptiform abnormalitieson urgent EEG. We analyzed 228 consecutive patients admitted to Emergency Room during thepast 12 months and referred for urgent EEG evaluation. All patients had either a briefloss ofconsciousness or acute brain disorder, with a clinical diagnosis of epilepsy, syncope, head trauma, headache, transient ischemic attack (TIA) or vertigo. Statistical analysis was performed using Spearman'srho test for group comparison and multivariate regression analysis. The mean age of patients was48±20 years. The frequency of referring clinical diagnoses was as follows: epilepsy 44.7% (1021228),TIA 15.8% (36/228), syncope 15.4% (35/228), headache 11% (25/228), vertigo 7.9% (18/228) andacute head trauma 5.3% (12/228). EEG indicated epileptiform abnormalities in 14.9%(34/228) andfocal slowing in 9.2% (21/228) ofpatients. The majority ofthem (26%; 21/81) had a clinical diagnosis ofepilepsy. There was a significant correlation between clinical diagnosis of epilepsy and epileptiform EEG (Spearman's rho=O.13;P<O.04). Multivariate regression analysis showed that there wasno predictive value in the clinical diagnosis ofepilepsy and epileptiform EEG (~=1.483,P=0.16). Inconclusion, epilepsy was the most common clinical diagnosis in patients referred for urgent EEG.There was a significant correlation between the diagnosis and specific EEG abnormalities, however,the diagnosis of epilepsy failed to predict epileptiform activity on EEG. Study results suggestedurgent EEG to have a high yield in patients with epilepsy.
Key words: Seirures-:diagnosis; Seizures- etiology; Electroencephalography; Status epilepticus - diagnosis
Introduction
Diagnostic evaluation of patients with transient
loss of consciousness, change in mental status or abnormal motor activity often presents a challenge forthe physician!". Differential diagnosis is complexand needs to be performed without delay. Electroencephalography (EEG) has a great value in diagnosingcerebral dysfunction, from seizure activity to EEGchanges in infectious, encephalopathic and neuro-
Correspondence to: Hrooje Heomooic, MD, PhD, Zagreb Epilepsy Center, University Department of Neurology, Sestre milosrdnice University Hospital, Vinogradska c. 29, HR-l0000 Zagreb,Croatia
E-mail: Hecimovicei'inet.hr
degenerative disorders'r':". EEG can be performed in
emergency situations, as it is noninvasive and technically simple for use.
The aim of the present study was to test the hypothesis that the emergency room (ER) clinician canwith high specificity diagnose seizure as being epileptic on the basis of the patient's clinical history. Thismeans that EEG findings will be concordant withclinical diagnosis established at ER and predict 'posi
tive' EEG findings, i.e. EEG epileptic abnormalityin this group. We evaluated patients admitted to ERwith transient loss of consciousness, change in mentalstatus or acute cerebral symptoms, such as epilepsy,syncope, head trauma, headache, transient ischemicattack (TIA) and vertigo.
283
Hrvoje He Cimovic eta!
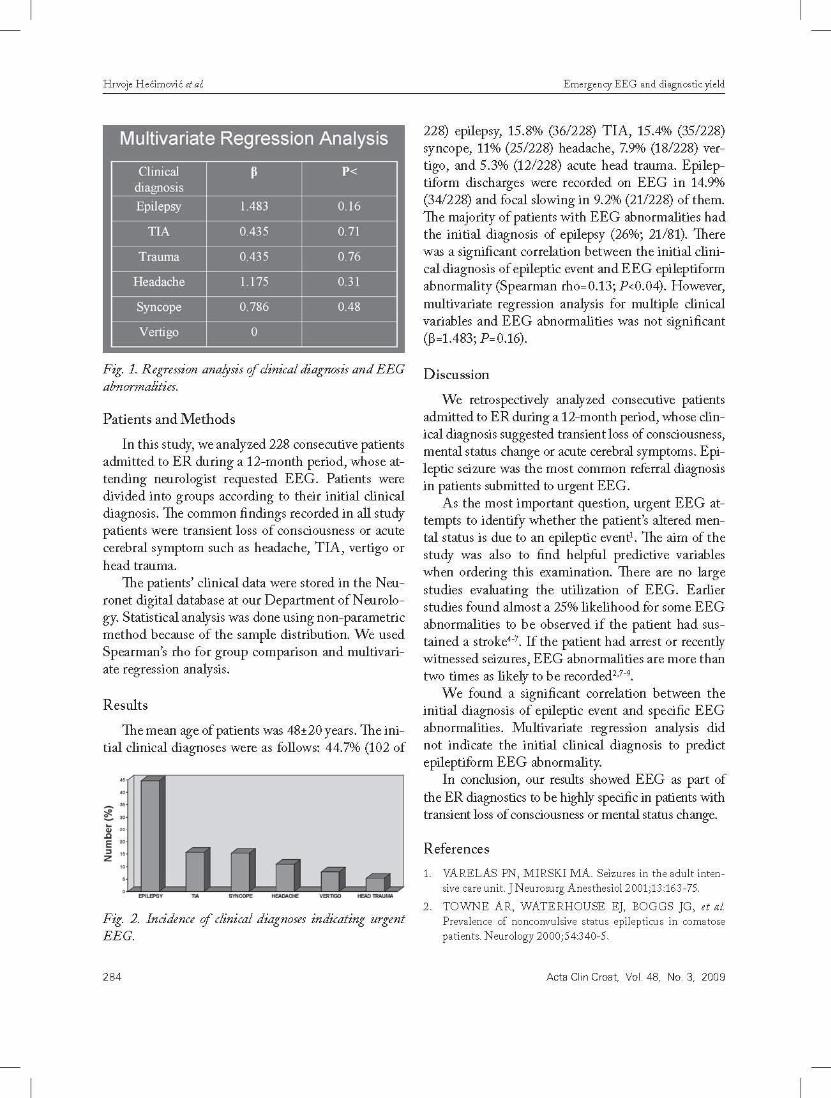
Multivariate Regression Analysis
Clinical ~ P<diagnosis
Epilepsy 1.483 0.16
TJA 0.435 0.71
Trauma 0.435 0.76
Headache ..,1 175 0.31
Syncope 0.786 0.48
Vertigo 0
Fig. 1. Regression analysis cfclinical diagnosis and EEGabnormalities.
Patients and Methods
In this study, we analyzed 228 consecutive patientsadmitted to ER during a 12-month period, whose attending neurologist requested EEG. Patients weredivided into groups according to their initial clinicaldiagnosis. The common findings recorded in all studypatients were transient loss of consciousness or acutecerebral symptom such as headache, TIA, vertigo orhead trauma.
The patients' clinical data were stored in the Neuronet digital database at our Department of Neurology. Statistical analysis was done using non-parametricmethod because of the sample distribution. We usedSpearman's rho for group comparison and multivariate regression analysis.
Results
The mean age of patients was 48±20 years. The initial clinical diagnoses were as follows: 44.7% (102 of
- "~ ..ZE ",z
"
-- --Fig. 2. Incidence cfclinical diagnoses indicating urgentEEG.
284
Emergency EE G and diagnosticyield
228) epilepsy, 15.8% (36/228) TIA, 15.4% (35/228)syncope, 11% (25/228) headache, 7.9% (18/228) vertigo, and 5.3% (12/228) acute head trauma. Epileptiform discharges were recorded on EEG in 14.9%(34/228) and focal slowing in 9.2% (21/228) of them.The majority of patients with EEG abnormalities hadthe initial diagnosis of epilepsy (26%; 21/81). Therewas a significant correlation between the initial clinical diagnosis of epileptic event and EEG epileptiformabnormality (Spearman rho-n.B; P<0.04). However,multivariate regression analysis for multiple clinicalvariables and EEG abnormalities was not significant(~o1.483; poO.16).
Discussion
We retrospectively analyzed consecutive patientsadmitted to ER during a 12-month period, whose clinical diagnosis suggested transient loss of consciousness,mental status change or acute cerebral symptoms. Epileptic seizure was the most common referral diagnosisin patients submitted to urgent EEG.
As the most important question, urgent EEG attempts to identify whether the patient's altered mental status is due to an epileptic event'. The aim of thestudy was also to find helpful predictive variableswhen ordering this examination. There are no largestudies evaluating the utilization of EEG. Earlierstudies found almost a 25% likelihood for some EEGabnormalities to be observed if the patient had sustained a stroke':". If the patient had arrest or recentlywitnessed seizures, EEG abnormalities are more thantwo times as likely to be recorded-?",
We found a significant correlation between theinitial diagnosis of epileptic event and specific EEGabnormalities. Multivariate regression analysis didnot indicate the initial clinical diagnosis to predictepileptiform EEG abnormality.
In conclusion, our results showed EEG as part ofthe ER diagnostics to be highly specific in patients withtransient loss of consciousness or mental status change.
References
1, VAR ELAS PN , MIRSKI MA, Seizures in the adul t inten
sive care unh] Neurosurg Anes thesioI2001;13:163-75,
2, TO 'WNE AR, WAT E RHOUS E E] , BOGGS ] G , et al.
Prevalence of nonconvulsive status epilepticus in comatosepatients, Neurology 2000;54:340-5,
Acta Clin Croat, Vol. 48, NO.3, 2009

Hrvoje Hedmovtc et al.
3. CLAASSEN], MAYER SA, KOWALSKI RG, et al. Detection ofelectrographic seizures with continuous EEG mon
itoring in critically ill patients. Neurology 2004;62:1743-8.
4. BLADIN CF, ALEXANDROV AV, BELLAVANCE A, etal. Seizures after stroke: a prospective multicenter study. Arch
Neuml2000:5H617-22.
5. BURN], DENNIS M, BAMFORD J. et al. Epileptic sei
zures after a first stroke: the Oxfordshire Community Stroke
Project. BM] 1997:315:1582-7.
6. KILPATRICK C], DAVIS SM, TRESS BM, et at. Epilepticseizures in acute stroke. Arch NeuroI1990;47:157-60.
Emergency EEG and diagnostic yield
7. ARBOIX A, COMES E, MASSONS], et al. Relevance ofearly seizures for in-hospital mortality in acute cerebrovascu
lar disease. Neurology 1996;47:1429-35.
8. REITH], ]ORGENSEN HS, NAKAYAMA H, et aI. Seizures in acute stroke: predictors and prognostic significance:
the Copenhagen Stroke Study. Stroke 1997;28:1585-9.
9. LABOVITZ DL, HAUSER WA, SACCO RL. Prevalence
and predictors of early seizure and status epilepticus after first
stroke. Neurology 2001;57:200-6.
Sazetak
HITNI EEG I DIJAGNOSTICKI DOPRINOS
H Hetirnoui/, j. Bosnjae, S. Miskov, R. Covii-Negovetiii V Demarin
Zeljeli smo utvrditi korelira li akutni gubitak svijesti, promjena psiholoSkog statusa iii s tim poveazni simptomi s prisutnoscu epileptiform nih nenormalnosti na hitnom EEG. Analizirali smo 228 susljednih bolesnika primljenih u Hitnusluzbu tijekom posljednjih 12 mjeseci, koji su upuceni na procjenu pomocu hitnog EEG. Svi bolesnici su imali kratakgubitak svijesti ili akutni mozdam poremecaj uz klmicku dijagnozu epilepsije, sinkope, traume glave, glavobolje, prolaznog ishemijskog napada (TIA) ili vrtoglavice. U statrsrckoj analizi rabio se Spearmanov rho test za usporedbu skupina imultivarijatna regresijska analiza. Srednja dob bolesnika bila je 48±20 godina. Ucestalost uputnih dijagnoza bila je kakoslijedi: 44,7% (102/228) epilepsija; 15,8% (36/228) TIA; 15,4% (35/228) sinkopa; 11% (25/228) glavobolja; 7,9% (18/228)vrtoglavica i 5,3% (121228) akutna trauma glave. EEG je otkrio epileptiformne nenormalnosti u 14,9% (341228) i zarrsnuusporenost u 9,2% (21/228) bolesnika. Vecina bolesnika (26%; 21/81) je imala klnncku dijagnozu epilepsije. Utvrdena jeznacajna korelacija izmedu kl inicke dijagnoze epilepsije i epileptiformnog EEG (Spearmanov rho 0,13; P=0,04). Multivanjatna regresijska analiza pokazala [e kako kl inicka dijagnoza epilepsije i epileptiformni EEG nemaju nikakve prediktivnevrijednosti (,+,=1,483; P=0,16). Zakljucrh smo kako je epilepsija najcesca klmicka dijagnoza u bolesnika upucenrh na hitniEEG. Zabiljeiena je znacajna korelacija izmedu dijagnoze i specificnrh nenormalnosti na EEG, medutim, dijagnozaepilepsije nije predvidjela epileptiformnu aktivnost na EEG. Nasi podaci ukazuju na to da hitni EEG ima visok rezultatu bolesnika s epilepsijom.
Kljucne rijeci: Epilepticni napadaji - diJagnostika;Epilepticni napadaji - etiologija;Elektroenceftlograjija; Status epilepticus- diJagnostika
Acta Clin Croat, Vol. 48, No.3, 2009 285


















